User login
A Cost-Effectiveness and Psychological Evaluation of Early Skin Biopsies vs Later-Onset Surgeries in Melanoma Management
Compared to later-onset procedures, early diagnosis of melanoma using affordable skin biopsies can result in better patient outcomes, lower health care expenditures, and enhanced psychological well-being.1 Numerous research and economic evaluations that highlight the possible advantages of early intervention in melanoma care lend support to this strategy. In health care systems, the cost of early identification and screening for skin cancer is a critical factor.1 There has been debate in the literature regarding performing more frequent biopsies earlier for skin cancers, which may greatly improve patient outcomes at the expense of increased financial cost, compared with performing fewer biopsies, which reduces costs at the potential expense of managing later-onset melanoma.1,2 We sought to summarize the current literature and address some considerations that may help bring more clarity to this topic.
According to a study of a large health care system, the average cost of a skin cancer screening visit was $150, of which $105 (70%) went toward the costs of the office visit and $45 (30%) went toward the costs of the biopsy.1 In the changing health care landscape, it is crucial to take into account the possible compounded savings from early diagnosis and treatment. While biopsies do involve some expenses, consideration of immunotherapy costs for advanced melanoma also should be considered, as they provide an alternative viewpoint on the financial effects of melanoma treatment.2 The use of new systemic treatments such as immunotherapy has led to a notable rise in Medicare users’ first-year melanoma treatment expenses. The average expense of treating stage IV melanoma rose from $47,739 in 2007 through 2012 to $117,450 in 2018 through 2019. This sharp rise highlights how much more expensive treating advanced melanoma is than performing biopsies for early detection and treatment. Hundreds of biopsies might be carried out for the cost of a single advanced melanoma therapy, possibly identifying several cases at an earlier, more manageable stage.2
Patient quality of life and survival rates also can be considerably improved by early melanoma detection through screening.3 Compared to patients with later-stage diagnoses, those with early-stage melanoma reported a higher overall quality of life. Better physical functioning and reduced levels of anxiety and sadness were linked to early identification using skin biopsies. Patients with more advanced melanoma who had later-onset procedures, on the other hand, experience worsening psychological symptoms and physical health.3
A cost-effectiveness analysis using a Markov cohort model compared the long-term economic impact of early detection and primary prevention of melanoma. It found that daily use of sunscreen could prevent a substantial number of new skin tumors and melanoma deaths and reduce health care costs when compared to early detection strategies such as performing extra biopsies.4 There already are programs across the United States that aim to educate the public on the importance of wearing sunscreen; this has, in turn, reduced the prevalence of skin cancer in certain communities. Primary prevention resulted in just 1364 new melanomas and more than $430 million in expenditures per 100,000 individuals, whereas early diagnosis produced 2446 new melanomas and more than $660 million in economic expenses per 100,000 individuals.4 It is imperative to acknowledge that skin biopsies remain a vital tool for the early identification of melanoma, particularly in high-risk groups.
By using technologies such as teledermoscopy, the cost-effectiveness of skin cancer referral and consultation can be further enhanced; for example, teledermoscopy for skin cancer referral and triage would result in faster clinical resolution at an average cost of $54.64 per case. This method may reduce the need for redundant in-person consultations and increase the effectiveness of melanoma identification.5
Large-scale public health initiatives in skin cancer prevention and early detection have the potential to be very effective, as evidenced by the War on Melanoma project at Oregon Health & Science University (Portland, Oregon). This all-encompassing strategy, which uses cutting-edge technologies, public education, and health care professional training, has improved melanoma outcomes and decreased health care expenditures with encouraging results.6
A few tactics can be used to best balance the costs of later-onset procedures and early skin biopsies. These include using advanced technologies such as teledermoscopy and dermoscopy, provider training to increase diagnostic accuracy, public health campaigns to raise awareness and promote prevention, and a comprehensive strategy combining targeted early detection strategies with primary prevention.5,6 Health care systems can optimize the financial efficiency and clinical results of melanoma treatment by putting these principles into practice.
Compared to later-onset melanoma procedures, early skin biopsies typically are more cost-effective, produce better patient outcomes, and offer psychological advantages, even if they may have a higher initial cost. Health care systems can optimize the trade-off between early detection and cost effectiveness in melanoma management by putting sophisticated technology to use, enhancing provider training, and implementing focused screening programs.5,6 To support evidence-based policies and guidelines, future research should assess the long-term economic impact of different melanoma prevention and detection measures.
- Matsumoto M, Secrest A, Anderson A, et al. Estimating the cost of skin cancer detection by dermatology providers in a large health care system. J Am Acad Dermatol. 2018;78:701-709.e1. doi:10.1016/j.jaad.2017.11.033
- Gogebakan KC, Mukherjee K, Berry EG, et al. Impact of novel systemic therapies on the first-year costs of care for melanoma among Medicare beneficiaries. Cancer. 2021;127:2926-2933. doi:10.1002/cncr.33515
- Young JN, Griffith-Bauer K, Hill E, et al. The benefit of early-stage diagnosis: a registry-based survey evaluating the quality of life in patients with melanoma. Skin Health Dis. 2023;3:E237. doi:10.1002/ski2.237
- Gordon L, Olsen C, Whiteman DC, et al. Prevention versus early detection for long-term control of melanoma and keratinocyte carcinomas: a cost-effectiveness modelling study. BMJ Open. 2020;10:E034388. doi:10.1136/bmjopen-2019-034388
- Buja A, Rivera M, Girardi G, et al. Cost-effectiveness of a melanoma screening programme using whole disease modelling. J Med Screen. 2020;27:157-167. doi:10.1177/0969141319885998
- Gogebakan KC, Berry EG, Geller AC, et al. Strategizing screening for melanoma in an era of novel treatments: a model-based approach. Cancer Epidemiol Biomarkers Prev. 2020;29:2599-2607. doi:10.1158/1055-9965.EPI-20-0881
Compared to later-onset procedures, early diagnosis of melanoma using affordable skin biopsies can result in better patient outcomes, lower health care expenditures, and enhanced psychological well-being.1 Numerous research and economic evaluations that highlight the possible advantages of early intervention in melanoma care lend support to this strategy. In health care systems, the cost of early identification and screening for skin cancer is a critical factor.1 There has been debate in the literature regarding performing more frequent biopsies earlier for skin cancers, which may greatly improve patient outcomes at the expense of increased financial cost, compared with performing fewer biopsies, which reduces costs at the potential expense of managing later-onset melanoma.1,2 We sought to summarize the current literature and address some considerations that may help bring more clarity to this topic.
According to a study of a large health care system, the average cost of a skin cancer screening visit was $150, of which $105 (70%) went toward the costs of the office visit and $45 (30%) went toward the costs of the biopsy.1 In the changing health care landscape, it is crucial to take into account the possible compounded savings from early diagnosis and treatment. While biopsies do involve some expenses, consideration of immunotherapy costs for advanced melanoma also should be considered, as they provide an alternative viewpoint on the financial effects of melanoma treatment.2 The use of new systemic treatments such as immunotherapy has led to a notable rise in Medicare users’ first-year melanoma treatment expenses. The average expense of treating stage IV melanoma rose from $47,739 in 2007 through 2012 to $117,450 in 2018 through 2019. This sharp rise highlights how much more expensive treating advanced melanoma is than performing biopsies for early detection and treatment. Hundreds of biopsies might be carried out for the cost of a single advanced melanoma therapy, possibly identifying several cases at an earlier, more manageable stage.2
Patient quality of life and survival rates also can be considerably improved by early melanoma detection through screening.3 Compared to patients with later-stage diagnoses, those with early-stage melanoma reported a higher overall quality of life. Better physical functioning and reduced levels of anxiety and sadness were linked to early identification using skin biopsies. Patients with more advanced melanoma who had later-onset procedures, on the other hand, experience worsening psychological symptoms and physical health.3
A cost-effectiveness analysis using a Markov cohort model compared the long-term economic impact of early detection and primary prevention of melanoma. It found that daily use of sunscreen could prevent a substantial number of new skin tumors and melanoma deaths and reduce health care costs when compared to early detection strategies such as performing extra biopsies.4 There already are programs across the United States that aim to educate the public on the importance of wearing sunscreen; this has, in turn, reduced the prevalence of skin cancer in certain communities. Primary prevention resulted in just 1364 new melanomas and more than $430 million in expenditures per 100,000 individuals, whereas early diagnosis produced 2446 new melanomas and more than $660 million in economic expenses per 100,000 individuals.4 It is imperative to acknowledge that skin biopsies remain a vital tool for the early identification of melanoma, particularly in high-risk groups.
By using technologies such as teledermoscopy, the cost-effectiveness of skin cancer referral and consultation can be further enhanced; for example, teledermoscopy for skin cancer referral and triage would result in faster clinical resolution at an average cost of $54.64 per case. This method may reduce the need for redundant in-person consultations and increase the effectiveness of melanoma identification.5
Large-scale public health initiatives in skin cancer prevention and early detection have the potential to be very effective, as evidenced by the War on Melanoma project at Oregon Health & Science University (Portland, Oregon). This all-encompassing strategy, which uses cutting-edge technologies, public education, and health care professional training, has improved melanoma outcomes and decreased health care expenditures with encouraging results.6
A few tactics can be used to best balance the costs of later-onset procedures and early skin biopsies. These include using advanced technologies such as teledermoscopy and dermoscopy, provider training to increase diagnostic accuracy, public health campaigns to raise awareness and promote prevention, and a comprehensive strategy combining targeted early detection strategies with primary prevention.5,6 Health care systems can optimize the financial efficiency and clinical results of melanoma treatment by putting these principles into practice.
Compared to later-onset melanoma procedures, early skin biopsies typically are more cost-effective, produce better patient outcomes, and offer psychological advantages, even if they may have a higher initial cost. Health care systems can optimize the trade-off between early detection and cost effectiveness in melanoma management by putting sophisticated technology to use, enhancing provider training, and implementing focused screening programs.5,6 To support evidence-based policies and guidelines, future research should assess the long-term economic impact of different melanoma prevention and detection measures.
Compared to later-onset procedures, early diagnosis of melanoma using affordable skin biopsies can result in better patient outcomes, lower health care expenditures, and enhanced psychological well-being.1 Numerous research and economic evaluations that highlight the possible advantages of early intervention in melanoma care lend support to this strategy. In health care systems, the cost of early identification and screening for skin cancer is a critical factor.1 There has been debate in the literature regarding performing more frequent biopsies earlier for skin cancers, which may greatly improve patient outcomes at the expense of increased financial cost, compared with performing fewer biopsies, which reduces costs at the potential expense of managing later-onset melanoma.1,2 We sought to summarize the current literature and address some considerations that may help bring more clarity to this topic.
According to a study of a large health care system, the average cost of a skin cancer screening visit was $150, of which $105 (70%) went toward the costs of the office visit and $45 (30%) went toward the costs of the biopsy.1 In the changing health care landscape, it is crucial to take into account the possible compounded savings from early diagnosis and treatment. While biopsies do involve some expenses, consideration of immunotherapy costs for advanced melanoma also should be considered, as they provide an alternative viewpoint on the financial effects of melanoma treatment.2 The use of new systemic treatments such as immunotherapy has led to a notable rise in Medicare users’ first-year melanoma treatment expenses. The average expense of treating stage IV melanoma rose from $47,739 in 2007 through 2012 to $117,450 in 2018 through 2019. This sharp rise highlights how much more expensive treating advanced melanoma is than performing biopsies for early detection and treatment. Hundreds of biopsies might be carried out for the cost of a single advanced melanoma therapy, possibly identifying several cases at an earlier, more manageable stage.2
Patient quality of life and survival rates also can be considerably improved by early melanoma detection through screening.3 Compared to patients with later-stage diagnoses, those with early-stage melanoma reported a higher overall quality of life. Better physical functioning and reduced levels of anxiety and sadness were linked to early identification using skin biopsies. Patients with more advanced melanoma who had later-onset procedures, on the other hand, experience worsening psychological symptoms and physical health.3
A cost-effectiveness analysis using a Markov cohort model compared the long-term economic impact of early detection and primary prevention of melanoma. It found that daily use of sunscreen could prevent a substantial number of new skin tumors and melanoma deaths and reduce health care costs when compared to early detection strategies such as performing extra biopsies.4 There already are programs across the United States that aim to educate the public on the importance of wearing sunscreen; this has, in turn, reduced the prevalence of skin cancer in certain communities. Primary prevention resulted in just 1364 new melanomas and more than $430 million in expenditures per 100,000 individuals, whereas early diagnosis produced 2446 new melanomas and more than $660 million in economic expenses per 100,000 individuals.4 It is imperative to acknowledge that skin biopsies remain a vital tool for the early identification of melanoma, particularly in high-risk groups.
By using technologies such as teledermoscopy, the cost-effectiveness of skin cancer referral and consultation can be further enhanced; for example, teledermoscopy for skin cancer referral and triage would result in faster clinical resolution at an average cost of $54.64 per case. This method may reduce the need for redundant in-person consultations and increase the effectiveness of melanoma identification.5
Large-scale public health initiatives in skin cancer prevention and early detection have the potential to be very effective, as evidenced by the War on Melanoma project at Oregon Health & Science University (Portland, Oregon). This all-encompassing strategy, which uses cutting-edge technologies, public education, and health care professional training, has improved melanoma outcomes and decreased health care expenditures with encouraging results.6
A few tactics can be used to best balance the costs of later-onset procedures and early skin biopsies. These include using advanced technologies such as teledermoscopy and dermoscopy, provider training to increase diagnostic accuracy, public health campaigns to raise awareness and promote prevention, and a comprehensive strategy combining targeted early detection strategies with primary prevention.5,6 Health care systems can optimize the financial efficiency and clinical results of melanoma treatment by putting these principles into practice.
Compared to later-onset melanoma procedures, early skin biopsies typically are more cost-effective, produce better patient outcomes, and offer psychological advantages, even if they may have a higher initial cost. Health care systems can optimize the trade-off between early detection and cost effectiveness in melanoma management by putting sophisticated technology to use, enhancing provider training, and implementing focused screening programs.5,6 To support evidence-based policies and guidelines, future research should assess the long-term economic impact of different melanoma prevention and detection measures.
- Matsumoto M, Secrest A, Anderson A, et al. Estimating the cost of skin cancer detection by dermatology providers in a large health care system. J Am Acad Dermatol. 2018;78:701-709.e1. doi:10.1016/j.jaad.2017.11.033
- Gogebakan KC, Mukherjee K, Berry EG, et al. Impact of novel systemic therapies on the first-year costs of care for melanoma among Medicare beneficiaries. Cancer. 2021;127:2926-2933. doi:10.1002/cncr.33515
- Young JN, Griffith-Bauer K, Hill E, et al. The benefit of early-stage diagnosis: a registry-based survey evaluating the quality of life in patients with melanoma. Skin Health Dis. 2023;3:E237. doi:10.1002/ski2.237
- Gordon L, Olsen C, Whiteman DC, et al. Prevention versus early detection for long-term control of melanoma and keratinocyte carcinomas: a cost-effectiveness modelling study. BMJ Open. 2020;10:E034388. doi:10.1136/bmjopen-2019-034388
- Buja A, Rivera M, Girardi G, et al. Cost-effectiveness of a melanoma screening programme using whole disease modelling. J Med Screen. 2020;27:157-167. doi:10.1177/0969141319885998
- Gogebakan KC, Berry EG, Geller AC, et al. Strategizing screening for melanoma in an era of novel treatments: a model-based approach. Cancer Epidemiol Biomarkers Prev. 2020;29:2599-2607. doi:10.1158/1055-9965.EPI-20-0881
- Matsumoto M, Secrest A, Anderson A, et al. Estimating the cost of skin cancer detection by dermatology providers in a large health care system. J Am Acad Dermatol. 2018;78:701-709.e1. doi:10.1016/j.jaad.2017.11.033
- Gogebakan KC, Mukherjee K, Berry EG, et al. Impact of novel systemic therapies on the first-year costs of care for melanoma among Medicare beneficiaries. Cancer. 2021;127:2926-2933. doi:10.1002/cncr.33515
- Young JN, Griffith-Bauer K, Hill E, et al. The benefit of early-stage diagnosis: a registry-based survey evaluating the quality of life in patients with melanoma. Skin Health Dis. 2023;3:E237. doi:10.1002/ski2.237
- Gordon L, Olsen C, Whiteman DC, et al. Prevention versus early detection for long-term control of melanoma and keratinocyte carcinomas: a cost-effectiveness modelling study. BMJ Open. 2020;10:E034388. doi:10.1136/bmjopen-2019-034388
- Buja A, Rivera M, Girardi G, et al. Cost-effectiveness of a melanoma screening programme using whole disease modelling. J Med Screen. 2020;27:157-167. doi:10.1177/0969141319885998
- Gogebakan KC, Berry EG, Geller AC, et al. Strategizing screening for melanoma in an era of novel treatments: a model-based approach. Cancer Epidemiol Biomarkers Prev. 2020;29:2599-2607. doi:10.1158/1055-9965.EPI-20-0881
Practice Points
- Early melanoma detection via skin biopsy is generally more cost-effective than managing advanced-stage disease, largely due to the high costs associated with systemic therapies (eg, immunotherapy) used in later-stage melanoma.
- Earlier diagnosis is associated with improved patient outcomes, including better quality of life and reduced psychological distress, compared with later-stage melanoma diagnoses requiring more extensive intervention.
- Integrated prevention and early detection strategies—such as dermoscopy, teledermoscopy, and public health initiatives—may optimize melanoma outcomes while reducing overall health care expenditures.
Training Lifeguards to Assist in Skin Cancer Prevention
Training Lifeguards to Assist in Skin Cancer Prevention
Lifeguards play a crucial role in ensuring water safety, but they also are uniquely positioned to promote skin cancer prevention and proper sunscreen use.1,2 There are several benefits and challenges to offering skin cancer prevention training for lifeguards.3 We examine the advantages of training, highlight the role lifeguards can play in larger public skin cancer prevention efforts, and address practical techniques for developing lifeguardfocused skin cancer education programs. By providing this knowledge to lifeguards, we can improve community health outcomes and encourage sun-safe behaviors in high-risk outdoor locations.
Benefits of Skin Cancer Prevention Training for Lifeguards
Research has shown that lifeguards are at an elevated risk for basal cell carcinoma, squamous cell carcinoma, and melanoma due to frequent prolonged occupational sun exposure.1,2,4-6 Therefore, comprehensive education on skin cancer prevention—including instruction on proper sunscreen application techniques and the importance of regular reapplication as well as how to recognize suspicious skin lesions—should be incorporated into lifeguard certification programs. One study evaluating the effectiveness of a skin cancer prevention program for lifeguards found that many of the participants lacked a thorough understanding of the different types of skin cancer.5 Another study found that lifeguards at pools in areas where societal norms supporting sun safety are stronger exhibited noticeably more sun protection practices, with regression estimates of 0.22 (95% CI, 0.17-0.26).7 Empowering lifeguards with valuable health knowledge during their regular training could potentially reduce their risk for skin cancer,4 as they may be more inclined to use sunscreen appropriately and reach out to a dermatologist for regular skin checks and evaluation of suspicious lesions.
Role of Lifeguards in Public Skin Cancer Prevention Efforts
Once trained on skin cancer prevention, lifeguards also can play a pivotal role in promoting sunscreen use among the public. Despite the widespread availability of high-quality sunscreens, many swimmers and beachgoers neglect to regularly apply or reapply sunscreen, especially on commonly exposed areas such as the back, shoulders, and face.8 Educating lifeguards on skin cancer prevention could enhance health outcomes by increasing early detection rates and promoting sun-safe behaviors among the general public.9 However, additional training requirements might increase the cost and time commitment for lifeguard certification, potentially leading to staffing shortages.3,7 There also is a risk of lifeguards overstepping their role and providing inaccurate medical advice, which could cause distress or even lead to liability issues.7 Balancing these factors will be crucial in developing effective and sustainable skin cancer prevention programs for lifeguards.
Implementing Lifeguard Skin Cancer Training
Implementing skin cancer prevention training programs for lifeguards requires strategic collaboration between dermatologists, and lifeguard training organizations to ensure that the participants receive consistent and comprehensive training.10 Additionally, public health campaigns can support these efforts by raising awareness about the importance of sun safety and regular skin checks.6 Tailored training modules/materials, ongoing technical assistance, and active, multicomponent approaches that account for both individual and environmental factors can increase program implementation in a variety of community settings.
Final Thoughts
Through effective education, lifeguards can potentially have a substantial impact on skin cancer prevention, both among lifeguards themselves and the general public. By promoting proper sunscreen use, lifeguards can help reduce the incidence and mortality associated with skin cancers. Future studies should focus on developing and implementing targeted education initiatives for lifeguards, fostering collaboration between relevant stakeholders, and raising public awareness about the importance of sun safety and early skin cancer detection. These efforts ultimately could lead to improved public health outcomes and reduced skin cancer rates, particularly in high-risk populations that frequently are exposed to UV radiation.
- Enos CW, Rey S, Slocum J, et al. Sun-protection behaviors among active members of the United States Lifesaving Association. J Clin Aesthet Dermatol. 2021;14:14-20.
- Verma K, Lewis DJ, Siddiqui FS, et al. Mohs micrographic surgery management of melanoma and melanoma in situ. StatPearls. Updated August 28, 2024. Accessed April 15, 2025. https://www.ncbi.nlm.nih.gov/books/NBK606123/
- Verma KK, Joshi TP, Lewis DJ, et al. Nail technicians as partners in early melanoma detection: bridging the knowledge gap. Arch Dermatol Res. 2024;316:586. doi:10.1007/s00403-024-03342-0
- Geller AC, Glanz K, Shigaki D, et al. Impact of skin cancer prevention on outdoor aquatics staff: the Pool Cool program in Hawaii and Massachusetts. Prev Med. 2001;33:155-161. doi:10.1006/pmed.2001.0870
- Hiemstra M, Glanz K, Nehl E. Changes in sunburn and tanning attitudes among lifeguards over a summer season. J Am Acad Dermatol. 2012;66:430-437. doi:10.1016/j.jaad.2010.11.050
- Verma KK, Ahmad N, Friedmann DP, et al. Melanoma in tattooed skin: diagnostic challenges and the potential for tattoo artists in early detection. Arch Dermatol Res. 2024;316:690. doi:10.1007/s00403-024-03415-0
- Hall DM, McCarty F, Elliott T, et al. Lifeguards’ sun protection habits and sunburns: association with sun-safe environments and skin cancer prevention program participation. Arch Dermatol. 2009;145:139-144. doi:10.1001/archdermatol.2008.553
- Emmons KM, Geller AC, Puleo E, et al. Skin cancer education and early detection at the beach: a randomized trial of dermatologist examination and biometric feedback. J Am Acad Dermatol. 2011;64:282-289. doi:10.1016/j.jaad.2010.01.040
- Rabin BA, Nehl E, Elliott T, et al. Individual and setting level predictors of the implementation of a skin cancer prevention program: a multilevel analysis. Implement Sci. 2010;5:40. doi:10.1186/1748-5908-5-40
- Walkosz BJ, Buller D, Buller M, et al. Sun safe workplaces: effect of an occupational skin cancer prevention program on employee sun safety practices. J Occup Environ Med. 2018;60:900-997. doi:10.1097 /JOM.0000000000001427
Lifeguards play a crucial role in ensuring water safety, but they also are uniquely positioned to promote skin cancer prevention and proper sunscreen use.1,2 There are several benefits and challenges to offering skin cancer prevention training for lifeguards.3 We examine the advantages of training, highlight the role lifeguards can play in larger public skin cancer prevention efforts, and address practical techniques for developing lifeguardfocused skin cancer education programs. By providing this knowledge to lifeguards, we can improve community health outcomes and encourage sun-safe behaviors in high-risk outdoor locations.
Benefits of Skin Cancer Prevention Training for Lifeguards
Research has shown that lifeguards are at an elevated risk for basal cell carcinoma, squamous cell carcinoma, and melanoma due to frequent prolonged occupational sun exposure.1,2,4-6 Therefore, comprehensive education on skin cancer prevention—including instruction on proper sunscreen application techniques and the importance of regular reapplication as well as how to recognize suspicious skin lesions—should be incorporated into lifeguard certification programs. One study evaluating the effectiveness of a skin cancer prevention program for lifeguards found that many of the participants lacked a thorough understanding of the different types of skin cancer.5 Another study found that lifeguards at pools in areas where societal norms supporting sun safety are stronger exhibited noticeably more sun protection practices, with regression estimates of 0.22 (95% CI, 0.17-0.26).7 Empowering lifeguards with valuable health knowledge during their regular training could potentially reduce their risk for skin cancer,4 as they may be more inclined to use sunscreen appropriately and reach out to a dermatologist for regular skin checks and evaluation of suspicious lesions.
Role of Lifeguards in Public Skin Cancer Prevention Efforts
Once trained on skin cancer prevention, lifeguards also can play a pivotal role in promoting sunscreen use among the public. Despite the widespread availability of high-quality sunscreens, many swimmers and beachgoers neglect to regularly apply or reapply sunscreen, especially on commonly exposed areas such as the back, shoulders, and face.8 Educating lifeguards on skin cancer prevention could enhance health outcomes by increasing early detection rates and promoting sun-safe behaviors among the general public.9 However, additional training requirements might increase the cost and time commitment for lifeguard certification, potentially leading to staffing shortages.3,7 There also is a risk of lifeguards overstepping their role and providing inaccurate medical advice, which could cause distress or even lead to liability issues.7 Balancing these factors will be crucial in developing effective and sustainable skin cancer prevention programs for lifeguards.
Implementing Lifeguard Skin Cancer Training
Implementing skin cancer prevention training programs for lifeguards requires strategic collaboration between dermatologists, and lifeguard training organizations to ensure that the participants receive consistent and comprehensive training.10 Additionally, public health campaigns can support these efforts by raising awareness about the importance of sun safety and regular skin checks.6 Tailored training modules/materials, ongoing technical assistance, and active, multicomponent approaches that account for both individual and environmental factors can increase program implementation in a variety of community settings.
Final Thoughts
Through effective education, lifeguards can potentially have a substantial impact on skin cancer prevention, both among lifeguards themselves and the general public. By promoting proper sunscreen use, lifeguards can help reduce the incidence and mortality associated with skin cancers. Future studies should focus on developing and implementing targeted education initiatives for lifeguards, fostering collaboration between relevant stakeholders, and raising public awareness about the importance of sun safety and early skin cancer detection. These efforts ultimately could lead to improved public health outcomes and reduced skin cancer rates, particularly in high-risk populations that frequently are exposed to UV radiation.
Lifeguards play a crucial role in ensuring water safety, but they also are uniquely positioned to promote skin cancer prevention and proper sunscreen use.1,2 There are several benefits and challenges to offering skin cancer prevention training for lifeguards.3 We examine the advantages of training, highlight the role lifeguards can play in larger public skin cancer prevention efforts, and address practical techniques for developing lifeguardfocused skin cancer education programs. By providing this knowledge to lifeguards, we can improve community health outcomes and encourage sun-safe behaviors in high-risk outdoor locations.
Benefits of Skin Cancer Prevention Training for Lifeguards
Research has shown that lifeguards are at an elevated risk for basal cell carcinoma, squamous cell carcinoma, and melanoma due to frequent prolonged occupational sun exposure.1,2,4-6 Therefore, comprehensive education on skin cancer prevention—including instruction on proper sunscreen application techniques and the importance of regular reapplication as well as how to recognize suspicious skin lesions—should be incorporated into lifeguard certification programs. One study evaluating the effectiveness of a skin cancer prevention program for lifeguards found that many of the participants lacked a thorough understanding of the different types of skin cancer.5 Another study found that lifeguards at pools in areas where societal norms supporting sun safety are stronger exhibited noticeably more sun protection practices, with regression estimates of 0.22 (95% CI, 0.17-0.26).7 Empowering lifeguards with valuable health knowledge during their regular training could potentially reduce their risk for skin cancer,4 as they may be more inclined to use sunscreen appropriately and reach out to a dermatologist for regular skin checks and evaluation of suspicious lesions.
Role of Lifeguards in Public Skin Cancer Prevention Efforts
Once trained on skin cancer prevention, lifeguards also can play a pivotal role in promoting sunscreen use among the public. Despite the widespread availability of high-quality sunscreens, many swimmers and beachgoers neglect to regularly apply or reapply sunscreen, especially on commonly exposed areas such as the back, shoulders, and face.8 Educating lifeguards on skin cancer prevention could enhance health outcomes by increasing early detection rates and promoting sun-safe behaviors among the general public.9 However, additional training requirements might increase the cost and time commitment for lifeguard certification, potentially leading to staffing shortages.3,7 There also is a risk of lifeguards overstepping their role and providing inaccurate medical advice, which could cause distress or even lead to liability issues.7 Balancing these factors will be crucial in developing effective and sustainable skin cancer prevention programs for lifeguards.
Implementing Lifeguard Skin Cancer Training
Implementing skin cancer prevention training programs for lifeguards requires strategic collaboration between dermatologists, and lifeguard training organizations to ensure that the participants receive consistent and comprehensive training.10 Additionally, public health campaigns can support these efforts by raising awareness about the importance of sun safety and regular skin checks.6 Tailored training modules/materials, ongoing technical assistance, and active, multicomponent approaches that account for both individual and environmental factors can increase program implementation in a variety of community settings.
Final Thoughts
Through effective education, lifeguards can potentially have a substantial impact on skin cancer prevention, both among lifeguards themselves and the general public. By promoting proper sunscreen use, lifeguards can help reduce the incidence and mortality associated with skin cancers. Future studies should focus on developing and implementing targeted education initiatives for lifeguards, fostering collaboration between relevant stakeholders, and raising public awareness about the importance of sun safety and early skin cancer detection. These efforts ultimately could lead to improved public health outcomes and reduced skin cancer rates, particularly in high-risk populations that frequently are exposed to UV radiation.
- Enos CW, Rey S, Slocum J, et al. Sun-protection behaviors among active members of the United States Lifesaving Association. J Clin Aesthet Dermatol. 2021;14:14-20.
- Verma K, Lewis DJ, Siddiqui FS, et al. Mohs micrographic surgery management of melanoma and melanoma in situ. StatPearls. Updated August 28, 2024. Accessed April 15, 2025. https://www.ncbi.nlm.nih.gov/books/NBK606123/
- Verma KK, Joshi TP, Lewis DJ, et al. Nail technicians as partners in early melanoma detection: bridging the knowledge gap. Arch Dermatol Res. 2024;316:586. doi:10.1007/s00403-024-03342-0
- Geller AC, Glanz K, Shigaki D, et al. Impact of skin cancer prevention on outdoor aquatics staff: the Pool Cool program in Hawaii and Massachusetts. Prev Med. 2001;33:155-161. doi:10.1006/pmed.2001.0870
- Hiemstra M, Glanz K, Nehl E. Changes in sunburn and tanning attitudes among lifeguards over a summer season. J Am Acad Dermatol. 2012;66:430-437. doi:10.1016/j.jaad.2010.11.050
- Verma KK, Ahmad N, Friedmann DP, et al. Melanoma in tattooed skin: diagnostic challenges and the potential for tattoo artists in early detection. Arch Dermatol Res. 2024;316:690. doi:10.1007/s00403-024-03415-0
- Hall DM, McCarty F, Elliott T, et al. Lifeguards’ sun protection habits and sunburns: association with sun-safe environments and skin cancer prevention program participation. Arch Dermatol. 2009;145:139-144. doi:10.1001/archdermatol.2008.553
- Emmons KM, Geller AC, Puleo E, et al. Skin cancer education and early detection at the beach: a randomized trial of dermatologist examination and biometric feedback. J Am Acad Dermatol. 2011;64:282-289. doi:10.1016/j.jaad.2010.01.040
- Rabin BA, Nehl E, Elliott T, et al. Individual and setting level predictors of the implementation of a skin cancer prevention program: a multilevel analysis. Implement Sci. 2010;5:40. doi:10.1186/1748-5908-5-40
- Walkosz BJ, Buller D, Buller M, et al. Sun safe workplaces: effect of an occupational skin cancer prevention program on employee sun safety practices. J Occup Environ Med. 2018;60:900-997. doi:10.1097 /JOM.0000000000001427
- Enos CW, Rey S, Slocum J, et al. Sun-protection behaviors among active members of the United States Lifesaving Association. J Clin Aesthet Dermatol. 2021;14:14-20.
- Verma K, Lewis DJ, Siddiqui FS, et al. Mohs micrographic surgery management of melanoma and melanoma in situ. StatPearls. Updated August 28, 2024. Accessed April 15, 2025. https://www.ncbi.nlm.nih.gov/books/NBK606123/
- Verma KK, Joshi TP, Lewis DJ, et al. Nail technicians as partners in early melanoma detection: bridging the knowledge gap. Arch Dermatol Res. 2024;316:586. doi:10.1007/s00403-024-03342-0
- Geller AC, Glanz K, Shigaki D, et al. Impact of skin cancer prevention on outdoor aquatics staff: the Pool Cool program in Hawaii and Massachusetts. Prev Med. 2001;33:155-161. doi:10.1006/pmed.2001.0870
- Hiemstra M, Glanz K, Nehl E. Changes in sunburn and tanning attitudes among lifeguards over a summer season. J Am Acad Dermatol. 2012;66:430-437. doi:10.1016/j.jaad.2010.11.050
- Verma KK, Ahmad N, Friedmann DP, et al. Melanoma in tattooed skin: diagnostic challenges and the potential for tattoo artists in early detection. Arch Dermatol Res. 2024;316:690. doi:10.1007/s00403-024-03415-0
- Hall DM, McCarty F, Elliott T, et al. Lifeguards’ sun protection habits and sunburns: association with sun-safe environments and skin cancer prevention program participation. Arch Dermatol. 2009;145:139-144. doi:10.1001/archdermatol.2008.553
- Emmons KM, Geller AC, Puleo E, et al. Skin cancer education and early detection at the beach: a randomized trial of dermatologist examination and biometric feedback. J Am Acad Dermatol. 2011;64:282-289. doi:10.1016/j.jaad.2010.01.040
- Rabin BA, Nehl E, Elliott T, et al. Individual and setting level predictors of the implementation of a skin cancer prevention program: a multilevel analysis. Implement Sci. 2010;5:40. doi:10.1186/1748-5908-5-40
- Walkosz BJ, Buller D, Buller M, et al. Sun safe workplaces: effect of an occupational skin cancer prevention program on employee sun safety practices. J Occup Environ Med. 2018;60:900-997. doi:10.1097 /JOM.0000000000001427
Training Lifeguards to Assist in Skin Cancer Prevention
Training Lifeguards to Assist in Skin Cancer Prevention

Leukocytoclastic Vasculitis Resolution With Topical Dapsone
Leukocytoclastic vasculitis (LCV) is a disease characterized by inflammation of small vessels with characteristic clinical findings of petechiae and palpable purpura.1 Numerous etiologies have been described, but the disease commonly remains idiopathic.2,3 Leukocytoclastic vasculitis often spontaneously resolves within weeks and requires only symptomatic treatment. Chronic or severe disease can require systemic medical treatment with agents such as colchicine, dapsone, and corticosteroids. These agents are effective but carry risks of serious side effects.4,5 These side effects and/or medical contraindications prevent some patients from taking systemic medications for LCV. We present a case of LCV that resolved after treatment with topical dapsone, highlighting a potential new treatment ofLCV with a markedly better side-effect profile.
Case Report
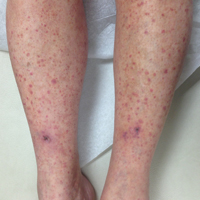
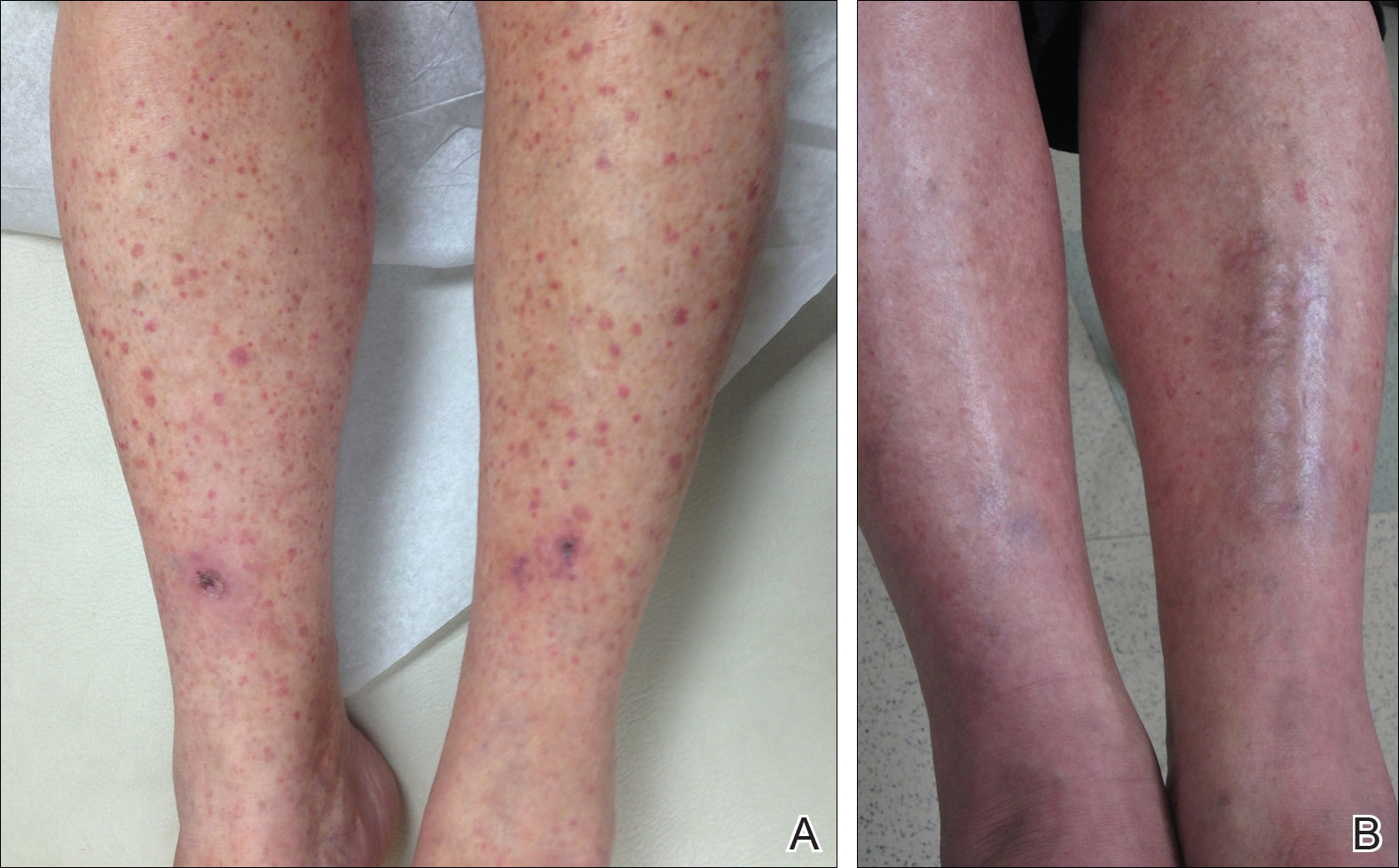
A 60-year-old woman with recent upper respiratory tract and sinus infections presented to our dermatology clinic with painful palpable purpura on the bilateral shins, thighs, and dorsal aspects of the feet of several months’ duration (Figure, A). Her primary care provider initiated treatment with amoxicillin and doxycycline for the infections. When the rash developed approximately 1.5 weeks following initiation of her symptoms, the patient was referred to the dermatology and rheumatology departments at our institution. The treating dermatologist (M.B.T.) obtained a 4-mm punch biopsy from the right lower leg and LCV was shown on histology. The patient completed a 14-day course of doxycycline and amoxicillin without resolution of the eruption. After an extensive investigation, the treating rheumatologist concluded that the LCV was idiopathic or secondary to an infection or drug exposure. The rheumatologist started the patient on oral prednisone for the chronic symptomatic LCV, but she was intolerant of this medication and discontinued it after 1 week. Our dermatology clinic started her on triamcinolone cream 0.1% twice daily, but she continued to experience new and worsening lesions. At her follow-up appointment 1 month later, triamcinolone cream was discontinued and dapsone gel 5% twice daily was started. She experienced resolution of her previously recalcitrant LCV within 3 weeks (Figure, B).
Comment
Established therapies for LCV carry serious side-effect profiles, which can preclude their use.5 Therefore, a topical therapeutic alternative for LCV would be ideal. Systemic prednisone is the first-line therapy for chronic and/or symptomatic LCV, but its side effects include suppression of the hypothalamic-pituitary-adrenal axis, immunosuppression, osteonecrosis, and glucose intolerance.5 Colchicine therapy carries risks for blood dyscrasia, immunosuppression, and gastrointestinal tract upset. Systemic dapsone also is an effective therapy for chronic and/or symptomatic LCV.5,6 However, systemic dapsone requires glucose-6-phosphate dehydrogenase deficiency screening and routine monitoring of blood counts, and it also carries the risk for serious adverse effects including neuropathy, blood dyscrasia, and hypersensitivity syndrome.5,6 Topical dapsone may provide similar efficacy with far fewer adverse effects and has proven to be a safe treatment of acne, even when used in patients with glucose-6-phosphate dehydrogenase deficiency. It displays low systemic absorption and does not accumulate over time once a steady state is reached.7 It also has been shown to be beneficial in other vasculopathies such as erythema elevatum diutinum and in other neutrophilic inflammatory disorders such as pyoderma gangrenosum.8,9 A case of methemoglobinemia due to topical dapsone has been reported.10 Although this effect is rare, clinicians should be aware of such adverse effects when using medications for off-label purposes.
Leukocytoclastic vasculitis can spontaneously resolve; however, our patient’s disease was chronic for several months, and she continued to develop new lesions without signs of resolution. After initiating topical dapsone, she experienced resolution within 3 weeks.
Conclusion
Topical dapsone is a novel approach for treating LCV. Given this drug’s favorable side-effect profile compared to the currently available therapeutic alternatives, we believe it is a reasonable option in select patients. Further investigation is needed to prove its efficacy, but it could be an ideal alternative for patients with contraindications to traditional therapies and/or for those unable to tolerate systemic therapy.
- Koutkia P, Mylonakis E, Rounds S, et al. Leucocytoclastic vasculitis: an update for the clinician. Scand J Rheumatol. 2001;30:315-322.
- Af Ekenstam E, Callen JP. Cutaneous leukocytoclastic vasculitis. clinical and laboratory features of 82 patients seen in private practice. Arch Dermatol. 1984;120:484-489.
- Gyselbrecht L, de Keyser F, Ongenae K, et al. Etiological factors and underlying conditions in patientswith leucocytoclastic vasculitis. Clin Exp Rheumatol. 1996;14:665-668.
- Sais G, Vidaller A, Jucglà A, et al. Colchicine in the treatment of cutaneous leukocytoclastic vasculitis. results of a prospective, randomized controlled trial. Arch Dermatol. 1995;131:1399-1402.
- Sunderkotter C, Bonsmann G, Sindrilaru A, et al. Management of leukocytoclastic vasculitis: clinical review. J Dermatol Treat. 2005;16:193-206.
- Zhu YI, Stiller MJ. Dapsone and sulfones in dermatology: overview and update. J Am Acad Dermatol. 2001;45:420-434.
- Stotland M, Shalita AR, Kissling RF. Dapsone 5% gel: a review of its efficacy and safety in the treatment of acne vulgaris. Am J Clin Dermatol. 2009;10:221-227.
- Frieling GW, Williams NL, Lim SJ, et al. Novel use of topical dapsone 5% gel for erythema elevatum diutinum: safer and effective. J Drugs Dermatol. 2013;12:481-484.
- Handler MZ, Hamilton H, Aires D. Treatment of peristomal pyoderma gangrenosum with topical crushed dapsone. J Drugs Dermatol. 2011;10:1059-1061.
- Swartzentruber GS, Yanta JH, Pizon AF. Methemoglobi-nemia as a complication of topical dapsone. N Engl J Med. 2015;372:491-492.
Leukocytoclastic vasculitis (LCV) is a disease characterized by inflammation of small vessels with characteristic clinical findings of petechiae and palpable purpura.1 Numerous etiologies have been described, but the disease commonly remains idiopathic.2,3 Leukocytoclastic vasculitis often spontaneously resolves within weeks and requires only symptomatic treatment. Chronic or severe disease can require systemic medical treatment with agents such as colchicine, dapsone, and corticosteroids. These agents are effective but carry risks of serious side effects.4,5 These side effects and/or medical contraindications prevent some patients from taking systemic medications for LCV. We present a case of LCV that resolved after treatment with topical dapsone, highlighting a potential new treatment ofLCV with a markedly better side-effect profile.
Case Report
A 60-year-old woman with recent upper respiratory tract and sinus infections presented to our dermatology clinic with painful palpable purpura on the bilateral shins, thighs, and dorsal aspects of the feet of several months’ duration (Figure, A). Her primary care provider initiated treatment with amoxicillin and doxycycline for the infections. When the rash developed approximately 1.5 weeks following initiation of her symptoms, the patient was referred to the dermatology and rheumatology departments at our institution. The treating dermatologist (M.B.T.) obtained a 4-mm punch biopsy from the right lower leg and LCV was shown on histology. The patient completed a 14-day course of doxycycline and amoxicillin without resolution of the eruption. After an extensive investigation, the treating rheumatologist concluded that the LCV was idiopathic or secondary to an infection or drug exposure. The rheumatologist started the patient on oral prednisone for the chronic symptomatic LCV, but she was intolerant of this medication and discontinued it after 1 week. Our dermatology clinic started her on triamcinolone cream 0.1% twice daily, but she continued to experience new and worsening lesions. At her follow-up appointment 1 month later, triamcinolone cream was discontinued and dapsone gel 5% twice daily was started. She experienced resolution of her previously recalcitrant LCV within 3 weeks (Figure, B).
Comment
Established therapies for LCV carry serious side-effect profiles, which can preclude their use.5 Therefore, a topical therapeutic alternative for LCV would be ideal. Systemic prednisone is the first-line therapy for chronic and/or symptomatic LCV, but its side effects include suppression of the hypothalamic-pituitary-adrenal axis, immunosuppression, osteonecrosis, and glucose intolerance.5 Colchicine therapy carries risks for blood dyscrasia, immunosuppression, and gastrointestinal tract upset. Systemic dapsone also is an effective therapy for chronic and/or symptomatic LCV.5,6 However, systemic dapsone requires glucose-6-phosphate dehydrogenase deficiency screening and routine monitoring of blood counts, and it also carries the risk for serious adverse effects including neuropathy, blood dyscrasia, and hypersensitivity syndrome.5,6 Topical dapsone may provide similar efficacy with far fewer adverse effects and has proven to be a safe treatment of acne, even when used in patients with glucose-6-phosphate dehydrogenase deficiency. It displays low systemic absorption and does not accumulate over time once a steady state is reached.7 It also has been shown to be beneficial in other vasculopathies such as erythema elevatum diutinum and in other neutrophilic inflammatory disorders such as pyoderma gangrenosum.8,9 A case of methemoglobinemia due to topical dapsone has been reported.10 Although this effect is rare, clinicians should be aware of such adverse effects when using medications for off-label purposes.
Leukocytoclastic vasculitis can spontaneously resolve; however, our patient’s disease was chronic for several months, and she continued to develop new lesions without signs of resolution. After initiating topical dapsone, she experienced resolution within 3 weeks.
Conclusion
Topical dapsone is a novel approach for treating LCV. Given this drug’s favorable side-effect profile compared to the currently available therapeutic alternatives, we believe it is a reasonable option in select patients. Further investigation is needed to prove its efficacy, but it could be an ideal alternative for patients with contraindications to traditional therapies and/or for those unable to tolerate systemic therapy.
Leukocytoclastic vasculitis (LCV) is a disease characterized by inflammation of small vessels with characteristic clinical findings of petechiae and palpable purpura.1 Numerous etiologies have been described, but the disease commonly remains idiopathic.2,3 Leukocytoclastic vasculitis often spontaneously resolves within weeks and requires only symptomatic treatment. Chronic or severe disease can require systemic medical treatment with agents such as colchicine, dapsone, and corticosteroids. These agents are effective but carry risks of serious side effects.4,5 These side effects and/or medical contraindications prevent some patients from taking systemic medications for LCV. We present a case of LCV that resolved after treatment with topical dapsone, highlighting a potential new treatment ofLCV with a markedly better side-effect profile.
Case Report
A 60-year-old woman with recent upper respiratory tract and sinus infections presented to our dermatology clinic with painful palpable purpura on the bilateral shins, thighs, and dorsal aspects of the feet of several months’ duration (Figure, A). Her primary care provider initiated treatment with amoxicillin and doxycycline for the infections. When the rash developed approximately 1.5 weeks following initiation of her symptoms, the patient was referred to the dermatology and rheumatology departments at our institution. The treating dermatologist (M.B.T.) obtained a 4-mm punch biopsy from the right lower leg and LCV was shown on histology. The patient completed a 14-day course of doxycycline and amoxicillin without resolution of the eruption. After an extensive investigation, the treating rheumatologist concluded that the LCV was idiopathic or secondary to an infection or drug exposure. The rheumatologist started the patient on oral prednisone for the chronic symptomatic LCV, but she was intolerant of this medication and discontinued it after 1 week. Our dermatology clinic started her on triamcinolone cream 0.1% twice daily, but she continued to experience new and worsening lesions. At her follow-up appointment 1 month later, triamcinolone cream was discontinued and dapsone gel 5% twice daily was started. She experienced resolution of her previously recalcitrant LCV within 3 weeks (Figure, B).
Comment
Established therapies for LCV carry serious side-effect profiles, which can preclude their use.5 Therefore, a topical therapeutic alternative for LCV would be ideal. Systemic prednisone is the first-line therapy for chronic and/or symptomatic LCV, but its side effects include suppression of the hypothalamic-pituitary-adrenal axis, immunosuppression, osteonecrosis, and glucose intolerance.5 Colchicine therapy carries risks for blood dyscrasia, immunosuppression, and gastrointestinal tract upset. Systemic dapsone also is an effective therapy for chronic and/or symptomatic LCV.5,6 However, systemic dapsone requires glucose-6-phosphate dehydrogenase deficiency screening and routine monitoring of blood counts, and it also carries the risk for serious adverse effects including neuropathy, blood dyscrasia, and hypersensitivity syndrome.5,6 Topical dapsone may provide similar efficacy with far fewer adverse effects and has proven to be a safe treatment of acne, even when used in patients with glucose-6-phosphate dehydrogenase deficiency. It displays low systemic absorption and does not accumulate over time once a steady state is reached.7 It also has been shown to be beneficial in other vasculopathies such as erythema elevatum diutinum and in other neutrophilic inflammatory disorders such as pyoderma gangrenosum.8,9 A case of methemoglobinemia due to topical dapsone has been reported.10 Although this effect is rare, clinicians should be aware of such adverse effects when using medications for off-label purposes.
Leukocytoclastic vasculitis can spontaneously resolve; however, our patient’s disease was chronic for several months, and she continued to develop new lesions without signs of resolution. After initiating topical dapsone, she experienced resolution within 3 weeks.
Conclusion
Topical dapsone is a novel approach for treating LCV. Given this drug’s favorable side-effect profile compared to the currently available therapeutic alternatives, we believe it is a reasonable option in select patients. Further investigation is needed to prove its efficacy, but it could be an ideal alternative for patients with contraindications to traditional therapies and/or for those unable to tolerate systemic therapy.
- Koutkia P, Mylonakis E, Rounds S, et al. Leucocytoclastic vasculitis: an update for the clinician. Scand J Rheumatol. 2001;30:315-322.
- Af Ekenstam E, Callen JP. Cutaneous leukocytoclastic vasculitis. clinical and laboratory features of 82 patients seen in private practice. Arch Dermatol. 1984;120:484-489.
- Gyselbrecht L, de Keyser F, Ongenae K, et al. Etiological factors and underlying conditions in patientswith leucocytoclastic vasculitis. Clin Exp Rheumatol. 1996;14:665-668.
- Sais G, Vidaller A, Jucglà A, et al. Colchicine in the treatment of cutaneous leukocytoclastic vasculitis. results of a prospective, randomized controlled trial. Arch Dermatol. 1995;131:1399-1402.
- Sunderkotter C, Bonsmann G, Sindrilaru A, et al. Management of leukocytoclastic vasculitis: clinical review. J Dermatol Treat. 2005;16:193-206.
- Zhu YI, Stiller MJ. Dapsone and sulfones in dermatology: overview and update. J Am Acad Dermatol. 2001;45:420-434.
- Stotland M, Shalita AR, Kissling RF. Dapsone 5% gel: a review of its efficacy and safety in the treatment of acne vulgaris. Am J Clin Dermatol. 2009;10:221-227.
- Frieling GW, Williams NL, Lim SJ, et al. Novel use of topical dapsone 5% gel for erythema elevatum diutinum: safer and effective. J Drugs Dermatol. 2013;12:481-484.
- Handler MZ, Hamilton H, Aires D. Treatment of peristomal pyoderma gangrenosum with topical crushed dapsone. J Drugs Dermatol. 2011;10:1059-1061.
- Swartzentruber GS, Yanta JH, Pizon AF. Methemoglobi-nemia as a complication of topical dapsone. N Engl J Med. 2015;372:491-492.
- Koutkia P, Mylonakis E, Rounds S, et al. Leucocytoclastic vasculitis: an update for the clinician. Scand J Rheumatol. 2001;30:315-322.
- Af Ekenstam E, Callen JP. Cutaneous leukocytoclastic vasculitis. clinical and laboratory features of 82 patients seen in private practice. Arch Dermatol. 1984;120:484-489.
- Gyselbrecht L, de Keyser F, Ongenae K, et al. Etiological factors and underlying conditions in patientswith leucocytoclastic vasculitis. Clin Exp Rheumatol. 1996;14:665-668.
- Sais G, Vidaller A, Jucglà A, et al. Colchicine in the treatment of cutaneous leukocytoclastic vasculitis. results of a prospective, randomized controlled trial. Arch Dermatol. 1995;131:1399-1402.
- Sunderkotter C, Bonsmann G, Sindrilaru A, et al. Management of leukocytoclastic vasculitis: clinical review. J Dermatol Treat. 2005;16:193-206.
- Zhu YI, Stiller MJ. Dapsone and sulfones in dermatology: overview and update. J Am Acad Dermatol. 2001;45:420-434.
- Stotland M, Shalita AR, Kissling RF. Dapsone 5% gel: a review of its efficacy and safety in the treatment of acne vulgaris. Am J Clin Dermatol. 2009;10:221-227.
- Frieling GW, Williams NL, Lim SJ, et al. Novel use of topical dapsone 5% gel for erythema elevatum diutinum: safer and effective. J Drugs Dermatol. 2013;12:481-484.
- Handler MZ, Hamilton H, Aires D. Treatment of peristomal pyoderma gangrenosum with topical crushed dapsone. J Drugs Dermatol. 2011;10:1059-1061.
- Swartzentruber GS, Yanta JH, Pizon AF. Methemoglobi-nemia as a complication of topical dapsone. N Engl J Med. 2015;372:491-492.
Practice Points
- Leukocytoclastic vasculitis is characterized by inflammation of small vessels with characteristic clinical findings of petechiae and palpable purpura.
- Leukocytoclastic vasculitis often spontaneously resolves within weeks and requires only symptomatic treatment, but chronic or severe disease can require systemic medical treatment with agents such as colchicine, dapsone, and corticosteroids.