User login
No heroic measures
The page came around 2 a.m. It had been a very busy night, with a dozen or so surgical consults from an overflowing emergency department in a large urban hospital. Most of the patients referred to the surgical service were immigrants with a limited knowledge of English. Most were elderly. And most were alone.
I was 2 months out of medical school, on call without a senior resident and with staff backup at home. I struggled to remain awake while catering to the seemingly endless pages from the ward and the emergency department. It was a rite of passage that every intern has had to endure.

The patient was an 85-year-old Cantonese-speaking woman transferred to the emergency department by ambulance from her nursing home. The accompanying note, mostly illegible, suggested that she had been complaining of abdominal pain and distention for the past 2 days and had been initially managed with laxatives.
That afternoon, however, her level of consciousness began to deteriorate and she became febrile and hypotensive, so she was transferred to our hospital. She had a history of atrial fibrillation, hypertension, and advanced Alzheimer’s dementia. She also had an accompanying "Do Not Resuscitate/No Life Support" form.
A CT scan of the abdomen arranged by the emergency department physician identified a clot in the superior mesenteric artery and extensive ischemic changes in most of her small bowel. She had a high white blood cell count, and her serum lactate was alarmingly elevated, despite several boluses of intravenous crystalloid solution. She was also becoming hemodynamically unstable.
I immediately called the staff surgeon to advocate for an emergency laparotomy. Given the patient’s multiple comorbidities and grim prognosis, we decided not to operate. The staff surgeon’s instructions were as abrupt as they were clear: "Turf her to medicine; she’s palliative."
The medical senior resident, however, would have none of it. Equally overwhelmed with consults and not in a particularly good mood, he refused to even see the patient. If she was expected to die overnight because of a surgical issue, he argued, then the surgery team was just as equipped as he to take care of her. The emergency department physician agreed, and so the patient was admitted to the surgical service for her few remaining hours of life.
What followed was agonizing for the entire surgical team. The nurses on the ward were asking some very reasonable questions that I could not answer: Do we keep titrating the patient’s oxygen to keep up with her desaturation? What do we give her for pain control? How do we manage her shortness of breath? Should we continue giving her intravenous fluids? Can you help us find her family members? Should we keep the bladder catheter in place?

I strained to remember what we had learned in our few palliative care lectures back in medical school. Intravenous fluids were OK, but oxygen was not. Or was it the other way around? Google, the ever-faithful guardian of the panicking intern, was unhelpful. I could not find a reputable online resource to help guide the management of this patient and, given the other sick patients who needed attention, I could not sit down to perform a thorough online literature search. The hospital’s switchboard was equally disappointing – there were no palliative care physicians on call, and the palliative team only accepted pages after 8 a.m., an appalling 5 hours away.
Eventually, I decided to support the patient with an oxygen mask and to continue her intravenous fluid resuscitation. I gave her plenty of narcotics and antiemetics to soothe the discomfort. We were unable to reach any family members despite several attempts. She died just after 5 a.m., without any visible signs of discomfort. It was the first death certificate I had ever signed.
Reflecting on this experience, I was upset at my inability to quickly and adequately care for this patient’s end-of-life needs. I was also angry that I had not prepared myself appropriately for that night on call, and I would have done several things differently had I had the chance.
General surgeons take immense pride in being internists who can operate. We enjoy debating antibiotic, diuretics, and anticoagulation choices with the specialists consulting on our patients, but we often simply "switch off" whenever the patient is labeled "palliative" or "end of life" – relying entirely on the palliative care team for help. And yet, we’re the ones who admit, operate on, and develop therapeutic relationships with those patients and their families. It just doesn’t seem right, but there are several reasons for this dilemma.
First, the fast pace and busy nature of any surgical service means that trainees and staff are under a lot of pressure to round as quickly and efficiently as possible and get to the operating room early in the morning. Given current trainee work-hour limitations and mandated hand-over, today’s junior staff feel this pressure all the more acutely. There simply isn’t enough time or opportunity for continuity of care. Surgical teams can’t engage palliative patients and their families in the way that dedicated palliative care teams can, and so surgical teams are often more comfortable delegating this responsibility entirely to their palliative care colleagues.
Second, there is an emotional burden to caring for palliative patients and their families. Palliation and end-of-life care imply that surgery is neither possible nor advisable any longer. It can be difficult for the surgeon to make that mental segue and assume the dual role of the psychological and medical care giver. Just as surgeons prefer that cardiologists manage their patients’ arrhythmias and nephrologists their patients’ kidney failures, they may prefer that palliative care specialists manage the emotional and medical needs of the patients on whom they can no longer operate.
Furthermore, surgical trainees have limited exposure to palliative care in the clinical setting. As the field of surgery becomes progressively more complex, palliative care training has not been at the forefront of the educational agenda. While it is taught in medical schools and in the surgical residency curriculum, there are few formalized core rotations that offer the surgical resident an insight into the clinical applications of palliative care, except for those who are particularly interested and seek such learning opportunities out in the form of an elective rotation.
The development of dedicated and multidisciplinary palliative care teams that include staff, nurse practitioners, and palliative fellows has further limited surgical resident exposure to the field. Simply put, the current medical system encourages surgical trainees to sign off on the surgical palliative patient.
This, however, isn’t good enough. Palliative care of the surgical patient needs to be a pillar of surgical training. Trainees need to be as comfortable with managing the symptoms of the dying surgical patient as they are administering fluid boluses and ordering narcotics for postoperative pain, especially late at night when there is no palliative care support.
The American College of Surgeons has responded to this challenge by developing numerous educational initiatives through its Palliative Workgroup. It has published a comprehensive surgical palliative care self-study guide specifically for residents (Surgical Palliative Care: A Residents Guide, available for free download).
There are also several regularly updated online palliative care references available either through subscription websites such as UpToDate or for free, such as the Medical College of Wisconsin’s End of Life/Palliative Education Resource Center, which offers "Fast Facts" on the management of the dying patient.
Palliative care is widely accepted today as an important clinical discipline that provides vital support to a growing proportion of the patient population. Surgical training must keep pace with this evolving reality because, at the end of the day, to be without agony and discomfort is a standard of care that every dying patient expects – not just a heroic measure that we can simply ignore.
Dr. Kayssi is a PGY IV in the general surgery program at the University of Toronto.
Dr. Easson is an ACS Fellow and assistant professor in the department of surgery and the Institute of Health, Policy, Management and Evaluation at the University of Toronto.
The page came around 2 a.m. It had been a very busy night, with a dozen or so surgical consults from an overflowing emergency department in a large urban hospital. Most of the patients referred to the surgical service were immigrants with a limited knowledge of English. Most were elderly. And most were alone.
I was 2 months out of medical school, on call without a senior resident and with staff backup at home. I struggled to remain awake while catering to the seemingly endless pages from the ward and the emergency department. It was a rite of passage that every intern has had to endure.
The patient was an 85-year-old Cantonese-speaking woman transferred to the emergency department by ambulance from her nursing home. The accompanying note, mostly illegible, suggested that she had been complaining of abdominal pain and distention for the past 2 days and had been initially managed with laxatives.
That afternoon, however, her level of consciousness began to deteriorate and she became febrile and hypotensive, so she was transferred to our hospital. She had a history of atrial fibrillation, hypertension, and advanced Alzheimer’s dementia. She also had an accompanying "Do Not Resuscitate/No Life Support" form.
A CT scan of the abdomen arranged by the emergency department physician identified a clot in the superior mesenteric artery and extensive ischemic changes in most of her small bowel. She had a high white blood cell count, and her serum lactate was alarmingly elevated, despite several boluses of intravenous crystalloid solution. She was also becoming hemodynamically unstable.
I immediately called the staff surgeon to advocate for an emergency laparotomy. Given the patient’s multiple comorbidities and grim prognosis, we decided not to operate. The staff surgeon’s instructions were as abrupt as they were clear: "Turf her to medicine; she’s palliative."
The medical senior resident, however, would have none of it. Equally overwhelmed with consults and not in a particularly good mood, he refused to even see the patient. If she was expected to die overnight because of a surgical issue, he argued, then the surgery team was just as equipped as he to take care of her. The emergency department physician agreed, and so the patient was admitted to the surgical service for her few remaining hours of life.
What followed was agonizing for the entire surgical team. The nurses on the ward were asking some very reasonable questions that I could not answer: Do we keep titrating the patient’s oxygen to keep up with her desaturation? What do we give her for pain control? How do we manage her shortness of breath? Should we continue giving her intravenous fluids? Can you help us find her family members? Should we keep the bladder catheter in place?
I strained to remember what we had learned in our few palliative care lectures back in medical school. Intravenous fluids were OK, but oxygen was not. Or was it the other way around? Google, the ever-faithful guardian of the panicking intern, was unhelpful. I could not find a reputable online resource to help guide the management of this patient and, given the other sick patients who needed attention, I could not sit down to perform a thorough online literature search. The hospital’s switchboard was equally disappointing – there were no palliative care physicians on call, and the palliative team only accepted pages after 8 a.m., an appalling 5 hours away.
Eventually, I decided to support the patient with an oxygen mask and to continue her intravenous fluid resuscitation. I gave her plenty of narcotics and antiemetics to soothe the discomfort. We were unable to reach any family members despite several attempts. She died just after 5 a.m., without any visible signs of discomfort. It was the first death certificate I had ever signed.
Reflecting on this experience, I was upset at my inability to quickly and adequately care for this patient’s end-of-life needs. I was also angry that I had not prepared myself appropriately for that night on call, and I would have done several things differently had I had the chance.
General surgeons take immense pride in being internists who can operate. We enjoy debating antibiotic, diuretics, and anticoagulation choices with the specialists consulting on our patients, but we often simply "switch off" whenever the patient is labeled "palliative" or "end of life" – relying entirely on the palliative care team for help. And yet, we’re the ones who admit, operate on, and develop therapeutic relationships with those patients and their families. It just doesn’t seem right, but there are several reasons for this dilemma.
First, the fast pace and busy nature of any surgical service means that trainees and staff are under a lot of pressure to round as quickly and efficiently as possible and get to the operating room early in the morning. Given current trainee work-hour limitations and mandated hand-over, today’s junior staff feel this pressure all the more acutely. There simply isn’t enough time or opportunity for continuity of care. Surgical teams can’t engage palliative patients and their families in the way that dedicated palliative care teams can, and so surgical teams are often more comfortable delegating this responsibility entirely to their palliative care colleagues.
Second, there is an emotional burden to caring for palliative patients and their families. Palliation and end-of-life care imply that surgery is neither possible nor advisable any longer. It can be difficult for the surgeon to make that mental segue and assume the dual role of the psychological and medical care giver. Just as surgeons prefer that cardiologists manage their patients’ arrhythmias and nephrologists their patients’ kidney failures, they may prefer that palliative care specialists manage the emotional and medical needs of the patients on whom they can no longer operate.
Furthermore, surgical trainees have limited exposure to palliative care in the clinical setting. As the field of surgery becomes progressively more complex, palliative care training has not been at the forefront of the educational agenda. While it is taught in medical schools and in the surgical residency curriculum, there are few formalized core rotations that offer the surgical resident an insight into the clinical applications of palliative care, except for those who are particularly interested and seek such learning opportunities out in the form of an elective rotation.
The development of dedicated and multidisciplinary palliative care teams that include staff, nurse practitioners, and palliative fellows has further limited surgical resident exposure to the field. Simply put, the current medical system encourages surgical trainees to sign off on the surgical palliative patient.
This, however, isn’t good enough. Palliative care of the surgical patient needs to be a pillar of surgical training. Trainees need to be as comfortable with managing the symptoms of the dying surgical patient as they are administering fluid boluses and ordering narcotics for postoperative pain, especially late at night when there is no palliative care support.
The American College of Surgeons has responded to this challenge by developing numerous educational initiatives through its Palliative Workgroup. It has published a comprehensive surgical palliative care self-study guide specifically for residents (Surgical Palliative Care: A Residents Guide, available for free download).
There are also several regularly updated online palliative care references available either through subscription websites such as UpToDate or for free, such as the Medical College of Wisconsin’s End of Life/Palliative Education Resource Center, which offers "Fast Facts" on the management of the dying patient.
Palliative care is widely accepted today as an important clinical discipline that provides vital support to a growing proportion of the patient population. Surgical training must keep pace with this evolving reality because, at the end of the day, to be without agony and discomfort is a standard of care that every dying patient expects – not just a heroic measure that we can simply ignore.
Dr. Kayssi is a PGY IV in the general surgery program at the University of Toronto.
Dr. Easson is an ACS Fellow and assistant professor in the department of surgery and the Institute of Health, Policy, Management and Evaluation at the University of Toronto.
The page came around 2 a.m. It had been a very busy night, with a dozen or so surgical consults from an overflowing emergency department in a large urban hospital. Most of the patients referred to the surgical service were immigrants with a limited knowledge of English. Most were elderly. And most were alone.
I was 2 months out of medical school, on call without a senior resident and with staff backup at home. I struggled to remain awake while catering to the seemingly endless pages from the ward and the emergency department. It was a rite of passage that every intern has had to endure.
The patient was an 85-year-old Cantonese-speaking woman transferred to the emergency department by ambulance from her nursing home. The accompanying note, mostly illegible, suggested that she had been complaining of abdominal pain and distention for the past 2 days and had been initially managed with laxatives.
That afternoon, however, her level of consciousness began to deteriorate and she became febrile and hypotensive, so she was transferred to our hospital. She had a history of atrial fibrillation, hypertension, and advanced Alzheimer’s dementia. She also had an accompanying "Do Not Resuscitate/No Life Support" form.
A CT scan of the abdomen arranged by the emergency department physician identified a clot in the superior mesenteric artery and extensive ischemic changes in most of her small bowel. She had a high white blood cell count, and her serum lactate was alarmingly elevated, despite several boluses of intravenous crystalloid solution. She was also becoming hemodynamically unstable.
I immediately called the staff surgeon to advocate for an emergency laparotomy. Given the patient’s multiple comorbidities and grim prognosis, we decided not to operate. The staff surgeon’s instructions were as abrupt as they were clear: "Turf her to medicine; she’s palliative."
The medical senior resident, however, would have none of it. Equally overwhelmed with consults and not in a particularly good mood, he refused to even see the patient. If she was expected to die overnight because of a surgical issue, he argued, then the surgery team was just as equipped as he to take care of her. The emergency department physician agreed, and so the patient was admitted to the surgical service for her few remaining hours of life.
What followed was agonizing for the entire surgical team. The nurses on the ward were asking some very reasonable questions that I could not answer: Do we keep titrating the patient’s oxygen to keep up with her desaturation? What do we give her for pain control? How do we manage her shortness of breath? Should we continue giving her intravenous fluids? Can you help us find her family members? Should we keep the bladder catheter in place?
I strained to remember what we had learned in our few palliative care lectures back in medical school. Intravenous fluids were OK, but oxygen was not. Or was it the other way around? Google, the ever-faithful guardian of the panicking intern, was unhelpful. I could not find a reputable online resource to help guide the management of this patient and, given the other sick patients who needed attention, I could not sit down to perform a thorough online literature search. The hospital’s switchboard was equally disappointing – there were no palliative care physicians on call, and the palliative team only accepted pages after 8 a.m., an appalling 5 hours away.
Eventually, I decided to support the patient with an oxygen mask and to continue her intravenous fluid resuscitation. I gave her plenty of narcotics and antiemetics to soothe the discomfort. We were unable to reach any family members despite several attempts. She died just after 5 a.m., without any visible signs of discomfort. It was the first death certificate I had ever signed.
Reflecting on this experience, I was upset at my inability to quickly and adequately care for this patient’s end-of-life needs. I was also angry that I had not prepared myself appropriately for that night on call, and I would have done several things differently had I had the chance.
General surgeons take immense pride in being internists who can operate. We enjoy debating antibiotic, diuretics, and anticoagulation choices with the specialists consulting on our patients, but we often simply "switch off" whenever the patient is labeled "palliative" or "end of life" – relying entirely on the palliative care team for help. And yet, we’re the ones who admit, operate on, and develop therapeutic relationships with those patients and their families. It just doesn’t seem right, but there are several reasons for this dilemma.
First, the fast pace and busy nature of any surgical service means that trainees and staff are under a lot of pressure to round as quickly and efficiently as possible and get to the operating room early in the morning. Given current trainee work-hour limitations and mandated hand-over, today’s junior staff feel this pressure all the more acutely. There simply isn’t enough time or opportunity for continuity of care. Surgical teams can’t engage palliative patients and their families in the way that dedicated palliative care teams can, and so surgical teams are often more comfortable delegating this responsibility entirely to their palliative care colleagues.
Second, there is an emotional burden to caring for palliative patients and their families. Palliation and end-of-life care imply that surgery is neither possible nor advisable any longer. It can be difficult for the surgeon to make that mental segue and assume the dual role of the psychological and medical care giver. Just as surgeons prefer that cardiologists manage their patients’ arrhythmias and nephrologists their patients’ kidney failures, they may prefer that palliative care specialists manage the emotional and medical needs of the patients on whom they can no longer operate.
Furthermore, surgical trainees have limited exposure to palliative care in the clinical setting. As the field of surgery becomes progressively more complex, palliative care training has not been at the forefront of the educational agenda. While it is taught in medical schools and in the surgical residency curriculum, there are few formalized core rotations that offer the surgical resident an insight into the clinical applications of palliative care, except for those who are particularly interested and seek such learning opportunities out in the form of an elective rotation.
The development of dedicated and multidisciplinary palliative care teams that include staff, nurse practitioners, and palliative fellows has further limited surgical resident exposure to the field. Simply put, the current medical system encourages surgical trainees to sign off on the surgical palliative patient.
This, however, isn’t good enough. Palliative care of the surgical patient needs to be a pillar of surgical training. Trainees need to be as comfortable with managing the symptoms of the dying surgical patient as they are administering fluid boluses and ordering narcotics for postoperative pain, especially late at night when there is no palliative care support.
The American College of Surgeons has responded to this challenge by developing numerous educational initiatives through its Palliative Workgroup. It has published a comprehensive surgical palliative care self-study guide specifically for residents (Surgical Palliative Care: A Residents Guide, available for free download).
There are also several regularly updated online palliative care references available either through subscription websites such as UpToDate or for free, such as the Medical College of Wisconsin’s End of Life/Palliative Education Resource Center, which offers "Fast Facts" on the management of the dying patient.
Palliative care is widely accepted today as an important clinical discipline that provides vital support to a growing proportion of the patient population. Surgical training must keep pace with this evolving reality because, at the end of the day, to be without agony and discomfort is a standard of care that every dying patient expects – not just a heroic measure that we can simply ignore.
Dr. Kayssi is a PGY IV in the general surgery program at the University of Toronto.
Dr. Easson is an ACS Fellow and assistant professor in the department of surgery and the Institute of Health, Policy, Management and Evaluation at the University of Toronto.

End-of-life care gains increasing prominence
From Hollywood to Washington, care at the end of life increasingly is part of the national conversation.
As more than 70 million baby boomers (Americans born between 1946 and 1964) approach the end of their life spans, the cultural, clinical and socioeconomic impacts of end-of-life care have become high-profile topics. The French film "Amour," which depicts the challenges faced by an octogenarian couple after the wife has a series of strokes, has received an Academy Award Best Picture nomination. The Institute of Medicine will convene a panel of experts on Feb. 22-24 in Washington to examine the state of end-of-life care. The goal of the IOM Committee on Transforming End of Life Care is to produce a consensus report by 2014 to address end-of-life care. "Coordinated, expert, compassionate care for people dying from chronic diseases continues to challenge the American health care system," according to the IOM’s online announcement of the meeting.
In addition, the Coalition to Transform Advanced Care is hosting a National Summit on Advanced Illness Care on Jan. 29-30 in Washington. The Coalition includes a wide range of constituencies including the IOM, the American Heart Association, the American Academy of Hospice and Palliative Medicine, and the American Geriatrics Society, as well as insurers, health systems, patient advocacy groups, and others.
As policy issues are discussed and begin to take shape, outcomes research focused on end-of-life care will increasingly gain importance. In the area of cancer care, here are some of the highlights of such research presented at a Quality Care Symposium sponsored by the American Society of Clinical Oncology in December 2012 in San Diego.

Palliative care teams: A palliative care team formed by Dr. Allen R. Chen and his associates at Johns Hopkins’s comprehensive cancer center helped change patient and family decisions regarding end-of-life care during a 4-year period and decreased use of intensive or invasive procedures in the last 6 months of life.
The team offered inpatient and clinic consultations and didactic sessions to physicians to improve how they discuss end-of-life issues with patients, plus support for family meetings to discuss and document the goals of care, said Dr. Chen, associate professor of oncology and pediatrics at Johns Hopkins University, Baltimore.
Of the 525 oncology patients who died in the cancer center while hospitalized from 2008 through 2011, the proportion who chose to have do-not-resuscitate (DNR) orders, withdrew ICU support, or chose comfort care instead of more aggressive care increased from 81% to 95% over the course of the 4 years, a statistically significant difference, he reported.
The rate of ICU care during patients’ final hospitalizations did not change significantly, but the proportion of patients who were put on mechanical ventilation for more than 14 days decreased significantly from 10% to 5%. These earlier withdrawals of care did not increase the risk of death, Dr. Chen said – the rate of survival to discharge from the oncology ICU did not change significantly.
The investigators now are looking for ways to minimize ICU visits at the end of life, he said. The presence of advanced cancer, being on a cardiac monitor, or needing supplemental oxygen foreshadowed critical illness in patients in the study. "We want to facilitate the difficult discussion" about end-of-life care choices "before critical care is needed," he said. So far, their efforts haven’t resulted in decreased use of ICU services at the end of life.

Minimizing surgical risks: One of the first comprehensive analyses of surgical outcomes in patients with disseminated cancer found that the risk of death increases greatly with emergency surgery.
John Pesavento, a medical student at Creighton University, Omaha, Neb., and his associates analyzed preoperative and postoperative data from the American College of Surgeon’s National Surgical Quality Improvement Program database on move than 147,000 patients who underwent surgical procedures between 2005 and 2008.
Eight of the 10 most common procedures resulted in significantly higher 30-day mortality rates in the cancer patients as compared with the same surgeries in patients who did not have disseminated cancer.
Comparing patients with and without disseminated cancer, 30-day mortality rates were 21% and 15%, respectively, after exploration of the abdomen, 15% and 9% after removal of the small bowel, 11% and 6% after colon removal, 11% and 5% after colostomy, 10% and 5% after partial removal of the colon, 10% and 0.5% after cholecystectomy, 1.8% and 0.9% after repair of a bowel opening, and 1% and 0.1% after mastectomy, he reported. The most common operations in patients with disseminated cancer were partial removal of the colon (in 11%), partial removal of the liver (9%), partial removal of the intestine (5%), and abdominal exploration (5%), he reported in a poster presentation.
When done as emergency procedures, however, 7 of the top 10 surgeries led to significantly higher 30-day mortality rates for disseminated cancer patients. Death rates in patients with disseminated cancer were 44% for emergency surgery and 12% for nonemergent surgery to explore the abdomen; the respective rates were 33% and 6% after bowel-to-bowel fusion, 31% and 4% after removal of the colon, 28% and 10% after removal of the small intestine, 23% and 5% after cholecystectomy, 22% and 7% after partial removal of the colon, and 19% and 9% after colostomy.
The findings should help physicians counsel their patients with disseminated cancer to help them decide whether it’s worth undergoing surgery – especially emergency surgery – given the higher risks of death, Mr. Pesavento said.
Physicians’ attitudes and education: In a separate study, 16 urologists and four primary care physicians who were undergoing surgical training in urology were interviewed about their attitudes regarding end-of-life care for men dying of prostate cancer. They viewed current end-of-life care as shoddily organized and poorly integrated, and said that ideal outcomes should be defined by patients’ own values and preferences, Dr. Jonathan Bergman and his associates reported in a poster presentation.
The physicians said that, ideally, a multidisciplinary team would care for dying patients, but respondents varied in the degree to which they saw themselves participating, reported Dr. Bergman of the University of California, Los Angeles.
The findings suggest that physician education about end-of-life care needs improvement, and that clinicians should be guided to deliver end-of-life care that is patient-centered and congruent with patients’ values, he said.
Dying in the hospital: Among 2,621 patients with solid tumors, those who had contact with a specialist palliative care team more than a month before their deaths were less likely to die in the hospital (16%) than were patients who had later or no contact with the team (20%), J. Brian Cassel, Ph.D., reported in a poster presentation.
Dr. Cassel and his associates analyzed claims data on the last 6 months of life for 3,128 adults with cancer who had at least one contact with the Virginia Commonwealth University cancer center in Richmond between January 2009 and July 2011. The data set included patients who had solid tumors, underwent bone marrow transfer, or had other hematologic malignancies.
The findings provided a snapshot of end-of-life care at the university, where 32% of the cancer patients were admitted to the hospital within their last 30 days of life, 19% had at least one readmission during their last 6 months of life, and 15% died in the hospital. Chemotherapy was given to 11% in their last month of life, and to 7% in their last 2 weeks of life, said Dr. Cassel of the university.
The specialist palliative care team made contact with 28% of patients a median of 6-10 days before the death of patients with bone marrow transfer or other nonhematologic malignancies and a median of 25 days before the death of patients with solid tumors.
Chemotherapy at the end of life: Patients with hematologic malignancies were significantly more likely to get chemotherapy in the last 30 days of life (38%) compared with patients with solid tumors (8%), Dr. Alma Rodriguez and her associates reported in a poster presentation.
The investigators reviewed data on 7,399 patients who received care for a solid tumor or hematological malignancy at the University of Texas M.D. Anderson Cancer Center, Houston, and died between December 2010 and May 2012. Overall, 14% of patients received chemotherapy within the last 30 days of life.
Of the 1,262 patients who died in the hospital, 44% received chemotherapy within the last 30 days of life, compared with 7% of the 6,137 patients who died in other locations, reported Dr. Rodriguez, professor of medicine at the cancer center.
Chemotherapy within the last 30 days of life was 3 times more likely in patients with metastatic solid tumors, 14 times more likely in patients with nonrelapsed hematologic malignancy, and 36 times more likely in patients with historical or current relapse of hematologic malignancy.
Patients 65 years or older were 38% less likely than were younger patients to get chemotherapy within the last 30 days of life. Patients with one or more comorbidity (most frequently heart failure and coronary artery diseases) were 28% less likely to get chemotherapy within the last 30 days of life as compared with patients without comorbidities.
"As oncologists, we must communicate clearly with our patients about realistic goals of treatment and the likelihood of life-threatening complications of chemotherapy," Dr. Rodriguez said in the poster.
Outpatient palliative care: Dr. Kavitha Ramchandran and her associates at Stanford (Calif.) University studied their system’s electronic medical records to look at the use of palliative care in outpatient clinics from January through September 2012. The number of palliative care contacts with outpatient clinic patients increased from 10 in January to 45 in September. The number of physicians referring outpatients to palliative care increased from 6 in January to 21 in September, she said in a poster presentation.
More than 65% of patients who were referred for palliative care were younger than 65 years, said Dr. Ramchandran of the university. Most patients had only one visit with palliative care (41%) or two visits (23%).
The findings suggest that outpatient palliative care is a growing specialty, she suggested. The data are not mature enough to assess any impact on the quality of end-of-life care or on the efficiency of care, she added.
Dr. Chen and Mr. Pesavento reported having no financial disclosures. Dr. Ramchandran’s study was funded in part by the Stanford Corporate Partners Fund and by various Stanford departments. No financial disclosures were available for the other presenters.
Regarding Dr. Chen’s study, this study does find that we can provide support to patients and their families with appropriately staffed and trained medical teams that specialize in palliative care to really decrease futile, invasive, and expensive care at the end of life. This is broad implications to our patients and their families as they talk about prognosis with their physicians, and also to the physicians taking care of these patients, who may have not had a longitudinal relationship with these patients. Immediate feedback to the caring physicians can decrease some of these high resource utilization maneuvers that don’t provide improvement in quality of life.
Dr. Jyoti D. Patel is a member of ASCO’s Cancer Communications Committee and a thoracic oncologist at Northwestern University, Chicago. She gave these remarks in an online press conference organized by ASCO.
Regarding Dr. Chen’s study, this study does find that we can provide support to patients and their families with appropriately staffed and trained medical teams that specialize in palliative care to really decrease futile, invasive, and expensive care at the end of life. This is broad implications to our patients and their families as they talk about prognosis with their physicians, and also to the physicians taking care of these patients, who may have not had a longitudinal relationship with these patients. Immediate feedback to the caring physicians can decrease some of these high resource utilization maneuvers that don’t provide improvement in quality of life.
Dr. Jyoti D. Patel is a member of ASCO’s Cancer Communications Committee and a thoracic oncologist at Northwestern University, Chicago. She gave these remarks in an online press conference organized by ASCO.
Regarding Dr. Chen’s study, this study does find that we can provide support to patients and their families with appropriately staffed and trained medical teams that specialize in palliative care to really decrease futile, invasive, and expensive care at the end of life. This is broad implications to our patients and their families as they talk about prognosis with their physicians, and also to the physicians taking care of these patients, who may have not had a longitudinal relationship with these patients. Immediate feedback to the caring physicians can decrease some of these high resource utilization maneuvers that don’t provide improvement in quality of life.
Dr. Jyoti D. Patel is a member of ASCO’s Cancer Communications Committee and a thoracic oncologist at Northwestern University, Chicago. She gave these remarks in an online press conference organized by ASCO.
From Hollywood to Washington, care at the end of life increasingly is part of the national conversation.
As more than 70 million baby boomers (Americans born between 1946 and 1964) approach the end of their life spans, the cultural, clinical and socioeconomic impacts of end-of-life care have become high-profile topics. The French film "Amour," which depicts the challenges faced by an octogenarian couple after the wife has a series of strokes, has received an Academy Award Best Picture nomination. The Institute of Medicine will convene a panel of experts on Feb. 22-24 in Washington to examine the state of end-of-life care. The goal of the IOM Committee on Transforming End of Life Care is to produce a consensus report by 2014 to address end-of-life care. "Coordinated, expert, compassionate care for people dying from chronic diseases continues to challenge the American health care system," according to the IOM’s online announcement of the meeting.
In addition, the Coalition to Transform Advanced Care is hosting a National Summit on Advanced Illness Care on Jan. 29-30 in Washington. The Coalition includes a wide range of constituencies including the IOM, the American Heart Association, the American Academy of Hospice and Palliative Medicine, and the American Geriatrics Society, as well as insurers, health systems, patient advocacy groups, and others.
As policy issues are discussed and begin to take shape, outcomes research focused on end-of-life care will increasingly gain importance. In the area of cancer care, here are some of the highlights of such research presented at a Quality Care Symposium sponsored by the American Society of Clinical Oncology in December 2012 in San Diego.
Palliative care teams: A palliative care team formed by Dr. Allen R. Chen and his associates at Johns Hopkins’s comprehensive cancer center helped change patient and family decisions regarding end-of-life care during a 4-year period and decreased use of intensive or invasive procedures in the last 6 months of life.
The team offered inpatient and clinic consultations and didactic sessions to physicians to improve how they discuss end-of-life issues with patients, plus support for family meetings to discuss and document the goals of care, said Dr. Chen, associate professor of oncology and pediatrics at Johns Hopkins University, Baltimore.
Of the 525 oncology patients who died in the cancer center while hospitalized from 2008 through 2011, the proportion who chose to have do-not-resuscitate (DNR) orders, withdrew ICU support, or chose comfort care instead of more aggressive care increased from 81% to 95% over the course of the 4 years, a statistically significant difference, he reported.
The rate of ICU care during patients’ final hospitalizations did not change significantly, but the proportion of patients who were put on mechanical ventilation for more than 14 days decreased significantly from 10% to 5%. These earlier withdrawals of care did not increase the risk of death, Dr. Chen said – the rate of survival to discharge from the oncology ICU did not change significantly.
The investigators now are looking for ways to minimize ICU visits at the end of life, he said. The presence of advanced cancer, being on a cardiac monitor, or needing supplemental oxygen foreshadowed critical illness in patients in the study. "We want to facilitate the difficult discussion" about end-of-life care choices "before critical care is needed," he said. So far, their efforts haven’t resulted in decreased use of ICU services at the end of life.
Minimizing surgical risks: One of the first comprehensive analyses of surgical outcomes in patients with disseminated cancer found that the risk of death increases greatly with emergency surgery.
John Pesavento, a medical student at Creighton University, Omaha, Neb., and his associates analyzed preoperative and postoperative data from the American College of Surgeon’s National Surgical Quality Improvement Program database on move than 147,000 patients who underwent surgical procedures between 2005 and 2008.
Eight of the 10 most common procedures resulted in significantly higher 30-day mortality rates in the cancer patients as compared with the same surgeries in patients who did not have disseminated cancer.
Comparing patients with and without disseminated cancer, 30-day mortality rates were 21% and 15%, respectively, after exploration of the abdomen, 15% and 9% after removal of the small bowel, 11% and 6% after colon removal, 11% and 5% after colostomy, 10% and 5% after partial removal of the colon, 10% and 0.5% after cholecystectomy, 1.8% and 0.9% after repair of a bowel opening, and 1% and 0.1% after mastectomy, he reported. The most common operations in patients with disseminated cancer were partial removal of the colon (in 11%), partial removal of the liver (9%), partial removal of the intestine (5%), and abdominal exploration (5%), he reported in a poster presentation.
When done as emergency procedures, however, 7 of the top 10 surgeries led to significantly higher 30-day mortality rates for disseminated cancer patients. Death rates in patients with disseminated cancer were 44% for emergency surgery and 12% for nonemergent surgery to explore the abdomen; the respective rates were 33% and 6% after bowel-to-bowel fusion, 31% and 4% after removal of the colon, 28% and 10% after removal of the small intestine, 23% and 5% after cholecystectomy, 22% and 7% after partial removal of the colon, and 19% and 9% after colostomy.
The findings should help physicians counsel their patients with disseminated cancer to help them decide whether it’s worth undergoing surgery – especially emergency surgery – given the higher risks of death, Mr. Pesavento said.
Physicians’ attitudes and education: In a separate study, 16 urologists and four primary care physicians who were undergoing surgical training in urology were interviewed about their attitudes regarding end-of-life care for men dying of prostate cancer. They viewed current end-of-life care as shoddily organized and poorly integrated, and said that ideal outcomes should be defined by patients’ own values and preferences, Dr. Jonathan Bergman and his associates reported in a poster presentation.
The physicians said that, ideally, a multidisciplinary team would care for dying patients, but respondents varied in the degree to which they saw themselves participating, reported Dr. Bergman of the University of California, Los Angeles.
The findings suggest that physician education about end-of-life care needs improvement, and that clinicians should be guided to deliver end-of-life care that is patient-centered and congruent with patients’ values, he said.
Dying in the hospital: Among 2,621 patients with solid tumors, those who had contact with a specialist palliative care team more than a month before their deaths were less likely to die in the hospital (16%) than were patients who had later or no contact with the team (20%), J. Brian Cassel, Ph.D., reported in a poster presentation.
Dr. Cassel and his associates analyzed claims data on the last 6 months of life for 3,128 adults with cancer who had at least one contact with the Virginia Commonwealth University cancer center in Richmond between January 2009 and July 2011. The data set included patients who had solid tumors, underwent bone marrow transfer, or had other hematologic malignancies.
The findings provided a snapshot of end-of-life care at the university, where 32% of the cancer patients were admitted to the hospital within their last 30 days of life, 19% had at least one readmission during their last 6 months of life, and 15% died in the hospital. Chemotherapy was given to 11% in their last month of life, and to 7% in their last 2 weeks of life, said Dr. Cassel of the university.
The specialist palliative care team made contact with 28% of patients a median of 6-10 days before the death of patients with bone marrow transfer or other nonhematologic malignancies and a median of 25 days before the death of patients with solid tumors.
Chemotherapy at the end of life: Patients with hematologic malignancies were significantly more likely to get chemotherapy in the last 30 days of life (38%) compared with patients with solid tumors (8%), Dr. Alma Rodriguez and her associates reported in a poster presentation.
The investigators reviewed data on 7,399 patients who received care for a solid tumor or hematological malignancy at the University of Texas M.D. Anderson Cancer Center, Houston, and died between December 2010 and May 2012. Overall, 14% of patients received chemotherapy within the last 30 days of life.
Of the 1,262 patients who died in the hospital, 44% received chemotherapy within the last 30 days of life, compared with 7% of the 6,137 patients who died in other locations, reported Dr. Rodriguez, professor of medicine at the cancer center.
Chemotherapy within the last 30 days of life was 3 times more likely in patients with metastatic solid tumors, 14 times more likely in patients with nonrelapsed hematologic malignancy, and 36 times more likely in patients with historical or current relapse of hematologic malignancy.
Patients 65 years or older were 38% less likely than were younger patients to get chemotherapy within the last 30 days of life. Patients with one or more comorbidity (most frequently heart failure and coronary artery diseases) were 28% less likely to get chemotherapy within the last 30 days of life as compared with patients without comorbidities.
"As oncologists, we must communicate clearly with our patients about realistic goals of treatment and the likelihood of life-threatening complications of chemotherapy," Dr. Rodriguez said in the poster.
Outpatient palliative care: Dr. Kavitha Ramchandran and her associates at Stanford (Calif.) University studied their system’s electronic medical records to look at the use of palliative care in outpatient clinics from January through September 2012. The number of palliative care contacts with outpatient clinic patients increased from 10 in January to 45 in September. The number of physicians referring outpatients to palliative care increased from 6 in January to 21 in September, she said in a poster presentation.
More than 65% of patients who were referred for palliative care were younger than 65 years, said Dr. Ramchandran of the university. Most patients had only one visit with palliative care (41%) or two visits (23%).
The findings suggest that outpatient palliative care is a growing specialty, she suggested. The data are not mature enough to assess any impact on the quality of end-of-life care or on the efficiency of care, she added.
Dr. Chen and Mr. Pesavento reported having no financial disclosures. Dr. Ramchandran’s study was funded in part by the Stanford Corporate Partners Fund and by various Stanford departments. No financial disclosures were available for the other presenters.
From Hollywood to Washington, care at the end of life increasingly is part of the national conversation.
As more than 70 million baby boomers (Americans born between 1946 and 1964) approach the end of their life spans, the cultural, clinical and socioeconomic impacts of end-of-life care have become high-profile topics. The French film "Amour," which depicts the challenges faced by an octogenarian couple after the wife has a series of strokes, has received an Academy Award Best Picture nomination. The Institute of Medicine will convene a panel of experts on Feb. 22-24 in Washington to examine the state of end-of-life care. The goal of the IOM Committee on Transforming End of Life Care is to produce a consensus report by 2014 to address end-of-life care. "Coordinated, expert, compassionate care for people dying from chronic diseases continues to challenge the American health care system," according to the IOM’s online announcement of the meeting.
In addition, the Coalition to Transform Advanced Care is hosting a National Summit on Advanced Illness Care on Jan. 29-30 in Washington. The Coalition includes a wide range of constituencies including the IOM, the American Heart Association, the American Academy of Hospice and Palliative Medicine, and the American Geriatrics Society, as well as insurers, health systems, patient advocacy groups, and others.
As policy issues are discussed and begin to take shape, outcomes research focused on end-of-life care will increasingly gain importance. In the area of cancer care, here are some of the highlights of such research presented at a Quality Care Symposium sponsored by the American Society of Clinical Oncology in December 2012 in San Diego.
Palliative care teams: A palliative care team formed by Dr. Allen R. Chen and his associates at Johns Hopkins’s comprehensive cancer center helped change patient and family decisions regarding end-of-life care during a 4-year period and decreased use of intensive or invasive procedures in the last 6 months of life.
The team offered inpatient and clinic consultations and didactic sessions to physicians to improve how they discuss end-of-life issues with patients, plus support for family meetings to discuss and document the goals of care, said Dr. Chen, associate professor of oncology and pediatrics at Johns Hopkins University, Baltimore.
Of the 525 oncology patients who died in the cancer center while hospitalized from 2008 through 2011, the proportion who chose to have do-not-resuscitate (DNR) orders, withdrew ICU support, or chose comfort care instead of more aggressive care increased from 81% to 95% over the course of the 4 years, a statistically significant difference, he reported.
The rate of ICU care during patients’ final hospitalizations did not change significantly, but the proportion of patients who were put on mechanical ventilation for more than 14 days decreased significantly from 10% to 5%. These earlier withdrawals of care did not increase the risk of death, Dr. Chen said – the rate of survival to discharge from the oncology ICU did not change significantly.
The investigators now are looking for ways to minimize ICU visits at the end of life, he said. The presence of advanced cancer, being on a cardiac monitor, or needing supplemental oxygen foreshadowed critical illness in patients in the study. "We want to facilitate the difficult discussion" about end-of-life care choices "before critical care is needed," he said. So far, their efforts haven’t resulted in decreased use of ICU services at the end of life.
Minimizing surgical risks: One of the first comprehensive analyses of surgical outcomes in patients with disseminated cancer found that the risk of death increases greatly with emergency surgery.
John Pesavento, a medical student at Creighton University, Omaha, Neb., and his associates analyzed preoperative and postoperative data from the American College of Surgeon’s National Surgical Quality Improvement Program database on move than 147,000 patients who underwent surgical procedures between 2005 and 2008.
Eight of the 10 most common procedures resulted in significantly higher 30-day mortality rates in the cancer patients as compared with the same surgeries in patients who did not have disseminated cancer.
Comparing patients with and without disseminated cancer, 30-day mortality rates were 21% and 15%, respectively, after exploration of the abdomen, 15% and 9% after removal of the small bowel, 11% and 6% after colon removal, 11% and 5% after colostomy, 10% and 5% after partial removal of the colon, 10% and 0.5% after cholecystectomy, 1.8% and 0.9% after repair of a bowel opening, and 1% and 0.1% after mastectomy, he reported. The most common operations in patients with disseminated cancer were partial removal of the colon (in 11%), partial removal of the liver (9%), partial removal of the intestine (5%), and abdominal exploration (5%), he reported in a poster presentation.
When done as emergency procedures, however, 7 of the top 10 surgeries led to significantly higher 30-day mortality rates for disseminated cancer patients. Death rates in patients with disseminated cancer were 44% for emergency surgery and 12% for nonemergent surgery to explore the abdomen; the respective rates were 33% and 6% after bowel-to-bowel fusion, 31% and 4% after removal of the colon, 28% and 10% after removal of the small intestine, 23% and 5% after cholecystectomy, 22% and 7% after partial removal of the colon, and 19% and 9% after colostomy.
The findings should help physicians counsel their patients with disseminated cancer to help them decide whether it’s worth undergoing surgery – especially emergency surgery – given the higher risks of death, Mr. Pesavento said.
Physicians’ attitudes and education: In a separate study, 16 urologists and four primary care physicians who were undergoing surgical training in urology were interviewed about their attitudes regarding end-of-life care for men dying of prostate cancer. They viewed current end-of-life care as shoddily organized and poorly integrated, and said that ideal outcomes should be defined by patients’ own values and preferences, Dr. Jonathan Bergman and his associates reported in a poster presentation.
The physicians said that, ideally, a multidisciplinary team would care for dying patients, but respondents varied in the degree to which they saw themselves participating, reported Dr. Bergman of the University of California, Los Angeles.
The findings suggest that physician education about end-of-life care needs improvement, and that clinicians should be guided to deliver end-of-life care that is patient-centered and congruent with patients’ values, he said.
Dying in the hospital: Among 2,621 patients with solid tumors, those who had contact with a specialist palliative care team more than a month before their deaths were less likely to die in the hospital (16%) than were patients who had later or no contact with the team (20%), J. Brian Cassel, Ph.D., reported in a poster presentation.
Dr. Cassel and his associates analyzed claims data on the last 6 months of life for 3,128 adults with cancer who had at least one contact with the Virginia Commonwealth University cancer center in Richmond between January 2009 and July 2011. The data set included patients who had solid tumors, underwent bone marrow transfer, or had other hematologic malignancies.
The findings provided a snapshot of end-of-life care at the university, where 32% of the cancer patients were admitted to the hospital within their last 30 days of life, 19% had at least one readmission during their last 6 months of life, and 15% died in the hospital. Chemotherapy was given to 11% in their last month of life, and to 7% in their last 2 weeks of life, said Dr. Cassel of the university.
The specialist palliative care team made contact with 28% of patients a median of 6-10 days before the death of patients with bone marrow transfer or other nonhematologic malignancies and a median of 25 days before the death of patients with solid tumors.
Chemotherapy at the end of life: Patients with hematologic malignancies were significantly more likely to get chemotherapy in the last 30 days of life (38%) compared with patients with solid tumors (8%), Dr. Alma Rodriguez and her associates reported in a poster presentation.
The investigators reviewed data on 7,399 patients who received care for a solid tumor or hematological malignancy at the University of Texas M.D. Anderson Cancer Center, Houston, and died between December 2010 and May 2012. Overall, 14% of patients received chemotherapy within the last 30 days of life.
Of the 1,262 patients who died in the hospital, 44% received chemotherapy within the last 30 days of life, compared with 7% of the 6,137 patients who died in other locations, reported Dr. Rodriguez, professor of medicine at the cancer center.
Chemotherapy within the last 30 days of life was 3 times more likely in patients with metastatic solid tumors, 14 times more likely in patients with nonrelapsed hematologic malignancy, and 36 times more likely in patients with historical or current relapse of hematologic malignancy.
Patients 65 years or older were 38% less likely than were younger patients to get chemotherapy within the last 30 days of life. Patients with one or more comorbidity (most frequently heart failure and coronary artery diseases) were 28% less likely to get chemotherapy within the last 30 days of life as compared with patients without comorbidities.
"As oncologists, we must communicate clearly with our patients about realistic goals of treatment and the likelihood of life-threatening complications of chemotherapy," Dr. Rodriguez said in the poster.
Outpatient palliative care: Dr. Kavitha Ramchandran and her associates at Stanford (Calif.) University studied their system’s electronic medical records to look at the use of palliative care in outpatient clinics from January through September 2012. The number of palliative care contacts with outpatient clinic patients increased from 10 in January to 45 in September. The number of physicians referring outpatients to palliative care increased from 6 in January to 21 in September, she said in a poster presentation.
More than 65% of patients who were referred for palliative care were younger than 65 years, said Dr. Ramchandran of the university. Most patients had only one visit with palliative care (41%) or two visits (23%).
The findings suggest that outpatient palliative care is a growing specialty, she suggested. The data are not mature enough to assess any impact on the quality of end-of-life care or on the efficiency of care, she added.
Dr. Chen and Mr. Pesavento reported having no financial disclosures. Dr. Ramchandran’s study was funded in part by the Stanford Corporate Partners Fund and by various Stanford departments. No financial disclosures were available for the other presenters.

Optimizing Home Health Care: Enhanced Value and Improved Outcomes
Supplement Editor:
William Zafirau, MD
Supplement Co-Editors:
Steven H. Landers, MD, MPH, and Cindy Vunovich, RN, BSN, MSM
Contents
Introduction—Medicine’s future: Helping patients stay healthy at home
Steven H. Landers, MD, MPH
Care transitions and advanced home care models
Improving patient outcomes with better care transitions: The role for home health
Michael O. Fleming, MD, and Tara Trahan Haney
Improving outcomes and lowering costs by applying advanced models of in-home care
Peter A. Boling, MD; Rashmi V. Chandekar, MD; Beth Hungate, MS, ANP-BC; Martha Purvis, MSN; Rachel Selby-Penczak, MD; and Linda J. Abbey, MD
Home care for knee replacement and heart failure
In-home care following total knee replacement
Mark I. Froimson, MD, MBA
Home-based care for heart failure: Cleveland Clinic's "Heart Care at Home" transitional care program
Eiran Z. Gorodeski, MD, MPH; Sandra Chlad, NP; and Seth Vilensky, MBA
Technology innovations and palliative care
The case for "connected health" at home
Steven H. Landers, MD, MPH
Innovative models of home-based palliative care
Margherita C. Labson, RN, MSHSA, CPHQ, CCM; Michele M. Sacco, MS; David E. Weissman, MD; Betsy Gornet, FACHE; and Brad Stuart, MD
Cleveland Clinic Journal of Medicine interview
Accountable care and patient-centered medical homes: Implications for office-based practice
An interview with David L. Longworth, MD
Supplement Editor:
William Zafirau, MD
Supplement Co-Editors:
Steven H. Landers, MD, MPH, and Cindy Vunovich, RN, BSN, MSM
Contents
Introduction—Medicine’s future: Helping patients stay healthy at home
Steven H. Landers, MD, MPH
Care transitions and advanced home care models
Improving patient outcomes with better care transitions: The role for home health
Michael O. Fleming, MD, and Tara Trahan Haney
Improving outcomes and lowering costs by applying advanced models of in-home care
Peter A. Boling, MD; Rashmi V. Chandekar, MD; Beth Hungate, MS, ANP-BC; Martha Purvis, MSN; Rachel Selby-Penczak, MD; and Linda J. Abbey, MD
Home care for knee replacement and heart failure
In-home care following total knee replacement
Mark I. Froimson, MD, MBA
Home-based care for heart failure: Cleveland Clinic's "Heart Care at Home" transitional care program
Eiran Z. Gorodeski, MD, MPH; Sandra Chlad, NP; and Seth Vilensky, MBA
Technology innovations and palliative care
The case for "connected health" at home
Steven H. Landers, MD, MPH
Innovative models of home-based palliative care
Margherita C. Labson, RN, MSHSA, CPHQ, CCM; Michele M. Sacco, MS; David E. Weissman, MD; Betsy Gornet, FACHE; and Brad Stuart, MD
Cleveland Clinic Journal of Medicine interview
Accountable care and patient-centered medical homes: Implications for office-based practice
An interview with David L. Longworth, MD
Supplement Editor:
William Zafirau, MD
Supplement Co-Editors:
Steven H. Landers, MD, MPH, and Cindy Vunovich, RN, BSN, MSM
Contents
Introduction—Medicine’s future: Helping patients stay healthy at home
Steven H. Landers, MD, MPH
Care transitions and advanced home care models
Improving patient outcomes with better care transitions: The role for home health
Michael O. Fleming, MD, and Tara Trahan Haney
Improving outcomes and lowering costs by applying advanced models of in-home care
Peter A. Boling, MD; Rashmi V. Chandekar, MD; Beth Hungate, MS, ANP-BC; Martha Purvis, MSN; Rachel Selby-Penczak, MD; and Linda J. Abbey, MD
Home care for knee replacement and heart failure
In-home care following total knee replacement
Mark I. Froimson, MD, MBA
Home-based care for heart failure: Cleveland Clinic's "Heart Care at Home" transitional care program
Eiran Z. Gorodeski, MD, MPH; Sandra Chlad, NP; and Seth Vilensky, MBA
Technology innovations and palliative care
The case for "connected health" at home
Steven H. Landers, MD, MPH
Innovative models of home-based palliative care
Margherita C. Labson, RN, MSHSA, CPHQ, CCM; Michele M. Sacco, MS; David E. Weissman, MD; Betsy Gornet, FACHE; and Brad Stuart, MD
Cleveland Clinic Journal of Medicine interview
Accountable care and patient-centered medical homes: Implications for office-based practice
An interview with David L. Longworth, MD
Analgesia for the Body, Mind, and Soul: It’s Complicated
Cancer pain wasn’t on my mind when I carved out time this week to attend Cottage Health System’s psychiatric grand rounds entitled, “Dueling Diagnosis: Complicated Pain and Substance Use Disorders,” in Santa Barbara. But the lecture by Dr. Jerry Lerner, chief of pain medicine at Arizona’s Sierra Tucson residential treatment center, soon had me thinking about the many levels of pain suffered by patients diagnosed with cancer and other organic diseases.
Ironically, the oncology community has struggled for years against the erroneous belief among patients and family members that effectively managing cancer pain will make addicts of patients once they’re cured. It’s simply not true, of course, but the barriers to effective cancer pain management are vast, multifactorial, and deeply held, as documented by the International Association for the Study of Pain.
As they say in the pain medicine world, it’s complicated.

And becoming even more so, it would seem.
A growing epidemic of prescription painkiller abuse, especially among young adults, will mean that a growing number of cancer patients arrive at our doorsteps already grappling with pre-existing addictions to opioids. The past decade has seen a 400% increase in substance disorders arising from prescription painkiller use, resulting in an overdose rate that today outpaces deaths from heroin and cocaine combined, according to the Centers for Disease Control and Prevention.
Dr. Lerner outlined a delicate strategy for treating moderate to severe pain in patients with preexisting addiction or dependency problems. Any pain at a 6 or above on a 0-10 pain scale must be treated medically, he said, or attempts at treating the substance problem will be undermined by a diminishment of therapeutic trust and a lack of “attendance, attention, and intention.”
On the other hand, pain is more than the mere presence of nerve signals to the brain because of compromised tissue.
Long-term opioid use can create hyperalgesia, a condition where the body is actually more sensitized to pain, Dr. Lerner explained. “Things that didn’t hurt before, hurt,” he said.
With 1 in 20 Americans over the age of 12 years – an estimated 12 million people – diverting and using prescription painkillers “nonmedically,” chances are that many present and future cancer patients will present to oncologists already resistant to the relief such medications might offer for cancer-related pain.
Dr. Lerner emphasized as well that pain of all kinds is influenced not only by physical biological events (tumor growth, for example), but by other factors as well: inflammation (sometimes activated or exacerbated by stress and fear), hypersensitivity from overactivity of the sympathetic nervous system, unresolved emotional trauma, and dysfunctional relationships.
He views each of these as “tumblers” in the combination lock that must be cracked to adequately treat pain, be it the result of a broken bone, a tumor, or a body-wide pain syndrome of unknown origin.
With most cancer patients, the physical source of pain is clear, and no preexisting painkiller addiction will interfere with the action of appropriately prescribed analgesics. Still, the evidence is growing that pain is a multisystemic, multifactorial challenge, felt more acutely in the face of fear or stress, so the wise guidance of those who treat “Dueling Diagnoses” will add value to the treatment of cancer pain, even in the most straightforward of cases.
Dr. Freed is a psychologist in Santa Barbara, Calif., and a medical journalist.
Cancer pain wasn’t on my mind when I carved out time this week to attend Cottage Health System’s psychiatric grand rounds entitled, “Dueling Diagnosis: Complicated Pain and Substance Use Disorders,” in Santa Barbara. But the lecture by Dr. Jerry Lerner, chief of pain medicine at Arizona’s Sierra Tucson residential treatment center, soon had me thinking about the many levels of pain suffered by patients diagnosed with cancer and other organic diseases.
Ironically, the oncology community has struggled for years against the erroneous belief among patients and family members that effectively managing cancer pain will make addicts of patients once they’re cured. It’s simply not true, of course, but the barriers to effective cancer pain management are vast, multifactorial, and deeply held, as documented by the International Association for the Study of Pain.
As they say in the pain medicine world, it’s complicated.
And becoming even more so, it would seem.
A growing epidemic of prescription painkiller abuse, especially among young adults, will mean that a growing number of cancer patients arrive at our doorsteps already grappling with pre-existing addictions to opioids. The past decade has seen a 400% increase in substance disorders arising from prescription painkiller use, resulting in an overdose rate that today outpaces deaths from heroin and cocaine combined, according to the Centers for Disease Control and Prevention.
Dr. Lerner outlined a delicate strategy for treating moderate to severe pain in patients with preexisting addiction or dependency problems. Any pain at a 6 or above on a 0-10 pain scale must be treated medically, he said, or attempts at treating the substance problem will be undermined by a diminishment of therapeutic trust and a lack of “attendance, attention, and intention.”
On the other hand, pain is more than the mere presence of nerve signals to the brain because of compromised tissue.
Long-term opioid use can create hyperalgesia, a condition where the body is actually more sensitized to pain, Dr. Lerner explained. “Things that didn’t hurt before, hurt,” he said.
With 1 in 20 Americans over the age of 12 years – an estimated 12 million people – diverting and using prescription painkillers “nonmedically,” chances are that many present and future cancer patients will present to oncologists already resistant to the relief such medications might offer for cancer-related pain.
Dr. Lerner emphasized as well that pain of all kinds is influenced not only by physical biological events (tumor growth, for example), but by other factors as well: inflammation (sometimes activated or exacerbated by stress and fear), hypersensitivity from overactivity of the sympathetic nervous system, unresolved emotional trauma, and dysfunctional relationships.
He views each of these as “tumblers” in the combination lock that must be cracked to adequately treat pain, be it the result of a broken bone, a tumor, or a body-wide pain syndrome of unknown origin.
With most cancer patients, the physical source of pain is clear, and no preexisting painkiller addiction will interfere with the action of appropriately prescribed analgesics. Still, the evidence is growing that pain is a multisystemic, multifactorial challenge, felt more acutely in the face of fear or stress, so the wise guidance of those who treat “Dueling Diagnoses” will add value to the treatment of cancer pain, even in the most straightforward of cases.
Dr. Freed is a psychologist in Santa Barbara, Calif., and a medical journalist.
Cancer pain wasn’t on my mind when I carved out time this week to attend Cottage Health System’s psychiatric grand rounds entitled, “Dueling Diagnosis: Complicated Pain and Substance Use Disorders,” in Santa Barbara. But the lecture by Dr. Jerry Lerner, chief of pain medicine at Arizona’s Sierra Tucson residential treatment center, soon had me thinking about the many levels of pain suffered by patients diagnosed with cancer and other organic diseases.
Ironically, the oncology community has struggled for years against the erroneous belief among patients and family members that effectively managing cancer pain will make addicts of patients once they’re cured. It’s simply not true, of course, but the barriers to effective cancer pain management are vast, multifactorial, and deeply held, as documented by the International Association for the Study of Pain.
As they say in the pain medicine world, it’s complicated.
And becoming even more so, it would seem.
A growing epidemic of prescription painkiller abuse, especially among young adults, will mean that a growing number of cancer patients arrive at our doorsteps already grappling with pre-existing addictions to opioids. The past decade has seen a 400% increase in substance disorders arising from prescription painkiller use, resulting in an overdose rate that today outpaces deaths from heroin and cocaine combined, according to the Centers for Disease Control and Prevention.
Dr. Lerner outlined a delicate strategy for treating moderate to severe pain in patients with preexisting addiction or dependency problems. Any pain at a 6 or above on a 0-10 pain scale must be treated medically, he said, or attempts at treating the substance problem will be undermined by a diminishment of therapeutic trust and a lack of “attendance, attention, and intention.”
On the other hand, pain is more than the mere presence of nerve signals to the brain because of compromised tissue.
Long-term opioid use can create hyperalgesia, a condition where the body is actually more sensitized to pain, Dr. Lerner explained. “Things that didn’t hurt before, hurt,” he said.
With 1 in 20 Americans over the age of 12 years – an estimated 12 million people – diverting and using prescription painkillers “nonmedically,” chances are that many present and future cancer patients will present to oncologists already resistant to the relief such medications might offer for cancer-related pain.
Dr. Lerner emphasized as well that pain of all kinds is influenced not only by physical biological events (tumor growth, for example), but by other factors as well: inflammation (sometimes activated or exacerbated by stress and fear), hypersensitivity from overactivity of the sympathetic nervous system, unresolved emotional trauma, and dysfunctional relationships.
He views each of these as “tumblers” in the combination lock that must be cracked to adequately treat pain, be it the result of a broken bone, a tumor, or a body-wide pain syndrome of unknown origin.
With most cancer patients, the physical source of pain is clear, and no preexisting painkiller addiction will interfere with the action of appropriately prescribed analgesics. Still, the evidence is growing that pain is a multisystemic, multifactorial challenge, felt more acutely in the face of fear or stress, so the wise guidance of those who treat “Dueling Diagnoses” will add value to the treatment of cancer pain, even in the most straightforward of cases.
Dr. Freed is a psychologist in Santa Barbara, Calif., and a medical journalist.

Tips to Facing Difficult Patient Conversations
At the eighth annual Chicago Supportive Oncology Conference, we spoke with Dr. Anthony Back about talking to patients about the cost of care and whether the costs are worth it. Dr. Back stressed that it is crucial for cost to be a part of the decision making process, and not a separate stand-alone issue. He added that it is the physician who should take the lead in initiating this discussion.
Dr. Back is a professor in the Department of Medicine, Division of Oncology at the University of Washington's School of Medicine and a medical oncologist with the Seattle Cancer Care Alliance in Seattle, Washington.
At the eighth annual Chicago Supportive Oncology Conference, we spoke with Dr. Anthony Back about talking to patients about the cost of care and whether the costs are worth it. Dr. Back stressed that it is crucial for cost to be a part of the decision making process, and not a separate stand-alone issue. He added that it is the physician who should take the lead in initiating this discussion.
Dr. Back is a professor in the Department of Medicine, Division of Oncology at the University of Washington's School of Medicine and a medical oncologist with the Seattle Cancer Care Alliance in Seattle, Washington.
At the eighth annual Chicago Supportive Oncology Conference, we spoke with Dr. Anthony Back about talking to patients about the cost of care and whether the costs are worth it. Dr. Back stressed that it is crucial for cost to be a part of the decision making process, and not a separate stand-alone issue. He added that it is the physician who should take the lead in initiating this discussion.
Dr. Back is a professor in the Department of Medicine, Division of Oncology at the University of Washington's School of Medicine and a medical oncologist with the Seattle Cancer Care Alliance in Seattle, Washington.
End-of-Life Care Can Bring on Challenges for Hospitalists
How do you cope with a family that wants you to "do everything" for their seriously ill loved one? This dilemma was one of the topics explored at the Management of the Hospitalized Patient conference held last month at the University of California at San Francisco (UCSF).
"We don't actually know what 'everything' means to the family, not without probing into a range of possible meanings," said presenter Steve Pantilat, MD, FACP, SFHM, hospitalist and director of the palliative-care service at UCSF Medical Center. "The family may not have a clear understanding of what 'everything' entails, including mechanical ventilation or cardio-pulmonary resuscitation. I prefer to ask, 'How were you hoping we could help?' The answer can provide a great deal of insight."
In spite of various tools to aid decisions, prognosis is inherently uncertain, said co-presenter Matthew Gonzales, MD, assistant professor of hospital medicine and palliative care at UCSF Medical Center. "We use the Palliative Performance Scale [PDF]."
The family might not trust the hospitalist’s prognosis, especially when meeting the doctor for the first time in a stressful situation, and there might be disagreements within the family about the course of treatment, Dr. Gonzales said. Cultural differences also come into play.
"I have started to ask, 'How do you decide these questions in your family?' because of the differences within a cultural group," Dr. Pantilat said. "If they talk about hoping for a miracle, I probe the meaning of 'miracle' to them. Physicians can't work on the basis of miracles; they have to practice medicine. And you should resist getting drawn into a religious debate. That's a loser for the physician."
Visit our website for more information about palliative care.
How do you cope with a family that wants you to "do everything" for their seriously ill loved one? This dilemma was one of the topics explored at the Management of the Hospitalized Patient conference held last month at the University of California at San Francisco (UCSF).
"We don't actually know what 'everything' means to the family, not without probing into a range of possible meanings," said presenter Steve Pantilat, MD, FACP, SFHM, hospitalist and director of the palliative-care service at UCSF Medical Center. "The family may not have a clear understanding of what 'everything' entails, including mechanical ventilation or cardio-pulmonary resuscitation. I prefer to ask, 'How were you hoping we could help?' The answer can provide a great deal of insight."
In spite of various tools to aid decisions, prognosis is inherently uncertain, said co-presenter Matthew Gonzales, MD, assistant professor of hospital medicine and palliative care at UCSF Medical Center. "We use the Palliative Performance Scale [PDF]."
The family might not trust the hospitalist’s prognosis, especially when meeting the doctor for the first time in a stressful situation, and there might be disagreements within the family about the course of treatment, Dr. Gonzales said. Cultural differences also come into play.
"I have started to ask, 'How do you decide these questions in your family?' because of the differences within a cultural group," Dr. Pantilat said. "If they talk about hoping for a miracle, I probe the meaning of 'miracle' to them. Physicians can't work on the basis of miracles; they have to practice medicine. And you should resist getting drawn into a religious debate. That's a loser for the physician."
Visit our website for more information about palliative care.
How do you cope with a family that wants you to "do everything" for their seriously ill loved one? This dilemma was one of the topics explored at the Management of the Hospitalized Patient conference held last month at the University of California at San Francisco (UCSF).
"We don't actually know what 'everything' means to the family, not without probing into a range of possible meanings," said presenter Steve Pantilat, MD, FACP, SFHM, hospitalist and director of the palliative-care service at UCSF Medical Center. "The family may not have a clear understanding of what 'everything' entails, including mechanical ventilation or cardio-pulmonary resuscitation. I prefer to ask, 'How were you hoping we could help?' The answer can provide a great deal of insight."
In spite of various tools to aid decisions, prognosis is inherently uncertain, said co-presenter Matthew Gonzales, MD, assistant professor of hospital medicine and palliative care at UCSF Medical Center. "We use the Palliative Performance Scale [PDF]."
The family might not trust the hospitalist’s prognosis, especially when meeting the doctor for the first time in a stressful situation, and there might be disagreements within the family about the course of treatment, Dr. Gonzales said. Cultural differences also come into play.
"I have started to ask, 'How do you decide these questions in your family?' because of the differences within a cultural group," Dr. Pantilat said. "If they talk about hoping for a miracle, I probe the meaning of 'miracle' to them. Physicians can't work on the basis of miracles; they have to practice medicine. And you should resist getting drawn into a religious debate. That's a loser for the physician."
Visit our website for more information about palliative care.
Earlier End-of-Life Talks Deter Aggressive Care of Terminal Cancer Patients
Patients with stage IV lung or colorectal cancer who had end-of-life discussions with caregivers before the last 30 days of life were significantly less likely to receive aggressive care in their final days and more likely to get hospice care and to enter hospice earlier, a study of 1,231 patients found.
Nearly half received some kind of aggressive care in their last 30 days (47%), including chemotherapy in the last 14 days (16%), ICU care in the last 30 days (6%), and/or acute hospital-based care in the last 30 days of life (40%), Dr. Jennifer W. Mack and her associates reported.
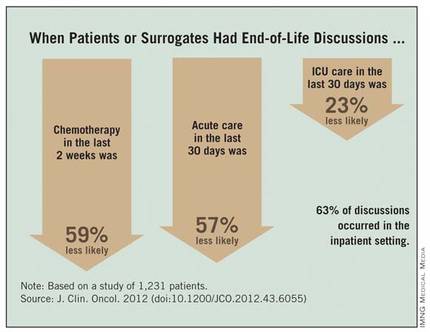
Multiple current guidelines recommend starting end-of-life care planning for patients with incurable cancer early in the course of the disease while patients are relatively stable, not when they are acutely deteriorating.
Many physicians in the study postponed the discussion until the final month of life, and many patients didn’t remember or didn’t recognize the end-of-life discussions. Discussions that were documented in charts were not associated with less-aggressive care or greater hospice use, if patients or their surrogates said no end-of-life discussions took place.
Eighty-eight percent of patients in the current study had end-of-life discussions. Twenty-three percent of the discussion were reported by patients or their surrogates in interviews but not documented in records, 17% were documented in medical records but not reported by patients or surrogates, and 48% were both reported and documented.
Among the 794 patients with end-of-life discussions documented in medical records, 39% took place in the last 30 days of life, 63% happened in the inpatient setting, and 40% included an oncologist. Fifty-eight percent of patients entered hospice care, which started in the last 7 days of life for 15% of them, reported Dr. Mack, a pediatric oncologist at the Dana-Farber Cancer Institute and Harvard Medical School, Boston.
The study was published online Nov. 13, 2012 by the Journal of Clinical Oncology (doi:10.1200/JCO.2012.43.6055).
Chemotherapy in the last 2 weeks of life was 59% less likely, acute care in the last 30 days was 57% less likely, and ICU care in the last 30 days was 23% less likely when patients or surrogates reported having end-of-life discussions.
Patients Followed 15 Months After Diagnosis
Patients whose first end-of-life discussion happened while they were hospitalized were more than twice as likely to get any kind of aggressive care at the end of life and three times more likely to get acute care or ICU care in the last 30 days and to have hospice care start within the last week before death.

Having a medical oncologist present at the first end-of-life discussion increased the odds of having chemotherapy in the last 2 weeks of life by 48%, decreased the odds of ICU care in the last 30 days by 56%, increased the likelihood of hospice care by 43%, and doubled the chance of hospice care starting in the last 7 days of life. All of these odds ratios were significant after controlling for other factors.
Data came from a larger cohort of 2,155 patients with stage IV lung or colorectal cancer receiving care in HMOs or Veterans Affairs medical centers in five states. All were followed for 15 months after diagnosis in the Cancer Care Outcomes Research and Surveillance Consortium.
An earlier analysis by the same investigators showed that 87% of the 1,470 patients who died and 41% of the 685 still alive by the end of follow-up had end-of-life care discussions, but oncologists documented end-of-life discussions with only 27% of their patients, suggesting that most discussions were with non-oncologists. Among those who died, documented discussions took place a median of 33 days before death (Ann. Intern. Med. 2012;156:204-10).
"Our previous study on this database found that most physicians do have end-of-life discussions before death, but most occur near the end of life," Dr. Mack said in an interview.
The current study analyzed data for 1,231 of the patients who died but who lived at least 1 month after diagnosis, in order to assess whether the timing of discussions influenced end-of-life care. "Besides the fact that that seems like logical practice, there really wasn’t a clear evidence base that that affects care," she said.
Patients were significantly less likely to say they’d had an end-of-life discussion if they were unmarried, black or non-white Hispanic, or not in an HMO.
Start Talks Closer to Diagnosis
When discussions don’t begin until the last 30 days of life, the end-of-life period usually is already underway, the investigators noted. Physicians should consider moving end-of-life care discussions closer to diagnosis, they suggested, while patients are relatively well and have time to plan for what’s ahead.
"It’s something that any physician can do," but some previous studies report that physicians are reluctant to start end-of-life discussions early because these are emotionally difficult conversations, they worry about taking away hope, and they are concerned about the psychological impact on patients – though there is no clear evidence that it does have psychological consequences for patients, Dr. Mack said.
"It’s a compassionate instinct," she said. "Being in the room with a family when I deliver this kind of news, that emotional impact is right in front of me. I believe there are bigger consequences" from not discussing end-of-life care, such as perpetuating false hopes and asking people to make decisions about what’s ahead without a clear picture of the situation, she added.
The conversation should take place more than once because patient preferences may change over time and patients need time to process the information and their thoughts about it, Dr. Mack said.
Ask Patients What They Hear
Further work is needed on why some documented end-of-life discussions were not reported by patients/surrogates. "Every physician can relate to this, that sometimes we have conversations but they’re not heard or understood by patients," she said. "It reminds me that I need to ask patients what they’re taking away from these conversations and use that to guide me going forward."
That finding echoes two recent large, population-based studies that found many patients with terminal cancer mistakenly think that palliative chemotherapy or radiation will cure their disease.
Some previous studies suggest that patients dying of cancer increasingly are receiving aggressive care at the end of life and that this trend may be modifiable. Cross-sectional studies that assessed one point in time between diagnosis and death have shown that many patients don’t have end-of-life discussions, but these studies probably missed discussions closer to death, Dr. Mack noted.
Other studies have reported an association between having end-of-life discussions and reduced intensity in care. The current study was longitudinal and is one of the first to look at the effects of the timing of these discussions and other factors.
Most patients who realize that they are dying do not want aggressive care, previous studies have shown. Other studies report that less-aggressive end-of-life care is easier on family members and less expensive.
Guidelines from the National Comprehensive Cancer Network, the National Consensus Project for Quality Palliative Care, the American Society of Clinical Oncology, and the American College of Physicians and American Society of Internal Medicine recommend beginning end-of-life discussions early for patients with incurable cancer.
When investigators conducted secondary analyses that excluded patients from Veterans Affairs sites or excluded interviews with patient surrogates, the findings were similar to results of the main analysis.
In the current analysis, 82% of patients had lung cancer, and the rest had colorectal cancer.
Future research on this topic could take many paths, Dr. Mack suggested, including implementing routine early discussions and seeing whether that alters the intensity of final care. Much more could be learned about the quality of discussions between physicians and patients. The current study had no data on discussions led by nurses or social workers or that took place among family members without a medical provider present.
"We’re also interested in looking at a longer trajectory of end-of-life decision making" for patients with incurable cancer – from diagnosis to death, she said.
Dr. Mack and her associates reported having no financial disclosures.
This is an important study that documents the fact that early discussions about end-of-life care for patients with stage IV cancer are associated with decreased intensity of care at the end of life, and that the timing of the initiation of these discussions is very important and should happen earlier than it does much of the time.
This is not the first study to show that this communication is associated with decreased intensity of care (JAMA 2008;300:1665-73). However, this is an important study because it is the first to document that early discussions are important (prior to the last 30 days of life).

|
|
Moving end-of-life discussions closer to diagnosis definitely is realistic and the way this should occur. However, it is not an "either-or" situation. Early discussions don’t mean that later discussions aren’t necessary and important. Early discussions set the frame and make it easier to have later discussions if/when patients get worse.
There is a need for physicians to improve communication to make sure patients or their surrogates understand end-of-life discussions. Our challenge now is to find successful ways to teach these communication skills to physicians and help physicians implement these discussions in clinical practice. It is not useful to tell physicians to have these discussions if they haven’t been trained to do it well, and we don’t create systems that make it practical and feasible.
When the Obama administration tried to implement a policy of paying physicians to conduct advance care planning on an annual basis through Medicare, Sarah Palin and others used the "death panel" scare tactics to defeat this important effort. We need to change the public discussion to be more aware of the importance of early and regular discussions about advance care planning.
We also need research to figure out how best to implement "earlier discussions" in clinical practice and to identify the long-term consequences of such a practice.
Dr. J. Randall Curtis is director of the University of Washington Palliative Care Center of Excellence and head of Pulmonary and Critical Care Medicine at Harborview Medical Center, Seattle. He provided these comments in an interview. Dr. Curtis reported having no financial disclosures.
This is an important study that documents the fact that early discussions about end-of-life care for patients with stage IV cancer are associated with decreased intensity of care at the end of life, and that the timing of the initiation of these discussions is very important and should happen earlier than it does much of the time.
This is not the first study to show that this communication is associated with decreased intensity of care (JAMA 2008;300:1665-73). However, this is an important study because it is the first to document that early discussions are important (prior to the last 30 days of life).
|
|
|
Moving end-of-life discussions closer to diagnosis definitely is realistic and the way this should occur. However, it is not an "either-or" situation. Early discussions don’t mean that later discussions aren’t necessary and important. Early discussions set the frame and make it easier to have later discussions if/when patients get worse.
There is a need for physicians to improve communication to make sure patients or their surrogates understand end-of-life discussions. Our challenge now is to find successful ways to teach these communication skills to physicians and help physicians implement these discussions in clinical practice. It is not useful to tell physicians to have these discussions if they haven’t been trained to do it well, and we don’t create systems that make it practical and feasible.
When the Obama administration tried to implement a policy of paying physicians to conduct advance care planning on an annual basis through Medicare, Sarah Palin and others used the "death panel" scare tactics to defeat this important effort. We need to change the public discussion to be more aware of the importance of early and regular discussions about advance care planning.
We also need research to figure out how best to implement "earlier discussions" in clinical practice and to identify the long-term consequences of such a practice.
Dr. J. Randall Curtis is director of the University of Washington Palliative Care Center of Excellence and head of Pulmonary and Critical Care Medicine at Harborview Medical Center, Seattle. He provided these comments in an interview. Dr. Curtis reported having no financial disclosures.
This is an important study that documents the fact that early discussions about end-of-life care for patients with stage IV cancer are associated with decreased intensity of care at the end of life, and that the timing of the initiation of these discussions is very important and should happen earlier than it does much of the time.
This is not the first study to show that this communication is associated with decreased intensity of care (JAMA 2008;300:1665-73). However, this is an important study because it is the first to document that early discussions are important (prior to the last 30 days of life).
|
|
|
Moving end-of-life discussions closer to diagnosis definitely is realistic and the way this should occur. However, it is not an "either-or" situation. Early discussions don’t mean that later discussions aren’t necessary and important. Early discussions set the frame and make it easier to have later discussions if/when patients get worse.
There is a need for physicians to improve communication to make sure patients or their surrogates understand end-of-life discussions. Our challenge now is to find successful ways to teach these communication skills to physicians and help physicians implement these discussions in clinical practice. It is not useful to tell physicians to have these discussions if they haven’t been trained to do it well, and we don’t create systems that make it practical and feasible.
When the Obama administration tried to implement a policy of paying physicians to conduct advance care planning on an annual basis through Medicare, Sarah Palin and others used the "death panel" scare tactics to defeat this important effort. We need to change the public discussion to be more aware of the importance of early and regular discussions about advance care planning.
We also need research to figure out how best to implement "earlier discussions" in clinical practice and to identify the long-term consequences of such a practice.
Dr. J. Randall Curtis is director of the University of Washington Palliative Care Center of Excellence and head of Pulmonary and Critical Care Medicine at Harborview Medical Center, Seattle. He provided these comments in an interview. Dr. Curtis reported having no financial disclosures.
Patients with stage IV lung or colorectal cancer who had end-of-life discussions with caregivers before the last 30 days of life were significantly less likely to receive aggressive care in their final days and more likely to get hospice care and to enter hospice earlier, a study of 1,231 patients found.
Nearly half received some kind of aggressive care in their last 30 days (47%), including chemotherapy in the last 14 days (16%), ICU care in the last 30 days (6%), and/or acute hospital-based care in the last 30 days of life (40%), Dr. Jennifer W. Mack and her associates reported.
Multiple current guidelines recommend starting end-of-life care planning for patients with incurable cancer early in the course of the disease while patients are relatively stable, not when they are acutely deteriorating.
Many physicians in the study postponed the discussion until the final month of life, and many patients didn’t remember or didn’t recognize the end-of-life discussions. Discussions that were documented in charts were not associated with less-aggressive care or greater hospice use, if patients or their surrogates said no end-of-life discussions took place.
Eighty-eight percent of patients in the current study had end-of-life discussions. Twenty-three percent of the discussion were reported by patients or their surrogates in interviews but not documented in records, 17% were documented in medical records but not reported by patients or surrogates, and 48% were both reported and documented.
Among the 794 patients with end-of-life discussions documented in medical records, 39% took place in the last 30 days of life, 63% happened in the inpatient setting, and 40% included an oncologist. Fifty-eight percent of patients entered hospice care, which started in the last 7 days of life for 15% of them, reported Dr. Mack, a pediatric oncologist at the Dana-Farber Cancer Institute and Harvard Medical School, Boston.
The study was published online Nov. 13, 2012 by the Journal of Clinical Oncology (doi:10.1200/JCO.2012.43.6055).
Chemotherapy in the last 2 weeks of life was 59% less likely, acute care in the last 30 days was 57% less likely, and ICU care in the last 30 days was 23% less likely when patients or surrogates reported having end-of-life discussions.
Patients Followed 15 Months After Diagnosis
Patients whose first end-of-life discussion happened while they were hospitalized were more than twice as likely to get any kind of aggressive care at the end of life and three times more likely to get acute care or ICU care in the last 30 days and to have hospice care start within the last week before death.
Having a medical oncologist present at the first end-of-life discussion increased the odds of having chemotherapy in the last 2 weeks of life by 48%, decreased the odds of ICU care in the last 30 days by 56%, increased the likelihood of hospice care by 43%, and doubled the chance of hospice care starting in the last 7 days of life. All of these odds ratios were significant after controlling for other factors.
Data came from a larger cohort of 2,155 patients with stage IV lung or colorectal cancer receiving care in HMOs or Veterans Affairs medical centers in five states. All were followed for 15 months after diagnosis in the Cancer Care Outcomes Research and Surveillance Consortium.
An earlier analysis by the same investigators showed that 87% of the 1,470 patients who died and 41% of the 685 still alive by the end of follow-up had end-of-life care discussions, but oncologists documented end-of-life discussions with only 27% of their patients, suggesting that most discussions were with non-oncologists. Among those who died, documented discussions took place a median of 33 days before death (Ann. Intern. Med. 2012;156:204-10).
"Our previous study on this database found that most physicians do have end-of-life discussions before death, but most occur near the end of life," Dr. Mack said in an interview.
The current study analyzed data for 1,231 of the patients who died but who lived at least 1 month after diagnosis, in order to assess whether the timing of discussions influenced end-of-life care. "Besides the fact that that seems like logical practice, there really wasn’t a clear evidence base that that affects care," she said.
Patients were significantly less likely to say they’d had an end-of-life discussion if they were unmarried, black or non-white Hispanic, or not in an HMO.
Start Talks Closer to Diagnosis
When discussions don’t begin until the last 30 days of life, the end-of-life period usually is already underway, the investigators noted. Physicians should consider moving end-of-life care discussions closer to diagnosis, they suggested, while patients are relatively well and have time to plan for what’s ahead.
"It’s something that any physician can do," but some previous studies report that physicians are reluctant to start end-of-life discussions early because these are emotionally difficult conversations, they worry about taking away hope, and they are concerned about the psychological impact on patients – though there is no clear evidence that it does have psychological consequences for patients, Dr. Mack said.
"It’s a compassionate instinct," she said. "Being in the room with a family when I deliver this kind of news, that emotional impact is right in front of me. I believe there are bigger consequences" from not discussing end-of-life care, such as perpetuating false hopes and asking people to make decisions about what’s ahead without a clear picture of the situation, she added.
The conversation should take place more than once because patient preferences may change over time and patients need time to process the information and their thoughts about it, Dr. Mack said.
Ask Patients What They Hear
Further work is needed on why some documented end-of-life discussions were not reported by patients/surrogates. "Every physician can relate to this, that sometimes we have conversations but they’re not heard or understood by patients," she said. "It reminds me that I need to ask patients what they’re taking away from these conversations and use that to guide me going forward."
That finding echoes two recent large, population-based studies that found many patients with terminal cancer mistakenly think that palliative chemotherapy or radiation will cure their disease.
Some previous studies suggest that patients dying of cancer increasingly are receiving aggressive care at the end of life and that this trend may be modifiable. Cross-sectional studies that assessed one point in time between diagnosis and death have shown that many patients don’t have end-of-life discussions, but these studies probably missed discussions closer to death, Dr. Mack noted.
Other studies have reported an association between having end-of-life discussions and reduced intensity in care. The current study was longitudinal and is one of the first to look at the effects of the timing of these discussions and other factors.
Most patients who realize that they are dying do not want aggressive care, previous studies have shown. Other studies report that less-aggressive end-of-life care is easier on family members and less expensive.
Guidelines from the National Comprehensive Cancer Network, the National Consensus Project for Quality Palliative Care, the American Society of Clinical Oncology, and the American College of Physicians and American Society of Internal Medicine recommend beginning end-of-life discussions early for patients with incurable cancer.
When investigators conducted secondary analyses that excluded patients from Veterans Affairs sites or excluded interviews with patient surrogates, the findings were similar to results of the main analysis.
In the current analysis, 82% of patients had lung cancer, and the rest had colorectal cancer.
Future research on this topic could take many paths, Dr. Mack suggested, including implementing routine early discussions and seeing whether that alters the intensity of final care. Much more could be learned about the quality of discussions between physicians and patients. The current study had no data on discussions led by nurses or social workers or that took place among family members without a medical provider present.
"We’re also interested in looking at a longer trajectory of end-of-life decision making" for patients with incurable cancer – from diagnosis to death, she said.
Dr. Mack and her associates reported having no financial disclosures.
Patients with stage IV lung or colorectal cancer who had end-of-life discussions with caregivers before the last 30 days of life were significantly less likely to receive aggressive care in their final days and more likely to get hospice care and to enter hospice earlier, a study of 1,231 patients found.
Nearly half received some kind of aggressive care in their last 30 days (47%), including chemotherapy in the last 14 days (16%), ICU care in the last 30 days (6%), and/or acute hospital-based care in the last 30 days of life (40%), Dr. Jennifer W. Mack and her associates reported.
Multiple current guidelines recommend starting end-of-life care planning for patients with incurable cancer early in the course of the disease while patients are relatively stable, not when they are acutely deteriorating.
Many physicians in the study postponed the discussion until the final month of life, and many patients didn’t remember or didn’t recognize the end-of-life discussions. Discussions that were documented in charts were not associated with less-aggressive care or greater hospice use, if patients or their surrogates said no end-of-life discussions took place.
Eighty-eight percent of patients in the current study had end-of-life discussions. Twenty-three percent of the discussion were reported by patients or their surrogates in interviews but not documented in records, 17% were documented in medical records but not reported by patients or surrogates, and 48% were both reported and documented.
Among the 794 patients with end-of-life discussions documented in medical records, 39% took place in the last 30 days of life, 63% happened in the inpatient setting, and 40% included an oncologist. Fifty-eight percent of patients entered hospice care, which started in the last 7 days of life for 15% of them, reported Dr. Mack, a pediatric oncologist at the Dana-Farber Cancer Institute and Harvard Medical School, Boston.
The study was published online Nov. 13, 2012 by the Journal of Clinical Oncology (doi:10.1200/JCO.2012.43.6055).
Chemotherapy in the last 2 weeks of life was 59% less likely, acute care in the last 30 days was 57% less likely, and ICU care in the last 30 days was 23% less likely when patients or surrogates reported having end-of-life discussions.
Patients Followed 15 Months After Diagnosis
Patients whose first end-of-life discussion happened while they were hospitalized were more than twice as likely to get any kind of aggressive care at the end of life and three times more likely to get acute care or ICU care in the last 30 days and to have hospice care start within the last week before death.
Having a medical oncologist present at the first end-of-life discussion increased the odds of having chemotherapy in the last 2 weeks of life by 48%, decreased the odds of ICU care in the last 30 days by 56%, increased the likelihood of hospice care by 43%, and doubled the chance of hospice care starting in the last 7 days of life. All of these odds ratios were significant after controlling for other factors.
Data came from a larger cohort of 2,155 patients with stage IV lung or colorectal cancer receiving care in HMOs or Veterans Affairs medical centers in five states. All were followed for 15 months after diagnosis in the Cancer Care Outcomes Research and Surveillance Consortium.
An earlier analysis by the same investigators showed that 87% of the 1,470 patients who died and 41% of the 685 still alive by the end of follow-up had end-of-life care discussions, but oncologists documented end-of-life discussions with only 27% of their patients, suggesting that most discussions were with non-oncologists. Among those who died, documented discussions took place a median of 33 days before death (Ann. Intern. Med. 2012;156:204-10).
"Our previous study on this database found that most physicians do have end-of-life discussions before death, but most occur near the end of life," Dr. Mack said in an interview.
The current study analyzed data for 1,231 of the patients who died but who lived at least 1 month after diagnosis, in order to assess whether the timing of discussions influenced end-of-life care. "Besides the fact that that seems like logical practice, there really wasn’t a clear evidence base that that affects care," she said.
Patients were significantly less likely to say they’d had an end-of-life discussion if they were unmarried, black or non-white Hispanic, or not in an HMO.
Start Talks Closer to Diagnosis
When discussions don’t begin until the last 30 days of life, the end-of-life period usually is already underway, the investigators noted. Physicians should consider moving end-of-life care discussions closer to diagnosis, they suggested, while patients are relatively well and have time to plan for what’s ahead.
"It’s something that any physician can do," but some previous studies report that physicians are reluctant to start end-of-life discussions early because these are emotionally difficult conversations, they worry about taking away hope, and they are concerned about the psychological impact on patients – though there is no clear evidence that it does have psychological consequences for patients, Dr. Mack said.
"It’s a compassionate instinct," she said. "Being in the room with a family when I deliver this kind of news, that emotional impact is right in front of me. I believe there are bigger consequences" from not discussing end-of-life care, such as perpetuating false hopes and asking people to make decisions about what’s ahead without a clear picture of the situation, she added.
The conversation should take place more than once because patient preferences may change over time and patients need time to process the information and their thoughts about it, Dr. Mack said.
Ask Patients What They Hear
Further work is needed on why some documented end-of-life discussions were not reported by patients/surrogates. "Every physician can relate to this, that sometimes we have conversations but they’re not heard or understood by patients," she said. "It reminds me that I need to ask patients what they’re taking away from these conversations and use that to guide me going forward."
That finding echoes two recent large, population-based studies that found many patients with terminal cancer mistakenly think that palliative chemotherapy or radiation will cure their disease.
Some previous studies suggest that patients dying of cancer increasingly are receiving aggressive care at the end of life and that this trend may be modifiable. Cross-sectional studies that assessed one point in time between diagnosis and death have shown that many patients don’t have end-of-life discussions, but these studies probably missed discussions closer to death, Dr. Mack noted.
Other studies have reported an association between having end-of-life discussions and reduced intensity in care. The current study was longitudinal and is one of the first to look at the effects of the timing of these discussions and other factors.
Most patients who realize that they are dying do not want aggressive care, previous studies have shown. Other studies report that less-aggressive end-of-life care is easier on family members and less expensive.
Guidelines from the National Comprehensive Cancer Network, the National Consensus Project for Quality Palliative Care, the American Society of Clinical Oncology, and the American College of Physicians and American Society of Internal Medicine recommend beginning end-of-life discussions early for patients with incurable cancer.
When investigators conducted secondary analyses that excluded patients from Veterans Affairs sites or excluded interviews with patient surrogates, the findings were similar to results of the main analysis.
In the current analysis, 82% of patients had lung cancer, and the rest had colorectal cancer.
Future research on this topic could take many paths, Dr. Mack suggested, including implementing routine early discussions and seeing whether that alters the intensity of final care. Much more could be learned about the quality of discussions between physicians and patients. The current study had no data on discussions led by nurses or social workers or that took place among family members without a medical provider present.
"We’re also interested in looking at a longer trajectory of end-of-life decision making" for patients with incurable cancer – from diagnosis to death, she said.
Dr. Mack and her associates reported having no financial disclosures.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Major Finding: Chemotherapy in the last 2 weeks of life was 59% less likely, acute care in the last 30 days was 57% less likely, and ICU care in the last 30 days was 23% less likely when patients or their surrogates reported having end-of-life discussions.
Data Source: This was a longitudinal study of 1,231 patients with stage IV lung or colorectal cancer at HMOs or Veterans Affairs sites in five states.
Disclosures: Dr. Mack and her associates reported having no financial disclosures.

Experts: Palliative Care Lowers Costs
It is very common for health care professionals to want to shy away from those difficult conversations with patients when caring for them throughout their cancer treatment.
At the eighth annual Chicago Supportive Oncology Conference, Thomas J. Smith, M.D., Director of Palliative Care for Johns Hopkins Medicine and the Hopkins’ Sidney Kimmel Comprehensive Cancer Center, offered practical insight on the economics of integrating palliative care.
When it comes to discussing patient preferences for end-of-life and treatment decisions, Dr. Smith said: "People do want this information; it won't make [them] depressed; it won’t take away their hope; it won’t make them die sooner. We can give realistic forecasts for survival. It is always culturally appropriate to ask, 'How much do you know about your illness?' "
Is it possible to provide the best in care while "bending the cost curve" by having open and honest discussions with your patients? Absolutely, said Dr. Smith, because "we are asking [them] what is important to them." (See the commentary, "Talking with Patients about Dying,” by Dr. Smith and Dan L. Longo, M.D.; N Engl J Med 2012;367:1651-2.)
It is very common for health care professionals to want to shy away from those difficult conversations with patients when caring for them throughout their cancer treatment.
At the eighth annual Chicago Supportive Oncology Conference, Thomas J. Smith, M.D., Director of Palliative Care for Johns Hopkins Medicine and the Hopkins’ Sidney Kimmel Comprehensive Cancer Center, offered practical insight on the economics of integrating palliative care.
When it comes to discussing patient preferences for end-of-life and treatment decisions, Dr. Smith said: "People do want this information; it won't make [them] depressed; it won’t take away their hope; it won’t make them die sooner. We can give realistic forecasts for survival. It is always culturally appropriate to ask, 'How much do you know about your illness?' "
Is it possible to provide the best in care while "bending the cost curve" by having open and honest discussions with your patients? Absolutely, said Dr. Smith, because "we are asking [them] what is important to them." (See the commentary, "Talking with Patients about Dying,” by Dr. Smith and Dan L. Longo, M.D.; N Engl J Med 2012;367:1651-2.)
It is very common for health care professionals to want to shy away from those difficult conversations with patients when caring for them throughout their cancer treatment.
At the eighth annual Chicago Supportive Oncology Conference, Thomas J. Smith, M.D., Director of Palliative Care for Johns Hopkins Medicine and the Hopkins’ Sidney Kimmel Comprehensive Cancer Center, offered practical insight on the economics of integrating palliative care.
When it comes to discussing patient preferences for end-of-life and treatment decisions, Dr. Smith said: "People do want this information; it won't make [them] depressed; it won’t take away their hope; it won’t make them die sooner. We can give realistic forecasts for survival. It is always culturally appropriate to ask, 'How much do you know about your illness?' "
Is it possible to provide the best in care while "bending the cost curve" by having open and honest discussions with your patients? Absolutely, said Dr. Smith, because "we are asking [them] what is important to them." (See the commentary, "Talking with Patients about Dying,” by Dr. Smith and Dan L. Longo, M.D.; N Engl J Med 2012;367:1651-2.)

Palliative Care Teams in 65% of Hospitals
Portion of hospitals that had palliative-care teams in 2010, according to the latest tally from the Center to Advance Palliative Care at Mount Sinai School of Medicine in New York City (www.capc.org), an increase of 148.5% from 2000. Hospitals of 300-plus beds are more likely to have a palliative-care team than those with fewer than 300 beds (87.9% vs. 56.5%).
Portion of hospitals that had palliative-care teams in 2010, according to the latest tally from the Center to Advance Palliative Care at Mount Sinai School of Medicine in New York City (www.capc.org), an increase of 148.5% from 2000. Hospitals of 300-plus beds are more likely to have a palliative-care team than those with fewer than 300 beds (87.9% vs. 56.5%).
Portion of hospitals that had palliative-care teams in 2010, according to the latest tally from the Center to Advance Palliative Care at Mount Sinai School of Medicine in New York City (www.capc.org), an increase of 148.5% from 2000. Hospitals of 300-plus beds are more likely to have a palliative-care team than those with fewer than 300 beds (87.9% vs. 56.5%).
Medical Coding: Hospice Care vs. Palliative Care
Hospice care” and “palliative care” are not synonymous terms. Hospice care is defined as a comprehensive set of services (see “Hospice Coverage,” below) identified and coordinated by an interdisciplinary group to provide for the physical, psychosocial, spiritual, and emotional needs of a terminally ill patient and/or family members, as delineated in a specific patient plan of care.1 Palliative care is defined as patient- and family-centered care that optimizes quality of life by anticipating, preventing, and treating suffering. Palliative care throughout the continuum of illness involves addressing physical, intellectual, emotional, social, and spiritual needs, and facilitates patient autonomy, access to information, and choice.1
As an approach, hospice care of terminally ill individuals involves palliative care (relief of pain and uncomfortable symptoms), and emphasizes maintaining the patient at home with family and friends as long as possible. Hospice services can be provided in a home, center, skilled-nursing facility, or hospital setting. In contrast, palliative-care services can be provided during hospice care, or coincide with care that is focused on a cure.
Many hospitalists provide both hospice care and palliative-care services to their patients. Different factors affect how to report these services. These programs can be quite costly, as they involve several team members and a substantial amount of time delivering these services. Capturing services appropriately and obtaining reimbursement to help continue program initiatives are significant issues.
Hospice Care
When a patient enrolls in hospice, all rights to Medicare Part B payments are waived during the benefit period involving professional services related to the treatment and management of the terminal illness. Payment is made through the Part A benefit for the associated costs of daily care and the services provided by the hospice-employed physician. An exception occurs for professional services of an independent attending physician who is not an employee of the designated hospice and does not receive compensation from the hospice for those services. The “attending physician” for hospice services must be an individual who is a doctor of medicine or osteopathy, or a nurse practitioner identified by the individual, at the time they elect hospice coverage, as having the most significant role in the determination and delivery of their medical care.2
Patients often receive hospice in the hospital setting, where the hospitalist manages the patient’s daily care. If the hospitalist is designated as the “attending physician” for hospice services, the visits should be reported to Medicare Part B with modifier GV (e.g. 99232-GV).3 This will allow for separate payment to the hospitalist (the independent attending physician), while the hospice agency maintains its daily-care rate. Reporting services absent this modifier will result in denial.
In some cases, the hospitalist is not identified as the “attending physician” for hospice services but occasionally provides care related to the terminal illness. This situation proves most difficult. Although the hospitalist might be the most accessible physician to the staff and is putting the patient’s needs first, reimbursement is unlikely. Regulations stipulate that patients must not see independent physicians other than their “attending physician” for care related to their terminal illness unless the hospice arranges it. When the service is related to the hospice patient’s terminal illness but was furnished by someone other than the designated “attending physician,” this “other physician” must look to the hospice for payment.3
Nonhospice Palliative Care
Members of the palliative-care team often are called to provide management options to assist in reducing pain and suffering. When the palliative-care specialist is asked to provide opinions or advice, the initial service may qualify as a consultation for those payors that still recognize these codes. However, all of the requirements4 must be met in order to report the service as an inpatient consultation (99251-99255):3
- There must be a written request from a qualified healthcare provider who is involved in the patient’s care (e.g. physician, resident, nurse practitioner); this may be documented as a physician order or in the assessment/plan of the requesting provider’s progress note. Standing orders for consultation are not permitted.
- The requesting provider should clearly and accurately identify the reason for consult request to support the medical necessity of the service.
- The palliative-care physician renders and documents the service.
- The palliative-care physician reports his or her findings to the requesting physician via written communication; because the requesting physician and the consultant share a common inpatient medical record, the consultant’s inpatient progress note satisfies the “written report” requirement.
Consider the nature of the request when reporting a consultation. If the request demonstrates the need for opinions or advice from the palliative-care specialist, the service can be reported as a consultation. If the indication cites “medical management” or “palliative management,” payors are less likely to consider the service as a consultation because the physician is not seeking opinions or advice from the consultant to incorporate into his or her own plan of care for the patient and would rather the consultant just take over that portion of patient care. When consultations do not meet the requirements, subsequent hospital care services should be reported (99231-99233).3
The requesting physician can be in the same or a different provider group as the consultant. The consultant must possess expertise in an area that is beyond that of the requesting provider. Because most hospitalists carry a specialty designation of internal medicine (physician specialty code 11), hospitalists providing palliative-care services can distinguish themselves by their own code (physician specialty code 17, hospice and palliative care).5 Payor concerns arise when physicians of the same designated specialty submit a claim for the same patient on the same date. The payor is likely to pay the first claim received and deny the second claim received pending review of documentation. If this occurs, submit a copy of both progress notes for the date in question to distinguish the services provided. The payor may still require that both encounters be reported as one cumulative service under one physician.
Consultations are not an option for Medicare beneficiaries. Hospitalists providing palliative care can report initial hospital care codes (99221-99223) for their first encounter with the patient.3 This is only acceptable when no other hospitalist from the group has reported initial hospital care during the patient stay, unless the palliative-care hospitalist carries the corresponding designation (i.e. enrolled with Medicare as physician specialty code 17). Without this separate designation, the palliative-care hospitalist can only report subsequent hospital care codes (99231-99233) as the patient was seen previously by a hospitalist in the same group.3
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- U.S. Government Printing Office. Electronic Code of Federal Regulations: Title 42: Public Health, Part 418: Hospice Care, §418.3. June 2012. U.S. Government Printing Office website. Available at: http://ecfr.gpoaccess.gov/cgi/t/text/text-idx?c=ecfr&sid=818258235647b14d2961ad30fa3e68e6&rgn=div5&view=text&node=42:3.0.1.1.5&idno=42#42:3.0.1.1.5.1.3.3. Accessed June 23, 2012.
- Centers for Medicare & Medicaid Services. Medicare Claims Processing Manual: Chapter 11: processing hospice claims. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c11.pdf. Accessed June 23, 2012.
- Abraham M, Ahlman J, Anderson C, Boudreau A, Connelly J. Current Procedural Terminology 2012 Professional Edition. Chicago: American Medical Association Press; 2011.
- American Medical Association. Consultation services and transfer of care. American Medical Association website. Available at: http://www.ama-assn.org/resources/doc/cpt/cpt-consultation-services.pdf. Accessed June 23, 2012.
- Centers for Medicare & Medicaid Services. Medicare Claims Processing Manual: Chapter 26: completing and processing form CMS-1500 data set. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c26.pdf. Accessed June 23, 2012. Department of Health and Human Services.
- Hospice Payment System: payment system fact sheet series. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/hospice_pay_sys_fs.pdf. Accessed June 23, 2012.
Hospice care” and “palliative care” are not synonymous terms. Hospice care is defined as a comprehensive set of services (see “Hospice Coverage,” below) identified and coordinated by an interdisciplinary group to provide for the physical, psychosocial, spiritual, and emotional needs of a terminally ill patient and/or family members, as delineated in a specific patient plan of care.1 Palliative care is defined as patient- and family-centered care that optimizes quality of life by anticipating, preventing, and treating suffering. Palliative care throughout the continuum of illness involves addressing physical, intellectual, emotional, social, and spiritual needs, and facilitates patient autonomy, access to information, and choice.1
As an approach, hospice care of terminally ill individuals involves palliative care (relief of pain and uncomfortable symptoms), and emphasizes maintaining the patient at home with family and friends as long as possible. Hospice services can be provided in a home, center, skilled-nursing facility, or hospital setting. In contrast, palliative-care services can be provided during hospice care, or coincide with care that is focused on a cure.
Many hospitalists provide both hospice care and palliative-care services to their patients. Different factors affect how to report these services. These programs can be quite costly, as they involve several team members and a substantial amount of time delivering these services. Capturing services appropriately and obtaining reimbursement to help continue program initiatives are significant issues.
Hospice Care
When a patient enrolls in hospice, all rights to Medicare Part B payments are waived during the benefit period involving professional services related to the treatment and management of the terminal illness. Payment is made through the Part A benefit for the associated costs of daily care and the services provided by the hospice-employed physician. An exception occurs for professional services of an independent attending physician who is not an employee of the designated hospice and does not receive compensation from the hospice for those services. The “attending physician” for hospice services must be an individual who is a doctor of medicine or osteopathy, or a nurse practitioner identified by the individual, at the time they elect hospice coverage, as having the most significant role in the determination and delivery of their medical care.2
Patients often receive hospice in the hospital setting, where the hospitalist manages the patient’s daily care. If the hospitalist is designated as the “attending physician” for hospice services, the visits should be reported to Medicare Part B with modifier GV (e.g. 99232-GV).3 This will allow for separate payment to the hospitalist (the independent attending physician), while the hospice agency maintains its daily-care rate. Reporting services absent this modifier will result in denial.
In some cases, the hospitalist is not identified as the “attending physician” for hospice services but occasionally provides care related to the terminal illness. This situation proves most difficult. Although the hospitalist might be the most accessible physician to the staff and is putting the patient’s needs first, reimbursement is unlikely. Regulations stipulate that patients must not see independent physicians other than their “attending physician” for care related to their terminal illness unless the hospice arranges it. When the service is related to the hospice patient’s terminal illness but was furnished by someone other than the designated “attending physician,” this “other physician” must look to the hospice for payment.3
Nonhospice Palliative Care
Members of the palliative-care team often are called to provide management options to assist in reducing pain and suffering. When the palliative-care specialist is asked to provide opinions or advice, the initial service may qualify as a consultation for those payors that still recognize these codes. However, all of the requirements4 must be met in order to report the service as an inpatient consultation (99251-99255):3
- There must be a written request from a qualified healthcare provider who is involved in the patient’s care (e.g. physician, resident, nurse practitioner); this may be documented as a physician order or in the assessment/plan of the requesting provider’s progress note. Standing orders for consultation are not permitted.
- The requesting provider should clearly and accurately identify the reason for consult request to support the medical necessity of the service.
- The palliative-care physician renders and documents the service.
- The palliative-care physician reports his or her findings to the requesting physician via written communication; because the requesting physician and the consultant share a common inpatient medical record, the consultant’s inpatient progress note satisfies the “written report” requirement.
Consider the nature of the request when reporting a consultation. If the request demonstrates the need for opinions or advice from the palliative-care specialist, the service can be reported as a consultation. If the indication cites “medical management” or “palliative management,” payors are less likely to consider the service as a consultation because the physician is not seeking opinions or advice from the consultant to incorporate into his or her own plan of care for the patient and would rather the consultant just take over that portion of patient care. When consultations do not meet the requirements, subsequent hospital care services should be reported (99231-99233).3
The requesting physician can be in the same or a different provider group as the consultant. The consultant must possess expertise in an area that is beyond that of the requesting provider. Because most hospitalists carry a specialty designation of internal medicine (physician specialty code 11), hospitalists providing palliative-care services can distinguish themselves by their own code (physician specialty code 17, hospice and palliative care).5 Payor concerns arise when physicians of the same designated specialty submit a claim for the same patient on the same date. The payor is likely to pay the first claim received and deny the second claim received pending review of documentation. If this occurs, submit a copy of both progress notes for the date in question to distinguish the services provided. The payor may still require that both encounters be reported as one cumulative service under one physician.
Consultations are not an option for Medicare beneficiaries. Hospitalists providing palliative care can report initial hospital care codes (99221-99223) for their first encounter with the patient.3 This is only acceptable when no other hospitalist from the group has reported initial hospital care during the patient stay, unless the palliative-care hospitalist carries the corresponding designation (i.e. enrolled with Medicare as physician specialty code 17). Without this separate designation, the palliative-care hospitalist can only report subsequent hospital care codes (99231-99233) as the patient was seen previously by a hospitalist in the same group.3
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- U.S. Government Printing Office. Electronic Code of Federal Regulations: Title 42: Public Health, Part 418: Hospice Care, §418.3. June 2012. U.S. Government Printing Office website. Available at: http://ecfr.gpoaccess.gov/cgi/t/text/text-idx?c=ecfr&sid=818258235647b14d2961ad30fa3e68e6&rgn=div5&view=text&node=42:3.0.1.1.5&idno=42#42:3.0.1.1.5.1.3.3. Accessed June 23, 2012.
- Centers for Medicare & Medicaid Services. Medicare Claims Processing Manual: Chapter 11: processing hospice claims. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c11.pdf. Accessed June 23, 2012.
- Abraham M, Ahlman J, Anderson C, Boudreau A, Connelly J. Current Procedural Terminology 2012 Professional Edition. Chicago: American Medical Association Press; 2011.
- American Medical Association. Consultation services and transfer of care. American Medical Association website. Available at: http://www.ama-assn.org/resources/doc/cpt/cpt-consultation-services.pdf. Accessed June 23, 2012.
- Centers for Medicare & Medicaid Services. Medicare Claims Processing Manual: Chapter 26: completing and processing form CMS-1500 data set. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c26.pdf. Accessed June 23, 2012. Department of Health and Human Services.
- Hospice Payment System: payment system fact sheet series. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/hospice_pay_sys_fs.pdf. Accessed June 23, 2012.
Hospice care” and “palliative care” are not synonymous terms. Hospice care is defined as a comprehensive set of services (see “Hospice Coverage,” below) identified and coordinated by an interdisciplinary group to provide for the physical, psychosocial, spiritual, and emotional needs of a terminally ill patient and/or family members, as delineated in a specific patient plan of care.1 Palliative care is defined as patient- and family-centered care that optimizes quality of life by anticipating, preventing, and treating suffering. Palliative care throughout the continuum of illness involves addressing physical, intellectual, emotional, social, and spiritual needs, and facilitates patient autonomy, access to information, and choice.1
As an approach, hospice care of terminally ill individuals involves palliative care (relief of pain and uncomfortable symptoms), and emphasizes maintaining the patient at home with family and friends as long as possible. Hospice services can be provided in a home, center, skilled-nursing facility, or hospital setting. In contrast, palliative-care services can be provided during hospice care, or coincide with care that is focused on a cure.
Many hospitalists provide both hospice care and palliative-care services to their patients. Different factors affect how to report these services. These programs can be quite costly, as they involve several team members and a substantial amount of time delivering these services. Capturing services appropriately and obtaining reimbursement to help continue program initiatives are significant issues.
Hospice Care
When a patient enrolls in hospice, all rights to Medicare Part B payments are waived during the benefit period involving professional services related to the treatment and management of the terminal illness. Payment is made through the Part A benefit for the associated costs of daily care and the services provided by the hospice-employed physician. An exception occurs for professional services of an independent attending physician who is not an employee of the designated hospice and does not receive compensation from the hospice for those services. The “attending physician” for hospice services must be an individual who is a doctor of medicine or osteopathy, or a nurse practitioner identified by the individual, at the time they elect hospice coverage, as having the most significant role in the determination and delivery of their medical care.2
Patients often receive hospice in the hospital setting, where the hospitalist manages the patient’s daily care. If the hospitalist is designated as the “attending physician” for hospice services, the visits should be reported to Medicare Part B with modifier GV (e.g. 99232-GV).3 This will allow for separate payment to the hospitalist (the independent attending physician), while the hospice agency maintains its daily-care rate. Reporting services absent this modifier will result in denial.
In some cases, the hospitalist is not identified as the “attending physician” for hospice services but occasionally provides care related to the terminal illness. This situation proves most difficult. Although the hospitalist might be the most accessible physician to the staff and is putting the patient’s needs first, reimbursement is unlikely. Regulations stipulate that patients must not see independent physicians other than their “attending physician” for care related to their terminal illness unless the hospice arranges it. When the service is related to the hospice patient’s terminal illness but was furnished by someone other than the designated “attending physician,” this “other physician” must look to the hospice for payment.3
Nonhospice Palliative Care
Members of the palliative-care team often are called to provide management options to assist in reducing pain and suffering. When the palliative-care specialist is asked to provide opinions or advice, the initial service may qualify as a consultation for those payors that still recognize these codes. However, all of the requirements4 must be met in order to report the service as an inpatient consultation (99251-99255):3
- There must be a written request from a qualified healthcare provider who is involved in the patient’s care (e.g. physician, resident, nurse practitioner); this may be documented as a physician order or in the assessment/plan of the requesting provider’s progress note. Standing orders for consultation are not permitted.
- The requesting provider should clearly and accurately identify the reason for consult request to support the medical necessity of the service.
- The palliative-care physician renders and documents the service.
- The palliative-care physician reports his or her findings to the requesting physician via written communication; because the requesting physician and the consultant share a common inpatient medical record, the consultant’s inpatient progress note satisfies the “written report” requirement.
Consider the nature of the request when reporting a consultation. If the request demonstrates the need for opinions or advice from the palliative-care specialist, the service can be reported as a consultation. If the indication cites “medical management” or “palliative management,” payors are less likely to consider the service as a consultation because the physician is not seeking opinions or advice from the consultant to incorporate into his or her own plan of care for the patient and would rather the consultant just take over that portion of patient care. When consultations do not meet the requirements, subsequent hospital care services should be reported (99231-99233).3
The requesting physician can be in the same or a different provider group as the consultant. The consultant must possess expertise in an area that is beyond that of the requesting provider. Because most hospitalists carry a specialty designation of internal medicine (physician specialty code 11), hospitalists providing palliative-care services can distinguish themselves by their own code (physician specialty code 17, hospice and palliative care).5 Payor concerns arise when physicians of the same designated specialty submit a claim for the same patient on the same date. The payor is likely to pay the first claim received and deny the second claim received pending review of documentation. If this occurs, submit a copy of both progress notes for the date in question to distinguish the services provided. The payor may still require that both encounters be reported as one cumulative service under one physician.
Consultations are not an option for Medicare beneficiaries. Hospitalists providing palliative care can report initial hospital care codes (99221-99223) for their first encounter with the patient.3 This is only acceptable when no other hospitalist from the group has reported initial hospital care during the patient stay, unless the palliative-care hospitalist carries the corresponding designation (i.e. enrolled with Medicare as physician specialty code 17). Without this separate designation, the palliative-care hospitalist can only report subsequent hospital care codes (99231-99233) as the patient was seen previously by a hospitalist in the same group.3
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- U.S. Government Printing Office. Electronic Code of Federal Regulations: Title 42: Public Health, Part 418: Hospice Care, §418.3. June 2012. U.S. Government Printing Office website. Available at: http://ecfr.gpoaccess.gov/cgi/t/text/text-idx?c=ecfr&sid=818258235647b14d2961ad30fa3e68e6&rgn=div5&view=text&node=42:3.0.1.1.5&idno=42#42:3.0.1.1.5.1.3.3. Accessed June 23, 2012.
- Centers for Medicare & Medicaid Services. Medicare Claims Processing Manual: Chapter 11: processing hospice claims. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c11.pdf. Accessed June 23, 2012.
- Abraham M, Ahlman J, Anderson C, Boudreau A, Connelly J. Current Procedural Terminology 2012 Professional Edition. Chicago: American Medical Association Press; 2011.
- American Medical Association. Consultation services and transfer of care. American Medical Association website. Available at: http://www.ama-assn.org/resources/doc/cpt/cpt-consultation-services.pdf. Accessed June 23, 2012.
- Centers for Medicare & Medicaid Services. Medicare Claims Processing Manual: Chapter 26: completing and processing form CMS-1500 data set. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c26.pdf. Accessed June 23, 2012. Department of Health and Human Services.
- Hospice Payment System: payment system fact sheet series. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/hospice_pay_sys_fs.pdf. Accessed June 23, 2012.