User login
VAM ’17 Will Be a ‘Spectacular Meeting’
Participants at the Vascular Annual Meeting (VAM) have lots more to look forward to than sunny skies, beaches and palm trees. A number of new program features are planned to add interest and value to the meeting, said Dr. Ron Dalman.
Dr. Dalman chairs the SVS Program Committee, which develops programming and content for VAM, the premiere meeting for vascular specialists.
The 2017 meeting will be May 31-June 3 in beautiful San Diego, with plenaries and exhibits set for June 1-3.
Changes for 2017 include:
• More and potentially longer sessions with collaborative specialty societies, such as the American Venous Forum, the Society for Vascular Ultrasound and the Society of Thoracic Surgeons. “These sessions provide a multi-disciplinary perspective on our common problems and showcase the SVS’ leadership role in vascular health and disease management,” said Dr. Dalman. Members provided positive feedback on last year’s partnership sessions, so this year, these program features will be significantly expanded.
• An educational review course highlighting some of the more frequently missed questions from the latest version of the Vascular Education Self-Assessment Program (VESAP3).
• Guideline summaries, organized by the SVS Document Oversight Committee and presented by the authorship group for each, on critical topics such as abdominal aortic aneurysms, aortic dissection, venous disease and more. These summaries will be incorporated into post-graduate programming. “It makes sense to cover current practice guidelines and consensus documents, as several high-profile efforts are being updated this year,” said Dr. Dalman. “We can give attendees an executive summary of current guidelines by their respective authors, and attendees will come away with unique insights into why the most impactful and significant changes were included in each respective document.”
• Sessions of potential interest to surgeons in community practice environments, marked in the schedule as such by the SVS Community Practice Committee.
“These improvements will increase the value of the Annual Meeting for all attendees,” Dr. Dalman said. “We’re emphasizing interactive education, not simply passive learning. It’s going to be very exciting – and different in both style and substance.”
A Californian himself, Dr. Dalman also is looking forward to showing off his state. “San Diego is a wonderful place to vacation and the meeting venue provides convenient access to the Gaslamp District, the waterfront and the world-famous beaches,” he said.
“We encourage our members to bring their families to San Diego and make a vacation out of it.”
With the programming additions, increased opportunities for participation, the educational activities planned plus the perfect location, he added, “This is going to be a spectacular meeting.”
Participants at the Vascular Annual Meeting (VAM) have lots more to look forward to than sunny skies, beaches and palm trees. A number of new program features are planned to add interest and value to the meeting, said Dr. Ron Dalman.
Dr. Dalman chairs the SVS Program Committee, which develops programming and content for VAM, the premiere meeting for vascular specialists.
The 2017 meeting will be May 31-June 3 in beautiful San Diego, with plenaries and exhibits set for June 1-3.
Changes for 2017 include:
• More and potentially longer sessions with collaborative specialty societies, such as the American Venous Forum, the Society for Vascular Ultrasound and the Society of Thoracic Surgeons. “These sessions provide a multi-disciplinary perspective on our common problems and showcase the SVS’ leadership role in vascular health and disease management,” said Dr. Dalman. Members provided positive feedback on last year’s partnership sessions, so this year, these program features will be significantly expanded.
• An educational review course highlighting some of the more frequently missed questions from the latest version of the Vascular Education Self-Assessment Program (VESAP3).
• Guideline summaries, organized by the SVS Document Oversight Committee and presented by the authorship group for each, on critical topics such as abdominal aortic aneurysms, aortic dissection, venous disease and more. These summaries will be incorporated into post-graduate programming. “It makes sense to cover current practice guidelines and consensus documents, as several high-profile efforts are being updated this year,” said Dr. Dalman. “We can give attendees an executive summary of current guidelines by their respective authors, and attendees will come away with unique insights into why the most impactful and significant changes were included in each respective document.”
• Sessions of potential interest to surgeons in community practice environments, marked in the schedule as such by the SVS Community Practice Committee.
“These improvements will increase the value of the Annual Meeting for all attendees,” Dr. Dalman said. “We’re emphasizing interactive education, not simply passive learning. It’s going to be very exciting – and different in both style and substance.”
A Californian himself, Dr. Dalman also is looking forward to showing off his state. “San Diego is a wonderful place to vacation and the meeting venue provides convenient access to the Gaslamp District, the waterfront and the world-famous beaches,” he said.
“We encourage our members to bring their families to San Diego and make a vacation out of it.”
With the programming additions, increased opportunities for participation, the educational activities planned plus the perfect location, he added, “This is going to be a spectacular meeting.”
Participants at the Vascular Annual Meeting (VAM) have lots more to look forward to than sunny skies, beaches and palm trees. A number of new program features are planned to add interest and value to the meeting, said Dr. Ron Dalman.
Dr. Dalman chairs the SVS Program Committee, which develops programming and content for VAM, the premiere meeting for vascular specialists.
The 2017 meeting will be May 31-June 3 in beautiful San Diego, with plenaries and exhibits set for June 1-3.
Changes for 2017 include:
• More and potentially longer sessions with collaborative specialty societies, such as the American Venous Forum, the Society for Vascular Ultrasound and the Society of Thoracic Surgeons. “These sessions provide a multi-disciplinary perspective on our common problems and showcase the SVS’ leadership role in vascular health and disease management,” said Dr. Dalman. Members provided positive feedback on last year’s partnership sessions, so this year, these program features will be significantly expanded.
• An educational review course highlighting some of the more frequently missed questions from the latest version of the Vascular Education Self-Assessment Program (VESAP3).
• Guideline summaries, organized by the SVS Document Oversight Committee and presented by the authorship group for each, on critical topics such as abdominal aortic aneurysms, aortic dissection, venous disease and more. These summaries will be incorporated into post-graduate programming. “It makes sense to cover current practice guidelines and consensus documents, as several high-profile efforts are being updated this year,” said Dr. Dalman. “We can give attendees an executive summary of current guidelines by their respective authors, and attendees will come away with unique insights into why the most impactful and significant changes were included in each respective document.”
• Sessions of potential interest to surgeons in community practice environments, marked in the schedule as such by the SVS Community Practice Committee.
“These improvements will increase the value of the Annual Meeting for all attendees,” Dr. Dalman said. “We’re emphasizing interactive education, not simply passive learning. It’s going to be very exciting – and different in both style and substance.”
A Californian himself, Dr. Dalman also is looking forward to showing off his state. “San Diego is a wonderful place to vacation and the meeting venue provides convenient access to the Gaslamp District, the waterfront and the world-famous beaches,” he said.
“We encourage our members to bring their families to San Diego and make a vacation out of it.”
With the programming additions, increased opportunities for participation, the educational activities planned plus the perfect location, he added, “This is going to be a spectacular meeting.”
Ready for post-acute care?
The definition of “hospitalist,” according to the SHM website, is a clinician “dedicated to delivering comprehensive medical care to hospitalized patients.” For years, the hospital setting was the specialties’ identifier. But as hospitalists’ scope has expanded, and post-acute care (PAC) in the United States has grown, more hospitalists are extending their roles into this space.
PAC today is more than the traditional nursing home, according to Manoj K. Mathew, MD, SFHM, national medical director of Agilon Health in Los Angeles.

Many of those expanded settings Dr. Mathew describes emerged as a result of the Affordable Care Act. Since its enactment in 2010, the ACA has heightened providers’ focus on the “Triple Aim” of improving the patient experience (including quality and satisfaction), improving the health of populations, and reducing the per capita cost of healthcare.1 Vishal Kuchaculla, MD, New England regional post-acute medical director of Knoxville,Tenn.-based TeamHealth, says new service lines also developed as Medicare clamped down on long-term inpatient hospital stays by giving financial impetus to discharge patients as soon as possible.
“Over the last few years, there’s been a major shift from fee-for-service to risk-based payment models,” Dr. Kuchaculla says. “The government’s financial incentives are driving outcomes to improve performance initiatives.”

“Today, LTACHs can be used as substitutes for short-term acute care,” says Sean R. Muldoon, MD, MPH, FCCP, chief medical officer of Kindred Healthcare in Louisville, Ky., and former chair of SHM’s Post-Acute Care Committee. “This means that a patient can be directly admitted from their home to an LTACH. In fact, many hospice and home-care patients are referred from physicians’ offices without a preceding hospitalization.”
Hospitalists can fill a need
More hospitalists are working in PACs for a number of reasons. Dr. Mathew says PAC facilities and services have “typically lacked the clinical structure and processes to obtain the results that patients and payors expect.
“These deficits needed to be quickly remedied as patients discharged from hospitals have increased acuity and higher disease burdens,” he adds. “Hospitalists were the natural choice to fill roles requiring their expertise and experience.”
Dr. Muldoon considers the expanded scope of practice into PACs an additional layer to hospital medicine’s value proposition to the healthcare system.
“As experts in the management of inpatient populations, it’s natural for hospitalists to expand to other facilities with inpatient-like populations,” he says, noting SNFs are the most popular choice, with IRFs and LTACHs also being common places to work. Few hospitalists work in home care or hospice.
PAC settings are designed to help patients who are transitioning from an inpatient setting back to their home or other setting.
“Many patients go home after a SNF stay, while others will move to a nursing home or other longer-term care setting for the first time,” says Tiffany Radcliff, PhD, a health economist in the department of health policy and management at Texas A&M University School of Public Health in College Station. “With this in mind, hospitalists working in PAC have the opportunity to address each patient’s ongoing care needs and prepare them for their next setting. Hospitalists can manage medication or other care regimen changes that resulted from an inpatient stay, reinforce discharge instructions to the patient and their caregivers, and identify any other issues with continuing care that need to be addressed before discharge to the next care setting.”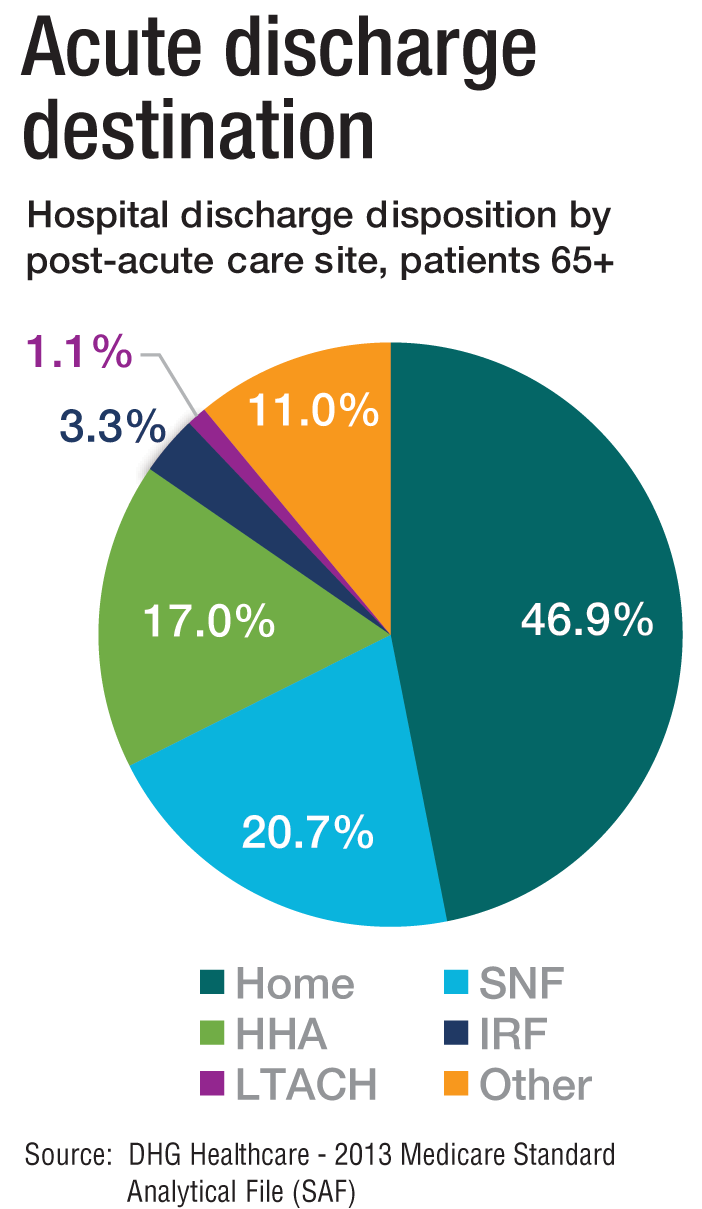
Transitioning Care
Even if a hospitalist is not employed at a PAC, it’s important that they know something about them.
“As patients are moved downstream earlier, hospitalists are being asked to help make a judgment regarding when and where an inpatient is transitioned,” Dr. Muldoon says. As organizations move toward becoming fully risk capable, it is necessary to develop referral networks of high-quality PAC providers to achieve the best clinical outcomes, reduce readmissions, and lower costs.2“Therefore, hospitalists should have a working knowledge of the different sites of service as well as some opinion on the suitability of available options in their community,” Dr. Muldoon says. “The hospitalist can also help to educate the hospitalized patient on what to expect at a PAC.”
If a patient is inappropriately prepared for the PAC setting, it could lead to incomplete management of their condition, which ultimately could lead to readmission.
“When hospitalists know how care is provided in a PAC setting, they are better able to ensure a smoother transition of care between settings,” says Tochi Iroku-Malize, MD, MPH, MBA, FAAFP, SFHM, chair of family medicine at Northwell Health in Long Island, N.Y. “This will ultimately prevent unnecessary readmissions.”
Further, the quality metrics that hospitals and thereby hospitalists are judged by no longer end at the hospital’s exit.
“The ownership of acute-care outcomes requires extending the accountability to outside of the institution’s four walls,” Dr. Mathew says. “The inpatient team needs to place great importance on the transition of care and the subsequent quality of that care when the patient is discharged.”
Robert W. Harrington Jr., MD, SFHM, chief medical officer of Plano, Texas–based Reliant Post-Acute Care Solutions and former SHM president, says the health system landscapes are pushing HM beyond the hospitals’ walls.

How PAC settings differ from hospitals
Practicing in PAC has some important nuances that hospitalists from short-term acute care need to get accustomed to, Dr. Muldoon says. Primarily, the diagnostic capabilities are much more limited, as is the presence of high-level staffing. Further, patients are less resilient to medication changes and interventions, so changes need to be done gradually.
“Hospitalists who try to practice acute-care medicine in a PAC setting may become frustrated by the length of time it takes to do a work-up, get a consultation, and respond to a patient’s change of condition,” Dr. Muldoon says. “Nonetheless, hospitalists can overcome this once recognizing this mind shift.”
According to Dr. Harrington, another challenge hospitalists may face is the inability of the hospital’s and PAC facility’s IT platforms to exchange electronic information.
“The major vendors on both sides need to figure out an interoperability strategy,” he says. “Currently, it often takes 1-3 days to receive a new patient’s discharge summary. The summary may consist of a stack of paper that takes significant time to sort through and requires the PAC facility to perform duplicate data entry. It’s a very highly inefficient process that opens up the doors to mistakes and errors of omission and commission that can result in bad patient outcomes.”
Arif Nazir, MD, CMD, FACP, AGSF, chief medical officer of Signature HealthCARE and president of SHC Medical Partners, both in Louisville, Ky., cites additional reasons the lack of seamless communication between a hospital and PAC facility is problematic. “I see physicians order laboratory tests and investigations that were already done in the hospital because they didn’t know they were already performed or never received the results,” he says. “Similarly, I see patients continue to take medications prescribed in the hospital long term even though they were only supposed to take them short term. I’ve also seen patients come to a PAC setting from a hospital without any formal understanding of their rehabilitative period and expectations for recovery.”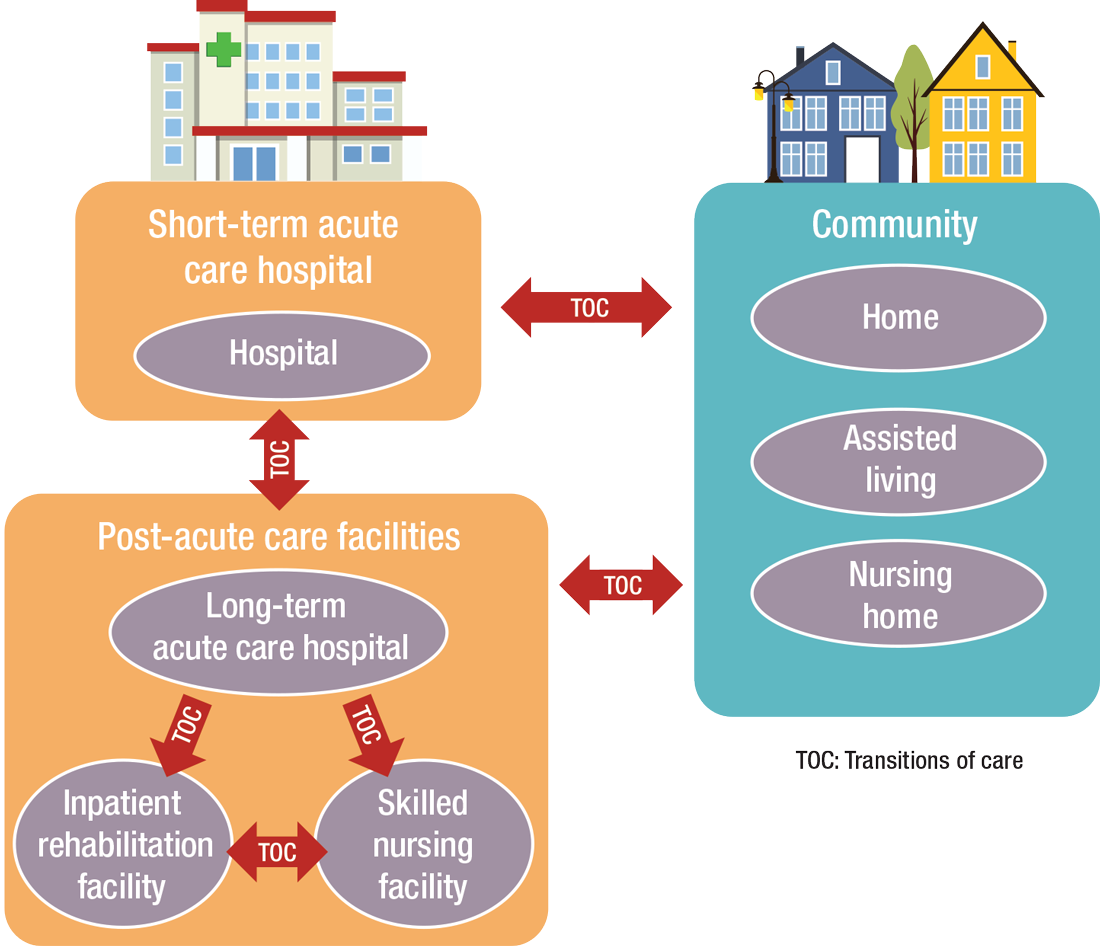
What’s ahead?
Looking to the future, Surafel Tsega, MD, clinical instructor at Mount Sinai Hospital in New York, says he thinks there will be a move toward greater collaboration among inpatient and PAC facilities, particularly in the discharge process, given that hospitals have an added incentive to ensure safe transitions because reimbursement from the Centers for Medicare & Medicaid Services is tied to readmissions and there are penalties for readmission. This involves more comprehensive planning regarding “warm handoffs” (e.g., real-time discussions with PAC providers about a patient’s hospital course and plan of care upon discharge), transferring of information, and so forth.
And while it can still be challenging to identify high-risk patients or determine the intensity and duration of their care, Dr. Mathew says risk-stratification tools and care pathways are continually being refined to maximize value with the limited resources available. In addition, with an increased emphasis on employing a team approach to care, there will be better integration of non-medical services to address the social determinants of health, which play significant roles in overall health and healing.
“Working with community-based organizations for this purpose will be a valuable tool for any of the population health–based initiatives,” he says.
Dr. Muldoon says he believes healthcare reform will increasingly view an inpatient admission as something to be avoided.
“If hospitalization can’t be avoided, then it should be shortened as much as possible,” he says. “This will shift inpatient care into LTACHs, SNFs, and IRFs. Hospitalists would be wise to follow patients into those settings as traditional inpatient census is reduced. This will take a few years, so hospitalists should start now in preparing for that downstream transition of individuals who were previously inpatients.”
The cost of care, and other PAC facts and figures
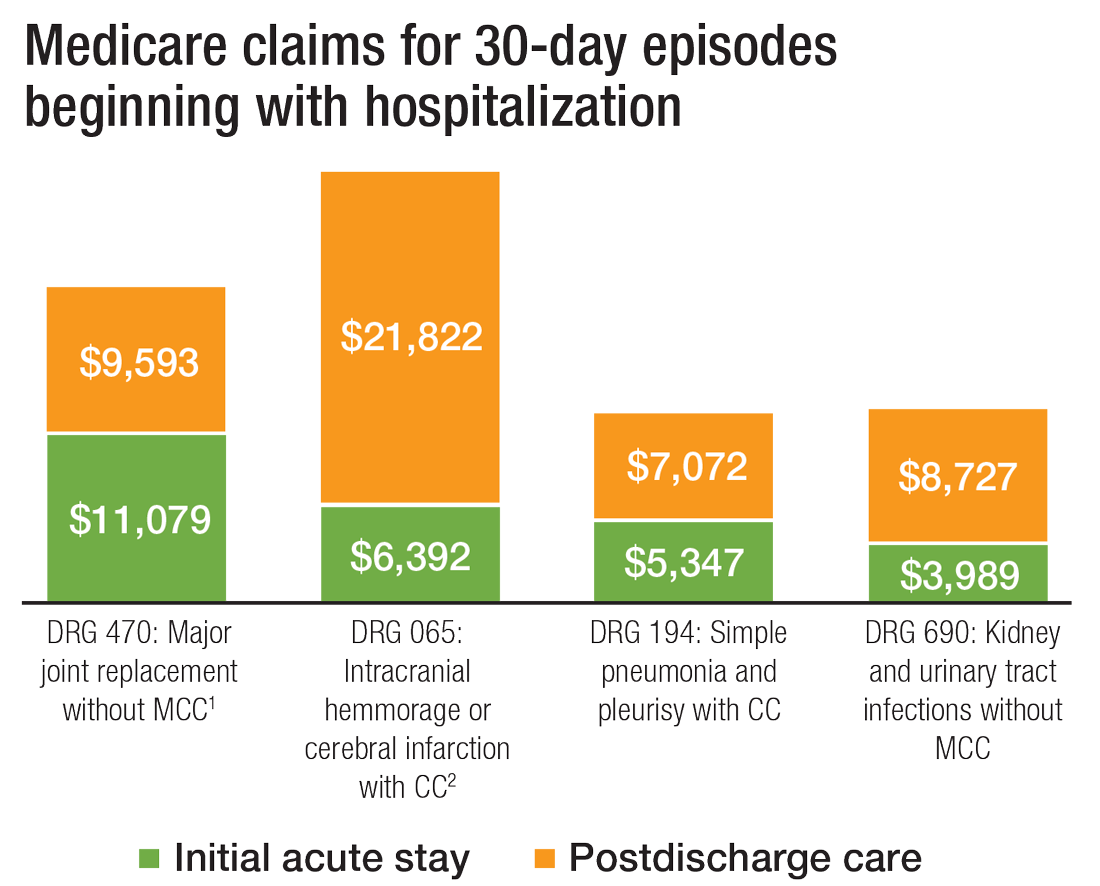
The amount of money that Medicare spends on post-acute care (PAC) has been increasing. In 2012, 12.6% of Medicare beneficiaries used some form of PAC, costing $62 billion.2 That amounts to the Centers for Medicare & Medicaid Services spending close to 25% of Medicare beneficiary expenses on PAC, a 133% increase from 2001 to 2012. Among the different types, $30.4 billion was spent on skilled nursing facilities (SNFs), $18.6 billion on home health, and $13.1 billion on long-term acute care (LTAC) and acute-care rehabilitation.2
It’s also been reported that after short-term acute-care hospitalization, about one in five Medicare beneficiaries requires continued specialized treatment in one of the three typical Medicare PAC settings: inpatient rehabilitation facilities (IRFs), LTAC hospitals, and SNFs.3
What’s more, hospital readmission nearly doubles the cost of an episode, so the financial implications for organizations operating in risk-bearing arrangements are significant. In 2013, 2,213 hospitals were charged $280 million in readmission penalties.2
References
1. The role of post-acute care in new care delivery models. American Hospital Association website. Available at: http://www.aha.org/research/reports/tw/15dec-tw-postacute.pdf. Accessed Nov. 7, 2016.
2. Post-acute care integration: Today and in the future. DHG Healthcare website. Available at: http://www2.dhgllp.com/res_pubs/HCG-Post-Acute-Care-Integration.pdf. Accessed Nov. 7, 2016.
3. Overview: Post-acute care transitions toolkit. Society for Hospital Medicine website. Available at: http://www.hospitalmedicine.org/Web/Quality___Innovation/Implementation_Toolkit/pact/Overview_PACT.aspx?hkey=dea3da3c-8620-46db-a00f-89f07f021958. Accessed Nov. 10, 2016.
The definition of “hospitalist,” according to the SHM website, is a clinician “dedicated to delivering comprehensive medical care to hospitalized patients.” For years, the hospital setting was the specialties’ identifier. But as hospitalists’ scope has expanded, and post-acute care (PAC) in the United States has grown, more hospitalists are extending their roles into this space.
PAC today is more than the traditional nursing home, according to Manoj K. Mathew, MD, SFHM, national medical director of Agilon Health in Los Angeles.
Many of those expanded settings Dr. Mathew describes emerged as a result of the Affordable Care Act. Since its enactment in 2010, the ACA has heightened providers’ focus on the “Triple Aim” of improving the patient experience (including quality and satisfaction), improving the health of populations, and reducing the per capita cost of healthcare.1 Vishal Kuchaculla, MD, New England regional post-acute medical director of Knoxville,Tenn.-based TeamHealth, says new service lines also developed as Medicare clamped down on long-term inpatient hospital stays by giving financial impetus to discharge patients as soon as possible.
“Over the last few years, there’s been a major shift from fee-for-service to risk-based payment models,” Dr. Kuchaculla says. “The government’s financial incentives are driving outcomes to improve performance initiatives.”
“Today, LTACHs can be used as substitutes for short-term acute care,” says Sean R. Muldoon, MD, MPH, FCCP, chief medical officer of Kindred Healthcare in Louisville, Ky., and former chair of SHM’s Post-Acute Care Committee. “This means that a patient can be directly admitted from their home to an LTACH. In fact, many hospice and home-care patients are referred from physicians’ offices without a preceding hospitalization.”
Hospitalists can fill a need
More hospitalists are working in PACs for a number of reasons. Dr. Mathew says PAC facilities and services have “typically lacked the clinical structure and processes to obtain the results that patients and payors expect.
“These deficits needed to be quickly remedied as patients discharged from hospitals have increased acuity and higher disease burdens,” he adds. “Hospitalists were the natural choice to fill roles requiring their expertise and experience.”
Dr. Muldoon considers the expanded scope of practice into PACs an additional layer to hospital medicine’s value proposition to the healthcare system.
“As experts in the management of inpatient populations, it’s natural for hospitalists to expand to other facilities with inpatient-like populations,” he says, noting SNFs are the most popular choice, with IRFs and LTACHs also being common places to work. Few hospitalists work in home care or hospice.
PAC settings are designed to help patients who are transitioning from an inpatient setting back to their home or other setting.
“Many patients go home after a SNF stay, while others will move to a nursing home or other longer-term care setting for the first time,” says Tiffany Radcliff, PhD, a health economist in the department of health policy and management at Texas A&M University School of Public Health in College Station. “With this in mind, hospitalists working in PAC have the opportunity to address each patient’s ongoing care needs and prepare them for their next setting. Hospitalists can manage medication or other care regimen changes that resulted from an inpatient stay, reinforce discharge instructions to the patient and their caregivers, and identify any other issues with continuing care that need to be addressed before discharge to the next care setting.”
Transitioning Care
Even if a hospitalist is not employed at a PAC, it’s important that they know something about them.
“As patients are moved downstream earlier, hospitalists are being asked to help make a judgment regarding when and where an inpatient is transitioned,” Dr. Muldoon says. As organizations move toward becoming fully risk capable, it is necessary to develop referral networks of high-quality PAC providers to achieve the best clinical outcomes, reduce readmissions, and lower costs.2“Therefore, hospitalists should have a working knowledge of the different sites of service as well as some opinion on the suitability of available options in their community,” Dr. Muldoon says. “The hospitalist can also help to educate the hospitalized patient on what to expect at a PAC.”
If a patient is inappropriately prepared for the PAC setting, it could lead to incomplete management of their condition, which ultimately could lead to readmission.
“When hospitalists know how care is provided in a PAC setting, they are better able to ensure a smoother transition of care between settings,” says Tochi Iroku-Malize, MD, MPH, MBA, FAAFP, SFHM, chair of family medicine at Northwell Health in Long Island, N.Y. “This will ultimately prevent unnecessary readmissions.”
Further, the quality metrics that hospitals and thereby hospitalists are judged by no longer end at the hospital’s exit.
“The ownership of acute-care outcomes requires extending the accountability to outside of the institution’s four walls,” Dr. Mathew says. “The inpatient team needs to place great importance on the transition of care and the subsequent quality of that care when the patient is discharged.”
Robert W. Harrington Jr., MD, SFHM, chief medical officer of Plano, Texas–based Reliant Post-Acute Care Solutions and former SHM president, says the health system landscapes are pushing HM beyond the hospitals’ walls.
How PAC settings differ from hospitals
Practicing in PAC has some important nuances that hospitalists from short-term acute care need to get accustomed to, Dr. Muldoon says. Primarily, the diagnostic capabilities are much more limited, as is the presence of high-level staffing. Further, patients are less resilient to medication changes and interventions, so changes need to be done gradually.
“Hospitalists who try to practice acute-care medicine in a PAC setting may become frustrated by the length of time it takes to do a work-up, get a consultation, and respond to a patient’s change of condition,” Dr. Muldoon says. “Nonetheless, hospitalists can overcome this once recognizing this mind shift.”
According to Dr. Harrington, another challenge hospitalists may face is the inability of the hospital’s and PAC facility’s IT platforms to exchange electronic information.
“The major vendors on both sides need to figure out an interoperability strategy,” he says. “Currently, it often takes 1-3 days to receive a new patient’s discharge summary. The summary may consist of a stack of paper that takes significant time to sort through and requires the PAC facility to perform duplicate data entry. It’s a very highly inefficient process that opens up the doors to mistakes and errors of omission and commission that can result in bad patient outcomes.”
Arif Nazir, MD, CMD, FACP, AGSF, chief medical officer of Signature HealthCARE and president of SHC Medical Partners, both in Louisville, Ky., cites additional reasons the lack of seamless communication between a hospital and PAC facility is problematic. “I see physicians order laboratory tests and investigations that were already done in the hospital because they didn’t know they were already performed or never received the results,” he says. “Similarly, I see patients continue to take medications prescribed in the hospital long term even though they were only supposed to take them short term. I’ve also seen patients come to a PAC setting from a hospital without any formal understanding of their rehabilitative period and expectations for recovery.”
What’s ahead?
Looking to the future, Surafel Tsega, MD, clinical instructor at Mount Sinai Hospital in New York, says he thinks there will be a move toward greater collaboration among inpatient and PAC facilities, particularly in the discharge process, given that hospitals have an added incentive to ensure safe transitions because reimbursement from the Centers for Medicare & Medicaid Services is tied to readmissions and there are penalties for readmission. This involves more comprehensive planning regarding “warm handoffs” (e.g., real-time discussions with PAC providers about a patient’s hospital course and plan of care upon discharge), transferring of information, and so forth.
And while it can still be challenging to identify high-risk patients or determine the intensity and duration of their care, Dr. Mathew says risk-stratification tools and care pathways are continually being refined to maximize value with the limited resources available. In addition, with an increased emphasis on employing a team approach to care, there will be better integration of non-medical services to address the social determinants of health, which play significant roles in overall health and healing.
“Working with community-based organizations for this purpose will be a valuable tool for any of the population health–based initiatives,” he says.
Dr. Muldoon says he believes healthcare reform will increasingly view an inpatient admission as something to be avoided.
“If hospitalization can’t be avoided, then it should be shortened as much as possible,” he says. “This will shift inpatient care into LTACHs, SNFs, and IRFs. Hospitalists would be wise to follow patients into those settings as traditional inpatient census is reduced. This will take a few years, so hospitalists should start now in preparing for that downstream transition of individuals who were previously inpatients.”
The cost of care, and other PAC facts and figures
The amount of money that Medicare spends on post-acute care (PAC) has been increasing. In 2012, 12.6% of Medicare beneficiaries used some form of PAC, costing $62 billion.2 That amounts to the Centers for Medicare & Medicaid Services spending close to 25% of Medicare beneficiary expenses on PAC, a 133% increase from 2001 to 2012. Among the different types, $30.4 billion was spent on skilled nursing facilities (SNFs), $18.6 billion on home health, and $13.1 billion on long-term acute care (LTAC) and acute-care rehabilitation.2
It’s also been reported that after short-term acute-care hospitalization, about one in five Medicare beneficiaries requires continued specialized treatment in one of the three typical Medicare PAC settings: inpatient rehabilitation facilities (IRFs), LTAC hospitals, and SNFs.3
What’s more, hospital readmission nearly doubles the cost of an episode, so the financial implications for organizations operating in risk-bearing arrangements are significant. In 2013, 2,213 hospitals were charged $280 million in readmission penalties.2
References
1. The role of post-acute care in new care delivery models. American Hospital Association website. Available at: http://www.aha.org/research/reports/tw/15dec-tw-postacute.pdf. Accessed Nov. 7, 2016.
2. Post-acute care integration: Today and in the future. DHG Healthcare website. Available at: http://www2.dhgllp.com/res_pubs/HCG-Post-Acute-Care-Integration.pdf. Accessed Nov. 7, 2016.
3. Overview: Post-acute care transitions toolkit. Society for Hospital Medicine website. Available at: http://www.hospitalmedicine.org/Web/Quality___Innovation/Implementation_Toolkit/pact/Overview_PACT.aspx?hkey=dea3da3c-8620-46db-a00f-89f07f021958. Accessed Nov. 10, 2016.
The definition of “hospitalist,” according to the SHM website, is a clinician “dedicated to delivering comprehensive medical care to hospitalized patients.” For years, the hospital setting was the specialties’ identifier. But as hospitalists’ scope has expanded, and post-acute care (PAC) in the United States has grown, more hospitalists are extending their roles into this space.
PAC today is more than the traditional nursing home, according to Manoj K. Mathew, MD, SFHM, national medical director of Agilon Health in Los Angeles.
Many of those expanded settings Dr. Mathew describes emerged as a result of the Affordable Care Act. Since its enactment in 2010, the ACA has heightened providers’ focus on the “Triple Aim” of improving the patient experience (including quality and satisfaction), improving the health of populations, and reducing the per capita cost of healthcare.1 Vishal Kuchaculla, MD, New England regional post-acute medical director of Knoxville,Tenn.-based TeamHealth, says new service lines also developed as Medicare clamped down on long-term inpatient hospital stays by giving financial impetus to discharge patients as soon as possible.
“Over the last few years, there’s been a major shift from fee-for-service to risk-based payment models,” Dr. Kuchaculla says. “The government’s financial incentives are driving outcomes to improve performance initiatives.”
“Today, LTACHs can be used as substitutes for short-term acute care,” says Sean R. Muldoon, MD, MPH, FCCP, chief medical officer of Kindred Healthcare in Louisville, Ky., and former chair of SHM’s Post-Acute Care Committee. “This means that a patient can be directly admitted from their home to an LTACH. In fact, many hospice and home-care patients are referred from physicians’ offices without a preceding hospitalization.”
Hospitalists can fill a need
More hospitalists are working in PACs for a number of reasons. Dr. Mathew says PAC facilities and services have “typically lacked the clinical structure and processes to obtain the results that patients and payors expect.
“These deficits needed to be quickly remedied as patients discharged from hospitals have increased acuity and higher disease burdens,” he adds. “Hospitalists were the natural choice to fill roles requiring their expertise and experience.”
Dr. Muldoon considers the expanded scope of practice into PACs an additional layer to hospital medicine’s value proposition to the healthcare system.
“As experts in the management of inpatient populations, it’s natural for hospitalists to expand to other facilities with inpatient-like populations,” he says, noting SNFs are the most popular choice, with IRFs and LTACHs also being common places to work. Few hospitalists work in home care or hospice.
PAC settings are designed to help patients who are transitioning from an inpatient setting back to their home or other setting.
“Many patients go home after a SNF stay, while others will move to a nursing home or other longer-term care setting for the first time,” says Tiffany Radcliff, PhD, a health economist in the department of health policy and management at Texas A&M University School of Public Health in College Station. “With this in mind, hospitalists working in PAC have the opportunity to address each patient’s ongoing care needs and prepare them for their next setting. Hospitalists can manage medication or other care regimen changes that resulted from an inpatient stay, reinforce discharge instructions to the patient and their caregivers, and identify any other issues with continuing care that need to be addressed before discharge to the next care setting.”
Transitioning Care
Even if a hospitalist is not employed at a PAC, it’s important that they know something about them.
“As patients are moved downstream earlier, hospitalists are being asked to help make a judgment regarding when and where an inpatient is transitioned,” Dr. Muldoon says. As organizations move toward becoming fully risk capable, it is necessary to develop referral networks of high-quality PAC providers to achieve the best clinical outcomes, reduce readmissions, and lower costs.2“Therefore, hospitalists should have a working knowledge of the different sites of service as well as some opinion on the suitability of available options in their community,” Dr. Muldoon says. “The hospitalist can also help to educate the hospitalized patient on what to expect at a PAC.”
If a patient is inappropriately prepared for the PAC setting, it could lead to incomplete management of their condition, which ultimately could lead to readmission.
“When hospitalists know how care is provided in a PAC setting, they are better able to ensure a smoother transition of care between settings,” says Tochi Iroku-Malize, MD, MPH, MBA, FAAFP, SFHM, chair of family medicine at Northwell Health in Long Island, N.Y. “This will ultimately prevent unnecessary readmissions.”
Further, the quality metrics that hospitals and thereby hospitalists are judged by no longer end at the hospital’s exit.
“The ownership of acute-care outcomes requires extending the accountability to outside of the institution’s four walls,” Dr. Mathew says. “The inpatient team needs to place great importance on the transition of care and the subsequent quality of that care when the patient is discharged.”
Robert W. Harrington Jr., MD, SFHM, chief medical officer of Plano, Texas–based Reliant Post-Acute Care Solutions and former SHM president, says the health system landscapes are pushing HM beyond the hospitals’ walls.
How PAC settings differ from hospitals
Practicing in PAC has some important nuances that hospitalists from short-term acute care need to get accustomed to, Dr. Muldoon says. Primarily, the diagnostic capabilities are much more limited, as is the presence of high-level staffing. Further, patients are less resilient to medication changes and interventions, so changes need to be done gradually.
“Hospitalists who try to practice acute-care medicine in a PAC setting may become frustrated by the length of time it takes to do a work-up, get a consultation, and respond to a patient’s change of condition,” Dr. Muldoon says. “Nonetheless, hospitalists can overcome this once recognizing this mind shift.”
According to Dr. Harrington, another challenge hospitalists may face is the inability of the hospital’s and PAC facility’s IT platforms to exchange electronic information.
“The major vendors on both sides need to figure out an interoperability strategy,” he says. “Currently, it often takes 1-3 days to receive a new patient’s discharge summary. The summary may consist of a stack of paper that takes significant time to sort through and requires the PAC facility to perform duplicate data entry. It’s a very highly inefficient process that opens up the doors to mistakes and errors of omission and commission that can result in bad patient outcomes.”
Arif Nazir, MD, CMD, FACP, AGSF, chief medical officer of Signature HealthCARE and president of SHC Medical Partners, both in Louisville, Ky., cites additional reasons the lack of seamless communication between a hospital and PAC facility is problematic. “I see physicians order laboratory tests and investigations that were already done in the hospital because they didn’t know they were already performed or never received the results,” he says. “Similarly, I see patients continue to take medications prescribed in the hospital long term even though they were only supposed to take them short term. I’ve also seen patients come to a PAC setting from a hospital without any formal understanding of their rehabilitative period and expectations for recovery.”
What’s ahead?
Looking to the future, Surafel Tsega, MD, clinical instructor at Mount Sinai Hospital in New York, says he thinks there will be a move toward greater collaboration among inpatient and PAC facilities, particularly in the discharge process, given that hospitals have an added incentive to ensure safe transitions because reimbursement from the Centers for Medicare & Medicaid Services is tied to readmissions and there are penalties for readmission. This involves more comprehensive planning regarding “warm handoffs” (e.g., real-time discussions with PAC providers about a patient’s hospital course and plan of care upon discharge), transferring of information, and so forth.
And while it can still be challenging to identify high-risk patients or determine the intensity and duration of their care, Dr. Mathew says risk-stratification tools and care pathways are continually being refined to maximize value with the limited resources available. In addition, with an increased emphasis on employing a team approach to care, there will be better integration of non-medical services to address the social determinants of health, which play significant roles in overall health and healing.
“Working with community-based organizations for this purpose will be a valuable tool for any of the population health–based initiatives,” he says.
Dr. Muldoon says he believes healthcare reform will increasingly view an inpatient admission as something to be avoided.
“If hospitalization can’t be avoided, then it should be shortened as much as possible,” he says. “This will shift inpatient care into LTACHs, SNFs, and IRFs. Hospitalists would be wise to follow patients into those settings as traditional inpatient census is reduced. This will take a few years, so hospitalists should start now in preparing for that downstream transition of individuals who were previously inpatients.”
The cost of care, and other PAC facts and figures
The amount of money that Medicare spends on post-acute care (PAC) has been increasing. In 2012, 12.6% of Medicare beneficiaries used some form of PAC, costing $62 billion.2 That amounts to the Centers for Medicare & Medicaid Services spending close to 25% of Medicare beneficiary expenses on PAC, a 133% increase from 2001 to 2012. Among the different types, $30.4 billion was spent on skilled nursing facilities (SNFs), $18.6 billion on home health, and $13.1 billion on long-term acute care (LTAC) and acute-care rehabilitation.2
It’s also been reported that after short-term acute-care hospitalization, about one in five Medicare beneficiaries requires continued specialized treatment in one of the three typical Medicare PAC settings: inpatient rehabilitation facilities (IRFs), LTAC hospitals, and SNFs.3
What’s more, hospital readmission nearly doubles the cost of an episode, so the financial implications for organizations operating in risk-bearing arrangements are significant. In 2013, 2,213 hospitals were charged $280 million in readmission penalties.2
References
1. The role of post-acute care in new care delivery models. American Hospital Association website. Available at: http://www.aha.org/research/reports/tw/15dec-tw-postacute.pdf. Accessed Nov. 7, 2016.
2. Post-acute care integration: Today and in the future. DHG Healthcare website. Available at: http://www2.dhgllp.com/res_pubs/HCG-Post-Acute-Care-Integration.pdf. Accessed Nov. 7, 2016.
3. Overview: Post-acute care transitions toolkit. Society for Hospital Medicine website. Available at: http://www.hospitalmedicine.org/Web/Quality___Innovation/Implementation_Toolkit/pact/Overview_PACT.aspx?hkey=dea3da3c-8620-46db-a00f-89f07f021958. Accessed Nov. 10, 2016.
Transplantation palliative care: The time is ripe
Over 10 years ago, a challenge was made in a surgical publication for increased collaboration between the fields of transplantation and palliative care.1
Since that time not much progress has been made bringing these fields together in a consistent way that would mutually benefit patients and the specialties. However, other progress has been made, particularly in the field of palliative care, which could brighten the prospects and broaden the opportunities to accomplish collaboration between palliative care and transplantation.
Growth of palliative services
During the past decade there has been a robust proliferation of hospital-based palliative care programs in the United States. In all, 67% of U.S. hospitals with 50 or more beds report palliative care teams, up from 63% in 2011 and 53% in 2008.
Only a decade ago, critical care and palliative care were generally considered mutually exclusive. Evidence is trickling in to suggest that this is no longer the case. Although palliative care was not an integral part of critical care at that time, patients, families, and even practitioners began to demand these services. Cook and Rocker have eloquently advocated the rightful place of palliative care in the ICU.2
Studies in recent years have shown that the integration of palliative care into critical care decreases in length of ICU and hospital stay, decreases costs, enhances patient/family satisfaction, and promotes a more rapid consensus about goals of care, without increasing mortality. The ICU experience to date could be considered a reassuring precedent for transplantation palliative care.
Integration of palliative care with transplantation
Early palliative care intervention has been shown to improve symptom burden and depression scores in end-stage liver disease patients awaiting transplant. In addition, early palliative care consultation in conjunction with cancer treatment has been associated with increased survival in non–small-cell lung cancer patients. It has been demonstrated that early integration of palliative care in the surgical ICU alongside disease-directed curative care can be accomplished without change in mortality, while improving end-of-life practice in liver transplant patients.3

What palliative care can do for transplant patients
What does palliative care mean for the person (and family) awaiting transplantation? For the cirrhotic patient with cachexia, ascites, and encephalopathy, it means access to the services of a team trained in the management of these symptoms. Palliative care teams can also provide psychosocial and spiritual support for patients and families who are intimidated by the complex navigation of the health care system and the existential threat that end-stage organ failure presents to them. Skilled palliative care and services can be the difference between failing and extended life with a higher quality of life for these very sick patients
Resuscitation of a patient, whether through restoration of organ function or interdicting the progression of disease, begins with resuscitation of hope. Nothing achieves this more quickly than amelioration of burdensome symptoms for the patient and family.
The barriers for transplant surgeons and teams referring and incorporating palliative care services in their practices are multiple and profound. The unique dilemma facing the transplant team is to balance the treatment of the failing organ, the treatment of the patient (and family and friends), and the best use of the graft, a precious gift of society.
Palliative surgery has been defined as any invasive procedure in which the main intention is to mitigate physical symptoms in patients with noncurable disease without causing premature death. The very success of transplantation over the past 3 decades has obscured our memory of transplantation as a type of palliative surgery. It is a well-known axiom of reconstructive surgery that the reconstructed site should be compared to what was there, not to “normal.” Even in the current era of improved immunosuppression and posttransplant support services, one could hardly describe even a successful transplant patient’s experience as “normal.” These patients’ lives may be extended and/or enhanced but they need palliative care before, during, and after transplantation. The growing availability of trained palliative care clinicians and teams, the increased familiarity of palliative and end-of-life care to surgical residents and fellows, and quality metrics measuring palliative care outcomes will provide reassurance and guidance to address reservations about the convergence of the two seemingly opposite realities.
A modest proposal
We propose that palliative care be presented to the entire spectrum of transplantation care: on the ward, in the ICU, and after transplantation. More specific “triggers” for palliative care for referral of transplant patients should be identified. Wentlandt et al.4 have described a promising model for an ambulatory clinic, which provides early, integrated palliative care to patients awaiting and receiving organ transplantation. In addition, we propose an application for grant funding for a conference and eventual formation of a work group of transplant surgeons and team members, palliative care clinicians, and patient/families who have experienced one of the aspects of the transplant spectrum. We await the subspecialty certification in hospice and palliative medicine of a transplant surgeon. Outside of transplantation, every other surgical specialty in the United States has diplomates certified in hospice and palliative medicine. We await the benefits that will accrue from research about the merging of these fields.
1. Molmenti EP, Dunn GP: Transplantation and palliative care: The convergence of two seemingly opposite realities. Surg Clin North Am. 2005;85:373-82.
2. Cook D, Rocker G. Dying with dignity in the intensive care unit. N Engl J Med. 2014;370:2506-14.
3. Lamba S, Murphy P, McVicker S, Smith JH, and Mosenthal AC. Changing end-of-life care practice for liver transplant patients: structured palliative care intervention in the surgical intensive care unit. J Pain Symptom Manage. 2012; 44(4):508-19.
4. Wentlandt, K., Dall’Osto, A., Freeman, N., Le, L. W., Kaya, E., Ross, H., Singer, L. G., Abbey, S., Clarke, H. and Zimmermann, C. (2016), The Transplant Palliative Care Clinic: An early palliative care model for patients in a transplant program. Clin Transplant. 2016 Nov 4; doi: 10.1111/ctr.12838.
Dr. Azoulay is a transplantation specialist of Assistance Publique – Hôpitaux de Paris, and the University of Paris. Dr. Dunn is medical director of the Palliative Care Consultation Service at the University of Pittsburgh Medical Center Hamot, and vice-chair of the ACS Committee on Surgical Palliative Care.
Over 10 years ago, a challenge was made in a surgical publication for increased collaboration between the fields of transplantation and palliative care.1
Since that time not much progress has been made bringing these fields together in a consistent way that would mutually benefit patients and the specialties. However, other progress has been made, particularly in the field of palliative care, which could brighten the prospects and broaden the opportunities to accomplish collaboration between palliative care and transplantation.
Growth of palliative services
During the past decade there has been a robust proliferation of hospital-based palliative care programs in the United States. In all, 67% of U.S. hospitals with 50 or more beds report palliative care teams, up from 63% in 2011 and 53% in 2008.
Only a decade ago, critical care and palliative care were generally considered mutually exclusive. Evidence is trickling in to suggest that this is no longer the case. Although palliative care was not an integral part of critical care at that time, patients, families, and even practitioners began to demand these services. Cook and Rocker have eloquently advocated the rightful place of palliative care in the ICU.2
Studies in recent years have shown that the integration of palliative care into critical care decreases in length of ICU and hospital stay, decreases costs, enhances patient/family satisfaction, and promotes a more rapid consensus about goals of care, without increasing mortality. The ICU experience to date could be considered a reassuring precedent for transplantation palliative care.
Integration of palliative care with transplantation
Early palliative care intervention has been shown to improve symptom burden and depression scores in end-stage liver disease patients awaiting transplant. In addition, early palliative care consultation in conjunction with cancer treatment has been associated with increased survival in non–small-cell lung cancer patients. It has been demonstrated that early integration of palliative care in the surgical ICU alongside disease-directed curative care can be accomplished without change in mortality, while improving end-of-life practice in liver transplant patients.3
What palliative care can do for transplant patients
What does palliative care mean for the person (and family) awaiting transplantation? For the cirrhotic patient with cachexia, ascites, and encephalopathy, it means access to the services of a team trained in the management of these symptoms. Palliative care teams can also provide psychosocial and spiritual support for patients and families who are intimidated by the complex navigation of the health care system and the existential threat that end-stage organ failure presents to them. Skilled palliative care and services can be the difference between failing and extended life with a higher quality of life for these very sick patients
Resuscitation of a patient, whether through restoration of organ function or interdicting the progression of disease, begins with resuscitation of hope. Nothing achieves this more quickly than amelioration of burdensome symptoms for the patient and family.
The barriers for transplant surgeons and teams referring and incorporating palliative care services in their practices are multiple and profound. The unique dilemma facing the transplant team is to balance the treatment of the failing organ, the treatment of the patient (and family and friends), and the best use of the graft, a precious gift of society.
Palliative surgery has been defined as any invasive procedure in which the main intention is to mitigate physical symptoms in patients with noncurable disease without causing premature death. The very success of transplantation over the past 3 decades has obscured our memory of transplantation as a type of palliative surgery. It is a well-known axiom of reconstructive surgery that the reconstructed site should be compared to what was there, not to “normal.” Even in the current era of improved immunosuppression and posttransplant support services, one could hardly describe even a successful transplant patient’s experience as “normal.” These patients’ lives may be extended and/or enhanced but they need palliative care before, during, and after transplantation. The growing availability of trained palliative care clinicians and teams, the increased familiarity of palliative and end-of-life care to surgical residents and fellows, and quality metrics measuring palliative care outcomes will provide reassurance and guidance to address reservations about the convergence of the two seemingly opposite realities.
A modest proposal
We propose that palliative care be presented to the entire spectrum of transplantation care: on the ward, in the ICU, and after transplantation. More specific “triggers” for palliative care for referral of transplant patients should be identified. Wentlandt et al.4 have described a promising model for an ambulatory clinic, which provides early, integrated palliative care to patients awaiting and receiving organ transplantation. In addition, we propose an application for grant funding for a conference and eventual formation of a work group of transplant surgeons and team members, palliative care clinicians, and patient/families who have experienced one of the aspects of the transplant spectrum. We await the subspecialty certification in hospice and palliative medicine of a transplant surgeon. Outside of transplantation, every other surgical specialty in the United States has diplomates certified in hospice and palliative medicine. We await the benefits that will accrue from research about the merging of these fields.
1. Molmenti EP, Dunn GP: Transplantation and palliative care: The convergence of two seemingly opposite realities. Surg Clin North Am. 2005;85:373-82.
2. Cook D, Rocker G. Dying with dignity in the intensive care unit. N Engl J Med. 2014;370:2506-14.
3. Lamba S, Murphy P, McVicker S, Smith JH, and Mosenthal AC. Changing end-of-life care practice for liver transplant patients: structured palliative care intervention in the surgical intensive care unit. J Pain Symptom Manage. 2012; 44(4):508-19.
4. Wentlandt, K., Dall’Osto, A., Freeman, N., Le, L. W., Kaya, E., Ross, H., Singer, L. G., Abbey, S., Clarke, H. and Zimmermann, C. (2016), The Transplant Palliative Care Clinic: An early palliative care model for patients in a transplant program. Clin Transplant. 2016 Nov 4; doi: 10.1111/ctr.12838.
Dr. Azoulay is a transplantation specialist of Assistance Publique – Hôpitaux de Paris, and the University of Paris. Dr. Dunn is medical director of the Palliative Care Consultation Service at the University of Pittsburgh Medical Center Hamot, and vice-chair of the ACS Committee on Surgical Palliative Care.
Over 10 years ago, a challenge was made in a surgical publication for increased collaboration between the fields of transplantation and palliative care.1
Since that time not much progress has been made bringing these fields together in a consistent way that would mutually benefit patients and the specialties. However, other progress has been made, particularly in the field of palliative care, which could brighten the prospects and broaden the opportunities to accomplish collaboration between palliative care and transplantation.
Growth of palliative services
During the past decade there has been a robust proliferation of hospital-based palliative care programs in the United States. In all, 67% of U.S. hospitals with 50 or more beds report palliative care teams, up from 63% in 2011 and 53% in 2008.
Only a decade ago, critical care and palliative care were generally considered mutually exclusive. Evidence is trickling in to suggest that this is no longer the case. Although palliative care was not an integral part of critical care at that time, patients, families, and even practitioners began to demand these services. Cook and Rocker have eloquently advocated the rightful place of palliative care in the ICU.2
Studies in recent years have shown that the integration of palliative care into critical care decreases in length of ICU and hospital stay, decreases costs, enhances patient/family satisfaction, and promotes a more rapid consensus about goals of care, without increasing mortality. The ICU experience to date could be considered a reassuring precedent for transplantation palliative care.
Integration of palliative care with transplantation
Early palliative care intervention has been shown to improve symptom burden and depression scores in end-stage liver disease patients awaiting transplant. In addition, early palliative care consultation in conjunction with cancer treatment has been associated with increased survival in non–small-cell lung cancer patients. It has been demonstrated that early integration of palliative care in the surgical ICU alongside disease-directed curative care can be accomplished without change in mortality, while improving end-of-life practice in liver transplant patients.3
What palliative care can do for transplant patients
What does palliative care mean for the person (and family) awaiting transplantation? For the cirrhotic patient with cachexia, ascites, and encephalopathy, it means access to the services of a team trained in the management of these symptoms. Palliative care teams can also provide psychosocial and spiritual support for patients and families who are intimidated by the complex navigation of the health care system and the existential threat that end-stage organ failure presents to them. Skilled palliative care and services can be the difference between failing and extended life with a higher quality of life for these very sick patients
Resuscitation of a patient, whether through restoration of organ function or interdicting the progression of disease, begins with resuscitation of hope. Nothing achieves this more quickly than amelioration of burdensome symptoms for the patient and family.
The barriers for transplant surgeons and teams referring and incorporating palliative care services in their practices are multiple and profound. The unique dilemma facing the transplant team is to balance the treatment of the failing organ, the treatment of the patient (and family and friends), and the best use of the graft, a precious gift of society.
Palliative surgery has been defined as any invasive procedure in which the main intention is to mitigate physical symptoms in patients with noncurable disease without causing premature death. The very success of transplantation over the past 3 decades has obscured our memory of transplantation as a type of palliative surgery. It is a well-known axiom of reconstructive surgery that the reconstructed site should be compared to what was there, not to “normal.” Even in the current era of improved immunosuppression and posttransplant support services, one could hardly describe even a successful transplant patient’s experience as “normal.” These patients’ lives may be extended and/or enhanced but they need palliative care before, during, and after transplantation. The growing availability of trained palliative care clinicians and teams, the increased familiarity of palliative and end-of-life care to surgical residents and fellows, and quality metrics measuring palliative care outcomes will provide reassurance and guidance to address reservations about the convergence of the two seemingly opposite realities.
A modest proposal
We propose that palliative care be presented to the entire spectrum of transplantation care: on the ward, in the ICU, and after transplantation. More specific “triggers” for palliative care for referral of transplant patients should be identified. Wentlandt et al.4 have described a promising model for an ambulatory clinic, which provides early, integrated palliative care to patients awaiting and receiving organ transplantation. In addition, we propose an application for grant funding for a conference and eventual formation of a work group of transplant surgeons and team members, palliative care clinicians, and patient/families who have experienced one of the aspects of the transplant spectrum. We await the subspecialty certification in hospice and palliative medicine of a transplant surgeon. Outside of transplantation, every other surgical specialty in the United States has diplomates certified in hospice and palliative medicine. We await the benefits that will accrue from research about the merging of these fields.
1. Molmenti EP, Dunn GP: Transplantation and palliative care: The convergence of two seemingly opposite realities. Surg Clin North Am. 2005;85:373-82.
2. Cook D, Rocker G. Dying with dignity in the intensive care unit. N Engl J Med. 2014;370:2506-14.
3. Lamba S, Murphy P, McVicker S, Smith JH, and Mosenthal AC. Changing end-of-life care practice for liver transplant patients: structured palliative care intervention in the surgical intensive care unit. J Pain Symptom Manage. 2012; 44(4):508-19.
4. Wentlandt, K., Dall’Osto, A., Freeman, N., Le, L. W., Kaya, E., Ross, H., Singer, L. G., Abbey, S., Clarke, H. and Zimmermann, C. (2016), The Transplant Palliative Care Clinic: An early palliative care model for patients in a transplant program. Clin Transplant. 2016 Nov 4; doi: 10.1111/ctr.12838.
Dr. Azoulay is a transplantation specialist of Assistance Publique – Hôpitaux de Paris, and the University of Paris. Dr. Dunn is medical director of the Palliative Care Consultation Service at the University of Pittsburgh Medical Center Hamot, and vice-chair of the ACS Committee on Surgical Palliative Care.
Best Practices: Protecting Dry Vulnerable Skin with CeraVe® Healing Ointment
A supplement to Dermatology News. This advertising supplement is sponsored by Valeant Pharmaceuticals.

- Reinforcing the Skin Barrier
- NEA Seal of Acceptance
- A Preventative Approach to Dry, Cracked Skin
- CeraVe Ointment in the Clinical Setting
Faculty/Faculty Disclosure
Sheila Fallon Friedlander, MD
Professor of Clinical Dermatology & Pediatrics
Director, Pediatric Dermatology Fellowship Training Program
University of California at San Diego School of Medicine
Rady Children’s Hospital,
San Diego, California
Dr. Friedlander was compensated for her participation in the development of this article.
CeraVe is a registered trademark of Valeant Pharmaceuticals International, Inc. or its affiliates.
A supplement to Dermatology News. This advertising supplement is sponsored by Valeant Pharmaceuticals.
- Reinforcing the Skin Barrier
- NEA Seal of Acceptance
- A Preventative Approach to Dry, Cracked Skin
- CeraVe Ointment in the Clinical Setting
Faculty/Faculty Disclosure
Sheila Fallon Friedlander, MD
Professor of Clinical Dermatology & Pediatrics
Director, Pediatric Dermatology Fellowship Training Program
University of California at San Diego School of Medicine
Rady Children’s Hospital,
San Diego, California
Dr. Friedlander was compensated for her participation in the development of this article.
CeraVe is a registered trademark of Valeant Pharmaceuticals International, Inc. or its affiliates.
A supplement to Dermatology News. This advertising supplement is sponsored by Valeant Pharmaceuticals.
- Reinforcing the Skin Barrier
- NEA Seal of Acceptance
- A Preventative Approach to Dry, Cracked Skin
- CeraVe Ointment in the Clinical Setting
Faculty/Faculty Disclosure
Sheila Fallon Friedlander, MD
Professor of Clinical Dermatology & Pediatrics
Director, Pediatric Dermatology Fellowship Training Program
University of California at San Diego School of Medicine
Rady Children’s Hospital,
San Diego, California
Dr. Friedlander was compensated for her participation in the development of this article.
CeraVe is a registered trademark of Valeant Pharmaceuticals International, Inc. or its affiliates.

Impact of a Pharmacist ICS Deprescribing Intervention on COPD Exacerbations and Adverse Events
Impact of a Pharmacist ICS Deprescribing Intervention on COPD Exacerbations and Adverse Events
Chronic obstructive pulmonary disease (COPD) affects about 25% of the veteran population and is the third-leading cause of death globally.1,2 In patients with COPD, cigarette smoking leads to increased respiratory symptoms, a greater annual rate of decline in forced expiratory volume in 1 second (FEV1), and an increase in COPD mortality rate vs nonsmokers.3 Veterans are at a higher risk of COPD due to increased prevalence of smoking within this population as well as military activities leading to environmental and occupational exposure.4
According to the 2024 Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines, the primary treatment goals of COPD therapy are to reduce symptoms and future risk of exacerbations.3 Bronchodilators are recommended for initial COPD pharmacotherapy, including long-acting muscarinic antagonists (LAMAs) and/or long-acting Β2-agonists (LABAs). In some cases, treatment may include inhaled corticosteroids (ICS). Evidence supports ICS therapy in patients with COPD experiencing hospitalizations for exacerbations, ≥ 2 moderate exacerbations per year, blood eosinophil count ≥ 300 cells/μL or concomitant asthma.3
While the 2024 GOLD guidelines caution against the use of ICS outside of certain patient groups, previous GOLD guidelines recommended the use of ICS more broadly.5 Due to these changes, many patients may be using ICS therapy unnecessarily. At the Sioux Falls Veterans Affairs Health Care System (SFVAHCS), ICS overuse was identified as a driver of increased medication burden and potential adverse effects (AEs). To help reduce unnecessary ICS use, a data dashboard was created to identify potential candidates for ICS deprescribing. SFVAHCS clinical pharmacy practitioners are licensed pharmacists who work as independent practitioners with a scope of practice that allows them to initiate, modify, or discontinue medication therapy within medication management clinics. Pharmacists contacted dashboard patients to de-escalate ICS therapy when appropriate.
The SUNSET trial directly compared the continuation of triple therapy (tiotropium + salmeterol/fluticasone propionate) vs deprescribing to LABA/LAMA (indacaterol/ glycopyrronium) in patients with COPD.6 It evaluated whether LABA/LAMA was noninferior to LABA/LAMA/ICS therapy when comparing COPD exacerbations in patients whose COPD exacerbations were infrequent. Participants were randomized to triple therapy continuation or indacaterol/glycopyrronium and followed for 26 weeks. Patients on indacaterol/glycopyrronium did not have a significant difference in exacerbations than patients utilizing triple therapy.
The Implementation of a Targeted ICS De-Escalation in Patients with COPD in the Primary Care Setting trial evaluated the success of pharmacist-led ICS deprescribing in appropriate patients with COPD.7 Pharmacists followed GOLD guidelines to recommend ICS deprescribing and have risk vs benefit discussions with certain patients. Patients were considered for ICS deprescribing if they had a history of recurrent pneumonia or had no exacerbations within the previous year and eosinophils < 300 cells/μL (risk-benefit discussion if no eosinophil count available). This study found that 19.6% of patients were unable to tolerate ICS withdrawal and resumed either a standard or reduced dose of ICS therapy.7
Current guidelines and evidence recommend deprescribing ICS for appropriate patients. There is no current literature defining the impact of pharmacists on ICS deprescribing within the US Department of Veterans Affairs (VA) system. This study will allow for a quantifiable measure of pharmacists’ impact on reducing AEs associated with unnecessary ICS use.
Methods
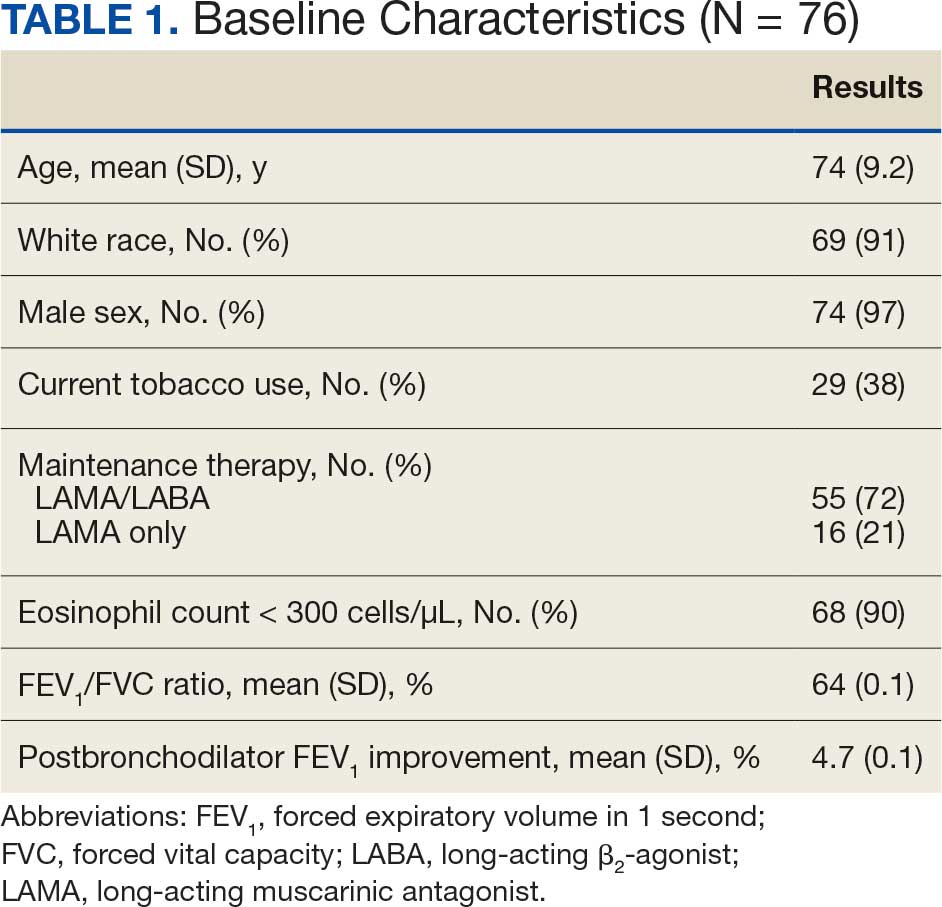
This retrospective, single-center study was conducted at the SFVAHCS. Data were collected through manual chart review of SFVAHCS electronic health records. Veterans aged ≥ 18 years with a COPD diagnosis who underwent ICS deprescribing by a SFVAHCS pharmacist between February 2022 and December 2023 were included. Records were examined for 52 weeks prior to ICS withdrawal (baseline) and 52 weeks following withdrawal. Patients were excluded from the study if they had a history of asthma or ICS was used for < 52 weeks before deprescribing. Baseline characteristics were collected, including age, race, sex, current tobacco use, eosinophil count, COPD maintenance therapy, FEV1/forced vital capacity (FVC) ratio, and mean postbronchodilator FEV1 improvement.
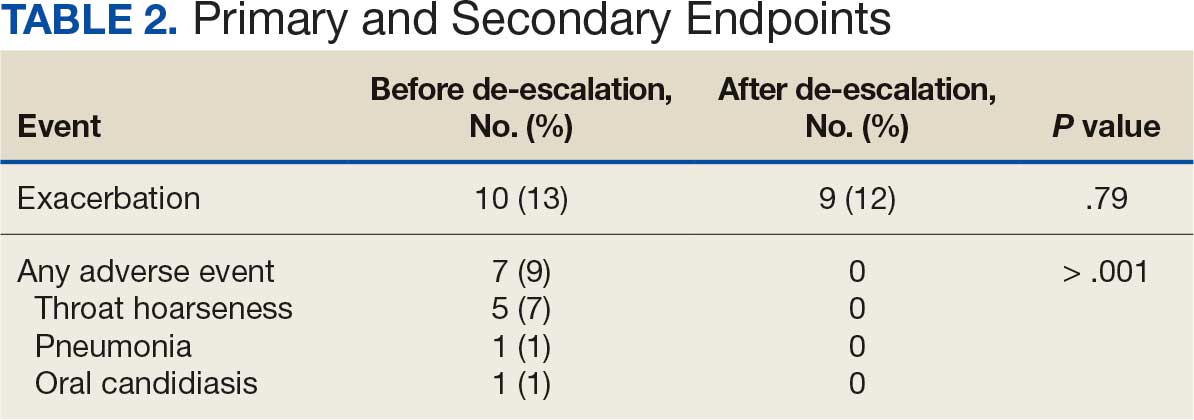
The primary endpoint was number of COPD exacerbations at 52 weeks before vs after deprescribing. Secondary endpoints included the number of patients restarted on an ICS within 52 weeks of deprescribing, as well as ICS AEs, including pneumonia, oral candidiasis, and throat hoarseness.
Statistical Analysis
The primary endpoint was analyzed using the Wilcoxon signed rank test and secondary endpoints were analyzed using the McNemar exact test. Results with P < .05 were considered statistically significant for both tests.
Results
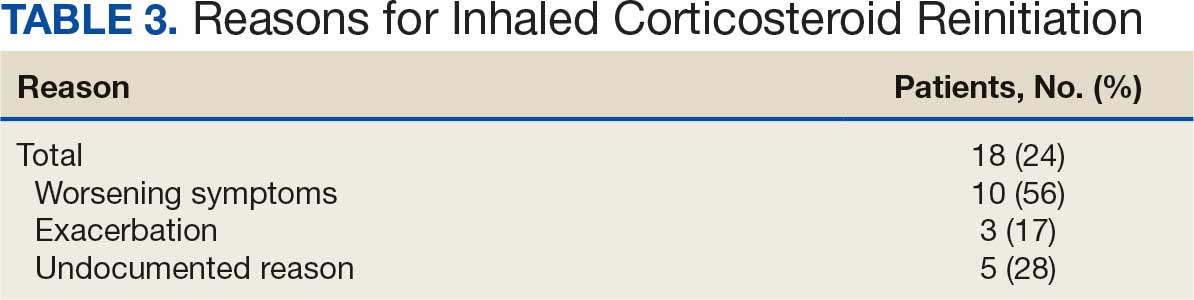
Seventy-six patients were included. Patients had a mean age of 75 years and 91% identified as White, which is representative of the SFVAHCS patient population (Table 1). Twenty-nine (38%) patients were current tobacco users and 55 patients (72%) used LAMA/LABA therapy (after ICS deprescribing) with an eosinophil count < 300 cells/μL. There was no significant difference in exacerbations before vs after ICS deprescribing (P = .78) (Table 2). There were 7 AEs reported before ICS deprescribing vs 0 following ICS deprescribing (P < .001). Five patients (7%) reported throat hoarseness, 1 (1%) reported pneumonia, and 1 (1%) reported oral candidiasis. Eighteen patients were reinitiated on ICS (24%). ICS reinitiation was most commonly due to patients reporting worsening symptoms (56%) (Table 3).
Discussion
This study sought to determine the impact of pharmacist-led ICS deprescribing on AEs and exacerbations experienced by patients with COPD. COPD exacerbations were not significantly different before vs after ICS deprescribing. The pharmacist-led ICS deprescribing program did not lead to increased COPD exacerbations. Similar to the SUNSET trial, the results of this study showed exacerbations did not significantly increase upon ICS deprescribing; however, this study differed by specifying pharmacist- led intervention.6
There was a decrease in ICS-related AEs following ICS deprescribing. Several patients were reinitiated on an ICS. As expected with deprescribing, some patients were not able to tolerate ICS withdrawal or had clinical indications to resume therapy (ie, an exacerbation). Similar results were found in another study where 8.9% of patients were restarted on ICS and 10.9% were de-escalated to a lower dose but were unable to stop completely.7 A 2024 systematic review by Georgiou et al found a wide range of patients resumed ICS therapy following withdrawal (21%-74%). Of note, only 2 of the randomized controlled trials and 3 observational studies included this meta-analysis included data on ICS reinitiation. Georgiou et al concluded there was insufficient evidence to determine the proportion of patients reinitiated on ICS but patients were commonly resumed on ICS therapy due to worsening symptoms, experiencing an exacerbation or decline in FEV1.8 Although the rate of ICS reinitiation was unclear in the Georgiou et al meta-analysis, reasons for re-initiation were similar to what was found in our study.8
Strengths and Limitations
The retrospective nature of this study and its small sample size of 76 patients limit its findings. The retrospective nature of the study required researchers to rely on proper chart documentation, which is not always accurate or up to date. Lack of documentation of COPD exacerbations or patients who received care outside the VA following initial deprescribing could have biased study results. This patient population is representative of the veteran population in South Dakota but is not representative of the female or non-White patient population which may be more prevalent at other VA Health Care Systems as well as nonveteran patient populations. Additionally, this study was limited to a review of 52 weeks pre- and post-ICS deprescribing which may have impacted results. Patients may have had a COPD exacerbation or were restarted on ICS therapy beyond 52 weeks. Finally, the retrospective nature and small sample size limited the findings for the primary endpoint which could have been improved with a larger sample size and a randomized controlled design.
The comparison of patients with themselves before and after ICS deprescribing reduced the potential for bias seen in retrospective studies. This method did not require a second control group which would potentially introduce confounding factors.
Conclusions
This study found that in a small population of veterans with COPD, pharmacist-led ICS deprescribing did not lead to an increase in COPD exacerbations and decreased the risk of AEs related to ICS therapy. Some patients were reinitiated on ICS therapy; however, reinitiation was rarely attributable to a COPD exacerbation. This study suggests that pharmacists were able to appropriately identify candidates for ICS deprescribing without increasing their risk of exacerbations. By de-escalating ICS therapy, pharmacists decreased medication burden and potential AEs caused by ICS therapy. These findings support expanding the role of clinical pharmacists in COPD management, particularly in identifying candidates for safe ICS deprescribing.
- Li HY, Gao TY, Fang W, et al. Global, regional and national burden of chronic obstructive pulmonary disease over a 30-year period: estimates from the 1990 to 2019 Global Burden of Disease Study. Respirology. 2023;28:29-36. doi:10.1111/resp.14349/
- Anderson E, Wiener RS, Resnick K, et al. Care coordination for veterans with COPD: a positive deviance study. Am J Manag Care. 2020;26:63-68. doi:10.37765/ajmc.2020.42394
- Global Initiative for Chronic Obstructive Lung Disease. 2024 GOLD Report. November 12, 2023. Accessed April 1, 2026. https://goldcopd.org/2023-gold-report-2/
- US Department of Veterans Affairs, Department of Defense. VA/DoD clinical practice guideline for the management of chronic obstructive pulmonary disease. April 2021. Accessed April 1, 2026. https://www.healthquality.va.gov /guidelines/cd/copd/
- Gruffydd-Jones K. GOLD guidelines 2011: what are the implications for primary care? Prim Care Respir J. 2012;21:437-441. doi:10.4104/pcrj.2012.00058
- Chapman KR, Hurst JR, Frent SM, et al. Long-term triple therapy de-escalation to indacaterol/glycopyrronium in patients with chronic obstructive pulmonary disease (SUNSET): a randomized, double-blind, triple-dummy clinical trial. Am J Respir Crit Care Med. 2018;198:329-339. doi:10.1164/rccm.201803-0405OC
- Hahn NM, Nagy MW. Implementation of a targeted inhaled corticosteroid de-escalation process in patients with chronic obstructive pulmonary disease in the primary care setting. Innov Pharm. 2022;13:10.24926/iip.v13i1.4349. doi:10.24926/iip.v13i1.4349
- Georgiou A, Ramesh R, Schofield P, et al. Withdrawal of inhaled corticosteroids from patients with COPD; effect on exacerbation frequency and lung function: a systematic review. Int J Chron Obstruct Pulmon Dis. 2024;19:1403- 1419. doi:10.2147/COPD.S436525
Chronic obstructive pulmonary disease (COPD) affects about 25% of the veteran population and is the third-leading cause of death globally.1,2 In patients with COPD, cigarette smoking leads to increased respiratory symptoms, a greater annual rate of decline in forced expiratory volume in 1 second (FEV1), and an increase in COPD mortality rate vs nonsmokers.3 Veterans are at a higher risk of COPD due to increased prevalence of smoking within this population as well as military activities leading to environmental and occupational exposure.4
According to the 2024 Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines, the primary treatment goals of COPD therapy are to reduce symptoms and future risk of exacerbations.3 Bronchodilators are recommended for initial COPD pharmacotherapy, including long-acting muscarinic antagonists (LAMAs) and/or long-acting Β2-agonists (LABAs). In some cases, treatment may include inhaled corticosteroids (ICS). Evidence supports ICS therapy in patients with COPD experiencing hospitalizations for exacerbations, ≥ 2 moderate exacerbations per year, blood eosinophil count ≥ 300 cells/μL or concomitant asthma.3
While the 2024 GOLD guidelines caution against the use of ICS outside of certain patient groups, previous GOLD guidelines recommended the use of ICS more broadly.5 Due to these changes, many patients may be using ICS therapy unnecessarily. At the Sioux Falls Veterans Affairs Health Care System (SFVAHCS), ICS overuse was identified as a driver of increased medication burden and potential adverse effects (AEs). To help reduce unnecessary ICS use, a data dashboard was created to identify potential candidates for ICS deprescribing. SFVAHCS clinical pharmacy practitioners are licensed pharmacists who work as independent practitioners with a scope of practice that allows them to initiate, modify, or discontinue medication therapy within medication management clinics. Pharmacists contacted dashboard patients to de-escalate ICS therapy when appropriate.
The SUNSET trial directly compared the continuation of triple therapy (tiotropium + salmeterol/fluticasone propionate) vs deprescribing to LABA/LAMA (indacaterol/ glycopyrronium) in patients with COPD.6 It evaluated whether LABA/LAMA was noninferior to LABA/LAMA/ICS therapy when comparing COPD exacerbations in patients whose COPD exacerbations were infrequent. Participants were randomized to triple therapy continuation or indacaterol/glycopyrronium and followed for 26 weeks. Patients on indacaterol/glycopyrronium did not have a significant difference in exacerbations than patients utilizing triple therapy.
The Implementation of a Targeted ICS De-Escalation in Patients with COPD in the Primary Care Setting trial evaluated the success of pharmacist-led ICS deprescribing in appropriate patients with COPD.7 Pharmacists followed GOLD guidelines to recommend ICS deprescribing and have risk vs benefit discussions with certain patients. Patients were considered for ICS deprescribing if they had a history of recurrent pneumonia or had no exacerbations within the previous year and eosinophils < 300 cells/μL (risk-benefit discussion if no eosinophil count available). This study found that 19.6% of patients were unable to tolerate ICS withdrawal and resumed either a standard or reduced dose of ICS therapy.7
Current guidelines and evidence recommend deprescribing ICS for appropriate patients. There is no current literature defining the impact of pharmacists on ICS deprescribing within the US Department of Veterans Affairs (VA) system. This study will allow for a quantifiable measure of pharmacists’ impact on reducing AEs associated with unnecessary ICS use.
Methods
This retrospective, single-center study was conducted at the SFVAHCS. Data were collected through manual chart review of SFVAHCS electronic health records. Veterans aged ≥ 18 years with a COPD diagnosis who underwent ICS deprescribing by a SFVAHCS pharmacist between February 2022 and December 2023 were included. Records were examined for 52 weeks prior to ICS withdrawal (baseline) and 52 weeks following withdrawal. Patients were excluded from the study if they had a history of asthma or ICS was used for < 52 weeks before deprescribing. Baseline characteristics were collected, including age, race, sex, current tobacco use, eosinophil count, COPD maintenance therapy, FEV1/forced vital capacity (FVC) ratio, and mean postbronchodilator FEV1 improvement.
The primary endpoint was number of COPD exacerbations at 52 weeks before vs after deprescribing. Secondary endpoints included the number of patients restarted on an ICS within 52 weeks of deprescribing, as well as ICS AEs, including pneumonia, oral candidiasis, and throat hoarseness.
Statistical Analysis
The primary endpoint was analyzed using the Wilcoxon signed rank test and secondary endpoints were analyzed using the McNemar exact test. Results with P < .05 were considered statistically significant for both tests.
Results
Seventy-six patients were included. Patients had a mean age of 75 years and 91% identified as White, which is representative of the SFVAHCS patient population (Table 1). Twenty-nine (38%) patients were current tobacco users and 55 patients (72%) used LAMA/LABA therapy (after ICS deprescribing) with an eosinophil count < 300 cells/μL. There was no significant difference in exacerbations before vs after ICS deprescribing (P = .78) (Table 2). There were 7 AEs reported before ICS deprescribing vs 0 following ICS deprescribing (P < .001). Five patients (7%) reported throat hoarseness, 1 (1%) reported pneumonia, and 1 (1%) reported oral candidiasis. Eighteen patients were reinitiated on ICS (24%). ICS reinitiation was most commonly due to patients reporting worsening symptoms (56%) (Table 3).
Discussion
This study sought to determine the impact of pharmacist-led ICS deprescribing on AEs and exacerbations experienced by patients with COPD. COPD exacerbations were not significantly different before vs after ICS deprescribing. The pharmacist-led ICS deprescribing program did not lead to increased COPD exacerbations. Similar to the SUNSET trial, the results of this study showed exacerbations did not significantly increase upon ICS deprescribing; however, this study differed by specifying pharmacist- led intervention.6
There was a decrease in ICS-related AEs following ICS deprescribing. Several patients were reinitiated on an ICS. As expected with deprescribing, some patients were not able to tolerate ICS withdrawal or had clinical indications to resume therapy (ie, an exacerbation). Similar results were found in another study where 8.9% of patients were restarted on ICS and 10.9% were de-escalated to a lower dose but were unable to stop completely.7 A 2024 systematic review by Georgiou et al found a wide range of patients resumed ICS therapy following withdrawal (21%-74%). Of note, only 2 of the randomized controlled trials and 3 observational studies included this meta-analysis included data on ICS reinitiation. Georgiou et al concluded there was insufficient evidence to determine the proportion of patients reinitiated on ICS but patients were commonly resumed on ICS therapy due to worsening symptoms, experiencing an exacerbation or decline in FEV1.8 Although the rate of ICS reinitiation was unclear in the Georgiou et al meta-analysis, reasons for re-initiation were similar to what was found in our study.8
Strengths and Limitations
The retrospective nature of this study and its small sample size of 76 patients limit its findings. The retrospective nature of the study required researchers to rely on proper chart documentation, which is not always accurate or up to date. Lack of documentation of COPD exacerbations or patients who received care outside the VA following initial deprescribing could have biased study results. This patient population is representative of the veteran population in South Dakota but is not representative of the female or non-White patient population which may be more prevalent at other VA Health Care Systems as well as nonveteran patient populations. Additionally, this study was limited to a review of 52 weeks pre- and post-ICS deprescribing which may have impacted results. Patients may have had a COPD exacerbation or were restarted on ICS therapy beyond 52 weeks. Finally, the retrospective nature and small sample size limited the findings for the primary endpoint which could have been improved with a larger sample size and a randomized controlled design.
The comparison of patients with themselves before and after ICS deprescribing reduced the potential for bias seen in retrospective studies. This method did not require a second control group which would potentially introduce confounding factors.
Conclusions
This study found that in a small population of veterans with COPD, pharmacist-led ICS deprescribing did not lead to an increase in COPD exacerbations and decreased the risk of AEs related to ICS therapy. Some patients were reinitiated on ICS therapy; however, reinitiation was rarely attributable to a COPD exacerbation. This study suggests that pharmacists were able to appropriately identify candidates for ICS deprescribing without increasing their risk of exacerbations. By de-escalating ICS therapy, pharmacists decreased medication burden and potential AEs caused by ICS therapy. These findings support expanding the role of clinical pharmacists in COPD management, particularly in identifying candidates for safe ICS deprescribing.
Chronic obstructive pulmonary disease (COPD) affects about 25% of the veteran population and is the third-leading cause of death globally.1,2 In patients with COPD, cigarette smoking leads to increased respiratory symptoms, a greater annual rate of decline in forced expiratory volume in 1 second (FEV1), and an increase in COPD mortality rate vs nonsmokers.3 Veterans are at a higher risk of COPD due to increased prevalence of smoking within this population as well as military activities leading to environmental and occupational exposure.4
According to the 2024 Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines, the primary treatment goals of COPD therapy are to reduce symptoms and future risk of exacerbations.3 Bronchodilators are recommended for initial COPD pharmacotherapy, including long-acting muscarinic antagonists (LAMAs) and/or long-acting Β2-agonists (LABAs). In some cases, treatment may include inhaled corticosteroids (ICS). Evidence supports ICS therapy in patients with COPD experiencing hospitalizations for exacerbations, ≥ 2 moderate exacerbations per year, blood eosinophil count ≥ 300 cells/μL or concomitant asthma.3
While the 2024 GOLD guidelines caution against the use of ICS outside of certain patient groups, previous GOLD guidelines recommended the use of ICS more broadly.5 Due to these changes, many patients may be using ICS therapy unnecessarily. At the Sioux Falls Veterans Affairs Health Care System (SFVAHCS), ICS overuse was identified as a driver of increased medication burden and potential adverse effects (AEs). To help reduce unnecessary ICS use, a data dashboard was created to identify potential candidates for ICS deprescribing. SFVAHCS clinical pharmacy practitioners are licensed pharmacists who work as independent practitioners with a scope of practice that allows them to initiate, modify, or discontinue medication therapy within medication management clinics. Pharmacists contacted dashboard patients to de-escalate ICS therapy when appropriate.
The SUNSET trial directly compared the continuation of triple therapy (tiotropium + salmeterol/fluticasone propionate) vs deprescribing to LABA/LAMA (indacaterol/ glycopyrronium) in patients with COPD.6 It evaluated whether LABA/LAMA was noninferior to LABA/LAMA/ICS therapy when comparing COPD exacerbations in patients whose COPD exacerbations were infrequent. Participants were randomized to triple therapy continuation or indacaterol/glycopyrronium and followed for 26 weeks. Patients on indacaterol/glycopyrronium did not have a significant difference in exacerbations than patients utilizing triple therapy.
The Implementation of a Targeted ICS De-Escalation in Patients with COPD in the Primary Care Setting trial evaluated the success of pharmacist-led ICS deprescribing in appropriate patients with COPD.7 Pharmacists followed GOLD guidelines to recommend ICS deprescribing and have risk vs benefit discussions with certain patients. Patients were considered for ICS deprescribing if they had a history of recurrent pneumonia or had no exacerbations within the previous year and eosinophils < 300 cells/μL (risk-benefit discussion if no eosinophil count available). This study found that 19.6% of patients were unable to tolerate ICS withdrawal and resumed either a standard or reduced dose of ICS therapy.7
Current guidelines and evidence recommend deprescribing ICS for appropriate patients. There is no current literature defining the impact of pharmacists on ICS deprescribing within the US Department of Veterans Affairs (VA) system. This study will allow for a quantifiable measure of pharmacists’ impact on reducing AEs associated with unnecessary ICS use.
Methods
This retrospective, single-center study was conducted at the SFVAHCS. Data were collected through manual chart review of SFVAHCS electronic health records. Veterans aged ≥ 18 years with a COPD diagnosis who underwent ICS deprescribing by a SFVAHCS pharmacist between February 2022 and December 2023 were included. Records were examined for 52 weeks prior to ICS withdrawal (baseline) and 52 weeks following withdrawal. Patients were excluded from the study if they had a history of asthma or ICS was used for < 52 weeks before deprescribing. Baseline characteristics were collected, including age, race, sex, current tobacco use, eosinophil count, COPD maintenance therapy, FEV1/forced vital capacity (FVC) ratio, and mean postbronchodilator FEV1 improvement.
The primary endpoint was number of COPD exacerbations at 52 weeks before vs after deprescribing. Secondary endpoints included the number of patients restarted on an ICS within 52 weeks of deprescribing, as well as ICS AEs, including pneumonia, oral candidiasis, and throat hoarseness.
Statistical Analysis
The primary endpoint was analyzed using the Wilcoxon signed rank test and secondary endpoints were analyzed using the McNemar exact test. Results with P < .05 were considered statistically significant for both tests.
Results
Seventy-six patients were included. Patients had a mean age of 75 years and 91% identified as White, which is representative of the SFVAHCS patient population (Table 1). Twenty-nine (38%) patients were current tobacco users and 55 patients (72%) used LAMA/LABA therapy (after ICS deprescribing) with an eosinophil count < 300 cells/μL. There was no significant difference in exacerbations before vs after ICS deprescribing (P = .78) (Table 2). There were 7 AEs reported before ICS deprescribing vs 0 following ICS deprescribing (P < .001). Five patients (7%) reported throat hoarseness, 1 (1%) reported pneumonia, and 1 (1%) reported oral candidiasis. Eighteen patients were reinitiated on ICS (24%). ICS reinitiation was most commonly due to patients reporting worsening symptoms (56%) (Table 3).
Discussion
This study sought to determine the impact of pharmacist-led ICS deprescribing on AEs and exacerbations experienced by patients with COPD. COPD exacerbations were not significantly different before vs after ICS deprescribing. The pharmacist-led ICS deprescribing program did not lead to increased COPD exacerbations. Similar to the SUNSET trial, the results of this study showed exacerbations did not significantly increase upon ICS deprescribing; however, this study differed by specifying pharmacist- led intervention.6
There was a decrease in ICS-related AEs following ICS deprescribing. Several patients were reinitiated on an ICS. As expected with deprescribing, some patients were not able to tolerate ICS withdrawal or had clinical indications to resume therapy (ie, an exacerbation). Similar results were found in another study where 8.9% of patients were restarted on ICS and 10.9% were de-escalated to a lower dose but were unable to stop completely.7 A 2024 systematic review by Georgiou et al found a wide range of patients resumed ICS therapy following withdrawal (21%-74%). Of note, only 2 of the randomized controlled trials and 3 observational studies included this meta-analysis included data on ICS reinitiation. Georgiou et al concluded there was insufficient evidence to determine the proportion of patients reinitiated on ICS but patients were commonly resumed on ICS therapy due to worsening symptoms, experiencing an exacerbation or decline in FEV1.8 Although the rate of ICS reinitiation was unclear in the Georgiou et al meta-analysis, reasons for re-initiation were similar to what was found in our study.8
Strengths and Limitations
The retrospective nature of this study and its small sample size of 76 patients limit its findings. The retrospective nature of the study required researchers to rely on proper chart documentation, which is not always accurate or up to date. Lack of documentation of COPD exacerbations or patients who received care outside the VA following initial deprescribing could have biased study results. This patient population is representative of the veteran population in South Dakota but is not representative of the female or non-White patient population which may be more prevalent at other VA Health Care Systems as well as nonveteran patient populations. Additionally, this study was limited to a review of 52 weeks pre- and post-ICS deprescribing which may have impacted results. Patients may have had a COPD exacerbation or were restarted on ICS therapy beyond 52 weeks. Finally, the retrospective nature and small sample size limited the findings for the primary endpoint which could have been improved with a larger sample size and a randomized controlled design.
The comparison of patients with themselves before and after ICS deprescribing reduced the potential for bias seen in retrospective studies. This method did not require a second control group which would potentially introduce confounding factors.
Conclusions
This study found that in a small population of veterans with COPD, pharmacist-led ICS deprescribing did not lead to an increase in COPD exacerbations and decreased the risk of AEs related to ICS therapy. Some patients were reinitiated on ICS therapy; however, reinitiation was rarely attributable to a COPD exacerbation. This study suggests that pharmacists were able to appropriately identify candidates for ICS deprescribing without increasing their risk of exacerbations. By de-escalating ICS therapy, pharmacists decreased medication burden and potential AEs caused by ICS therapy. These findings support expanding the role of clinical pharmacists in COPD management, particularly in identifying candidates for safe ICS deprescribing.
- Li HY, Gao TY, Fang W, et al. Global, regional and national burden of chronic obstructive pulmonary disease over a 30-year period: estimates from the 1990 to 2019 Global Burden of Disease Study. Respirology. 2023;28:29-36. doi:10.1111/resp.14349/
- Anderson E, Wiener RS, Resnick K, et al. Care coordination for veterans with COPD: a positive deviance study. Am J Manag Care. 2020;26:63-68. doi:10.37765/ajmc.2020.42394
- Global Initiative for Chronic Obstructive Lung Disease. 2024 GOLD Report. November 12, 2023. Accessed April 1, 2026. https://goldcopd.org/2023-gold-report-2/
- US Department of Veterans Affairs, Department of Defense. VA/DoD clinical practice guideline for the management of chronic obstructive pulmonary disease. April 2021. Accessed April 1, 2026. https://www.healthquality.va.gov /guidelines/cd/copd/
- Gruffydd-Jones K. GOLD guidelines 2011: what are the implications for primary care? Prim Care Respir J. 2012;21:437-441. doi:10.4104/pcrj.2012.00058
- Chapman KR, Hurst JR, Frent SM, et al. Long-term triple therapy de-escalation to indacaterol/glycopyrronium in patients with chronic obstructive pulmonary disease (SUNSET): a randomized, double-blind, triple-dummy clinical trial. Am J Respir Crit Care Med. 2018;198:329-339. doi:10.1164/rccm.201803-0405OC
- Hahn NM, Nagy MW. Implementation of a targeted inhaled corticosteroid de-escalation process in patients with chronic obstructive pulmonary disease in the primary care setting. Innov Pharm. 2022;13:10.24926/iip.v13i1.4349. doi:10.24926/iip.v13i1.4349
- Georgiou A, Ramesh R, Schofield P, et al. Withdrawal of inhaled corticosteroids from patients with COPD; effect on exacerbation frequency and lung function: a systematic review. Int J Chron Obstruct Pulmon Dis. 2024;19:1403- 1419. doi:10.2147/COPD.S436525
- Li HY, Gao TY, Fang W, et al. Global, regional and national burden of chronic obstructive pulmonary disease over a 30-year period: estimates from the 1990 to 2019 Global Burden of Disease Study. Respirology. 2023;28:29-36. doi:10.1111/resp.14349/
- Anderson E, Wiener RS, Resnick K, et al. Care coordination for veterans with COPD: a positive deviance study. Am J Manag Care. 2020;26:63-68. doi:10.37765/ajmc.2020.42394
- Global Initiative for Chronic Obstructive Lung Disease. 2024 GOLD Report. November 12, 2023. Accessed April 1, 2026. https://goldcopd.org/2023-gold-report-2/
- US Department of Veterans Affairs, Department of Defense. VA/DoD clinical practice guideline for the management of chronic obstructive pulmonary disease. April 2021. Accessed April 1, 2026. https://www.healthquality.va.gov /guidelines/cd/copd/
- Gruffydd-Jones K. GOLD guidelines 2011: what are the implications for primary care? Prim Care Respir J. 2012;21:437-441. doi:10.4104/pcrj.2012.00058
- Chapman KR, Hurst JR, Frent SM, et al. Long-term triple therapy de-escalation to indacaterol/glycopyrronium in patients with chronic obstructive pulmonary disease (SUNSET): a randomized, double-blind, triple-dummy clinical trial. Am J Respir Crit Care Med. 2018;198:329-339. doi:10.1164/rccm.201803-0405OC
- Hahn NM, Nagy MW. Implementation of a targeted inhaled corticosteroid de-escalation process in patients with chronic obstructive pulmonary disease in the primary care setting. Innov Pharm. 2022;13:10.24926/iip.v13i1.4349. doi:10.24926/iip.v13i1.4349
- Georgiou A, Ramesh R, Schofield P, et al. Withdrawal of inhaled corticosteroids from patients with COPD; effect on exacerbation frequency and lung function: a systematic review. Int J Chron Obstruct Pulmon Dis. 2024;19:1403- 1419. doi:10.2147/COPD.S436525
Impact of a Pharmacist ICS Deprescribing Intervention on COPD Exacerbations and Adverse Events
Impact of a Pharmacist ICS Deprescribing Intervention on COPD Exacerbations and Adverse Events
Pembrolizumab-Induced Bullous Pemphigoid: Navigating Diagnostic Challenges and Treatment Resistance
Pembrolizumab-Induced Bullous Pemphigoid: Navigating Diagnostic Challenges and Treatment Resistance
Bullous pemphigoid (BP) is an autoimmune blistering disorder characterized by the development of tense subepidermal blisters and erosions primarily on the skin, commonly affecting the elderly.1 It is attributed to autoantibodies targeting 2 hemidesmosomal components within the dermoepidermal junction—transmembrane collagen XVII (BP180/BPAG2) and plakin family protein BP230 (BPAG1)—resulting in blister formation due to loss of structural integrity.2 Typically, patients present with pruritic urticarial plaques and tense bullae localized on flexural areas, but cutaneous manifestations vary and can be nonspecific. Histologically, a subepidermal blister with eosinophilic infiltration is characteristic, and detection of circulating autoantibodies against BP180 and BP230 antigens aids in diagnosis.3,4
Drug-induced BP (DIBP) is a subset triggered by medications, including immune checkpoint inhibitors (ICIs) targeting programmed cell death protein-1 (PD-1) or its ligand, programmed death ligand-1 (PD-L1).5,6 Often overexpressed in malignant tumors, PD-L1 inhibits host lymphocytic and apoptotic immune responses. Anti‒PD-1 and anti‒PD-L1 agents, designed to enhance the immune system’s ability to recognize and eliminate cancer cells,7,8 have improved oncologic outcomes for various cancers, including urothelial cancer.9-11 Before 2016, platinum-based chemotherapy was the mainstay for metastatic urothelial cancer management, but US Food and Drug Administration approval of 5 ICIs—nivolumab, pembrolizumab, avelumab, atezolizumab, and durvalumab—transformed treatment options.12Despite robust antitumor responses to ICIs, these medications are increasingly associated with immune-related adverse events (IRAEs), including DIBP, due to inhibition of negative regulators of immunity crucial for maintaining immunologic homeostasis.13,14 Up to 30% to 40% of patients treated with PD-1 inhibitors experience dermatologic complications, such as lichenoid reactions, eczema, vitiligo, and pruritus,15 and patients undergoing treatment with the PD-1 inhibitor pembrolizumab are estimated to be 2.6 times more likely to develop a rash than those receiving standard chemotherapy.16,17 The pathogenesis of DIBP involves autoreactive T-cell activation and subsequent autoantibody production against BP antigens.18 We present the case of DIBP secondary to pembrolizumab immunotherapy in a man with PD-L1–negative metastatic bladder cancer.
Case Report
An 81-year-old man with metastatic urothelial carcinoma presented to dermatology with a pruritic rash characterized by blisters of 5 months’ duration following treatment with pembrolizumab. He had a history of non–muscle invasive urothelial carcinoma and underwent intravesical bacillus Calmette-Guerin treatment. Thirty years later, after surveillance cystoscopies, the patient developed hematuria, which prompted pelvic ultrasonography and cystoscopy that revealed a tumor. Transurethral resection of the bladder tumor confirmed invasive, high-grade papillary urothelial carcinoma with vascular and muscle invasion (clinical stage T2NxMx). Due to elevated creatinine levels, neoadjuvant chemotherapy was contraindicated. Instead, the patient underwent cystoprostatectomy with ureteroileal conduit creation and pelvic lymphadenectomy one month later; final pathology revealed pT2aN0M0 disease with multifocal carcinoma in situ. At that time, there was no evidence of distant metastasis. Surveillance 5 months later identified pulmonary nodules that were confirmed as metastatic urothelial cancer by positron emission tomography/computed tomography (CT). The patient received 6 cycles of paclitaxel (175 mg/m² on day 1) and gemcitabine (1000 mg/m² on days 1 and 8 every 21 days), with progressive disease 16 months later. Despite 0% PD-L1 expression, pembrolizumab 400 mg intravenous (IV) treatment every 6 weeks was initiated 2 months later, and subsequent positron emission tomography/CT showed a positive response at 3 and 7 months after treatment initiation. After the patient’s sixth cycle of pembrolizumab, a generalized maculopapular rash involving approximately 50% of the body surface area led to discontinuation of pembrolizumab, initiation of multiple courses of prednisone and prednisolone, and a dermatology referral.
At the current presentation, the patient exhibited excoriated red patches on the abdomen, wrists, arms, upper chest, and legs (Figure 1). Tense blisters were observed on various areas, including the ear and arms. The provisional diagnosis was pembrolizumab-induced BP, supported by the clinical history, presentation, and an initial positive response to steroids. Treatment included topical triamcinolone 0.1% ointment and prednisone 40 mg daily. Biopsies revealed subepidermal blisters with underlying eosinophils on histopathology (Figure 2). Direct immunofluorescence showed strong linear basement membrane zone staining with IgG and C3, consistent with a diagnosis of BP.
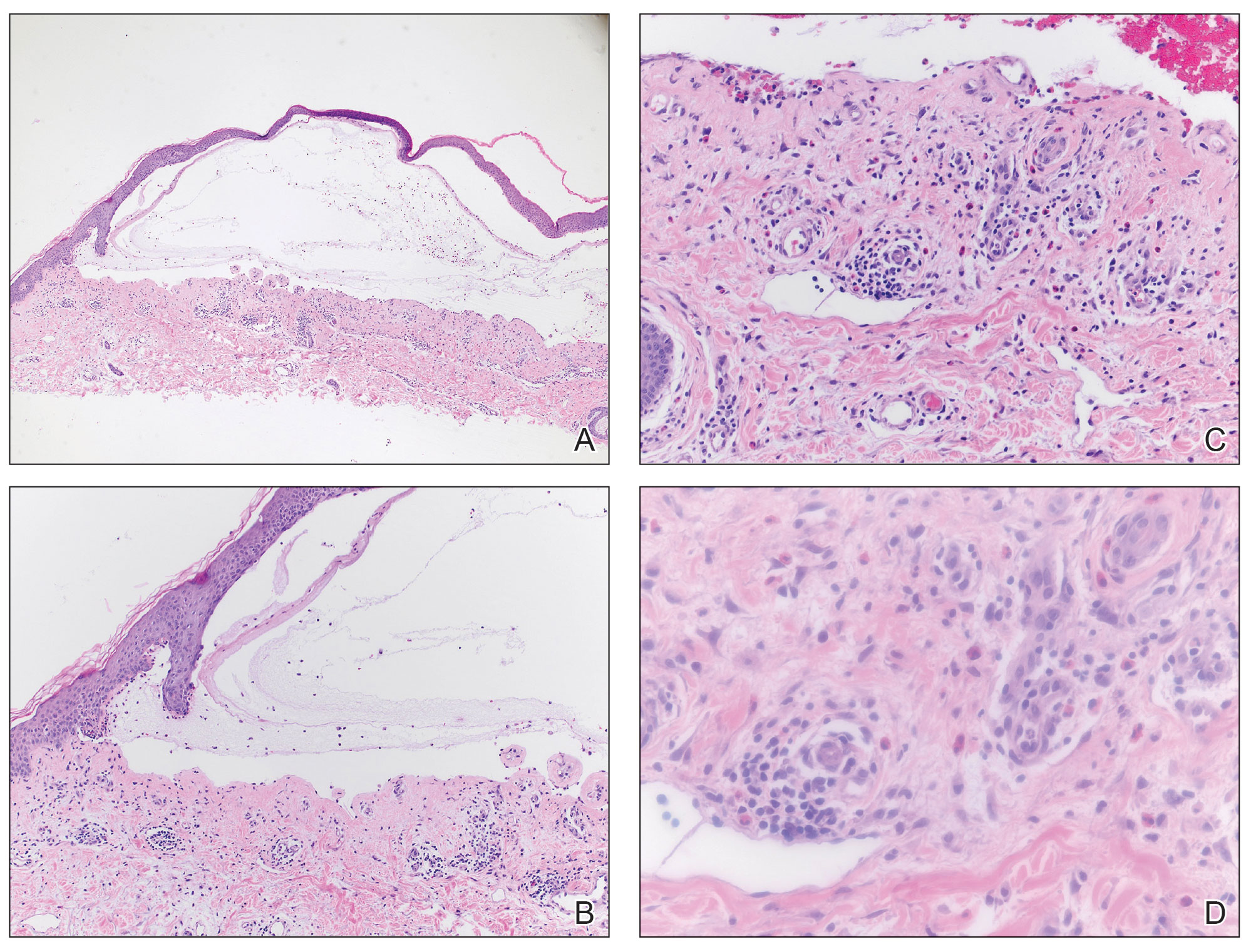
One month later, the patient was given the first of two 1-g doses of rituximab, chosen as a treatment due to metastatic cancer history and ongoing severity of the DIBP. In addition, a slow prednisone taper was initiated. Atovaquone 1500 mg daily was ordered for Pneumocystis jirovecii prophylaxis. Following the first rituximab dose, the patient became clear of DIBP but required treatment for a chronic urinary tract infection, delaying the second rituximab dose. The prednisone taper continued, however, and the patient reported re-emergence of several blisters, followed by resolution of pruritus following the second rituximab dose. Bilateral pulmonary embolisms were noted on a restaging CT, attributed to the underlying malignancy and inflammation from DIBP. Doxycycline was initiated at 100 mg twice daily, and prednisone was slowly tapered (as tolerated by the patient’s symptoms) down to 2.5 mg daily approximately 6 months after rituximab initiation. The patient remains in clinical remission at last follow-up; however, considerations for further treatments have included intravenous immunoglobulin.
Comment
This case highlights major clinical challenges in the diagnosis and management of DIBP in a patient with metastatic urothelial carcinoma receiving ICI therapy. Our patient’s clinical course offers several high-yield lessons regarding diagnostic latency, treatment resistance, and a multidisciplinary approach to management.
Pruritus as a Precursor—Since an initial report in 2015, the emergence of DIBP postpembrolizumab has been well described in the literature.19-22 Pruritus is frequently the earliest symptom, preceding bullous eruption. Similar to our case—in which DIBP developed 30 weeks after pembrolizumab initiation—the classic clinical presentation and formation of bullae often are delayed, typically occurring 28 and 39 weeks.
Beyond Corticosteroids to Manage Refractory DIBP—Our patient’s DIBP persisted despite multiple interventions, including pembrolizumab discontinuation, corticosteroid therapy, and rituximab administration. Although cases of DIBP in pembrolizumab-treated metastatic urothelial carcinoma patients have been reported, they did not exhibit similar treatment resistance.23-25 As observed in our patient, immunotherapy discontinuation has been reported in at least 40% of all ICI-mediated cases of BP.14 Subsequent management involves low-dose oral corticosteroids and potent topical corticosteroids; the duration of steroid treatment varies widely, ranging from a few weeks to longer than 12 months, with no standardized approach.26 In cases where ICI withdrawal and corticosteroids fail to produce a complete response, monoclonal antibodies such as rituximab, dupilumab, and omalizumab have been used as alternative treatments, with dupilumab recently receiving US Food and Drug Administration approval for moderate to severe BP.27-31 These biologics selectively inhibit autoantibody formation and the inflammatory cascade, and research has pointed toward them as safe and effective options for refractory BP. Although robust randomized, controlled clinical trials on rituximab for DIBP still are lacking, prospective and retrospective cohort studies have shown promising results, including complete remission rates of 67% to 90%, along with a decline in circulating BP180-specific B lymphocytes, anti-BP180 IgG, and the expression of proinflammatory IL-15 and IL-6.32
Despite receiving 2 doses of rituximab, our patient experienced recurrence of blisters when prednisone was tapered, prompting discussions about alternative tapering timelines and additional therapies such as doxycycline33 or intravenous immunoglobulin,34 which have emerged as steroid-sparing agents for BP following initial steroid therapy.
Systemic Barriers and the Need for Multidisciplinary Care—This case underscores systemic barriers within the health care system that impede prompt diagnosis and management of conditions such as DIBP. The 5-month delay between the patient’s referral to dermatology and the actual consultation, potentially due to shortages of dermatologists, highlights the need for more systematic urgent dermatologic referrals and streamlined diagnostic pathways in suspected cases of IRAEs. Diagnosis requires comprehensive evaluation, including skin biopsy for histopathologic examination and immunofluorescence studies. Ruling out alternative blistering disorders, such as epidermolysis bullosa acquisita, is crucial before confirming a BP diagnosis. Encouraging direct communication between referring physicians and consultants often can expedite the process, as a call from the referring physician can alert the consultant and speed up scheduling. Notably, the patient’s daughter, who was a patient of the dermatologist herself, played a crucial role in advocating for the dermatology referral. Although this should not be necessary, it highlights the pivotal role families can play in ensuring timely access to specialized care for challenging conditions such as BP.
Lastly, the refractory nature of the patient’s condition, coupled with concurrent chronic urinary tract infection and bilateral pulmonary embolisms, emphasizes the necessity of multidisciplinary collaboration among oncology, dermatology, and primary care in managing DIBP. Consulting experts on IRAEs and coordinating with the oncologist were essential for making informed treatment decisions and facilitating the timely exchange of clinical information.
Conclusion
This case underscores the importance of timely recognition and diagnosis of DIBP in patients undergoing ICI therapy but also highlights the need for individualized treatment approaches and multidisciplinary collaboration when managing adverse cutaneous reactions.
- Schmidt E, Zillikens D. Pemphigoid diseases. Lancet. 2013;381:320-332.
- Nishie W. Update on the pathogenesis of bullous pemphigoid: an autoantibody-mediated blistering disease targeting collagen XVII. J Dermatol Sci. 2014;73:179-186.
- Sárdy M, Kostaki D, Varga R, et al. Comparative study of direct and indirect immunofluorescence and of bullous pemphigoid 180 and 230 enzyme-linked immunosorbent assays for diagnosis of bullous pemphigoid. J Am Acad Dermatol. 2013;69:748-753.
- Smith EP, Taylor TB, Meyer LJ, et al. Antigen identification in drug-induced bullous pemphigoid. J Am Acad Dermatol. 1993;29(5 Pt 2):879-882.
- Siegel J, Totonchy M, Damsky W, et al. Bullous disorders associated with anti-PD-1 and anti-PD-L1 therapy: a retrospective analysis evaluating the clinical and histopathologic features, frequency, and impact on cancer therapy. J Am Acad Dermatol. 2018;79:1081-1088.
- Asdourian MS, Shah N, Jacoby TV, et al. Association of bullous pemphigoid with immune checkpoint inhibitor therapy in patients with cancer: a systematic review. JAMA Dermatol. 2022;158:933-941.
- Pardoll DM. The blockade of immune checkpoints in cancer immunotherapy. Nat Rev Cancer. 2012;12:252-264.
- Dunn GP, Bruce AT, Ikeda H, et al. Cancer immunoediting: from immunosurveillance to tumor escape. Nat Immunol. 2002;3:991-998.
- Powles T, Eder JP, Fine GD, et al. MPDL3280A (anti-PD-L1) treatment leads to clinical activity in metastatic bladder cancer. Nature. 2014;515:558-562.
- Bellmunt J, de Wit R, Vaughn DJ, et al. Pembrolizumab as second-line therapy for advanced urothelial carcinoma. N Engl J Med. 2017;376:1015-1026.
- Fradet Y, Bellmunt J, Vaughn DJ, et al. Randomized phase III KEYNOTE-045 trial of pembrolizumab versus paclitaxel, docetaxel, or vinflunine in recurrent advanced urothelial cancer: results of >2 years of follow-up. Ann Oncol. 2019;30:970-976.
- Felsenstein KM, Theodorescu D. Precision medicine for urothelial bladder cancer: update on tumour genomics and immunotherapy. Nat Rev Urol. 2018;15:92-111.
- Sibaud V. Dermatologic reactions to immune checkpoint inhibitors: skin toxicities and immunotherapy. Am J Clin Dermatol. 2018;19:345-361.
- Lopez AT, Khanna T, Antonov N, et al. A review of bullous pemphigoid associated with PD-1 and PD-L1 inhibitors. Int J Dermatol. 2018;57:664-669.
- Hwang SJE, Carlos G, Wakade D, et al. Cutaneous adverse events (AEs) of anti-programmed cell death (PD)-1 therapy in patients with metastatic melanoma: a single-institution cohort. J Am Acad Dermatol. 2016;74:455-461.e1.
- Belum VR, Benhuri B, Postow MA, et al. Characterisation and management of dermatologic adverse events to agents targeting the PD-1 receptor. Eur J Cancer. 2016;60:12-25.
- Naidoo J, Page DB, Li BT, et al. Toxicities of the anti-PD-1 and anti-PD-L1 immune checkpoint antibodies. Ann Oncol. 2015;26:2375-2391.
- Weber JS, Yang JC, Atkins MB, et al. Toxicities of immunotherapy for the practitioner. J Clin Oncol. 2015;33:2092-2099.
- Carlos G, Anforth R, Chou S, et al. A case of bullous pemphigoid in a patient with metastatic melanoma treated with pembrolizumab. Melanoma Res. 2015;25:265-268.
- Adachi E, Honda T, Nonoyama S, al. Severe bullous pemphigoid in a metastatic lung cancer patient treated with pembrolizumab. J Dermatol. 2019;46:E232-E233.
- Cardona AF, Ruiz-Patiño A, Zatarain-Barron ZL, et al. Refractory bullous pemphigoid in a patient with metastatic lung adenocarcinoma treated with pembrolizumab. Case Rep Oncol. 2021;14:386-390.
- Sun CW, Grossman SK, Aphale A, et al. Pembrolizumab-induced bullous pemphigoid. JAAD Case Rep. 2019;5:362-364.
- Correia C, Fernandes S, Soares-de-Almeida L, et al. Bullous pemphigoid probably associated with pembrolizumab: a case of delayed toxicity. Int J Dermatol. 2022;61:E129-E131.
- Shalata W, Weissmann S, Itzhaki Gabay S, et al. A retrospective, single-institution experience of bullous pemphigoid as an adverse effect of immune checkpoint inhibitors. Cancers. 2022;14:5451. doi:10.3390/cancers14215451
- Garje R, Chau JJ, Chung J, et al. Acute flare of bullous pemphigus with pembrolizumab used for treatment of metastatic urothelial cancer. J Immunother. 2018;41:42-44.
- Wang J, Hu X, Jiang W, et al. Analysis of the clinical characteristics of pembrolizumab-induced bullous pemphigoid. Front Oncol. 2023;13:1095694.
- Thomas RM, Colon A, Motaparthi K. Rituximab in autoimmune pemphigoid diseases: indications, optimized regimens, and practice gaps. Clin Dermatol. 2020;38:384-396.
- Sowerby L, Dewan AK, Granter S, et al. Rituximab treatment of nivolumab-induced bullous pemphigoid. JAMA Dermatol. 2017;153:603-605.
- Sharma P, Barnes M, Nabeel S, et al. Pembrolizumab-induced bullous pemphigoid treated with rituximab. JCO Oncol Pract. 2020;16:764-766.
- Abdat R, Waldman RA, de Bedout V, et al. Dupilumab as a novel therapy for bullous pemphigoid: a multicenter case series. J Am Acad Dermatol. 2020;83:46-52.
- Cao P, Xu W, Zhang L. Rituximab, omalizumab, and dupilumab treatment outcomes in bullous pemphigoid: a systematic review. Front Immunol. 2022;13:928621.
- Karakioulaki M, Eyerich K, Patsatsi A. Advancements in bullous pemphigoid treatment: a comprehensive pipeline update. Am J Clin Dermatol. 2024;25:195-212.
- Jin XX, Wang X, Shan Y, et al. Efficacy and safety of tetracyclines for pemphigoid: a systematic review and meta-analysis. Arch Dermatol Res. 2022;314:191-201.
- Kianfar N, Dasdar S, Daneshpazhooh M, et al. A systematic review on efficacy, safety and treatment durability of intravenous immunoglobulin in autoimmune bullous dermatoses: special focus on indication and combination therapy. Exp Dermatol. 2023;32:934-944.
Bullous pemphigoid (BP) is an autoimmune blistering disorder characterized by the development of tense subepidermal blisters and erosions primarily on the skin, commonly affecting the elderly.1 It is attributed to autoantibodies targeting 2 hemidesmosomal components within the dermoepidermal junction—transmembrane collagen XVII (BP180/BPAG2) and plakin family protein BP230 (BPAG1)—resulting in blister formation due to loss of structural integrity.2 Typically, patients present with pruritic urticarial plaques and tense bullae localized on flexural areas, but cutaneous manifestations vary and can be nonspecific. Histologically, a subepidermal blister with eosinophilic infiltration is characteristic, and detection of circulating autoantibodies against BP180 and BP230 antigens aids in diagnosis.3,4
Drug-induced BP (DIBP) is a subset triggered by medications, including immune checkpoint inhibitors (ICIs) targeting programmed cell death protein-1 (PD-1) or its ligand, programmed death ligand-1 (PD-L1).5,6 Often overexpressed in malignant tumors, PD-L1 inhibits host lymphocytic and apoptotic immune responses. Anti‒PD-1 and anti‒PD-L1 agents, designed to enhance the immune system’s ability to recognize and eliminate cancer cells,7,8 have improved oncologic outcomes for various cancers, including urothelial cancer.9-11 Before 2016, platinum-based chemotherapy was the mainstay for metastatic urothelial cancer management, but US Food and Drug Administration approval of 5 ICIs—nivolumab, pembrolizumab, avelumab, atezolizumab, and durvalumab—transformed treatment options.12Despite robust antitumor responses to ICIs, these medications are increasingly associated with immune-related adverse events (IRAEs), including DIBP, due to inhibition of negative regulators of immunity crucial for maintaining immunologic homeostasis.13,14 Up to 30% to 40% of patients treated with PD-1 inhibitors experience dermatologic complications, such as lichenoid reactions, eczema, vitiligo, and pruritus,15 and patients undergoing treatment with the PD-1 inhibitor pembrolizumab are estimated to be 2.6 times more likely to develop a rash than those receiving standard chemotherapy.16,17 The pathogenesis of DIBP involves autoreactive T-cell activation and subsequent autoantibody production against BP antigens.18 We present the case of DIBP secondary to pembrolizumab immunotherapy in a man with PD-L1–negative metastatic bladder cancer.
Case Report
An 81-year-old man with metastatic urothelial carcinoma presented to dermatology with a pruritic rash characterized by blisters of 5 months’ duration following treatment with pembrolizumab. He had a history of non–muscle invasive urothelial carcinoma and underwent intravesical bacillus Calmette-Guerin treatment. Thirty years later, after surveillance cystoscopies, the patient developed hematuria, which prompted pelvic ultrasonography and cystoscopy that revealed a tumor. Transurethral resection of the bladder tumor confirmed invasive, high-grade papillary urothelial carcinoma with vascular and muscle invasion (clinical stage T2NxMx). Due to elevated creatinine levels, neoadjuvant chemotherapy was contraindicated. Instead, the patient underwent cystoprostatectomy with ureteroileal conduit creation and pelvic lymphadenectomy one month later; final pathology revealed pT2aN0M0 disease with multifocal carcinoma in situ. At that time, there was no evidence of distant metastasis. Surveillance 5 months later identified pulmonary nodules that were confirmed as metastatic urothelial cancer by positron emission tomography/computed tomography (CT). The patient received 6 cycles of paclitaxel (175 mg/m² on day 1) and gemcitabine (1000 mg/m² on days 1 and 8 every 21 days), with progressive disease 16 months later. Despite 0% PD-L1 expression, pembrolizumab 400 mg intravenous (IV) treatment every 6 weeks was initiated 2 months later, and subsequent positron emission tomography/CT showed a positive response at 3 and 7 months after treatment initiation. After the patient’s sixth cycle of pembrolizumab, a generalized maculopapular rash involving approximately 50% of the body surface area led to discontinuation of pembrolizumab, initiation of multiple courses of prednisone and prednisolone, and a dermatology referral.
At the current presentation, the patient exhibited excoriated red patches on the abdomen, wrists, arms, upper chest, and legs (Figure 1). Tense blisters were observed on various areas, including the ear and arms. The provisional diagnosis was pembrolizumab-induced BP, supported by the clinical history, presentation, and an initial positive response to steroids. Treatment included topical triamcinolone 0.1% ointment and prednisone 40 mg daily. Biopsies revealed subepidermal blisters with underlying eosinophils on histopathology (Figure 2). Direct immunofluorescence showed strong linear basement membrane zone staining with IgG and C3, consistent with a diagnosis of BP.
One month later, the patient was given the first of two 1-g doses of rituximab, chosen as a treatment due to metastatic cancer history and ongoing severity of the DIBP. In addition, a slow prednisone taper was initiated. Atovaquone 1500 mg daily was ordered for Pneumocystis jirovecii prophylaxis. Following the first rituximab dose, the patient became clear of DIBP but required treatment for a chronic urinary tract infection, delaying the second rituximab dose. The prednisone taper continued, however, and the patient reported re-emergence of several blisters, followed by resolution of pruritus following the second rituximab dose. Bilateral pulmonary embolisms were noted on a restaging CT, attributed to the underlying malignancy and inflammation from DIBP. Doxycycline was initiated at 100 mg twice daily, and prednisone was slowly tapered (as tolerated by the patient’s symptoms) down to 2.5 mg daily approximately 6 months after rituximab initiation. The patient remains in clinical remission at last follow-up; however, considerations for further treatments have included intravenous immunoglobulin.
Comment
This case highlights major clinical challenges in the diagnosis and management of DIBP in a patient with metastatic urothelial carcinoma receiving ICI therapy. Our patient’s clinical course offers several high-yield lessons regarding diagnostic latency, treatment resistance, and a multidisciplinary approach to management.
Pruritus as a Precursor—Since an initial report in 2015, the emergence of DIBP postpembrolizumab has been well described in the literature.19-22 Pruritus is frequently the earliest symptom, preceding bullous eruption. Similar to our case—in which DIBP developed 30 weeks after pembrolizumab initiation—the classic clinical presentation and formation of bullae often are delayed, typically occurring 28 and 39 weeks.
Beyond Corticosteroids to Manage Refractory DIBP—Our patient’s DIBP persisted despite multiple interventions, including pembrolizumab discontinuation, corticosteroid therapy, and rituximab administration. Although cases of DIBP in pembrolizumab-treated metastatic urothelial carcinoma patients have been reported, they did not exhibit similar treatment resistance.23-25 As observed in our patient, immunotherapy discontinuation has been reported in at least 40% of all ICI-mediated cases of BP.14 Subsequent management involves low-dose oral corticosteroids and potent topical corticosteroids; the duration of steroid treatment varies widely, ranging from a few weeks to longer than 12 months, with no standardized approach.26 In cases where ICI withdrawal and corticosteroids fail to produce a complete response, monoclonal antibodies such as rituximab, dupilumab, and omalizumab have been used as alternative treatments, with dupilumab recently receiving US Food and Drug Administration approval for moderate to severe BP.27-31 These biologics selectively inhibit autoantibody formation and the inflammatory cascade, and research has pointed toward them as safe and effective options for refractory BP. Although robust randomized, controlled clinical trials on rituximab for DIBP still are lacking, prospective and retrospective cohort studies have shown promising results, including complete remission rates of 67% to 90%, along with a decline in circulating BP180-specific B lymphocytes, anti-BP180 IgG, and the expression of proinflammatory IL-15 and IL-6.32
Despite receiving 2 doses of rituximab, our patient experienced recurrence of blisters when prednisone was tapered, prompting discussions about alternative tapering timelines and additional therapies such as doxycycline33 or intravenous immunoglobulin,34 which have emerged as steroid-sparing agents for BP following initial steroid therapy.
Systemic Barriers and the Need for Multidisciplinary Care—This case underscores systemic barriers within the health care system that impede prompt diagnosis and management of conditions such as DIBP. The 5-month delay between the patient’s referral to dermatology and the actual consultation, potentially due to shortages of dermatologists, highlights the need for more systematic urgent dermatologic referrals and streamlined diagnostic pathways in suspected cases of IRAEs. Diagnosis requires comprehensive evaluation, including skin biopsy for histopathologic examination and immunofluorescence studies. Ruling out alternative blistering disorders, such as epidermolysis bullosa acquisita, is crucial before confirming a BP diagnosis. Encouraging direct communication between referring physicians and consultants often can expedite the process, as a call from the referring physician can alert the consultant and speed up scheduling. Notably, the patient’s daughter, who was a patient of the dermatologist herself, played a crucial role in advocating for the dermatology referral. Although this should not be necessary, it highlights the pivotal role families can play in ensuring timely access to specialized care for challenging conditions such as BP.
Lastly, the refractory nature of the patient’s condition, coupled with concurrent chronic urinary tract infection and bilateral pulmonary embolisms, emphasizes the necessity of multidisciplinary collaboration among oncology, dermatology, and primary care in managing DIBP. Consulting experts on IRAEs and coordinating with the oncologist were essential for making informed treatment decisions and facilitating the timely exchange of clinical information.
Conclusion
This case underscores the importance of timely recognition and diagnosis of DIBP in patients undergoing ICI therapy but also highlights the need for individualized treatment approaches and multidisciplinary collaboration when managing adverse cutaneous reactions.
Bullous pemphigoid (BP) is an autoimmune blistering disorder characterized by the development of tense subepidermal blisters and erosions primarily on the skin, commonly affecting the elderly.1 It is attributed to autoantibodies targeting 2 hemidesmosomal components within the dermoepidermal junction—transmembrane collagen XVII (BP180/BPAG2) and plakin family protein BP230 (BPAG1)—resulting in blister formation due to loss of structural integrity.2 Typically, patients present with pruritic urticarial plaques and tense bullae localized on flexural areas, but cutaneous manifestations vary and can be nonspecific. Histologically, a subepidermal blister with eosinophilic infiltration is characteristic, and detection of circulating autoantibodies against BP180 and BP230 antigens aids in diagnosis.3,4
Drug-induced BP (DIBP) is a subset triggered by medications, including immune checkpoint inhibitors (ICIs) targeting programmed cell death protein-1 (PD-1) or its ligand, programmed death ligand-1 (PD-L1).5,6 Often overexpressed in malignant tumors, PD-L1 inhibits host lymphocytic and apoptotic immune responses. Anti‒PD-1 and anti‒PD-L1 agents, designed to enhance the immune system’s ability to recognize and eliminate cancer cells,7,8 have improved oncologic outcomes for various cancers, including urothelial cancer.9-11 Before 2016, platinum-based chemotherapy was the mainstay for metastatic urothelial cancer management, but US Food and Drug Administration approval of 5 ICIs—nivolumab, pembrolizumab, avelumab, atezolizumab, and durvalumab—transformed treatment options.12Despite robust antitumor responses to ICIs, these medications are increasingly associated with immune-related adverse events (IRAEs), including DIBP, due to inhibition of negative regulators of immunity crucial for maintaining immunologic homeostasis.13,14 Up to 30% to 40% of patients treated with PD-1 inhibitors experience dermatologic complications, such as lichenoid reactions, eczema, vitiligo, and pruritus,15 and patients undergoing treatment with the PD-1 inhibitor pembrolizumab are estimated to be 2.6 times more likely to develop a rash than those receiving standard chemotherapy.16,17 The pathogenesis of DIBP involves autoreactive T-cell activation and subsequent autoantibody production against BP antigens.18 We present the case of DIBP secondary to pembrolizumab immunotherapy in a man with PD-L1–negative metastatic bladder cancer.
Case Report
An 81-year-old man with metastatic urothelial carcinoma presented to dermatology with a pruritic rash characterized by blisters of 5 months’ duration following treatment with pembrolizumab. He had a history of non–muscle invasive urothelial carcinoma and underwent intravesical bacillus Calmette-Guerin treatment. Thirty years later, after surveillance cystoscopies, the patient developed hematuria, which prompted pelvic ultrasonography and cystoscopy that revealed a tumor. Transurethral resection of the bladder tumor confirmed invasive, high-grade papillary urothelial carcinoma with vascular and muscle invasion (clinical stage T2NxMx). Due to elevated creatinine levels, neoadjuvant chemotherapy was contraindicated. Instead, the patient underwent cystoprostatectomy with ureteroileal conduit creation and pelvic lymphadenectomy one month later; final pathology revealed pT2aN0M0 disease with multifocal carcinoma in situ. At that time, there was no evidence of distant metastasis. Surveillance 5 months later identified pulmonary nodules that were confirmed as metastatic urothelial cancer by positron emission tomography/computed tomography (CT). The patient received 6 cycles of paclitaxel (175 mg/m² on day 1) and gemcitabine (1000 mg/m² on days 1 and 8 every 21 days), with progressive disease 16 months later. Despite 0% PD-L1 expression, pembrolizumab 400 mg intravenous (IV) treatment every 6 weeks was initiated 2 months later, and subsequent positron emission tomography/CT showed a positive response at 3 and 7 months after treatment initiation. After the patient’s sixth cycle of pembrolizumab, a generalized maculopapular rash involving approximately 50% of the body surface area led to discontinuation of pembrolizumab, initiation of multiple courses of prednisone and prednisolone, and a dermatology referral.
At the current presentation, the patient exhibited excoriated red patches on the abdomen, wrists, arms, upper chest, and legs (Figure 1). Tense blisters were observed on various areas, including the ear and arms. The provisional diagnosis was pembrolizumab-induced BP, supported by the clinical history, presentation, and an initial positive response to steroids. Treatment included topical triamcinolone 0.1% ointment and prednisone 40 mg daily. Biopsies revealed subepidermal blisters with underlying eosinophils on histopathology (Figure 2). Direct immunofluorescence showed strong linear basement membrane zone staining with IgG and C3, consistent with a diagnosis of BP.
One month later, the patient was given the first of two 1-g doses of rituximab, chosen as a treatment due to metastatic cancer history and ongoing severity of the DIBP. In addition, a slow prednisone taper was initiated. Atovaquone 1500 mg daily was ordered for Pneumocystis jirovecii prophylaxis. Following the first rituximab dose, the patient became clear of DIBP but required treatment for a chronic urinary tract infection, delaying the second rituximab dose. The prednisone taper continued, however, and the patient reported re-emergence of several blisters, followed by resolution of pruritus following the second rituximab dose. Bilateral pulmonary embolisms were noted on a restaging CT, attributed to the underlying malignancy and inflammation from DIBP. Doxycycline was initiated at 100 mg twice daily, and prednisone was slowly tapered (as tolerated by the patient’s symptoms) down to 2.5 mg daily approximately 6 months after rituximab initiation. The patient remains in clinical remission at last follow-up; however, considerations for further treatments have included intravenous immunoglobulin.
Comment
This case highlights major clinical challenges in the diagnosis and management of DIBP in a patient with metastatic urothelial carcinoma receiving ICI therapy. Our patient’s clinical course offers several high-yield lessons regarding diagnostic latency, treatment resistance, and a multidisciplinary approach to management.
Pruritus as a Precursor—Since an initial report in 2015, the emergence of DIBP postpembrolizumab has been well described in the literature.19-22 Pruritus is frequently the earliest symptom, preceding bullous eruption. Similar to our case—in which DIBP developed 30 weeks after pembrolizumab initiation—the classic clinical presentation and formation of bullae often are delayed, typically occurring 28 and 39 weeks.
Beyond Corticosteroids to Manage Refractory DIBP—Our patient’s DIBP persisted despite multiple interventions, including pembrolizumab discontinuation, corticosteroid therapy, and rituximab administration. Although cases of DIBP in pembrolizumab-treated metastatic urothelial carcinoma patients have been reported, they did not exhibit similar treatment resistance.23-25 As observed in our patient, immunotherapy discontinuation has been reported in at least 40% of all ICI-mediated cases of BP.14 Subsequent management involves low-dose oral corticosteroids and potent topical corticosteroids; the duration of steroid treatment varies widely, ranging from a few weeks to longer than 12 months, with no standardized approach.26 In cases where ICI withdrawal and corticosteroids fail to produce a complete response, monoclonal antibodies such as rituximab, dupilumab, and omalizumab have been used as alternative treatments, with dupilumab recently receiving US Food and Drug Administration approval for moderate to severe BP.27-31 These biologics selectively inhibit autoantibody formation and the inflammatory cascade, and research has pointed toward them as safe and effective options for refractory BP. Although robust randomized, controlled clinical trials on rituximab for DIBP still are lacking, prospective and retrospective cohort studies have shown promising results, including complete remission rates of 67% to 90%, along with a decline in circulating BP180-specific B lymphocytes, anti-BP180 IgG, and the expression of proinflammatory IL-15 and IL-6.32
Despite receiving 2 doses of rituximab, our patient experienced recurrence of blisters when prednisone was tapered, prompting discussions about alternative tapering timelines and additional therapies such as doxycycline33 or intravenous immunoglobulin,34 which have emerged as steroid-sparing agents for BP following initial steroid therapy.
Systemic Barriers and the Need for Multidisciplinary Care—This case underscores systemic barriers within the health care system that impede prompt diagnosis and management of conditions such as DIBP. The 5-month delay between the patient’s referral to dermatology and the actual consultation, potentially due to shortages of dermatologists, highlights the need for more systematic urgent dermatologic referrals and streamlined diagnostic pathways in suspected cases of IRAEs. Diagnosis requires comprehensive evaluation, including skin biopsy for histopathologic examination and immunofluorescence studies. Ruling out alternative blistering disorders, such as epidermolysis bullosa acquisita, is crucial before confirming a BP diagnosis. Encouraging direct communication between referring physicians and consultants often can expedite the process, as a call from the referring physician can alert the consultant and speed up scheduling. Notably, the patient’s daughter, who was a patient of the dermatologist herself, played a crucial role in advocating for the dermatology referral. Although this should not be necessary, it highlights the pivotal role families can play in ensuring timely access to specialized care for challenging conditions such as BP.
Lastly, the refractory nature of the patient’s condition, coupled with concurrent chronic urinary tract infection and bilateral pulmonary embolisms, emphasizes the necessity of multidisciplinary collaboration among oncology, dermatology, and primary care in managing DIBP. Consulting experts on IRAEs and coordinating with the oncologist were essential for making informed treatment decisions and facilitating the timely exchange of clinical information.
Conclusion
This case underscores the importance of timely recognition and diagnosis of DIBP in patients undergoing ICI therapy but also highlights the need for individualized treatment approaches and multidisciplinary collaboration when managing adverse cutaneous reactions.
- Schmidt E, Zillikens D. Pemphigoid diseases. Lancet. 2013;381:320-332.
- Nishie W. Update on the pathogenesis of bullous pemphigoid: an autoantibody-mediated blistering disease targeting collagen XVII. J Dermatol Sci. 2014;73:179-186.
- Sárdy M, Kostaki D, Varga R, et al. Comparative study of direct and indirect immunofluorescence and of bullous pemphigoid 180 and 230 enzyme-linked immunosorbent assays for diagnosis of bullous pemphigoid. J Am Acad Dermatol. 2013;69:748-753.
- Smith EP, Taylor TB, Meyer LJ, et al. Antigen identification in drug-induced bullous pemphigoid. J Am Acad Dermatol. 1993;29(5 Pt 2):879-882.
- Siegel J, Totonchy M, Damsky W, et al. Bullous disorders associated with anti-PD-1 and anti-PD-L1 therapy: a retrospective analysis evaluating the clinical and histopathologic features, frequency, and impact on cancer therapy. J Am Acad Dermatol. 2018;79:1081-1088.
- Asdourian MS, Shah N, Jacoby TV, et al. Association of bullous pemphigoid with immune checkpoint inhibitor therapy in patients with cancer: a systematic review. JAMA Dermatol. 2022;158:933-941.
- Pardoll DM. The blockade of immune checkpoints in cancer immunotherapy. Nat Rev Cancer. 2012;12:252-264.
- Dunn GP, Bruce AT, Ikeda H, et al. Cancer immunoediting: from immunosurveillance to tumor escape. Nat Immunol. 2002;3:991-998.
- Powles T, Eder JP, Fine GD, et al. MPDL3280A (anti-PD-L1) treatment leads to clinical activity in metastatic bladder cancer. Nature. 2014;515:558-562.
- Bellmunt J, de Wit R, Vaughn DJ, et al. Pembrolizumab as second-line therapy for advanced urothelial carcinoma. N Engl J Med. 2017;376:1015-1026.
- Fradet Y, Bellmunt J, Vaughn DJ, et al. Randomized phase III KEYNOTE-045 trial of pembrolizumab versus paclitaxel, docetaxel, or vinflunine in recurrent advanced urothelial cancer: results of >2 years of follow-up. Ann Oncol. 2019;30:970-976.
- Felsenstein KM, Theodorescu D. Precision medicine for urothelial bladder cancer: update on tumour genomics and immunotherapy. Nat Rev Urol. 2018;15:92-111.
- Sibaud V. Dermatologic reactions to immune checkpoint inhibitors: skin toxicities and immunotherapy. Am J Clin Dermatol. 2018;19:345-361.
- Lopez AT, Khanna T, Antonov N, et al. A review of bullous pemphigoid associated with PD-1 and PD-L1 inhibitors. Int J Dermatol. 2018;57:664-669.
- Hwang SJE, Carlos G, Wakade D, et al. Cutaneous adverse events (AEs) of anti-programmed cell death (PD)-1 therapy in patients with metastatic melanoma: a single-institution cohort. J Am Acad Dermatol. 2016;74:455-461.e1.
- Belum VR, Benhuri B, Postow MA, et al. Characterisation and management of dermatologic adverse events to agents targeting the PD-1 receptor. Eur J Cancer. 2016;60:12-25.
- Naidoo J, Page DB, Li BT, et al. Toxicities of the anti-PD-1 and anti-PD-L1 immune checkpoint antibodies. Ann Oncol. 2015;26:2375-2391.
- Weber JS, Yang JC, Atkins MB, et al. Toxicities of immunotherapy for the practitioner. J Clin Oncol. 2015;33:2092-2099.
- Carlos G, Anforth R, Chou S, et al. A case of bullous pemphigoid in a patient with metastatic melanoma treated with pembrolizumab. Melanoma Res. 2015;25:265-268.
- Adachi E, Honda T, Nonoyama S, al. Severe bullous pemphigoid in a metastatic lung cancer patient treated with pembrolizumab. J Dermatol. 2019;46:E232-E233.
- Cardona AF, Ruiz-Patiño A, Zatarain-Barron ZL, et al. Refractory bullous pemphigoid in a patient with metastatic lung adenocarcinoma treated with pembrolizumab. Case Rep Oncol. 2021;14:386-390.
- Sun CW, Grossman SK, Aphale A, et al. Pembrolizumab-induced bullous pemphigoid. JAAD Case Rep. 2019;5:362-364.
- Correia C, Fernandes S, Soares-de-Almeida L, et al. Bullous pemphigoid probably associated with pembrolizumab: a case of delayed toxicity. Int J Dermatol. 2022;61:E129-E131.
- Shalata W, Weissmann S, Itzhaki Gabay S, et al. A retrospective, single-institution experience of bullous pemphigoid as an adverse effect of immune checkpoint inhibitors. Cancers. 2022;14:5451. doi:10.3390/cancers14215451
- Garje R, Chau JJ, Chung J, et al. Acute flare of bullous pemphigus with pembrolizumab used for treatment of metastatic urothelial cancer. J Immunother. 2018;41:42-44.
- Wang J, Hu X, Jiang W, et al. Analysis of the clinical characteristics of pembrolizumab-induced bullous pemphigoid. Front Oncol. 2023;13:1095694.
- Thomas RM, Colon A, Motaparthi K. Rituximab in autoimmune pemphigoid diseases: indications, optimized regimens, and practice gaps. Clin Dermatol. 2020;38:384-396.
- Sowerby L, Dewan AK, Granter S, et al. Rituximab treatment of nivolumab-induced bullous pemphigoid. JAMA Dermatol. 2017;153:603-605.
- Sharma P, Barnes M, Nabeel S, et al. Pembrolizumab-induced bullous pemphigoid treated with rituximab. JCO Oncol Pract. 2020;16:764-766.
- Abdat R, Waldman RA, de Bedout V, et al. Dupilumab as a novel therapy for bullous pemphigoid: a multicenter case series. J Am Acad Dermatol. 2020;83:46-52.
- Cao P, Xu W, Zhang L. Rituximab, omalizumab, and dupilumab treatment outcomes in bullous pemphigoid: a systematic review. Front Immunol. 2022;13:928621.
- Karakioulaki M, Eyerich K, Patsatsi A. Advancements in bullous pemphigoid treatment: a comprehensive pipeline update. Am J Clin Dermatol. 2024;25:195-212.
- Jin XX, Wang X, Shan Y, et al. Efficacy and safety of tetracyclines for pemphigoid: a systematic review and meta-analysis. Arch Dermatol Res. 2022;314:191-201.
- Kianfar N, Dasdar S, Daneshpazhooh M, et al. A systematic review on efficacy, safety and treatment durability of intravenous immunoglobulin in autoimmune bullous dermatoses: special focus on indication and combination therapy. Exp Dermatol. 2023;32:934-944.
- Schmidt E, Zillikens D. Pemphigoid diseases. Lancet. 2013;381:320-332.
- Nishie W. Update on the pathogenesis of bullous pemphigoid: an autoantibody-mediated blistering disease targeting collagen XVII. J Dermatol Sci. 2014;73:179-186.
- Sárdy M, Kostaki D, Varga R, et al. Comparative study of direct and indirect immunofluorescence and of bullous pemphigoid 180 and 230 enzyme-linked immunosorbent assays for diagnosis of bullous pemphigoid. J Am Acad Dermatol. 2013;69:748-753.
- Smith EP, Taylor TB, Meyer LJ, et al. Antigen identification in drug-induced bullous pemphigoid. J Am Acad Dermatol. 1993;29(5 Pt 2):879-882.
- Siegel J, Totonchy M, Damsky W, et al. Bullous disorders associated with anti-PD-1 and anti-PD-L1 therapy: a retrospective analysis evaluating the clinical and histopathologic features, frequency, and impact on cancer therapy. J Am Acad Dermatol. 2018;79:1081-1088.
- Asdourian MS, Shah N, Jacoby TV, et al. Association of bullous pemphigoid with immune checkpoint inhibitor therapy in patients with cancer: a systematic review. JAMA Dermatol. 2022;158:933-941.
- Pardoll DM. The blockade of immune checkpoints in cancer immunotherapy. Nat Rev Cancer. 2012;12:252-264.
- Dunn GP, Bruce AT, Ikeda H, et al. Cancer immunoediting: from immunosurveillance to tumor escape. Nat Immunol. 2002;3:991-998.
- Powles T, Eder JP, Fine GD, et al. MPDL3280A (anti-PD-L1) treatment leads to clinical activity in metastatic bladder cancer. Nature. 2014;515:558-562.
- Bellmunt J, de Wit R, Vaughn DJ, et al. Pembrolizumab as second-line therapy for advanced urothelial carcinoma. N Engl J Med. 2017;376:1015-1026.
- Fradet Y, Bellmunt J, Vaughn DJ, et al. Randomized phase III KEYNOTE-045 trial of pembrolizumab versus paclitaxel, docetaxel, or vinflunine in recurrent advanced urothelial cancer: results of >2 years of follow-up. Ann Oncol. 2019;30:970-976.
- Felsenstein KM, Theodorescu D. Precision medicine for urothelial bladder cancer: update on tumour genomics and immunotherapy. Nat Rev Urol. 2018;15:92-111.
- Sibaud V. Dermatologic reactions to immune checkpoint inhibitors: skin toxicities and immunotherapy. Am J Clin Dermatol. 2018;19:345-361.
- Lopez AT, Khanna T, Antonov N, et al. A review of bullous pemphigoid associated with PD-1 and PD-L1 inhibitors. Int J Dermatol. 2018;57:664-669.
- Hwang SJE, Carlos G, Wakade D, et al. Cutaneous adverse events (AEs) of anti-programmed cell death (PD)-1 therapy in patients with metastatic melanoma: a single-institution cohort. J Am Acad Dermatol. 2016;74:455-461.e1.
- Belum VR, Benhuri B, Postow MA, et al. Characterisation and management of dermatologic adverse events to agents targeting the PD-1 receptor. Eur J Cancer. 2016;60:12-25.
- Naidoo J, Page DB, Li BT, et al. Toxicities of the anti-PD-1 and anti-PD-L1 immune checkpoint antibodies. Ann Oncol. 2015;26:2375-2391.
- Weber JS, Yang JC, Atkins MB, et al. Toxicities of immunotherapy for the practitioner. J Clin Oncol. 2015;33:2092-2099.
- Carlos G, Anforth R, Chou S, et al. A case of bullous pemphigoid in a patient with metastatic melanoma treated with pembrolizumab. Melanoma Res. 2015;25:265-268.
- Adachi E, Honda T, Nonoyama S, al. Severe bullous pemphigoid in a metastatic lung cancer patient treated with pembrolizumab. J Dermatol. 2019;46:E232-E233.
- Cardona AF, Ruiz-Patiño A, Zatarain-Barron ZL, et al. Refractory bullous pemphigoid in a patient with metastatic lung adenocarcinoma treated with pembrolizumab. Case Rep Oncol. 2021;14:386-390.
- Sun CW, Grossman SK, Aphale A, et al. Pembrolizumab-induced bullous pemphigoid. JAAD Case Rep. 2019;5:362-364.
- Correia C, Fernandes S, Soares-de-Almeida L, et al. Bullous pemphigoid probably associated with pembrolizumab: a case of delayed toxicity. Int J Dermatol. 2022;61:E129-E131.
- Shalata W, Weissmann S, Itzhaki Gabay S, et al. A retrospective, single-institution experience of bullous pemphigoid as an adverse effect of immune checkpoint inhibitors. Cancers. 2022;14:5451. doi:10.3390/cancers14215451
- Garje R, Chau JJ, Chung J, et al. Acute flare of bullous pemphigus with pembrolizumab used for treatment of metastatic urothelial cancer. J Immunother. 2018;41:42-44.
- Wang J, Hu X, Jiang W, et al. Analysis of the clinical characteristics of pembrolizumab-induced bullous pemphigoid. Front Oncol. 2023;13:1095694.
- Thomas RM, Colon A, Motaparthi K. Rituximab in autoimmune pemphigoid diseases: indications, optimized regimens, and practice gaps. Clin Dermatol. 2020;38:384-396.
- Sowerby L, Dewan AK, Granter S, et al. Rituximab treatment of nivolumab-induced bullous pemphigoid. JAMA Dermatol. 2017;153:603-605.
- Sharma P, Barnes M, Nabeel S, et al. Pembrolizumab-induced bullous pemphigoid treated with rituximab. JCO Oncol Pract. 2020;16:764-766.
- Abdat R, Waldman RA, de Bedout V, et al. Dupilumab as a novel therapy for bullous pemphigoid: a multicenter case series. J Am Acad Dermatol. 2020;83:46-52.
- Cao P, Xu W, Zhang L. Rituximab, omalizumab, and dupilumab treatment outcomes in bullous pemphigoid: a systematic review. Front Immunol. 2022;13:928621.
- Karakioulaki M, Eyerich K, Patsatsi A. Advancements in bullous pemphigoid treatment: a comprehensive pipeline update. Am J Clin Dermatol. 2024;25:195-212.
- Jin XX, Wang X, Shan Y, et al. Efficacy and safety of tetracyclines for pemphigoid: a systematic review and meta-analysis. Arch Dermatol Res. 2022;314:191-201.
- Kianfar N, Dasdar S, Daneshpazhooh M, et al. A systematic review on efficacy, safety and treatment durability of intravenous immunoglobulin in autoimmune bullous dermatoses: special focus on indication and combination therapy. Exp Dermatol. 2023;32:934-944.
Pembrolizumab-Induced Bullous Pemphigoid: Navigating Diagnostic Challenges and Treatment Resistance
Pembrolizumab-Induced Bullous Pemphigoid: Navigating Diagnostic Challenges and Treatment Resistance
Practice Points
- Suspect bullous pemphigoid (BP) in patients receiving immune checkpoint inhibitors (ICIs) with new-onset pruritus or dermatologic lesions; blisters may be delayed for months.
- Treatment-resistant cases of drug-induced BP warrant consideration of alternative therapies, including rituximab, doxycycline, or intravenous immunoglobulin.
- Multidisciplinary management with dermatology and oncology is essential, as immune-related effects may persist even after ICI discontinuation.
- Encourage patients to report new skin changes promptly to their primary care physician to allow for early intervention.

Cemiplimab for Unresectable Cutaneous Squamous Cell Carcinoma: Experience From a Tertiary Center
Cemiplimab for Unresectable Cutaneous Squamous Cell Carcinoma: Experience From a Tertiary Center
Cutaneous squamous cell carcinoma (cSCC) is the second most prevalent skin cancer and ranks sixth in prevalence among all cancers in the United Kingdom.1,2 The etiologic factors underlying cSCC are well established, with major efforts undertaken by governments and public health organizations over the past 2 decades to increase public awareness globally. Known risk factors for cSCC include chronic exposure to UV radiation, radiotherapy, chemical injury, and immunosuppression. The first 3 risk factors amplify risk by increasing accumulation of abnormal gene mutations. Immunosuppression hampers the immune system’s ability to eradicate cells bearing malignant genetic aberrations. Notable gene mutations implicated in cSCC include p53, p16, telomerase reverse transcriptase, NOTCH1, ROS1, mitogen-activated protein kinases, forkhead box M1, and cyclooxygenase 2, in addition to matrix metalloproteinases, which are most commonly associated with Marjolin ulcers.3
The incidence of cSCC continues to surge worldwide,3,4 with more patients presenting with advanced stages of disease and a notable increase in those presenting with unresectable cSCC due to either locally advanced disease or distant metastases.5 Existing therapies for cSCC include surgical excision (including Mohs micrographic surgery); radiotherapy (indicated for cosmetic reasons, locally advanced disease, and/or patient factors); and systemic treatments, encompassing chemotherapy (eg, 5-fluorouracil), and epidermal growth factor receptor inhibitors (indicated locally advanced disease or distant metastases).4
In recent years, immunotherapy has emerged as a potent and effective treatment modality for unresectable cSCC, both locally advanced and metastatic. The success of immunotherapy in cSCC treatment can be attributed to the unique tumor microenvironment of cSCC, which is characterized by high tumor mutational burden, increased density of tumor-infiltrating lymphocytes (TILs), and heightened programmed cell death ligand 1 (PD-L1) expression on neoplastic cells. The elevated TIL density enables a robust immune response, rendering checkpoint inhibitors particularly effective. Greater tumor mutational burden further augments this enhanced TIL activity, amplifying the response to checkpoint inhibitors. Additionally, heightened PD-L1 expression facilitates more effective unmasking by checkpoint inhibitors, thereby enhancing the immune response.6
Cemiplimab is a programmed cell death protein 1/PD-L1 that was approved by the US Food and Drug Administration in September 2018 for treatment of cSCC. It also gained a European Union endorsement in June 2019 and National Institute for Health and Care Excellence approval in August 2019 based on the highly promising results of a phase 2 trial that involved only 59 adult patients with metastatic cSCC.7 The trial reported an overall response rate (ORR) of 47%, durable disease control in 61% of patients, a median time to response of 1.9 months, and response duration exceeding 6 months in 57% of patients. The phase 2 trials reported an estimated 12-month progression-free survival (PFS) of 53% and an estimated 12-month overall survival (OS) of 81%.7
Despite the noteworthy response statistics demonstrated by these studies, it is imperative to recognize that immunotherapies, while potent, are not without challenges. They can precipitate severe immune-related adverse events (AEs), including myocarditis, adrenal failure, and pneumonitis, which can negatively impact patient health outcomes and lead to early treatment cessation. The initial trials reported high-grade AEs such as pneumonitis, pleural effusion, and, notably 11 total deaths, with 8 (72.7%) attributed to disease progression and 3 (27.3%) to AEs.7 Additionally, cost and access to immunotherapy are inherent limitations of the treatment; immunotherapy agents are expensive, and not all centers or patients are able to access them.
The aim of this study was to assess the efficacy of cemiplimab in patients with inoperable cSCC, including locally advanced and metastatic disease, treated at a tertiary referral center in the United Kingdom, and to compare outcomes with the pivotal phase 2 trial that supported regulatory approval of cemiplimab.7 The primary objective was ORR, with secondary objectives including PFS, OS, and AEs.
Methods
The patients included in this study had unresectable cSCC and therefore were not candidates for surgery or radiotherapy. Patient demographics are presented in Table 1. The main indications for cemiplimab in place of surgery or radiotherapy included local recurrence, locally advanced disease involving deep structures, advanced nodal disease, and distant metastatic disease. Patients meeting these criteria and the following inclusion criteria for cemiplimab treatment from November 2018 through March 2023 at a single tertiary referral center were included in the study:
- Age 18 years or older
- Histologically confirmed cSCC with locoregional recurrence after surgery or radiotherapy, or histologically confirmed advanced or metastatic disease deemed to be inoperable
- Eastern Cooperative Oncology Group performance status of 0 to 2
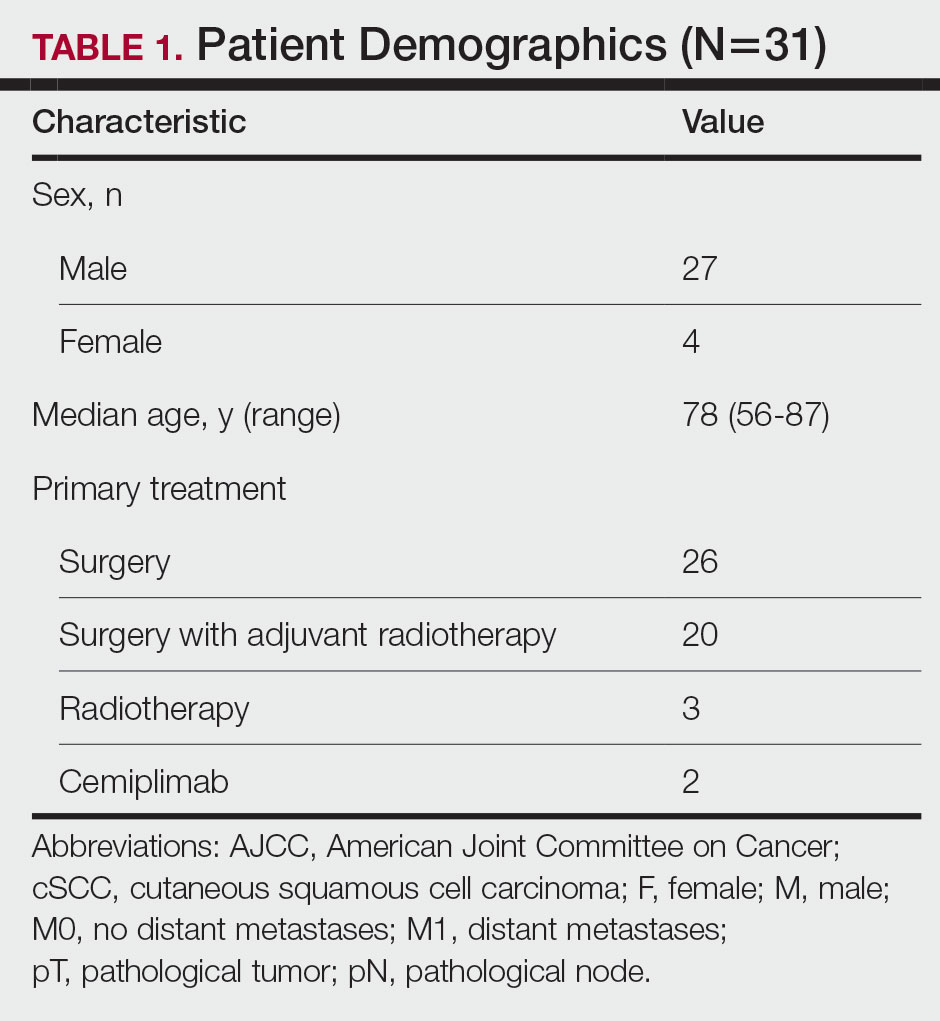
All enrolled patients received intravenous infusions of cemiplimab 3 times weekly at a dosage of 350 mg. Treatment was continued until complete response, unacceptable toxicity, or disease progression, with a maximum duration of 2 years or 35 cycles. Patients underwent regular follow-up, typically 3 weeks preceding each treatment cycle. Monitoring adhered to the Common Terminology Criteria for Adverse Events, version 4.0, as outlined by the National Cancer Institute.8 Response to treatment was reported according to the guidelines stipulated by the Response Evaluation Criteria in Solid Tumours, version 1.1.9 Written informed consent was obtained for all patients.
Comprehensive patient demographics, histologic profiles, and clinical data were meticulously captured on a retrospective basis. The primary objective centered on elucidating the ORR. Secondary objectives encompassed evaluating PFS, OS, and a comprehensive analysis of AEs. Progression-free survival and OS were calculated by generating Kaplan-Meier curves using Python 3.9 (Python Software Foundation).
Results
Patient Characteristics—From November 2018 through March 2023, a cohort of 31 patients with inoperable cSCC underwent treatment with cemiplimab at our tertiary referral center. The median duration of follow-up was 13 months. Clinical characteristics are outlined in the Table 2. Four (12.9%) patients successfully completed the full 2-year treatment course. Nine (29.0%) continued to receive cemiplimab therapy at the conclusion of this study in March 2023, with treatment courses ranging from 2 to 11 months since initiation. Ten (32.3%) patients discontinued treatment due to AEs, while 5 (16.1%) regrettably ceased treatment due to mortality. Two (6.5%) patients terminated treatment due to the COVID-19 pandemic, and 1 (3.2%) discontinued treatment as a result of disease progression.
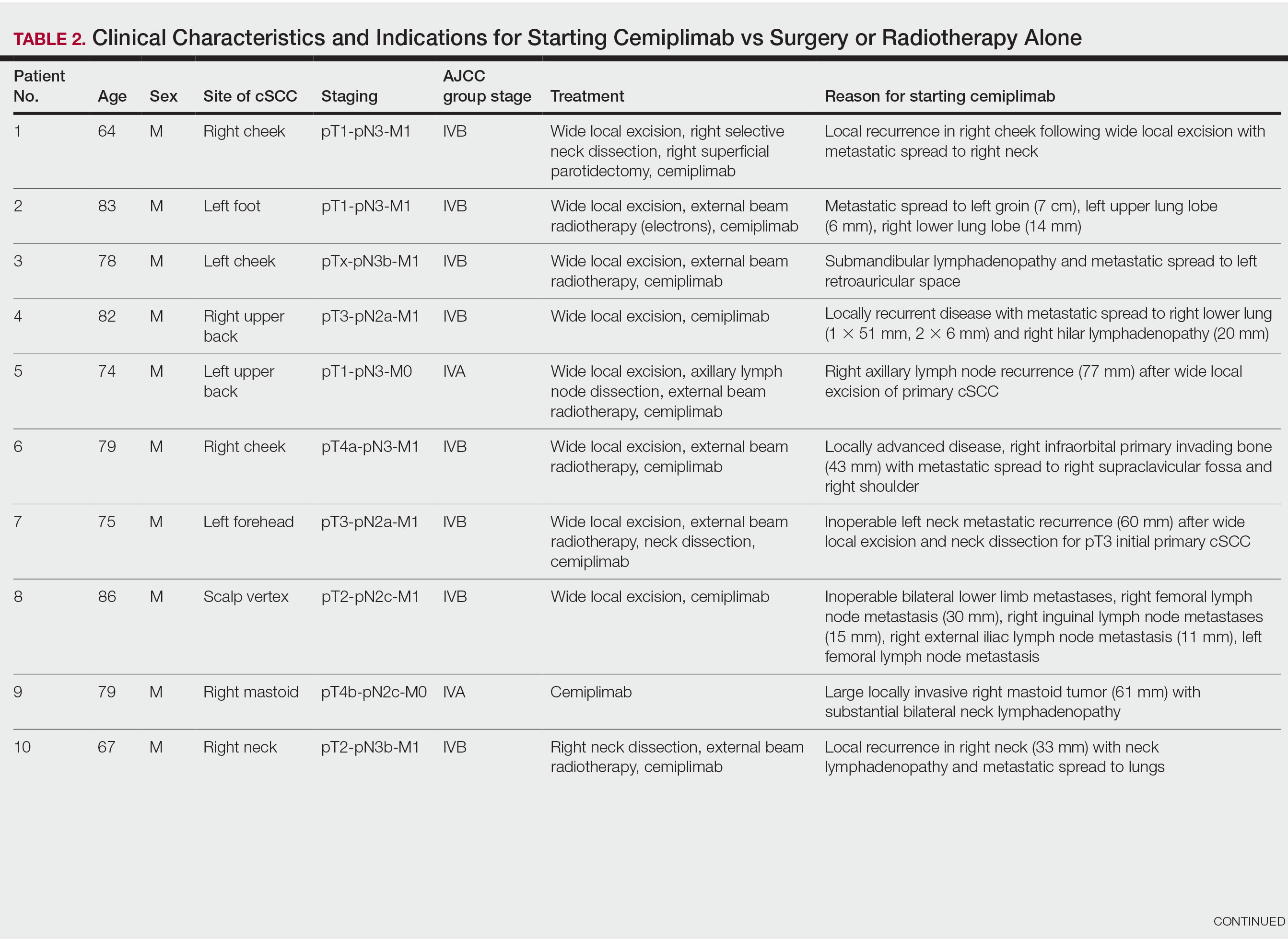
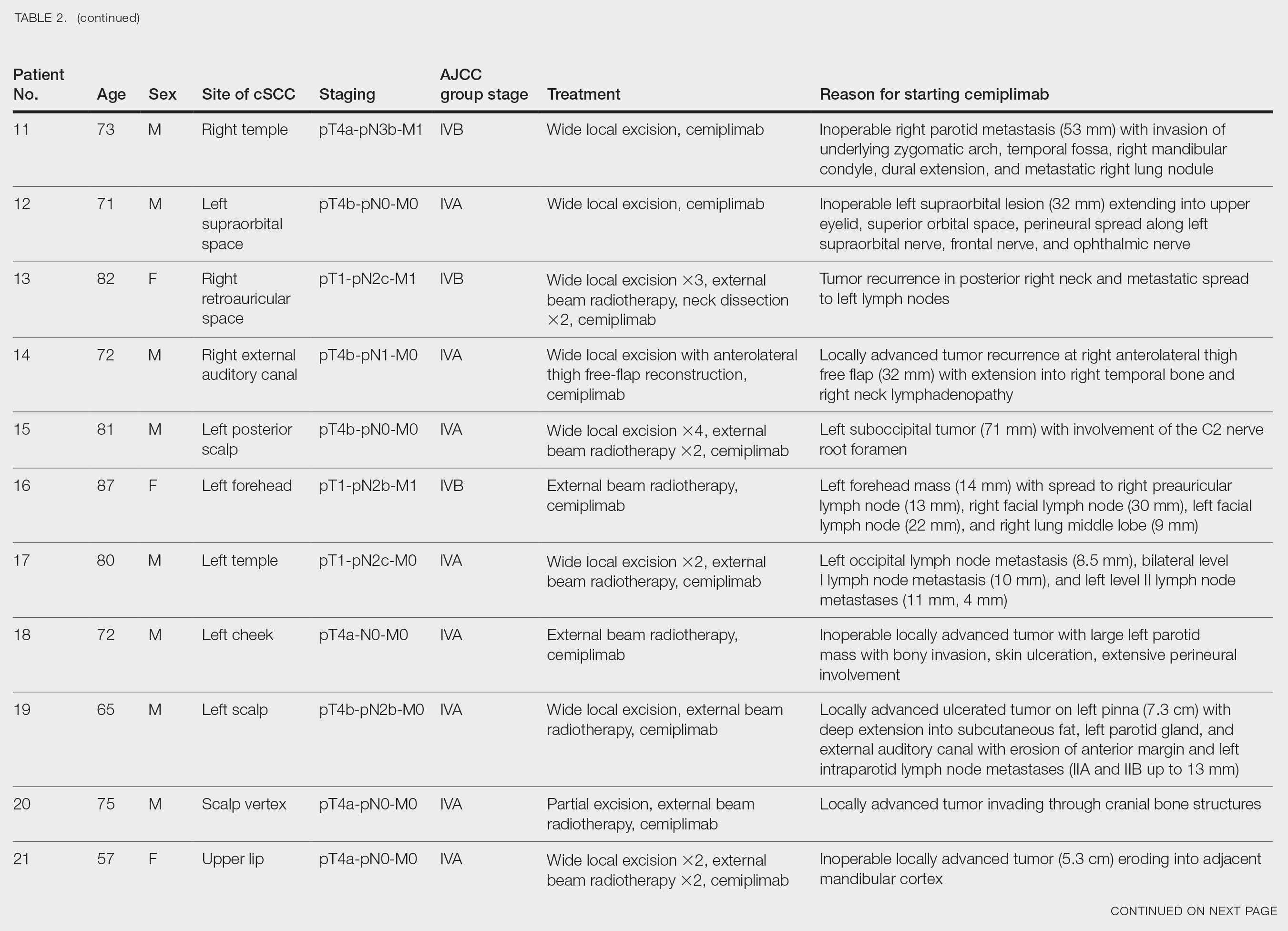
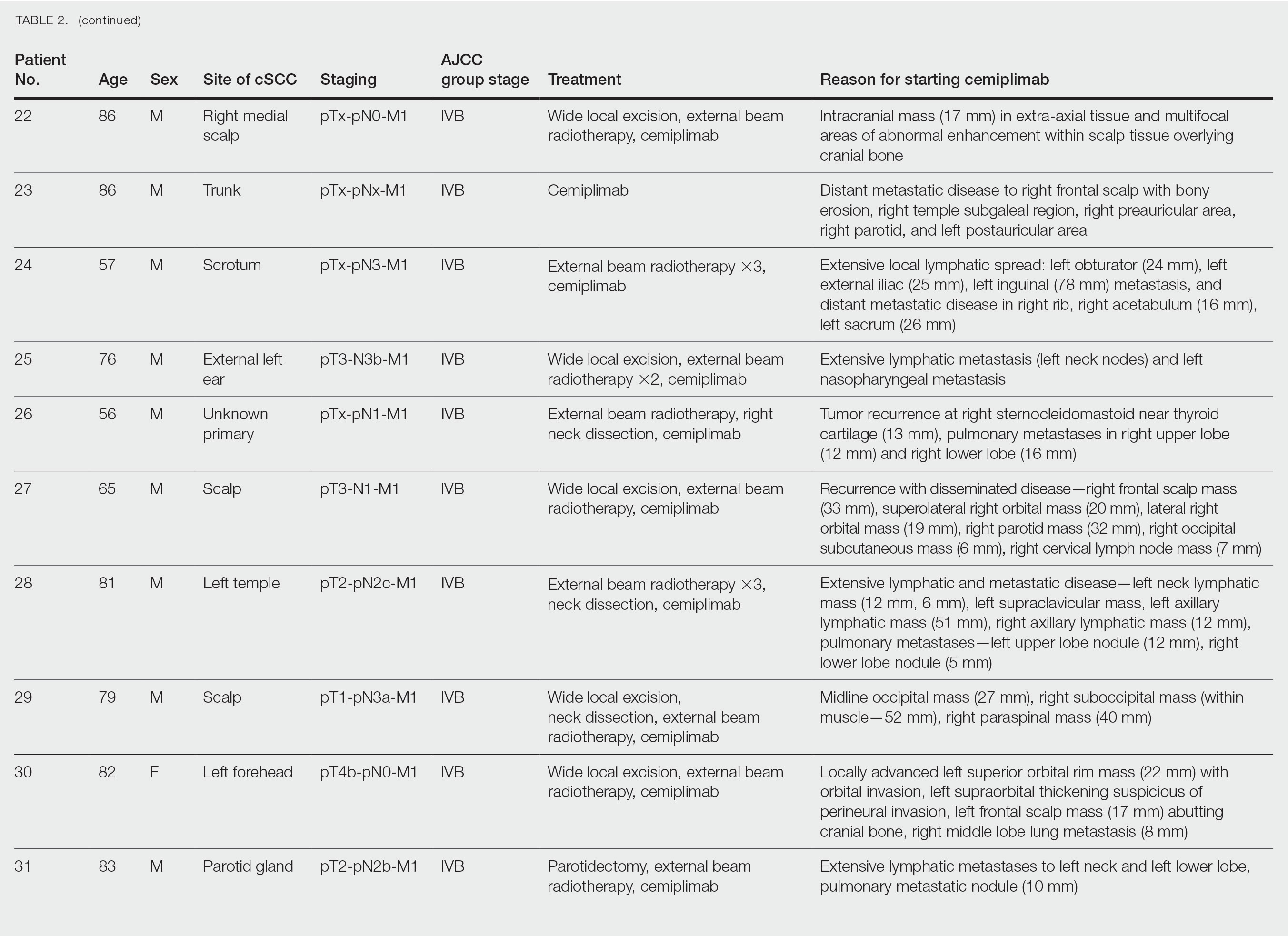
Clinical Efficacy—Of the 31 enrolled patients, a substantial proportion experienced positive clinical outcomes, with 20 (64.5%) achieving complete response and 6 (19.4%) achieving partial response. A total of 26 patients achieved a response on cemiplimab, with an ORR of 83.9% (95% CI, 66.3%-94.6%). Regrettably, 2 (6.5%) patients experienced disease progression, while 3 (9.7%) died before response to cemiplimab could be assessed. Following a median follow-up period of 13 months, the median PFS and OS remained unreached, emphasizing the efficacy of cemiplimab in treating inoperable cSCC (Figures 1 and 2).
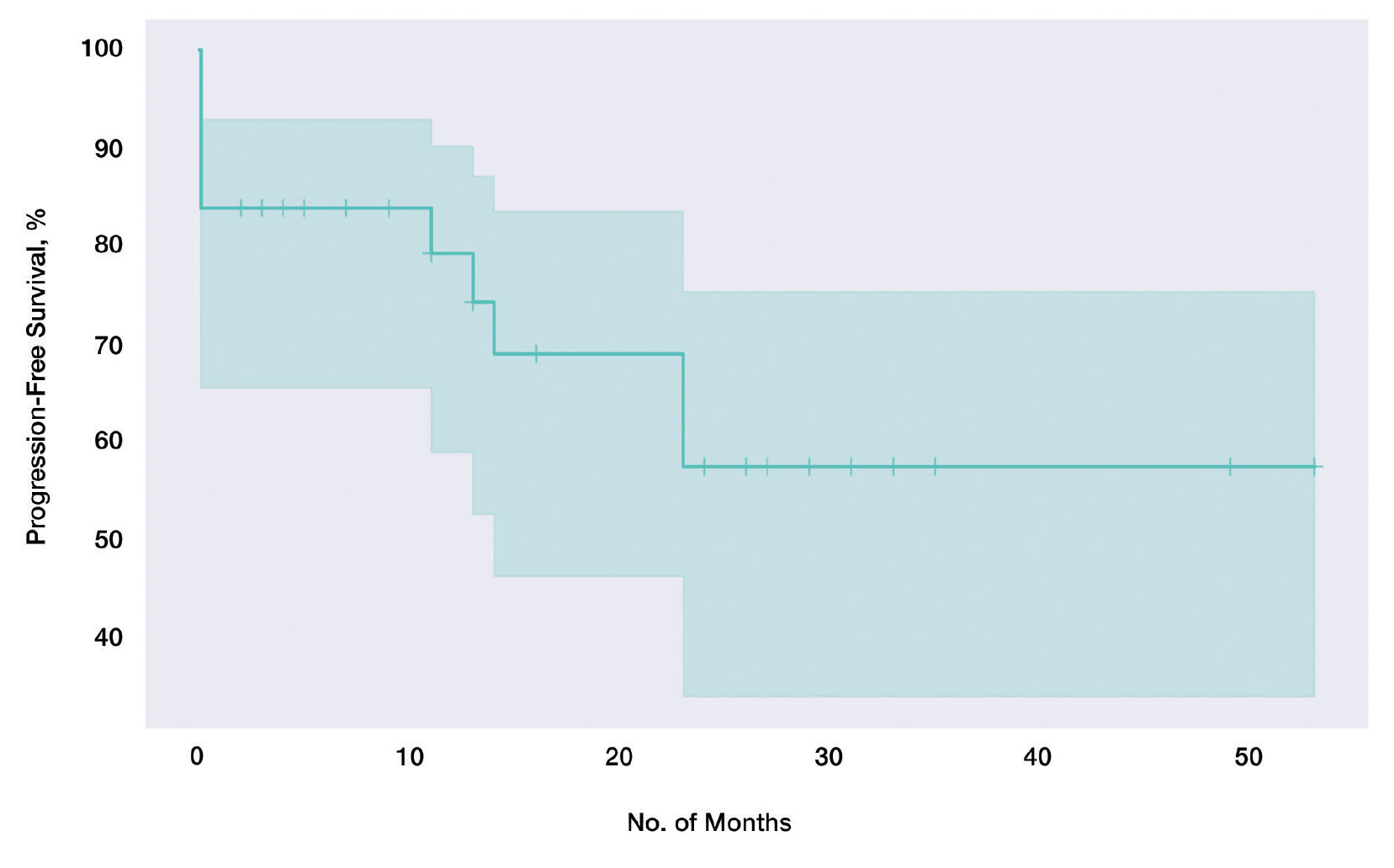
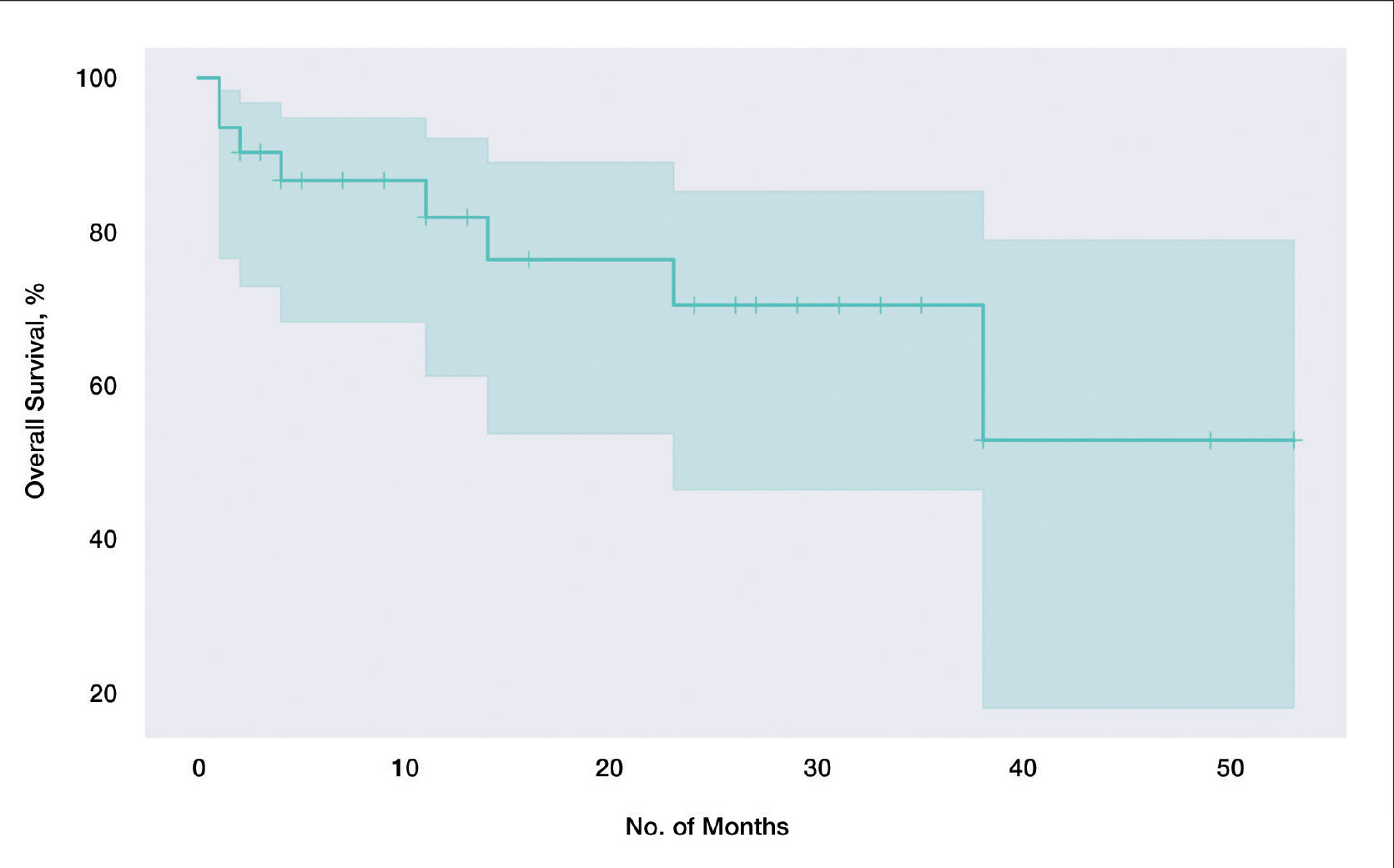
In our cohort, 2-year PFS was 57.5% (95% CI, 33.9%-75.5%) with cemiplimab and 2-year OS was 70.6% (95% CI, 46.5%-85.4%). For PFS, we observed the steepest drops at onset and at the 23-month mark (Figure 1), while for OS we observed the steepest drop at the 38-month mark (Figure 2). Clinically, we observed cemiplimab causing near-complete regression of previously large, ulcerating, fungating cSCC in patients who responded to cemiplimab, mirroring results seen elsewhere.7
Adverse Events and Treatment Cessation—A substantial proportion of patients (24/31 [77.4%]) reported AEs during treatment. Notably, treatment discontinuation was necessary in 10 (32.3%) patients due to a range of AEs, including myocarditis, atrial flutter, pneumonitis, nephritis, derangement of liver function tests, and arthritis. Additional relevant side effects included adrenal insufficiency (3/31 [9.7%]), fatigue (3/31 [9.7%]), diarrhea (2/31 [6.5%]), and type 1 diabetes 1/31 [3.2%]). These outcomes emphasize the importance of vigilance and monitoring when administering cemiplimab in the context of advanced cSCC.
Comment
Historically, advanced cSCC has had a bleak prognosis. The nature of the disease generally meant these patients could not be operated on due to metastatic spread or local invasion, and radiotherapy was not curative. The only option remaining was palliation, but new therapies have shown promise due to specific inherent characteristics of advanced cSCC; for example, the characteristic high mutation burden prevalent in advanced cSCC has paved the way for the emergence of immunotherapy as a promising avenue for intervention.10 Cemiplimab in particular has emerged as a feasible treatment for patients who would otherwise be confined to palliation. Our findings derived from a local cohort reinforce this notion, with a remarkable 83.9% (26/31) exhibiting a favorable response to cemiplimab. Although this local sample of 31 patients is small in absolute terms, in the context of the trial with 59 participants7 that gained global approval for the use of cemiplimab, our study adds a substantial amount of data to the growing body of evidence on the long-term efficacy of cemiplimab. Notably, our results emphasize the potential applicability of cemiplimab among elderly patients and individuals with lower performance statuses: populations historically excluded from immunotherapeutic considerations.
Immunotherapeutic AEs and Tolerance—As anticipated with immunotherapeutic agents, cemiplimab is associated with AEs that also are seen in its counterparts.11 A total of 77.4% (24/31) of our cohort reported immune-related AEs, although the severity warranted treatment discontinuation in only 10 (10/24 [41.7%]) patients, representing less than half of those who encountered side effects and less than a third of the entire cohort. Furthermore, most of these immune-related AEs were managed effectively with short courses of oral steroids, further substantiating the notion that cemiplimab is generally well tolerated across patients of diverse performance statuses. Even for patients who discontinued treatment early due to immune-related side effects, benefits persisted despite the partial course of cemiplimab. Of the 10 patients who discontinued treatment due to immune AEs, 6 (60%) demonstrated stable complete response, 2 (20%) experienced relapse after stopping cemiplimab, and 2 (20%) demonstrated a partial response with stable disease.
Challenges in the Most Vulnerable Patient—Of the 5 recorded mortalities, 2 (40%) were attributed to disease progression, while 3 (60%) occurred before response assessment could be undertaken. The 3 patients who died prior to response evaluation were among the most medically fragile in the cohort, characterized by extensive metastatic cSCC and major comorbidities that, in isolation, posed life-threatening risks. For individuals grappling with widespread metastatic cSCC and substantial life-threatening comorbidities, it is plausible that the necessary physiologic resilience necessary for cemiplimab therapy may be absent. We hypothesize that an immune reconstitution syndrome–like response may be responsible for this early mortality, and these patients may lack the necessary physiological resilience to tolerate this response. This subset of patients warrants careful consideration when considering therapy with cemiplimab.
Conclusion
In summary, our results underscore the efficacy of cemiplimab, as it supported a response in more than three-quarters of our patient cohort. Additionally, the associated AEs, similar to those with other programmed cell death protein 1 inhibitors, generally were manageable with medical intervention. Our findings corroborate earlier studies that have demonstrated the therapeutic potential of cemiplimab in advanced, inoperable cSCC management. In addition to efficacy, our results also suggest that cemiplimab holds promise as a therapeutic option for patients who might not be amenable to the stresses of general anesthesia, surgery, or prolonged hospitalization, although cemiplimab should likely be used with caution in patients with severe, life-threatening medical comorbidities and/or concurrent severe illness. Furthermore, our data demonstrate that the benefits persist not only beyond the completion of the full 2-year course, but also after partial treatment courses discontinued due to patient-specific factors. Future studies would be useful to better understand and optimize dose and duration of cemiplimab treatment to maximize therapeutic effectiveness while minimizing risk of immune-related AEs. Among individuals confronting advanced, inoperable cSCC, cemiplimab is emerging as a viable and beneficial intervention.
- Waldman A, Schmults C. Cutaneous squamous cell carcinoma. Hematol Oncol Clin North Am. 2019;33:1-12. doi:10.1016/j.hoc.2018.08.001
- Venables ZC, Nijsten T, Wong KF, et al. Epidemiology of basal and cutaneous squamous cell carcinoma in the U.K. 2013–15: a cohort study. Br J Dermatol. 2019;181:474-482. doi:10.1111/bjd.17873
- Que SKT, Zwald FO, Schmults CD. Cutaneous squamous cell carcinoma. J Am Acad Dermatol. 2018;78:237-247. doi:10.1016/j.jaad.2017.08.059
- Green AC, Olsen CM. Cutaneous squamous cell carcinoma: an epidemiological review. Br J Dermatol. 2017;177:373-381. doi:10.1111/bjd.15324
- Jovic’ M, Marinkovic’ M, Sud‐ecki B, et al. COVID-19 and cutaneous squamous cell carcinoma—impact of the pandemic on unequal access to healthcare. Healthcare (Basel). 2023;11:1994. doi:10.3390/healthcare11141994
- Ansary TM, Hossain MDR, Komine M, et al. Immunotherapy for the treatment of squamous cell carcinoma: potential benefits and challenges. Int J Mol Sci. 2022;23:8530. doi:10.3390/ijms23158530
- Migden MR, Rischin D, Schmults CD, et al. PD-1 blockade with cemiplimab in advanced cutaneous squamous-cell carcinoma. N Engl J Med. 2018;379:341-351. doi:10.1056/nejmoa1805131
- National Cancer Institute. Lead organizations: NCI network trial development and conduct. Updated September 29, 2025. Accessed March 10, 2026. https://dctd.cancer.gov/research/ctep-trials/trial-development#ctc_40
- Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45:228-247. doi:10.1016/j.ejca.2008.10.026
- Goodman AM, Kato S, Bazhenova L, et al. Tumor mutational burden as an independent predictor of response to immunotherapy in diverse cancers. Mol Cancer Ther. 2017;16:2598-2608. doi:10.1158/1535-7163.mct-17-0386
- Kroschinsky F, Stölzel F, von Bonin S, et al. New drugs, new toxicities: severe side effects of modern targeted and immunotherapy of cancer and their management. Crit Care. 2017;21:89. doi:10.1186/s13054-017-1678-1
Cutaneous squamous cell carcinoma (cSCC) is the second most prevalent skin cancer and ranks sixth in prevalence among all cancers in the United Kingdom.1,2 The etiologic factors underlying cSCC are well established, with major efforts undertaken by governments and public health organizations over the past 2 decades to increase public awareness globally. Known risk factors for cSCC include chronic exposure to UV radiation, radiotherapy, chemical injury, and immunosuppression. The first 3 risk factors amplify risk by increasing accumulation of abnormal gene mutations. Immunosuppression hampers the immune system’s ability to eradicate cells bearing malignant genetic aberrations. Notable gene mutations implicated in cSCC include p53, p16, telomerase reverse transcriptase, NOTCH1, ROS1, mitogen-activated protein kinases, forkhead box M1, and cyclooxygenase 2, in addition to matrix metalloproteinases, which are most commonly associated with Marjolin ulcers.3
The incidence of cSCC continues to surge worldwide,3,4 with more patients presenting with advanced stages of disease and a notable increase in those presenting with unresectable cSCC due to either locally advanced disease or distant metastases.5 Existing therapies for cSCC include surgical excision (including Mohs micrographic surgery); radiotherapy (indicated for cosmetic reasons, locally advanced disease, and/or patient factors); and systemic treatments, encompassing chemotherapy (eg, 5-fluorouracil), and epidermal growth factor receptor inhibitors (indicated locally advanced disease or distant metastases).4
In recent years, immunotherapy has emerged as a potent and effective treatment modality for unresectable cSCC, both locally advanced and metastatic. The success of immunotherapy in cSCC treatment can be attributed to the unique tumor microenvironment of cSCC, which is characterized by high tumor mutational burden, increased density of tumor-infiltrating lymphocytes (TILs), and heightened programmed cell death ligand 1 (PD-L1) expression on neoplastic cells. The elevated TIL density enables a robust immune response, rendering checkpoint inhibitors particularly effective. Greater tumor mutational burden further augments this enhanced TIL activity, amplifying the response to checkpoint inhibitors. Additionally, heightened PD-L1 expression facilitates more effective unmasking by checkpoint inhibitors, thereby enhancing the immune response.6
Cemiplimab is a programmed cell death protein 1/PD-L1 that was approved by the US Food and Drug Administration in September 2018 for treatment of cSCC. It also gained a European Union endorsement in June 2019 and National Institute for Health and Care Excellence approval in August 2019 based on the highly promising results of a phase 2 trial that involved only 59 adult patients with metastatic cSCC.7 The trial reported an overall response rate (ORR) of 47%, durable disease control in 61% of patients, a median time to response of 1.9 months, and response duration exceeding 6 months in 57% of patients. The phase 2 trials reported an estimated 12-month progression-free survival (PFS) of 53% and an estimated 12-month overall survival (OS) of 81%.7
Despite the noteworthy response statistics demonstrated by these studies, it is imperative to recognize that immunotherapies, while potent, are not without challenges. They can precipitate severe immune-related adverse events (AEs), including myocarditis, adrenal failure, and pneumonitis, which can negatively impact patient health outcomes and lead to early treatment cessation. The initial trials reported high-grade AEs such as pneumonitis, pleural effusion, and, notably 11 total deaths, with 8 (72.7%) attributed to disease progression and 3 (27.3%) to AEs.7 Additionally, cost and access to immunotherapy are inherent limitations of the treatment; immunotherapy agents are expensive, and not all centers or patients are able to access them.
The aim of this study was to assess the efficacy of cemiplimab in patients with inoperable cSCC, including locally advanced and metastatic disease, treated at a tertiary referral center in the United Kingdom, and to compare outcomes with the pivotal phase 2 trial that supported regulatory approval of cemiplimab.7 The primary objective was ORR, with secondary objectives including PFS, OS, and AEs.
Methods
The patients included in this study had unresectable cSCC and therefore were not candidates for surgery or radiotherapy. Patient demographics are presented in Table 1. The main indications for cemiplimab in place of surgery or radiotherapy included local recurrence, locally advanced disease involving deep structures, advanced nodal disease, and distant metastatic disease. Patients meeting these criteria and the following inclusion criteria for cemiplimab treatment from November 2018 through March 2023 at a single tertiary referral center were included in the study:
- Age 18 years or older
- Histologically confirmed cSCC with locoregional recurrence after surgery or radiotherapy, or histologically confirmed advanced or metastatic disease deemed to be inoperable
- Eastern Cooperative Oncology Group performance status of 0 to 2
All enrolled patients received intravenous infusions of cemiplimab 3 times weekly at a dosage of 350 mg. Treatment was continued until complete response, unacceptable toxicity, or disease progression, with a maximum duration of 2 years or 35 cycles. Patients underwent regular follow-up, typically 3 weeks preceding each treatment cycle. Monitoring adhered to the Common Terminology Criteria for Adverse Events, version 4.0, as outlined by the National Cancer Institute.8 Response to treatment was reported according to the guidelines stipulated by the Response Evaluation Criteria in Solid Tumours, version 1.1.9 Written informed consent was obtained for all patients.
Comprehensive patient demographics, histologic profiles, and clinical data were meticulously captured on a retrospective basis. The primary objective centered on elucidating the ORR. Secondary objectives encompassed evaluating PFS, OS, and a comprehensive analysis of AEs. Progression-free survival and OS were calculated by generating Kaplan-Meier curves using Python 3.9 (Python Software Foundation).
Results
Patient Characteristics—From November 2018 through March 2023, a cohort of 31 patients with inoperable cSCC underwent treatment with cemiplimab at our tertiary referral center. The median duration of follow-up was 13 months. Clinical characteristics are outlined in the Table 2. Four (12.9%) patients successfully completed the full 2-year treatment course. Nine (29.0%) continued to receive cemiplimab therapy at the conclusion of this study in March 2023, with treatment courses ranging from 2 to 11 months since initiation. Ten (32.3%) patients discontinued treatment due to AEs, while 5 (16.1%) regrettably ceased treatment due to mortality. Two (6.5%) patients terminated treatment due to the COVID-19 pandemic, and 1 (3.2%) discontinued treatment as a result of disease progression.
Clinical Efficacy—Of the 31 enrolled patients, a substantial proportion experienced positive clinical outcomes, with 20 (64.5%) achieving complete response and 6 (19.4%) achieving partial response. A total of 26 patients achieved a response on cemiplimab, with an ORR of 83.9% (95% CI, 66.3%-94.6%). Regrettably, 2 (6.5%) patients experienced disease progression, while 3 (9.7%) died before response to cemiplimab could be assessed. Following a median follow-up period of 13 months, the median PFS and OS remained unreached, emphasizing the efficacy of cemiplimab in treating inoperable cSCC (Figures 1 and 2).
In our cohort, 2-year PFS was 57.5% (95% CI, 33.9%-75.5%) with cemiplimab and 2-year OS was 70.6% (95% CI, 46.5%-85.4%). For PFS, we observed the steepest drops at onset and at the 23-month mark (Figure 1), while for OS we observed the steepest drop at the 38-month mark (Figure 2). Clinically, we observed cemiplimab causing near-complete regression of previously large, ulcerating, fungating cSCC in patients who responded to cemiplimab, mirroring results seen elsewhere.7
Adverse Events and Treatment Cessation—A substantial proportion of patients (24/31 [77.4%]) reported AEs during treatment. Notably, treatment discontinuation was necessary in 10 (32.3%) patients due to a range of AEs, including myocarditis, atrial flutter, pneumonitis, nephritis, derangement of liver function tests, and arthritis. Additional relevant side effects included adrenal insufficiency (3/31 [9.7%]), fatigue (3/31 [9.7%]), diarrhea (2/31 [6.5%]), and type 1 diabetes 1/31 [3.2%]). These outcomes emphasize the importance of vigilance and monitoring when administering cemiplimab in the context of advanced cSCC.
Comment
Historically, advanced cSCC has had a bleak prognosis. The nature of the disease generally meant these patients could not be operated on due to metastatic spread or local invasion, and radiotherapy was not curative. The only option remaining was palliation, but new therapies have shown promise due to specific inherent characteristics of advanced cSCC; for example, the characteristic high mutation burden prevalent in advanced cSCC has paved the way for the emergence of immunotherapy as a promising avenue for intervention.10 Cemiplimab in particular has emerged as a feasible treatment for patients who would otherwise be confined to palliation. Our findings derived from a local cohort reinforce this notion, with a remarkable 83.9% (26/31) exhibiting a favorable response to cemiplimab. Although this local sample of 31 patients is small in absolute terms, in the context of the trial with 59 participants7 that gained global approval for the use of cemiplimab, our study adds a substantial amount of data to the growing body of evidence on the long-term efficacy of cemiplimab. Notably, our results emphasize the potential applicability of cemiplimab among elderly patients and individuals with lower performance statuses: populations historically excluded from immunotherapeutic considerations.
Immunotherapeutic AEs and Tolerance—As anticipated with immunotherapeutic agents, cemiplimab is associated with AEs that also are seen in its counterparts.11 A total of 77.4% (24/31) of our cohort reported immune-related AEs, although the severity warranted treatment discontinuation in only 10 (10/24 [41.7%]) patients, representing less than half of those who encountered side effects and less than a third of the entire cohort. Furthermore, most of these immune-related AEs were managed effectively with short courses of oral steroids, further substantiating the notion that cemiplimab is generally well tolerated across patients of diverse performance statuses. Even for patients who discontinued treatment early due to immune-related side effects, benefits persisted despite the partial course of cemiplimab. Of the 10 patients who discontinued treatment due to immune AEs, 6 (60%) demonstrated stable complete response, 2 (20%) experienced relapse after stopping cemiplimab, and 2 (20%) demonstrated a partial response with stable disease.
Challenges in the Most Vulnerable Patient—Of the 5 recorded mortalities, 2 (40%) were attributed to disease progression, while 3 (60%) occurred before response assessment could be undertaken. The 3 patients who died prior to response evaluation were among the most medically fragile in the cohort, characterized by extensive metastatic cSCC and major comorbidities that, in isolation, posed life-threatening risks. For individuals grappling with widespread metastatic cSCC and substantial life-threatening comorbidities, it is plausible that the necessary physiologic resilience necessary for cemiplimab therapy may be absent. We hypothesize that an immune reconstitution syndrome–like response may be responsible for this early mortality, and these patients may lack the necessary physiological resilience to tolerate this response. This subset of patients warrants careful consideration when considering therapy with cemiplimab.
Conclusion
In summary, our results underscore the efficacy of cemiplimab, as it supported a response in more than three-quarters of our patient cohort. Additionally, the associated AEs, similar to those with other programmed cell death protein 1 inhibitors, generally were manageable with medical intervention. Our findings corroborate earlier studies that have demonstrated the therapeutic potential of cemiplimab in advanced, inoperable cSCC management. In addition to efficacy, our results also suggest that cemiplimab holds promise as a therapeutic option for patients who might not be amenable to the stresses of general anesthesia, surgery, or prolonged hospitalization, although cemiplimab should likely be used with caution in patients with severe, life-threatening medical comorbidities and/or concurrent severe illness. Furthermore, our data demonstrate that the benefits persist not only beyond the completion of the full 2-year course, but also after partial treatment courses discontinued due to patient-specific factors. Future studies would be useful to better understand and optimize dose and duration of cemiplimab treatment to maximize therapeutic effectiveness while minimizing risk of immune-related AEs. Among individuals confronting advanced, inoperable cSCC, cemiplimab is emerging as a viable and beneficial intervention.
Cutaneous squamous cell carcinoma (cSCC) is the second most prevalent skin cancer and ranks sixth in prevalence among all cancers in the United Kingdom.1,2 The etiologic factors underlying cSCC are well established, with major efforts undertaken by governments and public health organizations over the past 2 decades to increase public awareness globally. Known risk factors for cSCC include chronic exposure to UV radiation, radiotherapy, chemical injury, and immunosuppression. The first 3 risk factors amplify risk by increasing accumulation of abnormal gene mutations. Immunosuppression hampers the immune system’s ability to eradicate cells bearing malignant genetic aberrations. Notable gene mutations implicated in cSCC include p53, p16, telomerase reverse transcriptase, NOTCH1, ROS1, mitogen-activated protein kinases, forkhead box M1, and cyclooxygenase 2, in addition to matrix metalloproteinases, which are most commonly associated with Marjolin ulcers.3
The incidence of cSCC continues to surge worldwide,3,4 with more patients presenting with advanced stages of disease and a notable increase in those presenting with unresectable cSCC due to either locally advanced disease or distant metastases.5 Existing therapies for cSCC include surgical excision (including Mohs micrographic surgery); radiotherapy (indicated for cosmetic reasons, locally advanced disease, and/or patient factors); and systemic treatments, encompassing chemotherapy (eg, 5-fluorouracil), and epidermal growth factor receptor inhibitors (indicated locally advanced disease or distant metastases).4
In recent years, immunotherapy has emerged as a potent and effective treatment modality for unresectable cSCC, both locally advanced and metastatic. The success of immunotherapy in cSCC treatment can be attributed to the unique tumor microenvironment of cSCC, which is characterized by high tumor mutational burden, increased density of tumor-infiltrating lymphocytes (TILs), and heightened programmed cell death ligand 1 (PD-L1) expression on neoplastic cells. The elevated TIL density enables a robust immune response, rendering checkpoint inhibitors particularly effective. Greater tumor mutational burden further augments this enhanced TIL activity, amplifying the response to checkpoint inhibitors. Additionally, heightened PD-L1 expression facilitates more effective unmasking by checkpoint inhibitors, thereby enhancing the immune response.6
Cemiplimab is a programmed cell death protein 1/PD-L1 that was approved by the US Food and Drug Administration in September 2018 for treatment of cSCC. It also gained a European Union endorsement in June 2019 and National Institute for Health and Care Excellence approval in August 2019 based on the highly promising results of a phase 2 trial that involved only 59 adult patients with metastatic cSCC.7 The trial reported an overall response rate (ORR) of 47%, durable disease control in 61% of patients, a median time to response of 1.9 months, and response duration exceeding 6 months in 57% of patients. The phase 2 trials reported an estimated 12-month progression-free survival (PFS) of 53% and an estimated 12-month overall survival (OS) of 81%.7
Despite the noteworthy response statistics demonstrated by these studies, it is imperative to recognize that immunotherapies, while potent, are not without challenges. They can precipitate severe immune-related adverse events (AEs), including myocarditis, adrenal failure, and pneumonitis, which can negatively impact patient health outcomes and lead to early treatment cessation. The initial trials reported high-grade AEs such as pneumonitis, pleural effusion, and, notably 11 total deaths, with 8 (72.7%) attributed to disease progression and 3 (27.3%) to AEs.7 Additionally, cost and access to immunotherapy are inherent limitations of the treatment; immunotherapy agents are expensive, and not all centers or patients are able to access them.
The aim of this study was to assess the efficacy of cemiplimab in patients with inoperable cSCC, including locally advanced and metastatic disease, treated at a tertiary referral center in the United Kingdom, and to compare outcomes with the pivotal phase 2 trial that supported regulatory approval of cemiplimab.7 The primary objective was ORR, with secondary objectives including PFS, OS, and AEs.
Methods
The patients included in this study had unresectable cSCC and therefore were not candidates for surgery or radiotherapy. Patient demographics are presented in Table 1. The main indications for cemiplimab in place of surgery or radiotherapy included local recurrence, locally advanced disease involving deep structures, advanced nodal disease, and distant metastatic disease. Patients meeting these criteria and the following inclusion criteria for cemiplimab treatment from November 2018 through March 2023 at a single tertiary referral center were included in the study:
- Age 18 years or older
- Histologically confirmed cSCC with locoregional recurrence after surgery or radiotherapy, or histologically confirmed advanced or metastatic disease deemed to be inoperable
- Eastern Cooperative Oncology Group performance status of 0 to 2
All enrolled patients received intravenous infusions of cemiplimab 3 times weekly at a dosage of 350 mg. Treatment was continued until complete response, unacceptable toxicity, or disease progression, with a maximum duration of 2 years or 35 cycles. Patients underwent regular follow-up, typically 3 weeks preceding each treatment cycle. Monitoring adhered to the Common Terminology Criteria for Adverse Events, version 4.0, as outlined by the National Cancer Institute.8 Response to treatment was reported according to the guidelines stipulated by the Response Evaluation Criteria in Solid Tumours, version 1.1.9 Written informed consent was obtained for all patients.
Comprehensive patient demographics, histologic profiles, and clinical data were meticulously captured on a retrospective basis. The primary objective centered on elucidating the ORR. Secondary objectives encompassed evaluating PFS, OS, and a comprehensive analysis of AEs. Progression-free survival and OS were calculated by generating Kaplan-Meier curves using Python 3.9 (Python Software Foundation).
Results
Patient Characteristics—From November 2018 through March 2023, a cohort of 31 patients with inoperable cSCC underwent treatment with cemiplimab at our tertiary referral center. The median duration of follow-up was 13 months. Clinical characteristics are outlined in the Table 2. Four (12.9%) patients successfully completed the full 2-year treatment course. Nine (29.0%) continued to receive cemiplimab therapy at the conclusion of this study in March 2023, with treatment courses ranging from 2 to 11 months since initiation. Ten (32.3%) patients discontinued treatment due to AEs, while 5 (16.1%) regrettably ceased treatment due to mortality. Two (6.5%) patients terminated treatment due to the COVID-19 pandemic, and 1 (3.2%) discontinued treatment as a result of disease progression.
Clinical Efficacy—Of the 31 enrolled patients, a substantial proportion experienced positive clinical outcomes, with 20 (64.5%) achieving complete response and 6 (19.4%) achieving partial response. A total of 26 patients achieved a response on cemiplimab, with an ORR of 83.9% (95% CI, 66.3%-94.6%). Regrettably, 2 (6.5%) patients experienced disease progression, while 3 (9.7%) died before response to cemiplimab could be assessed. Following a median follow-up period of 13 months, the median PFS and OS remained unreached, emphasizing the efficacy of cemiplimab in treating inoperable cSCC (Figures 1 and 2).
In our cohort, 2-year PFS was 57.5% (95% CI, 33.9%-75.5%) with cemiplimab and 2-year OS was 70.6% (95% CI, 46.5%-85.4%). For PFS, we observed the steepest drops at onset and at the 23-month mark (Figure 1), while for OS we observed the steepest drop at the 38-month mark (Figure 2). Clinically, we observed cemiplimab causing near-complete regression of previously large, ulcerating, fungating cSCC in patients who responded to cemiplimab, mirroring results seen elsewhere.7
Adverse Events and Treatment Cessation—A substantial proportion of patients (24/31 [77.4%]) reported AEs during treatment. Notably, treatment discontinuation was necessary in 10 (32.3%) patients due to a range of AEs, including myocarditis, atrial flutter, pneumonitis, nephritis, derangement of liver function tests, and arthritis. Additional relevant side effects included adrenal insufficiency (3/31 [9.7%]), fatigue (3/31 [9.7%]), diarrhea (2/31 [6.5%]), and type 1 diabetes 1/31 [3.2%]). These outcomes emphasize the importance of vigilance and monitoring when administering cemiplimab in the context of advanced cSCC.
Comment
Historically, advanced cSCC has had a bleak prognosis. The nature of the disease generally meant these patients could not be operated on due to metastatic spread or local invasion, and radiotherapy was not curative. The only option remaining was palliation, but new therapies have shown promise due to specific inherent characteristics of advanced cSCC; for example, the characteristic high mutation burden prevalent in advanced cSCC has paved the way for the emergence of immunotherapy as a promising avenue for intervention.10 Cemiplimab in particular has emerged as a feasible treatment for patients who would otherwise be confined to palliation. Our findings derived from a local cohort reinforce this notion, with a remarkable 83.9% (26/31) exhibiting a favorable response to cemiplimab. Although this local sample of 31 patients is small in absolute terms, in the context of the trial with 59 participants7 that gained global approval for the use of cemiplimab, our study adds a substantial amount of data to the growing body of evidence on the long-term efficacy of cemiplimab. Notably, our results emphasize the potential applicability of cemiplimab among elderly patients and individuals with lower performance statuses: populations historically excluded from immunotherapeutic considerations.
Immunotherapeutic AEs and Tolerance—As anticipated with immunotherapeutic agents, cemiplimab is associated with AEs that also are seen in its counterparts.11 A total of 77.4% (24/31) of our cohort reported immune-related AEs, although the severity warranted treatment discontinuation in only 10 (10/24 [41.7%]) patients, representing less than half of those who encountered side effects and less than a third of the entire cohort. Furthermore, most of these immune-related AEs were managed effectively with short courses of oral steroids, further substantiating the notion that cemiplimab is generally well tolerated across patients of diverse performance statuses. Even for patients who discontinued treatment early due to immune-related side effects, benefits persisted despite the partial course of cemiplimab. Of the 10 patients who discontinued treatment due to immune AEs, 6 (60%) demonstrated stable complete response, 2 (20%) experienced relapse after stopping cemiplimab, and 2 (20%) demonstrated a partial response with stable disease.
Challenges in the Most Vulnerable Patient—Of the 5 recorded mortalities, 2 (40%) were attributed to disease progression, while 3 (60%) occurred before response assessment could be undertaken. The 3 patients who died prior to response evaluation were among the most medically fragile in the cohort, characterized by extensive metastatic cSCC and major comorbidities that, in isolation, posed life-threatening risks. For individuals grappling with widespread metastatic cSCC and substantial life-threatening comorbidities, it is plausible that the necessary physiologic resilience necessary for cemiplimab therapy may be absent. We hypothesize that an immune reconstitution syndrome–like response may be responsible for this early mortality, and these patients may lack the necessary physiological resilience to tolerate this response. This subset of patients warrants careful consideration when considering therapy with cemiplimab.
Conclusion
In summary, our results underscore the efficacy of cemiplimab, as it supported a response in more than three-quarters of our patient cohort. Additionally, the associated AEs, similar to those with other programmed cell death protein 1 inhibitors, generally were manageable with medical intervention. Our findings corroborate earlier studies that have demonstrated the therapeutic potential of cemiplimab in advanced, inoperable cSCC management. In addition to efficacy, our results also suggest that cemiplimab holds promise as a therapeutic option for patients who might not be amenable to the stresses of general anesthesia, surgery, or prolonged hospitalization, although cemiplimab should likely be used with caution in patients with severe, life-threatening medical comorbidities and/or concurrent severe illness. Furthermore, our data demonstrate that the benefits persist not only beyond the completion of the full 2-year course, but also after partial treatment courses discontinued due to patient-specific factors. Future studies would be useful to better understand and optimize dose and duration of cemiplimab treatment to maximize therapeutic effectiveness while minimizing risk of immune-related AEs. Among individuals confronting advanced, inoperable cSCC, cemiplimab is emerging as a viable and beneficial intervention.
- Waldman A, Schmults C. Cutaneous squamous cell carcinoma. Hematol Oncol Clin North Am. 2019;33:1-12. doi:10.1016/j.hoc.2018.08.001
- Venables ZC, Nijsten T, Wong KF, et al. Epidemiology of basal and cutaneous squamous cell carcinoma in the U.K. 2013–15: a cohort study. Br J Dermatol. 2019;181:474-482. doi:10.1111/bjd.17873
- Que SKT, Zwald FO, Schmults CD. Cutaneous squamous cell carcinoma. J Am Acad Dermatol. 2018;78:237-247. doi:10.1016/j.jaad.2017.08.059
- Green AC, Olsen CM. Cutaneous squamous cell carcinoma: an epidemiological review. Br J Dermatol. 2017;177:373-381. doi:10.1111/bjd.15324
- Jovic’ M, Marinkovic’ M, Sud‐ecki B, et al. COVID-19 and cutaneous squamous cell carcinoma—impact of the pandemic on unequal access to healthcare. Healthcare (Basel). 2023;11:1994. doi:10.3390/healthcare11141994
- Ansary TM, Hossain MDR, Komine M, et al. Immunotherapy for the treatment of squamous cell carcinoma: potential benefits and challenges. Int J Mol Sci. 2022;23:8530. doi:10.3390/ijms23158530
- Migden MR, Rischin D, Schmults CD, et al. PD-1 blockade with cemiplimab in advanced cutaneous squamous-cell carcinoma. N Engl J Med. 2018;379:341-351. doi:10.1056/nejmoa1805131
- National Cancer Institute. Lead organizations: NCI network trial development and conduct. Updated September 29, 2025. Accessed March 10, 2026. https://dctd.cancer.gov/research/ctep-trials/trial-development#ctc_40
- Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45:228-247. doi:10.1016/j.ejca.2008.10.026
- Goodman AM, Kato S, Bazhenova L, et al. Tumor mutational burden as an independent predictor of response to immunotherapy in diverse cancers. Mol Cancer Ther. 2017;16:2598-2608. doi:10.1158/1535-7163.mct-17-0386
- Kroschinsky F, Stölzel F, von Bonin S, et al. New drugs, new toxicities: severe side effects of modern targeted and immunotherapy of cancer and their management. Crit Care. 2017;21:89. doi:10.1186/s13054-017-1678-1
- Waldman A, Schmults C. Cutaneous squamous cell carcinoma. Hematol Oncol Clin North Am. 2019;33:1-12. doi:10.1016/j.hoc.2018.08.001
- Venables ZC, Nijsten T, Wong KF, et al. Epidemiology of basal and cutaneous squamous cell carcinoma in the U.K. 2013–15: a cohort study. Br J Dermatol. 2019;181:474-482. doi:10.1111/bjd.17873
- Que SKT, Zwald FO, Schmults CD. Cutaneous squamous cell carcinoma. J Am Acad Dermatol. 2018;78:237-247. doi:10.1016/j.jaad.2017.08.059
- Green AC, Olsen CM. Cutaneous squamous cell carcinoma: an epidemiological review. Br J Dermatol. 2017;177:373-381. doi:10.1111/bjd.15324
- Jovic’ M, Marinkovic’ M, Sud‐ecki B, et al. COVID-19 and cutaneous squamous cell carcinoma—impact of the pandemic on unequal access to healthcare. Healthcare (Basel). 2023;11:1994. doi:10.3390/healthcare11141994
- Ansary TM, Hossain MDR, Komine M, et al. Immunotherapy for the treatment of squamous cell carcinoma: potential benefits and challenges. Int J Mol Sci. 2022;23:8530. doi:10.3390/ijms23158530
- Migden MR, Rischin D, Schmults CD, et al. PD-1 blockade with cemiplimab in advanced cutaneous squamous-cell carcinoma. N Engl J Med. 2018;379:341-351. doi:10.1056/nejmoa1805131
- National Cancer Institute. Lead organizations: NCI network trial development and conduct. Updated September 29, 2025. Accessed March 10, 2026. https://dctd.cancer.gov/research/ctep-trials/trial-development#ctc_40
- Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45:228-247. doi:10.1016/j.ejca.2008.10.026
- Goodman AM, Kato S, Bazhenova L, et al. Tumor mutational burden as an independent predictor of response to immunotherapy in diverse cancers. Mol Cancer Ther. 2017;16:2598-2608. doi:10.1158/1535-7163.mct-17-0386
- Kroschinsky F, Stölzel F, von Bonin S, et al. New drugs, new toxicities: severe side effects of modern targeted and immunotherapy of cancer and their management. Crit Care. 2017;21:89. doi:10.1186/s13054-017-1678-1
Cemiplimab for Unresectable Cutaneous Squamous Cell Carcinoma: Experience From a Tertiary Center
Cemiplimab for Unresectable Cutaneous Squamous Cell Carcinoma: Experience From a Tertiary Center
PRACTICE POINTS
- In a cohort of patients with advanced cutaneous squamous cell carcinoma not amenable to surgery or radiotherapy, cemiplimab achieved an 83.9% overall response rate, with 64.5% achieving complete response.
- Two-year overall survival was 73.5%, indicating cemiplimab can provide durable benefit and may improve prognosis in this difficult-to-treat group.
- Adverse events are an ongoing concern; 77.4% of patients experienced adverse events. While cemiplimab is effective, patients taking it need regular monitoring.
A Cost-Effectiveness and Psychological Evaluation of Early Skin Biopsies vs Later-Onset Surgeries in Melanoma Management
Compared to later-onset procedures, early diagnosis of melanoma using affordable skin biopsies can result in better patient outcomes, lower health care expenditures, and enhanced psychological well-being.1 Numerous research and economic evaluations that highlight the possible advantages of early intervention in melanoma care lend support to this strategy. In health care systems, the cost of early identification and screening for skin cancer is a critical factor.1 There has been debate in the literature regarding performing more frequent biopsies earlier for skin cancers, which may greatly improve patient outcomes at the expense of increased financial cost, compared with performing fewer biopsies, which reduces costs at the potential expense of managing later-onset melanoma.1,2 We sought to summarize the current literature and address some considerations that may help bring more clarity to this topic.
According to a study of a large health care system, the average cost of a skin cancer screening visit was $150, of which $105 (70%) went toward the costs of the office visit and $45 (30%) went toward the costs of the biopsy.1 In the changing health care landscape, it is crucial to take into account the possible compounded savings from early diagnosis and treatment. While biopsies do involve some expenses, consideration of immunotherapy costs for advanced melanoma also should be considered, as they provide an alternative viewpoint on the financial effects of melanoma treatment.2 The use of new systemic treatments such as immunotherapy has led to a notable rise in Medicare users’ first-year melanoma treatment expenses. The average expense of treating stage IV melanoma rose from $47,739 in 2007 through 2012 to $117,450 in 2018 through 2019. This sharp rise highlights how much more expensive treating advanced melanoma is than performing biopsies for early detection and treatment. Hundreds of biopsies might be carried out for the cost of a single advanced melanoma therapy, possibly identifying several cases at an earlier, more manageable stage.2
Patient quality of life and survival rates also can be considerably improved by early melanoma detection through screening.3 Compared to patients with later-stage diagnoses, those with early-stage melanoma reported a higher overall quality of life. Better physical functioning and reduced levels of anxiety and sadness were linked to early identification using skin biopsies. Patients with more advanced melanoma who had later-onset procedures, on the other hand, experience worsening psychological symptoms and physical health.3
A cost-effectiveness analysis using a Markov cohort model compared the long-term economic impact of early detection and primary prevention of melanoma. It found that daily use of sunscreen could prevent a substantial number of new skin tumors and melanoma deaths and reduce health care costs when compared to early detection strategies such as performing extra biopsies.4 There already are programs across the United States that aim to educate the public on the importance of wearing sunscreen; this has, in turn, reduced the prevalence of skin cancer in certain communities. Primary prevention resulted in just 1364 new melanomas and more than $430 million in expenditures per 100,000 individuals, whereas early diagnosis produced 2446 new melanomas and more than $660 million in economic expenses per 100,000 individuals.4 It is imperative to acknowledge that skin biopsies remain a vital tool for the early identification of melanoma, particularly in high-risk groups.
By using technologies such as teledermoscopy, the cost-effectiveness of skin cancer referral and consultation can be further enhanced; for example, teledermoscopy for skin cancer referral and triage would result in faster clinical resolution at an average cost of $54.64 per case. This method may reduce the need for redundant in-person consultations and increase the effectiveness of melanoma identification.5
Large-scale public health initiatives in skin cancer prevention and early detection have the potential to be very effective, as evidenced by the War on Melanoma project at Oregon Health & Science University (Portland, Oregon). This all-encompassing strategy, which uses cutting-edge technologies, public education, and health care professional training, has improved melanoma outcomes and decreased health care expenditures with encouraging results.6
A few tactics can be used to best balance the costs of later-onset procedures and early skin biopsies. These include using advanced technologies such as teledermoscopy and dermoscopy, provider training to increase diagnostic accuracy, public health campaigns to raise awareness and promote prevention, and a comprehensive strategy combining targeted early detection strategies with primary prevention.5,6 Health care systems can optimize the financial efficiency and clinical results of melanoma treatment by putting these principles into practice.
Compared to later-onset melanoma procedures, early skin biopsies typically are more cost-effective, produce better patient outcomes, and offer psychological advantages, even if they may have a higher initial cost. Health care systems can optimize the trade-off between early detection and cost effectiveness in melanoma management by putting sophisticated technology to use, enhancing provider training, and implementing focused screening programs.5,6 To support evidence-based policies and guidelines, future research should assess the long-term economic impact of different melanoma prevention and detection measures.
- Matsumoto M, Secrest A, Anderson A, et al. Estimating the cost of skin cancer detection by dermatology providers in a large health care system. J Am Acad Dermatol. 2018;78:701-709.e1. doi:10.1016/j.jaad.2017.11.033
- Gogebakan KC, Mukherjee K, Berry EG, et al. Impact of novel systemic therapies on the first-year costs of care for melanoma among Medicare beneficiaries. Cancer. 2021;127:2926-2933. doi:10.1002/cncr.33515
- Young JN, Griffith-Bauer K, Hill E, et al. The benefit of early-stage diagnosis: a registry-based survey evaluating the quality of life in patients with melanoma. Skin Health Dis. 2023;3:E237. doi:10.1002/ski2.237
- Gordon L, Olsen C, Whiteman DC, et al. Prevention versus early detection for long-term control of melanoma and keratinocyte carcinomas: a cost-effectiveness modelling study. BMJ Open. 2020;10:E034388. doi:10.1136/bmjopen-2019-034388
- Buja A, Rivera M, Girardi G, et al. Cost-effectiveness of a melanoma screening programme using whole disease modelling. J Med Screen. 2020;27:157-167. doi:10.1177/0969141319885998
- Gogebakan KC, Berry EG, Geller AC, et al. Strategizing screening for melanoma in an era of novel treatments: a model-based approach. Cancer Epidemiol Biomarkers Prev. 2020;29:2599-2607. doi:10.1158/1055-9965.EPI-20-0881
Compared to later-onset procedures, early diagnosis of melanoma using affordable skin biopsies can result in better patient outcomes, lower health care expenditures, and enhanced psychological well-being.1 Numerous research and economic evaluations that highlight the possible advantages of early intervention in melanoma care lend support to this strategy. In health care systems, the cost of early identification and screening for skin cancer is a critical factor.1 There has been debate in the literature regarding performing more frequent biopsies earlier for skin cancers, which may greatly improve patient outcomes at the expense of increased financial cost, compared with performing fewer biopsies, which reduces costs at the potential expense of managing later-onset melanoma.1,2 We sought to summarize the current literature and address some considerations that may help bring more clarity to this topic.
According to a study of a large health care system, the average cost of a skin cancer screening visit was $150, of which $105 (70%) went toward the costs of the office visit and $45 (30%) went toward the costs of the biopsy.1 In the changing health care landscape, it is crucial to take into account the possible compounded savings from early diagnosis and treatment. While biopsies do involve some expenses, consideration of immunotherapy costs for advanced melanoma also should be considered, as they provide an alternative viewpoint on the financial effects of melanoma treatment.2 The use of new systemic treatments such as immunotherapy has led to a notable rise in Medicare users’ first-year melanoma treatment expenses. The average expense of treating stage IV melanoma rose from $47,739 in 2007 through 2012 to $117,450 in 2018 through 2019. This sharp rise highlights how much more expensive treating advanced melanoma is than performing biopsies for early detection and treatment. Hundreds of biopsies might be carried out for the cost of a single advanced melanoma therapy, possibly identifying several cases at an earlier, more manageable stage.2
Patient quality of life and survival rates also can be considerably improved by early melanoma detection through screening.3 Compared to patients with later-stage diagnoses, those with early-stage melanoma reported a higher overall quality of life. Better physical functioning and reduced levels of anxiety and sadness were linked to early identification using skin biopsies. Patients with more advanced melanoma who had later-onset procedures, on the other hand, experience worsening psychological symptoms and physical health.3
A cost-effectiveness analysis using a Markov cohort model compared the long-term economic impact of early detection and primary prevention of melanoma. It found that daily use of sunscreen could prevent a substantial number of new skin tumors and melanoma deaths and reduce health care costs when compared to early detection strategies such as performing extra biopsies.4 There already are programs across the United States that aim to educate the public on the importance of wearing sunscreen; this has, in turn, reduced the prevalence of skin cancer in certain communities. Primary prevention resulted in just 1364 new melanomas and more than $430 million in expenditures per 100,000 individuals, whereas early diagnosis produced 2446 new melanomas and more than $660 million in economic expenses per 100,000 individuals.4 It is imperative to acknowledge that skin biopsies remain a vital tool for the early identification of melanoma, particularly in high-risk groups.
By using technologies such as teledermoscopy, the cost-effectiveness of skin cancer referral and consultation can be further enhanced; for example, teledermoscopy for skin cancer referral and triage would result in faster clinical resolution at an average cost of $54.64 per case. This method may reduce the need for redundant in-person consultations and increase the effectiveness of melanoma identification.5
Large-scale public health initiatives in skin cancer prevention and early detection have the potential to be very effective, as evidenced by the War on Melanoma project at Oregon Health & Science University (Portland, Oregon). This all-encompassing strategy, which uses cutting-edge technologies, public education, and health care professional training, has improved melanoma outcomes and decreased health care expenditures with encouraging results.6
A few tactics can be used to best balance the costs of later-onset procedures and early skin biopsies. These include using advanced technologies such as teledermoscopy and dermoscopy, provider training to increase diagnostic accuracy, public health campaigns to raise awareness and promote prevention, and a comprehensive strategy combining targeted early detection strategies with primary prevention.5,6 Health care systems can optimize the financial efficiency and clinical results of melanoma treatment by putting these principles into practice.
Compared to later-onset melanoma procedures, early skin biopsies typically are more cost-effective, produce better patient outcomes, and offer psychological advantages, even if they may have a higher initial cost. Health care systems can optimize the trade-off between early detection and cost effectiveness in melanoma management by putting sophisticated technology to use, enhancing provider training, and implementing focused screening programs.5,6 To support evidence-based policies and guidelines, future research should assess the long-term economic impact of different melanoma prevention and detection measures.
Compared to later-onset procedures, early diagnosis of melanoma using affordable skin biopsies can result in better patient outcomes, lower health care expenditures, and enhanced psychological well-being.1 Numerous research and economic evaluations that highlight the possible advantages of early intervention in melanoma care lend support to this strategy. In health care systems, the cost of early identification and screening for skin cancer is a critical factor.1 There has been debate in the literature regarding performing more frequent biopsies earlier for skin cancers, which may greatly improve patient outcomes at the expense of increased financial cost, compared with performing fewer biopsies, which reduces costs at the potential expense of managing later-onset melanoma.1,2 We sought to summarize the current literature and address some considerations that may help bring more clarity to this topic.
According to a study of a large health care system, the average cost of a skin cancer screening visit was $150, of which $105 (70%) went toward the costs of the office visit and $45 (30%) went toward the costs of the biopsy.1 In the changing health care landscape, it is crucial to take into account the possible compounded savings from early diagnosis and treatment. While biopsies do involve some expenses, consideration of immunotherapy costs for advanced melanoma also should be considered, as they provide an alternative viewpoint on the financial effects of melanoma treatment.2 The use of new systemic treatments such as immunotherapy has led to a notable rise in Medicare users’ first-year melanoma treatment expenses. The average expense of treating stage IV melanoma rose from $47,739 in 2007 through 2012 to $117,450 in 2018 through 2019. This sharp rise highlights how much more expensive treating advanced melanoma is than performing biopsies for early detection and treatment. Hundreds of biopsies might be carried out for the cost of a single advanced melanoma therapy, possibly identifying several cases at an earlier, more manageable stage.2
Patient quality of life and survival rates also can be considerably improved by early melanoma detection through screening.3 Compared to patients with later-stage diagnoses, those with early-stage melanoma reported a higher overall quality of life. Better physical functioning and reduced levels of anxiety and sadness were linked to early identification using skin biopsies. Patients with more advanced melanoma who had later-onset procedures, on the other hand, experience worsening psychological symptoms and physical health.3
A cost-effectiveness analysis using a Markov cohort model compared the long-term economic impact of early detection and primary prevention of melanoma. It found that daily use of sunscreen could prevent a substantial number of new skin tumors and melanoma deaths and reduce health care costs when compared to early detection strategies such as performing extra biopsies.4 There already are programs across the United States that aim to educate the public on the importance of wearing sunscreen; this has, in turn, reduced the prevalence of skin cancer in certain communities. Primary prevention resulted in just 1364 new melanomas and more than $430 million in expenditures per 100,000 individuals, whereas early diagnosis produced 2446 new melanomas and more than $660 million in economic expenses per 100,000 individuals.4 It is imperative to acknowledge that skin biopsies remain a vital tool for the early identification of melanoma, particularly in high-risk groups.
By using technologies such as teledermoscopy, the cost-effectiveness of skin cancer referral and consultation can be further enhanced; for example, teledermoscopy for skin cancer referral and triage would result in faster clinical resolution at an average cost of $54.64 per case. This method may reduce the need for redundant in-person consultations and increase the effectiveness of melanoma identification.5
Large-scale public health initiatives in skin cancer prevention and early detection have the potential to be very effective, as evidenced by the War on Melanoma project at Oregon Health & Science University (Portland, Oregon). This all-encompassing strategy, which uses cutting-edge technologies, public education, and health care professional training, has improved melanoma outcomes and decreased health care expenditures with encouraging results.6
A few tactics can be used to best balance the costs of later-onset procedures and early skin biopsies. These include using advanced technologies such as teledermoscopy and dermoscopy, provider training to increase diagnostic accuracy, public health campaigns to raise awareness and promote prevention, and a comprehensive strategy combining targeted early detection strategies with primary prevention.5,6 Health care systems can optimize the financial efficiency and clinical results of melanoma treatment by putting these principles into practice.
Compared to later-onset melanoma procedures, early skin biopsies typically are more cost-effective, produce better patient outcomes, and offer psychological advantages, even if they may have a higher initial cost. Health care systems can optimize the trade-off between early detection and cost effectiveness in melanoma management by putting sophisticated technology to use, enhancing provider training, and implementing focused screening programs.5,6 To support evidence-based policies and guidelines, future research should assess the long-term economic impact of different melanoma prevention and detection measures.
- Matsumoto M, Secrest A, Anderson A, et al. Estimating the cost of skin cancer detection by dermatology providers in a large health care system. J Am Acad Dermatol. 2018;78:701-709.e1. doi:10.1016/j.jaad.2017.11.033
- Gogebakan KC, Mukherjee K, Berry EG, et al. Impact of novel systemic therapies on the first-year costs of care for melanoma among Medicare beneficiaries. Cancer. 2021;127:2926-2933. doi:10.1002/cncr.33515
- Young JN, Griffith-Bauer K, Hill E, et al. The benefit of early-stage diagnosis: a registry-based survey evaluating the quality of life in patients with melanoma. Skin Health Dis. 2023;3:E237. doi:10.1002/ski2.237
- Gordon L, Olsen C, Whiteman DC, et al. Prevention versus early detection for long-term control of melanoma and keratinocyte carcinomas: a cost-effectiveness modelling study. BMJ Open. 2020;10:E034388. doi:10.1136/bmjopen-2019-034388
- Buja A, Rivera M, Girardi G, et al. Cost-effectiveness of a melanoma screening programme using whole disease modelling. J Med Screen. 2020;27:157-167. doi:10.1177/0969141319885998
- Gogebakan KC, Berry EG, Geller AC, et al. Strategizing screening for melanoma in an era of novel treatments: a model-based approach. Cancer Epidemiol Biomarkers Prev. 2020;29:2599-2607. doi:10.1158/1055-9965.EPI-20-0881
- Matsumoto M, Secrest A, Anderson A, et al. Estimating the cost of skin cancer detection by dermatology providers in a large health care system. J Am Acad Dermatol. 2018;78:701-709.e1. doi:10.1016/j.jaad.2017.11.033
- Gogebakan KC, Mukherjee K, Berry EG, et al. Impact of novel systemic therapies on the first-year costs of care for melanoma among Medicare beneficiaries. Cancer. 2021;127:2926-2933. doi:10.1002/cncr.33515
- Young JN, Griffith-Bauer K, Hill E, et al. The benefit of early-stage diagnosis: a registry-based survey evaluating the quality of life in patients with melanoma. Skin Health Dis. 2023;3:E237. doi:10.1002/ski2.237
- Gordon L, Olsen C, Whiteman DC, et al. Prevention versus early detection for long-term control of melanoma and keratinocyte carcinomas: a cost-effectiveness modelling study. BMJ Open. 2020;10:E034388. doi:10.1136/bmjopen-2019-034388
- Buja A, Rivera M, Girardi G, et al. Cost-effectiveness of a melanoma screening programme using whole disease modelling. J Med Screen. 2020;27:157-167. doi:10.1177/0969141319885998
- Gogebakan KC, Berry EG, Geller AC, et al. Strategizing screening for melanoma in an era of novel treatments: a model-based approach. Cancer Epidemiol Biomarkers Prev. 2020;29:2599-2607. doi:10.1158/1055-9965.EPI-20-0881
Practice Points
- Early melanoma detection via skin biopsy is generally more cost-effective than managing advanced-stage disease, largely due to the high costs associated with systemic therapies (eg, immunotherapy) used in later-stage melanoma.
- Earlier diagnosis is associated with improved patient outcomes, including better quality of life and reduced psychological distress, compared with later-stage melanoma diagnoses requiring more extensive intervention.
- Integrated prevention and early detection strategies—such as dermoscopy, teledermoscopy, and public health initiatives—may optimize melanoma outcomes while reducing overall health care expenditures.
Case Series of Patients With Cardiac Amyloidosis at VA New York Harbor Healthcare-Brooklyn
Case Series of Patients With Cardiac Amyloidosis at VA New York Harbor Healthcare-Brooklyn
Transthyretin amyloid cardiomyopathy (ATTR-CM) is caused by the misfolding of the TTR protein, which results in aggregation of amyloid fibrils that deposit in the myocardium and causes restrictive cardiomyopathy. Though it remains underdiagnosed, ATTR-CM is increasingly being recognized as a cause of heart failure in geriatric patients.1 There are 2 categories of ATTRCM: wild-type ATTR-CM (wtATTR-CM), in which there is no mutation in the TTR gene, and hereditary ATTR-CM (hATTR-CM), in which a mutation is present in the TTR gene. Research has shown that wtATTR-CM accounted for as many as 30% of cases of heart failure (HF) with preserved ejection fraction (HFpEF) in patients aged > 75 years.2 A significant percentage of the veteran patient population consists of older males. Given their age, these patients are at greater risk for ATTR diagnosis.3
Identifying red flags for patients within this population may allow clinicians to make earlier diagnoses and improve outcomes. A high index of suspicion is needed to diagnose ATTR because many early signs and symptoms are extracardiac, which leads to delayed diagnoses and worse outcomes. This article describes 8 cases of ATTR-CM within the US Department of Veterans Affairs (VA) New York Harbor Healthcare System-Brooklyn (VANYHHSB).
Methods
This retrospective case series was reviewed and approved by the VANYHHSB Institutional Review Board where it was conducted. Patients diagnosed with ATTR between 2017 and 2024 were identified using International Classification of Diseases, Tenth Revision codes. Eleven patients were identified; 3 were excluded due to insufficient medical records. The remaining 8 patient records were retrospectively reviewed and included.
Case 1
A 67-year-old male with a history of carpal tunnel syndrome (CTS) presented following a syncopal episode. Initial electrocardiogram (ECG) showed sinus rhythm, first-degree atrioventricular block, and a bifascicular block. Transthoracic echocardiogram (TTE) showed moderate asymmetric left ventricular (LV) hypertrophy (LVH) and biatrial enlargement with an ejection fraction (EF) > 55%. The patient was discharged with a loop recorder and an outpatient follow-up appointment scheduled. One month later, he presented with worsening dyspnea on exertion with clinical signs of hypervolemia. A repeat TTE showed global LV wall thickening, moderately reduced LV systolic function (EF 40%), and moderate pulmonary hypertension. Given these findings, the patient underwent cardiac magnetic resonance imaging (CMR), which suggested an infiltrative cardiomyopathy. Amyloid light-chain (AL) amyloidosis evaluation, technetium-99m (99mTC) pyrophosphate imaging, and a fat pad biopsy were unrevealing. An endomyocardial biopsy was performed with electron microscopy, which confirmed amyloidosis. Genetic testing was negative, and the patient began taking tafamidis. There were no later admissions for decompensated HF; however, the patient developed atrial fibrillation (AF) and an interval TTE demonstrated no improvement in his EF. He died at age 73 years.
Case 2
A 78-year-old male with a history of CTS presented with lightheadedness. Initial ECG showed rate-controlled AF and TTE revealed a moderately thickened LV wall with normal LV size, mild left atrial enlargement, and an EF of 65%. The patient was discharged with a scheduled outpatient CMR appointment; however, he defaulted from follow-up. Two years later, he presented with recurrent syncopal episodes and physical examination was consistent with hypervolemia. Repeat TTE revealed moderate LVH, biatrial enlargement, and an EF of 55%. An inpatient CMR was suggestive of cardiac amyloidosis, and a pyrophosphate scan was diagnostic for ATTR. The patient started taking tafamidis, but continued to have recurrent admissions for HF exacerbation. He died at age 81 years.
Case 3
A 71-year-old male with a history of CTS presented with exertional dyspnea. The initial ECG showed sinus rhythm with left atrial enlargement and left axis deviation. Subsequent TTE revealed severe LVH, mildly reduced LV cavity size, moderate to severe biatrial enlargement, and an EF of 25% to 30%. Outpatient 99mTC pyrophosphate imaging suggested cardiac amyloidosis, and laboratory testing showed no evidence of monoclonal proteins. The patient was started on tafamidis for ATTR. At 2-year follow-up, he had new AF and to date has had no further hospitalizations for acute decompensated HF.
Case 4
A 92-year-old male with a history of AF and bilateral CTS presented with lightheadedness. An ECG revealed AF with a slowed ventricular response. Subsequent Holter monitoring demonstrated pauses exceeding 3 seconds, and a permanent pacemaker was recommended. During his preoperative evaluation, TTE revealed severe concentric LVH with a speckled appearance of the myocardium, mild-tomoderate biatrial enlargement, and an EF of 50% to 55%. 99mTC pyrophosphate imaging was positive for amyloidosis and the patient started taking tafamidis. Recurrent hospital admissions for decompensated HF complicated his progression. The patient died at age 95 years.
Case 5
A 72-year-old male with a history of bilateral CTS and cervical spinal stenosis presented with dyspnea on exertion. An ECG revealed a normal sinus rhythm. A TTE found severely reduced systolic function with an EF ≤ 25%, mild concentric LVH, grade 3 diastolic dysfunction, mild-tomoderate biatrial enlargement, and moderate pulmonary hypertension (Figure 1). He was started on guideline-directed medical therapy (GDMT) for HF, which included sacubitril/valsartan, metoprolol succinate, and empagliflozin. The patient’s dyspnea improved, and a workup for nonischemic cardiomyopathy was initiated. 99mTC pyrophosphate imaging 1 year after his initial presentation was positive, leading to ATTR-CM diagnosis. The patient started taking tafamidis and he has since had a stable progression and continued to demonstrate good exercise tolerance with no hospitalizations. His most recent TTE indicated an EF of 40% to 45%.
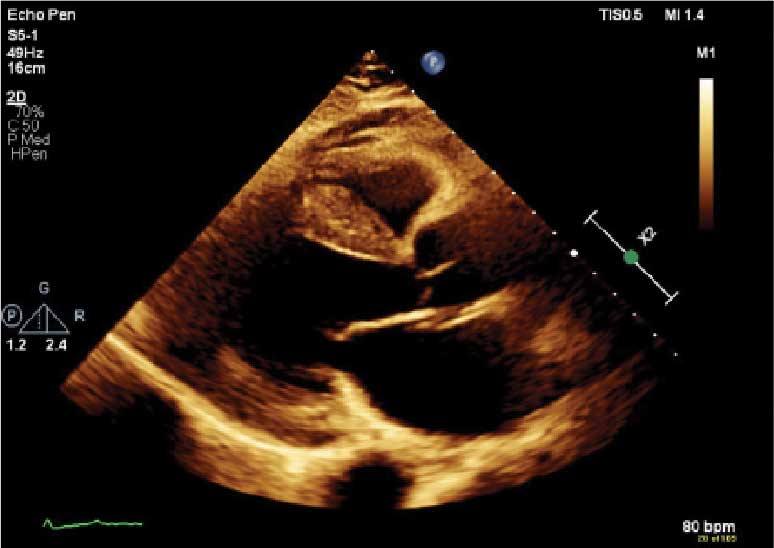
(parasternal long axis view) of patient 5
demonstrating concentric left ventricular
hypertrophy with a speckled myocardium
and dilated left atrium.
Case 6
A 76-year-old male with a history of paroxysmal AF status after multiple ablations, bilateral CTS, and severe cervical spinal stenosis presented with dyspnea on exertion. The patient’s ECG showed normal sinus rhythm and left axis deviation with concern for left anterior hemiblock. A TTE revealed moderate LVH with a speckled appearance of the myocardium and grade 3 diastolic dysfunction with preserved EF. Before completing the workup for underlying cardiomyopathy, the patient underwent an interventional radiology procedure for an angiomyolipoma, and his postoperative course was complicated by pulmonary edema, requiring admission to the coronary care unit for diuresis. A repeat TTE revealed a reduced EF of 35%, and he was discharged on GDMT. No monoclonal protein was seen in the serum or urine. The patient’s progression was complicated by recurrent admissions for acute decompensated HF and supraventricular tachycardia despite being on amiodarone, which led to a delay in obtaining 99mTC pyrophosphate imaging. Due to hypotension, the patient was unable to tolerate GDMT. He eventually underwent 99mTC pyrophosphate imaging that confirmed ATTR-CM and was started on tafamidis. One year following initial presentation, the patient’s EF progressively declined to 20% to 25%, and he died shortly after discharge to subacute rehabilitation.
Case 7
A 95-year-old male with a history of longstanding persistent AF and bilateral CTS presented with dyspnea on exertion, bendopnea, and worsening bilateral pedal edema for a week. An ECG showed AF with a controlled ventricular response and low-voltage QRS waves (Figure 2). A TTE showed biatrial enlargement, LVH, and preserved EF > 55%. He started taking furosemide and was discharged with a diagnosis of HFpEF. The patient missed cardiology follow-up and presented 1 year later with decompensated HF. An amyloidosis workup was recommended, but due to intermittent periods of being lost to follow-up, the patient did not pursue this workup until 3 years after his initial presentation when 99mTC pyrophosphate imaging confirmed ATTR-CM. The patient declined tafamidis and continued to be followed by the cardiology team. His HF is managed with furosemide as needed due to intolerance to GDMT.

demonstrating atrial fibrillation with controlled
ventricular response and low-voltage QRS.
Case 8
A 74-year-old male with history of bilateral CTS presented with right-sided chest pain associated with shortness of breath, diaphoresis, dizziness, and worsening abdominal pain. He was found to have inferior wall myocardial infarction on ECG with later percutaneous coronary intervention to the left circumflex. His hospital course was complicated by decompensated HF (EF 45% to 50%) and AF with rapid ventricular response. He was treated and discharged with follow-up visits scheduled in the cardiology clinic. Multiple attempts were made to place him on GDMT; however, the patient was unable to tolerate these medications due to recurrent admissions for syncope. During a cardiology clinic visit 3 years after his initial presentation, an amyloidosis workup was initiated. 99mTC pyrophosphate imaging was positive for ATTR-CM, and he started taking tafamidis. Before this diagnosis, ECG indicated low-voltage QRS complexes. His progression has since been complicated by admissions for decompensated HF, recurrent episodes of AF requiring atrioventricular node ablation, and biventricular implantable cardioverter-defibrillator implantation after failed attempts at electrical cardioversion. He continued to follow up in the HF clinic.
Discussion
ATTR-CM is an underdiagnosed cause of cardiomyopathy, particularly in older adults. TTR is a transport protein produced in the liver, and misfolding can occur due to age-related instability of the wild-type protein (wtATTR) or pathologic variants in the TTR (hATTR). The misfolding leads to restrictive physiology, HF (often with preserved EF) arrhythmias, and conduction system disease.1 It is likely that the predominantly older male veteran population would be predisposed to wtATTR cardiomyopathy given that misfolding in the condition is believed to be age-related.
Current criteria for ATTR diagnosis require a combination of clinical suspicion, imaging, laboratory testing, and, in some cases, tissue biopsy confirmation and genetic testing.1,4,5 The diagnostic algorithm is as follows:
Clinical suspicion. Consider ATTR in patients with unexplained HFpEF, LV wall thickness ≥ 12 to 14 mm, discordance between ECG voltage and wall thickness, or associated extracardiac manifestations such as CTS, lumbar spinal stenosis, or peripheral/ autonomic neuropathy.
Exclusion of AL amyloidosis. Bone scintigraphy alone cannot distinguish between AL amyloidosis and ATTR, so patients with suspected amyloid cardiomyopathy should undergo serum and urine immunofixation electrophoresis and serum free light chain assay to rule out a monoclonal gammopathy as seen in AL amyloidosis.
Cardiac scintigraphy. Once AL amyloidosis is excluded, a positive 99mTC-labeled boneavid tracer image (such as a pyrophosphate scan) with grade 2 or grade 3 myocardial uptake is diagnostic of ATTR.
Tissue biopsy. If there is monoclonal gammopathy or equivocal imaging, tissue biopsy (eg, endomyocardial) with Congo red staining and amyloid typing by mass spectrometry or immunohistochemistry is necessary.
Genetic testing. Once ATTR is confirmed, genetic testing distinguishes hATTR from wtATTR, which impacts management and determines the need to screen family members.
Currently, there are 3 therapies approved by the US Food and Drug Administration (FDA) to treat ATTR-CM: tafamidis, acoramidis, and vutrisiran.6-8 Tafamidis and acoramidis stabilize the TTR tetramer, preventing amyloid formation. Vutrisiran uses RNA interference to silence the gene that produces TTR. Tafamidis has been found to improve cardiovascular outcomes in ATTR-CM. In the ATTR-ACT trial, it reduced all-cause mortality and cardiovascular hospitalizations in patients with ATTR-CM and New York Heart Association class I-III symptoms.6 There are other disease-modifying therapies, such the TTR gene silencers inotersen and patisiran; however, these are only FDA-approved for hATTR polyneuropathy and not for ATTRCM; ongoing trials are evaluating their cardiac efficacy.
The mean age of ATTR-CM diagnosis in the patients described in this case series was 79 years, which is older than the mean age of 74 years reported in prior research.4 All patients were male, and the most common presenting symptom was dyspnea on exertion. Table 1 outlines baseline characteristics and associated comorbidities of patients in this case series. The patients presented with many red-flag signs of ATTR-CM (Figure 3). Among them included syncope (4 of 8 patients), spinal stenosis (2 of 8 patients), arrhythmia (7 of 8 patients), heart failure (7 of 8 patients), and bilateral CTS (all patients).
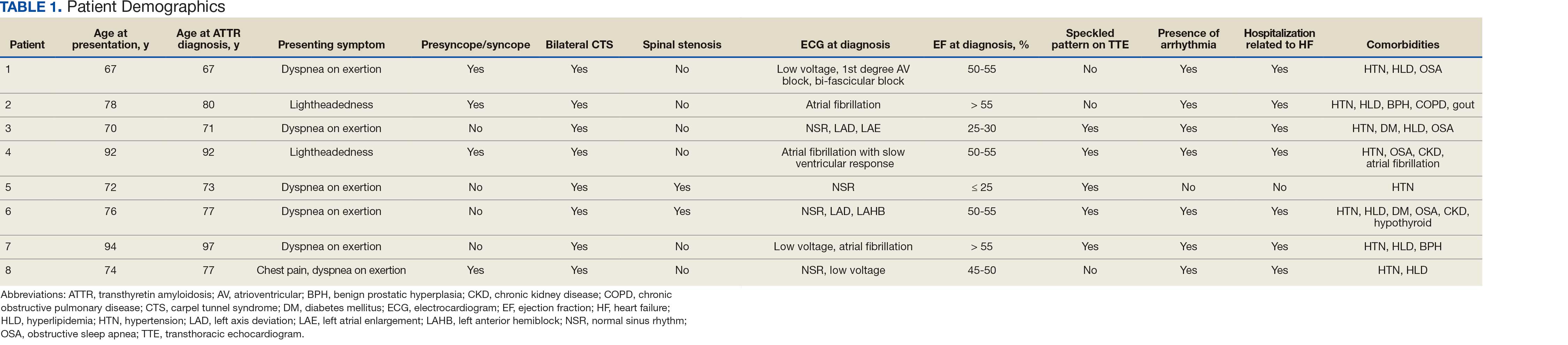
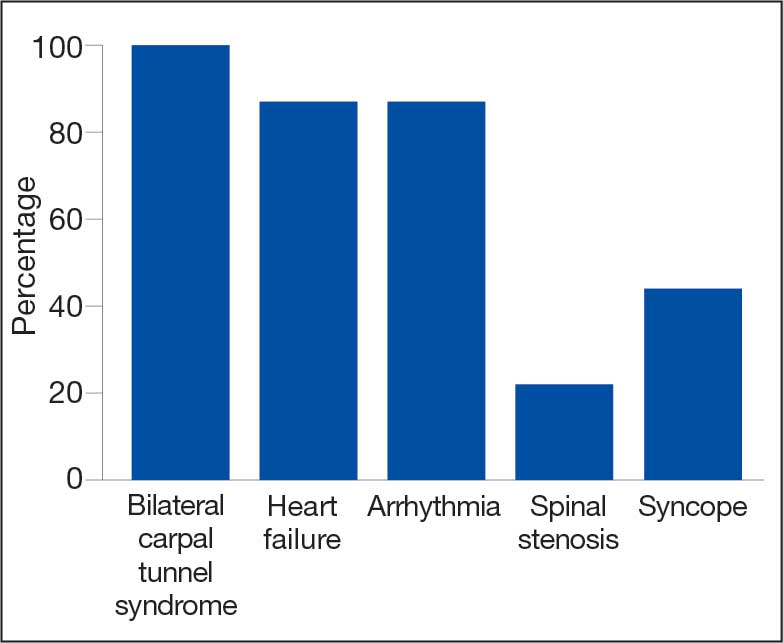
amyloidosis red-flag signs identified.
Bilateral CTS was diagnosed in all patients before their diagnosis of ATTR-CM. Patient 7 had a diagnosis of CTS 9 years before his ATTR-CM diagnosis, underscoring a subtle, yet important extracardiac sign that may increase clinical suspicion for ATTR-CM. Previous research found that the probability of having CTS is highest 5 to 9 years prior to the development of cardiomyopathy. Its presence is also a prognostic marker in ATTR, independent of cardiac involvement.9 The median interval between CTS diagnosis and cardiomyopathy diagnosis was 5 years in this series.
Although screening criteria for ATTR have been proposed, none have been incorporated into formal guidelines.10,11 We propose that a baseline ECG and screening TTE be obtained in any patient aged > 65 years with cardiac risk equivalents such as hypertension and diabetes, presenting with ≥ 1 extracardiac red-flag signs, such as bilateral CTS and spinal stenosis. This will likely facilitate an earlier diagnosis of ATTR-CM, leading to earlier treatment initiation and better patient outcomes. This initiative can be started in the primary care setting and facilitates early cardiology referral. This recommendation is based on literature supporting clinical patterns and observations the authors have made in clinical practice.
Obstructive sleep apnea (OSA) was a comorbidity present in 50% of the patients described in this case series. The literature describing this association is sparse; however, a prospective observational study reported that disorders of sleep inclusive of OSA are frequent in patients with cardiac amyloidosis.12 A theory behind this association is that amyloid deposits in the upper airway tissues lead to airway narrowing. 13 More research is needed to further assess the relationship between OSA and cardiac amyloidosis, particularly with respect to the timing of OSA prior to the development of cardiomyopathy as it may be a potential early sign for clinicians to acknowledge.
An important observation from this case series is the variability in the timing of tafamidis initiation relative to symptom onset and confirmed diagnosis of ATTR-CM (Table 2). Although tafamidis has been found to slow disease progression, several patients in this series began treatment at advanced stages or years after the onset of cardiac symptoms, potentially limiting its clinical benefit.
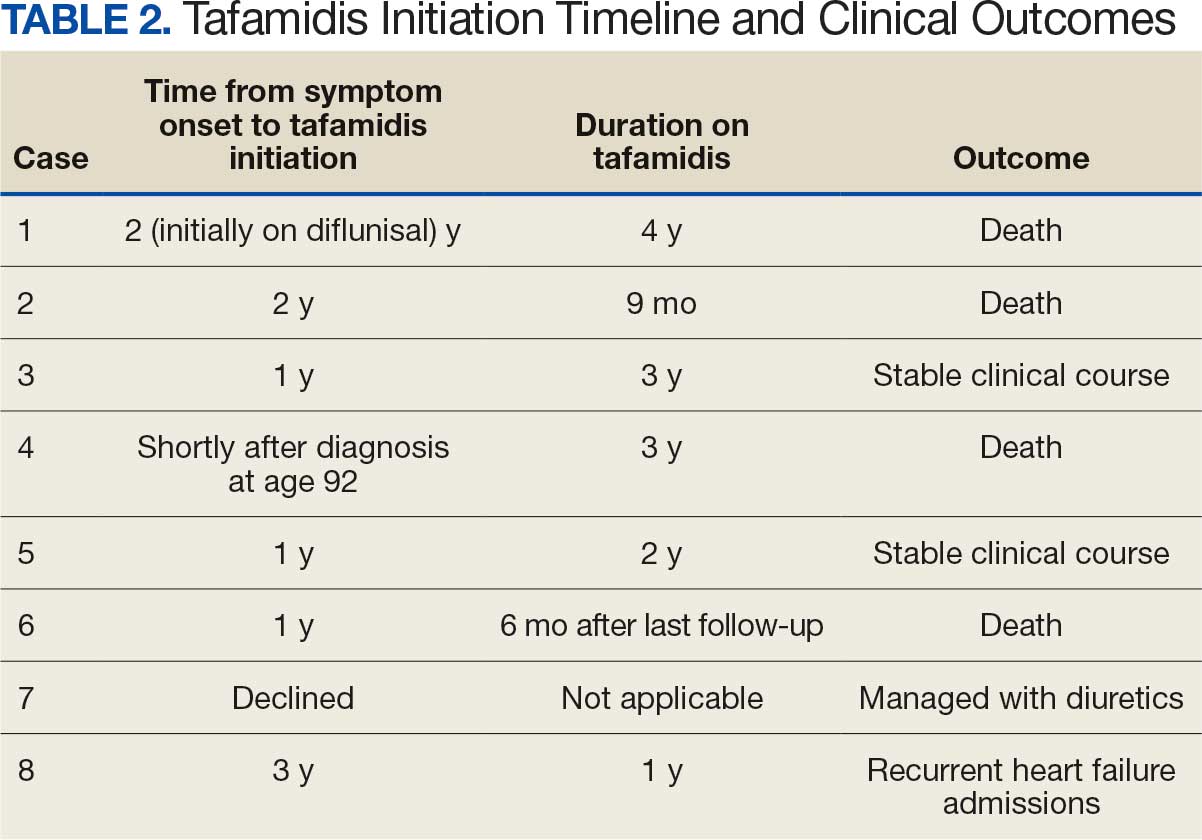
For example, patient 1 was diagnosed with ATTR 2 years before tafamidis became available on the market and was initially treated with diflunisal. Patients who started tafamidis earlier in the disease course (eg, patients 3 and 5) appeared to have better long-term outcomes, including an absence of heart failure hospitalizations after initiation. In contrast, patients with delayed treatment initiation (eg, patients 2, 6, and 8) experienced ongoing decompensations or early mortality. Patient 7 declined tafamidis, underscoring challenges in medication uptake among older adults. Randomized controlled trials are warranted to compare the effectiveness of tafamidis with other recently FDA-approved therapies, such as acoramidis and vutrisiran, particularly in terms of cardiovascular outcomes.
AF was the most common arrhythmia observed in these patients and may occur years before the development of HF symptoms in the setting of ATTR-CM. Due to inherent conduction system disease, AF in this population may have a controlled or slow ventricular response, as observed in patient 4. Patients with atrial fibrillation and cardiac amyloidosis should receive anticoagulation regardless of CHA2DS2- VASc score due to their high risk of intracardiac thrombus formation.4
Limitations
This case series lacked genetic testing following a confirmed ATTR-CM diagnosis. Although much of the treatment is the same regardless of the presence of a TTR mutation, knowing the specific subtype of ATTR-CM has implications for prognosis and for screening family members.
Conclusions
Following analysis of 8 patients diagnosed with ATTR, this case series could serve as a blueprint for research into ATTR in veterans. In clinical practice, following military service, veterans may not be routinely seen by an outpatient physician and may present with sequelae of advanced stages of ATTR. Early identification of red-flag symptoms can lead to a higher clinical suspicion, prompting early diagnostic evaluation and treatment initiation and ultimately mitigating adverse outcomes. Future research that includes genetic testing for those with confirmed ATTR-CM may prove useful as a foundation for detailed and informed discussions with patients and their families regarding prognosis and, if indicated, screening for family members.
- Kittleson MM, Maurer MS, Ambardekar AV, et al. Cardiac amyloidosis: evolving diagnosis and management: a scientific statement from the American Heart Association. Circulation. 2020;142:e7-e22. doi:10.1161/CIR.0000000000000792
- Dharmarajan K, Maurer MS. Transthyretin cardiac amyloidoses in older North Americans. J Am Geriatr Soc. 2012;60:765-774. doi:10.1111/j.1532-5415.2011.03868.x
- Nativi-Nicolau J, Redd A, Kelly N, et al. Increasing number of amyloidosis diagnosis in the Veterans Affairs populations. J Card Fail. 2019;25:S96.
- Ruberg FL, Grogan M, Hanna M, et al. Transthyretin amyloid cardiomyopathy: JACC state-of-the-art review. J Am Coll Cardiol. 2019;73:2872-2891. doi:10.1016/j.jacc.2019.04.003
- Gillmore JD, Maurer, Falk RH, et al. Nonbiopsy diagnosis of cardiac transthyretin amyloidosis. Circulation. 2016;133:2404-2412. doi:10.1161/CIRCULATIONAHA.116.021612
- Maurer MS, Schwartz JH, Gundapaneni B, et al. Tafamidis treatment for patients with transthyretin amyloid cardiomyopathy. N Engl J Med. 2018;379:1007-1016. doi:10.1056/NEJMoa1805689
- Gillmore JD, Judge DP, Cappelli F, et al. Efficacy and safety of acoramidis in transthyretin amyloid cardiomyopathy. N Engl J Med. 2024;390:132-142. doi:10.1056/NEJMoa2305434
- Fontana M, Berk JL, Gillmore JD, et al. Vutrisiran in patients with transthyretin amyloidosis with cardiomyopathy. N Engl J Med. 2025;392:33-44. doi:10.1056/NEJMoa2409134
- Milandri A, Farioli A, Gagliardi C, et al. Carpal tunnel syndrome in cardiac amyloidosis: implications for early diagnosis and prognostic role across the spectrum of aetiologies. Eur J Heart Fail. 2020;22:507-515. doi:10.1002/ejhf.1742
- Garcia-Pavia P, Rapezzi C, Adler Y, et al. Diagnosis and treatment of cardiac amyloidosis: a position statement of the ESC Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2021;42:1554-1568. doi:10.1093/eurheartj/ehab072
- Brito D, Albrecht FC, de Arenaza DP, et al. World Heart Federation consensus on transthyretin amyloidosis cardiomyopathy (ATTR-CM). Glob Heart. 2023;18:59. doi:10.5334/gh.1262
- Bodez D, Guellich A, Kharoubi M, et al. Prevalence, severity, and prognostic value of sleep apnea syndromes in cardiac amyloidosis. Sleep. 2016;39:1333-1341. doi:10.5665/sleep.5958
- Colaco B, Colaco C, Lipford M. A forgotten problem: sleep-disordered breathing in amyloidosis. Chest. 2016;150:1293A. doi:10.1016/j.chest.2016.08.1407
Transthyretin amyloid cardiomyopathy (ATTR-CM) is caused by the misfolding of the TTR protein, which results in aggregation of amyloid fibrils that deposit in the myocardium and causes restrictive cardiomyopathy. Though it remains underdiagnosed, ATTR-CM is increasingly being recognized as a cause of heart failure in geriatric patients.1 There are 2 categories of ATTRCM: wild-type ATTR-CM (wtATTR-CM), in which there is no mutation in the TTR gene, and hereditary ATTR-CM (hATTR-CM), in which a mutation is present in the TTR gene. Research has shown that wtATTR-CM accounted for as many as 30% of cases of heart failure (HF) with preserved ejection fraction (HFpEF) in patients aged > 75 years.2 A significant percentage of the veteran patient population consists of older males. Given their age, these patients are at greater risk for ATTR diagnosis.3
Identifying red flags for patients within this population may allow clinicians to make earlier diagnoses and improve outcomes. A high index of suspicion is needed to diagnose ATTR because many early signs and symptoms are extracardiac, which leads to delayed diagnoses and worse outcomes. This article describes 8 cases of ATTR-CM within the US Department of Veterans Affairs (VA) New York Harbor Healthcare System-Brooklyn (VANYHHSB).
Methods
This retrospective case series was reviewed and approved by the VANYHHSB Institutional Review Board where it was conducted. Patients diagnosed with ATTR between 2017 and 2024 were identified using International Classification of Diseases, Tenth Revision codes. Eleven patients were identified; 3 were excluded due to insufficient medical records. The remaining 8 patient records were retrospectively reviewed and included.
Case 1
A 67-year-old male with a history of carpal tunnel syndrome (CTS) presented following a syncopal episode. Initial electrocardiogram (ECG) showed sinus rhythm, first-degree atrioventricular block, and a bifascicular block. Transthoracic echocardiogram (TTE) showed moderate asymmetric left ventricular (LV) hypertrophy (LVH) and biatrial enlargement with an ejection fraction (EF) > 55%. The patient was discharged with a loop recorder and an outpatient follow-up appointment scheduled. One month later, he presented with worsening dyspnea on exertion with clinical signs of hypervolemia. A repeat TTE showed global LV wall thickening, moderately reduced LV systolic function (EF 40%), and moderate pulmonary hypertension. Given these findings, the patient underwent cardiac magnetic resonance imaging (CMR), which suggested an infiltrative cardiomyopathy. Amyloid light-chain (AL) amyloidosis evaluation, technetium-99m (99mTC) pyrophosphate imaging, and a fat pad biopsy were unrevealing. An endomyocardial biopsy was performed with electron microscopy, which confirmed amyloidosis. Genetic testing was negative, and the patient began taking tafamidis. There were no later admissions for decompensated HF; however, the patient developed atrial fibrillation (AF) and an interval TTE demonstrated no improvement in his EF. He died at age 73 years.
Case 2
A 78-year-old male with a history of CTS presented with lightheadedness. Initial ECG showed rate-controlled AF and TTE revealed a moderately thickened LV wall with normal LV size, mild left atrial enlargement, and an EF of 65%. The patient was discharged with a scheduled outpatient CMR appointment; however, he defaulted from follow-up. Two years later, he presented with recurrent syncopal episodes and physical examination was consistent with hypervolemia. Repeat TTE revealed moderate LVH, biatrial enlargement, and an EF of 55%. An inpatient CMR was suggestive of cardiac amyloidosis, and a pyrophosphate scan was diagnostic for ATTR. The patient started taking tafamidis, but continued to have recurrent admissions for HF exacerbation. He died at age 81 years.
Case 3
A 71-year-old male with a history of CTS presented with exertional dyspnea. The initial ECG showed sinus rhythm with left atrial enlargement and left axis deviation. Subsequent TTE revealed severe LVH, mildly reduced LV cavity size, moderate to severe biatrial enlargement, and an EF of 25% to 30%. Outpatient 99mTC pyrophosphate imaging suggested cardiac amyloidosis, and laboratory testing showed no evidence of monoclonal proteins. The patient was started on tafamidis for ATTR. At 2-year follow-up, he had new AF and to date has had no further hospitalizations for acute decompensated HF.
Case 4
A 92-year-old male with a history of AF and bilateral CTS presented with lightheadedness. An ECG revealed AF with a slowed ventricular response. Subsequent Holter monitoring demonstrated pauses exceeding 3 seconds, and a permanent pacemaker was recommended. During his preoperative evaluation, TTE revealed severe concentric LVH with a speckled appearance of the myocardium, mild-tomoderate biatrial enlargement, and an EF of 50% to 55%. 99mTC pyrophosphate imaging was positive for amyloidosis and the patient started taking tafamidis. Recurrent hospital admissions for decompensated HF complicated his progression. The patient died at age 95 years.
Case 5
A 72-year-old male with a history of bilateral CTS and cervical spinal stenosis presented with dyspnea on exertion. An ECG revealed a normal sinus rhythm. A TTE found severely reduced systolic function with an EF ≤ 25%, mild concentric LVH, grade 3 diastolic dysfunction, mild-tomoderate biatrial enlargement, and moderate pulmonary hypertension (Figure 1). He was started on guideline-directed medical therapy (GDMT) for HF, which included sacubitril/valsartan, metoprolol succinate, and empagliflozin. The patient’s dyspnea improved, and a workup for nonischemic cardiomyopathy was initiated. 99mTC pyrophosphate imaging 1 year after his initial presentation was positive, leading to ATTR-CM diagnosis. The patient started taking tafamidis and he has since had a stable progression and continued to demonstrate good exercise tolerance with no hospitalizations. His most recent TTE indicated an EF of 40% to 45%.
(parasternal long axis view) of patient 5
demonstrating concentric left ventricular
hypertrophy with a speckled myocardium
and dilated left atrium.
Case 6
A 76-year-old male with a history of paroxysmal AF status after multiple ablations, bilateral CTS, and severe cervical spinal stenosis presented with dyspnea on exertion. The patient’s ECG showed normal sinus rhythm and left axis deviation with concern for left anterior hemiblock. A TTE revealed moderate LVH with a speckled appearance of the myocardium and grade 3 diastolic dysfunction with preserved EF. Before completing the workup for underlying cardiomyopathy, the patient underwent an interventional radiology procedure for an angiomyolipoma, and his postoperative course was complicated by pulmonary edema, requiring admission to the coronary care unit for diuresis. A repeat TTE revealed a reduced EF of 35%, and he was discharged on GDMT. No monoclonal protein was seen in the serum or urine. The patient’s progression was complicated by recurrent admissions for acute decompensated HF and supraventricular tachycardia despite being on amiodarone, which led to a delay in obtaining 99mTC pyrophosphate imaging. Due to hypotension, the patient was unable to tolerate GDMT. He eventually underwent 99mTC pyrophosphate imaging that confirmed ATTR-CM and was started on tafamidis. One year following initial presentation, the patient’s EF progressively declined to 20% to 25%, and he died shortly after discharge to subacute rehabilitation.
Case 7
A 95-year-old male with a history of longstanding persistent AF and bilateral CTS presented with dyspnea on exertion, bendopnea, and worsening bilateral pedal edema for a week. An ECG showed AF with a controlled ventricular response and low-voltage QRS waves (Figure 2). A TTE showed biatrial enlargement, LVH, and preserved EF > 55%. He started taking furosemide and was discharged with a diagnosis of HFpEF. The patient missed cardiology follow-up and presented 1 year later with decompensated HF. An amyloidosis workup was recommended, but due to intermittent periods of being lost to follow-up, the patient did not pursue this workup until 3 years after his initial presentation when 99mTC pyrophosphate imaging confirmed ATTR-CM. The patient declined tafamidis and continued to be followed by the cardiology team. His HF is managed with furosemide as needed due to intolerance to GDMT.
demonstrating atrial fibrillation with controlled
ventricular response and low-voltage QRS.
Case 8
A 74-year-old male with history of bilateral CTS presented with right-sided chest pain associated with shortness of breath, diaphoresis, dizziness, and worsening abdominal pain. He was found to have inferior wall myocardial infarction on ECG with later percutaneous coronary intervention to the left circumflex. His hospital course was complicated by decompensated HF (EF 45% to 50%) and AF with rapid ventricular response. He was treated and discharged with follow-up visits scheduled in the cardiology clinic. Multiple attempts were made to place him on GDMT; however, the patient was unable to tolerate these medications due to recurrent admissions for syncope. During a cardiology clinic visit 3 years after his initial presentation, an amyloidosis workup was initiated. 99mTC pyrophosphate imaging was positive for ATTR-CM, and he started taking tafamidis. Before this diagnosis, ECG indicated low-voltage QRS complexes. His progression has since been complicated by admissions for decompensated HF, recurrent episodes of AF requiring atrioventricular node ablation, and biventricular implantable cardioverter-defibrillator implantation after failed attempts at electrical cardioversion. He continued to follow up in the HF clinic.
Discussion
ATTR-CM is an underdiagnosed cause of cardiomyopathy, particularly in older adults. TTR is a transport protein produced in the liver, and misfolding can occur due to age-related instability of the wild-type protein (wtATTR) or pathologic variants in the TTR (hATTR). The misfolding leads to restrictive physiology, HF (often with preserved EF) arrhythmias, and conduction system disease.1 It is likely that the predominantly older male veteran population would be predisposed to wtATTR cardiomyopathy given that misfolding in the condition is believed to be age-related.
Current criteria for ATTR diagnosis require a combination of clinical suspicion, imaging, laboratory testing, and, in some cases, tissue biopsy confirmation and genetic testing.1,4,5 The diagnostic algorithm is as follows:
Clinical suspicion. Consider ATTR in patients with unexplained HFpEF, LV wall thickness ≥ 12 to 14 mm, discordance between ECG voltage and wall thickness, or associated extracardiac manifestations such as CTS, lumbar spinal stenosis, or peripheral/ autonomic neuropathy.
Exclusion of AL amyloidosis. Bone scintigraphy alone cannot distinguish between AL amyloidosis and ATTR, so patients with suspected amyloid cardiomyopathy should undergo serum and urine immunofixation electrophoresis and serum free light chain assay to rule out a monoclonal gammopathy as seen in AL amyloidosis.
Cardiac scintigraphy. Once AL amyloidosis is excluded, a positive 99mTC-labeled boneavid tracer image (such as a pyrophosphate scan) with grade 2 or grade 3 myocardial uptake is diagnostic of ATTR.
Tissue biopsy. If there is monoclonal gammopathy or equivocal imaging, tissue biopsy (eg, endomyocardial) with Congo red staining and amyloid typing by mass spectrometry or immunohistochemistry is necessary.
Genetic testing. Once ATTR is confirmed, genetic testing distinguishes hATTR from wtATTR, which impacts management and determines the need to screen family members.
Currently, there are 3 therapies approved by the US Food and Drug Administration (FDA) to treat ATTR-CM: tafamidis, acoramidis, and vutrisiran.6-8 Tafamidis and acoramidis stabilize the TTR tetramer, preventing amyloid formation. Vutrisiran uses RNA interference to silence the gene that produces TTR. Tafamidis has been found to improve cardiovascular outcomes in ATTR-CM. In the ATTR-ACT trial, it reduced all-cause mortality and cardiovascular hospitalizations in patients with ATTR-CM and New York Heart Association class I-III symptoms.6 There are other disease-modifying therapies, such the TTR gene silencers inotersen and patisiran; however, these are only FDA-approved for hATTR polyneuropathy and not for ATTRCM; ongoing trials are evaluating their cardiac efficacy.
The mean age of ATTR-CM diagnosis in the patients described in this case series was 79 years, which is older than the mean age of 74 years reported in prior research.4 All patients were male, and the most common presenting symptom was dyspnea on exertion. Table 1 outlines baseline characteristics and associated comorbidities of patients in this case series. The patients presented with many red-flag signs of ATTR-CM (Figure 3). Among them included syncope (4 of 8 patients), spinal stenosis (2 of 8 patients), arrhythmia (7 of 8 patients), heart failure (7 of 8 patients), and bilateral CTS (all patients).
amyloidosis red-flag signs identified.
Bilateral CTS was diagnosed in all patients before their diagnosis of ATTR-CM. Patient 7 had a diagnosis of CTS 9 years before his ATTR-CM diagnosis, underscoring a subtle, yet important extracardiac sign that may increase clinical suspicion for ATTR-CM. Previous research found that the probability of having CTS is highest 5 to 9 years prior to the development of cardiomyopathy. Its presence is also a prognostic marker in ATTR, independent of cardiac involvement.9 The median interval between CTS diagnosis and cardiomyopathy diagnosis was 5 years in this series.
Although screening criteria for ATTR have been proposed, none have been incorporated into formal guidelines.10,11 We propose that a baseline ECG and screening TTE be obtained in any patient aged > 65 years with cardiac risk equivalents such as hypertension and diabetes, presenting with ≥ 1 extracardiac red-flag signs, such as bilateral CTS and spinal stenosis. This will likely facilitate an earlier diagnosis of ATTR-CM, leading to earlier treatment initiation and better patient outcomes. This initiative can be started in the primary care setting and facilitates early cardiology referral. This recommendation is based on literature supporting clinical patterns and observations the authors have made in clinical practice.
Obstructive sleep apnea (OSA) was a comorbidity present in 50% of the patients described in this case series. The literature describing this association is sparse; however, a prospective observational study reported that disorders of sleep inclusive of OSA are frequent in patients with cardiac amyloidosis.12 A theory behind this association is that amyloid deposits in the upper airway tissues lead to airway narrowing. 13 More research is needed to further assess the relationship between OSA and cardiac amyloidosis, particularly with respect to the timing of OSA prior to the development of cardiomyopathy as it may be a potential early sign for clinicians to acknowledge.
An important observation from this case series is the variability in the timing of tafamidis initiation relative to symptom onset and confirmed diagnosis of ATTR-CM (Table 2). Although tafamidis has been found to slow disease progression, several patients in this series began treatment at advanced stages or years after the onset of cardiac symptoms, potentially limiting its clinical benefit.
For example, patient 1 was diagnosed with ATTR 2 years before tafamidis became available on the market and was initially treated with diflunisal. Patients who started tafamidis earlier in the disease course (eg, patients 3 and 5) appeared to have better long-term outcomes, including an absence of heart failure hospitalizations after initiation. In contrast, patients with delayed treatment initiation (eg, patients 2, 6, and 8) experienced ongoing decompensations or early mortality. Patient 7 declined tafamidis, underscoring challenges in medication uptake among older adults. Randomized controlled trials are warranted to compare the effectiveness of tafamidis with other recently FDA-approved therapies, such as acoramidis and vutrisiran, particularly in terms of cardiovascular outcomes.
AF was the most common arrhythmia observed in these patients and may occur years before the development of HF symptoms in the setting of ATTR-CM. Due to inherent conduction system disease, AF in this population may have a controlled or slow ventricular response, as observed in patient 4. Patients with atrial fibrillation and cardiac amyloidosis should receive anticoagulation regardless of CHA2DS2- VASc score due to their high risk of intracardiac thrombus formation.4
Limitations
This case series lacked genetic testing following a confirmed ATTR-CM diagnosis. Although much of the treatment is the same regardless of the presence of a TTR mutation, knowing the specific subtype of ATTR-CM has implications for prognosis and for screening family members.
Conclusions
Following analysis of 8 patients diagnosed with ATTR, this case series could serve as a blueprint for research into ATTR in veterans. In clinical practice, following military service, veterans may not be routinely seen by an outpatient physician and may present with sequelae of advanced stages of ATTR. Early identification of red-flag symptoms can lead to a higher clinical suspicion, prompting early diagnostic evaluation and treatment initiation and ultimately mitigating adverse outcomes. Future research that includes genetic testing for those with confirmed ATTR-CM may prove useful as a foundation for detailed and informed discussions with patients and their families regarding prognosis and, if indicated, screening for family members.
Transthyretin amyloid cardiomyopathy (ATTR-CM) is caused by the misfolding of the TTR protein, which results in aggregation of amyloid fibrils that deposit in the myocardium and causes restrictive cardiomyopathy. Though it remains underdiagnosed, ATTR-CM is increasingly being recognized as a cause of heart failure in geriatric patients.1 There are 2 categories of ATTRCM: wild-type ATTR-CM (wtATTR-CM), in which there is no mutation in the TTR gene, and hereditary ATTR-CM (hATTR-CM), in which a mutation is present in the TTR gene. Research has shown that wtATTR-CM accounted for as many as 30% of cases of heart failure (HF) with preserved ejection fraction (HFpEF) in patients aged > 75 years.2 A significant percentage of the veteran patient population consists of older males. Given their age, these patients are at greater risk for ATTR diagnosis.3
Identifying red flags for patients within this population may allow clinicians to make earlier diagnoses and improve outcomes. A high index of suspicion is needed to diagnose ATTR because many early signs and symptoms are extracardiac, which leads to delayed diagnoses and worse outcomes. This article describes 8 cases of ATTR-CM within the US Department of Veterans Affairs (VA) New York Harbor Healthcare System-Brooklyn (VANYHHSB).
Methods
This retrospective case series was reviewed and approved by the VANYHHSB Institutional Review Board where it was conducted. Patients diagnosed with ATTR between 2017 and 2024 were identified using International Classification of Diseases, Tenth Revision codes. Eleven patients were identified; 3 were excluded due to insufficient medical records. The remaining 8 patient records were retrospectively reviewed and included.
Case 1
A 67-year-old male with a history of carpal tunnel syndrome (CTS) presented following a syncopal episode. Initial electrocardiogram (ECG) showed sinus rhythm, first-degree atrioventricular block, and a bifascicular block. Transthoracic echocardiogram (TTE) showed moderate asymmetric left ventricular (LV) hypertrophy (LVH) and biatrial enlargement with an ejection fraction (EF) > 55%. The patient was discharged with a loop recorder and an outpatient follow-up appointment scheduled. One month later, he presented with worsening dyspnea on exertion with clinical signs of hypervolemia. A repeat TTE showed global LV wall thickening, moderately reduced LV systolic function (EF 40%), and moderate pulmonary hypertension. Given these findings, the patient underwent cardiac magnetic resonance imaging (CMR), which suggested an infiltrative cardiomyopathy. Amyloid light-chain (AL) amyloidosis evaluation, technetium-99m (99mTC) pyrophosphate imaging, and a fat pad biopsy were unrevealing. An endomyocardial biopsy was performed with electron microscopy, which confirmed amyloidosis. Genetic testing was negative, and the patient began taking tafamidis. There were no later admissions for decompensated HF; however, the patient developed atrial fibrillation (AF) and an interval TTE demonstrated no improvement in his EF. He died at age 73 years.
Case 2
A 78-year-old male with a history of CTS presented with lightheadedness. Initial ECG showed rate-controlled AF and TTE revealed a moderately thickened LV wall with normal LV size, mild left atrial enlargement, and an EF of 65%. The patient was discharged with a scheduled outpatient CMR appointment; however, he defaulted from follow-up. Two years later, he presented with recurrent syncopal episodes and physical examination was consistent with hypervolemia. Repeat TTE revealed moderate LVH, biatrial enlargement, and an EF of 55%. An inpatient CMR was suggestive of cardiac amyloidosis, and a pyrophosphate scan was diagnostic for ATTR. The patient started taking tafamidis, but continued to have recurrent admissions for HF exacerbation. He died at age 81 years.
Case 3
A 71-year-old male with a history of CTS presented with exertional dyspnea. The initial ECG showed sinus rhythm with left atrial enlargement and left axis deviation. Subsequent TTE revealed severe LVH, mildly reduced LV cavity size, moderate to severe biatrial enlargement, and an EF of 25% to 30%. Outpatient 99mTC pyrophosphate imaging suggested cardiac amyloidosis, and laboratory testing showed no evidence of monoclonal proteins. The patient was started on tafamidis for ATTR. At 2-year follow-up, he had new AF and to date has had no further hospitalizations for acute decompensated HF.
Case 4
A 92-year-old male with a history of AF and bilateral CTS presented with lightheadedness. An ECG revealed AF with a slowed ventricular response. Subsequent Holter monitoring demonstrated pauses exceeding 3 seconds, and a permanent pacemaker was recommended. During his preoperative evaluation, TTE revealed severe concentric LVH with a speckled appearance of the myocardium, mild-tomoderate biatrial enlargement, and an EF of 50% to 55%. 99mTC pyrophosphate imaging was positive for amyloidosis and the patient started taking tafamidis. Recurrent hospital admissions for decompensated HF complicated his progression. The patient died at age 95 years.
Case 5
A 72-year-old male with a history of bilateral CTS and cervical spinal stenosis presented with dyspnea on exertion. An ECG revealed a normal sinus rhythm. A TTE found severely reduced systolic function with an EF ≤ 25%, mild concentric LVH, grade 3 diastolic dysfunction, mild-tomoderate biatrial enlargement, and moderate pulmonary hypertension (Figure 1). He was started on guideline-directed medical therapy (GDMT) for HF, which included sacubitril/valsartan, metoprolol succinate, and empagliflozin. The patient’s dyspnea improved, and a workup for nonischemic cardiomyopathy was initiated. 99mTC pyrophosphate imaging 1 year after his initial presentation was positive, leading to ATTR-CM diagnosis. The patient started taking tafamidis and he has since had a stable progression and continued to demonstrate good exercise tolerance with no hospitalizations. His most recent TTE indicated an EF of 40% to 45%.
(parasternal long axis view) of patient 5
demonstrating concentric left ventricular
hypertrophy with a speckled myocardium
and dilated left atrium.
Case 6
A 76-year-old male with a history of paroxysmal AF status after multiple ablations, bilateral CTS, and severe cervical spinal stenosis presented with dyspnea on exertion. The patient’s ECG showed normal sinus rhythm and left axis deviation with concern for left anterior hemiblock. A TTE revealed moderate LVH with a speckled appearance of the myocardium and grade 3 diastolic dysfunction with preserved EF. Before completing the workup for underlying cardiomyopathy, the patient underwent an interventional radiology procedure for an angiomyolipoma, and his postoperative course was complicated by pulmonary edema, requiring admission to the coronary care unit for diuresis. A repeat TTE revealed a reduced EF of 35%, and he was discharged on GDMT. No monoclonal protein was seen in the serum or urine. The patient’s progression was complicated by recurrent admissions for acute decompensated HF and supraventricular tachycardia despite being on amiodarone, which led to a delay in obtaining 99mTC pyrophosphate imaging. Due to hypotension, the patient was unable to tolerate GDMT. He eventually underwent 99mTC pyrophosphate imaging that confirmed ATTR-CM and was started on tafamidis. One year following initial presentation, the patient’s EF progressively declined to 20% to 25%, and he died shortly after discharge to subacute rehabilitation.
Case 7
A 95-year-old male with a history of longstanding persistent AF and bilateral CTS presented with dyspnea on exertion, bendopnea, and worsening bilateral pedal edema for a week. An ECG showed AF with a controlled ventricular response and low-voltage QRS waves (Figure 2). A TTE showed biatrial enlargement, LVH, and preserved EF > 55%. He started taking furosemide and was discharged with a diagnosis of HFpEF. The patient missed cardiology follow-up and presented 1 year later with decompensated HF. An amyloidosis workup was recommended, but due to intermittent periods of being lost to follow-up, the patient did not pursue this workup until 3 years after his initial presentation when 99mTC pyrophosphate imaging confirmed ATTR-CM. The patient declined tafamidis and continued to be followed by the cardiology team. His HF is managed with furosemide as needed due to intolerance to GDMT.
demonstrating atrial fibrillation with controlled
ventricular response and low-voltage QRS.
Case 8
A 74-year-old male with history of bilateral CTS presented with right-sided chest pain associated with shortness of breath, diaphoresis, dizziness, and worsening abdominal pain. He was found to have inferior wall myocardial infarction on ECG with later percutaneous coronary intervention to the left circumflex. His hospital course was complicated by decompensated HF (EF 45% to 50%) and AF with rapid ventricular response. He was treated and discharged with follow-up visits scheduled in the cardiology clinic. Multiple attempts were made to place him on GDMT; however, the patient was unable to tolerate these medications due to recurrent admissions for syncope. During a cardiology clinic visit 3 years after his initial presentation, an amyloidosis workup was initiated. 99mTC pyrophosphate imaging was positive for ATTR-CM, and he started taking tafamidis. Before this diagnosis, ECG indicated low-voltage QRS complexes. His progression has since been complicated by admissions for decompensated HF, recurrent episodes of AF requiring atrioventricular node ablation, and biventricular implantable cardioverter-defibrillator implantation after failed attempts at electrical cardioversion. He continued to follow up in the HF clinic.
Discussion
ATTR-CM is an underdiagnosed cause of cardiomyopathy, particularly in older adults. TTR is a transport protein produced in the liver, and misfolding can occur due to age-related instability of the wild-type protein (wtATTR) or pathologic variants in the TTR (hATTR). The misfolding leads to restrictive physiology, HF (often with preserved EF) arrhythmias, and conduction system disease.1 It is likely that the predominantly older male veteran population would be predisposed to wtATTR cardiomyopathy given that misfolding in the condition is believed to be age-related.
Current criteria for ATTR diagnosis require a combination of clinical suspicion, imaging, laboratory testing, and, in some cases, tissue biopsy confirmation and genetic testing.1,4,5 The diagnostic algorithm is as follows:
Clinical suspicion. Consider ATTR in patients with unexplained HFpEF, LV wall thickness ≥ 12 to 14 mm, discordance between ECG voltage and wall thickness, or associated extracardiac manifestations such as CTS, lumbar spinal stenosis, or peripheral/ autonomic neuropathy.
Exclusion of AL amyloidosis. Bone scintigraphy alone cannot distinguish between AL amyloidosis and ATTR, so patients with suspected amyloid cardiomyopathy should undergo serum and urine immunofixation electrophoresis and serum free light chain assay to rule out a monoclonal gammopathy as seen in AL amyloidosis.
Cardiac scintigraphy. Once AL amyloidosis is excluded, a positive 99mTC-labeled boneavid tracer image (such as a pyrophosphate scan) with grade 2 or grade 3 myocardial uptake is diagnostic of ATTR.
Tissue biopsy. If there is monoclonal gammopathy or equivocal imaging, tissue biopsy (eg, endomyocardial) with Congo red staining and amyloid typing by mass spectrometry or immunohistochemistry is necessary.
Genetic testing. Once ATTR is confirmed, genetic testing distinguishes hATTR from wtATTR, which impacts management and determines the need to screen family members.
Currently, there are 3 therapies approved by the US Food and Drug Administration (FDA) to treat ATTR-CM: tafamidis, acoramidis, and vutrisiran.6-8 Tafamidis and acoramidis stabilize the TTR tetramer, preventing amyloid formation. Vutrisiran uses RNA interference to silence the gene that produces TTR. Tafamidis has been found to improve cardiovascular outcomes in ATTR-CM. In the ATTR-ACT trial, it reduced all-cause mortality and cardiovascular hospitalizations in patients with ATTR-CM and New York Heart Association class I-III symptoms.6 There are other disease-modifying therapies, such the TTR gene silencers inotersen and patisiran; however, these are only FDA-approved for hATTR polyneuropathy and not for ATTRCM; ongoing trials are evaluating their cardiac efficacy.
The mean age of ATTR-CM diagnosis in the patients described in this case series was 79 years, which is older than the mean age of 74 years reported in prior research.4 All patients were male, and the most common presenting symptom was dyspnea on exertion. Table 1 outlines baseline characteristics and associated comorbidities of patients in this case series. The patients presented with many red-flag signs of ATTR-CM (Figure 3). Among them included syncope (4 of 8 patients), spinal stenosis (2 of 8 patients), arrhythmia (7 of 8 patients), heart failure (7 of 8 patients), and bilateral CTS (all patients).
amyloidosis red-flag signs identified.
Bilateral CTS was diagnosed in all patients before their diagnosis of ATTR-CM. Patient 7 had a diagnosis of CTS 9 years before his ATTR-CM diagnosis, underscoring a subtle, yet important extracardiac sign that may increase clinical suspicion for ATTR-CM. Previous research found that the probability of having CTS is highest 5 to 9 years prior to the development of cardiomyopathy. Its presence is also a prognostic marker in ATTR, independent of cardiac involvement.9 The median interval between CTS diagnosis and cardiomyopathy diagnosis was 5 years in this series.
Although screening criteria for ATTR have been proposed, none have been incorporated into formal guidelines.10,11 We propose that a baseline ECG and screening TTE be obtained in any patient aged > 65 years with cardiac risk equivalents such as hypertension and diabetes, presenting with ≥ 1 extracardiac red-flag signs, such as bilateral CTS and spinal stenosis. This will likely facilitate an earlier diagnosis of ATTR-CM, leading to earlier treatment initiation and better patient outcomes. This initiative can be started in the primary care setting and facilitates early cardiology referral. This recommendation is based on literature supporting clinical patterns and observations the authors have made in clinical practice.
Obstructive sleep apnea (OSA) was a comorbidity present in 50% of the patients described in this case series. The literature describing this association is sparse; however, a prospective observational study reported that disorders of sleep inclusive of OSA are frequent in patients with cardiac amyloidosis.12 A theory behind this association is that amyloid deposits in the upper airway tissues lead to airway narrowing. 13 More research is needed to further assess the relationship between OSA and cardiac amyloidosis, particularly with respect to the timing of OSA prior to the development of cardiomyopathy as it may be a potential early sign for clinicians to acknowledge.
An important observation from this case series is the variability in the timing of tafamidis initiation relative to symptom onset and confirmed diagnosis of ATTR-CM (Table 2). Although tafamidis has been found to slow disease progression, several patients in this series began treatment at advanced stages or years after the onset of cardiac symptoms, potentially limiting its clinical benefit.
For example, patient 1 was diagnosed with ATTR 2 years before tafamidis became available on the market and was initially treated with diflunisal. Patients who started tafamidis earlier in the disease course (eg, patients 3 and 5) appeared to have better long-term outcomes, including an absence of heart failure hospitalizations after initiation. In contrast, patients with delayed treatment initiation (eg, patients 2, 6, and 8) experienced ongoing decompensations or early mortality. Patient 7 declined tafamidis, underscoring challenges in medication uptake among older adults. Randomized controlled trials are warranted to compare the effectiveness of tafamidis with other recently FDA-approved therapies, such as acoramidis and vutrisiran, particularly in terms of cardiovascular outcomes.
AF was the most common arrhythmia observed in these patients and may occur years before the development of HF symptoms in the setting of ATTR-CM. Due to inherent conduction system disease, AF in this population may have a controlled or slow ventricular response, as observed in patient 4. Patients with atrial fibrillation and cardiac amyloidosis should receive anticoagulation regardless of CHA2DS2- VASc score due to their high risk of intracardiac thrombus formation.4
Limitations
This case series lacked genetic testing following a confirmed ATTR-CM diagnosis. Although much of the treatment is the same regardless of the presence of a TTR mutation, knowing the specific subtype of ATTR-CM has implications for prognosis and for screening family members.
Conclusions
Following analysis of 8 patients diagnosed with ATTR, this case series could serve as a blueprint for research into ATTR in veterans. In clinical practice, following military service, veterans may not be routinely seen by an outpatient physician and may present with sequelae of advanced stages of ATTR. Early identification of red-flag symptoms can lead to a higher clinical suspicion, prompting early diagnostic evaluation and treatment initiation and ultimately mitigating adverse outcomes. Future research that includes genetic testing for those with confirmed ATTR-CM may prove useful as a foundation for detailed and informed discussions with patients and their families regarding prognosis and, if indicated, screening for family members.
- Kittleson MM, Maurer MS, Ambardekar AV, et al. Cardiac amyloidosis: evolving diagnosis and management: a scientific statement from the American Heart Association. Circulation. 2020;142:e7-e22. doi:10.1161/CIR.0000000000000792
- Dharmarajan K, Maurer MS. Transthyretin cardiac amyloidoses in older North Americans. J Am Geriatr Soc. 2012;60:765-774. doi:10.1111/j.1532-5415.2011.03868.x
- Nativi-Nicolau J, Redd A, Kelly N, et al. Increasing number of amyloidosis diagnosis in the Veterans Affairs populations. J Card Fail. 2019;25:S96.
- Ruberg FL, Grogan M, Hanna M, et al. Transthyretin amyloid cardiomyopathy: JACC state-of-the-art review. J Am Coll Cardiol. 2019;73:2872-2891. doi:10.1016/j.jacc.2019.04.003
- Gillmore JD, Maurer, Falk RH, et al. Nonbiopsy diagnosis of cardiac transthyretin amyloidosis. Circulation. 2016;133:2404-2412. doi:10.1161/CIRCULATIONAHA.116.021612
- Maurer MS, Schwartz JH, Gundapaneni B, et al. Tafamidis treatment for patients with transthyretin amyloid cardiomyopathy. N Engl J Med. 2018;379:1007-1016. doi:10.1056/NEJMoa1805689
- Gillmore JD, Judge DP, Cappelli F, et al. Efficacy and safety of acoramidis in transthyretin amyloid cardiomyopathy. N Engl J Med. 2024;390:132-142. doi:10.1056/NEJMoa2305434
- Fontana M, Berk JL, Gillmore JD, et al. Vutrisiran in patients with transthyretin amyloidosis with cardiomyopathy. N Engl J Med. 2025;392:33-44. doi:10.1056/NEJMoa2409134
- Milandri A, Farioli A, Gagliardi C, et al. Carpal tunnel syndrome in cardiac amyloidosis: implications for early diagnosis and prognostic role across the spectrum of aetiologies. Eur J Heart Fail. 2020;22:507-515. doi:10.1002/ejhf.1742
- Garcia-Pavia P, Rapezzi C, Adler Y, et al. Diagnosis and treatment of cardiac amyloidosis: a position statement of the ESC Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2021;42:1554-1568. doi:10.1093/eurheartj/ehab072
- Brito D, Albrecht FC, de Arenaza DP, et al. World Heart Federation consensus on transthyretin amyloidosis cardiomyopathy (ATTR-CM). Glob Heart. 2023;18:59. doi:10.5334/gh.1262
- Bodez D, Guellich A, Kharoubi M, et al. Prevalence, severity, and prognostic value of sleep apnea syndromes in cardiac amyloidosis. Sleep. 2016;39:1333-1341. doi:10.5665/sleep.5958
- Colaco B, Colaco C, Lipford M. A forgotten problem: sleep-disordered breathing in amyloidosis. Chest. 2016;150:1293A. doi:10.1016/j.chest.2016.08.1407
- Kittleson MM, Maurer MS, Ambardekar AV, et al. Cardiac amyloidosis: evolving diagnosis and management: a scientific statement from the American Heart Association. Circulation. 2020;142:e7-e22. doi:10.1161/CIR.0000000000000792
- Dharmarajan K, Maurer MS. Transthyretin cardiac amyloidoses in older North Americans. J Am Geriatr Soc. 2012;60:765-774. doi:10.1111/j.1532-5415.2011.03868.x
- Nativi-Nicolau J, Redd A, Kelly N, et al. Increasing number of amyloidosis diagnosis in the Veterans Affairs populations. J Card Fail. 2019;25:S96.
- Ruberg FL, Grogan M, Hanna M, et al. Transthyretin amyloid cardiomyopathy: JACC state-of-the-art review. J Am Coll Cardiol. 2019;73:2872-2891. doi:10.1016/j.jacc.2019.04.003
- Gillmore JD, Maurer, Falk RH, et al. Nonbiopsy diagnosis of cardiac transthyretin amyloidosis. Circulation. 2016;133:2404-2412. doi:10.1161/CIRCULATIONAHA.116.021612
- Maurer MS, Schwartz JH, Gundapaneni B, et al. Tafamidis treatment for patients with transthyretin amyloid cardiomyopathy. N Engl J Med. 2018;379:1007-1016. doi:10.1056/NEJMoa1805689
- Gillmore JD, Judge DP, Cappelli F, et al. Efficacy and safety of acoramidis in transthyretin amyloid cardiomyopathy. N Engl J Med. 2024;390:132-142. doi:10.1056/NEJMoa2305434
- Fontana M, Berk JL, Gillmore JD, et al. Vutrisiran in patients with transthyretin amyloidosis with cardiomyopathy. N Engl J Med. 2025;392:33-44. doi:10.1056/NEJMoa2409134
- Milandri A, Farioli A, Gagliardi C, et al. Carpal tunnel syndrome in cardiac amyloidosis: implications for early diagnosis and prognostic role across the spectrum of aetiologies. Eur J Heart Fail. 2020;22:507-515. doi:10.1002/ejhf.1742
- Garcia-Pavia P, Rapezzi C, Adler Y, et al. Diagnosis and treatment of cardiac amyloidosis: a position statement of the ESC Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2021;42:1554-1568. doi:10.1093/eurheartj/ehab072
- Brito D, Albrecht FC, de Arenaza DP, et al. World Heart Federation consensus on transthyretin amyloidosis cardiomyopathy (ATTR-CM). Glob Heart. 2023;18:59. doi:10.5334/gh.1262
- Bodez D, Guellich A, Kharoubi M, et al. Prevalence, severity, and prognostic value of sleep apnea syndromes in cardiac amyloidosis. Sleep. 2016;39:1333-1341. doi:10.5665/sleep.5958
- Colaco B, Colaco C, Lipford M. A forgotten problem: sleep-disordered breathing in amyloidosis. Chest. 2016;150:1293A. doi:10.1016/j.chest.2016.08.1407
Case Series of Patients With Cardiac Amyloidosis at VA New York Harbor Healthcare-Brooklyn
Case Series of Patients With Cardiac Amyloidosis at VA New York Harbor Healthcare-Brooklyn