User login
The importance of character
Early autumn is typically a quiet time for outpatient pediatricians. The school physicals are finished. The last-minute school physicals are finished. The “I forgot to get my child’s physical” physicals are finished. Respiratory syncytial virus and influenza seasons haven’t started. There is time for some self-reflection and sharpening the saw.

My reflective period each year tends to start with the unresolved “What do I want to be when I grow up?” Mind you, just because I’ve grown old doesn’t mean I’ve grown up. I never wanted to be a “grande personne” who, per Antoine de Saint-Exupéry in “Le Petit Prince,” will never understand why a minor item (Did the lamb eat the flower?) makes all the difference in the universe to a child. Awe and wonderment should remain a part of life. I enjoy reading that short story in the original French because, as my high school French vocabulary and conjugation have faded, any word I don’t recognize means exactly what my journey of a lifetime tells me it means, neither more nor less, just as Humpty Dumpty explained to Alice in Lewis Carroll’s “Through the Looking Glass.”
Along with my perennial favorites like “Le Petit Prince” and the Gettysburg Address, in this year’s folder for reflection are two essays I’ve collected this year. The first is a letter addressed from medical ethicist Ira Bedzow, PhD, to this year’s incoming class of medical students.
The essay gives advice to first-year medical students entering the profession of medicine. It talks about finding “something to say that you communicate with the whole and essence of your being.” There is lots of great counsel in the letter. It claims, “Only in a professional does one’s voice sing in harmony with one’s being. Want that for yourselves, for only a life undivided is a life of full integrity.”
I agree with the harmony part. I hesitate with the undivided part. A professional singer could be dedicated to opera but still sing in a barbershop quartet and a church choir, motivated by fun and fellowship. It is important to emphasize integrity and dedication to medical students. The letter does that well, but students must also develop a work-life balance. The ascetic life is not for everyone.
Life needs balance and moderation. I am pretty sure that Aristotle said that, but I never did spend much time studying the Classics. I use my periods of self-reflection to chart my life’s vector. I choose new skills to learn and challenges to meet. But as I grow older, I spend more time pruning those roles that no longer give me joy. Delayed gratification is an important character trait for success, but its value lessens as it becomes clear there are more days behind me than ahead.
The second essay reflects the views of Canon Brodar, a third-year medical student and divinity school graduate.
He attests to the willingness of medical trainees to accept their duties and personal risk during the crisis of the COVID-19 pandemic. He correctly points out the contributions his fellow students could make, but underestimates the negatives. During March 2020 when decisions were made to send third-year medical students home, the administrative focus was on the cost of their participation (consumption of scarce personal protective equipment) and the potential negative consequences (an additional person who might transmit the virus among patients.) Four months later, most medical students were back on the job.
Mr. Brodar’s eloquent description of duty and responsibility complement, and perhaps have evolved from, the integrity and dedication that Dr. Bedzow emphasized to incoming medical students. These are all character traits. These traits are not knowledge of anatomy or skill with a scalpel. With experience come two more key character traits – the moderation of a work-life balance and the judgment to weigh benefits, risks, and costs.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. He has no relevant financial disclosures. Email him at pdnews@mdedge.com.
Early autumn is typically a quiet time for outpatient pediatricians. The school physicals are finished. The last-minute school physicals are finished. The “I forgot to get my child’s physical” physicals are finished. Respiratory syncytial virus and influenza seasons haven’t started. There is time for some self-reflection and sharpening the saw.
My reflective period each year tends to start with the unresolved “What do I want to be when I grow up?” Mind you, just because I’ve grown old doesn’t mean I’ve grown up. I never wanted to be a “grande personne” who, per Antoine de Saint-Exupéry in “Le Petit Prince,” will never understand why a minor item (Did the lamb eat the flower?) makes all the difference in the universe to a child. Awe and wonderment should remain a part of life. I enjoy reading that short story in the original French because, as my high school French vocabulary and conjugation have faded, any word I don’t recognize means exactly what my journey of a lifetime tells me it means, neither more nor less, just as Humpty Dumpty explained to Alice in Lewis Carroll’s “Through the Looking Glass.”
Along with my perennial favorites like “Le Petit Prince” and the Gettysburg Address, in this year’s folder for reflection are two essays I’ve collected this year. The first is a letter addressed from medical ethicist Ira Bedzow, PhD, to this year’s incoming class of medical students.
The essay gives advice to first-year medical students entering the profession of medicine. It talks about finding “something to say that you communicate with the whole and essence of your being.” There is lots of great counsel in the letter. It claims, “Only in a professional does one’s voice sing in harmony with one’s being. Want that for yourselves, for only a life undivided is a life of full integrity.”
I agree with the harmony part. I hesitate with the undivided part. A professional singer could be dedicated to opera but still sing in a barbershop quartet and a church choir, motivated by fun and fellowship. It is important to emphasize integrity and dedication to medical students. The letter does that well, but students must also develop a work-life balance. The ascetic life is not for everyone.
Life needs balance and moderation. I am pretty sure that Aristotle said that, but I never did spend much time studying the Classics. I use my periods of self-reflection to chart my life’s vector. I choose new skills to learn and challenges to meet. But as I grow older, I spend more time pruning those roles that no longer give me joy. Delayed gratification is an important character trait for success, but its value lessens as it becomes clear there are more days behind me than ahead.
The second essay reflects the views of Canon Brodar, a third-year medical student and divinity school graduate.
He attests to the willingness of medical trainees to accept their duties and personal risk during the crisis of the COVID-19 pandemic. He correctly points out the contributions his fellow students could make, but underestimates the negatives. During March 2020 when decisions were made to send third-year medical students home, the administrative focus was on the cost of their participation (consumption of scarce personal protective equipment) and the potential negative consequences (an additional person who might transmit the virus among patients.) Four months later, most medical students were back on the job.
Mr. Brodar’s eloquent description of duty and responsibility complement, and perhaps have evolved from, the integrity and dedication that Dr. Bedzow emphasized to incoming medical students. These are all character traits. These traits are not knowledge of anatomy or skill with a scalpel. With experience come two more key character traits – the moderation of a work-life balance and the judgment to weigh benefits, risks, and costs.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. He has no relevant financial disclosures. Email him at pdnews@mdedge.com.
Early autumn is typically a quiet time for outpatient pediatricians. The school physicals are finished. The last-minute school physicals are finished. The “I forgot to get my child’s physical” physicals are finished. Respiratory syncytial virus and influenza seasons haven’t started. There is time for some self-reflection and sharpening the saw.
My reflective period each year tends to start with the unresolved “What do I want to be when I grow up?” Mind you, just because I’ve grown old doesn’t mean I’ve grown up. I never wanted to be a “grande personne” who, per Antoine de Saint-Exupéry in “Le Petit Prince,” will never understand why a minor item (Did the lamb eat the flower?) makes all the difference in the universe to a child. Awe and wonderment should remain a part of life. I enjoy reading that short story in the original French because, as my high school French vocabulary and conjugation have faded, any word I don’t recognize means exactly what my journey of a lifetime tells me it means, neither more nor less, just as Humpty Dumpty explained to Alice in Lewis Carroll’s “Through the Looking Glass.”
Along with my perennial favorites like “Le Petit Prince” and the Gettysburg Address, in this year’s folder for reflection are two essays I’ve collected this year. The first is a letter addressed from medical ethicist Ira Bedzow, PhD, to this year’s incoming class of medical students.
The essay gives advice to first-year medical students entering the profession of medicine. It talks about finding “something to say that you communicate with the whole and essence of your being.” There is lots of great counsel in the letter. It claims, “Only in a professional does one’s voice sing in harmony with one’s being. Want that for yourselves, for only a life undivided is a life of full integrity.”
I agree with the harmony part. I hesitate with the undivided part. A professional singer could be dedicated to opera but still sing in a barbershop quartet and a church choir, motivated by fun and fellowship. It is important to emphasize integrity and dedication to medical students. The letter does that well, but students must also develop a work-life balance. The ascetic life is not for everyone.
Life needs balance and moderation. I am pretty sure that Aristotle said that, but I never did spend much time studying the Classics. I use my periods of self-reflection to chart my life’s vector. I choose new skills to learn and challenges to meet. But as I grow older, I spend more time pruning those roles that no longer give me joy. Delayed gratification is an important character trait for success, but its value lessens as it becomes clear there are more days behind me than ahead.
The second essay reflects the views of Canon Brodar, a third-year medical student and divinity school graduate.
He attests to the willingness of medical trainees to accept their duties and personal risk during the crisis of the COVID-19 pandemic. He correctly points out the contributions his fellow students could make, but underestimates the negatives. During March 2020 when decisions were made to send third-year medical students home, the administrative focus was on the cost of their participation (consumption of scarce personal protective equipment) and the potential negative consequences (an additional person who might transmit the virus among patients.) Four months later, most medical students were back on the job.
Mr. Brodar’s eloquent description of duty and responsibility complement, and perhaps have evolved from, the integrity and dedication that Dr. Bedzow emphasized to incoming medical students. These are all character traits. These traits are not knowledge of anatomy or skill with a scalpel. With experience come two more key character traits – the moderation of a work-life balance and the judgment to weigh benefits, risks, and costs.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. He has no relevant financial disclosures. Email him at pdnews@mdedge.com.
Virtual school is especially difficult for children with ADHD
The school year has begun, but for most families it is a school year without precedent. Parents have to monitor and support their children through school days that are partially or completely virtual, juggling sudden class transitions, troubleshooting technology, and trying to manage lessons and assignments. Most related activities such as sports and orchestra are cancelled. Parents themselves are anxious about completing their work, if they have jobs at all. On top of this, all of us have faced months of challenge and disruption with virtually no relief, with regard to seeing friends, traveling, or going out to dinner or a movie. For your patients with ADHD, the challenges of this school year will be even more difficult. Offering parents some guidance about how to approach and manage these challenges can support their adaptation and lessen the chances of compounded problems by the time in-person school resumes.

Children with ADHD, particularly those in elementary school, are managing symptoms of difficulty shifting their attention, sustaining focus on less-engaging material, and motor hyperactivity. They often have difficulty with organization and planning, working memory, and impulse control. Even with effective medication management, they typically are dependent on external cues and support to manage the demands of school. They benefit from attentive teachers who can redirect their attention, offer serial prompts before transitions, and provide patient support, reassurance, and confidence when they grow frustrated. And it often is easier for teachers to do this than for parents, as they have years of experience and training, and the support of their professionals in the school setting. And of course they are less likely to personalize these challenges than are parents, who are likely to feel worried, guilty, or discouraged by the child’s persistent difficulties with attention. Parents who are stressed or who may be managing difficulties with attention themselves – as ADHD is one of the more heritable psychiatric disorders – will be vulnerable to feeling frustration and losing their temper.
Suggest to the parents of your patients with ADHD that there will be frustrations and challenges as they manage the learning curve of virtual school with their children. Increasing the dose of an effective stimulant may be tempting, but there are a few strategies that may better help the children adapt to a virtual classroom without too much distress.
Promote good sleep patterns
Adequate, restful sleep is critical to our physical and psychological health and to healthy development. Children with ADHD are prone to sleep difficulties, and stimulants may exacerbate these.

So, it is critical that parents prioritize setting and maintaining healthy routines around sleep. All screens should power down at least 1 hour before lights out, and parents can help their children know when to accept “good enough” homework, so they also may get good enough sleep.
Daily physical activity helps enormously with restful sleep. A warm bath or shower and quiet reading (not homework!) can help wired kids unwind and be truly ready for lights out. Bedtime may start to slide later as life’s routines are disrupted with work and school happening at home, but it is important to maintain a consistent bedtime that will allow for 8-10 hours of sleep.
Create routines around the “school day”
Good schools involve a predictable rhythm and a lot of caring adults engaging with children. They have very consistent routines at the start of each day, and families can create their own to offer structure and cues to their children.
Start the day with a consistent wake up time and routine plus a healthy breakfast. Take advantage of the extra time that no commute to school or bus ride allow, whether by supporting more sleep, cooking a hot breakfast together, or by letting the children engage in a beloved activity, such as listening to music, reading a comic book, or working on a craft before the computer goes on.
The routine should be centered on the rhythm of the school, and realistic for parents. It matters most that it is consistent, incorporates nutritious food and exercise, and is pleasant and even fun.
Set the stage
Teachers will often put their students with ADHD in the front of the class, so they can offer prompts and so the students are less distracted by peers. Consider where in the home is a good spot for the children, one that minimizes distractions and where a parent is near enough to support and monitor them.
Parents might want to avoid rooms with a lot of toys or games that may tempt children, and children will need to be apart from (noisy) siblings. If they forget to mute themselves or are tempted to open another window on their computer, it is helpful for a parent to be near enough to be unobtrusively following along. Parents will hear the sounds of trouble and be able to help if their children get lost in an assignment or are otherwise off-track.
Create reasonable expectations and positive rewards
Reassure parents that this adjustment is going to be hard for all children and families. Now is not the season for perfectionism or focusing too intensely on mastering a challenging subject.
Reasonable goals for the first month might be for the child to get some enjoyment from school and to get better at specific tasks (being on time, managing the technology, asking for help when needed).
Parents may even set this goal with their children: “What do you want to be better at by the end of the first month?” If children with ADHD improve at managing the distractions of a virtual class, they will have accomplished a great deal cognitively. It will be hard work for them.
So parents should think about what reward can come at the end of each school day, whether a walk outside together, a game of Uno, or even an afterschool treat together, so children get a sense of success for even incremental adaptation.
Build in breaks from the screen
Spending much more than an hour in a virtual interaction is taxing even for adult attention spans. Parents should feel empowered to speak with their children’s teachers to find ways to build in regular 10- to 15-minute breaks during which their children can have a snack, take a bathroom break, or get their wiggles out.
Ensure there is some physical activity
Recess is usually the most important class of the day in elementary school, and especially for children with ADHD. If parents can make physical activity part of their children’s routines, breaks, and afterschool rewards, their attention, energy, and sleep will be improved.

They might do a workout with the child for 20 minutes before school starts, go for a short walk, or do jumping jacks during breaks. And getting outside to kick a ball, go for a swim, or otherwise get the heart rate up in the sunshine will be the most important thing parents do for their children after protecting their sleep.
Know your child
Remember parents are the experts on their children. School is the setting in which children are both cultivating their strengths and facing challenges. Ask the parents what has been most challenging for their children about school and what was most cherished about it.

Parents should get creative to cultivate their children’s strengths. If a child adores art, it will be so important to try to provide that experience during this school year. There might be other virtual resources (virtual museum tours, YouTube art lessons), a local teacher who can offer socially distant lessons, or even another student who might be able to safely share a teacher – getting a creative and social outlet together.
Are there special teachers that the children are missing? Maybe there is a way to send them emails or have some virtual time with them each week.
If a child struggles with the classroom but excells on the soccer pitch, it will be critical to find a physically distant way for the child to develop that strength, whether with a small, informal practice or a new physical undertaking.

Likewise, parents may need to look elsewhere to help their children manage important challenges. Whether a child is learning how to face anxiety or improve social skills, virtual school might seem like a relief as it takes the pressure off. Help parents consider alternate ways that their children could continue to work on these developmental projects while school is virtual, so they don’t lose ground developmentally.
If parents can set reasonable goals, be patient, and focus on the daily routines, and consider the child’s individual developmental strengths and challenges, they may be better able to manage this challenging year. They may even find improved connection, patience, and perspective for both themselves and their children.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Neither Dr. Swick nor Dr. Jellinek had any relevant financial disclosures. Email them at pdnews@mdedge.com.
The school year has begun, but for most families it is a school year without precedent. Parents have to monitor and support their children through school days that are partially or completely virtual, juggling sudden class transitions, troubleshooting technology, and trying to manage lessons and assignments. Most related activities such as sports and orchestra are cancelled. Parents themselves are anxious about completing their work, if they have jobs at all. On top of this, all of us have faced months of challenge and disruption with virtually no relief, with regard to seeing friends, traveling, or going out to dinner or a movie. For your patients with ADHD, the challenges of this school year will be even more difficult. Offering parents some guidance about how to approach and manage these challenges can support their adaptation and lessen the chances of compounded problems by the time in-person school resumes.
Children with ADHD, particularly those in elementary school, are managing symptoms of difficulty shifting their attention, sustaining focus on less-engaging material, and motor hyperactivity. They often have difficulty with organization and planning, working memory, and impulse control. Even with effective medication management, they typically are dependent on external cues and support to manage the demands of school. They benefit from attentive teachers who can redirect their attention, offer serial prompts before transitions, and provide patient support, reassurance, and confidence when they grow frustrated. And it often is easier for teachers to do this than for parents, as they have years of experience and training, and the support of their professionals in the school setting. And of course they are less likely to personalize these challenges than are parents, who are likely to feel worried, guilty, or discouraged by the child’s persistent difficulties with attention. Parents who are stressed or who may be managing difficulties with attention themselves – as ADHD is one of the more heritable psychiatric disorders – will be vulnerable to feeling frustration and losing their temper.
Suggest to the parents of your patients with ADHD that there will be frustrations and challenges as they manage the learning curve of virtual school with their children. Increasing the dose of an effective stimulant may be tempting, but there are a few strategies that may better help the children adapt to a virtual classroom without too much distress.
Promote good sleep patterns
Adequate, restful sleep is critical to our physical and psychological health and to healthy development. Children with ADHD are prone to sleep difficulties, and stimulants may exacerbate these.
So, it is critical that parents prioritize setting and maintaining healthy routines around sleep. All screens should power down at least 1 hour before lights out, and parents can help their children know when to accept “good enough” homework, so they also may get good enough sleep.
Daily physical activity helps enormously with restful sleep. A warm bath or shower and quiet reading (not homework!) can help wired kids unwind and be truly ready for lights out. Bedtime may start to slide later as life’s routines are disrupted with work and school happening at home, but it is important to maintain a consistent bedtime that will allow for 8-10 hours of sleep.
Create routines around the “school day”
Good schools involve a predictable rhythm and a lot of caring adults engaging with children. They have very consistent routines at the start of each day, and families can create their own to offer structure and cues to their children.
Start the day with a consistent wake up time and routine plus a healthy breakfast. Take advantage of the extra time that no commute to school or bus ride allow, whether by supporting more sleep, cooking a hot breakfast together, or by letting the children engage in a beloved activity, such as listening to music, reading a comic book, or working on a craft before the computer goes on.
The routine should be centered on the rhythm of the school, and realistic for parents. It matters most that it is consistent, incorporates nutritious food and exercise, and is pleasant and even fun.
Set the stage
Teachers will often put their students with ADHD in the front of the class, so they can offer prompts and so the students are less distracted by peers. Consider where in the home is a good spot for the children, one that minimizes distractions and where a parent is near enough to support and monitor them.
Parents might want to avoid rooms with a lot of toys or games that may tempt children, and children will need to be apart from (noisy) siblings. If they forget to mute themselves or are tempted to open another window on their computer, it is helpful for a parent to be near enough to be unobtrusively following along. Parents will hear the sounds of trouble and be able to help if their children get lost in an assignment or are otherwise off-track.
Create reasonable expectations and positive rewards
Reassure parents that this adjustment is going to be hard for all children and families. Now is not the season for perfectionism or focusing too intensely on mastering a challenging subject.
Reasonable goals for the first month might be for the child to get some enjoyment from school and to get better at specific tasks (being on time, managing the technology, asking for help when needed).
Parents may even set this goal with their children: “What do you want to be better at by the end of the first month?” If children with ADHD improve at managing the distractions of a virtual class, they will have accomplished a great deal cognitively. It will be hard work for them.
So parents should think about what reward can come at the end of each school day, whether a walk outside together, a game of Uno, or even an afterschool treat together, so children get a sense of success for even incremental adaptation.
Build in breaks from the screen
Spending much more than an hour in a virtual interaction is taxing even for adult attention spans. Parents should feel empowered to speak with their children’s teachers to find ways to build in regular 10- to 15-minute breaks during which their children can have a snack, take a bathroom break, or get their wiggles out.
Ensure there is some physical activity
Recess is usually the most important class of the day in elementary school, and especially for children with ADHD. If parents can make physical activity part of their children’s routines, breaks, and afterschool rewards, their attention, energy, and sleep will be improved.
They might do a workout with the child for 20 minutes before school starts, go for a short walk, or do jumping jacks during breaks. And getting outside to kick a ball, go for a swim, or otherwise get the heart rate up in the sunshine will be the most important thing parents do for their children after protecting their sleep.
Know your child
Remember parents are the experts on their children. School is the setting in which children are both cultivating their strengths and facing challenges. Ask the parents what has been most challenging for their children about school and what was most cherished about it.
Parents should get creative to cultivate their children’s strengths. If a child adores art, it will be so important to try to provide that experience during this school year. There might be other virtual resources (virtual museum tours, YouTube art lessons), a local teacher who can offer socially distant lessons, or even another student who might be able to safely share a teacher – getting a creative and social outlet together.
Are there special teachers that the children are missing? Maybe there is a way to send them emails or have some virtual time with them each week.
If a child struggles with the classroom but excells on the soccer pitch, it will be critical to find a physically distant way for the child to develop that strength, whether with a small, informal practice or a new physical undertaking.
Likewise, parents may need to look elsewhere to help their children manage important challenges. Whether a child is learning how to face anxiety or improve social skills, virtual school might seem like a relief as it takes the pressure off. Help parents consider alternate ways that their children could continue to work on these developmental projects while school is virtual, so they don’t lose ground developmentally.
If parents can set reasonable goals, be patient, and focus on the daily routines, and consider the child’s individual developmental strengths and challenges, they may be better able to manage this challenging year. They may even find improved connection, patience, and perspective for both themselves and their children.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Neither Dr. Swick nor Dr. Jellinek had any relevant financial disclosures. Email them at pdnews@mdedge.com.
The school year has begun, but for most families it is a school year without precedent. Parents have to monitor and support their children through school days that are partially or completely virtual, juggling sudden class transitions, troubleshooting technology, and trying to manage lessons and assignments. Most related activities such as sports and orchestra are cancelled. Parents themselves are anxious about completing their work, if they have jobs at all. On top of this, all of us have faced months of challenge and disruption with virtually no relief, with regard to seeing friends, traveling, or going out to dinner or a movie. For your patients with ADHD, the challenges of this school year will be even more difficult. Offering parents some guidance about how to approach and manage these challenges can support their adaptation and lessen the chances of compounded problems by the time in-person school resumes.
Children with ADHD, particularly those in elementary school, are managing symptoms of difficulty shifting their attention, sustaining focus on less-engaging material, and motor hyperactivity. They often have difficulty with organization and planning, working memory, and impulse control. Even with effective medication management, they typically are dependent on external cues and support to manage the demands of school. They benefit from attentive teachers who can redirect their attention, offer serial prompts before transitions, and provide patient support, reassurance, and confidence when they grow frustrated. And it often is easier for teachers to do this than for parents, as they have years of experience and training, and the support of their professionals in the school setting. And of course they are less likely to personalize these challenges than are parents, who are likely to feel worried, guilty, or discouraged by the child’s persistent difficulties with attention. Parents who are stressed or who may be managing difficulties with attention themselves – as ADHD is one of the more heritable psychiatric disorders – will be vulnerable to feeling frustration and losing their temper.
Suggest to the parents of your patients with ADHD that there will be frustrations and challenges as they manage the learning curve of virtual school with their children. Increasing the dose of an effective stimulant may be tempting, but there are a few strategies that may better help the children adapt to a virtual classroom without too much distress.
Promote good sleep patterns
Adequate, restful sleep is critical to our physical and psychological health and to healthy development. Children with ADHD are prone to sleep difficulties, and stimulants may exacerbate these.
So, it is critical that parents prioritize setting and maintaining healthy routines around sleep. All screens should power down at least 1 hour before lights out, and parents can help their children know when to accept “good enough” homework, so they also may get good enough sleep.
Daily physical activity helps enormously with restful sleep. A warm bath or shower and quiet reading (not homework!) can help wired kids unwind and be truly ready for lights out. Bedtime may start to slide later as life’s routines are disrupted with work and school happening at home, but it is important to maintain a consistent bedtime that will allow for 8-10 hours of sleep.
Create routines around the “school day”
Good schools involve a predictable rhythm and a lot of caring adults engaging with children. They have very consistent routines at the start of each day, and families can create their own to offer structure and cues to their children.
Start the day with a consistent wake up time and routine plus a healthy breakfast. Take advantage of the extra time that no commute to school or bus ride allow, whether by supporting more sleep, cooking a hot breakfast together, or by letting the children engage in a beloved activity, such as listening to music, reading a comic book, or working on a craft before the computer goes on.
The routine should be centered on the rhythm of the school, and realistic for parents. It matters most that it is consistent, incorporates nutritious food and exercise, and is pleasant and even fun.
Set the stage
Teachers will often put their students with ADHD in the front of the class, so they can offer prompts and so the students are less distracted by peers. Consider where in the home is a good spot for the children, one that minimizes distractions and where a parent is near enough to support and monitor them.
Parents might want to avoid rooms with a lot of toys or games that may tempt children, and children will need to be apart from (noisy) siblings. If they forget to mute themselves or are tempted to open another window on their computer, it is helpful for a parent to be near enough to be unobtrusively following along. Parents will hear the sounds of trouble and be able to help if their children get lost in an assignment or are otherwise off-track.
Create reasonable expectations and positive rewards
Reassure parents that this adjustment is going to be hard for all children and families. Now is not the season for perfectionism or focusing too intensely on mastering a challenging subject.
Reasonable goals for the first month might be for the child to get some enjoyment from school and to get better at specific tasks (being on time, managing the technology, asking for help when needed).
Parents may even set this goal with their children: “What do you want to be better at by the end of the first month?” If children with ADHD improve at managing the distractions of a virtual class, they will have accomplished a great deal cognitively. It will be hard work for them.
So parents should think about what reward can come at the end of each school day, whether a walk outside together, a game of Uno, or even an afterschool treat together, so children get a sense of success for even incremental adaptation.
Build in breaks from the screen
Spending much more than an hour in a virtual interaction is taxing even for adult attention spans. Parents should feel empowered to speak with their children’s teachers to find ways to build in regular 10- to 15-minute breaks during which their children can have a snack, take a bathroom break, or get their wiggles out.
Ensure there is some physical activity
Recess is usually the most important class of the day in elementary school, and especially for children with ADHD. If parents can make physical activity part of their children’s routines, breaks, and afterschool rewards, their attention, energy, and sleep will be improved.
They might do a workout with the child for 20 minutes before school starts, go for a short walk, or do jumping jacks during breaks. And getting outside to kick a ball, go for a swim, or otherwise get the heart rate up in the sunshine will be the most important thing parents do for their children after protecting their sleep.
Know your child
Remember parents are the experts on their children. School is the setting in which children are both cultivating their strengths and facing challenges. Ask the parents what has been most challenging for their children about school and what was most cherished about it.
Parents should get creative to cultivate their children’s strengths. If a child adores art, it will be so important to try to provide that experience during this school year. There might be other virtual resources (virtual museum tours, YouTube art lessons), a local teacher who can offer socially distant lessons, or even another student who might be able to safely share a teacher – getting a creative and social outlet together.
Are there special teachers that the children are missing? Maybe there is a way to send them emails or have some virtual time with them each week.
If a child struggles with the classroom but excells on the soccer pitch, it will be critical to find a physically distant way for the child to develop that strength, whether with a small, informal practice or a new physical undertaking.
Likewise, parents may need to look elsewhere to help their children manage important challenges. Whether a child is learning how to face anxiety or improve social skills, virtual school might seem like a relief as it takes the pressure off. Help parents consider alternate ways that their children could continue to work on these developmental projects while school is virtual, so they don’t lose ground developmentally.
If parents can set reasonable goals, be patient, and focus on the daily routines, and consider the child’s individual developmental strengths and challenges, they may be better able to manage this challenging year. They may even find improved connection, patience, and perspective for both themselves and their children.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Neither Dr. Swick nor Dr. Jellinek had any relevant financial disclosures. Email them at pdnews@mdedge.com.
Getting the most out of a psychiatric consultation
You’ve been struggling with what to do for a patient who has a significant mental health problem and really would love to have some help. You’re willing to fill out the requisite referral forms and wait your turn for what seems like an excruciating amount of time. But how do you ensure that you, your patient, and the family get the most out of the consultative experience so that everyone’s questions are answered and ongoing care, if needed, can continue?

To be fair, most of the burden of doing a good psychiatric or mental health consultation rests on the consultant, not the person making the request. It is their job to do a thorough evaluation and to identify any additional pieces of information that may be missing before a strong conclusion can be made. That said, however, this is the real world where everyone is busy and few have the time to track down every loose end that may exist regarding a patient’s history.
To that end, here are some recommendations for how to increase the chance that the outcome of your consultation with a child psychiatrist or other mental health professional will be maximally helpful for everyone involved. These tips are based on having been on the receiving end of psychiatric consultations for almost 2 decades and having worked closely with primary care clinicians in a number of different capacities.
The first question to ask yourself, and this may be the most important one of all, is whether or not you really need an actual psychiatrist at all at this stage versus another type of mental health professional. Physicians often are most comfortable dealing with other physicians. If a pediatrician has a question about a patient’s heart, it’s logical to consult a cardiologist. Thus if there’s a question about mental health, the knee-jerk reaction is to consult a psychiatrist. While understandable, looking first to a psychiatrist to help with a patient’s mental health struggles often is not the best move. Psychiatrists make up only one small part of all mental health professionals that also include psychologists, counselors, and clinical social workers, among others. The availability of child and adolescent psychiatrists can been exceedingly sparse while other types of mental health professionals generally are much more available. Moreover, these other types of mental health professionals also can do a great job at assessment and treatment. It is true that most can’t prescribe medication, but best practice recommendations for most of the common mental health diagnoses in youth (anxiety, depression, obsessive compulsive disorder, etc.) explicitly outline that nonpharmacologic treatments should be used first. It breaks my heart every time I do a consult for a family who has waited 6 months only to have me recommend a good therapist they could have seen right off in a week.
Get to know the mental health resources of your community beyond the small number of psychiatrists who might be there. And if you aren’t sure whether or not a referral might best go first to a mental health professional who is not a psychiatrist, just ask. That quick phone call or email might save the family a needless delay in treatment and a lot of aggravation for you.
If you are confident that it is a child & adolescent psychiatrist you want your patient to see, here are some things that will help you get the most out of that consultation and help you avoid the disappointment (for both you and the family) of an evaluation that completely misses the mark.
Select the best site (if you have an option)
Broadly speaking, psychiatrists often can be found in three main areas: academic clinics, private practice, and community mental health centers. While of course there is huge variation of clinicians at each of the sites, some generalizations regarding typical advantages and disadvantages of each setting are probably fair.

Academic settings often have psychiatrists who are local or even national experts on particular topics and can be good places to get evaluations for patients with complicated histories. At the same time, however, these settings typically rely on trainees to do much of the actual work. Many of the residents and fellows are excellent, but they turn over quickly because of graduation and finishing rotations, which can force patients to get to know a lot of different people. Academic centers also can be quite a distance from a family’s home, which often makes follow-up care a challenge (especially when we go back to more in-person visits).
Private practice psychiatrists can provide a more local option and can give families access to experienced clinicians, but many of these practices (especially the ones that take insurance) have practice models that involve seeing a lot of patients for short amounts of time and with less coordination with other types of services.
Finally, psychiatrists working at community mental health centers often work in teams that can help families get access to a lot of useful ancillary services (case management, home supports, etc.) but are part of a public mental health system that sadly is all too often overstretched and underfunded.
If you have choices for where to go for psychiatric services, keeping these things in mind can help you find the best fit for families.
Provide a medication history
While I’m not a big fan of the “what medicine do I try next?” consultation, don’t rely on families to provide this information accurately. Medications are confusing, and I can’t tell you how many times I’ve heard: “I tried the little blue pill and then the big white capsule.” Nobody feels good if the end result of a long consultative process includes a recommendation for a medication that the patient has already tried and failed. Some EMRs now have this information in a way that can be more easily packaged and shared.
State what you are looking for
If you really want the psychiatrist to take over the care of the patient, are just looking for some guidance for what to do next, or are seeking a second opinion for a patient that already works with a psychiatrist, stating so specifically can help tailor the consultation to best address the situation.
Send along past evaluations
Many patients have accumulated detailed psychological or educational evaluations over time that can include some really important information like cognitive profiles, other diagnostic impressions, and past treatment recommendations that may or may not have been implemented. Having these available to the consulting psychiatrist (of course parents need to give permission to send these along) can help the consultant avoid asking redundant questions or recommend things that already have been tried.
Rule outs of medical causes
There are a lot of psychiatric symptoms that can be caused by nonpsychiatric causes. Sometimes, there can be an assumption on the part of the psychiatrist that the pediatrician already has evaluated for these possibilities while the pediatrician assumes that the psychiatrist will work those up if needed. This is how the care of some patients fall through the cracks, and how those unflattering stories of how patients were forced to live with undiagnosed ailments (seizures, encephalopathy, Lyme disease, etc.) for years are generated. Being clear what work-up and tests already have been done to look for other causes can help everyone involved decide what should be done next and who should do it.
Yes, it is true that most of the recommendations specified here involve more work that the quick “behavioral problems: eval and treat” note that may be tempting to write when consulting with a mental health professional, but they will help avoid a lot of headaches for you down the road and, most importantly, get patients and families the timely and comprehensive care they deserve.
Dr. Rettew is a child and adolescent psychiatrist and associate professor of psychiatry and pediatrics at the University of Vermont, Burlington. Follow him on Twitter @PediPsych. Dr. Rettew said he had no relevant financial disclosures. Email Dr. Rettew at pdnews@mdedge.com.
You’ve been struggling with what to do for a patient who has a significant mental health problem and really would love to have some help. You’re willing to fill out the requisite referral forms and wait your turn for what seems like an excruciating amount of time. But how do you ensure that you, your patient, and the family get the most out of the consultative experience so that everyone’s questions are answered and ongoing care, if needed, can continue?
To be fair, most of the burden of doing a good psychiatric or mental health consultation rests on the consultant, not the person making the request. It is their job to do a thorough evaluation and to identify any additional pieces of information that may be missing before a strong conclusion can be made. That said, however, this is the real world where everyone is busy and few have the time to track down every loose end that may exist regarding a patient’s history.
To that end, here are some recommendations for how to increase the chance that the outcome of your consultation with a child psychiatrist or other mental health professional will be maximally helpful for everyone involved. These tips are based on having been on the receiving end of psychiatric consultations for almost 2 decades and having worked closely with primary care clinicians in a number of different capacities.
The first question to ask yourself, and this may be the most important one of all, is whether or not you really need an actual psychiatrist at all at this stage versus another type of mental health professional. Physicians often are most comfortable dealing with other physicians. If a pediatrician has a question about a patient’s heart, it’s logical to consult a cardiologist. Thus if there’s a question about mental health, the knee-jerk reaction is to consult a psychiatrist. While understandable, looking first to a psychiatrist to help with a patient’s mental health struggles often is not the best move. Psychiatrists make up only one small part of all mental health professionals that also include psychologists, counselors, and clinical social workers, among others. The availability of child and adolescent psychiatrists can been exceedingly sparse while other types of mental health professionals generally are much more available. Moreover, these other types of mental health professionals also can do a great job at assessment and treatment. It is true that most can’t prescribe medication, but best practice recommendations for most of the common mental health diagnoses in youth (anxiety, depression, obsessive compulsive disorder, etc.) explicitly outline that nonpharmacologic treatments should be used first. It breaks my heart every time I do a consult for a family who has waited 6 months only to have me recommend a good therapist they could have seen right off in a week.
Get to know the mental health resources of your community beyond the small number of psychiatrists who might be there. And if you aren’t sure whether or not a referral might best go first to a mental health professional who is not a psychiatrist, just ask. That quick phone call or email might save the family a needless delay in treatment and a lot of aggravation for you.
If you are confident that it is a child & adolescent psychiatrist you want your patient to see, here are some things that will help you get the most out of that consultation and help you avoid the disappointment (for both you and the family) of an evaluation that completely misses the mark.
Select the best site (if you have an option)
Broadly speaking, psychiatrists often can be found in three main areas: academic clinics, private practice, and community mental health centers. While of course there is huge variation of clinicians at each of the sites, some generalizations regarding typical advantages and disadvantages of each setting are probably fair.
Academic settings often have psychiatrists who are local or even national experts on particular topics and can be good places to get evaluations for patients with complicated histories. At the same time, however, these settings typically rely on trainees to do much of the actual work. Many of the residents and fellows are excellent, but they turn over quickly because of graduation and finishing rotations, which can force patients to get to know a lot of different people. Academic centers also can be quite a distance from a family’s home, which often makes follow-up care a challenge (especially when we go back to more in-person visits).
Private practice psychiatrists can provide a more local option and can give families access to experienced clinicians, but many of these practices (especially the ones that take insurance) have practice models that involve seeing a lot of patients for short amounts of time and with less coordination with other types of services.
Finally, psychiatrists working at community mental health centers often work in teams that can help families get access to a lot of useful ancillary services (case management, home supports, etc.) but are part of a public mental health system that sadly is all too often overstretched and underfunded.
If you have choices for where to go for psychiatric services, keeping these things in mind can help you find the best fit for families.
Provide a medication history
While I’m not a big fan of the “what medicine do I try next?” consultation, don’t rely on families to provide this information accurately. Medications are confusing, and I can’t tell you how many times I’ve heard: “I tried the little blue pill and then the big white capsule.” Nobody feels good if the end result of a long consultative process includes a recommendation for a medication that the patient has already tried and failed. Some EMRs now have this information in a way that can be more easily packaged and shared.
State what you are looking for
If you really want the psychiatrist to take over the care of the patient, are just looking for some guidance for what to do next, or are seeking a second opinion for a patient that already works with a psychiatrist, stating so specifically can help tailor the consultation to best address the situation.
Send along past evaluations
Many patients have accumulated detailed psychological or educational evaluations over time that can include some really important information like cognitive profiles, other diagnostic impressions, and past treatment recommendations that may or may not have been implemented. Having these available to the consulting psychiatrist (of course parents need to give permission to send these along) can help the consultant avoid asking redundant questions or recommend things that already have been tried.
Rule outs of medical causes
There are a lot of psychiatric symptoms that can be caused by nonpsychiatric causes. Sometimes, there can be an assumption on the part of the psychiatrist that the pediatrician already has evaluated for these possibilities while the pediatrician assumes that the psychiatrist will work those up if needed. This is how the care of some patients fall through the cracks, and how those unflattering stories of how patients were forced to live with undiagnosed ailments (seizures, encephalopathy, Lyme disease, etc.) for years are generated. Being clear what work-up and tests already have been done to look for other causes can help everyone involved decide what should be done next and who should do it.
Yes, it is true that most of the recommendations specified here involve more work that the quick “behavioral problems: eval and treat” note that may be tempting to write when consulting with a mental health professional, but they will help avoid a lot of headaches for you down the road and, most importantly, get patients and families the timely and comprehensive care they deserve.
Dr. Rettew is a child and adolescent psychiatrist and associate professor of psychiatry and pediatrics at the University of Vermont, Burlington. Follow him on Twitter @PediPsych. Dr. Rettew said he had no relevant financial disclosures. Email Dr. Rettew at pdnews@mdedge.com.
You’ve been struggling with what to do for a patient who has a significant mental health problem and really would love to have some help. You’re willing to fill out the requisite referral forms and wait your turn for what seems like an excruciating amount of time. But how do you ensure that you, your patient, and the family get the most out of the consultative experience so that everyone’s questions are answered and ongoing care, if needed, can continue?
To be fair, most of the burden of doing a good psychiatric or mental health consultation rests on the consultant, not the person making the request. It is their job to do a thorough evaluation and to identify any additional pieces of information that may be missing before a strong conclusion can be made. That said, however, this is the real world where everyone is busy and few have the time to track down every loose end that may exist regarding a patient’s history.
To that end, here are some recommendations for how to increase the chance that the outcome of your consultation with a child psychiatrist or other mental health professional will be maximally helpful for everyone involved. These tips are based on having been on the receiving end of psychiatric consultations for almost 2 decades and having worked closely with primary care clinicians in a number of different capacities.
The first question to ask yourself, and this may be the most important one of all, is whether or not you really need an actual psychiatrist at all at this stage versus another type of mental health professional. Physicians often are most comfortable dealing with other physicians. If a pediatrician has a question about a patient’s heart, it’s logical to consult a cardiologist. Thus if there’s a question about mental health, the knee-jerk reaction is to consult a psychiatrist. While understandable, looking first to a psychiatrist to help with a patient’s mental health struggles often is not the best move. Psychiatrists make up only one small part of all mental health professionals that also include psychologists, counselors, and clinical social workers, among others. The availability of child and adolescent psychiatrists can been exceedingly sparse while other types of mental health professionals generally are much more available. Moreover, these other types of mental health professionals also can do a great job at assessment and treatment. It is true that most can’t prescribe medication, but best practice recommendations for most of the common mental health diagnoses in youth (anxiety, depression, obsessive compulsive disorder, etc.) explicitly outline that nonpharmacologic treatments should be used first. It breaks my heart every time I do a consult for a family who has waited 6 months only to have me recommend a good therapist they could have seen right off in a week.
Get to know the mental health resources of your community beyond the small number of psychiatrists who might be there. And if you aren’t sure whether or not a referral might best go first to a mental health professional who is not a psychiatrist, just ask. That quick phone call or email might save the family a needless delay in treatment and a lot of aggravation for you.
If you are confident that it is a child & adolescent psychiatrist you want your patient to see, here are some things that will help you get the most out of that consultation and help you avoid the disappointment (for both you and the family) of an evaluation that completely misses the mark.
Select the best site (if you have an option)
Broadly speaking, psychiatrists often can be found in three main areas: academic clinics, private practice, and community mental health centers. While of course there is huge variation of clinicians at each of the sites, some generalizations regarding typical advantages and disadvantages of each setting are probably fair.
Academic settings often have psychiatrists who are local or even national experts on particular topics and can be good places to get evaluations for patients with complicated histories. At the same time, however, these settings typically rely on trainees to do much of the actual work. Many of the residents and fellows are excellent, but they turn over quickly because of graduation and finishing rotations, which can force patients to get to know a lot of different people. Academic centers also can be quite a distance from a family’s home, which often makes follow-up care a challenge (especially when we go back to more in-person visits).
Private practice psychiatrists can provide a more local option and can give families access to experienced clinicians, but many of these practices (especially the ones that take insurance) have practice models that involve seeing a lot of patients for short amounts of time and with less coordination with other types of services.
Finally, psychiatrists working at community mental health centers often work in teams that can help families get access to a lot of useful ancillary services (case management, home supports, etc.) but are part of a public mental health system that sadly is all too often overstretched and underfunded.
If you have choices for where to go for psychiatric services, keeping these things in mind can help you find the best fit for families.
Provide a medication history
While I’m not a big fan of the “what medicine do I try next?” consultation, don’t rely on families to provide this information accurately. Medications are confusing, and I can’t tell you how many times I’ve heard: “I tried the little blue pill and then the big white capsule.” Nobody feels good if the end result of a long consultative process includes a recommendation for a medication that the patient has already tried and failed. Some EMRs now have this information in a way that can be more easily packaged and shared.
State what you are looking for
If you really want the psychiatrist to take over the care of the patient, are just looking for some guidance for what to do next, or are seeking a second opinion for a patient that already works with a psychiatrist, stating so specifically can help tailor the consultation to best address the situation.
Send along past evaluations
Many patients have accumulated detailed psychological or educational evaluations over time that can include some really important information like cognitive profiles, other diagnostic impressions, and past treatment recommendations that may or may not have been implemented. Having these available to the consulting psychiatrist (of course parents need to give permission to send these along) can help the consultant avoid asking redundant questions or recommend things that already have been tried.
Rule outs of medical causes
There are a lot of psychiatric symptoms that can be caused by nonpsychiatric causes. Sometimes, there can be an assumption on the part of the psychiatrist that the pediatrician already has evaluated for these possibilities while the pediatrician assumes that the psychiatrist will work those up if needed. This is how the care of some patients fall through the cracks, and how those unflattering stories of how patients were forced to live with undiagnosed ailments (seizures, encephalopathy, Lyme disease, etc.) for years are generated. Being clear what work-up and tests already have been done to look for other causes can help everyone involved decide what should be done next and who should do it.
Yes, it is true that most of the recommendations specified here involve more work that the quick “behavioral problems: eval and treat” note that may be tempting to write when consulting with a mental health professional, but they will help avoid a lot of headaches for you down the road and, most importantly, get patients and families the timely and comprehensive care they deserve.
Dr. Rettew is a child and adolescent psychiatrist and associate professor of psychiatry and pediatrics at the University of Vermont, Burlington. Follow him on Twitter @PediPsych. Dr. Rettew said he had no relevant financial disclosures. Email Dr. Rettew at pdnews@mdedge.com.

Rural areas with local obstetrical care have better perinatal outcomes
according to a retrospective study using county-level data from the Alabama Department of Public Health.

Although association does not establish causation, these data raise concern “for the current trend of diminishing L&D units that is occurring in many rural settings,” according to the authors of the study, led by John B. Waits, MD, of Cahaba Medical Care, Centreville, Ala., in Annals of Family Medicine.
When mortality per 1,000 live births was compared over a 15-year period (2003-2017) between 15 counties with and 21 counties without local L&D units, those with the units had lower overall infant mortality (9.23 vs. 7.89; P = .0011), perinatal mortality (8.89 vs. 10.82; P < .001), and neonatal mortality (4.74 vs. 5.67; P = .0034). The percentages of low-birth-weight babies born between 2003 and 2014 were 9.86% versus 10.61% (P < .001) for counties with and without L&D units, respectively.
The relative increased risks (RR) for these adverse outcomes in counties without L&D units were statistically significant and substantial, ranging from about 8% for a pregnancy resulting in a low-birth-weight infant to slightly more than 21% for perinatal mortality.
Over the study period, there were 165,525 live births in the 15 counties with L&D units and 72,177 births in the 21 counties with no such units. In counties without L&D units, the average proportion of White people was higher (73.47% vs. 60.86%), and that of African Americans was lower (22.76% vs. 36.23%). Median income ($40,759 vs. $35,604) and per capita income ($22,474 vs. $20,641) was slightly higher.
Of the 67 counties in Alabama, this study did not include those considered urbanized by the Alabama Office of Management and Budget even if classified rural by other statewide offices, such as the Alabama Rural Health Association. Any county with at least one L&D unit was considered to have a local unit. Three counties with L&D units that closed before the observation period was completed were excluded from the analysis.

The Alabama data appear to identify a major problem in need of an urgent solution, according to John S. Cullen, MD, a family physician in Valdez, Alaska, and chair of the American Academy of Family Physicians Board of Directors.
“Almost 20% of U.S. women of reproductive age live in rural communities,” he said in an interview. The data from this study provides compelling evidence “that the loss of rural maternity care in this country has contributed to the increase in newborn mortality in rural communities.”
There are many limitations for this study, according to the authors. They acknowledged that they could not control for many potentially important variables, such as travel time to hospitals for those in counties with L&D units when compared with those without. They also acknowledged the lack of data regarding availability of prenatal care in places with or without L&D units.
If lack of L&D services in rural areas is a source of adverse outcomes, data suggesting that the ongoing decline in L&D units are worrisome, according to the authors. Of studies they cited, one showed nearly a 10% loss in rural L&D services in a recent 10-year period.
The authors also noted that about half of the 3,143 counties in the United States do not have a practicing obstetrician, and that fewer than 7% of obstetricians-gynecologists practice in rural settings.
In many rural counties, including the county where the lead author practices, family practitioners provide 100% of local obstetric care, but access to these clinicians also appears to be declining, according to the paper. The ratio of primary care physicians to patients is already lower in non-metropolitan than metropolitan areas (39.8 vs. 53.3). The American Board of Family Medicine has reported that fewer than 10% of family physicians now provide maternity care, the authors wrote.
“If a causal relationship does exist [between lack of L&D units and adverse perinatal outcomes], then rural populations would definitively benefit from having local access to a L&D unit,” the authors stated.
The lead author, Dr. Waits, said in an interview that there are two obstacles to an increase in rural L&D units: malpractice premiums and reimbursement for indigent deliveries. The large malpractice premiums required to cover OB care are hurdles for caregivers, such as family physicians, as well as the hospitals where they practice.
Reforms from the legislative or regulatory perspective are needed to permit malpractice insurance to be issued at a reasonable cost, according to Dr. Waits. Such reforms are a “moral imperative” so that the malpractice issue is not allowed to “shipwreck infant and maternal mortality,” he said.
Of the many potential solutions, such as increased use of telemedicine, legislative initiatives to reduce the malpractice burden, or new support and incentives for family physicians to deliver OB care, each is burdened with obstacles to overcome, according to Dr. Waits. This does not mean these solutions should not be pursued alone or together, but he made it clear that the no solution is easy. In the meantime, Dr. Waits indicated a need to consider practical and immediate strategies to fix the problem.
“There should be incentives for rural emergency departments and ambulance systems to train in the [American Academy of Family Physicians’] Basic Life Support in Obstetrics (BLSO) certification courses each year. I am not aware of any specific evidence around this, but it is a known fact that, when L&Ds close, institutional memory of OB emergencies recede, and preparedness suffers,” he said.
Dr. Cullen agreed that if the closing of L&D units explains the higher rate of perinatal mortality in rural areas, both short-term and long-term solutions are needed.
“Every community must have a plan for obstetric and newborn emergencies. The decision to not offer maternity care means that rural providers will still provide maternity care but not be ready for emergencies,” he said, echoing a point made by Dr. Waits.
The study authors disclosed no conflicts. Dr. Cullen reported having no disclosures.
SOURCE: Waits JB et al. Ann Fam Med. 2020;18:446-51.
according to a retrospective study using county-level data from the Alabama Department of Public Health.
Although association does not establish causation, these data raise concern “for the current trend of diminishing L&D units that is occurring in many rural settings,” according to the authors of the study, led by John B. Waits, MD, of Cahaba Medical Care, Centreville, Ala., in Annals of Family Medicine.
When mortality per 1,000 live births was compared over a 15-year period (2003-2017) between 15 counties with and 21 counties without local L&D units, those with the units had lower overall infant mortality (9.23 vs. 7.89; P = .0011), perinatal mortality (8.89 vs. 10.82; P < .001), and neonatal mortality (4.74 vs. 5.67; P = .0034). The percentages of low-birth-weight babies born between 2003 and 2014 were 9.86% versus 10.61% (P < .001) for counties with and without L&D units, respectively.
The relative increased risks (RR) for these adverse outcomes in counties without L&D units were statistically significant and substantial, ranging from about 8% for a pregnancy resulting in a low-birth-weight infant to slightly more than 21% for perinatal mortality.
Over the study period, there were 165,525 live births in the 15 counties with L&D units and 72,177 births in the 21 counties with no such units. In counties without L&D units, the average proportion of White people was higher (73.47% vs. 60.86%), and that of African Americans was lower (22.76% vs. 36.23%). Median income ($40,759 vs. $35,604) and per capita income ($22,474 vs. $20,641) was slightly higher.
Of the 67 counties in Alabama, this study did not include those considered urbanized by the Alabama Office of Management and Budget even if classified rural by other statewide offices, such as the Alabama Rural Health Association. Any county with at least one L&D unit was considered to have a local unit. Three counties with L&D units that closed before the observation period was completed were excluded from the analysis.
The Alabama data appear to identify a major problem in need of an urgent solution, according to John S. Cullen, MD, a family physician in Valdez, Alaska, and chair of the American Academy of Family Physicians Board of Directors.
“Almost 20% of U.S. women of reproductive age live in rural communities,” he said in an interview. The data from this study provides compelling evidence “that the loss of rural maternity care in this country has contributed to the increase in newborn mortality in rural communities.”
There are many limitations for this study, according to the authors. They acknowledged that they could not control for many potentially important variables, such as travel time to hospitals for those in counties with L&D units when compared with those without. They also acknowledged the lack of data regarding availability of prenatal care in places with or without L&D units.
If lack of L&D services in rural areas is a source of adverse outcomes, data suggesting that the ongoing decline in L&D units are worrisome, according to the authors. Of studies they cited, one showed nearly a 10% loss in rural L&D services in a recent 10-year period.
The authors also noted that about half of the 3,143 counties in the United States do not have a practicing obstetrician, and that fewer than 7% of obstetricians-gynecologists practice in rural settings.
In many rural counties, including the county where the lead author practices, family practitioners provide 100% of local obstetric care, but access to these clinicians also appears to be declining, according to the paper. The ratio of primary care physicians to patients is already lower in non-metropolitan than metropolitan areas (39.8 vs. 53.3). The American Board of Family Medicine has reported that fewer than 10% of family physicians now provide maternity care, the authors wrote.
“If a causal relationship does exist [between lack of L&D units and adverse perinatal outcomes], then rural populations would definitively benefit from having local access to a L&D unit,” the authors stated.
The lead author, Dr. Waits, said in an interview that there are two obstacles to an increase in rural L&D units: malpractice premiums and reimbursement for indigent deliveries. The large malpractice premiums required to cover OB care are hurdles for caregivers, such as family physicians, as well as the hospitals where they practice.
Reforms from the legislative or regulatory perspective are needed to permit malpractice insurance to be issued at a reasonable cost, according to Dr. Waits. Such reforms are a “moral imperative” so that the malpractice issue is not allowed to “shipwreck infant and maternal mortality,” he said.
Of the many potential solutions, such as increased use of telemedicine, legislative initiatives to reduce the malpractice burden, or new support and incentives for family physicians to deliver OB care, each is burdened with obstacles to overcome, according to Dr. Waits. This does not mean these solutions should not be pursued alone or together, but he made it clear that the no solution is easy. In the meantime, Dr. Waits indicated a need to consider practical and immediate strategies to fix the problem.
“There should be incentives for rural emergency departments and ambulance systems to train in the [American Academy of Family Physicians’] Basic Life Support in Obstetrics (BLSO) certification courses each year. I am not aware of any specific evidence around this, but it is a known fact that, when L&Ds close, institutional memory of OB emergencies recede, and preparedness suffers,” he said.
Dr. Cullen agreed that if the closing of L&D units explains the higher rate of perinatal mortality in rural areas, both short-term and long-term solutions are needed.
“Every community must have a plan for obstetric and newborn emergencies. The decision to not offer maternity care means that rural providers will still provide maternity care but not be ready for emergencies,” he said, echoing a point made by Dr. Waits.
The study authors disclosed no conflicts. Dr. Cullen reported having no disclosures.
SOURCE: Waits JB et al. Ann Fam Med. 2020;18:446-51.
according to a retrospective study using county-level data from the Alabama Department of Public Health.
Although association does not establish causation, these data raise concern “for the current trend of diminishing L&D units that is occurring in many rural settings,” according to the authors of the study, led by John B. Waits, MD, of Cahaba Medical Care, Centreville, Ala., in Annals of Family Medicine.
When mortality per 1,000 live births was compared over a 15-year period (2003-2017) between 15 counties with and 21 counties without local L&D units, those with the units had lower overall infant mortality (9.23 vs. 7.89; P = .0011), perinatal mortality (8.89 vs. 10.82; P < .001), and neonatal mortality (4.74 vs. 5.67; P = .0034). The percentages of low-birth-weight babies born between 2003 and 2014 were 9.86% versus 10.61% (P < .001) for counties with and without L&D units, respectively.
The relative increased risks (RR) for these adverse outcomes in counties without L&D units were statistically significant and substantial, ranging from about 8% for a pregnancy resulting in a low-birth-weight infant to slightly more than 21% for perinatal mortality.
Over the study period, there were 165,525 live births in the 15 counties with L&D units and 72,177 births in the 21 counties with no such units. In counties without L&D units, the average proportion of White people was higher (73.47% vs. 60.86%), and that of African Americans was lower (22.76% vs. 36.23%). Median income ($40,759 vs. $35,604) and per capita income ($22,474 vs. $20,641) was slightly higher.
Of the 67 counties in Alabama, this study did not include those considered urbanized by the Alabama Office of Management and Budget even if classified rural by other statewide offices, such as the Alabama Rural Health Association. Any county with at least one L&D unit was considered to have a local unit. Three counties with L&D units that closed before the observation period was completed were excluded from the analysis.
The Alabama data appear to identify a major problem in need of an urgent solution, according to John S. Cullen, MD, a family physician in Valdez, Alaska, and chair of the American Academy of Family Physicians Board of Directors.
“Almost 20% of U.S. women of reproductive age live in rural communities,” he said in an interview. The data from this study provides compelling evidence “that the loss of rural maternity care in this country has contributed to the increase in newborn mortality in rural communities.”
There are many limitations for this study, according to the authors. They acknowledged that they could not control for many potentially important variables, such as travel time to hospitals for those in counties with L&D units when compared with those without. They also acknowledged the lack of data regarding availability of prenatal care in places with or without L&D units.
If lack of L&D services in rural areas is a source of adverse outcomes, data suggesting that the ongoing decline in L&D units are worrisome, according to the authors. Of studies they cited, one showed nearly a 10% loss in rural L&D services in a recent 10-year period.
The authors also noted that about half of the 3,143 counties in the United States do not have a practicing obstetrician, and that fewer than 7% of obstetricians-gynecologists practice in rural settings.
In many rural counties, including the county where the lead author practices, family practitioners provide 100% of local obstetric care, but access to these clinicians also appears to be declining, according to the paper. The ratio of primary care physicians to patients is already lower in non-metropolitan than metropolitan areas (39.8 vs. 53.3). The American Board of Family Medicine has reported that fewer than 10% of family physicians now provide maternity care, the authors wrote.
“If a causal relationship does exist [between lack of L&D units and adverse perinatal outcomes], then rural populations would definitively benefit from having local access to a L&D unit,” the authors stated.
The lead author, Dr. Waits, said in an interview that there are two obstacles to an increase in rural L&D units: malpractice premiums and reimbursement for indigent deliveries. The large malpractice premiums required to cover OB care are hurdles for caregivers, such as family physicians, as well as the hospitals where they practice.
Reforms from the legislative or regulatory perspective are needed to permit malpractice insurance to be issued at a reasonable cost, according to Dr. Waits. Such reforms are a “moral imperative” so that the malpractice issue is not allowed to “shipwreck infant and maternal mortality,” he said.
Of the many potential solutions, such as increased use of telemedicine, legislative initiatives to reduce the malpractice burden, or new support and incentives for family physicians to deliver OB care, each is burdened with obstacles to overcome, according to Dr. Waits. This does not mean these solutions should not be pursued alone or together, but he made it clear that the no solution is easy. In the meantime, Dr. Waits indicated a need to consider practical and immediate strategies to fix the problem.
“There should be incentives for rural emergency departments and ambulance systems to train in the [American Academy of Family Physicians’] Basic Life Support in Obstetrics (BLSO) certification courses each year. I am not aware of any specific evidence around this, but it is a known fact that, when L&Ds close, institutional memory of OB emergencies recede, and preparedness suffers,” he said.
Dr. Cullen agreed that if the closing of L&D units explains the higher rate of perinatal mortality in rural areas, both short-term and long-term solutions are needed.
“Every community must have a plan for obstetric and newborn emergencies. The decision to not offer maternity care means that rural providers will still provide maternity care but not be ready for emergencies,” he said, echoing a point made by Dr. Waits.
The study authors disclosed no conflicts. Dr. Cullen reported having no disclosures.
SOURCE: Waits JB et al. Ann Fam Med. 2020;18:446-51.
FROM ANNALS OF FAMILY MEDICINE
Key clinical point: The absence of labor and delivery (L&D) services in rural counties predicts adverse outcomes, including higher child mortality.
Major finding: In the absence of L&D units, the risk of perinatal mortality per 1,000 live births is 19% higher (5.67 vs. 4.74; P = .0034).
Data Source: Retrospective cohort study.
Disclosures: Potential conflicts of interest involving this topic were not reported.
Source: Waits JB et al. Ann Fam Med. 2020;18:446-51.
Distinguishing COVID-19 from flu in kids remains challenging
For children with COVID-19, rates of hospitalization, ICU admission, and ventilator use were similar to those of children with influenza, but rates differed in other respects, according to results of a study published online Sept. 11 in JAMA Network Open.
As winter approaches, distinguishing patients with COVID-19 from those with influenza will become a problem. To assist with that, Xiaoyan Song, PhD, director of the office of infection control and epidemiology at Children’s National Hospital in Washington, D.C., and colleagues investigated commonalities and differences between the clinical symptoms of COVID-19 and influenza in children.
“Distinguishing COVID-19 from flu and other respiratory viral infections remains a challenge to clinicians. Although our study showed that patients with COVID-19 were more likely than patients with flu to report fever, gastrointestinal, and other clinical symptoms at the time of diagnosis, the two groups do have many overlapping clinical symptoms,” Dr. Song said. “Until future data show us otherwise, clinicians need to prepare for managing coinfections of COVID-19 with flu and/or other respiratory viral infections in the upcoming flu season.”
The retrospective cohort study included 315 children diagnosed with laboratory-confirmed COVID-19 between March 25 and May 15, 2020, and 1,402 children diagnosed with laboratory-confirmed seasonal influenza A or influenza B between Oct. 1, 2019, and June 6, 2020, at Children’s National Hospital. The investigation excluded asymptomatic patients who tested positive for COVID-19.
Patients with COVID-19 and patients with influenza were similar with respect to rates of hospitalization (17% vs. 21%; odds ratio, 0.8; 95% confidence interval, 0.6-1.1; P = .15), admission to the ICU (6% vs. 7%; OR, 0.8; 95% CI, 0.5-1.3; P = .42), and use of mechanical ventilation (3% vs. 2%; OR, 1.5; 95% CI, 0.9-2.6; P =.17).
The difference in the duration of ventilation for the two groups was not statistically significant. None of the patients who had COVID-19 or influenza B died, but two patients with influenza A did.
No patients had coinfections, which the researchers attribute to the mid-March shutdown of many schools, which they believe limited the spread of seasonal influenza.
Patients who were hospitalized with COVID-19 were older (median age, 9.7 years; range, 0.06-23.2 years) than those hospitalized with either type of influenza (median age, 4.2 years; range, 0.04-23.1). Patients older than 15 years made up 37% of patients with COVID-19 but only 6% of those with influenza.
Among patients hospitalized with COVID-19, 65% had at least one underlying medical condition, compared with 42% of those hospitalized for either type of influenza (OR, 2.6; 95% CI, 1.4-4.7; P = .002).
The most common underlying condition was neurologic problems from global developmental delay or seizures, identified in 11 patients (20%) hospitalized with COVID-19 and in 24 patients (8%) hospitalized with influenza (OR, 2.8; 95% CI, 1.3-6.2; P = .002). There was no significant difference between the two groups with respect to a history of asthma, cardiac disease, hematologic disease, and cancer.
For both groups, fever and cough were the most frequently reported symptoms at the time of diagnosis. However, more patients hospitalized with COVID-19 reported fever (76% vs. 55%; OR, 2.6; 95% CI, 1.4-5.1; P = 01), diarrhea or vomiting (26% vs. 12%; OR, 2.5; 95% CI, 1.2-5.0; P = .01), headache (11% vs. 3%; OR, 3.9; 95% CI, 1.3-11.5; P = .01), myalgia (22% vs. 7%; OR, 3.9; 95% CI, 1.8-8.5; P = .001), or chest pain (11% vs. 3%; OR, 3.9; 95% CI, 1.3-11.5; P = .01).
The researchers found no statistically significant differences between the two groups in rates of cough, congestion, sore throat, or shortness of breath.
Comparison of the symptom spectrum between COVID-19 and flu differed with respect to influenza type. More patients with COVID-19 reported fever, cough, diarrhea and vomiting, and myalgia than patients hospitalized with influenza A. But rates of fever, cough, diarrhea or vomiting, headache, or chest pain didn’t differ significantly in patients with COVID-19 and those with influenza B.
Larry K. Kociolek, MD, medical director of infection prevention and control at Ann and Robert H. Lurie Children’s Hospital of Chicago, noted the lower age of patients with flu. “Differentiating the two infections, which is difficult if not impossible based on symptoms alone, may have prognostic implications, depending on the age of the child. Because this study was performed outside peak influenza season, when coinfections would be less likely to occur, we must be vigilant about the potential clinical implications of influenza and SARS-CoV-2 coinfection this fall and winter.”
Clinicians will still have to use a combination of symptoms, examinations, and testing to distinguish the two diseases, said Aimee Sznewajs, MD, medical director of the pediatric hospital medicine department at Children’s Minnesota, Minneapolis. “We will continue to test for influenza and COVID-19 prior to hospitalizations and make decisions about whether to hospitalize based on other clinical factors, such as dehydration, oxygen requirement, and vital sign changes.”
Dr. Sznewajs stressed the importance of maintaining public health strategies, including “ensuring all children get the flu vaccine, encouraging mask wearing and hand hygiene, adequate testing to determine which virus is present, and other mitigation measures if the prevalence of COVID-19 is increasing in the community.”
Dr. Song reiterated those points, noting that clinicians need to make the most of the options they have. “Clinicians already have many great tools on hand. It is extremely important to get the flu vaccine now, especially for kids with underlying medical conditions. Diagnostic tests are available for both COVID-19 and flu. Antiviral treatment for flu is available. Judicious use of these tools will protect the health of providers, kids, and well-being at large.”
The authors noted several limitations for the study, including its retrospective design, that the data came from a single center, and that different platforms were used to detect the viruses.
A version of this article originally appeared on Medscape.com.
For children with COVID-19, rates of hospitalization, ICU admission, and ventilator use were similar to those of children with influenza, but rates differed in other respects, according to results of a study published online Sept. 11 in JAMA Network Open.
As winter approaches, distinguishing patients with COVID-19 from those with influenza will become a problem. To assist with that, Xiaoyan Song, PhD, director of the office of infection control and epidemiology at Children’s National Hospital in Washington, D.C., and colleagues investigated commonalities and differences between the clinical symptoms of COVID-19 and influenza in children.
“Distinguishing COVID-19 from flu and other respiratory viral infections remains a challenge to clinicians. Although our study showed that patients with COVID-19 were more likely than patients with flu to report fever, gastrointestinal, and other clinical symptoms at the time of diagnosis, the two groups do have many overlapping clinical symptoms,” Dr. Song said. “Until future data show us otherwise, clinicians need to prepare for managing coinfections of COVID-19 with flu and/or other respiratory viral infections in the upcoming flu season.”
The retrospective cohort study included 315 children diagnosed with laboratory-confirmed COVID-19 between March 25 and May 15, 2020, and 1,402 children diagnosed with laboratory-confirmed seasonal influenza A or influenza B between Oct. 1, 2019, and June 6, 2020, at Children’s National Hospital. The investigation excluded asymptomatic patients who tested positive for COVID-19.
Patients with COVID-19 and patients with influenza were similar with respect to rates of hospitalization (17% vs. 21%; odds ratio, 0.8; 95% confidence interval, 0.6-1.1; P = .15), admission to the ICU (6% vs. 7%; OR, 0.8; 95% CI, 0.5-1.3; P = .42), and use of mechanical ventilation (3% vs. 2%; OR, 1.5; 95% CI, 0.9-2.6; P =.17).
The difference in the duration of ventilation for the two groups was not statistically significant. None of the patients who had COVID-19 or influenza B died, but two patients with influenza A did.
No patients had coinfections, which the researchers attribute to the mid-March shutdown of many schools, which they believe limited the spread of seasonal influenza.
Patients who were hospitalized with COVID-19 were older (median age, 9.7 years; range, 0.06-23.2 years) than those hospitalized with either type of influenza (median age, 4.2 years; range, 0.04-23.1). Patients older than 15 years made up 37% of patients with COVID-19 but only 6% of those with influenza.
Among patients hospitalized with COVID-19, 65% had at least one underlying medical condition, compared with 42% of those hospitalized for either type of influenza (OR, 2.6; 95% CI, 1.4-4.7; P = .002).
The most common underlying condition was neurologic problems from global developmental delay or seizures, identified in 11 patients (20%) hospitalized with COVID-19 and in 24 patients (8%) hospitalized with influenza (OR, 2.8; 95% CI, 1.3-6.2; P = .002). There was no significant difference between the two groups with respect to a history of asthma, cardiac disease, hematologic disease, and cancer.
For both groups, fever and cough were the most frequently reported symptoms at the time of diagnosis. However, more patients hospitalized with COVID-19 reported fever (76% vs. 55%; OR, 2.6; 95% CI, 1.4-5.1; P = 01), diarrhea or vomiting (26% vs. 12%; OR, 2.5; 95% CI, 1.2-5.0; P = .01), headache (11% vs. 3%; OR, 3.9; 95% CI, 1.3-11.5; P = .01), myalgia (22% vs. 7%; OR, 3.9; 95% CI, 1.8-8.5; P = .001), or chest pain (11% vs. 3%; OR, 3.9; 95% CI, 1.3-11.5; P = .01).
The researchers found no statistically significant differences between the two groups in rates of cough, congestion, sore throat, or shortness of breath.
Comparison of the symptom spectrum between COVID-19 and flu differed with respect to influenza type. More patients with COVID-19 reported fever, cough, diarrhea and vomiting, and myalgia than patients hospitalized with influenza A. But rates of fever, cough, diarrhea or vomiting, headache, or chest pain didn’t differ significantly in patients with COVID-19 and those with influenza B.
Larry K. Kociolek, MD, medical director of infection prevention and control at Ann and Robert H. Lurie Children’s Hospital of Chicago, noted the lower age of patients with flu. “Differentiating the two infections, which is difficult if not impossible based on symptoms alone, may have prognostic implications, depending on the age of the child. Because this study was performed outside peak influenza season, when coinfections would be less likely to occur, we must be vigilant about the potential clinical implications of influenza and SARS-CoV-2 coinfection this fall and winter.”
Clinicians will still have to use a combination of symptoms, examinations, and testing to distinguish the two diseases, said Aimee Sznewajs, MD, medical director of the pediatric hospital medicine department at Children’s Minnesota, Minneapolis. “We will continue to test for influenza and COVID-19 prior to hospitalizations and make decisions about whether to hospitalize based on other clinical factors, such as dehydration, oxygen requirement, and vital sign changes.”
Dr. Sznewajs stressed the importance of maintaining public health strategies, including “ensuring all children get the flu vaccine, encouraging mask wearing and hand hygiene, adequate testing to determine which virus is present, and other mitigation measures if the prevalence of COVID-19 is increasing in the community.”
Dr. Song reiterated those points, noting that clinicians need to make the most of the options they have. “Clinicians already have many great tools on hand. It is extremely important to get the flu vaccine now, especially for kids with underlying medical conditions. Diagnostic tests are available for both COVID-19 and flu. Antiviral treatment for flu is available. Judicious use of these tools will protect the health of providers, kids, and well-being at large.”
The authors noted several limitations for the study, including its retrospective design, that the data came from a single center, and that different platforms were used to detect the viruses.
A version of this article originally appeared on Medscape.com.
For children with COVID-19, rates of hospitalization, ICU admission, and ventilator use were similar to those of children with influenza, but rates differed in other respects, according to results of a study published online Sept. 11 in JAMA Network Open.
As winter approaches, distinguishing patients with COVID-19 from those with influenza will become a problem. To assist with that, Xiaoyan Song, PhD, director of the office of infection control and epidemiology at Children’s National Hospital in Washington, D.C., and colleagues investigated commonalities and differences between the clinical symptoms of COVID-19 and influenza in children.
“Distinguishing COVID-19 from flu and other respiratory viral infections remains a challenge to clinicians. Although our study showed that patients with COVID-19 were more likely than patients with flu to report fever, gastrointestinal, and other clinical symptoms at the time of diagnosis, the two groups do have many overlapping clinical symptoms,” Dr. Song said. “Until future data show us otherwise, clinicians need to prepare for managing coinfections of COVID-19 with flu and/or other respiratory viral infections in the upcoming flu season.”
The retrospective cohort study included 315 children diagnosed with laboratory-confirmed COVID-19 between March 25 and May 15, 2020, and 1,402 children diagnosed with laboratory-confirmed seasonal influenza A or influenza B between Oct. 1, 2019, and June 6, 2020, at Children’s National Hospital. The investigation excluded asymptomatic patients who tested positive for COVID-19.
Patients with COVID-19 and patients with influenza were similar with respect to rates of hospitalization (17% vs. 21%; odds ratio, 0.8; 95% confidence interval, 0.6-1.1; P = .15), admission to the ICU (6% vs. 7%; OR, 0.8; 95% CI, 0.5-1.3; P = .42), and use of mechanical ventilation (3% vs. 2%; OR, 1.5; 95% CI, 0.9-2.6; P =.17).
The difference in the duration of ventilation for the two groups was not statistically significant. None of the patients who had COVID-19 or influenza B died, but two patients with influenza A did.
No patients had coinfections, which the researchers attribute to the mid-March shutdown of many schools, which they believe limited the spread of seasonal influenza.
Patients who were hospitalized with COVID-19 were older (median age, 9.7 years; range, 0.06-23.2 years) than those hospitalized with either type of influenza (median age, 4.2 years; range, 0.04-23.1). Patients older than 15 years made up 37% of patients with COVID-19 but only 6% of those with influenza.
Among patients hospitalized with COVID-19, 65% had at least one underlying medical condition, compared with 42% of those hospitalized for either type of influenza (OR, 2.6; 95% CI, 1.4-4.7; P = .002).
The most common underlying condition was neurologic problems from global developmental delay or seizures, identified in 11 patients (20%) hospitalized with COVID-19 and in 24 patients (8%) hospitalized with influenza (OR, 2.8; 95% CI, 1.3-6.2; P = .002). There was no significant difference between the two groups with respect to a history of asthma, cardiac disease, hematologic disease, and cancer.
For both groups, fever and cough were the most frequently reported symptoms at the time of diagnosis. However, more patients hospitalized with COVID-19 reported fever (76% vs. 55%; OR, 2.6; 95% CI, 1.4-5.1; P = 01), diarrhea or vomiting (26% vs. 12%; OR, 2.5; 95% CI, 1.2-5.0; P = .01), headache (11% vs. 3%; OR, 3.9; 95% CI, 1.3-11.5; P = .01), myalgia (22% vs. 7%; OR, 3.9; 95% CI, 1.8-8.5; P = .001), or chest pain (11% vs. 3%; OR, 3.9; 95% CI, 1.3-11.5; P = .01).
The researchers found no statistically significant differences between the two groups in rates of cough, congestion, sore throat, or shortness of breath.
Comparison of the symptom spectrum between COVID-19 and flu differed with respect to influenza type. More patients with COVID-19 reported fever, cough, diarrhea and vomiting, and myalgia than patients hospitalized with influenza A. But rates of fever, cough, diarrhea or vomiting, headache, or chest pain didn’t differ significantly in patients with COVID-19 and those with influenza B.
Larry K. Kociolek, MD, medical director of infection prevention and control at Ann and Robert H. Lurie Children’s Hospital of Chicago, noted the lower age of patients with flu. “Differentiating the two infections, which is difficult if not impossible based on symptoms alone, may have prognostic implications, depending on the age of the child. Because this study was performed outside peak influenza season, when coinfections would be less likely to occur, we must be vigilant about the potential clinical implications of influenza and SARS-CoV-2 coinfection this fall and winter.”
Clinicians will still have to use a combination of symptoms, examinations, and testing to distinguish the two diseases, said Aimee Sznewajs, MD, medical director of the pediatric hospital medicine department at Children’s Minnesota, Minneapolis. “We will continue to test for influenza and COVID-19 prior to hospitalizations and make decisions about whether to hospitalize based on other clinical factors, such as dehydration, oxygen requirement, and vital sign changes.”
Dr. Sznewajs stressed the importance of maintaining public health strategies, including “ensuring all children get the flu vaccine, encouraging mask wearing and hand hygiene, adequate testing to determine which virus is present, and other mitigation measures if the prevalence of COVID-19 is increasing in the community.”
Dr. Song reiterated those points, noting that clinicians need to make the most of the options they have. “Clinicians already have many great tools on hand. It is extremely important to get the flu vaccine now, especially for kids with underlying medical conditions. Diagnostic tests are available for both COVID-19 and flu. Antiviral treatment for flu is available. Judicious use of these tools will protect the health of providers, kids, and well-being at large.”
The authors noted several limitations for the study, including its retrospective design, that the data came from a single center, and that different platforms were used to detect the viruses.
A version of this article originally appeared on Medscape.com.
Filling Gaps: Moving Toward Better Treatment of Children With Atopic Dermatitis
It is a brand-new day for the treatment of children with severe inflammatory skin diseases. Not coincidentally, it also is a new day for the treatment of atopic dermatitis (AD). Why?
Historically, children have largely been ignored by pharmaceutical companies and the US Food and Drug Administration (FDA). Drug trials of new medications have been the exclusive province of adults; therefore, information they have generated has had only derivative relevance to the pediatric population. Pediatricians and providers who care for children, aware that they are not simply “little adults,” have been forced to extrapolate best practices.
My institution is poised to enroll a 3-year-old child with severe AD into a biologic trial (ClinicalTrials.gov identifier NCT03346434). The age range for this study is 6 months to 6 years. This extraordinary democratization of clinical trials is no accident. The Best Pharmaceuticals for Children Act, which was passed in 2002, was a first step. This legislation incentivized pharmaceutical companies to include children, who are notoriously more costly to study for myriad reasons, by extending patent protection for approved medications. Subsequent efforts spearheaded by advocacy groups such as the National Eczema Association included the production of guidance documents for industry1 and presentations directly to the FDA’s Dermatologic and Ophthalmic Drugs Advisory Committee meeting punctuated by powerful patient testimonials.2
Serendipitously, AD, a disease that presents by kindergarten in up to 90% of affected individuals, also has caught the eye of the pharmaceutical industry. Remarkable advances in the understanding of AD inflammation have led to an explosion of new therapeutic targets of interest. By way of context, between the introduction of topical calcineurin inhibitors in 2001 and the FDA approval of dupilumab and crisaborole in 2017, there were precisely zero new molecules approved for the treatment of AD. Viewed through another lens, prior to 2017, the only FDA-approved systemic medication for AD was prednisone, a drug most AD experts would list as the least appropriate choice for treatment of this condition.
Fast-forward to 2020 and we have a plethora of new possibilities. The National Eczema Association’s research web page
This confluence of better science, powerful advocacy, and enlightened self-interest has been revolutionary. It is most evident when parents/guardians—many of whom had long ago given up on new therapies for themselves—are gobsmacked by the new therapeutic landscape outlined for their children. Parents/guardians realize their children need not struggle as they may have themselves. The impact on quality of life has long been known, but several recent publications have brought it into finer relief. Drucker et al5 highlighted the overall burden of disease, and several subsequent papers have focused specifically on affective impacts including increased risk for depression, suicidal ideation, and suicide.6,7 In this issue of Cutis, Tracy et al8 provide an update on pediatric AD with an emphasis on comorbidities, quality of life, and evolving practices and therapies.
Better science, better drugs, better advocacy, better outcomes—it has not been a straight line, but it has indisputably been a forward-marching one. It is a new day, indeed.
- Siegfried EC, Jaworski JC, Eichenfield LF, et al. Developing drugs for the treatment of atopic dermatitis in children (≥3 months to <18 years of age): draft guidance for industry [published online March 30, 2018]. Pediatr Dermatol. 2018; May 35:303-322.
- Pediatric trials for AD systemic treatments. Dermatology Times. May 21, 2015. https://www.dermatologytimes.com/view/pediatric-trials-ad-systemic-treatments. Accessed August 11, 2020.
- Solimani F, Meier K, Ghoreschi K. Emerging topical and systemic JAK inhibitors in dermatology. Front Immunol. 2019;10:2847.
- Chan S, Cornelius V, Cro S, et al. Treatment effect of omalizumab on severe pediatric atopic dermatitis: the ADAPT randomized controlled trial. JAMA Pediatr. 2019;174:29-37.
- Drucker AM, Wang AR, Li W-Q, et al. The burden of atopic dermatitis: summary of a report for the National Eczema Association [published online September 8, 2016]. J Invest Dermatol. 2017;137:26-30.
- Sandhu JK, Wu KK, Bui T-L, et al. Association between atopic dermatitis and suicidality: a systematic review and meta-analysis. JAMA Dermatol. 2019;155:178-187.
- Patel KR, Immaneni S, Singam V, et al. Association between atopic dermatitis, depression, and suicidal ideation: a systematic review and meta-analysis [published online October 23, 2018]. J Am Acad Dermatol. 2019;80:402-410.
- Tracy A, Bhatti S, Eichenfield LF. Update on pediatric atopic dermatitis. Cutis. 2020;106:143-146.
It is a brand-new day for the treatment of children with severe inflammatory skin diseases. Not coincidentally, it also is a new day for the treatment of atopic dermatitis (AD). Why?
Historically, children have largely been ignored by pharmaceutical companies and the US Food and Drug Administration (FDA). Drug trials of new medications have been the exclusive province of adults; therefore, information they have generated has had only derivative relevance to the pediatric population. Pediatricians and providers who care for children, aware that they are not simply “little adults,” have been forced to extrapolate best practices.
My institution is poised to enroll a 3-year-old child with severe AD into a biologic trial (ClinicalTrials.gov identifier NCT03346434). The age range for this study is 6 months to 6 years. This extraordinary democratization of clinical trials is no accident. The Best Pharmaceuticals for Children Act, which was passed in 2002, was a first step. This legislation incentivized pharmaceutical companies to include children, who are notoriously more costly to study for myriad reasons, by extending patent protection for approved medications. Subsequent efforts spearheaded by advocacy groups such as the National Eczema Association included the production of guidance documents for industry1 and presentations directly to the FDA’s Dermatologic and Ophthalmic Drugs Advisory Committee meeting punctuated by powerful patient testimonials.2
Serendipitously, AD, a disease that presents by kindergarten in up to 90% of affected individuals, also has caught the eye of the pharmaceutical industry. Remarkable advances in the understanding of AD inflammation have led to an explosion of new therapeutic targets of interest. By way of context, between the introduction of topical calcineurin inhibitors in 2001 and the FDA approval of dupilumab and crisaborole in 2017, there were precisely zero new molecules approved for the treatment of AD. Viewed through another lens, prior to 2017, the only FDA-approved systemic medication for AD was prednisone, a drug most AD experts would list as the least appropriate choice for treatment of this condition.
Fast-forward to 2020 and we have a plethora of new possibilities. The National Eczema Association’s research web page
This confluence of better science, powerful advocacy, and enlightened self-interest has been revolutionary. It is most evident when parents/guardians—many of whom had long ago given up on new therapies for themselves—are gobsmacked by the new therapeutic landscape outlined for their children. Parents/guardians realize their children need not struggle as they may have themselves. The impact on quality of life has long been known, but several recent publications have brought it into finer relief. Drucker et al5 highlighted the overall burden of disease, and several subsequent papers have focused specifically on affective impacts including increased risk for depression, suicidal ideation, and suicide.6,7 In this issue of Cutis, Tracy et al8 provide an update on pediatric AD with an emphasis on comorbidities, quality of life, and evolving practices and therapies.
Better science, better drugs, better advocacy, better outcomes—it has not been a straight line, but it has indisputably been a forward-marching one. It is a new day, indeed.
It is a brand-new day for the treatment of children with severe inflammatory skin diseases. Not coincidentally, it also is a new day for the treatment of atopic dermatitis (AD). Why?
Historically, children have largely been ignored by pharmaceutical companies and the US Food and Drug Administration (FDA). Drug trials of new medications have been the exclusive province of adults; therefore, information they have generated has had only derivative relevance to the pediatric population. Pediatricians and providers who care for children, aware that they are not simply “little adults,” have been forced to extrapolate best practices.
My institution is poised to enroll a 3-year-old child with severe AD into a biologic trial (ClinicalTrials.gov identifier NCT03346434). The age range for this study is 6 months to 6 years. This extraordinary democratization of clinical trials is no accident. The Best Pharmaceuticals for Children Act, which was passed in 2002, was a first step. This legislation incentivized pharmaceutical companies to include children, who are notoriously more costly to study for myriad reasons, by extending patent protection for approved medications. Subsequent efforts spearheaded by advocacy groups such as the National Eczema Association included the production of guidance documents for industry1 and presentations directly to the FDA’s Dermatologic and Ophthalmic Drugs Advisory Committee meeting punctuated by powerful patient testimonials.2
Serendipitously, AD, a disease that presents by kindergarten in up to 90% of affected individuals, also has caught the eye of the pharmaceutical industry. Remarkable advances in the understanding of AD inflammation have led to an explosion of new therapeutic targets of interest. By way of context, between the introduction of topical calcineurin inhibitors in 2001 and the FDA approval of dupilumab and crisaborole in 2017, there were precisely zero new molecules approved for the treatment of AD. Viewed through another lens, prior to 2017, the only FDA-approved systemic medication for AD was prednisone, a drug most AD experts would list as the least appropriate choice for treatment of this condition.
Fast-forward to 2020 and we have a plethora of new possibilities. The National Eczema Association’s research web page
This confluence of better science, powerful advocacy, and enlightened self-interest has been revolutionary. It is most evident when parents/guardians—many of whom had long ago given up on new therapies for themselves—are gobsmacked by the new therapeutic landscape outlined for their children. Parents/guardians realize their children need not struggle as they may have themselves. The impact on quality of life has long been known, but several recent publications have brought it into finer relief. Drucker et al5 highlighted the overall burden of disease, and several subsequent papers have focused specifically on affective impacts including increased risk for depression, suicidal ideation, and suicide.6,7 In this issue of Cutis, Tracy et al8 provide an update on pediatric AD with an emphasis on comorbidities, quality of life, and evolving practices and therapies.
Better science, better drugs, better advocacy, better outcomes—it has not been a straight line, but it has indisputably been a forward-marching one. It is a new day, indeed.
- Siegfried EC, Jaworski JC, Eichenfield LF, et al. Developing drugs for the treatment of atopic dermatitis in children (≥3 months to <18 years of age): draft guidance for industry [published online March 30, 2018]. Pediatr Dermatol. 2018; May 35:303-322.
- Pediatric trials for AD systemic treatments. Dermatology Times. May 21, 2015. https://www.dermatologytimes.com/view/pediatric-trials-ad-systemic-treatments. Accessed August 11, 2020.
- Solimani F, Meier K, Ghoreschi K. Emerging topical and systemic JAK inhibitors in dermatology. Front Immunol. 2019;10:2847.
- Chan S, Cornelius V, Cro S, et al. Treatment effect of omalizumab on severe pediatric atopic dermatitis: the ADAPT randomized controlled trial. JAMA Pediatr. 2019;174:29-37.
- Drucker AM, Wang AR, Li W-Q, et al. The burden of atopic dermatitis: summary of a report for the National Eczema Association [published online September 8, 2016]. J Invest Dermatol. 2017;137:26-30.
- Sandhu JK, Wu KK, Bui T-L, et al. Association between atopic dermatitis and suicidality: a systematic review and meta-analysis. JAMA Dermatol. 2019;155:178-187.
- Patel KR, Immaneni S, Singam V, et al. Association between atopic dermatitis, depression, and suicidal ideation: a systematic review and meta-analysis [published online October 23, 2018]. J Am Acad Dermatol. 2019;80:402-410.
- Tracy A, Bhatti S, Eichenfield LF. Update on pediatric atopic dermatitis. Cutis. 2020;106:143-146.
- Siegfried EC, Jaworski JC, Eichenfield LF, et al. Developing drugs for the treatment of atopic dermatitis in children (≥3 months to <18 years of age): draft guidance for industry [published online March 30, 2018]. Pediatr Dermatol. 2018; May 35:303-322.
- Pediatric trials for AD systemic treatments. Dermatology Times. May 21, 2015. https://www.dermatologytimes.com/view/pediatric-trials-ad-systemic-treatments. Accessed August 11, 2020.
- Solimani F, Meier K, Ghoreschi K. Emerging topical and systemic JAK inhibitors in dermatology. Front Immunol. 2019;10:2847.
- Chan S, Cornelius V, Cro S, et al. Treatment effect of omalizumab on severe pediatric atopic dermatitis: the ADAPT randomized controlled trial. JAMA Pediatr. 2019;174:29-37.
- Drucker AM, Wang AR, Li W-Q, et al. The burden of atopic dermatitis: summary of a report for the National Eczema Association [published online September 8, 2016]. J Invest Dermatol. 2017;137:26-30.
- Sandhu JK, Wu KK, Bui T-L, et al. Association between atopic dermatitis and suicidality: a systematic review and meta-analysis. JAMA Dermatol. 2019;155:178-187.
- Patel KR, Immaneni S, Singam V, et al. Association between atopic dermatitis, depression, and suicidal ideation: a systematic review and meta-analysis [published online October 23, 2018]. J Am Acad Dermatol. 2019;80:402-410.
- Tracy A, Bhatti S, Eichenfield LF. Update on pediatric atopic dermatitis. Cutis. 2020;106:143-146.
Update on Pediatric Atopic Dermatitis
Atopic dermatitis (AD) is a chronic, pruritic, inflammatory skin disease that occurs most frequently in children but also affects many adolescents and adults. There has been a tremendous evolution of knowledge in AD, with insights into pathogenesis, epidemiology, impact of disease, and new therapies. A variety of studies examine the epidemiology of AD and associated comorbidities. The broad developments in disease state research are reflected in new publication numbers of AD citations on PubMed. A PubMed search of articles indexed for MEDLINE at the end of 2010 using the term atopic dermatitis would have shown 965 citations during the preceding 1-year period. In the 1-year period of June 2019 to June 2020, there were more than 2000 articles. The large body of research includes work of great significance in pediatric AD, and in this article we review recent findings that are important in understanding the progress being made in the field.
Epidemiology and Comorbidities
The epidemiology of AD has evolved over the last few decades, with emerging trends and novel insights into the burden of disease.1 In a recent cross-sectional study on the epidemiology of AD in children aged 6 to 11 years, the 1-year diagnosed AD prevalence estimates worldwide included the following: United States, 10.0%; Canada, 13.3%; the EU5 Countries, 15.5%; Japan, 10.3%; and all countries studied, 12.2%.2 Another recent paper that analyzed data from the Fragile Families and Child Wellbeing Study showed that the prevalence and persistence of AD in urban US children was 15.0%.3Although pediatric AD may spontaneously remit over time, disease continuing into adolescence and adulthood is common. Paternoster et al4 studied the longitudinal course of AD in children from 2 birth cohort prospective studies, showing distinct AD phenotypes having differing course trajectories over time. Disease subsets included patients with early-onset-persistent and early-onset-late-resolving disease.4 Whether phenotyping or subgroup analysis can be used to predict disease course or risk for development of comorbidities is unknown, but it is interesting to consider how such work could influence tailoring of specific therapies to early disease presentation.
Atopic dermatitis poses a serious public health burden owing to its high prevalence, considerable morbidity and disability, increased health care utilization, and cost of care.1 Recent studies have found notably higher rates of multiple medical and mental health comorbidities in both children and adults with AD, including infections, atopic comorbidities (eg, allergic rhinitis, asthma, food allergies), eye diseases (eg, keratitis, conjunctivitis, keratoconus), and possible cardiovascular diseases and autoimmune disorders.1,5-9 Allergic comorbidities are quite common in pediatric AD patients.10 In a recent study examining the efficacy and safety of dupilumab monotherapy in 251 adolescents with moderate to severe inadequately controlled AD, most had comorbid type 2 diseases including asthma (53.6%), food allergies (60.8%), and allergic rhinitis (65.6%).11
Quality of Life/Life Impact of AD
Pediatric AD has a major impact on the quality of life of patients and their families.12 The well-being and development of children are strongly influenced by the physical and psychosocial health of parents/guardians. Two studies by Ramirez and colleagues13,14 published in 2019 examined sleep disturbances and exhaustion in mothers of children with AD. Data for the studies came from the Avon Longitudinal Study of Parents and Children. Children with active AD reported worse sleep quality than those without AD, with nearly 50% higher odds of sleep-quality disturbances. Analysis of the cohort data from 11,649 mother-child pairs who were followed up with a time-varying measure of child AD activity and severity as well as self-reported maternal sleep measures repeated at multiple time points for children aged 6 months to 11 years showed that mothers of children with AD reported difficulty falling asleep, subjectively insufficient sleep, and daytime exhaustion throughout the first 11 years of childhood.13,14 These data suggest that sleep disturbance may be a family affair.
A cross-sectional, real-world study on the burden of AD in children aged 6 to 11 years assessed by self-report demonstrated a substantial and multidimensional impact of AD, including itch, sleep disturbance, skin pain, and health-related quality-of-life impact, as well as comorbidities and school productivity losses. The burden associated with AD was remarkable and increased with disease severity.15
Drucker et al16 completed a comprehensive literature review on the burden of AD, summarized as a report for the National Eczema Association. Quality-of-life impact on pediatric patients included high rates of emotional distress; social isolation; depression; limitations in activities due to lesions with fear of triggers; and behavioral problems such as irritability, crying, and sleep disturbance resulting in difficulty performing at school.16 The psychological impact on children as well as emotional and behavioral difficulties may impact the ability for parents/guardians to implement treatment plans.17
There is a striking association between mental health disorders and AD in the US pediatric population, with a clear dose-dependent relationship that has been observed between the prevalence of a mental health disorder and the reported severity of the skin disease. Data suggest children with AD may be at increased risk for developing mental health disorders. The National Survey of Children’s Health found statistically significant increases in the likelihood of attention deficit hyperactivity disorder (odds ratio [OR], 1.87), depression (OR, 1.81), anxiety (OR, 1.77), conduct disorder (OR, 1.87), and autism (OR, 3.04).6
Evolving Practices and Therapies
Bathing Practices
There has long been much controversy regarding best bathing habits for patients with AD. In a 2009 study, cutaneous hydration was quantified after various bathing and moisturizing regimens.18 The study showed clear benefits of emollient application on skin hydration, either after bathing or without bathing. Bathing followed by emollient applications did not decrease skin hydration in contrast to bathing without emollient application.18
There are limited studies evaluating bathing frequency in pediatric patients, and many families receive conflicting information regarding best practice. In one study that surveyed 354 parents, more than 75% of parents/guardians who had seen multiple providers for their child’s AD reported a substantial amount of confusion and frustration from conflicting advice on bathing frequency.19 Cardona et al20 undertook a randomized clinical trial of frequent bathing and moisturizing vs less-frequent bathing and moisturizing in pediatric patients with AD aged 6 months to 11 years. Patients were divided into 2 groups: 1 being bathed twice daily with immediate moisturizer application and the other being bathed twice weekly followed by moisturization, then a switch to the other method. Patients used standardized topical corticosteroids (TCSs) in both groups. There were significant improvements in scoring AD and other objective measures during the frequent bathing time period vs infrequent bathing; in the group that bathed more frequently, SCORAD (SCORing Atopic Dermatitis) decreased by 21.2 compared with the group that bathed less frequently (95% confidence interval, 14.9-27.6; P<.0001). These findings suggest that more-frequent bathing with immediate moisturization is superior as an acute treatment intervention for improving AD disease severity in comparison to less-frequent bathing with immediate moisturization.20
Expanding Treatment Options
Topical Phosphodiesterase Inhibitors
There are several new and evolving topical therapies in AD. Crisaborole ointment 2% is a steroid-free phosphodiesterase inhibitor approved in 2016 by the US Food and Drug Administration (FDA) for mild to moderate AD in patients aged 2 years and older. A recent multicenter, open-label, single-arm study in 137 infants (CrisADe CARE 1) evaluated the pharmacokinetics and efficacy of crisaborole ointment 2% applied twice daily for 4 weeks in pediatric patients aged 3 months to less than 24 months of age with mild to moderate AD.21 The study had 2 cohorts: one with a minimum of 5% body surface area involvement and another (the pharmacokinetic cohort) with a minimum of 35% body surface area involvement. Both cohorts demonstrated similar efficacy data. From baseline to day 29, the mean percentage change in eczema area and severity index (EASI) score was −57.5%, and an investigator global assessment (IGA) score of clear or almost clear with at least a 2-grade improvement was achieved in 30.2% of patients. Crisaborole systemic exposures in infants were comparable with those in patients aged 2 years or older. Patients tolerated crisaborole well, with a 4% rate of burning, which was similar to other studies in children and adults but perhaps lower than seen in clinical practice. Pharmacokinetic studies did not show any remarkable noticeable concern with accumulation of propylene glycol absorption.21
Based on the CrisADe CARE 1 study data, in March 2020 the FDA extended the indication of crisaborole ointment 2% from a prior lower age limit of 24 months to approval for use in treating mild to moderate AD in children as young as 3 months, making it the first nonsteroidal topical anti-inflammatory medication to be approved in children younger than 2 years in the United States.
Evolving Topical Therapies
Topical Janus Kinase Inhibitors
Ruxolitinib is a potent inhibitor of Janus kinase 1 (JAK-1) and Janus kinase 2 (JAK-2) and has been developed in topical formulations. In recent phase 3 clinical trials of patients with AD aged 12 years and older with mild to moderate disease (TRuE-AD1 and TRuE-AD2), more than half of the patients treated with either ruxolitinib cream in a 0.75% or 1.5% concentration reached EASI-75 after 8 weeks of treatment.22 Additionally, more patients treated with topical ruxolitinib reached an IGA score of clear to almost clear than patients treated with vehicle at the end of treatment. Thus far, it appears to be very well tolerated, significantly decreases EASI score (P<.0001), and improves overall pruritus.22
Delgocitinib is a topical pan-JAK inhibitor that blocks several cytokine-signaling cascade pathways. It was first developed and approved in Japan in an ointment formulation for use in patients with AD aged 16 years and older.23 The efficacy and safety profile of delgocitinib is currently being evaluated in pediatric patients with AD in Japan. In a recent phase 2 clinical study of 103 Japanese patients aged 2 to 15 years with moderate to severe AD, patients were randomized to receive either delgocitinib ointment in 0.25% or 0.5% concentrations or vehicle ointment twice daily for 4 weeks. The proportion of patients with a modified EASI-75 score was 38.2% (13/34) in the 0.25% group and 50.0% (17/34) in the 0.5% group vs 8.6% (3/35) in the placebo group. More patients treated with delgocitinib ointment received an IGA score of clear or almost clear than patients treated with vehicle at the end of treatment. Overall, both delgocitinib groups demonstrated superior improvement in clinical symptoms and signs without notable side effects.24
Tapinarof
Tapinarof is a topical therapeutic aryl hydrocarbon receptor agonist. In a recent phase 2 randomized study of 2 concentrations and 2 frequencies of tapinarof cream vs vehicle in 247 randomized patients aged 12 to 65 years with moderate to severe disease, tapinarof demonstrated greater success with both concentrations than vehicle at all visits beyond week 2.25 Additionally, in patients treated with tapinarof cream 1%, nearly 50% reached an IGA score of clear to almost clear with at least a 2-grade improvement. More than 50% of patients achieved EASI-75 improvement at 12 weeks of treatment with tapinarof cream 1% used daily. These findings suggest that tapinarof may be an efficacious and well-tolerated treatment for both adolescents and adults with AD; however, large confirmation trials are needed to further investigate.25
Systemic Treatments
Oral JAK Inhibitors
Some of the most exciting novel therapies include several oral JAK inhibitors that target different combinations of kinases and have been shown to decrease AD severity and symptoms. Some of these agents have indications in other disease states, such as baricitinib and upadacitinib, which are both FDA approved for the treatment of rheumatoid arthritis, whereas others, such as abrocitinib, have been studied specifically for AD.
Although some agents have only been studied in adults to date, others have included adolescents in their core studies, such as abrocitinib, which received Breakthrough Therapy designation from the FDA for the treatment of patients with moderate to severe AD in February 2018. In recent phase 3 trials of patients aged 12 years and older with moderate to severe AD (JADE MONO-1 and JADE MONO-2), both doses of abrocitinib improved the IGA and EASI-75 outcomes compared with placebo.26 Additional studies will be conducted to further investigate the relative efficacy and safety in patients younger than 18 years.
Biologics
Dupilumab is a fully human monoclonal antibody that inhibits IL-4 and IL-13 signaling without suppressing the immune system. It is approved for use in patients aged 12 years and older with moderate to severe asthma and in adults with chronic rhinosinusitis with nasal polyposis. It is the first biologic to show positive results in the moderate to severe pediatric AD population. There are now extended data available exhibiting sustained benefit in adolescent patients who were continued on dupilumab therapy, evidenced by further improvement in EASI scores at the 1-year mark.27
Recently, dupilumab received approval for use in patients aged 6 to 11 years, making it the first biologic for AD to be approved for use in patients younger than 12 years. The expedited FDA approval was based on the phase 3 results in which the efficacy and safety of dupilumab combined with TCSs were compared to TCSs alone (N=367).28 In this trial, more than twice as many children achieved clear or almost clear skin and more than 4 times as many achieved itch reduction with dupilumab plus TCSs than with TCSs alone. Three-quarters of patients receiving dupilumab at the subsequently approved dosing achieved at least a 75% improvement in overall disease.28 An additional study is being conducted that includes pediatric patients aged 6 months to younger than 6 years (ClinicalTrials.gov Identifier NCT03346434).
Future Directions in Pediatric AD
Our review summarizes only some of the agents under clinical investigation for use in pediatric AD. Early treatment to establish excellent long-term disease control with aggressive topical regimens or with systemic agents may alter the course of AD and influence the development of comorbidities, though this has not yet been shown in clinical studies. The long-term impact of early treatment, along with many other intriguing issues, will be studied more in the near future.
- Silverberg JI. Public health burden and epidemiology of atopic dermatitis. Dermatol Clin. 2017;35:283-289.
- Silverberg JI, Barbarot S, Gadkari A, et al. Epidemiology of atopic dermatitis in children aged 6–11 years: a cross-sectional study in the United States (US), Canada, Europe, and Japan. Paper presented at: American Academy of Dermatology Annual Meeting; March 20-24, 2020; Denver, CO.
- McKenzie C, Silverberg JI. The prevalence and persistence of atopic dermatitis in urban United States children. Ann Allergy Asthma Immunol. 2019;123:173-178.e1.
- Paternoster L, Savenije OEM, Heron J, et al. IJ Allergy Clin Immunol. 2018;141:964-971.
- Silverberg JI, Simpson EL. Association between severe eczema in children and multiple comorbid conditions and increased healthcare utilization. Pediatr Allergy Immunol. 2013;24:476-486.
- Yaghmaie P, Koudelka CW, Simpson Mental health comorbidity in patients with atopic dermatitis. J Allergy Clin Immunol. 2013;131:428-433.
- Narla S, Silverberg JI. Association between childhood atopic dermatitis and cutaneous, extracutaneous and systemic infections. Br J Dermatol. 2018;178:1467-1468.
- al. Incidence, prevalence, and risk of selected ocular disease in adults with atopic dermatitis. J Am Acad Dermatol. 2017;77:280-286.
- Association of atopic dermatitis with cardiovascular risk factors and diseases. J Invest Dermatol. 2017;137:1074-1081.
- Major comorbidities of atopic dermatitis: beyond allergic disorders. Am J Clin Dermatol. 2018;19:821-838.
- Efficacy and safety of dupilumab in adolescents with uncontrolled moderate to severe atopic dermatitis.
- Quality of life in families with children with atopic dermatitis. Pediatr Dermatol. 2016;33:28-32.
- Assessment of sleep disturbances and exhaustion in mothers of children with atopic dermatitis. JAMA Dermatol. 2019;155:556-563.
- Association of atopic dermatitis with sleep quality in children.
- Weidinger S, Simpson EL, Eckert L, et al. The patient-reported disease burden in pediatric patients with atopic dermatitis: a cross-sectional study in the United States (US), Canada, Europe, and Japan. Paperpresented at: American Academy of Dermatology Annual Meeting; March 20-24, 2020; Denver, CO.
- The burden of atopic dermatitis: summary of a report for the National Eczema Association. J Invest Dermatol. 2017;137:26-30.
- Mitchell AE. Bidirectional relationships between psychological health and dermatological conditions in children. Psychol Res Behav Manag. 2018;11:289-298.
- Chiang C, Eichenfield LF. Quantitative assessment of combination bathing and moisturizing regimens on skin hydration in atopic dermatitis. Pediatr Dermatol. 2009;26:273-278.
- Kempe E, Jain N, Cardona I. Bathing frequency recommendations for pediatric atopic dermatitis: are we adding to parental frustration? Ann Allergy Asthma Immunol. 2013;111:298‐299.
- Cardona ID, Kempe EE, Lary C, et al. Frequent versus infrequent bathing in pediatric atopic dermatitis: a randomized clinical trial. J Allergy Clin Immunol Pract. 2020;8:1014‐1021.
- Gower , Safety, effectiveness, and pharmacokinetics of crisaborole in infants aged 3 to <24 months with mild‐to‐moderate atopic dermatitis: a phase IV open‐label study (CrisADe CARE 1). Am J Clin Dermatol. 2020;21:275-284.
- Papp K, Szepietowski JC, Kircik L, et al. Efficacy and safety of ruxolitinib cream for the treatment atopic dermatitis: results from two phase 3, randomized, double-blind studies. Presented at: 2nd Annual Revolutionizing Atopic Dermatitis Conference; April 5, 2020; Chicago, IL.
- Dhillon S. Delgocitinib: first approval. Drugs. 2020;80:609‐615.
- Nakagawa H, Nemoto O, Igarashi A, et al. Phase 2 clinical study of delgocitinib ointment in pediatric patients with atopic dermatitis. J Allergy Clin Immunol. 2019;144:1575‐1583.
- Peppers J, Paller AS, Maeda-Chubachi T, et al. A phase 2, randomized dose-finding study of tapinarof (GSK2894512 cream) for the treatment of atopic dermatitis. J Am Acad Dermatol. 2019;80:89‐98.e3.
- Simpson EL, Sinclair R, Forman S, et al. Efficacy and safety of abrocitinib in adults and adolescents with moderate-to-severe atopic dermatitis (JADE MONO-1): a multicentre, double-blind, randomised, placebo-controlled, phase 3 trial. Lancet. 2020;396:255-266.
- Cork MJ, Thaçi D, Eichenfield LF, et al. Dupilumab in adolescents with uncontrolled moderate-to-severe atopic dermatitis: results from a phase IIa open-label trial and subsequent phase III open-label extension. Br J Dermatol. 2020;182:85‐96.
- Paller AS, Siegfried EC, Thaçi D, et al. Efficacy and safety of dupilumab with concomitant topical corticosteroids in children 6 to 11 years old with severe atopic dermatitis: a randomized, double-blinded, placebo-controlled phase 3 trial [published online June 20, 2020]. J Am Acad Dermatol. doi:10.1016/j.jaad.2020.06.054.
Atopic dermatitis (AD) is a chronic, pruritic, inflammatory skin disease that occurs most frequently in children but also affects many adolescents and adults. There has been a tremendous evolution of knowledge in AD, with insights into pathogenesis, epidemiology, impact of disease, and new therapies. A variety of studies examine the epidemiology of AD and associated comorbidities. The broad developments in disease state research are reflected in new publication numbers of AD citations on PubMed. A PubMed search of articles indexed for MEDLINE at the end of 2010 using the term atopic dermatitis would have shown 965 citations during the preceding 1-year period. In the 1-year period of June 2019 to June 2020, there were more than 2000 articles. The large body of research includes work of great significance in pediatric AD, and in this article we review recent findings that are important in understanding the progress being made in the field.
Epidemiology and Comorbidities
The epidemiology of AD has evolved over the last few decades, with emerging trends and novel insights into the burden of disease.1 In a recent cross-sectional study on the epidemiology of AD in children aged 6 to 11 years, the 1-year diagnosed AD prevalence estimates worldwide included the following: United States, 10.0%; Canada, 13.3%; the EU5 Countries, 15.5%; Japan, 10.3%; and all countries studied, 12.2%.2 Another recent paper that analyzed data from the Fragile Families and Child Wellbeing Study showed that the prevalence and persistence of AD in urban US children was 15.0%.3Although pediatric AD may spontaneously remit over time, disease continuing into adolescence and adulthood is common. Paternoster et al4 studied the longitudinal course of AD in children from 2 birth cohort prospective studies, showing distinct AD phenotypes having differing course trajectories over time. Disease subsets included patients with early-onset-persistent and early-onset-late-resolving disease.4 Whether phenotyping or subgroup analysis can be used to predict disease course or risk for development of comorbidities is unknown, but it is interesting to consider how such work could influence tailoring of specific therapies to early disease presentation.
Atopic dermatitis poses a serious public health burden owing to its high prevalence, considerable morbidity and disability, increased health care utilization, and cost of care.1 Recent studies have found notably higher rates of multiple medical and mental health comorbidities in both children and adults with AD, including infections, atopic comorbidities (eg, allergic rhinitis, asthma, food allergies), eye diseases (eg, keratitis, conjunctivitis, keratoconus), and possible cardiovascular diseases and autoimmune disorders.1,5-9 Allergic comorbidities are quite common in pediatric AD patients.10 In a recent study examining the efficacy and safety of dupilumab monotherapy in 251 adolescents with moderate to severe inadequately controlled AD, most had comorbid type 2 diseases including asthma (53.6%), food allergies (60.8%), and allergic rhinitis (65.6%).11
Quality of Life/Life Impact of AD
Pediatric AD has a major impact on the quality of life of patients and their families.12 The well-being and development of children are strongly influenced by the physical and psychosocial health of parents/guardians. Two studies by Ramirez and colleagues13,14 published in 2019 examined sleep disturbances and exhaustion in mothers of children with AD. Data for the studies came from the Avon Longitudinal Study of Parents and Children. Children with active AD reported worse sleep quality than those without AD, with nearly 50% higher odds of sleep-quality disturbances. Analysis of the cohort data from 11,649 mother-child pairs who were followed up with a time-varying measure of child AD activity and severity as well as self-reported maternal sleep measures repeated at multiple time points for children aged 6 months to 11 years showed that mothers of children with AD reported difficulty falling asleep, subjectively insufficient sleep, and daytime exhaustion throughout the first 11 years of childhood.13,14 These data suggest that sleep disturbance may be a family affair.
A cross-sectional, real-world study on the burden of AD in children aged 6 to 11 years assessed by self-report demonstrated a substantial and multidimensional impact of AD, including itch, sleep disturbance, skin pain, and health-related quality-of-life impact, as well as comorbidities and school productivity losses. The burden associated with AD was remarkable and increased with disease severity.15
Drucker et al16 completed a comprehensive literature review on the burden of AD, summarized as a report for the National Eczema Association. Quality-of-life impact on pediatric patients included high rates of emotional distress; social isolation; depression; limitations in activities due to lesions with fear of triggers; and behavioral problems such as irritability, crying, and sleep disturbance resulting in difficulty performing at school.16 The psychological impact on children as well as emotional and behavioral difficulties may impact the ability for parents/guardians to implement treatment plans.17
There is a striking association between mental health disorders and AD in the US pediatric population, with a clear dose-dependent relationship that has been observed between the prevalence of a mental health disorder and the reported severity of the skin disease. Data suggest children with AD may be at increased risk for developing mental health disorders. The National Survey of Children’s Health found statistically significant increases in the likelihood of attention deficit hyperactivity disorder (odds ratio [OR], 1.87), depression (OR, 1.81), anxiety (OR, 1.77), conduct disorder (OR, 1.87), and autism (OR, 3.04).6
Evolving Practices and Therapies
Bathing Practices
There has long been much controversy regarding best bathing habits for patients with AD. In a 2009 study, cutaneous hydration was quantified after various bathing and moisturizing regimens.18 The study showed clear benefits of emollient application on skin hydration, either after bathing or without bathing. Bathing followed by emollient applications did not decrease skin hydration in contrast to bathing without emollient application.18
There are limited studies evaluating bathing frequency in pediatric patients, and many families receive conflicting information regarding best practice. In one study that surveyed 354 parents, more than 75% of parents/guardians who had seen multiple providers for their child’s AD reported a substantial amount of confusion and frustration from conflicting advice on bathing frequency.19 Cardona et al20 undertook a randomized clinical trial of frequent bathing and moisturizing vs less-frequent bathing and moisturizing in pediatric patients with AD aged 6 months to 11 years. Patients were divided into 2 groups: 1 being bathed twice daily with immediate moisturizer application and the other being bathed twice weekly followed by moisturization, then a switch to the other method. Patients used standardized topical corticosteroids (TCSs) in both groups. There were significant improvements in scoring AD and other objective measures during the frequent bathing time period vs infrequent bathing; in the group that bathed more frequently, SCORAD (SCORing Atopic Dermatitis) decreased by 21.2 compared with the group that bathed less frequently (95% confidence interval, 14.9-27.6; P<.0001). These findings suggest that more-frequent bathing with immediate moisturization is superior as an acute treatment intervention for improving AD disease severity in comparison to less-frequent bathing with immediate moisturization.20
Expanding Treatment Options
Topical Phosphodiesterase Inhibitors
There are several new and evolving topical therapies in AD. Crisaborole ointment 2% is a steroid-free phosphodiesterase inhibitor approved in 2016 by the US Food and Drug Administration (FDA) for mild to moderate AD in patients aged 2 years and older. A recent multicenter, open-label, single-arm study in 137 infants (CrisADe CARE 1) evaluated the pharmacokinetics and efficacy of crisaborole ointment 2% applied twice daily for 4 weeks in pediatric patients aged 3 months to less than 24 months of age with mild to moderate AD.21 The study had 2 cohorts: one with a minimum of 5% body surface area involvement and another (the pharmacokinetic cohort) with a minimum of 35% body surface area involvement. Both cohorts demonstrated similar efficacy data. From baseline to day 29, the mean percentage change in eczema area and severity index (EASI) score was −57.5%, and an investigator global assessment (IGA) score of clear or almost clear with at least a 2-grade improvement was achieved in 30.2% of patients. Crisaborole systemic exposures in infants were comparable with those in patients aged 2 years or older. Patients tolerated crisaborole well, with a 4% rate of burning, which was similar to other studies in children and adults but perhaps lower than seen in clinical practice. Pharmacokinetic studies did not show any remarkable noticeable concern with accumulation of propylene glycol absorption.21
Based on the CrisADe CARE 1 study data, in March 2020 the FDA extended the indication of crisaborole ointment 2% from a prior lower age limit of 24 months to approval for use in treating mild to moderate AD in children as young as 3 months, making it the first nonsteroidal topical anti-inflammatory medication to be approved in children younger than 2 years in the United States.
Evolving Topical Therapies
Topical Janus Kinase Inhibitors
Ruxolitinib is a potent inhibitor of Janus kinase 1 (JAK-1) and Janus kinase 2 (JAK-2) and has been developed in topical formulations. In recent phase 3 clinical trials of patients with AD aged 12 years and older with mild to moderate disease (TRuE-AD1 and TRuE-AD2), more than half of the patients treated with either ruxolitinib cream in a 0.75% or 1.5% concentration reached EASI-75 after 8 weeks of treatment.22 Additionally, more patients treated with topical ruxolitinib reached an IGA score of clear to almost clear than patients treated with vehicle at the end of treatment. Thus far, it appears to be very well tolerated, significantly decreases EASI score (P<.0001), and improves overall pruritus.22
Delgocitinib is a topical pan-JAK inhibitor that blocks several cytokine-signaling cascade pathways. It was first developed and approved in Japan in an ointment formulation for use in patients with AD aged 16 years and older.23 The efficacy and safety profile of delgocitinib is currently being evaluated in pediatric patients with AD in Japan. In a recent phase 2 clinical study of 103 Japanese patients aged 2 to 15 years with moderate to severe AD, patients were randomized to receive either delgocitinib ointment in 0.25% or 0.5% concentrations or vehicle ointment twice daily for 4 weeks. The proportion of patients with a modified EASI-75 score was 38.2% (13/34) in the 0.25% group and 50.0% (17/34) in the 0.5% group vs 8.6% (3/35) in the placebo group. More patients treated with delgocitinib ointment received an IGA score of clear or almost clear than patients treated with vehicle at the end of treatment. Overall, both delgocitinib groups demonstrated superior improvement in clinical symptoms and signs without notable side effects.24
Tapinarof
Tapinarof is a topical therapeutic aryl hydrocarbon receptor agonist. In a recent phase 2 randomized study of 2 concentrations and 2 frequencies of tapinarof cream vs vehicle in 247 randomized patients aged 12 to 65 years with moderate to severe disease, tapinarof demonstrated greater success with both concentrations than vehicle at all visits beyond week 2.25 Additionally, in patients treated with tapinarof cream 1%, nearly 50% reached an IGA score of clear to almost clear with at least a 2-grade improvement. More than 50% of patients achieved EASI-75 improvement at 12 weeks of treatment with tapinarof cream 1% used daily. These findings suggest that tapinarof may be an efficacious and well-tolerated treatment for both adolescents and adults with AD; however, large confirmation trials are needed to further investigate.25
Systemic Treatments
Oral JAK Inhibitors
Some of the most exciting novel therapies include several oral JAK inhibitors that target different combinations of kinases and have been shown to decrease AD severity and symptoms. Some of these agents have indications in other disease states, such as baricitinib and upadacitinib, which are both FDA approved for the treatment of rheumatoid arthritis, whereas others, such as abrocitinib, have been studied specifically for AD.
Although some agents have only been studied in adults to date, others have included adolescents in their core studies, such as abrocitinib, which received Breakthrough Therapy designation from the FDA for the treatment of patients with moderate to severe AD in February 2018. In recent phase 3 trials of patients aged 12 years and older with moderate to severe AD (JADE MONO-1 and JADE MONO-2), both doses of abrocitinib improved the IGA and EASI-75 outcomes compared with placebo.26 Additional studies will be conducted to further investigate the relative efficacy and safety in patients younger than 18 years.
Biologics
Dupilumab is a fully human monoclonal antibody that inhibits IL-4 and IL-13 signaling without suppressing the immune system. It is approved for use in patients aged 12 years and older with moderate to severe asthma and in adults with chronic rhinosinusitis with nasal polyposis. It is the first biologic to show positive results in the moderate to severe pediatric AD population. There are now extended data available exhibiting sustained benefit in adolescent patients who were continued on dupilumab therapy, evidenced by further improvement in EASI scores at the 1-year mark.27
Recently, dupilumab received approval for use in patients aged 6 to 11 years, making it the first biologic for AD to be approved for use in patients younger than 12 years. The expedited FDA approval was based on the phase 3 results in which the efficacy and safety of dupilumab combined with TCSs were compared to TCSs alone (N=367).28 In this trial, more than twice as many children achieved clear or almost clear skin and more than 4 times as many achieved itch reduction with dupilumab plus TCSs than with TCSs alone. Three-quarters of patients receiving dupilumab at the subsequently approved dosing achieved at least a 75% improvement in overall disease.28 An additional study is being conducted that includes pediatric patients aged 6 months to younger than 6 years (ClinicalTrials.gov Identifier NCT03346434).
Future Directions in Pediatric AD
Our review summarizes only some of the agents under clinical investigation for use in pediatric AD. Early treatment to establish excellent long-term disease control with aggressive topical regimens or with systemic agents may alter the course of AD and influence the development of comorbidities, though this has not yet been shown in clinical studies. The long-term impact of early treatment, along with many other intriguing issues, will be studied more in the near future.
Atopic dermatitis (AD) is a chronic, pruritic, inflammatory skin disease that occurs most frequently in children but also affects many adolescents and adults. There has been a tremendous evolution of knowledge in AD, with insights into pathogenesis, epidemiology, impact of disease, and new therapies. A variety of studies examine the epidemiology of AD and associated comorbidities. The broad developments in disease state research are reflected in new publication numbers of AD citations on PubMed. A PubMed search of articles indexed for MEDLINE at the end of 2010 using the term atopic dermatitis would have shown 965 citations during the preceding 1-year period. In the 1-year period of June 2019 to June 2020, there were more than 2000 articles. The large body of research includes work of great significance in pediatric AD, and in this article we review recent findings that are important in understanding the progress being made in the field.
Epidemiology and Comorbidities
The epidemiology of AD has evolved over the last few decades, with emerging trends and novel insights into the burden of disease.1 In a recent cross-sectional study on the epidemiology of AD in children aged 6 to 11 years, the 1-year diagnosed AD prevalence estimates worldwide included the following: United States, 10.0%; Canada, 13.3%; the EU5 Countries, 15.5%; Japan, 10.3%; and all countries studied, 12.2%.2 Another recent paper that analyzed data from the Fragile Families and Child Wellbeing Study showed that the prevalence and persistence of AD in urban US children was 15.0%.3Although pediatric AD may spontaneously remit over time, disease continuing into adolescence and adulthood is common. Paternoster et al4 studied the longitudinal course of AD in children from 2 birth cohort prospective studies, showing distinct AD phenotypes having differing course trajectories over time. Disease subsets included patients with early-onset-persistent and early-onset-late-resolving disease.4 Whether phenotyping or subgroup analysis can be used to predict disease course or risk for development of comorbidities is unknown, but it is interesting to consider how such work could influence tailoring of specific therapies to early disease presentation.
Atopic dermatitis poses a serious public health burden owing to its high prevalence, considerable morbidity and disability, increased health care utilization, and cost of care.1 Recent studies have found notably higher rates of multiple medical and mental health comorbidities in both children and adults with AD, including infections, atopic comorbidities (eg, allergic rhinitis, asthma, food allergies), eye diseases (eg, keratitis, conjunctivitis, keratoconus), and possible cardiovascular diseases and autoimmune disorders.1,5-9 Allergic comorbidities are quite common in pediatric AD patients.10 In a recent study examining the efficacy and safety of dupilumab monotherapy in 251 adolescents with moderate to severe inadequately controlled AD, most had comorbid type 2 diseases including asthma (53.6%), food allergies (60.8%), and allergic rhinitis (65.6%).11
Quality of Life/Life Impact of AD
Pediatric AD has a major impact on the quality of life of patients and their families.12 The well-being and development of children are strongly influenced by the physical and psychosocial health of parents/guardians. Two studies by Ramirez and colleagues13,14 published in 2019 examined sleep disturbances and exhaustion in mothers of children with AD. Data for the studies came from the Avon Longitudinal Study of Parents and Children. Children with active AD reported worse sleep quality than those without AD, with nearly 50% higher odds of sleep-quality disturbances. Analysis of the cohort data from 11,649 mother-child pairs who were followed up with a time-varying measure of child AD activity and severity as well as self-reported maternal sleep measures repeated at multiple time points for children aged 6 months to 11 years showed that mothers of children with AD reported difficulty falling asleep, subjectively insufficient sleep, and daytime exhaustion throughout the first 11 years of childhood.13,14 These data suggest that sleep disturbance may be a family affair.
A cross-sectional, real-world study on the burden of AD in children aged 6 to 11 years assessed by self-report demonstrated a substantial and multidimensional impact of AD, including itch, sleep disturbance, skin pain, and health-related quality-of-life impact, as well as comorbidities and school productivity losses. The burden associated with AD was remarkable and increased with disease severity.15
Drucker et al16 completed a comprehensive literature review on the burden of AD, summarized as a report for the National Eczema Association. Quality-of-life impact on pediatric patients included high rates of emotional distress; social isolation; depression; limitations in activities due to lesions with fear of triggers; and behavioral problems such as irritability, crying, and sleep disturbance resulting in difficulty performing at school.16 The psychological impact on children as well as emotional and behavioral difficulties may impact the ability for parents/guardians to implement treatment plans.17
There is a striking association between mental health disorders and AD in the US pediatric population, with a clear dose-dependent relationship that has been observed between the prevalence of a mental health disorder and the reported severity of the skin disease. Data suggest children with AD may be at increased risk for developing mental health disorders. The National Survey of Children’s Health found statistically significant increases in the likelihood of attention deficit hyperactivity disorder (odds ratio [OR], 1.87), depression (OR, 1.81), anxiety (OR, 1.77), conduct disorder (OR, 1.87), and autism (OR, 3.04).6
Evolving Practices and Therapies
Bathing Practices
There has long been much controversy regarding best bathing habits for patients with AD. In a 2009 study, cutaneous hydration was quantified after various bathing and moisturizing regimens.18 The study showed clear benefits of emollient application on skin hydration, either after bathing or without bathing. Bathing followed by emollient applications did not decrease skin hydration in contrast to bathing without emollient application.18
There are limited studies evaluating bathing frequency in pediatric patients, and many families receive conflicting information regarding best practice. In one study that surveyed 354 parents, more than 75% of parents/guardians who had seen multiple providers for their child’s AD reported a substantial amount of confusion and frustration from conflicting advice on bathing frequency.19 Cardona et al20 undertook a randomized clinical trial of frequent bathing and moisturizing vs less-frequent bathing and moisturizing in pediatric patients with AD aged 6 months to 11 years. Patients were divided into 2 groups: 1 being bathed twice daily with immediate moisturizer application and the other being bathed twice weekly followed by moisturization, then a switch to the other method. Patients used standardized topical corticosteroids (TCSs) in both groups. There were significant improvements in scoring AD and other objective measures during the frequent bathing time period vs infrequent bathing; in the group that bathed more frequently, SCORAD (SCORing Atopic Dermatitis) decreased by 21.2 compared with the group that bathed less frequently (95% confidence interval, 14.9-27.6; P<.0001). These findings suggest that more-frequent bathing with immediate moisturization is superior as an acute treatment intervention for improving AD disease severity in comparison to less-frequent bathing with immediate moisturization.20
Expanding Treatment Options
Topical Phosphodiesterase Inhibitors
There are several new and evolving topical therapies in AD. Crisaborole ointment 2% is a steroid-free phosphodiesterase inhibitor approved in 2016 by the US Food and Drug Administration (FDA) for mild to moderate AD in patients aged 2 years and older. A recent multicenter, open-label, single-arm study in 137 infants (CrisADe CARE 1) evaluated the pharmacokinetics and efficacy of crisaborole ointment 2% applied twice daily for 4 weeks in pediatric patients aged 3 months to less than 24 months of age with mild to moderate AD.21 The study had 2 cohorts: one with a minimum of 5% body surface area involvement and another (the pharmacokinetic cohort) with a minimum of 35% body surface area involvement. Both cohorts demonstrated similar efficacy data. From baseline to day 29, the mean percentage change in eczema area and severity index (EASI) score was −57.5%, and an investigator global assessment (IGA) score of clear or almost clear with at least a 2-grade improvement was achieved in 30.2% of patients. Crisaborole systemic exposures in infants were comparable with those in patients aged 2 years or older. Patients tolerated crisaborole well, with a 4% rate of burning, which was similar to other studies in children and adults but perhaps lower than seen in clinical practice. Pharmacokinetic studies did not show any remarkable noticeable concern with accumulation of propylene glycol absorption.21
Based on the CrisADe CARE 1 study data, in March 2020 the FDA extended the indication of crisaborole ointment 2% from a prior lower age limit of 24 months to approval for use in treating mild to moderate AD in children as young as 3 months, making it the first nonsteroidal topical anti-inflammatory medication to be approved in children younger than 2 years in the United States.
Evolving Topical Therapies
Topical Janus Kinase Inhibitors
Ruxolitinib is a potent inhibitor of Janus kinase 1 (JAK-1) and Janus kinase 2 (JAK-2) and has been developed in topical formulations. In recent phase 3 clinical trials of patients with AD aged 12 years and older with mild to moderate disease (TRuE-AD1 and TRuE-AD2), more than half of the patients treated with either ruxolitinib cream in a 0.75% or 1.5% concentration reached EASI-75 after 8 weeks of treatment.22 Additionally, more patients treated with topical ruxolitinib reached an IGA score of clear to almost clear than patients treated with vehicle at the end of treatment. Thus far, it appears to be very well tolerated, significantly decreases EASI score (P<.0001), and improves overall pruritus.22
Delgocitinib is a topical pan-JAK inhibitor that blocks several cytokine-signaling cascade pathways. It was first developed and approved in Japan in an ointment formulation for use in patients with AD aged 16 years and older.23 The efficacy and safety profile of delgocitinib is currently being evaluated in pediatric patients with AD in Japan. In a recent phase 2 clinical study of 103 Japanese patients aged 2 to 15 years with moderate to severe AD, patients were randomized to receive either delgocitinib ointment in 0.25% or 0.5% concentrations or vehicle ointment twice daily for 4 weeks. The proportion of patients with a modified EASI-75 score was 38.2% (13/34) in the 0.25% group and 50.0% (17/34) in the 0.5% group vs 8.6% (3/35) in the placebo group. More patients treated with delgocitinib ointment received an IGA score of clear or almost clear than patients treated with vehicle at the end of treatment. Overall, both delgocitinib groups demonstrated superior improvement in clinical symptoms and signs without notable side effects.24
Tapinarof
Tapinarof is a topical therapeutic aryl hydrocarbon receptor agonist. In a recent phase 2 randomized study of 2 concentrations and 2 frequencies of tapinarof cream vs vehicle in 247 randomized patients aged 12 to 65 years with moderate to severe disease, tapinarof demonstrated greater success with both concentrations than vehicle at all visits beyond week 2.25 Additionally, in patients treated with tapinarof cream 1%, nearly 50% reached an IGA score of clear to almost clear with at least a 2-grade improvement. More than 50% of patients achieved EASI-75 improvement at 12 weeks of treatment with tapinarof cream 1% used daily. These findings suggest that tapinarof may be an efficacious and well-tolerated treatment for both adolescents and adults with AD; however, large confirmation trials are needed to further investigate.25
Systemic Treatments
Oral JAK Inhibitors
Some of the most exciting novel therapies include several oral JAK inhibitors that target different combinations of kinases and have been shown to decrease AD severity and symptoms. Some of these agents have indications in other disease states, such as baricitinib and upadacitinib, which are both FDA approved for the treatment of rheumatoid arthritis, whereas others, such as abrocitinib, have been studied specifically for AD.
Although some agents have only been studied in adults to date, others have included adolescents in their core studies, such as abrocitinib, which received Breakthrough Therapy designation from the FDA for the treatment of patients with moderate to severe AD in February 2018. In recent phase 3 trials of patients aged 12 years and older with moderate to severe AD (JADE MONO-1 and JADE MONO-2), both doses of abrocitinib improved the IGA and EASI-75 outcomes compared with placebo.26 Additional studies will be conducted to further investigate the relative efficacy and safety in patients younger than 18 years.
Biologics
Dupilumab is a fully human monoclonal antibody that inhibits IL-4 and IL-13 signaling without suppressing the immune system. It is approved for use in patients aged 12 years and older with moderate to severe asthma and in adults with chronic rhinosinusitis with nasal polyposis. It is the first biologic to show positive results in the moderate to severe pediatric AD population. There are now extended data available exhibiting sustained benefit in adolescent patients who were continued on dupilumab therapy, evidenced by further improvement in EASI scores at the 1-year mark.27
Recently, dupilumab received approval for use in patients aged 6 to 11 years, making it the first biologic for AD to be approved for use in patients younger than 12 years. The expedited FDA approval was based on the phase 3 results in which the efficacy and safety of dupilumab combined with TCSs were compared to TCSs alone (N=367).28 In this trial, more than twice as many children achieved clear or almost clear skin and more than 4 times as many achieved itch reduction with dupilumab plus TCSs than with TCSs alone. Three-quarters of patients receiving dupilumab at the subsequently approved dosing achieved at least a 75% improvement in overall disease.28 An additional study is being conducted that includes pediatric patients aged 6 months to younger than 6 years (ClinicalTrials.gov Identifier NCT03346434).
Future Directions in Pediatric AD
Our review summarizes only some of the agents under clinical investigation for use in pediatric AD. Early treatment to establish excellent long-term disease control with aggressive topical regimens or with systemic agents may alter the course of AD and influence the development of comorbidities, though this has not yet been shown in clinical studies. The long-term impact of early treatment, along with many other intriguing issues, will be studied more in the near future.
- Silverberg JI. Public health burden and epidemiology of atopic dermatitis. Dermatol Clin. 2017;35:283-289.
- Silverberg JI, Barbarot S, Gadkari A, et al. Epidemiology of atopic dermatitis in children aged 6–11 years: a cross-sectional study in the United States (US), Canada, Europe, and Japan. Paper presented at: American Academy of Dermatology Annual Meeting; March 20-24, 2020; Denver, CO.
- McKenzie C, Silverberg JI. The prevalence and persistence of atopic dermatitis in urban United States children. Ann Allergy Asthma Immunol. 2019;123:173-178.e1.
- Paternoster L, Savenije OEM, Heron J, et al. IJ Allergy Clin Immunol. 2018;141:964-971.
- Silverberg JI, Simpson EL. Association between severe eczema in children and multiple comorbid conditions and increased healthcare utilization. Pediatr Allergy Immunol. 2013;24:476-486.
- Yaghmaie P, Koudelka CW, Simpson Mental health comorbidity in patients with atopic dermatitis. J Allergy Clin Immunol. 2013;131:428-433.
- Narla S, Silverberg JI. Association between childhood atopic dermatitis and cutaneous, extracutaneous and systemic infections. Br J Dermatol. 2018;178:1467-1468.
- al. Incidence, prevalence, and risk of selected ocular disease in adults with atopic dermatitis. J Am Acad Dermatol. 2017;77:280-286.
- Association of atopic dermatitis with cardiovascular risk factors and diseases. J Invest Dermatol. 2017;137:1074-1081.
- Major comorbidities of atopic dermatitis: beyond allergic disorders. Am J Clin Dermatol. 2018;19:821-838.
- Efficacy and safety of dupilumab in adolescents with uncontrolled moderate to severe atopic dermatitis.
- Quality of life in families with children with atopic dermatitis. Pediatr Dermatol. 2016;33:28-32.
- Assessment of sleep disturbances and exhaustion in mothers of children with atopic dermatitis. JAMA Dermatol. 2019;155:556-563.
- Association of atopic dermatitis with sleep quality in children.
- Weidinger S, Simpson EL, Eckert L, et al. The patient-reported disease burden in pediatric patients with atopic dermatitis: a cross-sectional study in the United States (US), Canada, Europe, and Japan. Paperpresented at: American Academy of Dermatology Annual Meeting; March 20-24, 2020; Denver, CO.
- The burden of atopic dermatitis: summary of a report for the National Eczema Association. J Invest Dermatol. 2017;137:26-30.
- Mitchell AE. Bidirectional relationships between psychological health and dermatological conditions in children. Psychol Res Behav Manag. 2018;11:289-298.
- Chiang C, Eichenfield LF. Quantitative assessment of combination bathing and moisturizing regimens on skin hydration in atopic dermatitis. Pediatr Dermatol. 2009;26:273-278.
- Kempe E, Jain N, Cardona I. Bathing frequency recommendations for pediatric atopic dermatitis: are we adding to parental frustration? Ann Allergy Asthma Immunol. 2013;111:298‐299.
- Cardona ID, Kempe EE, Lary C, et al. Frequent versus infrequent bathing in pediatric atopic dermatitis: a randomized clinical trial. J Allergy Clin Immunol Pract. 2020;8:1014‐1021.
- Gower , Safety, effectiveness, and pharmacokinetics of crisaborole in infants aged 3 to <24 months with mild‐to‐moderate atopic dermatitis: a phase IV open‐label study (CrisADe CARE 1). Am J Clin Dermatol. 2020;21:275-284.
- Papp K, Szepietowski JC, Kircik L, et al. Efficacy and safety of ruxolitinib cream for the treatment atopic dermatitis: results from two phase 3, randomized, double-blind studies. Presented at: 2nd Annual Revolutionizing Atopic Dermatitis Conference; April 5, 2020; Chicago, IL.
- Dhillon S. Delgocitinib: first approval. Drugs. 2020;80:609‐615.
- Nakagawa H, Nemoto O, Igarashi A, et al. Phase 2 clinical study of delgocitinib ointment in pediatric patients with atopic dermatitis. J Allergy Clin Immunol. 2019;144:1575‐1583.
- Peppers J, Paller AS, Maeda-Chubachi T, et al. A phase 2, randomized dose-finding study of tapinarof (GSK2894512 cream) for the treatment of atopic dermatitis. J Am Acad Dermatol. 2019;80:89‐98.e3.
- Simpson EL, Sinclair R, Forman S, et al. Efficacy and safety of abrocitinib in adults and adolescents with moderate-to-severe atopic dermatitis (JADE MONO-1): a multicentre, double-blind, randomised, placebo-controlled, phase 3 trial. Lancet. 2020;396:255-266.
- Cork MJ, Thaçi D, Eichenfield LF, et al. Dupilumab in adolescents with uncontrolled moderate-to-severe atopic dermatitis: results from a phase IIa open-label trial and subsequent phase III open-label extension. Br J Dermatol. 2020;182:85‐96.
- Paller AS, Siegfried EC, Thaçi D, et al. Efficacy and safety of dupilumab with concomitant topical corticosteroids in children 6 to 11 years old with severe atopic dermatitis: a randomized, double-blinded, placebo-controlled phase 3 trial [published online June 20, 2020]. J Am Acad Dermatol. doi:10.1016/j.jaad.2020.06.054.
- Silverberg JI. Public health burden and epidemiology of atopic dermatitis. Dermatol Clin. 2017;35:283-289.
- Silverberg JI, Barbarot S, Gadkari A, et al. Epidemiology of atopic dermatitis in children aged 6–11 years: a cross-sectional study in the United States (US), Canada, Europe, and Japan. Paper presented at: American Academy of Dermatology Annual Meeting; March 20-24, 2020; Denver, CO.
- McKenzie C, Silverberg JI. The prevalence and persistence of atopic dermatitis in urban United States children. Ann Allergy Asthma Immunol. 2019;123:173-178.e1.
- Paternoster L, Savenije OEM, Heron J, et al. IJ Allergy Clin Immunol. 2018;141:964-971.
- Silverberg JI, Simpson EL. Association between severe eczema in children and multiple comorbid conditions and increased healthcare utilization. Pediatr Allergy Immunol. 2013;24:476-486.
- Yaghmaie P, Koudelka CW, Simpson Mental health comorbidity in patients with atopic dermatitis. J Allergy Clin Immunol. 2013;131:428-433.
- Narla S, Silverberg JI. Association between childhood atopic dermatitis and cutaneous, extracutaneous and systemic infections. Br J Dermatol. 2018;178:1467-1468.
- al. Incidence, prevalence, and risk of selected ocular disease in adults with atopic dermatitis. J Am Acad Dermatol. 2017;77:280-286.
- Association of atopic dermatitis with cardiovascular risk factors and diseases. J Invest Dermatol. 2017;137:1074-1081.
- Major comorbidities of atopic dermatitis: beyond allergic disorders. Am J Clin Dermatol. 2018;19:821-838.
- Efficacy and safety of dupilumab in adolescents with uncontrolled moderate to severe atopic dermatitis.
- Quality of life in families with children with atopic dermatitis. Pediatr Dermatol. 2016;33:28-32.
- Assessment of sleep disturbances and exhaustion in mothers of children with atopic dermatitis. JAMA Dermatol. 2019;155:556-563.
- Association of atopic dermatitis with sleep quality in children.
- Weidinger S, Simpson EL, Eckert L, et al. The patient-reported disease burden in pediatric patients with atopic dermatitis: a cross-sectional study in the United States (US), Canada, Europe, and Japan. Paperpresented at: American Academy of Dermatology Annual Meeting; March 20-24, 2020; Denver, CO.
- The burden of atopic dermatitis: summary of a report for the National Eczema Association. J Invest Dermatol. 2017;137:26-30.
- Mitchell AE. Bidirectional relationships between psychological health and dermatological conditions in children. Psychol Res Behav Manag. 2018;11:289-298.
- Chiang C, Eichenfield LF. Quantitative assessment of combination bathing and moisturizing regimens on skin hydration in atopic dermatitis. Pediatr Dermatol. 2009;26:273-278.
- Kempe E, Jain N, Cardona I. Bathing frequency recommendations for pediatric atopic dermatitis: are we adding to parental frustration? Ann Allergy Asthma Immunol. 2013;111:298‐299.
- Cardona ID, Kempe EE, Lary C, et al. Frequent versus infrequent bathing in pediatric atopic dermatitis: a randomized clinical trial. J Allergy Clin Immunol Pract. 2020;8:1014‐1021.
- Gower , Safety, effectiveness, and pharmacokinetics of crisaborole in infants aged 3 to <24 months with mild‐to‐moderate atopic dermatitis: a phase IV open‐label study (CrisADe CARE 1). Am J Clin Dermatol. 2020;21:275-284.
- Papp K, Szepietowski JC, Kircik L, et al. Efficacy and safety of ruxolitinib cream for the treatment atopic dermatitis: results from two phase 3, randomized, double-blind studies. Presented at: 2nd Annual Revolutionizing Atopic Dermatitis Conference; April 5, 2020; Chicago, IL.
- Dhillon S. Delgocitinib: first approval. Drugs. 2020;80:609‐615.
- Nakagawa H, Nemoto O, Igarashi A, et al. Phase 2 clinical study of delgocitinib ointment in pediatric patients with atopic dermatitis. J Allergy Clin Immunol. 2019;144:1575‐1583.
- Peppers J, Paller AS, Maeda-Chubachi T, et al. A phase 2, randomized dose-finding study of tapinarof (GSK2894512 cream) for the treatment of atopic dermatitis. J Am Acad Dermatol. 2019;80:89‐98.e3.
- Simpson EL, Sinclair R, Forman S, et al. Efficacy and safety of abrocitinib in adults and adolescents with moderate-to-severe atopic dermatitis (JADE MONO-1): a multicentre, double-blind, randomised, placebo-controlled, phase 3 trial. Lancet. 2020;396:255-266.
- Cork MJ, Thaçi D, Eichenfield LF, et al. Dupilumab in adolescents with uncontrolled moderate-to-severe atopic dermatitis: results from a phase IIa open-label trial and subsequent phase III open-label extension. Br J Dermatol. 2020;182:85‐96.
- Paller AS, Siegfried EC, Thaçi D, et al. Efficacy and safety of dupilumab with concomitant topical corticosteroids in children 6 to 11 years old with severe atopic dermatitis: a randomized, double-blinded, placebo-controlled phase 3 trial [published online June 20, 2020]. J Am Acad Dermatol. doi:10.1016/j.jaad.2020.06.054.
Practice Points
- There has been tremendous growth in our understanding of atopic dermatitis, with further insight into epidemiology, the impact on quality of life of affected individuals and their families, best bathing practices, and expanding treatment options.
- There are several novel topical and systemic agents recently approved and in late-stage clinical development programs that are evolving therapeutic approaches to pediatric disease.

4-year-old girl • limited movement & diffuse pain in both arms • pronated hands • Dx?
THE CASE
A 4-year-old girl was triaged to the Pediatric Emergency Department (PED) Fast Track, complaining of pain and limited movement in both arms. For an unknown reason, she had attempted to lift a heavy, 3-person sofa several hours earlier.
Her prior medical history included left nursemaid elbow (NME) at both 15 months and 33 months of age. Neither event had a known mechanism of injury. In both episodes, it was noted in the medical record that the child was not using her arm, “was holding it funny,” and was complaining of pain. Each time, she presented about 24 hours after symptom onset.
During the physical exam in the PED, the patient showed no signs of acute distress. She held both arms close to her body, with a slight flexion at the elbows, and her hands were pronated. She could not pinpoint the location of her discomfort and described diffuse pain in her forearms, elbows, and upper arms. Examination revealed no localized pain or tenderness in her hands, wrists, or clavicles. Radial pulses were easily palpated, and capillary refill was less than 2 seconds. There was no swelling or bruising. The rest of her physical exam was normal.
DIAGNOSIS
The patient was given a diagnosis of self-inflicted bilateral
DISCUSSION
BNME is an uncommon diagnosis; a literature review of reported cases indicates none were self-inflicted.1-4 However, NME is a common injury and is easily reduced. The classic mechanism of injury for NME involves the elbow in extension, while the forearm is pronated, and a sudden brisk axial traction is applied. This combination of motions causes the annular ligament to slip over the head of the radius and become displaced downward into the radiohumeral joint, where it becomes entrapped. In this case, the patient apparently exerted enough longitudinal traction while trying to lift the couch to produce the injury.
NME occurs most commonly in the left arm of girls between the ages of 4 months and 7 years and peaks at around the age of 2 years.5 A 2014 study by Irie et al6 corroborated the findings on left-side predominance and increased incidence with age, noting that frequency of injury peaked at 6 months in those younger than 1 year of age and at 2 years for those 1 year or older. However, the researchers found no significant sex difference.6
NME is radiographically indistinguishable from a healthy elbow.7 To prevent unnecessary expense and radiation exposure in young children, prereduction radiographs should only be used to rule out the possibility of fracture or other injury.7 Krul et al8 recommend restricting x-ray use to cases with an unclear history or those that are due to trauma other than an arm pull.
Continue to: Methods of reduction
Methods of reduction. Once NME is diagnosed, there are 2 methods of reduction: hyper-pronation and supination-flexion. Reduction is best performed with the child sitting in the parent’s lap with the injured arm facing the examiner.
Success rates for both methods of NME reduction are statistically similar; however, first-attempt success rates are significantly higher with the hyper-pronation method than with supination-flexion.9 Furthermore, physicians have deemed the hyper-pronation method significantly easier to perform than supination-flexion.9 A Cochrane review by Krul et al10 concluded that the hyper-pronation method may result in lower failure rates than supination-flexion, but due to limited evidence, the researchers were unable to draw any conclusions on other outcomes, such as pain. Green et al11 noted that hyper-pronation is perceived by parents of children with NME as being less painful. For these reasons, hyper-pronation should be utilized as the first method of reduction, followed by supination-flexion if the former does not work.12
Additional management. In a limited study of 50 children with pulled-elbow injuries, ultrasound revealed that 78% had an intact yet interposed radial annular ligament and 22% had a tear in the radial annular ligament.13 The authors propose that if, after appropriate reduction methods are attempted, no pop is felt, or there is no prompt clinical improvement, and ultrasound is not available to assess the integrity of the annular ligament, the child should be placed in a splint for 7 days
Our patient returned to the PED 3 days later, complaining of pain and an inability to move her left arm after her older sibling pulled her by her outstretched arms. She was once again diagnosed with NME, the injury was reduced, and she was using the arm within minutes. She has not presented to either the PED or the pediatric clinic with a similar complaint since. Discarding outliers, NME recurrence rates fall within a range of 23.7% to 32.9%.14,15
THE TAKEAWAY
Pre-reduction x-rays are not warranted in cases of NME unless there is suspicion for fracture or another injury. The 2 reduction methods, hyper-pronation and supination-flexion, are easily mastered. Any reduction should be quick, easy, and as painless as possible. Hyper-pronation should be utilized first, as this maneuver seems to be the more successful and is perceived by parents as being less painful. However, it is always most helpful to be proficient in both methods. If, after appropriate attempts at reduction, the child has not regained the use of the arm, 7 days of splinting is recommended, along with an orthopedic referral.
CORRESPONDENCE
Robert N. Anderson, DNP, APRN, (F)NP-C, ENP-BC, Vanderbilt Health, 512 Autumn Springs Court, Suite 100 C, Franklin, TN 37067; bob.anderson@vumc.org
1. Quan L, Marcuse EK. The epidemiology and treatment of radial head subluxation. Am J Dis Child. 1985;139:1194-1197.
2. Michaels MG. A case of bilateral nursemaid’s elbow. Pediatr Emerg Care. 1989;5:226-227.
3. Meiner EV, Sama AE, Lee DC, et al. Bilateral nursemaid’s elbow. Am J Emerg Med. 2004;6:502-503.
4. Wang YX, Zhang G, Song B, et al. Radial head subluxation in pediatric clinics and emergency departments in China. Chin J Traum. 2019;22:340-344.
5. Schunk JE. Radial head subluxation: epidemiology and treatment of 87 episodes. Ann Emerg Med. 1990;19:1019-1023.
6. Irie T, Sono T, Hayama Y, et al. Investigation on 2331 cases of pulled elbow over the last 10 years. Pediatr Rep. 2014;6:5090. doi: 10.4081/pr.2014.5090
7. Eismann EA, Cosco ED, Wall EJ. Absence of radiographic abnormalities in nursemaid’s elbows. J Pediatr Orthop. 2014;34:426-431.
8. Krul M, van der Wouden JC, Koes BW, et al. Nursemaid’s Elbow: its diagnostic clues and preferred means of reduction. J Fam Pract. 2010:59:E5-E7.
9. Bek D, Yildiz C, Köse O, et al. Pronation versus supination maneuvers for the reduction of ‘pulled elbow’: a randomized clinical trial. Eur J Emerg Med. 2009;16:135-138.
10. Krul M, van der Wouden JC, Kruithof EJ, et al. Manipulative interventions for reducing pulled elbow in young children. Cochrane Database Syst Rev. 2017.
11. Green DA, Linares MYR, Garcia Peña BM, et al. Randomized comparison of pain perception during radial head subluxation reduction using supination-flexion of forced pronation. Pediatr Emerg Care. 2006;22:235-238.
12. García-Mata S, Hidalgo-Ovejero A. Efficacy of reduction maneuvers for “pulled elbow” in children: a prospective study of 115 cases. J Pediatr Orthop. 2014;34:432-436.
13. Diab HS, Hamed MMS, Allam Y. Obscure pathology of pulled elbow: dynamic high-resolution ultrasound-assisted classification. J Child Orthop. 2010;4:539-543.
14. Teach SJ, Schutzman SA. Prospective study of recurrent radial head subluxation. Arch Pediatr Adolesc Med. 1996;150:164-166.
15. Macias CG, Bothner J, Wiebe R. Comparison of supination/flexion to hyperpronation in the reduction of radial head subluxation. Pediatrics. 1998;102:E10. doi: 10.1542/peds.102.1.e10.
THE CASE
A 4-year-old girl was triaged to the Pediatric Emergency Department (PED) Fast Track, complaining of pain and limited movement in both arms. For an unknown reason, she had attempted to lift a heavy, 3-person sofa several hours earlier.
Her prior medical history included left nursemaid elbow (NME) at both 15 months and 33 months of age. Neither event had a known mechanism of injury. In both episodes, it was noted in the medical record that the child was not using her arm, “was holding it funny,” and was complaining of pain. Each time, she presented about 24 hours after symptom onset.
During the physical exam in the PED, the patient showed no signs of acute distress. She held both arms close to her body, with a slight flexion at the elbows, and her hands were pronated. She could not pinpoint the location of her discomfort and described diffuse pain in her forearms, elbows, and upper arms. Examination revealed no localized pain or tenderness in her hands, wrists, or clavicles. Radial pulses were easily palpated, and capillary refill was less than 2 seconds. There was no swelling or bruising. The rest of her physical exam was normal.
DIAGNOSIS
The patient was given a diagnosis of self-inflicted bilateral
DISCUSSION
BNME is an uncommon diagnosis; a literature review of reported cases indicates none were self-inflicted.1-4 However, NME is a common injury and is easily reduced. The classic mechanism of injury for NME involves the elbow in extension, while the forearm is pronated, and a sudden brisk axial traction is applied. This combination of motions causes the annular ligament to slip over the head of the radius and become displaced downward into the radiohumeral joint, where it becomes entrapped. In this case, the patient apparently exerted enough longitudinal traction while trying to lift the couch to produce the injury.
NME occurs most commonly in the left arm of girls between the ages of 4 months and 7 years and peaks at around the age of 2 years.5 A 2014 study by Irie et al6 corroborated the findings on left-side predominance and increased incidence with age, noting that frequency of injury peaked at 6 months in those younger than 1 year of age and at 2 years for those 1 year or older. However, the researchers found no significant sex difference.6
NME is radiographically indistinguishable from a healthy elbow.7 To prevent unnecessary expense and radiation exposure in young children, prereduction radiographs should only be used to rule out the possibility of fracture or other injury.7 Krul et al8 recommend restricting x-ray use to cases with an unclear history or those that are due to trauma other than an arm pull.
Continue to: Methods of reduction
Methods of reduction. Once NME is diagnosed, there are 2 methods of reduction: hyper-pronation and supination-flexion. Reduction is best performed with the child sitting in the parent’s lap with the injured arm facing the examiner.
Success rates for both methods of NME reduction are statistically similar; however, first-attempt success rates are significantly higher with the hyper-pronation method than with supination-flexion.9 Furthermore, physicians have deemed the hyper-pronation method significantly easier to perform than supination-flexion.9 A Cochrane review by Krul et al10 concluded that the hyper-pronation method may result in lower failure rates than supination-flexion, but due to limited evidence, the researchers were unable to draw any conclusions on other outcomes, such as pain. Green et al11 noted that hyper-pronation is perceived by parents of children with NME as being less painful. For these reasons, hyper-pronation should be utilized as the first method of reduction, followed by supination-flexion if the former does not work.12
Additional management. In a limited study of 50 children with pulled-elbow injuries, ultrasound revealed that 78% had an intact yet interposed radial annular ligament and 22% had a tear in the radial annular ligament.13 The authors propose that if, after appropriate reduction methods are attempted, no pop is felt, or there is no prompt clinical improvement, and ultrasound is not available to assess the integrity of the annular ligament, the child should be placed in a splint for 7 days
Our patient returned to the PED 3 days later, complaining of pain and an inability to move her left arm after her older sibling pulled her by her outstretched arms. She was once again diagnosed with NME, the injury was reduced, and she was using the arm within minutes. She has not presented to either the PED or the pediatric clinic with a similar complaint since. Discarding outliers, NME recurrence rates fall within a range of 23.7% to 32.9%.14,15
THE TAKEAWAY
Pre-reduction x-rays are not warranted in cases of NME unless there is suspicion for fracture or another injury. The 2 reduction methods, hyper-pronation and supination-flexion, are easily mastered. Any reduction should be quick, easy, and as painless as possible. Hyper-pronation should be utilized first, as this maneuver seems to be the more successful and is perceived by parents as being less painful. However, it is always most helpful to be proficient in both methods. If, after appropriate attempts at reduction, the child has not regained the use of the arm, 7 days of splinting is recommended, along with an orthopedic referral.
CORRESPONDENCE
Robert N. Anderson, DNP, APRN, (F)NP-C, ENP-BC, Vanderbilt Health, 512 Autumn Springs Court, Suite 100 C, Franklin, TN 37067; bob.anderson@vumc.org
THE CASE
A 4-year-old girl was triaged to the Pediatric Emergency Department (PED) Fast Track, complaining of pain and limited movement in both arms. For an unknown reason, she had attempted to lift a heavy, 3-person sofa several hours earlier.
Her prior medical history included left nursemaid elbow (NME) at both 15 months and 33 months of age. Neither event had a known mechanism of injury. In both episodes, it was noted in the medical record that the child was not using her arm, “was holding it funny,” and was complaining of pain. Each time, she presented about 24 hours after symptom onset.
During the physical exam in the PED, the patient showed no signs of acute distress. She held both arms close to her body, with a slight flexion at the elbows, and her hands were pronated. She could not pinpoint the location of her discomfort and described diffuse pain in her forearms, elbows, and upper arms. Examination revealed no localized pain or tenderness in her hands, wrists, or clavicles. Radial pulses were easily palpated, and capillary refill was less than 2 seconds. There was no swelling or bruising. The rest of her physical exam was normal.
DIAGNOSIS
The patient was given a diagnosis of self-inflicted bilateral
DISCUSSION
BNME is an uncommon diagnosis; a literature review of reported cases indicates none were self-inflicted.1-4 However, NME is a common injury and is easily reduced. The classic mechanism of injury for NME involves the elbow in extension, while the forearm is pronated, and a sudden brisk axial traction is applied. This combination of motions causes the annular ligament to slip over the head of the radius and become displaced downward into the radiohumeral joint, where it becomes entrapped. In this case, the patient apparently exerted enough longitudinal traction while trying to lift the couch to produce the injury.
NME occurs most commonly in the left arm of girls between the ages of 4 months and 7 years and peaks at around the age of 2 years.5 A 2014 study by Irie et al6 corroborated the findings on left-side predominance and increased incidence with age, noting that frequency of injury peaked at 6 months in those younger than 1 year of age and at 2 years for those 1 year or older. However, the researchers found no significant sex difference.6
NME is radiographically indistinguishable from a healthy elbow.7 To prevent unnecessary expense and radiation exposure in young children, prereduction radiographs should only be used to rule out the possibility of fracture or other injury.7 Krul et al8 recommend restricting x-ray use to cases with an unclear history or those that are due to trauma other than an arm pull.
Continue to: Methods of reduction
Methods of reduction. Once NME is diagnosed, there are 2 methods of reduction: hyper-pronation and supination-flexion. Reduction is best performed with the child sitting in the parent’s lap with the injured arm facing the examiner.
Success rates for both methods of NME reduction are statistically similar; however, first-attempt success rates are significantly higher with the hyper-pronation method than with supination-flexion.9 Furthermore, physicians have deemed the hyper-pronation method significantly easier to perform than supination-flexion.9 A Cochrane review by Krul et al10 concluded that the hyper-pronation method may result in lower failure rates than supination-flexion, but due to limited evidence, the researchers were unable to draw any conclusions on other outcomes, such as pain. Green et al11 noted that hyper-pronation is perceived by parents of children with NME as being less painful. For these reasons, hyper-pronation should be utilized as the first method of reduction, followed by supination-flexion if the former does not work.12
Additional management. In a limited study of 50 children with pulled-elbow injuries, ultrasound revealed that 78% had an intact yet interposed radial annular ligament and 22% had a tear in the radial annular ligament.13 The authors propose that if, after appropriate reduction methods are attempted, no pop is felt, or there is no prompt clinical improvement, and ultrasound is not available to assess the integrity of the annular ligament, the child should be placed in a splint for 7 days
Our patient returned to the PED 3 days later, complaining of pain and an inability to move her left arm after her older sibling pulled her by her outstretched arms. She was once again diagnosed with NME, the injury was reduced, and she was using the arm within minutes. She has not presented to either the PED or the pediatric clinic with a similar complaint since. Discarding outliers, NME recurrence rates fall within a range of 23.7% to 32.9%.14,15
THE TAKEAWAY
Pre-reduction x-rays are not warranted in cases of NME unless there is suspicion for fracture or another injury. The 2 reduction methods, hyper-pronation and supination-flexion, are easily mastered. Any reduction should be quick, easy, and as painless as possible. Hyper-pronation should be utilized first, as this maneuver seems to be the more successful and is perceived by parents as being less painful. However, it is always most helpful to be proficient in both methods. If, after appropriate attempts at reduction, the child has not regained the use of the arm, 7 days of splinting is recommended, along with an orthopedic referral.
CORRESPONDENCE
Robert N. Anderson, DNP, APRN, (F)NP-C, ENP-BC, Vanderbilt Health, 512 Autumn Springs Court, Suite 100 C, Franklin, TN 37067; bob.anderson@vumc.org
1. Quan L, Marcuse EK. The epidemiology and treatment of radial head subluxation. Am J Dis Child. 1985;139:1194-1197.
2. Michaels MG. A case of bilateral nursemaid’s elbow. Pediatr Emerg Care. 1989;5:226-227.
3. Meiner EV, Sama AE, Lee DC, et al. Bilateral nursemaid’s elbow. Am J Emerg Med. 2004;6:502-503.
4. Wang YX, Zhang G, Song B, et al. Radial head subluxation in pediatric clinics and emergency departments in China. Chin J Traum. 2019;22:340-344.
5. Schunk JE. Radial head subluxation: epidemiology and treatment of 87 episodes. Ann Emerg Med. 1990;19:1019-1023.
6. Irie T, Sono T, Hayama Y, et al. Investigation on 2331 cases of pulled elbow over the last 10 years. Pediatr Rep. 2014;6:5090. doi: 10.4081/pr.2014.5090
7. Eismann EA, Cosco ED, Wall EJ. Absence of radiographic abnormalities in nursemaid’s elbows. J Pediatr Orthop. 2014;34:426-431.
8. Krul M, van der Wouden JC, Koes BW, et al. Nursemaid’s Elbow: its diagnostic clues and preferred means of reduction. J Fam Pract. 2010:59:E5-E7.
9. Bek D, Yildiz C, Köse O, et al. Pronation versus supination maneuvers for the reduction of ‘pulled elbow’: a randomized clinical trial. Eur J Emerg Med. 2009;16:135-138.
10. Krul M, van der Wouden JC, Kruithof EJ, et al. Manipulative interventions for reducing pulled elbow in young children. Cochrane Database Syst Rev. 2017.
11. Green DA, Linares MYR, Garcia Peña BM, et al. Randomized comparison of pain perception during radial head subluxation reduction using supination-flexion of forced pronation. Pediatr Emerg Care. 2006;22:235-238.
12. García-Mata S, Hidalgo-Ovejero A. Efficacy of reduction maneuvers for “pulled elbow” in children: a prospective study of 115 cases. J Pediatr Orthop. 2014;34:432-436.
13. Diab HS, Hamed MMS, Allam Y. Obscure pathology of pulled elbow: dynamic high-resolution ultrasound-assisted classification. J Child Orthop. 2010;4:539-543.
14. Teach SJ, Schutzman SA. Prospective study of recurrent radial head subluxation. Arch Pediatr Adolesc Med. 1996;150:164-166.
15. Macias CG, Bothner J, Wiebe R. Comparison of supination/flexion to hyperpronation in the reduction of radial head subluxation. Pediatrics. 1998;102:E10. doi: 10.1542/peds.102.1.e10.
1. Quan L, Marcuse EK. The epidemiology and treatment of radial head subluxation. Am J Dis Child. 1985;139:1194-1197.
2. Michaels MG. A case of bilateral nursemaid’s elbow. Pediatr Emerg Care. 1989;5:226-227.
3. Meiner EV, Sama AE, Lee DC, et al. Bilateral nursemaid’s elbow. Am J Emerg Med. 2004;6:502-503.
4. Wang YX, Zhang G, Song B, et al. Radial head subluxation in pediatric clinics and emergency departments in China. Chin J Traum. 2019;22:340-344.
5. Schunk JE. Radial head subluxation: epidemiology and treatment of 87 episodes. Ann Emerg Med. 1990;19:1019-1023.
6. Irie T, Sono T, Hayama Y, et al. Investigation on 2331 cases of pulled elbow over the last 10 years. Pediatr Rep. 2014;6:5090. doi: 10.4081/pr.2014.5090
7. Eismann EA, Cosco ED, Wall EJ. Absence of radiographic abnormalities in nursemaid’s elbows. J Pediatr Orthop. 2014;34:426-431.
8. Krul M, van der Wouden JC, Koes BW, et al. Nursemaid’s Elbow: its diagnostic clues and preferred means of reduction. J Fam Pract. 2010:59:E5-E7.
9. Bek D, Yildiz C, Köse O, et al. Pronation versus supination maneuvers for the reduction of ‘pulled elbow’: a randomized clinical trial. Eur J Emerg Med. 2009;16:135-138.
10. Krul M, van der Wouden JC, Kruithof EJ, et al. Manipulative interventions for reducing pulled elbow in young children. Cochrane Database Syst Rev. 2017.
11. Green DA, Linares MYR, Garcia Peña BM, et al. Randomized comparison of pain perception during radial head subluxation reduction using supination-flexion of forced pronation. Pediatr Emerg Care. 2006;22:235-238.
12. García-Mata S, Hidalgo-Ovejero A. Efficacy of reduction maneuvers for “pulled elbow” in children: a prospective study of 115 cases. J Pediatr Orthop. 2014;34:432-436.
13. Diab HS, Hamed MMS, Allam Y. Obscure pathology of pulled elbow: dynamic high-resolution ultrasound-assisted classification. J Child Orthop. 2010;4:539-543.
14. Teach SJ, Schutzman SA. Prospective study of recurrent radial head subluxation. Arch Pediatr Adolesc Med. 1996;150:164-166.
15. Macias CG, Bothner J, Wiebe R. Comparison of supination/flexion to hyperpronation in the reduction of radial head subluxation. Pediatrics. 1998;102:E10. doi: 10.1542/peds.102.1.e10.

One in seven high schoolers is misusing opioids
according to an analysis from the Centers for Disease Control and Prevention.
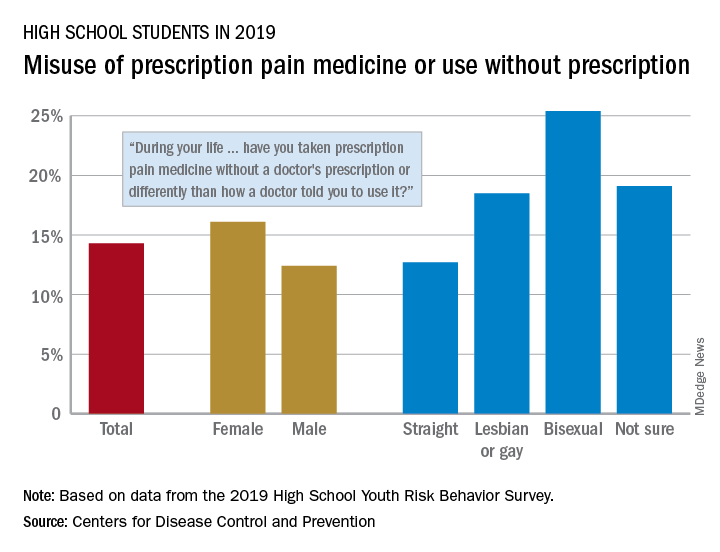
That type of opioid use/misuse, reported by 14.3% of respondents to the 2019 Youth Risk Behavior Survey, was more common among females (16.1%) than males (12.4%) and even more prevalent among nonheterosexuals and those who are unsure about their sexual identity, Christopher M. Jones, PharmD, DrPH, and associates at the CDC said in the Morbidity and Mortality Weekly Report.
The YRBS data show that 18.5% of gay or lesbian students had, at some point in their lives, used a prescription opioid differently than a physician had told them to or taken one without a prescription. That figure was slightly higher (19.1%) for those unsure of their sexual identity, considerably higher (25.4%) for bisexuals, and lower for heterosexuals (12.7%), they reported.
The pattern for current use/misuse of opioids, defined as use one or more times in the 30 days before the survey, was similar to ever use but somewhat less pronounced in 2019. Prevalence was 7.2% for all students in grades 9-12, 8.3% for females, and 6.1% for males. By sexual identity, prevalence was 6.4% for heterosexuals, 7.6% for gays or lesbians, 11.5% for those unsure about their sexual identity, and 13.1% for bisexuals, based on the YRBS data.
This increased misuse of opioids among sexual minority youths, “even after controlling for other demographic and substance use characteristics ... emphasizes the importance of identifying tailored prevention strategies to address disparities among this vulnerable population,” the CDC researchers wrote.
SOURCE: Jones CM et al. MMWR Suppl. 2020 Aug 21;69(1):38-46.
according to an analysis from the Centers for Disease Control and Prevention.
That type of opioid use/misuse, reported by 14.3% of respondents to the 2019 Youth Risk Behavior Survey, was more common among females (16.1%) than males (12.4%) and even more prevalent among nonheterosexuals and those who are unsure about their sexual identity, Christopher M. Jones, PharmD, DrPH, and associates at the CDC said in the Morbidity and Mortality Weekly Report.
The YRBS data show that 18.5% of gay or lesbian students had, at some point in their lives, used a prescription opioid differently than a physician had told them to or taken one without a prescription. That figure was slightly higher (19.1%) for those unsure of their sexual identity, considerably higher (25.4%) for bisexuals, and lower for heterosexuals (12.7%), they reported.
The pattern for current use/misuse of opioids, defined as use one or more times in the 30 days before the survey, was similar to ever use but somewhat less pronounced in 2019. Prevalence was 7.2% for all students in grades 9-12, 8.3% for females, and 6.1% for males. By sexual identity, prevalence was 6.4% for heterosexuals, 7.6% for gays or lesbians, 11.5% for those unsure about their sexual identity, and 13.1% for bisexuals, based on the YRBS data.
This increased misuse of opioids among sexual minority youths, “even after controlling for other demographic and substance use characteristics ... emphasizes the importance of identifying tailored prevention strategies to address disparities among this vulnerable population,” the CDC researchers wrote.
SOURCE: Jones CM et al. MMWR Suppl. 2020 Aug 21;69(1):38-46.
according to an analysis from the Centers for Disease Control and Prevention.
That type of opioid use/misuse, reported by 14.3% of respondents to the 2019 Youth Risk Behavior Survey, was more common among females (16.1%) than males (12.4%) and even more prevalent among nonheterosexuals and those who are unsure about their sexual identity, Christopher M. Jones, PharmD, DrPH, and associates at the CDC said in the Morbidity and Mortality Weekly Report.
The YRBS data show that 18.5% of gay or lesbian students had, at some point in their lives, used a prescription opioid differently than a physician had told them to or taken one without a prescription. That figure was slightly higher (19.1%) for those unsure of their sexual identity, considerably higher (25.4%) for bisexuals, and lower for heterosexuals (12.7%), they reported.
The pattern for current use/misuse of opioids, defined as use one or more times in the 30 days before the survey, was similar to ever use but somewhat less pronounced in 2019. Prevalence was 7.2% for all students in grades 9-12, 8.3% for females, and 6.1% for males. By sexual identity, prevalence was 6.4% for heterosexuals, 7.6% for gays or lesbians, 11.5% for those unsure about their sexual identity, and 13.1% for bisexuals, based on the YRBS data.
This increased misuse of opioids among sexual minority youths, “even after controlling for other demographic and substance use characteristics ... emphasizes the importance of identifying tailored prevention strategies to address disparities among this vulnerable population,” the CDC researchers wrote.
SOURCE: Jones CM et al. MMWR Suppl. 2020 Aug 21;69(1):38-46.
FROM MMWR
U.S. tops 500,000 COVID-19 cases in children
according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
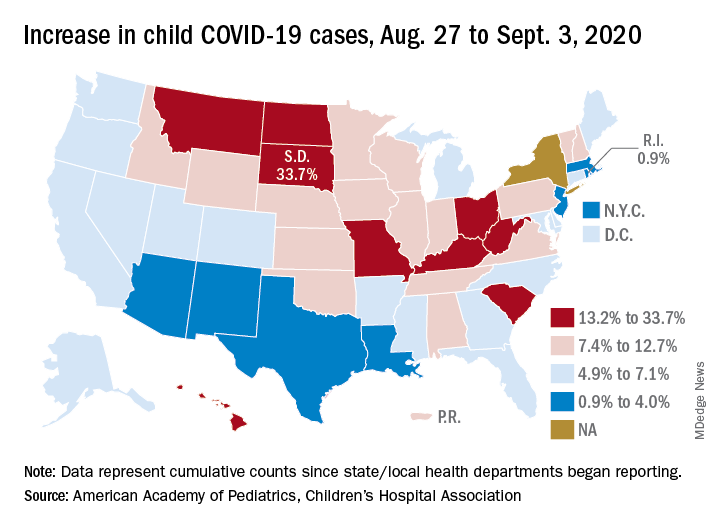
States have reported 513,415 cases of COVID-19 in children since the beginning of the pandemic, with almost 37,000 coming in the last week, the AAP and the CHA said Sept. 8 in the weekly report. That figure includes New York City – the rest of New York State is not reporting ages for COVID-19 patients – as well as Puerto Rico, the District of Columbia, and Guam.
“These numbers are a chilling reminder of why we need to take this virus seriously,” AAP President Sara Goza, MD, said in a written statement.
Children now represent 9.8% of the almost 5.3 million cases that have been reported in Americans of all ages. The proportion of child cases has continued to increase as the pandemic has progressed – it was 8.0% as of mid-July and 5.2% in early June, the data show.
“Throughout the summer, surges in the virus have occurred in Southern, Western, and Midwestern states,” the AAP statement said.
The latest AAP/CHA report shows that, from Aug. 27 to Sept. 3, the total number of child cases jumped by 33.7% in South Dakota, more than any other state. North Dakota was next at 22.7%, followed by Hawaii (18.1%), Missouri (16.8%), and Kentucky (16.4%).
“This rapid rise in positive cases occurred over the summer, and as the weather cools, we know people will spend more time indoors,” said Sean O’Leary, MD, MPH, vice chair of the AAP Committee on Infectious Diseases. “The goal is to get children back into schools for in-person learning, but in many communities, this is not possible as the virus spreads unchecked.”
The smallest increase over the last week, just 0.9%, came in Rhode Island, with Massachusetts just a bit higher at 1.0%. Also at the low end of the increase scale are Arizona (3.3%) and Louisiana (4.0%), two states that have very high rates of cumulative cases: 1,380 per 100,000 children for Arizona and 1,234 per 100,000 for Louisiana, the report said.
To give those figures some context, Tennessee has the highest cumulative count of any state at 1,553 cases per 100,000 children and Vermont has the lowest at 151, based on the data gathered by the AAP and CHA.
“While much remains unknown about COVID-19, we do know that the spread among children reflects what is happening in the broader communities. A disproportionate number of cases are reported in Black and Hispanic children and in places where there is high poverty. We must work harder to address societal inequities that contribute to these disparities,” Dr. Goza said.
according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
States have reported 513,415 cases of COVID-19 in children since the beginning of the pandemic, with almost 37,000 coming in the last week, the AAP and the CHA said Sept. 8 in the weekly report. That figure includes New York City – the rest of New York State is not reporting ages for COVID-19 patients – as well as Puerto Rico, the District of Columbia, and Guam.
“These numbers are a chilling reminder of why we need to take this virus seriously,” AAP President Sara Goza, MD, said in a written statement.
Children now represent 9.8% of the almost 5.3 million cases that have been reported in Americans of all ages. The proportion of child cases has continued to increase as the pandemic has progressed – it was 8.0% as of mid-July and 5.2% in early June, the data show.
“Throughout the summer, surges in the virus have occurred in Southern, Western, and Midwestern states,” the AAP statement said.
The latest AAP/CHA report shows that, from Aug. 27 to Sept. 3, the total number of child cases jumped by 33.7% in South Dakota, more than any other state. North Dakota was next at 22.7%, followed by Hawaii (18.1%), Missouri (16.8%), and Kentucky (16.4%).
“This rapid rise in positive cases occurred over the summer, and as the weather cools, we know people will spend more time indoors,” said Sean O’Leary, MD, MPH, vice chair of the AAP Committee on Infectious Diseases. “The goal is to get children back into schools for in-person learning, but in many communities, this is not possible as the virus spreads unchecked.”
The smallest increase over the last week, just 0.9%, came in Rhode Island, with Massachusetts just a bit higher at 1.0%. Also at the low end of the increase scale are Arizona (3.3%) and Louisiana (4.0%), two states that have very high rates of cumulative cases: 1,380 per 100,000 children for Arizona and 1,234 per 100,000 for Louisiana, the report said.
To give those figures some context, Tennessee has the highest cumulative count of any state at 1,553 cases per 100,000 children and Vermont has the lowest at 151, based on the data gathered by the AAP and CHA.
“While much remains unknown about COVID-19, we do know that the spread among children reflects what is happening in the broader communities. A disproportionate number of cases are reported in Black and Hispanic children and in places where there is high poverty. We must work harder to address societal inequities that contribute to these disparities,” Dr. Goza said.
according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
States have reported 513,415 cases of COVID-19 in children since the beginning of the pandemic, with almost 37,000 coming in the last week, the AAP and the CHA said Sept. 8 in the weekly report. That figure includes New York City – the rest of New York State is not reporting ages for COVID-19 patients – as well as Puerto Rico, the District of Columbia, and Guam.
“These numbers are a chilling reminder of why we need to take this virus seriously,” AAP President Sara Goza, MD, said in a written statement.
Children now represent 9.8% of the almost 5.3 million cases that have been reported in Americans of all ages. The proportion of child cases has continued to increase as the pandemic has progressed – it was 8.0% as of mid-July and 5.2% in early June, the data show.
“Throughout the summer, surges in the virus have occurred in Southern, Western, and Midwestern states,” the AAP statement said.
The latest AAP/CHA report shows that, from Aug. 27 to Sept. 3, the total number of child cases jumped by 33.7% in South Dakota, more than any other state. North Dakota was next at 22.7%, followed by Hawaii (18.1%), Missouri (16.8%), and Kentucky (16.4%).
“This rapid rise in positive cases occurred over the summer, and as the weather cools, we know people will spend more time indoors,” said Sean O’Leary, MD, MPH, vice chair of the AAP Committee on Infectious Diseases. “The goal is to get children back into schools for in-person learning, but in many communities, this is not possible as the virus spreads unchecked.”
The smallest increase over the last week, just 0.9%, came in Rhode Island, with Massachusetts just a bit higher at 1.0%. Also at the low end of the increase scale are Arizona (3.3%) and Louisiana (4.0%), two states that have very high rates of cumulative cases: 1,380 per 100,000 children for Arizona and 1,234 per 100,000 for Louisiana, the report said.
To give those figures some context, Tennessee has the highest cumulative count of any state at 1,553 cases per 100,000 children and Vermont has the lowest at 151, based on the data gathered by the AAP and CHA.
“While much remains unknown about COVID-19, we do know that the spread among children reflects what is happening in the broader communities. A disproportionate number of cases are reported in Black and Hispanic children and in places where there is high poverty. We must work harder to address societal inequities that contribute to these disparities,” Dr. Goza said.