User login
Michigan police receive training to recognize mental illness
Responding to a police call can prove dangerous. In those kinds of high-pressure situations, agitation or other manifestations of mental illness might be mistaken for violent intent – with disastrous results.

In Kalamazoo, Mich., crime response training now includes subduing suspects without using violent force. “Through training and education, and scenarios that we use in the training, [the officers] start to detect the different cues or indicators where they start to see that this is really a crisis event. And we treat it as a medical issue and get that person the help that they need,” said Rafael Diaz, executive lieutenant with the Kalamazoo Department of Public Safety in an interview on Michigan NPR.
In the training, called the Crisis Intervention Team model, the goal is to slow down the pace of the interaction and keep some distance between themselves and the suspect after officers recognize signs of mental illness. Both responses can lower the chances of a lash-out response.
“The number of injuries to officers goes down, the number of injuries to the person in crisis goes down, and there is a huge benefit to society there if you don’t have to use physical force,” Mr. Diaz said.
Animal neglect and mental health
Images of neglected and abused livestock on farms can inspire thoughts of how someone could mistreat the animals in their care. “Frankly, if you can’t understand that, it’s probably a good thing. It means you haven’t been in the depths of low, low mental health, depression, and anxiety,” Andria Jones-Bitton, DVM, PhD, said in an interview with the Western Producer.
Dr. Jones-Bitton is a veterinarian and epidemiologist at the Ontario Veterinary College in Guelph. She is studying the mental health and mental resilience of farmers and veterinarians.
“If farmers are struggling with their own well-being and motivation, they’re likely going to find it difficult to invest in improving animal welfare. When we’re mentally unwell, it’s hard to care for ourselves, let alone to care for others, even when those others are really important to us,” she said.
A national survey of Canadian farmers by Dr. Jones-Bitton showed high levels of stress and diminished ability to cope with the pressures that come with running a livestock farm. “What makes me the most upset is I have everything I’ve ever dreamed of – love, family, and a farm, and all I feel is overwhelmed out of control and sad,” one respondent said.
The problems are not unique to Canada. Studies from Ireland, for example, documented an association between animal neglect cases and the mental health, drug/alcohol addiction, and social problems of farmers.
“Even if you didn’t care about the humans that were struggling and you only cared about the animal welfare, you’d be wise to address the issue of farmer stress,” Dr. Jones-Britton said.
Depression and rural America
A recent “Farming in Tough Times” workshop that convened in Minnesota focused on the mental health of farmers. Making a living is challenging for many reasons. One is that prices for commodities are set by others.
“I realized that I can’t change the situation that we’re in. I can’t change milk prices. I can’t stop farms from going bankrupt. But I can change how we are. And we are together, and that really does matter,” said dairy farmer Brenda Rudolph during the workshop, according to a report from the St. Cloud Times, which is part of the USA Today network.
“There is a conversation you people have to have in America, rural America, that says, depression is part of your life. It is not a sign of weakness. It’s a sign of reality,” said Dennis Hoiberg, a farming consultant based in Australia who spoke at the workshop. He added that, from his perspective, the United States still tends to be more repressed about mental health issues than elsewhere in the world – with the focus on stress and not on resiliency.
“Most of you folk are proud folk, and most you folk are very proud of what you do,” Mr. Hoiberg said. “You’re also psychologically exposed because you are a true believer [in what you do].”
Advice offered to lessen the tough times included noticing the beauty in the world, breaking down problems into small chunks that are more easily dealt with and then moving on to the next, sleep, and a good diet.
People with mental illness languishing
Public defenders in Colorado are seeking to have dozens of people diagnosed with mental illness who are in jail awaiting trial set free until their court date. The usual scenario in Colorado for someone charged with a crime and jailed who is deemed mentally incompetent is treatment within 28 days. However, this system is broken and wait times are far longer – in one instance 270 days.
“Many of them are there for very, very low level offenses and they’re holding in jail for way longer than a person who did not suffer from mental illness would be in custody,” said Maureen Cain, policy liaison for the public defender’s office in an interview with the Denver Post. “They are being incarcerated for their mental illness, not really because of the crime they committed.” Responses from judges have ranged from immediate release to finding the incarcerated person guilty of contempt and sending them back to jail.
The Colorado Department of Human Services is in charge of people who have been jailed but have been found to be incompetent to stand trial. Officials there have say they do not have enough bed space or capacity to get people moved out of jail within 28 days.
“We are in a situation where [the human services department] is in breach, and I need to know what efforts are being made to bring it back into compliance,” said federal Judge Nina Y. Wang. “These individuals are not being served, and frankly, the state is not being served.”
“Cruel” practice confined youth
A federal class action lawsuit filed against the Departmental of Children and Family Services (DCFS) in the Chicago area alleges that, from 2015 to 2017, more than 800 youth were being confined to psychiatric hospitals even when they were cleared for discharge. The problem goes back decades and is getting worse, the lawsuit contends.
“I spent Thanksgiving, Christmas, New Year’s, Easter, and my 16th birthday in the hospital,” said Skylar, who’s now 19 years old. “I only got to go outside one time. I felt like a prisoner; I felt very depressed.”
As reported on Chicago’s WGN9 News, the delay between clearance for discharge and actual freedom is a month or more in many of the cases. Acting Cook County Public Guardian Charles Golbert said the practice is “cruel, unusual, and illegal. It’s a violation of the children’s civil and most basic human rights.”
Many of the youth had been incarcerated for setting fires and self-harm and had been rejected by foster parents and other providers, in some cases their own families, who were concerned with the possible behavior of the youth after their release.
“Blame the children is the wrong response from DCFS,” said attorney Russell Ainsworth. “DCFS should be apologizing for not addressing this issue and for violating the Constitution.”
Responding to a police call can prove dangerous. In those kinds of high-pressure situations, agitation or other manifestations of mental illness might be mistaken for violent intent – with disastrous results.
In Kalamazoo, Mich., crime response training now includes subduing suspects without using violent force. “Through training and education, and scenarios that we use in the training, [the officers] start to detect the different cues or indicators where they start to see that this is really a crisis event. And we treat it as a medical issue and get that person the help that they need,” said Rafael Diaz, executive lieutenant with the Kalamazoo Department of Public Safety in an interview on Michigan NPR.
In the training, called the Crisis Intervention Team model, the goal is to slow down the pace of the interaction and keep some distance between themselves and the suspect after officers recognize signs of mental illness. Both responses can lower the chances of a lash-out response.
“The number of injuries to officers goes down, the number of injuries to the person in crisis goes down, and there is a huge benefit to society there if you don’t have to use physical force,” Mr. Diaz said.
Animal neglect and mental health
Images of neglected and abused livestock on farms can inspire thoughts of how someone could mistreat the animals in their care. “Frankly, if you can’t understand that, it’s probably a good thing. It means you haven’t been in the depths of low, low mental health, depression, and anxiety,” Andria Jones-Bitton, DVM, PhD, said in an interview with the Western Producer.
Dr. Jones-Bitton is a veterinarian and epidemiologist at the Ontario Veterinary College in Guelph. She is studying the mental health and mental resilience of farmers and veterinarians.
“If farmers are struggling with their own well-being and motivation, they’re likely going to find it difficult to invest in improving animal welfare. When we’re mentally unwell, it’s hard to care for ourselves, let alone to care for others, even when those others are really important to us,” she said.
A national survey of Canadian farmers by Dr. Jones-Bitton showed high levels of stress and diminished ability to cope with the pressures that come with running a livestock farm. “What makes me the most upset is I have everything I’ve ever dreamed of – love, family, and a farm, and all I feel is overwhelmed out of control and sad,” one respondent said.
The problems are not unique to Canada. Studies from Ireland, for example, documented an association between animal neglect cases and the mental health, drug/alcohol addiction, and social problems of farmers.
“Even if you didn’t care about the humans that were struggling and you only cared about the animal welfare, you’d be wise to address the issue of farmer stress,” Dr. Jones-Britton said.
Depression and rural America
A recent “Farming in Tough Times” workshop that convened in Minnesota focused on the mental health of farmers. Making a living is challenging for many reasons. One is that prices for commodities are set by others.
“I realized that I can’t change the situation that we’re in. I can’t change milk prices. I can’t stop farms from going bankrupt. But I can change how we are. And we are together, and that really does matter,” said dairy farmer Brenda Rudolph during the workshop, according to a report from the St. Cloud Times, which is part of the USA Today network.
“There is a conversation you people have to have in America, rural America, that says, depression is part of your life. It is not a sign of weakness. It’s a sign of reality,” said Dennis Hoiberg, a farming consultant based in Australia who spoke at the workshop. He added that, from his perspective, the United States still tends to be more repressed about mental health issues than elsewhere in the world – with the focus on stress and not on resiliency.
“Most of you folk are proud folk, and most you folk are very proud of what you do,” Mr. Hoiberg said. “You’re also psychologically exposed because you are a true believer [in what you do].”
Advice offered to lessen the tough times included noticing the beauty in the world, breaking down problems into small chunks that are more easily dealt with and then moving on to the next, sleep, and a good diet.
People with mental illness languishing
Public defenders in Colorado are seeking to have dozens of people diagnosed with mental illness who are in jail awaiting trial set free until their court date. The usual scenario in Colorado for someone charged with a crime and jailed who is deemed mentally incompetent is treatment within 28 days. However, this system is broken and wait times are far longer – in one instance 270 days.
“Many of them are there for very, very low level offenses and they’re holding in jail for way longer than a person who did not suffer from mental illness would be in custody,” said Maureen Cain, policy liaison for the public defender’s office in an interview with the Denver Post. “They are being incarcerated for their mental illness, not really because of the crime they committed.” Responses from judges have ranged from immediate release to finding the incarcerated person guilty of contempt and sending them back to jail.
The Colorado Department of Human Services is in charge of people who have been jailed but have been found to be incompetent to stand trial. Officials there have say they do not have enough bed space or capacity to get people moved out of jail within 28 days.
“We are in a situation where [the human services department] is in breach, and I need to know what efforts are being made to bring it back into compliance,” said federal Judge Nina Y. Wang. “These individuals are not being served, and frankly, the state is not being served.”
“Cruel” practice confined youth
A federal class action lawsuit filed against the Departmental of Children and Family Services (DCFS) in the Chicago area alleges that, from 2015 to 2017, more than 800 youth were being confined to psychiatric hospitals even when they were cleared for discharge. The problem goes back decades and is getting worse, the lawsuit contends.
“I spent Thanksgiving, Christmas, New Year’s, Easter, and my 16th birthday in the hospital,” said Skylar, who’s now 19 years old. “I only got to go outside one time. I felt like a prisoner; I felt very depressed.”
As reported on Chicago’s WGN9 News, the delay between clearance for discharge and actual freedom is a month or more in many of the cases. Acting Cook County Public Guardian Charles Golbert said the practice is “cruel, unusual, and illegal. It’s a violation of the children’s civil and most basic human rights.”
Many of the youth had been incarcerated for setting fires and self-harm and had been rejected by foster parents and other providers, in some cases their own families, who were concerned with the possible behavior of the youth after their release.
“Blame the children is the wrong response from DCFS,” said attorney Russell Ainsworth. “DCFS should be apologizing for not addressing this issue and for violating the Constitution.”
Responding to a police call can prove dangerous. In those kinds of high-pressure situations, agitation or other manifestations of mental illness might be mistaken for violent intent – with disastrous results.
In Kalamazoo, Mich., crime response training now includes subduing suspects without using violent force. “Through training and education, and scenarios that we use in the training, [the officers] start to detect the different cues or indicators where they start to see that this is really a crisis event. And we treat it as a medical issue and get that person the help that they need,” said Rafael Diaz, executive lieutenant with the Kalamazoo Department of Public Safety in an interview on Michigan NPR.
In the training, called the Crisis Intervention Team model, the goal is to slow down the pace of the interaction and keep some distance between themselves and the suspect after officers recognize signs of mental illness. Both responses can lower the chances of a lash-out response.
“The number of injuries to officers goes down, the number of injuries to the person in crisis goes down, and there is a huge benefit to society there if you don’t have to use physical force,” Mr. Diaz said.
Animal neglect and mental health
Images of neglected and abused livestock on farms can inspire thoughts of how someone could mistreat the animals in their care. “Frankly, if you can’t understand that, it’s probably a good thing. It means you haven’t been in the depths of low, low mental health, depression, and anxiety,” Andria Jones-Bitton, DVM, PhD, said in an interview with the Western Producer.
Dr. Jones-Bitton is a veterinarian and epidemiologist at the Ontario Veterinary College in Guelph. She is studying the mental health and mental resilience of farmers and veterinarians.
“If farmers are struggling with their own well-being and motivation, they’re likely going to find it difficult to invest in improving animal welfare. When we’re mentally unwell, it’s hard to care for ourselves, let alone to care for others, even when those others are really important to us,” she said.
A national survey of Canadian farmers by Dr. Jones-Bitton showed high levels of stress and diminished ability to cope with the pressures that come with running a livestock farm. “What makes me the most upset is I have everything I’ve ever dreamed of – love, family, and a farm, and all I feel is overwhelmed out of control and sad,” one respondent said.
The problems are not unique to Canada. Studies from Ireland, for example, documented an association between animal neglect cases and the mental health, drug/alcohol addiction, and social problems of farmers.
“Even if you didn’t care about the humans that were struggling and you only cared about the animal welfare, you’d be wise to address the issue of farmer stress,” Dr. Jones-Britton said.
Depression and rural America
A recent “Farming in Tough Times” workshop that convened in Minnesota focused on the mental health of farmers. Making a living is challenging for many reasons. One is that prices for commodities are set by others.
“I realized that I can’t change the situation that we’re in. I can’t change milk prices. I can’t stop farms from going bankrupt. But I can change how we are. And we are together, and that really does matter,” said dairy farmer Brenda Rudolph during the workshop, according to a report from the St. Cloud Times, which is part of the USA Today network.
“There is a conversation you people have to have in America, rural America, that says, depression is part of your life. It is not a sign of weakness. It’s a sign of reality,” said Dennis Hoiberg, a farming consultant based in Australia who spoke at the workshop. He added that, from his perspective, the United States still tends to be more repressed about mental health issues than elsewhere in the world – with the focus on stress and not on resiliency.
“Most of you folk are proud folk, and most you folk are very proud of what you do,” Mr. Hoiberg said. “You’re also psychologically exposed because you are a true believer [in what you do].”
Advice offered to lessen the tough times included noticing the beauty in the world, breaking down problems into small chunks that are more easily dealt with and then moving on to the next, sleep, and a good diet.
People with mental illness languishing
Public defenders in Colorado are seeking to have dozens of people diagnosed with mental illness who are in jail awaiting trial set free until their court date. The usual scenario in Colorado for someone charged with a crime and jailed who is deemed mentally incompetent is treatment within 28 days. However, this system is broken and wait times are far longer – in one instance 270 days.
“Many of them are there for very, very low level offenses and they’re holding in jail for way longer than a person who did not suffer from mental illness would be in custody,” said Maureen Cain, policy liaison for the public defender’s office in an interview with the Denver Post. “They are being incarcerated for their mental illness, not really because of the crime they committed.” Responses from judges have ranged from immediate release to finding the incarcerated person guilty of contempt and sending them back to jail.
The Colorado Department of Human Services is in charge of people who have been jailed but have been found to be incompetent to stand trial. Officials there have say they do not have enough bed space or capacity to get people moved out of jail within 28 days.
“We are in a situation where [the human services department] is in breach, and I need to know what efforts are being made to bring it back into compliance,” said federal Judge Nina Y. Wang. “These individuals are not being served, and frankly, the state is not being served.”
“Cruel” practice confined youth
A federal class action lawsuit filed against the Departmental of Children and Family Services (DCFS) in the Chicago area alleges that, from 2015 to 2017, more than 800 youth were being confined to psychiatric hospitals even when they were cleared for discharge. The problem goes back decades and is getting worse, the lawsuit contends.
“I spent Thanksgiving, Christmas, New Year’s, Easter, and my 16th birthday in the hospital,” said Skylar, who’s now 19 years old. “I only got to go outside one time. I felt like a prisoner; I felt very depressed.”
As reported on Chicago’s WGN9 News, the delay between clearance for discharge and actual freedom is a month or more in many of the cases. Acting Cook County Public Guardian Charles Golbert said the practice is “cruel, unusual, and illegal. It’s a violation of the children’s civil and most basic human rights.”
Many of the youth had been incarcerated for setting fires and self-harm and had been rejected by foster parents and other providers, in some cases their own families, who were concerned with the possible behavior of the youth after their release.
“Blame the children is the wrong response from DCFS,” said attorney Russell Ainsworth. “DCFS should be apologizing for not addressing this issue and for violating the Constitution.”
FDA approves calaspargase pegol-mknl for ALL

The U.S. Food and Drug Administration (FDA) has approved calaspargase pegol-mknl (Asparlas) as a component of a multi-agent chemotherapeutic regimen to treat acute lymphoblastic leukemia (ALL) in pediatric and young adult patients age 1 month to 21 years.
Calaspargase pegol-mknl is an asparagine-specific enzyme intended to provide a longer interval between doses compared to other available pegaspargase products.
The recommended dosage of calaspargase pegol-mknl is 2,500 U/m2 given no more frequently than every 21 days.
The FDA said it approved calaspargase pegol-mknl because the drug maintained nadir serum asparaginase activity above the level of 0.1 U/mL when given at 2,500 U/m2 every 3 weeks.
Calaspargase pegol-mknl was evaluated in Study DFCI 11-001, a trial of 237 children and adolescents with newly diagnosed ALL or lymphoblastic lymphoma. The patients’ median age was 5 years (range, 1 to 20 years).
They received calaspargase pegol-mknl at 2,500 U/m2 (n=118) or pegaspargase at 2,500 U/m2 (n=119) as part of a Dana-Farber Cancer Institute (DFCI) ALL Consortium backbone therapy.
The median duration of exposure was 8 months for both calaspargase pegol-mknl and pegaspargase.
Among the patients with B-cell lineage ALL, the complete remission rate was 98% in the calaspargase pegol-mknl arm and 99% in the pegaspargase arm. Estimated overall survival rates were comparable between the arms.
Common grade 3 or higher adverse events (in the calaspargase pegol-mknl and pegaspargase arms, respectively) included elevated transaminase (52% and 66%), bilirubin increase (20% and 25%), pancreatitis (18% and 24%), and abnormal clotting studies (14% and 21%).
There was one fatal adverse event among patients on calaspargase pegol-mknl—multi-organ failure in the setting of chronic pancreatitis associated with a pancreatic pseudocyst.
The safety of calaspargase pegol-mknl was also evaluated in Study AALL07P4, a trial of patients with newly diagnosed, high-risk B-precursor ALL.
The patients received calaspargase pegol-mknl at 2,500 U/m2 (n=43) or 2,100 U/m2 (n=68) or pegaspargase at 2,500 U/m2 (n=52) as a component of an augmented Berlin-Frankfurt-Münster regimen.
The patients’ median age was 11 years (range, 1 to 26 years). The median duration of exposure was 7 months for both calaspargase pegol-mknl and pegaspargase.
There were three induction deaths among the 111 patients who received calaspargase pegol-mknl (2.8%) but no induction deaths among the 52 patients treated with pegaspargase.
Additional details on these studies and calaspargase pegol-mknl can be found in the drug’s prescribing information.
Calaspargase pegol-mknl is a product of Servier Pharmaceuticals LLC.
The U.S. Food and Drug Administration (FDA) has approved calaspargase pegol-mknl (Asparlas) as a component of a multi-agent chemotherapeutic regimen to treat acute lymphoblastic leukemia (ALL) in pediatric and young adult patients age 1 month to 21 years.
Calaspargase pegol-mknl is an asparagine-specific enzyme intended to provide a longer interval between doses compared to other available pegaspargase products.
The recommended dosage of calaspargase pegol-mknl is 2,500 U/m2 given no more frequently than every 21 days.
The FDA said it approved calaspargase pegol-mknl because the drug maintained nadir serum asparaginase activity above the level of 0.1 U/mL when given at 2,500 U/m2 every 3 weeks.
Calaspargase pegol-mknl was evaluated in Study DFCI 11-001, a trial of 237 children and adolescents with newly diagnosed ALL or lymphoblastic lymphoma. The patients’ median age was 5 years (range, 1 to 20 years).
They received calaspargase pegol-mknl at 2,500 U/m2 (n=118) or pegaspargase at 2,500 U/m2 (n=119) as part of a Dana-Farber Cancer Institute (DFCI) ALL Consortium backbone therapy.
The median duration of exposure was 8 months for both calaspargase pegol-mknl and pegaspargase.
Among the patients with B-cell lineage ALL, the complete remission rate was 98% in the calaspargase pegol-mknl arm and 99% in the pegaspargase arm. Estimated overall survival rates were comparable between the arms.
Common grade 3 or higher adverse events (in the calaspargase pegol-mknl and pegaspargase arms, respectively) included elevated transaminase (52% and 66%), bilirubin increase (20% and 25%), pancreatitis (18% and 24%), and abnormal clotting studies (14% and 21%).
There was one fatal adverse event among patients on calaspargase pegol-mknl—multi-organ failure in the setting of chronic pancreatitis associated with a pancreatic pseudocyst.
The safety of calaspargase pegol-mknl was also evaluated in Study AALL07P4, a trial of patients with newly diagnosed, high-risk B-precursor ALL.
The patients received calaspargase pegol-mknl at 2,500 U/m2 (n=43) or 2,100 U/m2 (n=68) or pegaspargase at 2,500 U/m2 (n=52) as a component of an augmented Berlin-Frankfurt-Münster regimen.
The patients’ median age was 11 years (range, 1 to 26 years). The median duration of exposure was 7 months for both calaspargase pegol-mknl and pegaspargase.
There were three induction deaths among the 111 patients who received calaspargase pegol-mknl (2.8%) but no induction deaths among the 52 patients treated with pegaspargase.
Additional details on these studies and calaspargase pegol-mknl can be found in the drug’s prescribing information.
Calaspargase pegol-mknl is a product of Servier Pharmaceuticals LLC.
The U.S. Food and Drug Administration (FDA) has approved calaspargase pegol-mknl (Asparlas) as a component of a multi-agent chemotherapeutic regimen to treat acute lymphoblastic leukemia (ALL) in pediatric and young adult patients age 1 month to 21 years.
Calaspargase pegol-mknl is an asparagine-specific enzyme intended to provide a longer interval between doses compared to other available pegaspargase products.
The recommended dosage of calaspargase pegol-mknl is 2,500 U/m2 given no more frequently than every 21 days.
The FDA said it approved calaspargase pegol-mknl because the drug maintained nadir serum asparaginase activity above the level of 0.1 U/mL when given at 2,500 U/m2 every 3 weeks.
Calaspargase pegol-mknl was evaluated in Study DFCI 11-001, a trial of 237 children and adolescents with newly diagnosed ALL or lymphoblastic lymphoma. The patients’ median age was 5 years (range, 1 to 20 years).
They received calaspargase pegol-mknl at 2,500 U/m2 (n=118) or pegaspargase at 2,500 U/m2 (n=119) as part of a Dana-Farber Cancer Institute (DFCI) ALL Consortium backbone therapy.
The median duration of exposure was 8 months for both calaspargase pegol-mknl and pegaspargase.
Among the patients with B-cell lineage ALL, the complete remission rate was 98% in the calaspargase pegol-mknl arm and 99% in the pegaspargase arm. Estimated overall survival rates were comparable between the arms.
Common grade 3 or higher adverse events (in the calaspargase pegol-mknl and pegaspargase arms, respectively) included elevated transaminase (52% and 66%), bilirubin increase (20% and 25%), pancreatitis (18% and 24%), and abnormal clotting studies (14% and 21%).
There was one fatal adverse event among patients on calaspargase pegol-mknl—multi-organ failure in the setting of chronic pancreatitis associated with a pancreatic pseudocyst.
The safety of calaspargase pegol-mknl was also evaluated in Study AALL07P4, a trial of patients with newly diagnosed, high-risk B-precursor ALL.
The patients received calaspargase pegol-mknl at 2,500 U/m2 (n=43) or 2,100 U/m2 (n=68) or pegaspargase at 2,500 U/m2 (n=52) as a component of an augmented Berlin-Frankfurt-Münster regimen.
The patients’ median age was 11 years (range, 1 to 26 years). The median duration of exposure was 7 months for both calaspargase pegol-mknl and pegaspargase.
There were three induction deaths among the 111 patients who received calaspargase pegol-mknl (2.8%) but no induction deaths among the 52 patients treated with pegaspargase.
Additional details on these studies and calaspargase pegol-mknl can be found in the drug’s prescribing information.
Calaspargase pegol-mknl is a product of Servier Pharmaceuticals LLC.
Blanchable Erythematous Patches on the Fingers
The Diagnosis: Irritant Contact Dermatitis
The diagnosis of irritant contact dermatitis secondary to skateboarding is similar to pool palms, a benign, self-limiting irritant contact dermatitis.1 We propose that contact with concrete surfaces during skateboarding can lead to a presentation similar to pool palms. In our case, it was likely that the finger pulpitis noted in the physical examination was due to daily skateboarding rather than once-weekly swimming. Furthermore, the fingertip contact with concrete in pool palms is similar to the rough surface exposure on the skateboard.
Pool palms is more commonly reported in children due to their participation in sports and other activities with recent exposure to rough surfaces, most commonly the floor of swimming pools.2 The condition resolves after eliminating exposures.3 The frequency and duration of exposure to rough surfaces in swimming pools leading to development of this condition is unknown.
There have been mixed reports on the pathogenesis of pool palms. Some literature supports the idea that it is a wet dermatitis, a combination of prolonged water contact, friction, chemicals, and microbes leading to a chronic dermatitis. This theory states that the primary factor influencing the development of erythematous patches on the fingers, palms, and soles is the hyperhydration of the corneal layer at these sites.4 A different theory attributes pool palms to a mechanical origin, such as repeated microtrauma from contact with the rough concrete surfaces of swimming pools.5 This theory further states that the chemicals in pool water, such as chlorine and sodium hypochlorite, rarely produce irritant, allergic, or urticarial reactions.3
Based on these theories, we hypothesized that fingertip pulpitis can result from activities other than swimming (eg, skateboarding). Our case supports the latter theory on fingertip pulpitis in pool palms being a result of frictional dermatitis rather than wet dermatitis because we attributed our patient’s findings to contact with rough surfaces during skateboarding. Although the patient did swim, he only did so once weekly in the summer months, and the lesions had been persistent for 2 years consistently. His skateboarding hobby was more frequent, and he endorsed contact of the pads of the bilateral second to fifth fingers to the rough surfaces of the road and skateboard. The patient did not have lesions on the toes, further supporting the hypothesis that skateboarding led to the current presentation.
In children, hand-foot-and-mouth disease classically presents with oval-shaped, erythematous vesicles on the palmar surfaces of the hands and feet and generally is accompanied by fever and sore throat.6 Furthermore, unlike in our case, the viral exanthem usually would be present for up to 3 weeks and would not persist for more than 2 years. Erythema multiforme has an erythematous color and can present on the palms; however, the lesions have a classic targetoid appearance. It would be unique for erythema multiforme to present only on the fingertips rather than more diffusely on the palms or in other areas such as the face.7 Limited cutaneous sclerosis (scleroderma) initially can present with edematous pitted scars on the digital tips; however, with time the fingers will have a taut, white, shiny appearance that can develop into contractures and debilitating ulcerations.8 In our patient, the plaques did not advance to any further disease. Lastly, in contrast to our patient, punctate palmoplantar keratoderma presents as hyperkeratotic, firm, translucent, or opaque papules on the palms and soles. Over time, the papules can appear verrucous or callouslike.9 In our case, the plaques on the fingertips were erythematous rather than translucent or opaque papules.
Our case raises questions on whether prior reports of pool palms can be attributed to other activities involving contact with rough surfaces. More research is needed on the frequency and duration of rough surface exposure resulting in fingertip pulpitis.
- Lopez-Neyra A, Vano-Galvan S, Alvarez-Twose I, et al. Pool palms [in Spanish]. Dermatol Online J. 2009;15:17.
- Wong LC, Rogers M. Pool palms. Pediatr Dermatol. 2007;24:95.
- Mandojana RM. Pool palms. J Am Acad Dermatol. 1993;28(2 pt 1):280-281.
- Novoa A, Klear S. Pool palms [published online September 30, 2015]. Arch Dis Child. 2016;101:41.
- Martín JM, Martín JM, Ricart JM. Erythematous-violaceous lesions on the palms [in Spanish]. Actas Dermosifiliogr. 2009;100:507-508.
- Marcini AJ, Shani-Adir A. Other viral diseases. In: Bolognia J, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. Philadelphia, PA: Elsevier Ltd; 2012:1345-1366.
- French LE, Prins C. Erythema multiforme, Stevens-Johnson syndrome, and toxic epidermal necrosis. In: Bolognia J, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. Philadelphia, PA: Elsevier Ltd; 2012:319-334.
- Connoly MK. Systemic sclerosis (scleroderma) and related disorders. In: Bolognia J, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. Philadelphia, PA: Elsevier Ltd; 2012:643-646.
- Krol AL, Siegel D. Keratodermas. In: Bolognia J, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. Philadelphia, PA: Elsevier Ltd; 2012:871-886.
The Diagnosis: Irritant Contact Dermatitis
The diagnosis of irritant contact dermatitis secondary to skateboarding is similar to pool palms, a benign, self-limiting irritant contact dermatitis.1 We propose that contact with concrete surfaces during skateboarding can lead to a presentation similar to pool palms. In our case, it was likely that the finger pulpitis noted in the physical examination was due to daily skateboarding rather than once-weekly swimming. Furthermore, the fingertip contact with concrete in pool palms is similar to the rough surface exposure on the skateboard.
Pool palms is more commonly reported in children due to their participation in sports and other activities with recent exposure to rough surfaces, most commonly the floor of swimming pools.2 The condition resolves after eliminating exposures.3 The frequency and duration of exposure to rough surfaces in swimming pools leading to development of this condition is unknown.
There have been mixed reports on the pathogenesis of pool palms. Some literature supports the idea that it is a wet dermatitis, a combination of prolonged water contact, friction, chemicals, and microbes leading to a chronic dermatitis. This theory states that the primary factor influencing the development of erythematous patches on the fingers, palms, and soles is the hyperhydration of the corneal layer at these sites.4 A different theory attributes pool palms to a mechanical origin, such as repeated microtrauma from contact with the rough concrete surfaces of swimming pools.5 This theory further states that the chemicals in pool water, such as chlorine and sodium hypochlorite, rarely produce irritant, allergic, or urticarial reactions.3
Based on these theories, we hypothesized that fingertip pulpitis can result from activities other than swimming (eg, skateboarding). Our case supports the latter theory on fingertip pulpitis in pool palms being a result of frictional dermatitis rather than wet dermatitis because we attributed our patient’s findings to contact with rough surfaces during skateboarding. Although the patient did swim, he only did so once weekly in the summer months, and the lesions had been persistent for 2 years consistently. His skateboarding hobby was more frequent, and he endorsed contact of the pads of the bilateral second to fifth fingers to the rough surfaces of the road and skateboard. The patient did not have lesions on the toes, further supporting the hypothesis that skateboarding led to the current presentation.
In children, hand-foot-and-mouth disease classically presents with oval-shaped, erythematous vesicles on the palmar surfaces of the hands and feet and generally is accompanied by fever and sore throat.6 Furthermore, unlike in our case, the viral exanthem usually would be present for up to 3 weeks and would not persist for more than 2 years. Erythema multiforme has an erythematous color and can present on the palms; however, the lesions have a classic targetoid appearance. It would be unique for erythema multiforme to present only on the fingertips rather than more diffusely on the palms or in other areas such as the face.7 Limited cutaneous sclerosis (scleroderma) initially can present with edematous pitted scars on the digital tips; however, with time the fingers will have a taut, white, shiny appearance that can develop into contractures and debilitating ulcerations.8 In our patient, the plaques did not advance to any further disease. Lastly, in contrast to our patient, punctate palmoplantar keratoderma presents as hyperkeratotic, firm, translucent, or opaque papules on the palms and soles. Over time, the papules can appear verrucous or callouslike.9 In our case, the plaques on the fingertips were erythematous rather than translucent or opaque papules.
Our case raises questions on whether prior reports of pool palms can be attributed to other activities involving contact with rough surfaces. More research is needed on the frequency and duration of rough surface exposure resulting in fingertip pulpitis.
The Diagnosis: Irritant Contact Dermatitis
The diagnosis of irritant contact dermatitis secondary to skateboarding is similar to pool palms, a benign, self-limiting irritant contact dermatitis.1 We propose that contact with concrete surfaces during skateboarding can lead to a presentation similar to pool palms. In our case, it was likely that the finger pulpitis noted in the physical examination was due to daily skateboarding rather than once-weekly swimming. Furthermore, the fingertip contact with concrete in pool palms is similar to the rough surface exposure on the skateboard.
Pool palms is more commonly reported in children due to their participation in sports and other activities with recent exposure to rough surfaces, most commonly the floor of swimming pools.2 The condition resolves after eliminating exposures.3 The frequency and duration of exposure to rough surfaces in swimming pools leading to development of this condition is unknown.
There have been mixed reports on the pathogenesis of pool palms. Some literature supports the idea that it is a wet dermatitis, a combination of prolonged water contact, friction, chemicals, and microbes leading to a chronic dermatitis. This theory states that the primary factor influencing the development of erythematous patches on the fingers, palms, and soles is the hyperhydration of the corneal layer at these sites.4 A different theory attributes pool palms to a mechanical origin, such as repeated microtrauma from contact with the rough concrete surfaces of swimming pools.5 This theory further states that the chemicals in pool water, such as chlorine and sodium hypochlorite, rarely produce irritant, allergic, or urticarial reactions.3
Based on these theories, we hypothesized that fingertip pulpitis can result from activities other than swimming (eg, skateboarding). Our case supports the latter theory on fingertip pulpitis in pool palms being a result of frictional dermatitis rather than wet dermatitis because we attributed our patient’s findings to contact with rough surfaces during skateboarding. Although the patient did swim, he only did so once weekly in the summer months, and the lesions had been persistent for 2 years consistently. His skateboarding hobby was more frequent, and he endorsed contact of the pads of the bilateral second to fifth fingers to the rough surfaces of the road and skateboard. The patient did not have lesions on the toes, further supporting the hypothesis that skateboarding led to the current presentation.
In children, hand-foot-and-mouth disease classically presents with oval-shaped, erythematous vesicles on the palmar surfaces of the hands and feet and generally is accompanied by fever and sore throat.6 Furthermore, unlike in our case, the viral exanthem usually would be present for up to 3 weeks and would not persist for more than 2 years. Erythema multiforme has an erythematous color and can present on the palms; however, the lesions have a classic targetoid appearance. It would be unique for erythema multiforme to present only on the fingertips rather than more diffusely on the palms or in other areas such as the face.7 Limited cutaneous sclerosis (scleroderma) initially can present with edematous pitted scars on the digital tips; however, with time the fingers will have a taut, white, shiny appearance that can develop into contractures and debilitating ulcerations.8 In our patient, the plaques did not advance to any further disease. Lastly, in contrast to our patient, punctate palmoplantar keratoderma presents as hyperkeratotic, firm, translucent, or opaque papules on the palms and soles. Over time, the papules can appear verrucous or callouslike.9 In our case, the plaques on the fingertips were erythematous rather than translucent or opaque papules.
Our case raises questions on whether prior reports of pool palms can be attributed to other activities involving contact with rough surfaces. More research is needed on the frequency and duration of rough surface exposure resulting in fingertip pulpitis.
- Lopez-Neyra A, Vano-Galvan S, Alvarez-Twose I, et al. Pool palms [in Spanish]. Dermatol Online J. 2009;15:17.
- Wong LC, Rogers M. Pool palms. Pediatr Dermatol. 2007;24:95.
- Mandojana RM. Pool palms. J Am Acad Dermatol. 1993;28(2 pt 1):280-281.
- Novoa A, Klear S. Pool palms [published online September 30, 2015]. Arch Dis Child. 2016;101:41.
- Martín JM, Martín JM, Ricart JM. Erythematous-violaceous lesions on the palms [in Spanish]. Actas Dermosifiliogr. 2009;100:507-508.
- Marcini AJ, Shani-Adir A. Other viral diseases. In: Bolognia J, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. Philadelphia, PA: Elsevier Ltd; 2012:1345-1366.
- French LE, Prins C. Erythema multiforme, Stevens-Johnson syndrome, and toxic epidermal necrosis. In: Bolognia J, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. Philadelphia, PA: Elsevier Ltd; 2012:319-334.
- Connoly MK. Systemic sclerosis (scleroderma) and related disorders. In: Bolognia J, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. Philadelphia, PA: Elsevier Ltd; 2012:643-646.
- Krol AL, Siegel D. Keratodermas. In: Bolognia J, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. Philadelphia, PA: Elsevier Ltd; 2012:871-886.
- Lopez-Neyra A, Vano-Galvan S, Alvarez-Twose I, et al. Pool palms [in Spanish]. Dermatol Online J. 2009;15:17.
- Wong LC, Rogers M. Pool palms. Pediatr Dermatol. 2007;24:95.
- Mandojana RM. Pool palms. J Am Acad Dermatol. 1993;28(2 pt 1):280-281.
- Novoa A, Klear S. Pool palms [published online September 30, 2015]. Arch Dis Child. 2016;101:41.
- Martín JM, Martín JM, Ricart JM. Erythematous-violaceous lesions on the palms [in Spanish]. Actas Dermosifiliogr. 2009;100:507-508.
- Marcini AJ, Shani-Adir A. Other viral diseases. In: Bolognia J, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. Philadelphia, PA: Elsevier Ltd; 2012:1345-1366.
- French LE, Prins C. Erythema multiforme, Stevens-Johnson syndrome, and toxic epidermal necrosis. In: Bolognia J, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. Philadelphia, PA: Elsevier Ltd; 2012:319-334.
- Connoly MK. Systemic sclerosis (scleroderma) and related disorders. In: Bolognia J, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. Philadelphia, PA: Elsevier Ltd; 2012:643-646.
- Krol AL, Siegel D. Keratodermas. In: Bolognia J, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. Philadelphia, PA: Elsevier Ltd; 2012:871-886.

A 12-year-old boy presented with well-defined, blanchable, erythematous patches on the distal bilateral palmar aspects of the second to fifth fingers of 2 years’ duration. The patient stated that he skateboarded daily throughout the year and swam once weekly in the summer months. Furthermore, the patient cited frequent contact with the rough undersurface of the skateboard and concrete road surfaces while skateboarding. He stated that the lesions were always present and worsened in the summer months. The lesions had an occasional burning sensation when they were more prominently erythematous, and the patient denied any pattern of exacerbation, numbness, bleeding, or itching. There was no notable family history or evidence of systemic disease.

Survivors of childhood Hodgkin lymphoma face 14-fold risk of second cancers
Survivors of childhood Hodgkin lymphoma have a 14-fold greater risk for second cancers, compared with the general population, according to newly published data.
The subsequent malignant neoplasms (SMNs) tend to follow specific patterns depending on the patient’s age at treatment, sex, treatment modality, and body region treated.
And although the risk of SMNs appears to be somewhat lower for patients treated in more recent decades, it is still significantly elevated, compared with that of the general population, according to Anna S. Holmqvist, MD, PhD, from Lund University (Sweden), and her colleagues.
“A major goal of the current study was to develop evidence with which to guide the screening of survivors of HL for the development of [solid] SMNs,” the investigators wrote in Cancer.
They examined at data from the Late Effects Study Group, a multinational cohort of patients aged 16 years or younger who were treated for Hodgkin lymphoma and other cancers from 1955 to 1986.
The current report is the third update from an expanded cohort, including data on 1,136 patients with a median follow-up of 26.6 years. The median patient age at diagnosis was 11 years and the patients were followed for 23,212 person-years following the Hodgkin lymphoma diagnosis.
In all, 162 patients developed a total of 196 solid SMNs, including breast cancer in 54 patients, basal cell carcinoma in 34 patients, thyroid cancer in 30, colorectal cancer in 15, lung cancer in 11, other malignancies in 40, and disease site not available in 12 patients.
The cumulative incidence of any solid SMN 40 years after a diagnosis of Hodgkin lymphoma was 26.4%. The standardized incidence ratio for the entire cohort was 14.0, compared with the general population as derived from the Surveillance, Epidemiology and End Results database.
Predisposing factors for breast cancer in females included a Hodgkin lymphoma diagnosis from the ages of 10-16 years, and treatment with radiotherapy to the chest.
The patients at highest risk for subsequent development of lung cancer were males treated with chest radiotherapy before age 10 years. Those at highest risk for colorectal cancer were males and females who had received abdominal/pelvic radiotherapy and high-dose alkylating agents. Patients at highest risk for thyroid cancers were females who had been treated with radiotherapy to the neck before the age of 10.
The cumulative incidence for breast cancer by age 50 years for those at highest risk was 45.3%. The respective cumulative incidences for lung, colorectal, and thyroid cancers by age 50 were 4.2%, 9.5%, and 17.3%.
The investigators noted that patients treated more recently are likely to have received lower doses and volumes of radiotherapy, compared with patients treated in 1970s and earlier. “However, for the cohort of patients treated between 1955 and 1986, it is clear that continued surveillance for [solid] SMNs is essential because their risk continues to increase as these survivors enter their fourth and subsequent decades of life.”
No specific funding source for the study was reported. The authors made no financial disclosures.
SOURCE: Holmqvist AS et al. Cancer. 2018 Dec 17. doi: 10.1002/cncr.31807.
Survivors of childhood Hodgkin lymphoma have a 14-fold greater risk for second cancers, compared with the general population, according to newly published data.
The subsequent malignant neoplasms (SMNs) tend to follow specific patterns depending on the patient’s age at treatment, sex, treatment modality, and body region treated.
And although the risk of SMNs appears to be somewhat lower for patients treated in more recent decades, it is still significantly elevated, compared with that of the general population, according to Anna S. Holmqvist, MD, PhD, from Lund University (Sweden), and her colleagues.
“A major goal of the current study was to develop evidence with which to guide the screening of survivors of HL for the development of [solid] SMNs,” the investigators wrote in Cancer.
They examined at data from the Late Effects Study Group, a multinational cohort of patients aged 16 years or younger who were treated for Hodgkin lymphoma and other cancers from 1955 to 1986.
The current report is the third update from an expanded cohort, including data on 1,136 patients with a median follow-up of 26.6 years. The median patient age at diagnosis was 11 years and the patients were followed for 23,212 person-years following the Hodgkin lymphoma diagnosis.
In all, 162 patients developed a total of 196 solid SMNs, including breast cancer in 54 patients, basal cell carcinoma in 34 patients, thyroid cancer in 30, colorectal cancer in 15, lung cancer in 11, other malignancies in 40, and disease site not available in 12 patients.
The cumulative incidence of any solid SMN 40 years after a diagnosis of Hodgkin lymphoma was 26.4%. The standardized incidence ratio for the entire cohort was 14.0, compared with the general population as derived from the Surveillance, Epidemiology and End Results database.
Predisposing factors for breast cancer in females included a Hodgkin lymphoma diagnosis from the ages of 10-16 years, and treatment with radiotherapy to the chest.
The patients at highest risk for subsequent development of lung cancer were males treated with chest radiotherapy before age 10 years. Those at highest risk for colorectal cancer were males and females who had received abdominal/pelvic radiotherapy and high-dose alkylating agents. Patients at highest risk for thyroid cancers were females who had been treated with radiotherapy to the neck before the age of 10.
The cumulative incidence for breast cancer by age 50 years for those at highest risk was 45.3%. The respective cumulative incidences for lung, colorectal, and thyroid cancers by age 50 were 4.2%, 9.5%, and 17.3%.
The investigators noted that patients treated more recently are likely to have received lower doses and volumes of radiotherapy, compared with patients treated in 1970s and earlier. “However, for the cohort of patients treated between 1955 and 1986, it is clear that continued surveillance for [solid] SMNs is essential because their risk continues to increase as these survivors enter their fourth and subsequent decades of life.”
No specific funding source for the study was reported. The authors made no financial disclosures.
SOURCE: Holmqvist AS et al. Cancer. 2018 Dec 17. doi: 10.1002/cncr.31807.
Survivors of childhood Hodgkin lymphoma have a 14-fold greater risk for second cancers, compared with the general population, according to newly published data.
The subsequent malignant neoplasms (SMNs) tend to follow specific patterns depending on the patient’s age at treatment, sex, treatment modality, and body region treated.
And although the risk of SMNs appears to be somewhat lower for patients treated in more recent decades, it is still significantly elevated, compared with that of the general population, according to Anna S. Holmqvist, MD, PhD, from Lund University (Sweden), and her colleagues.
“A major goal of the current study was to develop evidence with which to guide the screening of survivors of HL for the development of [solid] SMNs,” the investigators wrote in Cancer.
They examined at data from the Late Effects Study Group, a multinational cohort of patients aged 16 years or younger who were treated for Hodgkin lymphoma and other cancers from 1955 to 1986.
The current report is the third update from an expanded cohort, including data on 1,136 patients with a median follow-up of 26.6 years. The median patient age at diagnosis was 11 years and the patients were followed for 23,212 person-years following the Hodgkin lymphoma diagnosis.
In all, 162 patients developed a total of 196 solid SMNs, including breast cancer in 54 patients, basal cell carcinoma in 34 patients, thyroid cancer in 30, colorectal cancer in 15, lung cancer in 11, other malignancies in 40, and disease site not available in 12 patients.
The cumulative incidence of any solid SMN 40 years after a diagnosis of Hodgkin lymphoma was 26.4%. The standardized incidence ratio for the entire cohort was 14.0, compared with the general population as derived from the Surveillance, Epidemiology and End Results database.
Predisposing factors for breast cancer in females included a Hodgkin lymphoma diagnosis from the ages of 10-16 years, and treatment with radiotherapy to the chest.
The patients at highest risk for subsequent development of lung cancer were males treated with chest radiotherapy before age 10 years. Those at highest risk for colorectal cancer were males and females who had received abdominal/pelvic radiotherapy and high-dose alkylating agents. Patients at highest risk for thyroid cancers were females who had been treated with radiotherapy to the neck before the age of 10.
The cumulative incidence for breast cancer by age 50 years for those at highest risk was 45.3%. The respective cumulative incidences for lung, colorectal, and thyroid cancers by age 50 were 4.2%, 9.5%, and 17.3%.
The investigators noted that patients treated more recently are likely to have received lower doses and volumes of radiotherapy, compared with patients treated in 1970s and earlier. “However, for the cohort of patients treated between 1955 and 1986, it is clear that continued surveillance for [solid] SMNs is essential because their risk continues to increase as these survivors enter their fourth and subsequent decades of life.”
No specific funding source for the study was reported. The authors made no financial disclosures.
SOURCE: Holmqvist AS et al. Cancer. 2018 Dec 17. doi: 10.1002/cncr.31807.
FROM CANCER
Key clinical point:
Major finding: The risk for a subsequent malignant neoplasm among survivors of childhood Hodgkin lymphoma was 14-fold higher than that of the general population.
Study details: The third update of data on a cohort of 1,136 childhood Hodgkin lymphoma survivors followed for a median of 26.6 years.
Disclosures: No specific funding source for the study was reported. The authors made no financial disclosures.
Source: Holmqvist AS et al. Cancer. 2018 Dec 17. doi: 10.1002/cncr.31807.
Hippocampal abnormalities seen in epilepsy subtypes may be congenital
NEW ORLEANS – , although to a lesser extent, based on findings from two studies presented at the annual meeting of the American Epilepsy Society.
While the studies suggest an imaging endophenotype associated with these disorders, it’s unclear if a larger degree of abnormality causes disease manifestation, or whether there are other predisposing actors at work.
“What our study tells us is that hippocampal abnormalities can occur in the absence of seizure,” Marian Galovic, MD, said in an interview. “It may be that, in some cases, hippocampal abnormalities could be the cause, rather than the consequence, of seizures.”
Dr. Galovic of University College London was on hand to discuss the work of his colleague, Lili Long, MD, PhD, of the Xiangya Hospital of Central South University, Changsha, China. Visa issues prevented her from attending the meeting.
The study included 18 sibling pairs in which the affected siblings had sporadic, nonlesional temporal lobe epilepsy (TLE), involving the right lobe in 12 and the left in 6. The patients, siblings, and 18 healthy, age-matched controls underwent clinical, electrophysiologic, and high-resolution structural neuroimaging.
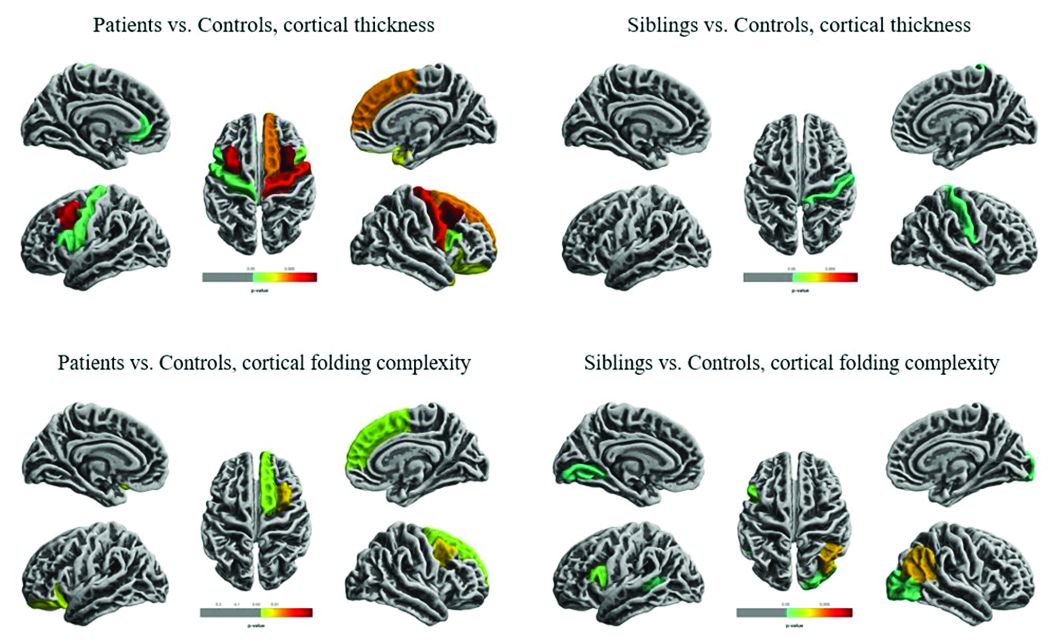
The researchers compared overall hippocampal volumes between groups and determined the subregional extent of hippocampal abnormalities using shape analysis. They also looked at whole-brain differences in cortical thickness and folding complexity.
As expected, median hippocampal volumes were largest in the healthy controls (left = 2.82 mL, right = 2.94 mL), and smallest in patients. Patients with left TLE had a median left hippocampal volume of 2.23 mL, while those with right TLE had a median right hippocampal volume of 1.92 mL.
However, volume in the unaffected siblings was a surprise. Like the patients, these subjects also had significant reductions in hippocampal volume when compared with controls (left = 2.47 mL, right = 2.65 mL). “The atrophy was relatively similar in siblings and patients, although not as pronounced in siblings,” Dr. Galovic said. “It was mostly unilateral in the siblings and bilateral in the patients, but it was still more pronounced on the side where the epilepsy of the affected sibling was coming from.”
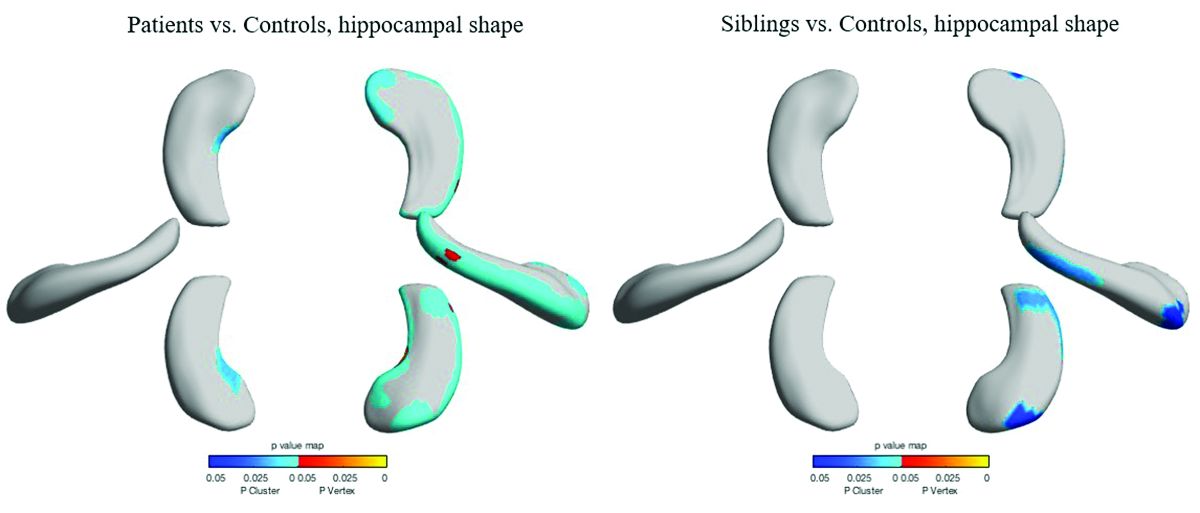
Patients and siblings also shared morphologic variations of the hippocampus, with atrophy more pronounced on the right than the left. The right lateral body and anterior head of the hippocampus were most affected, Dr. Galovic said, with reductions in the right cornu ammonis 1 subfield and subiculum.
Widespread cortical thinning was present in patients, including the pericentral, frontal, and temporal areas. Unaffected siblings also showed cortical thinning, but this was mostly restricted to the right postcentral gyrus. Patients and siblings also demonstrated increased cortical folding complexity, but in different areas: predominantly frontal in patients, but predominantly parieto-occipital in siblings. Both were significantly different than healthy control subjects.
The study didn’t examine any association with memory, which is often impaired in patients with TLE. However, Dr. Galovic said, “We have just submitted for publication a study in which we did find an association between focal hippocampal atrophy and memory performance.”
A different study by a team at University College London looked at hippocampal structure and function in patients with juvenile myoclonic epilepsy (JME) and their unaffected siblings. The imaging study, lead by Lorenzo Caciagli, MD, of the university comprised 37 patients with JME, 16 unaffected siblings, and 20 healthy controls. It employed multimodal MRI and neuropsychological measures to examine the form and function of the mesiotemporal lobe.
The subjects were matched for age, sex, handedness, and hemispheric dominance, which was assessed with language lateralization indices. This measures the number of active voxels on functional MRI, showing which hemisphere is dominant for language.
Both patients and their siblings showed reductions in left hippocampal volume on the order of 5%-8%, significantly smaller than the volumes seen in healthy controls. About half of patients and half of siblings also showed either unilateral or bilateral hippocampal malrotation. This was present in just 15% of controls, another significant difference. The structural differences weren’t associated with seizure control or age at disease onset, or with any impairments in verbal or visual memory. But when the investigators performed functional mapping, they found unusual patterns of hippocampal activation in both patients and siblings, pointing to a dysfunction of verbal encoding. In patients, there appeared to be distinct patterns of underactivation along the hippocampal long axis, regardless of whether malrotation was present. But among patients who had malrotation, the left posterior hippocampus showed more activation during visual memory.
The team concluded that the hippocampal abnormalities in volume, shape, and positioning in patients with JME and their siblings are related to functional reorganization. The abnormalities probably occur during prenatal neurodevelopment, they noted.
“Cosegregation of imaging patterns in patients and their siblings is suggestive of genetic imaging phenotypes, and independent of disease activity,” Dr. Caciagli and his coinvestigators wrote in their abstract.
Funding for the TLE study came from the National Natural Science Foundation of China, the Ministry of Science and Technology of China, and Xiangya Hospital. Funding for the JME study came from a variety of U.K. charities and government agencies.
SOURCES: Long L et al. AES 2018, Abstract 2.183; Caciagli L et al. AES 2018, Abstract 2.166.
NEW ORLEANS – , although to a lesser extent, based on findings from two studies presented at the annual meeting of the American Epilepsy Society.
While the studies suggest an imaging endophenotype associated with these disorders, it’s unclear if a larger degree of abnormality causes disease manifestation, or whether there are other predisposing actors at work.
“What our study tells us is that hippocampal abnormalities can occur in the absence of seizure,” Marian Galovic, MD, said in an interview. “It may be that, in some cases, hippocampal abnormalities could be the cause, rather than the consequence, of seizures.”
Dr. Galovic of University College London was on hand to discuss the work of his colleague, Lili Long, MD, PhD, of the Xiangya Hospital of Central South University, Changsha, China. Visa issues prevented her from attending the meeting.
The study included 18 sibling pairs in which the affected siblings had sporadic, nonlesional temporal lobe epilepsy (TLE), involving the right lobe in 12 and the left in 6. The patients, siblings, and 18 healthy, age-matched controls underwent clinical, electrophysiologic, and high-resolution structural neuroimaging.
The researchers compared overall hippocampal volumes between groups and determined the subregional extent of hippocampal abnormalities using shape analysis. They also looked at whole-brain differences in cortical thickness and folding complexity.
As expected, median hippocampal volumes were largest in the healthy controls (left = 2.82 mL, right = 2.94 mL), and smallest in patients. Patients with left TLE had a median left hippocampal volume of 2.23 mL, while those with right TLE had a median right hippocampal volume of 1.92 mL.
However, volume in the unaffected siblings was a surprise. Like the patients, these subjects also had significant reductions in hippocampal volume when compared with controls (left = 2.47 mL, right = 2.65 mL). “The atrophy was relatively similar in siblings and patients, although not as pronounced in siblings,” Dr. Galovic said. “It was mostly unilateral in the siblings and bilateral in the patients, but it was still more pronounced on the side where the epilepsy of the affected sibling was coming from.”
Patients and siblings also shared morphologic variations of the hippocampus, with atrophy more pronounced on the right than the left. The right lateral body and anterior head of the hippocampus were most affected, Dr. Galovic said, with reductions in the right cornu ammonis 1 subfield and subiculum.
Widespread cortical thinning was present in patients, including the pericentral, frontal, and temporal areas. Unaffected siblings also showed cortical thinning, but this was mostly restricted to the right postcentral gyrus. Patients and siblings also demonstrated increased cortical folding complexity, but in different areas: predominantly frontal in patients, but predominantly parieto-occipital in siblings. Both were significantly different than healthy control subjects.
The study didn’t examine any association with memory, which is often impaired in patients with TLE. However, Dr. Galovic said, “We have just submitted for publication a study in which we did find an association between focal hippocampal atrophy and memory performance.”
A different study by a team at University College London looked at hippocampal structure and function in patients with juvenile myoclonic epilepsy (JME) and their unaffected siblings. The imaging study, lead by Lorenzo Caciagli, MD, of the university comprised 37 patients with JME, 16 unaffected siblings, and 20 healthy controls. It employed multimodal MRI and neuropsychological measures to examine the form and function of the mesiotemporal lobe.
The subjects were matched for age, sex, handedness, and hemispheric dominance, which was assessed with language lateralization indices. This measures the number of active voxels on functional MRI, showing which hemisphere is dominant for language.
Both patients and their siblings showed reductions in left hippocampal volume on the order of 5%-8%, significantly smaller than the volumes seen in healthy controls. About half of patients and half of siblings also showed either unilateral or bilateral hippocampal malrotation. This was present in just 15% of controls, another significant difference. The structural differences weren’t associated with seizure control or age at disease onset, or with any impairments in verbal or visual memory. But when the investigators performed functional mapping, they found unusual patterns of hippocampal activation in both patients and siblings, pointing to a dysfunction of verbal encoding. In patients, there appeared to be distinct patterns of underactivation along the hippocampal long axis, regardless of whether malrotation was present. But among patients who had malrotation, the left posterior hippocampus showed more activation during visual memory.
The team concluded that the hippocampal abnormalities in volume, shape, and positioning in patients with JME and their siblings are related to functional reorganization. The abnormalities probably occur during prenatal neurodevelopment, they noted.
“Cosegregation of imaging patterns in patients and their siblings is suggestive of genetic imaging phenotypes, and independent of disease activity,” Dr. Caciagli and his coinvestigators wrote in their abstract.
Funding for the TLE study came from the National Natural Science Foundation of China, the Ministry of Science and Technology of China, and Xiangya Hospital. Funding for the JME study came from a variety of U.K. charities and government agencies.
SOURCES: Long L et al. AES 2018, Abstract 2.183; Caciagli L et al. AES 2018, Abstract 2.166.
NEW ORLEANS – , although to a lesser extent, based on findings from two studies presented at the annual meeting of the American Epilepsy Society.
While the studies suggest an imaging endophenotype associated with these disorders, it’s unclear if a larger degree of abnormality causes disease manifestation, or whether there are other predisposing actors at work.
“What our study tells us is that hippocampal abnormalities can occur in the absence of seizure,” Marian Galovic, MD, said in an interview. “It may be that, in some cases, hippocampal abnormalities could be the cause, rather than the consequence, of seizures.”
Dr. Galovic of University College London was on hand to discuss the work of his colleague, Lili Long, MD, PhD, of the Xiangya Hospital of Central South University, Changsha, China. Visa issues prevented her from attending the meeting.
The study included 18 sibling pairs in which the affected siblings had sporadic, nonlesional temporal lobe epilepsy (TLE), involving the right lobe in 12 and the left in 6. The patients, siblings, and 18 healthy, age-matched controls underwent clinical, electrophysiologic, and high-resolution structural neuroimaging.
The researchers compared overall hippocampal volumes between groups and determined the subregional extent of hippocampal abnormalities using shape analysis. They also looked at whole-brain differences in cortical thickness and folding complexity.
As expected, median hippocampal volumes were largest in the healthy controls (left = 2.82 mL, right = 2.94 mL), and smallest in patients. Patients with left TLE had a median left hippocampal volume of 2.23 mL, while those with right TLE had a median right hippocampal volume of 1.92 mL.
However, volume in the unaffected siblings was a surprise. Like the patients, these subjects also had significant reductions in hippocampal volume when compared with controls (left = 2.47 mL, right = 2.65 mL). “The atrophy was relatively similar in siblings and patients, although not as pronounced in siblings,” Dr. Galovic said. “It was mostly unilateral in the siblings and bilateral in the patients, but it was still more pronounced on the side where the epilepsy of the affected sibling was coming from.”
Patients and siblings also shared morphologic variations of the hippocampus, with atrophy more pronounced on the right than the left. The right lateral body and anterior head of the hippocampus were most affected, Dr. Galovic said, with reductions in the right cornu ammonis 1 subfield and subiculum.
Widespread cortical thinning was present in patients, including the pericentral, frontal, and temporal areas. Unaffected siblings also showed cortical thinning, but this was mostly restricted to the right postcentral gyrus. Patients and siblings also demonstrated increased cortical folding complexity, but in different areas: predominantly frontal in patients, but predominantly parieto-occipital in siblings. Both were significantly different than healthy control subjects.
The study didn’t examine any association with memory, which is often impaired in patients with TLE. However, Dr. Galovic said, “We have just submitted for publication a study in which we did find an association between focal hippocampal atrophy and memory performance.”
A different study by a team at University College London looked at hippocampal structure and function in patients with juvenile myoclonic epilepsy (JME) and their unaffected siblings. The imaging study, lead by Lorenzo Caciagli, MD, of the university comprised 37 patients with JME, 16 unaffected siblings, and 20 healthy controls. It employed multimodal MRI and neuropsychological measures to examine the form and function of the mesiotemporal lobe.
The subjects were matched for age, sex, handedness, and hemispheric dominance, which was assessed with language lateralization indices. This measures the number of active voxels on functional MRI, showing which hemisphere is dominant for language.
Both patients and their siblings showed reductions in left hippocampal volume on the order of 5%-8%, significantly smaller than the volumes seen in healthy controls. About half of patients and half of siblings also showed either unilateral or bilateral hippocampal malrotation. This was present in just 15% of controls, another significant difference. The structural differences weren’t associated with seizure control or age at disease onset, or with any impairments in verbal or visual memory. But when the investigators performed functional mapping, they found unusual patterns of hippocampal activation in both patients and siblings, pointing to a dysfunction of verbal encoding. In patients, there appeared to be distinct patterns of underactivation along the hippocampal long axis, regardless of whether malrotation was present. But among patients who had malrotation, the left posterior hippocampus showed more activation during visual memory.
The team concluded that the hippocampal abnormalities in volume, shape, and positioning in patients with JME and their siblings are related to functional reorganization. The abnormalities probably occur during prenatal neurodevelopment, they noted.
“Cosegregation of imaging patterns in patients and their siblings is suggestive of genetic imaging phenotypes, and independent of disease activity,” Dr. Caciagli and his coinvestigators wrote in their abstract.
Funding for the TLE study came from the National Natural Science Foundation of China, the Ministry of Science and Technology of China, and Xiangya Hospital. Funding for the JME study came from a variety of U.K. charities and government agencies.
SOURCES: Long L et al. AES 2018, Abstract 2.183; Caciagli L et al. AES 2018, Abstract 2.166.
REPORTING FROM AES 2018
Unintentional injuries top killer of U.S. children
Unintentional injuries accounted for more than half of all deaths among U.S. children aged 1-19 years in 2016, according to a new study based on data from the Centers for Disease Control and Prevention Wide-Ranging Online Data for Epidemiologic Research (WONDER) database. 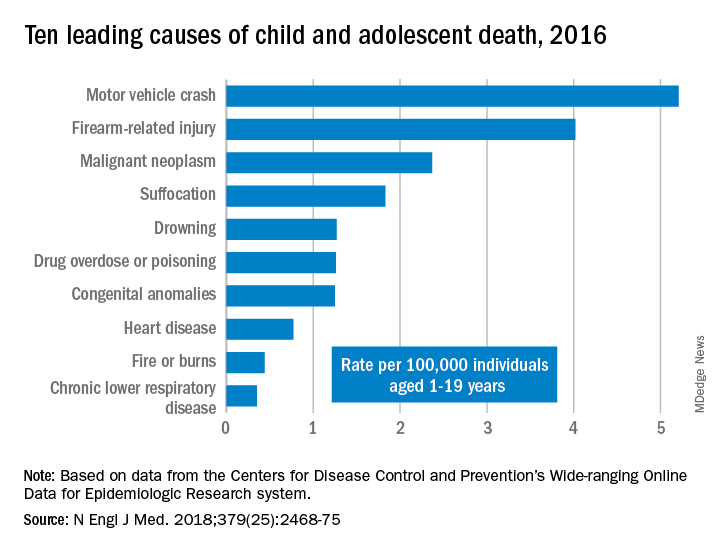
WONDER collects data from U.S. death certificates for 57 vital-statistics jurisdictions, and the 2016 data included 20,360 deaths. Injuries accounted for 12,336 deaths; unintentional injuries accounted for 57% or 7,057 deaths. Approximately one in five U.S. youth deaths (21%) were suicides, and another one in five (20%) were homicides.
Motor vehicle accidents, also responsible for one in five (20%) of all deaths, were the leading cause of accidental deaths, followed by firearm-related injuries, which accounted for 15% of all deaths. Of the firearm-related deaths, 59% were homicides, 35% suicides, 4% accidental, and 2% undetermined.
The only high-ranking noninjury cause of death overall was neoplasms, yet childhood cancer accounted for just 9% of all deaths. Suffocation was the cause of 7% of deaths, and included homicides, suicides and unintentional injuries.
The remaining causes included drowning (5.9%), drug overdose or poisoning (4.8%), congenital anomalies (4.8%), heart disease (2.9%), fire or burns (1.7%) and chronic lower respiratory disease (1.3%).
“Progress toward further reducing deaths among children and adolescents will require a shift in public perceptions so that injury deaths are viewed not as ‘accidents,’ but rather as social ecologic phenomena that are amenable to prevention,” wrote Rebecca M. Cunningham, MD, and her colleagues at the University of Michigan, Ann Arbor (N Engl J Med. 2018 Dec 20. doi: 10.1056/NEJMsr1804754). The findings “highlight the need to implement public health strategies that are tailored according to age, underlying developmental factors, and injury-related intent” to reduce the risk for death in children.”
“The sad fact is that a child or adolescent in the United States is 57% more likely to die by the age of 19 years than those in other wealthy nations,” Edward W. Campion, MD, executive editor and online editor of the New England Journal of Medicine, wrote in an editorial that accompanied the study (N Engl J Med. 2018 Dec. 20;379[25]:2466-7. doi: 10.1056/NEJMe1814600). “Children in America are dying or being killed at rates that are shameful.
“Our country has led the way in so much medical research, but the facts summarized by Cunningham et al. reveal a need to invest far more in research on the prevention of the injuries that threaten the lives of children and adolescents,” he said.
In an interview, Ben Hoffman, MD, professor of pediatrics at Oregon Health and Science University, Portland, said the only thing surprising in this report is that nothing is surprising.
“This is the stuff that those of us in injury prevention have been screaming about for decades,” said Dr. Hoffman, also medical director of the Tom Sargent Safety Center at OHSU Doernbecher Children’s Hospital.
“Unintentional injuries are what kill kids. We have made such tremendous progress in other areas, and we’ve made progress in terms of preventing injuries, but what we see is unacceptable,” he said. “The fact that [injuries] remain such an issue is a testament to the fact that our collective will [to address these issues] has failed us.”
Among children aged 1-4, drowning was the leading cause of death, followed by congenital anomalies and motor vehicle crashes.
Mandated four-sided fencing around pools is a highly effective intervention for reducing drowning risks, Dr. Hoffman said.
Children aged 5-9 represented the smallest proportion of all youth deaths (12%) and were the only age group not to have injuries as the leading cause of death. Malignant neoplasms led the causes of death in this group, followed by car accidents and congenital anomalies.
Adolescents aged 10-19, the widest age range, comprised 68% of all youth deaths, led by motor vehicle accidents, firearms, and suffocation.
“These findings reflect social and developmental factors that are associated with adolescence, including increased risk-taking behavior, differential peer and parental influence, and initiation of substance use,” Dr. Cunningham and her colleagues wrote.
The most concerning trends, according to Dr. Hoffman, were the upticks in motor vehicle deaths, suffocation, and poisonings, the latter driven largely by opioid overdoses, which were responsible for more than half of all overdoses in adolescents.
Addressing these issues “will require an investment in kids, which is not something that our society does really well,” Dr. Hoffman said. “We talk about it, we tiptoe around it, but when push comes to shove, nobody is really willing to support and fund the efforts to do it.”
In his editorial, Dr. Campion observed that despite a decades-long trend of decreasing mortality from car accidents, these deaths began steadily increasing from 2013 to 2016.
Previous gains in this area came from “the widespread adoption of seat belts and appropriate child safety seats, the production of cars with improved safety standards, better constructed roads, graduated driver-licensing programs, and a focus on reducing teen drinking and driving,” the authors stated. Multiple reasons likely account for the reversal, including distracted driving and possibly marijuana use, though the latter requires more data.
Firearm deaths increased by 28% from 2013 to 2016, driven by suicides (a 26% increase) and homicides (a 32% increase), including increasing school shootings.
Dr. Hoffman acknowledged the complexities of addressing firearm deaths, but “there are effective common sense interventions that could be made ... there’s just not the will.” An example is passing child access prevention (CAP) laws, such as mandating safe storage of guns and imposing criminal liability when children negligently acquire access to firearms. While a variety of small groups address child injury issues, a large, coordinated, centralized national advocacy for kids is lacking, he added.
“The approach to this underrecognized public health problem has to be social as well as technological, and the risks are highest in areas of poverty and social isolation,” Dr. Campion wrote. “We are living in a divisive era in which there are few areas of consensus and agreement. Perhaps one of the few core beliefs that all can agree on is that deaths in childhood and adolescence are tragedies that we must find ways to prevent.”
“Every day, 10 babies die in their sleep, 1.7 kids under age 4 drown, and 4 kids over the age of 1 die in car crashes,” Dr. Hoffman said. “We need to acknowledge the impact of unintentional and intentional injuries and recognize that there are things we can do, that we’re complicit in all of those deaths because in every circumstance, there is something we as a society could have done.”
SOURCE: Cunningham et al. N Engl J Med. 2018 Dec 20;379(25):2468-75. doi: 10.1056/NEJMsr1804754.
Unintentional injuries accounted for more than half of all deaths among U.S. children aged 1-19 years in 2016, according to a new study based on data from the Centers for Disease Control and Prevention Wide-Ranging Online Data for Epidemiologic Research (WONDER) database.
WONDER collects data from U.S. death certificates for 57 vital-statistics jurisdictions, and the 2016 data included 20,360 deaths. Injuries accounted for 12,336 deaths; unintentional injuries accounted for 57% or 7,057 deaths. Approximately one in five U.S. youth deaths (21%) were suicides, and another one in five (20%) were homicides.
Motor vehicle accidents, also responsible for one in five (20%) of all deaths, were the leading cause of accidental deaths, followed by firearm-related injuries, which accounted for 15% of all deaths. Of the firearm-related deaths, 59% were homicides, 35% suicides, 4% accidental, and 2% undetermined.
The only high-ranking noninjury cause of death overall was neoplasms, yet childhood cancer accounted for just 9% of all deaths. Suffocation was the cause of 7% of deaths, and included homicides, suicides and unintentional injuries.
The remaining causes included drowning (5.9%), drug overdose or poisoning (4.8%), congenital anomalies (4.8%), heart disease (2.9%), fire or burns (1.7%) and chronic lower respiratory disease (1.3%).
“Progress toward further reducing deaths among children and adolescents will require a shift in public perceptions so that injury deaths are viewed not as ‘accidents,’ but rather as social ecologic phenomena that are amenable to prevention,” wrote Rebecca M. Cunningham, MD, and her colleagues at the University of Michigan, Ann Arbor (N Engl J Med. 2018 Dec 20. doi: 10.1056/NEJMsr1804754). The findings “highlight the need to implement public health strategies that are tailored according to age, underlying developmental factors, and injury-related intent” to reduce the risk for death in children.”
“The sad fact is that a child or adolescent in the United States is 57% more likely to die by the age of 19 years than those in other wealthy nations,” Edward W. Campion, MD, executive editor and online editor of the New England Journal of Medicine, wrote in an editorial that accompanied the study (N Engl J Med. 2018 Dec. 20;379[25]:2466-7. doi: 10.1056/NEJMe1814600). “Children in America are dying or being killed at rates that are shameful.
“Our country has led the way in so much medical research, but the facts summarized by Cunningham et al. reveal a need to invest far more in research on the prevention of the injuries that threaten the lives of children and adolescents,” he said.
In an interview, Ben Hoffman, MD, professor of pediatrics at Oregon Health and Science University, Portland, said the only thing surprising in this report is that nothing is surprising.
“This is the stuff that those of us in injury prevention have been screaming about for decades,” said Dr. Hoffman, also medical director of the Tom Sargent Safety Center at OHSU Doernbecher Children’s Hospital.
“Unintentional injuries are what kill kids. We have made such tremendous progress in other areas, and we’ve made progress in terms of preventing injuries, but what we see is unacceptable,” he said. “The fact that [injuries] remain such an issue is a testament to the fact that our collective will [to address these issues] has failed us.”
Among children aged 1-4, drowning was the leading cause of death, followed by congenital anomalies and motor vehicle crashes.
Mandated four-sided fencing around pools is a highly effective intervention for reducing drowning risks, Dr. Hoffman said.
Children aged 5-9 represented the smallest proportion of all youth deaths (12%) and were the only age group not to have injuries as the leading cause of death. Malignant neoplasms led the causes of death in this group, followed by car accidents and congenital anomalies.
Adolescents aged 10-19, the widest age range, comprised 68% of all youth deaths, led by motor vehicle accidents, firearms, and suffocation.
“These findings reflect social and developmental factors that are associated with adolescence, including increased risk-taking behavior, differential peer and parental influence, and initiation of substance use,” Dr. Cunningham and her colleagues wrote.
The most concerning trends, according to Dr. Hoffman, were the upticks in motor vehicle deaths, suffocation, and poisonings, the latter driven largely by opioid overdoses, which were responsible for more than half of all overdoses in adolescents.
Addressing these issues “will require an investment in kids, which is not something that our society does really well,” Dr. Hoffman said. “We talk about it, we tiptoe around it, but when push comes to shove, nobody is really willing to support and fund the efforts to do it.”
In his editorial, Dr. Campion observed that despite a decades-long trend of decreasing mortality from car accidents, these deaths began steadily increasing from 2013 to 2016.
Previous gains in this area came from “the widespread adoption of seat belts and appropriate child safety seats, the production of cars with improved safety standards, better constructed roads, graduated driver-licensing programs, and a focus on reducing teen drinking and driving,” the authors stated. Multiple reasons likely account for the reversal, including distracted driving and possibly marijuana use, though the latter requires more data.
Firearm deaths increased by 28% from 2013 to 2016, driven by suicides (a 26% increase) and homicides (a 32% increase), including increasing school shootings.
Dr. Hoffman acknowledged the complexities of addressing firearm deaths, but “there are effective common sense interventions that could be made ... there’s just not the will.” An example is passing child access prevention (CAP) laws, such as mandating safe storage of guns and imposing criminal liability when children negligently acquire access to firearms. While a variety of small groups address child injury issues, a large, coordinated, centralized national advocacy for kids is lacking, he added.
“The approach to this underrecognized public health problem has to be social as well as technological, and the risks are highest in areas of poverty and social isolation,” Dr. Campion wrote. “We are living in a divisive era in which there are few areas of consensus and agreement. Perhaps one of the few core beliefs that all can agree on is that deaths in childhood and adolescence are tragedies that we must find ways to prevent.”
“Every day, 10 babies die in their sleep, 1.7 kids under age 4 drown, and 4 kids over the age of 1 die in car crashes,” Dr. Hoffman said. “We need to acknowledge the impact of unintentional and intentional injuries and recognize that there are things we can do, that we’re complicit in all of those deaths because in every circumstance, there is something we as a society could have done.”
SOURCE: Cunningham et al. N Engl J Med. 2018 Dec 20;379(25):2468-75. doi: 10.1056/NEJMsr1804754.
Unintentional injuries accounted for more than half of all deaths among U.S. children aged 1-19 years in 2016, according to a new study based on data from the Centers for Disease Control and Prevention Wide-Ranging Online Data for Epidemiologic Research (WONDER) database.
WONDER collects data from U.S. death certificates for 57 vital-statistics jurisdictions, and the 2016 data included 20,360 deaths. Injuries accounted for 12,336 deaths; unintentional injuries accounted for 57% or 7,057 deaths. Approximately one in five U.S. youth deaths (21%) were suicides, and another one in five (20%) were homicides.
Motor vehicle accidents, also responsible for one in five (20%) of all deaths, were the leading cause of accidental deaths, followed by firearm-related injuries, which accounted for 15% of all deaths. Of the firearm-related deaths, 59% were homicides, 35% suicides, 4% accidental, and 2% undetermined.
The only high-ranking noninjury cause of death overall was neoplasms, yet childhood cancer accounted for just 9% of all deaths. Suffocation was the cause of 7% of deaths, and included homicides, suicides and unintentional injuries.
The remaining causes included drowning (5.9%), drug overdose or poisoning (4.8%), congenital anomalies (4.8%), heart disease (2.9%), fire or burns (1.7%) and chronic lower respiratory disease (1.3%).
“Progress toward further reducing deaths among children and adolescents will require a shift in public perceptions so that injury deaths are viewed not as ‘accidents,’ but rather as social ecologic phenomena that are amenable to prevention,” wrote Rebecca M. Cunningham, MD, and her colleagues at the University of Michigan, Ann Arbor (N Engl J Med. 2018 Dec 20. doi: 10.1056/NEJMsr1804754). The findings “highlight the need to implement public health strategies that are tailored according to age, underlying developmental factors, and injury-related intent” to reduce the risk for death in children.”
“The sad fact is that a child or adolescent in the United States is 57% more likely to die by the age of 19 years than those in other wealthy nations,” Edward W. Campion, MD, executive editor and online editor of the New England Journal of Medicine, wrote in an editorial that accompanied the study (N Engl J Med. 2018 Dec. 20;379[25]:2466-7. doi: 10.1056/NEJMe1814600). “Children in America are dying or being killed at rates that are shameful.
“Our country has led the way in so much medical research, but the facts summarized by Cunningham et al. reveal a need to invest far more in research on the prevention of the injuries that threaten the lives of children and adolescents,” he said.
In an interview, Ben Hoffman, MD, professor of pediatrics at Oregon Health and Science University, Portland, said the only thing surprising in this report is that nothing is surprising.
“This is the stuff that those of us in injury prevention have been screaming about for decades,” said Dr. Hoffman, also medical director of the Tom Sargent Safety Center at OHSU Doernbecher Children’s Hospital.
“Unintentional injuries are what kill kids. We have made such tremendous progress in other areas, and we’ve made progress in terms of preventing injuries, but what we see is unacceptable,” he said. “The fact that [injuries] remain such an issue is a testament to the fact that our collective will [to address these issues] has failed us.”
Among children aged 1-4, drowning was the leading cause of death, followed by congenital anomalies and motor vehicle crashes.
Mandated four-sided fencing around pools is a highly effective intervention for reducing drowning risks, Dr. Hoffman said.
Children aged 5-9 represented the smallest proportion of all youth deaths (12%) and were the only age group not to have injuries as the leading cause of death. Malignant neoplasms led the causes of death in this group, followed by car accidents and congenital anomalies.
Adolescents aged 10-19, the widest age range, comprised 68% of all youth deaths, led by motor vehicle accidents, firearms, and suffocation.
“These findings reflect social and developmental factors that are associated with adolescence, including increased risk-taking behavior, differential peer and parental influence, and initiation of substance use,” Dr. Cunningham and her colleagues wrote.
The most concerning trends, according to Dr. Hoffman, were the upticks in motor vehicle deaths, suffocation, and poisonings, the latter driven largely by opioid overdoses, which were responsible for more than half of all overdoses in adolescents.
Addressing these issues “will require an investment in kids, which is not something that our society does really well,” Dr. Hoffman said. “We talk about it, we tiptoe around it, but when push comes to shove, nobody is really willing to support and fund the efforts to do it.”
In his editorial, Dr. Campion observed that despite a decades-long trend of decreasing mortality from car accidents, these deaths began steadily increasing from 2013 to 2016.
Previous gains in this area came from “the widespread adoption of seat belts and appropriate child safety seats, the production of cars with improved safety standards, better constructed roads, graduated driver-licensing programs, and a focus on reducing teen drinking and driving,” the authors stated. Multiple reasons likely account for the reversal, including distracted driving and possibly marijuana use, though the latter requires more data.
Firearm deaths increased by 28% from 2013 to 2016, driven by suicides (a 26% increase) and homicides (a 32% increase), including increasing school shootings.
Dr. Hoffman acknowledged the complexities of addressing firearm deaths, but “there are effective common sense interventions that could be made ... there’s just not the will.” An example is passing child access prevention (CAP) laws, such as mandating safe storage of guns and imposing criminal liability when children negligently acquire access to firearms. While a variety of small groups address child injury issues, a large, coordinated, centralized national advocacy for kids is lacking, he added.
“The approach to this underrecognized public health problem has to be social as well as technological, and the risks are highest in areas of poverty and social isolation,” Dr. Campion wrote. “We are living in a divisive era in which there are few areas of consensus and agreement. Perhaps one of the few core beliefs that all can agree on is that deaths in childhood and adolescence are tragedies that we must find ways to prevent.”
“Every day, 10 babies die in their sleep, 1.7 kids under age 4 drown, and 4 kids over the age of 1 die in car crashes,” Dr. Hoffman said. “We need to acknowledge the impact of unintentional and intentional injuries and recognize that there are things we can do, that we’re complicit in all of those deaths because in every circumstance, there is something we as a society could have done.”
SOURCE: Cunningham et al. N Engl J Med. 2018 Dec 20;379(25):2468-75. doi: 10.1056/NEJMsr1804754.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Injury prevention efforts are needed to address unintentional injuries, the leading cause of death in U.S. children.
Major finding: Unintentional injuries were the cause of death for 57% of U.S. children aged 1-19 in 2016.
Study details: The findings are based on an analysis of the CDC WONDER database mortality data on 20,360 deaths of U.S. youth aged 1-19.
Disclosures: No external funding was noted. The authors and Dr. Hoffman had no relevant financial disclosures. Dr. Campion is executive editor of the New England Journal of Medicine.
Source: Cunningham et al. N Engl J Med. 2018 Dec 20;379(25):2468-75. doi: 10.1056/NEJMsr1804754.
How does CBD compare and interact with other AEDs?
according to a review published in Developmental Medicine & Child Neurology. “Careful down-titration of benzodiazepines is essential to minimize sedation with adjunctive CBD,” the authors said.
Although CBD’s antiepileptic mechanisms “are not fully elucidated, it is clear that administration of CBD as adjunct therapy decreases seizure frequency in patients with Dravet syndrome and Lennox-Gastaut syndrome,” wrote Shayma Ali, a doctoral student in the department of pediatrics and child health at the University of Otago in Wellington, New Zealand, and her colleagues. “Contrary to public expectation of miraculous results, CBD has a similar antiepileptic and side effect profile to other AEDs. Nevertheless, as individual children with these developmental and epileptic encephalopathies are often refractory to available AEDs, the addition of another potentially effective therapeutic medicine will be warmly welcomed by families and physicians.”
The FDA approved Epidiolex, a pharmaceutical-grade oral solution that is 98% CBD, in June of 2018. In September of 2018, the Drug Enforcement Administration classified it as a Schedule V controlled substance. Patients’ use of nonpharmaceutical grade CBD products, including those combined with tetrahydrocannabinol (THC), “raises concerns about the use of products with THC on the developing brain,” the review authors said.
Randomized trials
Three randomized, controlled, double-blind trials in patients with Dravet syndrome and Lennox-Gastaut syndrome found that CBD, compared with placebo, results in greater median seizure reductions (38%-41% vs. 13%-19%) and responder rates (i.e., the proportion of patients with 50% reductions in convulsive or drop seizures; 39%-46% vs. 14%-27%).
Common adverse effects include somnolence, diarrhea, decreased appetite, fatigue, lethargy, pyrexia, and vomiting. Hepatic transaminases became elevated in some patients, and this result occurred more often in patients taking valproate.
No phase 2 or phase 3 trials have assessed the efficacy of CBD without coadministration of other AEDs, and CBD’s efficacy may relate to its impact on the pharmacokinetics of coadministered AEDs. “The most important clinical interaction is between CBD and clobazam, as [the dose of] clobazam often needs to be lowered because of excessive sedation,” wrote Ms. Ali and her colleagues. CBD inhibits CYP2C19 and CYP3A4 – enzymes that are involved in clobazam metabolism – which results in high plasma concentrations of clobazam’s active metabolite, norclobazam. Plasma levels of topiramate, rufinamide, zonisamide, and eslicarbazepine also may increase when these drugs are taken with CBD.
Challenges and opportunities
Of the hundreds of compounds in the marijuana plant, CBD “has the most evidence of antiepileptic efficacy and does not have the psychoactive effects” of THC, the authors said. Little evidence supports the combination of THC and CBD for the treatment of epilepsy. In addition, research indicates that THC can have a proconvulsive effect in animal models and harm the development of the human brain.
Investigators are evaluating alternative routes of CBD delivery to avoid first-pass metabolism, such as oromucosal sprays, transdermal gels, eye drops, intranasal sprays, and rectal suppositories. “Alternative methods of administration ... deserve consideration, particularly for the developmental and epileptic encephalopathies population, as administration of oral medication can be challenging,” they said.
SOURCE: Ali S et al. Dev Med Child Neurol. 2018. doi: 10.1111/dmcn.14087.
according to a review published in Developmental Medicine & Child Neurology. “Careful down-titration of benzodiazepines is essential to minimize sedation with adjunctive CBD,” the authors said.
Although CBD’s antiepileptic mechanisms “are not fully elucidated, it is clear that administration of CBD as adjunct therapy decreases seizure frequency in patients with Dravet syndrome and Lennox-Gastaut syndrome,” wrote Shayma Ali, a doctoral student in the department of pediatrics and child health at the University of Otago in Wellington, New Zealand, and her colleagues. “Contrary to public expectation of miraculous results, CBD has a similar antiepileptic and side effect profile to other AEDs. Nevertheless, as individual children with these developmental and epileptic encephalopathies are often refractory to available AEDs, the addition of another potentially effective therapeutic medicine will be warmly welcomed by families and physicians.”
The FDA approved Epidiolex, a pharmaceutical-grade oral solution that is 98% CBD, in June of 2018. In September of 2018, the Drug Enforcement Administration classified it as a Schedule V controlled substance. Patients’ use of nonpharmaceutical grade CBD products, including those combined with tetrahydrocannabinol (THC), “raises concerns about the use of products with THC on the developing brain,” the review authors said.
Randomized trials
Three randomized, controlled, double-blind trials in patients with Dravet syndrome and Lennox-Gastaut syndrome found that CBD, compared with placebo, results in greater median seizure reductions (38%-41% vs. 13%-19%) and responder rates (i.e., the proportion of patients with 50% reductions in convulsive or drop seizures; 39%-46% vs. 14%-27%).
Common adverse effects include somnolence, diarrhea, decreased appetite, fatigue, lethargy, pyrexia, and vomiting. Hepatic transaminases became elevated in some patients, and this result occurred more often in patients taking valproate.
No phase 2 or phase 3 trials have assessed the efficacy of CBD without coadministration of other AEDs, and CBD’s efficacy may relate to its impact on the pharmacokinetics of coadministered AEDs. “The most important clinical interaction is between CBD and clobazam, as [the dose of] clobazam often needs to be lowered because of excessive sedation,” wrote Ms. Ali and her colleagues. CBD inhibits CYP2C19 and CYP3A4 – enzymes that are involved in clobazam metabolism – which results in high plasma concentrations of clobazam’s active metabolite, norclobazam. Plasma levels of topiramate, rufinamide, zonisamide, and eslicarbazepine also may increase when these drugs are taken with CBD.
Challenges and opportunities
Of the hundreds of compounds in the marijuana plant, CBD “has the most evidence of antiepileptic efficacy and does not have the psychoactive effects” of THC, the authors said. Little evidence supports the combination of THC and CBD for the treatment of epilepsy. In addition, research indicates that THC can have a proconvulsive effect in animal models and harm the development of the human brain.
Investigators are evaluating alternative routes of CBD delivery to avoid first-pass metabolism, such as oromucosal sprays, transdermal gels, eye drops, intranasal sprays, and rectal suppositories. “Alternative methods of administration ... deserve consideration, particularly for the developmental and epileptic encephalopathies population, as administration of oral medication can be challenging,” they said.
SOURCE: Ali S et al. Dev Med Child Neurol. 2018. doi: 10.1111/dmcn.14087.
according to a review published in Developmental Medicine & Child Neurology. “Careful down-titration of benzodiazepines is essential to minimize sedation with adjunctive CBD,” the authors said.
Although CBD’s antiepileptic mechanisms “are not fully elucidated, it is clear that administration of CBD as adjunct therapy decreases seizure frequency in patients with Dravet syndrome and Lennox-Gastaut syndrome,” wrote Shayma Ali, a doctoral student in the department of pediatrics and child health at the University of Otago in Wellington, New Zealand, and her colleagues. “Contrary to public expectation of miraculous results, CBD has a similar antiepileptic and side effect profile to other AEDs. Nevertheless, as individual children with these developmental and epileptic encephalopathies are often refractory to available AEDs, the addition of another potentially effective therapeutic medicine will be warmly welcomed by families and physicians.”
The FDA approved Epidiolex, a pharmaceutical-grade oral solution that is 98% CBD, in June of 2018. In September of 2018, the Drug Enforcement Administration classified it as a Schedule V controlled substance. Patients’ use of nonpharmaceutical grade CBD products, including those combined with tetrahydrocannabinol (THC), “raises concerns about the use of products with THC on the developing brain,” the review authors said.
Randomized trials
Three randomized, controlled, double-blind trials in patients with Dravet syndrome and Lennox-Gastaut syndrome found that CBD, compared with placebo, results in greater median seizure reductions (38%-41% vs. 13%-19%) and responder rates (i.e., the proportion of patients with 50% reductions in convulsive or drop seizures; 39%-46% vs. 14%-27%).
Common adverse effects include somnolence, diarrhea, decreased appetite, fatigue, lethargy, pyrexia, and vomiting. Hepatic transaminases became elevated in some patients, and this result occurred more often in patients taking valproate.
No phase 2 or phase 3 trials have assessed the efficacy of CBD without coadministration of other AEDs, and CBD’s efficacy may relate to its impact on the pharmacokinetics of coadministered AEDs. “The most important clinical interaction is between CBD and clobazam, as [the dose of] clobazam often needs to be lowered because of excessive sedation,” wrote Ms. Ali and her colleagues. CBD inhibits CYP2C19 and CYP3A4 – enzymes that are involved in clobazam metabolism – which results in high plasma concentrations of clobazam’s active metabolite, norclobazam. Plasma levels of topiramate, rufinamide, zonisamide, and eslicarbazepine also may increase when these drugs are taken with CBD.
Challenges and opportunities
Of the hundreds of compounds in the marijuana plant, CBD “has the most evidence of antiepileptic efficacy and does not have the psychoactive effects” of THC, the authors said. Little evidence supports the combination of THC and CBD for the treatment of epilepsy. In addition, research indicates that THC can have a proconvulsive effect in animal models and harm the development of the human brain.
Investigators are evaluating alternative routes of CBD delivery to avoid first-pass metabolism, such as oromucosal sprays, transdermal gels, eye drops, intranasal sprays, and rectal suppositories. “Alternative methods of administration ... deserve consideration, particularly for the developmental and epileptic encephalopathies population, as administration of oral medication can be challenging,” they said.
SOURCE: Ali S et al. Dev Med Child Neurol. 2018. doi: 10.1111/dmcn.14087.
FROM DEVELOPMENTAL MEDICINE & CHILD NEUROLOGY
Key clinical point: Cannabidiol’s efficacy is similar to that of other antiepileptic drugs.
Major finding: Cannabidiol inhibits CYP2C19 and CYP3A4, which are involved in clobazam metabolism.
Study details: An invited review.
Disclosures: No disclosures were reported.
Source: Ali S et al. Dev Med Child Neurol. 2018. doi: 10.1111/dmcn.14087.
Guideline-concordant treatment still unlikely in nonchildren’s hospitals for pediatric CAP
according to new research.

“This gap is concerning because approximately 70% of children hospitalized with pneumonia receive care in nonchildren’s hospitals,” wrote Alison C. Tribble, MD, of C. S. Mott Children’s Hospital, University of Michigan, Ann Arbor, and her associates. The report is in JAMA Pediatrics.
Data were collected from the Pediatric Health Information System (children’s hospitals) and Premier Perspectives (all hospitals) databases and included a total of 120,238 children aged 1-17 years diagnosed with CAP between Jan. 1, 2009, and Sept. 30, 2015. Before the publication of the new guideline in October 2011, the probability of receiving what would become guideline-concordant antibiotics was 0.25 in children’s hospitals and 0.06 in nonchildren’s hospitals.
By the end of the study period, the probability of receiving guideline-concordant antibiotics for pediatric CAP was 0.61 in children’s hospitals and 0.27 in nonchildren’s hospitals. Without the interventions, the probabilities would have been 0.31 and 0.08, respectively. The rate of growth over the 4-year postintervention period was similar in both children’s and nonchildren’s hospitals.
“Studies in children’s hospitals have suggested that local implementation efforts may be important in facilitating guideline uptake. Nonchildren’s hospitals likely have fewer resources to lead pediatric-specific efforts, and care may be influenced by adult CAP guidelines,” the authors noted.
No conflicts of interest were reported.
SOURCE: Tribble AC et al. JAMA Pediatr. 2018 Dec 10. doi: 10.1001/jamapediatrics.2018.4270.
according to new research.
“This gap is concerning because approximately 70% of children hospitalized with pneumonia receive care in nonchildren’s hospitals,” wrote Alison C. Tribble, MD, of C. S. Mott Children’s Hospital, University of Michigan, Ann Arbor, and her associates. The report is in JAMA Pediatrics.
Data were collected from the Pediatric Health Information System (children’s hospitals) and Premier Perspectives (all hospitals) databases and included a total of 120,238 children aged 1-17 years diagnosed with CAP between Jan. 1, 2009, and Sept. 30, 2015. Before the publication of the new guideline in October 2011, the probability of receiving what would become guideline-concordant antibiotics was 0.25 in children’s hospitals and 0.06 in nonchildren’s hospitals.
By the end of the study period, the probability of receiving guideline-concordant antibiotics for pediatric CAP was 0.61 in children’s hospitals and 0.27 in nonchildren’s hospitals. Without the interventions, the probabilities would have been 0.31 and 0.08, respectively. The rate of growth over the 4-year postintervention period was similar in both children’s and nonchildren’s hospitals.
“Studies in children’s hospitals have suggested that local implementation efforts may be important in facilitating guideline uptake. Nonchildren’s hospitals likely have fewer resources to lead pediatric-specific efforts, and care may be influenced by adult CAP guidelines,” the authors noted.
No conflicts of interest were reported.
SOURCE: Tribble AC et al. JAMA Pediatr. 2018 Dec 10. doi: 10.1001/jamapediatrics.2018.4270.
according to new research.
“This gap is concerning because approximately 70% of children hospitalized with pneumonia receive care in nonchildren’s hospitals,” wrote Alison C. Tribble, MD, of C. S. Mott Children’s Hospital, University of Michigan, Ann Arbor, and her associates. The report is in JAMA Pediatrics.
Data were collected from the Pediatric Health Information System (children’s hospitals) and Premier Perspectives (all hospitals) databases and included a total of 120,238 children aged 1-17 years diagnosed with CAP between Jan. 1, 2009, and Sept. 30, 2015. Before the publication of the new guideline in October 2011, the probability of receiving what would become guideline-concordant antibiotics was 0.25 in children’s hospitals and 0.06 in nonchildren’s hospitals.
By the end of the study period, the probability of receiving guideline-concordant antibiotics for pediatric CAP was 0.61 in children’s hospitals and 0.27 in nonchildren’s hospitals. Without the interventions, the probabilities would have been 0.31 and 0.08, respectively. The rate of growth over the 4-year postintervention period was similar in both children’s and nonchildren’s hospitals.
“Studies in children’s hospitals have suggested that local implementation efforts may be important in facilitating guideline uptake. Nonchildren’s hospitals likely have fewer resources to lead pediatric-specific efforts, and care may be influenced by adult CAP guidelines,” the authors noted.
No conflicts of interest were reported.
SOURCE: Tribble AC et al. JAMA Pediatr. 2018 Dec 10. doi: 10.1001/jamapediatrics.2018.4270.
FROM JAMA PEDIATRICS
CHMP backs dasatinib for kids with newly diagnosed ALL

The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended expanding the marketing authorization for dasatinib (Sprycel).
The CHMP’s recommendation is to approve dasatinib in combination with chemotherapy to treat pediatric patients with newly diagnosed, Philadelphia chromosome-positive (Ph+) acute lymphoblastic leukemia (ALL).
The CHMP’s recommendation will be reviewed by the European Commission (EC), which has the authority to approve medicines for use in the European Union, Norway, Iceland, and Liechtenstein.
The EC usually makes a decision within 67 days of a CHMP recommendation.
Dasatinib is already EC-approved to treat:
- Adults with newly diagnosed, Ph+ chronic myelogenous leukemia (CML) in the chronic phase
- Adults with chronic, accelerated, or blast phase CML with resistance or intolerance to prior therapy including imatinib
- Adults with Ph+ ALL and lymphoid blast CML with resistance or intolerance to prior therapy
- Pediatric patients with newly diagnosed, Ph+ CML in chronic phase
- Pediatric patients with Ph+ CML in chronic phase that is resistant or intolerant to prior therapy including imatinib.
Phase 2 trial
The CHMP’s recommendation to approve dasatinib in pediatric patients with newly diagnosed, Ph+ ALL is based on data from a phase 2 trial (NCT01460160). In this trial, researchers are evaluating dasatinib in combination with a chemotherapy regimen modeled on a Berlin-Frankfurt-Munster high-risk backbone.
Results from the trial were presented at the 2017 ASH Annual Meeting.
At that time, 106 patients had been treated. They received continuous daily dasatinib (60 mg/m2) beginning at day 15 of induction chemotherapy. All treated patients achieved complete remission.
Patients who had evidence of minimal residual disease (MRD) ≥ 0.05% at the end of the first block of treatment (day 78) and those with MRD 0.005% to 0.05% who remained MRD-positive at any detectable level after three additional high-risk chemotherapy blocks were eligible for hematopoietic stem cell transplant (HSCT) in first remission.
Nineteen patients met these criteria, and 15 (14.2%) received HSCT. The remaining 85.8% of patients received dasatinib plus chemotherapy for two years.
The 3-year event-free survival rate was 65.5%, and the 3-year overall survival rate was 91.5%.
Two patients discontinued dasatinib due to toxicity—one due to allergy and one due to prolonged thrombocytopenia.
Grade 3/4 adverse events attributed to dasatinib included elevated alanine aminotransferase (21.7%), elevated aspartate transaminase (10.4%), pleural effusion (3.8%), edema (2.8%), hemorrhage (5.7%), and cardiac failure (0.8%).
Five patients died while receiving chemotherapy (three from sepsis, one due to pneumonia, and one of an unknown cause). Two deaths were HSCT-related.
This trial was sponsored by Bristol-Myers Squibb.
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended expanding the marketing authorization for dasatinib (Sprycel).
The CHMP’s recommendation is to approve dasatinib in combination with chemotherapy to treat pediatric patients with newly diagnosed, Philadelphia chromosome-positive (Ph+) acute lymphoblastic leukemia (ALL).
The CHMP’s recommendation will be reviewed by the European Commission (EC), which has the authority to approve medicines for use in the European Union, Norway, Iceland, and Liechtenstein.
The EC usually makes a decision within 67 days of a CHMP recommendation.
Dasatinib is already EC-approved to treat:
- Adults with newly diagnosed, Ph+ chronic myelogenous leukemia (CML) in the chronic phase
- Adults with chronic, accelerated, or blast phase CML with resistance or intolerance to prior therapy including imatinib
- Adults with Ph+ ALL and lymphoid blast CML with resistance or intolerance to prior therapy
- Pediatric patients with newly diagnosed, Ph+ CML in chronic phase
- Pediatric patients with Ph+ CML in chronic phase that is resistant or intolerant to prior therapy including imatinib.
Phase 2 trial
The CHMP’s recommendation to approve dasatinib in pediatric patients with newly diagnosed, Ph+ ALL is based on data from a phase 2 trial (NCT01460160). In this trial, researchers are evaluating dasatinib in combination with a chemotherapy regimen modeled on a Berlin-Frankfurt-Munster high-risk backbone.
Results from the trial were presented at the 2017 ASH Annual Meeting.
At that time, 106 patients had been treated. They received continuous daily dasatinib (60 mg/m2) beginning at day 15 of induction chemotherapy. All treated patients achieved complete remission.
Patients who had evidence of minimal residual disease (MRD) ≥ 0.05% at the end of the first block of treatment (day 78) and those with MRD 0.005% to 0.05% who remained MRD-positive at any detectable level after three additional high-risk chemotherapy blocks were eligible for hematopoietic stem cell transplant (HSCT) in first remission.
Nineteen patients met these criteria, and 15 (14.2%) received HSCT. The remaining 85.8% of patients received dasatinib plus chemotherapy for two years.
The 3-year event-free survival rate was 65.5%, and the 3-year overall survival rate was 91.5%.
Two patients discontinued dasatinib due to toxicity—one due to allergy and one due to prolonged thrombocytopenia.
Grade 3/4 adverse events attributed to dasatinib included elevated alanine aminotransferase (21.7%), elevated aspartate transaminase (10.4%), pleural effusion (3.8%), edema (2.8%), hemorrhage (5.7%), and cardiac failure (0.8%).
Five patients died while receiving chemotherapy (three from sepsis, one due to pneumonia, and one of an unknown cause). Two deaths were HSCT-related.
This trial was sponsored by Bristol-Myers Squibb.
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended expanding the marketing authorization for dasatinib (Sprycel).
The CHMP’s recommendation is to approve dasatinib in combination with chemotherapy to treat pediatric patients with newly diagnosed, Philadelphia chromosome-positive (Ph+) acute lymphoblastic leukemia (ALL).
The CHMP’s recommendation will be reviewed by the European Commission (EC), which has the authority to approve medicines for use in the European Union, Norway, Iceland, and Liechtenstein.
The EC usually makes a decision within 67 days of a CHMP recommendation.
Dasatinib is already EC-approved to treat:
- Adults with newly diagnosed, Ph+ chronic myelogenous leukemia (CML) in the chronic phase
- Adults with chronic, accelerated, or blast phase CML with resistance or intolerance to prior therapy including imatinib
- Adults with Ph+ ALL and lymphoid blast CML with resistance or intolerance to prior therapy
- Pediatric patients with newly diagnosed, Ph+ CML in chronic phase
- Pediatric patients with Ph+ CML in chronic phase that is resistant or intolerant to prior therapy including imatinib.
Phase 2 trial
The CHMP’s recommendation to approve dasatinib in pediatric patients with newly diagnosed, Ph+ ALL is based on data from a phase 2 trial (NCT01460160). In this trial, researchers are evaluating dasatinib in combination with a chemotherapy regimen modeled on a Berlin-Frankfurt-Munster high-risk backbone.
Results from the trial were presented at the 2017 ASH Annual Meeting.
At that time, 106 patients had been treated. They received continuous daily dasatinib (60 mg/m2) beginning at day 15 of induction chemotherapy. All treated patients achieved complete remission.
Patients who had evidence of minimal residual disease (MRD) ≥ 0.05% at the end of the first block of treatment (day 78) and those with MRD 0.005% to 0.05% who remained MRD-positive at any detectable level after three additional high-risk chemotherapy blocks were eligible for hematopoietic stem cell transplant (HSCT) in first remission.
Nineteen patients met these criteria, and 15 (14.2%) received HSCT. The remaining 85.8% of patients received dasatinib plus chemotherapy for two years.
The 3-year event-free survival rate was 65.5%, and the 3-year overall survival rate was 91.5%.
Two patients discontinued dasatinib due to toxicity—one due to allergy and one due to prolonged thrombocytopenia.
Grade 3/4 adverse events attributed to dasatinib included elevated alanine aminotransferase (21.7%), elevated aspartate transaminase (10.4%), pleural effusion (3.8%), edema (2.8%), hemorrhage (5.7%), and cardiac failure (0.8%).
Five patients died while receiving chemotherapy (three from sepsis, one due to pneumonia, and one of an unknown cause). Two deaths were HSCT-related.
This trial was sponsored by Bristol-Myers Squibb.
BMI compares favorably with body scanning for ID of cardiometabolic traits
Although body mass index is criticized for not distinguishing fat from lean mass, its ability to detect subclinical cardiometabolic abnormalities was on par with more sophisticated body scanning technology, according a recent analysis.
BMI and dual-energy x-ray absorptiometry (DXA) had similar associations with cardiometabolic traits associated with coronary heart disease in individuals evaluated at 10 and 18 years of age in a population-based birth cohort study, the study investigators said.
Changes over time in BMI and DXA also were strongly associated with changes in blood pressure, cholesterol, and other markers, according to Joshua A. Bell, PhD, of MRC Integrative Epidemiology Unit, University of Bristol, England, and his coinvestigators.
“Altogether, the results support abdominal fatness as a primary driver of cardiometabolic dysfunction and BMI as a useful tool for detecting its effects,” Dr. Bell and his colleagues said in a report on the study appearing in the Journal of the American College of Cardiology.
In their analysis, Dr. Bell and coinvestigators used Pearson correlation coefficients to compare BMI and total and regional fat indexes from DXA in offspring participants from ALSPAC, (the Avon Longitudinal Study of Parents and Children), in which BMI and DXA measurements were collected at 10 and 18 years of age.
Researchers identified a total of 2,840 participants with at least one measurement at each of those time points. The mean BMI was 17.5 kg/m2 at 10 years of age and 22.7 kg/m2 at 18 years of age, with greater than 10% of participants classified as obese at each of those time points.
High BMI and high total fat mass index were similarly associated with a variety of cardiometabolic traits, including systolic and diastolic blood pressure, higher low-density lipoprotein (LDL) and very-low-density lipoprotein (VLDL) cholesterol levels and lower high-density lipoprotein (HDL) cholesterol levels, and more inflammation, investigators found.
BMI was strongly correlated with DXA total and regional fat indexes at 10 years of age, and again at 18 years of age, they reported.
Moreover, gains in BMI from 10 to 18 years of age were strongly associated with higher blood pressure, higher LDL and VLDL cholesterol, lower HDL cholesterol, and other cardiometabolic traits, while associations between DXA measurements and those traits closely tracked those of BMI in pattern and magnitude, investigators added.
Fatness is most often measured in populations using BMI, and causal analyses suggest linkage between higher BMI and coronary heart disease and its intermediates, including blood pressure, LDL and remnant cholesterol, and glucose; despite that, BMI is often disparaged as a tool for assessing cardiometabolic abnormalities because it does not distinguish fat from lean mass and cannot quantify fat distribution, investigators said.
However, based on results of this analysis, it is reasonable to depend on BMI to indirectly measure body and abdominal fatness in future studies, they said in their report.
Dr. Bell and his colleagues reported that they had no relationships relevant to the study publication.
SOURCE: Bell JA et al. J Am Coll Cardiol. 2018 Dec 18;72(24):3142-54.
This study reinforces fatness, quantified by body mass index, as the key modifiable factor for maintaining healthy metabolism in young people, according to Ville-Petteri Mäkinen, ScD.
“The good news is that a single BMI measurement may be enough to capture the same essential information as a detailed body scan and serial measurements,” Dr. Mäkinen wrote in an accompanying editorial.
One other important take-home message of the study is that fat gain is not beneficial in any body region; that finding is important with respect to changes in BMI and fat mass index observed in the second decade of life that were associated with cardiometabolic risk factors in the late teens, he noted.
However, the broader take-home message for society is that children are being exposed to an “adverse metabolic milieu” that predicts cardiovascular disease in adulthood, according to Dr. Mäkinen.
“Childhood obesity must not be seen as a phase that passes but as a looming public health crisis that needs to be addressed by all of us,” he concluded.
Dr. Mäkinen is with the South Australian Health and Medical Research Institute, Adelaide. He had no relationships relevant to the contents of his editorial (J Am College Cardiol. 2018 Dec 18;74[24]3155-7).
This study reinforces fatness, quantified by body mass index, as the key modifiable factor for maintaining healthy metabolism in young people, according to Ville-Petteri Mäkinen, ScD.
“The good news is that a single BMI measurement may be enough to capture the same essential information as a detailed body scan and serial measurements,” Dr. Mäkinen wrote in an accompanying editorial.
One other important take-home message of the study is that fat gain is not beneficial in any body region; that finding is important with respect to changes in BMI and fat mass index observed in the second decade of life that were associated with cardiometabolic risk factors in the late teens, he noted.
However, the broader take-home message for society is that children are being exposed to an “adverse metabolic milieu” that predicts cardiovascular disease in adulthood, according to Dr. Mäkinen.
“Childhood obesity must not be seen as a phase that passes but as a looming public health crisis that needs to be addressed by all of us,” he concluded.
Dr. Mäkinen is with the South Australian Health and Medical Research Institute, Adelaide. He had no relationships relevant to the contents of his editorial (J Am College Cardiol. 2018 Dec 18;74[24]3155-7).
This study reinforces fatness, quantified by body mass index, as the key modifiable factor for maintaining healthy metabolism in young people, according to Ville-Petteri Mäkinen, ScD.
“The good news is that a single BMI measurement may be enough to capture the same essential information as a detailed body scan and serial measurements,” Dr. Mäkinen wrote in an accompanying editorial.
One other important take-home message of the study is that fat gain is not beneficial in any body region; that finding is important with respect to changes in BMI and fat mass index observed in the second decade of life that were associated with cardiometabolic risk factors in the late teens, he noted.
However, the broader take-home message for society is that children are being exposed to an “adverse metabolic milieu” that predicts cardiovascular disease in adulthood, according to Dr. Mäkinen.
“Childhood obesity must not be seen as a phase that passes but as a looming public health crisis that needs to be addressed by all of us,” he concluded.
Dr. Mäkinen is with the South Australian Health and Medical Research Institute, Adelaide. He had no relationships relevant to the contents of his editorial (J Am College Cardiol. 2018 Dec 18;74[24]3155-7).
Although body mass index is criticized for not distinguishing fat from lean mass, its ability to detect subclinical cardiometabolic abnormalities was on par with more sophisticated body scanning technology, according a recent analysis.
BMI and dual-energy x-ray absorptiometry (DXA) had similar associations with cardiometabolic traits associated with coronary heart disease in individuals evaluated at 10 and 18 years of age in a population-based birth cohort study, the study investigators said.
Changes over time in BMI and DXA also were strongly associated with changes in blood pressure, cholesterol, and other markers, according to Joshua A. Bell, PhD, of MRC Integrative Epidemiology Unit, University of Bristol, England, and his coinvestigators.
“Altogether, the results support abdominal fatness as a primary driver of cardiometabolic dysfunction and BMI as a useful tool for detecting its effects,” Dr. Bell and his colleagues said in a report on the study appearing in the Journal of the American College of Cardiology.
In their analysis, Dr. Bell and coinvestigators used Pearson correlation coefficients to compare BMI and total and regional fat indexes from DXA in offspring participants from ALSPAC, (the Avon Longitudinal Study of Parents and Children), in which BMI and DXA measurements were collected at 10 and 18 years of age.
Researchers identified a total of 2,840 participants with at least one measurement at each of those time points. The mean BMI was 17.5 kg/m2 at 10 years of age and 22.7 kg/m2 at 18 years of age, with greater than 10% of participants classified as obese at each of those time points.
High BMI and high total fat mass index were similarly associated with a variety of cardiometabolic traits, including systolic and diastolic blood pressure, higher low-density lipoprotein (LDL) and very-low-density lipoprotein (VLDL) cholesterol levels and lower high-density lipoprotein (HDL) cholesterol levels, and more inflammation, investigators found.
BMI was strongly correlated with DXA total and regional fat indexes at 10 years of age, and again at 18 years of age, they reported.
Moreover, gains in BMI from 10 to 18 years of age were strongly associated with higher blood pressure, higher LDL and VLDL cholesterol, lower HDL cholesterol, and other cardiometabolic traits, while associations between DXA measurements and those traits closely tracked those of BMI in pattern and magnitude, investigators added.
Fatness is most often measured in populations using BMI, and causal analyses suggest linkage between higher BMI and coronary heart disease and its intermediates, including blood pressure, LDL and remnant cholesterol, and glucose; despite that, BMI is often disparaged as a tool for assessing cardiometabolic abnormalities because it does not distinguish fat from lean mass and cannot quantify fat distribution, investigators said.
However, based on results of this analysis, it is reasonable to depend on BMI to indirectly measure body and abdominal fatness in future studies, they said in their report.
Dr. Bell and his colleagues reported that they had no relationships relevant to the study publication.
SOURCE: Bell JA et al. J Am Coll Cardiol. 2018 Dec 18;72(24):3142-54.
Although body mass index is criticized for not distinguishing fat from lean mass, its ability to detect subclinical cardiometabolic abnormalities was on par with more sophisticated body scanning technology, according a recent analysis.
BMI and dual-energy x-ray absorptiometry (DXA) had similar associations with cardiometabolic traits associated with coronary heart disease in individuals evaluated at 10 and 18 years of age in a population-based birth cohort study, the study investigators said.
Changes over time in BMI and DXA also were strongly associated with changes in blood pressure, cholesterol, and other markers, according to Joshua A. Bell, PhD, of MRC Integrative Epidemiology Unit, University of Bristol, England, and his coinvestigators.
“Altogether, the results support abdominal fatness as a primary driver of cardiometabolic dysfunction and BMI as a useful tool for detecting its effects,” Dr. Bell and his colleagues said in a report on the study appearing in the Journal of the American College of Cardiology.
In their analysis, Dr. Bell and coinvestigators used Pearson correlation coefficients to compare BMI and total and regional fat indexes from DXA in offspring participants from ALSPAC, (the Avon Longitudinal Study of Parents and Children), in which BMI and DXA measurements were collected at 10 and 18 years of age.
Researchers identified a total of 2,840 participants with at least one measurement at each of those time points. The mean BMI was 17.5 kg/m2 at 10 years of age and 22.7 kg/m2 at 18 years of age, with greater than 10% of participants classified as obese at each of those time points.
High BMI and high total fat mass index were similarly associated with a variety of cardiometabolic traits, including systolic and diastolic blood pressure, higher low-density lipoprotein (LDL) and very-low-density lipoprotein (VLDL) cholesterol levels and lower high-density lipoprotein (HDL) cholesterol levels, and more inflammation, investigators found.
BMI was strongly correlated with DXA total and regional fat indexes at 10 years of age, and again at 18 years of age, they reported.
Moreover, gains in BMI from 10 to 18 years of age were strongly associated with higher blood pressure, higher LDL and VLDL cholesterol, lower HDL cholesterol, and other cardiometabolic traits, while associations between DXA measurements and those traits closely tracked those of BMI in pattern and magnitude, investigators added.
Fatness is most often measured in populations using BMI, and causal analyses suggest linkage between higher BMI and coronary heart disease and its intermediates, including blood pressure, LDL and remnant cholesterol, and glucose; despite that, BMI is often disparaged as a tool for assessing cardiometabolic abnormalities because it does not distinguish fat from lean mass and cannot quantify fat distribution, investigators said.
However, based on results of this analysis, it is reasonable to depend on BMI to indirectly measure body and abdominal fatness in future studies, they said in their report.
Dr. Bell and his colleagues reported that they had no relationships relevant to the study publication.
SOURCE: Bell JA et al. J Am Coll Cardiol. 2018 Dec 18;72(24):3142-54.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Key clinical point: Body mass index and dual-energy x-ray absorptiometry had similar associations with cardiometabolic abnormalities in individuals evaluated at 10 and 18 years of age.
Major finding: BMI was strongly correlated with DXA total and regional fat indexes at age 10 years (0.9) and age 18 years.
Study details: Analysis of 2,840 offspring participants in ALSPAC (the Avon Longitudinal Study of Parents and Children).
Disclosures: Study authors reported that they had no relationships relevant to the study or its publication.
Source: Bell JA et al. J Am Coll Cardiol. 2018 Dec 10;72(24):3142-54.