User login
Consumer Trends Driving Contact Dermatitis: Insights from JiaDe Yu, MD, MS
Consumer Trends Driving Contact Dermatitis: Insights from JiaDe Yu, MD, MS
How do social media trends and influencer driven product fads affect the patterns of contact dermatitis you are seeing?
DR. YU: Social media and influencers are huge marketing opportunities for cosmetic and personal care companies and drive consumer demand. One example from a few years ago is slime as a toy for kids. For a period of time, every kid was making slime at home, resulting in high numbers of hand allergic contact dermatitis. Making slime requires a combination of borax (irritant), glue (irritant and allergen), laundry detergent or dish soap (irritant and allergen), and fragrances (irritant and allergen). This fad has been slowing since I cowrote an article on it (doi:10.1111 /pde.13792). More recently, the rise of “Sephora kids” (preteens and adolescents influenced by social media trends promoting multistep skin care and anti-aging products) has raised concerns about contact dermatitis, as many of these products contain ingredients that can disrupt the skin barrier or trigger sensitization in younger patients.
How can products labeled free of fragrances or preservatives still trigger allergic contact dermatitis?
DR. YU: Fragrances are frequently in the top 10 ingredients that cause allergic contact dermatitis in adults and children. For people with sensitive skin, we almost unequivocally recommend fragrance-free products. Now, not all fragrance-free products are truly free of fragrance allergens. Some fragrance chemicals may be used for another purpose (benzyl alcohol as a preservative, for example), so the product can still be fragrance free even though benzyl alcohol has a fragrance. Most products cannot truly be preservative free if they are expected to have a shelf life. One-time-use products do exist and can be preservative free, but they are very rare and very expensive to manufacture and maintain.
Have you seen spikes in reactions from trendy products like CBD-infused creams, botanical serums, or exfoliating acids?
DR. YU: Not yet, but I would not be surprised that this is rising in prevalence. The issue might not be CBD itself; it’s really the other additives in these CBD products that will cause problems. Looking at some CBD products for sale from major retailers, many contain fragrances such as lemongrass oil and botanical extracts such as calendula that have been noted to cause allergic contact dermatitis.
Do certain patient behaviors (eg, layering multiple natural products, frequent product switching, prolonged leave-on use) increase the risk for ACD?
DR. YU: Absolutely possible. The more products you use, the more likely you will develop allergic contact dermatitis due to increased exposure to potential allergens. We know that leave-on products are higher risk than rinse-offs in general. Furthermore, more products used also increase the risk for irritant dermatitis that might break the skin barrier, increasing the odds that someone will develop allergic contact dermatitis. We see this often with facial skin care products where some people might layer on glycolic acid with retinoid acid with vitamin C oil with kojic acid, etc, all leading to irritation on the face.
How do emerging consumer product trends influence your patch-testing approach?
DR. YU: We try to customize our patch-tested allergens to the patient’s rash and symptoms. If it’s a patient with facial dermatitis, for example, we would patch test the patient to a core allergen series (eg, American Contact Dermatitis Society 90, North American Comprehensive 80, North American Contact Dermatitis Group 80) and add on other supplemental panels including cosmetic series if applicable. It is also preferable to patch test for products that are used and/or suspected of causing the rash. For example, if a blush is a suspected cause of dermatitis, we would certainly patch test to that as well. We generally try to encourage the patient to bring in all their products so we can evaluate them for appropriateness for patch testing.
Which consumer-driven ingredients do you now consider high-yield targets for testing?
DR. YU: Fragrances, preservatives, and botanical extracts are all likely causes of allergic contact dermatitis. We are uncovering new allergens all the time, so testing directly to patient products is also important. Just because something has not been reported to be a contact allergen doesn’t mean it can’t become one.
Have you observed any demographic or cultural trends in patients with allergic contact dermatitis related to consumer products?
DR. YU: There are various papers that outline different allergens in adults vs children vs older adults. However, in general, the prevalence of contact dermatitis is very similar across all age groups and distributions. I do think there are definitely gender and cultural variations. Women are more likely to be allergic to nickel, for example, which is more often found in jewelry. However, there really aren’t studies that demonstrate one population is more likely to develop allergic contact dermatitis than others. It really comes down to exposure. For example, neomycin, which is contained in triple antibiotics in the United States and is sold over the counter, is a common allergen here. However, it’s not readily available in other countries, and therefore, neomycin is a rare allergen in those countries.
Looking forward, which emerging consumer trends do you anticipate will create the next wave of contact dermatitis cases?
DR. YU: We have seen an increase in allergic contact dermatitis in the wearables industry, especially in continuous glucose monitors. They are now being sold over the counter so people without diabetes and without a prescription will be able to purchase them from retailers like Amazon or CVS. The adhesives in these glucose monitors have been shown to cause allergic contact dermatitis in a sizeable number of kids and adults. I suspect this problem will continue to increase with increased exposure to the allergens in these adhesives.
How do social media trends and influencer driven product fads affect the patterns of contact dermatitis you are seeing?
DR. YU: Social media and influencers are huge marketing opportunities for cosmetic and personal care companies and drive consumer demand. One example from a few years ago is slime as a toy for kids. For a period of time, every kid was making slime at home, resulting in high numbers of hand allergic contact dermatitis. Making slime requires a combination of borax (irritant), glue (irritant and allergen), laundry detergent or dish soap (irritant and allergen), and fragrances (irritant and allergen). This fad has been slowing since I cowrote an article on it (doi:10.1111 /pde.13792). More recently, the rise of “Sephora kids” (preteens and adolescents influenced by social media trends promoting multistep skin care and anti-aging products) has raised concerns about contact dermatitis, as many of these products contain ingredients that can disrupt the skin barrier or trigger sensitization in younger patients.
How can products labeled free of fragrances or preservatives still trigger allergic contact dermatitis?
DR. YU: Fragrances are frequently in the top 10 ingredients that cause allergic contact dermatitis in adults and children. For people with sensitive skin, we almost unequivocally recommend fragrance-free products. Now, not all fragrance-free products are truly free of fragrance allergens. Some fragrance chemicals may be used for another purpose (benzyl alcohol as a preservative, for example), so the product can still be fragrance free even though benzyl alcohol has a fragrance. Most products cannot truly be preservative free if they are expected to have a shelf life. One-time-use products do exist and can be preservative free, but they are very rare and very expensive to manufacture and maintain.
Have you seen spikes in reactions from trendy products like CBD-infused creams, botanical serums, or exfoliating acids?
DR. YU: Not yet, but I would not be surprised that this is rising in prevalence. The issue might not be CBD itself; it’s really the other additives in these CBD products that will cause problems. Looking at some CBD products for sale from major retailers, many contain fragrances such as lemongrass oil and botanical extracts such as calendula that have been noted to cause allergic contact dermatitis.
Do certain patient behaviors (eg, layering multiple natural products, frequent product switching, prolonged leave-on use) increase the risk for ACD?
DR. YU: Absolutely possible. The more products you use, the more likely you will develop allergic contact dermatitis due to increased exposure to potential allergens. We know that leave-on products are higher risk than rinse-offs in general. Furthermore, more products used also increase the risk for irritant dermatitis that might break the skin barrier, increasing the odds that someone will develop allergic contact dermatitis. We see this often with facial skin care products where some people might layer on glycolic acid with retinoid acid with vitamin C oil with kojic acid, etc, all leading to irritation on the face.
How do emerging consumer product trends influence your patch-testing approach?
DR. YU: We try to customize our patch-tested allergens to the patient’s rash and symptoms. If it’s a patient with facial dermatitis, for example, we would patch test the patient to a core allergen series (eg, American Contact Dermatitis Society 90, North American Comprehensive 80, North American Contact Dermatitis Group 80) and add on other supplemental panels including cosmetic series if applicable. It is also preferable to patch test for products that are used and/or suspected of causing the rash. For example, if a blush is a suspected cause of dermatitis, we would certainly patch test to that as well. We generally try to encourage the patient to bring in all their products so we can evaluate them for appropriateness for patch testing.
Which consumer-driven ingredients do you now consider high-yield targets for testing?
DR. YU: Fragrances, preservatives, and botanical extracts are all likely causes of allergic contact dermatitis. We are uncovering new allergens all the time, so testing directly to patient products is also important. Just because something has not been reported to be a contact allergen doesn’t mean it can’t become one.
Have you observed any demographic or cultural trends in patients with allergic contact dermatitis related to consumer products?
DR. YU: There are various papers that outline different allergens in adults vs children vs older adults. However, in general, the prevalence of contact dermatitis is very similar across all age groups and distributions. I do think there are definitely gender and cultural variations. Women are more likely to be allergic to nickel, for example, which is more often found in jewelry. However, there really aren’t studies that demonstrate one population is more likely to develop allergic contact dermatitis than others. It really comes down to exposure. For example, neomycin, which is contained in triple antibiotics in the United States and is sold over the counter, is a common allergen here. However, it’s not readily available in other countries, and therefore, neomycin is a rare allergen in those countries.
Looking forward, which emerging consumer trends do you anticipate will create the next wave of contact dermatitis cases?
DR. YU: We have seen an increase in allergic contact dermatitis in the wearables industry, especially in continuous glucose monitors. They are now being sold over the counter so people without diabetes and without a prescription will be able to purchase them from retailers like Amazon or CVS. The adhesives in these glucose monitors have been shown to cause allergic contact dermatitis in a sizeable number of kids and adults. I suspect this problem will continue to increase with increased exposure to the allergens in these adhesives.
How do social media trends and influencer driven product fads affect the patterns of contact dermatitis you are seeing?
DR. YU: Social media and influencers are huge marketing opportunities for cosmetic and personal care companies and drive consumer demand. One example from a few years ago is slime as a toy for kids. For a period of time, every kid was making slime at home, resulting in high numbers of hand allergic contact dermatitis. Making slime requires a combination of borax (irritant), glue (irritant and allergen), laundry detergent or dish soap (irritant and allergen), and fragrances (irritant and allergen). This fad has been slowing since I cowrote an article on it (doi:10.1111 /pde.13792). More recently, the rise of “Sephora kids” (preteens and adolescents influenced by social media trends promoting multistep skin care and anti-aging products) has raised concerns about contact dermatitis, as many of these products contain ingredients that can disrupt the skin barrier or trigger sensitization in younger patients.
How can products labeled free of fragrances or preservatives still trigger allergic contact dermatitis?
DR. YU: Fragrances are frequently in the top 10 ingredients that cause allergic contact dermatitis in adults and children. For people with sensitive skin, we almost unequivocally recommend fragrance-free products. Now, not all fragrance-free products are truly free of fragrance allergens. Some fragrance chemicals may be used for another purpose (benzyl alcohol as a preservative, for example), so the product can still be fragrance free even though benzyl alcohol has a fragrance. Most products cannot truly be preservative free if they are expected to have a shelf life. One-time-use products do exist and can be preservative free, but they are very rare and very expensive to manufacture and maintain.
Have you seen spikes in reactions from trendy products like CBD-infused creams, botanical serums, or exfoliating acids?
DR. YU: Not yet, but I would not be surprised that this is rising in prevalence. The issue might not be CBD itself; it’s really the other additives in these CBD products that will cause problems. Looking at some CBD products for sale from major retailers, many contain fragrances such as lemongrass oil and botanical extracts such as calendula that have been noted to cause allergic contact dermatitis.
Do certain patient behaviors (eg, layering multiple natural products, frequent product switching, prolonged leave-on use) increase the risk for ACD?
DR. YU: Absolutely possible. The more products you use, the more likely you will develop allergic contact dermatitis due to increased exposure to potential allergens. We know that leave-on products are higher risk than rinse-offs in general. Furthermore, more products used also increase the risk for irritant dermatitis that might break the skin barrier, increasing the odds that someone will develop allergic contact dermatitis. We see this often with facial skin care products where some people might layer on glycolic acid with retinoid acid with vitamin C oil with kojic acid, etc, all leading to irritation on the face.
How do emerging consumer product trends influence your patch-testing approach?
DR. YU: We try to customize our patch-tested allergens to the patient’s rash and symptoms. If it’s a patient with facial dermatitis, for example, we would patch test the patient to a core allergen series (eg, American Contact Dermatitis Society 90, North American Comprehensive 80, North American Contact Dermatitis Group 80) and add on other supplemental panels including cosmetic series if applicable. It is also preferable to patch test for products that are used and/or suspected of causing the rash. For example, if a blush is a suspected cause of dermatitis, we would certainly patch test to that as well. We generally try to encourage the patient to bring in all their products so we can evaluate them for appropriateness for patch testing.
Which consumer-driven ingredients do you now consider high-yield targets for testing?
DR. YU: Fragrances, preservatives, and botanical extracts are all likely causes of allergic contact dermatitis. We are uncovering new allergens all the time, so testing directly to patient products is also important. Just because something has not been reported to be a contact allergen doesn’t mean it can’t become one.
Have you observed any demographic or cultural trends in patients with allergic contact dermatitis related to consumer products?
DR. YU: There are various papers that outline different allergens in adults vs children vs older adults. However, in general, the prevalence of contact dermatitis is very similar across all age groups and distributions. I do think there are definitely gender and cultural variations. Women are more likely to be allergic to nickel, for example, which is more often found in jewelry. However, there really aren’t studies that demonstrate one population is more likely to develop allergic contact dermatitis than others. It really comes down to exposure. For example, neomycin, which is contained in triple antibiotics in the United States and is sold over the counter, is a common allergen here. However, it’s not readily available in other countries, and therefore, neomycin is a rare allergen in those countries.
Looking forward, which emerging consumer trends do you anticipate will create the next wave of contact dermatitis cases?
DR. YU: We have seen an increase in allergic contact dermatitis in the wearables industry, especially in continuous glucose monitors. They are now being sold over the counter so people without diabetes and without a prescription will be able to purchase them from retailers like Amazon or CVS. The adhesives in these glucose monitors have been shown to cause allergic contact dermatitis in a sizeable number of kids and adults. I suspect this problem will continue to increase with increased exposure to the allergens in these adhesives.
Consumer Trends Driving Contact Dermatitis: Insights from JiaDe Yu, MD, MS
Consumer Trends Driving Contact Dermatitis: Insights from JiaDe Yu, MD, MS

Using Intralesional Adalimumab for Chronic Refractory Cutaneous Granulomatous Inflammation
Using Intralesional Adalimumab for Chronic Refractory Cutaneous Granulomatous Inflammation
Practice Gap
Chronic localized granulomatous inflammation can be difficult to manage, particularly when manifesting on the face. Intralesional corticosteroids may lead to atrophy and dyspigmentation and therefore must be used cautiously in cosmetically sensitive areas.1 Surgical removal can lead to recurrence, and systemic agents may carry risks disproportionate to disease burden. Although tumor necrosis factor (TNF) α inhibitors are effective systemically, their localized use in cutaneous granulomatous dermatoses remains underreported.1-3 We describe a technique using intralesional injection of adalimumab to treat chronic refractory cutaneous granulomatous inflammation.
The Technique
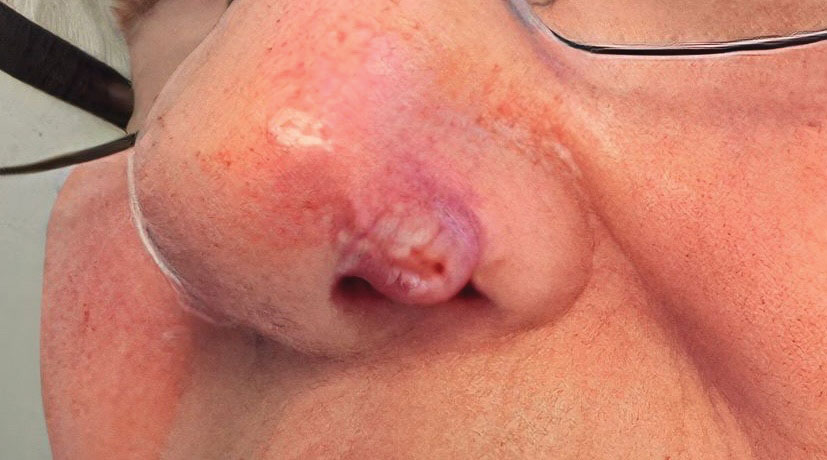
A 69-year-old woman presented with a crusted erythematous papule with surrounding inflammation on the left nasal ala of 5 years’ duration (Figure 1). Histopathology demonstrated a localized cutaneous granulomatous process. There was no clinical, radiographic, or laboratory evidence of systemic sarcoidosis. Infectious causes were excluded through negative tissue cultures and special stains, including auramine-rhodamine. Over a 3-month period following initial presentation, the lesion proved refractory to intralesional 5-fluorouracil, intralesional triamcinolone acetonide, pentoxifylline, N-acetylcysteine, and shave excision (Figure 2).

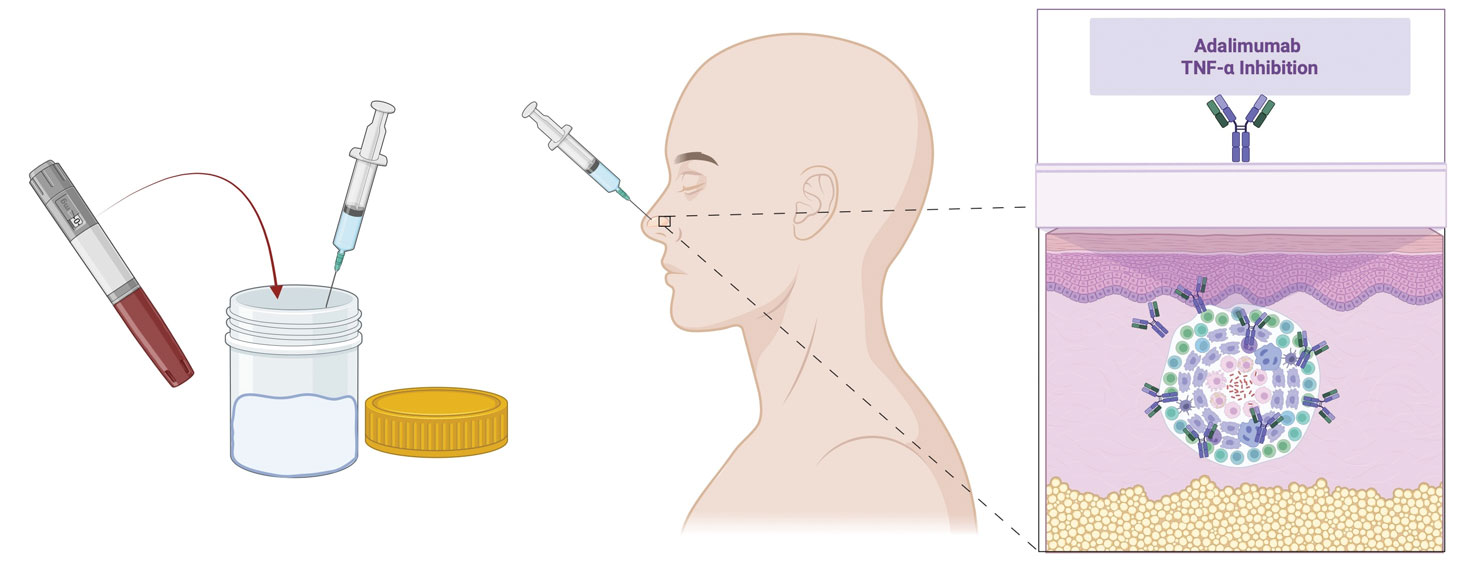
At 3-month follow-up, given the lesion’s persistence despite local and systemic anti-inflammatory approaches and our intent to avoid repeated corticosteroid exposure or more aggressive surgery in a cosmetically sensitive facial site, we attempted treatment with intralesional adalimumab. A 40-mg/0.4-mL dose of adalimumab was withdrawn directly from a prefilled autoinjector and placed into a sterile container, then transferred to a syringe fitted with a 30-gauge needle. Finally, the full 0.4 mL was injected intralesionally (Figure 3) until complete blanching of the lesion was achieved.
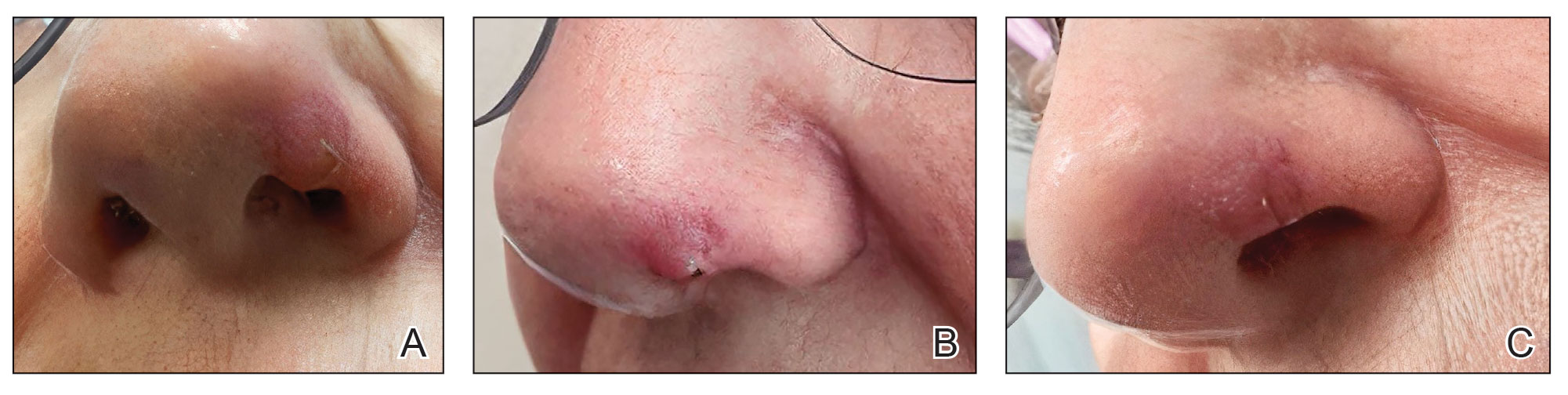
At 1-month follow-up, the lesion demonstrated decreased erythema and crusting (Figure 4A). The patient subsequently underwent 12 adalimumab injections over an 18-month period with marked reduction in size and erythema of the lesion without complications (Figure 4B). In addition, doxycycline 100 mg/d was started 11 months after the first adalimumab injection to address mild residual inflammation (Figure 4C); after 4 months, the dose was reduced to 50 mg/d due to gastrointestinal adverse effects. Doxycycline was maintained for 3 additional months with persistent improvement of the lesion.
Practice Implication
Intralesional administration of adalimumab may represent a useful therapeutic option for localized refractory granulomatous inflammation, particularly in sensitive areas such as the face, where conventional therapies may be limited by adverse effects or suboptimal response. Localized delivery of TNF-α inhibition directly to the site of inflammation may allow for clinical improvement while minimizing systemic exposure associated with biologic therapy.2 This approach may be particularly advantageous in cases in which repeated intralesional corticosteroid injections raise concern for atrophy or dyspigmentation, or when surgical intervention carries a risk for recurrence or cosmetic morbidity.1,2 Given the established role of TNF-α in granuloma formation and maintenance, intralesional adalimumab provides a biologically plausible targeted therapeutic strategy. Further studies are needed to evaluate the potential applications in other cutaneous granulomatous dermatoses.2,3
- Philips MA, Lynch J, Azmi FH. Ulcerative cutaneous sarcoidosis responding to adalimumab. J Am Acad Dermatol. 2005;53:917. doi:10.1016/j.jaad.2005.02.023
- Balan K, Sagut P, Ederle AC, et al. Cutaneous sarcoidosis treated with intralesional adalimumab. Int J Dermatol. 2025;64:1120-1121. doi:10.1111/ijd.17549
- Dunn C, Whitney Z, Foss M, et al. Intralesional certolizumab for refractory lupus pernio. JAMA Dermatol. 2023;159:890-891. doi:10.1001 /jamadermatol.2023.0987
Practice Gap
Chronic localized granulomatous inflammation can be difficult to manage, particularly when manifesting on the face. Intralesional corticosteroids may lead to atrophy and dyspigmentation and therefore must be used cautiously in cosmetically sensitive areas.1 Surgical removal can lead to recurrence, and systemic agents may carry risks disproportionate to disease burden. Although tumor necrosis factor (TNF) α inhibitors are effective systemically, their localized use in cutaneous granulomatous dermatoses remains underreported.1-3 We describe a technique using intralesional injection of adalimumab to treat chronic refractory cutaneous granulomatous inflammation.
The Technique
A 69-year-old woman presented with a crusted erythematous papule with surrounding inflammation on the left nasal ala of 5 years’ duration (Figure 1). Histopathology demonstrated a localized cutaneous granulomatous process. There was no clinical, radiographic, or laboratory evidence of systemic sarcoidosis. Infectious causes were excluded through negative tissue cultures and special stains, including auramine-rhodamine. Over a 3-month period following initial presentation, the lesion proved refractory to intralesional 5-fluorouracil, intralesional triamcinolone acetonide, pentoxifylline, N-acetylcysteine, and shave excision (Figure 2).
At 3-month follow-up, given the lesion’s persistence despite local and systemic anti-inflammatory approaches and our intent to avoid repeated corticosteroid exposure or more aggressive surgery in a cosmetically sensitive facial site, we attempted treatment with intralesional adalimumab. A 40-mg/0.4-mL dose of adalimumab was withdrawn directly from a prefilled autoinjector and placed into a sterile container, then transferred to a syringe fitted with a 30-gauge needle. Finally, the full 0.4 mL was injected intralesionally (Figure 3) until complete blanching of the lesion was achieved.
At 1-month follow-up, the lesion demonstrated decreased erythema and crusting (Figure 4A). The patient subsequently underwent 12 adalimumab injections over an 18-month period with marked reduction in size and erythema of the lesion without complications (Figure 4B). In addition, doxycycline 100 mg/d was started 11 months after the first adalimumab injection to address mild residual inflammation (Figure 4C); after 4 months, the dose was reduced to 50 mg/d due to gastrointestinal adverse effects. Doxycycline was maintained for 3 additional months with persistent improvement of the lesion.
Practice Implication
Intralesional administration of adalimumab may represent a useful therapeutic option for localized refractory granulomatous inflammation, particularly in sensitive areas such as the face, where conventional therapies may be limited by adverse effects or suboptimal response. Localized delivery of TNF-α inhibition directly to the site of inflammation may allow for clinical improvement while minimizing systemic exposure associated with biologic therapy.2 This approach may be particularly advantageous in cases in which repeated intralesional corticosteroid injections raise concern for atrophy or dyspigmentation, or when surgical intervention carries a risk for recurrence or cosmetic morbidity.1,2 Given the established role of TNF-α in granuloma formation and maintenance, intralesional adalimumab provides a biologically plausible targeted therapeutic strategy. Further studies are needed to evaluate the potential applications in other cutaneous granulomatous dermatoses.2,3
Practice Gap
Chronic localized granulomatous inflammation can be difficult to manage, particularly when manifesting on the face. Intralesional corticosteroids may lead to atrophy and dyspigmentation and therefore must be used cautiously in cosmetically sensitive areas.1 Surgical removal can lead to recurrence, and systemic agents may carry risks disproportionate to disease burden. Although tumor necrosis factor (TNF) α inhibitors are effective systemically, their localized use in cutaneous granulomatous dermatoses remains underreported.1-3 We describe a technique using intralesional injection of adalimumab to treat chronic refractory cutaneous granulomatous inflammation.
The Technique
A 69-year-old woman presented with a crusted erythematous papule with surrounding inflammation on the left nasal ala of 5 years’ duration (Figure 1). Histopathology demonstrated a localized cutaneous granulomatous process. There was no clinical, radiographic, or laboratory evidence of systemic sarcoidosis. Infectious causes were excluded through negative tissue cultures and special stains, including auramine-rhodamine. Over a 3-month period following initial presentation, the lesion proved refractory to intralesional 5-fluorouracil, intralesional triamcinolone acetonide, pentoxifylline, N-acetylcysteine, and shave excision (Figure 2).
At 3-month follow-up, given the lesion’s persistence despite local and systemic anti-inflammatory approaches and our intent to avoid repeated corticosteroid exposure or more aggressive surgery in a cosmetically sensitive facial site, we attempted treatment with intralesional adalimumab. A 40-mg/0.4-mL dose of adalimumab was withdrawn directly from a prefilled autoinjector and placed into a sterile container, then transferred to a syringe fitted with a 30-gauge needle. Finally, the full 0.4 mL was injected intralesionally (Figure 3) until complete blanching of the lesion was achieved.
At 1-month follow-up, the lesion demonstrated decreased erythema and crusting (Figure 4A). The patient subsequently underwent 12 adalimumab injections over an 18-month period with marked reduction in size and erythema of the lesion without complications (Figure 4B). In addition, doxycycline 100 mg/d was started 11 months after the first adalimumab injection to address mild residual inflammation (Figure 4C); after 4 months, the dose was reduced to 50 mg/d due to gastrointestinal adverse effects. Doxycycline was maintained for 3 additional months with persistent improvement of the lesion.
Practice Implication
Intralesional administration of adalimumab may represent a useful therapeutic option for localized refractory granulomatous inflammation, particularly in sensitive areas such as the face, where conventional therapies may be limited by adverse effects or suboptimal response. Localized delivery of TNF-α inhibition directly to the site of inflammation may allow for clinical improvement while minimizing systemic exposure associated with biologic therapy.2 This approach may be particularly advantageous in cases in which repeated intralesional corticosteroid injections raise concern for atrophy or dyspigmentation, or when surgical intervention carries a risk for recurrence or cosmetic morbidity.1,2 Given the established role of TNF-α in granuloma formation and maintenance, intralesional adalimumab provides a biologically plausible targeted therapeutic strategy. Further studies are needed to evaluate the potential applications in other cutaneous granulomatous dermatoses.2,3
- Philips MA, Lynch J, Azmi FH. Ulcerative cutaneous sarcoidosis responding to adalimumab. J Am Acad Dermatol. 2005;53:917. doi:10.1016/j.jaad.2005.02.023
- Balan K, Sagut P, Ederle AC, et al. Cutaneous sarcoidosis treated with intralesional adalimumab. Int J Dermatol. 2025;64:1120-1121. doi:10.1111/ijd.17549
- Dunn C, Whitney Z, Foss M, et al. Intralesional certolizumab for refractory lupus pernio. JAMA Dermatol. 2023;159:890-891. doi:10.1001 /jamadermatol.2023.0987
- Philips MA, Lynch J, Azmi FH. Ulcerative cutaneous sarcoidosis responding to adalimumab. J Am Acad Dermatol. 2005;53:917. doi:10.1016/j.jaad.2005.02.023
- Balan K, Sagut P, Ederle AC, et al. Cutaneous sarcoidosis treated with intralesional adalimumab. Int J Dermatol. 2025;64:1120-1121. doi:10.1111/ijd.17549
- Dunn C, Whitney Z, Foss M, et al. Intralesional certolizumab for refractory lupus pernio. JAMA Dermatol. 2023;159:890-891. doi:10.1001 /jamadermatol.2023.0987
Using Intralesional Adalimumab for Chronic Refractory Cutaneous Granulomatous Inflammation
Using Intralesional Adalimumab for Chronic Refractory Cutaneous Granulomatous Inflammation

Pink Papulonodular Eruption on the Trunk and Arms
Pink Papulonodular Eruption on the Trunk and Arms
THE DIAGNOSIS: Sarcoidlike Reaction
Sarcoidlike reaction (SLR) is a rare cutaneous immune-related adverse event characterized by a multisystem granulomatous reaction indistinguishable from sarcoidosis but temporally associated with a trigger.1 Drug-induced SLR typically involves the mediastinal or hilar lymph nodes, with frequent involvement of the lungs and skin; cutaneous manifestations typically encompass erythematous papulonodular eruptions on the trunk and extremities.1-3 Sarcoidosis predominantly affects middle-aged women of African American or Scandinavian descent; genetic predisposition likely is a contributing factor.4 Unlike sarcoidosis, SLR is linked to various triggers such as medication or malignancy.
Immune checkpoint inhibitors (ICIs), particularly anti–PD-1 agents, have been linked to SLR through overexpression of proinflammatory cytokines, resulting in excessive T-helper 1 cell and macrophage activation and granulomatous eruption; notably, cutaneous immune-related adverse events often are correlated with greater treatment efficacy.5,6 Overall, anticancer therapy–induced SLR is most commonly reported in patients receiving ICIs for melanoma but it also has been described with ICI therapy for other cancers and with chemotherapy for melanoma. 1,3 Although most cases demonstrate both cutaneous and extracutaneous involvement, approximately 13 reported cases have been exclusively cutaneous.1 Recognition of SLR is important because misdiagnosis as true sarcoidosis may prompt unnecessary testing or therapy; furthermore, distinction from tumor progression is critical.3 The lesions can mimic other granulomatous or inflammatory dermatoses, posing a diagnostic challenge.
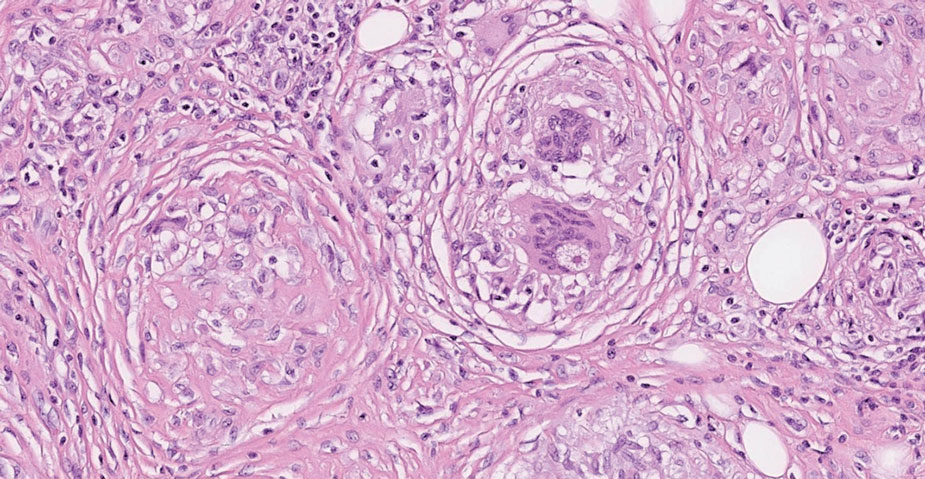
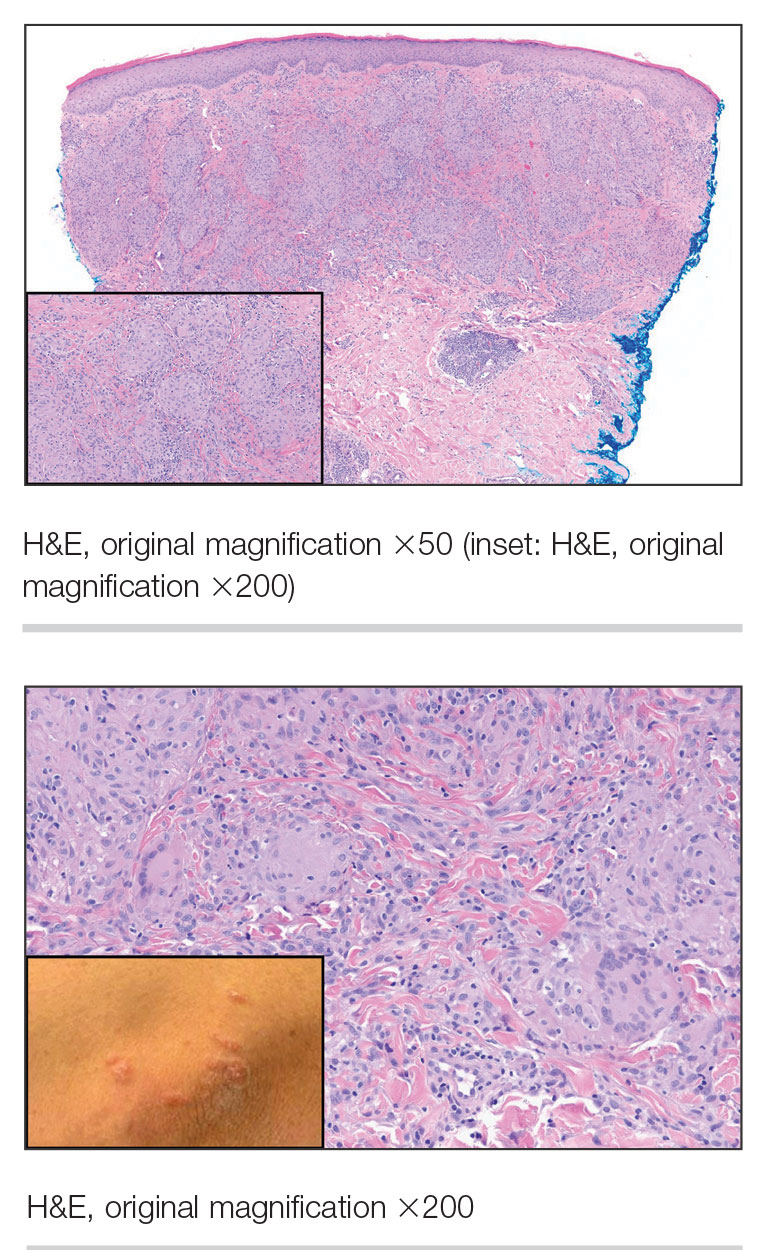
On histopathology, SLR typically demonstrates well-formed, noncaseating dermal granulomas composed of epithelioid histiocytes and Langhans or foreign-body giant cells, a sparse lymphocytic rim, and few plasma cells.2,4 Immunohistochemistry shows CD68-positive histiocytes predominating within the granulomas. Asteroid and Schaumann bodies occasionally are present.7 Special stains will be negative for microorganisms. Sarcoidosis manifests essentially identically from both a clinical and histopathologic perspective (Figure 1). Temporal association with an offending agent and symptomatic resolution following drug cessation remain the most reliable features for distinguishing SLR from sarcoidosis.7
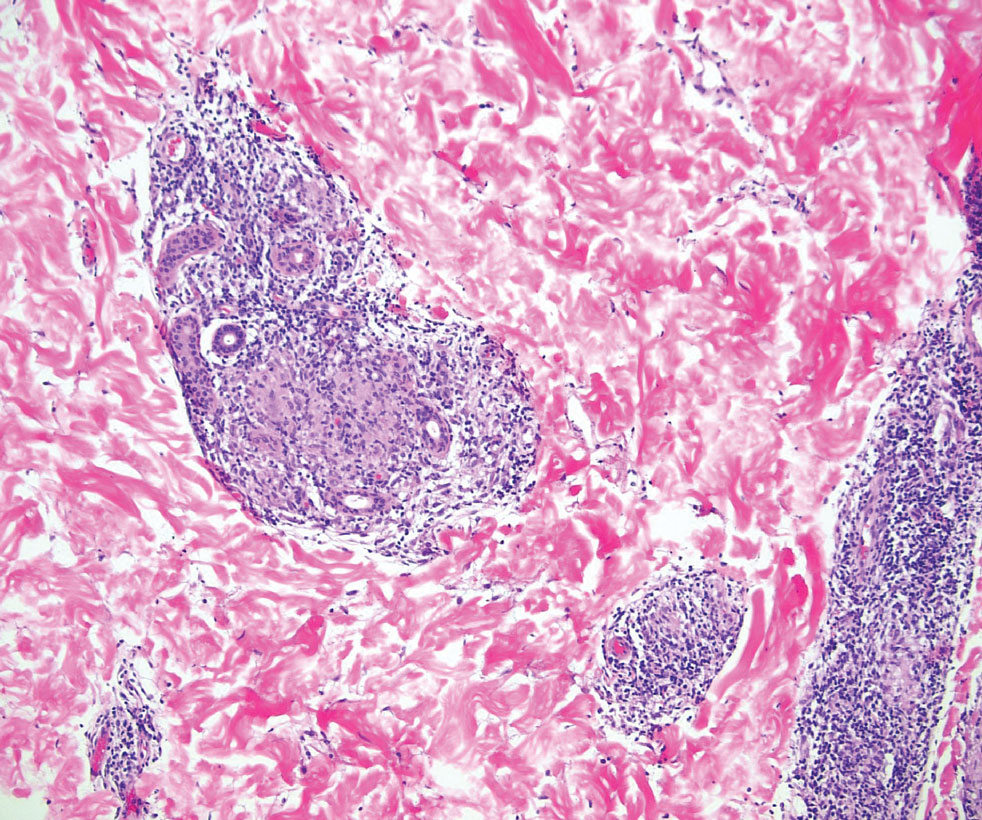
Tuberculoid leprosy is a chronic infectious disease caused by Mycobacterium leprae (found most commonly in tropical regions) and manifesting as localized hypopigmented macules or papules with raised erythematous margins.8 Histopathologically, lesions show well-formed granulomas composed of epithelioid histiocytes and Langhans giant cells without necrosis, surrounded by a prominent lymphocytic rim (Figure 2).9 Rarely, focal caseous necrosis occurs, particularly in involved nerves.10 Hallmark features include enlarged cutaneous nerves surrounded by dermal granulomas and absence of bacilli on special stains; eccrine glands are infrequently involved.9 Standard treatment is 6 months of combination therapy with dapsone and rifampin.
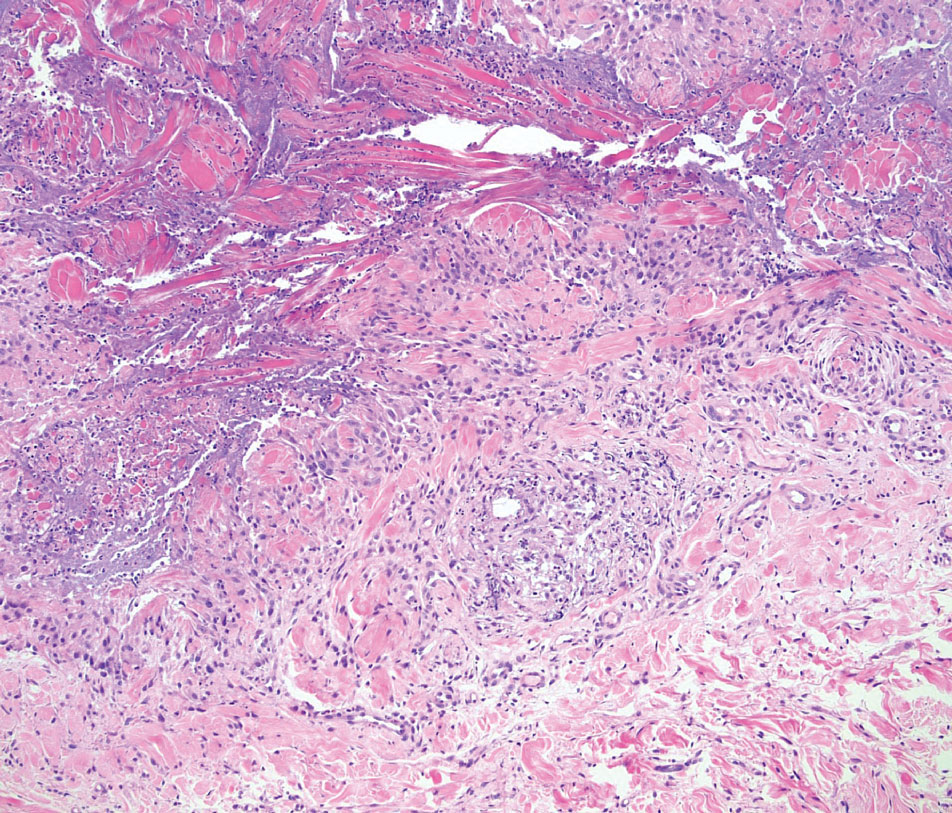
Generalized granuloma annulare is an inflammatory dermatosis manifesting as diffuse erythematous annular papules, classically on the trunk and extremities.11 It predominantly affects individuals in their fifth and sixth decades of life and may be drug induced.2 Histopathology may reveal palisaded granulomas with central necrobiotic collagen, intercalating histiocytes, and interstitial mucin (Figure 3).2 Pathology also may show interstitial histiocytes and lymphocytes intercalating between collagen bundles with increased mucin but absent palisading or necrobiosis or a mixed pattern.2,12 Alcian blue or colloidal iron stains highlight mucin to help distinguish from other granulomatous processes. Multinucleated giant cells are rare. The nonnecrobiotic histologic pattern can mimic sarcoidosis, necessitating clinical correlation for correct diagnosis.13 Certain cases show genetic predisposition, such as HLA-B35, with a relapsing course often requiring combined systemic immunosuppression and phototherapy.14
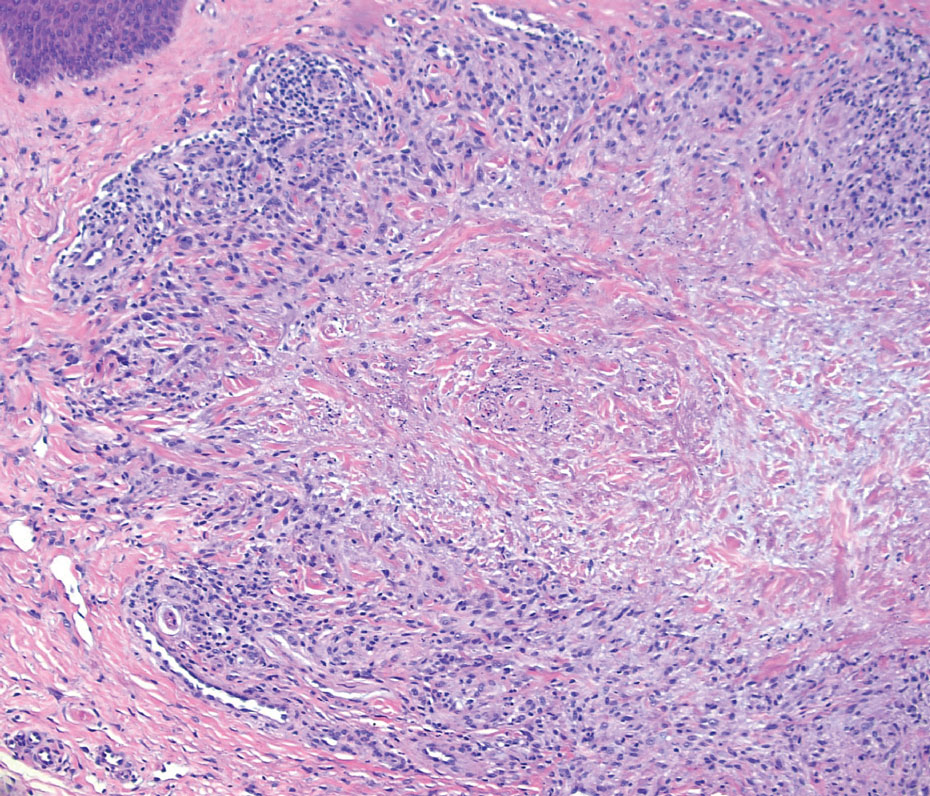
Granulomatosis with polyangiitis is a systemic vasculitis that classically manifests as palpable purpura on the lower extremities, often with ulceration. Localized erythematous papules on the extensor surfaces may occur less commonly.15 Pathogenesis involves antineutrophil cytoplasmic antibodies inducing neutrophil degranulation, release of reactive oxygen species and proinflammatory cytokines, and subsequent endothelial damage.15 Histopathology shows necrotizing granulomatous inflammation and necrotizing vasculitis of small and medium vessels with nuclear debris.15 Poorly formed granulomas containing abundant neutrophils and mixed perivascular inflammatory infiltrates may be seen with or without vasculitis (Figure 4). Systemic features commonly include chronic rhinosinusitis, pauci-immune glomerulonephritis, and pulmonary nodules.15 Pharmacotherapy includes glucocorticoids combined with a glucocorticoid-sparing agent.
- Mazumder A, Mehrmal S, Chaudhry S. Immunotherapy-induced exclusively cutaneous sarcoid-like reaction. BMJ Case Rep. 2023;16:E252766. doi:10.1136/bcr-2022-252766
- Shah N, Shah M, Drucker AM, et al. Granulomatous cutaneous drug eruptions: a systematic review. Am J Clin Dermatol. 2021;22:39-53. doi:10.1007/s40257-020-00566-4
- Nykaza I, Murciano-Goroff YR, Desilets A, et al. Sarcoid-like reactions in patients treated with checkpoint inhibitors for advanced solid tumors. Oncologist. 2025;30:oyaf017. doi:10.1093/oncolo /oyaf017
- Tana C, Donatiello I, Caputo A, et al. Clinical features, histopathology and differential diagnosis of sarcoidosis. Cells. 2021;11:59. doi:10.3390/cells11010059
- Sibaud V. Dermatologic reactions to immune checkpoint inhibitors: skin toxicities and immunotherapy. Am J Clin Dermatol. 2018;19:345-361. doi:10.1007/s40257-017-0336-3
- Diaz-Perez JA, Beveridge MG, Victor TA, et al. Granulomatous and lichenoid dermatitis after IgG4 anti-PD-1 monoclonal antibody therapy for advanced cancer. J Cutan Pathol. 2018;45:434-438. doi:10.1111/cup.13133
- Chopra A, Nautiyal A, Kalkanis A, et al. Drug-induced sarcoidosis-like reactions. Chest. 2018;154:664-677. doi:10.1016 /j.chest.2018.03.056
- Froes LAR Jr, Sotto MN, Trindade MAB. Leprosy: clinical and immunopathological characteristics. An Bras Dermatol. 2022;97:338-347. doi:10.1016/j.abd.2021.08.006
- Magaña M, Vargas Bornacini MF, Landeta-Sa AP, et al. Lucio phenomenon: a review. Am J Dermatopathol. 2025;47:1-8. doi:10.1097 /DAD.0000000000002833
- Jayalakshmy PS, Prasad PH, Kamala VV, et al. Segmental necrotizing granulomatous neuritis: a rare manifestation of Hansen disease-report of 2 cases. Case Rep Dermatol Med. 2012;2012:758093. doi:10.1155/2012/758093
- Lee JH, Cho S. Resolution of refractory generalized granuloma annulare after treatment with alitretinoin. JAAD Case Rep. 2022;24:38-41. doi:10.1016/j.jdcr.2022.04.006
- Yun JH, Lee JY, Kim MK, et al. Clinical and pathological features of generalized granuloma annulare with their correlation: a retrospective multicenter study in Korea. Ann Dermatol. 2009; 21:113-119. doi:10.5021/ad.2009.21.2.113
- Cohen PR, Carlos CA. Granuloma annulare mimicking sarcoidosis: report of patient with localized granuloma annulare whose skin lesions show 3 clinical morphologies and 2 histology patterns. Am J Dermatopathol. 2015;37:547-550. doi:10.1097/DAD.0000000000000125
- Rankin BD, Haber RM. Familial granuloma annulare: first report of occurrence in a father and daughter and updated review of the literature. JAAD Case Rep. 2021;17:61-64. doi:10.1016 /j.jdcr.2021.09.023
- Rout P, Garlapati P, Qurie A. Granulomatosis with polyangiitis. StatPearls (Internet). Updated August 31, 2024. Accessed May 4, 2026. https://www.ncbi.nlm.nih.gov/books/NBK557827/
THE DIAGNOSIS: Sarcoidlike Reaction
Sarcoidlike reaction (SLR) is a rare cutaneous immune-related adverse event characterized by a multisystem granulomatous reaction indistinguishable from sarcoidosis but temporally associated with a trigger.1 Drug-induced SLR typically involves the mediastinal or hilar lymph nodes, with frequent involvement of the lungs and skin; cutaneous manifestations typically encompass erythematous papulonodular eruptions on the trunk and extremities.1-3 Sarcoidosis predominantly affects middle-aged women of African American or Scandinavian descent; genetic predisposition likely is a contributing factor.4 Unlike sarcoidosis, SLR is linked to various triggers such as medication or malignancy.
Immune checkpoint inhibitors (ICIs), particularly anti–PD-1 agents, have been linked to SLR through overexpression of proinflammatory cytokines, resulting in excessive T-helper 1 cell and macrophage activation and granulomatous eruption; notably, cutaneous immune-related adverse events often are correlated with greater treatment efficacy.5,6 Overall, anticancer therapy–induced SLR is most commonly reported in patients receiving ICIs for melanoma but it also has been described with ICI therapy for other cancers and with chemotherapy for melanoma. 1,3 Although most cases demonstrate both cutaneous and extracutaneous involvement, approximately 13 reported cases have been exclusively cutaneous.1 Recognition of SLR is important because misdiagnosis as true sarcoidosis may prompt unnecessary testing or therapy; furthermore, distinction from tumor progression is critical.3 The lesions can mimic other granulomatous or inflammatory dermatoses, posing a diagnostic challenge.
On histopathology, SLR typically demonstrates well-formed, noncaseating dermal granulomas composed of epithelioid histiocytes and Langhans or foreign-body giant cells, a sparse lymphocytic rim, and few plasma cells.2,4 Immunohistochemistry shows CD68-positive histiocytes predominating within the granulomas. Asteroid and Schaumann bodies occasionally are present.7 Special stains will be negative for microorganisms. Sarcoidosis manifests essentially identically from both a clinical and histopathologic perspective (Figure 1). Temporal association with an offending agent and symptomatic resolution following drug cessation remain the most reliable features for distinguishing SLR from sarcoidosis.7
Tuberculoid leprosy is a chronic infectious disease caused by Mycobacterium leprae (found most commonly in tropical regions) and manifesting as localized hypopigmented macules or papules with raised erythematous margins.8 Histopathologically, lesions show well-formed granulomas composed of epithelioid histiocytes and Langhans giant cells without necrosis, surrounded by a prominent lymphocytic rim (Figure 2).9 Rarely, focal caseous necrosis occurs, particularly in involved nerves.10 Hallmark features include enlarged cutaneous nerves surrounded by dermal granulomas and absence of bacilli on special stains; eccrine glands are infrequently involved.9 Standard treatment is 6 months of combination therapy with dapsone and rifampin.
Generalized granuloma annulare is an inflammatory dermatosis manifesting as diffuse erythematous annular papules, classically on the trunk and extremities.11 It predominantly affects individuals in their fifth and sixth decades of life and may be drug induced.2 Histopathology may reveal palisaded granulomas with central necrobiotic collagen, intercalating histiocytes, and interstitial mucin (Figure 3).2 Pathology also may show interstitial histiocytes and lymphocytes intercalating between collagen bundles with increased mucin but absent palisading or necrobiosis or a mixed pattern.2,12 Alcian blue or colloidal iron stains highlight mucin to help distinguish from other granulomatous processes. Multinucleated giant cells are rare. The nonnecrobiotic histologic pattern can mimic sarcoidosis, necessitating clinical correlation for correct diagnosis.13 Certain cases show genetic predisposition, such as HLA-B35, with a relapsing course often requiring combined systemic immunosuppression and phototherapy.14
Granulomatosis with polyangiitis is a systemic vasculitis that classically manifests as palpable purpura on the lower extremities, often with ulceration. Localized erythematous papules on the extensor surfaces may occur less commonly.15 Pathogenesis involves antineutrophil cytoplasmic antibodies inducing neutrophil degranulation, release of reactive oxygen species and proinflammatory cytokines, and subsequent endothelial damage.15 Histopathology shows necrotizing granulomatous inflammation and necrotizing vasculitis of small and medium vessels with nuclear debris.15 Poorly formed granulomas containing abundant neutrophils and mixed perivascular inflammatory infiltrates may be seen with or without vasculitis (Figure 4). Systemic features commonly include chronic rhinosinusitis, pauci-immune glomerulonephritis, and pulmonary nodules.15 Pharmacotherapy includes glucocorticoids combined with a glucocorticoid-sparing agent.
THE DIAGNOSIS: Sarcoidlike Reaction
Sarcoidlike reaction (SLR) is a rare cutaneous immune-related adverse event characterized by a multisystem granulomatous reaction indistinguishable from sarcoidosis but temporally associated with a trigger.1 Drug-induced SLR typically involves the mediastinal or hilar lymph nodes, with frequent involvement of the lungs and skin; cutaneous manifestations typically encompass erythematous papulonodular eruptions on the trunk and extremities.1-3 Sarcoidosis predominantly affects middle-aged women of African American or Scandinavian descent; genetic predisposition likely is a contributing factor.4 Unlike sarcoidosis, SLR is linked to various triggers such as medication or malignancy.
Immune checkpoint inhibitors (ICIs), particularly anti–PD-1 agents, have been linked to SLR through overexpression of proinflammatory cytokines, resulting in excessive T-helper 1 cell and macrophage activation and granulomatous eruption; notably, cutaneous immune-related adverse events often are correlated with greater treatment efficacy.5,6 Overall, anticancer therapy–induced SLR is most commonly reported in patients receiving ICIs for melanoma but it also has been described with ICI therapy for other cancers and with chemotherapy for melanoma. 1,3 Although most cases demonstrate both cutaneous and extracutaneous involvement, approximately 13 reported cases have been exclusively cutaneous.1 Recognition of SLR is important because misdiagnosis as true sarcoidosis may prompt unnecessary testing or therapy; furthermore, distinction from tumor progression is critical.3 The lesions can mimic other granulomatous or inflammatory dermatoses, posing a diagnostic challenge.
On histopathology, SLR typically demonstrates well-formed, noncaseating dermal granulomas composed of epithelioid histiocytes and Langhans or foreign-body giant cells, a sparse lymphocytic rim, and few plasma cells.2,4 Immunohistochemistry shows CD68-positive histiocytes predominating within the granulomas. Asteroid and Schaumann bodies occasionally are present.7 Special stains will be negative for microorganisms. Sarcoidosis manifests essentially identically from both a clinical and histopathologic perspective (Figure 1). Temporal association with an offending agent and symptomatic resolution following drug cessation remain the most reliable features for distinguishing SLR from sarcoidosis.7
Tuberculoid leprosy is a chronic infectious disease caused by Mycobacterium leprae (found most commonly in tropical regions) and manifesting as localized hypopigmented macules or papules with raised erythematous margins.8 Histopathologically, lesions show well-formed granulomas composed of epithelioid histiocytes and Langhans giant cells without necrosis, surrounded by a prominent lymphocytic rim (Figure 2).9 Rarely, focal caseous necrosis occurs, particularly in involved nerves.10 Hallmark features include enlarged cutaneous nerves surrounded by dermal granulomas and absence of bacilli on special stains; eccrine glands are infrequently involved.9 Standard treatment is 6 months of combination therapy with dapsone and rifampin.
Generalized granuloma annulare is an inflammatory dermatosis manifesting as diffuse erythematous annular papules, classically on the trunk and extremities.11 It predominantly affects individuals in their fifth and sixth decades of life and may be drug induced.2 Histopathology may reveal palisaded granulomas with central necrobiotic collagen, intercalating histiocytes, and interstitial mucin (Figure 3).2 Pathology also may show interstitial histiocytes and lymphocytes intercalating between collagen bundles with increased mucin but absent palisading or necrobiosis or a mixed pattern.2,12 Alcian blue or colloidal iron stains highlight mucin to help distinguish from other granulomatous processes. Multinucleated giant cells are rare. The nonnecrobiotic histologic pattern can mimic sarcoidosis, necessitating clinical correlation for correct diagnosis.13 Certain cases show genetic predisposition, such as HLA-B35, with a relapsing course often requiring combined systemic immunosuppression and phototherapy.14
Granulomatosis with polyangiitis is a systemic vasculitis that classically manifests as palpable purpura on the lower extremities, often with ulceration. Localized erythematous papules on the extensor surfaces may occur less commonly.15 Pathogenesis involves antineutrophil cytoplasmic antibodies inducing neutrophil degranulation, release of reactive oxygen species and proinflammatory cytokines, and subsequent endothelial damage.15 Histopathology shows necrotizing granulomatous inflammation and necrotizing vasculitis of small and medium vessels with nuclear debris.15 Poorly formed granulomas containing abundant neutrophils and mixed perivascular inflammatory infiltrates may be seen with or without vasculitis (Figure 4). Systemic features commonly include chronic rhinosinusitis, pauci-immune glomerulonephritis, and pulmonary nodules.15 Pharmacotherapy includes glucocorticoids combined with a glucocorticoid-sparing agent.
- Mazumder A, Mehrmal S, Chaudhry S. Immunotherapy-induced exclusively cutaneous sarcoid-like reaction. BMJ Case Rep. 2023;16:E252766. doi:10.1136/bcr-2022-252766
- Shah N, Shah M, Drucker AM, et al. Granulomatous cutaneous drug eruptions: a systematic review. Am J Clin Dermatol. 2021;22:39-53. doi:10.1007/s40257-020-00566-4
- Nykaza I, Murciano-Goroff YR, Desilets A, et al. Sarcoid-like reactions in patients treated with checkpoint inhibitors for advanced solid tumors. Oncologist. 2025;30:oyaf017. doi:10.1093/oncolo /oyaf017
- Tana C, Donatiello I, Caputo A, et al. Clinical features, histopathology and differential diagnosis of sarcoidosis. Cells. 2021;11:59. doi:10.3390/cells11010059
- Sibaud V. Dermatologic reactions to immune checkpoint inhibitors: skin toxicities and immunotherapy. Am J Clin Dermatol. 2018;19:345-361. doi:10.1007/s40257-017-0336-3
- Diaz-Perez JA, Beveridge MG, Victor TA, et al. Granulomatous and lichenoid dermatitis after IgG4 anti-PD-1 monoclonal antibody therapy for advanced cancer. J Cutan Pathol. 2018;45:434-438. doi:10.1111/cup.13133
- Chopra A, Nautiyal A, Kalkanis A, et al. Drug-induced sarcoidosis-like reactions. Chest. 2018;154:664-677. doi:10.1016 /j.chest.2018.03.056
- Froes LAR Jr, Sotto MN, Trindade MAB. Leprosy: clinical and immunopathological characteristics. An Bras Dermatol. 2022;97:338-347. doi:10.1016/j.abd.2021.08.006
- Magaña M, Vargas Bornacini MF, Landeta-Sa AP, et al. Lucio phenomenon: a review. Am J Dermatopathol. 2025;47:1-8. doi:10.1097 /DAD.0000000000002833
- Jayalakshmy PS, Prasad PH, Kamala VV, et al. Segmental necrotizing granulomatous neuritis: a rare manifestation of Hansen disease-report of 2 cases. Case Rep Dermatol Med. 2012;2012:758093. doi:10.1155/2012/758093
- Lee JH, Cho S. Resolution of refractory generalized granuloma annulare after treatment with alitretinoin. JAAD Case Rep. 2022;24:38-41. doi:10.1016/j.jdcr.2022.04.006
- Yun JH, Lee JY, Kim MK, et al. Clinical and pathological features of generalized granuloma annulare with their correlation: a retrospective multicenter study in Korea. Ann Dermatol. 2009; 21:113-119. doi:10.5021/ad.2009.21.2.113
- Cohen PR, Carlos CA. Granuloma annulare mimicking sarcoidosis: report of patient with localized granuloma annulare whose skin lesions show 3 clinical morphologies and 2 histology patterns. Am J Dermatopathol. 2015;37:547-550. doi:10.1097/DAD.0000000000000125
- Rankin BD, Haber RM. Familial granuloma annulare: first report of occurrence in a father and daughter and updated review of the literature. JAAD Case Rep. 2021;17:61-64. doi:10.1016 /j.jdcr.2021.09.023
- Rout P, Garlapati P, Qurie A. Granulomatosis with polyangiitis. StatPearls (Internet). Updated August 31, 2024. Accessed May 4, 2026. https://www.ncbi.nlm.nih.gov/books/NBK557827/
- Mazumder A, Mehrmal S, Chaudhry S. Immunotherapy-induced exclusively cutaneous sarcoid-like reaction. BMJ Case Rep. 2023;16:E252766. doi:10.1136/bcr-2022-252766
- Shah N, Shah M, Drucker AM, et al. Granulomatous cutaneous drug eruptions: a systematic review. Am J Clin Dermatol. 2021;22:39-53. doi:10.1007/s40257-020-00566-4
- Nykaza I, Murciano-Goroff YR, Desilets A, et al. Sarcoid-like reactions in patients treated with checkpoint inhibitors for advanced solid tumors. Oncologist. 2025;30:oyaf017. doi:10.1093/oncolo /oyaf017
- Tana C, Donatiello I, Caputo A, et al. Clinical features, histopathology and differential diagnosis of sarcoidosis. Cells. 2021;11:59. doi:10.3390/cells11010059
- Sibaud V. Dermatologic reactions to immune checkpoint inhibitors: skin toxicities and immunotherapy. Am J Clin Dermatol. 2018;19:345-361. doi:10.1007/s40257-017-0336-3
- Diaz-Perez JA, Beveridge MG, Victor TA, et al. Granulomatous and lichenoid dermatitis after IgG4 anti-PD-1 monoclonal antibody therapy for advanced cancer. J Cutan Pathol. 2018;45:434-438. doi:10.1111/cup.13133
- Chopra A, Nautiyal A, Kalkanis A, et al. Drug-induced sarcoidosis-like reactions. Chest. 2018;154:664-677. doi:10.1016 /j.chest.2018.03.056
- Froes LAR Jr, Sotto MN, Trindade MAB. Leprosy: clinical and immunopathological characteristics. An Bras Dermatol. 2022;97:338-347. doi:10.1016/j.abd.2021.08.006
- Magaña M, Vargas Bornacini MF, Landeta-Sa AP, et al. Lucio phenomenon: a review. Am J Dermatopathol. 2025;47:1-8. doi:10.1097 /DAD.0000000000002833
- Jayalakshmy PS, Prasad PH, Kamala VV, et al. Segmental necrotizing granulomatous neuritis: a rare manifestation of Hansen disease-report of 2 cases. Case Rep Dermatol Med. 2012;2012:758093. doi:10.1155/2012/758093
- Lee JH, Cho S. Resolution of refractory generalized granuloma annulare after treatment with alitretinoin. JAAD Case Rep. 2022;24:38-41. doi:10.1016/j.jdcr.2022.04.006
- Yun JH, Lee JY, Kim MK, et al. Clinical and pathological features of generalized granuloma annulare with their correlation: a retrospective multicenter study in Korea. Ann Dermatol. 2009; 21:113-119. doi:10.5021/ad.2009.21.2.113
- Cohen PR, Carlos CA. Granuloma annulare mimicking sarcoidosis: report of patient with localized granuloma annulare whose skin lesions show 3 clinical morphologies and 2 histology patterns. Am J Dermatopathol. 2015;37:547-550. doi:10.1097/DAD.0000000000000125
- Rankin BD, Haber RM. Familial granuloma annulare: first report of occurrence in a father and daughter and updated review of the literature. JAAD Case Rep. 2021;17:61-64. doi:10.1016 /j.jdcr.2021.09.023
- Rout P, Garlapati P, Qurie A. Granulomatosis with polyangiitis. StatPearls (Internet). Updated August 31, 2024. Accessed May 4, 2026. https://www.ncbi.nlm.nih.gov/books/NBK557827/
Pink Papulonodular Eruption on the Trunk and Arms
Pink Papulonodular Eruption on the Trunk and Arms
A 47-year-old man with a history of chronic kidney disease and bilateral clear cell renal cell carcinoma who was undergoing treatment with adjuvant pembrolizumab presented to the dermatology department with a scattered papulonodular eruption of several weeks’ duration. Physical examination revealed pink papules and nodules with coalescing erythema over the trunk and upper extremities, most pronounced on the right elbow (bottom [inset]). A 4-mm punch biopsy demonstrated dermal granulomatous inflammation. Special stains were negative for microorganisms. Computed tomography of the chest revealed a new subpleural nodule and new hilar lymphadenopathy.

Association Between Hidradenitis Suppurativa and Polycystic Ovary Syndrome
Association Between Hidradenitis Suppurativa and Polycystic Ovary Syndrome
Hidradenitis suppurativa (HS) is a chronic inflammatory skin condition characterized by painful nodules, abscesses, scarring, and sinus tracts that commonly manifest in the axillary, inguinal, perianal, and inframammary regions.1 Hidradenitis suppurativa has been associated with several metabolic and cardiovascular comorbidities as well as polycystic ovary syndrome (PCOS)(recently renamed polyendocrine metabolic ovarian syndrome),2,3 a condition characterized by hyperandrogenism, chronic anovulation, and polycystic ovaries.2 Multiple comorbidities of PCOS overlap with those of HS, including type 2 diabetes, cardiovascular disease, and metabolic syndrome.1,3-5 While HS may be associated with PCOS, there is limited literature analyzing the association between these conditions. This study aimed to analyze the association between HS and PCOS using data from the National Institute of Health’s All of Us Research Program database (https://allofus.nih.gov/). While other studies have looked at the association between HS and PCOS, ours is among the first to analyze the relationship between multiple race/ ethnicity groups, which is especially important given racial disparities in HS and comorbid diseases.
Methods
A cross-sectional, population-based study of females included in the All of Us Research Program database was conducted. Patients with HS were identified using the Systematized Nomenclature of Medicine–Clinical Terms (SNOMED CT) code 59393003, while PCOS was identified with the code 237055002. Type 2 diabetes was identified with the following SNOMED CT codes: 44054006, 313436004, 237599002, 199230006, 359642000, and 81531005. Obesity was identified with the following codes: 414916001, 238136002, 190966007, 296526005, 294493008, 238134004, 83911000119104, and 415530009. Male patients and those who did not answer questions regarding sociodemographic variables were excluded from the final analysis. P values were calculated using Pearson χ2 tests. Multivariate logistic regression was used to calculate adjusted odds ratios and unadjusted odds ratios to analyze the association between HS and PCOS while controlling for age, race/ethnicity, smoking status, type 2 diabetes, and obesity. Statistical analyses were conducted using a 95% CI.
Results
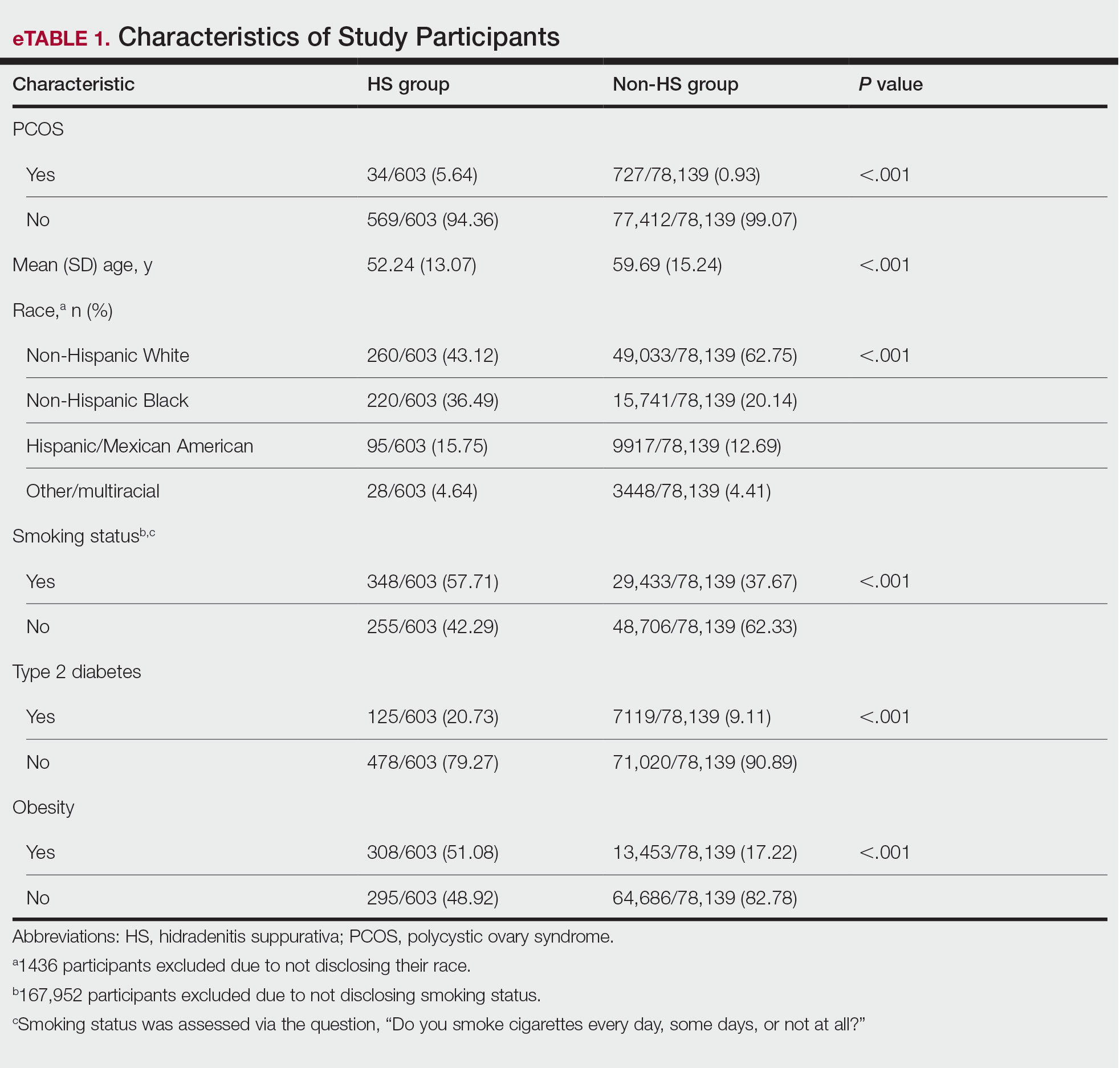
The final analysis included 78,742 patients. The prevalence of PCOS was 5.64% in the HS group vs 0.93% in the non-HS group (eTable 1). Individuals with HS had higher rates of smoking cigarettes (57.71% vs 37.67%), obesity (51.08% vs 17.22%), and type 2 diabetes (20.73% vs 9.11%) than individuals without HS, respectively.
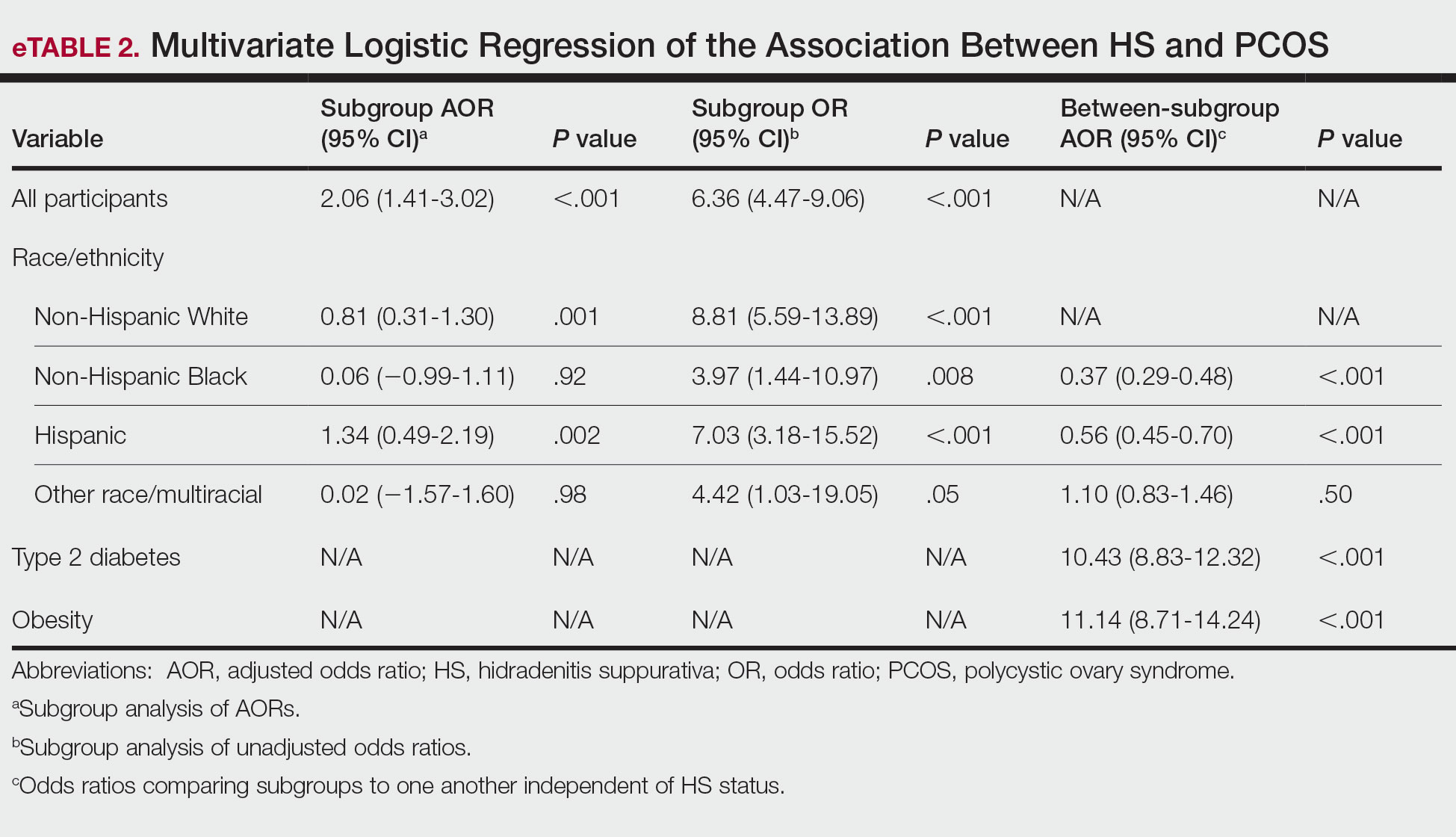
Multivariate logistic regression analyses revealed that individuals with HS were 2.06 times more likely to have PCOS after adjusting for sociodemographic variables and comorbidities (95% CI, 1.41-3.02; P<.001). Adjusted subgroup analyses by race/ethnicity did not yield statistically significant results; however, unadjusted analyses revealed that individuals with HS had significantly increased odds of PCOS across all race/ethnicity groups (eTable 2). Interaction terms analysis to determine if the relationship between HS and PCOS differs by race/ ethnicity did not yield statistically significant results. However, independent of HS status, non-Hispanic Black and Hispanic patients were less likely to have PCOS compared to White individuals (adjusted odds ratio, 0.37 and 0.56, respectively; P<.001). Disparities in access to care could have led to underdiagnosis of PCOS among non-Hispanic Black and Hispanic patients. Lastly, individuals with type 2 diabetes were 10.43 times more likely to have PCOS than those without, while patients with obesity were 11.14 times more likely to have PCOS than those without.
Comment
This study demonstrated that females with HS are 2.06 times more likely to have PCOS than those without HS, even after controlling for important sociodemographic variables and comorbidities. While adjusted subgroup analyses did not yield statistically significant results, unadjusted analyses demonstrated increased odds of PCOS in patients with HS across all race/ethnicity groups, suggesting that sociodemographic variables and comorbidities substantially influence the relationship between HS and PCOS; for instance, patients with type 2 diabetes and obesity are approximately 10- to 11-fold more likely to have PCOS than patients without these conditions. Non-Hispanic Black and Hispanic patients were less likely to have PCOS compared with White patients, indicating possible underdiagnosis of PCOS in these populations and highlighting the need for increased PCOS screening. Limitations of this study include the reliance on SNOMED CT codes, which may have led to underdiagnosis of HS or PCOS, as well as the inability to differentiate between mild and severe HS in the database.
Hyperandrogenism is believed to contribute to the pathogenesis of both HS and PCOS, supporting the potential use of antiandrogen therapies, such as spironolactone, in managing both conditions.2,3 Furthermore, oral contraceptives may have a role in managing both conditions. In HS, oral contraceptives help to mitigate flares associated with hormonal changes during menstruation, while in PCOS, they are used to regulate the hormonal cycle and reduce hirsutism.2-4 However, not all women experience menstrual flares of HS, suggesting that variations in HS phenotypes may influence individual responses to hormonal changes.1 Additionally, the considerable overlap in metabolic and cardiovascular comorbidities between HS and PCOS indicates that shared pathomechanisms may contribute to the association between these conditions.1,2 For example, proinflammatory adipokines released in both HS and PCOS may contribute to inflammation, cardiovascular disease, and insulin resistance.3,5
Conclusion
Further research is needed to better understand the shared pathophysiology that links these 2 diseases and to identify targeted approaches for optimizing management and improving patient outcomes. The association between HS and PCOS highlights the importance of screening for metabolic and reproductive comorbidities in patients with HS. Early recognition and management of both HS and PCOS can improve long-term outcomes.
- van Straalen KR, Prens EP, Gudjonsson JE. Insights into hidradenitis suppurativa. J Allergy Clin Immunol. 2022;149:1150-1161. doi:10.1016 /j.jaci.2022.02.003
- Choudhari R, Tayade S, Tiwari A, et al. Diagnosis, management, and associated comorbidities of polycystic ovary syndrome: a narrative review. Cureus. 2024;16:e58733. doi:10.7759/cureus.58733
- Abu Rached N, Gambichler T, Dietrich JW, et al. The role of hormones in hidradenitis suppurativa: a systematic review. Int J Mol Sci. 2022;23:15250. doi:10.3390/ijms232315250
- Montero-Vilchez T, Valenzuela-Amigo A, Cuenca-Barrales C, et al. The role of oral contraceptive pills in hidradenitis suppurativa: a cohort study. Life (Basel). 2021;11:697. doi:10.3390/life11070697
- Randeva HS, Tan BK, Weickert MO, et al. Cardiometabolic aspects of the polycystic ovary syndrome. Endocr Rev. 2012;33:812-841. doi:10.1210/er.2012-1003
Hidradenitis suppurativa (HS) is a chronic inflammatory skin condition characterized by painful nodules, abscesses, scarring, and sinus tracts that commonly manifest in the axillary, inguinal, perianal, and inframammary regions.1 Hidradenitis suppurativa has been associated with several metabolic and cardiovascular comorbidities as well as polycystic ovary syndrome (PCOS)(recently renamed polyendocrine metabolic ovarian syndrome),2,3 a condition characterized by hyperandrogenism, chronic anovulation, and polycystic ovaries.2 Multiple comorbidities of PCOS overlap with those of HS, including type 2 diabetes, cardiovascular disease, and metabolic syndrome.1,3-5 While HS may be associated with PCOS, there is limited literature analyzing the association between these conditions. This study aimed to analyze the association between HS and PCOS using data from the National Institute of Health’s All of Us Research Program database (https://allofus.nih.gov/). While other studies have looked at the association between HS and PCOS, ours is among the first to analyze the relationship between multiple race/ ethnicity groups, which is especially important given racial disparities in HS and comorbid diseases.
Methods
A cross-sectional, population-based study of females included in the All of Us Research Program database was conducted. Patients with HS were identified using the Systematized Nomenclature of Medicine–Clinical Terms (SNOMED CT) code 59393003, while PCOS was identified with the code 237055002. Type 2 diabetes was identified with the following SNOMED CT codes: 44054006, 313436004, 237599002, 199230006, 359642000, and 81531005. Obesity was identified with the following codes: 414916001, 238136002, 190966007, 296526005, 294493008, 238134004, 83911000119104, and 415530009. Male patients and those who did not answer questions regarding sociodemographic variables were excluded from the final analysis. P values were calculated using Pearson χ2 tests. Multivariate logistic regression was used to calculate adjusted odds ratios and unadjusted odds ratios to analyze the association between HS and PCOS while controlling for age, race/ethnicity, smoking status, type 2 diabetes, and obesity. Statistical analyses were conducted using a 95% CI.
Results
The final analysis included 78,742 patients. The prevalence of PCOS was 5.64% in the HS group vs 0.93% in the non-HS group (eTable 1). Individuals with HS had higher rates of smoking cigarettes (57.71% vs 37.67%), obesity (51.08% vs 17.22%), and type 2 diabetes (20.73% vs 9.11%) than individuals without HS, respectively.
Multivariate logistic regression analyses revealed that individuals with HS were 2.06 times more likely to have PCOS after adjusting for sociodemographic variables and comorbidities (95% CI, 1.41-3.02; P<.001). Adjusted subgroup analyses by race/ethnicity did not yield statistically significant results; however, unadjusted analyses revealed that individuals with HS had significantly increased odds of PCOS across all race/ethnicity groups (eTable 2). Interaction terms analysis to determine if the relationship between HS and PCOS differs by race/ ethnicity did not yield statistically significant results. However, independent of HS status, non-Hispanic Black and Hispanic patients were less likely to have PCOS compared to White individuals (adjusted odds ratio, 0.37 and 0.56, respectively; P<.001). Disparities in access to care could have led to underdiagnosis of PCOS among non-Hispanic Black and Hispanic patients. Lastly, individuals with type 2 diabetes were 10.43 times more likely to have PCOS than those without, while patients with obesity were 11.14 times more likely to have PCOS than those without.
Comment
This study demonstrated that females with HS are 2.06 times more likely to have PCOS than those without HS, even after controlling for important sociodemographic variables and comorbidities. While adjusted subgroup analyses did not yield statistically significant results, unadjusted analyses demonstrated increased odds of PCOS in patients with HS across all race/ethnicity groups, suggesting that sociodemographic variables and comorbidities substantially influence the relationship between HS and PCOS; for instance, patients with type 2 diabetes and obesity are approximately 10- to 11-fold more likely to have PCOS than patients without these conditions. Non-Hispanic Black and Hispanic patients were less likely to have PCOS compared with White patients, indicating possible underdiagnosis of PCOS in these populations and highlighting the need for increased PCOS screening. Limitations of this study include the reliance on SNOMED CT codes, which may have led to underdiagnosis of HS or PCOS, as well as the inability to differentiate between mild and severe HS in the database.
Hyperandrogenism is believed to contribute to the pathogenesis of both HS and PCOS, supporting the potential use of antiandrogen therapies, such as spironolactone, in managing both conditions.2,3 Furthermore, oral contraceptives may have a role in managing both conditions. In HS, oral contraceptives help to mitigate flares associated with hormonal changes during menstruation, while in PCOS, they are used to regulate the hormonal cycle and reduce hirsutism.2-4 However, not all women experience menstrual flares of HS, suggesting that variations in HS phenotypes may influence individual responses to hormonal changes.1 Additionally, the considerable overlap in metabolic and cardiovascular comorbidities between HS and PCOS indicates that shared pathomechanisms may contribute to the association between these conditions.1,2 For example, proinflammatory adipokines released in both HS and PCOS may contribute to inflammation, cardiovascular disease, and insulin resistance.3,5
Conclusion
Further research is needed to better understand the shared pathophysiology that links these 2 diseases and to identify targeted approaches for optimizing management and improving patient outcomes. The association between HS and PCOS highlights the importance of screening for metabolic and reproductive comorbidities in patients with HS. Early recognition and management of both HS and PCOS can improve long-term outcomes.
Hidradenitis suppurativa (HS) is a chronic inflammatory skin condition characterized by painful nodules, abscesses, scarring, and sinus tracts that commonly manifest in the axillary, inguinal, perianal, and inframammary regions.1 Hidradenitis suppurativa has been associated with several metabolic and cardiovascular comorbidities as well as polycystic ovary syndrome (PCOS)(recently renamed polyendocrine metabolic ovarian syndrome),2,3 a condition characterized by hyperandrogenism, chronic anovulation, and polycystic ovaries.2 Multiple comorbidities of PCOS overlap with those of HS, including type 2 diabetes, cardiovascular disease, and metabolic syndrome.1,3-5 While HS may be associated with PCOS, there is limited literature analyzing the association between these conditions. This study aimed to analyze the association between HS and PCOS using data from the National Institute of Health’s All of Us Research Program database (https://allofus.nih.gov/). While other studies have looked at the association between HS and PCOS, ours is among the first to analyze the relationship between multiple race/ ethnicity groups, which is especially important given racial disparities in HS and comorbid diseases.
Methods
A cross-sectional, population-based study of females included in the All of Us Research Program database was conducted. Patients with HS were identified using the Systematized Nomenclature of Medicine–Clinical Terms (SNOMED CT) code 59393003, while PCOS was identified with the code 237055002. Type 2 diabetes was identified with the following SNOMED CT codes: 44054006, 313436004, 237599002, 199230006, 359642000, and 81531005. Obesity was identified with the following codes: 414916001, 238136002, 190966007, 296526005, 294493008, 238134004, 83911000119104, and 415530009. Male patients and those who did not answer questions regarding sociodemographic variables were excluded from the final analysis. P values were calculated using Pearson χ2 tests. Multivariate logistic regression was used to calculate adjusted odds ratios and unadjusted odds ratios to analyze the association between HS and PCOS while controlling for age, race/ethnicity, smoking status, type 2 diabetes, and obesity. Statistical analyses were conducted using a 95% CI.
Results
The final analysis included 78,742 patients. The prevalence of PCOS was 5.64% in the HS group vs 0.93% in the non-HS group (eTable 1). Individuals with HS had higher rates of smoking cigarettes (57.71% vs 37.67%), obesity (51.08% vs 17.22%), and type 2 diabetes (20.73% vs 9.11%) than individuals without HS, respectively.
Multivariate logistic regression analyses revealed that individuals with HS were 2.06 times more likely to have PCOS after adjusting for sociodemographic variables and comorbidities (95% CI, 1.41-3.02; P<.001). Adjusted subgroup analyses by race/ethnicity did not yield statistically significant results; however, unadjusted analyses revealed that individuals with HS had significantly increased odds of PCOS across all race/ethnicity groups (eTable 2). Interaction terms analysis to determine if the relationship between HS and PCOS differs by race/ ethnicity did not yield statistically significant results. However, independent of HS status, non-Hispanic Black and Hispanic patients were less likely to have PCOS compared to White individuals (adjusted odds ratio, 0.37 and 0.56, respectively; P<.001). Disparities in access to care could have led to underdiagnosis of PCOS among non-Hispanic Black and Hispanic patients. Lastly, individuals with type 2 diabetes were 10.43 times more likely to have PCOS than those without, while patients with obesity were 11.14 times more likely to have PCOS than those without.
Comment
This study demonstrated that females with HS are 2.06 times more likely to have PCOS than those without HS, even after controlling for important sociodemographic variables and comorbidities. While adjusted subgroup analyses did not yield statistically significant results, unadjusted analyses demonstrated increased odds of PCOS in patients with HS across all race/ethnicity groups, suggesting that sociodemographic variables and comorbidities substantially influence the relationship between HS and PCOS; for instance, patients with type 2 diabetes and obesity are approximately 10- to 11-fold more likely to have PCOS than patients without these conditions. Non-Hispanic Black and Hispanic patients were less likely to have PCOS compared with White patients, indicating possible underdiagnosis of PCOS in these populations and highlighting the need for increased PCOS screening. Limitations of this study include the reliance on SNOMED CT codes, which may have led to underdiagnosis of HS or PCOS, as well as the inability to differentiate between mild and severe HS in the database.
Hyperandrogenism is believed to contribute to the pathogenesis of both HS and PCOS, supporting the potential use of antiandrogen therapies, such as spironolactone, in managing both conditions.2,3 Furthermore, oral contraceptives may have a role in managing both conditions. In HS, oral contraceptives help to mitigate flares associated with hormonal changes during menstruation, while in PCOS, they are used to regulate the hormonal cycle and reduce hirsutism.2-4 However, not all women experience menstrual flares of HS, suggesting that variations in HS phenotypes may influence individual responses to hormonal changes.1 Additionally, the considerable overlap in metabolic and cardiovascular comorbidities between HS and PCOS indicates that shared pathomechanisms may contribute to the association between these conditions.1,2 For example, proinflammatory adipokines released in both HS and PCOS may contribute to inflammation, cardiovascular disease, and insulin resistance.3,5
Conclusion
Further research is needed to better understand the shared pathophysiology that links these 2 diseases and to identify targeted approaches for optimizing management and improving patient outcomes. The association between HS and PCOS highlights the importance of screening for metabolic and reproductive comorbidities in patients with HS. Early recognition and management of both HS and PCOS can improve long-term outcomes.
- van Straalen KR, Prens EP, Gudjonsson JE. Insights into hidradenitis suppurativa. J Allergy Clin Immunol. 2022;149:1150-1161. doi:10.1016 /j.jaci.2022.02.003
- Choudhari R, Tayade S, Tiwari A, et al. Diagnosis, management, and associated comorbidities of polycystic ovary syndrome: a narrative review. Cureus. 2024;16:e58733. doi:10.7759/cureus.58733
- Abu Rached N, Gambichler T, Dietrich JW, et al. The role of hormones in hidradenitis suppurativa: a systematic review. Int J Mol Sci. 2022;23:15250. doi:10.3390/ijms232315250
- Montero-Vilchez T, Valenzuela-Amigo A, Cuenca-Barrales C, et al. The role of oral contraceptive pills in hidradenitis suppurativa: a cohort study. Life (Basel). 2021;11:697. doi:10.3390/life11070697
- Randeva HS, Tan BK, Weickert MO, et al. Cardiometabolic aspects of the polycystic ovary syndrome. Endocr Rev. 2012;33:812-841. doi:10.1210/er.2012-1003
- van Straalen KR, Prens EP, Gudjonsson JE. Insights into hidradenitis suppurativa. J Allergy Clin Immunol. 2022;149:1150-1161. doi:10.1016 /j.jaci.2022.02.003
- Choudhari R, Tayade S, Tiwari A, et al. Diagnosis, management, and associated comorbidities of polycystic ovary syndrome: a narrative review. Cureus. 2024;16:e58733. doi:10.7759/cureus.58733
- Abu Rached N, Gambichler T, Dietrich JW, et al. The role of hormones in hidradenitis suppurativa: a systematic review. Int J Mol Sci. 2022;23:15250. doi:10.3390/ijms232315250
- Montero-Vilchez T, Valenzuela-Amigo A, Cuenca-Barrales C, et al. The role of oral contraceptive pills in hidradenitis suppurativa: a cohort study. Life (Basel). 2021;11:697. doi:10.3390/life11070697
- Randeva HS, Tan BK, Weickert MO, et al. Cardiometabolic aspects of the polycystic ovary syndrome. Endocr Rev. 2012;33:812-841. doi:10.1210/er.2012-1003
Association Between Hidradenitis Suppurativa and Polycystic Ovary Syndrome
Association Between Hidradenitis Suppurativa and Polycystic Ovary Syndrome
PRACTICE POINTS
- Patients with hidradenitis suppurativa were 2.06 times more likely to have polycystic ovary syndrome (PCOS) than patients without HS after controlling for age, race/ ethnicity, tobacco use, type 2 diabetes, and obesity.
- Non-Hispanic Black and Hispanic patients were less likely than White patients to have a diagnosis of PCOS, potentially reflecting underdiagnosis in these populations.
- Individuals with type 2 diabetes and obesity were 10.43 and 11.14 times more likely, respectively, to have PCOS.

Atopic Dermatitis: New Insights and Expanded Treatment Options
Atopic Dermatitis: New Insights and Expanded Treatment Options
Atopic dermatitis (AD) is a chronic skin condition generally characterized by pruritic and erythematous papules and plaques.1 While AD commonly manifests in childhood, 1 in 4 patients living with AD report adult onset of the disease.2 The clinical presentation and prevalence of AD vary across age groups, skin tones, and racial and ethnic groups. Globally, AD is estimated to have a prevalence of 2.6%; however, rates vary widely by region.1 Morphology and distribution of AD lesions also vary by population; therefore, defining one classic presentation of AD is not sufficient in diverse patient populations.3
Epidemiology
The prevalence of AD ranges from 0.2% to 24.6% worldwide, with higher rates in Africa and Oceania and lower rates in India and Northern and Eastern Europe.1 In the United States, AD affects all racial and ethnic groups; however, prevalence and severity are increased in Black children compared with White children.4 In one prospective cohort study, Hispanic children and non-Hispanic Black children aged 3 years and younger had greater odds of AD persisting into mid childhood (approximately age 7 years) compared with non-Hispanic White children.5,6
Key Clinical Features
Clinical features of AD are heterogeneous and may include differences in color, morphology, and distribution. Brown, hyperpigmented, gray, and/or violaceous plaques may predominate in patients with skin of color (SOC) compared with the erythematous plaques commonly described in lighter skin tones.1,3 Established scoring systems for AD rely on erythema as a key diagnostic feature, but because erythema can be difficult to detect in darker skin tones, disease severity may be underestimated and diagnosis may be delayed in this population.4
Atopic dermatitis in SOC may manifest as lichenoid plaques,7 prurigo nodules,7,8 lichenification,1 and follicular accentuation.9 Lichen planus–like AD is a distinct variant characterized by lichenoid plaques with a predilection for the extensor surfaces and face in patients with darker skin tones1,8 occurring in approximately 9% of patients in one study.10
Other key clinical features of AD in patients with SOC include pityriasis alba,10 increased risk for postinflammatory pigment alteration (including hyperpigmentation and/or hypopigmentation),1 and greater trunk and extensor involvement.1,11
Worth Noting
The scientific landscape for AD has grown rapidly, increasing our understanding of its pathophysiology, treatment, and social impact. Nonsteroidal treatments available for pediatric and adult patients with AD have increased in recent years, including crisaborole (approved for use in those ages ≥3 months), tacrolimus (≥2 years), and pimecrolimus (≥2 years). Injectable options include dupilumab (≥6 months), lebrikizumab (≥12 years), nemolizumab (≥12 years), and tralokinumab (≥12 years). Oral options include abrocitinib (≥12 years) and upadacitinib (≥12 years).12 Topical options include roflumilast 0.15% cream (≥6 years)12 and 0.05% cream (≥2-5 years),13 ruxolitinib 1.5% cream (≥2 years),14 and tapinarof 1% cream (≥2 years).12
For some patients, postinflammatory pigment alteration associated with AD has a higher impact on quality of life than the AD itself.7 In a study of 260 US adults with AD, the emotional impact of pigmentary changes was greatest in Black patients, with 53.3% reporting that pigment changes bothered them “a lot” or “very much.”15
Genome-wide association studies have not identified a single determinant that explains racial and ethnic differences in susceptibility to AD.4 Instead, social determinants of health are thought to play a role in the difference in AD prevalence and severity across groups in the United States.16
Health Disparity Highlight
In an analysis of 20 US metropolitan cities, urban and inner-city residence was associated with approximately 1.7-fold increased odds of AD.4 Among pediatric patients with moderate to severe AD, Black children were more likely to be exposed to tobacco smoke17 and traffic-related air pollution.18 Low socioeconomic status and low income also have been associated with moderate16 and severe19 AD. At the same education level, Black individuals in the United States receive less income than their White counterparts and have markedly less wealth at equivalent incomes.20
In utero exposure to maternal stress is associated with AD.4 Increased IgE levels have been recorded in children who develop AD, with Black children having the highest IgE levels overall compared to other children.18
An analysis of medical records from an urban medical center in Baltimore, Maryland, from 2013 through 2018 showed that Black patients with AD were less likely to receive topical corticosteroids, topical calcineurin inhibitors, a topical phosphodiesterase 4 inhibitor, and a biologic compared to White patients with AD.21
Since the disproportionate burden experienced by patients with AD is not physiologic, it is imperative to address these systemic complexities and address the barriers impacting treatment availability to improve health outcomes for all patients living with AD.
- Kaufman BP, Guttman-Yassky E, Alexis AF. Atopic dermatitis in diverse racial and ethnic groups—variations in epidemiology, genetics, clinical presentation and treatment. Exp Dermatol. 2018;27:340-357.
- Lee HH, Patel KR, Singam V, et al. A systematic review and meta-analysis of the prevalence and phenotype of adult-onset atopic dermatitis. J Am Acad Dermatol. 2019;80:1526-1532.E7.
- Adawi W, Cornman H, Kambala A, et al. Diagnosing atopic dermatitis in skin of color. Dermatol Clin. 2023;41:417-429.
- Narla S, Silverberg JI. Current updates in the epidemiology and comorbidities of atopic dermatitis. Ann Allergy Asthma Immunol. 2025;135:511-520.
- Croce EA, Levy ML, Adamson AS, et al. Reframing racial and ethnic disparities in atopic dermatitis in Black and Latinx populations. J Allergy Clin Immunol. 2021;148:1104-1111.
- Kim Y, Blomberg M, Rifas-Shiman SL, et al. Racial/ethnic differences in incidence and persistence of childhood atopic dermatitis. J Invest Dermatol. 2019;139:827-834.
- Nomura T, Wu J, Kabashima K, et al. Endophenotypic variations of atopic dermatitis by age, race, and ethnicity. J Allergy Clin Immunol. 2020;8:1840-1852.
- McColl M, Boozalis E, Aguh C, et al. Pruritus in Black skin: unique molecular characteristics and clinical features. J Natl Med Assoc. 2021;114:30-38.
- Silverberg JI, Margolis DJ, Boguniewicz M, et al. Distribution of atopic dermatitis lesions in United States adults. J Eur Acad Dermatol Venereol. 2019;33:1341-1348.
- Summey BT, Bowen SE, Allen HB. Lichen planus-like atopic dermatitis: expanding the differential diagnosis of spongiotic dermatitis. J Cutan Pathol. 2008;35:311-314.
- Odhiambo JA, Williams HC, Clayton TO, et al; ISAAC Phase Three Study Group. Global variations in prevalence of eczema symptoms in children from ISAAC Phase Three. J Allergy Clin Immunol. 2009;124:1251-1258.E23.
- Gallagher K, Halperin-Goldstein S, Paller AS. New treatments in atopic dermatitis update. Ann Allergy Asthma Immunol. 2025;135:498-510.E10.
- Shaw ML. FDA expands roflumilast use for atopic dermatitis to children aged 2 to 5 years. Am J Managed Care. October 6, 2025. Accessed April 30, 2026. https://www.ajmc.com/view/fda-expands -roflumilast-use-for-atopic-dermatitis-to-children-aged-2-to-5-years
- Eichenfield LF, Stein Gold LF, Simpson EL, et al. Efficacy and safety of ruxolitinib cream in children aged 2 to 11 years with atopic dermatitis: results from TRuE-AD3, a phase 3, randomized double-blind study. J Am Acad of Dermatol. 2025;93:689-698.
- Heath CR, Dosono B, Shi VY, et al. Variability in skin tone changes by race and ethnicity among US adults with atopic dermatitis. Presented at: Skin of Color Update 2024, September 13-15, 2024, New York, NY.
- Tackett KJ, Jenkins F, Morrell DS, et al. Structural racism and its influence on the severity of atopic dermatitis in African American children. Pediatr Dermatol. 2020;37:142-146.
- Narla S, Silverberg JI. The role of environmental exposures in atopic dermatitis. Curr Allergy Asthma Rep. 2020;20:74.
- Bauer SJ, Spoer BR, Ehrman R, et al. A systematic review of historic neighborhood redlining and contemporary health outcomes. Public Health. 2025;238:181-187.
- Chung J, Simpson EL. The socioeconomics of atopic dermatitis. Ann Allergy Asthma Immunol. 2019;122:360-366.
- Martinez A, de la Rosa R, Mujahid M, et al. Structural racism and its pathways to asthma and atopic dermatitis. J Allergy Clin Immunol. 2021;148:1112-1120.
- Bell MA, Whang KA, Thomas J, et al. Racial and ethnic disparities in access to emerging and frontline therapies in common dermatological conditions: a cross-sectional study. J Natl Med Assoc. 2020;112:650-653.
Atopic dermatitis (AD) is a chronic skin condition generally characterized by pruritic and erythematous papules and plaques.1 While AD commonly manifests in childhood, 1 in 4 patients living with AD report adult onset of the disease.2 The clinical presentation and prevalence of AD vary across age groups, skin tones, and racial and ethnic groups. Globally, AD is estimated to have a prevalence of 2.6%; however, rates vary widely by region.1 Morphology and distribution of AD lesions also vary by population; therefore, defining one classic presentation of AD is not sufficient in diverse patient populations.3
Epidemiology
The prevalence of AD ranges from 0.2% to 24.6% worldwide, with higher rates in Africa and Oceania and lower rates in India and Northern and Eastern Europe.1 In the United States, AD affects all racial and ethnic groups; however, prevalence and severity are increased in Black children compared with White children.4 In one prospective cohort study, Hispanic children and non-Hispanic Black children aged 3 years and younger had greater odds of AD persisting into mid childhood (approximately age 7 years) compared with non-Hispanic White children.5,6
Key Clinical Features
Clinical features of AD are heterogeneous and may include differences in color, morphology, and distribution. Brown, hyperpigmented, gray, and/or violaceous plaques may predominate in patients with skin of color (SOC) compared with the erythematous plaques commonly described in lighter skin tones.1,3 Established scoring systems for AD rely on erythema as a key diagnostic feature, but because erythema can be difficult to detect in darker skin tones, disease severity may be underestimated and diagnosis may be delayed in this population.4
Atopic dermatitis in SOC may manifest as lichenoid plaques,7 prurigo nodules,7,8 lichenification,1 and follicular accentuation.9 Lichen planus–like AD is a distinct variant characterized by lichenoid plaques with a predilection for the extensor surfaces and face in patients with darker skin tones1,8 occurring in approximately 9% of patients in one study.10
Other key clinical features of AD in patients with SOC include pityriasis alba,10 increased risk for postinflammatory pigment alteration (including hyperpigmentation and/or hypopigmentation),1 and greater trunk and extensor involvement.1,11
Worth Noting
The scientific landscape for AD has grown rapidly, increasing our understanding of its pathophysiology, treatment, and social impact. Nonsteroidal treatments available for pediatric and adult patients with AD have increased in recent years, including crisaborole (approved for use in those ages ≥3 months), tacrolimus (≥2 years), and pimecrolimus (≥2 years). Injectable options include dupilumab (≥6 months), lebrikizumab (≥12 years), nemolizumab (≥12 years), and tralokinumab (≥12 years). Oral options include abrocitinib (≥12 years) and upadacitinib (≥12 years).12 Topical options include roflumilast 0.15% cream (≥6 years)12 and 0.05% cream (≥2-5 years),13 ruxolitinib 1.5% cream (≥2 years),14 and tapinarof 1% cream (≥2 years).12
For some patients, postinflammatory pigment alteration associated with AD has a higher impact on quality of life than the AD itself.7 In a study of 260 US adults with AD, the emotional impact of pigmentary changes was greatest in Black patients, with 53.3% reporting that pigment changes bothered them “a lot” or “very much.”15
Genome-wide association studies have not identified a single determinant that explains racial and ethnic differences in susceptibility to AD.4 Instead, social determinants of health are thought to play a role in the difference in AD prevalence and severity across groups in the United States.16
Health Disparity Highlight
In an analysis of 20 US metropolitan cities, urban and inner-city residence was associated with approximately 1.7-fold increased odds of AD.4 Among pediatric patients with moderate to severe AD, Black children were more likely to be exposed to tobacco smoke17 and traffic-related air pollution.18 Low socioeconomic status and low income also have been associated with moderate16 and severe19 AD. At the same education level, Black individuals in the United States receive less income than their White counterparts and have markedly less wealth at equivalent incomes.20
In utero exposure to maternal stress is associated with AD.4 Increased IgE levels have been recorded in children who develop AD, with Black children having the highest IgE levels overall compared to other children.18
An analysis of medical records from an urban medical center in Baltimore, Maryland, from 2013 through 2018 showed that Black patients with AD were less likely to receive topical corticosteroids, topical calcineurin inhibitors, a topical phosphodiesterase 4 inhibitor, and a biologic compared to White patients with AD.21
Since the disproportionate burden experienced by patients with AD is not physiologic, it is imperative to address these systemic complexities and address the barriers impacting treatment availability to improve health outcomes for all patients living with AD.
Atopic dermatitis (AD) is a chronic skin condition generally characterized by pruritic and erythematous papules and plaques.1 While AD commonly manifests in childhood, 1 in 4 patients living with AD report adult onset of the disease.2 The clinical presentation and prevalence of AD vary across age groups, skin tones, and racial and ethnic groups. Globally, AD is estimated to have a prevalence of 2.6%; however, rates vary widely by region.1 Morphology and distribution of AD lesions also vary by population; therefore, defining one classic presentation of AD is not sufficient in diverse patient populations.3
Epidemiology
The prevalence of AD ranges from 0.2% to 24.6% worldwide, with higher rates in Africa and Oceania and lower rates in India and Northern and Eastern Europe.1 In the United States, AD affects all racial and ethnic groups; however, prevalence and severity are increased in Black children compared with White children.4 In one prospective cohort study, Hispanic children and non-Hispanic Black children aged 3 years and younger had greater odds of AD persisting into mid childhood (approximately age 7 years) compared with non-Hispanic White children.5,6
Key Clinical Features
Clinical features of AD are heterogeneous and may include differences in color, morphology, and distribution. Brown, hyperpigmented, gray, and/or violaceous plaques may predominate in patients with skin of color (SOC) compared with the erythematous plaques commonly described in lighter skin tones.1,3 Established scoring systems for AD rely on erythema as a key diagnostic feature, but because erythema can be difficult to detect in darker skin tones, disease severity may be underestimated and diagnosis may be delayed in this population.4
Atopic dermatitis in SOC may manifest as lichenoid plaques,7 prurigo nodules,7,8 lichenification,1 and follicular accentuation.9 Lichen planus–like AD is a distinct variant characterized by lichenoid plaques with a predilection for the extensor surfaces and face in patients with darker skin tones1,8 occurring in approximately 9% of patients in one study.10
Other key clinical features of AD in patients with SOC include pityriasis alba,10 increased risk for postinflammatory pigment alteration (including hyperpigmentation and/or hypopigmentation),1 and greater trunk and extensor involvement.1,11
Worth Noting
The scientific landscape for AD has grown rapidly, increasing our understanding of its pathophysiology, treatment, and social impact. Nonsteroidal treatments available for pediatric and adult patients with AD have increased in recent years, including crisaborole (approved for use in those ages ≥3 months), tacrolimus (≥2 years), and pimecrolimus (≥2 years). Injectable options include dupilumab (≥6 months), lebrikizumab (≥12 years), nemolizumab (≥12 years), and tralokinumab (≥12 years). Oral options include abrocitinib (≥12 years) and upadacitinib (≥12 years).12 Topical options include roflumilast 0.15% cream (≥6 years)12 and 0.05% cream (≥2-5 years),13 ruxolitinib 1.5% cream (≥2 years),14 and tapinarof 1% cream (≥2 years).12
For some patients, postinflammatory pigment alteration associated with AD has a higher impact on quality of life than the AD itself.7 In a study of 260 US adults with AD, the emotional impact of pigmentary changes was greatest in Black patients, with 53.3% reporting that pigment changes bothered them “a lot” or “very much.”15
Genome-wide association studies have not identified a single determinant that explains racial and ethnic differences in susceptibility to AD.4 Instead, social determinants of health are thought to play a role in the difference in AD prevalence and severity across groups in the United States.16
Health Disparity Highlight
In an analysis of 20 US metropolitan cities, urban and inner-city residence was associated with approximately 1.7-fold increased odds of AD.4 Among pediatric patients with moderate to severe AD, Black children were more likely to be exposed to tobacco smoke17 and traffic-related air pollution.18 Low socioeconomic status and low income also have been associated with moderate16 and severe19 AD. At the same education level, Black individuals in the United States receive less income than their White counterparts and have markedly less wealth at equivalent incomes.20
In utero exposure to maternal stress is associated with AD.4 Increased IgE levels have been recorded in children who develop AD, with Black children having the highest IgE levels overall compared to other children.18
An analysis of medical records from an urban medical center in Baltimore, Maryland, from 2013 through 2018 showed that Black patients with AD were less likely to receive topical corticosteroids, topical calcineurin inhibitors, a topical phosphodiesterase 4 inhibitor, and a biologic compared to White patients with AD.21
Since the disproportionate burden experienced by patients with AD is not physiologic, it is imperative to address these systemic complexities and address the barriers impacting treatment availability to improve health outcomes for all patients living with AD.
- Kaufman BP, Guttman-Yassky E, Alexis AF. Atopic dermatitis in diverse racial and ethnic groups—variations in epidemiology, genetics, clinical presentation and treatment. Exp Dermatol. 2018;27:340-357.
- Lee HH, Patel KR, Singam V, et al. A systematic review and meta-analysis of the prevalence and phenotype of adult-onset atopic dermatitis. J Am Acad Dermatol. 2019;80:1526-1532.E7.
- Adawi W, Cornman H, Kambala A, et al. Diagnosing atopic dermatitis in skin of color. Dermatol Clin. 2023;41:417-429.
- Narla S, Silverberg JI. Current updates in the epidemiology and comorbidities of atopic dermatitis. Ann Allergy Asthma Immunol. 2025;135:511-520.
- Croce EA, Levy ML, Adamson AS, et al. Reframing racial and ethnic disparities in atopic dermatitis in Black and Latinx populations. J Allergy Clin Immunol. 2021;148:1104-1111.
- Kim Y, Blomberg M, Rifas-Shiman SL, et al. Racial/ethnic differences in incidence and persistence of childhood atopic dermatitis. J Invest Dermatol. 2019;139:827-834.
- Nomura T, Wu J, Kabashima K, et al. Endophenotypic variations of atopic dermatitis by age, race, and ethnicity. J Allergy Clin Immunol. 2020;8:1840-1852.
- McColl M, Boozalis E, Aguh C, et al. Pruritus in Black skin: unique molecular characteristics and clinical features. J Natl Med Assoc. 2021;114:30-38.
- Silverberg JI, Margolis DJ, Boguniewicz M, et al. Distribution of atopic dermatitis lesions in United States adults. J Eur Acad Dermatol Venereol. 2019;33:1341-1348.
- Summey BT, Bowen SE, Allen HB. Lichen planus-like atopic dermatitis: expanding the differential diagnosis of spongiotic dermatitis. J Cutan Pathol. 2008;35:311-314.
- Odhiambo JA, Williams HC, Clayton TO, et al; ISAAC Phase Three Study Group. Global variations in prevalence of eczema symptoms in children from ISAAC Phase Three. J Allergy Clin Immunol. 2009;124:1251-1258.E23.
- Gallagher K, Halperin-Goldstein S, Paller AS. New treatments in atopic dermatitis update. Ann Allergy Asthma Immunol. 2025;135:498-510.E10.
- Shaw ML. FDA expands roflumilast use for atopic dermatitis to children aged 2 to 5 years. Am J Managed Care. October 6, 2025. Accessed April 30, 2026. https://www.ajmc.com/view/fda-expands -roflumilast-use-for-atopic-dermatitis-to-children-aged-2-to-5-years
- Eichenfield LF, Stein Gold LF, Simpson EL, et al. Efficacy and safety of ruxolitinib cream in children aged 2 to 11 years with atopic dermatitis: results from TRuE-AD3, a phase 3, randomized double-blind study. J Am Acad of Dermatol. 2025;93:689-698.
- Heath CR, Dosono B, Shi VY, et al. Variability in skin tone changes by race and ethnicity among US adults with atopic dermatitis. Presented at: Skin of Color Update 2024, September 13-15, 2024, New York, NY.
- Tackett KJ, Jenkins F, Morrell DS, et al. Structural racism and its influence on the severity of atopic dermatitis in African American children. Pediatr Dermatol. 2020;37:142-146.
- Narla S, Silverberg JI. The role of environmental exposures in atopic dermatitis. Curr Allergy Asthma Rep. 2020;20:74.
- Bauer SJ, Spoer BR, Ehrman R, et al. A systematic review of historic neighborhood redlining and contemporary health outcomes. Public Health. 2025;238:181-187.
- Chung J, Simpson EL. The socioeconomics of atopic dermatitis. Ann Allergy Asthma Immunol. 2019;122:360-366.
- Martinez A, de la Rosa R, Mujahid M, et al. Structural racism and its pathways to asthma and atopic dermatitis. J Allergy Clin Immunol. 2021;148:1112-1120.
- Bell MA, Whang KA, Thomas J, et al. Racial and ethnic disparities in access to emerging and frontline therapies in common dermatological conditions: a cross-sectional study. J Natl Med Assoc. 2020;112:650-653.
- Kaufman BP, Guttman-Yassky E, Alexis AF. Atopic dermatitis in diverse racial and ethnic groups—variations in epidemiology, genetics, clinical presentation and treatment. Exp Dermatol. 2018;27:340-357.
- Lee HH, Patel KR, Singam V, et al. A systematic review and meta-analysis of the prevalence and phenotype of adult-onset atopic dermatitis. J Am Acad Dermatol. 2019;80:1526-1532.E7.
- Adawi W, Cornman H, Kambala A, et al. Diagnosing atopic dermatitis in skin of color. Dermatol Clin. 2023;41:417-429.
- Narla S, Silverberg JI. Current updates in the epidemiology and comorbidities of atopic dermatitis. Ann Allergy Asthma Immunol. 2025;135:511-520.
- Croce EA, Levy ML, Adamson AS, et al. Reframing racial and ethnic disparities in atopic dermatitis in Black and Latinx populations. J Allergy Clin Immunol. 2021;148:1104-1111.
- Kim Y, Blomberg M, Rifas-Shiman SL, et al. Racial/ethnic differences in incidence and persistence of childhood atopic dermatitis. J Invest Dermatol. 2019;139:827-834.
- Nomura T, Wu J, Kabashima K, et al. Endophenotypic variations of atopic dermatitis by age, race, and ethnicity. J Allergy Clin Immunol. 2020;8:1840-1852.
- McColl M, Boozalis E, Aguh C, et al. Pruritus in Black skin: unique molecular characteristics and clinical features. J Natl Med Assoc. 2021;114:30-38.
- Silverberg JI, Margolis DJ, Boguniewicz M, et al. Distribution of atopic dermatitis lesions in United States adults. J Eur Acad Dermatol Venereol. 2019;33:1341-1348.
- Summey BT, Bowen SE, Allen HB. Lichen planus-like atopic dermatitis: expanding the differential diagnosis of spongiotic dermatitis. J Cutan Pathol. 2008;35:311-314.
- Odhiambo JA, Williams HC, Clayton TO, et al; ISAAC Phase Three Study Group. Global variations in prevalence of eczema symptoms in children from ISAAC Phase Three. J Allergy Clin Immunol. 2009;124:1251-1258.E23.
- Gallagher K, Halperin-Goldstein S, Paller AS. New treatments in atopic dermatitis update. Ann Allergy Asthma Immunol. 2025;135:498-510.E10.
- Shaw ML. FDA expands roflumilast use for atopic dermatitis to children aged 2 to 5 years. Am J Managed Care. October 6, 2025. Accessed April 30, 2026. https://www.ajmc.com/view/fda-expands -roflumilast-use-for-atopic-dermatitis-to-children-aged-2-to-5-years
- Eichenfield LF, Stein Gold LF, Simpson EL, et al. Efficacy and safety of ruxolitinib cream in children aged 2 to 11 years with atopic dermatitis: results from TRuE-AD3, a phase 3, randomized double-blind study. J Am Acad of Dermatol. 2025;93:689-698.
- Heath CR, Dosono B, Shi VY, et al. Variability in skin tone changes by race and ethnicity among US adults with atopic dermatitis. Presented at: Skin of Color Update 2024, September 13-15, 2024, New York, NY.
- Tackett KJ, Jenkins F, Morrell DS, et al. Structural racism and its influence on the severity of atopic dermatitis in African American children. Pediatr Dermatol. 2020;37:142-146.
- Narla S, Silverberg JI. The role of environmental exposures in atopic dermatitis. Curr Allergy Asthma Rep. 2020;20:74.
- Bauer SJ, Spoer BR, Ehrman R, et al. A systematic review of historic neighborhood redlining and contemporary health outcomes. Public Health. 2025;238:181-187.
- Chung J, Simpson EL. The socioeconomics of atopic dermatitis. Ann Allergy Asthma Immunol. 2019;122:360-366.
- Martinez A, de la Rosa R, Mujahid M, et al. Structural racism and its pathways to asthma and atopic dermatitis. J Allergy Clin Immunol. 2021;148:1112-1120.
- Bell MA, Whang KA, Thomas J, et al. Racial and ethnic disparities in access to emerging and frontline therapies in common dermatological conditions: a cross-sectional study. J Natl Med Assoc. 2020;112:650-653.
Atopic Dermatitis: New Insights and Expanded Treatment Options
Atopic Dermatitis: New Insights and Expanded Treatment Options

Medical Decision-Making in Evaluation and Management Coding: Practical Applications and Key Clarifications
Medical Decision-Making in Evaluation and Management Coding: Practical Applications and Key Clarifications
The new coding guidelines for evaluation and management services have simplified coding by focusing on medical decision-making (MDM), but practicing clinicians often have questions about how to apply the rules. This article will focus on common mistakes and nuances clarified in communications from the American Medical Association. As before, the highest level of service in 2 of 3 categories—complexity, data, and risk—determine the level of service. Only medically necessary services should be reported, and all reported codes should accurately reflect the services provided.
Key Clarifications to MDM Criteria
Important clarifications that came after the initial distribution of the new coding rules include the following:
- An established problem not at treatment target requiring ongoing MDM counts as moderate complexity in column 1.
- Under the category of risk, prescription drug therapy includes discussion of risks, benefits, and alternatives with a decision to start, stop, or continue a prescription medication; this differs from a simple refill that does not require evaluation, discussion, and shared decision-making.
- Social determinants of health that are medically appropriate to address during the visit are considered moderate under the category of risk. These include issues that directly affect patient management (eg, transportation access, medication affordability, cultural norms, restrictions) and other factors influencing health and well-being (eg, income, education, occupation, environmental change, unemployment, working conditions, social support) when they impact the patient’s condition and inform treatment decisions.
- Independent interpretation of a laboratory test counts as moderate under the category of data; an example would be a biopsy reported as “consistent with lupus erythematosus” in a patient with a heliotrope rash and shawl sign, which may require clinicopathologic correlation and reinterpretation as “diagnostic of dermatomyositis.”
- The decision to perform a 0- or 10-day global procedure on the same date of service as the visit is already bundled in payment for the procedure and should not be reported as a separate service; however, if scheduled for a future date of service, it counts as low under the risk category if the patient has no unique risk factors or moderate if the patient does have unique risk factors that weigh into MDM. In contrast, the decision to perform a 90-day global procedure is reportable even on the same date of service (with modifier 57) and counts as moderate risk without unique risk factors and high with such factors.
Application of MDM Coding in Common Dermatology Encounters
Let’s look at some common scenarios and how they should be coded.
A patient presents with a new lesion of concern. On physical examination, it is a stuck-on keratotic papule with no inflammation, and you reassure them that it is merely a benign seborrheic keratosis. This encounter would be coded as straightforward MDM (level 2, new or established), reflecting the evaluation of a single minor problem.
A patient returns with localized eczema and is doing very well with triamcinolone cream applied as needed, and you simply refill the prescription. This encounter represents low-level MDM (level 3, established), reflecting a single stable problem managed with a simple prescription refill.
A patient presents with psoriasis that has had some response to topical therapy but is clearly not at target, and the patient now reports axial joint stiffness that is much worse in the morning and takes more than 30 minutes to resolve. You discuss risks, benefits, and alternatives; note that the patient already had recent screening for tuberculosis and other infectious diseases; and prescribe a T-helper 17 biologic because of the axial arthritis. This encounter represents moderate-level MDM (level 4, established), reflecting both a problem not at target and a new problem of uncertain prognosis under complexity, as well as shared decision-making to initiate prescription drug therapy under risk. Although review or ordering of 3 laboratory tests would also meet moderate criteria under data, only 2 of the 3 domains are required to establish the level of service.
A patient presents with a severe flare of eczema that requires treatment with cyclosporine. This encounter represents high-level MDM (level 5, established), reflecting a severe exacerbation of an existing condition requiring a high-risk medication with at least quarterly laboratory monitoring and uncertainty regarding long-term therapy needs.
Application of Moderate and High MDM in Dermatology
Many dermatology patients present with multiple problems, and the visit often falls into the moderate category for column 1 (complexity) of MDM (level 4, new or established). Under complexity, moderate could be 2 stable problems, one worsening problem, one new problem of uncertain prognosis, or one problem improved but not at target. Remember that moderate MDM also must be established in a second category, such as risk. Under the risk category, moderate could include prescription drug therapy, addressing a relevant social determinant of health, the decision to perform a 0- or 10-day global procedure not performed on the same date of service with unique patient risk factors, or the decision to perform a 90-day global procedure in a patient with no unique risk factors.
Don’t forget the data category, as it often is relevant to determining the correct level of service. Moderate under the data category includes review or ordering of 3 laboratory tests (a complete metabolic panel is a single laboratory test, and a complete blood count is a single laboratory test), independent interpretation of a laboratory test, or a phone call to another provider caring for the patient with a medically necessary discussion of management (eg, severe eczema in a patient on a calcium channel blocker—you call the primary care physician advising that calcium-channel blockers are the most common cause of eczematous drug eruption and advise a change in therapy). If 2 of the above categories were necessary (eg, order 3 laboratory tests and call the primary care physician), that would count as high MDM under the data category. Remember, 2 categories are required to establish the level of service.
Other examples of high MDM (level 5, new or established) include a new diagnosis with major risk to life or limb plus one of the following: high-risk medication requiring at least quarterly drug monitoring, the decision to perform a 90-day global surgery with documented additional patient risk factors, or the decision to admit to the hospital (eg, new invasive melanoma with excision and decision to perform adjacent tissue transfer in a patient who takes aspirin).
Final Thoughts
Physicians should perform medically necessary services that are in the best interest of their patients. Current coding rules focus on the complexity, risk, and data associated with MDM.
The new coding guidelines for evaluation and management services have simplified coding by focusing on medical decision-making (MDM), but practicing clinicians often have questions about how to apply the rules. This article will focus on common mistakes and nuances clarified in communications from the American Medical Association. As before, the highest level of service in 2 of 3 categories—complexity, data, and risk—determine the level of service. Only medically necessary services should be reported, and all reported codes should accurately reflect the services provided.
Key Clarifications to MDM Criteria
Important clarifications that came after the initial distribution of the new coding rules include the following:
- An established problem not at treatment target requiring ongoing MDM counts as moderate complexity in column 1.
- Under the category of risk, prescription drug therapy includes discussion of risks, benefits, and alternatives with a decision to start, stop, or continue a prescription medication; this differs from a simple refill that does not require evaluation, discussion, and shared decision-making.
- Social determinants of health that are medically appropriate to address during the visit are considered moderate under the category of risk. These include issues that directly affect patient management (eg, transportation access, medication affordability, cultural norms, restrictions) and other factors influencing health and well-being (eg, income, education, occupation, environmental change, unemployment, working conditions, social support) when they impact the patient’s condition and inform treatment decisions.
- Independent interpretation of a laboratory test counts as moderate under the category of data; an example would be a biopsy reported as “consistent with lupus erythematosus” in a patient with a heliotrope rash and shawl sign, which may require clinicopathologic correlation and reinterpretation as “diagnostic of dermatomyositis.”
- The decision to perform a 0- or 10-day global procedure on the same date of service as the visit is already bundled in payment for the procedure and should not be reported as a separate service; however, if scheduled for a future date of service, it counts as low under the risk category if the patient has no unique risk factors or moderate if the patient does have unique risk factors that weigh into MDM. In contrast, the decision to perform a 90-day global procedure is reportable even on the same date of service (with modifier 57) and counts as moderate risk without unique risk factors and high with such factors.
Application of MDM Coding in Common Dermatology Encounters
Let’s look at some common scenarios and how they should be coded.
A patient presents with a new lesion of concern. On physical examination, it is a stuck-on keratotic papule with no inflammation, and you reassure them that it is merely a benign seborrheic keratosis. This encounter would be coded as straightforward MDM (level 2, new or established), reflecting the evaluation of a single minor problem.
A patient returns with localized eczema and is doing very well with triamcinolone cream applied as needed, and you simply refill the prescription. This encounter represents low-level MDM (level 3, established), reflecting a single stable problem managed with a simple prescription refill.
A patient presents with psoriasis that has had some response to topical therapy but is clearly not at target, and the patient now reports axial joint stiffness that is much worse in the morning and takes more than 30 minutes to resolve. You discuss risks, benefits, and alternatives; note that the patient already had recent screening for tuberculosis and other infectious diseases; and prescribe a T-helper 17 biologic because of the axial arthritis. This encounter represents moderate-level MDM (level 4, established), reflecting both a problem not at target and a new problem of uncertain prognosis under complexity, as well as shared decision-making to initiate prescription drug therapy under risk. Although review or ordering of 3 laboratory tests would also meet moderate criteria under data, only 2 of the 3 domains are required to establish the level of service.
A patient presents with a severe flare of eczema that requires treatment with cyclosporine. This encounter represents high-level MDM (level 5, established), reflecting a severe exacerbation of an existing condition requiring a high-risk medication with at least quarterly laboratory monitoring and uncertainty regarding long-term therapy needs.
Application of Moderate and High MDM in Dermatology
Many dermatology patients present with multiple problems, and the visit often falls into the moderate category for column 1 (complexity) of MDM (level 4, new or established). Under complexity, moderate could be 2 stable problems, one worsening problem, one new problem of uncertain prognosis, or one problem improved but not at target. Remember that moderate MDM also must be established in a second category, such as risk. Under the risk category, moderate could include prescription drug therapy, addressing a relevant social determinant of health, the decision to perform a 0- or 10-day global procedure not performed on the same date of service with unique patient risk factors, or the decision to perform a 90-day global procedure in a patient with no unique risk factors.
Don’t forget the data category, as it often is relevant to determining the correct level of service. Moderate under the data category includes review or ordering of 3 laboratory tests (a complete metabolic panel is a single laboratory test, and a complete blood count is a single laboratory test), independent interpretation of a laboratory test, or a phone call to another provider caring for the patient with a medically necessary discussion of management (eg, severe eczema in a patient on a calcium channel blocker—you call the primary care physician advising that calcium-channel blockers are the most common cause of eczematous drug eruption and advise a change in therapy). If 2 of the above categories were necessary (eg, order 3 laboratory tests and call the primary care physician), that would count as high MDM under the data category. Remember, 2 categories are required to establish the level of service.
Other examples of high MDM (level 5, new or established) include a new diagnosis with major risk to life or limb plus one of the following: high-risk medication requiring at least quarterly drug monitoring, the decision to perform a 90-day global surgery with documented additional patient risk factors, or the decision to admit to the hospital (eg, new invasive melanoma with excision and decision to perform adjacent tissue transfer in a patient who takes aspirin).
Final Thoughts
Physicians should perform medically necessary services that are in the best interest of their patients. Current coding rules focus on the complexity, risk, and data associated with MDM.
The new coding guidelines for evaluation and management services have simplified coding by focusing on medical decision-making (MDM), but practicing clinicians often have questions about how to apply the rules. This article will focus on common mistakes and nuances clarified in communications from the American Medical Association. As before, the highest level of service in 2 of 3 categories—complexity, data, and risk—determine the level of service. Only medically necessary services should be reported, and all reported codes should accurately reflect the services provided.
Key Clarifications to MDM Criteria
Important clarifications that came after the initial distribution of the new coding rules include the following:
- An established problem not at treatment target requiring ongoing MDM counts as moderate complexity in column 1.
- Under the category of risk, prescription drug therapy includes discussion of risks, benefits, and alternatives with a decision to start, stop, or continue a prescription medication; this differs from a simple refill that does not require evaluation, discussion, and shared decision-making.
- Social determinants of health that are medically appropriate to address during the visit are considered moderate under the category of risk. These include issues that directly affect patient management (eg, transportation access, medication affordability, cultural norms, restrictions) and other factors influencing health and well-being (eg, income, education, occupation, environmental change, unemployment, working conditions, social support) when they impact the patient’s condition and inform treatment decisions.
- Independent interpretation of a laboratory test counts as moderate under the category of data; an example would be a biopsy reported as “consistent with lupus erythematosus” in a patient with a heliotrope rash and shawl sign, which may require clinicopathologic correlation and reinterpretation as “diagnostic of dermatomyositis.”
- The decision to perform a 0- or 10-day global procedure on the same date of service as the visit is already bundled in payment for the procedure and should not be reported as a separate service; however, if scheduled for a future date of service, it counts as low under the risk category if the patient has no unique risk factors or moderate if the patient does have unique risk factors that weigh into MDM. In contrast, the decision to perform a 90-day global procedure is reportable even on the same date of service (with modifier 57) and counts as moderate risk without unique risk factors and high with such factors.
Application of MDM Coding in Common Dermatology Encounters
Let’s look at some common scenarios and how they should be coded.
A patient presents with a new lesion of concern. On physical examination, it is a stuck-on keratotic papule with no inflammation, and you reassure them that it is merely a benign seborrheic keratosis. This encounter would be coded as straightforward MDM (level 2, new or established), reflecting the evaluation of a single minor problem.
A patient returns with localized eczema and is doing very well with triamcinolone cream applied as needed, and you simply refill the prescription. This encounter represents low-level MDM (level 3, established), reflecting a single stable problem managed with a simple prescription refill.
A patient presents with psoriasis that has had some response to topical therapy but is clearly not at target, and the patient now reports axial joint stiffness that is much worse in the morning and takes more than 30 minutes to resolve. You discuss risks, benefits, and alternatives; note that the patient already had recent screening for tuberculosis and other infectious diseases; and prescribe a T-helper 17 biologic because of the axial arthritis. This encounter represents moderate-level MDM (level 4, established), reflecting both a problem not at target and a new problem of uncertain prognosis under complexity, as well as shared decision-making to initiate prescription drug therapy under risk. Although review or ordering of 3 laboratory tests would also meet moderate criteria under data, only 2 of the 3 domains are required to establish the level of service.
A patient presents with a severe flare of eczema that requires treatment with cyclosporine. This encounter represents high-level MDM (level 5, established), reflecting a severe exacerbation of an existing condition requiring a high-risk medication with at least quarterly laboratory monitoring and uncertainty regarding long-term therapy needs.
Application of Moderate and High MDM in Dermatology
Many dermatology patients present with multiple problems, and the visit often falls into the moderate category for column 1 (complexity) of MDM (level 4, new or established). Under complexity, moderate could be 2 stable problems, one worsening problem, one new problem of uncertain prognosis, or one problem improved but not at target. Remember that moderate MDM also must be established in a second category, such as risk. Under the risk category, moderate could include prescription drug therapy, addressing a relevant social determinant of health, the decision to perform a 0- or 10-day global procedure not performed on the same date of service with unique patient risk factors, or the decision to perform a 90-day global procedure in a patient with no unique risk factors.
Don’t forget the data category, as it often is relevant to determining the correct level of service. Moderate under the data category includes review or ordering of 3 laboratory tests (a complete metabolic panel is a single laboratory test, and a complete blood count is a single laboratory test), independent interpretation of a laboratory test, or a phone call to another provider caring for the patient with a medically necessary discussion of management (eg, severe eczema in a patient on a calcium channel blocker—you call the primary care physician advising that calcium-channel blockers are the most common cause of eczematous drug eruption and advise a change in therapy). If 2 of the above categories were necessary (eg, order 3 laboratory tests and call the primary care physician), that would count as high MDM under the data category. Remember, 2 categories are required to establish the level of service.
Other examples of high MDM (level 5, new or established) include a new diagnosis with major risk to life or limb plus one of the following: high-risk medication requiring at least quarterly drug monitoring, the decision to perform a 90-day global surgery with documented additional patient risk factors, or the decision to admit to the hospital (eg, new invasive melanoma with excision and decision to perform adjacent tissue transfer in a patient who takes aspirin).
Final Thoughts
Physicians should perform medically necessary services that are in the best interest of their patients. Current coding rules focus on the complexity, risk, and data associated with MDM.
Medical Decision-Making in Evaluation and Management Coding: Practical Applications and Key Clarifications
Medical Decision-Making in Evaluation and Management Coding: Practical Applications and Key Clarifications
PRACTICE POINTS
- Evaluation and management coding is now based on medical decision-making (MDM), requiring 2 of 3 categories (complexity, data, risk) and strict adherence to medical necessity.
- Moderate MDM includes problems not at target, shared decision-making for prescription therapy (not simple refills), relevant social determinants of health, and independent test interpretation.
- Common errors include misclassifying refills, overlooking the data category, and improperly reporting procedural decisions, especially same-day minor procedures.

Limitations of Fitzpatrick Skin Type as a Proxy for Skin Color and Race
Limitations of Fitzpatrick Skin Type as a Proxy for Skin Color and Race
Recognizing inflammation in darker skin tones has important implications for diagnosis and management of skin disease, particularly in patients with skin of color.1 In this context, classification systems commonly are used—both in research and clinical practice—to standardize descriptions of skin tone across diverse populations. Fitzpatrick skin type (FST) originally was developed to classify cutaneous response to UV radiation exposure and remains one of the most widely used frameworks in dermatology.2 However, FST often is used beyond its intended purpose as a proxy for differentiating skin color and race.3,4 This mismatch risks obscuring clinically meaningful differences and limiting the accuracy of dermatologic research. Herein, we review the intended use of FST, its limitations in representing skin color and race, and considerations for more accurate characterization of skin pigmentation in clinical practice and research.
Origins and Intended Use of the FST Scale
Fitzpatrick skin type was developed by Thomas B. Fitzpatrick in the 1970s to guide UVA dosing for psoralen plus UVA therapy in patients with psoriasis.5,6 The scale was intended to estimate an individual’s erythematous and pigmentary response to UV exposure.6,7 Early iterations of FST largely were based on lighter skin types, reflecting its initial use in predominantly White populations, which limited representation of the full spectrum of skin tone diversity.5
Clinical, Educational, and Research Limitations of FST
Fitzpatrick skin type now is widely, albeit inaccurately, used in both research and clinical practice as a proxy for skin color and race,7,8 which reflects its ease of use and the lack of standardized alternatives; however, FST does not adequately capture variability in baseline skin pigmentation, undertone, or inflammatory response. These limitations are especially pronounced in phototypes IV to VI, which encompass highly heterogeneous populations. As a result, grouping patients by FST alone to describe skin color and race may obscure important differences and limit meaningful interpretation of clinical and research findings.
Clinically, recognition of dermatologic conditions such as erythema may be more challenging in darker skin tones, in which classic visual cues are less apparent.1,7 Relying on FST to stratify skin color may further compound diagnostic uncertainty by oversimplifying the cutaneous presentation. In addition, treatment decisions, including laser settings and assessment of pigmentary risk, often are guided by FST despite within-group variability.7 Further, educational frameworks that rely heavily on FST may inadequately prepare clinicians to recognize disease across diverse skin tones, contributing to delayed diagnosis and disparities in care in populations with skin of color.
The implications also extend to dermatologic research. Fitzpatrick skin type frequently is used to assess study populations; however, its limited ability to reflect true variation in pigmentation and ethnicity introduces misclassification bias.3,7 The broad FST scale may group heterogeneous populations, obscuring differences in treatment response. As a result, studies relying on FST to represent skin color or race may have reduced generalizability across diverse populations. Importantly, these limitations are not merely conceptual but may contribute to measurable disparities in dermatologic diagnosis and outcomes.
Rethinking Skin Classification Frameworks
Despite these shortcomings, FST remains deeply embedded in dermatology. Its decades-long use has led to widespread familiarity and integration into clinical guidelines, education, and research. At the same time, the absence of a universally accepted alternative has reinforced the continued use of FST as a proxy for skin color and race.
Alternative strategies for characterizing skin pigmentation include objective measures such as spectrophotometry and melanin index assessment.9
Although these approaches may provide more precise quantification of pigmentation, their use may be limited by the need for specialized equipment and reduced feasibility in routine clinical settings. Other proposed approaches incorporate multidimensional factors such as pigmentation, photoreactivity, and genetic ancestry.4 While these techniques represent important advances, none has achieved widespread adoption yet, and each presents challenges related to feasibility and standardization.
In the absence of a single ideal system, a more nuanced approach is needed. Fitzpatrick skin type should be used in the context for which it was designed: estimating UV response. Incorporating additional descriptors, including self-identified race and ethnicity, alongside more detailed assessments of pigmentation may improve the accuracy and relevance of both clinical evaluation and research. Combining FST with more precise and inclusive frameworks represents a pragmatic step toward better reflecting patient diversity.
- Taylor SC. Recognizing erythema in skin of color. J Am Acad Dermatol.
- Fitzpatrick TB. The validity and practicality of sun-reactive skin types I through VI. Arch Dermatol. 1988;124:869-871. doi:10.1001 /archderm.124.6.869
- Eilers S, Bach DQ, Gaber R, et al. Accuracy of self-reported Fitzpatrick skin phototype classification in US Hispanic and Latino populations. JAMA Dermatol. 2013;149:797-803. doi:10.1001 /jamadermatol.2013.4091
- Del Bino S, Bernerd F. Variations in skin colour and the biological consequences of ultraviolet radiation exposure. Br J Dermatol. 2013;169(S3):33-40. doi:10.1111/bjd.12529
- Goon P, Banfield C, Bello O, et al. Skin cancers in skin types IV–VI: does the Fitzpatrick scale give a false sense of security? Clin Exp Dermatol. 2022;47:1112-1117. doi:10.1002/ski2.40
- Fitzpatrick TB. Soleil et peau. J Med Asthet. 1975;2:33-34.
- Ware OR, Dawson JE, Shinohara MM, et al. Racial limitations of Fitzpatrick skin type. Cutis. 2020;105:77-80.
- Lester JC, Taylor SC, Chren MM. Under-representation of skin of colour in dermatology images: not just an educational issue. Br J Dermatol. 2019;180:1521-1522. doi:10.1111/bjd.17608
- Fullerton A, Fischer T, Lahti A, et al. Guidelines for measurement of skin colour and erythema. a report from the Standardization Group of the European Society of Contact Dermatitis. Contact Dermatitis. 1996;35:1-10. doi:10.1111/j.1600-0536.1996.tb02242.x
Recognizing inflammation in darker skin tones has important implications for diagnosis and management of skin disease, particularly in patients with skin of color.1 In this context, classification systems commonly are used—both in research and clinical practice—to standardize descriptions of skin tone across diverse populations. Fitzpatrick skin type (FST) originally was developed to classify cutaneous response to UV radiation exposure and remains one of the most widely used frameworks in dermatology.2 However, FST often is used beyond its intended purpose as a proxy for differentiating skin color and race.3,4 This mismatch risks obscuring clinically meaningful differences and limiting the accuracy of dermatologic research. Herein, we review the intended use of FST, its limitations in representing skin color and race, and considerations for more accurate characterization of skin pigmentation in clinical practice and research.
Origins and Intended Use of the FST Scale
Fitzpatrick skin type was developed by Thomas B. Fitzpatrick in the 1970s to guide UVA dosing for psoralen plus UVA therapy in patients with psoriasis.5,6 The scale was intended to estimate an individual’s erythematous and pigmentary response to UV exposure.6,7 Early iterations of FST largely were based on lighter skin types, reflecting its initial use in predominantly White populations, which limited representation of the full spectrum of skin tone diversity.5
Clinical, Educational, and Research Limitations of FST
Fitzpatrick skin type now is widely, albeit inaccurately, used in both research and clinical practice as a proxy for skin color and race,7,8 which reflects its ease of use and the lack of standardized alternatives; however, FST does not adequately capture variability in baseline skin pigmentation, undertone, or inflammatory response. These limitations are especially pronounced in phototypes IV to VI, which encompass highly heterogeneous populations. As a result, grouping patients by FST alone to describe skin color and race may obscure important differences and limit meaningful interpretation of clinical and research findings.
Clinically, recognition of dermatologic conditions such as erythema may be more challenging in darker skin tones, in which classic visual cues are less apparent.1,7 Relying on FST to stratify skin color may further compound diagnostic uncertainty by oversimplifying the cutaneous presentation. In addition, treatment decisions, including laser settings and assessment of pigmentary risk, often are guided by FST despite within-group variability.7 Further, educational frameworks that rely heavily on FST may inadequately prepare clinicians to recognize disease across diverse skin tones, contributing to delayed diagnosis and disparities in care in populations with skin of color.
The implications also extend to dermatologic research. Fitzpatrick skin type frequently is used to assess study populations; however, its limited ability to reflect true variation in pigmentation and ethnicity introduces misclassification bias.3,7 The broad FST scale may group heterogeneous populations, obscuring differences in treatment response. As a result, studies relying on FST to represent skin color or race may have reduced generalizability across diverse populations. Importantly, these limitations are not merely conceptual but may contribute to measurable disparities in dermatologic diagnosis and outcomes.
Rethinking Skin Classification Frameworks
Despite these shortcomings, FST remains deeply embedded in dermatology. Its decades-long use has led to widespread familiarity and integration into clinical guidelines, education, and research. At the same time, the absence of a universally accepted alternative has reinforced the continued use of FST as a proxy for skin color and race.
Alternative strategies for characterizing skin pigmentation include objective measures such as spectrophotometry and melanin index assessment.9
Although these approaches may provide more precise quantification of pigmentation, their use may be limited by the need for specialized equipment and reduced feasibility in routine clinical settings. Other proposed approaches incorporate multidimensional factors such as pigmentation, photoreactivity, and genetic ancestry.4 While these techniques represent important advances, none has achieved widespread adoption yet, and each presents challenges related to feasibility and standardization.
In the absence of a single ideal system, a more nuanced approach is needed. Fitzpatrick skin type should be used in the context for which it was designed: estimating UV response. Incorporating additional descriptors, including self-identified race and ethnicity, alongside more detailed assessments of pigmentation may improve the accuracy and relevance of both clinical evaluation and research. Combining FST with more precise and inclusive frameworks represents a pragmatic step toward better reflecting patient diversity.
Recognizing inflammation in darker skin tones has important implications for diagnosis and management of skin disease, particularly in patients with skin of color.1 In this context, classification systems commonly are used—both in research and clinical practice—to standardize descriptions of skin tone across diverse populations. Fitzpatrick skin type (FST) originally was developed to classify cutaneous response to UV radiation exposure and remains one of the most widely used frameworks in dermatology.2 However, FST often is used beyond its intended purpose as a proxy for differentiating skin color and race.3,4 This mismatch risks obscuring clinically meaningful differences and limiting the accuracy of dermatologic research. Herein, we review the intended use of FST, its limitations in representing skin color and race, and considerations for more accurate characterization of skin pigmentation in clinical practice and research.
Origins and Intended Use of the FST Scale
Fitzpatrick skin type was developed by Thomas B. Fitzpatrick in the 1970s to guide UVA dosing for psoralen plus UVA therapy in patients with psoriasis.5,6 The scale was intended to estimate an individual’s erythematous and pigmentary response to UV exposure.6,7 Early iterations of FST largely were based on lighter skin types, reflecting its initial use in predominantly White populations, which limited representation of the full spectrum of skin tone diversity.5
Clinical, Educational, and Research Limitations of FST
Fitzpatrick skin type now is widely, albeit inaccurately, used in both research and clinical practice as a proxy for skin color and race,7,8 which reflects its ease of use and the lack of standardized alternatives; however, FST does not adequately capture variability in baseline skin pigmentation, undertone, or inflammatory response. These limitations are especially pronounced in phototypes IV to VI, which encompass highly heterogeneous populations. As a result, grouping patients by FST alone to describe skin color and race may obscure important differences and limit meaningful interpretation of clinical and research findings.
Clinically, recognition of dermatologic conditions such as erythema may be more challenging in darker skin tones, in which classic visual cues are less apparent.1,7 Relying on FST to stratify skin color may further compound diagnostic uncertainty by oversimplifying the cutaneous presentation. In addition, treatment decisions, including laser settings and assessment of pigmentary risk, often are guided by FST despite within-group variability.7 Further, educational frameworks that rely heavily on FST may inadequately prepare clinicians to recognize disease across diverse skin tones, contributing to delayed diagnosis and disparities in care in populations with skin of color.
The implications also extend to dermatologic research. Fitzpatrick skin type frequently is used to assess study populations; however, its limited ability to reflect true variation in pigmentation and ethnicity introduces misclassification bias.3,7 The broad FST scale may group heterogeneous populations, obscuring differences in treatment response. As a result, studies relying on FST to represent skin color or race may have reduced generalizability across diverse populations. Importantly, these limitations are not merely conceptual but may contribute to measurable disparities in dermatologic diagnosis and outcomes.
Rethinking Skin Classification Frameworks
Despite these shortcomings, FST remains deeply embedded in dermatology. Its decades-long use has led to widespread familiarity and integration into clinical guidelines, education, and research. At the same time, the absence of a universally accepted alternative has reinforced the continued use of FST as a proxy for skin color and race.
Alternative strategies for characterizing skin pigmentation include objective measures such as spectrophotometry and melanin index assessment.9
Although these approaches may provide more precise quantification of pigmentation, their use may be limited by the need for specialized equipment and reduced feasibility in routine clinical settings. Other proposed approaches incorporate multidimensional factors such as pigmentation, photoreactivity, and genetic ancestry.4 While these techniques represent important advances, none has achieved widespread adoption yet, and each presents challenges related to feasibility and standardization.
In the absence of a single ideal system, a more nuanced approach is needed. Fitzpatrick skin type should be used in the context for which it was designed: estimating UV response. Incorporating additional descriptors, including self-identified race and ethnicity, alongside more detailed assessments of pigmentation may improve the accuracy and relevance of both clinical evaluation and research. Combining FST with more precise and inclusive frameworks represents a pragmatic step toward better reflecting patient diversity.
- Taylor SC. Recognizing erythema in skin of color. J Am Acad Dermatol.
- Fitzpatrick TB. The validity and practicality of sun-reactive skin types I through VI. Arch Dermatol. 1988;124:869-871. doi:10.1001 /archderm.124.6.869
- Eilers S, Bach DQ, Gaber R, et al. Accuracy of self-reported Fitzpatrick skin phototype classification in US Hispanic and Latino populations. JAMA Dermatol. 2013;149:797-803. doi:10.1001 /jamadermatol.2013.4091
- Del Bino S, Bernerd F. Variations in skin colour and the biological consequences of ultraviolet radiation exposure. Br J Dermatol. 2013;169(S3):33-40. doi:10.1111/bjd.12529
- Goon P, Banfield C, Bello O, et al. Skin cancers in skin types IV–VI: does the Fitzpatrick scale give a false sense of security? Clin Exp Dermatol. 2022;47:1112-1117. doi:10.1002/ski2.40
- Fitzpatrick TB. Soleil et peau. J Med Asthet. 1975;2:33-34.
- Ware OR, Dawson JE, Shinohara MM, et al. Racial limitations of Fitzpatrick skin type. Cutis. 2020;105:77-80.
- Lester JC, Taylor SC, Chren MM. Under-representation of skin of colour in dermatology images: not just an educational issue. Br J Dermatol. 2019;180:1521-1522. doi:10.1111/bjd.17608
- Fullerton A, Fischer T, Lahti A, et al. Guidelines for measurement of skin colour and erythema. a report from the Standardization Group of the European Society of Contact Dermatitis. Contact Dermatitis. 1996;35:1-10. doi:10.1111/j.1600-0536.1996.tb02242.x
- Taylor SC. Recognizing erythema in skin of color. J Am Acad Dermatol.
- Fitzpatrick TB. The validity and practicality of sun-reactive skin types I through VI. Arch Dermatol. 1988;124:869-871. doi:10.1001 /archderm.124.6.869
- Eilers S, Bach DQ, Gaber R, et al. Accuracy of self-reported Fitzpatrick skin phototype classification in US Hispanic and Latino populations. JAMA Dermatol. 2013;149:797-803. doi:10.1001 /jamadermatol.2013.4091
- Del Bino S, Bernerd F. Variations in skin colour and the biological consequences of ultraviolet radiation exposure. Br J Dermatol. 2013;169(S3):33-40. doi:10.1111/bjd.12529
- Goon P, Banfield C, Bello O, et al. Skin cancers in skin types IV–VI: does the Fitzpatrick scale give a false sense of security? Clin Exp Dermatol. 2022;47:1112-1117. doi:10.1002/ski2.40
- Fitzpatrick TB. Soleil et peau. J Med Asthet. 1975;2:33-34.
- Ware OR, Dawson JE, Shinohara MM, et al. Racial limitations of Fitzpatrick skin type. Cutis. 2020;105:77-80.
- Lester JC, Taylor SC, Chren MM. Under-representation of skin of colour in dermatology images: not just an educational issue. Br J Dermatol. 2019;180:1521-1522. doi:10.1111/bjd.17608
- Fullerton A, Fischer T, Lahti A, et al. Guidelines for measurement of skin colour and erythema. a report from the Standardization Group of the European Society of Contact Dermatitis. Contact Dermatitis. 1996;35:1-10. doi:10.1111/j.1600-0536.1996.tb02242.x
Limitations of Fitzpatrick Skin Type as a Proxy for Skin Color and Race
Limitations of Fitzpatrick Skin Type as a Proxy for Skin Color and Race

Exophytic Papule on the Hand
Exophytic Papule on the Hand
THE DIAGNOSIS: Kaposi Sarcoma
Histopathology revealed a serum crust on the surface of the specimen, and the dermis contained compact collections of spindled cells with interspersed erythrocytes (Figure 1). Human herpesvirus 8–stained sections highlighted many lesional cell nuclei (Figure 2). A diagnosis of Kaposi sarcoma (KS) was made based on these findings. The patient expressed interest in surgical excision; however, he was lost to follow-up.
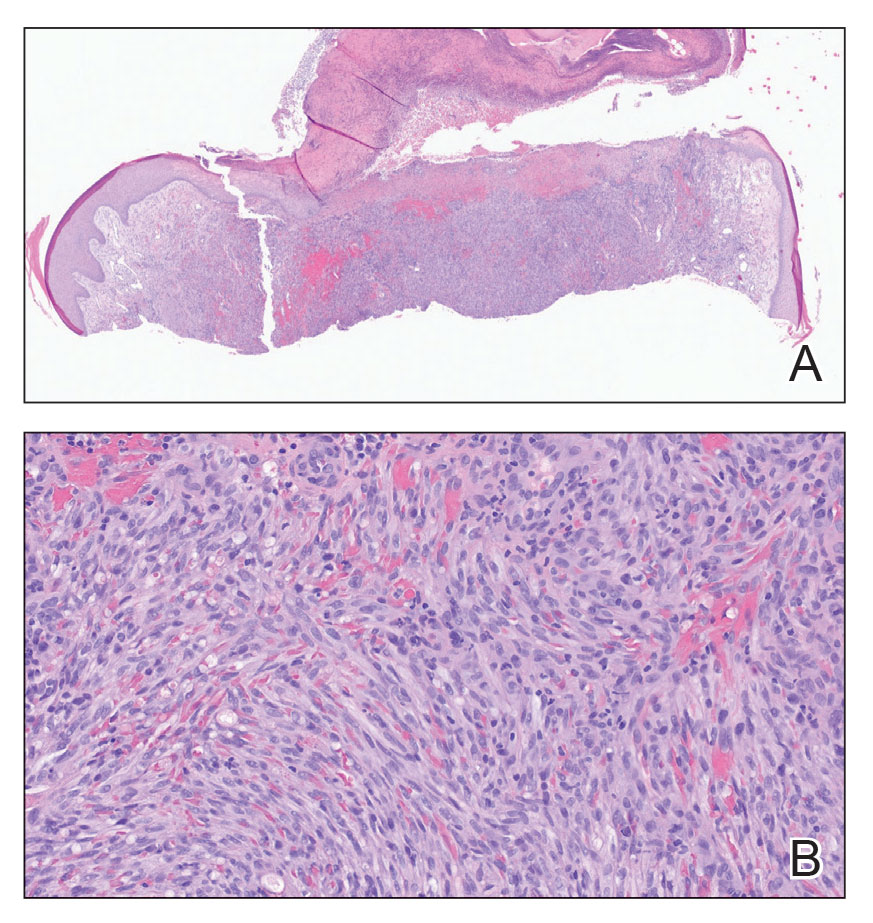
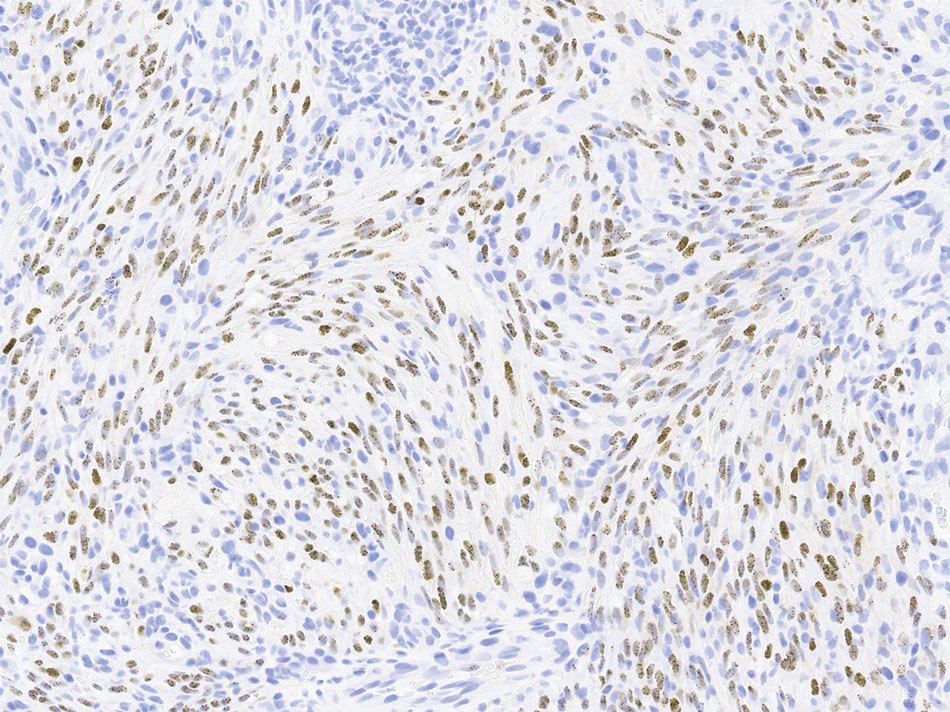
Kaposi sarcoma is an indolent, multifocal, angioproliferative tumor that predominantly affects mucocutaneous sites with less frequent involvement of visceral organs. Kaposi sarcoma is categorized into 4 subtypes: epidemic, iatrogenic, endemic, and classic. Human herpesvirus 8, primarily transmitted through saliva or sexual contact, plays a central role in the pathogenesis of KS, as it drives disease development across all subtypes. The virus causes proliferation of endothelial cells and the formation of angioproliferative lesions characteristic of KS.1
Prevalence is highest in the epidemic subtype, in which patients with advanced HIV and low CD4 T-cell counts may develop KS lesions. Although KS is associated most commonly with HIV, it also has been observed in men who have sex with men regardless of their HIV status.2 Patients undergoing immunosuppressive therapy also may not maintain immune tolerance to previously or newly acquired human herpesvirus 8, leading to the development of iatrogenic KS. This subtype particularly manifests in patients receiving therapy for autoimmune conditions or organ transplants and often only regresses if immunosuppressive therapy is withdrawn.3,4
The endemic and classic subtypes of KS may occur in patients without any known immunocompromise. Endemic KS demonstrates a predilection for pediatric populations in Africa and exhibits less pronounced sex disparity.5 In Uganda and Zimbabwe, endemic KS is the leading cancer in men and the second most frequently occurring cancer in women.6 In contrast, classic KS generally affects older men of Eastern European and Mediterranean descent or Ashkenazi Jewish ancestry. Patients with classic KS generally exhibit a less aggressive disease trajectory relative to other subtypes; however, these patients have a substantial risk for a secondary hematologic malignancy, which may already coexist at the time of diagnosis or emerge subsequently.1,7
Our patient, a native of Eastern Europe, was negative for HIV and was in a monogamous relationship with his wife; therefore, he was likely to have had the classic subtype of KS. As KS is a multifocal disease, lesions may independently emerge at different times and locations on the body. Our patient presented with a new lesion on the hand several years after excision of a similar lesion on the face. Lesions suspicious for KS include slow-growing, painless, red or violaceous patches, nodules, plaques, or patches on the extremities, most commonly manifesting on the feet and ankles. Our differential diagnosis included pyogenic granuloma, amelanotic melanoma, squamous cell carcinoma, and angiosarcoma.
The prognosis in patients with classic KS is favorable, as it often is limited to cutaneous sites and less commonly manifests on visceral organs. Nonetheless, pulmonary and gastrointestinal involvement manifesting as hemoptysis and rectal bleeding, respectively, can occur. This underscores the potential for more serious complications in instances with visceral involvement. Treatment focuses on managing symptoms and preventing growth and progression of individual lesions. Additionally, treatment strategies aim to improve cosmetic outcomes and address any underlying immunosuppression that may exacerbate the condition.8
For most patients, local therapies such as surgical excision, cryotherapy, laser therapy, or intralesional chemotherapy will remove or reduce individual lesions. Patients with widespread cutaneous or extracutaneous disease may require immunomodulatory agents such as interferon α or chemotherapeutic agents such as anthracyclines or paclitaxel.8
Our case highlights the importance of considering risk factors beyond HIV status when including KS as part of the differential diagnosis in patients with atypical vascular lesions. Early recognition enables timely evaluation of potential associated conditions and informs subsequent management decisions.
- Radu O, Pantanowitz L. Kaposi sarcoma. Arch Pathol Lab Med. 2013;137:289-294. doi:10.5858/arpa.2012-0101-RS
- Lanternier F, Lebbé C, Schartz N, et al. Kaposi’s sarcoma in HIV-negative men having sex with men. AIDS. 2008;22:1163-1168. doi:10.1097/QAD.0b013e3283031a8a
- Penn I. Kaposi’s sarcoma in transplant recipients. Transplantation. 1997;64:669-673. doi:10.1097/00007890-199709150-00001
- Gallo Marin B, Maymone MBC, El Rayess F, et al. Kaposi sarcoma associated with tofacitinib use in a patient with rheumatoid arthritis. R I Med J (2013). 2023;106:18-20.
- Bishop BN, Lynch DT. Kaposi sarcoma. StatPearls [Internet]. Updated June 5, 2023. Accessed May 15, 2026. https://www.ncbi.nlm .nih.gov/books/NBK534839/
- Dedicoat M, Newton R. Review of the distribution of Kaposi’s sarcoma-associated herpesvirus (KSHV) in Africa in relation to the incidence of Kaposi’s sarcoma. Br J Cancer. 2003;88:1-3. doi:10.1038 /sj.bjc.6600745
- Hiatt KM, Nelson AM, Lichy JH, et al. Classic Kaposi sarcoma in the United States over the last two decades: a clinicopathologic and molecular study of 438 non-HIV-related Kaposi sarcoma patients with comparison to HIV-related Kaposi sarcoma. Mod Pathol. 2008;21:572-582. doi:10.1038/modpathol.2008.15
- Ceccarelli M, Facciolà A, Taibi R, et al. The treatment of Kaposi’s sarcoma: present and future options, a review of the literature. Eur Rev Med Pharmacol Sci. 2019;23:7488-7497. doi:10.26355 /eurrev_201909_18860
THE DIAGNOSIS: Kaposi Sarcoma
Histopathology revealed a serum crust on the surface of the specimen, and the dermis contained compact collections of spindled cells with interspersed erythrocytes (Figure 1). Human herpesvirus 8–stained sections highlighted many lesional cell nuclei (Figure 2). A diagnosis of Kaposi sarcoma (KS) was made based on these findings. The patient expressed interest in surgical excision; however, he was lost to follow-up.
Kaposi sarcoma is an indolent, multifocal, angioproliferative tumor that predominantly affects mucocutaneous sites with less frequent involvement of visceral organs. Kaposi sarcoma is categorized into 4 subtypes: epidemic, iatrogenic, endemic, and classic. Human herpesvirus 8, primarily transmitted through saliva or sexual contact, plays a central role in the pathogenesis of KS, as it drives disease development across all subtypes. The virus causes proliferation of endothelial cells and the formation of angioproliferative lesions characteristic of KS.1
Prevalence is highest in the epidemic subtype, in which patients with advanced HIV and low CD4 T-cell counts may develop KS lesions. Although KS is associated most commonly with HIV, it also has been observed in men who have sex with men regardless of their HIV status.2 Patients undergoing immunosuppressive therapy also may not maintain immune tolerance to previously or newly acquired human herpesvirus 8, leading to the development of iatrogenic KS. This subtype particularly manifests in patients receiving therapy for autoimmune conditions or organ transplants and often only regresses if immunosuppressive therapy is withdrawn.3,4
The endemic and classic subtypes of KS may occur in patients without any known immunocompromise. Endemic KS demonstrates a predilection for pediatric populations in Africa and exhibits less pronounced sex disparity.5 In Uganda and Zimbabwe, endemic KS is the leading cancer in men and the second most frequently occurring cancer in women.6 In contrast, classic KS generally affects older men of Eastern European and Mediterranean descent or Ashkenazi Jewish ancestry. Patients with classic KS generally exhibit a less aggressive disease trajectory relative to other subtypes; however, these patients have a substantial risk for a secondary hematologic malignancy, which may already coexist at the time of diagnosis or emerge subsequently.1,7
Our patient, a native of Eastern Europe, was negative for HIV and was in a monogamous relationship with his wife; therefore, he was likely to have had the classic subtype of KS. As KS is a multifocal disease, lesions may independently emerge at different times and locations on the body. Our patient presented with a new lesion on the hand several years after excision of a similar lesion on the face. Lesions suspicious for KS include slow-growing, painless, red or violaceous patches, nodules, plaques, or patches on the extremities, most commonly manifesting on the feet and ankles. Our differential diagnosis included pyogenic granuloma, amelanotic melanoma, squamous cell carcinoma, and angiosarcoma.
The prognosis in patients with classic KS is favorable, as it often is limited to cutaneous sites and less commonly manifests on visceral organs. Nonetheless, pulmonary and gastrointestinal involvement manifesting as hemoptysis and rectal bleeding, respectively, can occur. This underscores the potential for more serious complications in instances with visceral involvement. Treatment focuses on managing symptoms and preventing growth and progression of individual lesions. Additionally, treatment strategies aim to improve cosmetic outcomes and address any underlying immunosuppression that may exacerbate the condition.8
For most patients, local therapies such as surgical excision, cryotherapy, laser therapy, or intralesional chemotherapy will remove or reduce individual lesions. Patients with widespread cutaneous or extracutaneous disease may require immunomodulatory agents such as interferon α or chemotherapeutic agents such as anthracyclines or paclitaxel.8
Our case highlights the importance of considering risk factors beyond HIV status when including KS as part of the differential diagnosis in patients with atypical vascular lesions. Early recognition enables timely evaluation of potential associated conditions and informs subsequent management decisions.
THE DIAGNOSIS: Kaposi Sarcoma
Histopathology revealed a serum crust on the surface of the specimen, and the dermis contained compact collections of spindled cells with interspersed erythrocytes (Figure 1). Human herpesvirus 8–stained sections highlighted many lesional cell nuclei (Figure 2). A diagnosis of Kaposi sarcoma (KS) was made based on these findings. The patient expressed interest in surgical excision; however, he was lost to follow-up.
Kaposi sarcoma is an indolent, multifocal, angioproliferative tumor that predominantly affects mucocutaneous sites with less frequent involvement of visceral organs. Kaposi sarcoma is categorized into 4 subtypes: epidemic, iatrogenic, endemic, and classic. Human herpesvirus 8, primarily transmitted through saliva or sexual contact, plays a central role in the pathogenesis of KS, as it drives disease development across all subtypes. The virus causes proliferation of endothelial cells and the formation of angioproliferative lesions characteristic of KS.1
Prevalence is highest in the epidemic subtype, in which patients with advanced HIV and low CD4 T-cell counts may develop KS lesions. Although KS is associated most commonly with HIV, it also has been observed in men who have sex with men regardless of their HIV status.2 Patients undergoing immunosuppressive therapy also may not maintain immune tolerance to previously or newly acquired human herpesvirus 8, leading to the development of iatrogenic KS. This subtype particularly manifests in patients receiving therapy for autoimmune conditions or organ transplants and often only regresses if immunosuppressive therapy is withdrawn.3,4
The endemic and classic subtypes of KS may occur in patients without any known immunocompromise. Endemic KS demonstrates a predilection for pediatric populations in Africa and exhibits less pronounced sex disparity.5 In Uganda and Zimbabwe, endemic KS is the leading cancer in men and the second most frequently occurring cancer in women.6 In contrast, classic KS generally affects older men of Eastern European and Mediterranean descent or Ashkenazi Jewish ancestry. Patients with classic KS generally exhibit a less aggressive disease trajectory relative to other subtypes; however, these patients have a substantial risk for a secondary hematologic malignancy, which may already coexist at the time of diagnosis or emerge subsequently.1,7
Our patient, a native of Eastern Europe, was negative for HIV and was in a monogamous relationship with his wife; therefore, he was likely to have had the classic subtype of KS. As KS is a multifocal disease, lesions may independently emerge at different times and locations on the body. Our patient presented with a new lesion on the hand several years after excision of a similar lesion on the face. Lesions suspicious for KS include slow-growing, painless, red or violaceous patches, nodules, plaques, or patches on the extremities, most commonly manifesting on the feet and ankles. Our differential diagnosis included pyogenic granuloma, amelanotic melanoma, squamous cell carcinoma, and angiosarcoma.
The prognosis in patients with classic KS is favorable, as it often is limited to cutaneous sites and less commonly manifests on visceral organs. Nonetheless, pulmonary and gastrointestinal involvement manifesting as hemoptysis and rectal bleeding, respectively, can occur. This underscores the potential for more serious complications in instances with visceral involvement. Treatment focuses on managing symptoms and preventing growth and progression of individual lesions. Additionally, treatment strategies aim to improve cosmetic outcomes and address any underlying immunosuppression that may exacerbate the condition.8
For most patients, local therapies such as surgical excision, cryotherapy, laser therapy, or intralesional chemotherapy will remove or reduce individual lesions. Patients with widespread cutaneous or extracutaneous disease may require immunomodulatory agents such as interferon α or chemotherapeutic agents such as anthracyclines or paclitaxel.8
Our case highlights the importance of considering risk factors beyond HIV status when including KS as part of the differential diagnosis in patients with atypical vascular lesions. Early recognition enables timely evaluation of potential associated conditions and informs subsequent management decisions.
- Radu O, Pantanowitz L. Kaposi sarcoma. Arch Pathol Lab Med. 2013;137:289-294. doi:10.5858/arpa.2012-0101-RS
- Lanternier F, Lebbé C, Schartz N, et al. Kaposi’s sarcoma in HIV-negative men having sex with men. AIDS. 2008;22:1163-1168. doi:10.1097/QAD.0b013e3283031a8a
- Penn I. Kaposi’s sarcoma in transplant recipients. Transplantation. 1997;64:669-673. doi:10.1097/00007890-199709150-00001
- Gallo Marin B, Maymone MBC, El Rayess F, et al. Kaposi sarcoma associated with tofacitinib use in a patient with rheumatoid arthritis. R I Med J (2013). 2023;106:18-20.
- Bishop BN, Lynch DT. Kaposi sarcoma. StatPearls [Internet]. Updated June 5, 2023. Accessed May 15, 2026. https://www.ncbi.nlm .nih.gov/books/NBK534839/
- Dedicoat M, Newton R. Review of the distribution of Kaposi’s sarcoma-associated herpesvirus (KSHV) in Africa in relation to the incidence of Kaposi’s sarcoma. Br J Cancer. 2003;88:1-3. doi:10.1038 /sj.bjc.6600745
- Hiatt KM, Nelson AM, Lichy JH, et al. Classic Kaposi sarcoma in the United States over the last two decades: a clinicopathologic and molecular study of 438 non-HIV-related Kaposi sarcoma patients with comparison to HIV-related Kaposi sarcoma. Mod Pathol. 2008;21:572-582. doi:10.1038/modpathol.2008.15
- Ceccarelli M, Facciolà A, Taibi R, et al. The treatment of Kaposi’s sarcoma: present and future options, a review of the literature. Eur Rev Med Pharmacol Sci. 2019;23:7488-7497. doi:10.26355 /eurrev_201909_18860
- Radu O, Pantanowitz L. Kaposi sarcoma. Arch Pathol Lab Med. 2013;137:289-294. doi:10.5858/arpa.2012-0101-RS
- Lanternier F, Lebbé C, Schartz N, et al. Kaposi’s sarcoma in HIV-negative men having sex with men. AIDS. 2008;22:1163-1168. doi:10.1097/QAD.0b013e3283031a8a
- Penn I. Kaposi’s sarcoma in transplant recipients. Transplantation. 1997;64:669-673. doi:10.1097/00007890-199709150-00001
- Gallo Marin B, Maymone MBC, El Rayess F, et al. Kaposi sarcoma associated with tofacitinib use in a patient with rheumatoid arthritis. R I Med J (2013). 2023;106:18-20.
- Bishop BN, Lynch DT. Kaposi sarcoma. StatPearls [Internet]. Updated June 5, 2023. Accessed May 15, 2026. https://www.ncbi.nlm .nih.gov/books/NBK534839/
- Dedicoat M, Newton R. Review of the distribution of Kaposi’s sarcoma-associated herpesvirus (KSHV) in Africa in relation to the incidence of Kaposi’s sarcoma. Br J Cancer. 2003;88:1-3. doi:10.1038 /sj.bjc.6600745
- Hiatt KM, Nelson AM, Lichy JH, et al. Classic Kaposi sarcoma in the United States over the last two decades: a clinicopathologic and molecular study of 438 non-HIV-related Kaposi sarcoma patients with comparison to HIV-related Kaposi sarcoma. Mod Pathol. 2008;21:572-582. doi:10.1038/modpathol.2008.15
- Ceccarelli M, Facciolà A, Taibi R, et al. The treatment of Kaposi’s sarcoma: present and future options, a review of the literature. Eur Rev Med Pharmacol Sci. 2019;23:7488-7497. doi:10.26355 /eurrev_201909_18860
Exophytic Papule on the Hand
Exophytic Papule on the Hand
A man in his 70s with a history of hypertension was admitted to the hospital for symptomatic bradycardia. On the day of admission, he reported a growth on the left second digit of 1 month’s duration, for which dermatology was consulted. The patient said the growth was asymptomatic but occasionally would get caught on objects. He denied any recent fevers, weight loss, or fatigue. He also denied any trauma to the area or other inciting factors. The patient reported there were no lesions anywhere else on the body, but he did mention a similar mass had been excised from his face several years prior. He noted that he had immigrated to the United States from Eastern Europe within the past several years.
Results of laboratory testing at the current presentation, including a basic metabolic panel, complete blood count with differential, hepatic function panel, thyroid-stimulating hormone level, and HIV antigen/antibody testing, were unremarkable. Physical examination revealed a single, well-circumscribed, 6×6–mm, round, red, exophytic papule with a collarette of scale on the volar surface of the left second digit. The skin on both arms was otherwise unremarkable. There was no evidence of lymphadenopathy or mucosal involvement. A shave biopsy of the lesion was performed.


Clinical Impact of Infra-Low Frequency Neurofeedback on Combat Veterans With Chronic Postconcussive Symptoms
Clinical Impact of Infra-Low Frequency Neurofeedback on Combat Veterans With Chronic Postconcussive Symptoms
Traumatic brain injury (TBI) is the signature injury of post-9/11 military operations, impacting > 441,000 combat veterans from 2001 to 2021 and 87% diagnosed with mild TBI (mTBI).1,2 The most common cause of mTBI during these operations was blast exposures stemming from improvised explosive devices, rocket-propelled grenades, or land mines. mTBI was once thought to be self-limiting, lasting hours or days postinjury, but is now recognized as a complex focal and diffuse injury causing a cascade of molecular and biochemical responses with significant physiologic effects lasting for a longer duration. A significant number of combat veterans with mTBI (23%-48%) experience long-standing postconcussive symptoms (PCSs) for many years postinjury.3-5
Developing and implementing strategies to reduce persistent symptoms associated with mTBI is of critical importance. Veterans diagnosed with mTBI and experiencing PCSs present ongoing treatment challenges to the health care system due to limited or suboptimal treatment options.6,7 According to the 2021 US Department of Veterans Affairs (VA) and US Department of Defense (DoD) clinical guidelines for postacute mTBI, treatment for PCSs should be symptom focused. 8,9 For instance, veterans with migraine headaches associated with mTBIs are often treated with abortive agents (eg, triptans) and preventive medications (eg, anticonvulsants and tricyclics).10 Cognitive dysfunction and insomnia are treated with cognitive rehabilitation programs, cognitive behavioral therapy, occupational therapy, and medications (eg, hypnotics for insomnia).11,12 The 2021 VA/DoD guidelines note that veteran and military focus groups described greater success with nonpharmacologic treatments than with pharmacologic treatments.8 The VA launched an enterprise-wide Whole Health Service program with the requirement that complementary and integrative health approaches must be available to veterans.13 As a nonpharmacologic, integrative, and noninvasive modality, neurofeedback (NFB) supports the VA Whole Health initiative and veterans’ preferences for integrative treatments.14
Neurofeedback
Rather than a symptom management approach, Defina et al described the possibilities of brain repair in TBI by treatments to enhance neuroplasticity, thereby establishing a more normalized or stable brain environment and enabling the brain to reorganize itself and function more normally.15 NFB has been shown to influence neuroplasticity,16 as evident in microstructural changes in white and gray matter17 and its ability to contribute to functional rehabilitation by restoring connectivity in specific areas of the brain that may have been impaired.18 The benefits of neuroenhancement strategies include potentially reduced pain for patients with mTBI and improved quality of life (QOL).19
NFB assists individuals by helping them become more aware of and self-regulate their physiology.20,21 Because there are several types of NFB (eg, quantitative electroencephalography, Z-scored, α-θ) that differ in terms of equipment, mechanism of action, focus, and patient and clinician procedures, it is important to note that this study used a novel technologically advanced form of NFB, referred to as infra-low frequency (ILF) NFB. It works by reflecting a person’s brain wave activity via conventional electroencephalography back to the person through the visual cortex, thus providing relevant information to which the brain responds to improve core state regulation.22
In 2006, ILF NFB developers sought to extend NFB capability into the slow cortical potential domain (< 0.1 Hz) and then gradually extended to lower frequencies on the basis of favorable clinical responses.22,23 In 2017, the technology reached an ILF capacity that appeared to be helpful for several clinical issues. These developments depended on instrumentation capable of low noise signal detection down to the lowest frequency of interest. Instrumentation was developed for the purpose (eg, Bee Medic Cygnet NFB).
Although mTBI has been a clinical focus in NFB since the 1980s, there are few published studies demonstrating the efficacy of ILF NFB relating to the PCSs of interest in this study, and 2 suggested ILF NFB positively affected change in PCS severity.24,25 Other studies found that ILF NFB decreased incidence of migraines and tension type headaches.26,27 However, the findings of these studies had limited generalizability due to methodologic limitations, such as selection bias and small sample sizes.24-27 Of importance to this article, there are also several publications on the efficacy of ILF NFB in clinical settings.28-33
This article presents the second analysis of data from veterans who completed ILF NFB intervention and control group procedures during a 5-year randomized controlled trial (RCT). The RCT included veterans who experienced an mTBI while participating in post-9/11 military operations to evaluate the impact of ILF NFB on chronic PCSs, including headache, insomnia, and attention dysfunction. Initial results of this trial demonstrated significant differences between the intervention and control groups with strong effect sizes on all outcome measures at the end of treatment.34
Methods
Participants included male and nonpregnant female veterans with a diagnosed mTBI during post-9/11 military operations; aged 18 to 65 years; reports of persistent (ie, > 3 months in duration) headaches, insomnia, and attention difficulties; and able to read and write English, comprehend what is read, and follow directions. mTBI diagnosis was verified for each veteran via the electronic health record. Patients were excluded if they had a severe TBI diagnosis or impaired decision-making capacity; were unable to comply with study visit schedule; or endorsed active suicidal intent on the Columbia-Suicide Severity Rating Scale.35
Recruitment efforts included: (1) letters sent to eligible veterans with mTBI who were identified by clinical informatics data after waiver of Health Insurance Portability and Accountability Act was obtained; veterans could contact the research team directly or the research team would call the veteran 2 weeks after the letter was sent; (2) veterans could be referred by a clinician; and (3) veterans could self-refer based on flyers and other study marketing materials.
The study was conducted from 2019 to 2024 at Spark M. Matsunaga VA Medical Center, in Honolulu, Hawaii. Four private research spaces in compliance with human research standards were used for consent, treatment, and assessment.
Consenting Procedure and Randomization
The privacy rights of potential participants were observed, and interested veterans who met the eligibility criteria underwent an informed consent procedure and were administered the Columbia-Suicide Severity Rating Scale.35 Those veterans not indicating active suicidal intent were randomized into the intervention or control group. Once randomized, the participant was enrolled and scheduled for baseline assessment.
All procedures of this study were performed in adherence with relevant laws and institutional guidelines. The study was reviewed and approved by the VA Pacific Islands Health Care System Institutional Review Board (#2019-06-JC/Promise 0003).
Outcome Measures
The outcome measures were administered at baseline, midpoint (3-7 weeks), end of treatment (6-12 weeks), and at a 2-month follow-up appointment with the research assistant or project coordinator.
The primary outcome measures included the Headache Impact Test (HIT-6), TBIQOL Headache Pain item short form, Insomnia Severity Index (ISI), Quality of Life in Neurological Disorders (Neuro-QOL) Sleep Disturbance short form, and attention measure: QIKtest Continuous Performance Test (QIKtest) (Table 1).36-44
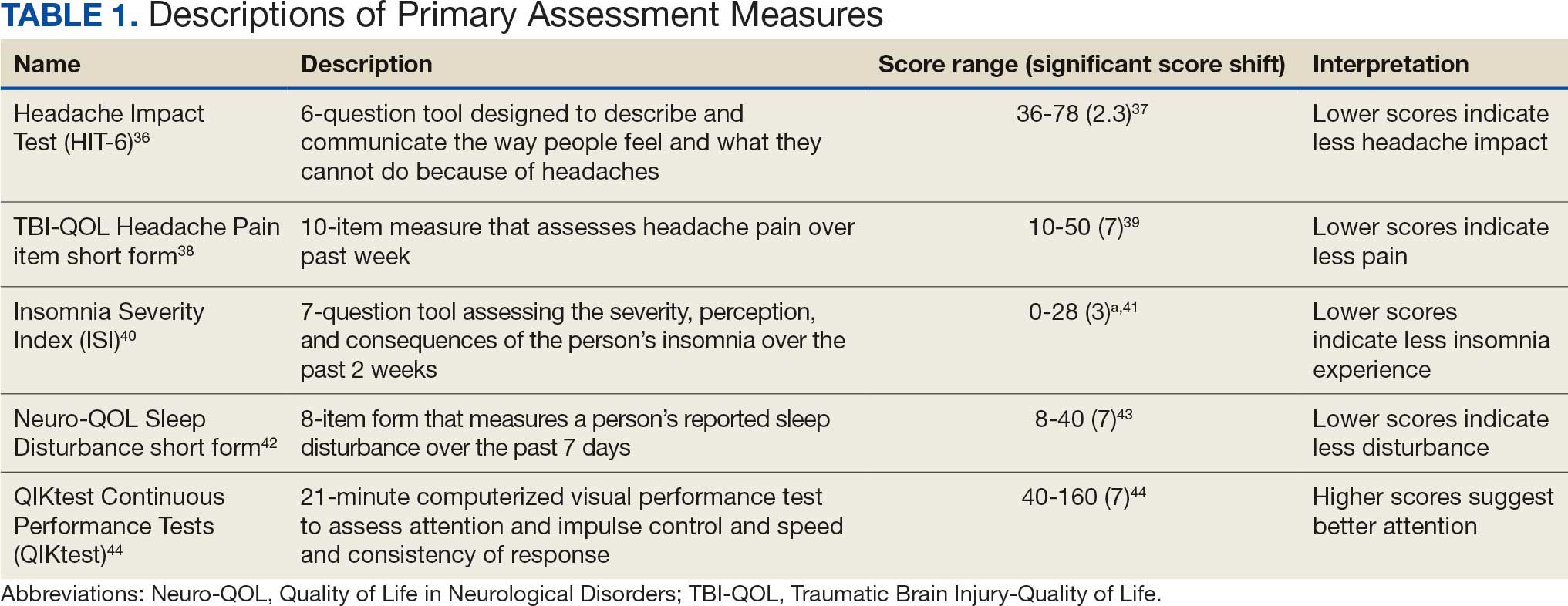
Secondary outcome measures included QOL After Brain Injury (QOLIBRI), Neuro- QOL Satisfaction With Roles/Activities short form (Neuro-QOL Satisfaction), Neuro-QOL Ability to Participate in Roles/Activities short form (Neuro-QOL Participate), Depression Anxiety Stress Scales (DASS-21), Patient Health Questionnaire-9 (PHQ-9), Posttraumatic Stress Disorder (PTSD) Checklist for DSM-5 (PCL-5), and the General Symptom Inventory (eAppendix 1).39,42,45-52
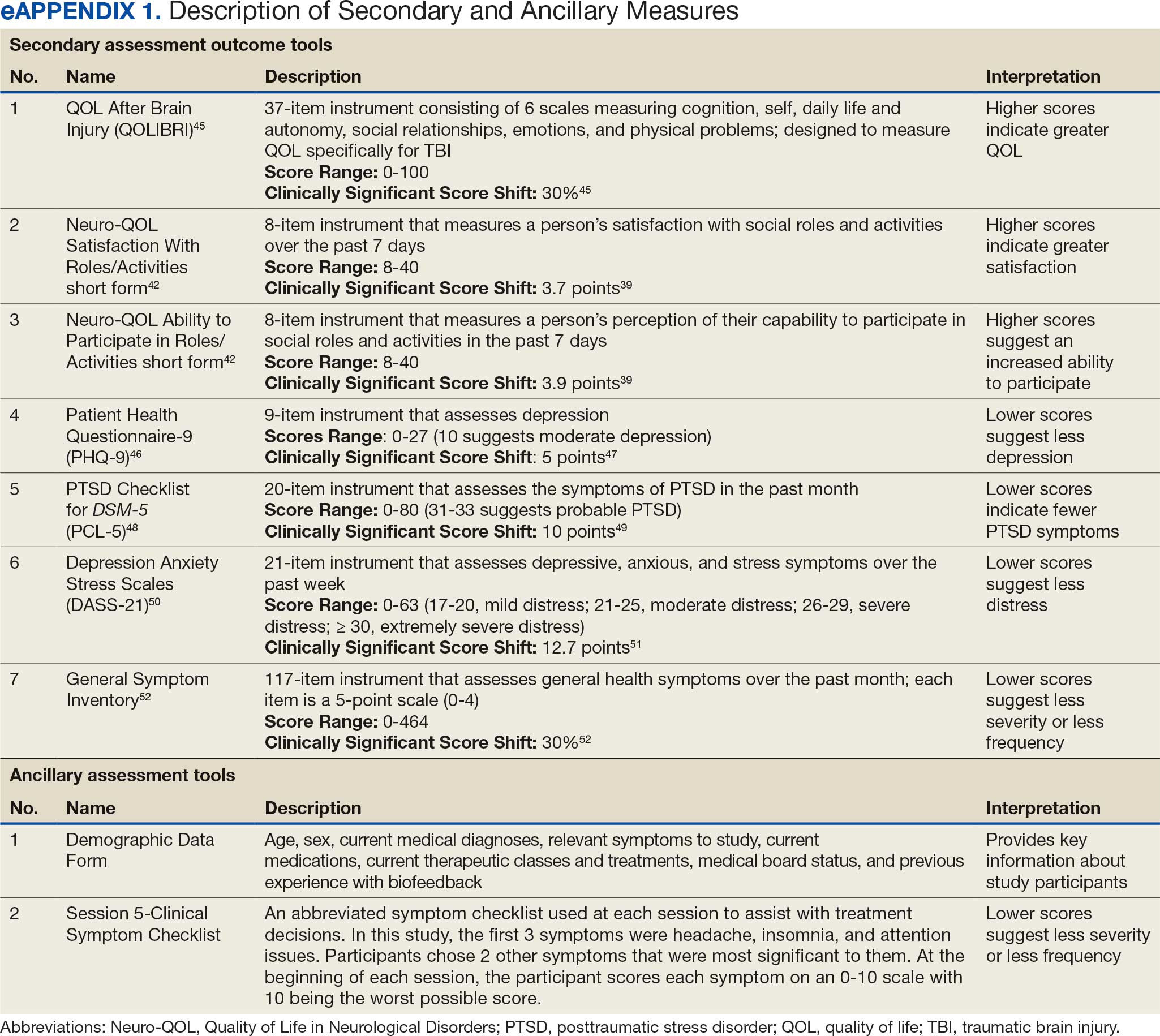
Sample
Seventy-two participants (36 in each group) were needed to have adequate statistical power for the analysis. Presuming attrition, the goal was to recruit 100 veterans. Literature on NFB studies of patients with mTBI have reported dropout rates ranging from 10% to 30%.53,54 Assuming a dropout rate of 28% and a moderate autocorrelation of 0.6 among repeated measures, this sample size ensured the detection of an average difference of at least 0.49 SDs with a power of 80% in the NFB intervention group compared with the control group using a 2-tailed significance level of 0.05.
Control Group
Following baseline assessment, control group participants received 8 phone calls (1 call/wk) from 1 of 4 clinical investigators over 8 to 10 weeks. During each 15-minute call, 1 of the following health topics was discussed: sleep hygiene, basic nutritional concepts, beverage choices, positive thinking, thought reframing, fitness, daily calming activity, and enhancement of focus strategies. A script for each topic was used to guide each call.
Intervention Group
Following baseline assessment, intervention group participants completed 20 half-hour ILF NFB sessions, typically receiving 3 sessions per week over an 8- to 10-week period. ILF NFB treatments were administered by 1 of 4 licensed health care employees who had received substantial ILF NFB training and achieved a skill reliability index score of 0.95, ensuring the skill level of the ILF NFB providers was equal. A script was used by the ILF NFB providers during the ILF NFB sessions to keep the interaction approach consistent with all participants.
All procedures were explained in advance to participants and voluntary participation affirmed. At the first session, participants filled out a clinical symptom checklist of 5 symptoms (eAppendix 1).39,42,45-49 The initial rating on the symptom checklist was reflective of their experience over the past month, while in each subsequent session, participants indicated their experience of those symptoms that day. ILF NFB providers were never privy to participants’ primary or secondary outcome measures data during the study, so these recurring clinical symptom checklist ratings, as well as other feedback provided by participants on their experience within and between sessions, were the clinical data used to make decisions about ILF NFB treatment protocol.
The Othmer Optimal Response Frequency (ORF) protocol was used for participants in this study.55 Through an iterative process, ORF protocol establishes the specific frequency point along the 0.000001 mHz to 0.1 Hz continuum, which is optimal to diminish symptoms experienced in real-time during the session (eg, tension or pain in shoulders; racing thoughts).
During each ILF NFB session, participants were seated comfortably and encouraged to look at the feedback screen. The moving images on the game screen provided almost instantaneous feedback (within 500 ms) to participants about their brain functioning, as ascertained by electrodes placed on the scalp as dictated by study protocol.56 A standardized protocol for site placement was used beginning with T3-T4, followed by the weekly addition of a site as tolerated in the following sequence: T4-P4, FP2-T4, and FP1-T4. More information about the ILF NFB procedures are outlined in the report of the pilot study and RCT initial results.22,34
Statistical Analysis
Eighty-seven participants were randomized, with 43 assigned to the intervention group and 44 to the control group to achieve the enrollment goal of ≥ 36 participants in each group. This report is the second analysis of data from this RCT that employed a per-protocol approach, analyzing a subset of participants who fully adhered to the study protocol and completed all study procedures. Outcome scores at baseline, midpoint, end of treatment, and 2-month follow-up were summarized as means with corresponding 95% CIs. Group comparisons at the end of treatment and 2-month follow-up time points were conducted using 2-sample t tests. All statistical tests were 2-sided with a significance level of .05 (Type I error rate). SAS software version 9.4 Maintenance 8 was used for statistical analysis. Cohen d analyses were used for effect sizes.
Results
Seventy-four participants fully adhered to the study protocol and were included in the present analyses, with 38 in the control group and 36 in the intervention group. eAppendix 2 depicts the flow of participants through this study. There were no adverse events related to treatment, and the 13 participants who withdrew typically reported difficulty with scheduling or transportation as the primary reason. This study also took place during the COVID-19 pandemic, which likely had some impact on enrollment; participants were differentially impacted by changes in employment and moves to the continental US.
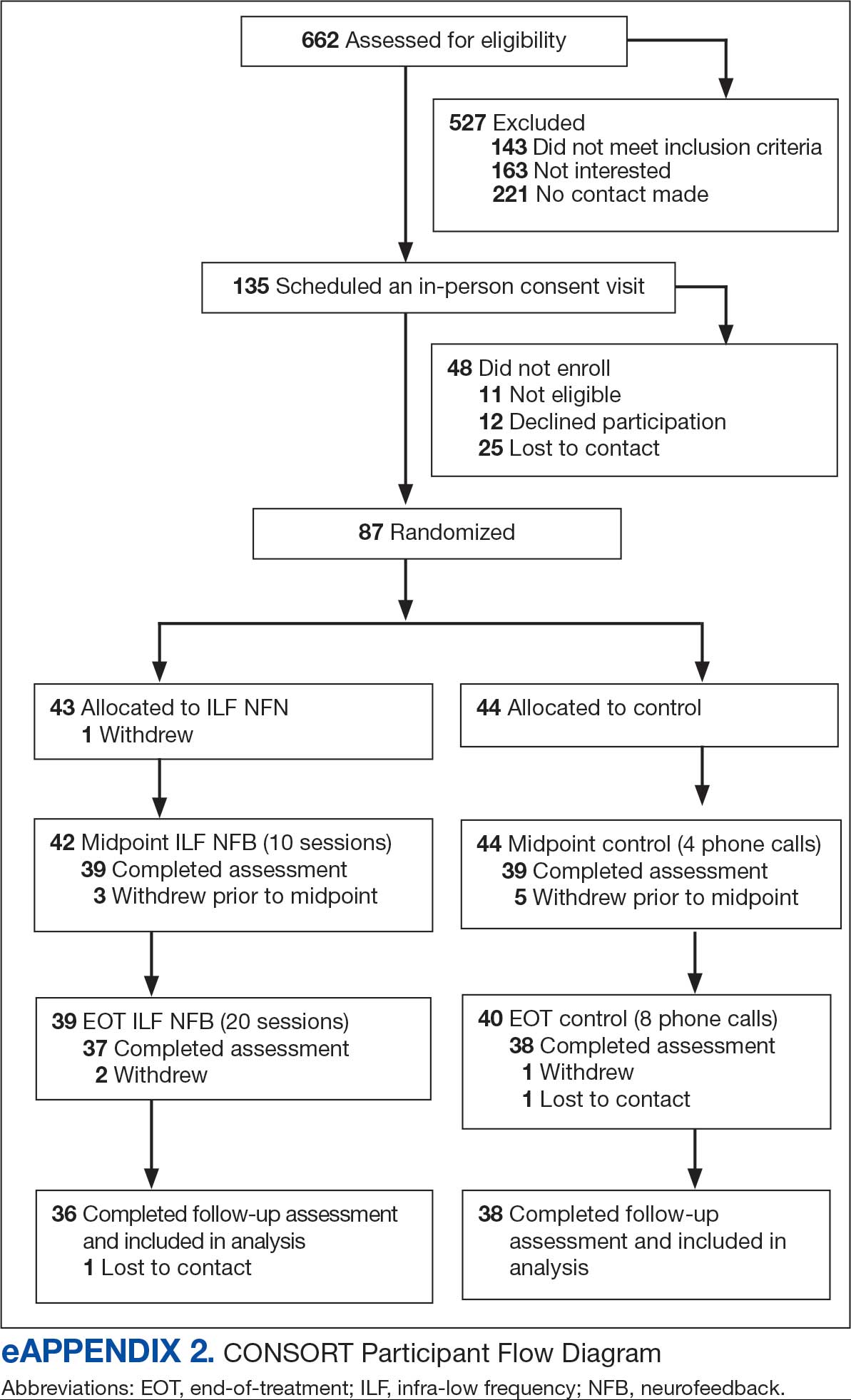
Participants were aged 30 to 60 years (mean [SD], 45.4 [8.0]). Most participants (90.5%) were male, and multiracial and White were the most common racial identities (Table 2). Participant characteristics were largely balanced across randomized groups. Similarly, test scores on the primary variables of interest in this study and secondary clinical variables assessed were comparable across participants (Table 3).
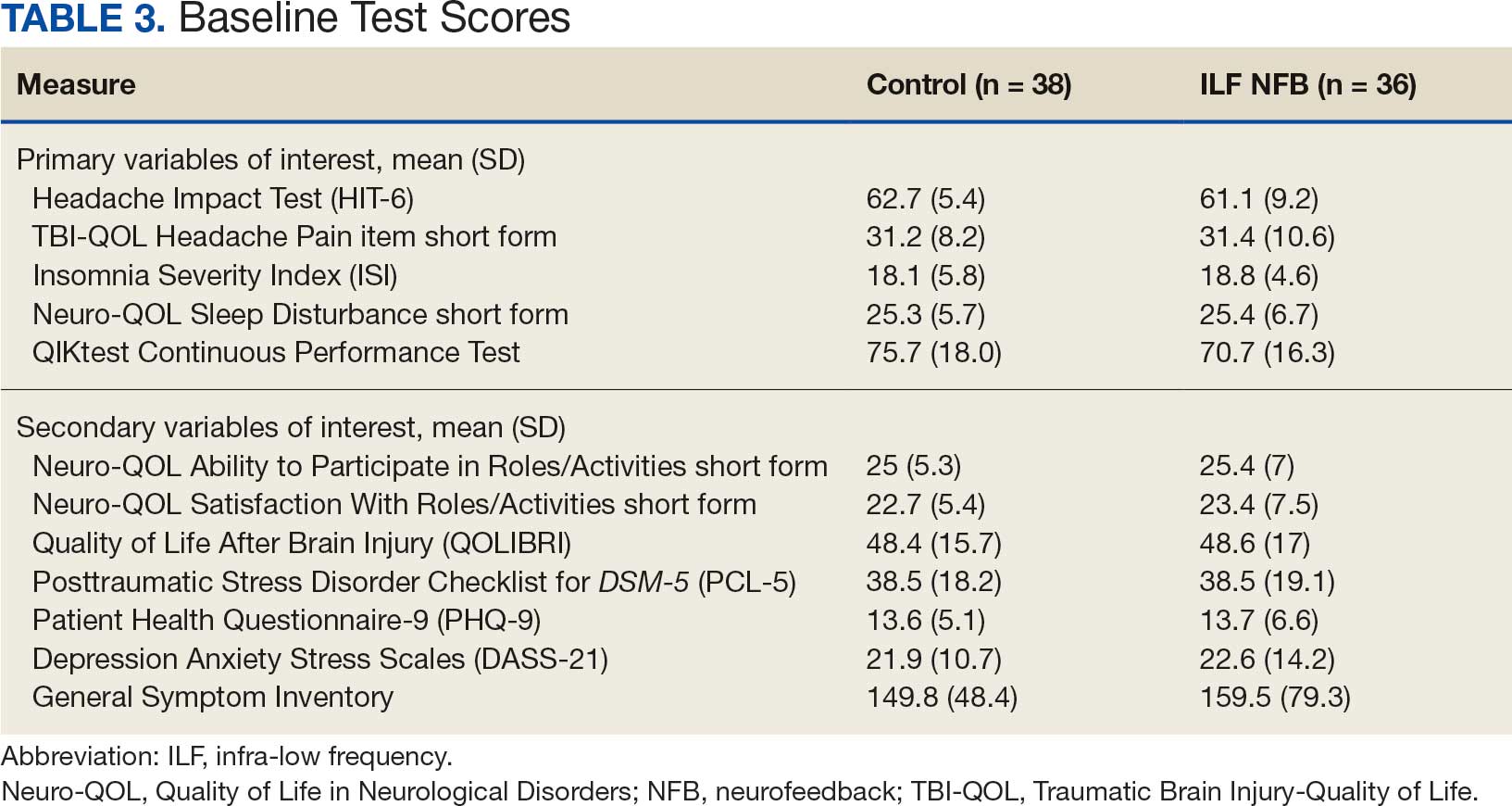
Primary Variables of Interest Analyses
This study’s hypothesis was that those who completed ILF NFB treatment per protocol would demonstrate statistically significant improvement in symptoms related to headaches, sleep disturbance, and difficulty with attention when compared with veterans in the control group. This hypothesis was partially supported. A 2-sample t test showed that veterans in the intervention group demonstrated significant improvement in headache symptoms compared with veterans in the control group on the HIT-6 at the end-of-treatment (P < .001, d = 1.53) and 2-month follow-up assessment (P < .001, d = 1.14). This pattern also was consistent with the TBI-QOL Headache Pain item short form, with veterans in the intervention group showing improvement beyond those in the control group at the end-of-treatment (P < .001, d = 0.89) and 2-month follow-up assessment (P < .001, d = 0.83). Two-sample t tests also demonstrated significant improvement in subjective reports of sleep; those in the intervention group had significantly lower scores on the ISI at the end-of-study (P < .001, d = 1.53) and 2-month follow-up assessment (P < .001, d = 0.97). This pattern also held true for the Neuro-QOL Sleep Disturbance short form subtest, which demonstrated significantly more improvement in the intervention group compared with the control group at the end-of-study (P < .001, d = 0.97) and 2-month follow- up assessment (P < .001, d = 0.92). improvement in attention was not supported by the present results. A 2-sample t test found no significant difference between performance on the QIKtest for veterans in the intervention group vs the control group at the end-of-study (P = .40, d = 0.19) or the 2-month follow-up (P = .43, d = 0.20) (eAppendix 3).
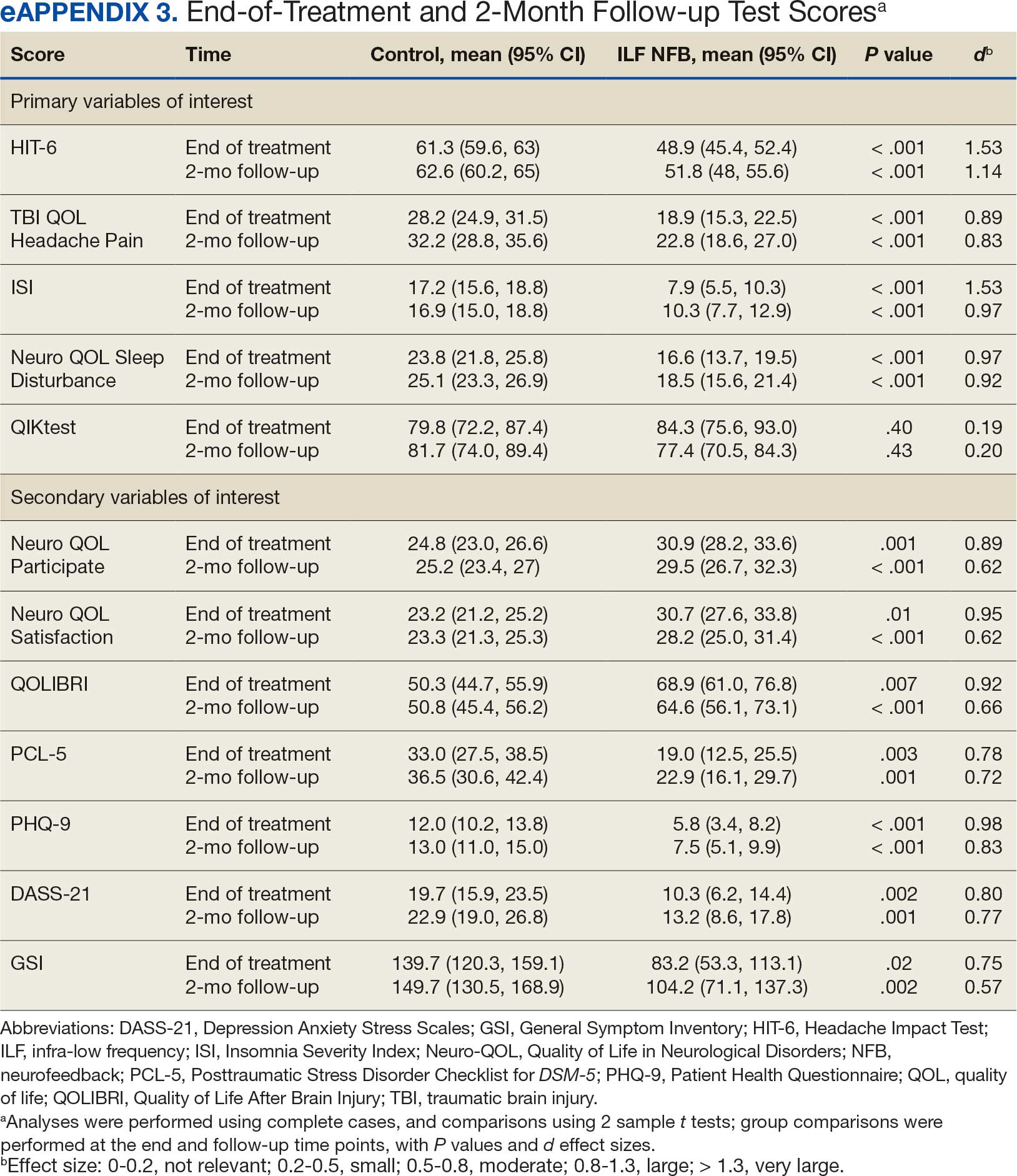
Secondary Variables of Interest Analysis
Secondary variables examined differences in QOL, PTSD, depressive symptoms, and general symptoms reported between veterans in the intervention and control groups. Results demonstrated that veterans in the intervention group showed improvement above and beyond those in the control group on all measures. In regard to QOL, veterans in the intervention group had significantly higher scores on the Neuro-QOL Participate subtest than those in the control group at the end-of-study (P = .01, d = 0.89) and 2-month follow-up assessment (P < .001, d = 0.62). A similar pattern was found for the Neuro-QOL Satisfaction subtest, with veterans in the intervention group showing significantly higher scores than those in the control group at the end-of-study (P = .001, d = 0.95) and 2-month follow-up assessment (P < .001, d = 0.62). This also held true on the QOLIBRI, with veterans in the intervention group demonstrating significantly higher scores than those in the control group at the end-of-study (P = .001, d = 0.92) and 2-month follow-up assessment (P < .001, d = 0.66).
Veterans in the intervention group had significantly lower scores on the PCL-5 than those in the control group at the end-of- study (P = .003, d = 0.78) and 2-month follow-up assessment (P = .001, d = 0.72). Veterans in the intervention group also had significantly lower scores on the PHQ-9 than those in the control group at the end-of-study (P < .001, d = 0.98) and 2-month follow-up assessment (P < .001, d = 0.83). Veterans in the intervention group had significantly lower scores on the DASS- 21 than those in the control group at the end-of-study (P = .002, d = 0.80) and 2-month follow-up assessment (P = .001, d = 0.77). They also had significantly lower scores on the General Symptom Inventory than those in the control group at the end-of-study (P = .02, d = 0.75) and 2-month follow-up assessment (P = .002, d = 0.57). A clinically significant shift of score occurred for each of the measures except DASS-21 (eAppendix 3). eAppendix 4 depicts the change in scores for the intervention group at the end of treatment and the clinically significant shift score of each measure.
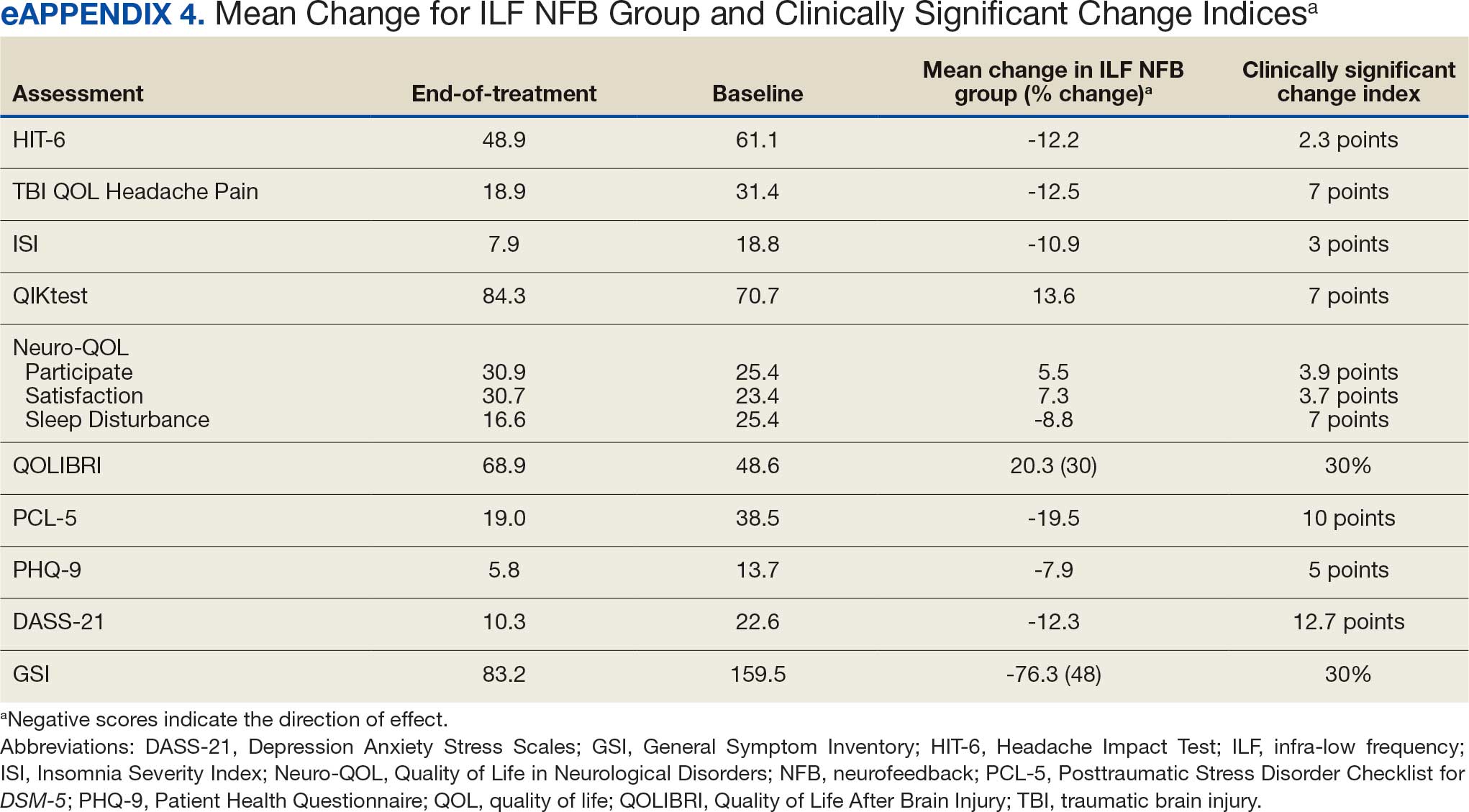
Discussion
The results of this RCT revealed a promising impact of ILF NFB on the commonly experienced persistent PCSs of headaches and disrupted sleep. Veterans in the intervention group demonstrated statistically significant improvement in headache symptoms compared with veterans in the control group when assessed at the end of treatment and during a 2-month follow-up. The statistical significance of these improvements was also supported by large or very large effect sizes. In addition to these primary variables of interest, veterans in the intervention group notably demonstrated significant improvement compared with those in the control group in a number of secondary clinical measures, including QOL, traumatic stress-related symptoms, depressive symptoms, and general symptom report. The clinical impact was further supported by the clinically relevant shift in scores in the intervention group.
The data did not support the hypothesis that attention concerns would show significant improvement following ILF NFB. Performance on an attention measure did not differ significantly between groups at either the end-of-treatment or 2-month follow up assessment. The QIKtest, a continuous performance test used to measure attention, was a go/no-go task and calculated based on a combination of various types of errors and outlier responses. The stimulus for this task is a series of computerized, blinking lights, for which participants are tasked with discriminating targets and nontargets under time pressure. However, the order of the stimuli are consistent across administrations, rather than being randomized, introducing a potential confound of practice effects on this task since patients were administered the QIKtest 3 times in a 2-month period and again 2 months later. Veterans in the control group notably improved in their average performance of this task from baseline to the endpoint of their treatment participation and demonstrated further improvement at the 2-month follow-up assessment; this pattern would be consistent with potential practice effects and warrants caution in its interpretation for both groups.
Previously published ILF NFB clinical studies that used the QIKtest and found positive results were mostly conducted among children and teen populations across longer treatment periods. This research may indicate the QIKtest is not an appropriate measure to assess adults who have specialized training in responding to stimuli (ie, trained military personnel). This suggests the concept of attention dysfunction experienced by veterans and the best method to measure it may need to be explored further. This construct may not be related to the focus and skill in prolonged attention needed in selecting go/ no-go tasks, but rather related to a broader conceptual basis involving memory, recall, clarity of rational thought, and decision making impacted by the mTBI. For instance, a study among combat veterans with mTBI and PTSD found that performance on objective cognitive measures did not significantly correlate with their subjective reports of cognitive difficulties.57 This reflects the pattern of the present study, in which subjective reports of attention improved over time on the clinical symptom checklist filled out by participants at each session, but the objective measure did not. The mean attention dysfunction score was 6 at session 1 and 1 to 2 at session 20 (lower scores are better on a 10-point scale).
Strengths and Limitations
This study presents results stemming from the first RCT examining clinical effectiveness of ILF NFB in a VA setting for veterans with diagnoses of mTBI. The study design shows promising external validity. Veterans were able to participate in a treatment consisting of 20 sessions over a period of typically 8 to 10 weeks, entailing 2 to 3 sessions per week, with an attrition of only 18% over the course of the study. Notably, attrition rates may have been impacted by the time course of the study, which was recruiting and running participants throughout the COVID-19 pandemic (March 2020 to May 2023). No attrition was due to the intervention itself, and no adverse reactions to ILF NFB were reported during the course of the study. Other strengths of the study include the ethnically and racially diverse participants, representative of the population of veterans in Hawaii. Additionally, all ILF NFB providers underwent supervised ILF NFB training and achieved a skill reliability index score of 0.95 prior to providing ILF NFB to the intervention group.
This study was not blinded. Neither veterans nor ILF NFB clinicians were blinded and were therefore aware of the randomly assigned groups. Research assistants administering the periodic assessments were meant to be blinded to condition by design; however, as the study progressed, a research assistant became unintentionally aware of each study participant's condition based on required documentation in the veteran’s health records; more notes were present for those in the intervention group (20 specialist notes) than the control group (8 notes). While the presence of a control group represents a strength relative to much of the existing ILF NFB literature, the control group in this case did not account for the total time spent with the researchers. Participants in the intervention group met with researchers for 20 total sessions as opposed to 8 telephone calls. Therefore, the study design cannot fully rule out the differential impact of demand characteristics between the 2 groups, nor can it fully address or rule out the impact of differential motivation and expectations between groups. There is also evidence that technological innovation can influence the expectations of research participants, meaning that the intervention group may have been unduly influenced by the novelty of the ILF NFB technology, to which the control group did not have exposure.58
A second attention measure for this study would have been beneficial, perhaps in identifying true change in attention ability or providing more insight into finding better methods to assess attention among veterans with mTBI. ILF NFB demonstrated significant impact across multiple outcome measures of clinical relevance for veterans diagnosed with mTBI, including the primary outcome variables of headache and sleep. The strength of the improvements seen in these areas, supported by large practical effects as well as veterans’ subjective reports, indicates much promise. Follow-up studies may also focus on the potential effectiveness of ILF NFB as a treatment of the secondary concerns measured in this study, including traumatic stress-related and depressive symptoms, and may explore the added benefit, if any, of ILF NFB alongside other evidence-based treatments for traumatic stress-related and mood disorders (eg, cognitive behavioral therapy). Using functional magnetic resonance imaging before and after assessments to determine actual brain enhancement with ILF NFB for certain disorders in which a brain signature exists (ie, migraine) should be explored. Further examination of ILF NFB as an intervention for attention may also be warranted, using more effective measures of attention in the population of veterans with mTBI, given the concerns noted earlier. Future research on this topic will need to clearly define attention in relation to the veteran experience and use relevant measures.
Conclusions
This study supports ILF NFB as a safe, noninvasive, nonpharmacologic treatment that may be effective in addressing the complex clinical concerns of veterans diagnosed with mTBI, a population for whom effective treatments have been difficult to identify. This intervention can provide veterans with a desirable and effective nonpharmacologic alternative in their care.
- Hayward P. Traumatic brain injury: the signature of modern conflicts. Lancet Neurol. 2008;7:200-201. doi:10.1016/S1474-4422(08)70032-2
- Whiteneck G, Williams W, Almeida E, et al. Two decades of Department of Veterans Affairs traumatic brain injury care and benefits for veterans of post-9/11 conflicts. J Head Trauma Rehabil. 2024;39:E462-E469. doi:10.1097/HTR.0000000000000952
- Chapman JC, Diaz-Arrastia R. Military traumatic brain injury: a review. Alzheimers Dement. 2014;10(3 suppl):S97- S104. doi:10.1016/j.jalz.2014.04.012
- Dean PJA, O’Neill D, Sterr A. Post-concussion syndrome: prevalence after mild traumatic brain injury in comparison with a sample without head injury. Brain Inj. 2012;26:14-26. doi:10.3109/02699052.2011.635354
- Agimi Y, Hai T, Gano A, et al. Clinical trajectories of comorbidity associated with military-sustained mild traumatic brain injury: pre- and post-injury. J Head Trauma Rehabil. 2024;39:E564-E575. doi:10.1097/HTR.0000000000000934
- Hoge CW, McGurk D, Thomas JL, et al. Mild traumatic brain injury in U.S. soldiers returning from Iraq. N Engl J Med. 2008;358:453-463. doi:10.1056/NEJMoa072972
- Bogdanova Y, Verfaellie M. Cognitive sequelae of blast-induced traumatic brain injury: recovery and rehabilitation. Neuropsychol Rev. 2012;22:4-20. doi:10.1007/s11065-012-9192-3
- Eapen BC, Bowles AO, Sall J, et al. The management and rehabilitation of post-acute mild traumatic brain injury. Brain Inj. 2022;36:693-702. doi:10.1080/02699052.2022.2033848
- Department of Veterans Affairs (VA) and Department of Defense (DoD). VA/DoD Clinical Practice Guideline for the management and Rehabilitation of Post-Acute Mild Traumatic Brain Injury, 2021, Version 3:1-128. https://www.healthquality.va.gov/HEALTHQUALITY/guidelines/Rehab/mtbi/index.asp
- Patil VK, St Andre JR, Crisan E, et al. Prevalence and treatment of headaches in veterans with mild traumatic brain injury. Headache. 2011;51:1112-1121. doi:10.1111/j.1526-4610.2011.01946.x
- Ayalon L, Borodkin K, Dishon L, Kanety H, Dagan Y. Circadian rhythm sleep disorders following mild traumatic brain injury. Neurology. 2007;68:1136-1140. doi:10.1212/01.wnl.0000258672.52836.30
- Bogdanova Y, Verfaellie M. Cognitive sequelae of blast-induced traumatic brain injury: recovery and rehabilitation, Neuropsychology Review. 2012;22:4-20. doi:10.1007/s11065-012-9192-3
- US Department of Veteran Affairs. VHA Directive 1137.December 13, 2022. https://www.va.gov/VHApublications/ViewPublication.asp?pub_ID=10072
- Taylor SL, Hoggatt KJ, Kligler B. Complementary and integrated health approaches: what do veterans use and want. J Gen Intern Med. 2019;34:1192-1199. doi:10.1007/s11606-019-04862-6
- DeFlna P, Fellus J, Polito MZ, et al. The new neuroscience frontier: promoting neuroplasticity and brain repair in traumatic brain injury. Clin Neuropsychol. 2009;23:1391-1399. doi:10.1080/13854040903058978
- Enriquez-Geppert S, Huster RJ, Herrmann CS. Boosting brain functions: improving executive functions with behavioral training, neurostimulation, and neurofeedback. Int J Psychophysiol. 2013;88:1-16. doi:10.1016/j.ijpsycho.2013.02.001
- Ghaziri J, Tucholka A, Larue V, et al. Neurofeedback training induces changes in white and gray matter. Clin EEG Neurosci. 2013;44:265-272. doi:10.1177/1550059413476031
- Ibric VL, Dragomirescu LG, Hudspeth WJ. Real-time changes in connectivities during neurofeedback. J Neurother. 2009;13:156-165. doi:10.1080/10874200903118378
- Clark VP, Parasuraman R. Neuroenhancement: enhancing brain and mind in health and in disease. Neuroimage. 2014;85:889-894. doi:10.1016/j.neuroimage.2013.08.071
- Larsen S, Sherlin L. Neurofeedback: an emerging technology for treating central nervous system dysregulation. Psychiatr Clin North Am. 2013;36:163-168. doi:10.1016/j.psc.2013.01.005
- Hammond DC. What is neurofeedback: an update. J Neurother. 2011; 15:305-336. doi:10.1080/10874208.2011.623090
- Othmer S. Endogenous neuromodulation at infra-low frequencies. In: Chartier DR, Dellinger MB, Evans JR, Budzynski HK, eds. Introduction to Quantitative EEG and Neurofeedback. 3rd ed. Academic Press; 2023:283-299. doi:10.1016/B978-0-323-89827-0.00001-2
- Othmer SF. History of the Othmer Method: an evolving clinical model and process. In: Evans JR, Dellinger MB, Russell HL, eds. Neurofeedback: The First Fifty Years. Academic Press; 2020:327-334. doi:10.1016/B978-0-12-817659-7.00043-9
- Legarda SB, Lahti CE, McDermott D, Michas-Martin A. Use of novel concussion protocol with infralow frequency neuromodulation demonstrates significant treatment response in patients with persistent postconcussion symptoms, a retrospective study. Front Hum Neurosci. 2022;16:894758. doi:10.3389/fnhum.2022.894758
- Carlson J, Ross GW. Neurofeedback impact on chronic headache, sleep, and attention disorders experienced by veterans with mild traumatic brain injury: a pilot study. Biofeedback. 2021;49:2-9. doi:10.5298/1081-5937-49.01.01
- Dobrushina O, Arina G, Osina E, Aziatskaya G. Clinical and psychological confirmation of stabilizing effect of neurofeedback in migraine. Eur Psychiatry. 2017;41:S253-S253. doi:10.1016/j.eurpsy.2017.02.045
- Arina GA, Dobrushina OR, Shvetsova ET, et al. Infra-low frequency neurofeedback in tension-type headache: a cross-over sham-controlled study. Front Hum Neurosci. 2022;16:891323. doi:10.3389/fnhum.2022.891323
- Kirk HW, Dahl MG. Infra low frequency neurofeedback training for trauma recovery: a case report. Front Hum Neurosci. 2022;16:905823. doi:10.3389/fnhum.2022.905823
- Benson A, LaDou T. The use of neurofeedback for combat veterans with post-traumatic stress. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. CRC Press; 2015.
- Legarda SB, McMahon D, Othmer S, Othmer S. Clinical neurofeedback: case studies, proposed mechanism, and implications for pediatric neurology practice. J Child Neurol. 2011;26:1045-1051. doi:10.1177/0883073811405052
- McMahon DE. Notes from clinical practice: an MD’s perspective on 9 years of neurofeedback practice. Semin Pediatr Neurol. 2013;20:258-260. doi:10.1016/j.spen.2013.10.007
- Othmer S, Othmer SF. Post traumatic stress disorder— the neurofeedback remedy. Biofeedback. 2009;37:24-31. doi:10.5298/1081-5937-37.1.24
- Shapero E, Prager J. ILF Neurofeedback and alpha-theta training in a multidisciplinary chronic pain program. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. 2nd ed. Routledge; 2020:223-243.
- Carlson J, Ross G, Tyrrell C, et al. Infra-low frequency neurofeedback impact on post-concussive symptoms of headache, insomnia and attention disorder: results of a randomized control trial. Explore (NY). 2025;21:103137. doi:10.1016/j.explore.2025.103137
- Posner K, Brown GK, Stanley B, et al. The Columbia– Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011;168:1266- 1277. doi:10.1176/appi.ajp.2011.10111704
- Kosinski M, Bayliss MS, Bjorner JB, et al. A six-item short-form survey for measuring headache impact: the HIT-6. Qual Life Res. 2003;12:963-974. doi:10.1023/a:1026119331193
- Coeytaux RR, Kaufman JS, Chao R, Mann JD, Devellis RF. Four methods of estimating the minimal important difference score were compared to establish a clinically significant change in Headache Impact Test. J Clin Epidemiol. 2006;59:374-380. doi:10.1016/j.jclinepi.2005.05.010
- Tulsky DS, Tyner CE, Boulton AJ, et al. Development of the TBI-QOL Headache Pain Item Bank and Short Form. J Head Trauma Rehabil. 2019;34:298-307. doi:10.1097/HTR.0000000000000532
- Poritz JMP, Sherer M, Kisala MA, et al. Responsiveness of the Traumatic Brain Injury-Quality of Life (TBI-QOL) measurement system. Arch Phys Med Rehabil. 2020;101:54- 61. doi:10.1016/j.apmr.2017.11.018
- Bastien CH, Vallières A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001;2:297-307. doi:10.1016/s1389-9457(00)00065-4
- Yang M, Morin CM, Schaefer M, Wallenstein GV. Interpreting score differences in the Insomnia Severity Index: using health-related outcomes to define the minimally important difference. Curr Med Res Opin. 2009;25:2487-2494. doi:10.1185/03007990903167415
- Cella D, Lai J-S, Nowinski CJ, et al. Neuro-QOL Brief measures of health-related quality of life for clinical research in neurology. Neurology. 2012;78:1860-1867. doi:10.1212/WNL.0b013e318258f744
- Kozlowski AJ, Cella D, Nitsch KP, Heinemann AW. Evaluating individual change with the Quality of Life in Neurological Disorders (Neuro-QoL) short forms. Arch Phys Med Rehabil. 2016;97:650-654.e8. doi:10.1016/j.apmr.2015.12.010
- Versace M. QIKTest Report on EEG Expert: introduction and overview. 2014. Accessed February 24, 2026. https://media.voog.com/0000/0044/8343/files/EEGexpert_manual_newreport2014_EN.pdf
- Truelle J-L, Koskinen S, Hawthorne G, et al. Quality of life after traumatic brain injury: the clinical use of the QOLIBRI, a novel disease-specific instrument. Brain Inj. 2010;24:1272-1291. doi:10.3109/02699052.2010.506865
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606-613. doi:10.1046/j.1525-1497.2001.016009606.x
- Kroenke K. Enhancing the clinical utility of depression screening. CMAJ. 2012;184:281-282. doi:10.1503/cmaj.112004
- Weathers FW, Litz BT, Keane TM, et al. PTSD checklist for DSM-5 (PCL-5). National Center for PTSD. Updated September 10, 2025. Accessed February 24, 2026. https:// www.ptsd.va.gov/professional/assessment/adult-sr/ptsd-checklist.asp
- Henry JD, Crawford JR. The short]form version of the Depression Anxiety Stress Scales (DASS]21): construct validity and normative data in a large non]clinical sample. Br J Clin Psychol. 2005;44:227-239. doi:10.1348/014466505X29657
- Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther. 1995;33(3):335-343. doi:10.1016/0005-7967(94)00075-u
- Ronk FR, Korman JR, Hooke GR, Page AC. Assessing clinical significance of treatment outcomes using the DASS-21. Psychol Assess. 2013;25:1103-1110. doi:10.1037/a0033100
- Carlson J. General symptom inventory. Description published online 2021.
- Nelson DV, Esty ML. Neurotherapy of traumatic brain injury/ posttraumatic stress symptoms in OEF/OIF veterans. J Neuropsychiatry Clin Neurosci. 2012;24:237-240. doi:10.1176/appi.neuropsych.11020041
- Zoefel B, Huster RJ, Herrmann CS. Neurofeedback training of the upper alpha frequency band in EEG improves cognitive performance. Neuroimage. 2011;54:1427-1431. doi:10.1016/j.neuroimage.2010.08.078
- Othmer S, Othmer S. Toward a theory of infra-low frequency neurofeedback. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. 2nd ed. Routledge; 2020.
- Huster RJ, Mokom ZN, Enriquez-Geppert S, Herrmann CS. Brain–computer interfaces for EEG neurofeedback: peculiarities and solutions. Int J Psychophysiol. 2014;91:36-45. doi:10.1016/j.ijpsycho.2013.08.011
- Ord AS, Martindale SL, Jenks ER, Rowland JA. Subjective cognitive complaints and objective cognitive functioning in combat veterans: effects of PTSD and deployment mild TBI. Appl Neuropsychol Adult. 2025;32:1400-1406. doi:10.1080/23279095.2023.2280807
- Lawton J, Blackburn M, Breckenridge J, Hallowell N, Farrington C, Rankin D. Ambassadors of hope, research pioneers and agents of change-individuals’ expectations and experiences of taking part in a randomised trial of an innovative health technology: longitudinal qualitative study. Trials. 2019;20:289. doi:10.1186/s13063-019-3373-9
Traumatic brain injury (TBI) is the signature injury of post-9/11 military operations, impacting > 441,000 combat veterans from 2001 to 2021 and 87% diagnosed with mild TBI (mTBI).1,2 The most common cause of mTBI during these operations was blast exposures stemming from improvised explosive devices, rocket-propelled grenades, or land mines. mTBI was once thought to be self-limiting, lasting hours or days postinjury, but is now recognized as a complex focal and diffuse injury causing a cascade of molecular and biochemical responses with significant physiologic effects lasting for a longer duration. A significant number of combat veterans with mTBI (23%-48%) experience long-standing postconcussive symptoms (PCSs) for many years postinjury.3-5
Developing and implementing strategies to reduce persistent symptoms associated with mTBI is of critical importance. Veterans diagnosed with mTBI and experiencing PCSs present ongoing treatment challenges to the health care system due to limited or suboptimal treatment options.6,7 According to the 2021 US Department of Veterans Affairs (VA) and US Department of Defense (DoD) clinical guidelines for postacute mTBI, treatment for PCSs should be symptom focused. 8,9 For instance, veterans with migraine headaches associated with mTBIs are often treated with abortive agents (eg, triptans) and preventive medications (eg, anticonvulsants and tricyclics).10 Cognitive dysfunction and insomnia are treated with cognitive rehabilitation programs, cognitive behavioral therapy, occupational therapy, and medications (eg, hypnotics for insomnia).11,12 The 2021 VA/DoD guidelines note that veteran and military focus groups described greater success with nonpharmacologic treatments than with pharmacologic treatments.8 The VA launched an enterprise-wide Whole Health Service program with the requirement that complementary and integrative health approaches must be available to veterans.13 As a nonpharmacologic, integrative, and noninvasive modality, neurofeedback (NFB) supports the VA Whole Health initiative and veterans’ preferences for integrative treatments.14
Neurofeedback
Rather than a symptom management approach, Defina et al described the possibilities of brain repair in TBI by treatments to enhance neuroplasticity, thereby establishing a more normalized or stable brain environment and enabling the brain to reorganize itself and function more normally.15 NFB has been shown to influence neuroplasticity,16 as evident in microstructural changes in white and gray matter17 and its ability to contribute to functional rehabilitation by restoring connectivity in specific areas of the brain that may have been impaired.18 The benefits of neuroenhancement strategies include potentially reduced pain for patients with mTBI and improved quality of life (QOL).19
NFB assists individuals by helping them become more aware of and self-regulate their physiology.20,21 Because there are several types of NFB (eg, quantitative electroencephalography, Z-scored, α-θ) that differ in terms of equipment, mechanism of action, focus, and patient and clinician procedures, it is important to note that this study used a novel technologically advanced form of NFB, referred to as infra-low frequency (ILF) NFB. It works by reflecting a person’s brain wave activity via conventional electroencephalography back to the person through the visual cortex, thus providing relevant information to which the brain responds to improve core state regulation.22
In 2006, ILF NFB developers sought to extend NFB capability into the slow cortical potential domain (< 0.1 Hz) and then gradually extended to lower frequencies on the basis of favorable clinical responses.22,23 In 2017, the technology reached an ILF capacity that appeared to be helpful for several clinical issues. These developments depended on instrumentation capable of low noise signal detection down to the lowest frequency of interest. Instrumentation was developed for the purpose (eg, Bee Medic Cygnet NFB).
Although mTBI has been a clinical focus in NFB since the 1980s, there are few published studies demonstrating the efficacy of ILF NFB relating to the PCSs of interest in this study, and 2 suggested ILF NFB positively affected change in PCS severity.24,25 Other studies found that ILF NFB decreased incidence of migraines and tension type headaches.26,27 However, the findings of these studies had limited generalizability due to methodologic limitations, such as selection bias and small sample sizes.24-27 Of importance to this article, there are also several publications on the efficacy of ILF NFB in clinical settings.28-33
This article presents the second analysis of data from veterans who completed ILF NFB intervention and control group procedures during a 5-year randomized controlled trial (RCT). The RCT included veterans who experienced an mTBI while participating in post-9/11 military operations to evaluate the impact of ILF NFB on chronic PCSs, including headache, insomnia, and attention dysfunction. Initial results of this trial demonstrated significant differences between the intervention and control groups with strong effect sizes on all outcome measures at the end of treatment.34
Methods
Participants included male and nonpregnant female veterans with a diagnosed mTBI during post-9/11 military operations; aged 18 to 65 years; reports of persistent (ie, > 3 months in duration) headaches, insomnia, and attention difficulties; and able to read and write English, comprehend what is read, and follow directions. mTBI diagnosis was verified for each veteran via the electronic health record. Patients were excluded if they had a severe TBI diagnosis or impaired decision-making capacity; were unable to comply with study visit schedule; or endorsed active suicidal intent on the Columbia-Suicide Severity Rating Scale.35
Recruitment efforts included: (1) letters sent to eligible veterans with mTBI who were identified by clinical informatics data after waiver of Health Insurance Portability and Accountability Act was obtained; veterans could contact the research team directly or the research team would call the veteran 2 weeks after the letter was sent; (2) veterans could be referred by a clinician; and (3) veterans could self-refer based on flyers and other study marketing materials.
The study was conducted from 2019 to 2024 at Spark M. Matsunaga VA Medical Center, in Honolulu, Hawaii. Four private research spaces in compliance with human research standards were used for consent, treatment, and assessment.
Consenting Procedure and Randomization
The privacy rights of potential participants were observed, and interested veterans who met the eligibility criteria underwent an informed consent procedure and were administered the Columbia-Suicide Severity Rating Scale.35 Those veterans not indicating active suicidal intent were randomized into the intervention or control group. Once randomized, the participant was enrolled and scheduled for baseline assessment.
All procedures of this study were performed in adherence with relevant laws and institutional guidelines. The study was reviewed and approved by the VA Pacific Islands Health Care System Institutional Review Board (#2019-06-JC/Promise 0003).
Outcome Measures
The outcome measures were administered at baseline, midpoint (3-7 weeks), end of treatment (6-12 weeks), and at a 2-month follow-up appointment with the research assistant or project coordinator.
The primary outcome measures included the Headache Impact Test (HIT-6), TBIQOL Headache Pain item short form, Insomnia Severity Index (ISI), Quality of Life in Neurological Disorders (Neuro-QOL) Sleep Disturbance short form, and attention measure: QIKtest Continuous Performance Test (QIKtest) (Table 1).36-44
Secondary outcome measures included QOL After Brain Injury (QOLIBRI), Neuro- QOL Satisfaction With Roles/Activities short form (Neuro-QOL Satisfaction), Neuro-QOL Ability to Participate in Roles/Activities short form (Neuro-QOL Participate), Depression Anxiety Stress Scales (DASS-21), Patient Health Questionnaire-9 (PHQ-9), Posttraumatic Stress Disorder (PTSD) Checklist for DSM-5 (PCL-5), and the General Symptom Inventory (eAppendix 1).39,42,45-52
Sample
Seventy-two participants (36 in each group) were needed to have adequate statistical power for the analysis. Presuming attrition, the goal was to recruit 100 veterans. Literature on NFB studies of patients with mTBI have reported dropout rates ranging from 10% to 30%.53,54 Assuming a dropout rate of 28% and a moderate autocorrelation of 0.6 among repeated measures, this sample size ensured the detection of an average difference of at least 0.49 SDs with a power of 80% in the NFB intervention group compared with the control group using a 2-tailed significance level of 0.05.
Control Group
Following baseline assessment, control group participants received 8 phone calls (1 call/wk) from 1 of 4 clinical investigators over 8 to 10 weeks. During each 15-minute call, 1 of the following health topics was discussed: sleep hygiene, basic nutritional concepts, beverage choices, positive thinking, thought reframing, fitness, daily calming activity, and enhancement of focus strategies. A script for each topic was used to guide each call.
Intervention Group
Following baseline assessment, intervention group participants completed 20 half-hour ILF NFB sessions, typically receiving 3 sessions per week over an 8- to 10-week period. ILF NFB treatments were administered by 1 of 4 licensed health care employees who had received substantial ILF NFB training and achieved a skill reliability index score of 0.95, ensuring the skill level of the ILF NFB providers was equal. A script was used by the ILF NFB providers during the ILF NFB sessions to keep the interaction approach consistent with all participants.
All procedures were explained in advance to participants and voluntary participation affirmed. At the first session, participants filled out a clinical symptom checklist of 5 symptoms (eAppendix 1).39,42,45-49 The initial rating on the symptom checklist was reflective of their experience over the past month, while in each subsequent session, participants indicated their experience of those symptoms that day. ILF NFB providers were never privy to participants’ primary or secondary outcome measures data during the study, so these recurring clinical symptom checklist ratings, as well as other feedback provided by participants on their experience within and between sessions, were the clinical data used to make decisions about ILF NFB treatment protocol.
The Othmer Optimal Response Frequency (ORF) protocol was used for participants in this study.55 Through an iterative process, ORF protocol establishes the specific frequency point along the 0.000001 mHz to 0.1 Hz continuum, which is optimal to diminish symptoms experienced in real-time during the session (eg, tension or pain in shoulders; racing thoughts).
During each ILF NFB session, participants were seated comfortably and encouraged to look at the feedback screen. The moving images on the game screen provided almost instantaneous feedback (within 500 ms) to participants about their brain functioning, as ascertained by electrodes placed on the scalp as dictated by study protocol.56 A standardized protocol for site placement was used beginning with T3-T4, followed by the weekly addition of a site as tolerated in the following sequence: T4-P4, FP2-T4, and FP1-T4. More information about the ILF NFB procedures are outlined in the report of the pilot study and RCT initial results.22,34
Statistical Analysis
Eighty-seven participants were randomized, with 43 assigned to the intervention group and 44 to the control group to achieve the enrollment goal of ≥ 36 participants in each group. This report is the second analysis of data from this RCT that employed a per-protocol approach, analyzing a subset of participants who fully adhered to the study protocol and completed all study procedures. Outcome scores at baseline, midpoint, end of treatment, and 2-month follow-up were summarized as means with corresponding 95% CIs. Group comparisons at the end of treatment and 2-month follow-up time points were conducted using 2-sample t tests. All statistical tests were 2-sided with a significance level of .05 (Type I error rate). SAS software version 9.4 Maintenance 8 was used for statistical analysis. Cohen d analyses were used for effect sizes.
Results
Seventy-four participants fully adhered to the study protocol and were included in the present analyses, with 38 in the control group and 36 in the intervention group. eAppendix 2 depicts the flow of participants through this study. There were no adverse events related to treatment, and the 13 participants who withdrew typically reported difficulty with scheduling or transportation as the primary reason. This study also took place during the COVID-19 pandemic, which likely had some impact on enrollment; participants were differentially impacted by changes in employment and moves to the continental US.
Participants were aged 30 to 60 years (mean [SD], 45.4 [8.0]). Most participants (90.5%) were male, and multiracial and White were the most common racial identities (Table 2). Participant characteristics were largely balanced across randomized groups. Similarly, test scores on the primary variables of interest in this study and secondary clinical variables assessed were comparable across participants (Table 3).
Primary Variables of Interest Analyses
This study’s hypothesis was that those who completed ILF NFB treatment per protocol would demonstrate statistically significant improvement in symptoms related to headaches, sleep disturbance, and difficulty with attention when compared with veterans in the control group. This hypothesis was partially supported. A 2-sample t test showed that veterans in the intervention group demonstrated significant improvement in headache symptoms compared with veterans in the control group on the HIT-6 at the end-of-treatment (P < .001, d = 1.53) and 2-month follow-up assessment (P < .001, d = 1.14). This pattern also was consistent with the TBI-QOL Headache Pain item short form, with veterans in the intervention group showing improvement beyond those in the control group at the end-of-treatment (P < .001, d = 0.89) and 2-month follow-up assessment (P < .001, d = 0.83). Two-sample t tests also demonstrated significant improvement in subjective reports of sleep; those in the intervention group had significantly lower scores on the ISI at the end-of-study (P < .001, d = 1.53) and 2-month follow-up assessment (P < .001, d = 0.97). This pattern also held true for the Neuro-QOL Sleep Disturbance short form subtest, which demonstrated significantly more improvement in the intervention group compared with the control group at the end-of-study (P < .001, d = 0.97) and 2-month follow- up assessment (P < .001, d = 0.92). improvement in attention was not supported by the present results. A 2-sample t test found no significant difference between performance on the QIKtest for veterans in the intervention group vs the control group at the end-of-study (P = .40, d = 0.19) or the 2-month follow-up (P = .43, d = 0.20) (eAppendix 3).
Secondary Variables of Interest Analysis
Secondary variables examined differences in QOL, PTSD, depressive symptoms, and general symptoms reported between veterans in the intervention and control groups. Results demonstrated that veterans in the intervention group showed improvement above and beyond those in the control group on all measures. In regard to QOL, veterans in the intervention group had significantly higher scores on the Neuro-QOL Participate subtest than those in the control group at the end-of-study (P = .01, d = 0.89) and 2-month follow-up assessment (P < .001, d = 0.62). A similar pattern was found for the Neuro-QOL Satisfaction subtest, with veterans in the intervention group showing significantly higher scores than those in the control group at the end-of-study (P = .001, d = 0.95) and 2-month follow-up assessment (P < .001, d = 0.62). This also held true on the QOLIBRI, with veterans in the intervention group demonstrating significantly higher scores than those in the control group at the end-of-study (P = .001, d = 0.92) and 2-month follow-up assessment (P < .001, d = 0.66).
Veterans in the intervention group had significantly lower scores on the PCL-5 than those in the control group at the end-of- study (P = .003, d = 0.78) and 2-month follow-up assessment (P = .001, d = 0.72). Veterans in the intervention group also had significantly lower scores on the PHQ-9 than those in the control group at the end-of-study (P < .001, d = 0.98) and 2-month follow-up assessment (P < .001, d = 0.83). Veterans in the intervention group had significantly lower scores on the DASS- 21 than those in the control group at the end-of-study (P = .002, d = 0.80) and 2-month follow-up assessment (P = .001, d = 0.77). They also had significantly lower scores on the General Symptom Inventory than those in the control group at the end-of-study (P = .02, d = 0.75) and 2-month follow-up assessment (P = .002, d = 0.57). A clinically significant shift of score occurred for each of the measures except DASS-21 (eAppendix 3). eAppendix 4 depicts the change in scores for the intervention group at the end of treatment and the clinically significant shift score of each measure.
Discussion
The results of this RCT revealed a promising impact of ILF NFB on the commonly experienced persistent PCSs of headaches and disrupted sleep. Veterans in the intervention group demonstrated statistically significant improvement in headache symptoms compared with veterans in the control group when assessed at the end of treatment and during a 2-month follow-up. The statistical significance of these improvements was also supported by large or very large effect sizes. In addition to these primary variables of interest, veterans in the intervention group notably demonstrated significant improvement compared with those in the control group in a number of secondary clinical measures, including QOL, traumatic stress-related symptoms, depressive symptoms, and general symptom report. The clinical impact was further supported by the clinically relevant shift in scores in the intervention group.
The data did not support the hypothesis that attention concerns would show significant improvement following ILF NFB. Performance on an attention measure did not differ significantly between groups at either the end-of-treatment or 2-month follow up assessment. The QIKtest, a continuous performance test used to measure attention, was a go/no-go task and calculated based on a combination of various types of errors and outlier responses. The stimulus for this task is a series of computerized, blinking lights, for which participants are tasked with discriminating targets and nontargets under time pressure. However, the order of the stimuli are consistent across administrations, rather than being randomized, introducing a potential confound of practice effects on this task since patients were administered the QIKtest 3 times in a 2-month period and again 2 months later. Veterans in the control group notably improved in their average performance of this task from baseline to the endpoint of their treatment participation and demonstrated further improvement at the 2-month follow-up assessment; this pattern would be consistent with potential practice effects and warrants caution in its interpretation for both groups.
Previously published ILF NFB clinical studies that used the QIKtest and found positive results were mostly conducted among children and teen populations across longer treatment periods. This research may indicate the QIKtest is not an appropriate measure to assess adults who have specialized training in responding to stimuli (ie, trained military personnel). This suggests the concept of attention dysfunction experienced by veterans and the best method to measure it may need to be explored further. This construct may not be related to the focus and skill in prolonged attention needed in selecting go/ no-go tasks, but rather related to a broader conceptual basis involving memory, recall, clarity of rational thought, and decision making impacted by the mTBI. For instance, a study among combat veterans with mTBI and PTSD found that performance on objective cognitive measures did not significantly correlate with their subjective reports of cognitive difficulties.57 This reflects the pattern of the present study, in which subjective reports of attention improved over time on the clinical symptom checklist filled out by participants at each session, but the objective measure did not. The mean attention dysfunction score was 6 at session 1 and 1 to 2 at session 20 (lower scores are better on a 10-point scale).
Strengths and Limitations
This study presents results stemming from the first RCT examining clinical effectiveness of ILF NFB in a VA setting for veterans with diagnoses of mTBI. The study design shows promising external validity. Veterans were able to participate in a treatment consisting of 20 sessions over a period of typically 8 to 10 weeks, entailing 2 to 3 sessions per week, with an attrition of only 18% over the course of the study. Notably, attrition rates may have been impacted by the time course of the study, which was recruiting and running participants throughout the COVID-19 pandemic (March 2020 to May 2023). No attrition was due to the intervention itself, and no adverse reactions to ILF NFB were reported during the course of the study. Other strengths of the study include the ethnically and racially diverse participants, representative of the population of veterans in Hawaii. Additionally, all ILF NFB providers underwent supervised ILF NFB training and achieved a skill reliability index score of 0.95 prior to providing ILF NFB to the intervention group.
This study was not blinded. Neither veterans nor ILF NFB clinicians were blinded and were therefore aware of the randomly assigned groups. Research assistants administering the periodic assessments were meant to be blinded to condition by design; however, as the study progressed, a research assistant became unintentionally aware of each study participant's condition based on required documentation in the veteran’s health records; more notes were present for those in the intervention group (20 specialist notes) than the control group (8 notes). While the presence of a control group represents a strength relative to much of the existing ILF NFB literature, the control group in this case did not account for the total time spent with the researchers. Participants in the intervention group met with researchers for 20 total sessions as opposed to 8 telephone calls. Therefore, the study design cannot fully rule out the differential impact of demand characteristics between the 2 groups, nor can it fully address or rule out the impact of differential motivation and expectations between groups. There is also evidence that technological innovation can influence the expectations of research participants, meaning that the intervention group may have been unduly influenced by the novelty of the ILF NFB technology, to which the control group did not have exposure.58
A second attention measure for this study would have been beneficial, perhaps in identifying true change in attention ability or providing more insight into finding better methods to assess attention among veterans with mTBI. ILF NFB demonstrated significant impact across multiple outcome measures of clinical relevance for veterans diagnosed with mTBI, including the primary outcome variables of headache and sleep. The strength of the improvements seen in these areas, supported by large practical effects as well as veterans’ subjective reports, indicates much promise. Follow-up studies may also focus on the potential effectiveness of ILF NFB as a treatment of the secondary concerns measured in this study, including traumatic stress-related and depressive symptoms, and may explore the added benefit, if any, of ILF NFB alongside other evidence-based treatments for traumatic stress-related and mood disorders (eg, cognitive behavioral therapy). Using functional magnetic resonance imaging before and after assessments to determine actual brain enhancement with ILF NFB for certain disorders in which a brain signature exists (ie, migraine) should be explored. Further examination of ILF NFB as an intervention for attention may also be warranted, using more effective measures of attention in the population of veterans with mTBI, given the concerns noted earlier. Future research on this topic will need to clearly define attention in relation to the veteran experience and use relevant measures.
Conclusions
This study supports ILF NFB as a safe, noninvasive, nonpharmacologic treatment that may be effective in addressing the complex clinical concerns of veterans diagnosed with mTBI, a population for whom effective treatments have been difficult to identify. This intervention can provide veterans with a desirable and effective nonpharmacologic alternative in their care.
Traumatic brain injury (TBI) is the signature injury of post-9/11 military operations, impacting > 441,000 combat veterans from 2001 to 2021 and 87% diagnosed with mild TBI (mTBI).1,2 The most common cause of mTBI during these operations was blast exposures stemming from improvised explosive devices, rocket-propelled grenades, or land mines. mTBI was once thought to be self-limiting, lasting hours or days postinjury, but is now recognized as a complex focal and diffuse injury causing a cascade of molecular and biochemical responses with significant physiologic effects lasting for a longer duration. A significant number of combat veterans with mTBI (23%-48%) experience long-standing postconcussive symptoms (PCSs) for many years postinjury.3-5
Developing and implementing strategies to reduce persistent symptoms associated with mTBI is of critical importance. Veterans diagnosed with mTBI and experiencing PCSs present ongoing treatment challenges to the health care system due to limited or suboptimal treatment options.6,7 According to the 2021 US Department of Veterans Affairs (VA) and US Department of Defense (DoD) clinical guidelines for postacute mTBI, treatment for PCSs should be symptom focused. 8,9 For instance, veterans with migraine headaches associated with mTBIs are often treated with abortive agents (eg, triptans) and preventive medications (eg, anticonvulsants and tricyclics).10 Cognitive dysfunction and insomnia are treated with cognitive rehabilitation programs, cognitive behavioral therapy, occupational therapy, and medications (eg, hypnotics for insomnia).11,12 The 2021 VA/DoD guidelines note that veteran and military focus groups described greater success with nonpharmacologic treatments than with pharmacologic treatments.8 The VA launched an enterprise-wide Whole Health Service program with the requirement that complementary and integrative health approaches must be available to veterans.13 As a nonpharmacologic, integrative, and noninvasive modality, neurofeedback (NFB) supports the VA Whole Health initiative and veterans’ preferences for integrative treatments.14
Neurofeedback
Rather than a symptom management approach, Defina et al described the possibilities of brain repair in TBI by treatments to enhance neuroplasticity, thereby establishing a more normalized or stable brain environment and enabling the brain to reorganize itself and function more normally.15 NFB has been shown to influence neuroplasticity,16 as evident in microstructural changes in white and gray matter17 and its ability to contribute to functional rehabilitation by restoring connectivity in specific areas of the brain that may have been impaired.18 The benefits of neuroenhancement strategies include potentially reduced pain for patients with mTBI and improved quality of life (QOL).19
NFB assists individuals by helping them become more aware of and self-regulate their physiology.20,21 Because there are several types of NFB (eg, quantitative electroencephalography, Z-scored, α-θ) that differ in terms of equipment, mechanism of action, focus, and patient and clinician procedures, it is important to note that this study used a novel technologically advanced form of NFB, referred to as infra-low frequency (ILF) NFB. It works by reflecting a person’s brain wave activity via conventional electroencephalography back to the person through the visual cortex, thus providing relevant information to which the brain responds to improve core state regulation.22
In 2006, ILF NFB developers sought to extend NFB capability into the slow cortical potential domain (< 0.1 Hz) and then gradually extended to lower frequencies on the basis of favorable clinical responses.22,23 In 2017, the technology reached an ILF capacity that appeared to be helpful for several clinical issues. These developments depended on instrumentation capable of low noise signal detection down to the lowest frequency of interest. Instrumentation was developed for the purpose (eg, Bee Medic Cygnet NFB).
Although mTBI has been a clinical focus in NFB since the 1980s, there are few published studies demonstrating the efficacy of ILF NFB relating to the PCSs of interest in this study, and 2 suggested ILF NFB positively affected change in PCS severity.24,25 Other studies found that ILF NFB decreased incidence of migraines and tension type headaches.26,27 However, the findings of these studies had limited generalizability due to methodologic limitations, such as selection bias and small sample sizes.24-27 Of importance to this article, there are also several publications on the efficacy of ILF NFB in clinical settings.28-33
This article presents the second analysis of data from veterans who completed ILF NFB intervention and control group procedures during a 5-year randomized controlled trial (RCT). The RCT included veterans who experienced an mTBI while participating in post-9/11 military operations to evaluate the impact of ILF NFB on chronic PCSs, including headache, insomnia, and attention dysfunction. Initial results of this trial demonstrated significant differences between the intervention and control groups with strong effect sizes on all outcome measures at the end of treatment.34
Methods
Participants included male and nonpregnant female veterans with a diagnosed mTBI during post-9/11 military operations; aged 18 to 65 years; reports of persistent (ie, > 3 months in duration) headaches, insomnia, and attention difficulties; and able to read and write English, comprehend what is read, and follow directions. mTBI diagnosis was verified for each veteran via the electronic health record. Patients were excluded if they had a severe TBI diagnosis or impaired decision-making capacity; were unable to comply with study visit schedule; or endorsed active suicidal intent on the Columbia-Suicide Severity Rating Scale.35
Recruitment efforts included: (1) letters sent to eligible veterans with mTBI who were identified by clinical informatics data after waiver of Health Insurance Portability and Accountability Act was obtained; veterans could contact the research team directly or the research team would call the veteran 2 weeks after the letter was sent; (2) veterans could be referred by a clinician; and (3) veterans could self-refer based on flyers and other study marketing materials.
The study was conducted from 2019 to 2024 at Spark M. Matsunaga VA Medical Center, in Honolulu, Hawaii. Four private research spaces in compliance with human research standards were used for consent, treatment, and assessment.
Consenting Procedure and Randomization
The privacy rights of potential participants were observed, and interested veterans who met the eligibility criteria underwent an informed consent procedure and were administered the Columbia-Suicide Severity Rating Scale.35 Those veterans not indicating active suicidal intent were randomized into the intervention or control group. Once randomized, the participant was enrolled and scheduled for baseline assessment.
All procedures of this study were performed in adherence with relevant laws and institutional guidelines. The study was reviewed and approved by the VA Pacific Islands Health Care System Institutional Review Board (#2019-06-JC/Promise 0003).
Outcome Measures
The outcome measures were administered at baseline, midpoint (3-7 weeks), end of treatment (6-12 weeks), and at a 2-month follow-up appointment with the research assistant or project coordinator.
The primary outcome measures included the Headache Impact Test (HIT-6), TBIQOL Headache Pain item short form, Insomnia Severity Index (ISI), Quality of Life in Neurological Disorders (Neuro-QOL) Sleep Disturbance short form, and attention measure: QIKtest Continuous Performance Test (QIKtest) (Table 1).36-44
Secondary outcome measures included QOL After Brain Injury (QOLIBRI), Neuro- QOL Satisfaction With Roles/Activities short form (Neuro-QOL Satisfaction), Neuro-QOL Ability to Participate in Roles/Activities short form (Neuro-QOL Participate), Depression Anxiety Stress Scales (DASS-21), Patient Health Questionnaire-9 (PHQ-9), Posttraumatic Stress Disorder (PTSD) Checklist for DSM-5 (PCL-5), and the General Symptom Inventory (eAppendix 1).39,42,45-52
Sample
Seventy-two participants (36 in each group) were needed to have adequate statistical power for the analysis. Presuming attrition, the goal was to recruit 100 veterans. Literature on NFB studies of patients with mTBI have reported dropout rates ranging from 10% to 30%.53,54 Assuming a dropout rate of 28% and a moderate autocorrelation of 0.6 among repeated measures, this sample size ensured the detection of an average difference of at least 0.49 SDs with a power of 80% in the NFB intervention group compared with the control group using a 2-tailed significance level of 0.05.
Control Group
Following baseline assessment, control group participants received 8 phone calls (1 call/wk) from 1 of 4 clinical investigators over 8 to 10 weeks. During each 15-minute call, 1 of the following health topics was discussed: sleep hygiene, basic nutritional concepts, beverage choices, positive thinking, thought reframing, fitness, daily calming activity, and enhancement of focus strategies. A script for each topic was used to guide each call.
Intervention Group
Following baseline assessment, intervention group participants completed 20 half-hour ILF NFB sessions, typically receiving 3 sessions per week over an 8- to 10-week period. ILF NFB treatments were administered by 1 of 4 licensed health care employees who had received substantial ILF NFB training and achieved a skill reliability index score of 0.95, ensuring the skill level of the ILF NFB providers was equal. A script was used by the ILF NFB providers during the ILF NFB sessions to keep the interaction approach consistent with all participants.
All procedures were explained in advance to participants and voluntary participation affirmed. At the first session, participants filled out a clinical symptom checklist of 5 symptoms (eAppendix 1).39,42,45-49 The initial rating on the symptom checklist was reflective of their experience over the past month, while in each subsequent session, participants indicated their experience of those symptoms that day. ILF NFB providers were never privy to participants’ primary or secondary outcome measures data during the study, so these recurring clinical symptom checklist ratings, as well as other feedback provided by participants on their experience within and between sessions, were the clinical data used to make decisions about ILF NFB treatment protocol.
The Othmer Optimal Response Frequency (ORF) protocol was used for participants in this study.55 Through an iterative process, ORF protocol establishes the specific frequency point along the 0.000001 mHz to 0.1 Hz continuum, which is optimal to diminish symptoms experienced in real-time during the session (eg, tension or pain in shoulders; racing thoughts).
During each ILF NFB session, participants were seated comfortably and encouraged to look at the feedback screen. The moving images on the game screen provided almost instantaneous feedback (within 500 ms) to participants about their brain functioning, as ascertained by electrodes placed on the scalp as dictated by study protocol.56 A standardized protocol for site placement was used beginning with T3-T4, followed by the weekly addition of a site as tolerated in the following sequence: T4-P4, FP2-T4, and FP1-T4. More information about the ILF NFB procedures are outlined in the report of the pilot study and RCT initial results.22,34
Statistical Analysis
Eighty-seven participants were randomized, with 43 assigned to the intervention group and 44 to the control group to achieve the enrollment goal of ≥ 36 participants in each group. This report is the second analysis of data from this RCT that employed a per-protocol approach, analyzing a subset of participants who fully adhered to the study protocol and completed all study procedures. Outcome scores at baseline, midpoint, end of treatment, and 2-month follow-up were summarized as means with corresponding 95% CIs. Group comparisons at the end of treatment and 2-month follow-up time points were conducted using 2-sample t tests. All statistical tests were 2-sided with a significance level of .05 (Type I error rate). SAS software version 9.4 Maintenance 8 was used for statistical analysis. Cohen d analyses were used for effect sizes.
Results
Seventy-four participants fully adhered to the study protocol and were included in the present analyses, with 38 in the control group and 36 in the intervention group. eAppendix 2 depicts the flow of participants through this study. There were no adverse events related to treatment, and the 13 participants who withdrew typically reported difficulty with scheduling or transportation as the primary reason. This study also took place during the COVID-19 pandemic, which likely had some impact on enrollment; participants were differentially impacted by changes in employment and moves to the continental US.
Participants were aged 30 to 60 years (mean [SD], 45.4 [8.0]). Most participants (90.5%) were male, and multiracial and White were the most common racial identities (Table 2). Participant characteristics were largely balanced across randomized groups. Similarly, test scores on the primary variables of interest in this study and secondary clinical variables assessed were comparable across participants (Table 3).
Primary Variables of Interest Analyses
This study’s hypothesis was that those who completed ILF NFB treatment per protocol would demonstrate statistically significant improvement in symptoms related to headaches, sleep disturbance, and difficulty with attention when compared with veterans in the control group. This hypothesis was partially supported. A 2-sample t test showed that veterans in the intervention group demonstrated significant improvement in headache symptoms compared with veterans in the control group on the HIT-6 at the end-of-treatment (P < .001, d = 1.53) and 2-month follow-up assessment (P < .001, d = 1.14). This pattern also was consistent with the TBI-QOL Headache Pain item short form, with veterans in the intervention group showing improvement beyond those in the control group at the end-of-treatment (P < .001, d = 0.89) and 2-month follow-up assessment (P < .001, d = 0.83). Two-sample t tests also demonstrated significant improvement in subjective reports of sleep; those in the intervention group had significantly lower scores on the ISI at the end-of-study (P < .001, d = 1.53) and 2-month follow-up assessment (P < .001, d = 0.97). This pattern also held true for the Neuro-QOL Sleep Disturbance short form subtest, which demonstrated significantly more improvement in the intervention group compared with the control group at the end-of-study (P < .001, d = 0.97) and 2-month follow- up assessment (P < .001, d = 0.92). improvement in attention was not supported by the present results. A 2-sample t test found no significant difference between performance on the QIKtest for veterans in the intervention group vs the control group at the end-of-study (P = .40, d = 0.19) or the 2-month follow-up (P = .43, d = 0.20) (eAppendix 3).
Secondary Variables of Interest Analysis
Secondary variables examined differences in QOL, PTSD, depressive symptoms, and general symptoms reported between veterans in the intervention and control groups. Results demonstrated that veterans in the intervention group showed improvement above and beyond those in the control group on all measures. In regard to QOL, veterans in the intervention group had significantly higher scores on the Neuro-QOL Participate subtest than those in the control group at the end-of-study (P = .01, d = 0.89) and 2-month follow-up assessment (P < .001, d = 0.62). A similar pattern was found for the Neuro-QOL Satisfaction subtest, with veterans in the intervention group showing significantly higher scores than those in the control group at the end-of-study (P = .001, d = 0.95) and 2-month follow-up assessment (P < .001, d = 0.62). This also held true on the QOLIBRI, with veterans in the intervention group demonstrating significantly higher scores than those in the control group at the end-of-study (P = .001, d = 0.92) and 2-month follow-up assessment (P < .001, d = 0.66).
Veterans in the intervention group had significantly lower scores on the PCL-5 than those in the control group at the end-of- study (P = .003, d = 0.78) and 2-month follow-up assessment (P = .001, d = 0.72). Veterans in the intervention group also had significantly lower scores on the PHQ-9 than those in the control group at the end-of-study (P < .001, d = 0.98) and 2-month follow-up assessment (P < .001, d = 0.83). Veterans in the intervention group had significantly lower scores on the DASS- 21 than those in the control group at the end-of-study (P = .002, d = 0.80) and 2-month follow-up assessment (P = .001, d = 0.77). They also had significantly lower scores on the General Symptom Inventory than those in the control group at the end-of-study (P = .02, d = 0.75) and 2-month follow-up assessment (P = .002, d = 0.57). A clinically significant shift of score occurred for each of the measures except DASS-21 (eAppendix 3). eAppendix 4 depicts the change in scores for the intervention group at the end of treatment and the clinically significant shift score of each measure.
Discussion
The results of this RCT revealed a promising impact of ILF NFB on the commonly experienced persistent PCSs of headaches and disrupted sleep. Veterans in the intervention group demonstrated statistically significant improvement in headache symptoms compared with veterans in the control group when assessed at the end of treatment and during a 2-month follow-up. The statistical significance of these improvements was also supported by large or very large effect sizes. In addition to these primary variables of interest, veterans in the intervention group notably demonstrated significant improvement compared with those in the control group in a number of secondary clinical measures, including QOL, traumatic stress-related symptoms, depressive symptoms, and general symptom report. The clinical impact was further supported by the clinically relevant shift in scores in the intervention group.
The data did not support the hypothesis that attention concerns would show significant improvement following ILF NFB. Performance on an attention measure did not differ significantly between groups at either the end-of-treatment or 2-month follow up assessment. The QIKtest, a continuous performance test used to measure attention, was a go/no-go task and calculated based on a combination of various types of errors and outlier responses. The stimulus for this task is a series of computerized, blinking lights, for which participants are tasked with discriminating targets and nontargets under time pressure. However, the order of the stimuli are consistent across administrations, rather than being randomized, introducing a potential confound of practice effects on this task since patients were administered the QIKtest 3 times in a 2-month period and again 2 months later. Veterans in the control group notably improved in their average performance of this task from baseline to the endpoint of their treatment participation and demonstrated further improvement at the 2-month follow-up assessment; this pattern would be consistent with potential practice effects and warrants caution in its interpretation for both groups.
Previously published ILF NFB clinical studies that used the QIKtest and found positive results were mostly conducted among children and teen populations across longer treatment periods. This research may indicate the QIKtest is not an appropriate measure to assess adults who have specialized training in responding to stimuli (ie, trained military personnel). This suggests the concept of attention dysfunction experienced by veterans and the best method to measure it may need to be explored further. This construct may not be related to the focus and skill in prolonged attention needed in selecting go/ no-go tasks, but rather related to a broader conceptual basis involving memory, recall, clarity of rational thought, and decision making impacted by the mTBI. For instance, a study among combat veterans with mTBI and PTSD found that performance on objective cognitive measures did not significantly correlate with their subjective reports of cognitive difficulties.57 This reflects the pattern of the present study, in which subjective reports of attention improved over time on the clinical symptom checklist filled out by participants at each session, but the objective measure did not. The mean attention dysfunction score was 6 at session 1 and 1 to 2 at session 20 (lower scores are better on a 10-point scale).
Strengths and Limitations
This study presents results stemming from the first RCT examining clinical effectiveness of ILF NFB in a VA setting for veterans with diagnoses of mTBI. The study design shows promising external validity. Veterans were able to participate in a treatment consisting of 20 sessions over a period of typically 8 to 10 weeks, entailing 2 to 3 sessions per week, with an attrition of only 18% over the course of the study. Notably, attrition rates may have been impacted by the time course of the study, which was recruiting and running participants throughout the COVID-19 pandemic (March 2020 to May 2023). No attrition was due to the intervention itself, and no adverse reactions to ILF NFB were reported during the course of the study. Other strengths of the study include the ethnically and racially diverse participants, representative of the population of veterans in Hawaii. Additionally, all ILF NFB providers underwent supervised ILF NFB training and achieved a skill reliability index score of 0.95 prior to providing ILF NFB to the intervention group.
This study was not blinded. Neither veterans nor ILF NFB clinicians were blinded and were therefore aware of the randomly assigned groups. Research assistants administering the periodic assessments were meant to be blinded to condition by design; however, as the study progressed, a research assistant became unintentionally aware of each study participant's condition based on required documentation in the veteran’s health records; more notes were present for those in the intervention group (20 specialist notes) than the control group (8 notes). While the presence of a control group represents a strength relative to much of the existing ILF NFB literature, the control group in this case did not account for the total time spent with the researchers. Participants in the intervention group met with researchers for 20 total sessions as opposed to 8 telephone calls. Therefore, the study design cannot fully rule out the differential impact of demand characteristics between the 2 groups, nor can it fully address or rule out the impact of differential motivation and expectations between groups. There is also evidence that technological innovation can influence the expectations of research participants, meaning that the intervention group may have been unduly influenced by the novelty of the ILF NFB technology, to which the control group did not have exposure.58
A second attention measure for this study would have been beneficial, perhaps in identifying true change in attention ability or providing more insight into finding better methods to assess attention among veterans with mTBI. ILF NFB demonstrated significant impact across multiple outcome measures of clinical relevance for veterans diagnosed with mTBI, including the primary outcome variables of headache and sleep. The strength of the improvements seen in these areas, supported by large practical effects as well as veterans’ subjective reports, indicates much promise. Follow-up studies may also focus on the potential effectiveness of ILF NFB as a treatment of the secondary concerns measured in this study, including traumatic stress-related and depressive symptoms, and may explore the added benefit, if any, of ILF NFB alongside other evidence-based treatments for traumatic stress-related and mood disorders (eg, cognitive behavioral therapy). Using functional magnetic resonance imaging before and after assessments to determine actual brain enhancement with ILF NFB for certain disorders in which a brain signature exists (ie, migraine) should be explored. Further examination of ILF NFB as an intervention for attention may also be warranted, using more effective measures of attention in the population of veterans with mTBI, given the concerns noted earlier. Future research on this topic will need to clearly define attention in relation to the veteran experience and use relevant measures.
Conclusions
This study supports ILF NFB as a safe, noninvasive, nonpharmacologic treatment that may be effective in addressing the complex clinical concerns of veterans diagnosed with mTBI, a population for whom effective treatments have been difficult to identify. This intervention can provide veterans with a desirable and effective nonpharmacologic alternative in their care.
- Hayward P. Traumatic brain injury: the signature of modern conflicts. Lancet Neurol. 2008;7:200-201. doi:10.1016/S1474-4422(08)70032-2
- Whiteneck G, Williams W, Almeida E, et al. Two decades of Department of Veterans Affairs traumatic brain injury care and benefits for veterans of post-9/11 conflicts. J Head Trauma Rehabil. 2024;39:E462-E469. doi:10.1097/HTR.0000000000000952
- Chapman JC, Diaz-Arrastia R. Military traumatic brain injury: a review. Alzheimers Dement. 2014;10(3 suppl):S97- S104. doi:10.1016/j.jalz.2014.04.012
- Dean PJA, O’Neill D, Sterr A. Post-concussion syndrome: prevalence after mild traumatic brain injury in comparison with a sample without head injury. Brain Inj. 2012;26:14-26. doi:10.3109/02699052.2011.635354
- Agimi Y, Hai T, Gano A, et al. Clinical trajectories of comorbidity associated with military-sustained mild traumatic brain injury: pre- and post-injury. J Head Trauma Rehabil. 2024;39:E564-E575. doi:10.1097/HTR.0000000000000934
- Hoge CW, McGurk D, Thomas JL, et al. Mild traumatic brain injury in U.S. soldiers returning from Iraq. N Engl J Med. 2008;358:453-463. doi:10.1056/NEJMoa072972
- Bogdanova Y, Verfaellie M. Cognitive sequelae of blast-induced traumatic brain injury: recovery and rehabilitation. Neuropsychol Rev. 2012;22:4-20. doi:10.1007/s11065-012-9192-3
- Eapen BC, Bowles AO, Sall J, et al. The management and rehabilitation of post-acute mild traumatic brain injury. Brain Inj. 2022;36:693-702. doi:10.1080/02699052.2022.2033848
- Department of Veterans Affairs (VA) and Department of Defense (DoD). VA/DoD Clinical Practice Guideline for the management and Rehabilitation of Post-Acute Mild Traumatic Brain Injury, 2021, Version 3:1-128. https://www.healthquality.va.gov/HEALTHQUALITY/guidelines/Rehab/mtbi/index.asp
- Patil VK, St Andre JR, Crisan E, et al. Prevalence and treatment of headaches in veterans with mild traumatic brain injury. Headache. 2011;51:1112-1121. doi:10.1111/j.1526-4610.2011.01946.x
- Ayalon L, Borodkin K, Dishon L, Kanety H, Dagan Y. Circadian rhythm sleep disorders following mild traumatic brain injury. Neurology. 2007;68:1136-1140. doi:10.1212/01.wnl.0000258672.52836.30
- Bogdanova Y, Verfaellie M. Cognitive sequelae of blast-induced traumatic brain injury: recovery and rehabilitation, Neuropsychology Review. 2012;22:4-20. doi:10.1007/s11065-012-9192-3
- US Department of Veteran Affairs. VHA Directive 1137.December 13, 2022. https://www.va.gov/VHApublications/ViewPublication.asp?pub_ID=10072
- Taylor SL, Hoggatt KJ, Kligler B. Complementary and integrated health approaches: what do veterans use and want. J Gen Intern Med. 2019;34:1192-1199. doi:10.1007/s11606-019-04862-6
- DeFlna P, Fellus J, Polito MZ, et al. The new neuroscience frontier: promoting neuroplasticity and brain repair in traumatic brain injury. Clin Neuropsychol. 2009;23:1391-1399. doi:10.1080/13854040903058978
- Enriquez-Geppert S, Huster RJ, Herrmann CS. Boosting brain functions: improving executive functions with behavioral training, neurostimulation, and neurofeedback. Int J Psychophysiol. 2013;88:1-16. doi:10.1016/j.ijpsycho.2013.02.001
- Ghaziri J, Tucholka A, Larue V, et al. Neurofeedback training induces changes in white and gray matter. Clin EEG Neurosci. 2013;44:265-272. doi:10.1177/1550059413476031
- Ibric VL, Dragomirescu LG, Hudspeth WJ. Real-time changes in connectivities during neurofeedback. J Neurother. 2009;13:156-165. doi:10.1080/10874200903118378
- Clark VP, Parasuraman R. Neuroenhancement: enhancing brain and mind in health and in disease. Neuroimage. 2014;85:889-894. doi:10.1016/j.neuroimage.2013.08.071
- Larsen S, Sherlin L. Neurofeedback: an emerging technology for treating central nervous system dysregulation. Psychiatr Clin North Am. 2013;36:163-168. doi:10.1016/j.psc.2013.01.005
- Hammond DC. What is neurofeedback: an update. J Neurother. 2011; 15:305-336. doi:10.1080/10874208.2011.623090
- Othmer S. Endogenous neuromodulation at infra-low frequencies. In: Chartier DR, Dellinger MB, Evans JR, Budzynski HK, eds. Introduction to Quantitative EEG and Neurofeedback. 3rd ed. Academic Press; 2023:283-299. doi:10.1016/B978-0-323-89827-0.00001-2
- Othmer SF. History of the Othmer Method: an evolving clinical model and process. In: Evans JR, Dellinger MB, Russell HL, eds. Neurofeedback: The First Fifty Years. Academic Press; 2020:327-334. doi:10.1016/B978-0-12-817659-7.00043-9
- Legarda SB, Lahti CE, McDermott D, Michas-Martin A. Use of novel concussion protocol with infralow frequency neuromodulation demonstrates significant treatment response in patients with persistent postconcussion symptoms, a retrospective study. Front Hum Neurosci. 2022;16:894758. doi:10.3389/fnhum.2022.894758
- Carlson J, Ross GW. Neurofeedback impact on chronic headache, sleep, and attention disorders experienced by veterans with mild traumatic brain injury: a pilot study. Biofeedback. 2021;49:2-9. doi:10.5298/1081-5937-49.01.01
- Dobrushina O, Arina G, Osina E, Aziatskaya G. Clinical and psychological confirmation of stabilizing effect of neurofeedback in migraine. Eur Psychiatry. 2017;41:S253-S253. doi:10.1016/j.eurpsy.2017.02.045
- Arina GA, Dobrushina OR, Shvetsova ET, et al. Infra-low frequency neurofeedback in tension-type headache: a cross-over sham-controlled study. Front Hum Neurosci. 2022;16:891323. doi:10.3389/fnhum.2022.891323
- Kirk HW, Dahl MG. Infra low frequency neurofeedback training for trauma recovery: a case report. Front Hum Neurosci. 2022;16:905823. doi:10.3389/fnhum.2022.905823
- Benson A, LaDou T. The use of neurofeedback for combat veterans with post-traumatic stress. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. CRC Press; 2015.
- Legarda SB, McMahon D, Othmer S, Othmer S. Clinical neurofeedback: case studies, proposed mechanism, and implications for pediatric neurology practice. J Child Neurol. 2011;26:1045-1051. doi:10.1177/0883073811405052
- McMahon DE. Notes from clinical practice: an MD’s perspective on 9 years of neurofeedback practice. Semin Pediatr Neurol. 2013;20:258-260. doi:10.1016/j.spen.2013.10.007
- Othmer S, Othmer SF. Post traumatic stress disorder— the neurofeedback remedy. Biofeedback. 2009;37:24-31. doi:10.5298/1081-5937-37.1.24
- Shapero E, Prager J. ILF Neurofeedback and alpha-theta training in a multidisciplinary chronic pain program. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. 2nd ed. Routledge; 2020:223-243.
- Carlson J, Ross G, Tyrrell C, et al. Infra-low frequency neurofeedback impact on post-concussive symptoms of headache, insomnia and attention disorder: results of a randomized control trial. Explore (NY). 2025;21:103137. doi:10.1016/j.explore.2025.103137
- Posner K, Brown GK, Stanley B, et al. The Columbia– Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011;168:1266- 1277. doi:10.1176/appi.ajp.2011.10111704
- Kosinski M, Bayliss MS, Bjorner JB, et al. A six-item short-form survey for measuring headache impact: the HIT-6. Qual Life Res. 2003;12:963-974. doi:10.1023/a:1026119331193
- Coeytaux RR, Kaufman JS, Chao R, Mann JD, Devellis RF. Four methods of estimating the minimal important difference score were compared to establish a clinically significant change in Headache Impact Test. J Clin Epidemiol. 2006;59:374-380. doi:10.1016/j.jclinepi.2005.05.010
- Tulsky DS, Tyner CE, Boulton AJ, et al. Development of the TBI-QOL Headache Pain Item Bank and Short Form. J Head Trauma Rehabil. 2019;34:298-307. doi:10.1097/HTR.0000000000000532
- Poritz JMP, Sherer M, Kisala MA, et al. Responsiveness of the Traumatic Brain Injury-Quality of Life (TBI-QOL) measurement system. Arch Phys Med Rehabil. 2020;101:54- 61. doi:10.1016/j.apmr.2017.11.018
- Bastien CH, Vallières A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001;2:297-307. doi:10.1016/s1389-9457(00)00065-4
- Yang M, Morin CM, Schaefer M, Wallenstein GV. Interpreting score differences in the Insomnia Severity Index: using health-related outcomes to define the minimally important difference. Curr Med Res Opin. 2009;25:2487-2494. doi:10.1185/03007990903167415
- Cella D, Lai J-S, Nowinski CJ, et al. Neuro-QOL Brief measures of health-related quality of life for clinical research in neurology. Neurology. 2012;78:1860-1867. doi:10.1212/WNL.0b013e318258f744
- Kozlowski AJ, Cella D, Nitsch KP, Heinemann AW. Evaluating individual change with the Quality of Life in Neurological Disorders (Neuro-QoL) short forms. Arch Phys Med Rehabil. 2016;97:650-654.e8. doi:10.1016/j.apmr.2015.12.010
- Versace M. QIKTest Report on EEG Expert: introduction and overview. 2014. Accessed February 24, 2026. https://media.voog.com/0000/0044/8343/files/EEGexpert_manual_newreport2014_EN.pdf
- Truelle J-L, Koskinen S, Hawthorne G, et al. Quality of life after traumatic brain injury: the clinical use of the QOLIBRI, a novel disease-specific instrument. Brain Inj. 2010;24:1272-1291. doi:10.3109/02699052.2010.506865
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606-613. doi:10.1046/j.1525-1497.2001.016009606.x
- Kroenke K. Enhancing the clinical utility of depression screening. CMAJ. 2012;184:281-282. doi:10.1503/cmaj.112004
- Weathers FW, Litz BT, Keane TM, et al. PTSD checklist for DSM-5 (PCL-5). National Center for PTSD. Updated September 10, 2025. Accessed February 24, 2026. https:// www.ptsd.va.gov/professional/assessment/adult-sr/ptsd-checklist.asp
- Henry JD, Crawford JR. The short]form version of the Depression Anxiety Stress Scales (DASS]21): construct validity and normative data in a large non]clinical sample. Br J Clin Psychol. 2005;44:227-239. doi:10.1348/014466505X29657
- Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther. 1995;33(3):335-343. doi:10.1016/0005-7967(94)00075-u
- Ronk FR, Korman JR, Hooke GR, Page AC. Assessing clinical significance of treatment outcomes using the DASS-21. Psychol Assess. 2013;25:1103-1110. doi:10.1037/a0033100
- Carlson J. General symptom inventory. Description published online 2021.
- Nelson DV, Esty ML. Neurotherapy of traumatic brain injury/ posttraumatic stress symptoms in OEF/OIF veterans. J Neuropsychiatry Clin Neurosci. 2012;24:237-240. doi:10.1176/appi.neuropsych.11020041
- Zoefel B, Huster RJ, Herrmann CS. Neurofeedback training of the upper alpha frequency band in EEG improves cognitive performance. Neuroimage. 2011;54:1427-1431. doi:10.1016/j.neuroimage.2010.08.078
- Othmer S, Othmer S. Toward a theory of infra-low frequency neurofeedback. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. 2nd ed. Routledge; 2020.
- Huster RJ, Mokom ZN, Enriquez-Geppert S, Herrmann CS. Brain–computer interfaces for EEG neurofeedback: peculiarities and solutions. Int J Psychophysiol. 2014;91:36-45. doi:10.1016/j.ijpsycho.2013.08.011
- Ord AS, Martindale SL, Jenks ER, Rowland JA. Subjective cognitive complaints and objective cognitive functioning in combat veterans: effects of PTSD and deployment mild TBI. Appl Neuropsychol Adult. 2025;32:1400-1406. doi:10.1080/23279095.2023.2280807
- Lawton J, Blackburn M, Breckenridge J, Hallowell N, Farrington C, Rankin D. Ambassadors of hope, research pioneers and agents of change-individuals’ expectations and experiences of taking part in a randomised trial of an innovative health technology: longitudinal qualitative study. Trials. 2019;20:289. doi:10.1186/s13063-019-3373-9
- Hayward P. Traumatic brain injury: the signature of modern conflicts. Lancet Neurol. 2008;7:200-201. doi:10.1016/S1474-4422(08)70032-2
- Whiteneck G, Williams W, Almeida E, et al. Two decades of Department of Veterans Affairs traumatic brain injury care and benefits for veterans of post-9/11 conflicts. J Head Trauma Rehabil. 2024;39:E462-E469. doi:10.1097/HTR.0000000000000952
- Chapman JC, Diaz-Arrastia R. Military traumatic brain injury: a review. Alzheimers Dement. 2014;10(3 suppl):S97- S104. doi:10.1016/j.jalz.2014.04.012
- Dean PJA, O’Neill D, Sterr A. Post-concussion syndrome: prevalence after mild traumatic brain injury in comparison with a sample without head injury. Brain Inj. 2012;26:14-26. doi:10.3109/02699052.2011.635354
- Agimi Y, Hai T, Gano A, et al. Clinical trajectories of comorbidity associated with military-sustained mild traumatic brain injury: pre- and post-injury. J Head Trauma Rehabil. 2024;39:E564-E575. doi:10.1097/HTR.0000000000000934
- Hoge CW, McGurk D, Thomas JL, et al. Mild traumatic brain injury in U.S. soldiers returning from Iraq. N Engl J Med. 2008;358:453-463. doi:10.1056/NEJMoa072972
- Bogdanova Y, Verfaellie M. Cognitive sequelae of blast-induced traumatic brain injury: recovery and rehabilitation. Neuropsychol Rev. 2012;22:4-20. doi:10.1007/s11065-012-9192-3
- Eapen BC, Bowles AO, Sall J, et al. The management and rehabilitation of post-acute mild traumatic brain injury. Brain Inj. 2022;36:693-702. doi:10.1080/02699052.2022.2033848
- Department of Veterans Affairs (VA) and Department of Defense (DoD). VA/DoD Clinical Practice Guideline for the management and Rehabilitation of Post-Acute Mild Traumatic Brain Injury, 2021, Version 3:1-128. https://www.healthquality.va.gov/HEALTHQUALITY/guidelines/Rehab/mtbi/index.asp
- Patil VK, St Andre JR, Crisan E, et al. Prevalence and treatment of headaches in veterans with mild traumatic brain injury. Headache. 2011;51:1112-1121. doi:10.1111/j.1526-4610.2011.01946.x
- Ayalon L, Borodkin K, Dishon L, Kanety H, Dagan Y. Circadian rhythm sleep disorders following mild traumatic brain injury. Neurology. 2007;68:1136-1140. doi:10.1212/01.wnl.0000258672.52836.30
- Bogdanova Y, Verfaellie M. Cognitive sequelae of blast-induced traumatic brain injury: recovery and rehabilitation, Neuropsychology Review. 2012;22:4-20. doi:10.1007/s11065-012-9192-3
- US Department of Veteran Affairs. VHA Directive 1137.December 13, 2022. https://www.va.gov/VHApublications/ViewPublication.asp?pub_ID=10072
- Taylor SL, Hoggatt KJ, Kligler B. Complementary and integrated health approaches: what do veterans use and want. J Gen Intern Med. 2019;34:1192-1199. doi:10.1007/s11606-019-04862-6
- DeFlna P, Fellus J, Polito MZ, et al. The new neuroscience frontier: promoting neuroplasticity and brain repair in traumatic brain injury. Clin Neuropsychol. 2009;23:1391-1399. doi:10.1080/13854040903058978
- Enriquez-Geppert S, Huster RJ, Herrmann CS. Boosting brain functions: improving executive functions with behavioral training, neurostimulation, and neurofeedback. Int J Psychophysiol. 2013;88:1-16. doi:10.1016/j.ijpsycho.2013.02.001
- Ghaziri J, Tucholka A, Larue V, et al. Neurofeedback training induces changes in white and gray matter. Clin EEG Neurosci. 2013;44:265-272. doi:10.1177/1550059413476031
- Ibric VL, Dragomirescu LG, Hudspeth WJ. Real-time changes in connectivities during neurofeedback. J Neurother. 2009;13:156-165. doi:10.1080/10874200903118378
- Clark VP, Parasuraman R. Neuroenhancement: enhancing brain and mind in health and in disease. Neuroimage. 2014;85:889-894. doi:10.1016/j.neuroimage.2013.08.071
- Larsen S, Sherlin L. Neurofeedback: an emerging technology for treating central nervous system dysregulation. Psychiatr Clin North Am. 2013;36:163-168. doi:10.1016/j.psc.2013.01.005
- Hammond DC. What is neurofeedback: an update. J Neurother. 2011; 15:305-336. doi:10.1080/10874208.2011.623090
- Othmer S. Endogenous neuromodulation at infra-low frequencies. In: Chartier DR, Dellinger MB, Evans JR, Budzynski HK, eds. Introduction to Quantitative EEG and Neurofeedback. 3rd ed. Academic Press; 2023:283-299. doi:10.1016/B978-0-323-89827-0.00001-2
- Othmer SF. History of the Othmer Method: an evolving clinical model and process. In: Evans JR, Dellinger MB, Russell HL, eds. Neurofeedback: The First Fifty Years. Academic Press; 2020:327-334. doi:10.1016/B978-0-12-817659-7.00043-9
- Legarda SB, Lahti CE, McDermott D, Michas-Martin A. Use of novel concussion protocol with infralow frequency neuromodulation demonstrates significant treatment response in patients with persistent postconcussion symptoms, a retrospective study. Front Hum Neurosci. 2022;16:894758. doi:10.3389/fnhum.2022.894758
- Carlson J, Ross GW. Neurofeedback impact on chronic headache, sleep, and attention disorders experienced by veterans with mild traumatic brain injury: a pilot study. Biofeedback. 2021;49:2-9. doi:10.5298/1081-5937-49.01.01
- Dobrushina O, Arina G, Osina E, Aziatskaya G. Clinical and psychological confirmation of stabilizing effect of neurofeedback in migraine. Eur Psychiatry. 2017;41:S253-S253. doi:10.1016/j.eurpsy.2017.02.045
- Arina GA, Dobrushina OR, Shvetsova ET, et al. Infra-low frequency neurofeedback in tension-type headache: a cross-over sham-controlled study. Front Hum Neurosci. 2022;16:891323. doi:10.3389/fnhum.2022.891323
- Kirk HW, Dahl MG. Infra low frequency neurofeedback training for trauma recovery: a case report. Front Hum Neurosci. 2022;16:905823. doi:10.3389/fnhum.2022.905823
- Benson A, LaDou T. The use of neurofeedback for combat veterans with post-traumatic stress. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. CRC Press; 2015.
- Legarda SB, McMahon D, Othmer S, Othmer S. Clinical neurofeedback: case studies, proposed mechanism, and implications for pediatric neurology practice. J Child Neurol. 2011;26:1045-1051. doi:10.1177/0883073811405052
- McMahon DE. Notes from clinical practice: an MD’s perspective on 9 years of neurofeedback practice. Semin Pediatr Neurol. 2013;20:258-260. doi:10.1016/j.spen.2013.10.007
- Othmer S, Othmer SF. Post traumatic stress disorder— the neurofeedback remedy. Biofeedback. 2009;37:24-31. doi:10.5298/1081-5937-37.1.24
- Shapero E, Prager J. ILF Neurofeedback and alpha-theta training in a multidisciplinary chronic pain program. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. 2nd ed. Routledge; 2020:223-243.
- Carlson J, Ross G, Tyrrell C, et al. Infra-low frequency neurofeedback impact on post-concussive symptoms of headache, insomnia and attention disorder: results of a randomized control trial. Explore (NY). 2025;21:103137. doi:10.1016/j.explore.2025.103137
- Posner K, Brown GK, Stanley B, et al. The Columbia– Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011;168:1266- 1277. doi:10.1176/appi.ajp.2011.10111704
- Kosinski M, Bayliss MS, Bjorner JB, et al. A six-item short-form survey for measuring headache impact: the HIT-6. Qual Life Res. 2003;12:963-974. doi:10.1023/a:1026119331193
- Coeytaux RR, Kaufman JS, Chao R, Mann JD, Devellis RF. Four methods of estimating the minimal important difference score were compared to establish a clinically significant change in Headache Impact Test. J Clin Epidemiol. 2006;59:374-380. doi:10.1016/j.jclinepi.2005.05.010
- Tulsky DS, Tyner CE, Boulton AJ, et al. Development of the TBI-QOL Headache Pain Item Bank and Short Form. J Head Trauma Rehabil. 2019;34:298-307. doi:10.1097/HTR.0000000000000532
- Poritz JMP, Sherer M, Kisala MA, et al. Responsiveness of the Traumatic Brain Injury-Quality of Life (TBI-QOL) measurement system. Arch Phys Med Rehabil. 2020;101:54- 61. doi:10.1016/j.apmr.2017.11.018
- Bastien CH, Vallières A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001;2:297-307. doi:10.1016/s1389-9457(00)00065-4
- Yang M, Morin CM, Schaefer M, Wallenstein GV. Interpreting score differences in the Insomnia Severity Index: using health-related outcomes to define the minimally important difference. Curr Med Res Opin. 2009;25:2487-2494. doi:10.1185/03007990903167415
- Cella D, Lai J-S, Nowinski CJ, et al. Neuro-QOL Brief measures of health-related quality of life for clinical research in neurology. Neurology. 2012;78:1860-1867. doi:10.1212/WNL.0b013e318258f744
- Kozlowski AJ, Cella D, Nitsch KP, Heinemann AW. Evaluating individual change with the Quality of Life in Neurological Disorders (Neuro-QoL) short forms. Arch Phys Med Rehabil. 2016;97:650-654.e8. doi:10.1016/j.apmr.2015.12.010
- Versace M. QIKTest Report on EEG Expert: introduction and overview. 2014. Accessed February 24, 2026. https://media.voog.com/0000/0044/8343/files/EEGexpert_manual_newreport2014_EN.pdf
- Truelle J-L, Koskinen S, Hawthorne G, et al. Quality of life after traumatic brain injury: the clinical use of the QOLIBRI, a novel disease-specific instrument. Brain Inj. 2010;24:1272-1291. doi:10.3109/02699052.2010.506865
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606-613. doi:10.1046/j.1525-1497.2001.016009606.x
- Kroenke K. Enhancing the clinical utility of depression screening. CMAJ. 2012;184:281-282. doi:10.1503/cmaj.112004
- Weathers FW, Litz BT, Keane TM, et al. PTSD checklist for DSM-5 (PCL-5). National Center for PTSD. Updated September 10, 2025. Accessed February 24, 2026. https:// www.ptsd.va.gov/professional/assessment/adult-sr/ptsd-checklist.asp
- Henry JD, Crawford JR. The short]form version of the Depression Anxiety Stress Scales (DASS]21): construct validity and normative data in a large non]clinical sample. Br J Clin Psychol. 2005;44:227-239. doi:10.1348/014466505X29657
- Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther. 1995;33(3):335-343. doi:10.1016/0005-7967(94)00075-u
- Ronk FR, Korman JR, Hooke GR, Page AC. Assessing clinical significance of treatment outcomes using the DASS-21. Psychol Assess. 2013;25:1103-1110. doi:10.1037/a0033100
- Carlson J. General symptom inventory. Description published online 2021.
- Nelson DV, Esty ML. Neurotherapy of traumatic brain injury/ posttraumatic stress symptoms in OEF/OIF veterans. J Neuropsychiatry Clin Neurosci. 2012;24:237-240. doi:10.1176/appi.neuropsych.11020041
- Zoefel B, Huster RJ, Herrmann CS. Neurofeedback training of the upper alpha frequency band in EEG improves cognitive performance. Neuroimage. 2011;54:1427-1431. doi:10.1016/j.neuroimage.2010.08.078
- Othmer S, Othmer S. Toward a theory of infra-low frequency neurofeedback. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. 2nd ed. Routledge; 2020.
- Huster RJ, Mokom ZN, Enriquez-Geppert S, Herrmann CS. Brain–computer interfaces for EEG neurofeedback: peculiarities and solutions. Int J Psychophysiol. 2014;91:36-45. doi:10.1016/j.ijpsycho.2013.08.011
- Ord AS, Martindale SL, Jenks ER, Rowland JA. Subjective cognitive complaints and objective cognitive functioning in combat veterans: effects of PTSD and deployment mild TBI. Appl Neuropsychol Adult. 2025;32:1400-1406. doi:10.1080/23279095.2023.2280807
- Lawton J, Blackburn M, Breckenridge J, Hallowell N, Farrington C, Rankin D. Ambassadors of hope, research pioneers and agents of change-individuals’ expectations and experiences of taking part in a randomised trial of an innovative health technology: longitudinal qualitative study. Trials. 2019;20:289. doi:10.1186/s13063-019-3373-9
Clinical Impact of Infra-Low Frequency Neurofeedback on Combat Veterans With Chronic Postconcussive Symptoms
Clinical Impact of Infra-Low Frequency Neurofeedback on Combat Veterans With Chronic Postconcussive Symptoms

Streamlining the Acute Care Pharmacy Consultation Process for Patients With Dysphagia or Enteral Feeding Tubes
Streamlining the Acute Care Pharmacy Consultation Process for Patients With Dysphagia or Enteral Feeding Tubes
Medication regimens may require adjustment in acute care settings due to dysphagia and/or enteral feeding tubes. When a patient has dysphagia and/or a feeding tube, the health care team must review the pharmacotherapy regimen to assess the appropriateness of medication formulations. Patient anatomy, the type of feeding tube in place, pharmacokinetic and pharmacodynamic properties of medications, risk of feeding tube obstruction, and potential for interactions between enteral nutrition and medications should be considered when clinicians administer medications through feeding tubes. The risk of feeding tube obstruction and clogging rises with increasing tube length and decreasing tube lumen. Incidence of obstructed percutaneous endoscopic gastrotomy tubes is reported to be 23% to 35%.1
A coordinated effort by all members of the health care team is essential to provide safe and effective care to patients with dysphagia and/or enteral feeding tubes. To decrease the risk of feeding tube obstruction, medications should be dissolved in water or administered in liquid form, saline fluids should be avoided, and the tube should be flushed with water before and after administering medications.
The pharmacokinetics of medications can be altered when tablets are crushed or capsules are opened. The bioavailability of dabigatran, for example, increases by 75% when the capsules are opened and pellets are taken orally.2 Medications may become intolerable after manipulation due to taste.3 Others may also increase the risk of feeding tube obstruction, such as omeprazole granules that increase the risk of small-bore feeding tube obstruction.4
Prior assessments of drug administration for patients with dysphagia and/or enteral feeding tubes has shown medication errors are prevalent.5-7 The Institute for Safe Medication Practices (ISMP) issued a Medication Safety Alert that provides a framework for preventing medication errors when preparing and administering medications via enteral feeding tubes.8 Other resources, such as monographs, are also available to guide pharmacotherapy decisions when oral medications require manipulation for administration to patients with dysphagia and/or enteral feeding tubes.9-11
In 2021, the Kansas City Veterans Affairs Medical Center (KCVAMC) was recognized as a Veterans Health Administration (VHA) Shark Tank finalist for improving the safety of medication administration for patients with enteral feeding tubes.12 This involved the addition of a Computerized Patient Record System (CPRS), clinical reminder order check (CROC), and a comprehensive medication review by a pharmacist. After implementing the CROC alert and pharmacy e-consultation workflow, the KCVAMC team reported that the number of inappropriate medications (ie, drugs on the ISMP do not crush list) was reduced from 41 to 6 in 1 year, resulting in an 85.4% reduction in potential medication errors.13
In 2014, the Richard L. Roudebush VAMC (RLRVAMC) created a pharmacy consultation process for patients with dysphagia and/or enteral feeding tubes. Any clinician could place a pharmacy consultation in CPRS. A pharmacist then reviewed patient charts, medication information resources, the VA formulary, and RLRVAMC pharmacy inventory. The pharmacist conferred with the patient’s care team to adjust pharmacotherapy, completed a consultation note, and updated medication order comments in Veterans Health Information Systems and Technology Architecture (VistA). These comments interfaced with the barcode medication administration software for the health care professional administering medications.
Despite the 2014 quality improvement (QI) process, medication errors involving the inappropriate ordering, preparation, and administration of medications for patients with dysphagia and/or enteral feeding tubes continued to be reported. Additionally, anonymous feedback revealed that only 3 of 10 responding pharmacists were satisfied with the existing medication use process for patients with dysphagia and/or enteral feeding tubes. Pharmacists expressed concerns that (1) clinicians were inappropriately crushing and/or manipulating new medications that were ordered after pharmacy consultations; (2) there was a lack of comprehensive documentation in CPRS; and (3) there were too many manual steps in the process. In response, RLRVAMC initiated a new QI initiative to improve the medication use process for patients with dysphagia and/or enteral feeding tubes in the acute care setting.
Quality Improvement Project
This multidisciplinary RLRVAMC QI project began November 2024 to improve pharmacotherapy care for patients with dysphagia and/or enteral feeding tubes in acute care. It was approved by the RLRVAMC Pharmacy Service. This intervention addressed the pharmacy consultation template, standardization of equipment, standardization of language, creation of clinical alerts, and sustainment (Table 1).
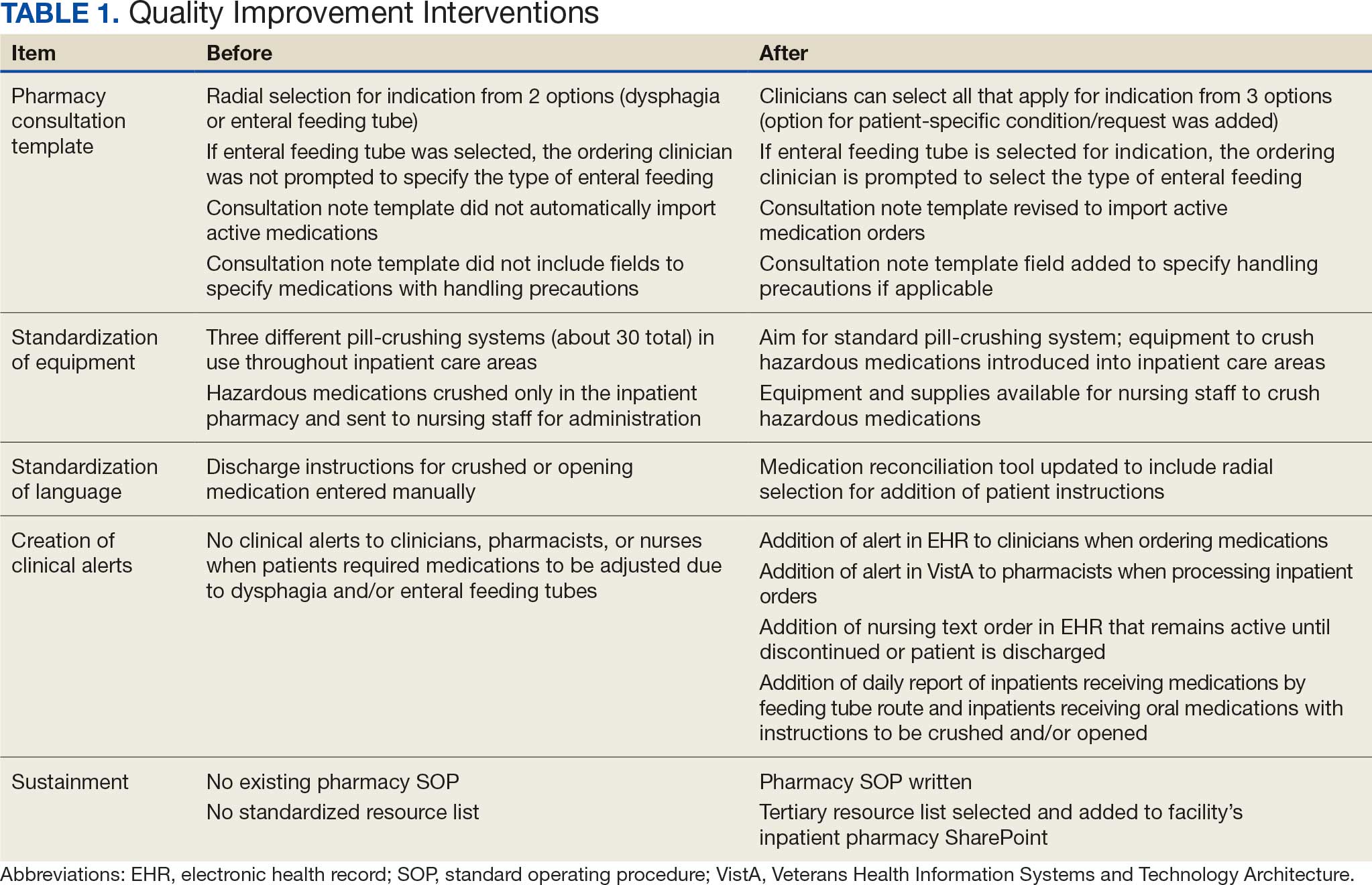
RLRVAMC has about 8600 annual inpatient admissions and 159 acute care beds.14 The project charter was drafted, and local stakeholders were identified including pharmacy technicians, pharmacists, nurses, speech language pathologists, and acute care clinicians. Pharmacy consultation workload was retrospectively reviewed to describe the scope of the existing state.
A workshop with 12 QI project stakeholders in December 2024 used A3 methodology to define the current process and the target state, barriers and solutions, prioritize interventions on an impact-effort matrix, perform a gap analysis, identify rapid plan-do-study-act (PDSA) experiments, and develop a completion plan (Figure). Five postworkshop PDSA experiments engaged additional stakeholders, clinical application coordinators, and medical supply representatives to ascertain the feasibility of the tools implemented.
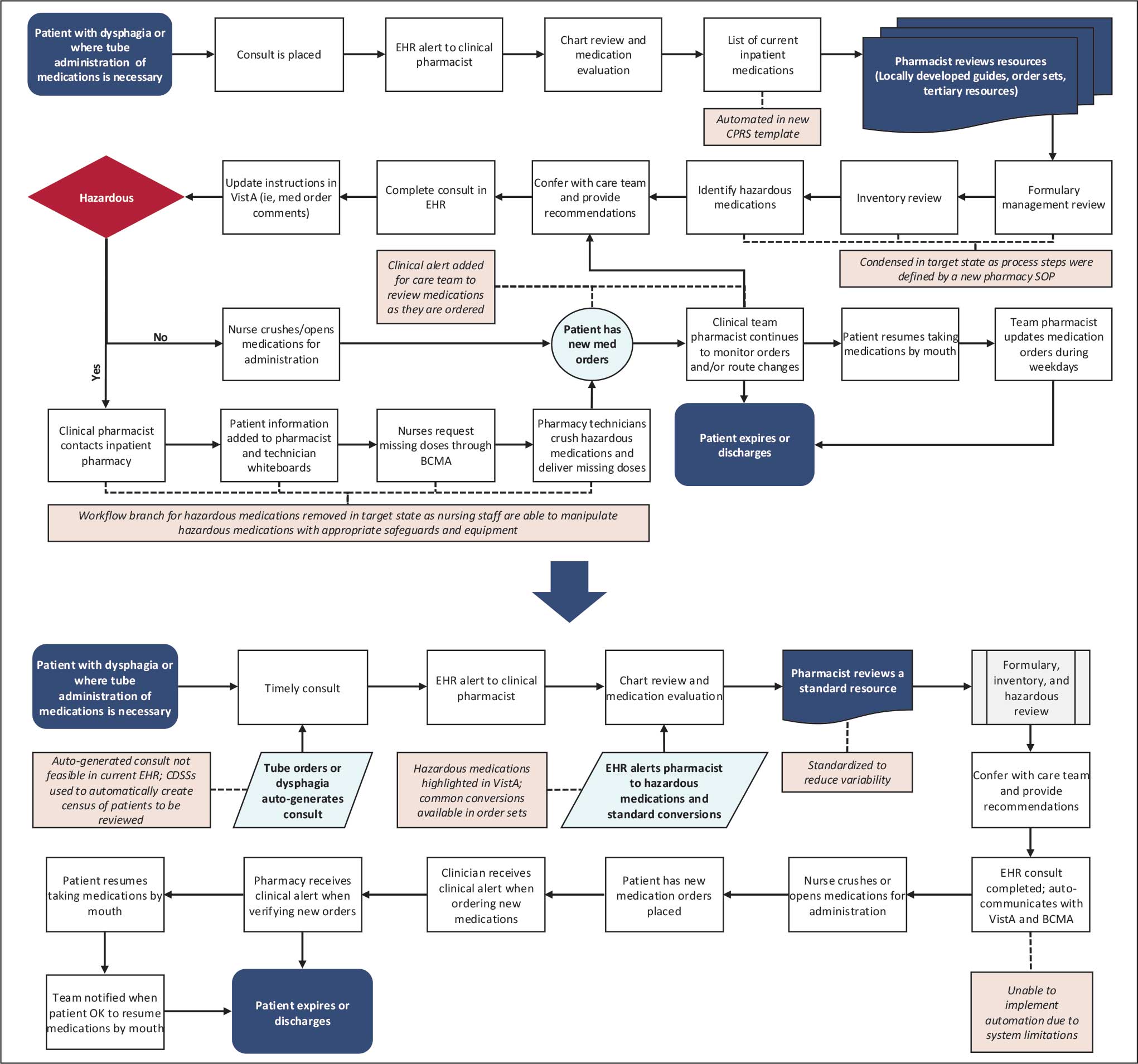
Abbreviations: BCMA, barcode medication administration; CDSS, clinical decision support system; CPRS, Computerized Patient Record System;
EHR, electronic health record; SOP, standard operating procedure; VistA, Veterans Health Information Systems and Technology Architecture.
About 3% of RLRVAMC admissions involve a pharmacy consultation to review medications for dysphagia and/or enteral feeding tubes. Clinicians reviewed 30 preimplementation inpatient pharmacy consultations involving 200 oral medications. Pharmacists were more frequently consulted for inpatients with dysphagia (19 [63%]) than for patients with enteral feeding tubes (11 [37%]) (Table 2).

Pharmacy Consultation Template
The pharmacy consultation was updated in CPRS. Prior to this QI project, the ordering clinician was prompted to select 1 option for the indication: dysphagia or enteral feeding tube. The type of enteral feeding tube was not prompted by the consultation text nor required to be specified in the consultation. The ordering clinician could provide free-text comments. Of 11 preimplementation consultations, the type of enteral feeding tube was specified in 5 (45%). The consultation template entry was updated to include an option to check a box for the consultation indication from 3 options: dysphagia, enteral feeding, or other patient- specific condition/request. If enteral feeding tube is selected, then the clinician is prompted to select the type of enteral feeding tube. Since the completion of the project, there have been no patient safety reports concerning an erroneous or incomplete consultation entry (Supplemental Material).
The note template was updated to import the list of active inpatient medications and provide sections for the adjudicating pharmacist to document which medications can be crushed (or opened), which require adjustment, and which are hazardous and require special handling. Additionally, the revised template added a statement clarifying that the documented recommendations apply only to the medication regimen at the time of the consultation (Supplemental Material).
Standardizations
There are multiple pill-crushing devices used at RLRVAMC that vary in crushing mechanism, corresponding medication pouches, and degree of protection when manipulating hazardous medications. Prior to this QI project, RLRVAMC used 3 pill-crushing devices (about 30 total devices in inpatient care areas). Only 1 device with corresponding closed pouches for preparation of hazardous medications was available, which was stored in the RLRVAMC inpatient pharmacy. This workflow resulted in waste and posed potential risks for delays in care. This project incorporated a standard pill-crushing system with the corresponding medication pouches in all inpatient care areas, which provided safeguards for clinicians to prepare and administer hazardous medications (Supplemental Material).
Patients requiring medications to be crushed or opened on discharge should receive education, written instruction, and have care plans documented in CPRS. RLRVAMC patients receive education and a printed medication list. Prior to this QI project, the instructions for crushing or opening medications could only be entered by free text in the electronic medication reconciliation tool, allowing for the potential for inconsistent language or omissions.
This QI project included an update to the electronic medication reconciliation tool. An optional checkbox selection was added for patients requiring medications to be manipulated. When checked, a radial selection for individual medications is displayed, prompting the clinician and pharmacist to indicate either do not crush tablet or OK to crush tablet. These selections appear in clinical care notes and on the printed medication list provided to the patient (Supplemental Material).
Clinical Alerts
As part of the RLRVAMC QI initiative, a CROC alert was implemented, based on the KCVAMC intervention for patients with enteral feeding tubes.13 The RLRVAMC CROC alert also included patients with dysphagia. A nursing text order was made available in CPRS for patients requiring medications and remains active throughout the duration of the patient’s admission or until discontinued. It generates CROC alerts in CPRS and VistA when new medication orders are entered and reviewed by pharmacists.
Clinicians used clinical decision support systems to create daily lists of patients receiving medications by feeding tube and patients receiving crushed/opened medications due to dysphagia. This allows pharmacists to perform a census review of all inpatients to confirm appropriateness of medication orders. Clinical alerts for patients with enteral feeding tubes are advised by the ISMP and have data demonstrating a reduction in medication errors (Supplemental Material).14,15
Sustainment
During the sustainment phase, process owners were identified and a Pharmacy Service standard operating procedure (SOP) was written. The development of an institutional do not crush medication list was discussed; however, it was determined to be difficult to develop and maintain. An institutional tertiary resource list was selected in favor of a locally developed resource. These resources include the Handbook of Drug Administration via Enteral Feeding Tubes, Third Edition, the Pharmacist’s Letter list, “Meds that Should Not be Crushed,” and the Up- ToDate Lexidrug list, “Oral Medications That Should Not Be Crushed or Altered.”9-11 Links to the resources were added to the RLRVAMC pharmacy service SharePoint. In addition to defining the preferred tertiary resources, the SOP defined the process for reviewing inventory and the process for reviewing medication orders for hazard risk.
Discussion
Continued patient safety reports and low satisfaction rates among pharmacists prompted this QI project to improve safety for patients with dysphagia and/or enteral feeding tubes at RLRVAMC. The project engaged stakeholders and also identified and addressed gaps with potential for patient harm.
The tools implemented by this initiative drew from previous work by the KCVAMC and from framework provided by the ISMP.8,13 We expanded the QI intervention to include acute care patients with dysphagia.
RLRVAMC did not take steps to track the impact of the interventions on medication errors. However, no patient safety reports concerning an erroneous or incomplete pharmacy consultation entry have been reported. We also think that it is reasonable to assume that the adoption of the safety tools described here will have a positive impact on patient safety. RLRVAMC pharmacists have noted an increased appreciation for medication safety when processing medication orders for patients with dysphagia and/or enteral feeding tubes. While the workflow took time to adopt and integrate, clinical pharmacists perceived it as an improvement in patient safety. Our future focus is aimed at translating the process improvement into the Oracle/Cerner electronic health record, which is scheduled to be deployed at the RLRVAMC in August 2026.
Limitations
This QI project did not aim to quantify or compare medication errors before and after the intervention. An accurate number of unreported errors in the medication use process for patients with dysphagia and/or enteral feeding tubes would be challenging to quantify without direct observation. Multiple clinicians are engaged in the medication use process and individual steps may not be documented at all, or documented properly. In addition, medication errors are often underreported and may not reflect the total number of errors and/or potential for errors. That said, reported medication errors in the medication use process for patients with dysphagia and/or enteral feeding tubes are reviewed on a monthly basis by the RLRVAMC Multidisciplinary Medication Safety committee to continuously improve patient safety.
Another potential limitation is the extent to which the project can be adapted at other VHA sites. For example, RLRVAMC uses CPRS; the framework and tools to improve medication safety may not translate to sites using the Oracle/Cerner electronic health record. Furthermore, this QI project included a pharmacy consultation workflow that relied on pharmacists who are available at any hour. Other facilities may not have continuous consultation coverage to review medications for patients with dysphagia and/or enteral feeding tubes.
Conclusions
This QI project drew from ISMP recommendations, previous work within the VHA, local practice, and insight from multiple disciplines on the health care team to revise and create tools to improve medication safety for patients with dysphagia and/or enteral feeding tubes in the acute care setting. These tools included a revised pharmacy consultation workflow with improvements to the pharmacy consultation template, standardization of the pill-crushing devices and language used for patient medication lists, implementation of CROC alerts within the EHR, and development of an SOP.
The RLRVAMC Pharmacy Service intends to continue reviewing patient safety reports, assessing staff perspectives, and refining (and potentially adding) tools for medication safety. Future QI initiatives may focus on improving medication safety for outpatients with dysphagia and/or enteral feeding tubes. We also hope that these tools can be adapted at other VAMCs to promote medication safety for patients with dysphagia and/or enteral feeding tubes.
- Blumenstein I, Shastri YM, Stein J. Gastroenteric tube feeding: techniques, problems and solutions. World J Gastroenterol. 2014;20:8505-8524. doi:10.3748/wjg.v20.i26.8505
- Pradaxa (dabigatran etexilate). Prescribing information. Boehringer Ingelheim Pharmaceuticals, Inc; 2025. https:// pro.boehringer-ingelheim.com/us/products/pradaxa/bipdf /pradaxa-capsules-us-pi
- Lovell AG, Protus BM, Dickman JR, et al. Palatability of crushed over-the-counter medications. J Pain Symptom Manage. 2021;61:755-762. doi:10.1016/j.jpainsymman.2020.09.020
- Messaouik D, Sautou-Miranda V, Bagel-Boithias S, et al. Comparative study and optimisation of the administration mode of three proton pump inhibitors by nasogastric tube. Int J Pharm. 2005;299:65-72. doi:10.1016/j.ijpharm.2005.04.034
- Demirkan K, Bayraktar-Ekincioglu A, Gulhan-Halil M, et al. Assessment of drug administration via feeding tube and the knowledge of health-care professionals in a university hospital. Eur J Clin Nutr. 2017;71:164-168. doi:10.1038/ejcn.2016.147
- Fodil M, Nghiem D, Colas M, et al. Assessment of clinical practices for crushing medication in geriatric units. J Nutr Health Aging. 2017;21:904-908. doi:10.1007/s12603-017-0886-3
- Zhu LL, Xu LC, Wang HQ, et al. Appropriateness of administration of nasogastric medication and preliminary intervention. Ther Clin Risk Manag. 2012;8:393-401. doi:10.2147/TCRM.S37785
- Institute for Safe Medication Practices (ISMP). Preventing errors when preparing and administering medications via enteral feeding tubes. Acute Care ISMP Medication Safety Alert. November 17, 2022. Accessed March 17, 2026. https://nutritioncare.org/wp-content/uploads/2025/02 /ISMP-Safety-Alert_Medications-and-Enteral-Feeding -Tubes.pdf
- White R, Bradnam V. Handbook of Drug Administration via Enteral Feeding Tubes. 3rd ed. Pharmaceutical Press; 2015.
- Clinical resource, meds that should not be crushed. Pharmacist’s Letter/Pharmacy Technician’s Letter/Prescriber Insights. Updated April 2025. Accessed March 17, 2026. https://pharmacist.therapeuticresearch.com/en/Content /Segments/PRL/2014/Aug/Meds-That-Should-Not-Be -Crushed-7309
- Oral medications that should not be crushed or altered. In: Lexidrug. UpToDate, Inc. https://online.lexi.com/lco /action/doc/retrieve/docid/patch_f/4227
- Uttaro E, Zhao F, Schweighardt A. Filling the gaps on the Institute for Safe Medication Practices (ISMP) do not crush list for immediate-release products. Int J Pharm Compd. 2021;25:364-371.
- US Dept of Veterans Affairs. VA Diffusion Marketplace. Improved safety of enteral tube medication administration. Updated 2024. Accessed March 17, 2026. https:// marketplace.va.gov/innovations/improved-safety-of -enteral-tube-medication-administration
- US Dept of Veterans Affairs. About us. VA Indiana Healthcare System. Updated October 17, 2024. Accessed March 2, 2026. https://www.va.gov/indiana-health-care/about-us/
- Wasylewicz ATM, van Grinsven RJB, Bikker JMW, et al. Clinical decision support system-assisted pharmacy intervention reduces feeding tube-related medication errors in hospitalized patients: a focus on medication suitable for feeding-tube administration. JPEN J Parenter Enteral Nutr. 2021;45:625-632. doi:10.1002/jpen.1869
Medication regimens may require adjustment in acute care settings due to dysphagia and/or enteral feeding tubes. When a patient has dysphagia and/or a feeding tube, the health care team must review the pharmacotherapy regimen to assess the appropriateness of medication formulations. Patient anatomy, the type of feeding tube in place, pharmacokinetic and pharmacodynamic properties of medications, risk of feeding tube obstruction, and potential for interactions between enteral nutrition and medications should be considered when clinicians administer medications through feeding tubes. The risk of feeding tube obstruction and clogging rises with increasing tube length and decreasing tube lumen. Incidence of obstructed percutaneous endoscopic gastrotomy tubes is reported to be 23% to 35%.1
A coordinated effort by all members of the health care team is essential to provide safe and effective care to patients with dysphagia and/or enteral feeding tubes. To decrease the risk of feeding tube obstruction, medications should be dissolved in water or administered in liquid form, saline fluids should be avoided, and the tube should be flushed with water before and after administering medications.
The pharmacokinetics of medications can be altered when tablets are crushed or capsules are opened. The bioavailability of dabigatran, for example, increases by 75% when the capsules are opened and pellets are taken orally.2 Medications may become intolerable after manipulation due to taste.3 Others may also increase the risk of feeding tube obstruction, such as omeprazole granules that increase the risk of small-bore feeding tube obstruction.4
Prior assessments of drug administration for patients with dysphagia and/or enteral feeding tubes has shown medication errors are prevalent.5-7 The Institute for Safe Medication Practices (ISMP) issued a Medication Safety Alert that provides a framework for preventing medication errors when preparing and administering medications via enteral feeding tubes.8 Other resources, such as monographs, are also available to guide pharmacotherapy decisions when oral medications require manipulation for administration to patients with dysphagia and/or enteral feeding tubes.9-11
In 2021, the Kansas City Veterans Affairs Medical Center (KCVAMC) was recognized as a Veterans Health Administration (VHA) Shark Tank finalist for improving the safety of medication administration for patients with enteral feeding tubes.12 This involved the addition of a Computerized Patient Record System (CPRS), clinical reminder order check (CROC), and a comprehensive medication review by a pharmacist. After implementing the CROC alert and pharmacy e-consultation workflow, the KCVAMC team reported that the number of inappropriate medications (ie, drugs on the ISMP do not crush list) was reduced from 41 to 6 in 1 year, resulting in an 85.4% reduction in potential medication errors.13
In 2014, the Richard L. Roudebush VAMC (RLRVAMC) created a pharmacy consultation process for patients with dysphagia and/or enteral feeding tubes. Any clinician could place a pharmacy consultation in CPRS. A pharmacist then reviewed patient charts, medication information resources, the VA formulary, and RLRVAMC pharmacy inventory. The pharmacist conferred with the patient’s care team to adjust pharmacotherapy, completed a consultation note, and updated medication order comments in Veterans Health Information Systems and Technology Architecture (VistA). These comments interfaced with the barcode medication administration software for the health care professional administering medications.
Despite the 2014 quality improvement (QI) process, medication errors involving the inappropriate ordering, preparation, and administration of medications for patients with dysphagia and/or enteral feeding tubes continued to be reported. Additionally, anonymous feedback revealed that only 3 of 10 responding pharmacists were satisfied with the existing medication use process for patients with dysphagia and/or enteral feeding tubes. Pharmacists expressed concerns that (1) clinicians were inappropriately crushing and/or manipulating new medications that were ordered after pharmacy consultations; (2) there was a lack of comprehensive documentation in CPRS; and (3) there were too many manual steps in the process. In response, RLRVAMC initiated a new QI initiative to improve the medication use process for patients with dysphagia and/or enteral feeding tubes in the acute care setting.
Quality Improvement Project
This multidisciplinary RLRVAMC QI project began November 2024 to improve pharmacotherapy care for patients with dysphagia and/or enteral feeding tubes in acute care. It was approved by the RLRVAMC Pharmacy Service. This intervention addressed the pharmacy consultation template, standardization of equipment, standardization of language, creation of clinical alerts, and sustainment (Table 1).
RLRVAMC has about 8600 annual inpatient admissions and 159 acute care beds.14 The project charter was drafted, and local stakeholders were identified including pharmacy technicians, pharmacists, nurses, speech language pathologists, and acute care clinicians. Pharmacy consultation workload was retrospectively reviewed to describe the scope of the existing state.
A workshop with 12 QI project stakeholders in December 2024 used A3 methodology to define the current process and the target state, barriers and solutions, prioritize interventions on an impact-effort matrix, perform a gap analysis, identify rapid plan-do-study-act (PDSA) experiments, and develop a completion plan (Figure). Five postworkshop PDSA experiments engaged additional stakeholders, clinical application coordinators, and medical supply representatives to ascertain the feasibility of the tools implemented.
Abbreviations: BCMA, barcode medication administration; CDSS, clinical decision support system; CPRS, Computerized Patient Record System;
EHR, electronic health record; SOP, standard operating procedure; VistA, Veterans Health Information Systems and Technology Architecture.
About 3% of RLRVAMC admissions involve a pharmacy consultation to review medications for dysphagia and/or enteral feeding tubes. Clinicians reviewed 30 preimplementation inpatient pharmacy consultations involving 200 oral medications. Pharmacists were more frequently consulted for inpatients with dysphagia (19 [63%]) than for patients with enteral feeding tubes (11 [37%]) (Table 2).
Pharmacy Consultation Template
The pharmacy consultation was updated in CPRS. Prior to this QI project, the ordering clinician was prompted to select 1 option for the indication: dysphagia or enteral feeding tube. The type of enteral feeding tube was not prompted by the consultation text nor required to be specified in the consultation. The ordering clinician could provide free-text comments. Of 11 preimplementation consultations, the type of enteral feeding tube was specified in 5 (45%). The consultation template entry was updated to include an option to check a box for the consultation indication from 3 options: dysphagia, enteral feeding, or other patient- specific condition/request. If enteral feeding tube is selected, then the clinician is prompted to select the type of enteral feeding tube. Since the completion of the project, there have been no patient safety reports concerning an erroneous or incomplete consultation entry (Supplemental Material).
The note template was updated to import the list of active inpatient medications and provide sections for the adjudicating pharmacist to document which medications can be crushed (or opened), which require adjustment, and which are hazardous and require special handling. Additionally, the revised template added a statement clarifying that the documented recommendations apply only to the medication regimen at the time of the consultation (Supplemental Material).
Standardizations
There are multiple pill-crushing devices used at RLRVAMC that vary in crushing mechanism, corresponding medication pouches, and degree of protection when manipulating hazardous medications. Prior to this QI project, RLRVAMC used 3 pill-crushing devices (about 30 total devices in inpatient care areas). Only 1 device with corresponding closed pouches for preparation of hazardous medications was available, which was stored in the RLRVAMC inpatient pharmacy. This workflow resulted in waste and posed potential risks for delays in care. This project incorporated a standard pill-crushing system with the corresponding medication pouches in all inpatient care areas, which provided safeguards for clinicians to prepare and administer hazardous medications (Supplemental Material).
Patients requiring medications to be crushed or opened on discharge should receive education, written instruction, and have care plans documented in CPRS. RLRVAMC patients receive education and a printed medication list. Prior to this QI project, the instructions for crushing or opening medications could only be entered by free text in the electronic medication reconciliation tool, allowing for the potential for inconsistent language or omissions.
This QI project included an update to the electronic medication reconciliation tool. An optional checkbox selection was added for patients requiring medications to be manipulated. When checked, a radial selection for individual medications is displayed, prompting the clinician and pharmacist to indicate either do not crush tablet or OK to crush tablet. These selections appear in clinical care notes and on the printed medication list provided to the patient (Supplemental Material).
Clinical Alerts
As part of the RLRVAMC QI initiative, a CROC alert was implemented, based on the KCVAMC intervention for patients with enteral feeding tubes.13 The RLRVAMC CROC alert also included patients with dysphagia. A nursing text order was made available in CPRS for patients requiring medications and remains active throughout the duration of the patient’s admission or until discontinued. It generates CROC alerts in CPRS and VistA when new medication orders are entered and reviewed by pharmacists.
Clinicians used clinical decision support systems to create daily lists of patients receiving medications by feeding tube and patients receiving crushed/opened medications due to dysphagia. This allows pharmacists to perform a census review of all inpatients to confirm appropriateness of medication orders. Clinical alerts for patients with enteral feeding tubes are advised by the ISMP and have data demonstrating a reduction in medication errors (Supplemental Material).14,15
Sustainment
During the sustainment phase, process owners were identified and a Pharmacy Service standard operating procedure (SOP) was written. The development of an institutional do not crush medication list was discussed; however, it was determined to be difficult to develop and maintain. An institutional tertiary resource list was selected in favor of a locally developed resource. These resources include the Handbook of Drug Administration via Enteral Feeding Tubes, Third Edition, the Pharmacist’s Letter list, “Meds that Should Not be Crushed,” and the Up- ToDate Lexidrug list, “Oral Medications That Should Not Be Crushed or Altered.”9-11 Links to the resources were added to the RLRVAMC pharmacy service SharePoint. In addition to defining the preferred tertiary resources, the SOP defined the process for reviewing inventory and the process for reviewing medication orders for hazard risk.
Discussion
Continued patient safety reports and low satisfaction rates among pharmacists prompted this QI project to improve safety for patients with dysphagia and/or enteral feeding tubes at RLRVAMC. The project engaged stakeholders and also identified and addressed gaps with potential for patient harm.
The tools implemented by this initiative drew from previous work by the KCVAMC and from framework provided by the ISMP.8,13 We expanded the QI intervention to include acute care patients with dysphagia.
RLRVAMC did not take steps to track the impact of the interventions on medication errors. However, no patient safety reports concerning an erroneous or incomplete pharmacy consultation entry have been reported. We also think that it is reasonable to assume that the adoption of the safety tools described here will have a positive impact on patient safety. RLRVAMC pharmacists have noted an increased appreciation for medication safety when processing medication orders for patients with dysphagia and/or enteral feeding tubes. While the workflow took time to adopt and integrate, clinical pharmacists perceived it as an improvement in patient safety. Our future focus is aimed at translating the process improvement into the Oracle/Cerner electronic health record, which is scheduled to be deployed at the RLRVAMC in August 2026.
Limitations
This QI project did not aim to quantify or compare medication errors before and after the intervention. An accurate number of unreported errors in the medication use process for patients with dysphagia and/or enteral feeding tubes would be challenging to quantify without direct observation. Multiple clinicians are engaged in the medication use process and individual steps may not be documented at all, or documented properly. In addition, medication errors are often underreported and may not reflect the total number of errors and/or potential for errors. That said, reported medication errors in the medication use process for patients with dysphagia and/or enteral feeding tubes are reviewed on a monthly basis by the RLRVAMC Multidisciplinary Medication Safety committee to continuously improve patient safety.
Another potential limitation is the extent to which the project can be adapted at other VHA sites. For example, RLRVAMC uses CPRS; the framework and tools to improve medication safety may not translate to sites using the Oracle/Cerner electronic health record. Furthermore, this QI project included a pharmacy consultation workflow that relied on pharmacists who are available at any hour. Other facilities may not have continuous consultation coverage to review medications for patients with dysphagia and/or enteral feeding tubes.
Conclusions
This QI project drew from ISMP recommendations, previous work within the VHA, local practice, and insight from multiple disciplines on the health care team to revise and create tools to improve medication safety for patients with dysphagia and/or enteral feeding tubes in the acute care setting. These tools included a revised pharmacy consultation workflow with improvements to the pharmacy consultation template, standardization of the pill-crushing devices and language used for patient medication lists, implementation of CROC alerts within the EHR, and development of an SOP.
The RLRVAMC Pharmacy Service intends to continue reviewing patient safety reports, assessing staff perspectives, and refining (and potentially adding) tools for medication safety. Future QI initiatives may focus on improving medication safety for outpatients with dysphagia and/or enteral feeding tubes. We also hope that these tools can be adapted at other VAMCs to promote medication safety for patients with dysphagia and/or enteral feeding tubes.
Medication regimens may require adjustment in acute care settings due to dysphagia and/or enteral feeding tubes. When a patient has dysphagia and/or a feeding tube, the health care team must review the pharmacotherapy regimen to assess the appropriateness of medication formulations. Patient anatomy, the type of feeding tube in place, pharmacokinetic and pharmacodynamic properties of medications, risk of feeding tube obstruction, and potential for interactions between enteral nutrition and medications should be considered when clinicians administer medications through feeding tubes. The risk of feeding tube obstruction and clogging rises with increasing tube length and decreasing tube lumen. Incidence of obstructed percutaneous endoscopic gastrotomy tubes is reported to be 23% to 35%.1
A coordinated effort by all members of the health care team is essential to provide safe and effective care to patients with dysphagia and/or enteral feeding tubes. To decrease the risk of feeding tube obstruction, medications should be dissolved in water or administered in liquid form, saline fluids should be avoided, and the tube should be flushed with water before and after administering medications.
The pharmacokinetics of medications can be altered when tablets are crushed or capsules are opened. The bioavailability of dabigatran, for example, increases by 75% when the capsules are opened and pellets are taken orally.2 Medications may become intolerable after manipulation due to taste.3 Others may also increase the risk of feeding tube obstruction, such as omeprazole granules that increase the risk of small-bore feeding tube obstruction.4
Prior assessments of drug administration for patients with dysphagia and/or enteral feeding tubes has shown medication errors are prevalent.5-7 The Institute for Safe Medication Practices (ISMP) issued a Medication Safety Alert that provides a framework for preventing medication errors when preparing and administering medications via enteral feeding tubes.8 Other resources, such as monographs, are also available to guide pharmacotherapy decisions when oral medications require manipulation for administration to patients with dysphagia and/or enteral feeding tubes.9-11
In 2021, the Kansas City Veterans Affairs Medical Center (KCVAMC) was recognized as a Veterans Health Administration (VHA) Shark Tank finalist for improving the safety of medication administration for patients with enteral feeding tubes.12 This involved the addition of a Computerized Patient Record System (CPRS), clinical reminder order check (CROC), and a comprehensive medication review by a pharmacist. After implementing the CROC alert and pharmacy e-consultation workflow, the KCVAMC team reported that the number of inappropriate medications (ie, drugs on the ISMP do not crush list) was reduced from 41 to 6 in 1 year, resulting in an 85.4% reduction in potential medication errors.13
In 2014, the Richard L. Roudebush VAMC (RLRVAMC) created a pharmacy consultation process for patients with dysphagia and/or enteral feeding tubes. Any clinician could place a pharmacy consultation in CPRS. A pharmacist then reviewed patient charts, medication information resources, the VA formulary, and RLRVAMC pharmacy inventory. The pharmacist conferred with the patient’s care team to adjust pharmacotherapy, completed a consultation note, and updated medication order comments in Veterans Health Information Systems and Technology Architecture (VistA). These comments interfaced with the barcode medication administration software for the health care professional administering medications.
Despite the 2014 quality improvement (QI) process, medication errors involving the inappropriate ordering, preparation, and administration of medications for patients with dysphagia and/or enteral feeding tubes continued to be reported. Additionally, anonymous feedback revealed that only 3 of 10 responding pharmacists were satisfied with the existing medication use process for patients with dysphagia and/or enteral feeding tubes. Pharmacists expressed concerns that (1) clinicians were inappropriately crushing and/or manipulating new medications that were ordered after pharmacy consultations; (2) there was a lack of comprehensive documentation in CPRS; and (3) there were too many manual steps in the process. In response, RLRVAMC initiated a new QI initiative to improve the medication use process for patients with dysphagia and/or enteral feeding tubes in the acute care setting.
Quality Improvement Project
This multidisciplinary RLRVAMC QI project began November 2024 to improve pharmacotherapy care for patients with dysphagia and/or enteral feeding tubes in acute care. It was approved by the RLRVAMC Pharmacy Service. This intervention addressed the pharmacy consultation template, standardization of equipment, standardization of language, creation of clinical alerts, and sustainment (Table 1).
RLRVAMC has about 8600 annual inpatient admissions and 159 acute care beds.14 The project charter was drafted, and local stakeholders were identified including pharmacy technicians, pharmacists, nurses, speech language pathologists, and acute care clinicians. Pharmacy consultation workload was retrospectively reviewed to describe the scope of the existing state.
A workshop with 12 QI project stakeholders in December 2024 used A3 methodology to define the current process and the target state, barriers and solutions, prioritize interventions on an impact-effort matrix, perform a gap analysis, identify rapid plan-do-study-act (PDSA) experiments, and develop a completion plan (Figure). Five postworkshop PDSA experiments engaged additional stakeholders, clinical application coordinators, and medical supply representatives to ascertain the feasibility of the tools implemented.
Abbreviations: BCMA, barcode medication administration; CDSS, clinical decision support system; CPRS, Computerized Patient Record System;
EHR, electronic health record; SOP, standard operating procedure; VistA, Veterans Health Information Systems and Technology Architecture.
About 3% of RLRVAMC admissions involve a pharmacy consultation to review medications for dysphagia and/or enteral feeding tubes. Clinicians reviewed 30 preimplementation inpatient pharmacy consultations involving 200 oral medications. Pharmacists were more frequently consulted for inpatients with dysphagia (19 [63%]) than for patients with enteral feeding tubes (11 [37%]) (Table 2).
Pharmacy Consultation Template
The pharmacy consultation was updated in CPRS. Prior to this QI project, the ordering clinician was prompted to select 1 option for the indication: dysphagia or enteral feeding tube. The type of enteral feeding tube was not prompted by the consultation text nor required to be specified in the consultation. The ordering clinician could provide free-text comments. Of 11 preimplementation consultations, the type of enteral feeding tube was specified in 5 (45%). The consultation template entry was updated to include an option to check a box for the consultation indication from 3 options: dysphagia, enteral feeding, or other patient- specific condition/request. If enteral feeding tube is selected, then the clinician is prompted to select the type of enteral feeding tube. Since the completion of the project, there have been no patient safety reports concerning an erroneous or incomplete consultation entry (Supplemental Material).
The note template was updated to import the list of active inpatient medications and provide sections for the adjudicating pharmacist to document which medications can be crushed (or opened), which require adjustment, and which are hazardous and require special handling. Additionally, the revised template added a statement clarifying that the documented recommendations apply only to the medication regimen at the time of the consultation (Supplemental Material).
Standardizations
There are multiple pill-crushing devices used at RLRVAMC that vary in crushing mechanism, corresponding medication pouches, and degree of protection when manipulating hazardous medications. Prior to this QI project, RLRVAMC used 3 pill-crushing devices (about 30 total devices in inpatient care areas). Only 1 device with corresponding closed pouches for preparation of hazardous medications was available, which was stored in the RLRVAMC inpatient pharmacy. This workflow resulted in waste and posed potential risks for delays in care. This project incorporated a standard pill-crushing system with the corresponding medication pouches in all inpatient care areas, which provided safeguards for clinicians to prepare and administer hazardous medications (Supplemental Material).
Patients requiring medications to be crushed or opened on discharge should receive education, written instruction, and have care plans documented in CPRS. RLRVAMC patients receive education and a printed medication list. Prior to this QI project, the instructions for crushing or opening medications could only be entered by free text in the electronic medication reconciliation tool, allowing for the potential for inconsistent language or omissions.
This QI project included an update to the electronic medication reconciliation tool. An optional checkbox selection was added for patients requiring medications to be manipulated. When checked, a radial selection for individual medications is displayed, prompting the clinician and pharmacist to indicate either do not crush tablet or OK to crush tablet. These selections appear in clinical care notes and on the printed medication list provided to the patient (Supplemental Material).
Clinical Alerts
As part of the RLRVAMC QI initiative, a CROC alert was implemented, based on the KCVAMC intervention for patients with enteral feeding tubes.13 The RLRVAMC CROC alert also included patients with dysphagia. A nursing text order was made available in CPRS for patients requiring medications and remains active throughout the duration of the patient’s admission or until discontinued. It generates CROC alerts in CPRS and VistA when new medication orders are entered and reviewed by pharmacists.
Clinicians used clinical decision support systems to create daily lists of patients receiving medications by feeding tube and patients receiving crushed/opened medications due to dysphagia. This allows pharmacists to perform a census review of all inpatients to confirm appropriateness of medication orders. Clinical alerts for patients with enteral feeding tubes are advised by the ISMP and have data demonstrating a reduction in medication errors (Supplemental Material).14,15
Sustainment
During the sustainment phase, process owners were identified and a Pharmacy Service standard operating procedure (SOP) was written. The development of an institutional do not crush medication list was discussed; however, it was determined to be difficult to develop and maintain. An institutional tertiary resource list was selected in favor of a locally developed resource. These resources include the Handbook of Drug Administration via Enteral Feeding Tubes, Third Edition, the Pharmacist’s Letter list, “Meds that Should Not be Crushed,” and the Up- ToDate Lexidrug list, “Oral Medications That Should Not Be Crushed or Altered.”9-11 Links to the resources were added to the RLRVAMC pharmacy service SharePoint. In addition to defining the preferred tertiary resources, the SOP defined the process for reviewing inventory and the process for reviewing medication orders for hazard risk.
Discussion
Continued patient safety reports and low satisfaction rates among pharmacists prompted this QI project to improve safety for patients with dysphagia and/or enteral feeding tubes at RLRVAMC. The project engaged stakeholders and also identified and addressed gaps with potential for patient harm.
The tools implemented by this initiative drew from previous work by the KCVAMC and from framework provided by the ISMP.8,13 We expanded the QI intervention to include acute care patients with dysphagia.
RLRVAMC did not take steps to track the impact of the interventions on medication errors. However, no patient safety reports concerning an erroneous or incomplete pharmacy consultation entry have been reported. We also think that it is reasonable to assume that the adoption of the safety tools described here will have a positive impact on patient safety. RLRVAMC pharmacists have noted an increased appreciation for medication safety when processing medication orders for patients with dysphagia and/or enteral feeding tubes. While the workflow took time to adopt and integrate, clinical pharmacists perceived it as an improvement in patient safety. Our future focus is aimed at translating the process improvement into the Oracle/Cerner electronic health record, which is scheduled to be deployed at the RLRVAMC in August 2026.
Limitations
This QI project did not aim to quantify or compare medication errors before and after the intervention. An accurate number of unreported errors in the medication use process for patients with dysphagia and/or enteral feeding tubes would be challenging to quantify without direct observation. Multiple clinicians are engaged in the medication use process and individual steps may not be documented at all, or documented properly. In addition, medication errors are often underreported and may not reflect the total number of errors and/or potential for errors. That said, reported medication errors in the medication use process for patients with dysphagia and/or enteral feeding tubes are reviewed on a monthly basis by the RLRVAMC Multidisciplinary Medication Safety committee to continuously improve patient safety.
Another potential limitation is the extent to which the project can be adapted at other VHA sites. For example, RLRVAMC uses CPRS; the framework and tools to improve medication safety may not translate to sites using the Oracle/Cerner electronic health record. Furthermore, this QI project included a pharmacy consultation workflow that relied on pharmacists who are available at any hour. Other facilities may not have continuous consultation coverage to review medications for patients with dysphagia and/or enteral feeding tubes.
Conclusions
This QI project drew from ISMP recommendations, previous work within the VHA, local practice, and insight from multiple disciplines on the health care team to revise and create tools to improve medication safety for patients with dysphagia and/or enteral feeding tubes in the acute care setting. These tools included a revised pharmacy consultation workflow with improvements to the pharmacy consultation template, standardization of the pill-crushing devices and language used for patient medication lists, implementation of CROC alerts within the EHR, and development of an SOP.
The RLRVAMC Pharmacy Service intends to continue reviewing patient safety reports, assessing staff perspectives, and refining (and potentially adding) tools for medication safety. Future QI initiatives may focus on improving medication safety for outpatients with dysphagia and/or enteral feeding tubes. We also hope that these tools can be adapted at other VAMCs to promote medication safety for patients with dysphagia and/or enteral feeding tubes.
- Blumenstein I, Shastri YM, Stein J. Gastroenteric tube feeding: techniques, problems and solutions. World J Gastroenterol. 2014;20:8505-8524. doi:10.3748/wjg.v20.i26.8505
- Pradaxa (dabigatran etexilate). Prescribing information. Boehringer Ingelheim Pharmaceuticals, Inc; 2025. https:// pro.boehringer-ingelheim.com/us/products/pradaxa/bipdf /pradaxa-capsules-us-pi
- Lovell AG, Protus BM, Dickman JR, et al. Palatability of crushed over-the-counter medications. J Pain Symptom Manage. 2021;61:755-762. doi:10.1016/j.jpainsymman.2020.09.020
- Messaouik D, Sautou-Miranda V, Bagel-Boithias S, et al. Comparative study and optimisation of the administration mode of three proton pump inhibitors by nasogastric tube. Int J Pharm. 2005;299:65-72. doi:10.1016/j.ijpharm.2005.04.034
- Demirkan K, Bayraktar-Ekincioglu A, Gulhan-Halil M, et al. Assessment of drug administration via feeding tube and the knowledge of health-care professionals in a university hospital. Eur J Clin Nutr. 2017;71:164-168. doi:10.1038/ejcn.2016.147
- Fodil M, Nghiem D, Colas M, et al. Assessment of clinical practices for crushing medication in geriatric units. J Nutr Health Aging. 2017;21:904-908. doi:10.1007/s12603-017-0886-3
- Zhu LL, Xu LC, Wang HQ, et al. Appropriateness of administration of nasogastric medication and preliminary intervention. Ther Clin Risk Manag. 2012;8:393-401. doi:10.2147/TCRM.S37785
- Institute for Safe Medication Practices (ISMP). Preventing errors when preparing and administering medications via enteral feeding tubes. Acute Care ISMP Medication Safety Alert. November 17, 2022. Accessed March 17, 2026. https://nutritioncare.org/wp-content/uploads/2025/02 /ISMP-Safety-Alert_Medications-and-Enteral-Feeding -Tubes.pdf
- White R, Bradnam V. Handbook of Drug Administration via Enteral Feeding Tubes. 3rd ed. Pharmaceutical Press; 2015.
- Clinical resource, meds that should not be crushed. Pharmacist’s Letter/Pharmacy Technician’s Letter/Prescriber Insights. Updated April 2025. Accessed March 17, 2026. https://pharmacist.therapeuticresearch.com/en/Content /Segments/PRL/2014/Aug/Meds-That-Should-Not-Be -Crushed-7309
- Oral medications that should not be crushed or altered. In: Lexidrug. UpToDate, Inc. https://online.lexi.com/lco /action/doc/retrieve/docid/patch_f/4227
- Uttaro E, Zhao F, Schweighardt A. Filling the gaps on the Institute for Safe Medication Practices (ISMP) do not crush list for immediate-release products. Int J Pharm Compd. 2021;25:364-371.
- US Dept of Veterans Affairs. VA Diffusion Marketplace. Improved safety of enteral tube medication administration. Updated 2024. Accessed March 17, 2026. https:// marketplace.va.gov/innovations/improved-safety-of -enteral-tube-medication-administration
- US Dept of Veterans Affairs. About us. VA Indiana Healthcare System. Updated October 17, 2024. Accessed March 2, 2026. https://www.va.gov/indiana-health-care/about-us/
- Wasylewicz ATM, van Grinsven RJB, Bikker JMW, et al. Clinical decision support system-assisted pharmacy intervention reduces feeding tube-related medication errors in hospitalized patients: a focus on medication suitable for feeding-tube administration. JPEN J Parenter Enteral Nutr. 2021;45:625-632. doi:10.1002/jpen.1869
- Blumenstein I, Shastri YM, Stein J. Gastroenteric tube feeding: techniques, problems and solutions. World J Gastroenterol. 2014;20:8505-8524. doi:10.3748/wjg.v20.i26.8505
- Pradaxa (dabigatran etexilate). Prescribing information. Boehringer Ingelheim Pharmaceuticals, Inc; 2025. https:// pro.boehringer-ingelheim.com/us/products/pradaxa/bipdf /pradaxa-capsules-us-pi
- Lovell AG, Protus BM, Dickman JR, et al. Palatability of crushed over-the-counter medications. J Pain Symptom Manage. 2021;61:755-762. doi:10.1016/j.jpainsymman.2020.09.020
- Messaouik D, Sautou-Miranda V, Bagel-Boithias S, et al. Comparative study and optimisation of the administration mode of three proton pump inhibitors by nasogastric tube. Int J Pharm. 2005;299:65-72. doi:10.1016/j.ijpharm.2005.04.034
- Demirkan K, Bayraktar-Ekincioglu A, Gulhan-Halil M, et al. Assessment of drug administration via feeding tube and the knowledge of health-care professionals in a university hospital. Eur J Clin Nutr. 2017;71:164-168. doi:10.1038/ejcn.2016.147
- Fodil M, Nghiem D, Colas M, et al. Assessment of clinical practices for crushing medication in geriatric units. J Nutr Health Aging. 2017;21:904-908. doi:10.1007/s12603-017-0886-3
- Zhu LL, Xu LC, Wang HQ, et al. Appropriateness of administration of nasogastric medication and preliminary intervention. Ther Clin Risk Manag. 2012;8:393-401. doi:10.2147/TCRM.S37785
- Institute for Safe Medication Practices (ISMP). Preventing errors when preparing and administering medications via enteral feeding tubes. Acute Care ISMP Medication Safety Alert. November 17, 2022. Accessed March 17, 2026. https://nutritioncare.org/wp-content/uploads/2025/02 /ISMP-Safety-Alert_Medications-and-Enteral-Feeding -Tubes.pdf
- White R, Bradnam V. Handbook of Drug Administration via Enteral Feeding Tubes. 3rd ed. Pharmaceutical Press; 2015.
- Clinical resource, meds that should not be crushed. Pharmacist’s Letter/Pharmacy Technician’s Letter/Prescriber Insights. Updated April 2025. Accessed March 17, 2026. https://pharmacist.therapeuticresearch.com/en/Content /Segments/PRL/2014/Aug/Meds-That-Should-Not-Be -Crushed-7309
- Oral medications that should not be crushed or altered. In: Lexidrug. UpToDate, Inc. https://online.lexi.com/lco /action/doc/retrieve/docid/patch_f/4227
- Uttaro E, Zhao F, Schweighardt A. Filling the gaps on the Institute for Safe Medication Practices (ISMP) do not crush list for immediate-release products. Int J Pharm Compd. 2021;25:364-371.
- US Dept of Veterans Affairs. VA Diffusion Marketplace. Improved safety of enteral tube medication administration. Updated 2024. Accessed March 17, 2026. https:// marketplace.va.gov/innovations/improved-safety-of -enteral-tube-medication-administration
- US Dept of Veterans Affairs. About us. VA Indiana Healthcare System. Updated October 17, 2024. Accessed March 2, 2026. https://www.va.gov/indiana-health-care/about-us/
- Wasylewicz ATM, van Grinsven RJB, Bikker JMW, et al. Clinical decision support system-assisted pharmacy intervention reduces feeding tube-related medication errors in hospitalized patients: a focus on medication suitable for feeding-tube administration. JPEN J Parenter Enteral Nutr. 2021;45:625-632. doi:10.1002/jpen.1869
Streamlining the Acute Care Pharmacy Consultation Process for Patients With Dysphagia or Enteral Feeding Tubes
Streamlining the Acute Care Pharmacy Consultation Process for Patients With Dysphagia or Enteral Feeding Tubes
