User login
Cancer diet studies: Veggies get another rave, while red meat’s busted again
Researchers report that high consumption of vegetables – especially lettuce, legumes, and cruciferous varieties – appears to lower the risk of liver cancer/liver disease. A separate team suggests that high consumption of red meat, organ meats, and processed meats boosts the risk of gastric cancer.
The findings of the latter study “reinforce the idea that avoidance of red meat and processed meat is probably good beyond [the prevention of] colorectal cancer,” said corresponding author and epidemiologist Paolo Boffetta, MD, MPH, of Stony Brook University Cancer Center, New York, in an interview. “The possible carcinogenic effect may extend beyond the colon.”
Both studies were released at the annual meeting of the American Association for Cancer Research.
For the red meat study, researchers examined statistics from the Golestan cohort study, which is prospectively tracking 50,045 people aged 40-75 from northeastern Iran. The study focuses on esophageal cancer due to the region’s high rate of the disease.
Red meat consumption is fairly rare in the region, where residents typically prefer chicken, said study lead author Giulia Collatuzzo, MD, a resident physician in occupational medicine at the University of Bologna, Italy, in an interview. On average, participants reported eating 18.4 grams daily of red meat and 72.1 grams daily of white meat.
The researchers tracked study participants for a median 12-year follow-up, during which 369 developed esophageal cancer and 368 developed gastric cancer. Red meat was only linked to more esophageal cancer in women (hazard ratio, 1.13, 95% confidence interval, 1.00-1.18, for each quintile increase in consumption).
Overall red meat consumption (including red meat, organ meat, and processed meat) was linked to higher rates of gastric cancer (HR, 1.08, 95% CI, 1.00-1.17) for each quartile increase in consumption, as was consumption of the red meat subtype alone (HR, 1.09, 95% CI, 1.00-1.18).
According to Dr. Collatuzzo, the findings suggest that those in the highest quartile of overall red meat consumption may have around a 25% increase in risk, compared with the lowest quartile.
Overall, she said, the study findings aren’t surprising. The lack of a connection between red meat consumption and esophageal cancer may be due to the fact that meat only temporarily transits through the esophagus, she said.
For the liver cancer/liver disease study, researchers examined the medical records of 470,653 subjects in the NIH-AARP Diet and Health Study. They were recruited in 1995-1996 when they were 50-71 years old. Over a median follow-up of 15.5 years, 899 developed liver cancer, and 934 died of chronic liver disease.
The median intakes of vegetables in quintile 5 (highest) and quintile 1 (lowest) were 3.7 cups daily and 1.0 cups daily, respectively, said study lead author Long-Gang Zhao, MS, a graduate student at Harvard University.
After adjusting for possible cofounders, those in the highest quintile of vegetable consumption were a third less likely to develop liver cancer, compared with the lowest quintile (HR, 0.66, 95% CI, 0.53-0.82, P < 0.01). Several types of vegetables appeared to be the strongest cancer fighters: cruciferous (broccoli, cauliflower), lettuce, legumes, and carrots. These kinds of vegetables were also linked to lower rates of chronic liver disease mortality (all P < 0.01), as was total vegetable intake for the top quintile versus the lowest quintile (HR, 0.60, 95% CI, 0.49-0.74, P = < 0.01).
“A one-cup increase (8 oz or 225 g) in vegetable intake was associated with about 20% decreased risk of liver cancer incidence and chronic liver mortality,” Zhao said.
There was no statistically significant link between fruit consumption and liver cancer or chronic liver disease mortality.
The findings provide more insight into diet and liver disease, Zhao said. “Chronic liver disease, which predisposes to liver cancer, is the tenth cause of death worldwide, causing two million deaths each year. It shares some etiological processes with liver cancer. Therefore, examining both chronic liver disease mortality and liver cancer incidence in our study may provide a more general picture for the prevention of liver diseases.”
As for limitations, both studies are based on self-reports about food consumption, which can be unreliable, and the subjects in the fruit/vegetable analysis were mainly of European origin.
The authors of both studies report no relevant disclosures. No funding is reported for either study.
Researchers report that high consumption of vegetables – especially lettuce, legumes, and cruciferous varieties – appears to lower the risk of liver cancer/liver disease. A separate team suggests that high consumption of red meat, organ meats, and processed meats boosts the risk of gastric cancer.
The findings of the latter study “reinforce the idea that avoidance of red meat and processed meat is probably good beyond [the prevention of] colorectal cancer,” said corresponding author and epidemiologist Paolo Boffetta, MD, MPH, of Stony Brook University Cancer Center, New York, in an interview. “The possible carcinogenic effect may extend beyond the colon.”
Both studies were released at the annual meeting of the American Association for Cancer Research.
For the red meat study, researchers examined statistics from the Golestan cohort study, which is prospectively tracking 50,045 people aged 40-75 from northeastern Iran. The study focuses on esophageal cancer due to the region’s high rate of the disease.
Red meat consumption is fairly rare in the region, where residents typically prefer chicken, said study lead author Giulia Collatuzzo, MD, a resident physician in occupational medicine at the University of Bologna, Italy, in an interview. On average, participants reported eating 18.4 grams daily of red meat and 72.1 grams daily of white meat.
The researchers tracked study participants for a median 12-year follow-up, during which 369 developed esophageal cancer and 368 developed gastric cancer. Red meat was only linked to more esophageal cancer in women (hazard ratio, 1.13, 95% confidence interval, 1.00-1.18, for each quintile increase in consumption).
Overall red meat consumption (including red meat, organ meat, and processed meat) was linked to higher rates of gastric cancer (HR, 1.08, 95% CI, 1.00-1.17) for each quartile increase in consumption, as was consumption of the red meat subtype alone (HR, 1.09, 95% CI, 1.00-1.18).
According to Dr. Collatuzzo, the findings suggest that those in the highest quartile of overall red meat consumption may have around a 25% increase in risk, compared with the lowest quartile.
Overall, she said, the study findings aren’t surprising. The lack of a connection between red meat consumption and esophageal cancer may be due to the fact that meat only temporarily transits through the esophagus, she said.
For the liver cancer/liver disease study, researchers examined the medical records of 470,653 subjects in the NIH-AARP Diet and Health Study. They were recruited in 1995-1996 when they were 50-71 years old. Over a median follow-up of 15.5 years, 899 developed liver cancer, and 934 died of chronic liver disease.
The median intakes of vegetables in quintile 5 (highest) and quintile 1 (lowest) were 3.7 cups daily and 1.0 cups daily, respectively, said study lead author Long-Gang Zhao, MS, a graduate student at Harvard University.
After adjusting for possible cofounders, those in the highest quintile of vegetable consumption were a third less likely to develop liver cancer, compared with the lowest quintile (HR, 0.66, 95% CI, 0.53-0.82, P < 0.01). Several types of vegetables appeared to be the strongest cancer fighters: cruciferous (broccoli, cauliflower), lettuce, legumes, and carrots. These kinds of vegetables were also linked to lower rates of chronic liver disease mortality (all P < 0.01), as was total vegetable intake for the top quintile versus the lowest quintile (HR, 0.60, 95% CI, 0.49-0.74, P = < 0.01).
“A one-cup increase (8 oz or 225 g) in vegetable intake was associated with about 20% decreased risk of liver cancer incidence and chronic liver mortality,” Zhao said.
There was no statistically significant link between fruit consumption and liver cancer or chronic liver disease mortality.
The findings provide more insight into diet and liver disease, Zhao said. “Chronic liver disease, which predisposes to liver cancer, is the tenth cause of death worldwide, causing two million deaths each year. It shares some etiological processes with liver cancer. Therefore, examining both chronic liver disease mortality and liver cancer incidence in our study may provide a more general picture for the prevention of liver diseases.”
As for limitations, both studies are based on self-reports about food consumption, which can be unreliable, and the subjects in the fruit/vegetable analysis were mainly of European origin.
The authors of both studies report no relevant disclosures. No funding is reported for either study.
Researchers report that high consumption of vegetables – especially lettuce, legumes, and cruciferous varieties – appears to lower the risk of liver cancer/liver disease. A separate team suggests that high consumption of red meat, organ meats, and processed meats boosts the risk of gastric cancer.
The findings of the latter study “reinforce the idea that avoidance of red meat and processed meat is probably good beyond [the prevention of] colorectal cancer,” said corresponding author and epidemiologist Paolo Boffetta, MD, MPH, of Stony Brook University Cancer Center, New York, in an interview. “The possible carcinogenic effect may extend beyond the colon.”
Both studies were released at the annual meeting of the American Association for Cancer Research.
For the red meat study, researchers examined statistics from the Golestan cohort study, which is prospectively tracking 50,045 people aged 40-75 from northeastern Iran. The study focuses on esophageal cancer due to the region’s high rate of the disease.
Red meat consumption is fairly rare in the region, where residents typically prefer chicken, said study lead author Giulia Collatuzzo, MD, a resident physician in occupational medicine at the University of Bologna, Italy, in an interview. On average, participants reported eating 18.4 grams daily of red meat and 72.1 grams daily of white meat.
The researchers tracked study participants for a median 12-year follow-up, during which 369 developed esophageal cancer and 368 developed gastric cancer. Red meat was only linked to more esophageal cancer in women (hazard ratio, 1.13, 95% confidence interval, 1.00-1.18, for each quintile increase in consumption).
Overall red meat consumption (including red meat, organ meat, and processed meat) was linked to higher rates of gastric cancer (HR, 1.08, 95% CI, 1.00-1.17) for each quartile increase in consumption, as was consumption of the red meat subtype alone (HR, 1.09, 95% CI, 1.00-1.18).
According to Dr. Collatuzzo, the findings suggest that those in the highest quartile of overall red meat consumption may have around a 25% increase in risk, compared with the lowest quartile.
Overall, she said, the study findings aren’t surprising. The lack of a connection between red meat consumption and esophageal cancer may be due to the fact that meat only temporarily transits through the esophagus, she said.
For the liver cancer/liver disease study, researchers examined the medical records of 470,653 subjects in the NIH-AARP Diet and Health Study. They were recruited in 1995-1996 when they were 50-71 years old. Over a median follow-up of 15.5 years, 899 developed liver cancer, and 934 died of chronic liver disease.
The median intakes of vegetables in quintile 5 (highest) and quintile 1 (lowest) were 3.7 cups daily and 1.0 cups daily, respectively, said study lead author Long-Gang Zhao, MS, a graduate student at Harvard University.
After adjusting for possible cofounders, those in the highest quintile of vegetable consumption were a third less likely to develop liver cancer, compared with the lowest quintile (HR, 0.66, 95% CI, 0.53-0.82, P < 0.01). Several types of vegetables appeared to be the strongest cancer fighters: cruciferous (broccoli, cauliflower), lettuce, legumes, and carrots. These kinds of vegetables were also linked to lower rates of chronic liver disease mortality (all P < 0.01), as was total vegetable intake for the top quintile versus the lowest quintile (HR, 0.60, 95% CI, 0.49-0.74, P = < 0.01).
“A one-cup increase (8 oz or 225 g) in vegetable intake was associated with about 20% decreased risk of liver cancer incidence and chronic liver mortality,” Zhao said.
There was no statistically significant link between fruit consumption and liver cancer or chronic liver disease mortality.
The findings provide more insight into diet and liver disease, Zhao said. “Chronic liver disease, which predisposes to liver cancer, is the tenth cause of death worldwide, causing two million deaths each year. It shares some etiological processes with liver cancer. Therefore, examining both chronic liver disease mortality and liver cancer incidence in our study may provide a more general picture for the prevention of liver diseases.”
As for limitations, both studies are based on self-reports about food consumption, which can be unreliable, and the subjects in the fruit/vegetable analysis were mainly of European origin.
The authors of both studies report no relevant disclosures. No funding is reported for either study.
FROM AACR 2022
‘Time is blood’: Researchers devise shortcut to AHA diagnosis
“A simple algorithm for unexplained bleeding might be helpful to emergency department physicians and other frontline workers to improve recognition of the disease,” said Amar Kelkar, MD, a fellow at the Dana-Farber Cancer Institute, Boston, and corresponding author of “Time is blood: The impact of diagnostic delays on acquired hemophilia A,” a report that appeared in the journal Cureus.
According to Dr. Kelkar, AHA is an autoimmune disease caused by the formation of autoantibodies against factor VIII (FVIII). “Classically, patients present with various forms of bleeding symptoms, including extensive bruising, spontaneous prolonged or persistent bleeding, and blood in the urine. These symptoms are usually accompanied by a prolonged activated partial thromboplastin time (aPTT) test,” he said in an interview. “While this is a rare diagnosis to be seen in primary, critical, or emergency care, it’s a disease that most hematologists should have seen and managed before.”
For the new study, researchers retrospectively tracked patients with AHA at the OSF Healthcare System in Illinois from 2010 to 2017. They focused on six patients (mean age, 79.5; male = 5). Cancer was considered a cause in four cases, and autoimmune disease in one. The sixth case was idiopathic. Five of the six patients died, with all but one death related to bleeding.
The researchers note that they saw more cases than expected (6 per 2.1 million vs. an estimated incidence of 1.48 per 1 million per year), although they attributed this high incidence to the population being made up of older hospitalized patients. In fact, Dr. Kelkar said, researchers believe this is an undercount reflecting diagnostic misses.
The median time to diagnosis was 14 days, the authors report, reflecting other studies that have also shown delays. Pseudo-thrombosis and preexisting anticoagulant therapy likely contribute to the diagnostic delays, they write.
In their new report, the authors developed an algorithm to speed diagnosis.
“The initial step is the identification of a patient with new, unexplained bleeding,” they write. “In the setting of unexplained bleeding, a detailed clinical history, including medication use, along with a thorough physical examination is critical. Prompt primary laboratory testing should include a complete blood count, a metabolic panel including creatinine and bilirubin, and coagulation testing including aPTT and prothrombin time with international normalized ratio (PT/INR). A resulting isolated aPTT elevation will initiate subsequent steps. Early inpatient hematology consultation is recommended.”
The authors add: “An important point to highlight is that we recommend concurrently ordering an aPTT mixing study and a factor VIII activity (FVIII:C) once a prolonged aPTT is confirmed. This may decrease the time to initiate treatment and improve patient outcomes. If the mixing study result is abnormal with low FVIII:C, hemostatic treatment could be initiated with concurrent confirmatory Bethesda assay or anti-FVIII ELISA, preventing further delay in patient recovery and hopefully reducing potential complications. If there is limited availability of specialty testing or prolonged delays in getting test results, such as for FVIII:C, or an inability to confirm a diagnosis at any stage of the algorithm, transferring the patient to a higher level of care with these laboratory and hematology services should be strongly considered.”
The authors also note that “when the diagnostic delay is greater than 1 month, there will be a significant increase in the days that the patient is required to be on hemostatic therapy, compared to diagnosis before 1 month (23.8 ± 13 vs. 7.6 ± 5.7 days, respectively; P = .003).”
The algorithm is meant to be widely available, Dr. Kelkar said. “That is why we targeted an open-source, general medicine journal like Cureus.”
Jerome Teitel, MD, a hematologist with St. Michael’s Hospital in Toronto, said in an interview that the algorithm “might be a useful guide for initial investigation at community hospitals.”
However, he recommended against emphasizing the use of mixing studies. They are “often ambiguous and just delay ordering the definitive tests (FVIII activity and inhibitor assay), which will need to be done regardless,” he said. “The most important message should be that patients with AHA should be referred to, or at least comanaged with, a hematologist who has specific experience and expertise in the field, and who will likely have access to specialized coagulation tests with short turnaround times.”
Another hematologist, George M. Rodgers III, MD, of the University of Utah, Salt Lake City, said in an interview that the algorithm is appropriate for the evaluation of possible AHA. “Patients with the disorder who present with minor bleeding are not evaluated with high priority by physicians,” he said. “Patients with bleeding and a prolonged PTT should be taken very seriously because AHA patients can develop spontaneous fatal bleeding.”
No study funding is reported. The authors, Dr. Teitel, and Dr. Rodgers report no relevant disclosures.
“A simple algorithm for unexplained bleeding might be helpful to emergency department physicians and other frontline workers to improve recognition of the disease,” said Amar Kelkar, MD, a fellow at the Dana-Farber Cancer Institute, Boston, and corresponding author of “Time is blood: The impact of diagnostic delays on acquired hemophilia A,” a report that appeared in the journal Cureus.
According to Dr. Kelkar, AHA is an autoimmune disease caused by the formation of autoantibodies against factor VIII (FVIII). “Classically, patients present with various forms of bleeding symptoms, including extensive bruising, spontaneous prolonged or persistent bleeding, and blood in the urine. These symptoms are usually accompanied by a prolonged activated partial thromboplastin time (aPTT) test,” he said in an interview. “While this is a rare diagnosis to be seen in primary, critical, or emergency care, it’s a disease that most hematologists should have seen and managed before.”
For the new study, researchers retrospectively tracked patients with AHA at the OSF Healthcare System in Illinois from 2010 to 2017. They focused on six patients (mean age, 79.5; male = 5). Cancer was considered a cause in four cases, and autoimmune disease in one. The sixth case was idiopathic. Five of the six patients died, with all but one death related to bleeding.
The researchers note that they saw more cases than expected (6 per 2.1 million vs. an estimated incidence of 1.48 per 1 million per year), although they attributed this high incidence to the population being made up of older hospitalized patients. In fact, Dr. Kelkar said, researchers believe this is an undercount reflecting diagnostic misses.
The median time to diagnosis was 14 days, the authors report, reflecting other studies that have also shown delays. Pseudo-thrombosis and preexisting anticoagulant therapy likely contribute to the diagnostic delays, they write.
In their new report, the authors developed an algorithm to speed diagnosis.
“The initial step is the identification of a patient with new, unexplained bleeding,” they write. “In the setting of unexplained bleeding, a detailed clinical history, including medication use, along with a thorough physical examination is critical. Prompt primary laboratory testing should include a complete blood count, a metabolic panel including creatinine and bilirubin, and coagulation testing including aPTT and prothrombin time with international normalized ratio (PT/INR). A resulting isolated aPTT elevation will initiate subsequent steps. Early inpatient hematology consultation is recommended.”
The authors add: “An important point to highlight is that we recommend concurrently ordering an aPTT mixing study and a factor VIII activity (FVIII:C) once a prolonged aPTT is confirmed. This may decrease the time to initiate treatment and improve patient outcomes. If the mixing study result is abnormal with low FVIII:C, hemostatic treatment could be initiated with concurrent confirmatory Bethesda assay or anti-FVIII ELISA, preventing further delay in patient recovery and hopefully reducing potential complications. If there is limited availability of specialty testing or prolonged delays in getting test results, such as for FVIII:C, or an inability to confirm a diagnosis at any stage of the algorithm, transferring the patient to a higher level of care with these laboratory and hematology services should be strongly considered.”
The authors also note that “when the diagnostic delay is greater than 1 month, there will be a significant increase in the days that the patient is required to be on hemostatic therapy, compared to diagnosis before 1 month (23.8 ± 13 vs. 7.6 ± 5.7 days, respectively; P = .003).”
The algorithm is meant to be widely available, Dr. Kelkar said. “That is why we targeted an open-source, general medicine journal like Cureus.”
Jerome Teitel, MD, a hematologist with St. Michael’s Hospital in Toronto, said in an interview that the algorithm “might be a useful guide for initial investigation at community hospitals.”
However, he recommended against emphasizing the use of mixing studies. They are “often ambiguous and just delay ordering the definitive tests (FVIII activity and inhibitor assay), which will need to be done regardless,” he said. “The most important message should be that patients with AHA should be referred to, or at least comanaged with, a hematologist who has specific experience and expertise in the field, and who will likely have access to specialized coagulation tests with short turnaround times.”
Another hematologist, George M. Rodgers III, MD, of the University of Utah, Salt Lake City, said in an interview that the algorithm is appropriate for the evaluation of possible AHA. “Patients with the disorder who present with minor bleeding are not evaluated with high priority by physicians,” he said. “Patients with bleeding and a prolonged PTT should be taken very seriously because AHA patients can develop spontaneous fatal bleeding.”
No study funding is reported. The authors, Dr. Teitel, and Dr. Rodgers report no relevant disclosures.
“A simple algorithm for unexplained bleeding might be helpful to emergency department physicians and other frontline workers to improve recognition of the disease,” said Amar Kelkar, MD, a fellow at the Dana-Farber Cancer Institute, Boston, and corresponding author of “Time is blood: The impact of diagnostic delays on acquired hemophilia A,” a report that appeared in the journal Cureus.
According to Dr. Kelkar, AHA is an autoimmune disease caused by the formation of autoantibodies against factor VIII (FVIII). “Classically, patients present with various forms of bleeding symptoms, including extensive bruising, spontaneous prolonged or persistent bleeding, and blood in the urine. These symptoms are usually accompanied by a prolonged activated partial thromboplastin time (aPTT) test,” he said in an interview. “While this is a rare diagnosis to be seen in primary, critical, or emergency care, it’s a disease that most hematologists should have seen and managed before.”
For the new study, researchers retrospectively tracked patients with AHA at the OSF Healthcare System in Illinois from 2010 to 2017. They focused on six patients (mean age, 79.5; male = 5). Cancer was considered a cause in four cases, and autoimmune disease in one. The sixth case was idiopathic. Five of the six patients died, with all but one death related to bleeding.
The researchers note that they saw more cases than expected (6 per 2.1 million vs. an estimated incidence of 1.48 per 1 million per year), although they attributed this high incidence to the population being made up of older hospitalized patients. In fact, Dr. Kelkar said, researchers believe this is an undercount reflecting diagnostic misses.
The median time to diagnosis was 14 days, the authors report, reflecting other studies that have also shown delays. Pseudo-thrombosis and preexisting anticoagulant therapy likely contribute to the diagnostic delays, they write.
In their new report, the authors developed an algorithm to speed diagnosis.
“The initial step is the identification of a patient with new, unexplained bleeding,” they write. “In the setting of unexplained bleeding, a detailed clinical history, including medication use, along with a thorough physical examination is critical. Prompt primary laboratory testing should include a complete blood count, a metabolic panel including creatinine and bilirubin, and coagulation testing including aPTT and prothrombin time with international normalized ratio (PT/INR). A resulting isolated aPTT elevation will initiate subsequent steps. Early inpatient hematology consultation is recommended.”
The authors add: “An important point to highlight is that we recommend concurrently ordering an aPTT mixing study and a factor VIII activity (FVIII:C) once a prolonged aPTT is confirmed. This may decrease the time to initiate treatment and improve patient outcomes. If the mixing study result is abnormal with low FVIII:C, hemostatic treatment could be initiated with concurrent confirmatory Bethesda assay or anti-FVIII ELISA, preventing further delay in patient recovery and hopefully reducing potential complications. If there is limited availability of specialty testing or prolonged delays in getting test results, such as for FVIII:C, or an inability to confirm a diagnosis at any stage of the algorithm, transferring the patient to a higher level of care with these laboratory and hematology services should be strongly considered.”
The authors also note that “when the diagnostic delay is greater than 1 month, there will be a significant increase in the days that the patient is required to be on hemostatic therapy, compared to diagnosis before 1 month (23.8 ± 13 vs. 7.6 ± 5.7 days, respectively; P = .003).”
The algorithm is meant to be widely available, Dr. Kelkar said. “That is why we targeted an open-source, general medicine journal like Cureus.”
Jerome Teitel, MD, a hematologist with St. Michael’s Hospital in Toronto, said in an interview that the algorithm “might be a useful guide for initial investigation at community hospitals.”
However, he recommended against emphasizing the use of mixing studies. They are “often ambiguous and just delay ordering the definitive tests (FVIII activity and inhibitor assay), which will need to be done regardless,” he said. “The most important message should be that patients with AHA should be referred to, or at least comanaged with, a hematologist who has specific experience and expertise in the field, and who will likely have access to specialized coagulation tests with short turnaround times.”
Another hematologist, George M. Rodgers III, MD, of the University of Utah, Salt Lake City, said in an interview that the algorithm is appropriate for the evaluation of possible AHA. “Patients with the disorder who present with minor bleeding are not evaluated with high priority by physicians,” he said. “Patients with bleeding and a prolonged PTT should be taken very seriously because AHA patients can develop spontaneous fatal bleeding.”
No study funding is reported. The authors, Dr. Teitel, and Dr. Rodgers report no relevant disclosures.
FROM CUREUS
Judge strikes down Biden mask mandate for planes, transit
The mandate, enacted in February 2021, is unconstitutional because Congress never granted the Centers for Disease Control and Prevention the power to create such a requirement, U.S. District Judge Kathryn Kimball Mizelle said in her order issued April 18.
“Congress addressed whether the CDC may enact preventative measures that condition the interstate travel of an entire population to CDC dictates. It may not,” the order says.
While the government argued that the definition of “sanitation” in federal law allows it to create travel restrictions like the use of masks, Judge Mizelle disagreed.
“A power to improve ‘sanitation’ would easily extend to requiring vaccinations against COVID-19, the seasonal flu, or other diseases. Or to mandatory social distancing, coughing-into-elbows, and daily multivitamins,” she wrote.
The Biden administration has extended the mask mandate several times since it was first announced. Most recently, the mandate was extended last week and was set to end May 3.
The rule has been alternately praised and criticized by airlines, pilots, and flight attendants. Lawsuits have been filed over the mandate, but Judge Mizelle ruled in favor of two people and the Health Freedom Defense Fund, who filed suit in July 2021.
It is not yet clear if the Biden administration will appeal the decision.
A version of this article first appeared on WebMD.com.
The mandate, enacted in February 2021, is unconstitutional because Congress never granted the Centers for Disease Control and Prevention the power to create such a requirement, U.S. District Judge Kathryn Kimball Mizelle said in her order issued April 18.
“Congress addressed whether the CDC may enact preventative measures that condition the interstate travel of an entire population to CDC dictates. It may not,” the order says.
While the government argued that the definition of “sanitation” in federal law allows it to create travel restrictions like the use of masks, Judge Mizelle disagreed.
“A power to improve ‘sanitation’ would easily extend to requiring vaccinations against COVID-19, the seasonal flu, or other diseases. Or to mandatory social distancing, coughing-into-elbows, and daily multivitamins,” she wrote.
The Biden administration has extended the mask mandate several times since it was first announced. Most recently, the mandate was extended last week and was set to end May 3.
The rule has been alternately praised and criticized by airlines, pilots, and flight attendants. Lawsuits have been filed over the mandate, but Judge Mizelle ruled in favor of two people and the Health Freedom Defense Fund, who filed suit in July 2021.
It is not yet clear if the Biden administration will appeal the decision.
A version of this article first appeared on WebMD.com.
The mandate, enacted in February 2021, is unconstitutional because Congress never granted the Centers for Disease Control and Prevention the power to create such a requirement, U.S. District Judge Kathryn Kimball Mizelle said in her order issued April 18.
“Congress addressed whether the CDC may enact preventative measures that condition the interstate travel of an entire population to CDC dictates. It may not,” the order says.
While the government argued that the definition of “sanitation” in federal law allows it to create travel restrictions like the use of masks, Judge Mizelle disagreed.
“A power to improve ‘sanitation’ would easily extend to requiring vaccinations against COVID-19, the seasonal flu, or other diseases. Or to mandatory social distancing, coughing-into-elbows, and daily multivitamins,” she wrote.
The Biden administration has extended the mask mandate several times since it was first announced. Most recently, the mandate was extended last week and was set to end May 3.
The rule has been alternately praised and criticized by airlines, pilots, and flight attendants. Lawsuits have been filed over the mandate, but Judge Mizelle ruled in favor of two people and the Health Freedom Defense Fund, who filed suit in July 2021.
It is not yet clear if the Biden administration will appeal the decision.
A version of this article first appeared on WebMD.com.
Fresh data confirm healthy plant foods link to lower diabetes risk
A scientific analysis of metabolites from plant-based-diets – especially those rich in whole grains, fruits, and vegetables – may in the future yield clues as to how such eating patterns lower the risk of type 2 diabetes, finds a new study of more than 8,000 people.
The research looked at healthy, unhealthy, and overall plant-based diets, but only metabolic profiles for the healthy and overall plant-based diets showed an inverse relationship with type 2 diabetes.
A primarily “unhealthy” plant-based diet was one including mainly refined grains (e.g., white bread and pasta), fruit juices, potatoes, sugar-sweetened beverages, and sweets/desserts.
“Individual metabolites from consumption of polyphenol-rich plant foods like fruits, vegetables, coffee, and legumes are all closely linked to healthy plant-based diet and lower risk of diabetes,” lead author Frank Hu, MD, said in a press release.
Dr. Hu, of the department of nutrition at Harvard T.H. Chan School of Public Health, Boston, and colleagues reported their findings in Diabetologia.
High-throughput profiling of the metabolome
Given that an individual’s metabolic profile reflects their diet, there is a growing trend in nutritional research to use a technique called high-throughput metabolomics to profile biological samples.
The team conducted an analysis of blood plasma samples and dietary intake using food frequency questionnaires of 10,684 participants from three prospective cohorts (Nurses’ Health Study, Nurses’ Health Study II, and Health Professionals Follow-Up Study). Participants were predominantly White and middle-aged (mean age 54 years), with a mean body mass index of 25.6 kg/m2.
Metabolite profile scores were generated from the blood samples, taken in the 1980s and 1990s, and matched to any cases of incident type 2 diabetes reported during follow-up, which ended in 2016-2017.
The team looked at three different plant-based diets – by definition, higher in plant foods and lower in animal foods – and further categorized them according to the actual foods consumed, to generate an overall plant diet index (PDI), a healthy PDI, or an unhealthy PDI.
In all, 8,827 participants completed the study, and 270 cases of diabetes were reported.
Multi-metabolite profiles were composed of 55 metabolites for the overall PDI, 93 metabolites for healthy PDI, and 75 metabolites for unhealthy PDI.
The findings are that metabolomics can be harnessed and “the identified metabolic profiles could be used to assess adherence to ... plant-based diets as part of type 2 diabetes prevention ... and provide new insights for future investigation,” the researchers concluded.
One coauthor received research support from the California Walnut Commission and Swiss ReManagement; another reported being a scientific consultant to LayerIV. The other authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A scientific analysis of metabolites from plant-based-diets – especially those rich in whole grains, fruits, and vegetables – may in the future yield clues as to how such eating patterns lower the risk of type 2 diabetes, finds a new study of more than 8,000 people.
The research looked at healthy, unhealthy, and overall plant-based diets, but only metabolic profiles for the healthy and overall plant-based diets showed an inverse relationship with type 2 diabetes.
A primarily “unhealthy” plant-based diet was one including mainly refined grains (e.g., white bread and pasta), fruit juices, potatoes, sugar-sweetened beverages, and sweets/desserts.
“Individual metabolites from consumption of polyphenol-rich plant foods like fruits, vegetables, coffee, and legumes are all closely linked to healthy plant-based diet and lower risk of diabetes,” lead author Frank Hu, MD, said in a press release.
Dr. Hu, of the department of nutrition at Harvard T.H. Chan School of Public Health, Boston, and colleagues reported their findings in Diabetologia.
High-throughput profiling of the metabolome
Given that an individual’s metabolic profile reflects their diet, there is a growing trend in nutritional research to use a technique called high-throughput metabolomics to profile biological samples.
The team conducted an analysis of blood plasma samples and dietary intake using food frequency questionnaires of 10,684 participants from three prospective cohorts (Nurses’ Health Study, Nurses’ Health Study II, and Health Professionals Follow-Up Study). Participants were predominantly White and middle-aged (mean age 54 years), with a mean body mass index of 25.6 kg/m2.
Metabolite profile scores were generated from the blood samples, taken in the 1980s and 1990s, and matched to any cases of incident type 2 diabetes reported during follow-up, which ended in 2016-2017.
The team looked at three different plant-based diets – by definition, higher in plant foods and lower in animal foods – and further categorized them according to the actual foods consumed, to generate an overall plant diet index (PDI), a healthy PDI, or an unhealthy PDI.
In all, 8,827 participants completed the study, and 270 cases of diabetes were reported.
Multi-metabolite profiles were composed of 55 metabolites for the overall PDI, 93 metabolites for healthy PDI, and 75 metabolites for unhealthy PDI.
The findings are that metabolomics can be harnessed and “the identified metabolic profiles could be used to assess adherence to ... plant-based diets as part of type 2 diabetes prevention ... and provide new insights for future investigation,” the researchers concluded.
One coauthor received research support from the California Walnut Commission and Swiss ReManagement; another reported being a scientific consultant to LayerIV. The other authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A scientific analysis of metabolites from plant-based-diets – especially those rich in whole grains, fruits, and vegetables – may in the future yield clues as to how such eating patterns lower the risk of type 2 diabetes, finds a new study of more than 8,000 people.
The research looked at healthy, unhealthy, and overall plant-based diets, but only metabolic profiles for the healthy and overall plant-based diets showed an inverse relationship with type 2 diabetes.
A primarily “unhealthy” plant-based diet was one including mainly refined grains (e.g., white bread and pasta), fruit juices, potatoes, sugar-sweetened beverages, and sweets/desserts.
“Individual metabolites from consumption of polyphenol-rich plant foods like fruits, vegetables, coffee, and legumes are all closely linked to healthy plant-based diet and lower risk of diabetes,” lead author Frank Hu, MD, said in a press release.
Dr. Hu, of the department of nutrition at Harvard T.H. Chan School of Public Health, Boston, and colleagues reported their findings in Diabetologia.
High-throughput profiling of the metabolome
Given that an individual’s metabolic profile reflects their diet, there is a growing trend in nutritional research to use a technique called high-throughput metabolomics to profile biological samples.
The team conducted an analysis of blood plasma samples and dietary intake using food frequency questionnaires of 10,684 participants from three prospective cohorts (Nurses’ Health Study, Nurses’ Health Study II, and Health Professionals Follow-Up Study). Participants were predominantly White and middle-aged (mean age 54 years), with a mean body mass index of 25.6 kg/m2.
Metabolite profile scores were generated from the blood samples, taken in the 1980s and 1990s, and matched to any cases of incident type 2 diabetes reported during follow-up, which ended in 2016-2017.
The team looked at three different plant-based diets – by definition, higher in plant foods and lower in animal foods – and further categorized them according to the actual foods consumed, to generate an overall plant diet index (PDI), a healthy PDI, or an unhealthy PDI.
In all, 8,827 participants completed the study, and 270 cases of diabetes were reported.
Multi-metabolite profiles were composed of 55 metabolites for the overall PDI, 93 metabolites for healthy PDI, and 75 metabolites for unhealthy PDI.
The findings are that metabolomics can be harnessed and “the identified metabolic profiles could be used to assess adherence to ... plant-based diets as part of type 2 diabetes prevention ... and provide new insights for future investigation,” the researchers concluded.
One coauthor received research support from the California Walnut Commission and Swiss ReManagement; another reported being a scientific consultant to LayerIV. The other authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM DIABETOLOGIA
Novel COVID-19 vaccine could fill the void for patients with blood cancers
according to study results presented at the annual meeting of the American Association for Cancer Research.
The phase 1/2 trial included 54 patients with a B-cell deficiency (mean age, 63 years; 28% female): 4 had congenital B-cell deficiency and 50 had a blood cancer (lymphocytic leukemia or lymphoma). T-cell immune responses were observed in 86% of patients 28 days after vaccination with a single CoVac-1 dose. The potency of CoVac-1–induced T-cell responses exceeded those seen typically with B cell–deficient patient responses after mRNA vaccine treatment and were comparable with those seen among nonimmunocompromised COVID-19 patients.
In the majority of individuals, currently approved SARS-CoV-2 vaccines induce a robust immune response, however, their efficacy, has been shown to be decreased among individuals who are immunocompromised. Patients treated for hematologic cancers, in particular, receive treatment regimens that damage healthy immune cells, particularly B cells, said Juliane Walz, MD, the study’s senior author and professor of medicine at University Hospital Tübingen (Germany).
“In the clinic, we see many cancer patients who do not mount sufficient humoral immune responses after vaccination with available SARS-CoV-2 vaccines,” Dr. Walz said. “These patients are at a high risk for a severe course of COVID-19.”
B-cell deficiency, she stated, can be compensated for by enhancing T-cell responses against SARS-CoV-2, which can then combat infections in the absence of neutralizing antibodies.
In a prior study of CoVac-1 among 36 adults without immune deficiency, the vaccine elicited T-cell responses that were still robust 3 months post vaccination, and that included responses against omicron and other key SARS-CoV-2 variants.
While mRNA-based or adenoviral vector-based vaccines are limited to the spike protein and are thus prone to loss of activity because of viral mutations, CoVac-1–induced T-cell immunity is far more intense and broader, Dr. Walz said.
CoVac-1 is a peptide vaccine that is injected directly rather than being encoded via mRNA and targets different viral components. It would not be given, however, to healthy, immunocompetent adults because it is important for them to have both B-cell antibody and T-cell response.
The patients with B-cell deficiency recruited for the study were given a single dose of CoVac-1 and assessed for safety and immunogenicity until day 56. Prior vaccinations with an approved SARS-CoV-2 vaccine had failed to elicit a humoral response in 87% of the subjects.
“Our vaccine does not induce antibody responses,” Dr. Walz said. “However, it could be used to induce broad T-cell responses as a complementary or additive vaccine for elderly adults. In the elderly, antibody responses decline very, very fast after vaccination.”
Dr. Walz said that CoVac-1 could find application in various syndromes associated with congenital B-cell deficiencies, in autoimmune diseases such as rheumatoid arthritis and multiple sclerosis, or diseases treated with rituximab or other B cell–depleting therapies (for example, ofatumumab, blinatumomab, or chimeric antigen receptor T cells), and in transplant patients.
A phase 3 study of CoVac-1 versus placebo is under discussion and would require about 300-500 subjects, Dr. Walz said.
“CoVac-1 is designed to induce broad and long-lasting SARS-CoV-2 T-cell immunity, even in individuals who have impaired ability to mount sufficient immunity from a currently approved vaccine, and thus protect these high-risk patients from a severe course of COVID-19,” Dr. Walz said.
“Having an option for these patients is just critical – so this is significant work,” said Ana Maria Lopez, MD, MPH, of the Sidney Kimmel Cancer Center–Jefferson Health, Philadelphia.
Limitations of this study included the small sample size with low racial and ethnic diversity, Dr. Walz stated.
Funding was provided by the Ministry of Science, Research and the Arts of the state of Baden-Württemberg; the Federal Ministry of Research and Education in Germany; the German Research Foundation under Germany’s Excellence Strategy; and the Clinical Cooperation Unit Translational Immunology at University Hospital Tübingen. Dr. Walz holds the CoVac-1 patent.
according to study results presented at the annual meeting of the American Association for Cancer Research.
The phase 1/2 trial included 54 patients with a B-cell deficiency (mean age, 63 years; 28% female): 4 had congenital B-cell deficiency and 50 had a blood cancer (lymphocytic leukemia or lymphoma). T-cell immune responses were observed in 86% of patients 28 days after vaccination with a single CoVac-1 dose. The potency of CoVac-1–induced T-cell responses exceeded those seen typically with B cell–deficient patient responses after mRNA vaccine treatment and were comparable with those seen among nonimmunocompromised COVID-19 patients.
In the majority of individuals, currently approved SARS-CoV-2 vaccines induce a robust immune response, however, their efficacy, has been shown to be decreased among individuals who are immunocompromised. Patients treated for hematologic cancers, in particular, receive treatment regimens that damage healthy immune cells, particularly B cells, said Juliane Walz, MD, the study’s senior author and professor of medicine at University Hospital Tübingen (Germany).
“In the clinic, we see many cancer patients who do not mount sufficient humoral immune responses after vaccination with available SARS-CoV-2 vaccines,” Dr. Walz said. “These patients are at a high risk for a severe course of COVID-19.”
B-cell deficiency, she stated, can be compensated for by enhancing T-cell responses against SARS-CoV-2, which can then combat infections in the absence of neutralizing antibodies.
In a prior study of CoVac-1 among 36 adults without immune deficiency, the vaccine elicited T-cell responses that were still robust 3 months post vaccination, and that included responses against omicron and other key SARS-CoV-2 variants.
While mRNA-based or adenoviral vector-based vaccines are limited to the spike protein and are thus prone to loss of activity because of viral mutations, CoVac-1–induced T-cell immunity is far more intense and broader, Dr. Walz said.
CoVac-1 is a peptide vaccine that is injected directly rather than being encoded via mRNA and targets different viral components. It would not be given, however, to healthy, immunocompetent adults because it is important for them to have both B-cell antibody and T-cell response.
The patients with B-cell deficiency recruited for the study were given a single dose of CoVac-1 and assessed for safety and immunogenicity until day 56. Prior vaccinations with an approved SARS-CoV-2 vaccine had failed to elicit a humoral response in 87% of the subjects.
“Our vaccine does not induce antibody responses,” Dr. Walz said. “However, it could be used to induce broad T-cell responses as a complementary or additive vaccine for elderly adults. In the elderly, antibody responses decline very, very fast after vaccination.”
Dr. Walz said that CoVac-1 could find application in various syndromes associated with congenital B-cell deficiencies, in autoimmune diseases such as rheumatoid arthritis and multiple sclerosis, or diseases treated with rituximab or other B cell–depleting therapies (for example, ofatumumab, blinatumomab, or chimeric antigen receptor T cells), and in transplant patients.
A phase 3 study of CoVac-1 versus placebo is under discussion and would require about 300-500 subjects, Dr. Walz said.
“CoVac-1 is designed to induce broad and long-lasting SARS-CoV-2 T-cell immunity, even in individuals who have impaired ability to mount sufficient immunity from a currently approved vaccine, and thus protect these high-risk patients from a severe course of COVID-19,” Dr. Walz said.
“Having an option for these patients is just critical – so this is significant work,” said Ana Maria Lopez, MD, MPH, of the Sidney Kimmel Cancer Center–Jefferson Health, Philadelphia.
Limitations of this study included the small sample size with low racial and ethnic diversity, Dr. Walz stated.
Funding was provided by the Ministry of Science, Research and the Arts of the state of Baden-Württemberg; the Federal Ministry of Research and Education in Germany; the German Research Foundation under Germany’s Excellence Strategy; and the Clinical Cooperation Unit Translational Immunology at University Hospital Tübingen. Dr. Walz holds the CoVac-1 patent.
according to study results presented at the annual meeting of the American Association for Cancer Research.
The phase 1/2 trial included 54 patients with a B-cell deficiency (mean age, 63 years; 28% female): 4 had congenital B-cell deficiency and 50 had a blood cancer (lymphocytic leukemia or lymphoma). T-cell immune responses were observed in 86% of patients 28 days after vaccination with a single CoVac-1 dose. The potency of CoVac-1–induced T-cell responses exceeded those seen typically with B cell–deficient patient responses after mRNA vaccine treatment and were comparable with those seen among nonimmunocompromised COVID-19 patients.
In the majority of individuals, currently approved SARS-CoV-2 vaccines induce a robust immune response, however, their efficacy, has been shown to be decreased among individuals who are immunocompromised. Patients treated for hematologic cancers, in particular, receive treatment regimens that damage healthy immune cells, particularly B cells, said Juliane Walz, MD, the study’s senior author and professor of medicine at University Hospital Tübingen (Germany).
“In the clinic, we see many cancer patients who do not mount sufficient humoral immune responses after vaccination with available SARS-CoV-2 vaccines,” Dr. Walz said. “These patients are at a high risk for a severe course of COVID-19.”
B-cell deficiency, she stated, can be compensated for by enhancing T-cell responses against SARS-CoV-2, which can then combat infections in the absence of neutralizing antibodies.
In a prior study of CoVac-1 among 36 adults without immune deficiency, the vaccine elicited T-cell responses that were still robust 3 months post vaccination, and that included responses against omicron and other key SARS-CoV-2 variants.
While mRNA-based or adenoviral vector-based vaccines are limited to the spike protein and are thus prone to loss of activity because of viral mutations, CoVac-1–induced T-cell immunity is far more intense and broader, Dr. Walz said.
CoVac-1 is a peptide vaccine that is injected directly rather than being encoded via mRNA and targets different viral components. It would not be given, however, to healthy, immunocompetent adults because it is important for them to have both B-cell antibody and T-cell response.
The patients with B-cell deficiency recruited for the study were given a single dose of CoVac-1 and assessed for safety and immunogenicity until day 56. Prior vaccinations with an approved SARS-CoV-2 vaccine had failed to elicit a humoral response in 87% of the subjects.
“Our vaccine does not induce antibody responses,” Dr. Walz said. “However, it could be used to induce broad T-cell responses as a complementary or additive vaccine for elderly adults. In the elderly, antibody responses decline very, very fast after vaccination.”
Dr. Walz said that CoVac-1 could find application in various syndromes associated with congenital B-cell deficiencies, in autoimmune diseases such as rheumatoid arthritis and multiple sclerosis, or diseases treated with rituximab or other B cell–depleting therapies (for example, ofatumumab, blinatumomab, or chimeric antigen receptor T cells), and in transplant patients.
A phase 3 study of CoVac-1 versus placebo is under discussion and would require about 300-500 subjects, Dr. Walz said.
“CoVac-1 is designed to induce broad and long-lasting SARS-CoV-2 T-cell immunity, even in individuals who have impaired ability to mount sufficient immunity from a currently approved vaccine, and thus protect these high-risk patients from a severe course of COVID-19,” Dr. Walz said.
“Having an option for these patients is just critical – so this is significant work,” said Ana Maria Lopez, MD, MPH, of the Sidney Kimmel Cancer Center–Jefferson Health, Philadelphia.
Limitations of this study included the small sample size with low racial and ethnic diversity, Dr. Walz stated.
Funding was provided by the Ministry of Science, Research and the Arts of the state of Baden-Württemberg; the Federal Ministry of Research and Education in Germany; the German Research Foundation under Germany’s Excellence Strategy; and the Clinical Cooperation Unit Translational Immunology at University Hospital Tübingen. Dr. Walz holds the CoVac-1 patent.
FROM AACR 2022
1 in 7 breast cancer patients report worsening personal finances
a new study found. Factors like disease severity and treatment type didn’t seem to have an impact on financial status.
The findings, presented at the annual meeting of the American Association for Cancer Research, were unexpected. “We were surprised that we did not find that patients who received more aggressive therapies were more likely to experience worsening financial concerns,” said corresponding author and medical oncologist Kathryn J. Ruddy, MD, of the Mayo Clinici in Rochester, Minn.
The study was undertaken to understand the financial stress facing patients with breast cancer. The question was whether individual or disease factors, or both, were at play.
The study is based on results from the Mayo Clinic Breast Disease Registry, a prospective cohort of patient who were at Mayo Clinic Rochester. Participants answered questions about their finances at baseline and then again at annual follow-ups.
Researchers examined survey findings from 1,957 patients (mean age 58.5, 99.1% female, 95.4% White, 54.9% bachelor degree or higher) who answered questions at least twice from 2015-2020. The average time between diagnosis and the most recent follow-up was 25.6 months.
Of the 1,957 patients, 357 (18.2%) said their finances deteriorated as measured by a 1 point or higher decline on a 10-point scale.
There was no statistically significant link between deteriorating finances and age, race, employment status, stage of cancer at diagnosis, type of cancer, or treatment type. There was a slight link between deteriorating finances and reporting that they were in the category of “pay bills, no money for special things” near diagnosis.
Other research has suggested that breast cancer may not disrupt finances to a large extent, at least early on. Earlier in 2022, Stanford (Calif.) University researchers reported the results of a survey of 273 breast and gynecologic cancer patients who were surveyed about their finances at a mean of 3.4 years after diagnosis. While one-third said their cancer caused career changes, the study described overall financial toxicity as mild.
In regard to limitations, the subject population of the new study is overwhelmingly White, and the finances were self-reported by those who participated in the survey. Also, “because our participants were recruited at a tertiary medical center, there were relatively financially secure at baseline,” Dr. Ruddy said. “More financial hardship would be expected in a more financially diverse population.”
In an interview, Cathy Bradley, PhD, associate dean for research at the University of Colorado at Denver and deputy director of the University of Colorado Cancer Center, both in Aurora, praised the study as “an important start toward assessing financial burden in the clinic. Having more universal assessments in the clinic would remove stigma.”
She cautioned about interpreting a seemingly low number of patients whose financial situation worsened. “This was for a single site where there is a high rate of health insurance either through Medicare or Medicaid. There may be some selection bias as well given that Mayo may attract a wealthier patient population. Most women completed treatment and may not have been on long-term therapies.”
Moving forward, Dr. Ruddy said, “we hope to study cost of oncologic care in more geographically and financially diverse populations with breast cancer and other cancers.”
The study was funded by the Breast Cancer Research Foundation and National Cancer Institute. The study authors and Dr. Ruddy report no relevant disclosures.
a new study found. Factors like disease severity and treatment type didn’t seem to have an impact on financial status.
The findings, presented at the annual meeting of the American Association for Cancer Research, were unexpected. “We were surprised that we did not find that patients who received more aggressive therapies were more likely to experience worsening financial concerns,” said corresponding author and medical oncologist Kathryn J. Ruddy, MD, of the Mayo Clinici in Rochester, Minn.
The study was undertaken to understand the financial stress facing patients with breast cancer. The question was whether individual or disease factors, or both, were at play.
The study is based on results from the Mayo Clinic Breast Disease Registry, a prospective cohort of patient who were at Mayo Clinic Rochester. Participants answered questions about their finances at baseline and then again at annual follow-ups.
Researchers examined survey findings from 1,957 patients (mean age 58.5, 99.1% female, 95.4% White, 54.9% bachelor degree or higher) who answered questions at least twice from 2015-2020. The average time between diagnosis and the most recent follow-up was 25.6 months.
Of the 1,957 patients, 357 (18.2%) said their finances deteriorated as measured by a 1 point or higher decline on a 10-point scale.
There was no statistically significant link between deteriorating finances and age, race, employment status, stage of cancer at diagnosis, type of cancer, or treatment type. There was a slight link between deteriorating finances and reporting that they were in the category of “pay bills, no money for special things” near diagnosis.
Other research has suggested that breast cancer may not disrupt finances to a large extent, at least early on. Earlier in 2022, Stanford (Calif.) University researchers reported the results of a survey of 273 breast and gynecologic cancer patients who were surveyed about their finances at a mean of 3.4 years after diagnosis. While one-third said their cancer caused career changes, the study described overall financial toxicity as mild.
In regard to limitations, the subject population of the new study is overwhelmingly White, and the finances were self-reported by those who participated in the survey. Also, “because our participants were recruited at a tertiary medical center, there were relatively financially secure at baseline,” Dr. Ruddy said. “More financial hardship would be expected in a more financially diverse population.”
In an interview, Cathy Bradley, PhD, associate dean for research at the University of Colorado at Denver and deputy director of the University of Colorado Cancer Center, both in Aurora, praised the study as “an important start toward assessing financial burden in the clinic. Having more universal assessments in the clinic would remove stigma.”
She cautioned about interpreting a seemingly low number of patients whose financial situation worsened. “This was for a single site where there is a high rate of health insurance either through Medicare or Medicaid. There may be some selection bias as well given that Mayo may attract a wealthier patient population. Most women completed treatment and may not have been on long-term therapies.”
Moving forward, Dr. Ruddy said, “we hope to study cost of oncologic care in more geographically and financially diverse populations with breast cancer and other cancers.”
The study was funded by the Breast Cancer Research Foundation and National Cancer Institute. The study authors and Dr. Ruddy report no relevant disclosures.
a new study found. Factors like disease severity and treatment type didn’t seem to have an impact on financial status.
The findings, presented at the annual meeting of the American Association for Cancer Research, were unexpected. “We were surprised that we did not find that patients who received more aggressive therapies were more likely to experience worsening financial concerns,” said corresponding author and medical oncologist Kathryn J. Ruddy, MD, of the Mayo Clinici in Rochester, Minn.
The study was undertaken to understand the financial stress facing patients with breast cancer. The question was whether individual or disease factors, or both, were at play.
The study is based on results from the Mayo Clinic Breast Disease Registry, a prospective cohort of patient who were at Mayo Clinic Rochester. Participants answered questions about their finances at baseline and then again at annual follow-ups.
Researchers examined survey findings from 1,957 patients (mean age 58.5, 99.1% female, 95.4% White, 54.9% bachelor degree or higher) who answered questions at least twice from 2015-2020. The average time between diagnosis and the most recent follow-up was 25.6 months.
Of the 1,957 patients, 357 (18.2%) said their finances deteriorated as measured by a 1 point or higher decline on a 10-point scale.
There was no statistically significant link between deteriorating finances and age, race, employment status, stage of cancer at diagnosis, type of cancer, or treatment type. There was a slight link between deteriorating finances and reporting that they were in the category of “pay bills, no money for special things” near diagnosis.
Other research has suggested that breast cancer may not disrupt finances to a large extent, at least early on. Earlier in 2022, Stanford (Calif.) University researchers reported the results of a survey of 273 breast and gynecologic cancer patients who were surveyed about their finances at a mean of 3.4 years after diagnosis. While one-third said their cancer caused career changes, the study described overall financial toxicity as mild.
In regard to limitations, the subject population of the new study is overwhelmingly White, and the finances were self-reported by those who participated in the survey. Also, “because our participants were recruited at a tertiary medical center, there were relatively financially secure at baseline,” Dr. Ruddy said. “More financial hardship would be expected in a more financially diverse population.”
In an interview, Cathy Bradley, PhD, associate dean for research at the University of Colorado at Denver and deputy director of the University of Colorado Cancer Center, both in Aurora, praised the study as “an important start toward assessing financial burden in the clinic. Having more universal assessments in the clinic would remove stigma.”
She cautioned about interpreting a seemingly low number of patients whose financial situation worsened. “This was for a single site where there is a high rate of health insurance either through Medicare or Medicaid. There may be some selection bias as well given that Mayo may attract a wealthier patient population. Most women completed treatment and may not have been on long-term therapies.”
Moving forward, Dr. Ruddy said, “we hope to study cost of oncologic care in more geographically and financially diverse populations with breast cancer and other cancers.”
The study was funded by the Breast Cancer Research Foundation and National Cancer Institute. The study authors and Dr. Ruddy report no relevant disclosures.
FROM AACR 2022
Aged black garlic supplement may help lower BP
After 6 weeks, consumption of ABG with a high concentration of s-allyl-L-cystine (SAC) was associated with a nearly 6-mm Hg reduction in DBP in men. Other cardiovascular disease (CVD) risk factors were not significantly affected.
“The observed reduction in DBP by ABG extract was similar to the effects of dietary approaches, including the effects of the Dietary Approaches to Stop Hypertension(DASH) diet on BP,” say Rosa M. Valls, PhD, Universitat Rovira i Virgili, Reus, Spain, and colleagues.
“The potential beneficial effects of ABG may contribute to obtaining an optimal DBP” but were “better observed in men and in nonoptimal DBP populations,” they write in the study, published in Nutrients.
Pure SAC and aged garlics have shown healthy effects on multiple targets in in vitro and in vivo tests. However, previous studies in humans have not focused on ABG but rather on other types of aged garlic in patients with some type of CVD risk factor and suffered from methodologic or design weaknesses, the authors note.
To address this gap, Dr. Valls and colleagues randomly assigned 67 individuals with moderate hypercholesterolemia (defined as LDL levels of at least 115 mg/dL) to receive one ABG tablet (250 mg ABG extract/1.25 mg SAC) or placebo daily for 6 weeks. Following a 3-week washout, the groups were reversed and the new intervention continued for another 6 weeks.
Participants received dietary recommendations regarding CVD risk factors and had their dietary habits assessed through a 3-day food record at baseline and after 6 weeks during both treatments.
Individuals receiving lipid-lowering treatment or antihypertensives were excluded, as were those with a body mass index of 35 kg/m2 or higher, those with a fasting blood glucose of at least 126 mg/dL, or active smokers.
There were no differences in baseline characteristics between the two groups. The mean systolic and diastolic pressures at baseline were 124/75 mm Hg in the ABG group and 121/74 mm Hg in the placebo group. Their mean age was 53 years.
Adherence with the protocol was “high” at 96.5% in both groups, and no adverse effects were reported.
Reduced risk of death from stroke, ischemic heart disease
Although no significant differences between ABG and placebo were observed at 3 weeks, the decline in DBP after consumption of the ABG extract became significant at 6 weeks (mean change, –3.7 mm Hg vs. –0.10 mm Hg; P = .007).
When stratified by sex and categories of DBP, the mean change in DBP after 6 weeks of ABG consumption was particularly prominent in men and in those with a baseline DBP of at least 75 mm Hg.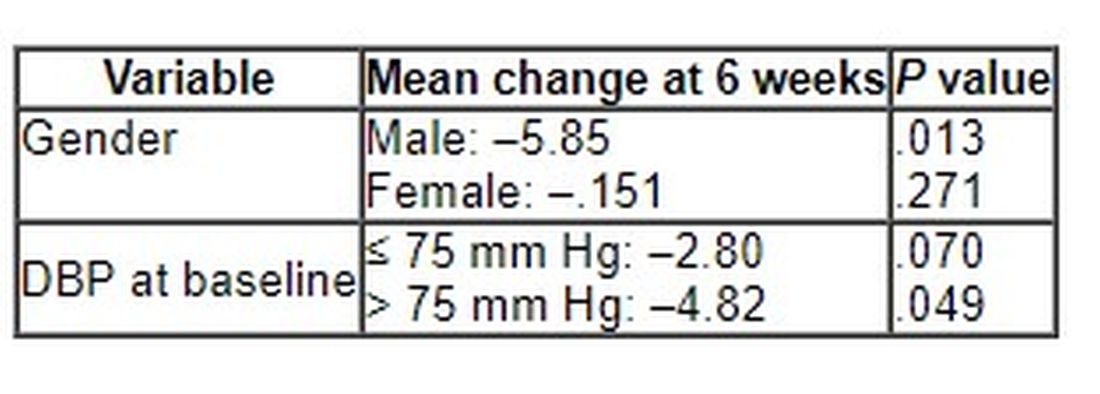
The 6-week change in systolic blood pressure with ABG and placebo was 1.32 mm Hg and 2.84 mm Hg, respectively (P = .694).
At week 6, total cholesterol levels showed a “quadratic decreasing trend” after ABG treatment (P = .047), but no other significant differences between groups were observed for lipid profile, apolipoproteins, or other outcomes of interest, including serum insulin, waist circumference, and body mass index.
The authors note that although systolic BP elevation “has a greater effect on outcomes, both systolic and diastolic hypertension independently influence the risk of adverse cardiovascular events, regardless of the definition of hypertension” and that the risk of death from ischemic heart disease and stroke doubles with every 10 mm Hg increase in DBP in people between the ages of 40 and 89 years.
“Thus, reducing DBP by 5 mm Hg results in a 40% lower risk of death from stroke and a 30% lower risk of death from ischemic heart disease or other vascular death,” they state.
Small study
Commenting for this news organization, Linda Van Horn, PhD, RDN, professor and chief of the department of preventive medicine’s nutrition division, Northwestern University, Chicago, said that for many years, garlic has been “reported to be an adjunct to the benefits of a healthy eating pattern, with inconclusive results.”
She noted that ABG is “literally aged for many months to years, and the resulting concentrate is found higher in many organosulfur compounds and phytochemicals that suggest enhanced response.”
Dr. Van Horn, a member of the American Heart Association’s Nutrition Committee, who was not involved with the study, continued: “The data suggest that ABG that is much more highly concentrated than fresh or processed garlic might be helpful in lowering BP in certain subgroups, in this case men with higher BP.”
However, she cautioned, “these results are limited in a small study, and ... potential other issues, such as sodium, potassium, or other nutrients known to be associated with blood pressure, were not reported, thereby raising questions about the exclusivity of the ABG over other accompanying dietary factors.”
The study was funded by the Center for the Development of Industrial Technology of the Spanish Ministry of Science and Innovation. Two authors are employees of Pharmactive Biotech Products, SL (Madrid), which manufactured the ABG product, but neither played a role in any result or conclusion. The other authors and Dr. Van Horn report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
After 6 weeks, consumption of ABG with a high concentration of s-allyl-L-cystine (SAC) was associated with a nearly 6-mm Hg reduction in DBP in men. Other cardiovascular disease (CVD) risk factors were not significantly affected.
“The observed reduction in DBP by ABG extract was similar to the effects of dietary approaches, including the effects of the Dietary Approaches to Stop Hypertension(DASH) diet on BP,” say Rosa M. Valls, PhD, Universitat Rovira i Virgili, Reus, Spain, and colleagues.
“The potential beneficial effects of ABG may contribute to obtaining an optimal DBP” but were “better observed in men and in nonoptimal DBP populations,” they write in the study, published in Nutrients.
Pure SAC and aged garlics have shown healthy effects on multiple targets in in vitro and in vivo tests. However, previous studies in humans have not focused on ABG but rather on other types of aged garlic in patients with some type of CVD risk factor and suffered from methodologic or design weaknesses, the authors note.
To address this gap, Dr. Valls and colleagues randomly assigned 67 individuals with moderate hypercholesterolemia (defined as LDL levels of at least 115 mg/dL) to receive one ABG tablet (250 mg ABG extract/1.25 mg SAC) or placebo daily for 6 weeks. Following a 3-week washout, the groups were reversed and the new intervention continued for another 6 weeks.
Participants received dietary recommendations regarding CVD risk factors and had their dietary habits assessed through a 3-day food record at baseline and after 6 weeks during both treatments.
Individuals receiving lipid-lowering treatment or antihypertensives were excluded, as were those with a body mass index of 35 kg/m2 or higher, those with a fasting blood glucose of at least 126 mg/dL, or active smokers.
There were no differences in baseline characteristics between the two groups. The mean systolic and diastolic pressures at baseline were 124/75 mm Hg in the ABG group and 121/74 mm Hg in the placebo group. Their mean age was 53 years.
Adherence with the protocol was “high” at 96.5% in both groups, and no adverse effects were reported.
Reduced risk of death from stroke, ischemic heart disease
Although no significant differences between ABG and placebo were observed at 3 weeks, the decline in DBP after consumption of the ABG extract became significant at 6 weeks (mean change, –3.7 mm Hg vs. –0.10 mm Hg; P = .007).
When stratified by sex and categories of DBP, the mean change in DBP after 6 weeks of ABG consumption was particularly prominent in men and in those with a baseline DBP of at least 75 mm Hg.
The 6-week change in systolic blood pressure with ABG and placebo was 1.32 mm Hg and 2.84 mm Hg, respectively (P = .694).
At week 6, total cholesterol levels showed a “quadratic decreasing trend” after ABG treatment (P = .047), but no other significant differences between groups were observed for lipid profile, apolipoproteins, or other outcomes of interest, including serum insulin, waist circumference, and body mass index.
The authors note that although systolic BP elevation “has a greater effect on outcomes, both systolic and diastolic hypertension independently influence the risk of adverse cardiovascular events, regardless of the definition of hypertension” and that the risk of death from ischemic heart disease and stroke doubles with every 10 mm Hg increase in DBP in people between the ages of 40 and 89 years.
“Thus, reducing DBP by 5 mm Hg results in a 40% lower risk of death from stroke and a 30% lower risk of death from ischemic heart disease or other vascular death,” they state.
Small study
Commenting for this news organization, Linda Van Horn, PhD, RDN, professor and chief of the department of preventive medicine’s nutrition division, Northwestern University, Chicago, said that for many years, garlic has been “reported to be an adjunct to the benefits of a healthy eating pattern, with inconclusive results.”
She noted that ABG is “literally aged for many months to years, and the resulting concentrate is found higher in many organosulfur compounds and phytochemicals that suggest enhanced response.”
Dr. Van Horn, a member of the American Heart Association’s Nutrition Committee, who was not involved with the study, continued: “The data suggest that ABG that is much more highly concentrated than fresh or processed garlic might be helpful in lowering BP in certain subgroups, in this case men with higher BP.”
However, she cautioned, “these results are limited in a small study, and ... potential other issues, such as sodium, potassium, or other nutrients known to be associated with blood pressure, were not reported, thereby raising questions about the exclusivity of the ABG over other accompanying dietary factors.”
The study was funded by the Center for the Development of Industrial Technology of the Spanish Ministry of Science and Innovation. Two authors are employees of Pharmactive Biotech Products, SL (Madrid), which manufactured the ABG product, but neither played a role in any result or conclusion. The other authors and Dr. Van Horn report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
After 6 weeks, consumption of ABG with a high concentration of s-allyl-L-cystine (SAC) was associated with a nearly 6-mm Hg reduction in DBP in men. Other cardiovascular disease (CVD) risk factors were not significantly affected.
“The observed reduction in DBP by ABG extract was similar to the effects of dietary approaches, including the effects of the Dietary Approaches to Stop Hypertension(DASH) diet on BP,” say Rosa M. Valls, PhD, Universitat Rovira i Virgili, Reus, Spain, and colleagues.
“The potential beneficial effects of ABG may contribute to obtaining an optimal DBP” but were “better observed in men and in nonoptimal DBP populations,” they write in the study, published in Nutrients.
Pure SAC and aged garlics have shown healthy effects on multiple targets in in vitro and in vivo tests. However, previous studies in humans have not focused on ABG but rather on other types of aged garlic in patients with some type of CVD risk factor and suffered from methodologic or design weaknesses, the authors note.
To address this gap, Dr. Valls and colleagues randomly assigned 67 individuals with moderate hypercholesterolemia (defined as LDL levels of at least 115 mg/dL) to receive one ABG tablet (250 mg ABG extract/1.25 mg SAC) or placebo daily for 6 weeks. Following a 3-week washout, the groups were reversed and the new intervention continued for another 6 weeks.
Participants received dietary recommendations regarding CVD risk factors and had their dietary habits assessed through a 3-day food record at baseline and after 6 weeks during both treatments.
Individuals receiving lipid-lowering treatment or antihypertensives were excluded, as were those with a body mass index of 35 kg/m2 or higher, those with a fasting blood glucose of at least 126 mg/dL, or active smokers.
There were no differences in baseline characteristics between the two groups. The mean systolic and diastolic pressures at baseline were 124/75 mm Hg in the ABG group and 121/74 mm Hg in the placebo group. Their mean age was 53 years.
Adherence with the protocol was “high” at 96.5% in both groups, and no adverse effects were reported.
Reduced risk of death from stroke, ischemic heart disease
Although no significant differences between ABG and placebo were observed at 3 weeks, the decline in DBP after consumption of the ABG extract became significant at 6 weeks (mean change, –3.7 mm Hg vs. –0.10 mm Hg; P = .007).
When stratified by sex and categories of DBP, the mean change in DBP after 6 weeks of ABG consumption was particularly prominent in men and in those with a baseline DBP of at least 75 mm Hg.
The 6-week change in systolic blood pressure with ABG and placebo was 1.32 mm Hg and 2.84 mm Hg, respectively (P = .694).
At week 6, total cholesterol levels showed a “quadratic decreasing trend” after ABG treatment (P = .047), but no other significant differences between groups were observed for lipid profile, apolipoproteins, or other outcomes of interest, including serum insulin, waist circumference, and body mass index.
The authors note that although systolic BP elevation “has a greater effect on outcomes, both systolic and diastolic hypertension independently influence the risk of adverse cardiovascular events, regardless of the definition of hypertension” and that the risk of death from ischemic heart disease and stroke doubles with every 10 mm Hg increase in DBP in people between the ages of 40 and 89 years.
“Thus, reducing DBP by 5 mm Hg results in a 40% lower risk of death from stroke and a 30% lower risk of death from ischemic heart disease or other vascular death,” they state.
Small study
Commenting for this news organization, Linda Van Horn, PhD, RDN, professor and chief of the department of preventive medicine’s nutrition division, Northwestern University, Chicago, said that for many years, garlic has been “reported to be an adjunct to the benefits of a healthy eating pattern, with inconclusive results.”
She noted that ABG is “literally aged for many months to years, and the resulting concentrate is found higher in many organosulfur compounds and phytochemicals that suggest enhanced response.”
Dr. Van Horn, a member of the American Heart Association’s Nutrition Committee, who was not involved with the study, continued: “The data suggest that ABG that is much more highly concentrated than fresh or processed garlic might be helpful in lowering BP in certain subgroups, in this case men with higher BP.”
However, she cautioned, “these results are limited in a small study, and ... potential other issues, such as sodium, potassium, or other nutrients known to be associated with blood pressure, were not reported, thereby raising questions about the exclusivity of the ABG over other accompanying dietary factors.”
The study was funded by the Center for the Development of Industrial Technology of the Spanish Ministry of Science and Innovation. Two authors are employees of Pharmactive Biotech Products, SL (Madrid), which manufactured the ABG product, but neither played a role in any result or conclusion. The other authors and Dr. Van Horn report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM NUTRIENTS
Pediatric hepatitis cases may be linked to adenovirus, CDC says
Internationally, 108 cases have been reported in the United Kingdom, with 79 cases occurring in England. There are three documented cases in Spain, and similar cases are being reported in Denmark and the Netherlands, according to an article in Science. In the United Kingdom, cases have been reported in children up to 16 years old, but most affected children are between 2 and 5 years old. Eight children in the United Kingdom have required liver transplants.
On April 14, the CDC said that nine cases have been recorded in Alabama since the fall of 2021. All of these cases have been in children between 1 and 6 years old, and two children have needed liver transplants. Two additional cases have been reported in North Carolina, according to Stat News, and both children have since recovered.
Hepatitis A, B, C, D, and E viruses—common causes of hepatitis—have been ruled out in the U.K. and Spanish cases. More than three-fourths (77%) of the children sickened in the United Kingdom and all nine cases in Alabama have tested positive for a form of the adenovirus. While adenovirus can cause hepatitis in children, it is usually in those who are immunocompromised.
The CDC health alert advises clinicians who have cases of unexplained hepatitis in children to test for adenovirus and report these cases to the CDC as well as state public health authorities. The agency recommends nucleic acid amplification testing to detect adenovirus using respiratory swabs, stool samples or rectal swabs, or blood.
Officials are exploring whether these cases are linked to a version of the virus called adenovirus 41, which is associated with gut inflammation. The most recent case in Alabama was reported in February, and five of the nine children in the state with these puzzling cases of hepatitis have tested positive for adenovirus 41.
There have yet to be any links among the cases in Alabama or North Carolina, and investigators in the United Kingdom have also not found any connections in their cases, STAT News reports.
“CDC is working with state health departments to see if there are additional U.S. cases and what may be causing these cases,” said Kristen Nordlund, a CDC spokesperson, in a statement to STAT News. “At this time, adenovirus may be the cause for these, but investigators are still learning more – including ruling out the more common causes of hepatitis.”
Looking for other explanations
None of the children in the United States with hepatitis had COVID-19, but a few children in the United Kingdom have tested positive for the virus; none of these children have received the COVID-19 vaccine.
While the U.K. Health Security Agency says their investigation “continues to point toward a link to adenovirus infection,” they are also considering other contributing factors such as an environmental cause or COVID-19.
“COVID has been consistently shown to increase liver test numbers,” Nancy Reau, MD, the section chief of hepatology at Rush University in Chicago, said in an interview with this news organization. “It has been shown to cause other organ involvement besides just pulmonary symptoms and respiratory failure. As this virus evolves, it might be that in children, it is more able to present as hepatitis.”
A version of this article first appeared on Medscape.com.
This article was updated 4/22/22.
Internationally, 108 cases have been reported in the United Kingdom, with 79 cases occurring in England. There are three documented cases in Spain, and similar cases are being reported in Denmark and the Netherlands, according to an article in Science. In the United Kingdom, cases have been reported in children up to 16 years old, but most affected children are between 2 and 5 years old. Eight children in the United Kingdom have required liver transplants.
On April 14, the CDC said that nine cases have been recorded in Alabama since the fall of 2021. All of these cases have been in children between 1 and 6 years old, and two children have needed liver transplants. Two additional cases have been reported in North Carolina, according to Stat News, and both children have since recovered.
Hepatitis A, B, C, D, and E viruses—common causes of hepatitis—have been ruled out in the U.K. and Spanish cases. More than three-fourths (77%) of the children sickened in the United Kingdom and all nine cases in Alabama have tested positive for a form of the adenovirus. While adenovirus can cause hepatitis in children, it is usually in those who are immunocompromised.
The CDC health alert advises clinicians who have cases of unexplained hepatitis in children to test for adenovirus and report these cases to the CDC as well as state public health authorities. The agency recommends nucleic acid amplification testing to detect adenovirus using respiratory swabs, stool samples or rectal swabs, or blood.
Officials are exploring whether these cases are linked to a version of the virus called adenovirus 41, which is associated with gut inflammation. The most recent case in Alabama was reported in February, and five of the nine children in the state with these puzzling cases of hepatitis have tested positive for adenovirus 41.
There have yet to be any links among the cases in Alabama or North Carolina, and investigators in the United Kingdom have also not found any connections in their cases, STAT News reports.
“CDC is working with state health departments to see if there are additional U.S. cases and what may be causing these cases,” said Kristen Nordlund, a CDC spokesperson, in a statement to STAT News. “At this time, adenovirus may be the cause for these, but investigators are still learning more – including ruling out the more common causes of hepatitis.”
Looking for other explanations
None of the children in the United States with hepatitis had COVID-19, but a few children in the United Kingdom have tested positive for the virus; none of these children have received the COVID-19 vaccine.
While the U.K. Health Security Agency says their investigation “continues to point toward a link to adenovirus infection,” they are also considering other contributing factors such as an environmental cause or COVID-19.
“COVID has been consistently shown to increase liver test numbers,” Nancy Reau, MD, the section chief of hepatology at Rush University in Chicago, said in an interview with this news organization. “It has been shown to cause other organ involvement besides just pulmonary symptoms and respiratory failure. As this virus evolves, it might be that in children, it is more able to present as hepatitis.”
A version of this article first appeared on Medscape.com.
This article was updated 4/22/22.
Internationally, 108 cases have been reported in the United Kingdom, with 79 cases occurring in England. There are three documented cases in Spain, and similar cases are being reported in Denmark and the Netherlands, according to an article in Science. In the United Kingdom, cases have been reported in children up to 16 years old, but most affected children are between 2 and 5 years old. Eight children in the United Kingdom have required liver transplants.
On April 14, the CDC said that nine cases have been recorded in Alabama since the fall of 2021. All of these cases have been in children between 1 and 6 years old, and two children have needed liver transplants. Two additional cases have been reported in North Carolina, according to Stat News, and both children have since recovered.
Hepatitis A, B, C, D, and E viruses—common causes of hepatitis—have been ruled out in the U.K. and Spanish cases. More than three-fourths (77%) of the children sickened in the United Kingdom and all nine cases in Alabama have tested positive for a form of the adenovirus. While adenovirus can cause hepatitis in children, it is usually in those who are immunocompromised.
The CDC health alert advises clinicians who have cases of unexplained hepatitis in children to test for adenovirus and report these cases to the CDC as well as state public health authorities. The agency recommends nucleic acid amplification testing to detect adenovirus using respiratory swabs, stool samples or rectal swabs, or blood.
Officials are exploring whether these cases are linked to a version of the virus called adenovirus 41, which is associated with gut inflammation. The most recent case in Alabama was reported in February, and five of the nine children in the state with these puzzling cases of hepatitis have tested positive for adenovirus 41.
There have yet to be any links among the cases in Alabama or North Carolina, and investigators in the United Kingdom have also not found any connections in their cases, STAT News reports.
“CDC is working with state health departments to see if there are additional U.S. cases and what may be causing these cases,” said Kristen Nordlund, a CDC spokesperson, in a statement to STAT News. “At this time, adenovirus may be the cause for these, but investigators are still learning more – including ruling out the more common causes of hepatitis.”
Looking for other explanations
None of the children in the United States with hepatitis had COVID-19, but a few children in the United Kingdom have tested positive for the virus; none of these children have received the COVID-19 vaccine.
While the U.K. Health Security Agency says their investigation “continues to point toward a link to adenovirus infection,” they are also considering other contributing factors such as an environmental cause or COVID-19.
“COVID has been consistently shown to increase liver test numbers,” Nancy Reau, MD, the section chief of hepatology at Rush University in Chicago, said in an interview with this news organization. “It has been shown to cause other organ involvement besides just pulmonary symptoms and respiratory failure. As this virus evolves, it might be that in children, it is more able to present as hepatitis.”
A version of this article first appeared on Medscape.com.
This article was updated 4/22/22.
Who doesn’t text in 2022? Most state Medicaid programs
West Virginia will use the U.S. Postal Service and an online account in the summer of 2022 to connect with Medicaid enrollees about the expected end of the COVID public health emergency, which will put many recipients at risk of losing their coverage.
What West Virginia won’t do is use a form of communication that’s ubiquitous worldwide: text messaging.
“West Virginia isn’t set up to text its members,” Allison Adler, the state’s Medicaid spokesperson, wrote to KHN in an email.
Indeed, most states’ Medicaid programs won’t text enrollees despite the urgency to reach them about renewing their coverage. A KFF report published in March found just 11 states said they would use texting to alert Medicaid recipients about the end of the COVID public health emergency. In contrast, 33 states plan to use snail mail and at least 20 will reach out with individual or automated phone calls.
“It doesn’t make any sense when texting is how most people communicate today,” said Kinda Serafi, a partner with the consulting firm Manatt Health.
State Medicaid agencies for months have been preparing for the end of the public health emergency. As part of a COVID relief law approved in March 2020, Congress prohibited states from dropping anyone from Medicaid coverage unless they moved out of state during the public health emergency. When the emergency ends, state Medicaid officials must reevaluate each enrollee’s eligibility. Millions of people could lose their coverage if they earn too much or fail to provide the information needed to verify income or residency.
As of November, about 86 million people were enrolled in Medicaid, according to the Centers for Medicare & Medicaid Services. That’s up from 71 million in February 2020, before COVID began to ravage the nation.
West Virginia has more than 600,000 Medicaid enrollees. Adler said about 100,000 of them could lose their eligibility at the end of the public health emergency because either the state has determined they’re ineligible or they’ve failed to respond to requests that they update their income information.
“It’s frustrating that texting is a means to meet people where they are and that this has not been picked up more by states,” said Jennifer Wagner, director of Medicaid eligibility and enrollment for the Center on Budget and Policy Priorities, a Washington-based research group.
The problem with relying on the Postal Service is that a letter can get hidden in “junk” mail or can fail to reach people who have moved or are homeless, Ms. Serafi said. And email, if people have an account, can end up in spam folders.
In contrast, surveys show lower-income Americans are just as likely to have smartphones and cellphones as the general population. And most people regularly use texting.
In Michigan, Medicaid officials started using text messaging to communicate with enrollees in 2020 after building a system with the help of federal COVID relief funding. They said texting is an economical way to reach enrollees.
“It costs us 2 cents per text message, which is incredibly cheap,” said Steph White, an enrollment coordinator for the Michigan Department of Health and Human Services. “It’s a great return on investment.”
CMS officials have told states they should consider texting, along with other communication methods, when trying to reach enrollees when the public health emergency ends. But many states don’t have the technology or information about enrollees to do it.
Efforts to add texting also face legal barriers, including a federal law that bars texting people without their consent. The Federal Communications Commission ruled in 2021 that state agencies are exempt from the law, but whether counties that handle Medicaid duties for some states and Medicaid managed-care organizations that work in more than 40 states are exempt as well is unclear, said Matt Salo, executive director of the National Association of Medicaid Directors.
CMS spokesperson Beth Lynk said the agency is trying to figure out how Medicaid agencies, counties, and health plans can text enrollees within the constraints of federal law.
Several states told KHN that Medicaid health plans will be helping connect with enrollees and that they expect the plans to use text messaging. But the requirement to get consent from enrollees before texting could limit that effort.
That’s the situation in Virginia, where only about 30,000 Medicaid enrollees – out of more than a million – have agreed to receive text messages directly from the state, said spokesperson Christina Nuckols.
In an effort to boost that number, the state plans to ask enrollees if they want to opt out of receiving text messages, rather than ask them to opt in, she said. This way enrollees would contact the state only if they don’t want to be texted. The state is reviewing its legal options to make that happen.
Meanwhile, Ms. Nuckols added, the state expects Medicaid health plans to contact enrollees about updating their contact information. Four of Virginia’s six Medicaid plans, which serve the bulk of the state’s enrollees, have permission to text about 316,000.
Craig Kennedy, CEO of Medicaid Health Plans of America, a trade group, said that most plans are using texting and that Medicaid officials will use multiple strategies to connect with enrollees. “I do not see this as a detriment, that states are not texting information about reenrollment,” he said. “I know we will be helping with that.”
California officials in March directed Medicaid health plans to use a variety of communication methods, including texting, to ensure that members can retain coverage if they remain eligible. The officials told health plans they could ask for consent through an initial text.
California officials say they also plan to ask enrollees for consent to be texted on the enrollment application, although federal approval for the change is not expected until the fall.
A few state Medicaid programs have experimented in recent years with pilot programs that included texting enrollees.
In 2019, Louisiana worked with the nonprofit group Code for America to send text messages that reminded people about renewing coverage and providing income information for verification. Compared with traditional communication methods, the texts led to a 67% increase in enrollees being renewed for coverage and a 56% increase in enrollees verifying their income in response to inquiries, said Medicaid spokesperson Alyson Neel.
Nonetheless, the state isn’t planning to text Medicaid enrollees about the end of the public health emergency because it hasn’t set up a system for that. “Medicaid has not yet been able to implement a text messaging system of its own due to other agency priorities,” Ms. Neel said.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
West Virginia will use the U.S. Postal Service and an online account in the summer of 2022 to connect with Medicaid enrollees about the expected end of the COVID public health emergency, which will put many recipients at risk of losing their coverage.
What West Virginia won’t do is use a form of communication that’s ubiquitous worldwide: text messaging.
“West Virginia isn’t set up to text its members,” Allison Adler, the state’s Medicaid spokesperson, wrote to KHN in an email.
Indeed, most states’ Medicaid programs won’t text enrollees despite the urgency to reach them about renewing their coverage. A KFF report published in March found just 11 states said they would use texting to alert Medicaid recipients about the end of the COVID public health emergency. In contrast, 33 states plan to use snail mail and at least 20 will reach out with individual or automated phone calls.
“It doesn’t make any sense when texting is how most people communicate today,” said Kinda Serafi, a partner with the consulting firm Manatt Health.
State Medicaid agencies for months have been preparing for the end of the public health emergency. As part of a COVID relief law approved in March 2020, Congress prohibited states from dropping anyone from Medicaid coverage unless they moved out of state during the public health emergency. When the emergency ends, state Medicaid officials must reevaluate each enrollee’s eligibility. Millions of people could lose their coverage if they earn too much or fail to provide the information needed to verify income or residency.
As of November, about 86 million people were enrolled in Medicaid, according to the Centers for Medicare & Medicaid Services. That’s up from 71 million in February 2020, before COVID began to ravage the nation.
West Virginia has more than 600,000 Medicaid enrollees. Adler said about 100,000 of them could lose their eligibility at the end of the public health emergency because either the state has determined they’re ineligible or they’ve failed to respond to requests that they update their income information.
“It’s frustrating that texting is a means to meet people where they are and that this has not been picked up more by states,” said Jennifer Wagner, director of Medicaid eligibility and enrollment for the Center on Budget and Policy Priorities, a Washington-based research group.
The problem with relying on the Postal Service is that a letter can get hidden in “junk” mail or can fail to reach people who have moved or are homeless, Ms. Serafi said. And email, if people have an account, can end up in spam folders.
In contrast, surveys show lower-income Americans are just as likely to have smartphones and cellphones as the general population. And most people regularly use texting.
In Michigan, Medicaid officials started using text messaging to communicate with enrollees in 2020 after building a system with the help of federal COVID relief funding. They said texting is an economical way to reach enrollees.
“It costs us 2 cents per text message, which is incredibly cheap,” said Steph White, an enrollment coordinator for the Michigan Department of Health and Human Services. “It’s a great return on investment.”
CMS officials have told states they should consider texting, along with other communication methods, when trying to reach enrollees when the public health emergency ends. But many states don’t have the technology or information about enrollees to do it.
Efforts to add texting also face legal barriers, including a federal law that bars texting people without their consent. The Federal Communications Commission ruled in 2021 that state agencies are exempt from the law, but whether counties that handle Medicaid duties for some states and Medicaid managed-care organizations that work in more than 40 states are exempt as well is unclear, said Matt Salo, executive director of the National Association of Medicaid Directors.
CMS spokesperson Beth Lynk said the agency is trying to figure out how Medicaid agencies, counties, and health plans can text enrollees within the constraints of federal law.
Several states told KHN that Medicaid health plans will be helping connect with enrollees and that they expect the plans to use text messaging. But the requirement to get consent from enrollees before texting could limit that effort.
That’s the situation in Virginia, where only about 30,000 Medicaid enrollees – out of more than a million – have agreed to receive text messages directly from the state, said spokesperson Christina Nuckols.
In an effort to boost that number, the state plans to ask enrollees if they want to opt out of receiving text messages, rather than ask them to opt in, she said. This way enrollees would contact the state only if they don’t want to be texted. The state is reviewing its legal options to make that happen.
Meanwhile, Ms. Nuckols added, the state expects Medicaid health plans to contact enrollees about updating their contact information. Four of Virginia’s six Medicaid plans, which serve the bulk of the state’s enrollees, have permission to text about 316,000.
Craig Kennedy, CEO of Medicaid Health Plans of America, a trade group, said that most plans are using texting and that Medicaid officials will use multiple strategies to connect with enrollees. “I do not see this as a detriment, that states are not texting information about reenrollment,” he said. “I know we will be helping with that.”
California officials in March directed Medicaid health plans to use a variety of communication methods, including texting, to ensure that members can retain coverage if they remain eligible. The officials told health plans they could ask for consent through an initial text.
California officials say they also plan to ask enrollees for consent to be texted on the enrollment application, although federal approval for the change is not expected until the fall.
A few state Medicaid programs have experimented in recent years with pilot programs that included texting enrollees.
In 2019, Louisiana worked with the nonprofit group Code for America to send text messages that reminded people about renewing coverage and providing income information for verification. Compared with traditional communication methods, the texts led to a 67% increase in enrollees being renewed for coverage and a 56% increase in enrollees verifying their income in response to inquiries, said Medicaid spokesperson Alyson Neel.
Nonetheless, the state isn’t planning to text Medicaid enrollees about the end of the public health emergency because it hasn’t set up a system for that. “Medicaid has not yet been able to implement a text messaging system of its own due to other agency priorities,” Ms. Neel said.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
West Virginia will use the U.S. Postal Service and an online account in the summer of 2022 to connect with Medicaid enrollees about the expected end of the COVID public health emergency, which will put many recipients at risk of losing their coverage.
What West Virginia won’t do is use a form of communication that’s ubiquitous worldwide: text messaging.
“West Virginia isn’t set up to text its members,” Allison Adler, the state’s Medicaid spokesperson, wrote to KHN in an email.
Indeed, most states’ Medicaid programs won’t text enrollees despite the urgency to reach them about renewing their coverage. A KFF report published in March found just 11 states said they would use texting to alert Medicaid recipients about the end of the COVID public health emergency. In contrast, 33 states plan to use snail mail and at least 20 will reach out with individual or automated phone calls.
“It doesn’t make any sense when texting is how most people communicate today,” said Kinda Serafi, a partner with the consulting firm Manatt Health.
State Medicaid agencies for months have been preparing for the end of the public health emergency. As part of a COVID relief law approved in March 2020, Congress prohibited states from dropping anyone from Medicaid coverage unless they moved out of state during the public health emergency. When the emergency ends, state Medicaid officials must reevaluate each enrollee’s eligibility. Millions of people could lose their coverage if they earn too much or fail to provide the information needed to verify income or residency.
As of November, about 86 million people were enrolled in Medicaid, according to the Centers for Medicare & Medicaid Services. That’s up from 71 million in February 2020, before COVID began to ravage the nation.
West Virginia has more than 600,000 Medicaid enrollees. Adler said about 100,000 of them could lose their eligibility at the end of the public health emergency because either the state has determined they’re ineligible or they’ve failed to respond to requests that they update their income information.
“It’s frustrating that texting is a means to meet people where they are and that this has not been picked up more by states,” said Jennifer Wagner, director of Medicaid eligibility and enrollment for the Center on Budget and Policy Priorities, a Washington-based research group.
The problem with relying on the Postal Service is that a letter can get hidden in “junk” mail or can fail to reach people who have moved or are homeless, Ms. Serafi said. And email, if people have an account, can end up in spam folders.
In contrast, surveys show lower-income Americans are just as likely to have smartphones and cellphones as the general population. And most people regularly use texting.
In Michigan, Medicaid officials started using text messaging to communicate with enrollees in 2020 after building a system with the help of federal COVID relief funding. They said texting is an economical way to reach enrollees.
“It costs us 2 cents per text message, which is incredibly cheap,” said Steph White, an enrollment coordinator for the Michigan Department of Health and Human Services. “It’s a great return on investment.”
CMS officials have told states they should consider texting, along with other communication methods, when trying to reach enrollees when the public health emergency ends. But many states don’t have the technology or information about enrollees to do it.
Efforts to add texting also face legal barriers, including a federal law that bars texting people without their consent. The Federal Communications Commission ruled in 2021 that state agencies are exempt from the law, but whether counties that handle Medicaid duties for some states and Medicaid managed-care organizations that work in more than 40 states are exempt as well is unclear, said Matt Salo, executive director of the National Association of Medicaid Directors.
CMS spokesperson Beth Lynk said the agency is trying to figure out how Medicaid agencies, counties, and health plans can text enrollees within the constraints of federal law.
Several states told KHN that Medicaid health plans will be helping connect with enrollees and that they expect the plans to use text messaging. But the requirement to get consent from enrollees before texting could limit that effort.
That’s the situation in Virginia, where only about 30,000 Medicaid enrollees – out of more than a million – have agreed to receive text messages directly from the state, said spokesperson Christina Nuckols.
In an effort to boost that number, the state plans to ask enrollees if they want to opt out of receiving text messages, rather than ask them to opt in, she said. This way enrollees would contact the state only if they don’t want to be texted. The state is reviewing its legal options to make that happen.
Meanwhile, Ms. Nuckols added, the state expects Medicaid health plans to contact enrollees about updating their contact information. Four of Virginia’s six Medicaid plans, which serve the bulk of the state’s enrollees, have permission to text about 316,000.
Craig Kennedy, CEO of Medicaid Health Plans of America, a trade group, said that most plans are using texting and that Medicaid officials will use multiple strategies to connect with enrollees. “I do not see this as a detriment, that states are not texting information about reenrollment,” he said. “I know we will be helping with that.”
California officials in March directed Medicaid health plans to use a variety of communication methods, including texting, to ensure that members can retain coverage if they remain eligible. The officials told health plans they could ask for consent through an initial text.
California officials say they also plan to ask enrollees for consent to be texted on the enrollment application, although federal approval for the change is not expected until the fall.
A few state Medicaid programs have experimented in recent years with pilot programs that included texting enrollees.
In 2019, Louisiana worked with the nonprofit group Code for America to send text messages that reminded people about renewing coverage and providing income information for verification. Compared with traditional communication methods, the texts led to a 67% increase in enrollees being renewed for coverage and a 56% increase in enrollees verifying their income in response to inquiries, said Medicaid spokesperson Alyson Neel.
Nonetheless, the state isn’t planning to text Medicaid enrollees about the end of the public health emergency because it hasn’t set up a system for that. “Medicaid has not yet been able to implement a text messaging system of its own due to other agency priorities,” Ms. Neel said.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Omega-3 fatty acids linked to less FOXA1 in benign breast tissue
in benign breast tissue, potentially pointing the way toward the use of the pioneer transcription factor as a helpful biomarker for breast cancer researchers.
The findings were released at the annual meeting of the American Association for Cancer Research.
In the study, researchers who were led by Bruce F. Kimler, PhD, a radiation biologist and breast cancer researcher at the University of Kansas Medical Center, Kansas City, examined benign breast tissue cells aspirated from 12 women (mean age, 53 years; 7 on low-dose hormone replacement) before and after 6 months of high-dose omega-3 fatty acid supplementation. After the supplementation, FOXA1 positive cells fell in 11 of 12 women (P = .019). “There was a robust linear relationship between stain positivity for FOXA1 and AGR2,” the researchers reported (P < .001).
Increased FOXA1 activity along with GRHL2) transcription factor can boost endocrine resistance, while omega-3 fatty acids can reduce it.
In an interview, Robert S. Chapkin, PhD, the Allen Endowed Chair in Nutrition and Chronic Disease Prevention at Texas A&M University, College Station, said it’s important to examine the value of omega-3 fatty acid supplementation, and the understanding of biomarkers is crucial. “Omega 3 fatty acids are pleiotropic, dose dependent, and likely impact multiple signaling mechanisms in select cells types and cancer contexts. The key is to dissect out the highest impact targets and pursue them in the context of preclinical and clinical studies.”
However, he said, “in many cases, the lack of a mechanistic understanding detracts from the merit of the work.”
Studies like this are useful in the development of clinical trials to test the value of high-dose omega-3 fatty acids in breast cancer prevention trials, said Carol Fabian, MD, a breast medical oncologist with the University of Kansas Medical Center, and the study’s first author.
“They help us understand both what dose will be needed and biomarkers that will likely be helpful in predicting response. Early-phase trials with biomarker modulation as a primary endpoint are generally necessary to make sure you have the right dose for the target population prior to committing to a long-term cancer incidence study involving thousands of women and tens of millions of dollars,” she said.
What’s next? “This work was done on reserved specimens from a prior pilot trial,” Dr. Fabian said. “We need a placebo-controlled study to know for sure that omega-3 FA in a dose of about 3.2g daily, or about 2% of calories, modulates FOXA1 and/or AGR2 in postmenopausal women.”
Previously, she said, the researchers “found that high dose omega-3 administered to overweight peri- and postmenopausal high-risk women undergoing a 6-month weight loss intervention increased the number of systemic risk biomarkers which were favorably modulated compared to placebo despite the same median weight loss in each group [–10%],” Dr. Fabian said. “We want to duplicate that finding in a larger study as well as determine if omega-3 fatty acids can block tamoxifen-induced increases in AGR2 associated with endocrine resistance.”
The study was funded by the Breast Cancer Research Foundation, the Morris Family Foundation, and the University of Kansas Cancer Center. The authors and Chapkin report no relevant disclosures.
in benign breast tissue, potentially pointing the way toward the use of the pioneer transcription factor as a helpful biomarker for breast cancer researchers.
The findings were released at the annual meeting of the American Association for Cancer Research.
In the study, researchers who were led by Bruce F. Kimler, PhD, a radiation biologist and breast cancer researcher at the University of Kansas Medical Center, Kansas City, examined benign breast tissue cells aspirated from 12 women (mean age, 53 years; 7 on low-dose hormone replacement) before and after 6 months of high-dose omega-3 fatty acid supplementation. After the supplementation, FOXA1 positive cells fell in 11 of 12 women (P = .019). “There was a robust linear relationship between stain positivity for FOXA1 and AGR2,” the researchers reported (P < .001).
Increased FOXA1 activity along with GRHL2) transcription factor can boost endocrine resistance, while omega-3 fatty acids can reduce it.
In an interview, Robert S. Chapkin, PhD, the Allen Endowed Chair in Nutrition and Chronic Disease Prevention at Texas A&M University, College Station, said it’s important to examine the value of omega-3 fatty acid supplementation, and the understanding of biomarkers is crucial. “Omega 3 fatty acids are pleiotropic, dose dependent, and likely impact multiple signaling mechanisms in select cells types and cancer contexts. The key is to dissect out the highest impact targets and pursue them in the context of preclinical and clinical studies.”
However, he said, “in many cases, the lack of a mechanistic understanding detracts from the merit of the work.”
Studies like this are useful in the development of clinical trials to test the value of high-dose omega-3 fatty acids in breast cancer prevention trials, said Carol Fabian, MD, a breast medical oncologist with the University of Kansas Medical Center, and the study’s first author.
“They help us understand both what dose will be needed and biomarkers that will likely be helpful in predicting response. Early-phase trials with biomarker modulation as a primary endpoint are generally necessary to make sure you have the right dose for the target population prior to committing to a long-term cancer incidence study involving thousands of women and tens of millions of dollars,” she said.
What’s next? “This work was done on reserved specimens from a prior pilot trial,” Dr. Fabian said. “We need a placebo-controlled study to know for sure that omega-3 FA in a dose of about 3.2g daily, or about 2% of calories, modulates FOXA1 and/or AGR2 in postmenopausal women.”
Previously, she said, the researchers “found that high dose omega-3 administered to overweight peri- and postmenopausal high-risk women undergoing a 6-month weight loss intervention increased the number of systemic risk biomarkers which were favorably modulated compared to placebo despite the same median weight loss in each group [–10%],” Dr. Fabian said. “We want to duplicate that finding in a larger study as well as determine if omega-3 fatty acids can block tamoxifen-induced increases in AGR2 associated with endocrine resistance.”
The study was funded by the Breast Cancer Research Foundation, the Morris Family Foundation, and the University of Kansas Cancer Center. The authors and Chapkin report no relevant disclosures.
in benign breast tissue, potentially pointing the way toward the use of the pioneer transcription factor as a helpful biomarker for breast cancer researchers.
The findings were released at the annual meeting of the American Association for Cancer Research.
In the study, researchers who were led by Bruce F. Kimler, PhD, a radiation biologist and breast cancer researcher at the University of Kansas Medical Center, Kansas City, examined benign breast tissue cells aspirated from 12 women (mean age, 53 years; 7 on low-dose hormone replacement) before and after 6 months of high-dose omega-3 fatty acid supplementation. After the supplementation, FOXA1 positive cells fell in 11 of 12 women (P = .019). “There was a robust linear relationship between stain positivity for FOXA1 and AGR2,” the researchers reported (P < .001).
Increased FOXA1 activity along with GRHL2) transcription factor can boost endocrine resistance, while omega-3 fatty acids can reduce it.
In an interview, Robert S. Chapkin, PhD, the Allen Endowed Chair in Nutrition and Chronic Disease Prevention at Texas A&M University, College Station, said it’s important to examine the value of omega-3 fatty acid supplementation, and the understanding of biomarkers is crucial. “Omega 3 fatty acids are pleiotropic, dose dependent, and likely impact multiple signaling mechanisms in select cells types and cancer contexts. The key is to dissect out the highest impact targets and pursue them in the context of preclinical and clinical studies.”
However, he said, “in many cases, the lack of a mechanistic understanding detracts from the merit of the work.”
Studies like this are useful in the development of clinical trials to test the value of high-dose omega-3 fatty acids in breast cancer prevention trials, said Carol Fabian, MD, a breast medical oncologist with the University of Kansas Medical Center, and the study’s first author.
“They help us understand both what dose will be needed and biomarkers that will likely be helpful in predicting response. Early-phase trials with biomarker modulation as a primary endpoint are generally necessary to make sure you have the right dose for the target population prior to committing to a long-term cancer incidence study involving thousands of women and tens of millions of dollars,” she said.
What’s next? “This work was done on reserved specimens from a prior pilot trial,” Dr. Fabian said. “We need a placebo-controlled study to know for sure that omega-3 FA in a dose of about 3.2g daily, or about 2% of calories, modulates FOXA1 and/or AGR2 in postmenopausal women.”
Previously, she said, the researchers “found that high dose omega-3 administered to overweight peri- and postmenopausal high-risk women undergoing a 6-month weight loss intervention increased the number of systemic risk biomarkers which were favorably modulated compared to placebo despite the same median weight loss in each group [–10%],” Dr. Fabian said. “We want to duplicate that finding in a larger study as well as determine if omega-3 fatty acids can block tamoxifen-induced increases in AGR2 associated with endocrine resistance.”
The study was funded by the Breast Cancer Research Foundation, the Morris Family Foundation, and the University of Kansas Cancer Center. The authors and Chapkin report no relevant disclosures.
FROM AACR 2022