User login
Statins in acute coronary syndromes: Start them in the hospital
Adverse events: Reducing the risk of litigation
Urticaria Associated With a Small Cell Carcinoma of the Lung
Terror-related stress: How ready are you to deal with it?
Since September 11, America has carried on under a cloud of fear. Though the cloud is lifting, it will not disappear for months or years. The terrorist attacks on New York City and Washington, DC, the resultant military action in Afghanistan, and the anthrax scare—combined with pervasive, nagging doubts about homeland security and the specter of another possible future terrorist attack—all are straining the nation’s collective emotional well-being.
Psychiatrists in America have reported new cases of terror-inspired acute stress disorder, anxiety, depression, and other illnesses, as well as recurrences of posttraumatic stress disorder (PTSD) in existing patients, in the weeks after the recent attacks and the anthrax scare. What will be the impact on psychiatric practice in the coming months and years?
“We are all at ground zero,” says Kenneth S. Thompson, MD, of Pittsburgh, an experienced disaster psychiatrist. But he and other subspecialists have identified four critical areas in which psychiatrists should be prepared:
- Identifying how terrorist attacks and scares can exacerbate symptoms in patients now in your practice;
- Diagnosing PTSD among comorbid conditions present in existing or new patients;
- Treating—and avoiding over-treatment—of patients with acute stress disorder and PTSD;
- Managing fear in your communities—in response to the Sept. 11 attacks, to the anthrax scare, or in anticipation of an impending catastrophe.
To bring you this special report, the editors of Current Psychiatry have reviewed the literature and interviewed psychiatrists nationwide and in countries such as Israel and Colombia, where terrorism has been a fact of life for years (see “PTSD lessons from Israel, Colombia,”).
Terror and your patients
Which symptoms are you most likely to see in existing patients subsequent to recent events? In the weeks following the Sept. 11 attacks, psychiatrists reported the most commonly seen symptoms as increased anxiety and worsened depression. Sleep disturbances, agoraphobia, suicidality, and severe reactions among patients with personality disorders also were reported.
Patients with previous PTSD or exposure to trauma face a high risk of new or recurrent PTSD in the wake of Sept. 11 than do those not previously exposed to trauma.1 War veterans with prior posttraumatic symptoms have been particularly prone to recurrent PTSD after the attacks. James Allen, MD, of the Department of Psychiatry and Behavioral Sciences at the University of Oklahoma Health Sciences Center, calls this the “additive effect”: patients traumatized by military service in Vietnam experience a recurrence after seeing a major disaster or atrocity. Dr. Allen, who was extensively involved with Oklahoma City’s disaster psychiatry effort after the 1995 bombing there, recalls seeing patients who were traumatized in Vietnam suffer a recurrence after the Alfred P. Murrah Building attack, and then another relapse after Sept. 11.
“The Sept. 11 attacks were very similar to the war for them,” says Juan Corvalan, MD, of the PTSD Unit of the St. Louis Veterans Administration Medical Center, referring to the numerous war veterans he treated after the atrocities. “Seeing it on TV triggered many memories.” By early November, however, many who experienced recurrent PTSD had returned to their pre-Sept. 11 mental states.
Craig Katz, MD, director of emergency psychiatry services at New York’s Mount Sinai Medical Center, says that a patient’s psychiatric history is crucial to determining risk for PTSD or other terror-related sequelae:
“You can recognize that a given person is at high risk for PTSD post-trauma, based on any combination of these factors—having a psychiatric history, past trauma, high exposure to the event, psychosocial problems pre-disaster, or lack of supports post-disaster.”
The clinical interview is a vital tool in assessing patients with suspected PTSD or posttraumatic sequelae, says Arieh Shalev, MD, of the department of psychiatry at Hadassah University Hospital in Jerusalem, Israel. “It provides the opportunity to discuss the traumatic event with the patient, and to listen to his or her perceptions of the event and its effects” in order to carefully appraise the patient’s symptoms.2
The guidelines set forth in the Diagnostic and Statistical Manual for Mental Disorders, Fourth Edition (DSM-IV) remain the gold standard for confirming a diagnosis of PTSD and discerning long-term posttraumatic sequelae from temporary acute stress disorder (Box 1). The guidelines have proved far from foolproof, however, and the existence of psychiatric comorbidities often clouds the picture.

- Exposure to a traumatic event with both of the following present:
- The traumatic event is persistently reexperienced in one or more of the following ways:
- Persistent avoidance of stimuli associated with the trauma and numbing of general responsiveness (not present before the trauma), as indicated by three or more of the following:
- Persistent symptoms of increased arousal (not present before the trauma), as indicated by two or more of the following:
- Duration of symptoms in criteria B, C or D exceeds 1 month.
- Disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
Specify if; Acute: if duration of symptoms is less than 3 months.
Chronic: if symptoms persist 3 months or more.
With delayed onset: if onset of symptoms is at least 6 months after the stressor.
Acute stress disorder, whose symptom pattern is similar to that of PTSD, is distinguished from PTSD because the symptom pattern must occur and resolve within 4 weeks of the traumatic event. If the symptoms persist for more than 1 month and meet the criteria for PTSD, the diagnosis is changed from acute stress disorder to PTSD.
Differential diagnosis of PTSD
Patients with PTSD are more likely to have substantial psychiatric comorbidity than are those without the disorder.3 Possible reasons include suspected self-medication of PTSD symptoms, particularly among patients with substance abuse, and the possible overreporting of symptoms by patients. Psychiatrists should maintain a high level of suspicion for PTSD when managing a new or existing patient with psychopathology.
Citing data from the National Comorbidity Study of the Institute for Social Research at the University of Michigan, Kessler and others in 1995 noted that more than 80 percent of individuals with PTSD meet criteria for at least one other psychiatric diagnosis. Roughly half of PTSD sufferers met criteria for three or more comorbidities.3
Kathleen Brady, MD, professor of psychiatry at the Medical University of South Carolina in Charleston, noted in a 1997 study that affective disorders, other anxiety disorders, somatization, substance abuse, and dissociative disorders are common comorbidities of PTSD.5 Dr. Shalev and colleagues in one study found that a history of major depressive disorder may increase the severity of posttraumatic morbidity.6 Dr. Brady and others also have found that PTSD patients with a comorbid substance abuse disorder experience severe PTSD symptoms while in a withdrawal state.7
| Disorder | Symptoms that overlap with PTSD |
|---|---|
| Adjustment disorder | Extreme response to stressor. Stressor is not necessarily extreme in nature (e.g., spouse leaving, being fired), and the response might not meet criteria for PTSD.4 |
| Depression | Diminished interest, restricted range of affect, sleep difficulties, or poor concentration.5 |
| Dissociative disorders | Inability to recall important information about past trauma, sense of detachment from oneself, derealization, nightmares, flashbacks, startle responses, or lack of affective response (e.g., onset of dissociative fugue may be tied to past trauma).4 |
| Generalized anxiety | Irritability, hypervigilance, or increased startle reflex.5 |
| Obsessive-compulsive disorder | Recurrent intrusive thoughts (not related to trauma in obsessive-compulsive disorder).4 |
| Panic attacks | Heart palpitations or increased heart rate, sense of detachment, nausea or abdominal distress.4 |
| Psychosis | Illusions, hallucinations, or other perceptual disturbances (may be confused with flashbacks in PTSD).4 |
| Substance abuse disorder | Hallucinations, illusions, diminished interest in or avoidance of significant activities, or social estrangement.4 |

PTSD often is overlooked in the presence of other psychiatric diagnoses. Meuser et al in 1998 studied 275 patients with schizophrenia and bipolar disorder. As many as 98 percent of patients reported lifetime exposure to at least one traumatic event. The researchers found diagnosable PTSD in 119 (43 %) of the subjects, but only three (2%) had the diagnosis in their charts.8
In a later study, Dr. Brady and others cited substantial symptom overlap between PTSD and other psychiatric diagnoses, particularly major depressive disorder. This can contribute to underdiagnosis of PTSD, the researchers found.7 (Box 2).

Children also have been experiencing stress disorders since Sept. 11, says Arshad Husain, MD, professor and chief of child and adolescent psychiatry and director of the International Center for Psychosocial Trauma at the University of Missouri-Columbia. Such disorders manifest as sleep disturbances, anxiety, hyperarousal/hyperactivity, and nightmares.
Young children regress and cling to their parents, and are frightened of the dark or noises, Dr, Husain notes. Those who are toilet-trained can suddenly wet the bed, become neurotic, and demand attention. School-age children are more fearful; they may not want to go to school, their schoolwork may decline, and they may have trouble paying attention. Dr. Husain suggests discussing the trauma and devising a plan of action with them in case the trauma recurs.
The media’s role in reporting on the aftermath of the attacks—and triggering traumatic reactions as an unintended consequence—cannot be overlooked. Two recent studies performed after the Oklahoma City bombing suggest that television reports of that atrocity precipitated PTSD symptoms in middle-school children 7 weeks after the bombing,23 and in geographically distant sixth-graders 2 years after the attack.12 It was not clear whether any of these students had prior PTSD or other psychopathology.
Psychiatric education in the schools is especially crucial in light of the school violence that has occurred in America in recent years. Dr. Husain believes that the children who commit violence are victims of abuse. If teachers early on can identify children who show evidence of stress disorders, they can refer them to trained psychiatrists, catching those who need help before tragedies occur. “It is the psychiatric equivalent of CPR,” Dr. Husain says.
Dr. Brady recommends that psychiatrists and primary care physicians routinely screen patients for exposure to traumatic events. Ask patients specifically about their reaction to such events and encourage them to talk about it. Patients often feel either guilty or embarrassed about the traumatic event, or do not believe it affects their presenting complaints, she notes. Other approaches may be needed to identify the risk of PTSD in children (Box 3).
Identifying a traumatic event of an extreme nature, for example, a life-threatening experience, is key to diagnosing PTSD in the presence of comorbidities, Dr. Corvalan says. “Some of the symptoms—such as avoidance, numbing, and increased arousal—are present in other disorders and may have occurred before exposure to the traumatic event.” If they did, he says, PTSD is ruled out.
Gauging the extent of the patient’s exposure to the traumatic event is critical to determining the likelihood of PTSD onset. Dr. Allen, of Oklahoma City, points to studies that show that the closer and longer the patient has been exposed to a catastrophic event, the more likely he or she will develop PTSD.9,10
Julia Frank, MD, associate professor and director of student education and psychiatry at George Washington University in Washington, DC, suggests screening for symptoms that are unique to PTSD as stated in the DSM-IV, such as nightmares, difficulty remembering the traumatic event, and extreme reactions to reminders of the trauma. She also proposes analyzing the past event and the patient’s reaction to it to confirm that it is a source of trauma.
Patients with PTSD symptoms are easily startled by loud or piercing noises. Dr. Shalev says this characteristic sets true PTSD cases apart from other psychopathology, particularly depression. In one study, Israeli combat veterans with PTSD exhibited a more pronounced heart rate and skin conductance when exposed to auditory stimuli than did combat veterans with no PTSD symptoms.11
Drs. Allen and Frank note that patients who have anthrax-related fears and no prior PTSD symptoms are not likely to develop PTSD. They may, however, manifest symptoms of chronic fatigue, fibromyalgia, and generalized anxiety disorder. Patients may be jumpy, intense, or lethargic, with autonomic instability and rapid heart rate. They may feel alienated and mistrustful of the government. A nonspecific stress disorder and mixed anxiety depression are other possible effects.
Who to treat—and how
Psychiatrists nationwide have reported increased patient presentations after the Sept. 11 attacks and throughout the anthrax scare. Studies conducted after the Oklahoma City bombing also suggest that psychiatrists could be seeing more patients in the coming months.12,13 As caseloads increase, so do the questions about who to treat, how, and how to avoid the possibility of overtreatment.
While many clinicians in the United States recently received their first taste of post-terror psychiatry, those in more violent parts of the world are well-versed in helping their patients manage fear.
Israel has repeatedly been at war throughout its 53-year history. During “peacetime,” terrorism and senseless violence have been a way of life.
“Sadly, Israel’s citizens and its medical and paramedical communities have accrued extensive experience in dealing with the ongoing threat of war and terrorist attacks and their sequelae,” says Zeev Kaplan, MD, director of the Beer-Sheva Mental Health Center and professor of psychiatry at the Ben Gurion University School of Medicine in Beer-Sheva.
Similarly, Colombia is a country long plagued by terrorist and gang violence. PTSD has been on the rise the past 5 years, according to Javier Leon-Silva, MD, chief of psychiatry at the Fundación Santafe de Bogotá. “There is not a single day without a terrorist attack in the news,” Dr. Leon-Silva notes. In addition, two major natural disasters in the last 20 years—the Armero flood and the earthquake in the coffee region—have resulted in tens of thousands of casualties.
Exposure to terror in Israel is widespread—be it direct, as a victim or witness, or secondary, as a victim’s close friend or relative. Recurrent PTSD, brought on by direct and indirect exposure, is common, Dr. Kaplan says. Holocaust survivors, almost as numerous within Israel’s population as combat veterans, have been especially prone to recurrent PTSD.
Children are particularly susceptible to PTSD. In Israel, someone’s parent, sibling or classmate often is among the casualties of a terrorist attack, Dr. Kaplan notes. In Colombia, “children grow up influenced by stories about family members or friends who have been victims of the consequences of war and terror, and by strict family security measures concerning behavior,” Dr. Leon-Silva adds.
Because of the Middle East’s volatile history, most of Israel’s psychiatric professionals have hands-on experience in treating traumatized patients in both military and civilian settings. Joseph Zohar, MD, chairman of Israel’s Consortium on PTSD, says that most psychiatrists have served at some point in the Israeli Defense Forces.
Further, as both Israel’s medical community and the public have learned more about PTSD and post-terror anxiety, physicians can now identify affected people more rapidly, and can refer them for treatment, Dr. Kaplan says. Civilians and veterans have access to five regional trauma and post trauma centers. Educators are trained to detect behavioral changes in the young, and Israel’s children are followed into adulthood to assess the long-term effects of terrorist events.
Colombia’s psychiatrists are also well-qualified to treat terror-inspired psychiatric illness, Dr. Leon-Silva says. However, most people in the impoverished nation cannot afford needed medicines, and psychiatrists are hard-pressed to reach many disaster or terror victims.
Dr. Zohar urges psychiatrists here to attend seminars and workshops on PTSD and acute stress reaction. He says such seminars in Israel have taught clinicians the long-term effects of exposure to terror and its effect on families, as well as how to help patients manage acute stress reactions.
Dr. Kaplan feels his U.S. counterparts should incorporate a multidisciplinary approach that addresses bio-medical, psychotherapeutic, familial, and social/occupational rehabilitation. He encourages national and local civic leaders to educate the public about terror-related stress.
Dr. Leon-Silva advises U.S. psychiatrists not to be ashamed to reveal their fears after a terrorist atrocity. “Sometimes expressing how the event impacts you will help the patient be more communicative and will more extensively show the patient’s symptoms.”
“In order to provide effective care to our patients it is necessary to have clear ideas on how to follow criteria for diagnosis and as a consequence for treatment,” Dr. Corvalan says. “The field at times is confusing; patients do not always follow the diagnostic criteria. The needs of the moment, limitations of recourses, intensity and variety of symptoms, urgency of the situation, etc., all conspire to make the job more difficult.”
Patients with anthrax-related anxiety should be encouraged to “try to function as normally as possible and keep an open communication with peers and those who they look to for information,” Dr. Frank notes. Dr. Allen adds that his patients with anthrax-inspired stress have responded well to breathing, meditation and other relaxation techniques.
Treatment of patients who are severely traumatized and exhibit true PTSD symptoms will vary based on severity of exposure, history of prior PTSD, and existence of comorbidities. A combination of pharmacological and psychosocial therapy is the common first-line treatment.
The selective serotonin reuptake inhibitor (SSRI) sertraline is specifically indicated for treating confirmed PTSD symptoms, and several studies have documented the agent’s effectiveness for this use.14,15 Dr. Frank recommends dosages between 50 and 200 mg/d depending on the patient’s body weight or complaint of side effects (e.g., diarrhea, nausea, or sexual dysfunction). Other SSRIs, as well as tricyclics and MAO inhibitors, are alternatives. Fluoxetine, amitriptyline, phenelzine, and imipramine have all been found more effective than a placebo;16-18 paroxetine also has been shown effective in specific populations.19
Kenneth S. Thompson, MD, a Pittsburgh-based disaster psychiatrist who helped coordinate Oklahoma City’s emergency psychiatry effort after the 1995 bombing, identified four stages that the public works through after a major disaster:
- Mobilization. Rebuilding—or just surviving—is foremost on people’s minds immediately after a traumatic event. Many people either throw themselves headfirst into the recovery and cleanup effort, or assist grieving families that have been hardest hit by the disaster. Others fear for their safety and leave town. Feelings of grief and loss are set aside to focus on the needs of the moment.
- Self-importance. As the media reports on their efforts to put their city—and their lives—back together, people at this stage tend to feel they are part of something. Those who have lost family members and coworkers seem to be coping well at this point, and feel as though they can draw ample moral support from friends and neighbors.
- Abandonment. Once the dust settles and the media coverage dies down, people who lost loved ones are left to confront their grief alone. Those who witnessed the tragedy, or who know someone who was killed or injured in the incident, must confront their demons one on one. It is at this point that PTSD and other psychiatric disorders can set in. Those who did not lose a friend or relative feel a more general sense of loss. Worse still, there may be “a disaster after the disaster,” in which a political official or emergency services officer is charged with some type of wrongdoing or abuse of power. People then feel used and betrayed.
- Acceptance. People begin to seek psychiatric or other help in dealing with the trauma, and begin to come to terms with their loss.
Benzodiazapenes also may be prescribed to manage PTSD symptoms. Patients should be counseled against taking these sedating agents in the daytime, however, as they can lead to fogginess, detachment, and trouble functioning.
Assessing the patient’s available social support also is crucial to PTSD treatment. “Do patients talk to other people about the event?” Dr. Frank asks. “Are they trying to get back to a daily routine? Can they make sense of this experience? Are they incorporating the event into a world view?”
Dr. Thompson, the Pittsburgh disaster psychiatrist, agrees. Psychiatrists should encourage their patients to talk more about their trauma and how fear is affecting their lives. “We don’t discuss with our trauma patients as much as we might what the experience has been like for them,” he says.
Small-group therapy is the most conducive approach to psychotherapy for PTSD, according to Dr. Frank, although individual counseling can work in many cases. Several studies have found group therapy effective,20,21 and 12-step group therapy has shown promise in PTSD patients with comorbid substance abuse disorder.22
Managing fear
Just as people grieve and confront death in stages, Dr. Thompson, who helped coordinate Oklahoma City’s disaster psychiatry effort, has discovered that the public usually employs a similar subconscious process to cope with a traumatic event (Box 4).
But Americans have had no time to recover. As U.S. troops seek justice in Afghanistan, back home people grapple with the threat of anthrax contamination and the prospect of another terrorist attack. The ominously enhanced presence of security at airports, major bridges, sporting and entertainment events, and in other aspects of everyday life, has further fueled the sensation that all is not right.
“The September 11 tragedy brings trauma home,” adds Arshad Husain, MD, professor and chief of child and adolescent psychiatry and director of the International Center for Psychosocial Trauma at the University of Missouri-Columbia. “The anthrax scare and the Nov. 12 plane crash of American Airlines Flight 587 only further remind people of their vulnerability and fears. If the anthrax scare were an accident, people would have been relieved. Since the plane crash was ruled an accident, it has offered people a chance to feel more in control. Accidents can be fixed with better maintenance. Terrorism cannot.”
Dr. Katz of New York City and other disaster psychiatrists are urging their colleagues to help manage public fear by reaching out through community efforts.
Dr. Katz is president of the volunteer group Disaster Psychiatry Outreach, which helped coordinate the city’s post-Sept. 11 trauma psychiatry effort. Visitors waiting at New York’s Family Assistance Center, a referral and help center for people who lost family and friends in the World Trade Center attack, were approached by Dr. Katz and other colleagues to let them know that psychiatric services were available if needed. By doing this, he says, Disaster Psychiatry Outreach clinicians have identified, treated, and referred scores of patients with terror-related stress who otherwise would have gone untreated.
Joseph Dorzab, MD, of the Holt-Krock Clinic in Fort Smith, Ark., also has offered his services. Members of his clinic’s psychiatry department have made several TV appearances, and have given and coordinated area lectures. Working with the local mental health association, the department also is starting a community forum called Mental Health Mondays, an open discussion group with coffee and cookies at a local coffee shop.
In Pittsburgh, Dr. Thompson is encouraging psychiatrists to educate their communities about how traumatic events affect the public. He proposes:
- Staging community meetings to brief religious and other leaders on how to manage traumatized people;
- Informing local news editors about the nature of psychiatric disorders;
- Instructing school administrators about detecting signs of distress in children;
- Contacting local government officials to offer input in devising the town’s emergency response plan.
Psychiatrists also can educate themselves about managing public trauma, thanks to scores of studies that have been done in recent years following major man-made and natural disasters, from Mount St. Helens and Hurricane Andrew, to Chernobyl and the Yom Kippur War. Dr. Thompson urges psychiatrists to seek out the papers of prominent leaders in trauma-related psychiatry, mentioning studies by Carol North, MD, Betty Pfefferbaum, MD, and Robert Ursano, MD, as examples. Other sources include the Web sites of the American Psychiatric Association and National Center for PTSD. (See Related Resources.)
In the end, psychiatrists have been well primed for dealing with public disaster—just by treating individual patients whose psychiatric disorders emanated from everyday life, Dr. Thompson says. “Psychiatrists know more about trauma than they recognize.”
- National Center for PTSD Web site
- National Institute of Mental Health:
- Linenthal EJ. The Unfinished Bombing: Oklahoma City in American Memory. Oxford University Press, 2001.
- Norwood AE, Ursano RJ, Fullerton CS. Disaster psychiatry: principles of practice. Psychiatr Q. 2000; 71(3):207-226.
- American Psychiatric Association Web site:
- The Psychiatric Training Manual for Teachers and Mental Health Professionals
Drug brand names
- Amitriptyline • Elavil
- Bupropion • Wellbutrin
- Fluoxetine • Prozac
- Imipramine • Tofranil
- Paroxetine • Paxil
- Phenelzine • Nardil
- Sertraline • Zoloft
1. Breslau N, Chilcoat HD, Kessler RC, Davis GC. Previous exposure to trauma and PTSD effects of subsequent trauma: results from the Detroit Area Survey of Trauma. Am J Psychiatry. 1999;156(6):902-7.
2. Shalev AY. What is posttraumtic stress disorder? J Clin Psychiatry. 2001;62(Suppl 17):4-10.
3. Kessler RC, Sonnega A, et al. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry. 1995;52(12):1048-60
4. Diagnostic and Statistical Manual of Mental Disorders, 4th ed. Washington, DC: American Psychiatric Association, 2000.
5. Brady KT. Posttraumatic stress disorder and comorbidity: recognizing the many faces of PTSD. J Clin Psychiatry. 1997;58 Suppl 9:12-5.
6. Shalev AY, Freedman S, Peri T, et al. Prospective study of posttraumatic stress disorder and depression following trauma. Am J Psychiatry. 1998;155:630-7.
7. Brady KT, Killeen TK, Brewerton T, Lucerini S. Comorbidity of psychiatric disorders and posttraumatic stress disorder. J Clin Psychiatry 2000;61 Suppl 7:22-32.
8. Mueser KT, Goodman LB, et al. Trauma and posttraumatic stress disorder in severe mental illness. J Consult Clin Psychol. 1998;66(3):493-9.
9. Cloitre M, Cohen LR, Edelman RE, Han H. Posttraumatic stress disorder and extent of trauma exposure as correlates of medical problems and perceived health among women with childhood abuse. Women Health. 2001;34(3):1-17.
10. Hodgins GA, Creamer M, Bell R. Risk factors for posttrauma reactions in police officers: a longitudinal study. J Nerv Ment Dis. 2001;189(8):541-7.
11. Orr SP, Solomon Z, Peri T, et al. Physiologic responses to loud tones in Israeli veterans of the 1973 Yom Kippur War. Biol Psychiatry. 1997;41:319-26.
12. Pfefferbaum B, Seale TW, et al. Posttraumatic stress two years after the Oklahoma City Bombing in youths geographically distant from the explosion. Psychiatry 2000;63(4):358-370.
13. Smith DW, Christiansen EH, Vincent R, Hann N. Population effects of the bombing of Oklahoma City. J Oklahoma State Med Association. 1999;92(4):193-198.
14. Londborg PD, Hegel MT, et al. Sertraline treatment of posttraumatic stress disorder: results of 24 weeks of open-label continuation treatment. J Clin Psychiatry. 2001;62(5):325-31.
15. Davidson JR. Pharmacotherapy of generalized anxiety disorder. J Clin Psychiatry. 2001;62 Suppl 11:46-50.discussion 51-2.
16. Connor KM, Sutherland SM, et al. Fluoxetine in post-traumatic stress disorder. Randomised, double-blind study. Br J Psychiatry. 1999;175:17-22.
17. Davidson J, Kudler H, et al. Treatment of posttraumatic stress disorder with amitriptyline and placebo. Arch Gen Psychiatry. 1990;47(3):259-66.
18. Kosten TR, Frank JB, et al. Pharmacotherapy for posttraumatic stress disorder using phenelzine or imipramine. J Nerv Ment Dis. 1991;179(6):366-70.
19. Smajkic A, Weine S, et al. Sertraline, paroxetine, and venlafaxine in refugee posttraumatic stress disorder with depression symptoms. J Trauma Stress. 2001;14(3):445-52.
20. Wolfsdorf BA, Zlotnick C. Affect management in group therapy for women with posttraumatic stress disorder and histories of childhood sexual abuse. J Clin Psychol 2001 Feb;57(2):169-81.
21. Jones L, Brazel D, et al. Group therapy program for African-American veterans with posttraumatic stress disorder. Psychiatr Serv. 2000;51(9):1177-9.
22. Ouimette P, Humphreys K, et al. Self-help group participation among substance use disorder patients with posttraumatic stress disorder. J Subst Abuse Treat. 2001;20(1):25-32.
23. Pfefferbaum B, Nixon SJ, Tivis RD, et al. Television exposure in children after a terrorist incident. Psychiatry. 2001;64(3):202-11.
Since September 11, America has carried on under a cloud of fear. Though the cloud is lifting, it will not disappear for months or years. The terrorist attacks on New York City and Washington, DC, the resultant military action in Afghanistan, and the anthrax scare—combined with pervasive, nagging doubts about homeland security and the specter of another possible future terrorist attack—all are straining the nation’s collective emotional well-being.
Psychiatrists in America have reported new cases of terror-inspired acute stress disorder, anxiety, depression, and other illnesses, as well as recurrences of posttraumatic stress disorder (PTSD) in existing patients, in the weeks after the recent attacks and the anthrax scare. What will be the impact on psychiatric practice in the coming months and years?
“We are all at ground zero,” says Kenneth S. Thompson, MD, of Pittsburgh, an experienced disaster psychiatrist. But he and other subspecialists have identified four critical areas in which psychiatrists should be prepared:
- Identifying how terrorist attacks and scares can exacerbate symptoms in patients now in your practice;
- Diagnosing PTSD among comorbid conditions present in existing or new patients;
- Treating—and avoiding over-treatment—of patients with acute stress disorder and PTSD;
- Managing fear in your communities—in response to the Sept. 11 attacks, to the anthrax scare, or in anticipation of an impending catastrophe.
To bring you this special report, the editors of Current Psychiatry have reviewed the literature and interviewed psychiatrists nationwide and in countries such as Israel and Colombia, where terrorism has been a fact of life for years (see “PTSD lessons from Israel, Colombia,”).
Terror and your patients
Which symptoms are you most likely to see in existing patients subsequent to recent events? In the weeks following the Sept. 11 attacks, psychiatrists reported the most commonly seen symptoms as increased anxiety and worsened depression. Sleep disturbances, agoraphobia, suicidality, and severe reactions among patients with personality disorders also were reported.
Patients with previous PTSD or exposure to trauma face a high risk of new or recurrent PTSD in the wake of Sept. 11 than do those not previously exposed to trauma.1 War veterans with prior posttraumatic symptoms have been particularly prone to recurrent PTSD after the attacks. James Allen, MD, of the Department of Psychiatry and Behavioral Sciences at the University of Oklahoma Health Sciences Center, calls this the “additive effect”: patients traumatized by military service in Vietnam experience a recurrence after seeing a major disaster or atrocity. Dr. Allen, who was extensively involved with Oklahoma City’s disaster psychiatry effort after the 1995 bombing there, recalls seeing patients who were traumatized in Vietnam suffer a recurrence after the Alfred P. Murrah Building attack, and then another relapse after Sept. 11.
“The Sept. 11 attacks were very similar to the war for them,” says Juan Corvalan, MD, of the PTSD Unit of the St. Louis Veterans Administration Medical Center, referring to the numerous war veterans he treated after the atrocities. “Seeing it on TV triggered many memories.” By early November, however, many who experienced recurrent PTSD had returned to their pre-Sept. 11 mental states.
Craig Katz, MD, director of emergency psychiatry services at New York’s Mount Sinai Medical Center, says that a patient’s psychiatric history is crucial to determining risk for PTSD or other terror-related sequelae:
“You can recognize that a given person is at high risk for PTSD post-trauma, based on any combination of these factors—having a psychiatric history, past trauma, high exposure to the event, psychosocial problems pre-disaster, or lack of supports post-disaster.”
The clinical interview is a vital tool in assessing patients with suspected PTSD or posttraumatic sequelae, says Arieh Shalev, MD, of the department of psychiatry at Hadassah University Hospital in Jerusalem, Israel. “It provides the opportunity to discuss the traumatic event with the patient, and to listen to his or her perceptions of the event and its effects” in order to carefully appraise the patient’s symptoms.2
The guidelines set forth in the Diagnostic and Statistical Manual for Mental Disorders, Fourth Edition (DSM-IV) remain the gold standard for confirming a diagnosis of PTSD and discerning long-term posttraumatic sequelae from temporary acute stress disorder (Box 1). The guidelines have proved far from foolproof, however, and the existence of psychiatric comorbidities often clouds the picture.
- Exposure to a traumatic event with both of the following present:
- The traumatic event is persistently reexperienced in one or more of the following ways:
- Persistent avoidance of stimuli associated with the trauma and numbing of general responsiveness (not present before the trauma), as indicated by three or more of the following:
- Persistent symptoms of increased arousal (not present before the trauma), as indicated by two or more of the following:
- Duration of symptoms in criteria B, C or D exceeds 1 month.
- Disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
Specify if; Acute: if duration of symptoms is less than 3 months.
Chronic: if symptoms persist 3 months or more.
With delayed onset: if onset of symptoms is at least 6 months after the stressor.
Acute stress disorder, whose symptom pattern is similar to that of PTSD, is distinguished from PTSD because the symptom pattern must occur and resolve within 4 weeks of the traumatic event. If the symptoms persist for more than 1 month and meet the criteria for PTSD, the diagnosis is changed from acute stress disorder to PTSD.
Differential diagnosis of PTSD
Patients with PTSD are more likely to have substantial psychiatric comorbidity than are those without the disorder.3 Possible reasons include suspected self-medication of PTSD symptoms, particularly among patients with substance abuse, and the possible overreporting of symptoms by patients. Psychiatrists should maintain a high level of suspicion for PTSD when managing a new or existing patient with psychopathology.
Citing data from the National Comorbidity Study of the Institute for Social Research at the University of Michigan, Kessler and others in 1995 noted that more than 80 percent of individuals with PTSD meet criteria for at least one other psychiatric diagnosis. Roughly half of PTSD sufferers met criteria for three or more comorbidities.3
Kathleen Brady, MD, professor of psychiatry at the Medical University of South Carolina in Charleston, noted in a 1997 study that affective disorders, other anxiety disorders, somatization, substance abuse, and dissociative disorders are common comorbidities of PTSD.5 Dr. Shalev and colleagues in one study found that a history of major depressive disorder may increase the severity of posttraumatic morbidity.6 Dr. Brady and others also have found that PTSD patients with a comorbid substance abuse disorder experience severe PTSD symptoms while in a withdrawal state.7
| Disorder | Symptoms that overlap with PTSD |
|---|---|
| Adjustment disorder | Extreme response to stressor. Stressor is not necessarily extreme in nature (e.g., spouse leaving, being fired), and the response might not meet criteria for PTSD.4 |
| Depression | Diminished interest, restricted range of affect, sleep difficulties, or poor concentration.5 |
| Dissociative disorders | Inability to recall important information about past trauma, sense of detachment from oneself, derealization, nightmares, flashbacks, startle responses, or lack of affective response (e.g., onset of dissociative fugue may be tied to past trauma).4 |
| Generalized anxiety | Irritability, hypervigilance, or increased startle reflex.5 |
| Obsessive-compulsive disorder | Recurrent intrusive thoughts (not related to trauma in obsessive-compulsive disorder).4 |
| Panic attacks | Heart palpitations or increased heart rate, sense of detachment, nausea or abdominal distress.4 |
| Psychosis | Illusions, hallucinations, or other perceptual disturbances (may be confused with flashbacks in PTSD).4 |
| Substance abuse disorder | Hallucinations, illusions, diminished interest in or avoidance of significant activities, or social estrangement.4 |
PTSD often is overlooked in the presence of other psychiatric diagnoses. Meuser et al in 1998 studied 275 patients with schizophrenia and bipolar disorder. As many as 98 percent of patients reported lifetime exposure to at least one traumatic event. The researchers found diagnosable PTSD in 119 (43 %) of the subjects, but only three (2%) had the diagnosis in their charts.8
In a later study, Dr. Brady and others cited substantial symptom overlap between PTSD and other psychiatric diagnoses, particularly major depressive disorder. This can contribute to underdiagnosis of PTSD, the researchers found.7 (Box 2).
Children also have been experiencing stress disorders since Sept. 11, says Arshad Husain, MD, professor and chief of child and adolescent psychiatry and director of the International Center for Psychosocial Trauma at the University of Missouri-Columbia. Such disorders manifest as sleep disturbances, anxiety, hyperarousal/hyperactivity, and nightmares.
Young children regress and cling to their parents, and are frightened of the dark or noises, Dr, Husain notes. Those who are toilet-trained can suddenly wet the bed, become neurotic, and demand attention. School-age children are more fearful; they may not want to go to school, their schoolwork may decline, and they may have trouble paying attention. Dr. Husain suggests discussing the trauma and devising a plan of action with them in case the trauma recurs.
The media’s role in reporting on the aftermath of the attacks—and triggering traumatic reactions as an unintended consequence—cannot be overlooked. Two recent studies performed after the Oklahoma City bombing suggest that television reports of that atrocity precipitated PTSD symptoms in middle-school children 7 weeks after the bombing,23 and in geographically distant sixth-graders 2 years after the attack.12 It was not clear whether any of these students had prior PTSD or other psychopathology.
Psychiatric education in the schools is especially crucial in light of the school violence that has occurred in America in recent years. Dr. Husain believes that the children who commit violence are victims of abuse. If teachers early on can identify children who show evidence of stress disorders, they can refer them to trained psychiatrists, catching those who need help before tragedies occur. “It is the psychiatric equivalent of CPR,” Dr. Husain says.
Dr. Brady recommends that psychiatrists and primary care physicians routinely screen patients for exposure to traumatic events. Ask patients specifically about their reaction to such events and encourage them to talk about it. Patients often feel either guilty or embarrassed about the traumatic event, or do not believe it affects their presenting complaints, she notes. Other approaches may be needed to identify the risk of PTSD in children (Box 3).
Identifying a traumatic event of an extreme nature, for example, a life-threatening experience, is key to diagnosing PTSD in the presence of comorbidities, Dr. Corvalan says. “Some of the symptoms—such as avoidance, numbing, and increased arousal—are present in other disorders and may have occurred before exposure to the traumatic event.” If they did, he says, PTSD is ruled out.
Gauging the extent of the patient’s exposure to the traumatic event is critical to determining the likelihood of PTSD onset. Dr. Allen, of Oklahoma City, points to studies that show that the closer and longer the patient has been exposed to a catastrophic event, the more likely he or she will develop PTSD.9,10
Julia Frank, MD, associate professor and director of student education and psychiatry at George Washington University in Washington, DC, suggests screening for symptoms that are unique to PTSD as stated in the DSM-IV, such as nightmares, difficulty remembering the traumatic event, and extreme reactions to reminders of the trauma. She also proposes analyzing the past event and the patient’s reaction to it to confirm that it is a source of trauma.
Patients with PTSD symptoms are easily startled by loud or piercing noises. Dr. Shalev says this characteristic sets true PTSD cases apart from other psychopathology, particularly depression. In one study, Israeli combat veterans with PTSD exhibited a more pronounced heart rate and skin conductance when exposed to auditory stimuli than did combat veterans with no PTSD symptoms.11
Drs. Allen and Frank note that patients who have anthrax-related fears and no prior PTSD symptoms are not likely to develop PTSD. They may, however, manifest symptoms of chronic fatigue, fibromyalgia, and generalized anxiety disorder. Patients may be jumpy, intense, or lethargic, with autonomic instability and rapid heart rate. They may feel alienated and mistrustful of the government. A nonspecific stress disorder and mixed anxiety depression are other possible effects.
Who to treat—and how
Psychiatrists nationwide have reported increased patient presentations after the Sept. 11 attacks and throughout the anthrax scare. Studies conducted after the Oklahoma City bombing also suggest that psychiatrists could be seeing more patients in the coming months.12,13 As caseloads increase, so do the questions about who to treat, how, and how to avoid the possibility of overtreatment.
While many clinicians in the United States recently received their first taste of post-terror psychiatry, those in more violent parts of the world are well-versed in helping their patients manage fear.
Israel has repeatedly been at war throughout its 53-year history. During “peacetime,” terrorism and senseless violence have been a way of life.
“Sadly, Israel’s citizens and its medical and paramedical communities have accrued extensive experience in dealing with the ongoing threat of war and terrorist attacks and their sequelae,” says Zeev Kaplan, MD, director of the Beer-Sheva Mental Health Center and professor of psychiatry at the Ben Gurion University School of Medicine in Beer-Sheva.
Similarly, Colombia is a country long plagued by terrorist and gang violence. PTSD has been on the rise the past 5 years, according to Javier Leon-Silva, MD, chief of psychiatry at the Fundación Santafe de Bogotá. “There is not a single day without a terrorist attack in the news,” Dr. Leon-Silva notes. In addition, two major natural disasters in the last 20 years—the Armero flood and the earthquake in the coffee region—have resulted in tens of thousands of casualties.
Exposure to terror in Israel is widespread—be it direct, as a victim or witness, or secondary, as a victim’s close friend or relative. Recurrent PTSD, brought on by direct and indirect exposure, is common, Dr. Kaplan says. Holocaust survivors, almost as numerous within Israel’s population as combat veterans, have been especially prone to recurrent PTSD.
Children are particularly susceptible to PTSD. In Israel, someone’s parent, sibling or classmate often is among the casualties of a terrorist attack, Dr. Kaplan notes. In Colombia, “children grow up influenced by stories about family members or friends who have been victims of the consequences of war and terror, and by strict family security measures concerning behavior,” Dr. Leon-Silva adds.
Because of the Middle East’s volatile history, most of Israel’s psychiatric professionals have hands-on experience in treating traumatized patients in both military and civilian settings. Joseph Zohar, MD, chairman of Israel’s Consortium on PTSD, says that most psychiatrists have served at some point in the Israeli Defense Forces.
Further, as both Israel’s medical community and the public have learned more about PTSD and post-terror anxiety, physicians can now identify affected people more rapidly, and can refer them for treatment, Dr. Kaplan says. Civilians and veterans have access to five regional trauma and post trauma centers. Educators are trained to detect behavioral changes in the young, and Israel’s children are followed into adulthood to assess the long-term effects of terrorist events.
Colombia’s psychiatrists are also well-qualified to treat terror-inspired psychiatric illness, Dr. Leon-Silva says. However, most people in the impoverished nation cannot afford needed medicines, and psychiatrists are hard-pressed to reach many disaster or terror victims.
Dr. Zohar urges psychiatrists here to attend seminars and workshops on PTSD and acute stress reaction. He says such seminars in Israel have taught clinicians the long-term effects of exposure to terror and its effect on families, as well as how to help patients manage acute stress reactions.
Dr. Kaplan feels his U.S. counterparts should incorporate a multidisciplinary approach that addresses bio-medical, psychotherapeutic, familial, and social/occupational rehabilitation. He encourages national and local civic leaders to educate the public about terror-related stress.
Dr. Leon-Silva advises U.S. psychiatrists not to be ashamed to reveal their fears after a terrorist atrocity. “Sometimes expressing how the event impacts you will help the patient be more communicative and will more extensively show the patient’s symptoms.”
“In order to provide effective care to our patients it is necessary to have clear ideas on how to follow criteria for diagnosis and as a consequence for treatment,” Dr. Corvalan says. “The field at times is confusing; patients do not always follow the diagnostic criteria. The needs of the moment, limitations of recourses, intensity and variety of symptoms, urgency of the situation, etc., all conspire to make the job more difficult.”
Patients with anthrax-related anxiety should be encouraged to “try to function as normally as possible and keep an open communication with peers and those who they look to for information,” Dr. Frank notes. Dr. Allen adds that his patients with anthrax-inspired stress have responded well to breathing, meditation and other relaxation techniques.
Treatment of patients who are severely traumatized and exhibit true PTSD symptoms will vary based on severity of exposure, history of prior PTSD, and existence of comorbidities. A combination of pharmacological and psychosocial therapy is the common first-line treatment.
The selective serotonin reuptake inhibitor (SSRI) sertraline is specifically indicated for treating confirmed PTSD symptoms, and several studies have documented the agent’s effectiveness for this use.14,15 Dr. Frank recommends dosages between 50 and 200 mg/d depending on the patient’s body weight or complaint of side effects (e.g., diarrhea, nausea, or sexual dysfunction). Other SSRIs, as well as tricyclics and MAO inhibitors, are alternatives. Fluoxetine, amitriptyline, phenelzine, and imipramine have all been found more effective than a placebo;16-18 paroxetine also has been shown effective in specific populations.19
Kenneth S. Thompson, MD, a Pittsburgh-based disaster psychiatrist who helped coordinate Oklahoma City’s emergency psychiatry effort after the 1995 bombing, identified four stages that the public works through after a major disaster:
- Mobilization. Rebuilding—or just surviving—is foremost on people’s minds immediately after a traumatic event. Many people either throw themselves headfirst into the recovery and cleanup effort, or assist grieving families that have been hardest hit by the disaster. Others fear for their safety and leave town. Feelings of grief and loss are set aside to focus on the needs of the moment.
- Self-importance. As the media reports on their efforts to put their city—and their lives—back together, people at this stage tend to feel they are part of something. Those who have lost family members and coworkers seem to be coping well at this point, and feel as though they can draw ample moral support from friends and neighbors.
- Abandonment. Once the dust settles and the media coverage dies down, people who lost loved ones are left to confront their grief alone. Those who witnessed the tragedy, or who know someone who was killed or injured in the incident, must confront their demons one on one. It is at this point that PTSD and other psychiatric disorders can set in. Those who did not lose a friend or relative feel a more general sense of loss. Worse still, there may be “a disaster after the disaster,” in which a political official or emergency services officer is charged with some type of wrongdoing or abuse of power. People then feel used and betrayed.
- Acceptance. People begin to seek psychiatric or other help in dealing with the trauma, and begin to come to terms with their loss.
Benzodiazapenes also may be prescribed to manage PTSD symptoms. Patients should be counseled against taking these sedating agents in the daytime, however, as they can lead to fogginess, detachment, and trouble functioning.
Assessing the patient’s available social support also is crucial to PTSD treatment. “Do patients talk to other people about the event?” Dr. Frank asks. “Are they trying to get back to a daily routine? Can they make sense of this experience? Are they incorporating the event into a world view?”
Dr. Thompson, the Pittsburgh disaster psychiatrist, agrees. Psychiatrists should encourage their patients to talk more about their trauma and how fear is affecting their lives. “We don’t discuss with our trauma patients as much as we might what the experience has been like for them,” he says.
Small-group therapy is the most conducive approach to psychotherapy for PTSD, according to Dr. Frank, although individual counseling can work in many cases. Several studies have found group therapy effective,20,21 and 12-step group therapy has shown promise in PTSD patients with comorbid substance abuse disorder.22
Managing fear
Just as people grieve and confront death in stages, Dr. Thompson, who helped coordinate Oklahoma City’s disaster psychiatry effort, has discovered that the public usually employs a similar subconscious process to cope with a traumatic event (Box 4).
But Americans have had no time to recover. As U.S. troops seek justice in Afghanistan, back home people grapple with the threat of anthrax contamination and the prospect of another terrorist attack. The ominously enhanced presence of security at airports, major bridges, sporting and entertainment events, and in other aspects of everyday life, has further fueled the sensation that all is not right.
“The September 11 tragedy brings trauma home,” adds Arshad Husain, MD, professor and chief of child and adolescent psychiatry and director of the International Center for Psychosocial Trauma at the University of Missouri-Columbia. “The anthrax scare and the Nov. 12 plane crash of American Airlines Flight 587 only further remind people of their vulnerability and fears. If the anthrax scare were an accident, people would have been relieved. Since the plane crash was ruled an accident, it has offered people a chance to feel more in control. Accidents can be fixed with better maintenance. Terrorism cannot.”
Dr. Katz of New York City and other disaster psychiatrists are urging their colleagues to help manage public fear by reaching out through community efforts.
Dr. Katz is president of the volunteer group Disaster Psychiatry Outreach, which helped coordinate the city’s post-Sept. 11 trauma psychiatry effort. Visitors waiting at New York’s Family Assistance Center, a referral and help center for people who lost family and friends in the World Trade Center attack, were approached by Dr. Katz and other colleagues to let them know that psychiatric services were available if needed. By doing this, he says, Disaster Psychiatry Outreach clinicians have identified, treated, and referred scores of patients with terror-related stress who otherwise would have gone untreated.
Joseph Dorzab, MD, of the Holt-Krock Clinic in Fort Smith, Ark., also has offered his services. Members of his clinic’s psychiatry department have made several TV appearances, and have given and coordinated area lectures. Working with the local mental health association, the department also is starting a community forum called Mental Health Mondays, an open discussion group with coffee and cookies at a local coffee shop.
In Pittsburgh, Dr. Thompson is encouraging psychiatrists to educate their communities about how traumatic events affect the public. He proposes:
- Staging community meetings to brief religious and other leaders on how to manage traumatized people;
- Informing local news editors about the nature of psychiatric disorders;
- Instructing school administrators about detecting signs of distress in children;
- Contacting local government officials to offer input in devising the town’s emergency response plan.
Psychiatrists also can educate themselves about managing public trauma, thanks to scores of studies that have been done in recent years following major man-made and natural disasters, from Mount St. Helens and Hurricane Andrew, to Chernobyl and the Yom Kippur War. Dr. Thompson urges psychiatrists to seek out the papers of prominent leaders in trauma-related psychiatry, mentioning studies by Carol North, MD, Betty Pfefferbaum, MD, and Robert Ursano, MD, as examples. Other sources include the Web sites of the American Psychiatric Association and National Center for PTSD. (See Related Resources.)
In the end, psychiatrists have been well primed for dealing with public disaster—just by treating individual patients whose psychiatric disorders emanated from everyday life, Dr. Thompson says. “Psychiatrists know more about trauma than they recognize.”
- National Center for PTSD Web site
- National Institute of Mental Health:
- Linenthal EJ. The Unfinished Bombing: Oklahoma City in American Memory. Oxford University Press, 2001.
- Norwood AE, Ursano RJ, Fullerton CS. Disaster psychiatry: principles of practice. Psychiatr Q. 2000; 71(3):207-226.
- American Psychiatric Association Web site:
- The Psychiatric Training Manual for Teachers and Mental Health Professionals
Drug brand names
- Amitriptyline • Elavil
- Bupropion • Wellbutrin
- Fluoxetine • Prozac
- Imipramine • Tofranil
- Paroxetine • Paxil
- Phenelzine • Nardil
- Sertraline • Zoloft
Since September 11, America has carried on under a cloud of fear. Though the cloud is lifting, it will not disappear for months or years. The terrorist attacks on New York City and Washington, DC, the resultant military action in Afghanistan, and the anthrax scare—combined with pervasive, nagging doubts about homeland security and the specter of another possible future terrorist attack—all are straining the nation’s collective emotional well-being.
Psychiatrists in America have reported new cases of terror-inspired acute stress disorder, anxiety, depression, and other illnesses, as well as recurrences of posttraumatic stress disorder (PTSD) in existing patients, in the weeks after the recent attacks and the anthrax scare. What will be the impact on psychiatric practice in the coming months and years?
“We are all at ground zero,” says Kenneth S. Thompson, MD, of Pittsburgh, an experienced disaster psychiatrist. But he and other subspecialists have identified four critical areas in which psychiatrists should be prepared:
- Identifying how terrorist attacks and scares can exacerbate symptoms in patients now in your practice;
- Diagnosing PTSD among comorbid conditions present in existing or new patients;
- Treating—and avoiding over-treatment—of patients with acute stress disorder and PTSD;
- Managing fear in your communities—in response to the Sept. 11 attacks, to the anthrax scare, or in anticipation of an impending catastrophe.
To bring you this special report, the editors of Current Psychiatry have reviewed the literature and interviewed psychiatrists nationwide and in countries such as Israel and Colombia, where terrorism has been a fact of life for years (see “PTSD lessons from Israel, Colombia,”).
Terror and your patients
Which symptoms are you most likely to see in existing patients subsequent to recent events? In the weeks following the Sept. 11 attacks, psychiatrists reported the most commonly seen symptoms as increased anxiety and worsened depression. Sleep disturbances, agoraphobia, suicidality, and severe reactions among patients with personality disorders also were reported.
Patients with previous PTSD or exposure to trauma face a high risk of new or recurrent PTSD in the wake of Sept. 11 than do those not previously exposed to trauma.1 War veterans with prior posttraumatic symptoms have been particularly prone to recurrent PTSD after the attacks. James Allen, MD, of the Department of Psychiatry and Behavioral Sciences at the University of Oklahoma Health Sciences Center, calls this the “additive effect”: patients traumatized by military service in Vietnam experience a recurrence after seeing a major disaster or atrocity. Dr. Allen, who was extensively involved with Oklahoma City’s disaster psychiatry effort after the 1995 bombing there, recalls seeing patients who were traumatized in Vietnam suffer a recurrence after the Alfred P. Murrah Building attack, and then another relapse after Sept. 11.
“The Sept. 11 attacks were very similar to the war for them,” says Juan Corvalan, MD, of the PTSD Unit of the St. Louis Veterans Administration Medical Center, referring to the numerous war veterans he treated after the atrocities. “Seeing it on TV triggered many memories.” By early November, however, many who experienced recurrent PTSD had returned to their pre-Sept. 11 mental states.
Craig Katz, MD, director of emergency psychiatry services at New York’s Mount Sinai Medical Center, says that a patient’s psychiatric history is crucial to determining risk for PTSD or other terror-related sequelae:
“You can recognize that a given person is at high risk for PTSD post-trauma, based on any combination of these factors—having a psychiatric history, past trauma, high exposure to the event, psychosocial problems pre-disaster, or lack of supports post-disaster.”
The clinical interview is a vital tool in assessing patients with suspected PTSD or posttraumatic sequelae, says Arieh Shalev, MD, of the department of psychiatry at Hadassah University Hospital in Jerusalem, Israel. “It provides the opportunity to discuss the traumatic event with the patient, and to listen to his or her perceptions of the event and its effects” in order to carefully appraise the patient’s symptoms.2
The guidelines set forth in the Diagnostic and Statistical Manual for Mental Disorders, Fourth Edition (DSM-IV) remain the gold standard for confirming a diagnosis of PTSD and discerning long-term posttraumatic sequelae from temporary acute stress disorder (Box 1). The guidelines have proved far from foolproof, however, and the existence of psychiatric comorbidities often clouds the picture.
- Exposure to a traumatic event with both of the following present:
- The traumatic event is persistently reexperienced in one or more of the following ways:
- Persistent avoidance of stimuli associated with the trauma and numbing of general responsiveness (not present before the trauma), as indicated by three or more of the following:
- Persistent symptoms of increased arousal (not present before the trauma), as indicated by two or more of the following:
- Duration of symptoms in criteria B, C or D exceeds 1 month.
- Disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
Specify if; Acute: if duration of symptoms is less than 3 months.
Chronic: if symptoms persist 3 months or more.
With delayed onset: if onset of symptoms is at least 6 months after the stressor.
Acute stress disorder, whose symptom pattern is similar to that of PTSD, is distinguished from PTSD because the symptom pattern must occur and resolve within 4 weeks of the traumatic event. If the symptoms persist for more than 1 month and meet the criteria for PTSD, the diagnosis is changed from acute stress disorder to PTSD.
Differential diagnosis of PTSD
Patients with PTSD are more likely to have substantial psychiatric comorbidity than are those without the disorder.3 Possible reasons include suspected self-medication of PTSD symptoms, particularly among patients with substance abuse, and the possible overreporting of symptoms by patients. Psychiatrists should maintain a high level of suspicion for PTSD when managing a new or existing patient with psychopathology.
Citing data from the National Comorbidity Study of the Institute for Social Research at the University of Michigan, Kessler and others in 1995 noted that more than 80 percent of individuals with PTSD meet criteria for at least one other psychiatric diagnosis. Roughly half of PTSD sufferers met criteria for three or more comorbidities.3
Kathleen Brady, MD, professor of psychiatry at the Medical University of South Carolina in Charleston, noted in a 1997 study that affective disorders, other anxiety disorders, somatization, substance abuse, and dissociative disorders are common comorbidities of PTSD.5 Dr. Shalev and colleagues in one study found that a history of major depressive disorder may increase the severity of posttraumatic morbidity.6 Dr. Brady and others also have found that PTSD patients with a comorbid substance abuse disorder experience severe PTSD symptoms while in a withdrawal state.7
| Disorder | Symptoms that overlap with PTSD |
|---|---|
| Adjustment disorder | Extreme response to stressor. Stressor is not necessarily extreme in nature (e.g., spouse leaving, being fired), and the response might not meet criteria for PTSD.4 |
| Depression | Diminished interest, restricted range of affect, sleep difficulties, or poor concentration.5 |
| Dissociative disorders | Inability to recall important information about past trauma, sense of detachment from oneself, derealization, nightmares, flashbacks, startle responses, or lack of affective response (e.g., onset of dissociative fugue may be tied to past trauma).4 |
| Generalized anxiety | Irritability, hypervigilance, or increased startle reflex.5 |
| Obsessive-compulsive disorder | Recurrent intrusive thoughts (not related to trauma in obsessive-compulsive disorder).4 |
| Panic attacks | Heart palpitations or increased heart rate, sense of detachment, nausea or abdominal distress.4 |
| Psychosis | Illusions, hallucinations, or other perceptual disturbances (may be confused with flashbacks in PTSD).4 |
| Substance abuse disorder | Hallucinations, illusions, diminished interest in or avoidance of significant activities, or social estrangement.4 |
PTSD often is overlooked in the presence of other psychiatric diagnoses. Meuser et al in 1998 studied 275 patients with schizophrenia and bipolar disorder. As many as 98 percent of patients reported lifetime exposure to at least one traumatic event. The researchers found diagnosable PTSD in 119 (43 %) of the subjects, but only three (2%) had the diagnosis in their charts.8
In a later study, Dr. Brady and others cited substantial symptom overlap between PTSD and other psychiatric diagnoses, particularly major depressive disorder. This can contribute to underdiagnosis of PTSD, the researchers found.7 (Box 2).
Children also have been experiencing stress disorders since Sept. 11, says Arshad Husain, MD, professor and chief of child and adolescent psychiatry and director of the International Center for Psychosocial Trauma at the University of Missouri-Columbia. Such disorders manifest as sleep disturbances, anxiety, hyperarousal/hyperactivity, and nightmares.
Young children regress and cling to their parents, and are frightened of the dark or noises, Dr, Husain notes. Those who are toilet-trained can suddenly wet the bed, become neurotic, and demand attention. School-age children are more fearful; they may not want to go to school, their schoolwork may decline, and they may have trouble paying attention. Dr. Husain suggests discussing the trauma and devising a plan of action with them in case the trauma recurs.
The media’s role in reporting on the aftermath of the attacks—and triggering traumatic reactions as an unintended consequence—cannot be overlooked. Two recent studies performed after the Oklahoma City bombing suggest that television reports of that atrocity precipitated PTSD symptoms in middle-school children 7 weeks after the bombing,23 and in geographically distant sixth-graders 2 years after the attack.12 It was not clear whether any of these students had prior PTSD or other psychopathology.
Psychiatric education in the schools is especially crucial in light of the school violence that has occurred in America in recent years. Dr. Husain believes that the children who commit violence are victims of abuse. If teachers early on can identify children who show evidence of stress disorders, they can refer them to trained psychiatrists, catching those who need help before tragedies occur. “It is the psychiatric equivalent of CPR,” Dr. Husain says.
Dr. Brady recommends that psychiatrists and primary care physicians routinely screen patients for exposure to traumatic events. Ask patients specifically about their reaction to such events and encourage them to talk about it. Patients often feel either guilty or embarrassed about the traumatic event, or do not believe it affects their presenting complaints, she notes. Other approaches may be needed to identify the risk of PTSD in children (Box 3).
Identifying a traumatic event of an extreme nature, for example, a life-threatening experience, is key to diagnosing PTSD in the presence of comorbidities, Dr. Corvalan says. “Some of the symptoms—such as avoidance, numbing, and increased arousal—are present in other disorders and may have occurred before exposure to the traumatic event.” If they did, he says, PTSD is ruled out.
Gauging the extent of the patient’s exposure to the traumatic event is critical to determining the likelihood of PTSD onset. Dr. Allen, of Oklahoma City, points to studies that show that the closer and longer the patient has been exposed to a catastrophic event, the more likely he or she will develop PTSD.9,10
Julia Frank, MD, associate professor and director of student education and psychiatry at George Washington University in Washington, DC, suggests screening for symptoms that are unique to PTSD as stated in the DSM-IV, such as nightmares, difficulty remembering the traumatic event, and extreme reactions to reminders of the trauma. She also proposes analyzing the past event and the patient’s reaction to it to confirm that it is a source of trauma.
Patients with PTSD symptoms are easily startled by loud or piercing noises. Dr. Shalev says this characteristic sets true PTSD cases apart from other psychopathology, particularly depression. In one study, Israeli combat veterans with PTSD exhibited a more pronounced heart rate and skin conductance when exposed to auditory stimuli than did combat veterans with no PTSD symptoms.11
Drs. Allen and Frank note that patients who have anthrax-related fears and no prior PTSD symptoms are not likely to develop PTSD. They may, however, manifest symptoms of chronic fatigue, fibromyalgia, and generalized anxiety disorder. Patients may be jumpy, intense, or lethargic, with autonomic instability and rapid heart rate. They may feel alienated and mistrustful of the government. A nonspecific stress disorder and mixed anxiety depression are other possible effects.
Who to treat—and how
Psychiatrists nationwide have reported increased patient presentations after the Sept. 11 attacks and throughout the anthrax scare. Studies conducted after the Oklahoma City bombing also suggest that psychiatrists could be seeing more patients in the coming months.12,13 As caseloads increase, so do the questions about who to treat, how, and how to avoid the possibility of overtreatment.
While many clinicians in the United States recently received their first taste of post-terror psychiatry, those in more violent parts of the world are well-versed in helping their patients manage fear.
Israel has repeatedly been at war throughout its 53-year history. During “peacetime,” terrorism and senseless violence have been a way of life.
“Sadly, Israel’s citizens and its medical and paramedical communities have accrued extensive experience in dealing with the ongoing threat of war and terrorist attacks and their sequelae,” says Zeev Kaplan, MD, director of the Beer-Sheva Mental Health Center and professor of psychiatry at the Ben Gurion University School of Medicine in Beer-Sheva.
Similarly, Colombia is a country long plagued by terrorist and gang violence. PTSD has been on the rise the past 5 years, according to Javier Leon-Silva, MD, chief of psychiatry at the Fundación Santafe de Bogotá. “There is not a single day without a terrorist attack in the news,” Dr. Leon-Silva notes. In addition, two major natural disasters in the last 20 years—the Armero flood and the earthquake in the coffee region—have resulted in tens of thousands of casualties.
Exposure to terror in Israel is widespread—be it direct, as a victim or witness, or secondary, as a victim’s close friend or relative. Recurrent PTSD, brought on by direct and indirect exposure, is common, Dr. Kaplan says. Holocaust survivors, almost as numerous within Israel’s population as combat veterans, have been especially prone to recurrent PTSD.
Children are particularly susceptible to PTSD. In Israel, someone’s parent, sibling or classmate often is among the casualties of a terrorist attack, Dr. Kaplan notes. In Colombia, “children grow up influenced by stories about family members or friends who have been victims of the consequences of war and terror, and by strict family security measures concerning behavior,” Dr. Leon-Silva adds.
Because of the Middle East’s volatile history, most of Israel’s psychiatric professionals have hands-on experience in treating traumatized patients in both military and civilian settings. Joseph Zohar, MD, chairman of Israel’s Consortium on PTSD, says that most psychiatrists have served at some point in the Israeli Defense Forces.
Further, as both Israel’s medical community and the public have learned more about PTSD and post-terror anxiety, physicians can now identify affected people more rapidly, and can refer them for treatment, Dr. Kaplan says. Civilians and veterans have access to five regional trauma and post trauma centers. Educators are trained to detect behavioral changes in the young, and Israel’s children are followed into adulthood to assess the long-term effects of terrorist events.
Colombia’s psychiatrists are also well-qualified to treat terror-inspired psychiatric illness, Dr. Leon-Silva says. However, most people in the impoverished nation cannot afford needed medicines, and psychiatrists are hard-pressed to reach many disaster or terror victims.
Dr. Zohar urges psychiatrists here to attend seminars and workshops on PTSD and acute stress reaction. He says such seminars in Israel have taught clinicians the long-term effects of exposure to terror and its effect on families, as well as how to help patients manage acute stress reactions.
Dr. Kaplan feels his U.S. counterparts should incorporate a multidisciplinary approach that addresses bio-medical, psychotherapeutic, familial, and social/occupational rehabilitation. He encourages national and local civic leaders to educate the public about terror-related stress.
Dr. Leon-Silva advises U.S. psychiatrists not to be ashamed to reveal their fears after a terrorist atrocity. “Sometimes expressing how the event impacts you will help the patient be more communicative and will more extensively show the patient’s symptoms.”
“In order to provide effective care to our patients it is necessary to have clear ideas on how to follow criteria for diagnosis and as a consequence for treatment,” Dr. Corvalan says. “The field at times is confusing; patients do not always follow the diagnostic criteria. The needs of the moment, limitations of recourses, intensity and variety of symptoms, urgency of the situation, etc., all conspire to make the job more difficult.”
Patients with anthrax-related anxiety should be encouraged to “try to function as normally as possible and keep an open communication with peers and those who they look to for information,” Dr. Frank notes. Dr. Allen adds that his patients with anthrax-inspired stress have responded well to breathing, meditation and other relaxation techniques.
Treatment of patients who are severely traumatized and exhibit true PTSD symptoms will vary based on severity of exposure, history of prior PTSD, and existence of comorbidities. A combination of pharmacological and psychosocial therapy is the common first-line treatment.
The selective serotonin reuptake inhibitor (SSRI) sertraline is specifically indicated for treating confirmed PTSD symptoms, and several studies have documented the agent’s effectiveness for this use.14,15 Dr. Frank recommends dosages between 50 and 200 mg/d depending on the patient’s body weight or complaint of side effects (e.g., diarrhea, nausea, or sexual dysfunction). Other SSRIs, as well as tricyclics and MAO inhibitors, are alternatives. Fluoxetine, amitriptyline, phenelzine, and imipramine have all been found more effective than a placebo;16-18 paroxetine also has been shown effective in specific populations.19
Kenneth S. Thompson, MD, a Pittsburgh-based disaster psychiatrist who helped coordinate Oklahoma City’s emergency psychiatry effort after the 1995 bombing, identified four stages that the public works through after a major disaster:
- Mobilization. Rebuilding—or just surviving—is foremost on people’s minds immediately after a traumatic event. Many people either throw themselves headfirst into the recovery and cleanup effort, or assist grieving families that have been hardest hit by the disaster. Others fear for their safety and leave town. Feelings of grief and loss are set aside to focus on the needs of the moment.
- Self-importance. As the media reports on their efforts to put their city—and their lives—back together, people at this stage tend to feel they are part of something. Those who have lost family members and coworkers seem to be coping well at this point, and feel as though they can draw ample moral support from friends and neighbors.
- Abandonment. Once the dust settles and the media coverage dies down, people who lost loved ones are left to confront their grief alone. Those who witnessed the tragedy, or who know someone who was killed or injured in the incident, must confront their demons one on one. It is at this point that PTSD and other psychiatric disorders can set in. Those who did not lose a friend or relative feel a more general sense of loss. Worse still, there may be “a disaster after the disaster,” in which a political official or emergency services officer is charged with some type of wrongdoing or abuse of power. People then feel used and betrayed.
- Acceptance. People begin to seek psychiatric or other help in dealing with the trauma, and begin to come to terms with their loss.
Benzodiazapenes also may be prescribed to manage PTSD symptoms. Patients should be counseled against taking these sedating agents in the daytime, however, as they can lead to fogginess, detachment, and trouble functioning.
Assessing the patient’s available social support also is crucial to PTSD treatment. “Do patients talk to other people about the event?” Dr. Frank asks. “Are they trying to get back to a daily routine? Can they make sense of this experience? Are they incorporating the event into a world view?”
Dr. Thompson, the Pittsburgh disaster psychiatrist, agrees. Psychiatrists should encourage their patients to talk more about their trauma and how fear is affecting their lives. “We don’t discuss with our trauma patients as much as we might what the experience has been like for them,” he says.
Small-group therapy is the most conducive approach to psychotherapy for PTSD, according to Dr. Frank, although individual counseling can work in many cases. Several studies have found group therapy effective,20,21 and 12-step group therapy has shown promise in PTSD patients with comorbid substance abuse disorder.22
Managing fear
Just as people grieve and confront death in stages, Dr. Thompson, who helped coordinate Oklahoma City’s disaster psychiatry effort, has discovered that the public usually employs a similar subconscious process to cope with a traumatic event (Box 4).
But Americans have had no time to recover. As U.S. troops seek justice in Afghanistan, back home people grapple with the threat of anthrax contamination and the prospect of another terrorist attack. The ominously enhanced presence of security at airports, major bridges, sporting and entertainment events, and in other aspects of everyday life, has further fueled the sensation that all is not right.
“The September 11 tragedy brings trauma home,” adds Arshad Husain, MD, professor and chief of child and adolescent psychiatry and director of the International Center for Psychosocial Trauma at the University of Missouri-Columbia. “The anthrax scare and the Nov. 12 plane crash of American Airlines Flight 587 only further remind people of their vulnerability and fears. If the anthrax scare were an accident, people would have been relieved. Since the plane crash was ruled an accident, it has offered people a chance to feel more in control. Accidents can be fixed with better maintenance. Terrorism cannot.”
Dr. Katz of New York City and other disaster psychiatrists are urging their colleagues to help manage public fear by reaching out through community efforts.
Dr. Katz is president of the volunteer group Disaster Psychiatry Outreach, which helped coordinate the city’s post-Sept. 11 trauma psychiatry effort. Visitors waiting at New York’s Family Assistance Center, a referral and help center for people who lost family and friends in the World Trade Center attack, were approached by Dr. Katz and other colleagues to let them know that psychiatric services were available if needed. By doing this, he says, Disaster Psychiatry Outreach clinicians have identified, treated, and referred scores of patients with terror-related stress who otherwise would have gone untreated.
Joseph Dorzab, MD, of the Holt-Krock Clinic in Fort Smith, Ark., also has offered his services. Members of his clinic’s psychiatry department have made several TV appearances, and have given and coordinated area lectures. Working with the local mental health association, the department also is starting a community forum called Mental Health Mondays, an open discussion group with coffee and cookies at a local coffee shop.
In Pittsburgh, Dr. Thompson is encouraging psychiatrists to educate their communities about how traumatic events affect the public. He proposes:
- Staging community meetings to brief religious and other leaders on how to manage traumatized people;
- Informing local news editors about the nature of psychiatric disorders;
- Instructing school administrators about detecting signs of distress in children;
- Contacting local government officials to offer input in devising the town’s emergency response plan.
Psychiatrists also can educate themselves about managing public trauma, thanks to scores of studies that have been done in recent years following major man-made and natural disasters, from Mount St. Helens and Hurricane Andrew, to Chernobyl and the Yom Kippur War. Dr. Thompson urges psychiatrists to seek out the papers of prominent leaders in trauma-related psychiatry, mentioning studies by Carol North, MD, Betty Pfefferbaum, MD, and Robert Ursano, MD, as examples. Other sources include the Web sites of the American Psychiatric Association and National Center for PTSD. (See Related Resources.)
In the end, psychiatrists have been well primed for dealing with public disaster—just by treating individual patients whose psychiatric disorders emanated from everyday life, Dr. Thompson says. “Psychiatrists know more about trauma than they recognize.”
- National Center for PTSD Web site
- National Institute of Mental Health:
- Linenthal EJ. The Unfinished Bombing: Oklahoma City in American Memory. Oxford University Press, 2001.
- Norwood AE, Ursano RJ, Fullerton CS. Disaster psychiatry: principles of practice. Psychiatr Q. 2000; 71(3):207-226.
- American Psychiatric Association Web site:
- The Psychiatric Training Manual for Teachers and Mental Health Professionals
Drug brand names
- Amitriptyline • Elavil
- Bupropion • Wellbutrin
- Fluoxetine • Prozac
- Imipramine • Tofranil
- Paroxetine • Paxil
- Phenelzine • Nardil
- Sertraline • Zoloft
1. Breslau N, Chilcoat HD, Kessler RC, Davis GC. Previous exposure to trauma and PTSD effects of subsequent trauma: results from the Detroit Area Survey of Trauma. Am J Psychiatry. 1999;156(6):902-7.
2. Shalev AY. What is posttraumtic stress disorder? J Clin Psychiatry. 2001;62(Suppl 17):4-10.
3. Kessler RC, Sonnega A, et al. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry. 1995;52(12):1048-60
4. Diagnostic and Statistical Manual of Mental Disorders, 4th ed. Washington, DC: American Psychiatric Association, 2000.
5. Brady KT. Posttraumatic stress disorder and comorbidity: recognizing the many faces of PTSD. J Clin Psychiatry. 1997;58 Suppl 9:12-5.
6. Shalev AY, Freedman S, Peri T, et al. Prospective study of posttraumatic stress disorder and depression following trauma. Am J Psychiatry. 1998;155:630-7.
7. Brady KT, Killeen TK, Brewerton T, Lucerini S. Comorbidity of psychiatric disorders and posttraumatic stress disorder. J Clin Psychiatry 2000;61 Suppl 7:22-32.
8. Mueser KT, Goodman LB, et al. Trauma and posttraumatic stress disorder in severe mental illness. J Consult Clin Psychol. 1998;66(3):493-9.
9. Cloitre M, Cohen LR, Edelman RE, Han H. Posttraumatic stress disorder and extent of trauma exposure as correlates of medical problems and perceived health among women with childhood abuse. Women Health. 2001;34(3):1-17.
10. Hodgins GA, Creamer M, Bell R. Risk factors for posttrauma reactions in police officers: a longitudinal study. J Nerv Ment Dis. 2001;189(8):541-7.
11. Orr SP, Solomon Z, Peri T, et al. Physiologic responses to loud tones in Israeli veterans of the 1973 Yom Kippur War. Biol Psychiatry. 1997;41:319-26.
12. Pfefferbaum B, Seale TW, et al. Posttraumatic stress two years after the Oklahoma City Bombing in youths geographically distant from the explosion. Psychiatry 2000;63(4):358-370.
13. Smith DW, Christiansen EH, Vincent R, Hann N. Population effects of the bombing of Oklahoma City. J Oklahoma State Med Association. 1999;92(4):193-198.
14. Londborg PD, Hegel MT, et al. Sertraline treatment of posttraumatic stress disorder: results of 24 weeks of open-label continuation treatment. J Clin Psychiatry. 2001;62(5):325-31.
15. Davidson JR. Pharmacotherapy of generalized anxiety disorder. J Clin Psychiatry. 2001;62 Suppl 11:46-50.discussion 51-2.
16. Connor KM, Sutherland SM, et al. Fluoxetine in post-traumatic stress disorder. Randomised, double-blind study. Br J Psychiatry. 1999;175:17-22.
17. Davidson J, Kudler H, et al. Treatment of posttraumatic stress disorder with amitriptyline and placebo. Arch Gen Psychiatry. 1990;47(3):259-66.
18. Kosten TR, Frank JB, et al. Pharmacotherapy for posttraumatic stress disorder using phenelzine or imipramine. J Nerv Ment Dis. 1991;179(6):366-70.
19. Smajkic A, Weine S, et al. Sertraline, paroxetine, and venlafaxine in refugee posttraumatic stress disorder with depression symptoms. J Trauma Stress. 2001;14(3):445-52.
20. Wolfsdorf BA, Zlotnick C. Affect management in group therapy for women with posttraumatic stress disorder and histories of childhood sexual abuse. J Clin Psychol 2001 Feb;57(2):169-81.
21. Jones L, Brazel D, et al. Group therapy program for African-American veterans with posttraumatic stress disorder. Psychiatr Serv. 2000;51(9):1177-9.
22. Ouimette P, Humphreys K, et al. Self-help group participation among substance use disorder patients with posttraumatic stress disorder. J Subst Abuse Treat. 2001;20(1):25-32.
23. Pfefferbaum B, Nixon SJ, Tivis RD, et al. Television exposure in children after a terrorist incident. Psychiatry. 2001;64(3):202-11.
1. Breslau N, Chilcoat HD, Kessler RC, Davis GC. Previous exposure to trauma and PTSD effects of subsequent trauma: results from the Detroit Area Survey of Trauma. Am J Psychiatry. 1999;156(6):902-7.
2. Shalev AY. What is posttraumtic stress disorder? J Clin Psychiatry. 2001;62(Suppl 17):4-10.
3. Kessler RC, Sonnega A, et al. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry. 1995;52(12):1048-60
4. Diagnostic and Statistical Manual of Mental Disorders, 4th ed. Washington, DC: American Psychiatric Association, 2000.
5. Brady KT. Posttraumatic stress disorder and comorbidity: recognizing the many faces of PTSD. J Clin Psychiatry. 1997;58 Suppl 9:12-5.
6. Shalev AY, Freedman S, Peri T, et al. Prospective study of posttraumatic stress disorder and depression following trauma. Am J Psychiatry. 1998;155:630-7.
7. Brady KT, Killeen TK, Brewerton T, Lucerini S. Comorbidity of psychiatric disorders and posttraumatic stress disorder. J Clin Psychiatry 2000;61 Suppl 7:22-32.
8. Mueser KT, Goodman LB, et al. Trauma and posttraumatic stress disorder in severe mental illness. J Consult Clin Psychol. 1998;66(3):493-9.
9. Cloitre M, Cohen LR, Edelman RE, Han H. Posttraumatic stress disorder and extent of trauma exposure as correlates of medical problems and perceived health among women with childhood abuse. Women Health. 2001;34(3):1-17.
10. Hodgins GA, Creamer M, Bell R. Risk factors for posttrauma reactions in police officers: a longitudinal study. J Nerv Ment Dis. 2001;189(8):541-7.
11. Orr SP, Solomon Z, Peri T, et al. Physiologic responses to loud tones in Israeli veterans of the 1973 Yom Kippur War. Biol Psychiatry. 1997;41:319-26.
12. Pfefferbaum B, Seale TW, et al. Posttraumatic stress two years after the Oklahoma City Bombing in youths geographically distant from the explosion. Psychiatry 2000;63(4):358-370.
13. Smith DW, Christiansen EH, Vincent R, Hann N. Population effects of the bombing of Oklahoma City. J Oklahoma State Med Association. 1999;92(4):193-198.
14. Londborg PD, Hegel MT, et al. Sertraline treatment of posttraumatic stress disorder: results of 24 weeks of open-label continuation treatment. J Clin Psychiatry. 2001;62(5):325-31.
15. Davidson JR. Pharmacotherapy of generalized anxiety disorder. J Clin Psychiatry. 2001;62 Suppl 11:46-50.discussion 51-2.
16. Connor KM, Sutherland SM, et al. Fluoxetine in post-traumatic stress disorder. Randomised, double-blind study. Br J Psychiatry. 1999;175:17-22.
17. Davidson J, Kudler H, et al. Treatment of posttraumatic stress disorder with amitriptyline and placebo. Arch Gen Psychiatry. 1990;47(3):259-66.
18. Kosten TR, Frank JB, et al. Pharmacotherapy for posttraumatic stress disorder using phenelzine or imipramine. J Nerv Ment Dis. 1991;179(6):366-70.
19. Smajkic A, Weine S, et al. Sertraline, paroxetine, and venlafaxine in refugee posttraumatic stress disorder with depression symptoms. J Trauma Stress. 2001;14(3):445-52.
20. Wolfsdorf BA, Zlotnick C. Affect management in group therapy for women with posttraumatic stress disorder and histories of childhood sexual abuse. J Clin Psychol 2001 Feb;57(2):169-81.
21. Jones L, Brazel D, et al. Group therapy program for African-American veterans with posttraumatic stress disorder. Psychiatr Serv. 2000;51(9):1177-9.
22. Ouimette P, Humphreys K, et al. Self-help group participation among substance use disorder patients with posttraumatic stress disorder. J Subst Abuse Treat. 2001;20(1):25-32.
23. Pfefferbaum B, Nixon SJ, Tivis RD, et al. Television exposure in children after a terrorist incident. Psychiatry. 2001;64(3):202-11.
Excessive daytime sleepiness: Diagnosing the causes
Untreated excessive daytime sleepiness (EDS) results in compromised quality of life, reduced productivity, and public safety concerns.1 Obstructive sleep apnea (OSA), restless legs syndrome, circadian rhythm disorders, and narcolepsy are frequently underdiagnosed sleep disorders that can cause EDS. These conditions commonly go undetected and untreated for several reasons:
- Patients may not recognize sleepiness as a legitimate medical concern.
- Physicians, with few exceptions, typically have little training in sleep disorders and limited time to diagnose them.2 Screening questions regarding sleep are typically absent.
- Definitive diagnostic tests are costly.
As a result, many patients go without appropriate sleep evaluations. Instead a depressive or other psychiatric disorder may be suspected because of the sleepy patient’s poor energy, hypersomnia, amotivation, irritability, and frustration. Because of ongoing behavioral symptoms, patients with an undiagnosed primary sleep disorder are often referred to psychiatrists. Thus, a clear understanding of the differential diagnosis of EDS is crucial.
Patients with sleep issues fall into three major categories:
- Patients with EDS.
- Individuals with insomnia, another large group often seen by psychiatrists. Generally, these patients are less hesitant than patients with EDS to seek help because of the marked distress they suffer nightly when trying to sleep. Insomniacs typically experience minimal EDS.
- Patients with unusual behaviors at night that range from arm waving to violent behaviors.
Assessing the sleepy patient
When evaluating a patient with sleep complaints, several valuable sources of data come into play.
Initially, observe the patient in the waiting room or office before starting the interview. Did the patient nod off while waiting for his or her appointment? Pay attention to any patient who appears sleepy—even if he or she denies having trouble staying awake. Over time, sleepy patients may have lost their perspective on alertness. Some patients have had EDS for so many years that they no longer recall what it is like to feel fully awake.
Collateral history is often important because family members generally observe the sleeping patient. The bed partner often provides valuable information about snoring, irregular breathing leg kicks, unplanned naps, and strained interpersonal relationships due to EDS. For the patient who does not have a bed partner, ask his or her travel companion, with whom the patient may have shared accommodations.
Unfortunately, few useful screening tests exist. Most questionnaires about sleepiness are neither very reliable nor valid. One of the better questionnaires, the Epworth Sleepiness Scale, helps confirm the presence of sleepiness with a score <8, differentiating the inability to stay awake from fatigue. (Box 1 can be cut out, copied, and handed to patients). This brief questionnaire also provides a useful measure of severity.3
The value of the Epworth scale is limited, however, because patient answers often are based on a specific time and context that may not be representative. Additional validated surveys include the Pittsburgh Sleep Quality Inventory and several that focus on OSA.4
How likely are you to doze off or fall asleep in the following situations, in contrast to feeling just tired? Even if you have not done some of these things recently, try to work out how each situation would affect you now. Use the scale below to choose the most appropriate number for each situation:
- 0 no chance of dozing
- 1 slight chance of dozing
- 2 moderate chance of dozing
- 3 high chance of dozing
| Chance of dozing | Situation |
|---|---|
| ○ | Sitting and reading |
| ○ | Watching TV |
| ○ | Sitting inactive in a public place (e.g., a theater or a meeting) |
| ○ | Sitting as a passenger in a car for an hour without a break |
| ○ | Lying down to rest in the afternoon when circumstances permit |
| ○ | Sitting and talking to someone |
| ○ | Sitting quietly after a lunch without alcohol |
| ○ | In a car, while stopped for a few minutes in traffic |
| Johns, M. Sleep 14:540-545, 1991. | |
Electroencephalographic (EEG) monitoring can accurately measure the patient’s degree of sleep disruption. This information is critical in understanding if a patient’s EDS is caused by a physiologic condition that prevents quality nocturnal sleep. At this time, however, no portable devices that employ EEG technology are used in clinical settings.
Additionally, none of the widely used screening devices that assess leg kicks indicate the presence of possible periodic limb movements.
Even though overnight pulse oximetry has been used to screen for sleep-disordered breathing,5 the technology has limitations. For one, most pulse oximeters do not provide information about sleep stage or body position. Some patients with significant sleep-disordered breathing lack adequate oxygen desaturations but have frequent EEG arousals due to sleep issues. In this case, pulse oximetry would generate a false negative result because EEG data is not collected. The inadequate sensitivity is most likely to occur with females and thin patients.
Oximetry provides only one or two types of data (oxygen saturation plus possibly heart rate), while other physiologic processes, e.g., body movement or sleep architecture, can repetitively be disrupted during sleep.
The most critical steps in detecting sleep disorders do not require technology or specialized expertise, but rather intuition and common sense. The psychiatrist should consider the possibility of a sleep disorder and incorporate pertinent questions into the clinical interview. Figure 1 lists sequential questions that might uncover specific sleep disorders. Once suspected, the decision whether to refer the patient to a sleep disorder center for diagnostic testing depends on the type of sleep disorder detected.
Diagnosing and treating OSA
Recent epidemiologic studies show that OSA affects at least 4% of men and 2% of women in the United States.6 Psychiatrists are virtually assured of seeing patients with undiagnosed OSA. The condition is caused by repeated collapse of the soft tissues surrounding the upper airway, decreasing airflow that is restored when the patient briefly awakens. Patients develop EDS because of sleep fragmented by frequent arousals.
Figure 1 THE SLEEPY PATIENT: Possible medical and psychiatric explanations
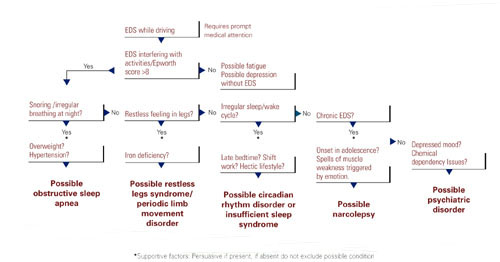
Obese patients are at higher risk than are patients at normal weight because of their body habitus. Alcohol or sedative medication use close to bedtime can aggravate OSA. These substances promote muscle relaxation and increase the arousal threshold, meaning that patients do not wake readily when apneas occur.
Long-term complications of untreated OSA include sleepiness leading to accidents, hypertension, cerebrovascular disease, and progressive obesity. New data associate OSA with multiple potential cardiovascular complications (arrhythmias, congestive heart failure, and myocardial infarction).7 Therefore, recognition and treatment are paramount.
The physical examination should focus on detecting nasal obstruction (having the patient sniff separately through each nostril can be helpful), big neck, crowded oropharynx (a low-hanging palate, reddened uvula, enlarged tonsils, large tongue size relative to oropharynx diameter) and jaw structure (particularly a small retrognathic mandible).
Referral for nocturnal polysomnography might be the next step. During a comprehensive sleep study, data is collected about respiratory, cardiovascular, and muscle activity at night, as well as the sounds the patient makes (e.g., snoring, coughing) when asleep. EEG monitoring also is performed. OSA may be diagnosed if repeated episodes of reduced airflow and oxygen desaturation are observed; these typically result in brief shifts in EEG frequency called arousals.
First-line interventions for OSA include avoidance of alcohol within 1 to 2 hours of bedtime, sleeping on the side instead of the back, weight loss (ideally with a regular exercise program), and nasal sprays for allergies.
If the first-line treatments for OSA are ineffective, nasal continuous positive airway pressure (CPAP) works well for almost all patients who adhere to the regimen.8 CPAP requires the patient to wear a nasal mask that delivers room air, splinting open the nasopharynx and the upper airway (Box 2). Some patients benefit from a brief trial of a sleeping medication, e.g., zolpidem or trazodone, for the first 1 to 2 weeks of nasal CPAP usage.

Nasal continuous positive airway pressure (CPAP) must be started in an observed setting so that the clinician can determine the optimal amount of positive pressure needed to keep the upper airway patent. CPAP can be started during the second half of a “split-night” sleep study after obstructive sleep apnea (OSA) has been diagnosed. Alternatively, the sleep laboratory might ask the patient to return for a second night for a trial of nasal CPAP.
Patients with severe OSA might notice improved sleep quality and reduced EDS, even after only a few hours of use. Such patients sometimes wish to start CPAP treatment immediately.
Overall, advances in masks and equipment have improved patient adherence to CPAP. Such innovations include auto-titrating machines, in which the pressure level can be varied depending on sleep state or body position. Many newer machines also have a data microchip that allows the clinician to determine the duration of usage, then use that information to counsel the patient about adherence if necessary.
Patient education also can promote CPAP adherence. Upon being first told they might need to sleep each night wearing a nasal mask, patients often voice well-founded concerns about comfort, claustrophobia, or sexual activity.
As part of a comprehensive approach at the Mayo Sleep Disorders Center, patients watch an educational videotape, tour the sleep laboratory bedrooms before the sleep study, and are carefully fitted for masks. Ideally, the technologists interact with the patient during the sleep study to adjust the headgear and fine-tune other aspects of the equipment. The sleep specialist meets with the patient to compare the baseline diagnostic study results with changes in breathing patterns after a trial of nasal CPAP.
Other useful patient compliance tools include a CPAP informational handout, telephone access to nursing staff, and a 30-day follow-up visit.
Obtaining the support of the bed partner by welcoming her or him to all appointments, including educational activities, is optimal. The bed partner was likely the impetus for the appointment in the first place because of concerns about excessive snoring or apneas.
Image reprinted from Oct. 2001 Mayo Clinic Health Letter with permission of Mayo Foundation for Medical Education and Research, Rochester, MN 55905
Surgical options exist for OSA. The most common procedures are uvulopalatopharyngoplasty (UPPP) and laser-assisted uvulopalatoplasty (LAUP). Other procedures in use include tongue reduction and mandibular advancement.
The response rate to OSA surgery averages around 50% but varies on the patient’s characteristics and procedure selected.9 Positive outcomes are most likely for thin patients with obvious upper airway obstruction, including a deviated nasal septum, large tonsils, a low-hanging palate, and large uvula. Potential complications include nasal regurgitation, voice change, postoperative pain, bleeding, infection, tongue numbness, and snoring without apnea (silent apnea).
Oral appliances have a vital niche in OSA treatment. Multiple devices have been developed that open the oropharynx by moving the mandible and tongue out of way. A growing body of data shows that oral appliances improve sleep and reduce EDS and promote patient satisfaction more effectively than nasal CPAP.10 Several studies also show that patients with mild to moderate OSA accept these devices well.
Oral devices do have drawbacks, however. In most settings, effectiveness cannot be observed during a “split-night” laboratory sleep study because the patient has not yet purchased the device. Also, multiple visits sometimes are required to custom fit the oral appliance; this can pose a hardship to patients who live a distance from the provider.
Restless legs syndrome, periodic limb movement disorder
The patient with restless legs syndrome typically reports a restless painful feeling in the limbs that occurs in the evening and at night, disrupting sleep. This condition, which affects 10% of the population, is associated with aging, blood loss, anemia, peripheral neuropathies, and pregnancy.11 Patients can have childhood onset and in some cases there is a familial tendency.
Most patients with restless legs syndrome have periodic limb movements (repetitive leg jerks or twitches). The clinical significance of periodic limb movements with no subjective disagreeable feelings in the limbs is controversial. Typically, treatment is not instituted in these cases.
The history usually confirms the diagnosis without a sleep study. Sleep studies are used only if a co-existing sleep problem is suspected or if the diagnosis is not clear-cut.
One suspected mechanism of restless legs syndrome is a dopamine-deficient state. A serum ferritin level can help detect a relative iron deficiency, iron being a cofactor for dopamine synthesis.12
Treatment can include iron repletion when indicated. Medications include dopaminergic agents, most notably pramipexole and levodopa/carbidopa. Other options include gabapentin, benzodiazepines, and narcotics. Antidepressants have been suspected to worsen this condition but definitive studies are lacking.13
Identifying, correcting circadian rhythm disorders
Instead of compromising the quality or quantity of sleep, circadian rhythm disorders cause sleep to occur at inappropriate times. Adolescents or young adults are most likely to confront these disorders.
The delayed sleep phase disorder—that is, a persistent pattern of staying up late and “sleeping in” the next morning—is the most common example. A careful assessment will reveal that the patient is getting a satisfactory amount of sleep that occurs at a socially unacceptable time, sometimes to the extreme that his or her nights and days are reversed.
Patients can be reluctant to acknowledge the severity of their problem, which can lead to both inaccurate sleep diaries and interviews. A portable device called a wrist actigraph provides data about limb movement, thus more objectively measuring the patient’s sleep schedule.
Psychiatrists frequently encounter patients with delayed sleep phase disorder because of a high degree of comorbidity with depressive disorders.14 The cause of this syndrome is unclear, but environmental factors including light exposure, social patterns, psychological issues, and possibly a genetic substrate, are known to contribute.
A less common circadian rhythm disorder, advanced sleep phase disorder, can also cause EDS. Patients have an inappropriately early time of sleep onset and then are fully awake in the middle of the night. A recent report describes a large family with a severe form of this disorder that is linked to an abnormality on chromosome two.15
Relatively few effective treatments have been identified for circadian rhythm disorders. Some patients elect not to pursue therapy, instead selecting activities that fit around their unconventional sleep schedules. Sometimes individuals with delayed sleep phase cannot arrange their education or work hours around their atypical sleep schedules. These patients experience poor early morning academic or work performance due to sleepiness.
The internal circadian clock can be gradually readjusted with either phototherapy or gradual shifting of the major sleep period (Box 4). Stimulant or hypnotic medications generally are not utilized.
Insufficient sleep syndrome
Studies indicate that more people are attempting to burn the candle at both ends and are consequently developing a newly identified condition, insufficient sleep syndrome.16 In our 24-hour society, people often are trying to make do with less than the required 7-1/2 hours sleep per day. This may have adverse consequences to their health. When people are required to perform shift work, the problem is compounded because of the difficulty in obtaining sufficient quality sleep during daylight hours.
Many patients do not seek out treatment for fatigue or sleepiness because they are aware of the lifestyle choices that they have made. Still, they might develop psychologic symptoms like irritability, mood swings, and strained interpersonal relationships. These symptoms often will prompt patients to request treatment.
The most common technique is to ask the patient to establish a consistent awakening time and subsequently a regular bedtime. Initially this could be unconventional by societal standards, i.e., bedtime at 5 a.m. and arising at 2 p.m. Once this pattern is in place, the patient gradually shifts the timing by an hour a day. For most patients it is easier to delay rather than advance the bedtime until it conforms to the desired time.
Reinforce this new sleep pattern with a structured daytime schedule that includes predictable mealtimes, regular exercise, social activities, and possibly bright light exposure. This reinforcement should occur in the morning for delayed sleep phase and in the evening for advanced sleep phase disorder. These interventions take time and discipline.
Another approach is for the patient to completely skip sleep one night and, in a sleep-deprived state, establish a new bedtime at the desired time. The same modalities listed above must be used to reinforce (or “entrain”) this schedule or the patient will gradually slip back into the previous abnormal sleep-wake rhythm.
Major medical centers and North American metropolitan areas are increasingly developing sleep disorder treatment centers. Insurance companies generally cover a specialty sleep evaluation, particularly if the referring physician documents a suspicion of sleep-disordered breathing or excessive daytime sleepiness (EDS)that jeopardizes safe driving.
The most appropriate conditions for an urgent sleep evaluation are:
- Difficulty staying alert while driving, nocturnal cardiac arrhythmias;
- Frequent observed apneas;
- EDS leading to academic or occupational problems.
Psychiatrists should take a careful history that includes a discussion of the patient’s daily and weekly schedule. Avoid psychostimulant medications. Instead, address the non-negotiable need to get adequate sleep and challenge the patients to prioritize his or her activities around a full night’s sleep.
When to consider narcolepsy
Narcolepsy, a less common sleep disorder, can lead to severe occupational, educational, and family disruption. Narcolepsy, which affects 0.05% of the population, is a potentially debilitating disease of the central nervous system that involves abnormal regulation of REM sleep. EDS is the cardinal symptom, often associated with cataplexy (75%), sleep paralysis (50%), vivid dreams, and insomnia, all of which can represent inappropriate intrusion of REM phenomena.
After obtaining a history suggestive of narcolepsy, the psychiatrist should employ either the history, a sleep diary, or wrist actigraphy to document whether the patient is getting adequate sleep with a consistent sleep/wake cycle. Next, consider referring the patient for polysomnography, primarily to rule out other causes of EDS like sleep disorder breathing. In some cases, the REM latency on the overnight sleep study will be less than 20 minutes after sleep onset, which supports the diagnosis of narcolepsy. A multiple sleep latency test (MSLT), a diagnostic test that consists of the patient taking four to five daytime naps, is performed the following day.
Narcolepsy is confirmed if the patient has a mean initial sleep latency of less than 10 minutes during these naps plus at least two REM episodes occurring within 15 minutes after sleep onset.
Recent research shows that most patients who have narcolepsy with cataplexy have undetectable levels of a specific neuropeptide (which is called either hypocretin or orexin) in the cerebrospinal fluid.17 Hypocretin/orexin replacement therapy is a theoretical future possibility, but for now treatment includes a combination of optimal sleep hygiene, psychostimulants, antidepressants, and hypnotics.
Other causes of EDS
Other causes of EDS include unrecognized alcohol dependence, inappropriate or excessive medication use, and depressive disorders. Overnight sleep studies are seldom indicated unless patients endorse the symptoms in Figure 1.
Before pursuing sleep studies (polysomnography or an MSLT), eliminate medications that might confound the results. Such agents include antidepressants, which alter the timing and duration of REM sleep, and sedating medications, which modify initial sleep latency and sleep efficiency and potentially aggravate sleep disordered breathing. Although initial REM latency provides a potential biologic marker of major depression, this measurement is more often used in research studies than in clinical psychiatry.
Primary insomnia is a distressing inability to sleep at night or nap during the day. This suggests a hyperarousal state in several ways, and is the opposite of EDS.18 In rare cases, however, patients who cannot sleep at night also do have EDS. When evaluated, these patients typically endorse at least one of the symptoms in Figure 1. Overnight sleep studies occasionally demonstrate that the insomnia is a symptom of another underlying specific sleep disorder, such as OSA or restless legs syndrome.
Psychiatrists treating a patient with chronic insomnia may appropriately undertake several trials of behavioral interventions or sedating medications before making a referral to a sleep disorder center. Patients can struggle with unrecognized primary sleep disorders for years, and many are evaluated by psychiatrists who institute an empiric trial of stimulating antidepressant medications. Use of antidepressants in these situations is unlikely to cause harm, but they might complicate diagnostic testing. When coexisting depression and a primary sleep disorder are confirmed, management of the sleepy patient optimally entails specific treatments that separately target each condition.
Related resources
- National Sleep Foundation www.sleepfoundation.org
- American Academy of Sleep Medicine www.asda.org
- American Sleep Apnea Association www.sleepapnea.org
- Restless Legs Syndrome Foundation www.rls.org
- Association for the Study of Light Therapy and Biological Rhythms www.sltbr.org
Disclosure
The author reports no affiliation or financial arrangements with any of the companies whose products are mentioned in this article.
Drug brand names
- Carbidopa/levodopa • Sinemet
- Gabapentin • Neurontin
- Pramipexole • Mirapex
- Trazodone • Desyrel
- Zolpidem • Ambien
1. Ronald J, Delaive K, et al. Health care utilization in the 10 years prior to diagnosis in obstructive sleep apnea syndrome patients. Sleep. 1999;22(2):225-29.
2. Punjabi N, Haponik E. Ask about daytime sleepiness. J Amer Geriatr Soc. 2000;48:228-29.
3. Johns M. A new method for measuring daytime sleepiness: The Epworth Sleepiness Scale. Sleep. 1991;14(6):540-45.
4. Rowley J, Aboussouan L, Badr M. The use of clinical prediction formulas in the evaluation of obstructive sleep apnea. Sleep. 2000;23:929-38.
5. Yamashiro Y, Kryger M. Nocturnal oximetry: Is it a screening tool for sleep disorders? Sleep. 1995;18:167-71.
6. Morrell M, Finn L, Kim H, Peppard P, Badr M, Young T. Sleep fragmentation, awake blood pressure, and sleep-disordered breathing in a population-based study. Am J Respir Critical Care Med. 2000;162(6):2091-96.
7. Roux F, D’Ambrosio C, Mohsenin V. Sleep-related breathing disorders and cardiovascular disease. Am J Med. 2000;108:396-402.
8. Engleman H, Martin S, Deary I, Douglas N. Effect of continuous positive airway pressure treatment on daytime function in sleep apnoea/hypopnoea syndrome. Lancet. 1994;343(8897):572-75.
9. Lojander J, Maasilta P, Partinen M, Brander P, Salmi T, Lehtonen H. Nasal-CPAP, surgery, and conservative management for treatment of obstructive sleep apnea syndrome. A randomized study. Chest. 1996;110(1):114-19.
10. Mehta A, Qian J, Petocz P, Darendeliler M, Cistulli P. A randomized, controlled study of a mandibular advancement splint for obstructive sleep apnea. Am J Respir Critical Care Med. 2001;163(6):1457-61.
11. Chesson A, Jr, Wise M, et al. Practice parameters for the treatment of restless legs syndrome and periodic limb movement disorder. Sleep. 1999;22(7):961-68.
12. Phillips B, Young T, Finn L, Asher K, Hening W, Purvis C. Epidemiology of restless legs symptoms in adults. Arch Intern Med. 2000;160(14):2137-41.
13. Thorpy M, Ehrenberg B, Hening W, et al. Restless legs syndrome: Detection and management in primary care. Amer Fam Phys. 2000;62:108-14.
14. Regestein Q, Monk T. Delayed sleep phase syndrome: A review of its clinical aspects. Am J Psychiatry. 1995;152:602-08.
15. Toh K, Jones C, et al. An hPer2 phosphorylation site mutation in familial advanced sleep phase syndrome. Science. 2001;291(5506):1040-43.
16. Yoshikawa N, Suzuki S, Ishimoto T, Matsumoto M, Miyagishi T. A case of insufficient sleep syndrome. Psychiatry Clin Neuro. 1998;52(2):200-01.
17. Nishino S, Ripley B, Overeem S, Lammers G, Mignot E. Hypocretin (orexin) deficiency in human narcolepsy. Lancet. 2000;355:39-40.
18. Hauri P, Esther M. Insomnia. Mayo Clin Proc. 1990;65:869-82.
Untreated excessive daytime sleepiness (EDS) results in compromised quality of life, reduced productivity, and public safety concerns.1 Obstructive sleep apnea (OSA), restless legs syndrome, circadian rhythm disorders, and narcolepsy are frequently underdiagnosed sleep disorders that can cause EDS. These conditions commonly go undetected and untreated for several reasons:
- Patients may not recognize sleepiness as a legitimate medical concern.
- Physicians, with few exceptions, typically have little training in sleep disorders and limited time to diagnose them.2 Screening questions regarding sleep are typically absent.
- Definitive diagnostic tests are costly.
As a result, many patients go without appropriate sleep evaluations. Instead a depressive or other psychiatric disorder may be suspected because of the sleepy patient’s poor energy, hypersomnia, amotivation, irritability, and frustration. Because of ongoing behavioral symptoms, patients with an undiagnosed primary sleep disorder are often referred to psychiatrists. Thus, a clear understanding of the differential diagnosis of EDS is crucial.
Patients with sleep issues fall into three major categories:
- Patients with EDS.
- Individuals with insomnia, another large group often seen by psychiatrists. Generally, these patients are less hesitant than patients with EDS to seek help because of the marked distress they suffer nightly when trying to sleep. Insomniacs typically experience minimal EDS.
- Patients with unusual behaviors at night that range from arm waving to violent behaviors.
Assessing the sleepy patient
When evaluating a patient with sleep complaints, several valuable sources of data come into play.
Initially, observe the patient in the waiting room or office before starting the interview. Did the patient nod off while waiting for his or her appointment? Pay attention to any patient who appears sleepy—even if he or she denies having trouble staying awake. Over time, sleepy patients may have lost their perspective on alertness. Some patients have had EDS for so many years that they no longer recall what it is like to feel fully awake.
Collateral history is often important because family members generally observe the sleeping patient. The bed partner often provides valuable information about snoring, irregular breathing leg kicks, unplanned naps, and strained interpersonal relationships due to EDS. For the patient who does not have a bed partner, ask his or her travel companion, with whom the patient may have shared accommodations.
Unfortunately, few useful screening tests exist. Most questionnaires about sleepiness are neither very reliable nor valid. One of the better questionnaires, the Epworth Sleepiness Scale, helps confirm the presence of sleepiness with a score <8, differentiating the inability to stay awake from fatigue. (Box 1 can be cut out, copied, and handed to patients). This brief questionnaire also provides a useful measure of severity.3
The value of the Epworth scale is limited, however, because patient answers often are based on a specific time and context that may not be representative. Additional validated surveys include the Pittsburgh Sleep Quality Inventory and several that focus on OSA.4
How likely are you to doze off or fall asleep in the following situations, in contrast to feeling just tired? Even if you have not done some of these things recently, try to work out how each situation would affect you now. Use the scale below to choose the most appropriate number for each situation:
- 0 no chance of dozing
- 1 slight chance of dozing
- 2 moderate chance of dozing
- 3 high chance of dozing
| Chance of dozing | Situation |
|---|---|
| ○ | Sitting and reading |
| ○ | Watching TV |
| ○ | Sitting inactive in a public place (e.g., a theater or a meeting) |
| ○ | Sitting as a passenger in a car for an hour without a break |
| ○ | Lying down to rest in the afternoon when circumstances permit |
| ○ | Sitting and talking to someone |
| ○ | Sitting quietly after a lunch without alcohol |
| ○ | In a car, while stopped for a few minutes in traffic |
| Johns, M. Sleep 14:540-545, 1991. | |
Electroencephalographic (EEG) monitoring can accurately measure the patient’s degree of sleep disruption. This information is critical in understanding if a patient’s EDS is caused by a physiologic condition that prevents quality nocturnal sleep. At this time, however, no portable devices that employ EEG technology are used in clinical settings.
Additionally, none of the widely used screening devices that assess leg kicks indicate the presence of possible periodic limb movements.
Even though overnight pulse oximetry has been used to screen for sleep-disordered breathing,5 the technology has limitations. For one, most pulse oximeters do not provide information about sleep stage or body position. Some patients with significant sleep-disordered breathing lack adequate oxygen desaturations but have frequent EEG arousals due to sleep issues. In this case, pulse oximetry would generate a false negative result because EEG data is not collected. The inadequate sensitivity is most likely to occur with females and thin patients.
Oximetry provides only one or two types of data (oxygen saturation plus possibly heart rate), while other physiologic processes, e.g., body movement or sleep architecture, can repetitively be disrupted during sleep.
The most critical steps in detecting sleep disorders do not require technology or specialized expertise, but rather intuition and common sense. The psychiatrist should consider the possibility of a sleep disorder and incorporate pertinent questions into the clinical interview. Figure 1 lists sequential questions that might uncover specific sleep disorders. Once suspected, the decision whether to refer the patient to a sleep disorder center for diagnostic testing depends on the type of sleep disorder detected.
Diagnosing and treating OSA
Recent epidemiologic studies show that OSA affects at least 4% of men and 2% of women in the United States.6 Psychiatrists are virtually assured of seeing patients with undiagnosed OSA. The condition is caused by repeated collapse of the soft tissues surrounding the upper airway, decreasing airflow that is restored when the patient briefly awakens. Patients develop EDS because of sleep fragmented by frequent arousals.
Figure 1 THE SLEEPY PATIENT: Possible medical and psychiatric explanations
Obese patients are at higher risk than are patients at normal weight because of their body habitus. Alcohol or sedative medication use close to bedtime can aggravate OSA. These substances promote muscle relaxation and increase the arousal threshold, meaning that patients do not wake readily when apneas occur.
Long-term complications of untreated OSA include sleepiness leading to accidents, hypertension, cerebrovascular disease, and progressive obesity. New data associate OSA with multiple potential cardiovascular complications (arrhythmias, congestive heart failure, and myocardial infarction).7 Therefore, recognition and treatment are paramount.
The physical examination should focus on detecting nasal obstruction (having the patient sniff separately through each nostril can be helpful), big neck, crowded oropharynx (a low-hanging palate, reddened uvula, enlarged tonsils, large tongue size relative to oropharynx diameter) and jaw structure (particularly a small retrognathic mandible).
Referral for nocturnal polysomnography might be the next step. During a comprehensive sleep study, data is collected about respiratory, cardiovascular, and muscle activity at night, as well as the sounds the patient makes (e.g., snoring, coughing) when asleep. EEG monitoring also is performed. OSA may be diagnosed if repeated episodes of reduced airflow and oxygen desaturation are observed; these typically result in brief shifts in EEG frequency called arousals.
First-line interventions for OSA include avoidance of alcohol within 1 to 2 hours of bedtime, sleeping on the side instead of the back, weight loss (ideally with a regular exercise program), and nasal sprays for allergies.
If the first-line treatments for OSA are ineffective, nasal continuous positive airway pressure (CPAP) works well for almost all patients who adhere to the regimen.8 CPAP requires the patient to wear a nasal mask that delivers room air, splinting open the nasopharynx and the upper airway (Box 2). Some patients benefit from a brief trial of a sleeping medication, e.g., zolpidem or trazodone, for the first 1 to 2 weeks of nasal CPAP usage.
Nasal continuous positive airway pressure (CPAP) must be started in an observed setting so that the clinician can determine the optimal amount of positive pressure needed to keep the upper airway patent. CPAP can be started during the second half of a “split-night” sleep study after obstructive sleep apnea (OSA) has been diagnosed. Alternatively, the sleep laboratory might ask the patient to return for a second night for a trial of nasal CPAP.
Patients with severe OSA might notice improved sleep quality and reduced EDS, even after only a few hours of use. Such patients sometimes wish to start CPAP treatment immediately.
Overall, advances in masks and equipment have improved patient adherence to CPAP. Such innovations include auto-titrating machines, in which the pressure level can be varied depending on sleep state or body position. Many newer machines also have a data microchip that allows the clinician to determine the duration of usage, then use that information to counsel the patient about adherence if necessary.
Patient education also can promote CPAP adherence. Upon being first told they might need to sleep each night wearing a nasal mask, patients often voice well-founded concerns about comfort, claustrophobia, or sexual activity.
As part of a comprehensive approach at the Mayo Sleep Disorders Center, patients watch an educational videotape, tour the sleep laboratory bedrooms before the sleep study, and are carefully fitted for masks. Ideally, the technologists interact with the patient during the sleep study to adjust the headgear and fine-tune other aspects of the equipment. The sleep specialist meets with the patient to compare the baseline diagnostic study results with changes in breathing patterns after a trial of nasal CPAP.
Other useful patient compliance tools include a CPAP informational handout, telephone access to nursing staff, and a 30-day follow-up visit.
Obtaining the support of the bed partner by welcoming her or him to all appointments, including educational activities, is optimal. The bed partner was likely the impetus for the appointment in the first place because of concerns about excessive snoring or apneas.
Image reprinted from Oct. 2001 Mayo Clinic Health Letter with permission of Mayo Foundation for Medical Education and Research, Rochester, MN 55905
Surgical options exist for OSA. The most common procedures are uvulopalatopharyngoplasty (UPPP) and laser-assisted uvulopalatoplasty (LAUP). Other procedures in use include tongue reduction and mandibular advancement.
The response rate to OSA surgery averages around 50% but varies on the patient’s characteristics and procedure selected.9 Positive outcomes are most likely for thin patients with obvious upper airway obstruction, including a deviated nasal septum, large tonsils, a low-hanging palate, and large uvula. Potential complications include nasal regurgitation, voice change, postoperative pain, bleeding, infection, tongue numbness, and snoring without apnea (silent apnea).
Oral appliances have a vital niche in OSA treatment. Multiple devices have been developed that open the oropharynx by moving the mandible and tongue out of way. A growing body of data shows that oral appliances improve sleep and reduce EDS and promote patient satisfaction more effectively than nasal CPAP.10 Several studies also show that patients with mild to moderate OSA accept these devices well.
Oral devices do have drawbacks, however. In most settings, effectiveness cannot be observed during a “split-night” laboratory sleep study because the patient has not yet purchased the device. Also, multiple visits sometimes are required to custom fit the oral appliance; this can pose a hardship to patients who live a distance from the provider.
Restless legs syndrome, periodic limb movement disorder
The patient with restless legs syndrome typically reports a restless painful feeling in the limbs that occurs in the evening and at night, disrupting sleep. This condition, which affects 10% of the population, is associated with aging, blood loss, anemia, peripheral neuropathies, and pregnancy.11 Patients can have childhood onset and in some cases there is a familial tendency.
Most patients with restless legs syndrome have periodic limb movements (repetitive leg jerks or twitches). The clinical significance of periodic limb movements with no subjective disagreeable feelings in the limbs is controversial. Typically, treatment is not instituted in these cases.
The history usually confirms the diagnosis without a sleep study. Sleep studies are used only if a co-existing sleep problem is suspected or if the diagnosis is not clear-cut.
One suspected mechanism of restless legs syndrome is a dopamine-deficient state. A serum ferritin level can help detect a relative iron deficiency, iron being a cofactor for dopamine synthesis.12
Treatment can include iron repletion when indicated. Medications include dopaminergic agents, most notably pramipexole and levodopa/carbidopa. Other options include gabapentin, benzodiazepines, and narcotics. Antidepressants have been suspected to worsen this condition but definitive studies are lacking.13
Identifying, correcting circadian rhythm disorders
Instead of compromising the quality or quantity of sleep, circadian rhythm disorders cause sleep to occur at inappropriate times. Adolescents or young adults are most likely to confront these disorders.
The delayed sleep phase disorder—that is, a persistent pattern of staying up late and “sleeping in” the next morning—is the most common example. A careful assessment will reveal that the patient is getting a satisfactory amount of sleep that occurs at a socially unacceptable time, sometimes to the extreme that his or her nights and days are reversed.
Patients can be reluctant to acknowledge the severity of their problem, which can lead to both inaccurate sleep diaries and interviews. A portable device called a wrist actigraph provides data about limb movement, thus more objectively measuring the patient’s sleep schedule.
Psychiatrists frequently encounter patients with delayed sleep phase disorder because of a high degree of comorbidity with depressive disorders.14 The cause of this syndrome is unclear, but environmental factors including light exposure, social patterns, psychological issues, and possibly a genetic substrate, are known to contribute.
A less common circadian rhythm disorder, advanced sleep phase disorder, can also cause EDS. Patients have an inappropriately early time of sleep onset and then are fully awake in the middle of the night. A recent report describes a large family with a severe form of this disorder that is linked to an abnormality on chromosome two.15
Relatively few effective treatments have been identified for circadian rhythm disorders. Some patients elect not to pursue therapy, instead selecting activities that fit around their unconventional sleep schedules. Sometimes individuals with delayed sleep phase cannot arrange their education or work hours around their atypical sleep schedules. These patients experience poor early morning academic or work performance due to sleepiness.
The internal circadian clock can be gradually readjusted with either phototherapy or gradual shifting of the major sleep period (Box 4). Stimulant or hypnotic medications generally are not utilized.
Insufficient sleep syndrome
Studies indicate that more people are attempting to burn the candle at both ends and are consequently developing a newly identified condition, insufficient sleep syndrome.16 In our 24-hour society, people often are trying to make do with less than the required 7-1/2 hours sleep per day. This may have adverse consequences to their health. When people are required to perform shift work, the problem is compounded because of the difficulty in obtaining sufficient quality sleep during daylight hours.
Many patients do not seek out treatment for fatigue or sleepiness because they are aware of the lifestyle choices that they have made. Still, they might develop psychologic symptoms like irritability, mood swings, and strained interpersonal relationships. These symptoms often will prompt patients to request treatment.
The most common technique is to ask the patient to establish a consistent awakening time and subsequently a regular bedtime. Initially this could be unconventional by societal standards, i.e., bedtime at 5 a.m. and arising at 2 p.m. Once this pattern is in place, the patient gradually shifts the timing by an hour a day. For most patients it is easier to delay rather than advance the bedtime until it conforms to the desired time.
Reinforce this new sleep pattern with a structured daytime schedule that includes predictable mealtimes, regular exercise, social activities, and possibly bright light exposure. This reinforcement should occur in the morning for delayed sleep phase and in the evening for advanced sleep phase disorder. These interventions take time and discipline.
Another approach is for the patient to completely skip sleep one night and, in a sleep-deprived state, establish a new bedtime at the desired time. The same modalities listed above must be used to reinforce (or “entrain”) this schedule or the patient will gradually slip back into the previous abnormal sleep-wake rhythm.
Major medical centers and North American metropolitan areas are increasingly developing sleep disorder treatment centers. Insurance companies generally cover a specialty sleep evaluation, particularly if the referring physician documents a suspicion of sleep-disordered breathing or excessive daytime sleepiness (EDS)that jeopardizes safe driving.
The most appropriate conditions for an urgent sleep evaluation are:
- Difficulty staying alert while driving, nocturnal cardiac arrhythmias;
- Frequent observed apneas;
- EDS leading to academic or occupational problems.
Psychiatrists should take a careful history that includes a discussion of the patient’s daily and weekly schedule. Avoid psychostimulant medications. Instead, address the non-negotiable need to get adequate sleep and challenge the patients to prioritize his or her activities around a full night’s sleep.
When to consider narcolepsy
Narcolepsy, a less common sleep disorder, can lead to severe occupational, educational, and family disruption. Narcolepsy, which affects 0.05% of the population, is a potentially debilitating disease of the central nervous system that involves abnormal regulation of REM sleep. EDS is the cardinal symptom, often associated with cataplexy (75%), sleep paralysis (50%), vivid dreams, and insomnia, all of which can represent inappropriate intrusion of REM phenomena.
After obtaining a history suggestive of narcolepsy, the psychiatrist should employ either the history, a sleep diary, or wrist actigraphy to document whether the patient is getting adequate sleep with a consistent sleep/wake cycle. Next, consider referring the patient for polysomnography, primarily to rule out other causes of EDS like sleep disorder breathing. In some cases, the REM latency on the overnight sleep study will be less than 20 minutes after sleep onset, which supports the diagnosis of narcolepsy. A multiple sleep latency test (MSLT), a diagnostic test that consists of the patient taking four to five daytime naps, is performed the following day.
Narcolepsy is confirmed if the patient has a mean initial sleep latency of less than 10 minutes during these naps plus at least two REM episodes occurring within 15 minutes after sleep onset.
Recent research shows that most patients who have narcolepsy with cataplexy have undetectable levels of a specific neuropeptide (which is called either hypocretin or orexin) in the cerebrospinal fluid.17 Hypocretin/orexin replacement therapy is a theoretical future possibility, but for now treatment includes a combination of optimal sleep hygiene, psychostimulants, antidepressants, and hypnotics.
Other causes of EDS
Other causes of EDS include unrecognized alcohol dependence, inappropriate or excessive medication use, and depressive disorders. Overnight sleep studies are seldom indicated unless patients endorse the symptoms in Figure 1.
Before pursuing sleep studies (polysomnography or an MSLT), eliminate medications that might confound the results. Such agents include antidepressants, which alter the timing and duration of REM sleep, and sedating medications, which modify initial sleep latency and sleep efficiency and potentially aggravate sleep disordered breathing. Although initial REM latency provides a potential biologic marker of major depression, this measurement is more often used in research studies than in clinical psychiatry.
Primary insomnia is a distressing inability to sleep at night or nap during the day. This suggests a hyperarousal state in several ways, and is the opposite of EDS.18 In rare cases, however, patients who cannot sleep at night also do have EDS. When evaluated, these patients typically endorse at least one of the symptoms in Figure 1. Overnight sleep studies occasionally demonstrate that the insomnia is a symptom of another underlying specific sleep disorder, such as OSA or restless legs syndrome.
Psychiatrists treating a patient with chronic insomnia may appropriately undertake several trials of behavioral interventions or sedating medications before making a referral to a sleep disorder center. Patients can struggle with unrecognized primary sleep disorders for years, and many are evaluated by psychiatrists who institute an empiric trial of stimulating antidepressant medications. Use of antidepressants in these situations is unlikely to cause harm, but they might complicate diagnostic testing. When coexisting depression and a primary sleep disorder are confirmed, management of the sleepy patient optimally entails specific treatments that separately target each condition.
Related resources
- National Sleep Foundation www.sleepfoundation.org
- American Academy of Sleep Medicine www.asda.org
- American Sleep Apnea Association www.sleepapnea.org
- Restless Legs Syndrome Foundation www.rls.org
- Association for the Study of Light Therapy and Biological Rhythms www.sltbr.org
Disclosure
The author reports no affiliation or financial arrangements with any of the companies whose products are mentioned in this article.
Drug brand names
- Carbidopa/levodopa • Sinemet
- Gabapentin • Neurontin
- Pramipexole • Mirapex
- Trazodone • Desyrel
- Zolpidem • Ambien
Untreated excessive daytime sleepiness (EDS) results in compromised quality of life, reduced productivity, and public safety concerns.1 Obstructive sleep apnea (OSA), restless legs syndrome, circadian rhythm disorders, and narcolepsy are frequently underdiagnosed sleep disorders that can cause EDS. These conditions commonly go undetected and untreated for several reasons:
- Patients may not recognize sleepiness as a legitimate medical concern.
- Physicians, with few exceptions, typically have little training in sleep disorders and limited time to diagnose them.2 Screening questions regarding sleep are typically absent.
- Definitive diagnostic tests are costly.
As a result, many patients go without appropriate sleep evaluations. Instead a depressive or other psychiatric disorder may be suspected because of the sleepy patient’s poor energy, hypersomnia, amotivation, irritability, and frustration. Because of ongoing behavioral symptoms, patients with an undiagnosed primary sleep disorder are often referred to psychiatrists. Thus, a clear understanding of the differential diagnosis of EDS is crucial.
Patients with sleep issues fall into three major categories:
- Patients with EDS.
- Individuals with insomnia, another large group often seen by psychiatrists. Generally, these patients are less hesitant than patients with EDS to seek help because of the marked distress they suffer nightly when trying to sleep. Insomniacs typically experience minimal EDS.
- Patients with unusual behaviors at night that range from arm waving to violent behaviors.
Assessing the sleepy patient
When evaluating a patient with sleep complaints, several valuable sources of data come into play.
Initially, observe the patient in the waiting room or office before starting the interview. Did the patient nod off while waiting for his or her appointment? Pay attention to any patient who appears sleepy—even if he or she denies having trouble staying awake. Over time, sleepy patients may have lost their perspective on alertness. Some patients have had EDS for so many years that they no longer recall what it is like to feel fully awake.
Collateral history is often important because family members generally observe the sleeping patient. The bed partner often provides valuable information about snoring, irregular breathing leg kicks, unplanned naps, and strained interpersonal relationships due to EDS. For the patient who does not have a bed partner, ask his or her travel companion, with whom the patient may have shared accommodations.
Unfortunately, few useful screening tests exist. Most questionnaires about sleepiness are neither very reliable nor valid. One of the better questionnaires, the Epworth Sleepiness Scale, helps confirm the presence of sleepiness with a score <8, differentiating the inability to stay awake from fatigue. (Box 1 can be cut out, copied, and handed to patients). This brief questionnaire also provides a useful measure of severity.3
The value of the Epworth scale is limited, however, because patient answers often are based on a specific time and context that may not be representative. Additional validated surveys include the Pittsburgh Sleep Quality Inventory and several that focus on OSA.4
How likely are you to doze off or fall asleep in the following situations, in contrast to feeling just tired? Even if you have not done some of these things recently, try to work out how each situation would affect you now. Use the scale below to choose the most appropriate number for each situation:
- 0 no chance of dozing
- 1 slight chance of dozing
- 2 moderate chance of dozing
- 3 high chance of dozing
| Chance of dozing | Situation |
|---|---|
| ○ | Sitting and reading |
| ○ | Watching TV |
| ○ | Sitting inactive in a public place (e.g., a theater or a meeting) |
| ○ | Sitting as a passenger in a car for an hour without a break |
| ○ | Lying down to rest in the afternoon when circumstances permit |
| ○ | Sitting and talking to someone |
| ○ | Sitting quietly after a lunch without alcohol |
| ○ | In a car, while stopped for a few minutes in traffic |
| Johns, M. Sleep 14:540-545, 1991. | |
Electroencephalographic (EEG) monitoring can accurately measure the patient’s degree of sleep disruption. This information is critical in understanding if a patient’s EDS is caused by a physiologic condition that prevents quality nocturnal sleep. At this time, however, no portable devices that employ EEG technology are used in clinical settings.
Additionally, none of the widely used screening devices that assess leg kicks indicate the presence of possible periodic limb movements.
Even though overnight pulse oximetry has been used to screen for sleep-disordered breathing,5 the technology has limitations. For one, most pulse oximeters do not provide information about sleep stage or body position. Some patients with significant sleep-disordered breathing lack adequate oxygen desaturations but have frequent EEG arousals due to sleep issues. In this case, pulse oximetry would generate a false negative result because EEG data is not collected. The inadequate sensitivity is most likely to occur with females and thin patients.
Oximetry provides only one or two types of data (oxygen saturation plus possibly heart rate), while other physiologic processes, e.g., body movement or sleep architecture, can repetitively be disrupted during sleep.
The most critical steps in detecting sleep disorders do not require technology or specialized expertise, but rather intuition and common sense. The psychiatrist should consider the possibility of a sleep disorder and incorporate pertinent questions into the clinical interview. Figure 1 lists sequential questions that might uncover specific sleep disorders. Once suspected, the decision whether to refer the patient to a sleep disorder center for diagnostic testing depends on the type of sleep disorder detected.
Diagnosing and treating OSA
Recent epidemiologic studies show that OSA affects at least 4% of men and 2% of women in the United States.6 Psychiatrists are virtually assured of seeing patients with undiagnosed OSA. The condition is caused by repeated collapse of the soft tissues surrounding the upper airway, decreasing airflow that is restored when the patient briefly awakens. Patients develop EDS because of sleep fragmented by frequent arousals.
Figure 1 THE SLEEPY PATIENT: Possible medical and psychiatric explanations
Obese patients are at higher risk than are patients at normal weight because of their body habitus. Alcohol or sedative medication use close to bedtime can aggravate OSA. These substances promote muscle relaxation and increase the arousal threshold, meaning that patients do not wake readily when apneas occur.
Long-term complications of untreated OSA include sleepiness leading to accidents, hypertension, cerebrovascular disease, and progressive obesity. New data associate OSA with multiple potential cardiovascular complications (arrhythmias, congestive heart failure, and myocardial infarction).7 Therefore, recognition and treatment are paramount.
The physical examination should focus on detecting nasal obstruction (having the patient sniff separately through each nostril can be helpful), big neck, crowded oropharynx (a low-hanging palate, reddened uvula, enlarged tonsils, large tongue size relative to oropharynx diameter) and jaw structure (particularly a small retrognathic mandible).
Referral for nocturnal polysomnography might be the next step. During a comprehensive sleep study, data is collected about respiratory, cardiovascular, and muscle activity at night, as well as the sounds the patient makes (e.g., snoring, coughing) when asleep. EEG monitoring also is performed. OSA may be diagnosed if repeated episodes of reduced airflow and oxygen desaturation are observed; these typically result in brief shifts in EEG frequency called arousals.
First-line interventions for OSA include avoidance of alcohol within 1 to 2 hours of bedtime, sleeping on the side instead of the back, weight loss (ideally with a regular exercise program), and nasal sprays for allergies.
If the first-line treatments for OSA are ineffective, nasal continuous positive airway pressure (CPAP) works well for almost all patients who adhere to the regimen.8 CPAP requires the patient to wear a nasal mask that delivers room air, splinting open the nasopharynx and the upper airway (Box 2). Some patients benefit from a brief trial of a sleeping medication, e.g., zolpidem or trazodone, for the first 1 to 2 weeks of nasal CPAP usage.
Nasal continuous positive airway pressure (CPAP) must be started in an observed setting so that the clinician can determine the optimal amount of positive pressure needed to keep the upper airway patent. CPAP can be started during the second half of a “split-night” sleep study after obstructive sleep apnea (OSA) has been diagnosed. Alternatively, the sleep laboratory might ask the patient to return for a second night for a trial of nasal CPAP.
Patients with severe OSA might notice improved sleep quality and reduced EDS, even after only a few hours of use. Such patients sometimes wish to start CPAP treatment immediately.
Overall, advances in masks and equipment have improved patient adherence to CPAP. Such innovations include auto-titrating machines, in which the pressure level can be varied depending on sleep state or body position. Many newer machines also have a data microchip that allows the clinician to determine the duration of usage, then use that information to counsel the patient about adherence if necessary.
Patient education also can promote CPAP adherence. Upon being first told they might need to sleep each night wearing a nasal mask, patients often voice well-founded concerns about comfort, claustrophobia, or sexual activity.
As part of a comprehensive approach at the Mayo Sleep Disorders Center, patients watch an educational videotape, tour the sleep laboratory bedrooms before the sleep study, and are carefully fitted for masks. Ideally, the technologists interact with the patient during the sleep study to adjust the headgear and fine-tune other aspects of the equipment. The sleep specialist meets with the patient to compare the baseline diagnostic study results with changes in breathing patterns after a trial of nasal CPAP.
Other useful patient compliance tools include a CPAP informational handout, telephone access to nursing staff, and a 30-day follow-up visit.
Obtaining the support of the bed partner by welcoming her or him to all appointments, including educational activities, is optimal. The bed partner was likely the impetus for the appointment in the first place because of concerns about excessive snoring or apneas.
Image reprinted from Oct. 2001 Mayo Clinic Health Letter with permission of Mayo Foundation for Medical Education and Research, Rochester, MN 55905
Surgical options exist for OSA. The most common procedures are uvulopalatopharyngoplasty (UPPP) and laser-assisted uvulopalatoplasty (LAUP). Other procedures in use include tongue reduction and mandibular advancement.
The response rate to OSA surgery averages around 50% but varies on the patient’s characteristics and procedure selected.9 Positive outcomes are most likely for thin patients with obvious upper airway obstruction, including a deviated nasal septum, large tonsils, a low-hanging palate, and large uvula. Potential complications include nasal regurgitation, voice change, postoperative pain, bleeding, infection, tongue numbness, and snoring without apnea (silent apnea).
Oral appliances have a vital niche in OSA treatment. Multiple devices have been developed that open the oropharynx by moving the mandible and tongue out of way. A growing body of data shows that oral appliances improve sleep and reduce EDS and promote patient satisfaction more effectively than nasal CPAP.10 Several studies also show that patients with mild to moderate OSA accept these devices well.
Oral devices do have drawbacks, however. In most settings, effectiveness cannot be observed during a “split-night” laboratory sleep study because the patient has not yet purchased the device. Also, multiple visits sometimes are required to custom fit the oral appliance; this can pose a hardship to patients who live a distance from the provider.
Restless legs syndrome, periodic limb movement disorder
The patient with restless legs syndrome typically reports a restless painful feeling in the limbs that occurs in the evening and at night, disrupting sleep. This condition, which affects 10% of the population, is associated with aging, blood loss, anemia, peripheral neuropathies, and pregnancy.11 Patients can have childhood onset and in some cases there is a familial tendency.
Most patients with restless legs syndrome have periodic limb movements (repetitive leg jerks or twitches). The clinical significance of periodic limb movements with no subjective disagreeable feelings in the limbs is controversial. Typically, treatment is not instituted in these cases.
The history usually confirms the diagnosis without a sleep study. Sleep studies are used only if a co-existing sleep problem is suspected or if the diagnosis is not clear-cut.
One suspected mechanism of restless legs syndrome is a dopamine-deficient state. A serum ferritin level can help detect a relative iron deficiency, iron being a cofactor for dopamine synthesis.12
Treatment can include iron repletion when indicated. Medications include dopaminergic agents, most notably pramipexole and levodopa/carbidopa. Other options include gabapentin, benzodiazepines, and narcotics. Antidepressants have been suspected to worsen this condition but definitive studies are lacking.13
Identifying, correcting circadian rhythm disorders
Instead of compromising the quality or quantity of sleep, circadian rhythm disorders cause sleep to occur at inappropriate times. Adolescents or young adults are most likely to confront these disorders.
The delayed sleep phase disorder—that is, a persistent pattern of staying up late and “sleeping in” the next morning—is the most common example. A careful assessment will reveal that the patient is getting a satisfactory amount of sleep that occurs at a socially unacceptable time, sometimes to the extreme that his or her nights and days are reversed.
Patients can be reluctant to acknowledge the severity of their problem, which can lead to both inaccurate sleep diaries and interviews. A portable device called a wrist actigraph provides data about limb movement, thus more objectively measuring the patient’s sleep schedule.
Psychiatrists frequently encounter patients with delayed sleep phase disorder because of a high degree of comorbidity with depressive disorders.14 The cause of this syndrome is unclear, but environmental factors including light exposure, social patterns, psychological issues, and possibly a genetic substrate, are known to contribute.
A less common circadian rhythm disorder, advanced sleep phase disorder, can also cause EDS. Patients have an inappropriately early time of sleep onset and then are fully awake in the middle of the night. A recent report describes a large family with a severe form of this disorder that is linked to an abnormality on chromosome two.15
Relatively few effective treatments have been identified for circadian rhythm disorders. Some patients elect not to pursue therapy, instead selecting activities that fit around their unconventional sleep schedules. Sometimes individuals with delayed sleep phase cannot arrange their education or work hours around their atypical sleep schedules. These patients experience poor early morning academic or work performance due to sleepiness.
The internal circadian clock can be gradually readjusted with either phototherapy or gradual shifting of the major sleep period (Box 4). Stimulant or hypnotic medications generally are not utilized.
Insufficient sleep syndrome
Studies indicate that more people are attempting to burn the candle at both ends and are consequently developing a newly identified condition, insufficient sleep syndrome.16 In our 24-hour society, people often are trying to make do with less than the required 7-1/2 hours sleep per day. This may have adverse consequences to their health. When people are required to perform shift work, the problem is compounded because of the difficulty in obtaining sufficient quality sleep during daylight hours.
Many patients do not seek out treatment for fatigue or sleepiness because they are aware of the lifestyle choices that they have made. Still, they might develop psychologic symptoms like irritability, mood swings, and strained interpersonal relationships. These symptoms often will prompt patients to request treatment.
The most common technique is to ask the patient to establish a consistent awakening time and subsequently a regular bedtime. Initially this could be unconventional by societal standards, i.e., bedtime at 5 a.m. and arising at 2 p.m. Once this pattern is in place, the patient gradually shifts the timing by an hour a day. For most patients it is easier to delay rather than advance the bedtime until it conforms to the desired time.
Reinforce this new sleep pattern with a structured daytime schedule that includes predictable mealtimes, regular exercise, social activities, and possibly bright light exposure. This reinforcement should occur in the morning for delayed sleep phase and in the evening for advanced sleep phase disorder. These interventions take time and discipline.
Another approach is for the patient to completely skip sleep one night and, in a sleep-deprived state, establish a new bedtime at the desired time. The same modalities listed above must be used to reinforce (or “entrain”) this schedule or the patient will gradually slip back into the previous abnormal sleep-wake rhythm.
Major medical centers and North American metropolitan areas are increasingly developing sleep disorder treatment centers. Insurance companies generally cover a specialty sleep evaluation, particularly if the referring physician documents a suspicion of sleep-disordered breathing or excessive daytime sleepiness (EDS)that jeopardizes safe driving.
The most appropriate conditions for an urgent sleep evaluation are:
- Difficulty staying alert while driving, nocturnal cardiac arrhythmias;
- Frequent observed apneas;
- EDS leading to academic or occupational problems.
Psychiatrists should take a careful history that includes a discussion of the patient’s daily and weekly schedule. Avoid psychostimulant medications. Instead, address the non-negotiable need to get adequate sleep and challenge the patients to prioritize his or her activities around a full night’s sleep.
When to consider narcolepsy
Narcolepsy, a less common sleep disorder, can lead to severe occupational, educational, and family disruption. Narcolepsy, which affects 0.05% of the population, is a potentially debilitating disease of the central nervous system that involves abnormal regulation of REM sleep. EDS is the cardinal symptom, often associated with cataplexy (75%), sleep paralysis (50%), vivid dreams, and insomnia, all of which can represent inappropriate intrusion of REM phenomena.
After obtaining a history suggestive of narcolepsy, the psychiatrist should employ either the history, a sleep diary, or wrist actigraphy to document whether the patient is getting adequate sleep with a consistent sleep/wake cycle. Next, consider referring the patient for polysomnography, primarily to rule out other causes of EDS like sleep disorder breathing. In some cases, the REM latency on the overnight sleep study will be less than 20 minutes after sleep onset, which supports the diagnosis of narcolepsy. A multiple sleep latency test (MSLT), a diagnostic test that consists of the patient taking four to five daytime naps, is performed the following day.
Narcolepsy is confirmed if the patient has a mean initial sleep latency of less than 10 minutes during these naps plus at least two REM episodes occurring within 15 minutes after sleep onset.
Recent research shows that most patients who have narcolepsy with cataplexy have undetectable levels of a specific neuropeptide (which is called either hypocretin or orexin) in the cerebrospinal fluid.17 Hypocretin/orexin replacement therapy is a theoretical future possibility, but for now treatment includes a combination of optimal sleep hygiene, psychostimulants, antidepressants, and hypnotics.
Other causes of EDS
Other causes of EDS include unrecognized alcohol dependence, inappropriate or excessive medication use, and depressive disorders. Overnight sleep studies are seldom indicated unless patients endorse the symptoms in Figure 1.
Before pursuing sleep studies (polysomnography or an MSLT), eliminate medications that might confound the results. Such agents include antidepressants, which alter the timing and duration of REM sleep, and sedating medications, which modify initial sleep latency and sleep efficiency and potentially aggravate sleep disordered breathing. Although initial REM latency provides a potential biologic marker of major depression, this measurement is more often used in research studies than in clinical psychiatry.
Primary insomnia is a distressing inability to sleep at night or nap during the day. This suggests a hyperarousal state in several ways, and is the opposite of EDS.18 In rare cases, however, patients who cannot sleep at night also do have EDS. When evaluated, these patients typically endorse at least one of the symptoms in Figure 1. Overnight sleep studies occasionally demonstrate that the insomnia is a symptom of another underlying specific sleep disorder, such as OSA or restless legs syndrome.
Psychiatrists treating a patient with chronic insomnia may appropriately undertake several trials of behavioral interventions or sedating medications before making a referral to a sleep disorder center. Patients can struggle with unrecognized primary sleep disorders for years, and many are evaluated by psychiatrists who institute an empiric trial of stimulating antidepressant medications. Use of antidepressants in these situations is unlikely to cause harm, but they might complicate diagnostic testing. When coexisting depression and a primary sleep disorder are confirmed, management of the sleepy patient optimally entails specific treatments that separately target each condition.
Related resources
- National Sleep Foundation www.sleepfoundation.org
- American Academy of Sleep Medicine www.asda.org
- American Sleep Apnea Association www.sleepapnea.org
- Restless Legs Syndrome Foundation www.rls.org
- Association for the Study of Light Therapy and Biological Rhythms www.sltbr.org
Disclosure
The author reports no affiliation or financial arrangements with any of the companies whose products are mentioned in this article.
Drug brand names
- Carbidopa/levodopa • Sinemet
- Gabapentin • Neurontin
- Pramipexole • Mirapex
- Trazodone • Desyrel
- Zolpidem • Ambien
1. Ronald J, Delaive K, et al. Health care utilization in the 10 years prior to diagnosis in obstructive sleep apnea syndrome patients. Sleep. 1999;22(2):225-29.
2. Punjabi N, Haponik E. Ask about daytime sleepiness. J Amer Geriatr Soc. 2000;48:228-29.
3. Johns M. A new method for measuring daytime sleepiness: The Epworth Sleepiness Scale. Sleep. 1991;14(6):540-45.
4. Rowley J, Aboussouan L, Badr M. The use of clinical prediction formulas in the evaluation of obstructive sleep apnea. Sleep. 2000;23:929-38.
5. Yamashiro Y, Kryger M. Nocturnal oximetry: Is it a screening tool for sleep disorders? Sleep. 1995;18:167-71.
6. Morrell M, Finn L, Kim H, Peppard P, Badr M, Young T. Sleep fragmentation, awake blood pressure, and sleep-disordered breathing in a population-based study. Am J Respir Critical Care Med. 2000;162(6):2091-96.
7. Roux F, D’Ambrosio C, Mohsenin V. Sleep-related breathing disorders and cardiovascular disease. Am J Med. 2000;108:396-402.
8. Engleman H, Martin S, Deary I, Douglas N. Effect of continuous positive airway pressure treatment on daytime function in sleep apnoea/hypopnoea syndrome. Lancet. 1994;343(8897):572-75.
9. Lojander J, Maasilta P, Partinen M, Brander P, Salmi T, Lehtonen H. Nasal-CPAP, surgery, and conservative management for treatment of obstructive sleep apnea syndrome. A randomized study. Chest. 1996;110(1):114-19.
10. Mehta A, Qian J, Petocz P, Darendeliler M, Cistulli P. A randomized, controlled study of a mandibular advancement splint for obstructive sleep apnea. Am J Respir Critical Care Med. 2001;163(6):1457-61.
11. Chesson A, Jr, Wise M, et al. Practice parameters for the treatment of restless legs syndrome and periodic limb movement disorder. Sleep. 1999;22(7):961-68.
12. Phillips B, Young T, Finn L, Asher K, Hening W, Purvis C. Epidemiology of restless legs symptoms in adults. Arch Intern Med. 2000;160(14):2137-41.
13. Thorpy M, Ehrenberg B, Hening W, et al. Restless legs syndrome: Detection and management in primary care. Amer Fam Phys. 2000;62:108-14.
14. Regestein Q, Monk T. Delayed sleep phase syndrome: A review of its clinical aspects. Am J Psychiatry. 1995;152:602-08.
15. Toh K, Jones C, et al. An hPer2 phosphorylation site mutation in familial advanced sleep phase syndrome. Science. 2001;291(5506):1040-43.
16. Yoshikawa N, Suzuki S, Ishimoto T, Matsumoto M, Miyagishi T. A case of insufficient sleep syndrome. Psychiatry Clin Neuro. 1998;52(2):200-01.
17. Nishino S, Ripley B, Overeem S, Lammers G, Mignot E. Hypocretin (orexin) deficiency in human narcolepsy. Lancet. 2000;355:39-40.
18. Hauri P, Esther M. Insomnia. Mayo Clin Proc. 1990;65:869-82.
1. Ronald J, Delaive K, et al. Health care utilization in the 10 years prior to diagnosis in obstructive sleep apnea syndrome patients. Sleep. 1999;22(2):225-29.
2. Punjabi N, Haponik E. Ask about daytime sleepiness. J Amer Geriatr Soc. 2000;48:228-29.
3. Johns M. A new method for measuring daytime sleepiness: The Epworth Sleepiness Scale. Sleep. 1991;14(6):540-45.
4. Rowley J, Aboussouan L, Badr M. The use of clinical prediction formulas in the evaluation of obstructive sleep apnea. Sleep. 2000;23:929-38.
5. Yamashiro Y, Kryger M. Nocturnal oximetry: Is it a screening tool for sleep disorders? Sleep. 1995;18:167-71.
6. Morrell M, Finn L, Kim H, Peppard P, Badr M, Young T. Sleep fragmentation, awake blood pressure, and sleep-disordered breathing in a population-based study. Am J Respir Critical Care Med. 2000;162(6):2091-96.
7. Roux F, D’Ambrosio C, Mohsenin V. Sleep-related breathing disorders and cardiovascular disease. Am J Med. 2000;108:396-402.
8. Engleman H, Martin S, Deary I, Douglas N. Effect of continuous positive airway pressure treatment on daytime function in sleep apnoea/hypopnoea syndrome. Lancet. 1994;343(8897):572-75.
9. Lojander J, Maasilta P, Partinen M, Brander P, Salmi T, Lehtonen H. Nasal-CPAP, surgery, and conservative management for treatment of obstructive sleep apnea syndrome. A randomized study. Chest. 1996;110(1):114-19.
10. Mehta A, Qian J, Petocz P, Darendeliler M, Cistulli P. A randomized, controlled study of a mandibular advancement splint for obstructive sleep apnea. Am J Respir Critical Care Med. 2001;163(6):1457-61.
11. Chesson A, Jr, Wise M, et al. Practice parameters for the treatment of restless legs syndrome and periodic limb movement disorder. Sleep. 1999;22(7):961-68.
12. Phillips B, Young T, Finn L, Asher K, Hening W, Purvis C. Epidemiology of restless legs symptoms in adults. Arch Intern Med. 2000;160(14):2137-41.
13. Thorpy M, Ehrenberg B, Hening W, et al. Restless legs syndrome: Detection and management in primary care. Amer Fam Phys. 2000;62:108-14.
14. Regestein Q, Monk T. Delayed sleep phase syndrome: A review of its clinical aspects. Am J Psychiatry. 1995;152:602-08.
15. Toh K, Jones C, et al. An hPer2 phosphorylation site mutation in familial advanced sleep phase syndrome. Science. 2001;291(5506):1040-43.
16. Yoshikawa N, Suzuki S, Ishimoto T, Matsumoto M, Miyagishi T. A case of insufficient sleep syndrome. Psychiatry Clin Neuro. 1998;52(2):200-01.
17. Nishino S, Ripley B, Overeem S, Lammers G, Mignot E. Hypocretin (orexin) deficiency in human narcolepsy. Lancet. 2000;355:39-40.
18. Hauri P, Esther M. Insomnia. Mayo Clin Proc. 1990;65:869-82.
Our new understanding of pulmonary alveolar proteinosis: What an internist needs to know
A 62-year-old man with an abnormal electrocardiogram
GP IIb/IIIa inhibitors in coronary artery disease management: What the latest trials tell us
Does losartan (Cozaar) slow the progression of renal disease in patients with type 2 diabetes and nephropathy?
BACKGROUND: Interruption of the renin-angiotensin system with angiotensin-converting enzyme (ACE) inhibitors is renoprotective both in patients with type 1 diabetes and in patients without diabetes who have overt nephropathy. This study evaluates the effectiveness of losartan, an angiotensin-receptor blocker (ARB), in slowing the progression of nephropathy in type 2 diabetes.
POPULATION STUDIED: The Reduction of Endpoints in Non-insulin– dependent diabetes with the Angiotensin II Antagonist Losartan (RENAAL) study included 1513 people with type 2 diabetes and nephropathy, ranging in age from 31 to 70 years. Nephropathy was defined as urinary protein excretion of at least 500 mg daily and a serum creatinine of 1.3 to 3.0 mg per dL. Patients were excluded if they had a diagnosis of nondiabetic nephropathy; had experienced a recent myocardial infarction, transient ischemic attack, or stroke; had recently undergone coronary artery bypass grafting or percutaneous coronary angioplasty; or had ever had heart failure.
STUDY DESIGN AND VALIDITY: The RENAAL study was a double-blind randomized placebo-controlled trial in which patients were assigned to receive either losartan 50 to 100 mg or placebo. All patients received other antihypertensive therapy (excluding ACE inhibitors and ARBs) as necessary to maintain a blood pressure level of less than 140/90 mm Hg. The groups were similar at baseline, with a mean serum creatinine was 1.9 mg per dL (standard deviation = 0.5). The patients were followed up for a mean of 3.4 years, and an intention-to-treat analysis was reported. The study methods appeared valid, although concealment of allocation was not described.
OUTCOMES MEASURED: The primary outcome was the combined outcomes of a doubling of the baseline serum creatinine concentration, end-stage renal disease, and death.
RESULTS: Treatment with losartan resulted in a 16% reduction in the primary composite end point (95% confidence interval [CI], 2%-28%; P =.02; number needed to treat [NNT]=28). The risk for doubling of serum creatinine concentration was reduced by 25% (95% CI, 8-39; P =.006; NNT=23). The likelihood of reaching end-stage renal disease was reduced by 28% (95% CI, 11-42; P =.002; NNT=17). Losartan also decreased the level of proteinuria by 35% (P < .001) and the rate of decline of renal function by 18% (P =.01). A 32% reduction in a patient’s first hospitalization for heart failure was observed (P =.005). There was no difference in the composite end point of morbidity and mortality due to cardiovascular causes, adverse events, or overall mortality.
Losartan showed significant renal benefits in patients with type 2 diabetes and nephropathy. Two other recent papers support this finding. In one, irbesartan (Avapro) protected against the progression of nephropathy in patients with type 2 diabetes compared with either amlodipine (Norvasc) or placebo.1 Treatment with irbesartan also reduced the rate of progression to overt nephropathy in hypertensive patients with type 2 diabetes and microalbuminuria.1
It is unknown whether ACE inhibitors induce the same degree of renoprotection as ARBs in patients with type 2 diabetes. However, ACE inhibitors slow progression of nephropathy due to type 1 diabetes and have significant cardiovascular benefits for patients with type 2 diabetes and hypertension. Interestingly, the RENAAL study was stopped early because of a recently published analysis of the Heart Outcome Prevention Evaluation study,2 which focused on the effects of an ACE inhibitor on patients with diabetes and mild renal insufficiency (serum creatinine = 1.4-2.3 mg/dL). That analysis showed that ramipril reduced a combined end point of cardiovascular death, myocardial infarction, or stroke by a hazard ratio of 0.48 (95% CI, 0.26-0.86). Although ARBs are clearly renoprotective in patients with type 2 diabetes, the data do not yet provide a rationale for sacrificing the cardiovascular protection of an ACE inhibitor in this high-risk population. For now, ACE inhibitors should be the first agent for patients with diabetes who have hypertension and renal disease, reserving ARBs for those who cannot tolerate the ACE inhibitors.
BACKGROUND: Interruption of the renin-angiotensin system with angiotensin-converting enzyme (ACE) inhibitors is renoprotective both in patients with type 1 diabetes and in patients without diabetes who have overt nephropathy. This study evaluates the effectiveness of losartan, an angiotensin-receptor blocker (ARB), in slowing the progression of nephropathy in type 2 diabetes.
POPULATION STUDIED: The Reduction of Endpoints in Non-insulin– dependent diabetes with the Angiotensin II Antagonist Losartan (RENAAL) study included 1513 people with type 2 diabetes and nephropathy, ranging in age from 31 to 70 years. Nephropathy was defined as urinary protein excretion of at least 500 mg daily and a serum creatinine of 1.3 to 3.0 mg per dL. Patients were excluded if they had a diagnosis of nondiabetic nephropathy; had experienced a recent myocardial infarction, transient ischemic attack, or stroke; had recently undergone coronary artery bypass grafting or percutaneous coronary angioplasty; or had ever had heart failure.
STUDY DESIGN AND VALIDITY: The RENAAL study was a double-blind randomized placebo-controlled trial in which patients were assigned to receive either losartan 50 to 100 mg or placebo. All patients received other antihypertensive therapy (excluding ACE inhibitors and ARBs) as necessary to maintain a blood pressure level of less than 140/90 mm Hg. The groups were similar at baseline, with a mean serum creatinine was 1.9 mg per dL (standard deviation = 0.5). The patients were followed up for a mean of 3.4 years, and an intention-to-treat analysis was reported. The study methods appeared valid, although concealment of allocation was not described.
OUTCOMES MEASURED: The primary outcome was the combined outcomes of a doubling of the baseline serum creatinine concentration, end-stage renal disease, and death.
RESULTS: Treatment with losartan resulted in a 16% reduction in the primary composite end point (95% confidence interval [CI], 2%-28%; P =.02; number needed to treat [NNT]=28). The risk for doubling of serum creatinine concentration was reduced by 25% (95% CI, 8-39; P =.006; NNT=23). The likelihood of reaching end-stage renal disease was reduced by 28% (95% CI, 11-42; P =.002; NNT=17). Losartan also decreased the level of proteinuria by 35% (P < .001) and the rate of decline of renal function by 18% (P =.01). A 32% reduction in a patient’s first hospitalization for heart failure was observed (P =.005). There was no difference in the composite end point of morbidity and mortality due to cardiovascular causes, adverse events, or overall mortality.
Losartan showed significant renal benefits in patients with type 2 diabetes and nephropathy. Two other recent papers support this finding. In one, irbesartan (Avapro) protected against the progression of nephropathy in patients with type 2 diabetes compared with either amlodipine (Norvasc) or placebo.1 Treatment with irbesartan also reduced the rate of progression to overt nephropathy in hypertensive patients with type 2 diabetes and microalbuminuria.1
It is unknown whether ACE inhibitors induce the same degree of renoprotection as ARBs in patients with type 2 diabetes. However, ACE inhibitors slow progression of nephropathy due to type 1 diabetes and have significant cardiovascular benefits for patients with type 2 diabetes and hypertension. Interestingly, the RENAAL study was stopped early because of a recently published analysis of the Heart Outcome Prevention Evaluation study,2 which focused on the effects of an ACE inhibitor on patients with diabetes and mild renal insufficiency (serum creatinine = 1.4-2.3 mg/dL). That analysis showed that ramipril reduced a combined end point of cardiovascular death, myocardial infarction, or stroke by a hazard ratio of 0.48 (95% CI, 0.26-0.86). Although ARBs are clearly renoprotective in patients with type 2 diabetes, the data do not yet provide a rationale for sacrificing the cardiovascular protection of an ACE inhibitor in this high-risk population. For now, ACE inhibitors should be the first agent for patients with diabetes who have hypertension and renal disease, reserving ARBs for those who cannot tolerate the ACE inhibitors.
BACKGROUND: Interruption of the renin-angiotensin system with angiotensin-converting enzyme (ACE) inhibitors is renoprotective both in patients with type 1 diabetes and in patients without diabetes who have overt nephropathy. This study evaluates the effectiveness of losartan, an angiotensin-receptor blocker (ARB), in slowing the progression of nephropathy in type 2 diabetes.
POPULATION STUDIED: The Reduction of Endpoints in Non-insulin– dependent diabetes with the Angiotensin II Antagonist Losartan (RENAAL) study included 1513 people with type 2 diabetes and nephropathy, ranging in age from 31 to 70 years. Nephropathy was defined as urinary protein excretion of at least 500 mg daily and a serum creatinine of 1.3 to 3.0 mg per dL. Patients were excluded if they had a diagnosis of nondiabetic nephropathy; had experienced a recent myocardial infarction, transient ischemic attack, or stroke; had recently undergone coronary artery bypass grafting or percutaneous coronary angioplasty; or had ever had heart failure.
STUDY DESIGN AND VALIDITY: The RENAAL study was a double-blind randomized placebo-controlled trial in which patients were assigned to receive either losartan 50 to 100 mg or placebo. All patients received other antihypertensive therapy (excluding ACE inhibitors and ARBs) as necessary to maintain a blood pressure level of less than 140/90 mm Hg. The groups were similar at baseline, with a mean serum creatinine was 1.9 mg per dL (standard deviation = 0.5). The patients were followed up for a mean of 3.4 years, and an intention-to-treat analysis was reported. The study methods appeared valid, although concealment of allocation was not described.
OUTCOMES MEASURED: The primary outcome was the combined outcomes of a doubling of the baseline serum creatinine concentration, end-stage renal disease, and death.
RESULTS: Treatment with losartan resulted in a 16% reduction in the primary composite end point (95% confidence interval [CI], 2%-28%; P =.02; number needed to treat [NNT]=28). The risk for doubling of serum creatinine concentration was reduced by 25% (95% CI, 8-39; P =.006; NNT=23). The likelihood of reaching end-stage renal disease was reduced by 28% (95% CI, 11-42; P =.002; NNT=17). Losartan also decreased the level of proteinuria by 35% (P < .001) and the rate of decline of renal function by 18% (P =.01). A 32% reduction in a patient’s first hospitalization for heart failure was observed (P =.005). There was no difference in the composite end point of morbidity and mortality due to cardiovascular causes, adverse events, or overall mortality.
Losartan showed significant renal benefits in patients with type 2 diabetes and nephropathy. Two other recent papers support this finding. In one, irbesartan (Avapro) protected against the progression of nephropathy in patients with type 2 diabetes compared with either amlodipine (Norvasc) or placebo.1 Treatment with irbesartan also reduced the rate of progression to overt nephropathy in hypertensive patients with type 2 diabetes and microalbuminuria.1
It is unknown whether ACE inhibitors induce the same degree of renoprotection as ARBs in patients with type 2 diabetes. However, ACE inhibitors slow progression of nephropathy due to type 1 diabetes and have significant cardiovascular benefits for patients with type 2 diabetes and hypertension. Interestingly, the RENAAL study was stopped early because of a recently published analysis of the Heart Outcome Prevention Evaluation study,2 which focused on the effects of an ACE inhibitor on patients with diabetes and mild renal insufficiency (serum creatinine = 1.4-2.3 mg/dL). That analysis showed that ramipril reduced a combined end point of cardiovascular death, myocardial infarction, or stroke by a hazard ratio of 0.48 (95% CI, 0.26-0.86). Although ARBs are clearly renoprotective in patients with type 2 diabetes, the data do not yet provide a rationale for sacrificing the cardiovascular protection of an ACE inhibitor in this high-risk population. For now, ACE inhibitors should be the first agent for patients with diabetes who have hypertension and renal disease, reserving ARBs for those who cannot tolerate the ACE inhibitors.
Is tolterodine (Detrol) or oxybutynin (Ditropan) the best for treatment of urge urinary incontinence?
BACKGROUND: Urge urinary incontinence has drawn attention recently, with a number of studies looking at which treatment provides the best results with the fewest side effects. The authors of this study performed a meta-analysis comparing treatment outcomes and side effects for short-acting oxybutynin and tolterodine.
POPULATION STUDIED: The trials included in this meta-analysis studied patients older than 18 years and who were complaining of urge incontinence or an association of frequency (> 8 times per day) and urgency, or had received a diagnosis of detrusor instability. Patients were excluded who had used co-interventions within the 14 days preceding the trial. No further information was available on the populations studied, making it difficult to determine if the patients were similar to those of a primary care practice.
STUDY DESIGN AND VALIDITY: The authors conducted a rigorous literature search without language constraint for published and unpublished studies that were randomized or quasirandomized and double blinded comparing tolterodine with oxybutynin. At least one arm of each study needed to be randomized to 1 to 2 mg tolterodine twice daily and the other arm to 2.5 to 5 mg of oxybutynin 3 times daily. Two independent reviewers decided which trials would be considered in the analysis according to priori eligibility criteria.
OUTCOMES MEASURED: The primary outcomes included the number of incontinent episodes per 24-hour period, the quantity of pads used per 24 hours, the number of micturitions per 24 hours, and the mean voided volume per micturition. Secondary outcomes included the number of patients with side effects and withdrawals attributed to side effects, the number of patients changing dose, urologic measurements, and quality of life.
RESULTS: Oxybutynin produced a statistically and clinically significant decrease in the number of incontinent episodes per 24-hour period (weighted mean difference = 0.41; 95% confidence interval [CI], 0.04-0.77). Both drugs decreased the number of episodes, but the oxybutynin-treated group averaged 0.5 fewer episodes per day. Patients taking tolterodine reported significantly less dry mouth (relative risk [RR] = 0.54; 95% CI, 0.48-0.61) and less moderate to severe dry mouth (RR=0.33; 95% CI, 0.24-0.45). The risk of withdrawing from the study because of side effects was decreased by 37% in the tolterodine group (RR=0.63; 95% CI, 0.46-0.88).
Oxybutynin is superior to tolterodine in efficacy, causing nearly one half fewer episodes of urinary incontinence per day. Tolterodine is better tolerated with less moderate-to-severe dry mouth and fewer dropouts because of medication side effects. For now, oxybutynin should be the first-line choice, since it is available generically and is considerably less expensive (approximately $20 per month for oxybutynin vs $75 per month for tolterodine). Tolterodine or extended-release oxybutynin should be used for those who cannot tolerate this medication because of side effects.
BACKGROUND: Urge urinary incontinence has drawn attention recently, with a number of studies looking at which treatment provides the best results with the fewest side effects. The authors of this study performed a meta-analysis comparing treatment outcomes and side effects for short-acting oxybutynin and tolterodine.
POPULATION STUDIED: The trials included in this meta-analysis studied patients older than 18 years and who were complaining of urge incontinence or an association of frequency (> 8 times per day) and urgency, or had received a diagnosis of detrusor instability. Patients were excluded who had used co-interventions within the 14 days preceding the trial. No further information was available on the populations studied, making it difficult to determine if the patients were similar to those of a primary care practice.
STUDY DESIGN AND VALIDITY: The authors conducted a rigorous literature search without language constraint for published and unpublished studies that were randomized or quasirandomized and double blinded comparing tolterodine with oxybutynin. At least one arm of each study needed to be randomized to 1 to 2 mg tolterodine twice daily and the other arm to 2.5 to 5 mg of oxybutynin 3 times daily. Two independent reviewers decided which trials would be considered in the analysis according to priori eligibility criteria.
OUTCOMES MEASURED: The primary outcomes included the number of incontinent episodes per 24-hour period, the quantity of pads used per 24 hours, the number of micturitions per 24 hours, and the mean voided volume per micturition. Secondary outcomes included the number of patients with side effects and withdrawals attributed to side effects, the number of patients changing dose, urologic measurements, and quality of life.
RESULTS: Oxybutynin produced a statistically and clinically significant decrease in the number of incontinent episodes per 24-hour period (weighted mean difference = 0.41; 95% confidence interval [CI], 0.04-0.77). Both drugs decreased the number of episodes, but the oxybutynin-treated group averaged 0.5 fewer episodes per day. Patients taking tolterodine reported significantly less dry mouth (relative risk [RR] = 0.54; 95% CI, 0.48-0.61) and less moderate to severe dry mouth (RR=0.33; 95% CI, 0.24-0.45). The risk of withdrawing from the study because of side effects was decreased by 37% in the tolterodine group (RR=0.63; 95% CI, 0.46-0.88).
Oxybutynin is superior to tolterodine in efficacy, causing nearly one half fewer episodes of urinary incontinence per day. Tolterodine is better tolerated with less moderate-to-severe dry mouth and fewer dropouts because of medication side effects. For now, oxybutynin should be the first-line choice, since it is available generically and is considerably less expensive (approximately $20 per month for oxybutynin vs $75 per month for tolterodine). Tolterodine or extended-release oxybutynin should be used for those who cannot tolerate this medication because of side effects.
BACKGROUND: Urge urinary incontinence has drawn attention recently, with a number of studies looking at which treatment provides the best results with the fewest side effects. The authors of this study performed a meta-analysis comparing treatment outcomes and side effects for short-acting oxybutynin and tolterodine.
POPULATION STUDIED: The trials included in this meta-analysis studied patients older than 18 years and who were complaining of urge incontinence or an association of frequency (> 8 times per day) and urgency, or had received a diagnosis of detrusor instability. Patients were excluded who had used co-interventions within the 14 days preceding the trial. No further information was available on the populations studied, making it difficult to determine if the patients were similar to those of a primary care practice.
STUDY DESIGN AND VALIDITY: The authors conducted a rigorous literature search without language constraint for published and unpublished studies that were randomized or quasirandomized and double blinded comparing tolterodine with oxybutynin. At least one arm of each study needed to be randomized to 1 to 2 mg tolterodine twice daily and the other arm to 2.5 to 5 mg of oxybutynin 3 times daily. Two independent reviewers decided which trials would be considered in the analysis according to priori eligibility criteria.
OUTCOMES MEASURED: The primary outcomes included the number of incontinent episodes per 24-hour period, the quantity of pads used per 24 hours, the number of micturitions per 24 hours, and the mean voided volume per micturition. Secondary outcomes included the number of patients with side effects and withdrawals attributed to side effects, the number of patients changing dose, urologic measurements, and quality of life.
RESULTS: Oxybutynin produced a statistically and clinically significant decrease in the number of incontinent episodes per 24-hour period (weighted mean difference = 0.41; 95% confidence interval [CI], 0.04-0.77). Both drugs decreased the number of episodes, but the oxybutynin-treated group averaged 0.5 fewer episodes per day. Patients taking tolterodine reported significantly less dry mouth (relative risk [RR] = 0.54; 95% CI, 0.48-0.61) and less moderate to severe dry mouth (RR=0.33; 95% CI, 0.24-0.45). The risk of withdrawing from the study because of side effects was decreased by 37% in the tolterodine group (RR=0.63; 95% CI, 0.46-0.88).
Oxybutynin is superior to tolterodine in efficacy, causing nearly one half fewer episodes of urinary incontinence per day. Tolterodine is better tolerated with less moderate-to-severe dry mouth and fewer dropouts because of medication side effects. For now, oxybutynin should be the first-line choice, since it is available generically and is considerably less expensive (approximately $20 per month for oxybutynin vs $75 per month for tolterodine). Tolterodine or extended-release oxybutynin should be used for those who cannot tolerate this medication because of side effects.