User login
Atezolizumab doubles survival of NSCLC patients with poor performance status
PARIS – Patients with untreated non–small cell lung cancer (NSCLC) who could not withstand the rigors of platinum-based chemotherapy regimens had significantly better overall survival when treated with the immune checkpoint inhibitor atezolizumab (Tecentriq), compared with their counterparts treated with either vinorelbine or gemcitabine in a phase 3 randomized trial.
Among 353 patients with treatment-naive stage 3B to 4 NSCLC who were not candidates for platinum-based chemotherapy because of poor performance status (PS), advanced age, or significant comorbidities, the median overall survival (OS) was 10.3 months for patients treated with atezolizumab vs. 9.2 months for patients assigned to receive the investigator’s choice of single-agent chemotherapy.
This difference translated into a hazard ratio for death with atezolizumab of 0.78 (P = .028), Siow Ming Lee, MD, PhD, of University College London, reported at the ESMO Congress.
The 2-year OS rate with atezolizumab was 24.3%, compared with 12.4% for single-agent chemotherapy.
“When I saw the data, I was amazed. One of four patients survived for 2 years!” he said in an interview.

, those with Eastern Cooperative Oncology Group PS scores of 2 or greater, or who have substantial comorbidities that preclude their ability to receive platinum doublet or single platinum agent chemotherapy, he said.
Invited discussant Natasha Leighl, MD, MMSc, of the Princess Margaret Cancer Center, Toronto, called the study “really extraordinary. This study enrolls patients that historically are excluded or underrepresented in trials, and yet really represent the majority of patients that we diagnose and treat around the world.”
Excluded from clinical trials
“Cancer chemotherapy has changed the treatment landscape for the metastatic NSCLC population, but these treatments are mainly recommended for fit patients,” Dr. Lee said during his presentation of the data in a presidential symposium.
First-line pivotal trials for lung cancer patients comparing either single-agent immunotherapy or an immunotherapy/chemotherapy combination have all been conducted in fit patients, with ECOG PS of 0 or 1, he noted.
“In reality, we still have a large population of unfit NSCLC patients, of at least 40%, many of which we cannot treat with standard platinum chemotherapy. There are many elderly patients with poor performance status, and the elderly with many comorbidities, and they are frequently on many drug medications, which we see frequently in our clinic,” he said.
Study details
To see whether immunotherapy could improve outcomes for unfit patients, investigators designed the IPSOS trial, a phase 3 multicenter open-label study of efficacy, safety, and patient-reported outcomes with atezolizumab compared with single-agent chemotherapy.
Patients from 23 centers in North America, South America, Europe, and Asia who were ineligible for platinum-based chemotherapy because of ECOG performance status of 2 or 3, or who were aged 70 or older with performance status 0 or 1 but with multiple comorbidities or other contraindications to platinum were stratified by histology, programmed death-ligand-1 (PD-L1) expression, and brain metastases, and were then randomly assigned to receive either atezolizumab 1,200 mg intravenously every 3 weeks (302 patients), or to investigator’s choice of either vinorelbine delivered orally or intravenously, according to local practice, or intravenous gemcitabine given intravenously per local practice (151 patients).
As noted before, overall survival, the primary endpoint, was significantly better with atezolizumab, translating into a 22% reduction in risk of death compared with chemotherapy.
The 1-year OS rates were 43.7% with atezolizumab vs. 36.6% with chemotherapy, and the 2-year rates were 24.3% vs. 12.4%, respectively.
A subgroup analysis showed trends toward better benefit for immunotherapy regardless of age, sex, race, performance status, history of tobacco use, tumor histology, stage, presence of liver metastases, number of metastatic sites, or PD-L1 expression levels. The benefit of atezolizumab was also significantly better among patients without brain metastases.
The median duration of response was 14 months with ateziluzmab vs. 7.8 months with chemotherapy. Respective objective response rates were 16.9% vs. 15.5%. Median progression-free survival, a secondary endpoint, was 4.2 months with atezolizumab and 4 months with chemotherapy, a difference that was not statistically significant. Median treatment duration was 3.5 months with atezolizumab, 2.3 months with gemcitabine, and 1.8 months with vinorelbine. Treatment-related adverse events of any grade occurred in 57% of patients on immunotherapy vs. 80.3% of those on chemotherapy. Grade 3 or 4 adverse events related to therapy occurred in 16.3% vs. 33.3%, respectively. About 13% of patients in each arm had an adverse event leading to drug discontinuation. There were three treatment-related deaths among patients on atezolizumab, and four among patients on chemotherapy. Compared with chemotherapy, atezolizumab was associated with stabilizing of health-related quality-of-life domains of functioning, and significant improvement in delaying the time to deterioration of chest pain.
Age is not prognostic
“I think it’s important though to remember that in this study there are very distinct populations of patients. Poor performance status and comorbidities are prognostic, but age is not,” Dr. Leighl said in her discussion.
“In terms of current standards, performance status 3 patients are currently recommended to have best supportive care unless a targeted therapy is available for them, and while PS 2 patients have been excluded from checkpoint inhibitor trials, we treat most of these patients the same way. In this study in particular, patients had to be ineligible for platinum doublet therapy, but of course this definition was subjective,” she said.
She also commented that “if we’re now going to treat everyone with atezolizumab, I think the budget impact of this is going to be huge.”
It will be important to identify more clearly those patients aged 80 and older who might benefit from atezolizumab in this setting by better incorporating biomarkers such as PD-L1 levels to determine who can benefit from therapy and who might be spared the necessity of coming into the hospital or clinic for regular intravenous infusions, she added.
The study was supported by F. Hoffman-La Roche. Dr. Lee disclosed research funding from the company to his institution. Dr. Leighl disclosed institutional grant funding and personal fees from Roche and others.
PARIS – Patients with untreated non–small cell lung cancer (NSCLC) who could not withstand the rigors of platinum-based chemotherapy regimens had significantly better overall survival when treated with the immune checkpoint inhibitor atezolizumab (Tecentriq), compared with their counterparts treated with either vinorelbine or gemcitabine in a phase 3 randomized trial.
Among 353 patients with treatment-naive stage 3B to 4 NSCLC who were not candidates for platinum-based chemotherapy because of poor performance status (PS), advanced age, or significant comorbidities, the median overall survival (OS) was 10.3 months for patients treated with atezolizumab vs. 9.2 months for patients assigned to receive the investigator’s choice of single-agent chemotherapy.
This difference translated into a hazard ratio for death with atezolizumab of 0.78 (P = .028), Siow Ming Lee, MD, PhD, of University College London, reported at the ESMO Congress.
The 2-year OS rate with atezolizumab was 24.3%, compared with 12.4% for single-agent chemotherapy.
“When I saw the data, I was amazed. One of four patients survived for 2 years!” he said in an interview.
, those with Eastern Cooperative Oncology Group PS scores of 2 or greater, or who have substantial comorbidities that preclude their ability to receive platinum doublet or single platinum agent chemotherapy, he said.
Invited discussant Natasha Leighl, MD, MMSc, of the Princess Margaret Cancer Center, Toronto, called the study “really extraordinary. This study enrolls patients that historically are excluded or underrepresented in trials, and yet really represent the majority of patients that we diagnose and treat around the world.”
Excluded from clinical trials
“Cancer chemotherapy has changed the treatment landscape for the metastatic NSCLC population, but these treatments are mainly recommended for fit patients,” Dr. Lee said during his presentation of the data in a presidential symposium.
First-line pivotal trials for lung cancer patients comparing either single-agent immunotherapy or an immunotherapy/chemotherapy combination have all been conducted in fit patients, with ECOG PS of 0 or 1, he noted.
“In reality, we still have a large population of unfit NSCLC patients, of at least 40%, many of which we cannot treat with standard platinum chemotherapy. There are many elderly patients with poor performance status, and the elderly with many comorbidities, and they are frequently on many drug medications, which we see frequently in our clinic,” he said.
Study details
To see whether immunotherapy could improve outcomes for unfit patients, investigators designed the IPSOS trial, a phase 3 multicenter open-label study of efficacy, safety, and patient-reported outcomes with atezolizumab compared with single-agent chemotherapy.
Patients from 23 centers in North America, South America, Europe, and Asia who were ineligible for platinum-based chemotherapy because of ECOG performance status of 2 or 3, or who were aged 70 or older with performance status 0 or 1 but with multiple comorbidities or other contraindications to platinum were stratified by histology, programmed death-ligand-1 (PD-L1) expression, and brain metastases, and were then randomly assigned to receive either atezolizumab 1,200 mg intravenously every 3 weeks (302 patients), or to investigator’s choice of either vinorelbine delivered orally or intravenously, according to local practice, or intravenous gemcitabine given intravenously per local practice (151 patients).
As noted before, overall survival, the primary endpoint, was significantly better with atezolizumab, translating into a 22% reduction in risk of death compared with chemotherapy.
The 1-year OS rates were 43.7% with atezolizumab vs. 36.6% with chemotherapy, and the 2-year rates were 24.3% vs. 12.4%, respectively.
A subgroup analysis showed trends toward better benefit for immunotherapy regardless of age, sex, race, performance status, history of tobacco use, tumor histology, stage, presence of liver metastases, number of metastatic sites, or PD-L1 expression levels. The benefit of atezolizumab was also significantly better among patients without brain metastases.
The median duration of response was 14 months with ateziluzmab vs. 7.8 months with chemotherapy. Respective objective response rates were 16.9% vs. 15.5%. Median progression-free survival, a secondary endpoint, was 4.2 months with atezolizumab and 4 months with chemotherapy, a difference that was not statistically significant. Median treatment duration was 3.5 months with atezolizumab, 2.3 months with gemcitabine, and 1.8 months with vinorelbine. Treatment-related adverse events of any grade occurred in 57% of patients on immunotherapy vs. 80.3% of those on chemotherapy. Grade 3 or 4 adverse events related to therapy occurred in 16.3% vs. 33.3%, respectively. About 13% of patients in each arm had an adverse event leading to drug discontinuation. There were three treatment-related deaths among patients on atezolizumab, and four among patients on chemotherapy. Compared with chemotherapy, atezolizumab was associated with stabilizing of health-related quality-of-life domains of functioning, and significant improvement in delaying the time to deterioration of chest pain.
Age is not prognostic
“I think it’s important though to remember that in this study there are very distinct populations of patients. Poor performance status and comorbidities are prognostic, but age is not,” Dr. Leighl said in her discussion.
“In terms of current standards, performance status 3 patients are currently recommended to have best supportive care unless a targeted therapy is available for them, and while PS 2 patients have been excluded from checkpoint inhibitor trials, we treat most of these patients the same way. In this study in particular, patients had to be ineligible for platinum doublet therapy, but of course this definition was subjective,” she said.
She also commented that “if we’re now going to treat everyone with atezolizumab, I think the budget impact of this is going to be huge.”
It will be important to identify more clearly those patients aged 80 and older who might benefit from atezolizumab in this setting by better incorporating biomarkers such as PD-L1 levels to determine who can benefit from therapy and who might be spared the necessity of coming into the hospital or clinic for regular intravenous infusions, she added.
The study was supported by F. Hoffman-La Roche. Dr. Lee disclosed research funding from the company to his institution. Dr. Leighl disclosed institutional grant funding and personal fees from Roche and others.
PARIS – Patients with untreated non–small cell lung cancer (NSCLC) who could not withstand the rigors of platinum-based chemotherapy regimens had significantly better overall survival when treated with the immune checkpoint inhibitor atezolizumab (Tecentriq), compared with their counterparts treated with either vinorelbine or gemcitabine in a phase 3 randomized trial.
Among 353 patients with treatment-naive stage 3B to 4 NSCLC who were not candidates for platinum-based chemotherapy because of poor performance status (PS), advanced age, or significant comorbidities, the median overall survival (OS) was 10.3 months for patients treated with atezolizumab vs. 9.2 months for patients assigned to receive the investigator’s choice of single-agent chemotherapy.
This difference translated into a hazard ratio for death with atezolizumab of 0.78 (P = .028), Siow Ming Lee, MD, PhD, of University College London, reported at the ESMO Congress.
The 2-year OS rate with atezolizumab was 24.3%, compared with 12.4% for single-agent chemotherapy.
“When I saw the data, I was amazed. One of four patients survived for 2 years!” he said in an interview.
, those with Eastern Cooperative Oncology Group PS scores of 2 or greater, or who have substantial comorbidities that preclude their ability to receive platinum doublet or single platinum agent chemotherapy, he said.
Invited discussant Natasha Leighl, MD, MMSc, of the Princess Margaret Cancer Center, Toronto, called the study “really extraordinary. This study enrolls patients that historically are excluded or underrepresented in trials, and yet really represent the majority of patients that we diagnose and treat around the world.”
Excluded from clinical trials
“Cancer chemotherapy has changed the treatment landscape for the metastatic NSCLC population, but these treatments are mainly recommended for fit patients,” Dr. Lee said during his presentation of the data in a presidential symposium.
First-line pivotal trials for lung cancer patients comparing either single-agent immunotherapy or an immunotherapy/chemotherapy combination have all been conducted in fit patients, with ECOG PS of 0 or 1, he noted.
“In reality, we still have a large population of unfit NSCLC patients, of at least 40%, many of which we cannot treat with standard platinum chemotherapy. There are many elderly patients with poor performance status, and the elderly with many comorbidities, and they are frequently on many drug medications, which we see frequently in our clinic,” he said.
Study details
To see whether immunotherapy could improve outcomes for unfit patients, investigators designed the IPSOS trial, a phase 3 multicenter open-label study of efficacy, safety, and patient-reported outcomes with atezolizumab compared with single-agent chemotherapy.
Patients from 23 centers in North America, South America, Europe, and Asia who were ineligible for platinum-based chemotherapy because of ECOG performance status of 2 or 3, or who were aged 70 or older with performance status 0 or 1 but with multiple comorbidities or other contraindications to platinum were stratified by histology, programmed death-ligand-1 (PD-L1) expression, and brain metastases, and were then randomly assigned to receive either atezolizumab 1,200 mg intravenously every 3 weeks (302 patients), or to investigator’s choice of either vinorelbine delivered orally or intravenously, according to local practice, or intravenous gemcitabine given intravenously per local practice (151 patients).
As noted before, overall survival, the primary endpoint, was significantly better with atezolizumab, translating into a 22% reduction in risk of death compared with chemotherapy.
The 1-year OS rates were 43.7% with atezolizumab vs. 36.6% with chemotherapy, and the 2-year rates were 24.3% vs. 12.4%, respectively.
A subgroup analysis showed trends toward better benefit for immunotherapy regardless of age, sex, race, performance status, history of tobacco use, tumor histology, stage, presence of liver metastases, number of metastatic sites, or PD-L1 expression levels. The benefit of atezolizumab was also significantly better among patients without brain metastases.
The median duration of response was 14 months with ateziluzmab vs. 7.8 months with chemotherapy. Respective objective response rates were 16.9% vs. 15.5%. Median progression-free survival, a secondary endpoint, was 4.2 months with atezolizumab and 4 months with chemotherapy, a difference that was not statistically significant. Median treatment duration was 3.5 months with atezolizumab, 2.3 months with gemcitabine, and 1.8 months with vinorelbine. Treatment-related adverse events of any grade occurred in 57% of patients on immunotherapy vs. 80.3% of those on chemotherapy. Grade 3 or 4 adverse events related to therapy occurred in 16.3% vs. 33.3%, respectively. About 13% of patients in each arm had an adverse event leading to drug discontinuation. There were three treatment-related deaths among patients on atezolizumab, and four among patients on chemotherapy. Compared with chemotherapy, atezolizumab was associated with stabilizing of health-related quality-of-life domains of functioning, and significant improvement in delaying the time to deterioration of chest pain.
Age is not prognostic
“I think it’s important though to remember that in this study there are very distinct populations of patients. Poor performance status and comorbidities are prognostic, but age is not,” Dr. Leighl said in her discussion.
“In terms of current standards, performance status 3 patients are currently recommended to have best supportive care unless a targeted therapy is available for them, and while PS 2 patients have been excluded from checkpoint inhibitor trials, we treat most of these patients the same way. In this study in particular, patients had to be ineligible for platinum doublet therapy, but of course this definition was subjective,” she said.
She also commented that “if we’re now going to treat everyone with atezolizumab, I think the budget impact of this is going to be huge.”
It will be important to identify more clearly those patients aged 80 and older who might benefit from atezolizumab in this setting by better incorporating biomarkers such as PD-L1 levels to determine who can benefit from therapy and who might be spared the necessity of coming into the hospital or clinic for regular intravenous infusions, she added.
The study was supported by F. Hoffman-La Roche. Dr. Lee disclosed research funding from the company to his institution. Dr. Leighl disclosed institutional grant funding and personal fees from Roche and others.
AT ESMO CONGRESS 2022
A farewell to arms? Drug approvals based on single-arm trials can be flawed
PARIS – with results that should only be used, under certain conditions, for accelerated approvals that should then be followed by confirmatory studies.
In fact, many drugs approved over the last decade based solely on data from single-arm trials have been subsequently withdrawn when put through the rigors of a head-to-head randomized controlled trial, according to Bishal Gyawali, MD, PhD, from the department of oncology at Queen’s University, Kingston, Ont.
“Single-arm trials are not meant to provide confirmatory evidence sufficient for approval; However, that ship has sailed, and we have several drugs that are approved on the basis of single-arm trials, but we need to make sure that those approvals are accelerated or conditional approvals, not regular approval,” he said in a presentation included in a special session on drug approvals at the European Society for Medical Oncology Congress.
“We should not allow premature regular approval based on single-arm trials, because once a drug gets conditional approval, access is not an issue. Patients will have access to the drug anyway, but we should ensure that robust evidence follows, and long-term follow-up data are needed to develop confidence in the efficacy outcomes that are seen in single-arm trials,” he said.
In many cases, single-arm trials are large enough or of long enough duration that investigators could have reasonably performed a randomized controlled trial (RCT) in the first place, Dr. Gyawali added.
Why do single-arm trials?
The term “single-arm registration trial” is something of an oxymoron, he said, noting that the purpose of such trials should be whether to take the drug to a phase 3, randomized trial. But as authors of a 2019 study in JAMA Network Open showed, of a sample of phase 3 RCTs, 42% did not have a prior phase 2 trial, and 28% had a negative phase 2 trial. Single-arm trials may be acceptable for conditional drug approvals if all of the following conditions are met:
- A RCT is not possible because the disease is rare or randomization would be unethical.
- The safety of the drug is established and its potential benefits outweigh its risks.
- The drug is associated with a high and durable overall or objective response rate.
- The mechanism of action is supported by a strong scientific rationale, and if the drug may meet an unmet medical need.
Survival endpoints won’t do
Efficacy endpoints typically used in RCTs, such as progression-free survival (PFS) and overall survival (OS) can be misleading because they may be a result of the natural history of the disease and not the drug being tested, whereas ORRs are almost certainly reflective of the action of the drug itself, because spontaneous tumor regression is a rare phenomenon, Dr. Gyawali said.
He cautioned, however, that the ORR of placebo is not zero percent. For example in a 2018 study of sorafenib (Nexavar) versus placebo for advanced or refractory desmoid tumors, the ORR with the active drug was 33%, and the ORR for placebo was 20%.
It’s also open to question, he said, what constitutes an acceptably high ORR and duration of response, pointing to Food and Drug Administration accelerated approval of an indication for nivolumab (Opdivo) for treatment of patients with hepatocellular carcinoma (HCC) that had progressed on sorafenib. In the single-arm trial used as the basis for approval, the ORRs as assessed by an independent central review committee blinded to the results was 14.3%.
“So, nivolumab in hepatocellular cancer was approved on the basis of a response rate lower than that of placebo, albeit in a different tumor. But the point I’m trying to show here is we don’t have a good definition of what is a good response rate,” he said.
In July 2021, Bristol-Myers Squibb voluntarily withdrew the HCC indication for nivolumab, following negative results of the CheckMate 459 trial and a 5-4 vote against continuing the accelerated approval.
On second thought ...
Citing data compiled by Nathan I. Cherny, MD, from Shaare Zedek Medical Center, Jerusalem, Dr. Gyawali noted that 58 of 161 FDA approvals from 2017 to 2021 of drugs for adult solid tumors were based on single-arm trials. Of the 58 drugs, 39 received accelerated approvals, and 19 received regular approvals; of the 39 that received accelerated approvals, 4 were subsequently withdrawn, 8 were converted to regular approvals, and the remainder continued as accelerated approvals.
Interestingly, the median response rate among all the drugs was 40%, and did not differ between the type of approval received, suggesting that response rates are not predictive of whether a drug will receive a conditional or full-fledged go-ahead.
What’s rare and safe?
The definition of a rare disease in the United States is one that affects fewer than 40,000 per year, and in Europe it’s an incidence rate of less than 6 per 100,000 population, Dr. Gyawali noted. But he argued that even non–small cell lung cancer, the most common form of cancer in the world, could be considered rare if it is broken down into subtypes that are treated according to specific mutations that may occur in a relatively small number of patients.
He also noted that a specific drug’s safety, one of the most important criteria for granting approval to a drug based on a single-arm trial, can be difficult to judge without adequate controls for comparison.
Cherry-picking patients
Winette van der Graaf, MD, president of the European Organization for the Research and Treatment of Cancer, who attended the session where Dr. Gyawali’s presentation was played, said in an interview that clinicians should cast a critical eye on how trials are designed and conducted, including patient selection and choice of endpoints.
“One of the most obvious things to be concerned about is that we’re still having patients with good performance status enrolled, mostly PS 0 or 1, so how representative are these clinical trials for the patients we see in front of us on a daily basis?” she said.
“The other question is radiological endpoints, which we focus on with OS and PFS are most important for patients, especially if you consider that if patients may have asymptomatic disease, and we are only treating them with potentially toxic medication, what are we doing for them? Median overall survival when you look at all of these trials is only 4 months, so we really need to take into account how we affect patients in clinical trials,” she added.
Dr. van der Graaf emphasized that clinical trial investigators need to more routinely incorporate quality of life measures and other patient-reported outcomes in clinical trial results to help regulators and clinicians in practice get a better sense of the true clinical benefit of a new drug.
Dr. Gyawali did not disclose a funding source for his presentation. He reported consulting fees from Vivio Health and research grants from the American Society of Clinical Oncology. Dr. van der Graaf reported no conflicts of interest.
PARIS – with results that should only be used, under certain conditions, for accelerated approvals that should then be followed by confirmatory studies.
In fact, many drugs approved over the last decade based solely on data from single-arm trials have been subsequently withdrawn when put through the rigors of a head-to-head randomized controlled trial, according to Bishal Gyawali, MD, PhD, from the department of oncology at Queen’s University, Kingston, Ont.
“Single-arm trials are not meant to provide confirmatory evidence sufficient for approval; However, that ship has sailed, and we have several drugs that are approved on the basis of single-arm trials, but we need to make sure that those approvals are accelerated or conditional approvals, not regular approval,” he said in a presentation included in a special session on drug approvals at the European Society for Medical Oncology Congress.
“We should not allow premature regular approval based on single-arm trials, because once a drug gets conditional approval, access is not an issue. Patients will have access to the drug anyway, but we should ensure that robust evidence follows, and long-term follow-up data are needed to develop confidence in the efficacy outcomes that are seen in single-arm trials,” he said.
In many cases, single-arm trials are large enough or of long enough duration that investigators could have reasonably performed a randomized controlled trial (RCT) in the first place, Dr. Gyawali added.
Why do single-arm trials?
The term “single-arm registration trial” is something of an oxymoron, he said, noting that the purpose of such trials should be whether to take the drug to a phase 3, randomized trial. But as authors of a 2019 study in JAMA Network Open showed, of a sample of phase 3 RCTs, 42% did not have a prior phase 2 trial, and 28% had a negative phase 2 trial. Single-arm trials may be acceptable for conditional drug approvals if all of the following conditions are met:
- A RCT is not possible because the disease is rare or randomization would be unethical.
- The safety of the drug is established and its potential benefits outweigh its risks.
- The drug is associated with a high and durable overall or objective response rate.
- The mechanism of action is supported by a strong scientific rationale, and if the drug may meet an unmet medical need.
Survival endpoints won’t do
Efficacy endpoints typically used in RCTs, such as progression-free survival (PFS) and overall survival (OS) can be misleading because they may be a result of the natural history of the disease and not the drug being tested, whereas ORRs are almost certainly reflective of the action of the drug itself, because spontaneous tumor regression is a rare phenomenon, Dr. Gyawali said.
He cautioned, however, that the ORR of placebo is not zero percent. For example in a 2018 study of sorafenib (Nexavar) versus placebo for advanced or refractory desmoid tumors, the ORR with the active drug was 33%, and the ORR for placebo was 20%.
It’s also open to question, he said, what constitutes an acceptably high ORR and duration of response, pointing to Food and Drug Administration accelerated approval of an indication for nivolumab (Opdivo) for treatment of patients with hepatocellular carcinoma (HCC) that had progressed on sorafenib. In the single-arm trial used as the basis for approval, the ORRs as assessed by an independent central review committee blinded to the results was 14.3%.
“So, nivolumab in hepatocellular cancer was approved on the basis of a response rate lower than that of placebo, albeit in a different tumor. But the point I’m trying to show here is we don’t have a good definition of what is a good response rate,” he said.
In July 2021, Bristol-Myers Squibb voluntarily withdrew the HCC indication for nivolumab, following negative results of the CheckMate 459 trial and a 5-4 vote against continuing the accelerated approval.
On second thought ...
Citing data compiled by Nathan I. Cherny, MD, from Shaare Zedek Medical Center, Jerusalem, Dr. Gyawali noted that 58 of 161 FDA approvals from 2017 to 2021 of drugs for adult solid tumors were based on single-arm trials. Of the 58 drugs, 39 received accelerated approvals, and 19 received regular approvals; of the 39 that received accelerated approvals, 4 were subsequently withdrawn, 8 were converted to regular approvals, and the remainder continued as accelerated approvals.
Interestingly, the median response rate among all the drugs was 40%, and did not differ between the type of approval received, suggesting that response rates are not predictive of whether a drug will receive a conditional or full-fledged go-ahead.
What’s rare and safe?
The definition of a rare disease in the United States is one that affects fewer than 40,000 per year, and in Europe it’s an incidence rate of less than 6 per 100,000 population, Dr. Gyawali noted. But he argued that even non–small cell lung cancer, the most common form of cancer in the world, could be considered rare if it is broken down into subtypes that are treated according to specific mutations that may occur in a relatively small number of patients.
He also noted that a specific drug’s safety, one of the most important criteria for granting approval to a drug based on a single-arm trial, can be difficult to judge without adequate controls for comparison.
Cherry-picking patients
Winette van der Graaf, MD, president of the European Organization for the Research and Treatment of Cancer, who attended the session where Dr. Gyawali’s presentation was played, said in an interview that clinicians should cast a critical eye on how trials are designed and conducted, including patient selection and choice of endpoints.
“One of the most obvious things to be concerned about is that we’re still having patients with good performance status enrolled, mostly PS 0 or 1, so how representative are these clinical trials for the patients we see in front of us on a daily basis?” she said.
“The other question is radiological endpoints, which we focus on with OS and PFS are most important for patients, especially if you consider that if patients may have asymptomatic disease, and we are only treating them with potentially toxic medication, what are we doing for them? Median overall survival when you look at all of these trials is only 4 months, so we really need to take into account how we affect patients in clinical trials,” she added.
Dr. van der Graaf emphasized that clinical trial investigators need to more routinely incorporate quality of life measures and other patient-reported outcomes in clinical trial results to help regulators and clinicians in practice get a better sense of the true clinical benefit of a new drug.
Dr. Gyawali did not disclose a funding source for his presentation. He reported consulting fees from Vivio Health and research grants from the American Society of Clinical Oncology. Dr. van der Graaf reported no conflicts of interest.
PARIS – with results that should only be used, under certain conditions, for accelerated approvals that should then be followed by confirmatory studies.
In fact, many drugs approved over the last decade based solely on data from single-arm trials have been subsequently withdrawn when put through the rigors of a head-to-head randomized controlled trial, according to Bishal Gyawali, MD, PhD, from the department of oncology at Queen’s University, Kingston, Ont.
“Single-arm trials are not meant to provide confirmatory evidence sufficient for approval; However, that ship has sailed, and we have several drugs that are approved on the basis of single-arm trials, but we need to make sure that those approvals are accelerated or conditional approvals, not regular approval,” he said in a presentation included in a special session on drug approvals at the European Society for Medical Oncology Congress.
“We should not allow premature regular approval based on single-arm trials, because once a drug gets conditional approval, access is not an issue. Patients will have access to the drug anyway, but we should ensure that robust evidence follows, and long-term follow-up data are needed to develop confidence in the efficacy outcomes that are seen in single-arm trials,” he said.
In many cases, single-arm trials are large enough or of long enough duration that investigators could have reasonably performed a randomized controlled trial (RCT) in the first place, Dr. Gyawali added.
Why do single-arm trials?
The term “single-arm registration trial” is something of an oxymoron, he said, noting that the purpose of such trials should be whether to take the drug to a phase 3, randomized trial. But as authors of a 2019 study in JAMA Network Open showed, of a sample of phase 3 RCTs, 42% did not have a prior phase 2 trial, and 28% had a negative phase 2 trial. Single-arm trials may be acceptable for conditional drug approvals if all of the following conditions are met:
- A RCT is not possible because the disease is rare or randomization would be unethical.
- The safety of the drug is established and its potential benefits outweigh its risks.
- The drug is associated with a high and durable overall or objective response rate.
- The mechanism of action is supported by a strong scientific rationale, and if the drug may meet an unmet medical need.
Survival endpoints won’t do
Efficacy endpoints typically used in RCTs, such as progression-free survival (PFS) and overall survival (OS) can be misleading because they may be a result of the natural history of the disease and not the drug being tested, whereas ORRs are almost certainly reflective of the action of the drug itself, because spontaneous tumor regression is a rare phenomenon, Dr. Gyawali said.
He cautioned, however, that the ORR of placebo is not zero percent. For example in a 2018 study of sorafenib (Nexavar) versus placebo for advanced or refractory desmoid tumors, the ORR with the active drug was 33%, and the ORR for placebo was 20%.
It’s also open to question, he said, what constitutes an acceptably high ORR and duration of response, pointing to Food and Drug Administration accelerated approval of an indication for nivolumab (Opdivo) for treatment of patients with hepatocellular carcinoma (HCC) that had progressed on sorafenib. In the single-arm trial used as the basis for approval, the ORRs as assessed by an independent central review committee blinded to the results was 14.3%.
“So, nivolumab in hepatocellular cancer was approved on the basis of a response rate lower than that of placebo, albeit in a different tumor. But the point I’m trying to show here is we don’t have a good definition of what is a good response rate,” he said.
In July 2021, Bristol-Myers Squibb voluntarily withdrew the HCC indication for nivolumab, following negative results of the CheckMate 459 trial and a 5-4 vote against continuing the accelerated approval.
On second thought ...
Citing data compiled by Nathan I. Cherny, MD, from Shaare Zedek Medical Center, Jerusalem, Dr. Gyawali noted that 58 of 161 FDA approvals from 2017 to 2021 of drugs for adult solid tumors were based on single-arm trials. Of the 58 drugs, 39 received accelerated approvals, and 19 received regular approvals; of the 39 that received accelerated approvals, 4 were subsequently withdrawn, 8 were converted to regular approvals, and the remainder continued as accelerated approvals.
Interestingly, the median response rate among all the drugs was 40%, and did not differ between the type of approval received, suggesting that response rates are not predictive of whether a drug will receive a conditional or full-fledged go-ahead.
What’s rare and safe?
The definition of a rare disease in the United States is one that affects fewer than 40,000 per year, and in Europe it’s an incidence rate of less than 6 per 100,000 population, Dr. Gyawali noted. But he argued that even non–small cell lung cancer, the most common form of cancer in the world, could be considered rare if it is broken down into subtypes that are treated according to specific mutations that may occur in a relatively small number of patients.
He also noted that a specific drug’s safety, one of the most important criteria for granting approval to a drug based on a single-arm trial, can be difficult to judge without adequate controls for comparison.
Cherry-picking patients
Winette van der Graaf, MD, president of the European Organization for the Research and Treatment of Cancer, who attended the session where Dr. Gyawali’s presentation was played, said in an interview that clinicians should cast a critical eye on how trials are designed and conducted, including patient selection and choice of endpoints.
“One of the most obvious things to be concerned about is that we’re still having patients with good performance status enrolled, mostly PS 0 or 1, so how representative are these clinical trials for the patients we see in front of us on a daily basis?” she said.
“The other question is radiological endpoints, which we focus on with OS and PFS are most important for patients, especially if you consider that if patients may have asymptomatic disease, and we are only treating them with potentially toxic medication, what are we doing for them? Median overall survival when you look at all of these trials is only 4 months, so we really need to take into account how we affect patients in clinical trials,” she added.
Dr. van der Graaf emphasized that clinical trial investigators need to more routinely incorporate quality of life measures and other patient-reported outcomes in clinical trial results to help regulators and clinicians in practice get a better sense of the true clinical benefit of a new drug.
Dr. Gyawali did not disclose a funding source for his presentation. He reported consulting fees from Vivio Health and research grants from the American Society of Clinical Oncology. Dr. van der Graaf reported no conflicts of interest.
AT ESMO CONGRESS 2022
Paresthesias along forearm
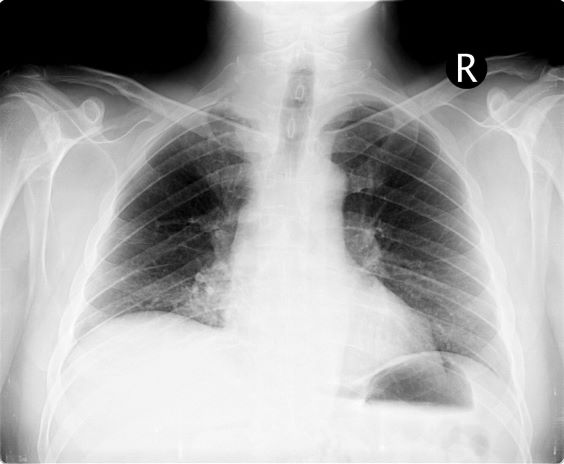
On the basis of this presentation, and the findings from the chest x-ray (as shown), the likely diagnosis is non–small cell lung cancer (NSCLC), Pancoast tumor, also known as superior sulcus tumor. Pancoast tumors are rare, representing about 3%-5% of all lung cancers, and invade the structures in the apex of the chest, including the first thoracic ribs or periosteum, the lower nerve roots of the bronchial plexus, the sympathetic chain and stellate ganglion, or the subclavian vessels. The majority of Pancoast tumors are non–small cell carcinomas.
Because of their pulmonary location, Pancoast tumors are characterized by several distinct symptoms. As seen in this case, patients often present with shoulder pain that worsens over time, especially with invasion of the chest wall and brachial plexus. The pain may radiate to the neck; axilla; anterior chest wall; and medial aspect of the arm, forearm, and wrist. If Pancoast tumors infiltrate the ulnar nerve, patients may present with weakness and muscle atrophy of the intrinsic muscles of the hand. In addition, invasion of the sympathetic chain and of the inferior cervical ganglion can cause Horner syndrome (ptosis, miosis, enophthalmos, and anhidrosis). Lastly, upper-arm edema may develop, signaling invasion and potentially occlusion of the subclavian vein.
During workup, CT-guided core biopsy is the first-line diagnostic test for Pancoast tumors. CT of the chest can confirm the presence of an apical mass and its position in relation to other structures of the thoracic inlet. MRI can further assess suspected brachial plexus, subclavian vessels, spine, and neural foramina invasion, specifying the extent of the disease and of the amount of nerve-root involvement.
For resectable Pancoast tumors, the National Comprehensive Cancer Network recommends chemoradiation, followed by surgical resection and chemotherapy. Preoperative chemoradiation together with surgical resection has shown a 2-year survival between 50% and 70%. Depending on biomarker status (certain EGFR mutations or programmed death ligand 1 levels ≥ 1%), the addition of either atezolizumab or osimertinib is advised. However, the positioning of Pancoast tumors can pose a surgical challenge, and if the lesion remains unresectable after preoperative concurrent chemoradiation, then consolidation immunotherapy with durvalumab is recommended.
Karl J. D'Silva, MD, Clinical Assistant Professor, Department of Medicine, Tufts University School of Medicine, Boston; Medical Director, Department of Oncology and Hematology, Lahey Hospital and Medical Center, Peabody, Massachusetts.
Karl J. D'Silva, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
On the basis of this presentation, and the findings from the chest x-ray (as shown), the likely diagnosis is non–small cell lung cancer (NSCLC), Pancoast tumor, also known as superior sulcus tumor. Pancoast tumors are rare, representing about 3%-5% of all lung cancers, and invade the structures in the apex of the chest, including the first thoracic ribs or periosteum, the lower nerve roots of the bronchial plexus, the sympathetic chain and stellate ganglion, or the subclavian vessels. The majority of Pancoast tumors are non–small cell carcinomas.
Because of their pulmonary location, Pancoast tumors are characterized by several distinct symptoms. As seen in this case, patients often present with shoulder pain that worsens over time, especially with invasion of the chest wall and brachial plexus. The pain may radiate to the neck; axilla; anterior chest wall; and medial aspect of the arm, forearm, and wrist. If Pancoast tumors infiltrate the ulnar nerve, patients may present with weakness and muscle atrophy of the intrinsic muscles of the hand. In addition, invasion of the sympathetic chain and of the inferior cervical ganglion can cause Horner syndrome (ptosis, miosis, enophthalmos, and anhidrosis). Lastly, upper-arm edema may develop, signaling invasion and potentially occlusion of the subclavian vein.
During workup, CT-guided core biopsy is the first-line diagnostic test for Pancoast tumors. CT of the chest can confirm the presence of an apical mass and its position in relation to other structures of the thoracic inlet. MRI can further assess suspected brachial plexus, subclavian vessels, spine, and neural foramina invasion, specifying the extent of the disease and of the amount of nerve-root involvement.
For resectable Pancoast tumors, the National Comprehensive Cancer Network recommends chemoradiation, followed by surgical resection and chemotherapy. Preoperative chemoradiation together with surgical resection has shown a 2-year survival between 50% and 70%. Depending on biomarker status (certain EGFR mutations or programmed death ligand 1 levels ≥ 1%), the addition of either atezolizumab or osimertinib is advised. However, the positioning of Pancoast tumors can pose a surgical challenge, and if the lesion remains unresectable after preoperative concurrent chemoradiation, then consolidation immunotherapy with durvalumab is recommended.
Karl J. D'Silva, MD, Clinical Assistant Professor, Department of Medicine, Tufts University School of Medicine, Boston; Medical Director, Department of Oncology and Hematology, Lahey Hospital and Medical Center, Peabody, Massachusetts.
Karl J. D'Silva, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
On the basis of this presentation, and the findings from the chest x-ray (as shown), the likely diagnosis is non–small cell lung cancer (NSCLC), Pancoast tumor, also known as superior sulcus tumor. Pancoast tumors are rare, representing about 3%-5% of all lung cancers, and invade the structures in the apex of the chest, including the first thoracic ribs or periosteum, the lower nerve roots of the bronchial plexus, the sympathetic chain and stellate ganglion, or the subclavian vessels. The majority of Pancoast tumors are non–small cell carcinomas.
Because of their pulmonary location, Pancoast tumors are characterized by several distinct symptoms. As seen in this case, patients often present with shoulder pain that worsens over time, especially with invasion of the chest wall and brachial plexus. The pain may radiate to the neck; axilla; anterior chest wall; and medial aspect of the arm, forearm, and wrist. If Pancoast tumors infiltrate the ulnar nerve, patients may present with weakness and muscle atrophy of the intrinsic muscles of the hand. In addition, invasion of the sympathetic chain and of the inferior cervical ganglion can cause Horner syndrome (ptosis, miosis, enophthalmos, and anhidrosis). Lastly, upper-arm edema may develop, signaling invasion and potentially occlusion of the subclavian vein.
During workup, CT-guided core biopsy is the first-line diagnostic test for Pancoast tumors. CT of the chest can confirm the presence of an apical mass and its position in relation to other structures of the thoracic inlet. MRI can further assess suspected brachial plexus, subclavian vessels, spine, and neural foramina invasion, specifying the extent of the disease and of the amount of nerve-root involvement.
For resectable Pancoast tumors, the National Comprehensive Cancer Network recommends chemoradiation, followed by surgical resection and chemotherapy. Preoperative chemoradiation together with surgical resection has shown a 2-year survival between 50% and 70%. Depending on biomarker status (certain EGFR mutations or programmed death ligand 1 levels ≥ 1%), the addition of either atezolizumab or osimertinib is advised. However, the positioning of Pancoast tumors can pose a surgical challenge, and if the lesion remains unresectable after preoperative concurrent chemoradiation, then consolidation immunotherapy with durvalumab is recommended.
Karl J. D'Silva, MD, Clinical Assistant Professor, Department of Medicine, Tufts University School of Medicine, Boston; Medical Director, Department of Oncology and Hematology, Lahey Hospital and Medical Center, Peabody, Massachusetts.
Karl J. D'Silva, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
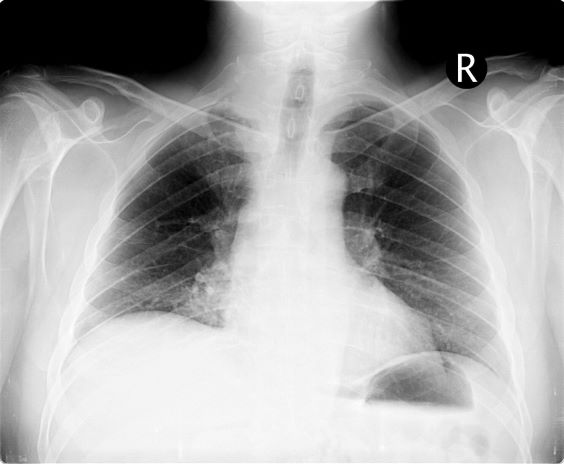
A 54-year-old man presents with shoulder pain and paresthesias along the medial side of the forearm. The patient has a 50–pack-year history of smoking. He reports that the pain began about 6 weeks ago, at which point he scheduled an orthopedic consultation. Physical examination is also notable for facial flushing. Breathing is normal, with no shortness of breath. Chest radiography reveals asymmetry of the apices (right apex is more opaque than the left). Invasion of the ribs is also seen.
Time to cancer diagnoses in U.S. averages 5 months
Time to diagnosis is a crucial factor in cancer. Delays can lead to diagnosis at later stages and prevent optimal therapeutic strategies, both of which have the potential to reduce survival. An estimated 63%-82% of cancers get diagnosed as a result of symptom presentation, and delays in diagnosis can hamper treatment efforts. Diagnosis can be challenging because common symptoms – such as weight loss, weakness, poor appetite, and shortness of breath – are nonspecific.
A new analysis of U.S.-based data shows that the average time to diagnosis is 5.2 months for patients with solid tumors. The authors of the study call for better cancer diagnosis pathways in the U.S.
“Several countries, including the UK, Denmark, Sweden, Canada and Australia, have identified the importance and potential impact of more timely diagnosis by establishing national guidelines, special programs, and treatment pathways. However, in the U.S., there’s relatively little research and effort focused on streamlining the diagnostic pathway. Currently, the U.S. does not have established cancer diagnostic pathways that are used consistently,” Matthew Gitlin, PharmD, said during a presentation at the annual meeting of the European Society for Medical Oncology.
“That is often associated with worse clinical outcomes, increased economic burden, and decreased health related quality of life,” said Dr. Gitlin, founder and managing director of the health economics consulting firm BluePath Solutions, which conducted the analysis.
The study retrospectively examined administrative billing data drawn from the Clinformatics for Managed Markets longitudinal database. The data represent individuals in Medicare Advantage and a large, U.S.-based private insurance plan. Between 2018 and 2019, there were 458,818 cancer diagnoses. The mean age was 70.6 years and 49.6% of the patients were female. Sixty-five percent were White, 11.1% Black, 8.3% Hispanic, and 2.5% Asian. No race data were available for 13.2%. Medicare Advantage was the primary insurance carrier for 74.0%, and 24.0% had a commercial plan.
The mean time to diagnosis across all tumors was 5.2 months (standard deviation, 5.5 months). There was significant variation across different tumor types, as well as within the same tumor type. The median value was 3.9 months (interquartile range, 1.1-7.2 months).
Mean time to diagnosis ranged from 121.6 days for bladder cancer to as high as 229 days for multiple myeloma. Standard deviations were nearly as large or even larger than the mean values. The study showed that 15.8% of patients waited 6 months or longer for a diagnosis. Delays were most common in kidney cancer, colorectal cancer, gallbladder cancer, esophageal cancer, stomach cancer, lymphoma, and multiple myeloma: More than 25% of patients had a time to diagnosis of at least 6 months in these tumors.
“Although there is limited research in the published literature, our findings are consistent with that literature that does exist. Development or modification of policies, guidelines or medical interventions that streamline the diagnostic pathway are needed to optimize patient outcomes and reduce resource burden and cost to the health care system,” Dr. Gitlin said.
Previous literature on this topic has seen wide variation in how time to diagnosis is defined, and most research is conducted in high-income countries, according to Felipe Roitberg, PhD, who served as a discussant during the session. “Most of the countries and patients in need are localized in low- and middle-income countries, so that is a call to action (for more research),” said Dr. Roitberg, a clinical oncologist at Hospital Sírio Libanês in São Paulo, Brazil.
The study did not look at the associations between race and time to diagnosis. “This is a source of analysis could further be explored,” said Dr. Roitberg.
He noted that the ABC-DO prospective cohort study in sub-Saharan Africa found large variations in breast cancer survival by country, and its authors predicted that downstaging and improvements in treatment could prevent up to one-third of projected breast cancer deaths over the next decade. “So these are the drivers of populational gain in terms of overall survival – not more drugs, not more services available, but coordination of services and making sure the patient has a right pathway (to diagnosis and treatment),” Dr. Roitberg said.
Dr. Gitlin has received consulting fees from GRAIL LLC, which is a subsidiary of Illumina. Dr. Roitberg has received honoraria from Boehringer Ingelheim, Sanofi, Roche, MSD Oncology, AstraZeneca, Nestle Health Science, Dr Reddy’s, and Oncologia Brazil. He has consulted for MSD Oncology. He has received research funding from Roche, Boehringer Ingelheim, MSD, Bayer, AstraZeneca, and Takeda.
Time to diagnosis is a crucial factor in cancer. Delays can lead to diagnosis at later stages and prevent optimal therapeutic strategies, both of which have the potential to reduce survival. An estimated 63%-82% of cancers get diagnosed as a result of symptom presentation, and delays in diagnosis can hamper treatment efforts. Diagnosis can be challenging because common symptoms – such as weight loss, weakness, poor appetite, and shortness of breath – are nonspecific.
A new analysis of U.S.-based data shows that the average time to diagnosis is 5.2 months for patients with solid tumors. The authors of the study call for better cancer diagnosis pathways in the U.S.
“Several countries, including the UK, Denmark, Sweden, Canada and Australia, have identified the importance and potential impact of more timely diagnosis by establishing national guidelines, special programs, and treatment pathways. However, in the U.S., there’s relatively little research and effort focused on streamlining the diagnostic pathway. Currently, the U.S. does not have established cancer diagnostic pathways that are used consistently,” Matthew Gitlin, PharmD, said during a presentation at the annual meeting of the European Society for Medical Oncology.
“That is often associated with worse clinical outcomes, increased economic burden, and decreased health related quality of life,” said Dr. Gitlin, founder and managing director of the health economics consulting firm BluePath Solutions, which conducted the analysis.
The study retrospectively examined administrative billing data drawn from the Clinformatics for Managed Markets longitudinal database. The data represent individuals in Medicare Advantage and a large, U.S.-based private insurance plan. Between 2018 and 2019, there were 458,818 cancer diagnoses. The mean age was 70.6 years and 49.6% of the patients were female. Sixty-five percent were White, 11.1% Black, 8.3% Hispanic, and 2.5% Asian. No race data were available for 13.2%. Medicare Advantage was the primary insurance carrier for 74.0%, and 24.0% had a commercial plan.
The mean time to diagnosis across all tumors was 5.2 months (standard deviation, 5.5 months). There was significant variation across different tumor types, as well as within the same tumor type. The median value was 3.9 months (interquartile range, 1.1-7.2 months).
Mean time to diagnosis ranged from 121.6 days for bladder cancer to as high as 229 days for multiple myeloma. Standard deviations were nearly as large or even larger than the mean values. The study showed that 15.8% of patients waited 6 months or longer for a diagnosis. Delays were most common in kidney cancer, colorectal cancer, gallbladder cancer, esophageal cancer, stomach cancer, lymphoma, and multiple myeloma: More than 25% of patients had a time to diagnosis of at least 6 months in these tumors.
“Although there is limited research in the published literature, our findings are consistent with that literature that does exist. Development or modification of policies, guidelines or medical interventions that streamline the diagnostic pathway are needed to optimize patient outcomes and reduce resource burden and cost to the health care system,” Dr. Gitlin said.
Previous literature on this topic has seen wide variation in how time to diagnosis is defined, and most research is conducted in high-income countries, according to Felipe Roitberg, PhD, who served as a discussant during the session. “Most of the countries and patients in need are localized in low- and middle-income countries, so that is a call to action (for more research),” said Dr. Roitberg, a clinical oncologist at Hospital Sírio Libanês in São Paulo, Brazil.
The study did not look at the associations between race and time to diagnosis. “This is a source of analysis could further be explored,” said Dr. Roitberg.
He noted that the ABC-DO prospective cohort study in sub-Saharan Africa found large variations in breast cancer survival by country, and its authors predicted that downstaging and improvements in treatment could prevent up to one-third of projected breast cancer deaths over the next decade. “So these are the drivers of populational gain in terms of overall survival – not more drugs, not more services available, but coordination of services and making sure the patient has a right pathway (to diagnosis and treatment),” Dr. Roitberg said.
Dr. Gitlin has received consulting fees from GRAIL LLC, which is a subsidiary of Illumina. Dr. Roitberg has received honoraria from Boehringer Ingelheim, Sanofi, Roche, MSD Oncology, AstraZeneca, Nestle Health Science, Dr Reddy’s, and Oncologia Brazil. He has consulted for MSD Oncology. He has received research funding from Roche, Boehringer Ingelheim, MSD, Bayer, AstraZeneca, and Takeda.
Time to diagnosis is a crucial factor in cancer. Delays can lead to diagnosis at later stages and prevent optimal therapeutic strategies, both of which have the potential to reduce survival. An estimated 63%-82% of cancers get diagnosed as a result of symptom presentation, and delays in diagnosis can hamper treatment efforts. Diagnosis can be challenging because common symptoms – such as weight loss, weakness, poor appetite, and shortness of breath – are nonspecific.
A new analysis of U.S.-based data shows that the average time to diagnosis is 5.2 months for patients with solid tumors. The authors of the study call for better cancer diagnosis pathways in the U.S.
“Several countries, including the UK, Denmark, Sweden, Canada and Australia, have identified the importance and potential impact of more timely diagnosis by establishing national guidelines, special programs, and treatment pathways. However, in the U.S., there’s relatively little research and effort focused on streamlining the diagnostic pathway. Currently, the U.S. does not have established cancer diagnostic pathways that are used consistently,” Matthew Gitlin, PharmD, said during a presentation at the annual meeting of the European Society for Medical Oncology.
“That is often associated with worse clinical outcomes, increased economic burden, and decreased health related quality of life,” said Dr. Gitlin, founder and managing director of the health economics consulting firm BluePath Solutions, which conducted the analysis.
The study retrospectively examined administrative billing data drawn from the Clinformatics for Managed Markets longitudinal database. The data represent individuals in Medicare Advantage and a large, U.S.-based private insurance plan. Between 2018 and 2019, there were 458,818 cancer diagnoses. The mean age was 70.6 years and 49.6% of the patients were female. Sixty-five percent were White, 11.1% Black, 8.3% Hispanic, and 2.5% Asian. No race data were available for 13.2%. Medicare Advantage was the primary insurance carrier for 74.0%, and 24.0% had a commercial plan.
The mean time to diagnosis across all tumors was 5.2 months (standard deviation, 5.5 months). There was significant variation across different tumor types, as well as within the same tumor type. The median value was 3.9 months (interquartile range, 1.1-7.2 months).
Mean time to diagnosis ranged from 121.6 days for bladder cancer to as high as 229 days for multiple myeloma. Standard deviations were nearly as large or even larger than the mean values. The study showed that 15.8% of patients waited 6 months or longer for a diagnosis. Delays were most common in kidney cancer, colorectal cancer, gallbladder cancer, esophageal cancer, stomach cancer, lymphoma, and multiple myeloma: More than 25% of patients had a time to diagnosis of at least 6 months in these tumors.
“Although there is limited research in the published literature, our findings are consistent with that literature that does exist. Development or modification of policies, guidelines or medical interventions that streamline the diagnostic pathway are needed to optimize patient outcomes and reduce resource burden and cost to the health care system,” Dr. Gitlin said.
Previous literature on this topic has seen wide variation in how time to diagnosis is defined, and most research is conducted in high-income countries, according to Felipe Roitberg, PhD, who served as a discussant during the session. “Most of the countries and patients in need are localized in low- and middle-income countries, so that is a call to action (for more research),” said Dr. Roitberg, a clinical oncologist at Hospital Sírio Libanês in São Paulo, Brazil.
The study did not look at the associations between race and time to diagnosis. “This is a source of analysis could further be explored,” said Dr. Roitberg.
He noted that the ABC-DO prospective cohort study in sub-Saharan Africa found large variations in breast cancer survival by country, and its authors predicted that downstaging and improvements in treatment could prevent up to one-third of projected breast cancer deaths over the next decade. “So these are the drivers of populational gain in terms of overall survival – not more drugs, not more services available, but coordination of services and making sure the patient has a right pathway (to diagnosis and treatment),” Dr. Roitberg said.
Dr. Gitlin has received consulting fees from GRAIL LLC, which is a subsidiary of Illumina. Dr. Roitberg has received honoraria from Boehringer Ingelheim, Sanofi, Roche, MSD Oncology, AstraZeneca, Nestle Health Science, Dr Reddy’s, and Oncologia Brazil. He has consulted for MSD Oncology. He has received research funding from Roche, Boehringer Ingelheim, MSD, Bayer, AstraZeneca, and Takeda.
FROM ESMO CONGRESS 2022
Opioids after lung cancer surgery may up all-cause mortality risk
Patients who undergo lung cancer surgery and who receive long-term opioids for pain relief have an elevated risk of all-cause mortality at 2 years, a new study suggests. That risk was 40% higher than among patients who did not receive opioids.
“This is the first study to identify the association of new long-term opioid use with poorer long-term survival outcomes after lung cancer surgery using real-world data based on a national registration database,” said the authors, led by In-Ae Song, MD, Seoul National University Bundang Hospital, Seongnam, South Korea.
“New long-term opioid use may be associated with poor long-term survival outcomes, especially in potent opioid users,” they concluded.
Long-term opioid use might promote protumor activity secondary to immunosuppression along with migration of tumor cells and angiogenesis, the authors suggested.
The study was published online in Regional Anesthesia and Pain.
The finding comes from a study that used the South Korean National Health Insurance database as a nationwide registration data source. “All patients undergoing lung cancer surgery between 2011 and 2018 were included,” the authors noted.
In total, 54,509 patients were included in the final analysis. Six months after undergoing the procedure, 3,325 patients (6.1%) had been prescribed opioids continuously and regularly. These patients constituted the new long-term opioid user group.
This finding fits in with those from past studies that have suggested that new long-term postoperative pain is reported in 4%-12% of patients who undergo lung cancer surgeries, the authors commented.
The new study found that all-cause mortality at 2 years was significantly higher in the new long-term opioid user group than it was in the non–opioid user group (17.3% vs. 9.3%; P < .001).
Moreover, the new long-term opioid user group were at 43% higher risk of 2-year lung cancer mortality and 29% higher risk of 2-year non–lung cancer mortality.
The investigators divided the patients who had received long-term opioids into two subgroups – those who received more potent opioids (1.6%), and those who received less potent opioids (4.5%).
There was a big difference in the results for all-cause mortality.
Compared with nonopioid users, long-term use of less potent opioids was associated with a 2-year mortality risk of only 22% (P < .001), whereas the patients who used potent opioids were at a 92% increased risk of all-cause mortality.
A number of risk factors were associated with an increased rate of new long-term opioid use. These included older age, being male, length of stay in hospital, and comorbidities.
In addition, patients who were more likely to receive long-term opioids included those who had received neoadjuvant and adjuvant chemotherapy and those who had experienced preoperative anxiety disorder or insomnia disorder.
In contrast, patients who underwent video-assisted thoracoscopic surgery were less likely to receive long-term opioids, the authors noted.
The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Patients who undergo lung cancer surgery and who receive long-term opioids for pain relief have an elevated risk of all-cause mortality at 2 years, a new study suggests. That risk was 40% higher than among patients who did not receive opioids.
“This is the first study to identify the association of new long-term opioid use with poorer long-term survival outcomes after lung cancer surgery using real-world data based on a national registration database,” said the authors, led by In-Ae Song, MD, Seoul National University Bundang Hospital, Seongnam, South Korea.
“New long-term opioid use may be associated with poor long-term survival outcomes, especially in potent opioid users,” they concluded.
Long-term opioid use might promote protumor activity secondary to immunosuppression along with migration of tumor cells and angiogenesis, the authors suggested.
The study was published online in Regional Anesthesia and Pain.
The finding comes from a study that used the South Korean National Health Insurance database as a nationwide registration data source. “All patients undergoing lung cancer surgery between 2011 and 2018 were included,” the authors noted.
In total, 54,509 patients were included in the final analysis. Six months after undergoing the procedure, 3,325 patients (6.1%) had been prescribed opioids continuously and regularly. These patients constituted the new long-term opioid user group.
This finding fits in with those from past studies that have suggested that new long-term postoperative pain is reported in 4%-12% of patients who undergo lung cancer surgeries, the authors commented.
The new study found that all-cause mortality at 2 years was significantly higher in the new long-term opioid user group than it was in the non–opioid user group (17.3% vs. 9.3%; P < .001).
Moreover, the new long-term opioid user group were at 43% higher risk of 2-year lung cancer mortality and 29% higher risk of 2-year non–lung cancer mortality.
The investigators divided the patients who had received long-term opioids into two subgroups – those who received more potent opioids (1.6%), and those who received less potent opioids (4.5%).
There was a big difference in the results for all-cause mortality.
Compared with nonopioid users, long-term use of less potent opioids was associated with a 2-year mortality risk of only 22% (P < .001), whereas the patients who used potent opioids were at a 92% increased risk of all-cause mortality.
A number of risk factors were associated with an increased rate of new long-term opioid use. These included older age, being male, length of stay in hospital, and comorbidities.
In addition, patients who were more likely to receive long-term opioids included those who had received neoadjuvant and adjuvant chemotherapy and those who had experienced preoperative anxiety disorder or insomnia disorder.
In contrast, patients who underwent video-assisted thoracoscopic surgery were less likely to receive long-term opioids, the authors noted.
The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Patients who undergo lung cancer surgery and who receive long-term opioids for pain relief have an elevated risk of all-cause mortality at 2 years, a new study suggests. That risk was 40% higher than among patients who did not receive opioids.
“This is the first study to identify the association of new long-term opioid use with poorer long-term survival outcomes after lung cancer surgery using real-world data based on a national registration database,” said the authors, led by In-Ae Song, MD, Seoul National University Bundang Hospital, Seongnam, South Korea.
“New long-term opioid use may be associated with poor long-term survival outcomes, especially in potent opioid users,” they concluded.
Long-term opioid use might promote protumor activity secondary to immunosuppression along with migration of tumor cells and angiogenesis, the authors suggested.
The study was published online in Regional Anesthesia and Pain.
The finding comes from a study that used the South Korean National Health Insurance database as a nationwide registration data source. “All patients undergoing lung cancer surgery between 2011 and 2018 were included,” the authors noted.
In total, 54,509 patients were included in the final analysis. Six months after undergoing the procedure, 3,325 patients (6.1%) had been prescribed opioids continuously and regularly. These patients constituted the new long-term opioid user group.
This finding fits in with those from past studies that have suggested that new long-term postoperative pain is reported in 4%-12% of patients who undergo lung cancer surgeries, the authors commented.
The new study found that all-cause mortality at 2 years was significantly higher in the new long-term opioid user group than it was in the non–opioid user group (17.3% vs. 9.3%; P < .001).
Moreover, the new long-term opioid user group were at 43% higher risk of 2-year lung cancer mortality and 29% higher risk of 2-year non–lung cancer mortality.
The investigators divided the patients who had received long-term opioids into two subgroups – those who received more potent opioids (1.6%), and those who received less potent opioids (4.5%).
There was a big difference in the results for all-cause mortality.
Compared with nonopioid users, long-term use of less potent opioids was associated with a 2-year mortality risk of only 22% (P < .001), whereas the patients who used potent opioids were at a 92% increased risk of all-cause mortality.
A number of risk factors were associated with an increased rate of new long-term opioid use. These included older age, being male, length of stay in hospital, and comorbidities.
In addition, patients who were more likely to receive long-term opioids included those who had received neoadjuvant and adjuvant chemotherapy and those who had experienced preoperative anxiety disorder or insomnia disorder.
In contrast, patients who underwent video-assisted thoracoscopic surgery were less likely to receive long-term opioids, the authors noted.
The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM REGIONAL ANESTHESIA AND PAIN
Could nivolumab prevent oral cancer in high-risk patients?
(PL), a high-risk precancerous disease, into oral cancer, suggest the results from a phase 2 study.
“We think that immunotherapy as a preventative strategy, either as first-line or even secondary prevention, should be further explored,” said lead researcher Glenn J. Hanna, MD, director, Center for Salivary and Rare Head and Neck Cancers, Dana-Farber Cancer Institute, Boston.
The research was presented at the European Society for Medical Oncology Annual Congress in Paris.
Oral leukoplakia refers to a white plaque of “questionable cancer risk” that affects about 4% of the global population, Dr. Hanna explained. However, about 5% of leukoplakia cases develop into oral proliferative leukoplakia, an aggressive form of the disease characterized by multifocal lesions. It has a high risk of transformation to oral squamous cell carcinoma (OSCC), at approaching 10% per year, and the 5-year cancer-free survival rate is estimated to be 47%.
While there are no effective therapies to prevent progression to oral cancer, the condition does have a “rich immune microenvironment,” potentially making it amenable to programmed death (PD)-1 blockade, Dr. Hanna said.
His team conducted a single-arm, phase 2 trial involving 33 patients with proliferative leukoplakia with greater than or equal to 2 multifocal lesions, or contiguous lesions of greater than or equal to 3 cm, or a single lesion greater than or equal to 4 cm with any degree of epithelial dysplasia. The median age was 63.2 years, and 55% were women. Just over half (52%) were never smokers.
The main disease subsite was the oral tongue in 39% of participants, followed by the buccal gingiva in 30%, and 24% of patients had a prior diagnosis of OSCC.
Following a pretreatment biopsy at one to three sites, the patients received four doses of nivolumab every 28 days, followed by rebiopsy. At each visit, the patients had intraoral photographs taken of the lesions and measurements taken.
The median time from study registration to the first dose of nivolumab was 9 days. The majority (88%) of patients completed all four doses of nivolumab.
The median time from the first dose of nivolumab to the posttreatment biopsy was 115 days and ranged from 29 to 171 days.
The overall response rate, defined as a greater than or equal to 40% decrease in a composite score combining the size and degree of dysplasia between the pre- and posttreatment assessments, was observed in 36.4% of patients.
After a median follow-up of 14.7 months, the median cancer-free survival was not reached, with cancer events recorded in 21.2% of patients. The median time from the last dose of nivolumab to the first OSCC event was 3.7 months.
Cancer-free survival at 1 year was calculated to be 77.7%, which was unchanged at 2 years. At the final follow-up, all patients were still alive.
Additional analysis of the biopsies revealed that the lesions had programmed death ligand 1 (PD-L1) combined positive scores that ranged from 0 to 80, with 66.7% of patients having a score of greater than or equal to 1. A cutoff score of greater than or equal to 20 did not reveal any significant differences in cancer-free survival rates.
Turning to safety, Dr. Hanna said that nivolumab was associated with “acceptable toxicity” in this “non-cancer population,” with 21.2% of patients experiencing a grade 3-4 adverse event.
The most common adverse events of any grade were fatigue (55%), diarrhea (27%), elevated alanine transaminase levels (18%), elevated aspartate transaminase levels (18%), and other skin disorders (18%).
With a relatively low rate of adverse events and a “clinical benefit” in up to a third of patients, Dr. Hanna said that this was the “first study to our knowledge to demonstrate the potential efficacy of anti–PD-L1 blockade among patients with a high-risk oral precancerous disease.”
Discussing this study at the meeting, Amanda Psyrri, MD, PhD, professor of medical oncology, Attikon University Hospital, Athens, who was not involved in the research, said these data were “very interesting,” but she expressed some reservations over the way the study was conducted.
She said that the composite score to measure response rates was “defined arbitrarily,” its prognostic value “has not been demonstrated,” and also pointed out that mixed responses by lesions within the same patient led to changes in scores.
In addition, the time interval between the end of treatment and lesion rebiopsy was “highly variable,” and the follow-up period was short.
Consequently, Dr. Psyrri believes the importance of the findings is “unclear,” especially as several patients who responded to nivolumab went on to develop cancer anyway, a finding that needs further investigation.
The study was funded by Bristol Myers Squibb.
Dr. Hanna declared relationships with BMS, Bicara, Exicure, Gateway for Cancer Research, GSK, Kite, NantKwest, Regeneron, Sanofi Genzyme, Maverick, and Merck.
A version of this article first appeared on Medscape.com.
(PL), a high-risk precancerous disease, into oral cancer, suggest the results from a phase 2 study.
“We think that immunotherapy as a preventative strategy, either as first-line or even secondary prevention, should be further explored,” said lead researcher Glenn J. Hanna, MD, director, Center for Salivary and Rare Head and Neck Cancers, Dana-Farber Cancer Institute, Boston.
The research was presented at the European Society for Medical Oncology Annual Congress in Paris.
Oral leukoplakia refers to a white plaque of “questionable cancer risk” that affects about 4% of the global population, Dr. Hanna explained. However, about 5% of leukoplakia cases develop into oral proliferative leukoplakia, an aggressive form of the disease characterized by multifocal lesions. It has a high risk of transformation to oral squamous cell carcinoma (OSCC), at approaching 10% per year, and the 5-year cancer-free survival rate is estimated to be 47%.
While there are no effective therapies to prevent progression to oral cancer, the condition does have a “rich immune microenvironment,” potentially making it amenable to programmed death (PD)-1 blockade, Dr. Hanna said.
His team conducted a single-arm, phase 2 trial involving 33 patients with proliferative leukoplakia with greater than or equal to 2 multifocal lesions, or contiguous lesions of greater than or equal to 3 cm, or a single lesion greater than or equal to 4 cm with any degree of epithelial dysplasia. The median age was 63.2 years, and 55% were women. Just over half (52%) were never smokers.
The main disease subsite was the oral tongue in 39% of participants, followed by the buccal gingiva in 30%, and 24% of patients had a prior diagnosis of OSCC.
Following a pretreatment biopsy at one to three sites, the patients received four doses of nivolumab every 28 days, followed by rebiopsy. At each visit, the patients had intraoral photographs taken of the lesions and measurements taken.
The median time from study registration to the first dose of nivolumab was 9 days. The majority (88%) of patients completed all four doses of nivolumab.
The median time from the first dose of nivolumab to the posttreatment biopsy was 115 days and ranged from 29 to 171 days.
The overall response rate, defined as a greater than or equal to 40% decrease in a composite score combining the size and degree of dysplasia between the pre- and posttreatment assessments, was observed in 36.4% of patients.
After a median follow-up of 14.7 months, the median cancer-free survival was not reached, with cancer events recorded in 21.2% of patients. The median time from the last dose of nivolumab to the first OSCC event was 3.7 months.
Cancer-free survival at 1 year was calculated to be 77.7%, which was unchanged at 2 years. At the final follow-up, all patients were still alive.
Additional analysis of the biopsies revealed that the lesions had programmed death ligand 1 (PD-L1) combined positive scores that ranged from 0 to 80, with 66.7% of patients having a score of greater than or equal to 1. A cutoff score of greater than or equal to 20 did not reveal any significant differences in cancer-free survival rates.
Turning to safety, Dr. Hanna said that nivolumab was associated with “acceptable toxicity” in this “non-cancer population,” with 21.2% of patients experiencing a grade 3-4 adverse event.
The most common adverse events of any grade were fatigue (55%), diarrhea (27%), elevated alanine transaminase levels (18%), elevated aspartate transaminase levels (18%), and other skin disorders (18%).
With a relatively low rate of adverse events and a “clinical benefit” in up to a third of patients, Dr. Hanna said that this was the “first study to our knowledge to demonstrate the potential efficacy of anti–PD-L1 blockade among patients with a high-risk oral precancerous disease.”
Discussing this study at the meeting, Amanda Psyrri, MD, PhD, professor of medical oncology, Attikon University Hospital, Athens, who was not involved in the research, said these data were “very interesting,” but she expressed some reservations over the way the study was conducted.
She said that the composite score to measure response rates was “defined arbitrarily,” its prognostic value “has not been demonstrated,” and also pointed out that mixed responses by lesions within the same patient led to changes in scores.
In addition, the time interval between the end of treatment and lesion rebiopsy was “highly variable,” and the follow-up period was short.
Consequently, Dr. Psyrri believes the importance of the findings is “unclear,” especially as several patients who responded to nivolumab went on to develop cancer anyway, a finding that needs further investigation.
The study was funded by Bristol Myers Squibb.
Dr. Hanna declared relationships with BMS, Bicara, Exicure, Gateway for Cancer Research, GSK, Kite, NantKwest, Regeneron, Sanofi Genzyme, Maverick, and Merck.
A version of this article first appeared on Medscape.com.
(PL), a high-risk precancerous disease, into oral cancer, suggest the results from a phase 2 study.
“We think that immunotherapy as a preventative strategy, either as first-line or even secondary prevention, should be further explored,” said lead researcher Glenn J. Hanna, MD, director, Center for Salivary and Rare Head and Neck Cancers, Dana-Farber Cancer Institute, Boston.
The research was presented at the European Society for Medical Oncology Annual Congress in Paris.
Oral leukoplakia refers to a white plaque of “questionable cancer risk” that affects about 4% of the global population, Dr. Hanna explained. However, about 5% of leukoplakia cases develop into oral proliferative leukoplakia, an aggressive form of the disease characterized by multifocal lesions. It has a high risk of transformation to oral squamous cell carcinoma (OSCC), at approaching 10% per year, and the 5-year cancer-free survival rate is estimated to be 47%.
While there are no effective therapies to prevent progression to oral cancer, the condition does have a “rich immune microenvironment,” potentially making it amenable to programmed death (PD)-1 blockade, Dr. Hanna said.
His team conducted a single-arm, phase 2 trial involving 33 patients with proliferative leukoplakia with greater than or equal to 2 multifocal lesions, or contiguous lesions of greater than or equal to 3 cm, or a single lesion greater than or equal to 4 cm with any degree of epithelial dysplasia. The median age was 63.2 years, and 55% were women. Just over half (52%) were never smokers.
The main disease subsite was the oral tongue in 39% of participants, followed by the buccal gingiva in 30%, and 24% of patients had a prior diagnosis of OSCC.
Following a pretreatment biopsy at one to three sites, the patients received four doses of nivolumab every 28 days, followed by rebiopsy. At each visit, the patients had intraoral photographs taken of the lesions and measurements taken.
The median time from study registration to the first dose of nivolumab was 9 days. The majority (88%) of patients completed all four doses of nivolumab.
The median time from the first dose of nivolumab to the posttreatment biopsy was 115 days and ranged from 29 to 171 days.
The overall response rate, defined as a greater than or equal to 40% decrease in a composite score combining the size and degree of dysplasia between the pre- and posttreatment assessments, was observed in 36.4% of patients.
After a median follow-up of 14.7 months, the median cancer-free survival was not reached, with cancer events recorded in 21.2% of patients. The median time from the last dose of nivolumab to the first OSCC event was 3.7 months.
Cancer-free survival at 1 year was calculated to be 77.7%, which was unchanged at 2 years. At the final follow-up, all patients were still alive.
Additional analysis of the biopsies revealed that the lesions had programmed death ligand 1 (PD-L1) combined positive scores that ranged from 0 to 80, with 66.7% of patients having a score of greater than or equal to 1. A cutoff score of greater than or equal to 20 did not reveal any significant differences in cancer-free survival rates.
Turning to safety, Dr. Hanna said that nivolumab was associated with “acceptable toxicity” in this “non-cancer population,” with 21.2% of patients experiencing a grade 3-4 adverse event.
The most common adverse events of any grade were fatigue (55%), diarrhea (27%), elevated alanine transaminase levels (18%), elevated aspartate transaminase levels (18%), and other skin disorders (18%).
With a relatively low rate of adverse events and a “clinical benefit” in up to a third of patients, Dr. Hanna said that this was the “first study to our knowledge to demonstrate the potential efficacy of anti–PD-L1 blockade among patients with a high-risk oral precancerous disease.”
Discussing this study at the meeting, Amanda Psyrri, MD, PhD, professor of medical oncology, Attikon University Hospital, Athens, who was not involved in the research, said these data were “very interesting,” but she expressed some reservations over the way the study was conducted.
She said that the composite score to measure response rates was “defined arbitrarily,” its prognostic value “has not been demonstrated,” and also pointed out that mixed responses by lesions within the same patient led to changes in scores.
In addition, the time interval between the end of treatment and lesion rebiopsy was “highly variable,” and the follow-up period was short.
Consequently, Dr. Psyrri believes the importance of the findings is “unclear,” especially as several patients who responded to nivolumab went on to develop cancer anyway, a finding that needs further investigation.
The study was funded by Bristol Myers Squibb.
Dr. Hanna declared relationships with BMS, Bicara, Exicure, Gateway for Cancer Research, GSK, Kite, NantKwest, Regeneron, Sanofi Genzyme, Maverick, and Merck.
A version of this article first appeared on Medscape.com.
In NSCLC, not all EGFR mutations are the same
In non–small cell lung cancer (NSCLC), . However, there is a range of different EGFR mutations, and different mutation combinations can lead to different tumor characteristics that might in turn affect response to therapy.
A new real-world analysis of 159 NSCLC patients found that a combination of a mutation of the TP53 tumor suppressor gene and the EGFR Ex20 mutation is associated with worse disease outcomes, compared to patients with the EGFR Ex20 mutation alone. But the news wasn’t all bad. The same group of patients also responded better to ICB (immune checkpoint blockade) therapy than did the broader population of EGFR Ex20 patients.
The EGFR Ex20 mutation occurs in about 4% of NSCLC cases, while TP53 is quite common: The new study found a frequency of 43.9%. “We first have to mention that the findings regarding TP53 do not reach statistical significance; however, the trend is very strong, and results might be hampered due to small sample sizes. We think it is [appropriate] to exhaust more treatment options for these patients, especially targeted approaches with newer drugs that specifically target exon 20 insertions, as these drugs were not applied in our cohort,” Anna Kron, Dr. rer. medic., said in an email exchange. Dr. Kron presented the results at a poster session in Paris at the ESMO Congress. She is a researcher at University Hospital of Cologne, Germany.
The ImmunoTarget study, published in 2019, examined over 500 NSCLC patients with a range of driver mutations including EGFR and found that they responded poorly to ICIs in comparison to KRAS mutations.
But Dr. Kron’s group was not convinced. “Ex20 mutations differ clinically from other tyrosine kinase mutations in EGFR. We set out this study to rechallenge the paradigm of impaired benefit from ICI in EGFR-mutated patients, as we consider these mutations not interchangeable with other EGFR mutations,” Dr. Kron said.
“We would postulate that in EGFR Exon 20 mutations, ICI and specific inhibitors should be part of the therapeutic course. In patients with co-occurring TP53 mutations, treatment escalation could be considered,” Dr. Kron said.
The study included 159 patients with advanced NSCLC with the EGFR exon 20 insertion, who were treated between 2014 and 2020 at German hospitals. Among the patients, 37.7% were female; mean age at diagnosis was 65.87 years; 50.3% had a smoking history and 38.4% did not (data were unavailable for the rest); and 9.4% of tumors were stage I, 4.4% stage II, 8.2% stage IIIA, 3.8% stage IIIB, and 74.2% stage IV.
Over a follow-up of 4.1 years, there was a trend toward longer survival among patients with TP53 wild type (OS, 20 versus 12 months; P = .092). Sixty-six patients who received ICI therapy had better OS compared with those who did not (22 versus 10 months; P = .018). Among patients with co-occurring TP53 mutations, receipt of ICI therapy was associated with longer OS (16 versus 8 months; P = .048). There was a trend toward patients with TP53 wild type treated with ICI faring better than those who didn’t receive ICI (27.0 months versus 11.0 months; P = .109).
The researchers are continuing to study patients with EGFR Ex20 to better understand the role of TP53 and ICI therapy in these patients.
The study received no funding. Dr. Kron has no relevant financial disclosures.
In non–small cell lung cancer (NSCLC), . However, there is a range of different EGFR mutations, and different mutation combinations can lead to different tumor characteristics that might in turn affect response to therapy.
A new real-world analysis of 159 NSCLC patients found that a combination of a mutation of the TP53 tumor suppressor gene and the EGFR Ex20 mutation is associated with worse disease outcomes, compared to patients with the EGFR Ex20 mutation alone. But the news wasn’t all bad. The same group of patients also responded better to ICB (immune checkpoint blockade) therapy than did the broader population of EGFR Ex20 patients.
The EGFR Ex20 mutation occurs in about 4% of NSCLC cases, while TP53 is quite common: The new study found a frequency of 43.9%. “We first have to mention that the findings regarding TP53 do not reach statistical significance; however, the trend is very strong, and results might be hampered due to small sample sizes. We think it is [appropriate] to exhaust more treatment options for these patients, especially targeted approaches with newer drugs that specifically target exon 20 insertions, as these drugs were not applied in our cohort,” Anna Kron, Dr. rer. medic., said in an email exchange. Dr. Kron presented the results at a poster session in Paris at the ESMO Congress. She is a researcher at University Hospital of Cologne, Germany.
The ImmunoTarget study, published in 2019, examined over 500 NSCLC patients with a range of driver mutations including EGFR and found that they responded poorly to ICIs in comparison to KRAS mutations.
But Dr. Kron’s group was not convinced. “Ex20 mutations differ clinically from other tyrosine kinase mutations in EGFR. We set out this study to rechallenge the paradigm of impaired benefit from ICI in EGFR-mutated patients, as we consider these mutations not interchangeable with other EGFR mutations,” Dr. Kron said.
“We would postulate that in EGFR Exon 20 mutations, ICI and specific inhibitors should be part of the therapeutic course. In patients with co-occurring TP53 mutations, treatment escalation could be considered,” Dr. Kron said.
The study included 159 patients with advanced NSCLC with the EGFR exon 20 insertion, who were treated between 2014 and 2020 at German hospitals. Among the patients, 37.7% were female; mean age at diagnosis was 65.87 years; 50.3% had a smoking history and 38.4% did not (data were unavailable for the rest); and 9.4% of tumors were stage I, 4.4% stage II, 8.2% stage IIIA, 3.8% stage IIIB, and 74.2% stage IV.
Over a follow-up of 4.1 years, there was a trend toward longer survival among patients with TP53 wild type (OS, 20 versus 12 months; P = .092). Sixty-six patients who received ICI therapy had better OS compared with those who did not (22 versus 10 months; P = .018). Among patients with co-occurring TP53 mutations, receipt of ICI therapy was associated with longer OS (16 versus 8 months; P = .048). There was a trend toward patients with TP53 wild type treated with ICI faring better than those who didn’t receive ICI (27.0 months versus 11.0 months; P = .109).
The researchers are continuing to study patients with EGFR Ex20 to better understand the role of TP53 and ICI therapy in these patients.
The study received no funding. Dr. Kron has no relevant financial disclosures.
In non–small cell lung cancer (NSCLC), . However, there is a range of different EGFR mutations, and different mutation combinations can lead to different tumor characteristics that might in turn affect response to therapy.
A new real-world analysis of 159 NSCLC patients found that a combination of a mutation of the TP53 tumor suppressor gene and the EGFR Ex20 mutation is associated with worse disease outcomes, compared to patients with the EGFR Ex20 mutation alone. But the news wasn’t all bad. The same group of patients also responded better to ICB (immune checkpoint blockade) therapy than did the broader population of EGFR Ex20 patients.
The EGFR Ex20 mutation occurs in about 4% of NSCLC cases, while TP53 is quite common: The new study found a frequency of 43.9%. “We first have to mention that the findings regarding TP53 do not reach statistical significance; however, the trend is very strong, and results might be hampered due to small sample sizes. We think it is [appropriate] to exhaust more treatment options for these patients, especially targeted approaches with newer drugs that specifically target exon 20 insertions, as these drugs were not applied in our cohort,” Anna Kron, Dr. rer. medic., said in an email exchange. Dr. Kron presented the results at a poster session in Paris at the ESMO Congress. She is a researcher at University Hospital of Cologne, Germany.
The ImmunoTarget study, published in 2019, examined over 500 NSCLC patients with a range of driver mutations including EGFR and found that they responded poorly to ICIs in comparison to KRAS mutations.
But Dr. Kron’s group was not convinced. “Ex20 mutations differ clinically from other tyrosine kinase mutations in EGFR. We set out this study to rechallenge the paradigm of impaired benefit from ICI in EGFR-mutated patients, as we consider these mutations not interchangeable with other EGFR mutations,” Dr. Kron said.
“We would postulate that in EGFR Exon 20 mutations, ICI and specific inhibitors should be part of the therapeutic course. In patients with co-occurring TP53 mutations, treatment escalation could be considered,” Dr. Kron said.
The study included 159 patients with advanced NSCLC with the EGFR exon 20 insertion, who were treated between 2014 and 2020 at German hospitals. Among the patients, 37.7% were female; mean age at diagnosis was 65.87 years; 50.3% had a smoking history and 38.4% did not (data were unavailable for the rest); and 9.4% of tumors were stage I, 4.4% stage II, 8.2% stage IIIA, 3.8% stage IIIB, and 74.2% stage IV.
Over a follow-up of 4.1 years, there was a trend toward longer survival among patients with TP53 wild type (OS, 20 versus 12 months; P = .092). Sixty-six patients who received ICI therapy had better OS compared with those who did not (22 versus 10 months; P = .018). Among patients with co-occurring TP53 mutations, receipt of ICI therapy was associated with longer OS (16 versus 8 months; P = .048). There was a trend toward patients with TP53 wild type treated with ICI faring better than those who didn’t receive ICI (27.0 months versus 11.0 months; P = .109).
The researchers are continuing to study patients with EGFR Ex20 to better understand the role of TP53 and ICI therapy in these patients.
The study received no funding. Dr. Kron has no relevant financial disclosures.
FROM ESMO CONGRESS 2022
In early NSCLC, comorbidities linked to survival
Cardiometabolic and respiratory comorbidities are associated with worse survival in patients with non–small cell lung cancer (NSCLC), and new research suggests a potential mechanism.
Prior studies had shown mixed results when it came to these comorbidities and survival, according to study coauthor author Geoffrey Liu, MD, who is an epidemiology researcher at the University of Toronto Princess Margaret Cancer Centre. The new work represents data from multiple continents, from various ethnicities and cultures.
“We found that comorbidities had much greater impact on earlier than later stages of lung cancer, consistent with this previous study,” said Dr. Liu in an email. The study was presented by Miguel Garcia-Pardo, who is a researcher at University of Toronto Princess Margaret Cancer Centre, during a poster session at the annual meeting of the European Society for Medical Oncology.
“Deaths from [cardiometabolic] comorbidities were mainly from non–lung cancer competing causes, whereas the deaths from respiratory comorbidities were primarily driven by lung cancer specific survival, i.e., deaths from lung cancer itself. We conclude that Dr. Liu said.
Dr. Liu noted that controlling cardiometabolic risk factors like diabetes and hypertension is typically de-emphasized after diagnosis with early-stage lung cancer. The rationale is often that the lung cancer is a more acute concern than longer-term cardiometabolic risks. “The data from our analyses suggest a rethinking of this strategy. We need to pay more attention to controlling cardiovascular risk factors in early-stage lung cancer,” Dr. Liu said.
The findings also suggest that respiratory comorbidities should be managed more aggressively. That would allow more patients to undergo treatments like surgery and stereotactic radiation.
The Clinical Outcome Studies of the International Lung Cancer Consortium drew from two dozen studies conducted across five continents. It examined clinical, epidemiologic, genetic, and genomic factors and their potential influence on NSCLC outcomes. Cardiometabolic comorbidities included coronary artery disease, diabetes, vascular related diseases, and other heart diseases. Respiratory comorbidities included chronic obstructive pulmonary disease and asthma.
The analysis included 16,354 patients. Among patients with stage I NSCLC, there was an association between reduced overall survival (OS) and cardiometabolic comorbidity (adjusted hazard ratio, 1.17; P = .01) and respiratory comorbidity (aHR, 1.36; P < .001). For stage II/III patients, there was no significant association between OS and cardiometabolic comorbidities, but respiratory comorbidity was associated with worse OS (aHR, 1.15; P < .001). In stage 4, worse OS was associated with both cardiometabolic health comorbidity (aHR, 1.11; P = .03), but not respiratory comorbidity.
Among patients with stage IV NSCLC, there were no associations between overall survival or lung cancer–specific survival (LCSS) and respiratory or cardiometabolic risk factors. However, an examination of cause of death found a different pattern in patients with stage IB-IIIA disease: LCSS was worse among patients with respiratory comorbidities (aHR, 1.21; 95% CI, 1.09-1.34). Among those with cardiovascular comorbidities, the risk of non-NSCLC mortality was higher (aHR, 1.36; 95% CI, 1.15-1.63). The presence of respiratory comorbidity was associated with a reduced probability of undergoing surgical resection for both stage I (adjusted odds ratio, 0.45; 95% CI, 0.35-0.59) and stage II/III patients (aOR, 0.66; 95% CI, 0.53-0.80).
There was an association between non-NSCLC mortality and cardiometabolic comorbidities in stage IA (aHR, 1.37; 95% CI, 1.06-1.77) and in stages IB-IIIA (aHR, 1.32; 95% CI, 1.03-1.71) NSCLC. There were also associations between NSCLC mortality and respiratory comorbidity among stage IA (aHR, 1.51; 95% CI, 1.17-1.95) and stages IB-IIIA (aHR, 1.20; 95% CI, 1.06-1.36) NSCLC. There were no associations between respiratory comorbidity and non-NSCLC mortality.
Respiratory comorbidity was associated with a lower chance of undergoing surgical resection in stage IA (aHR, 0.54; 95% CI, 0.35-0.83) and stage IB-IIIA (aHR, 0.57; 95% CI, 0.46-0.70) cancers. Cardiometabolic comorbidity was associated with a lower rate of surgical resection only in stage 1B-3A patients (aHR, 0.73; 95% CI, 0.56-0.96). Among those who underwent resection, stage IA patients were less likely to die of lung cancer (aHR, 0.38; 95% CI, 0.28-0.52) but more likely to die of other causes (aHR, 1.73; 95% CI, 1.07-1.78). Stage IB-IIIA patients who underwent resection were less likely to die of lung cancer (aHR, 0.37; 95%, 0.32-0.42), but there was no significant association with non–lung cancer mortality.
The study was funded by the Lusi Wong Family Fund and the Alan Brown Chair. Dr. Liu has no relevant financial disclosures.
Cardiometabolic and respiratory comorbidities are associated with worse survival in patients with non–small cell lung cancer (NSCLC), and new research suggests a potential mechanism.
Prior studies had shown mixed results when it came to these comorbidities and survival, according to study coauthor author Geoffrey Liu, MD, who is an epidemiology researcher at the University of Toronto Princess Margaret Cancer Centre. The new work represents data from multiple continents, from various ethnicities and cultures.
“We found that comorbidities had much greater impact on earlier than later stages of lung cancer, consistent with this previous study,” said Dr. Liu in an email. The study was presented by Miguel Garcia-Pardo, who is a researcher at University of Toronto Princess Margaret Cancer Centre, during a poster session at the annual meeting of the European Society for Medical Oncology.
“Deaths from [cardiometabolic] comorbidities were mainly from non–lung cancer competing causes, whereas the deaths from respiratory comorbidities were primarily driven by lung cancer specific survival, i.e., deaths from lung cancer itself. We conclude that Dr. Liu said.
Dr. Liu noted that controlling cardiometabolic risk factors like diabetes and hypertension is typically de-emphasized after diagnosis with early-stage lung cancer. The rationale is often that the lung cancer is a more acute concern than longer-term cardiometabolic risks. “The data from our analyses suggest a rethinking of this strategy. We need to pay more attention to controlling cardiovascular risk factors in early-stage lung cancer,” Dr. Liu said.
The findings also suggest that respiratory comorbidities should be managed more aggressively. That would allow more patients to undergo treatments like surgery and stereotactic radiation.
The Clinical Outcome Studies of the International Lung Cancer Consortium drew from two dozen studies conducted across five continents. It examined clinical, epidemiologic, genetic, and genomic factors and their potential influence on NSCLC outcomes. Cardiometabolic comorbidities included coronary artery disease, diabetes, vascular related diseases, and other heart diseases. Respiratory comorbidities included chronic obstructive pulmonary disease and asthma.
The analysis included 16,354 patients. Among patients with stage I NSCLC, there was an association between reduced overall survival (OS) and cardiometabolic comorbidity (adjusted hazard ratio, 1.17; P = .01) and respiratory comorbidity (aHR, 1.36; P < .001). For stage II/III patients, there was no significant association between OS and cardiometabolic comorbidities, but respiratory comorbidity was associated with worse OS (aHR, 1.15; P < .001). In stage 4, worse OS was associated with both cardiometabolic health comorbidity (aHR, 1.11; P = .03), but not respiratory comorbidity.
Among patients with stage IV NSCLC, there were no associations between overall survival or lung cancer–specific survival (LCSS) and respiratory or cardiometabolic risk factors. However, an examination of cause of death found a different pattern in patients with stage IB-IIIA disease: LCSS was worse among patients with respiratory comorbidities (aHR, 1.21; 95% CI, 1.09-1.34). Among those with cardiovascular comorbidities, the risk of non-NSCLC mortality was higher (aHR, 1.36; 95% CI, 1.15-1.63). The presence of respiratory comorbidity was associated with a reduced probability of undergoing surgical resection for both stage I (adjusted odds ratio, 0.45; 95% CI, 0.35-0.59) and stage II/III patients (aOR, 0.66; 95% CI, 0.53-0.80).
There was an association between non-NSCLC mortality and cardiometabolic comorbidities in stage IA (aHR, 1.37; 95% CI, 1.06-1.77) and in stages IB-IIIA (aHR, 1.32; 95% CI, 1.03-1.71) NSCLC. There were also associations between NSCLC mortality and respiratory comorbidity among stage IA (aHR, 1.51; 95% CI, 1.17-1.95) and stages IB-IIIA (aHR, 1.20; 95% CI, 1.06-1.36) NSCLC. There were no associations between respiratory comorbidity and non-NSCLC mortality.
Respiratory comorbidity was associated with a lower chance of undergoing surgical resection in stage IA (aHR, 0.54; 95% CI, 0.35-0.83) and stage IB-IIIA (aHR, 0.57; 95% CI, 0.46-0.70) cancers. Cardiometabolic comorbidity was associated with a lower rate of surgical resection only in stage 1B-3A patients (aHR, 0.73; 95% CI, 0.56-0.96). Among those who underwent resection, stage IA patients were less likely to die of lung cancer (aHR, 0.38; 95% CI, 0.28-0.52) but more likely to die of other causes (aHR, 1.73; 95% CI, 1.07-1.78). Stage IB-IIIA patients who underwent resection were less likely to die of lung cancer (aHR, 0.37; 95%, 0.32-0.42), but there was no significant association with non–lung cancer mortality.
The study was funded by the Lusi Wong Family Fund and the Alan Brown Chair. Dr. Liu has no relevant financial disclosures.
Cardiometabolic and respiratory comorbidities are associated with worse survival in patients with non–small cell lung cancer (NSCLC), and new research suggests a potential mechanism.
Prior studies had shown mixed results when it came to these comorbidities and survival, according to study coauthor author Geoffrey Liu, MD, who is an epidemiology researcher at the University of Toronto Princess Margaret Cancer Centre. The new work represents data from multiple continents, from various ethnicities and cultures.
“We found that comorbidities had much greater impact on earlier than later stages of lung cancer, consistent with this previous study,” said Dr. Liu in an email. The study was presented by Miguel Garcia-Pardo, who is a researcher at University of Toronto Princess Margaret Cancer Centre, during a poster session at the annual meeting of the European Society for Medical Oncology.
“Deaths from [cardiometabolic] comorbidities were mainly from non–lung cancer competing causes, whereas the deaths from respiratory comorbidities were primarily driven by lung cancer specific survival, i.e., deaths from lung cancer itself. We conclude that Dr. Liu said.
Dr. Liu noted that controlling cardiometabolic risk factors like diabetes and hypertension is typically de-emphasized after diagnosis with early-stage lung cancer. The rationale is often that the lung cancer is a more acute concern than longer-term cardiometabolic risks. “The data from our analyses suggest a rethinking of this strategy. We need to pay more attention to controlling cardiovascular risk factors in early-stage lung cancer,” Dr. Liu said.
The findings also suggest that respiratory comorbidities should be managed more aggressively. That would allow more patients to undergo treatments like surgery and stereotactic radiation.
The Clinical Outcome Studies of the International Lung Cancer Consortium drew from two dozen studies conducted across five continents. It examined clinical, epidemiologic, genetic, and genomic factors and their potential influence on NSCLC outcomes. Cardiometabolic comorbidities included coronary artery disease, diabetes, vascular related diseases, and other heart diseases. Respiratory comorbidities included chronic obstructive pulmonary disease and asthma.
The analysis included 16,354 patients. Among patients with stage I NSCLC, there was an association between reduced overall survival (OS) and cardiometabolic comorbidity (adjusted hazard ratio, 1.17; P = .01) and respiratory comorbidity (aHR, 1.36; P < .001). For stage II/III patients, there was no significant association between OS and cardiometabolic comorbidities, but respiratory comorbidity was associated with worse OS (aHR, 1.15; P < .001). In stage 4, worse OS was associated with both cardiometabolic health comorbidity (aHR, 1.11; P = .03), but not respiratory comorbidity.
Among patients with stage IV NSCLC, there were no associations between overall survival or lung cancer–specific survival (LCSS) and respiratory or cardiometabolic risk factors. However, an examination of cause of death found a different pattern in patients with stage IB-IIIA disease: LCSS was worse among patients with respiratory comorbidities (aHR, 1.21; 95% CI, 1.09-1.34). Among those with cardiovascular comorbidities, the risk of non-NSCLC mortality was higher (aHR, 1.36; 95% CI, 1.15-1.63). The presence of respiratory comorbidity was associated with a reduced probability of undergoing surgical resection for both stage I (adjusted odds ratio, 0.45; 95% CI, 0.35-0.59) and stage II/III patients (aOR, 0.66; 95% CI, 0.53-0.80).
There was an association between non-NSCLC mortality and cardiometabolic comorbidities in stage IA (aHR, 1.37; 95% CI, 1.06-1.77) and in stages IB-IIIA (aHR, 1.32; 95% CI, 1.03-1.71) NSCLC. There were also associations between NSCLC mortality and respiratory comorbidity among stage IA (aHR, 1.51; 95% CI, 1.17-1.95) and stages IB-IIIA (aHR, 1.20; 95% CI, 1.06-1.36) NSCLC. There were no associations between respiratory comorbidity and non-NSCLC mortality.
Respiratory comorbidity was associated with a lower chance of undergoing surgical resection in stage IA (aHR, 0.54; 95% CI, 0.35-0.83) and stage IB-IIIA (aHR, 0.57; 95% CI, 0.46-0.70) cancers. Cardiometabolic comorbidity was associated with a lower rate of surgical resection only in stage 1B-3A patients (aHR, 0.73; 95% CI, 0.56-0.96). Among those who underwent resection, stage IA patients were less likely to die of lung cancer (aHR, 0.38; 95% CI, 0.28-0.52) but more likely to die of other causes (aHR, 1.73; 95% CI, 1.07-1.78). Stage IB-IIIA patients who underwent resection were less likely to die of lung cancer (aHR, 0.37; 95%, 0.32-0.42), but there was no significant association with non–lung cancer mortality.
The study was funded by the Lusi Wong Family Fund and the Alan Brown Chair. Dr. Liu has no relevant financial disclosures.
FROM ESMO CONGRESS 2022
‘Smoking gun–level’ evidence found linking air pollution with lung cancer
PARIS – Air pollution has been recognized as a risk factor for lung cancer for about 2 decades, and already present in normal lung cells to cause cancer.
Think of it as “smoking gun–level” evidence that may explain why many nonsmokers still develop non–small cell lung cancer, said Charles Swanton, PhD, from the Francis Crick Institute and Cancer Research UK Chief Clinician, London.
“What this work shows is that air pollution is directly causing lung cancer but through a slightly unexpected pathway,” he said at a briefing prior to his presentation of the data in a presidential symposium held earlier this month in Paris at the European Society for Medical Oncology Congress 2022.
Importantly, he and his team also propose a mechanism for blocking the effects of air pollution with monoclonal antibodies directed against the inflammatory cytokine interleukein-1 beta.
Carcinogenesis explored
Lung cancer in never-smokers has a low mutational burden, with about 5- to 10-fold fewer mutations in a nonsmoker, compared with an ever smoker or current smoker, Dr. Swanton noted.
“The other thing to say about never-smokers is that they don’t have a clear environmental carcinogenic signature. So how do you square the circle? You’ve got the problem that you know that air pollution is associated with lung cancer – we don’t know if it causes it – but we also see that we’ve got no DNA mutations due to an environmental carcinogen,” he said during his symposium presentation.
The traditional model proposed to explain how carcinogens cause cancer holds that exposure to a carcinogen causes DNA mutations that lead to clonal expansion and tumor growth.
“But there are some major problems with this model,” Dr. Swanton said.
For example, normal skin contains a “patchwork of mutant clones,” but skin cancer is still uncommon, he said, and in studies in mice, 17 of 20 environmental carcinogens did not induce DNA mutations. He also noted that a common melanoma driver mutation, BRAF V600E, is not induced by exposure to a ultraviolet light.
“Any explanation for never-smoking lung cancer would have to fulfill three criteria: one, you have to explain why geographic variation exists; two, you have to prove causation; and three, you have to explain how cancers can be initiated without directly causing DNA mutations,” he said.
Normal lung tissues in nonsmoking adults can harbor pre-existing mutations, with the number of mutations increasing likely as a consequence of aging. In fact, more than 50% of normal lung biopsy tissues have been shown to harbor driver KRAS and/or EGFR mutations, Dr. Swanton said.
“In our research, these mutations alone only weakly potentiated cancer in laboratory models. However, when lung cells with these mutations were exposed to air pollutants, we saw more cancers and these occurred more quickly than when lung cells with these mutations were not exposed to pollutants, suggesting that air pollution promotes the initiation of lung cancer in cells harboring driver gene mutations. The next step is to discover why some lung cells with mutations become cancerous when exposed to pollutants while others don’t,” he said.
Geographical exposures
Looking at data on 447,932 participants in the UK Biobank, the investigators found that increasing exposure to ambient air particles smaller than 2.5 mcm (PM2.5) was significantly associated with seven cancer types, including lung cancer. They also saw an association between PM2.5 exposure levels and EGFR-mutated lung cancer incidence in the United Kingdom, South Korea, and Taiwan.
And crucially, as Dr. Swanton and associates showed in mouse models, exposure of lung cells bearing somatic EGFR and KRAS mutations to PM2.5 causes recruitment of macrophages that in turn secrete IL-1B, resulting in a transdifferentiation of EGFR-mutated cells into a cancer stem cell state, and tumor formation.
Importantly, pollution-induced tumor formation can be blocked by antibodies directed against IL-1B, Dr. Swanton said.
He pointed to a 2017 study in The Lancet suggesting that anti-inflammatory therapy with the anti–IL-1 antibody canakinumab (Ilaris) could reduce incident lung cancer and lung cancer deaths.
‘Elegant first demonstration’
“This is a very meaningful demonstration, from epidemiological data to preclinical models of the role of PM2.5 air pollutants in the promotion of lung cancer, and it provides us with very important insights into the mechanism through which nonsmokers can get lung cancer,” commented Suzette Delaloge, MD, from the cancer interception program at Institut Goustave Roussy in Villejuif, France, the invited discussant.
“But beyond that, it also has a great impact on our vision of carcinogenesis, with this very elegant first demonstration of the alternative nonmutagenic, carcinogenetic promotion hypothesis for fine particulate matter,” she said.
Questions still to be answered include whether PM2.5 pollutants could also be mutagenic, is the oncogenic pathway ubiquitous in tissue, which components of PM2.5 might drive the effect, how long of an exposure is required to promote lung cancer, and why and how persons without cancer develop specific driver mutations such as EGFR, she said.
“This research is intriguing and exciting as it means that we can ask whether, in the future, it will be possible to use lung scans to look for precancerous lesions in the lungs and try to reverse them with medicines such as interleukin-1B inhibitors,” said Tony Mok, MD, a lung cancer specialist at the Chinese University of Hong Kong, who was not involved in the study.
“We don’t yet know whether it will be possible to use highly sensitive EGFR profiling on blood or other samples to find nonsmokers who are predisposed to lung cancer and may benefit from lung scanning, so discussions are still very speculative,” he said in a statement.
The study was supported by Cancer Research UK, the Lung Cancer Research Foundations, Rosetrees Trust, the Mark Foundation for Cancer Research and the Ruth Strauss Foundation. Dr. Swanton disclosed grants/research support, honoraria, and stock ownership with multiple entities. Dr. Delaloge disclosed institutional financing and research funding from multiple companies. Dr. Mok disclosed stock ownership and honoraria with multiple companies.
PARIS – Air pollution has been recognized as a risk factor for lung cancer for about 2 decades, and already present in normal lung cells to cause cancer.
Think of it as “smoking gun–level” evidence that may explain why many nonsmokers still develop non–small cell lung cancer, said Charles Swanton, PhD, from the Francis Crick Institute and Cancer Research UK Chief Clinician, London.
“What this work shows is that air pollution is directly causing lung cancer but through a slightly unexpected pathway,” he said at a briefing prior to his presentation of the data in a presidential symposium held earlier this month in Paris at the European Society for Medical Oncology Congress 2022.
Importantly, he and his team also propose a mechanism for blocking the effects of air pollution with monoclonal antibodies directed against the inflammatory cytokine interleukein-1 beta.
Carcinogenesis explored
Lung cancer in never-smokers has a low mutational burden, with about 5- to 10-fold fewer mutations in a nonsmoker, compared with an ever smoker or current smoker, Dr. Swanton noted.
“The other thing to say about never-smokers is that they don’t have a clear environmental carcinogenic signature. So how do you square the circle? You’ve got the problem that you know that air pollution is associated with lung cancer – we don’t know if it causes it – but we also see that we’ve got no DNA mutations due to an environmental carcinogen,” he said during his symposium presentation.
The traditional model proposed to explain how carcinogens cause cancer holds that exposure to a carcinogen causes DNA mutations that lead to clonal expansion and tumor growth.
“But there are some major problems with this model,” Dr. Swanton said.
For example, normal skin contains a “patchwork of mutant clones,” but skin cancer is still uncommon, he said, and in studies in mice, 17 of 20 environmental carcinogens did not induce DNA mutations. He also noted that a common melanoma driver mutation, BRAF V600E, is not induced by exposure to a ultraviolet light.
“Any explanation for never-smoking lung cancer would have to fulfill three criteria: one, you have to explain why geographic variation exists; two, you have to prove causation; and three, you have to explain how cancers can be initiated without directly causing DNA mutations,” he said.
Normal lung tissues in nonsmoking adults can harbor pre-existing mutations, with the number of mutations increasing likely as a consequence of aging. In fact, more than 50% of normal lung biopsy tissues have been shown to harbor driver KRAS and/or EGFR mutations, Dr. Swanton said.
“In our research, these mutations alone only weakly potentiated cancer in laboratory models. However, when lung cells with these mutations were exposed to air pollutants, we saw more cancers and these occurred more quickly than when lung cells with these mutations were not exposed to pollutants, suggesting that air pollution promotes the initiation of lung cancer in cells harboring driver gene mutations. The next step is to discover why some lung cells with mutations become cancerous when exposed to pollutants while others don’t,” he said.
Geographical exposures
Looking at data on 447,932 participants in the UK Biobank, the investigators found that increasing exposure to ambient air particles smaller than 2.5 mcm (PM2.5) was significantly associated with seven cancer types, including lung cancer. They also saw an association between PM2.5 exposure levels and EGFR-mutated lung cancer incidence in the United Kingdom, South Korea, and Taiwan.
And crucially, as Dr. Swanton and associates showed in mouse models, exposure of lung cells bearing somatic EGFR and KRAS mutations to PM2.5 causes recruitment of macrophages that in turn secrete IL-1B, resulting in a transdifferentiation of EGFR-mutated cells into a cancer stem cell state, and tumor formation.
Importantly, pollution-induced tumor formation can be blocked by antibodies directed against IL-1B, Dr. Swanton said.
He pointed to a 2017 study in The Lancet suggesting that anti-inflammatory therapy with the anti–IL-1 antibody canakinumab (Ilaris) could reduce incident lung cancer and lung cancer deaths.
‘Elegant first demonstration’
“This is a very meaningful demonstration, from epidemiological data to preclinical models of the role of PM2.5 air pollutants in the promotion of lung cancer, and it provides us with very important insights into the mechanism through which nonsmokers can get lung cancer,” commented Suzette Delaloge, MD, from the cancer interception program at Institut Goustave Roussy in Villejuif, France, the invited discussant.
“But beyond that, it also has a great impact on our vision of carcinogenesis, with this very elegant first demonstration of the alternative nonmutagenic, carcinogenetic promotion hypothesis for fine particulate matter,” she said.
Questions still to be answered include whether PM2.5 pollutants could also be mutagenic, is the oncogenic pathway ubiquitous in tissue, which components of PM2.5 might drive the effect, how long of an exposure is required to promote lung cancer, and why and how persons without cancer develop specific driver mutations such as EGFR, she said.
“This research is intriguing and exciting as it means that we can ask whether, in the future, it will be possible to use lung scans to look for precancerous lesions in the lungs and try to reverse them with medicines such as interleukin-1B inhibitors,” said Tony Mok, MD, a lung cancer specialist at the Chinese University of Hong Kong, who was not involved in the study.
“We don’t yet know whether it will be possible to use highly sensitive EGFR profiling on blood or other samples to find nonsmokers who are predisposed to lung cancer and may benefit from lung scanning, so discussions are still very speculative,” he said in a statement.
The study was supported by Cancer Research UK, the Lung Cancer Research Foundations, Rosetrees Trust, the Mark Foundation for Cancer Research and the Ruth Strauss Foundation. Dr. Swanton disclosed grants/research support, honoraria, and stock ownership with multiple entities. Dr. Delaloge disclosed institutional financing and research funding from multiple companies. Dr. Mok disclosed stock ownership and honoraria with multiple companies.
PARIS – Air pollution has been recognized as a risk factor for lung cancer for about 2 decades, and already present in normal lung cells to cause cancer.
Think of it as “smoking gun–level” evidence that may explain why many nonsmokers still develop non–small cell lung cancer, said Charles Swanton, PhD, from the Francis Crick Institute and Cancer Research UK Chief Clinician, London.
“What this work shows is that air pollution is directly causing lung cancer but through a slightly unexpected pathway,” he said at a briefing prior to his presentation of the data in a presidential symposium held earlier this month in Paris at the European Society for Medical Oncology Congress 2022.
Importantly, he and his team also propose a mechanism for blocking the effects of air pollution with monoclonal antibodies directed against the inflammatory cytokine interleukein-1 beta.
Carcinogenesis explored
Lung cancer in never-smokers has a low mutational burden, with about 5- to 10-fold fewer mutations in a nonsmoker, compared with an ever smoker or current smoker, Dr. Swanton noted.
“The other thing to say about never-smokers is that they don’t have a clear environmental carcinogenic signature. So how do you square the circle? You’ve got the problem that you know that air pollution is associated with lung cancer – we don’t know if it causes it – but we also see that we’ve got no DNA mutations due to an environmental carcinogen,” he said during his symposium presentation.
The traditional model proposed to explain how carcinogens cause cancer holds that exposure to a carcinogen causes DNA mutations that lead to clonal expansion and tumor growth.
“But there are some major problems with this model,” Dr. Swanton said.
For example, normal skin contains a “patchwork of mutant clones,” but skin cancer is still uncommon, he said, and in studies in mice, 17 of 20 environmental carcinogens did not induce DNA mutations. He also noted that a common melanoma driver mutation, BRAF V600E, is not induced by exposure to a ultraviolet light.
“Any explanation for never-smoking lung cancer would have to fulfill three criteria: one, you have to explain why geographic variation exists; two, you have to prove causation; and three, you have to explain how cancers can be initiated without directly causing DNA mutations,” he said.
Normal lung tissues in nonsmoking adults can harbor pre-existing mutations, with the number of mutations increasing likely as a consequence of aging. In fact, more than 50% of normal lung biopsy tissues have been shown to harbor driver KRAS and/or EGFR mutations, Dr. Swanton said.
“In our research, these mutations alone only weakly potentiated cancer in laboratory models. However, when lung cells with these mutations were exposed to air pollutants, we saw more cancers and these occurred more quickly than when lung cells with these mutations were not exposed to pollutants, suggesting that air pollution promotes the initiation of lung cancer in cells harboring driver gene mutations. The next step is to discover why some lung cells with mutations become cancerous when exposed to pollutants while others don’t,” he said.
Geographical exposures
Looking at data on 447,932 participants in the UK Biobank, the investigators found that increasing exposure to ambient air particles smaller than 2.5 mcm (PM2.5) was significantly associated with seven cancer types, including lung cancer. They also saw an association between PM2.5 exposure levels and EGFR-mutated lung cancer incidence in the United Kingdom, South Korea, and Taiwan.
And crucially, as Dr. Swanton and associates showed in mouse models, exposure of lung cells bearing somatic EGFR and KRAS mutations to PM2.5 causes recruitment of macrophages that in turn secrete IL-1B, resulting in a transdifferentiation of EGFR-mutated cells into a cancer stem cell state, and tumor formation.
Importantly, pollution-induced tumor formation can be blocked by antibodies directed against IL-1B, Dr. Swanton said.
He pointed to a 2017 study in The Lancet suggesting that anti-inflammatory therapy with the anti–IL-1 antibody canakinumab (Ilaris) could reduce incident lung cancer and lung cancer deaths.
‘Elegant first demonstration’
“This is a very meaningful demonstration, from epidemiological data to preclinical models of the role of PM2.5 air pollutants in the promotion of lung cancer, and it provides us with very important insights into the mechanism through which nonsmokers can get lung cancer,” commented Suzette Delaloge, MD, from the cancer interception program at Institut Goustave Roussy in Villejuif, France, the invited discussant.
“But beyond that, it also has a great impact on our vision of carcinogenesis, with this very elegant first demonstration of the alternative nonmutagenic, carcinogenetic promotion hypothesis for fine particulate matter,” she said.
Questions still to be answered include whether PM2.5 pollutants could also be mutagenic, is the oncogenic pathway ubiquitous in tissue, which components of PM2.5 might drive the effect, how long of an exposure is required to promote lung cancer, and why and how persons without cancer develop specific driver mutations such as EGFR, she said.
“This research is intriguing and exciting as it means that we can ask whether, in the future, it will be possible to use lung scans to look for precancerous lesions in the lungs and try to reverse them with medicines such as interleukin-1B inhibitors,” said Tony Mok, MD, a lung cancer specialist at the Chinese University of Hong Kong, who was not involved in the study.
“We don’t yet know whether it will be possible to use highly sensitive EGFR profiling on blood or other samples to find nonsmokers who are predisposed to lung cancer and may benefit from lung scanning, so discussions are still very speculative,” he said in a statement.
The study was supported by Cancer Research UK, the Lung Cancer Research Foundations, Rosetrees Trust, the Mark Foundation for Cancer Research and the Ruth Strauss Foundation. Dr. Swanton disclosed grants/research support, honoraria, and stock ownership with multiple entities. Dr. Delaloge disclosed institutional financing and research funding from multiple companies. Dr. Mok disclosed stock ownership and honoraria with multiple companies.
AT ESMO CONGRESS 2022
Gene mutations may drive lung cancer in never-smokers
Small cell lung cancer has traditionally been attributed almost exclusively to tobacco exposure, but some recent studies have suggested a higher than expected prevalence among nonsmokers. indicating that the subgroups may have unique disease characteristics. Key differences included a lower frequency of TP53 gene mutations and a higher frequency of epidermal growth factor receptor (EGFR) alterations in never smokers.
About 6.9% of small cell lung cancer patients in the CASPIAN study were nonsmokers, as were 3.0% in the IMpower133 study.
“Given that the pathogenesis of small cell lung cancer is often tied to the damaging effects of tobacco, we hypothesized that small cell lung cancer in never-smokers would possess distinct molecular attributes. Our data does not provide any solid evidence for any treatment implications, though it does raise therapeutic questions which we believe deserve further exploration,” said Michael Oh, MD, during a presentation of the study results at the annual meeting of the European Society for Medical Oncology. Dr. Oh is a fellow at the University of California, Los Angeles.
The topic is important clinically, according to Antonio Passaro, MD, PhD, who served as a discussant during the session. He noted that small cell lung cancer in never-smokers is the seventh-most common cause of cancer-related mortality worldwide. In non–small cell lung cancer, rates of tobacco-associated disease have been decreasing, but there are increases in diagnoses among never smokers. Nonsmoking small cell lung cancer patients do not have better prognoses, and novel therapies and advances like immunotherapy and low-dose CT lung cancer screening disproportionately benefit current or former smokers.
Potential risk factors for never-smokers include environmental exposures like radon gas, cooking oil vapors, indoor and outdoor wood burning, and genetic and viral factors. “At the present time we do not have the knowledge to identify the most important factor in development of lung cancer in never-smoking [patients],” said Dr. Passaro, who is a medical oncologist at the European Institute of Oncology in Milan.
He added that the current study results are interesting but need much more follow-up, such as “longitudinal studies combining detailed clinical annotation with tissue and blood sampling. Here there is a need for collaborative efforts.” Key questions include the roles of the genomic landscape in normal lung tissue may play, the lung micro-environment, genetic factors, and environmental exposures.
One key possibility is air pollution. “We know that lung cancer in never-smokers is frequent in some countries, for example in Asian countries and it is more frequent in the United States than in Europe, but to find an explanation to this kind of data is difficult at the present time,” Dr. Passaro said.
The researchers retrospectively analyzed data from 608 current or former smokers and 54 never-smokers with small cell lung cancer, with the latter making up 8% of the total population. 70.4% of never-smokers and 55.1% of current or former smokers were female (P = .031). There was no significant between-group difference with respect to age at diagnosis or race.
Somatic mutations were similar to what has been found in previous studies for current or former smokers. 85.2% had changes in TP53, compared with just 59.3% of never-smokers (Q < .001). Changes to EGFR were more common in never-smokers, occurring in 25.9% versus 2.6% (Q < .001). PIK3CA alterations were also more common in never-smokers (14.8% vs. 3.6%; Q = 0.022). There was no significant difference between the two groups with respect to changes in RB1.
Never smokers had tumors with less immune cell infiltration (P = .008), including fewer CD4+ T cells, CD8+ T cells, and macrophages. Their tumor mutation burden was also lower (median, 2.59 vs. 4.99; P < .001).
Dr. Oh has no relevant financial disclosures. Dr. Passaro has consulted, advised, and received research funding from a wide range of pharmaceutical companies.
Small cell lung cancer has traditionally been attributed almost exclusively to tobacco exposure, but some recent studies have suggested a higher than expected prevalence among nonsmokers. indicating that the subgroups may have unique disease characteristics. Key differences included a lower frequency of TP53 gene mutations and a higher frequency of epidermal growth factor receptor (EGFR) alterations in never smokers.
About 6.9% of small cell lung cancer patients in the CASPIAN study were nonsmokers, as were 3.0% in the IMpower133 study.
“Given that the pathogenesis of small cell lung cancer is often tied to the damaging effects of tobacco, we hypothesized that small cell lung cancer in never-smokers would possess distinct molecular attributes. Our data does not provide any solid evidence for any treatment implications, though it does raise therapeutic questions which we believe deserve further exploration,” said Michael Oh, MD, during a presentation of the study results at the annual meeting of the European Society for Medical Oncology. Dr. Oh is a fellow at the University of California, Los Angeles.
The topic is important clinically, according to Antonio Passaro, MD, PhD, who served as a discussant during the session. He noted that small cell lung cancer in never-smokers is the seventh-most common cause of cancer-related mortality worldwide. In non–small cell lung cancer, rates of tobacco-associated disease have been decreasing, but there are increases in diagnoses among never smokers. Nonsmoking small cell lung cancer patients do not have better prognoses, and novel therapies and advances like immunotherapy and low-dose CT lung cancer screening disproportionately benefit current or former smokers.
Potential risk factors for never-smokers include environmental exposures like radon gas, cooking oil vapors, indoor and outdoor wood burning, and genetic and viral factors. “At the present time we do not have the knowledge to identify the most important factor in development of lung cancer in never-smoking [patients],” said Dr. Passaro, who is a medical oncologist at the European Institute of Oncology in Milan.
He added that the current study results are interesting but need much more follow-up, such as “longitudinal studies combining detailed clinical annotation with tissue and blood sampling. Here there is a need for collaborative efforts.” Key questions include the roles of the genomic landscape in normal lung tissue may play, the lung micro-environment, genetic factors, and environmental exposures.
One key possibility is air pollution. “We know that lung cancer in never-smokers is frequent in some countries, for example in Asian countries and it is more frequent in the United States than in Europe, but to find an explanation to this kind of data is difficult at the present time,” Dr. Passaro said.
The researchers retrospectively analyzed data from 608 current or former smokers and 54 never-smokers with small cell lung cancer, with the latter making up 8% of the total population. 70.4% of never-smokers and 55.1% of current or former smokers were female (P = .031). There was no significant between-group difference with respect to age at diagnosis or race.
Somatic mutations were similar to what has been found in previous studies for current or former smokers. 85.2% had changes in TP53, compared with just 59.3% of never-smokers (Q < .001). Changes to EGFR were more common in never-smokers, occurring in 25.9% versus 2.6% (Q < .001). PIK3CA alterations were also more common in never-smokers (14.8% vs. 3.6%; Q = 0.022). There was no significant difference between the two groups with respect to changes in RB1.
Never smokers had tumors with less immune cell infiltration (P = .008), including fewer CD4+ T cells, CD8+ T cells, and macrophages. Their tumor mutation burden was also lower (median, 2.59 vs. 4.99; P < .001).
Dr. Oh has no relevant financial disclosures. Dr. Passaro has consulted, advised, and received research funding from a wide range of pharmaceutical companies.
Small cell lung cancer has traditionally been attributed almost exclusively to tobacco exposure, but some recent studies have suggested a higher than expected prevalence among nonsmokers. indicating that the subgroups may have unique disease characteristics. Key differences included a lower frequency of TP53 gene mutations and a higher frequency of epidermal growth factor receptor (EGFR) alterations in never smokers.
About 6.9% of small cell lung cancer patients in the CASPIAN study were nonsmokers, as were 3.0% in the IMpower133 study.
“Given that the pathogenesis of small cell lung cancer is often tied to the damaging effects of tobacco, we hypothesized that small cell lung cancer in never-smokers would possess distinct molecular attributes. Our data does not provide any solid evidence for any treatment implications, though it does raise therapeutic questions which we believe deserve further exploration,” said Michael Oh, MD, during a presentation of the study results at the annual meeting of the European Society for Medical Oncology. Dr. Oh is a fellow at the University of California, Los Angeles.
The topic is important clinically, according to Antonio Passaro, MD, PhD, who served as a discussant during the session. He noted that small cell lung cancer in never-smokers is the seventh-most common cause of cancer-related mortality worldwide. In non–small cell lung cancer, rates of tobacco-associated disease have been decreasing, but there are increases in diagnoses among never smokers. Nonsmoking small cell lung cancer patients do not have better prognoses, and novel therapies and advances like immunotherapy and low-dose CT lung cancer screening disproportionately benefit current or former smokers.
Potential risk factors for never-smokers include environmental exposures like radon gas, cooking oil vapors, indoor and outdoor wood burning, and genetic and viral factors. “At the present time we do not have the knowledge to identify the most important factor in development of lung cancer in never-smoking [patients],” said Dr. Passaro, who is a medical oncologist at the European Institute of Oncology in Milan.
He added that the current study results are interesting but need much more follow-up, such as “longitudinal studies combining detailed clinical annotation with tissue and blood sampling. Here there is a need for collaborative efforts.” Key questions include the roles of the genomic landscape in normal lung tissue may play, the lung micro-environment, genetic factors, and environmental exposures.
One key possibility is air pollution. “We know that lung cancer in never-smokers is frequent in some countries, for example in Asian countries and it is more frequent in the United States than in Europe, but to find an explanation to this kind of data is difficult at the present time,” Dr. Passaro said.
The researchers retrospectively analyzed data from 608 current or former smokers and 54 never-smokers with small cell lung cancer, with the latter making up 8% of the total population. 70.4% of never-smokers and 55.1% of current or former smokers were female (P = .031). There was no significant between-group difference with respect to age at diagnosis or race.
Somatic mutations were similar to what has been found in previous studies for current or former smokers. 85.2% had changes in TP53, compared with just 59.3% of never-smokers (Q < .001). Changes to EGFR were more common in never-smokers, occurring in 25.9% versus 2.6% (Q < .001). PIK3CA alterations were also more common in never-smokers (14.8% vs. 3.6%; Q = 0.022). There was no significant difference between the two groups with respect to changes in RB1.
Never smokers had tumors with less immune cell infiltration (P = .008), including fewer CD4+ T cells, CD8+ T cells, and macrophages. Their tumor mutation burden was also lower (median, 2.59 vs. 4.99; P < .001).
Dr. Oh has no relevant financial disclosures. Dr. Passaro has consulted, advised, and received research funding from a wide range of pharmaceutical companies.
AT ESMO CONGRESS 2022