User login
Inside the Patient-Oncologist Bond: Why It’s Often So Strong
Rose Gerber was 39, mother to a third grader and a kindergartener, when the diagnosis came: Advanced HER2-positive breast cancer.
“On one of my first or second appointments, I took in a little picture of Alexander and Isabella,” Gerber said. Gerber showed her oncologist the picture and told her: “I’ll do anything. I just want to be there for them.”
That was 21 years ago. Today, her current cancer status is “no evidence of disease.”
Over the past 2 decades, Gerber has gotten to be there for her children. Her youngest is now a television producer and her oldest, a CPA.
In that time,
“I’ve seen multiple physicians over my 21 years, but my oncologist has always been the focal point, guiding me in the right direction,” Gerber said in an interview.
Over the years, Jaga guided Gerber through a range of treatment decisions, including a Herceptin clinical trial that the mom of two views as lifesaving. Jaga often took on the role of both doctor and therapist, even providing comfort in the smaller moments when Gerber would fret about her weight gain.
The oncologist-patient “bond is very, very, very special,” said Gerber, who now works as director of patient advocacy and education at the Community Oncology Alliance.
Gerber isn’t alone in calling out the depth of the oncologist-patient bond.
Over years, sometimes decades, patients and oncologists can experience a whole world together: The treatment successes, relapses, uncertainties, and tough calls. As a result, a deep therapeutic alliance often develops. And with each new hurdle or decision, that collaborative, human connection between doctor and patient continues to form new layers.
“It’s like a shared bonding experience over trauma, like strangers trapped on a subway and then we get out, and we’re now on the other side, celebrating together,” said Saad Khan, MD, an associate professor of medicine (oncology) at Stanford University in California.
Connecting Through Stress
Although studies exploring the oncologist-patient bond are limited, some research suggests that a strong therapeutic alliance between patients and oncologists not only provides a foundation for quality care but can also help improve patients’ quality of life, protect against suicidal ideation, and increase treatment adherence.
Because of how stressful and frightening a cancer diagnosis can be, creating “a trusting, uninterrupted, almost sacred environment for them” is paramount for Khan. “I have no doubt that the most important part of their treatment is that they find an oncologist in whom they have total confidence,” Khan wrote in a blog.
The stress that patients with cancer experience is well documented, but oncologists take on a lot themselves and can also experience intense stress (.
“I consider my patient’s battles to be my battles,” Khan wrote.
The stress can start with the daily schedule. Oncologists often have a high volume of patients and tend to spend more time with each individual than most.
According to a 2023 survey, oncologists see about 68 patients a week, on average, but some oncologists, like Khan, have many more. Khan typically sees 20-30 patients a day and continues to care for many over years.
The survey also found that oncologists tend to spend a lot of time with their patients. Compared with other physicians, oncologists are two times more likely to spend at least 25 minutes with each patient.
With this kind of patient volume and time, Khan said, “you’re going to be exhausted.”
What can compound the exhaustion are the occasions oncologists need to deliver bad news — this treatment isn’t working, your cancer has come roaring back and, perhaps the hardest, we have no therapeutic options left. The end-of-life conversations, in particular, can be heartbreaking, especially when a patient is young and not ready to stop trying.
“It can be hard for doctors to discuss the end of life,” Don Dizon, MD, director of the Pelvic Malignancies Program at Lifespan Cancer Institute and director of Medical Oncology at Rhode Island Hospital, Providence, wrote in a column in 2023. Instead, it can be tempting and is often easier to focus on the next treatment, “instilling hope that there’s more that can be done,” even if doing more will only do harm.
In the face of these challenging decisions, growing a personal connection with patients over time can help keep oncologists going.
“We’re not just chemotherapy salesmen,” Khan said in an interview. “We get to know their social support network, who’s going to be driving them [to and from appointments], where they go on vacation, their cat’s name, who their neighbors are.”
A ‘Special Relationship’
Ralph V. Boccia, MD, is often asked what he does.
The next question that often comes — “Why do I do what I do?” — is Boccia’s favorite.
“Someone needs to take these patients through their journey,” Boccia, the founder of The Center for Cancer and Blood Disorders, Bethesda, Maryland, typically responds. He also often notes that “it is a special relationship you develop with the patient and their families.”
Boccia thinks about one long-term patient who captures this bond.
Joan Pinson, 70, was diagnosed with multiple myeloma about 25 years ago, when patients’ average survival was about 4 years.
Over a quarter century, Pinson has pivoted to different treatments, amid multiple relapses and remissions. Throughout most of this cancer journey, Boccia has been her primary oncologist, performing a stem cell transplant in 2000 and steering her to six clinical trials.
Her last relapse was 2 years ago, and since then she has been doing well on oral chemotherapy.
“Every time I relapsed, by the next appointment, he’d say, ‘here is what we are going to do,’ ” Pinson recalled. “I never worried, I never panicked. I knew he would take care of me.”
Over the years, Pinson and Boccia have shared many personal moments, sometimes by accident. One special moment happened early on in Pinson’s cancer journey. During an appointment, Boccia had “one ear to the phone” as his wife was about to deliver their first baby, Pinson recalled.
Later, Pinson met that child as a young man working in Boccia’s lab. She has also met Boccia’s wife, a nurse, when she filled in one day in the chemotherapy room.
Boccia now also treats Pinson’s husband who has prostate cancer, and he ruled out cancer when Pinson’s son, now in his 40s, had some worrisome symptoms.
More than 2 decades ago, Pinson told Boccia her goal was to see her youngest child graduate from high school. Now, six grandsons later, she has lived far beyond that goal.
“He has kept me alive,” said Pinson.
The Dying Patient
Harsha Vyas, MD, FACP, remembers the first encounter his office had with a 29-year-old woman referred with a diagnosis of stage IV breast cancer.
After just 15 minutes in the waiting room, the woman announced she was leaving. Although office staff assured the woman that she was next, the patient walked out.
Several months later, Vyas was called for an inpatient consult. It was the same woman.
Her lungs were full of fluid, and she was struggling to breathe, said Vyas, president and CEO of the Cancer Center of Middle Georgia, Dublin, and assistant professor at Augusta University in Georgia.
The woman, a single mother, told Vyas about her three young kids at home and asked him, “Doc, do something, please help me,” he recalled.
“Absolutely,” Vyas told her. But he had to be brutally honest about her prognosis and firm that she needed to follow his instructions. “You have a breast cancer I cannot cure,” he said. “All I can do is control the disease.”
From that first day, until the day she died, she came to every appointment and followed the treatment plan Vyas laid out.
For about 2 years, she responded well to treatment. And as the time passed and the trust grew, she began to open up to him. She showed him pictures. She talked about her children and being a mother.
“I’ve got to get my kids in a better place. I’m going to be there for them,” he recalled her saying.
Vyas admired her resourcefulness. She held down a part-time job, working retail and at a local restaurant. She figured out childcare so she could get to her chemotherapy appointments every 3 weeks and manage the copays.
Several years later, when she knew she was approaching the end of her life, she asked Vyas a question that hit hard.
“Doc, I don’t want to die and my kids find me dead. What can we do about it?”
Vyas, who has three daughters, imagined how traumatic this would be for a child. She and Vyas made the shared decision to cease treatment and begin home hospice. When the end was approaching, a hospice worker took over, waiting for bodily functions to cease.
When news of a death comes, “I say a little prayer, it’s almost like a send-off for that soul. That helps me absorb the news ... and let it go.”
But when the bond grows strong over time, as with his patient with breast cancer, Vyas said, “a piece of her is still with me.”
Khan had no relevant disclosures. Boccia and Vyas had no disclosures.
A version of this article appeared on Medscape.com.
Rose Gerber was 39, mother to a third grader and a kindergartener, when the diagnosis came: Advanced HER2-positive breast cancer.
“On one of my first or second appointments, I took in a little picture of Alexander and Isabella,” Gerber said. Gerber showed her oncologist the picture and told her: “I’ll do anything. I just want to be there for them.”
That was 21 years ago. Today, her current cancer status is “no evidence of disease.”
Over the past 2 decades, Gerber has gotten to be there for her children. Her youngest is now a television producer and her oldest, a CPA.
In that time,
“I’ve seen multiple physicians over my 21 years, but my oncologist has always been the focal point, guiding me in the right direction,” Gerber said in an interview.
Over the years, Jaga guided Gerber through a range of treatment decisions, including a Herceptin clinical trial that the mom of two views as lifesaving. Jaga often took on the role of both doctor and therapist, even providing comfort in the smaller moments when Gerber would fret about her weight gain.
The oncologist-patient “bond is very, very, very special,” said Gerber, who now works as director of patient advocacy and education at the Community Oncology Alliance.
Gerber isn’t alone in calling out the depth of the oncologist-patient bond.
Over years, sometimes decades, patients and oncologists can experience a whole world together: The treatment successes, relapses, uncertainties, and tough calls. As a result, a deep therapeutic alliance often develops. And with each new hurdle or decision, that collaborative, human connection between doctor and patient continues to form new layers.
“It’s like a shared bonding experience over trauma, like strangers trapped on a subway and then we get out, and we’re now on the other side, celebrating together,” said Saad Khan, MD, an associate professor of medicine (oncology) at Stanford University in California.
Connecting Through Stress
Although studies exploring the oncologist-patient bond are limited, some research suggests that a strong therapeutic alliance between patients and oncologists not only provides a foundation for quality care but can also help improve patients’ quality of life, protect against suicidal ideation, and increase treatment adherence.
Because of how stressful and frightening a cancer diagnosis can be, creating “a trusting, uninterrupted, almost sacred environment for them” is paramount for Khan. “I have no doubt that the most important part of their treatment is that they find an oncologist in whom they have total confidence,” Khan wrote in a blog.
The stress that patients with cancer experience is well documented, but oncologists take on a lot themselves and can also experience intense stress (.
“I consider my patient’s battles to be my battles,” Khan wrote.
The stress can start with the daily schedule. Oncologists often have a high volume of patients and tend to spend more time with each individual than most.
According to a 2023 survey, oncologists see about 68 patients a week, on average, but some oncologists, like Khan, have many more. Khan typically sees 20-30 patients a day and continues to care for many over years.
The survey also found that oncologists tend to spend a lot of time with their patients. Compared with other physicians, oncologists are two times more likely to spend at least 25 minutes with each patient.
With this kind of patient volume and time, Khan said, “you’re going to be exhausted.”
What can compound the exhaustion are the occasions oncologists need to deliver bad news — this treatment isn’t working, your cancer has come roaring back and, perhaps the hardest, we have no therapeutic options left. The end-of-life conversations, in particular, can be heartbreaking, especially when a patient is young and not ready to stop trying.
“It can be hard for doctors to discuss the end of life,” Don Dizon, MD, director of the Pelvic Malignancies Program at Lifespan Cancer Institute and director of Medical Oncology at Rhode Island Hospital, Providence, wrote in a column in 2023. Instead, it can be tempting and is often easier to focus on the next treatment, “instilling hope that there’s more that can be done,” even if doing more will only do harm.
In the face of these challenging decisions, growing a personal connection with patients over time can help keep oncologists going.
“We’re not just chemotherapy salesmen,” Khan said in an interview. “We get to know their social support network, who’s going to be driving them [to and from appointments], where they go on vacation, their cat’s name, who their neighbors are.”
A ‘Special Relationship’
Ralph V. Boccia, MD, is often asked what he does.
The next question that often comes — “Why do I do what I do?” — is Boccia’s favorite.
“Someone needs to take these patients through their journey,” Boccia, the founder of The Center for Cancer and Blood Disorders, Bethesda, Maryland, typically responds. He also often notes that “it is a special relationship you develop with the patient and their families.”
Boccia thinks about one long-term patient who captures this bond.
Joan Pinson, 70, was diagnosed with multiple myeloma about 25 years ago, when patients’ average survival was about 4 years.
Over a quarter century, Pinson has pivoted to different treatments, amid multiple relapses and remissions. Throughout most of this cancer journey, Boccia has been her primary oncologist, performing a stem cell transplant in 2000 and steering her to six clinical trials.
Her last relapse was 2 years ago, and since then she has been doing well on oral chemotherapy.
“Every time I relapsed, by the next appointment, he’d say, ‘here is what we are going to do,’ ” Pinson recalled. “I never worried, I never panicked. I knew he would take care of me.”
Over the years, Pinson and Boccia have shared many personal moments, sometimes by accident. One special moment happened early on in Pinson’s cancer journey. During an appointment, Boccia had “one ear to the phone” as his wife was about to deliver their first baby, Pinson recalled.
Later, Pinson met that child as a young man working in Boccia’s lab. She has also met Boccia’s wife, a nurse, when she filled in one day in the chemotherapy room.
Boccia now also treats Pinson’s husband who has prostate cancer, and he ruled out cancer when Pinson’s son, now in his 40s, had some worrisome symptoms.
More than 2 decades ago, Pinson told Boccia her goal was to see her youngest child graduate from high school. Now, six grandsons later, she has lived far beyond that goal.
“He has kept me alive,” said Pinson.
The Dying Patient
Harsha Vyas, MD, FACP, remembers the first encounter his office had with a 29-year-old woman referred with a diagnosis of stage IV breast cancer.
After just 15 minutes in the waiting room, the woman announced she was leaving. Although office staff assured the woman that she was next, the patient walked out.
Several months later, Vyas was called for an inpatient consult. It was the same woman.
Her lungs were full of fluid, and she was struggling to breathe, said Vyas, president and CEO of the Cancer Center of Middle Georgia, Dublin, and assistant professor at Augusta University in Georgia.
The woman, a single mother, told Vyas about her three young kids at home and asked him, “Doc, do something, please help me,” he recalled.
“Absolutely,” Vyas told her. But he had to be brutally honest about her prognosis and firm that she needed to follow his instructions. “You have a breast cancer I cannot cure,” he said. “All I can do is control the disease.”
From that first day, until the day she died, she came to every appointment and followed the treatment plan Vyas laid out.
For about 2 years, she responded well to treatment. And as the time passed and the trust grew, she began to open up to him. She showed him pictures. She talked about her children and being a mother.
“I’ve got to get my kids in a better place. I’m going to be there for them,” he recalled her saying.
Vyas admired her resourcefulness. She held down a part-time job, working retail and at a local restaurant. She figured out childcare so she could get to her chemotherapy appointments every 3 weeks and manage the copays.
Several years later, when she knew she was approaching the end of her life, she asked Vyas a question that hit hard.
“Doc, I don’t want to die and my kids find me dead. What can we do about it?”
Vyas, who has three daughters, imagined how traumatic this would be for a child. She and Vyas made the shared decision to cease treatment and begin home hospice. When the end was approaching, a hospice worker took over, waiting for bodily functions to cease.
When news of a death comes, “I say a little prayer, it’s almost like a send-off for that soul. That helps me absorb the news ... and let it go.”
But when the bond grows strong over time, as with his patient with breast cancer, Vyas said, “a piece of her is still with me.”
Khan had no relevant disclosures. Boccia and Vyas had no disclosures.
A version of this article appeared on Medscape.com.
Rose Gerber was 39, mother to a third grader and a kindergartener, when the diagnosis came: Advanced HER2-positive breast cancer.
“On one of my first or second appointments, I took in a little picture of Alexander and Isabella,” Gerber said. Gerber showed her oncologist the picture and told her: “I’ll do anything. I just want to be there for them.”
That was 21 years ago. Today, her current cancer status is “no evidence of disease.”
Over the past 2 decades, Gerber has gotten to be there for her children. Her youngest is now a television producer and her oldest, a CPA.
In that time,
“I’ve seen multiple physicians over my 21 years, but my oncologist has always been the focal point, guiding me in the right direction,” Gerber said in an interview.
Over the years, Jaga guided Gerber through a range of treatment decisions, including a Herceptin clinical trial that the mom of two views as lifesaving. Jaga often took on the role of both doctor and therapist, even providing comfort in the smaller moments when Gerber would fret about her weight gain.
The oncologist-patient “bond is very, very, very special,” said Gerber, who now works as director of patient advocacy and education at the Community Oncology Alliance.
Gerber isn’t alone in calling out the depth of the oncologist-patient bond.
Over years, sometimes decades, patients and oncologists can experience a whole world together: The treatment successes, relapses, uncertainties, and tough calls. As a result, a deep therapeutic alliance often develops. And with each new hurdle or decision, that collaborative, human connection between doctor and patient continues to form new layers.
“It’s like a shared bonding experience over trauma, like strangers trapped on a subway and then we get out, and we’re now on the other side, celebrating together,” said Saad Khan, MD, an associate professor of medicine (oncology) at Stanford University in California.
Connecting Through Stress
Although studies exploring the oncologist-patient bond are limited, some research suggests that a strong therapeutic alliance between patients and oncologists not only provides a foundation for quality care but can also help improve patients’ quality of life, protect against suicidal ideation, and increase treatment adherence.
Because of how stressful and frightening a cancer diagnosis can be, creating “a trusting, uninterrupted, almost sacred environment for them” is paramount for Khan. “I have no doubt that the most important part of their treatment is that they find an oncologist in whom they have total confidence,” Khan wrote in a blog.
The stress that patients with cancer experience is well documented, but oncologists take on a lot themselves and can also experience intense stress (.
“I consider my patient’s battles to be my battles,” Khan wrote.
The stress can start with the daily schedule. Oncologists often have a high volume of patients and tend to spend more time with each individual than most.
According to a 2023 survey, oncologists see about 68 patients a week, on average, but some oncologists, like Khan, have many more. Khan typically sees 20-30 patients a day and continues to care for many over years.
The survey also found that oncologists tend to spend a lot of time with their patients. Compared with other physicians, oncologists are two times more likely to spend at least 25 minutes with each patient.
With this kind of patient volume and time, Khan said, “you’re going to be exhausted.”
What can compound the exhaustion are the occasions oncologists need to deliver bad news — this treatment isn’t working, your cancer has come roaring back and, perhaps the hardest, we have no therapeutic options left. The end-of-life conversations, in particular, can be heartbreaking, especially when a patient is young and not ready to stop trying.
“It can be hard for doctors to discuss the end of life,” Don Dizon, MD, director of the Pelvic Malignancies Program at Lifespan Cancer Institute and director of Medical Oncology at Rhode Island Hospital, Providence, wrote in a column in 2023. Instead, it can be tempting and is often easier to focus on the next treatment, “instilling hope that there’s more that can be done,” even if doing more will only do harm.
In the face of these challenging decisions, growing a personal connection with patients over time can help keep oncologists going.
“We’re not just chemotherapy salesmen,” Khan said in an interview. “We get to know their social support network, who’s going to be driving them [to and from appointments], where they go on vacation, their cat’s name, who their neighbors are.”
A ‘Special Relationship’
Ralph V. Boccia, MD, is often asked what he does.
The next question that often comes — “Why do I do what I do?” — is Boccia’s favorite.
“Someone needs to take these patients through their journey,” Boccia, the founder of The Center for Cancer and Blood Disorders, Bethesda, Maryland, typically responds. He also often notes that “it is a special relationship you develop with the patient and their families.”
Boccia thinks about one long-term patient who captures this bond.
Joan Pinson, 70, was diagnosed with multiple myeloma about 25 years ago, when patients’ average survival was about 4 years.
Over a quarter century, Pinson has pivoted to different treatments, amid multiple relapses and remissions. Throughout most of this cancer journey, Boccia has been her primary oncologist, performing a stem cell transplant in 2000 and steering her to six clinical trials.
Her last relapse was 2 years ago, and since then she has been doing well on oral chemotherapy.
“Every time I relapsed, by the next appointment, he’d say, ‘here is what we are going to do,’ ” Pinson recalled. “I never worried, I never panicked. I knew he would take care of me.”
Over the years, Pinson and Boccia have shared many personal moments, sometimes by accident. One special moment happened early on in Pinson’s cancer journey. During an appointment, Boccia had “one ear to the phone” as his wife was about to deliver their first baby, Pinson recalled.
Later, Pinson met that child as a young man working in Boccia’s lab. She has also met Boccia’s wife, a nurse, when she filled in one day in the chemotherapy room.
Boccia now also treats Pinson’s husband who has prostate cancer, and he ruled out cancer when Pinson’s son, now in his 40s, had some worrisome symptoms.
More than 2 decades ago, Pinson told Boccia her goal was to see her youngest child graduate from high school. Now, six grandsons later, she has lived far beyond that goal.
“He has kept me alive,” said Pinson.
The Dying Patient
Harsha Vyas, MD, FACP, remembers the first encounter his office had with a 29-year-old woman referred with a diagnosis of stage IV breast cancer.
After just 15 minutes in the waiting room, the woman announced she was leaving. Although office staff assured the woman that she was next, the patient walked out.
Several months later, Vyas was called for an inpatient consult. It was the same woman.
Her lungs were full of fluid, and she was struggling to breathe, said Vyas, president and CEO of the Cancer Center of Middle Georgia, Dublin, and assistant professor at Augusta University in Georgia.
The woman, a single mother, told Vyas about her three young kids at home and asked him, “Doc, do something, please help me,” he recalled.
“Absolutely,” Vyas told her. But he had to be brutally honest about her prognosis and firm that she needed to follow his instructions. “You have a breast cancer I cannot cure,” he said. “All I can do is control the disease.”
From that first day, until the day she died, she came to every appointment and followed the treatment plan Vyas laid out.
For about 2 years, she responded well to treatment. And as the time passed and the trust grew, she began to open up to him. She showed him pictures. She talked about her children and being a mother.
“I’ve got to get my kids in a better place. I’m going to be there for them,” he recalled her saying.
Vyas admired her resourcefulness. She held down a part-time job, working retail and at a local restaurant. She figured out childcare so she could get to her chemotherapy appointments every 3 weeks and manage the copays.
Several years later, when she knew she was approaching the end of her life, she asked Vyas a question that hit hard.
“Doc, I don’t want to die and my kids find me dead. What can we do about it?”
Vyas, who has three daughters, imagined how traumatic this would be for a child. She and Vyas made the shared decision to cease treatment and begin home hospice. When the end was approaching, a hospice worker took over, waiting for bodily functions to cease.
When news of a death comes, “I say a little prayer, it’s almost like a send-off for that soul. That helps me absorb the news ... and let it go.”
But when the bond grows strong over time, as with his patient with breast cancer, Vyas said, “a piece of her is still with me.”
Khan had no relevant disclosures. Boccia and Vyas had no disclosures.
A version of this article appeared on Medscape.com.
Study Addresses Lichen Planus Prevalence, Treatment
TOPLINE:
METHODOLOGY:
- To evaluate the prevalence of LP, researchers analyzed 566,851 eligible patients from the Explorys database, comprising electronic medical records from over 40 healthcare networks and 53 million patients across the United States.
- They also assessed treatment plans separately among 1998 newly diagnosed patients with LP between October 2015 and January 2020, who required at least one dermatology encounter within the first year following diagnosis.
- The primary outcome was overall prevalence of LP in the United States, including prevalence across specific age, sex, and racial subgroups. Additionally, dermatologist-prescribed treatments for non-oral LP were also reported.
TAKEAWAY:
- Overall, there were 1098 cases of LP (median age, 66 years; 74% women); the crude prevalence of LP was 0.19% and the age- and sex-standardized overall prevalence was 0.15%. Prevalence in women was 1.77 times higher than in men.
- Asian patients showed the highest standardized prevalence (0.2%), followed by Black patients (0.16). Prevalence increased with age, ranging from 0.04% among those aged 18-29 years to 0.26% among those aged 60-69 years and 0.33% among those aged 70-79 years.
IN PRACTICE:
“LP is a fairly common disease, which disproportionately affects women and individuals older than 60 years of age,” the authors wrote. “Future research to help identify patients who may need systemic treatment and determine appropriate treatments for patients with LP to limit sequelae is important as no medication is currently FDA approved for LP.”
SOURCE:
The study was led by Natalia Pelet Del Toro, MD, Department of Dermatology, Northwell Health, New Hyde Park, New York, and was published online in The Journal of the American Academy of Dermatology.
LIMITATIONS:
The absence of a precise diagnosis code for non-oral LP introduces potential misclassification risks. Additionally, the study design did not allow for the establishment of disease severity levels, limiting the ability to correlate treatment choices with disease severity.
DISCLOSURES:
The study did not receive any funding. Two authors reported to have received advisory fees, grants, and/or honoraria from several pharmaceutical companies. Pelet Del Toro and another author did not declare any conflict of interests.
This article was created using several editorial tools, including artificial intelligence, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- To evaluate the prevalence of LP, researchers analyzed 566,851 eligible patients from the Explorys database, comprising electronic medical records from over 40 healthcare networks and 53 million patients across the United States.
- They also assessed treatment plans separately among 1998 newly diagnosed patients with LP between October 2015 and January 2020, who required at least one dermatology encounter within the first year following diagnosis.
- The primary outcome was overall prevalence of LP in the United States, including prevalence across specific age, sex, and racial subgroups. Additionally, dermatologist-prescribed treatments for non-oral LP were also reported.
TAKEAWAY:
- Overall, there were 1098 cases of LP (median age, 66 years; 74% women); the crude prevalence of LP was 0.19% and the age- and sex-standardized overall prevalence was 0.15%. Prevalence in women was 1.77 times higher than in men.
- Asian patients showed the highest standardized prevalence (0.2%), followed by Black patients (0.16). Prevalence increased with age, ranging from 0.04% among those aged 18-29 years to 0.26% among those aged 60-69 years and 0.33% among those aged 70-79 years.
IN PRACTICE:
“LP is a fairly common disease, which disproportionately affects women and individuals older than 60 years of age,” the authors wrote. “Future research to help identify patients who may need systemic treatment and determine appropriate treatments for patients with LP to limit sequelae is important as no medication is currently FDA approved for LP.”
SOURCE:
The study was led by Natalia Pelet Del Toro, MD, Department of Dermatology, Northwell Health, New Hyde Park, New York, and was published online in The Journal of the American Academy of Dermatology.
LIMITATIONS:
The absence of a precise diagnosis code for non-oral LP introduces potential misclassification risks. Additionally, the study design did not allow for the establishment of disease severity levels, limiting the ability to correlate treatment choices with disease severity.
DISCLOSURES:
The study did not receive any funding. Two authors reported to have received advisory fees, grants, and/or honoraria from several pharmaceutical companies. Pelet Del Toro and another author did not declare any conflict of interests.
This article was created using several editorial tools, including artificial intelligence, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- To evaluate the prevalence of LP, researchers analyzed 566,851 eligible patients from the Explorys database, comprising electronic medical records from over 40 healthcare networks and 53 million patients across the United States.
- They also assessed treatment plans separately among 1998 newly diagnosed patients with LP between October 2015 and January 2020, who required at least one dermatology encounter within the first year following diagnosis.
- The primary outcome was overall prevalence of LP in the United States, including prevalence across specific age, sex, and racial subgroups. Additionally, dermatologist-prescribed treatments for non-oral LP were also reported.
TAKEAWAY:
- Overall, there were 1098 cases of LP (median age, 66 years; 74% women); the crude prevalence of LP was 0.19% and the age- and sex-standardized overall prevalence was 0.15%. Prevalence in women was 1.77 times higher than in men.
- Asian patients showed the highest standardized prevalence (0.2%), followed by Black patients (0.16). Prevalence increased with age, ranging from 0.04% among those aged 18-29 years to 0.26% among those aged 60-69 years and 0.33% among those aged 70-79 years.
IN PRACTICE:
“LP is a fairly common disease, which disproportionately affects women and individuals older than 60 years of age,” the authors wrote. “Future research to help identify patients who may need systemic treatment and determine appropriate treatments for patients with LP to limit sequelae is important as no medication is currently FDA approved for LP.”
SOURCE:
The study was led by Natalia Pelet Del Toro, MD, Department of Dermatology, Northwell Health, New Hyde Park, New York, and was published online in The Journal of the American Academy of Dermatology.
LIMITATIONS:
The absence of a precise diagnosis code for non-oral LP introduces potential misclassification risks. Additionally, the study design did not allow for the establishment of disease severity levels, limiting the ability to correlate treatment choices with disease severity.
DISCLOSURES:
The study did not receive any funding. Two authors reported to have received advisory fees, grants, and/or honoraria from several pharmaceutical companies. Pelet Del Toro and another author did not declare any conflict of interests.
This article was created using several editorial tools, including artificial intelligence, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Is 1-Week Radiotherapy Safe for Breast Cancer?
TOPLINE:
Most patients also reported that the reduced treatment time was a major benefit of the 1-week radiotherapy schedule.
METHODOLOGY:
- In March 2020, during the COVID-19 pandemic, international and national guidelines recommended adopting a 1-week ultrahypofractionated radiotherapy schedule for patients with node-negative breast cancer. Subsequently, a phase 3 trial demonstrated that a 1-week regimen of 26 Gy in five fractions led to similar breast cancer outcomes compared with a standard moderately hypofractionated regimen.
- In this study, researchers wanted to assess real world toxicities following ultrahypofractionated radiotherapy and enrolled 135 consecutive patients who received 1-week ultrahypofractionated adjuvant radiation of 26 Gy in five fractions from March to August 2020 at three centers in Ireland, with 33 patients (25%) receiving a sequential boost.
- Researchers recorded patient-reported outcomes on breast pain, swelling, firmness, and hypersensitivity at baseline, 3, 6, and 12 months. Virtual consultations without video occurred at baseline, 3 months, 6 months, and video consultations were offered at 1 year for a physician-led breast evaluation.
- Researchers assessed patient perspectives on this new schedule and telehealth workflows using questionnaires.
- Overall, 90% of patients completed the 1-year assessment plus another assessment. The primary endpoint was the worst toxicity reported at each time point.
TAKEAWAY:
- Overall, 76% of patients reported no or mild toxicities at 3 and 6 months, and 82% reported no or mild toxicities 12 months.
- At 1 year, 20 patients (17%) reported moderate toxicity, most commonly breast pain, and only two patients (2%) reported marked toxicities, including breast firmness and skin changes.
- Researchers found no difference in toxicities between patients who received only 26 Gy in five fractions and those who received an additional sequential boost.
- Most patients reported reduced treatment time (78.6%) and infection control (59%) as major benefits of the 1-week radiotherapy regimen. Patients also reported high satisfaction with the use of telehealth, with 97.3% feeling well-informed about their diagnosis, 88% feeling well-informed about treatment side effects, and 94% feeling supported by the medical team. However, only 27% agreed to video consultations for breast inspections at 1 year.
IN PRACTICE:
“Ultrahypofractionated whole breast radiotherapy leads to acceptable late toxicity rates at 1 year even when followed by a hypofractionated tumour bed boost,” the authors wrote. “Patient satisfaction with ultrahypofractionated treatment and virtual consultations without video was high.”
SOURCE:
The study, led by Jill Nicholson, MBBS, MRCP, FFFRRCSI, St Luke’s Radiation Oncology Network, St. Luke’s Hospital, Dublin, Ireland, was published online in Advances in Radiation Oncology.
LIMITATIONS:
The short follow-up period might not capture all late toxicities. Variability in patient-reported outcomes could affect consistency. The range in boost received (four to eight fractions) could have influenced patients’ experiences.
DISCLOSURES:
Nicholson received funding from the St. Luke’s Institute of Cancer Research, Dublin, Ireland. No other relevant conflicts of interest were disclosed by the authors.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Most patients also reported that the reduced treatment time was a major benefit of the 1-week radiotherapy schedule.
METHODOLOGY:
- In March 2020, during the COVID-19 pandemic, international and national guidelines recommended adopting a 1-week ultrahypofractionated radiotherapy schedule for patients with node-negative breast cancer. Subsequently, a phase 3 trial demonstrated that a 1-week regimen of 26 Gy in five fractions led to similar breast cancer outcomes compared with a standard moderately hypofractionated regimen.
- In this study, researchers wanted to assess real world toxicities following ultrahypofractionated radiotherapy and enrolled 135 consecutive patients who received 1-week ultrahypofractionated adjuvant radiation of 26 Gy in five fractions from March to August 2020 at three centers in Ireland, with 33 patients (25%) receiving a sequential boost.
- Researchers recorded patient-reported outcomes on breast pain, swelling, firmness, and hypersensitivity at baseline, 3, 6, and 12 months. Virtual consultations without video occurred at baseline, 3 months, 6 months, and video consultations were offered at 1 year for a physician-led breast evaluation.
- Researchers assessed patient perspectives on this new schedule and telehealth workflows using questionnaires.
- Overall, 90% of patients completed the 1-year assessment plus another assessment. The primary endpoint was the worst toxicity reported at each time point.
TAKEAWAY:
- Overall, 76% of patients reported no or mild toxicities at 3 and 6 months, and 82% reported no or mild toxicities 12 months.
- At 1 year, 20 patients (17%) reported moderate toxicity, most commonly breast pain, and only two patients (2%) reported marked toxicities, including breast firmness and skin changes.
- Researchers found no difference in toxicities between patients who received only 26 Gy in five fractions and those who received an additional sequential boost.
- Most patients reported reduced treatment time (78.6%) and infection control (59%) as major benefits of the 1-week radiotherapy regimen. Patients also reported high satisfaction with the use of telehealth, with 97.3% feeling well-informed about their diagnosis, 88% feeling well-informed about treatment side effects, and 94% feeling supported by the medical team. However, only 27% agreed to video consultations for breast inspections at 1 year.
IN PRACTICE:
“Ultrahypofractionated whole breast radiotherapy leads to acceptable late toxicity rates at 1 year even when followed by a hypofractionated tumour bed boost,” the authors wrote. “Patient satisfaction with ultrahypofractionated treatment and virtual consultations without video was high.”
SOURCE:
The study, led by Jill Nicholson, MBBS, MRCP, FFFRRCSI, St Luke’s Radiation Oncology Network, St. Luke’s Hospital, Dublin, Ireland, was published online in Advances in Radiation Oncology.
LIMITATIONS:
The short follow-up period might not capture all late toxicities. Variability in patient-reported outcomes could affect consistency. The range in boost received (four to eight fractions) could have influenced patients’ experiences.
DISCLOSURES:
Nicholson received funding from the St. Luke’s Institute of Cancer Research, Dublin, Ireland. No other relevant conflicts of interest were disclosed by the authors.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Most patients also reported that the reduced treatment time was a major benefit of the 1-week radiotherapy schedule.
METHODOLOGY:
- In March 2020, during the COVID-19 pandemic, international and national guidelines recommended adopting a 1-week ultrahypofractionated radiotherapy schedule for patients with node-negative breast cancer. Subsequently, a phase 3 trial demonstrated that a 1-week regimen of 26 Gy in five fractions led to similar breast cancer outcomes compared with a standard moderately hypofractionated regimen.
- In this study, researchers wanted to assess real world toxicities following ultrahypofractionated radiotherapy and enrolled 135 consecutive patients who received 1-week ultrahypofractionated adjuvant radiation of 26 Gy in five fractions from March to August 2020 at three centers in Ireland, with 33 patients (25%) receiving a sequential boost.
- Researchers recorded patient-reported outcomes on breast pain, swelling, firmness, and hypersensitivity at baseline, 3, 6, and 12 months. Virtual consultations without video occurred at baseline, 3 months, 6 months, and video consultations were offered at 1 year for a physician-led breast evaluation.
- Researchers assessed patient perspectives on this new schedule and telehealth workflows using questionnaires.
- Overall, 90% of patients completed the 1-year assessment plus another assessment. The primary endpoint was the worst toxicity reported at each time point.
TAKEAWAY:
- Overall, 76% of patients reported no or mild toxicities at 3 and 6 months, and 82% reported no or mild toxicities 12 months.
- At 1 year, 20 patients (17%) reported moderate toxicity, most commonly breast pain, and only two patients (2%) reported marked toxicities, including breast firmness and skin changes.
- Researchers found no difference in toxicities between patients who received only 26 Gy in five fractions and those who received an additional sequential boost.
- Most patients reported reduced treatment time (78.6%) and infection control (59%) as major benefits of the 1-week radiotherapy regimen. Patients also reported high satisfaction with the use of telehealth, with 97.3% feeling well-informed about their diagnosis, 88% feeling well-informed about treatment side effects, and 94% feeling supported by the medical team. However, only 27% agreed to video consultations for breast inspections at 1 year.
IN PRACTICE:
“Ultrahypofractionated whole breast radiotherapy leads to acceptable late toxicity rates at 1 year even when followed by a hypofractionated tumour bed boost,” the authors wrote. “Patient satisfaction with ultrahypofractionated treatment and virtual consultations without video was high.”
SOURCE:
The study, led by Jill Nicholson, MBBS, MRCP, FFFRRCSI, St Luke’s Radiation Oncology Network, St. Luke’s Hospital, Dublin, Ireland, was published online in Advances in Radiation Oncology.
LIMITATIONS:
The short follow-up period might not capture all late toxicities. Variability in patient-reported outcomes could affect consistency. The range in boost received (four to eight fractions) could have influenced patients’ experiences.
DISCLOSURES:
Nicholson received funding from the St. Luke’s Institute of Cancer Research, Dublin, Ireland. No other relevant conflicts of interest were disclosed by the authors.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Triple Therapy Now Advised for Lupus Nephritis in Updated Guideline
WASHINGTON — A new guideline for management of lupus nephritis (LN) was unveiled at the annual meeting of the American College of Rheumatology (ACR), updating the 2012 LN guideline to recommend a more aggressive first-line approach to treating the disease.
“The biggest differences are that we are recommending what we’re calling triple therapy, where we incorporate the glucocorticoid therapy with baseline conventional immunosuppressants, usually mycophenolate with cyclophosphamide, and the addition of one of the newer agents more recently approved by the FDA [Food and Drug Administration] — belimumab, voclosporin, or another CNI [calcineurin inhibitor],” said Lisa Sammaritano, MD, director of the Rheumatology Reproductive Health Program of the Barbara Volcker Center for Women and Rheumatic Diseases at the Hospital for Special Surgery and professor of clinical medicine at Weill Cornell Medical College, both in New York City.

“This is a bit of a change from not only our previous guideline but some of the other guidelines out there, and it is based on the fact that we have very convincing evidence that starting with triple therapy yields to better long-term outcomes for our patients than starting with only two agents and waiting to see if they respond before escalating therapy,” she said. Other key updates include recommending use of pulse glucocorticoid therapy with a lower dose and more rapid steroid taper and treating patients with the recommended therapy for 3-5 years.
The guiding principles of the guideline are not only to preserve kidney function and minimize morbidity and mortality but also to ensure collaborative care with nephrology, to utilize shared decision-making that includes patients’ values and preferences, to reduce healthcare disparities, and to consider pediatric and geriatric populations. The guidelines are based on a quantitative synthesis of 105 studies that yielded 7 strong recommendations, 21 conditional recommendations, and 13 good practice statements — those commonly accepted as beneficial or practical advice even if there is little direct evidence to support them. The voting panel of 19 members included not only 3 nephrologists and 2 pediatric rheumatologists but also 2 patient representatives with LN.
The recommendations are just that, “a recommendation, not an order,” Sammaritano said, and strong recommendations are those “where we think, unequivocally, almost everybody should follow that recommendation. When we feel that we cannot make a strong recommendation, then we call our recommendation conditional, and it is conditional on looking at different things,” she said.
“Patients are different, especially lupus patients, and so one lupus nephritis patient may have different clinical characteristics, different thoughts about what therapy will work for them in their lives, or what therapy they really do not want to pursue,” Sammaritano said. “Maybe they can’t conceive of coming to the hospital once a month for intravenous therapy. Maybe they’re concerned about pill burden, which is something that our patient panel really emphasized to us. So, conditional recommendation means this voting panel thought that this was the best overall for most patients and most circumstances, recognizing there will still be a significant number of people, clinicians and patients, who may feel differently for that particular situation. So, that’s where you know the patient-clinician discussion can help with decision-making.”
What Are the Recommendations?
All patients with systemic lupus erythematosus (SLE) are strongly recommended to undergo proteinuria screening every 6-12 months or at the time of a flare. Those suspected of having LN should receive a prompt kidney biopsy and treatment with glucocorticoids while awaiting the biopsy and results. Two conditional recommendations for kidney biopsy include patients with SLE with unexplained impaired kidney function or a protein to creatinine ratio > 0.5 g/g, and patients with LN with a suspected flare after initial response or a lack of response or worsening after 6 months of therapy.
The guidelines include a strong recommendation for all patients with SLE to receive hydroxychloroquine and a conditional recommendation for all patients with elevated proteinuria (> 0.5 g/g) to receive renin-angiotensin-aldosterone system inhibitors (RAAS-I). Dosages in patients with LN with decreased glomerular filtration rate (GFR) should be adjusted as needed.
Sammaritano then reviewed the specifics on medication treatment. The glucocorticoid therapy in all patients with LN should begin with Pulse IV Therapy at 250-1000 mg/d for 1-3 days, followed by oral prednisone ≤ 0.5 mg/kg per day up to 40 mg/d, then tapered to a target dose > 5 mg/d within 6 months. The justification for this course comes from a 2024 systematic review finding pulse followed by oral glucocorticoids maximized complete renal response while minimizing toxicities, Sammaritano said.
“We have all become acutely aware of the very high risk of prolonged high dose of glucocorticoids for our patients,” she said, “and importantly, our patient panel participants strongly emphasized their preference for minimizing glucocorticoids dose.”
In addition to the recommendation of all patients receiving hydroxychloroquine and RAAS-I, first-line treatment of active, new-onset, or flaring LN should begin with triple therapy — glucocorticoids with two additional immunosuppressive agents. For patients with class III/IV LN, triple therapy includes the glucocorticoids course with a mycophenolic acid analog (MPAA) and either belimumab or a CNI. Conditional recommendations support MPAA with belimumab for significant extrarenal manifestations and MPAA with CNI for proteinuria ≥ 3 g/g.
An alternative triple therapy for class III/IV is glucocorticoids with low-dose cyclophosphamide and belimumab, but MPAA at 2-3 g/d is preferred over cyclophosphamide. The preferred regimen for cyclophosphamide is derived from the Euro-Lupus Nephritis Trial: Intravenous 500 mg every 2 weeks for six doses and then MPAA. Sammaritano noted that there are some limited data on using cyclophosphamide with belimumab, but “we do not specifically recommend cyclophosphamide with a CNI as one of our options because this combination has not been studied in randomized controlled trials.”
There are less data supporting class V recommendations, Sammaritano said, but for those with proteinuria of at least 1 g/g, the panel still recommends triple therapy with glucocorticoids, a MPAA, and a CNI. A CNI is preferred over belimumab because of its stabilizing effects on the podocyte cytoskeleton. Two alternative triple therapies for class V–only patients are glucocorticoids with belimumab and either low-dose cyclophosphamide or MPAA.
Dual therapy is only recommended if triple therapy is not available or not tolerated. The voting panel chose to recommend triple therapy over dual therapy with escalation for two reasons. First, the BLISS-LN and AURORA 1 trials showed improved outcomes with initial triple therapy over initial dual therapies.
Second, “nephron loss proceeds throughout a person’s lifetime even for those who do not have lupus nephritis, and every case of lupus nephritis or every period of time with uncontrolled lupus nephritis changes the course of that decline for the worse,” Sammaritano said. “So, we feel we can’t wait for nephron loss to implement what has been shown to be the most efficacious therapy. We want to gain rapid control of inflammation using the most effective regimen to prevent further damage and flare and maintain survival.”
Therapy is conditionally recommended for at least 3-5 years because “not only do we want to gain rapid control of disease activity [but we also] want to maintain control of disease activity until there’s sustained inactive disease,” Sammaritano said. “Repeat kidney biopsies show that immunologic activity persists in the kidneys for several years, and the withdrawal of immunosuppression when there is histologic activity predisposes patients to flare.” But immunosuppressive therapy can be tapered over time as determined by renal disease activity and medication tolerability.
For patients with refractory disease, consider additional factors that could be affecting the disease, such as adherence, the presence of other diagnoses, or advanced chronicity.
“If true refractory nephritis is present,” she said, “we recommend escalation to a more intensive regimen,” including the addition of anti-CD20 agents, combination therapy with three immunosuppressives, or referral for investigational therapy.
“We also emphasize the importance of other adjunctive therapies preventing comorbidities, such as cardiovascular disease, changes in bone health, or infection risk,” she said. In older patients, avoid polypharmacy as much as possible and be mindful of age-related GFR, she added.
A strong recommendation supported monitoring patients with LN and proteinuria at least every 3 months if they have not achieved complete renal response and every 3-6 months after sustained complete renal response.
Last, in patients with LN and end-stage kidney disease (ESKD), the voting panel strongly recommends transplant over dialysis and conditionally recommends proceeding to the transplant without requiring a complete clinical or serologic remission as long as no other organs are involved. In patients with LN at risk for ESKD, the guideline conditionally recommends consideration of a preemptive transplant, and patients on dialysis or post transplant are strongly recommended to regularly follow up with rheumatology.
Gabriel Kirsch, MD, a resident rheumatologist at the University of Florida College of Medicine, Jacksonville, said he found the guidelines helpful, “especially the guidance on the dichotomy between using belimumab and voclosporin and the clinical and patient preference that help you make that decision.”
Kirsch had hoped, however, to hear more about the impact of therapeutic drug monitoring of hydroxychloroquine on LN outcomes. He also noted a clinical scenario he’s come across that wasn’t addressed.
“When you’re checking GFR on these folks, a lot of our eGFR calculators are creatinine based, and creatinine at the extremes of muscle mass can be inaccurate,” such as getting artificially low creatinine readings from pediatric patients because of their low muscle mass or from patients with muscle atrophy caused by a lot of glucocorticoid exposure. “I was hoping for some more guidance on that,” he said.
Ellen Ginzler, MD, MPH, chief of rheumatology at SUNY Health Science Center in Brooklyn, New York, said the guidelines were pretty much what she expected them to be. She agreed with the panel’s advice that, when deciding between belimumab or voclosporin, “if it’s pure proteinuria, then you add voclosporin. If the patient has extra renal manifestations, you go with belimumab first.”
“They really made it quite clear that, despite the fact that people really want to reduce the amount of immunosuppression — and I agree you should taper steroids quickly — you really need to keep the immunosuppression for a prolonged period of time because all of the studies that have been done for years show that the longer you’re on immunosuppression after you achieve remission or a low disease activity state, the better your chance of not flaring,” Ginzler said. “Rapid tapering or discontinuation really increases the risk of flare.”
Sammaritano, Kirsch, and Ginzler had no disclosures. No external funding was used.
A version of this article appeared on Medscape.com.
WASHINGTON — A new guideline for management of lupus nephritis (LN) was unveiled at the annual meeting of the American College of Rheumatology (ACR), updating the 2012 LN guideline to recommend a more aggressive first-line approach to treating the disease.
“The biggest differences are that we are recommending what we’re calling triple therapy, where we incorporate the glucocorticoid therapy with baseline conventional immunosuppressants, usually mycophenolate with cyclophosphamide, and the addition of one of the newer agents more recently approved by the FDA [Food and Drug Administration] — belimumab, voclosporin, or another CNI [calcineurin inhibitor],” said Lisa Sammaritano, MD, director of the Rheumatology Reproductive Health Program of the Barbara Volcker Center for Women and Rheumatic Diseases at the Hospital for Special Surgery and professor of clinical medicine at Weill Cornell Medical College, both in New York City.
“This is a bit of a change from not only our previous guideline but some of the other guidelines out there, and it is based on the fact that we have very convincing evidence that starting with triple therapy yields to better long-term outcomes for our patients than starting with only two agents and waiting to see if they respond before escalating therapy,” she said. Other key updates include recommending use of pulse glucocorticoid therapy with a lower dose and more rapid steroid taper and treating patients with the recommended therapy for 3-5 years.
The guiding principles of the guideline are not only to preserve kidney function and minimize morbidity and mortality but also to ensure collaborative care with nephrology, to utilize shared decision-making that includes patients’ values and preferences, to reduce healthcare disparities, and to consider pediatric and geriatric populations. The guidelines are based on a quantitative synthesis of 105 studies that yielded 7 strong recommendations, 21 conditional recommendations, and 13 good practice statements — those commonly accepted as beneficial or practical advice even if there is little direct evidence to support them. The voting panel of 19 members included not only 3 nephrologists and 2 pediatric rheumatologists but also 2 patient representatives with LN.
The recommendations are just that, “a recommendation, not an order,” Sammaritano said, and strong recommendations are those “where we think, unequivocally, almost everybody should follow that recommendation. When we feel that we cannot make a strong recommendation, then we call our recommendation conditional, and it is conditional on looking at different things,” she said.
“Patients are different, especially lupus patients, and so one lupus nephritis patient may have different clinical characteristics, different thoughts about what therapy will work for them in their lives, or what therapy they really do not want to pursue,” Sammaritano said. “Maybe they can’t conceive of coming to the hospital once a month for intravenous therapy. Maybe they’re concerned about pill burden, which is something that our patient panel really emphasized to us. So, conditional recommendation means this voting panel thought that this was the best overall for most patients and most circumstances, recognizing there will still be a significant number of people, clinicians and patients, who may feel differently for that particular situation. So, that’s where you know the patient-clinician discussion can help with decision-making.”
What Are the Recommendations?
All patients with systemic lupus erythematosus (SLE) are strongly recommended to undergo proteinuria screening every 6-12 months or at the time of a flare. Those suspected of having LN should receive a prompt kidney biopsy and treatment with glucocorticoids while awaiting the biopsy and results. Two conditional recommendations for kidney biopsy include patients with SLE with unexplained impaired kidney function or a protein to creatinine ratio > 0.5 g/g, and patients with LN with a suspected flare after initial response or a lack of response or worsening after 6 months of therapy.
The guidelines include a strong recommendation for all patients with SLE to receive hydroxychloroquine and a conditional recommendation for all patients with elevated proteinuria (> 0.5 g/g) to receive renin-angiotensin-aldosterone system inhibitors (RAAS-I). Dosages in patients with LN with decreased glomerular filtration rate (GFR) should be adjusted as needed.
Sammaritano then reviewed the specifics on medication treatment. The glucocorticoid therapy in all patients with LN should begin with Pulse IV Therapy at 250-1000 mg/d for 1-3 days, followed by oral prednisone ≤ 0.5 mg/kg per day up to 40 mg/d, then tapered to a target dose > 5 mg/d within 6 months. The justification for this course comes from a 2024 systematic review finding pulse followed by oral glucocorticoids maximized complete renal response while minimizing toxicities, Sammaritano said.
“We have all become acutely aware of the very high risk of prolonged high dose of glucocorticoids for our patients,” she said, “and importantly, our patient panel participants strongly emphasized their preference for minimizing glucocorticoids dose.”
In addition to the recommendation of all patients receiving hydroxychloroquine and RAAS-I, first-line treatment of active, new-onset, or flaring LN should begin with triple therapy — glucocorticoids with two additional immunosuppressive agents. For patients with class III/IV LN, triple therapy includes the glucocorticoids course with a mycophenolic acid analog (MPAA) and either belimumab or a CNI. Conditional recommendations support MPAA with belimumab for significant extrarenal manifestations and MPAA with CNI for proteinuria ≥ 3 g/g.
An alternative triple therapy for class III/IV is glucocorticoids with low-dose cyclophosphamide and belimumab, but MPAA at 2-3 g/d is preferred over cyclophosphamide. The preferred regimen for cyclophosphamide is derived from the Euro-Lupus Nephritis Trial: Intravenous 500 mg every 2 weeks for six doses and then MPAA. Sammaritano noted that there are some limited data on using cyclophosphamide with belimumab, but “we do not specifically recommend cyclophosphamide with a CNI as one of our options because this combination has not been studied in randomized controlled trials.”
There are less data supporting class V recommendations, Sammaritano said, but for those with proteinuria of at least 1 g/g, the panel still recommends triple therapy with glucocorticoids, a MPAA, and a CNI. A CNI is preferred over belimumab because of its stabilizing effects on the podocyte cytoskeleton. Two alternative triple therapies for class V–only patients are glucocorticoids with belimumab and either low-dose cyclophosphamide or MPAA.
Dual therapy is only recommended if triple therapy is not available or not tolerated. The voting panel chose to recommend triple therapy over dual therapy with escalation for two reasons. First, the BLISS-LN and AURORA 1 trials showed improved outcomes with initial triple therapy over initial dual therapies.
Second, “nephron loss proceeds throughout a person’s lifetime even for those who do not have lupus nephritis, and every case of lupus nephritis or every period of time with uncontrolled lupus nephritis changes the course of that decline for the worse,” Sammaritano said. “So, we feel we can’t wait for nephron loss to implement what has been shown to be the most efficacious therapy. We want to gain rapid control of inflammation using the most effective regimen to prevent further damage and flare and maintain survival.”
Therapy is conditionally recommended for at least 3-5 years because “not only do we want to gain rapid control of disease activity [but we also] want to maintain control of disease activity until there’s sustained inactive disease,” Sammaritano said. “Repeat kidney biopsies show that immunologic activity persists in the kidneys for several years, and the withdrawal of immunosuppression when there is histologic activity predisposes patients to flare.” But immunosuppressive therapy can be tapered over time as determined by renal disease activity and medication tolerability.
For patients with refractory disease, consider additional factors that could be affecting the disease, such as adherence, the presence of other diagnoses, or advanced chronicity.
“If true refractory nephritis is present,” she said, “we recommend escalation to a more intensive regimen,” including the addition of anti-CD20 agents, combination therapy with three immunosuppressives, or referral for investigational therapy.
“We also emphasize the importance of other adjunctive therapies preventing comorbidities, such as cardiovascular disease, changes in bone health, or infection risk,” she said. In older patients, avoid polypharmacy as much as possible and be mindful of age-related GFR, she added.
A strong recommendation supported monitoring patients with LN and proteinuria at least every 3 months if they have not achieved complete renal response and every 3-6 months after sustained complete renal response.
Last, in patients with LN and end-stage kidney disease (ESKD), the voting panel strongly recommends transplant over dialysis and conditionally recommends proceeding to the transplant without requiring a complete clinical or serologic remission as long as no other organs are involved. In patients with LN at risk for ESKD, the guideline conditionally recommends consideration of a preemptive transplant, and patients on dialysis or post transplant are strongly recommended to regularly follow up with rheumatology.
Gabriel Kirsch, MD, a resident rheumatologist at the University of Florida College of Medicine, Jacksonville, said he found the guidelines helpful, “especially the guidance on the dichotomy between using belimumab and voclosporin and the clinical and patient preference that help you make that decision.”
Kirsch had hoped, however, to hear more about the impact of therapeutic drug monitoring of hydroxychloroquine on LN outcomes. He also noted a clinical scenario he’s come across that wasn’t addressed.
“When you’re checking GFR on these folks, a lot of our eGFR calculators are creatinine based, and creatinine at the extremes of muscle mass can be inaccurate,” such as getting artificially low creatinine readings from pediatric patients because of their low muscle mass or from patients with muscle atrophy caused by a lot of glucocorticoid exposure. “I was hoping for some more guidance on that,” he said.
Ellen Ginzler, MD, MPH, chief of rheumatology at SUNY Health Science Center in Brooklyn, New York, said the guidelines were pretty much what she expected them to be. She agreed with the panel’s advice that, when deciding between belimumab or voclosporin, “if it’s pure proteinuria, then you add voclosporin. If the patient has extra renal manifestations, you go with belimumab first.”
“They really made it quite clear that, despite the fact that people really want to reduce the amount of immunosuppression — and I agree you should taper steroids quickly — you really need to keep the immunosuppression for a prolonged period of time because all of the studies that have been done for years show that the longer you’re on immunosuppression after you achieve remission or a low disease activity state, the better your chance of not flaring,” Ginzler said. “Rapid tapering or discontinuation really increases the risk of flare.”
Sammaritano, Kirsch, and Ginzler had no disclosures. No external funding was used.
A version of this article appeared on Medscape.com.
WASHINGTON — A new guideline for management of lupus nephritis (LN) was unveiled at the annual meeting of the American College of Rheumatology (ACR), updating the 2012 LN guideline to recommend a more aggressive first-line approach to treating the disease.
“The biggest differences are that we are recommending what we’re calling triple therapy, where we incorporate the glucocorticoid therapy with baseline conventional immunosuppressants, usually mycophenolate with cyclophosphamide, and the addition of one of the newer agents more recently approved by the FDA [Food and Drug Administration] — belimumab, voclosporin, or another CNI [calcineurin inhibitor],” said Lisa Sammaritano, MD, director of the Rheumatology Reproductive Health Program of the Barbara Volcker Center for Women and Rheumatic Diseases at the Hospital for Special Surgery and professor of clinical medicine at Weill Cornell Medical College, both in New York City.
“This is a bit of a change from not only our previous guideline but some of the other guidelines out there, and it is based on the fact that we have very convincing evidence that starting with triple therapy yields to better long-term outcomes for our patients than starting with only two agents and waiting to see if they respond before escalating therapy,” she said. Other key updates include recommending use of pulse glucocorticoid therapy with a lower dose and more rapid steroid taper and treating patients with the recommended therapy for 3-5 years.
The guiding principles of the guideline are not only to preserve kidney function and minimize morbidity and mortality but also to ensure collaborative care with nephrology, to utilize shared decision-making that includes patients’ values and preferences, to reduce healthcare disparities, and to consider pediatric and geriatric populations. The guidelines are based on a quantitative synthesis of 105 studies that yielded 7 strong recommendations, 21 conditional recommendations, and 13 good practice statements — those commonly accepted as beneficial or practical advice even if there is little direct evidence to support them. The voting panel of 19 members included not only 3 nephrologists and 2 pediatric rheumatologists but also 2 patient representatives with LN.
The recommendations are just that, “a recommendation, not an order,” Sammaritano said, and strong recommendations are those “where we think, unequivocally, almost everybody should follow that recommendation. When we feel that we cannot make a strong recommendation, then we call our recommendation conditional, and it is conditional on looking at different things,” she said.
“Patients are different, especially lupus patients, and so one lupus nephritis patient may have different clinical characteristics, different thoughts about what therapy will work for them in their lives, or what therapy they really do not want to pursue,” Sammaritano said. “Maybe they can’t conceive of coming to the hospital once a month for intravenous therapy. Maybe they’re concerned about pill burden, which is something that our patient panel really emphasized to us. So, conditional recommendation means this voting panel thought that this was the best overall for most patients and most circumstances, recognizing there will still be a significant number of people, clinicians and patients, who may feel differently for that particular situation. So, that’s where you know the patient-clinician discussion can help with decision-making.”
What Are the Recommendations?
All patients with systemic lupus erythematosus (SLE) are strongly recommended to undergo proteinuria screening every 6-12 months or at the time of a flare. Those suspected of having LN should receive a prompt kidney biopsy and treatment with glucocorticoids while awaiting the biopsy and results. Two conditional recommendations for kidney biopsy include patients with SLE with unexplained impaired kidney function or a protein to creatinine ratio > 0.5 g/g, and patients with LN with a suspected flare after initial response or a lack of response or worsening after 6 months of therapy.
The guidelines include a strong recommendation for all patients with SLE to receive hydroxychloroquine and a conditional recommendation for all patients with elevated proteinuria (> 0.5 g/g) to receive renin-angiotensin-aldosterone system inhibitors (RAAS-I). Dosages in patients with LN with decreased glomerular filtration rate (GFR) should be adjusted as needed.
Sammaritano then reviewed the specifics on medication treatment. The glucocorticoid therapy in all patients with LN should begin with Pulse IV Therapy at 250-1000 mg/d for 1-3 days, followed by oral prednisone ≤ 0.5 mg/kg per day up to 40 mg/d, then tapered to a target dose > 5 mg/d within 6 months. The justification for this course comes from a 2024 systematic review finding pulse followed by oral glucocorticoids maximized complete renal response while minimizing toxicities, Sammaritano said.
“We have all become acutely aware of the very high risk of prolonged high dose of glucocorticoids for our patients,” she said, “and importantly, our patient panel participants strongly emphasized their preference for minimizing glucocorticoids dose.”
In addition to the recommendation of all patients receiving hydroxychloroquine and RAAS-I, first-line treatment of active, new-onset, or flaring LN should begin with triple therapy — glucocorticoids with two additional immunosuppressive agents. For patients with class III/IV LN, triple therapy includes the glucocorticoids course with a mycophenolic acid analog (MPAA) and either belimumab or a CNI. Conditional recommendations support MPAA with belimumab for significant extrarenal manifestations and MPAA with CNI for proteinuria ≥ 3 g/g.
An alternative triple therapy for class III/IV is glucocorticoids with low-dose cyclophosphamide and belimumab, but MPAA at 2-3 g/d is preferred over cyclophosphamide. The preferred regimen for cyclophosphamide is derived from the Euro-Lupus Nephritis Trial: Intravenous 500 mg every 2 weeks for six doses and then MPAA. Sammaritano noted that there are some limited data on using cyclophosphamide with belimumab, but “we do not specifically recommend cyclophosphamide with a CNI as one of our options because this combination has not been studied in randomized controlled trials.”
There are less data supporting class V recommendations, Sammaritano said, but for those with proteinuria of at least 1 g/g, the panel still recommends triple therapy with glucocorticoids, a MPAA, and a CNI. A CNI is preferred over belimumab because of its stabilizing effects on the podocyte cytoskeleton. Two alternative triple therapies for class V–only patients are glucocorticoids with belimumab and either low-dose cyclophosphamide or MPAA.
Dual therapy is only recommended if triple therapy is not available or not tolerated. The voting panel chose to recommend triple therapy over dual therapy with escalation for two reasons. First, the BLISS-LN and AURORA 1 trials showed improved outcomes with initial triple therapy over initial dual therapies.
Second, “nephron loss proceeds throughout a person’s lifetime even for those who do not have lupus nephritis, and every case of lupus nephritis or every period of time with uncontrolled lupus nephritis changes the course of that decline for the worse,” Sammaritano said. “So, we feel we can’t wait for nephron loss to implement what has been shown to be the most efficacious therapy. We want to gain rapid control of inflammation using the most effective regimen to prevent further damage and flare and maintain survival.”
Therapy is conditionally recommended for at least 3-5 years because “not only do we want to gain rapid control of disease activity [but we also] want to maintain control of disease activity until there’s sustained inactive disease,” Sammaritano said. “Repeat kidney biopsies show that immunologic activity persists in the kidneys for several years, and the withdrawal of immunosuppression when there is histologic activity predisposes patients to flare.” But immunosuppressive therapy can be tapered over time as determined by renal disease activity and medication tolerability.
For patients with refractory disease, consider additional factors that could be affecting the disease, such as adherence, the presence of other diagnoses, or advanced chronicity.
“If true refractory nephritis is present,” she said, “we recommend escalation to a more intensive regimen,” including the addition of anti-CD20 agents, combination therapy with three immunosuppressives, or referral for investigational therapy.
“We also emphasize the importance of other adjunctive therapies preventing comorbidities, such as cardiovascular disease, changes in bone health, or infection risk,” she said. In older patients, avoid polypharmacy as much as possible and be mindful of age-related GFR, she added.
A strong recommendation supported monitoring patients with LN and proteinuria at least every 3 months if they have not achieved complete renal response and every 3-6 months after sustained complete renal response.
Last, in patients with LN and end-stage kidney disease (ESKD), the voting panel strongly recommends transplant over dialysis and conditionally recommends proceeding to the transplant without requiring a complete clinical or serologic remission as long as no other organs are involved. In patients with LN at risk for ESKD, the guideline conditionally recommends consideration of a preemptive transplant, and patients on dialysis or post transplant are strongly recommended to regularly follow up with rheumatology.
Gabriel Kirsch, MD, a resident rheumatologist at the University of Florida College of Medicine, Jacksonville, said he found the guidelines helpful, “especially the guidance on the dichotomy between using belimumab and voclosporin and the clinical and patient preference that help you make that decision.”
Kirsch had hoped, however, to hear more about the impact of therapeutic drug monitoring of hydroxychloroquine on LN outcomes. He also noted a clinical scenario he’s come across that wasn’t addressed.
“When you’re checking GFR on these folks, a lot of our eGFR calculators are creatinine based, and creatinine at the extremes of muscle mass can be inaccurate,” such as getting artificially low creatinine readings from pediatric patients because of their low muscle mass or from patients with muscle atrophy caused by a lot of glucocorticoid exposure. “I was hoping for some more guidance on that,” he said.
Ellen Ginzler, MD, MPH, chief of rheumatology at SUNY Health Science Center in Brooklyn, New York, said the guidelines were pretty much what she expected them to be. She agreed with the panel’s advice that, when deciding between belimumab or voclosporin, “if it’s pure proteinuria, then you add voclosporin. If the patient has extra renal manifestations, you go with belimumab first.”
“They really made it quite clear that, despite the fact that people really want to reduce the amount of immunosuppression — and I agree you should taper steroids quickly — you really need to keep the immunosuppression for a prolonged period of time because all of the studies that have been done for years show that the longer you’re on immunosuppression after you achieve remission or a low disease activity state, the better your chance of not flaring,” Ginzler said. “Rapid tapering or discontinuation really increases the risk of flare.”
Sammaritano, Kirsch, and Ginzler had no disclosures. No external funding was used.
A version of this article appeared on Medscape.com.
FROM ACR 2024
Belly Fat Beats BMI in Predicting Colorectal Cancer Risk
TOPLINE:
METHODOLOGY:
- General obesity, often measured using BMI, is a recognized risk factor for colorectal cancer, but how much of this association is due to central obesity is unclear.
- Researchers assessed the associations between BMI, waist-to-hip ratio (WHR), and waist circumference (WC) with colorectal cancer risk and the degree of independence among these associations in patients aged 40-69 years recruited in the UK Biobank cohort study from 2006 to 2010.
- Anthropometric measurements were performed using standardized methods.
- Cancer registry and hospital data linkage identified colorectal cancer cases in the UK Biobank.
TAKEAWAY:
- Researchers included 460,784 participants (mean age, 56.3 years; 46.7% men), of whom 67.1% had either overweight or obesity, and 49.4% and 60.5% had high or very high WHR and WC, respectively.
- During the median 12.5-year follow-up period, 5977 participants developed colorectal cancer.
- Every SD increase in WHR (hazard ratio [HR], 1.18) showed a stronger association with colorectal cancer risk than in BMI (HR, 1.10).
- After adjustment for BMI, the association between WHR and colorectal cancer risk became slightly attenuated while still staying robust (HR, 1.15); however, after adjusting for WHR, the association between BMI and colorectal cancer risk became substantially weakened (HR, 1.04).
- WHR showed strongly significant associations with colorectal cancer risk across all BMI categories, whereas associations of BMI with colorectal cancer risk were weak and not statistically significant within all WHR categories.
- Central obesity demonstrated consistent associations with both colon and rectal cancer risks in both sexes before and after adjustment for BMI, whereas BMI showed no significant association with colorectal cancer risk in women or with rectal cancer risk after WHR adjustment.
IN PRACTICE:
“[The study] results also underline the importance of integrating additional anthropometric measures such as WHR alongside BMI into routine clinical practice for more effective prevention and management of obesity, whose prevalence is steadily increasing in many countries worldwide, in order to limit the global burden of colorectal cancer and many other obesity-related adverse health outcomes,” the authors wrote.
SOURCE:
The study was led by Fatemeh Safizadeh, German Cancer Research Center (DKFZ), Heidelberg. It was published online in The International Journal of Obesity.
LIMITATIONS:
This study relied on only one-time measurements of anthropometric measures at baseline, without considering previous lifetime history of overweight and obesity or changes during follow-up. Additionally, WHR and WC may not be the most accurate measures of central obesity, as WC includes both visceral and subcutaneous adipose tissue. The study population also showed evidence of healthy volunteer bias, with more health-conscious and socioeconomically advantaged participants being somewhat overrepresented.
DISCLOSURES:
The authors declared no competing interests.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- General obesity, often measured using BMI, is a recognized risk factor for colorectal cancer, but how much of this association is due to central obesity is unclear.
- Researchers assessed the associations between BMI, waist-to-hip ratio (WHR), and waist circumference (WC) with colorectal cancer risk and the degree of independence among these associations in patients aged 40-69 years recruited in the UK Biobank cohort study from 2006 to 2010.
- Anthropometric measurements were performed using standardized methods.
- Cancer registry and hospital data linkage identified colorectal cancer cases in the UK Biobank.
TAKEAWAY:
- Researchers included 460,784 participants (mean age, 56.3 years; 46.7% men), of whom 67.1% had either overweight or obesity, and 49.4% and 60.5% had high or very high WHR and WC, respectively.
- During the median 12.5-year follow-up period, 5977 participants developed colorectal cancer.
- Every SD increase in WHR (hazard ratio [HR], 1.18) showed a stronger association with colorectal cancer risk than in BMI (HR, 1.10).
- After adjustment for BMI, the association between WHR and colorectal cancer risk became slightly attenuated while still staying robust (HR, 1.15); however, after adjusting for WHR, the association between BMI and colorectal cancer risk became substantially weakened (HR, 1.04).
- WHR showed strongly significant associations with colorectal cancer risk across all BMI categories, whereas associations of BMI with colorectal cancer risk were weak and not statistically significant within all WHR categories.
- Central obesity demonstrated consistent associations with both colon and rectal cancer risks in both sexes before and after adjustment for BMI, whereas BMI showed no significant association with colorectal cancer risk in women or with rectal cancer risk after WHR adjustment.
IN PRACTICE:
“[The study] results also underline the importance of integrating additional anthropometric measures such as WHR alongside BMI into routine clinical practice for more effective prevention and management of obesity, whose prevalence is steadily increasing in many countries worldwide, in order to limit the global burden of colorectal cancer and many other obesity-related adverse health outcomes,” the authors wrote.
SOURCE:
The study was led by Fatemeh Safizadeh, German Cancer Research Center (DKFZ), Heidelberg. It was published online in The International Journal of Obesity.
LIMITATIONS:
This study relied on only one-time measurements of anthropometric measures at baseline, without considering previous lifetime history of overweight and obesity or changes during follow-up. Additionally, WHR and WC may not be the most accurate measures of central obesity, as WC includes both visceral and subcutaneous adipose tissue. The study population also showed evidence of healthy volunteer bias, with more health-conscious and socioeconomically advantaged participants being somewhat overrepresented.
DISCLOSURES:
The authors declared no competing interests.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- General obesity, often measured using BMI, is a recognized risk factor for colorectal cancer, but how much of this association is due to central obesity is unclear.
- Researchers assessed the associations between BMI, waist-to-hip ratio (WHR), and waist circumference (WC) with colorectal cancer risk and the degree of independence among these associations in patients aged 40-69 years recruited in the UK Biobank cohort study from 2006 to 2010.
- Anthropometric measurements were performed using standardized methods.
- Cancer registry and hospital data linkage identified colorectal cancer cases in the UK Biobank.
TAKEAWAY:
- Researchers included 460,784 participants (mean age, 56.3 years; 46.7% men), of whom 67.1% had either overweight or obesity, and 49.4% and 60.5% had high or very high WHR and WC, respectively.
- During the median 12.5-year follow-up period, 5977 participants developed colorectal cancer.
- Every SD increase in WHR (hazard ratio [HR], 1.18) showed a stronger association with colorectal cancer risk than in BMI (HR, 1.10).
- After adjustment for BMI, the association between WHR and colorectal cancer risk became slightly attenuated while still staying robust (HR, 1.15); however, after adjusting for WHR, the association between BMI and colorectal cancer risk became substantially weakened (HR, 1.04).
- WHR showed strongly significant associations with colorectal cancer risk across all BMI categories, whereas associations of BMI with colorectal cancer risk were weak and not statistically significant within all WHR categories.
- Central obesity demonstrated consistent associations with both colon and rectal cancer risks in both sexes before and after adjustment for BMI, whereas BMI showed no significant association with colorectal cancer risk in women or with rectal cancer risk after WHR adjustment.
IN PRACTICE:
“[The study] results also underline the importance of integrating additional anthropometric measures such as WHR alongside BMI into routine clinical practice for more effective prevention and management of obesity, whose prevalence is steadily increasing in many countries worldwide, in order to limit the global burden of colorectal cancer and many other obesity-related adverse health outcomes,” the authors wrote.
SOURCE:
The study was led by Fatemeh Safizadeh, German Cancer Research Center (DKFZ), Heidelberg. It was published online in The International Journal of Obesity.
LIMITATIONS:
This study relied on only one-time measurements of anthropometric measures at baseline, without considering previous lifetime history of overweight and obesity or changes during follow-up. Additionally, WHR and WC may not be the most accurate measures of central obesity, as WC includes both visceral and subcutaneous adipose tissue. The study population also showed evidence of healthy volunteer bias, with more health-conscious and socioeconomically advantaged participants being somewhat overrepresented.
DISCLOSURES:
The authors declared no competing interests.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Adalimumab for Psoriasis: Study Compares Biosimilars Vs. Originator
TOPLINE:
rate than those who remained on Humira.
METHODOLOGY:
- Researchers conducted a cohort study using data on patients with psoriasis who were treated with adalimumab, a tumor necrosis factor alpha inhibitor used to treat moderate to severe psoriasis, from the French National Health Data System, British Association of Dermatologists Biologics and Immunomodulators Register, and Spanish Registry of Systemic Therapy in Psoriasis.
- The analysis included 7387 adalimumab-naive patients who were new users of an adalimumab biosimilar and 3654 patients (switchers) who switched from Humira to a biosimilar. Patients were matched and compared with patients receiving Humira.
- Co-primary outcomes of the study were drug discontinuation and serious adverse events.
- Researchers assessed the following adalimumab biosimilar brands: Amgevita, Imraldi, Hyrimoz, Idacio, and Hulio.
TAKEAWAY:
- All-cause drug discontinuation rates were similar between new users of biosimilars and Humira new users (hazard ratio [HR], 0.99; 95% CI, 0.94-1.04).
- Discontinuation rates were higher among those who switched from Humira to a biosimilar (HR, 1.35; 95% CI, 1.19-1.52) than among those who stayed on Humira. Switching to Amgevita (HR, 1.25; 95% CI, 1.13-1.27), Imraldi (HR, 1.53; 95% CI, 1.33-1.76), and Hyrimoz (HR, 1.80; 95% CI, 1.29-2.52) was associated with higher discontinuation rates.
- Serious adverse events were not significantly different between new users of Humira and biosimilar new users (incidence rate ratio [IRR], 0.91; 95% CI, 0.80-1.05), and between patients who switched from a biosimilar to Humira and those who stayed on Humira (IRR, 0.92; 95% CI, 0.83-1.01).
- No significant differences in discontinuation because of ineffectiveness were found between biosimilar and Humira new users (HR, 0.97; 95% CI, 0.88-1.08). Discontinuation because of adverse events was also comparable for all biosimilars among new users, except for Hyrimoz (HR, 0.54; 95% CI, 0.35-0.85), which showed fewer discontinuations than Humira.
IN PRACTICE:
“This study found comparable drug survival and safety between adalimumab biosimilars and Humira in adalimumab-naive patients, supporting the use of biosimilars as viable alternatives for new patients,” the authors wrote. However, noting that discontinuation was more likely among those who switched from Humira to a biosimilar, they added: “Changes in treatment response, skin or injection site reactions, and nocebo effects may contribute to treatment discontinuation post-switch. Thus, patients who switch from Humira to biosimilars may require closer monitoring and support to alleviate these challenges.”
SOURCE:
The study was led by Duc Binh Phan, Dermatology Centre, Northern Care Alliance NHS Foundation Trust in Manchester, England. It was published online in The British Journal of Dermatology.
LIMITATIONS:
Unmeasured factors including psychological perceptions, regional policies, and drug availability could influence drug survival, making the results not fully reflective of treatment effectiveness or safety. Most Humira users in registries were enrolled before biosimilars became available, making it impractical to match new users on the basis of treatment initiation years. Additionally, reasons for discontinuation were not available in the French National Health Data System.
DISCLOSURES:
In the United Kingdom, the research was funded by the Psoriasis Association PhD studentship and supported by the NIHR Manchester Biomedical Research Centre. In France, the authors are employees of the French National Health Insurance, the French National Agency for the Safety of Medicines and Health Products, and the Assistance Publique — Hôpitaux de Paris and received no funding. The authors reported receiving consulting and speaker fees and clinical trial sponsorship from various pharmaceutical companies. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
rate than those who remained on Humira.
METHODOLOGY:
- Researchers conducted a cohort study using data on patients with psoriasis who were treated with adalimumab, a tumor necrosis factor alpha inhibitor used to treat moderate to severe psoriasis, from the French National Health Data System, British Association of Dermatologists Biologics and Immunomodulators Register, and Spanish Registry of Systemic Therapy in Psoriasis.
- The analysis included 7387 adalimumab-naive patients who were new users of an adalimumab biosimilar and 3654 patients (switchers) who switched from Humira to a biosimilar. Patients were matched and compared with patients receiving Humira.
- Co-primary outcomes of the study were drug discontinuation and serious adverse events.
- Researchers assessed the following adalimumab biosimilar brands: Amgevita, Imraldi, Hyrimoz, Idacio, and Hulio.
TAKEAWAY:
- All-cause drug discontinuation rates were similar between new users of biosimilars and Humira new users (hazard ratio [HR], 0.99; 95% CI, 0.94-1.04).
- Discontinuation rates were higher among those who switched from Humira to a biosimilar (HR, 1.35; 95% CI, 1.19-1.52) than among those who stayed on Humira. Switching to Amgevita (HR, 1.25; 95% CI, 1.13-1.27), Imraldi (HR, 1.53; 95% CI, 1.33-1.76), and Hyrimoz (HR, 1.80; 95% CI, 1.29-2.52) was associated with higher discontinuation rates.
- Serious adverse events were not significantly different between new users of Humira and biosimilar new users (incidence rate ratio [IRR], 0.91; 95% CI, 0.80-1.05), and between patients who switched from a biosimilar to Humira and those who stayed on Humira (IRR, 0.92; 95% CI, 0.83-1.01).
- No significant differences in discontinuation because of ineffectiveness were found between biosimilar and Humira new users (HR, 0.97; 95% CI, 0.88-1.08). Discontinuation because of adverse events was also comparable for all biosimilars among new users, except for Hyrimoz (HR, 0.54; 95% CI, 0.35-0.85), which showed fewer discontinuations than Humira.
IN PRACTICE:
“This study found comparable drug survival and safety between adalimumab biosimilars and Humira in adalimumab-naive patients, supporting the use of biosimilars as viable alternatives for new patients,” the authors wrote. However, noting that discontinuation was more likely among those who switched from Humira to a biosimilar, they added: “Changes in treatment response, skin or injection site reactions, and nocebo effects may contribute to treatment discontinuation post-switch. Thus, patients who switch from Humira to biosimilars may require closer monitoring and support to alleviate these challenges.”
SOURCE:
The study was led by Duc Binh Phan, Dermatology Centre, Northern Care Alliance NHS Foundation Trust in Manchester, England. It was published online in The British Journal of Dermatology.
LIMITATIONS:
Unmeasured factors including psychological perceptions, regional policies, and drug availability could influence drug survival, making the results not fully reflective of treatment effectiveness or safety. Most Humira users in registries were enrolled before biosimilars became available, making it impractical to match new users on the basis of treatment initiation years. Additionally, reasons for discontinuation were not available in the French National Health Data System.
DISCLOSURES:
In the United Kingdom, the research was funded by the Psoriasis Association PhD studentship and supported by the NIHR Manchester Biomedical Research Centre. In France, the authors are employees of the French National Health Insurance, the French National Agency for the Safety of Medicines and Health Products, and the Assistance Publique — Hôpitaux de Paris and received no funding. The authors reported receiving consulting and speaker fees and clinical trial sponsorship from various pharmaceutical companies. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
rate than those who remained on Humira.
METHODOLOGY:
- Researchers conducted a cohort study using data on patients with psoriasis who were treated with adalimumab, a tumor necrosis factor alpha inhibitor used to treat moderate to severe psoriasis, from the French National Health Data System, British Association of Dermatologists Biologics and Immunomodulators Register, and Spanish Registry of Systemic Therapy in Psoriasis.
- The analysis included 7387 adalimumab-naive patients who were new users of an adalimumab biosimilar and 3654 patients (switchers) who switched from Humira to a biosimilar. Patients were matched and compared with patients receiving Humira.
- Co-primary outcomes of the study were drug discontinuation and serious adverse events.
- Researchers assessed the following adalimumab biosimilar brands: Amgevita, Imraldi, Hyrimoz, Idacio, and Hulio.
TAKEAWAY:
- All-cause drug discontinuation rates were similar between new users of biosimilars and Humira new users (hazard ratio [HR], 0.99; 95% CI, 0.94-1.04).
- Discontinuation rates were higher among those who switched from Humira to a biosimilar (HR, 1.35; 95% CI, 1.19-1.52) than among those who stayed on Humira. Switching to Amgevita (HR, 1.25; 95% CI, 1.13-1.27), Imraldi (HR, 1.53; 95% CI, 1.33-1.76), and Hyrimoz (HR, 1.80; 95% CI, 1.29-2.52) was associated with higher discontinuation rates.
- Serious adverse events were not significantly different between new users of Humira and biosimilar new users (incidence rate ratio [IRR], 0.91; 95% CI, 0.80-1.05), and between patients who switched from a biosimilar to Humira and those who stayed on Humira (IRR, 0.92; 95% CI, 0.83-1.01).
- No significant differences in discontinuation because of ineffectiveness were found between biosimilar and Humira new users (HR, 0.97; 95% CI, 0.88-1.08). Discontinuation because of adverse events was also comparable for all biosimilars among new users, except for Hyrimoz (HR, 0.54; 95% CI, 0.35-0.85), which showed fewer discontinuations than Humira.
IN PRACTICE:
“This study found comparable drug survival and safety between adalimumab biosimilars and Humira in adalimumab-naive patients, supporting the use of biosimilars as viable alternatives for new patients,” the authors wrote. However, noting that discontinuation was more likely among those who switched from Humira to a biosimilar, they added: “Changes in treatment response, skin or injection site reactions, and nocebo effects may contribute to treatment discontinuation post-switch. Thus, patients who switch from Humira to biosimilars may require closer monitoring and support to alleviate these challenges.”
SOURCE:
The study was led by Duc Binh Phan, Dermatology Centre, Northern Care Alliance NHS Foundation Trust in Manchester, England. It was published online in The British Journal of Dermatology.
LIMITATIONS:
Unmeasured factors including psychological perceptions, regional policies, and drug availability could influence drug survival, making the results not fully reflective of treatment effectiveness or safety. Most Humira users in registries were enrolled before biosimilars became available, making it impractical to match new users on the basis of treatment initiation years. Additionally, reasons for discontinuation were not available in the French National Health Data System.
DISCLOSURES:
In the United Kingdom, the research was funded by the Psoriasis Association PhD studentship and supported by the NIHR Manchester Biomedical Research Centre. In France, the authors are employees of the French National Health Insurance, the French National Agency for the Safety of Medicines and Health Products, and the Assistance Publique — Hôpitaux de Paris and received no funding. The authors reported receiving consulting and speaker fees and clinical trial sponsorship from various pharmaceutical companies. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Treating Onychomycosis: Pearls from a Podiatrist
LAS VEGAS —
According to Tracey C. Vlahovic, DPM, a professor at the Samuel Merritt University College of Podiatric Medicine, Oakland, California, most cases of onychomycosis are caused by the dermatophytes Trichophyton rubrum and T mentagrophytes, although the cause can also be a mixed infection. “Dermatophytes are going to impact the nails first, and molds may come in and join the party later,” she said at the Society of Dermatology Physician Associates (SDPA) 22nd Annual Fall Dermatology Conference.

“The distal subungual onychomycosis (DSO) type is still the most common, but don’t forget that onychomycosis and nail psoriasis can happen at the same time. What we can’t lose sight of is that onychomycosis is a disease of the nail bed, which ultimately affects the nail plate; it’s not a disease of the nail plate first.”
Her diagnostic approach combines periodic acid-Schiff (PAS) staining with fungal culture “because I like to know the speciation,” she said. “PAS doesn’t give me the speciation; fungal cultures should. PCR can be expensive, but that can give me speciation.”
How Does This Happen?
Fungal DSO occurs because of exposure to a dermatophyte, which can be as simple as tinea pedis. “Perhaps it’s the environment in the shoe,” said Vlahovic, one of the authors of a textbook on onychomycosis. “That’s something I’m always concentrating on with the patient. What is your foot hygiene like? What’s your shoe and sock wear? What’s your level of physical activity? You can have trauma to the hyponychium, where the skin and the nail meet. Maybe they trim their nails too close to the skin, or maybe there’s another skin condition like psoriasis.”
The dermatophyte, she continued, enters and invades the nail at the hyponychium and uses the keratinase enzyme to digest keratin in the nail bed. Mild inflammation develops, and pH changes cause focal parakeratosis and subungual hyperkeratosis in the form of onycholysis and subungual debris. “Hyphae then invade the lamina of the nail plate, which causes brittle nails,” she said. “The compromised hyponychium creates a reservoir for molds and bacteria.”
Therapies approved by the Food and Drug Administration (FDA) for onychomycosis include the topical agents efinaconazole, tavaborole, and ciclopirox; the oral agents terbinafine and itraconazole; and laser therapy. Off-label, Vlahovic said that she sometimes uses oral fluconazole, pulsed dosing for terbinafine, and booster doses of terbinafine or any approved oral antifungal agent. Pulse dosing for itraconazole is FDA-approved for fingernails but not for toenails.
“We don’t have any oral antifungals that are approved for children, but we do have weight-based dosing,” she noted. Other off-label treatments for onychomycosis that patients may come across while browsing the internet but do not penetrate the nail plate, include products containing tolnaftate, tree oil, and undecylenic acid, “which is a very long-chain antifungal,” Vlahovic said. “It’s so huge that it can’t get through the nail plate. These products must get through the nail plate into the nail bed where the infection is.”
According to therapeutic recommendations for the treatment of toenail onychomycosis in the United States, published in 2021, terbinafine is the primary choice for oral treatment and efinaconazole 10% for topical treatment. There are no current treatment recommendations for pregnant or lactating patients. “I always defer to the obstetrician,” said Vlahovic, a coauthor of the recommendations. For pediatric patients, there are approved topical medications: Efinaconazole and tavaborole for ages 6 and up and ciclopirox for ages 12 years or older.
Treatment recommendations for adults vary based on clinical presentation and patient characteristics. Questions to consider: Are they older? Do they have diabetes? Are they able to reach their feet to apply medication? What other medications are they taking? Are there any kidney or liver issues that are cause for concern?
Another question to consider is whether they have concurrent nail psoriasis. “When I have those patients, I often treat the onychomycosis first and the nail psoriasis second,” she said.
Evidence for Lasers Weak
Though laser therapy is FDA approved for the temporary increase of clear nails in onychomycosis, Vlahovic is underwhelmed by the evidence of its use for onychomycosis. According to a systematic review of 261 studies, only 1 reported treatment success as 16.7%, and clinical cures ranged from 13% to 16%. “Many of the existing studies were so poorly done in terms of protocols; it was frustrating,” she said. “No study has reported complete cure. There’s a lack of standardization across laser companies and a lack of standardization across protocols.”
Before starting oral antifungal therapy, Vlahovic uses the Onychomycosis Severity Index to determine the number of nails involved and the proportion of nails that are affected. She also wants to know if the patient is taking any medication that might interfere with an oral antifungal and gets baseline liver function tests (LFTs) to document results in the chart. “You want to discuss the pros and cons of oral antifungal therapy, and you want to set realistic expectations,” she added. “These medications are not cosmetic products; they are meant to kill fungus. Sometimes patients lose sight of that.”
Vlahovic routinely offers pulse dosing of terbinafine, which is FDA approved at a dose of 250 mg/d for 90 days. Pulse dosing involves taking terbinafine 250 mg twice a day for 1 week, followed by a 3-week break. This cycle is repeated three or four times. A clinical trial found no significant difference in outcome between patients who received pulsed vs continuous terbinafine dosing for the treatment of dermatophyte onychomycosis.
What About Oral Antifungal Safety?
For patients who ask about the safety of oral antifungals, Vlahovic characterized them as “well tolerated and safe in an immunocompetent population.” In a meta-analysis of 122 studies of about 22,000 patients, the pooled risk for treatment discontinuation because of adverse events was 3.4% for terbinafine 250 mg/d and 4.21% for itraconazole 200 mg/d. The risk for liver injury requiring termination of treatment and the risk of having symptomatic elevation of LFTs were less than 2% for all regimens.
According to the best available published evidence, Vlahovic said, the onychomycosis recurrence rate ranges from 6% to 40%. “That’s a wild number. We really have no idea what the true recurrence rate is, and that’s a problem.”
Vlahovic disclosed having been a consultant to and an investigator for Ortho Dermatologics and Sagis Diagnostics.
A version of this article appeared on Medscape.com.
LAS VEGAS —
According to Tracey C. Vlahovic, DPM, a professor at the Samuel Merritt University College of Podiatric Medicine, Oakland, California, most cases of onychomycosis are caused by the dermatophytes Trichophyton rubrum and T mentagrophytes, although the cause can also be a mixed infection. “Dermatophytes are going to impact the nails first, and molds may come in and join the party later,” she said at the Society of Dermatology Physician Associates (SDPA) 22nd Annual Fall Dermatology Conference.
“The distal subungual onychomycosis (DSO) type is still the most common, but don’t forget that onychomycosis and nail psoriasis can happen at the same time. What we can’t lose sight of is that onychomycosis is a disease of the nail bed, which ultimately affects the nail plate; it’s not a disease of the nail plate first.”
Her diagnostic approach combines periodic acid-Schiff (PAS) staining with fungal culture “because I like to know the speciation,” she said. “PAS doesn’t give me the speciation; fungal cultures should. PCR can be expensive, but that can give me speciation.”
How Does This Happen?
Fungal DSO occurs because of exposure to a dermatophyte, which can be as simple as tinea pedis. “Perhaps it’s the environment in the shoe,” said Vlahovic, one of the authors of a textbook on onychomycosis. “That’s something I’m always concentrating on with the patient. What is your foot hygiene like? What’s your shoe and sock wear? What’s your level of physical activity? You can have trauma to the hyponychium, where the skin and the nail meet. Maybe they trim their nails too close to the skin, or maybe there’s another skin condition like psoriasis.”
The dermatophyte, she continued, enters and invades the nail at the hyponychium and uses the keratinase enzyme to digest keratin in the nail bed. Mild inflammation develops, and pH changes cause focal parakeratosis and subungual hyperkeratosis in the form of onycholysis and subungual debris. “Hyphae then invade the lamina of the nail plate, which causes brittle nails,” she said. “The compromised hyponychium creates a reservoir for molds and bacteria.”
Therapies approved by the Food and Drug Administration (FDA) for onychomycosis include the topical agents efinaconazole, tavaborole, and ciclopirox; the oral agents terbinafine and itraconazole; and laser therapy. Off-label, Vlahovic said that she sometimes uses oral fluconazole, pulsed dosing for terbinafine, and booster doses of terbinafine or any approved oral antifungal agent. Pulse dosing for itraconazole is FDA-approved for fingernails but not for toenails.
“We don’t have any oral antifungals that are approved for children, but we do have weight-based dosing,” she noted. Other off-label treatments for onychomycosis that patients may come across while browsing the internet but do not penetrate the nail plate, include products containing tolnaftate, tree oil, and undecylenic acid, “which is a very long-chain antifungal,” Vlahovic said. “It’s so huge that it can’t get through the nail plate. These products must get through the nail plate into the nail bed where the infection is.”
According to therapeutic recommendations for the treatment of toenail onychomycosis in the United States, published in 2021, terbinafine is the primary choice for oral treatment and efinaconazole 10% for topical treatment. There are no current treatment recommendations for pregnant or lactating patients. “I always defer to the obstetrician,” said Vlahovic, a coauthor of the recommendations. For pediatric patients, there are approved topical medications: Efinaconazole and tavaborole for ages 6 and up and ciclopirox for ages 12 years or older.
Treatment recommendations for adults vary based on clinical presentation and patient characteristics. Questions to consider: Are they older? Do they have diabetes? Are they able to reach their feet to apply medication? What other medications are they taking? Are there any kidney or liver issues that are cause for concern?
Another question to consider is whether they have concurrent nail psoriasis. “When I have those patients, I often treat the onychomycosis first and the nail psoriasis second,” she said.
Evidence for Lasers Weak
Though laser therapy is FDA approved for the temporary increase of clear nails in onychomycosis, Vlahovic is underwhelmed by the evidence of its use for onychomycosis. According to a systematic review of 261 studies, only 1 reported treatment success as 16.7%, and clinical cures ranged from 13% to 16%. “Many of the existing studies were so poorly done in terms of protocols; it was frustrating,” she said. “No study has reported complete cure. There’s a lack of standardization across laser companies and a lack of standardization across protocols.”
Before starting oral antifungal therapy, Vlahovic uses the Onychomycosis Severity Index to determine the number of nails involved and the proportion of nails that are affected. She also wants to know if the patient is taking any medication that might interfere with an oral antifungal and gets baseline liver function tests (LFTs) to document results in the chart. “You want to discuss the pros and cons of oral antifungal therapy, and you want to set realistic expectations,” she added. “These medications are not cosmetic products; they are meant to kill fungus. Sometimes patients lose sight of that.”
Vlahovic routinely offers pulse dosing of terbinafine, which is FDA approved at a dose of 250 mg/d for 90 days. Pulse dosing involves taking terbinafine 250 mg twice a day for 1 week, followed by a 3-week break. This cycle is repeated three or four times. A clinical trial found no significant difference in outcome between patients who received pulsed vs continuous terbinafine dosing for the treatment of dermatophyte onychomycosis.
What About Oral Antifungal Safety?
For patients who ask about the safety of oral antifungals, Vlahovic characterized them as “well tolerated and safe in an immunocompetent population.” In a meta-analysis of 122 studies of about 22,000 patients, the pooled risk for treatment discontinuation because of adverse events was 3.4% for terbinafine 250 mg/d and 4.21% for itraconazole 200 mg/d. The risk for liver injury requiring termination of treatment and the risk of having symptomatic elevation of LFTs were less than 2% for all regimens.
According to the best available published evidence, Vlahovic said, the onychomycosis recurrence rate ranges from 6% to 40%. “That’s a wild number. We really have no idea what the true recurrence rate is, and that’s a problem.”
Vlahovic disclosed having been a consultant to and an investigator for Ortho Dermatologics and Sagis Diagnostics.
A version of this article appeared on Medscape.com.
LAS VEGAS —
According to Tracey C. Vlahovic, DPM, a professor at the Samuel Merritt University College of Podiatric Medicine, Oakland, California, most cases of onychomycosis are caused by the dermatophytes Trichophyton rubrum and T mentagrophytes, although the cause can also be a mixed infection. “Dermatophytes are going to impact the nails first, and molds may come in and join the party later,” she said at the Society of Dermatology Physician Associates (SDPA) 22nd Annual Fall Dermatology Conference.
“The distal subungual onychomycosis (DSO) type is still the most common, but don’t forget that onychomycosis and nail psoriasis can happen at the same time. What we can’t lose sight of is that onychomycosis is a disease of the nail bed, which ultimately affects the nail plate; it’s not a disease of the nail plate first.”
Her diagnostic approach combines periodic acid-Schiff (PAS) staining with fungal culture “because I like to know the speciation,” she said. “PAS doesn’t give me the speciation; fungal cultures should. PCR can be expensive, but that can give me speciation.”
How Does This Happen?
Fungal DSO occurs because of exposure to a dermatophyte, which can be as simple as tinea pedis. “Perhaps it’s the environment in the shoe,” said Vlahovic, one of the authors of a textbook on onychomycosis. “That’s something I’m always concentrating on with the patient. What is your foot hygiene like? What’s your shoe and sock wear? What’s your level of physical activity? You can have trauma to the hyponychium, where the skin and the nail meet. Maybe they trim their nails too close to the skin, or maybe there’s another skin condition like psoriasis.”
The dermatophyte, she continued, enters and invades the nail at the hyponychium and uses the keratinase enzyme to digest keratin in the nail bed. Mild inflammation develops, and pH changes cause focal parakeratosis and subungual hyperkeratosis in the form of onycholysis and subungual debris. “Hyphae then invade the lamina of the nail plate, which causes brittle nails,” she said. “The compromised hyponychium creates a reservoir for molds and bacteria.”
Therapies approved by the Food and Drug Administration (FDA) for onychomycosis include the topical agents efinaconazole, tavaborole, and ciclopirox; the oral agents terbinafine and itraconazole; and laser therapy. Off-label, Vlahovic said that she sometimes uses oral fluconazole, pulsed dosing for terbinafine, and booster doses of terbinafine or any approved oral antifungal agent. Pulse dosing for itraconazole is FDA-approved for fingernails but not for toenails.
“We don’t have any oral antifungals that are approved for children, but we do have weight-based dosing,” she noted. Other off-label treatments for onychomycosis that patients may come across while browsing the internet but do not penetrate the nail plate, include products containing tolnaftate, tree oil, and undecylenic acid, “which is a very long-chain antifungal,” Vlahovic said. “It’s so huge that it can’t get through the nail plate. These products must get through the nail plate into the nail bed where the infection is.”
According to therapeutic recommendations for the treatment of toenail onychomycosis in the United States, published in 2021, terbinafine is the primary choice for oral treatment and efinaconazole 10% for topical treatment. There are no current treatment recommendations for pregnant or lactating patients. “I always defer to the obstetrician,” said Vlahovic, a coauthor of the recommendations. For pediatric patients, there are approved topical medications: Efinaconazole and tavaborole for ages 6 and up and ciclopirox for ages 12 years or older.
Treatment recommendations for adults vary based on clinical presentation and patient characteristics. Questions to consider: Are they older? Do they have diabetes? Are they able to reach their feet to apply medication? What other medications are they taking? Are there any kidney or liver issues that are cause for concern?
Another question to consider is whether they have concurrent nail psoriasis. “When I have those patients, I often treat the onychomycosis first and the nail psoriasis second,” she said.
Evidence for Lasers Weak
Though laser therapy is FDA approved for the temporary increase of clear nails in onychomycosis, Vlahovic is underwhelmed by the evidence of its use for onychomycosis. According to a systematic review of 261 studies, only 1 reported treatment success as 16.7%, and clinical cures ranged from 13% to 16%. “Many of the existing studies were so poorly done in terms of protocols; it was frustrating,” she said. “No study has reported complete cure. There’s a lack of standardization across laser companies and a lack of standardization across protocols.”
Before starting oral antifungal therapy, Vlahovic uses the Onychomycosis Severity Index to determine the number of nails involved and the proportion of nails that are affected. She also wants to know if the patient is taking any medication that might interfere with an oral antifungal and gets baseline liver function tests (LFTs) to document results in the chart. “You want to discuss the pros and cons of oral antifungal therapy, and you want to set realistic expectations,” she added. “These medications are not cosmetic products; they are meant to kill fungus. Sometimes patients lose sight of that.”
Vlahovic routinely offers pulse dosing of terbinafine, which is FDA approved at a dose of 250 mg/d for 90 days. Pulse dosing involves taking terbinafine 250 mg twice a day for 1 week, followed by a 3-week break. This cycle is repeated three or four times. A clinical trial found no significant difference in outcome between patients who received pulsed vs continuous terbinafine dosing for the treatment of dermatophyte onychomycosis.
What About Oral Antifungal Safety?
For patients who ask about the safety of oral antifungals, Vlahovic characterized them as “well tolerated and safe in an immunocompetent population.” In a meta-analysis of 122 studies of about 22,000 patients, the pooled risk for treatment discontinuation because of adverse events was 3.4% for terbinafine 250 mg/d and 4.21% for itraconazole 200 mg/d. The risk for liver injury requiring termination of treatment and the risk of having symptomatic elevation of LFTs were less than 2% for all regimens.
According to the best available published evidence, Vlahovic said, the onychomycosis recurrence rate ranges from 6% to 40%. “That’s a wild number. We really have no idea what the true recurrence rate is, and that’s a problem.”
Vlahovic disclosed having been a consultant to and an investigator for Ortho Dermatologics and Sagis Diagnostics.
A version of this article appeared on Medscape.com.
FROM SDPA 2024
Study Finds Different Survival Rates for Hidradenitis Suppurativa Treatments in Children
results from a small single-center study showed.
A previous study found that overall drug survival of adalimumab and infliximab in adults with HS at 12 and 24 months was 56.3% and 30.5%, and 58.3% and 48.6%, respectively. “They also found that older age, longer disease duration, higher body mass index (BMI), and surgery during treatment are associated with increased drug survival,” Robyn Guo, a third-year medical student at Duke University, Durham, North Carolina, told this news organization following the annual Symposium on Hidradenitis Suppurativa Advances, where the study was presented during an oral abstract session. “To our knowledge, the drug survival of biologic therapies in pediatric HS patients has not been previously investigated.”
Adalimumab and infliximab are tumor necrosis factor blockers approved for multiple indications; adalimumab is approved for treating moderate to severe HS in patients aged 12 years or older. Infliximab is not approved for HS but is used to treat the disease.
To determine the drug survival of adalimumab and infliximab in pediatric patients with HS and whether patient comorbidities and HS lesion location are associated with length of biologic survival in pediatric patients with HS, Guo and colleagues used Kaplan-Meier survival curves to calculate biologic survival at 12 and 24 months following biologic initiation and Cox proportional hazards regression to analyze potential factors associated with biologic survival. The study population included 49 pediatric patients in the adalimumab cohort and 11 in the infliximab cohort.
The researchers found that drug survival for adalimumab was 90.6% at 12 months (95% CI, 83.0%-98.8%) and 78.3% at 24 months (95% CI, 67.7%-90.6%), while drug survival for infliximab was 54.5% at 12 months (95% CI, 31.8%-93.6%) and 36.4% at 24 months, an overall difference that reached statistical significance (P = .0009). “Our data suggests that adalimumab survival is significantly higher than infliximab survival in pediatric HS patients,” Guo said.
On univariate Cox regression analysis, gluteal HS lesions were associated with shorter adalimumab survival, and obesity was associated with longer infliximab survival.
The researchers acknowledged certain limitations of their study, including the small sample size and that unadjusted Cox regression analysis did not account for baseline HS severity, biologic therapy dosing, and concomitant medication use. Also, there were patients in both cohorts who were not biologic-naive: Two in the adalimumab cohort were previously treated with infliximab, and five patients in the infliximab cohort were previously treated with adalimumab.
“We plan on conducting further analysis using adjusted Cox regression analysis to account for baseline disease severity measured by Hurley stage, BMI, medication dosing, and concomitant medication use,” Guo said.
The researchers reported having no financial disclosures.
A version of this article appeared on Medscape.com.
results from a small single-center study showed.
A previous study found that overall drug survival of adalimumab and infliximab in adults with HS at 12 and 24 months was 56.3% and 30.5%, and 58.3% and 48.6%, respectively. “They also found that older age, longer disease duration, higher body mass index (BMI), and surgery during treatment are associated with increased drug survival,” Robyn Guo, a third-year medical student at Duke University, Durham, North Carolina, told this news organization following the annual Symposium on Hidradenitis Suppurativa Advances, where the study was presented during an oral abstract session. “To our knowledge, the drug survival of biologic therapies in pediatric HS patients has not been previously investigated.”
Adalimumab and infliximab are tumor necrosis factor blockers approved for multiple indications; adalimumab is approved for treating moderate to severe HS in patients aged 12 years or older. Infliximab is not approved for HS but is used to treat the disease.
To determine the drug survival of adalimumab and infliximab in pediatric patients with HS and whether patient comorbidities and HS lesion location are associated with length of biologic survival in pediatric patients with HS, Guo and colleagues used Kaplan-Meier survival curves to calculate biologic survival at 12 and 24 months following biologic initiation and Cox proportional hazards regression to analyze potential factors associated with biologic survival. The study population included 49 pediatric patients in the adalimumab cohort and 11 in the infliximab cohort.
The researchers found that drug survival for adalimumab was 90.6% at 12 months (95% CI, 83.0%-98.8%) and 78.3% at 24 months (95% CI, 67.7%-90.6%), while drug survival for infliximab was 54.5% at 12 months (95% CI, 31.8%-93.6%) and 36.4% at 24 months, an overall difference that reached statistical significance (P = .0009). “Our data suggests that adalimumab survival is significantly higher than infliximab survival in pediatric HS patients,” Guo said.
On univariate Cox regression analysis, gluteal HS lesions were associated with shorter adalimumab survival, and obesity was associated with longer infliximab survival.
The researchers acknowledged certain limitations of their study, including the small sample size and that unadjusted Cox regression analysis did not account for baseline HS severity, biologic therapy dosing, and concomitant medication use. Also, there were patients in both cohorts who were not biologic-naive: Two in the adalimumab cohort were previously treated with infliximab, and five patients in the infliximab cohort were previously treated with adalimumab.
“We plan on conducting further analysis using adjusted Cox regression analysis to account for baseline disease severity measured by Hurley stage, BMI, medication dosing, and concomitant medication use,” Guo said.
The researchers reported having no financial disclosures.
A version of this article appeared on Medscape.com.
results from a small single-center study showed.
A previous study found that overall drug survival of adalimumab and infliximab in adults with HS at 12 and 24 months was 56.3% and 30.5%, and 58.3% and 48.6%, respectively. “They also found that older age, longer disease duration, higher body mass index (BMI), and surgery during treatment are associated with increased drug survival,” Robyn Guo, a third-year medical student at Duke University, Durham, North Carolina, told this news organization following the annual Symposium on Hidradenitis Suppurativa Advances, where the study was presented during an oral abstract session. “To our knowledge, the drug survival of biologic therapies in pediatric HS patients has not been previously investigated.”
Adalimumab and infliximab are tumor necrosis factor blockers approved for multiple indications; adalimumab is approved for treating moderate to severe HS in patients aged 12 years or older. Infliximab is not approved for HS but is used to treat the disease.
To determine the drug survival of adalimumab and infliximab in pediatric patients with HS and whether patient comorbidities and HS lesion location are associated with length of biologic survival in pediatric patients with HS, Guo and colleagues used Kaplan-Meier survival curves to calculate biologic survival at 12 and 24 months following biologic initiation and Cox proportional hazards regression to analyze potential factors associated with biologic survival. The study population included 49 pediatric patients in the adalimumab cohort and 11 in the infliximab cohort.
The researchers found that drug survival for adalimumab was 90.6% at 12 months (95% CI, 83.0%-98.8%) and 78.3% at 24 months (95% CI, 67.7%-90.6%), while drug survival for infliximab was 54.5% at 12 months (95% CI, 31.8%-93.6%) and 36.4% at 24 months, an overall difference that reached statistical significance (P = .0009). “Our data suggests that adalimumab survival is significantly higher than infliximab survival in pediatric HS patients,” Guo said.
On univariate Cox regression analysis, gluteal HS lesions were associated with shorter adalimumab survival, and obesity was associated with longer infliximab survival.
The researchers acknowledged certain limitations of their study, including the small sample size and that unadjusted Cox regression analysis did not account for baseline HS severity, biologic therapy dosing, and concomitant medication use. Also, there were patients in both cohorts who were not biologic-naive: Two in the adalimumab cohort were previously treated with infliximab, and five patients in the infliximab cohort were previously treated with adalimumab.
“We plan on conducting further analysis using adjusted Cox regression analysis to account for baseline disease severity measured by Hurley stage, BMI, medication dosing, and concomitant medication use,” Guo said.
The researchers reported having no financial disclosures.
A version of this article appeared on Medscape.com.
FROM SDPA 24
Varicella Outbreaks: 2022-2024
Practitioners providing care to children are familiar with the childhood immunization schedule and routinely administer varicella vaccine at the 12-month and 4- to 5-year visits. However, when is the last time most of us or any of the current trainees have seen a case?
Briefly, varicella is a highly contagious disease caused by varicella-zoster virus (VZV). It is characterized by a generalized pruritic erythematous rash in various stages of development beginning as macules, progressing to papules, and ultimately becoming vesicular lesions on an erythematous base (“dewdrop on a rose petal”) and resolves with crusting of the lesion (Figure 1). It has an incubation period of 10-21 days with symptoms usually developing within 14-16 days after exposure. The vesicular rash must be differentiated from enterovirus, Staphylococcus aureus, contact dermatitis, or insect bites, which initially may be difficult. Approximately 50% of children can have symptoms including fever, malaise, anorexia, headache, and occasionally, mild abdominal pain in the 24-48 hours prior to the appearance of rash. Lesions usually first appear on the scalp, face, or trunk in successive crops over several days. A person with varicella has lesions in various stages.
In a normal host, new vesicle formation usually stops within 4 days, and most lesions have fully crusted by day 6. VZV establishes latency in sensory ganglia and may reactivate years or decades later to cause herpes zoster (HZ). Most healthy children with varicella recover without sequelae so the disease is generally regarded as benign. However, varicella can lead to serious complications and deaths in healthy as well as immunocompromised persons.

Complications of Varicella: bacterial superinfection of skin lesions most often with Streptococcus pyogenes or S aureus manifested as cellulitis, myositis, or necrotizing fasciitis; neurologic complications include cerebellar ataxia and encephalitis with the latter seen most often in adults. Pneumonia occurs most often in adults, especially those infected during pregnancy. Another concern, infection during the first 20 weeks of pregnancy can lead to fetal death or severe birth defects, including limb hypoplasia, cutaneous scarring, ocular abnormalities, and central nervous system damage (congenital varicella syndrome).
The risk for development of severe disseminated disease was first noted in the 1960s as treatments for leukemia in children improved. They were surviving their cancer only to develop severe and often fatal varicella. Today it is recognized that development of disseminated disease is a risk for all infected persons with impaired T cell function, malignancies, HIV, or receiving immunosuppressive therapy.

Reye’s syndrome is rarely seen today since taking salicylates while infected with VZV was identified as a predisposing factor for development.
VZV is only found in humans and transmission is person to person or airborne. The secondary household attack rate is approximately 90%. In contrast, the secondary attack rates in classrooms may be as low as 12%-33%. Transmission rates in the tropics for unexplained reasons are also lower.
Vaccine History: Why do we rarely see this disease anymore? Varicella, a live attenuated vaccine, was developed in 1974 by Dr. Michiaki Takahashi. It remains the only vaccine directed against a herpes group virus. In 1979, the Collaborative Varicella Vaccine Study Group was established at the National Institutes of Health (NIH) and additional safety and efficacy trials were conducted in the United States initially in leukemic patients in remission and later in healthy children, which supported Takahashi’s data. Licensure of varicella vaccine was granted in 1995. That same year, due to continuing disease and societal burden, the United States was the first country to incorporate varicella into the routine childhood immunization schedule, which resulted in significant reductions in cases. To further improve control of varicella, in 2007 vaccine recommendations were revised and a routine two-dose schedule was implemented. The impact of varicella disease pre- and post-vaccine licensure is illustrated in Figure 2. Not listed, is that in the pre-vaccine era, there were approximately 44 cases of congenital varicella syndrome annually.
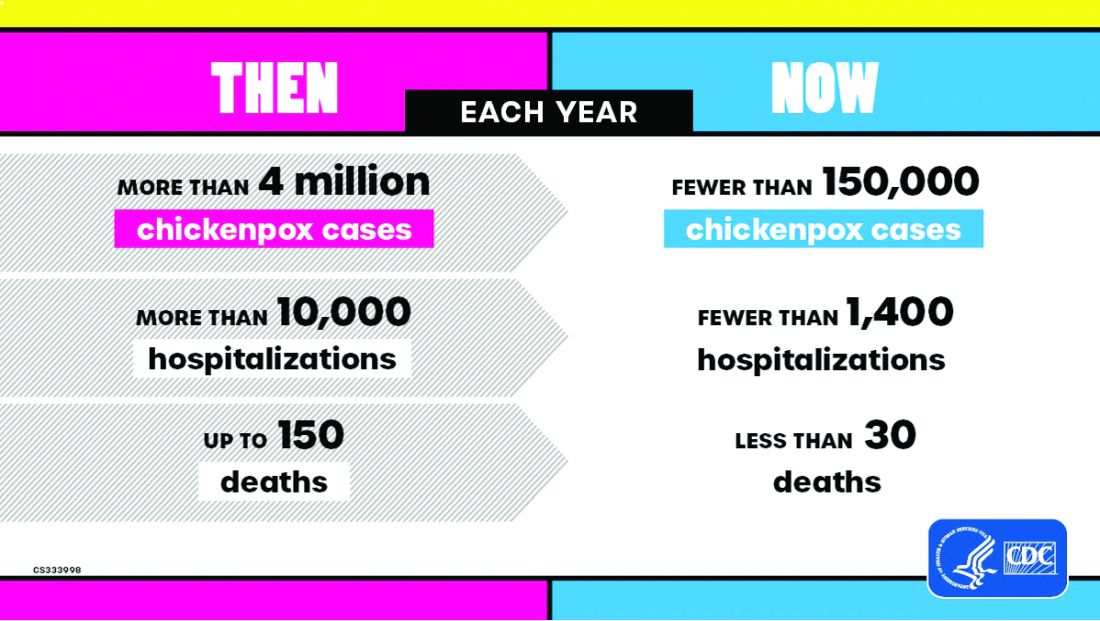
As of 2023 only 23% (45/195) of nations routinely administer this vaccine and 4% (8/195) have restricted recommendations. The remaining 73% of countries do not offer the vaccine, including all countries on the African continent, and Cuba, Guatemala, Haiti, Honduras, India, Jordan, Lebanon, Philippines, Portugal, and Venezuela to list a few.
Varicella Outbreak: In October 2022, New York City (NYC) identified a varicella outbreak primarily involving persons who recently migrated from Central and South America and lived in a shelter in NYC or residential facility (n = 105); the outbreak is ongoing. As of March 8, 2024, 873 cases (53%) were among children aged 4-18 years and 91.9% had no documentation of varicella vaccine at time of symptom onset. There were 28 hospitalizations, and no deaths reported. The most common sources of transmission were the residential facilities (41.3%) and importation or possible importation (39.4%). School transmission accounted for only 1.2% of cases.
Most migrants arrived from countries where varicella vaccination is not part of the routine childhood immunization schedule. Although most cases occurred in children, almost 30% occurred in adults. Many of the migrants arrived from tropical countries where susceptibility rates are also higher in adults. This outbreak is a reminder of the importance of limiting disease transmission by maintaining high vaccination rates. To curtail this outbreak, approximately 27,000 doses of varicella vaccine were administered to the arriving migrants. In addition, MMR, COVID-19, influenza, and all routine pediatric vaccines required for school entry were administered. Temporary closure of the residential facilities were required. Education was provided to residents regarding immunizations as well as assistance to help them establish a primary care home. Multiple agencies were mobilized to successfully coordinate these efforts.
Take Home Message
1. Each country has its own routine immunization schedule. It may not include all vaccines recommended in the US schedule. When questioned I’m frequently told that immunizations are up to date, only to review records and find they are not, especially when it is related to MMR. It is often administered at 9 months and/or MR or MM is administered depending on the country. As reported here, varicella is a routine vaccine in only 45 countries.
2.
3. Once an outbreak has been identified, the infrastructure to manage and contain it must already be established. In most instances there will be a need for a rapid and often large-scale effort involving multiple agencies including local health care providers.
4. Not all diseases are reportable. Only deaths by varicella are nationally notifiable. Otherwise, cases are reported voluntarily. As of November 2, 2024, there have been 5,157 cases of varicella reported, excluding any cases from NYC.
Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures.
Suggested Reading
CDC. Nationally Notifiable Infectious Diseases and Conditions, United States: Weekly Tables. https://wonder.cdc.gov/nndss/nndss_weekly_tables_menu.asp.
Graham KA et al. Varicella Outbreak Among Recent Arrivals to New York City, 2022-2024. MMWR Morb Mortal Wkly Rep. 2024 May 30;73(21):478-483. doi: 10.15585/mmwr.mm7321a1.
Marin M et al. Health and Economic Impact of the United States Varicella Vaccination Program, 1996-2020. J Infect Dis. 2022 Oct 21;226(Suppl 4):S463-S469. doi: 10.1093/infdis/jiac271.
Varicella-Zoster Virus Infections in Kimberkin DW et al, eds. Red Book: 2024 Report of the Committee on Infectious Diseases, 33rd Edition. American Academy of Pediatrics, 2024:938-951. https://www.aap.org/Red-Book-2024-Report-of-the-Committee-on-Infectious-Diseases-33rd-Edition-Paperback?srsltid=AfmBOoqyF60rR9ZwQ5jA8AouNhtRRTyPLnc_r7HWw7JVYV8v33Hr2vQS.
Practitioners providing care to children are familiar with the childhood immunization schedule and routinely administer varicella vaccine at the 12-month and 4- to 5-year visits. However, when is the last time most of us or any of the current trainees have seen a case?
Briefly, varicella is a highly contagious disease caused by varicella-zoster virus (VZV). It is characterized by a generalized pruritic erythematous rash in various stages of development beginning as macules, progressing to papules, and ultimately becoming vesicular lesions on an erythematous base (“dewdrop on a rose petal”) and resolves with crusting of the lesion (Figure 1). It has an incubation period of 10-21 days with symptoms usually developing within 14-16 days after exposure. The vesicular rash must be differentiated from enterovirus, Staphylococcus aureus, contact dermatitis, or insect bites, which initially may be difficult. Approximately 50% of children can have symptoms including fever, malaise, anorexia, headache, and occasionally, mild abdominal pain in the 24-48 hours prior to the appearance of rash. Lesions usually first appear on the scalp, face, or trunk in successive crops over several days. A person with varicella has lesions in various stages.
In a normal host, new vesicle formation usually stops within 4 days, and most lesions have fully crusted by day 6. VZV establishes latency in sensory ganglia and may reactivate years or decades later to cause herpes zoster (HZ). Most healthy children with varicella recover without sequelae so the disease is generally regarded as benign. However, varicella can lead to serious complications and deaths in healthy as well as immunocompromised persons.
Complications of Varicella: bacterial superinfection of skin lesions most often with Streptococcus pyogenes or S aureus manifested as cellulitis, myositis, or necrotizing fasciitis; neurologic complications include cerebellar ataxia and encephalitis with the latter seen most often in adults. Pneumonia occurs most often in adults, especially those infected during pregnancy. Another concern, infection during the first 20 weeks of pregnancy can lead to fetal death or severe birth defects, including limb hypoplasia, cutaneous scarring, ocular abnormalities, and central nervous system damage (congenital varicella syndrome).
The risk for development of severe disseminated disease was first noted in the 1960s as treatments for leukemia in children improved. They were surviving their cancer only to develop severe and often fatal varicella. Today it is recognized that development of disseminated disease is a risk for all infected persons with impaired T cell function, malignancies, HIV, or receiving immunosuppressive therapy.
Reye’s syndrome is rarely seen today since taking salicylates while infected with VZV was identified as a predisposing factor for development.
VZV is only found in humans and transmission is person to person or airborne. The secondary household attack rate is approximately 90%. In contrast, the secondary attack rates in classrooms may be as low as 12%-33%. Transmission rates in the tropics for unexplained reasons are also lower.
Vaccine History: Why do we rarely see this disease anymore? Varicella, a live attenuated vaccine, was developed in 1974 by Dr. Michiaki Takahashi. It remains the only vaccine directed against a herpes group virus. In 1979, the Collaborative Varicella Vaccine Study Group was established at the National Institutes of Health (NIH) and additional safety and efficacy trials were conducted in the United States initially in leukemic patients in remission and later in healthy children, which supported Takahashi’s data. Licensure of varicella vaccine was granted in 1995. That same year, due to continuing disease and societal burden, the United States was the first country to incorporate varicella into the routine childhood immunization schedule, which resulted in significant reductions in cases. To further improve control of varicella, in 2007 vaccine recommendations were revised and a routine two-dose schedule was implemented. The impact of varicella disease pre- and post-vaccine licensure is illustrated in Figure 2. Not listed, is that in the pre-vaccine era, there were approximately 44 cases of congenital varicella syndrome annually.
As of 2023 only 23% (45/195) of nations routinely administer this vaccine and 4% (8/195) have restricted recommendations. The remaining 73% of countries do not offer the vaccine, including all countries on the African continent, and Cuba, Guatemala, Haiti, Honduras, India, Jordan, Lebanon, Philippines, Portugal, and Venezuela to list a few.
Varicella Outbreak: In October 2022, New York City (NYC) identified a varicella outbreak primarily involving persons who recently migrated from Central and South America and lived in a shelter in NYC or residential facility (n = 105); the outbreak is ongoing. As of March 8, 2024, 873 cases (53%) were among children aged 4-18 years and 91.9% had no documentation of varicella vaccine at time of symptom onset. There were 28 hospitalizations, and no deaths reported. The most common sources of transmission were the residential facilities (41.3%) and importation or possible importation (39.4%). School transmission accounted for only 1.2% of cases.
Most migrants arrived from countries where varicella vaccination is not part of the routine childhood immunization schedule. Although most cases occurred in children, almost 30% occurred in adults. Many of the migrants arrived from tropical countries where susceptibility rates are also higher in adults. This outbreak is a reminder of the importance of limiting disease transmission by maintaining high vaccination rates. To curtail this outbreak, approximately 27,000 doses of varicella vaccine were administered to the arriving migrants. In addition, MMR, COVID-19, influenza, and all routine pediatric vaccines required for school entry were administered. Temporary closure of the residential facilities were required. Education was provided to residents regarding immunizations as well as assistance to help them establish a primary care home. Multiple agencies were mobilized to successfully coordinate these efforts.
Take Home Message
1. Each country has its own routine immunization schedule. It may not include all vaccines recommended in the US schedule. When questioned I’m frequently told that immunizations are up to date, only to review records and find they are not, especially when it is related to MMR. It is often administered at 9 months and/or MR or MM is administered depending on the country. As reported here, varicella is a routine vaccine in only 45 countries.
2.
3. Once an outbreak has been identified, the infrastructure to manage and contain it must already be established. In most instances there will be a need for a rapid and often large-scale effort involving multiple agencies including local health care providers.
4. Not all diseases are reportable. Only deaths by varicella are nationally notifiable. Otherwise, cases are reported voluntarily. As of November 2, 2024, there have been 5,157 cases of varicella reported, excluding any cases from NYC.
Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures.
Suggested Reading
CDC. Nationally Notifiable Infectious Diseases and Conditions, United States: Weekly Tables. https://wonder.cdc.gov/nndss/nndss_weekly_tables_menu.asp.
Graham KA et al. Varicella Outbreak Among Recent Arrivals to New York City, 2022-2024. MMWR Morb Mortal Wkly Rep. 2024 May 30;73(21):478-483. doi: 10.15585/mmwr.mm7321a1.
Marin M et al. Health and Economic Impact of the United States Varicella Vaccination Program, 1996-2020. J Infect Dis. 2022 Oct 21;226(Suppl 4):S463-S469. doi: 10.1093/infdis/jiac271.
Varicella-Zoster Virus Infections in Kimberkin DW et al, eds. Red Book: 2024 Report of the Committee on Infectious Diseases, 33rd Edition. American Academy of Pediatrics, 2024:938-951. https://www.aap.org/Red-Book-2024-Report-of-the-Committee-on-Infectious-Diseases-33rd-Edition-Paperback?srsltid=AfmBOoqyF60rR9ZwQ5jA8AouNhtRRTyPLnc_r7HWw7JVYV8v33Hr2vQS.
Practitioners providing care to children are familiar with the childhood immunization schedule and routinely administer varicella vaccine at the 12-month and 4- to 5-year visits. However, when is the last time most of us or any of the current trainees have seen a case?
Briefly, varicella is a highly contagious disease caused by varicella-zoster virus (VZV). It is characterized by a generalized pruritic erythematous rash in various stages of development beginning as macules, progressing to papules, and ultimately becoming vesicular lesions on an erythematous base (“dewdrop on a rose petal”) and resolves with crusting of the lesion (Figure 1). It has an incubation period of 10-21 days with symptoms usually developing within 14-16 days after exposure. The vesicular rash must be differentiated from enterovirus, Staphylococcus aureus, contact dermatitis, or insect bites, which initially may be difficult. Approximately 50% of children can have symptoms including fever, malaise, anorexia, headache, and occasionally, mild abdominal pain in the 24-48 hours prior to the appearance of rash. Lesions usually first appear on the scalp, face, or trunk in successive crops over several days. A person with varicella has lesions in various stages.
In a normal host, new vesicle formation usually stops within 4 days, and most lesions have fully crusted by day 6. VZV establishes latency in sensory ganglia and may reactivate years or decades later to cause herpes zoster (HZ). Most healthy children with varicella recover without sequelae so the disease is generally regarded as benign. However, varicella can lead to serious complications and deaths in healthy as well as immunocompromised persons.
Complications of Varicella: bacterial superinfection of skin lesions most often with Streptococcus pyogenes or S aureus manifested as cellulitis, myositis, or necrotizing fasciitis; neurologic complications include cerebellar ataxia and encephalitis with the latter seen most often in adults. Pneumonia occurs most often in adults, especially those infected during pregnancy. Another concern, infection during the first 20 weeks of pregnancy can lead to fetal death or severe birth defects, including limb hypoplasia, cutaneous scarring, ocular abnormalities, and central nervous system damage (congenital varicella syndrome).
The risk for development of severe disseminated disease was first noted in the 1960s as treatments for leukemia in children improved. They were surviving their cancer only to develop severe and often fatal varicella. Today it is recognized that development of disseminated disease is a risk for all infected persons with impaired T cell function, malignancies, HIV, or receiving immunosuppressive therapy.
Reye’s syndrome is rarely seen today since taking salicylates while infected with VZV was identified as a predisposing factor for development.
VZV is only found in humans and transmission is person to person or airborne. The secondary household attack rate is approximately 90%. In contrast, the secondary attack rates in classrooms may be as low as 12%-33%. Transmission rates in the tropics for unexplained reasons are also lower.
Vaccine History: Why do we rarely see this disease anymore? Varicella, a live attenuated vaccine, was developed in 1974 by Dr. Michiaki Takahashi. It remains the only vaccine directed against a herpes group virus. In 1979, the Collaborative Varicella Vaccine Study Group was established at the National Institutes of Health (NIH) and additional safety and efficacy trials were conducted in the United States initially in leukemic patients in remission and later in healthy children, which supported Takahashi’s data. Licensure of varicella vaccine was granted in 1995. That same year, due to continuing disease and societal burden, the United States was the first country to incorporate varicella into the routine childhood immunization schedule, which resulted in significant reductions in cases. To further improve control of varicella, in 2007 vaccine recommendations were revised and a routine two-dose schedule was implemented. The impact of varicella disease pre- and post-vaccine licensure is illustrated in Figure 2. Not listed, is that in the pre-vaccine era, there were approximately 44 cases of congenital varicella syndrome annually.
As of 2023 only 23% (45/195) of nations routinely administer this vaccine and 4% (8/195) have restricted recommendations. The remaining 73% of countries do not offer the vaccine, including all countries on the African continent, and Cuba, Guatemala, Haiti, Honduras, India, Jordan, Lebanon, Philippines, Portugal, and Venezuela to list a few.
Varicella Outbreak: In October 2022, New York City (NYC) identified a varicella outbreak primarily involving persons who recently migrated from Central and South America and lived in a shelter in NYC or residential facility (n = 105); the outbreak is ongoing. As of March 8, 2024, 873 cases (53%) were among children aged 4-18 years and 91.9% had no documentation of varicella vaccine at time of symptom onset. There were 28 hospitalizations, and no deaths reported. The most common sources of transmission were the residential facilities (41.3%) and importation or possible importation (39.4%). School transmission accounted for only 1.2% of cases.
Most migrants arrived from countries where varicella vaccination is not part of the routine childhood immunization schedule. Although most cases occurred in children, almost 30% occurred in adults. Many of the migrants arrived from tropical countries where susceptibility rates are also higher in adults. This outbreak is a reminder of the importance of limiting disease transmission by maintaining high vaccination rates. To curtail this outbreak, approximately 27,000 doses of varicella vaccine were administered to the arriving migrants. In addition, MMR, COVID-19, influenza, and all routine pediatric vaccines required for school entry were administered. Temporary closure of the residential facilities were required. Education was provided to residents regarding immunizations as well as assistance to help them establish a primary care home. Multiple agencies were mobilized to successfully coordinate these efforts.
Take Home Message
1. Each country has its own routine immunization schedule. It may not include all vaccines recommended in the US schedule. When questioned I’m frequently told that immunizations are up to date, only to review records and find they are not, especially when it is related to MMR. It is often administered at 9 months and/or MR or MM is administered depending on the country. As reported here, varicella is a routine vaccine in only 45 countries.
2.
3. Once an outbreak has been identified, the infrastructure to manage and contain it must already be established. In most instances there will be a need for a rapid and often large-scale effort involving multiple agencies including local health care providers.
4. Not all diseases are reportable. Only deaths by varicella are nationally notifiable. Otherwise, cases are reported voluntarily. As of November 2, 2024, there have been 5,157 cases of varicella reported, excluding any cases from NYC.
Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures.
Suggested Reading
CDC. Nationally Notifiable Infectious Diseases and Conditions, United States: Weekly Tables. https://wonder.cdc.gov/nndss/nndss_weekly_tables_menu.asp.
Graham KA et al. Varicella Outbreak Among Recent Arrivals to New York City, 2022-2024. MMWR Morb Mortal Wkly Rep. 2024 May 30;73(21):478-483. doi: 10.15585/mmwr.mm7321a1.
Marin M et al. Health and Economic Impact of the United States Varicella Vaccination Program, 1996-2020. J Infect Dis. 2022 Oct 21;226(Suppl 4):S463-S469. doi: 10.1093/infdis/jiac271.
Varicella-Zoster Virus Infections in Kimberkin DW et al, eds. Red Book: 2024 Report of the Committee on Infectious Diseases, 33rd Edition. American Academy of Pediatrics, 2024:938-951. https://www.aap.org/Red-Book-2024-Report-of-the-Committee-on-Infectious-Diseases-33rd-Edition-Paperback?srsltid=AfmBOoqyF60rR9ZwQ5jA8AouNhtRRTyPLnc_r7HWw7JVYV8v33Hr2vQS.
‘Being a Doctor Isn’t Healthy’: Train Your Body to Handle It
Heather K. Schopper, MD, a head and neck surgeon at Penn State Health, Hershey, Pennsylvania, wasn’t long into her career when she began feeling its physical demands. Standing for 12 hours at a time, holding awkward positions for long periods, and working with surgical tables and instruments made for doctors much taller and larger meant severe back, shoulder, and neck pain at the end of every shift.
“You just want to lie down on the floor at the end of the day,” Schopper explained. “The wear and tear of our profession is really challenging.”
Here’s the thing: At the time Schopper wasn’t particularly out of shape. She only knew she needed to build up her body for long days and a long career. What, physically, would that look like?
This was the catalyst for what she calls a “health and fitness journey” that transformed the way she practices.
“Medicine is unique in its physical demands,” said Meghan Wieser, PT, DPT, a doctor of physical therapy at Recharge Health and Fitness in Ellicott City, Maryland. Wieser frequently works with physicians and others in high-stress career environments, and she’s observed the serious toll that physically demanding medical practice can take on the body.
It’s not just about preventing acute or chronic injury, she said. It’s about performing better for longer periods. And every doctor knows the only way to build a more functional body is training.
The Fantasy of Physical Perfection vs the Reality of, Well, Reality
Jordan D. Metzl, MD, is a sports medicine physician at Hospital for Special Surgery (HSS) in New York City. He’s also a lifelong triathlete and marathon runner and has parlayed that passion into an online fitness community of more than 10,000 people called Ironstrength. Through that, Metzl has led free exercise classes in Central Park for years. He doesn’t dabble. Three times a year he leads a boot camp class of more than 1000 people on the flight deck of the USS Intrepid on the Hudson River.
“I get it, being a doctor is all about the hours,” he said. “The time sacrifices get brutal and you have to cut something out, sometimes every day. For a lot of us, that’s exercise.”
Metzl understands it so well that he recently began leading twice-monthly boot camp classes just for his HSS physician colleagues on Wednesday mornings. He says those doctors both want and need that extra boost and will be aggressive about making time for it.
“The better shape you’re in, the better job you’ll do as a physician,” he said. “You’ll feel better when the hours get long. In my own career, I have always been a better doctor when I’m active and in shape.”
Knowledge isn’t really the issue for physicians. Reality is. And reality dictates that doctors have just as much issue with achieving consistency as any patient they prescribe exercise to.
Metzl suggests total body functional training to mimic real-world movement, particularly core and lower body to keep you upright for hours at a time. How do you schedule that? He uses early mornings and weekends to train for his races and run his fitness classes, which is why his primary advice is to focus not on the activity, but on time.
“Schedule full workouts when you can and steal the rest,” he said.
Schopper agrees. “You may not be able to fit in 60 minutes of exercise every day, but 20-30 minutes of intentional movement is key,” she explained. “When you have a day off, prioritize a longer session of something you can’t fit in on workdays.”
Those shorter bouts of exercise might include “bookending” the day with 10 minutes of burpees in the morning and then 10 minutes of bodyweight strength moves like planks, push-ups, and air squats in the evening.
“Bodyweight exercises are low-hanging fruit,” said Wieser. “If you’ve got a short window, aim for something that can shoot your heart rate up quickly.”
You can also throw in “movement snacks” throughout the day — skip the elevator and run up a flight of stairs, walk around during a quick lunch break, or throw in a set of jumping jacks between patients. (Don’t worry — you won’t be dripping sweat when they walk in.)
Remember, the rehab room in the orthopedic wing may have a few dumbbells and exercise bands you can utilize when you have 5 extra minutes in your day. “Any way you can squeeze in extra movement counts,” said Wieser.
Feats of Strength? Neighborhood Sprints? It All Matters
Kissinger Goldman, DO, a Florida-based ER physician, began his dedication to exercise 17 years ago, after a high-cholesterol diagnosis. “Did I have time to exercise in medical school and residency? Yes,” Goldman admitted. “But I didn’t have the same commitment to my health until I received that number. I set about to change everything.”
Goldman follows the approach of dividing up his exercise routine into short or long sessions, depending on his schedule. “If I’m off, I’ll aim for 30 minutes of cardio and 30 minutes of strength and core work,” he explained. “When I have to work, I’ll do a compressed version of that routine as soon as I wake up, and make sure the cardio is very intense — I’ll sprint in my neighborhood, for instance.”
Matt Klein, a doctor of physical therapy and professor at George Fox University in Newberg, Oregon, who has treated many doctors, says that, when pushed for time, just 20 minutes of “heavy” strength training can deliver good results. “The definition of heavy will vary, but aim for a weight that is challenging, whether a beginner or a more experienced exerciser,” he said. “Most doctors won’t have time to go to the gym, so a simple set of dumbbells or kettlebells will work just fine. The easier it is to access, the more likely you are to do it consistently.”
Klein is a fan of strength training with good reason: “Strength is a predictor of chronic disease, so doing some high-level strength training or power training can go a long way,” he said.
The endorphin high and overall sense of improved well-being are an extra bonus. Goldman credits it with ensuring he rarely misses a workout.
Get Hardcore About Sleep
Consider the following passage: “There are clear negative effects of sleep deprivation on performance, including reaction time, accuracy, vigor, submaximal strength, and endurance. Cognitive functions such as judgment and decision-making also suffer.”
Does that sound like how you feel on suboptimal sleep? That’s from an International Journal of Sports Medicine study on the effects of sleep deprivation on athletes.
Athletes aren’t doctors — but when you consider “reaction time, accuracy, endurance, judgment, and decision-making” — doctors could certainly benefit by thinking like athletes.
Schopper is serious about sleep and sets firm boundaries.
“It’s hard,” she admitted. “We want to work, see our families, have fun. But I work hard to say, ‘I’m done,’ and go to bed.”
“Rest is crucial for this job,” agreed Goldman. “If you don’t have adequate sleep, your cortisone levels are going to go up. When you’re exhausted and you’re working, you’re likely to miss something.” Goldman is consistent with early bedtimes around 9:00 or 9:30 PM, and he allows for a bit of “wind-down” time by reading for about 20 minutes before nodding off.
Goldman also sees a link between rest and improved interactions with patients. “There’s a direct correlation between number of hours worked in a row with respect to ‘customer service’ with patients,” he said.
But don’t aim for perfection. Allow some wiggle room for the time you spend asleep, Klein recommends. “We’ve always aimed for 8 hours, but there’s evidence that even 6 or 7 hours can be enough to allow you to recover as needed,” he said. “Optimally, you want that to be uninterrupted, but if not, a 10-minute power nap can help with mental clarity.”
Keep Searching, Keep Trying, Keep Training
Schopper was never, nor has she become, a gym rat. Still, “I knew I needed to build upper body strength,” she said. That meant expanding her fitness possibilities beyond the obvious. She discovered aerial arts — intense workouts using straps and other suspension tools to work every muscle in her body while hanging from the ceiling. Increased strength was a given, but she also seriously increased her range of motion.
For Schopper, the improvements to her lifestyle have been game changers. “I still have long days, but I’m no longer sore and tired after them,” she said. “I sleep better and have more energy. I’m proud of myself for putting the effort into this.”
A journey toward health and fitness may look different for everyone, but (as doctors frequently tell their patients) it’s a path anyone can follow.
“Being a doctor is not necessarily good for your health,” said Klein. “The body can handle the job, however, if you train for it.”
A version of this article first appeared on Medscape.com.
Heather K. Schopper, MD, a head and neck surgeon at Penn State Health, Hershey, Pennsylvania, wasn’t long into her career when she began feeling its physical demands. Standing for 12 hours at a time, holding awkward positions for long periods, and working with surgical tables and instruments made for doctors much taller and larger meant severe back, shoulder, and neck pain at the end of every shift.
“You just want to lie down on the floor at the end of the day,” Schopper explained. “The wear and tear of our profession is really challenging.”
Here’s the thing: At the time Schopper wasn’t particularly out of shape. She only knew she needed to build up her body for long days and a long career. What, physically, would that look like?
This was the catalyst for what she calls a “health and fitness journey” that transformed the way she practices.
“Medicine is unique in its physical demands,” said Meghan Wieser, PT, DPT, a doctor of physical therapy at Recharge Health and Fitness in Ellicott City, Maryland. Wieser frequently works with physicians and others in high-stress career environments, and she’s observed the serious toll that physically demanding medical practice can take on the body.
It’s not just about preventing acute or chronic injury, she said. It’s about performing better for longer periods. And every doctor knows the only way to build a more functional body is training.
The Fantasy of Physical Perfection vs the Reality of, Well, Reality
Jordan D. Metzl, MD, is a sports medicine physician at Hospital for Special Surgery (HSS) in New York City. He’s also a lifelong triathlete and marathon runner and has parlayed that passion into an online fitness community of more than 10,000 people called Ironstrength. Through that, Metzl has led free exercise classes in Central Park for years. He doesn’t dabble. Three times a year he leads a boot camp class of more than 1000 people on the flight deck of the USS Intrepid on the Hudson River.
“I get it, being a doctor is all about the hours,” he said. “The time sacrifices get brutal and you have to cut something out, sometimes every day. For a lot of us, that’s exercise.”
Metzl understands it so well that he recently began leading twice-monthly boot camp classes just for his HSS physician colleagues on Wednesday mornings. He says those doctors both want and need that extra boost and will be aggressive about making time for it.
“The better shape you’re in, the better job you’ll do as a physician,” he said. “You’ll feel better when the hours get long. In my own career, I have always been a better doctor when I’m active and in shape.”
Knowledge isn’t really the issue for physicians. Reality is. And reality dictates that doctors have just as much issue with achieving consistency as any patient they prescribe exercise to.
Metzl suggests total body functional training to mimic real-world movement, particularly core and lower body to keep you upright for hours at a time. How do you schedule that? He uses early mornings and weekends to train for his races and run his fitness classes, which is why his primary advice is to focus not on the activity, but on time.
“Schedule full workouts when you can and steal the rest,” he said.
Schopper agrees. “You may not be able to fit in 60 minutes of exercise every day, but 20-30 minutes of intentional movement is key,” she explained. “When you have a day off, prioritize a longer session of something you can’t fit in on workdays.”
Those shorter bouts of exercise might include “bookending” the day with 10 minutes of burpees in the morning and then 10 minutes of bodyweight strength moves like planks, push-ups, and air squats in the evening.
“Bodyweight exercises are low-hanging fruit,” said Wieser. “If you’ve got a short window, aim for something that can shoot your heart rate up quickly.”
You can also throw in “movement snacks” throughout the day — skip the elevator and run up a flight of stairs, walk around during a quick lunch break, or throw in a set of jumping jacks between patients. (Don’t worry — you won’t be dripping sweat when they walk in.)
Remember, the rehab room in the orthopedic wing may have a few dumbbells and exercise bands you can utilize when you have 5 extra minutes in your day. “Any way you can squeeze in extra movement counts,” said Wieser.
Feats of Strength? Neighborhood Sprints? It All Matters
Kissinger Goldman, DO, a Florida-based ER physician, began his dedication to exercise 17 years ago, after a high-cholesterol diagnosis. “Did I have time to exercise in medical school and residency? Yes,” Goldman admitted. “But I didn’t have the same commitment to my health until I received that number. I set about to change everything.”
Goldman follows the approach of dividing up his exercise routine into short or long sessions, depending on his schedule. “If I’m off, I’ll aim for 30 minutes of cardio and 30 minutes of strength and core work,” he explained. “When I have to work, I’ll do a compressed version of that routine as soon as I wake up, and make sure the cardio is very intense — I’ll sprint in my neighborhood, for instance.”
Matt Klein, a doctor of physical therapy and professor at George Fox University in Newberg, Oregon, who has treated many doctors, says that, when pushed for time, just 20 minutes of “heavy” strength training can deliver good results. “The definition of heavy will vary, but aim for a weight that is challenging, whether a beginner or a more experienced exerciser,” he said. “Most doctors won’t have time to go to the gym, so a simple set of dumbbells or kettlebells will work just fine. The easier it is to access, the more likely you are to do it consistently.”
Klein is a fan of strength training with good reason: “Strength is a predictor of chronic disease, so doing some high-level strength training or power training can go a long way,” he said.
The endorphin high and overall sense of improved well-being are an extra bonus. Goldman credits it with ensuring he rarely misses a workout.
Get Hardcore About Sleep
Consider the following passage: “There are clear negative effects of sleep deprivation on performance, including reaction time, accuracy, vigor, submaximal strength, and endurance. Cognitive functions such as judgment and decision-making also suffer.”
Does that sound like how you feel on suboptimal sleep? That’s from an International Journal of Sports Medicine study on the effects of sleep deprivation on athletes.
Athletes aren’t doctors — but when you consider “reaction time, accuracy, endurance, judgment, and decision-making” — doctors could certainly benefit by thinking like athletes.
Schopper is serious about sleep and sets firm boundaries.
“It’s hard,” she admitted. “We want to work, see our families, have fun. But I work hard to say, ‘I’m done,’ and go to bed.”
“Rest is crucial for this job,” agreed Goldman. “If you don’t have adequate sleep, your cortisone levels are going to go up. When you’re exhausted and you’re working, you’re likely to miss something.” Goldman is consistent with early bedtimes around 9:00 or 9:30 PM, and he allows for a bit of “wind-down” time by reading for about 20 minutes before nodding off.
Goldman also sees a link between rest and improved interactions with patients. “There’s a direct correlation between number of hours worked in a row with respect to ‘customer service’ with patients,” he said.
But don’t aim for perfection. Allow some wiggle room for the time you spend asleep, Klein recommends. “We’ve always aimed for 8 hours, but there’s evidence that even 6 or 7 hours can be enough to allow you to recover as needed,” he said. “Optimally, you want that to be uninterrupted, but if not, a 10-minute power nap can help with mental clarity.”
Keep Searching, Keep Trying, Keep Training
Schopper was never, nor has she become, a gym rat. Still, “I knew I needed to build upper body strength,” she said. That meant expanding her fitness possibilities beyond the obvious. She discovered aerial arts — intense workouts using straps and other suspension tools to work every muscle in her body while hanging from the ceiling. Increased strength was a given, but she also seriously increased her range of motion.
For Schopper, the improvements to her lifestyle have been game changers. “I still have long days, but I’m no longer sore and tired after them,” she said. “I sleep better and have more energy. I’m proud of myself for putting the effort into this.”
A journey toward health and fitness may look different for everyone, but (as doctors frequently tell their patients) it’s a path anyone can follow.
“Being a doctor is not necessarily good for your health,” said Klein. “The body can handle the job, however, if you train for it.”
A version of this article first appeared on Medscape.com.
Heather K. Schopper, MD, a head and neck surgeon at Penn State Health, Hershey, Pennsylvania, wasn’t long into her career when she began feeling its physical demands. Standing for 12 hours at a time, holding awkward positions for long periods, and working with surgical tables and instruments made for doctors much taller and larger meant severe back, shoulder, and neck pain at the end of every shift.
“You just want to lie down on the floor at the end of the day,” Schopper explained. “The wear and tear of our profession is really challenging.”
Here’s the thing: At the time Schopper wasn’t particularly out of shape. She only knew she needed to build up her body for long days and a long career. What, physically, would that look like?
This was the catalyst for what she calls a “health and fitness journey” that transformed the way she practices.
“Medicine is unique in its physical demands,” said Meghan Wieser, PT, DPT, a doctor of physical therapy at Recharge Health and Fitness in Ellicott City, Maryland. Wieser frequently works with physicians and others in high-stress career environments, and she’s observed the serious toll that physically demanding medical practice can take on the body.
It’s not just about preventing acute or chronic injury, she said. It’s about performing better for longer periods. And every doctor knows the only way to build a more functional body is training.
The Fantasy of Physical Perfection vs the Reality of, Well, Reality
Jordan D. Metzl, MD, is a sports medicine physician at Hospital for Special Surgery (HSS) in New York City. He’s also a lifelong triathlete and marathon runner and has parlayed that passion into an online fitness community of more than 10,000 people called Ironstrength. Through that, Metzl has led free exercise classes in Central Park for years. He doesn’t dabble. Three times a year he leads a boot camp class of more than 1000 people on the flight deck of the USS Intrepid on the Hudson River.
“I get it, being a doctor is all about the hours,” he said. “The time sacrifices get brutal and you have to cut something out, sometimes every day. For a lot of us, that’s exercise.”
Metzl understands it so well that he recently began leading twice-monthly boot camp classes just for his HSS physician colleagues on Wednesday mornings. He says those doctors both want and need that extra boost and will be aggressive about making time for it.
“The better shape you’re in, the better job you’ll do as a physician,” he said. “You’ll feel better when the hours get long. In my own career, I have always been a better doctor when I’m active and in shape.”
Knowledge isn’t really the issue for physicians. Reality is. And reality dictates that doctors have just as much issue with achieving consistency as any patient they prescribe exercise to.
Metzl suggests total body functional training to mimic real-world movement, particularly core and lower body to keep you upright for hours at a time. How do you schedule that? He uses early mornings and weekends to train for his races and run his fitness classes, which is why his primary advice is to focus not on the activity, but on time.
“Schedule full workouts when you can and steal the rest,” he said.
Schopper agrees. “You may not be able to fit in 60 minutes of exercise every day, but 20-30 minutes of intentional movement is key,” she explained. “When you have a day off, prioritize a longer session of something you can’t fit in on workdays.”
Those shorter bouts of exercise might include “bookending” the day with 10 minutes of burpees in the morning and then 10 minutes of bodyweight strength moves like planks, push-ups, and air squats in the evening.
“Bodyweight exercises are low-hanging fruit,” said Wieser. “If you’ve got a short window, aim for something that can shoot your heart rate up quickly.”
You can also throw in “movement snacks” throughout the day — skip the elevator and run up a flight of stairs, walk around during a quick lunch break, or throw in a set of jumping jacks between patients. (Don’t worry — you won’t be dripping sweat when they walk in.)
Remember, the rehab room in the orthopedic wing may have a few dumbbells and exercise bands you can utilize when you have 5 extra minutes in your day. “Any way you can squeeze in extra movement counts,” said Wieser.
Feats of Strength? Neighborhood Sprints? It All Matters
Kissinger Goldman, DO, a Florida-based ER physician, began his dedication to exercise 17 years ago, after a high-cholesterol diagnosis. “Did I have time to exercise in medical school and residency? Yes,” Goldman admitted. “But I didn’t have the same commitment to my health until I received that number. I set about to change everything.”
Goldman follows the approach of dividing up his exercise routine into short or long sessions, depending on his schedule. “If I’m off, I’ll aim for 30 minutes of cardio and 30 minutes of strength and core work,” he explained. “When I have to work, I’ll do a compressed version of that routine as soon as I wake up, and make sure the cardio is very intense — I’ll sprint in my neighborhood, for instance.”
Matt Klein, a doctor of physical therapy and professor at George Fox University in Newberg, Oregon, who has treated many doctors, says that, when pushed for time, just 20 minutes of “heavy” strength training can deliver good results. “The definition of heavy will vary, but aim for a weight that is challenging, whether a beginner or a more experienced exerciser,” he said. “Most doctors won’t have time to go to the gym, so a simple set of dumbbells or kettlebells will work just fine. The easier it is to access, the more likely you are to do it consistently.”
Klein is a fan of strength training with good reason: “Strength is a predictor of chronic disease, so doing some high-level strength training or power training can go a long way,” he said.
The endorphin high and overall sense of improved well-being are an extra bonus. Goldman credits it with ensuring he rarely misses a workout.
Get Hardcore About Sleep
Consider the following passage: “There are clear negative effects of sleep deprivation on performance, including reaction time, accuracy, vigor, submaximal strength, and endurance. Cognitive functions such as judgment and decision-making also suffer.”
Does that sound like how you feel on suboptimal sleep? That’s from an International Journal of Sports Medicine study on the effects of sleep deprivation on athletes.
Athletes aren’t doctors — but when you consider “reaction time, accuracy, endurance, judgment, and decision-making” — doctors could certainly benefit by thinking like athletes.
Schopper is serious about sleep and sets firm boundaries.
“It’s hard,” she admitted. “We want to work, see our families, have fun. But I work hard to say, ‘I’m done,’ and go to bed.”
“Rest is crucial for this job,” agreed Goldman. “If you don’t have adequate sleep, your cortisone levels are going to go up. When you’re exhausted and you’re working, you’re likely to miss something.” Goldman is consistent with early bedtimes around 9:00 or 9:30 PM, and he allows for a bit of “wind-down” time by reading for about 20 minutes before nodding off.
Goldman also sees a link between rest and improved interactions with patients. “There’s a direct correlation between number of hours worked in a row with respect to ‘customer service’ with patients,” he said.
But don’t aim for perfection. Allow some wiggle room for the time you spend asleep, Klein recommends. “We’ve always aimed for 8 hours, but there’s evidence that even 6 or 7 hours can be enough to allow you to recover as needed,” he said. “Optimally, you want that to be uninterrupted, but if not, a 10-minute power nap can help with mental clarity.”
Keep Searching, Keep Trying, Keep Training
Schopper was never, nor has she become, a gym rat. Still, “I knew I needed to build upper body strength,” she said. That meant expanding her fitness possibilities beyond the obvious. She discovered aerial arts — intense workouts using straps and other suspension tools to work every muscle in her body while hanging from the ceiling. Increased strength was a given, but she also seriously increased her range of motion.
For Schopper, the improvements to her lifestyle have been game changers. “I still have long days, but I’m no longer sore and tired after them,” she said. “I sleep better and have more energy. I’m proud of myself for putting the effort into this.”
A journey toward health and fitness may look different for everyone, but (as doctors frequently tell their patients) it’s a path anyone can follow.
“Being a doctor is not necessarily good for your health,” said Klein. “The body can handle the job, however, if you train for it.”
A version of this article first appeared on Medscape.com.