User login
ALK inhibitor alectinib shows DFS benefit in early NSCLC
Alectinib, a potent anaplastic lymphoma kinase (ALK) inhibitor, significantly improved disease-free survival (DFS) at 2 years, compared with chemotherapy, in patients with completely resected ALK+ non–small cell lung cancer (NSCLC), according to interim findings from the open-label phase 3 ALINA trial.
The , said Ben Solomon, MBBS, PhD, who presented late-breaking data from the trial at the annual meeting of the European Society for Medical Oncology.
ALINA is the first phase 3 trial of an ALK inhibitor to show a DFS benefit in completely resected stage IB-IIIA disease, said Dr. Solomon, professor and medical oncologist at Peter MacCallum Cancer Centre, Melbourne.
The current treatment recommendation for after surgery in this patient population is platinum-based chemotherapy, which is associated with modest improvements in overall survival. But multiple trials looking at alectinib in stage I-III NSCLC are underway given the unmet need for treatment in the 4%-5% of NSCLC patients with ALK rearrangements, Dr. Solomon explained.
The ALINA trial enrolled adults with good performance status and completely resected stage IB-IIIA ALK+ NSCLC. Patients were randomized 1:1 to 600 mg of oral alectinib twice daily for up to 24 months or until disease recurrence, or up to four 21-day cycles of intravenous platinum-based chemotherapy.
At median follow-up of 27.8 months, Dr. Solomon and colleagues observed an overall DFS benefit in 130 patients with stage II-IIIA disease randomized to receive alectinib, compared with the 127 patients who received chemotherapy (median DFS not reached vs. 44.4 months; hazard ratio, 0.24). The benefit was observed in the overall intention-to-treat (ITT) population of patients with stage IB-IIIA disease (median DFS not reached vs. 41.3 months; HR, 0.24).
Two-year DFS was also improved with alectinib vs. chemotherapy for stage IB (HR, 0.21), stage II (HR, 0.24), and stage IIIA disease (HR, 0.25).
The investigators observed a clinically meaningful central nervous system DFS benefit in the ITT population as well (HR, 0.22). This finding is important, given that patients with ALK+ disease have a high risk of brain metastases, which occurs in 50%-60% of patients over the course of disease, Dr. Solomon noted.
Over the treatment duration in each arm, 23.4% of patients in the alectinib arm and 25.8% in the chemotherapy arm experienced grade 3 or 4 adverse events; 5 patients in the alectinib arm and 13 in the chemotherapy arm had adverse events that led to treatment discontinuation.
“Adjuvant alectinib was tolerable and in line with the known safety profile of alectinib,” Dr. Solomon concluded, but noted that the overall survival data were not yet mature.
Invited discussant Marina Garassino, MBBS, however, cautioned against rushing to judgment, calling the DFS findings “interesting, but early.”
“Are 2 years of alectinib enough to impact overall survival? We don’t know yet,” said Dr. Garassino, professor of medicine and director of the thoracic oncology program at the University of Chicago.
Chemotherapy, conversely, has been shown to improve overall survival, she noted.
Toxicity of alectinib in the adjuvant setting may be a concern as well, she said, explaining that patients have reported numerous side effects that can affect quality of life, such as sun sensitivity, difficulty focusing, neuropathy, lower back muscle soreness, and constipation.
“So, I think we should still wait for more results from this trial,” she said.
In the meantime, she said she will ask patients “if they want this kind of toxicity in the absence of a clear overall survival benefit.”
The ALINA trial is funded by F. Hoffmann-La Roche. Dr. Solomon and Dr. Garassino each reported numerous relationships with pharmaceutical companies and other entities.
A version of this article first appeared on Medscape.com.
Alectinib, a potent anaplastic lymphoma kinase (ALK) inhibitor, significantly improved disease-free survival (DFS) at 2 years, compared with chemotherapy, in patients with completely resected ALK+ non–small cell lung cancer (NSCLC), according to interim findings from the open-label phase 3 ALINA trial.
The , said Ben Solomon, MBBS, PhD, who presented late-breaking data from the trial at the annual meeting of the European Society for Medical Oncology.
ALINA is the first phase 3 trial of an ALK inhibitor to show a DFS benefit in completely resected stage IB-IIIA disease, said Dr. Solomon, professor and medical oncologist at Peter MacCallum Cancer Centre, Melbourne.
The current treatment recommendation for after surgery in this patient population is platinum-based chemotherapy, which is associated with modest improvements in overall survival. But multiple trials looking at alectinib in stage I-III NSCLC are underway given the unmet need for treatment in the 4%-5% of NSCLC patients with ALK rearrangements, Dr. Solomon explained.
The ALINA trial enrolled adults with good performance status and completely resected stage IB-IIIA ALK+ NSCLC. Patients were randomized 1:1 to 600 mg of oral alectinib twice daily for up to 24 months or until disease recurrence, or up to four 21-day cycles of intravenous platinum-based chemotherapy.
At median follow-up of 27.8 months, Dr. Solomon and colleagues observed an overall DFS benefit in 130 patients with stage II-IIIA disease randomized to receive alectinib, compared with the 127 patients who received chemotherapy (median DFS not reached vs. 44.4 months; hazard ratio, 0.24). The benefit was observed in the overall intention-to-treat (ITT) population of patients with stage IB-IIIA disease (median DFS not reached vs. 41.3 months; HR, 0.24).
Two-year DFS was also improved with alectinib vs. chemotherapy for stage IB (HR, 0.21), stage II (HR, 0.24), and stage IIIA disease (HR, 0.25).
The investigators observed a clinically meaningful central nervous system DFS benefit in the ITT population as well (HR, 0.22). This finding is important, given that patients with ALK+ disease have a high risk of brain metastases, which occurs in 50%-60% of patients over the course of disease, Dr. Solomon noted.
Over the treatment duration in each arm, 23.4% of patients in the alectinib arm and 25.8% in the chemotherapy arm experienced grade 3 or 4 adverse events; 5 patients in the alectinib arm and 13 in the chemotherapy arm had adverse events that led to treatment discontinuation.
“Adjuvant alectinib was tolerable and in line with the known safety profile of alectinib,” Dr. Solomon concluded, but noted that the overall survival data were not yet mature.
Invited discussant Marina Garassino, MBBS, however, cautioned against rushing to judgment, calling the DFS findings “interesting, but early.”
“Are 2 years of alectinib enough to impact overall survival? We don’t know yet,” said Dr. Garassino, professor of medicine and director of the thoracic oncology program at the University of Chicago.
Chemotherapy, conversely, has been shown to improve overall survival, she noted.
Toxicity of alectinib in the adjuvant setting may be a concern as well, she said, explaining that patients have reported numerous side effects that can affect quality of life, such as sun sensitivity, difficulty focusing, neuropathy, lower back muscle soreness, and constipation.
“So, I think we should still wait for more results from this trial,” she said.
In the meantime, she said she will ask patients “if they want this kind of toxicity in the absence of a clear overall survival benefit.”
The ALINA trial is funded by F. Hoffmann-La Roche. Dr. Solomon and Dr. Garassino each reported numerous relationships with pharmaceutical companies and other entities.
A version of this article first appeared on Medscape.com.
Alectinib, a potent anaplastic lymphoma kinase (ALK) inhibitor, significantly improved disease-free survival (DFS) at 2 years, compared with chemotherapy, in patients with completely resected ALK+ non–small cell lung cancer (NSCLC), according to interim findings from the open-label phase 3 ALINA trial.
The , said Ben Solomon, MBBS, PhD, who presented late-breaking data from the trial at the annual meeting of the European Society for Medical Oncology.
ALINA is the first phase 3 trial of an ALK inhibitor to show a DFS benefit in completely resected stage IB-IIIA disease, said Dr. Solomon, professor and medical oncologist at Peter MacCallum Cancer Centre, Melbourne.
The current treatment recommendation for after surgery in this patient population is platinum-based chemotherapy, which is associated with modest improvements in overall survival. But multiple trials looking at alectinib in stage I-III NSCLC are underway given the unmet need for treatment in the 4%-5% of NSCLC patients with ALK rearrangements, Dr. Solomon explained.
The ALINA trial enrolled adults with good performance status and completely resected stage IB-IIIA ALK+ NSCLC. Patients were randomized 1:1 to 600 mg of oral alectinib twice daily for up to 24 months or until disease recurrence, or up to four 21-day cycles of intravenous platinum-based chemotherapy.
At median follow-up of 27.8 months, Dr. Solomon and colleagues observed an overall DFS benefit in 130 patients with stage II-IIIA disease randomized to receive alectinib, compared with the 127 patients who received chemotherapy (median DFS not reached vs. 44.4 months; hazard ratio, 0.24). The benefit was observed in the overall intention-to-treat (ITT) population of patients with stage IB-IIIA disease (median DFS not reached vs. 41.3 months; HR, 0.24).
Two-year DFS was also improved with alectinib vs. chemotherapy for stage IB (HR, 0.21), stage II (HR, 0.24), and stage IIIA disease (HR, 0.25).
The investigators observed a clinically meaningful central nervous system DFS benefit in the ITT population as well (HR, 0.22). This finding is important, given that patients with ALK+ disease have a high risk of brain metastases, which occurs in 50%-60% of patients over the course of disease, Dr. Solomon noted.
Over the treatment duration in each arm, 23.4% of patients in the alectinib arm and 25.8% in the chemotherapy arm experienced grade 3 or 4 adverse events; 5 patients in the alectinib arm and 13 in the chemotherapy arm had adverse events that led to treatment discontinuation.
“Adjuvant alectinib was tolerable and in line with the known safety profile of alectinib,” Dr. Solomon concluded, but noted that the overall survival data were not yet mature.
Invited discussant Marina Garassino, MBBS, however, cautioned against rushing to judgment, calling the DFS findings “interesting, but early.”
“Are 2 years of alectinib enough to impact overall survival? We don’t know yet,” said Dr. Garassino, professor of medicine and director of the thoracic oncology program at the University of Chicago.
Chemotherapy, conversely, has been shown to improve overall survival, she noted.
Toxicity of alectinib in the adjuvant setting may be a concern as well, she said, explaining that patients have reported numerous side effects that can affect quality of life, such as sun sensitivity, difficulty focusing, neuropathy, lower back muscle soreness, and constipation.
“So, I think we should still wait for more results from this trial,” she said.
In the meantime, she said she will ask patients “if they want this kind of toxicity in the absence of a clear overall survival benefit.”
The ALINA trial is funded by F. Hoffmann-La Roche. Dr. Solomon and Dr. Garassino each reported numerous relationships with pharmaceutical companies and other entities.
A version of this article first appeared on Medscape.com.
FROM ESMO CONGRESS 2023
Perioperative nivolumab improves EFS in resectable NSCLC
Neoadjuvant nivolumab (Opdivo) plus chemotherapy followed by adjuvant nivolumab led to a statistically significant and clinically meaningful improvement in event-free survival (EFS) in patients with resectable non–small cell lung cancer (NSCLC), according to interim findings from the phase 3 CheckMate 77T trial.
In the interim analysis, median EFS was not reached in 229 patients randomly assigned to the adjuvant nivolumab treatment group vs. 18.4 months in 232 patients randomly assigned to a placebo group over a minimum follow-up of 15.7 months (hazard ratio, 0.58), first author Tina Cascone, MD, reported at the annual meeting of the European Society for Medical Oncology.
“CheckMate 77T is the first phase 3 perioperative study to build on the standard of care neoadjuvant nivolumab plus chemotherapy and supports perioperative nivolumab as a potential new treatment option for patients with resectable non–small cell lung cancer,” said Dr. Cascone, associate professor in the division of cancer medicine at University of Texas MD Anderson Cancer Center, Houston.
Invited discussant Marina Garassino, MBBS, professor of medicine and director of the thoracic oncology program at the University of Chicago, noted that the “practice-changing” CheckMate 77T findings – including the “highly statistically significant impressive hazard ratio of 0.58” – add to the increasing evidence supporting perioperative immunochemotherapy in the resectable NSCLC space.
This trial is the fourth to show an EFS benefit in this setting with a perioperative approach. Most recently, Merck’s pembrolizumab (Keytruda) demonstrated improvements in both EFS and overall survival when used in the perioperative setting for patients with resectable NSCLC, according to data from the pivotal KEYNOTE-671 trial. Those findings, also presented at the ESMO congress, led to the approval this past week of pembrolizumab in that population.
The CheckMate 77T included 461 adults with untreated resectable stage IIA-IIIB NSCLC, 77% of whom underwent definitive surgery. The median age of participants was 66 years. Patients were randomly assigned to active treatment with nivolumab plus platinum-doublet chemotherapy followed by surgery and adjuvant nivolumab or placebo. The neoadjuvant nivolumab dose was 360 mg every 3 weeks for four cycles, and the adjuvant dose was 480 mg every 4 weeks for 1 year.
Overall, adding adjuvant nivolumab led to a significant improvement in EFS over a follow-up spanning 15.7-44.2 months (not reached vs. 18.4 months; HR, 0.58; P = .00025).
The EFS benefits were observed across most key subgroups but was lower in patients with stage II vs. stage III disease (HR, 0.81 vs. 0.51), and in those with programmed death-ligand 1 (PD-L1) expression of less than 1% vs. 1% or greater (HR, 0.73 vs. 0.52).
Neoadjuvant/adjuvant nivolumab also led to a significant improvement in pathological complete response (25.3% vs. 4.7%; odds ratio, 6.64) and major pathological response (35.4% vs. 12.1%; OR, 4.01) – the trial’s secondary endpoints.
In an exploratory analysis, perioperative nivolumab showed a trend toward improved EFS in patients without a pathological complete response, Dr. Cascone added.
No new safety signals were observed. Grade 3-4 treatment-related adverse events occurred in 32% of patients in the treatment arm and 25% in the placebo arm. Surgery-related adverse events occurred in 12% in each arm.
Despite the promising findings, some questions remain, said Dr. Garassino.
First, should PD-L1–negative patients and those with stage II NSCLC receive perioperative treatment? Pooled data from recent perioperative trials indicated EFS benefits in the perioperative setting for both PD-L1-negative disease (HR, 0.72) and stage II disease (HR, 0.68), she said.
So, “the answer is yes, we should treat” these patients, she said.
But a big question is whether patients who don’t achieve a pathological complete response need adjuvant therapy. “We really don’t know,” she continued. “What we know is that those patients who achieve pathological complete response do very, very well, and I think for those patients who don’t achieve pathological complete response, we have to work with new biomarkers, [circulating tumor] DNA, new drugs, and we have to run proper trials to increase the power of these patients, that unfortunately is still very low.”
CheckMate 77T is funded by Bristol-Myers Squibb. Dr. Cascone and Dr. Garassino each reported relationships (personal and institutional) with numerous pharmaceutical companies and other entities.
A version of this article first appeared on Medscape.com.
Neoadjuvant nivolumab (Opdivo) plus chemotherapy followed by adjuvant nivolumab led to a statistically significant and clinically meaningful improvement in event-free survival (EFS) in patients with resectable non–small cell lung cancer (NSCLC), according to interim findings from the phase 3 CheckMate 77T trial.
In the interim analysis, median EFS was not reached in 229 patients randomly assigned to the adjuvant nivolumab treatment group vs. 18.4 months in 232 patients randomly assigned to a placebo group over a minimum follow-up of 15.7 months (hazard ratio, 0.58), first author Tina Cascone, MD, reported at the annual meeting of the European Society for Medical Oncology.
“CheckMate 77T is the first phase 3 perioperative study to build on the standard of care neoadjuvant nivolumab plus chemotherapy and supports perioperative nivolumab as a potential new treatment option for patients with resectable non–small cell lung cancer,” said Dr. Cascone, associate professor in the division of cancer medicine at University of Texas MD Anderson Cancer Center, Houston.
Invited discussant Marina Garassino, MBBS, professor of medicine and director of the thoracic oncology program at the University of Chicago, noted that the “practice-changing” CheckMate 77T findings – including the “highly statistically significant impressive hazard ratio of 0.58” – add to the increasing evidence supporting perioperative immunochemotherapy in the resectable NSCLC space.
This trial is the fourth to show an EFS benefit in this setting with a perioperative approach. Most recently, Merck’s pembrolizumab (Keytruda) demonstrated improvements in both EFS and overall survival when used in the perioperative setting for patients with resectable NSCLC, according to data from the pivotal KEYNOTE-671 trial. Those findings, also presented at the ESMO congress, led to the approval this past week of pembrolizumab in that population.
The CheckMate 77T included 461 adults with untreated resectable stage IIA-IIIB NSCLC, 77% of whom underwent definitive surgery. The median age of participants was 66 years. Patients were randomly assigned to active treatment with nivolumab plus platinum-doublet chemotherapy followed by surgery and adjuvant nivolumab or placebo. The neoadjuvant nivolumab dose was 360 mg every 3 weeks for four cycles, and the adjuvant dose was 480 mg every 4 weeks for 1 year.
Overall, adding adjuvant nivolumab led to a significant improvement in EFS over a follow-up spanning 15.7-44.2 months (not reached vs. 18.4 months; HR, 0.58; P = .00025).
The EFS benefits were observed across most key subgroups but was lower in patients with stage II vs. stage III disease (HR, 0.81 vs. 0.51), and in those with programmed death-ligand 1 (PD-L1) expression of less than 1% vs. 1% or greater (HR, 0.73 vs. 0.52).
Neoadjuvant/adjuvant nivolumab also led to a significant improvement in pathological complete response (25.3% vs. 4.7%; odds ratio, 6.64) and major pathological response (35.4% vs. 12.1%; OR, 4.01) – the trial’s secondary endpoints.
In an exploratory analysis, perioperative nivolumab showed a trend toward improved EFS in patients without a pathological complete response, Dr. Cascone added.
No new safety signals were observed. Grade 3-4 treatment-related adverse events occurred in 32% of patients in the treatment arm and 25% in the placebo arm. Surgery-related adverse events occurred in 12% in each arm.
Despite the promising findings, some questions remain, said Dr. Garassino.
First, should PD-L1–negative patients and those with stage II NSCLC receive perioperative treatment? Pooled data from recent perioperative trials indicated EFS benefits in the perioperative setting for both PD-L1-negative disease (HR, 0.72) and stage II disease (HR, 0.68), she said.
So, “the answer is yes, we should treat” these patients, she said.
But a big question is whether patients who don’t achieve a pathological complete response need adjuvant therapy. “We really don’t know,” she continued. “What we know is that those patients who achieve pathological complete response do very, very well, and I think for those patients who don’t achieve pathological complete response, we have to work with new biomarkers, [circulating tumor] DNA, new drugs, and we have to run proper trials to increase the power of these patients, that unfortunately is still very low.”
CheckMate 77T is funded by Bristol-Myers Squibb. Dr. Cascone and Dr. Garassino each reported relationships (personal and institutional) with numerous pharmaceutical companies and other entities.
A version of this article first appeared on Medscape.com.
Neoadjuvant nivolumab (Opdivo) plus chemotherapy followed by adjuvant nivolumab led to a statistically significant and clinically meaningful improvement in event-free survival (EFS) in patients with resectable non–small cell lung cancer (NSCLC), according to interim findings from the phase 3 CheckMate 77T trial.
In the interim analysis, median EFS was not reached in 229 patients randomly assigned to the adjuvant nivolumab treatment group vs. 18.4 months in 232 patients randomly assigned to a placebo group over a minimum follow-up of 15.7 months (hazard ratio, 0.58), first author Tina Cascone, MD, reported at the annual meeting of the European Society for Medical Oncology.
“CheckMate 77T is the first phase 3 perioperative study to build on the standard of care neoadjuvant nivolumab plus chemotherapy and supports perioperative nivolumab as a potential new treatment option for patients with resectable non–small cell lung cancer,” said Dr. Cascone, associate professor in the division of cancer medicine at University of Texas MD Anderson Cancer Center, Houston.
Invited discussant Marina Garassino, MBBS, professor of medicine and director of the thoracic oncology program at the University of Chicago, noted that the “practice-changing” CheckMate 77T findings – including the “highly statistically significant impressive hazard ratio of 0.58” – add to the increasing evidence supporting perioperative immunochemotherapy in the resectable NSCLC space.
This trial is the fourth to show an EFS benefit in this setting with a perioperative approach. Most recently, Merck’s pembrolizumab (Keytruda) demonstrated improvements in both EFS and overall survival when used in the perioperative setting for patients with resectable NSCLC, according to data from the pivotal KEYNOTE-671 trial. Those findings, also presented at the ESMO congress, led to the approval this past week of pembrolizumab in that population.
The CheckMate 77T included 461 adults with untreated resectable stage IIA-IIIB NSCLC, 77% of whom underwent definitive surgery. The median age of participants was 66 years. Patients were randomly assigned to active treatment with nivolumab plus platinum-doublet chemotherapy followed by surgery and adjuvant nivolumab or placebo. The neoadjuvant nivolumab dose was 360 mg every 3 weeks for four cycles, and the adjuvant dose was 480 mg every 4 weeks for 1 year.
Overall, adding adjuvant nivolumab led to a significant improvement in EFS over a follow-up spanning 15.7-44.2 months (not reached vs. 18.4 months; HR, 0.58; P = .00025).
The EFS benefits were observed across most key subgroups but was lower in patients with stage II vs. stage III disease (HR, 0.81 vs. 0.51), and in those with programmed death-ligand 1 (PD-L1) expression of less than 1% vs. 1% or greater (HR, 0.73 vs. 0.52).
Neoadjuvant/adjuvant nivolumab also led to a significant improvement in pathological complete response (25.3% vs. 4.7%; odds ratio, 6.64) and major pathological response (35.4% vs. 12.1%; OR, 4.01) – the trial’s secondary endpoints.
In an exploratory analysis, perioperative nivolumab showed a trend toward improved EFS in patients without a pathological complete response, Dr. Cascone added.
No new safety signals were observed. Grade 3-4 treatment-related adverse events occurred in 32% of patients in the treatment arm and 25% in the placebo arm. Surgery-related adverse events occurred in 12% in each arm.
Despite the promising findings, some questions remain, said Dr. Garassino.
First, should PD-L1–negative patients and those with stage II NSCLC receive perioperative treatment? Pooled data from recent perioperative trials indicated EFS benefits in the perioperative setting for both PD-L1-negative disease (HR, 0.72) and stage II disease (HR, 0.68), she said.
So, “the answer is yes, we should treat” these patients, she said.
But a big question is whether patients who don’t achieve a pathological complete response need adjuvant therapy. “We really don’t know,” she continued. “What we know is that those patients who achieve pathological complete response do very, very well, and I think for those patients who don’t achieve pathological complete response, we have to work with new biomarkers, [circulating tumor] DNA, new drugs, and we have to run proper trials to increase the power of these patients, that unfortunately is still very low.”
CheckMate 77T is funded by Bristol-Myers Squibb. Dr. Cascone and Dr. Garassino each reported relationships (personal and institutional) with numerous pharmaceutical companies and other entities.
A version of this article first appeared on Medscape.com.
FROM ESMO CONGRESS 2023
Neoadjuvant advantages: Treating locally advanced lung cancer
Many of you saw the press release from Merck announcing that their randomized trial comparing chemo with chemo plus pembrolizumab in the neoadjuvant setting led to improved event-free survival and also improved pathologic complete response rate.
This comes in addition to the data from the AstraZeneca trial with durvalumab saying they’ve already achieved their endpoint of higher pathologic complete response rate vs. chemotherapy alone and also the data with nivolumab from Bristol-Myers Squibb saying that nivolumab plus chemotherapy leads to a better event-free survival and a better pathologic complete response rate. That information has led to Food and Drug Administration approval for their regimen.
We’re running the table with these very positive data, and I think it’s just a sign that the approach is safe and effective.
A huge question has come up. I just came from a meeting of lung cancer experts asking what to do if you have a patient with a small tumor, for example, a 3-cm tumor. Do you recommend immediate surgery followed by adjuvant therapy, chemotherapy, and then a checkpoint inhibitor if appropriate? Or do you proceed with neoadjuvant therapy if appropriate? The truth is that it’s a very difficult decision.
We have overwhelming data that the neoadjuvant approach works for that patient. Please remember that this is a clinically staged patient. This is not the patient after their surgery, where I think we have a very clear path. We have adjuvant data and adjuvant trials for those patients.
For the patient who’s in your office with a small tumor or a small tumor and only hilar lymphadenopathy, the decision there isn’t data driven, but rather it is experience driven. The data that are out there right now suggest that neoadjuvant therapy is a better way to go. Why is that?
Well, I think that the first reason is that it is probably a better regimen. I think many of you saw the recent clinical trial by Patel and colleagues in the New England Journal of Medicine with melanoma. It was an interesting trial. They gave a checkpoint inhibitor for 18 doses after surgery for melanoma versus three doses of checkpoint inhibitor, surgery, and then 15 doses of the checkpoint inhibitor.
It was 18 doses versus 18 doses, with the only difference being the three doses before surgery. Lo and behold, the three doses before surgery led to a better event-free survival.
There are preclinical data in lung cancer demonstrating that the same thing is true. Tina Cascone published on that years ago. We could talk about why, but it appears that neoadjuvant is just better.
There are other advantages to it as well. I think a big one is that all the information shows that it’s better tolerated, so you’re more likely to give all the drug. You can see if the drug isn’t working, and you can stop the drug. Also, if the drug is causing a side effect, you can see whether it’s working or not and use that decision to stop. It’s different than when you’re giving a drug in the adjuvant setting where you don’t really know whether it is working or not.
I think that it’s time to change some of our standards. When patients appear with lung cancers other than tiny ones that might be detected through screening, you need to convene your multidisciplinary group. You need to weigh the pros and cons I think that it’s time to change some of our standards. When patients appear with lung cancers other than tiny ones that might be detected through screening, you need to convene your multidisciplinary group coming in. It’s already an FDA-approved regimen with nivolumab and chemotherapy, and I think we’re moving to making that our standard of care now.
The way to handle it today, though, is to convene your multidisciplinary panel about every patient other than those with the tiniest of lung cancers and put your heads together to see what the best treatment is for that patient.
Dr. Kris is professor of medicine, Weill Cornell Medicine, and the William and Joy Ruane Chair in Thoracic Oncology, Memorial Sloan Kettering Cancer Center, both in New York. He disclosed ties with Ariad Pharmaceuticals, AstraZeneca, Pfizer, PUMA, and Roche/Genentech.
A version of this article appeared on Medscape.com.
Many of you saw the press release from Merck announcing that their randomized trial comparing chemo with chemo plus pembrolizumab in the neoadjuvant setting led to improved event-free survival and also improved pathologic complete response rate.
This comes in addition to the data from the AstraZeneca trial with durvalumab saying they’ve already achieved their endpoint of higher pathologic complete response rate vs. chemotherapy alone and also the data with nivolumab from Bristol-Myers Squibb saying that nivolumab plus chemotherapy leads to a better event-free survival and a better pathologic complete response rate. That information has led to Food and Drug Administration approval for their regimen.
We’re running the table with these very positive data, and I think it’s just a sign that the approach is safe and effective.
A huge question has come up. I just came from a meeting of lung cancer experts asking what to do if you have a patient with a small tumor, for example, a 3-cm tumor. Do you recommend immediate surgery followed by adjuvant therapy, chemotherapy, and then a checkpoint inhibitor if appropriate? Or do you proceed with neoadjuvant therapy if appropriate? The truth is that it’s a very difficult decision.
We have overwhelming data that the neoadjuvant approach works for that patient. Please remember that this is a clinically staged patient. This is not the patient after their surgery, where I think we have a very clear path. We have adjuvant data and adjuvant trials for those patients.
For the patient who’s in your office with a small tumor or a small tumor and only hilar lymphadenopathy, the decision there isn’t data driven, but rather it is experience driven. The data that are out there right now suggest that neoadjuvant therapy is a better way to go. Why is that?
Well, I think that the first reason is that it is probably a better regimen. I think many of you saw the recent clinical trial by Patel and colleagues in the New England Journal of Medicine with melanoma. It was an interesting trial. They gave a checkpoint inhibitor for 18 doses after surgery for melanoma versus three doses of checkpoint inhibitor, surgery, and then 15 doses of the checkpoint inhibitor.
It was 18 doses versus 18 doses, with the only difference being the three doses before surgery. Lo and behold, the three doses before surgery led to a better event-free survival.
There are preclinical data in lung cancer demonstrating that the same thing is true. Tina Cascone published on that years ago. We could talk about why, but it appears that neoadjuvant is just better.
There are other advantages to it as well. I think a big one is that all the information shows that it’s better tolerated, so you’re more likely to give all the drug. You can see if the drug isn’t working, and you can stop the drug. Also, if the drug is causing a side effect, you can see whether it’s working or not and use that decision to stop. It’s different than when you’re giving a drug in the adjuvant setting where you don’t really know whether it is working or not.
I think that it’s time to change some of our standards. When patients appear with lung cancers other than tiny ones that might be detected through screening, you need to convene your multidisciplinary group. You need to weigh the pros and cons I think that it’s time to change some of our standards. When patients appear with lung cancers other than tiny ones that might be detected through screening, you need to convene your multidisciplinary group coming in. It’s already an FDA-approved regimen with nivolumab and chemotherapy, and I think we’re moving to making that our standard of care now.
The way to handle it today, though, is to convene your multidisciplinary panel about every patient other than those with the tiniest of lung cancers and put your heads together to see what the best treatment is for that patient.
Dr. Kris is professor of medicine, Weill Cornell Medicine, and the William and Joy Ruane Chair in Thoracic Oncology, Memorial Sloan Kettering Cancer Center, both in New York. He disclosed ties with Ariad Pharmaceuticals, AstraZeneca, Pfizer, PUMA, and Roche/Genentech.
A version of this article appeared on Medscape.com.
Many of you saw the press release from Merck announcing that their randomized trial comparing chemo with chemo plus pembrolizumab in the neoadjuvant setting led to improved event-free survival and also improved pathologic complete response rate.
This comes in addition to the data from the AstraZeneca trial with durvalumab saying they’ve already achieved their endpoint of higher pathologic complete response rate vs. chemotherapy alone and also the data with nivolumab from Bristol-Myers Squibb saying that nivolumab plus chemotherapy leads to a better event-free survival and a better pathologic complete response rate. That information has led to Food and Drug Administration approval for their regimen.
We’re running the table with these very positive data, and I think it’s just a sign that the approach is safe and effective.
A huge question has come up. I just came from a meeting of lung cancer experts asking what to do if you have a patient with a small tumor, for example, a 3-cm tumor. Do you recommend immediate surgery followed by adjuvant therapy, chemotherapy, and then a checkpoint inhibitor if appropriate? Or do you proceed with neoadjuvant therapy if appropriate? The truth is that it’s a very difficult decision.
We have overwhelming data that the neoadjuvant approach works for that patient. Please remember that this is a clinically staged patient. This is not the patient after their surgery, where I think we have a very clear path. We have adjuvant data and adjuvant trials for those patients.
For the patient who’s in your office with a small tumor or a small tumor and only hilar lymphadenopathy, the decision there isn’t data driven, but rather it is experience driven. The data that are out there right now suggest that neoadjuvant therapy is a better way to go. Why is that?
Well, I think that the first reason is that it is probably a better regimen. I think many of you saw the recent clinical trial by Patel and colleagues in the New England Journal of Medicine with melanoma. It was an interesting trial. They gave a checkpoint inhibitor for 18 doses after surgery for melanoma versus three doses of checkpoint inhibitor, surgery, and then 15 doses of the checkpoint inhibitor.
It was 18 doses versus 18 doses, with the only difference being the three doses before surgery. Lo and behold, the three doses before surgery led to a better event-free survival.
There are preclinical data in lung cancer demonstrating that the same thing is true. Tina Cascone published on that years ago. We could talk about why, but it appears that neoadjuvant is just better.
There are other advantages to it as well. I think a big one is that all the information shows that it’s better tolerated, so you’re more likely to give all the drug. You can see if the drug isn’t working, and you can stop the drug. Also, if the drug is causing a side effect, you can see whether it’s working or not and use that decision to stop. It’s different than when you’re giving a drug in the adjuvant setting where you don’t really know whether it is working or not.
I think that it’s time to change some of our standards. When patients appear with lung cancers other than tiny ones that might be detected through screening, you need to convene your multidisciplinary group. You need to weigh the pros and cons I think that it’s time to change some of our standards. When patients appear with lung cancers other than tiny ones that might be detected through screening, you need to convene your multidisciplinary group coming in. It’s already an FDA-approved regimen with nivolumab and chemotherapy, and I think we’re moving to making that our standard of care now.
The way to handle it today, though, is to convene your multidisciplinary panel about every patient other than those with the tiniest of lung cancers and put your heads together to see what the best treatment is for that patient.
Dr. Kris is professor of medicine, Weill Cornell Medicine, and the William and Joy Ruane Chair in Thoracic Oncology, Memorial Sloan Kettering Cancer Center, both in New York. He disclosed ties with Ariad Pharmaceuticals, AstraZeneca, Pfizer, PUMA, and Roche/Genentech.
A version of this article appeared on Medscape.com.
This is how you get patients back for follow-up cancer testing
according to authors of a new study published in the Journal of the American Medical Association.
Results from the clustered, randomized clinical trial indicate that systems-based interventions, such as automating reminders in electronic health records (EHRs), outreach in the form of phone calls or letters, and assistance with barriers to health care, such as housing insecurity, can increase the number of patients who complete appropriate diagnostic follow-up after an abnormal result.
Patients who received an EHR reminder, outreach call or letter, and additional calls to screen for and assist with nine barriers to health care – housing insecurity, food insecurity, paying for basic utilities, family caregiving, legal issues, transportation, financial compensation for treatment, education, and employment – completed follow-up within 120 days of study enrollment at a rate of 31.4%. The follow-up rate was 31% for those who received only an EHR reminder and outreach, 22.7% for those who received only an EHR reminder, and 22.9% for those who received usual care.
“The benefits of cancer screening won’t be fully realized without systems to ensure timely follow-up of abnormal results,” said Anna Tosteson, ScD, director of the Dartmouth Institute for Health Policy and Clinical Practice in Lebanon, N.H., a coauthor of the study.
Current payment incentives and quality-of-care indicators focus on getting people in for screening but should also address completion of screening – meaning timely and appropriate follow-up of results that could be indicative of cancer, Dr. Tosteson said.
“There’s a disconnect if you have screening rates that are high but once people have an abnormal result, which is potentially one step closer to a cancer diagnosis, there are no systems in place to help clinicians track them,” said study coauthor Jennifer Haas, MD, director of the Center for Primary Care Research at Massachusetts General Hospital in Boston.
In a 2016 study, researchers found that follow-up rates after abnormal cancer screenings varied widely. While 95.6% of patients with abnormal breast cancer screenings underwent timely follow-up testing, only 68.1% of patients with colorectal abnormalities and 44.8% of patients with cervical abnormalities did so.
Researchers for the new study used guideline recommendations and specialist input to create automated EHR algorithms that determined a follow-up period and diagnostic test.
They put the algorithm into practice with 11,980 patients who were part of 44 primary care practices within three health networks between August 2020 and December 2021. All patients had received abnormal test results for colorectal, breast, cervical, or lung cancer in varying risk categories.
All patients received usual care from their providers, which consisted of a “hodgepodge of whatever their clinic usually does,” Dr. Haas said. Without standards and systems in place for follow-up, the burden of testing and tracking patients with abnormal results typically falls on the primary care provider.
The researchers intervened only when patients were overdue for completion of follow-up. They then staggered the interventions sequentially.
All study participants received an automated, algorithm-triggered EHR reminder for follow-up in their patient portal along with routine health maintenance reminders. To view the reminder, patients had to log into their portal. Participants in the outreach and outreach and navigation groups also received a phone call, an EHR message, or a physical letter 2 weeks after receiving an EHR notification if they hadn’t completed follow-up. Research assistants performed the outreach after having been prompted by the algorithm.
After another 4 weeks, those in the EHR, outreach, and navigation group received a call from a patient navigator who helped them address nine barriers to health care, chiefly by providing them with referrals to free resources.
Among patients who received navigation, outcomes were not significantly better than among those who received EHR and outreach, indicating social determinants of health did not significantly affect the population studied or that the modest approach to navigation and the resources provided were insufficient, Dr. Haas said.
The complexity of an automated platform that encompasses many types of cancers, test results, and other data elements could prove difficult to apply in settings with less infrastructure, said Steven Atlas, MD, MPH, director of the Practice-Based Research and Quality Improvement Network in the division of general internal medicine at Mass General.
“I think there’s a role for the federal government to take on these initiatives,” Dr. Atlas said. Government intervention could help create “national IT systems to create standards for creating code for what an abnormal result is and how it should be followed,” he said.
While interventions improved patient follow-up, the overall rates were still low.
“What concerns me is that despite the various interventions implemented to encourage and support patients to return for follow-up testing, over 60% of patients still did not return for the recommended testing,” said Joann G. Elmore, MD, MPH, professor of medicine at the University of California, Los Angeles. Dr. Elmore was not involved with the study.
The research took place during the COVID-19 pandemic, which may have reduced follow-up, the study authors wrote. Still, given that previous research has shown that follow-up tends to be low, the rates highlight “the need to understand factors associated with not completing follow-up that go beyond reminder effort,” they wrote. These include a need for patient education about the meaning of test results and what follow-up procedures involve.
The study was supported by the National Cancer Institute and the American Cancer Society. The authors have disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
according to authors of a new study published in the Journal of the American Medical Association.
Results from the clustered, randomized clinical trial indicate that systems-based interventions, such as automating reminders in electronic health records (EHRs), outreach in the form of phone calls or letters, and assistance with barriers to health care, such as housing insecurity, can increase the number of patients who complete appropriate diagnostic follow-up after an abnormal result.
Patients who received an EHR reminder, outreach call or letter, and additional calls to screen for and assist with nine barriers to health care – housing insecurity, food insecurity, paying for basic utilities, family caregiving, legal issues, transportation, financial compensation for treatment, education, and employment – completed follow-up within 120 days of study enrollment at a rate of 31.4%. The follow-up rate was 31% for those who received only an EHR reminder and outreach, 22.7% for those who received only an EHR reminder, and 22.9% for those who received usual care.
“The benefits of cancer screening won’t be fully realized without systems to ensure timely follow-up of abnormal results,” said Anna Tosteson, ScD, director of the Dartmouth Institute for Health Policy and Clinical Practice in Lebanon, N.H., a coauthor of the study.
Current payment incentives and quality-of-care indicators focus on getting people in for screening but should also address completion of screening – meaning timely and appropriate follow-up of results that could be indicative of cancer, Dr. Tosteson said.
“There’s a disconnect if you have screening rates that are high but once people have an abnormal result, which is potentially one step closer to a cancer diagnosis, there are no systems in place to help clinicians track them,” said study coauthor Jennifer Haas, MD, director of the Center for Primary Care Research at Massachusetts General Hospital in Boston.
In a 2016 study, researchers found that follow-up rates after abnormal cancer screenings varied widely. While 95.6% of patients with abnormal breast cancer screenings underwent timely follow-up testing, only 68.1% of patients with colorectal abnormalities and 44.8% of patients with cervical abnormalities did so.
Researchers for the new study used guideline recommendations and specialist input to create automated EHR algorithms that determined a follow-up period and diagnostic test.
They put the algorithm into practice with 11,980 patients who were part of 44 primary care practices within three health networks between August 2020 and December 2021. All patients had received abnormal test results for colorectal, breast, cervical, or lung cancer in varying risk categories.
All patients received usual care from their providers, which consisted of a “hodgepodge of whatever their clinic usually does,” Dr. Haas said. Without standards and systems in place for follow-up, the burden of testing and tracking patients with abnormal results typically falls on the primary care provider.
The researchers intervened only when patients were overdue for completion of follow-up. They then staggered the interventions sequentially.
All study participants received an automated, algorithm-triggered EHR reminder for follow-up in their patient portal along with routine health maintenance reminders. To view the reminder, patients had to log into their portal. Participants in the outreach and outreach and navigation groups also received a phone call, an EHR message, or a physical letter 2 weeks after receiving an EHR notification if they hadn’t completed follow-up. Research assistants performed the outreach after having been prompted by the algorithm.
After another 4 weeks, those in the EHR, outreach, and navigation group received a call from a patient navigator who helped them address nine barriers to health care, chiefly by providing them with referrals to free resources.
Among patients who received navigation, outcomes were not significantly better than among those who received EHR and outreach, indicating social determinants of health did not significantly affect the population studied or that the modest approach to navigation and the resources provided were insufficient, Dr. Haas said.
The complexity of an automated platform that encompasses many types of cancers, test results, and other data elements could prove difficult to apply in settings with less infrastructure, said Steven Atlas, MD, MPH, director of the Practice-Based Research and Quality Improvement Network in the division of general internal medicine at Mass General.
“I think there’s a role for the federal government to take on these initiatives,” Dr. Atlas said. Government intervention could help create “national IT systems to create standards for creating code for what an abnormal result is and how it should be followed,” he said.
While interventions improved patient follow-up, the overall rates were still low.
“What concerns me is that despite the various interventions implemented to encourage and support patients to return for follow-up testing, over 60% of patients still did not return for the recommended testing,” said Joann G. Elmore, MD, MPH, professor of medicine at the University of California, Los Angeles. Dr. Elmore was not involved with the study.
The research took place during the COVID-19 pandemic, which may have reduced follow-up, the study authors wrote. Still, given that previous research has shown that follow-up tends to be low, the rates highlight “the need to understand factors associated with not completing follow-up that go beyond reminder effort,” they wrote. These include a need for patient education about the meaning of test results and what follow-up procedures involve.
The study was supported by the National Cancer Institute and the American Cancer Society. The authors have disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
according to authors of a new study published in the Journal of the American Medical Association.
Results from the clustered, randomized clinical trial indicate that systems-based interventions, such as automating reminders in electronic health records (EHRs), outreach in the form of phone calls or letters, and assistance with barriers to health care, such as housing insecurity, can increase the number of patients who complete appropriate diagnostic follow-up after an abnormal result.
Patients who received an EHR reminder, outreach call or letter, and additional calls to screen for and assist with nine barriers to health care – housing insecurity, food insecurity, paying for basic utilities, family caregiving, legal issues, transportation, financial compensation for treatment, education, and employment – completed follow-up within 120 days of study enrollment at a rate of 31.4%. The follow-up rate was 31% for those who received only an EHR reminder and outreach, 22.7% for those who received only an EHR reminder, and 22.9% for those who received usual care.
“The benefits of cancer screening won’t be fully realized without systems to ensure timely follow-up of abnormal results,” said Anna Tosteson, ScD, director of the Dartmouth Institute for Health Policy and Clinical Practice in Lebanon, N.H., a coauthor of the study.
Current payment incentives and quality-of-care indicators focus on getting people in for screening but should also address completion of screening – meaning timely and appropriate follow-up of results that could be indicative of cancer, Dr. Tosteson said.
“There’s a disconnect if you have screening rates that are high but once people have an abnormal result, which is potentially one step closer to a cancer diagnosis, there are no systems in place to help clinicians track them,” said study coauthor Jennifer Haas, MD, director of the Center for Primary Care Research at Massachusetts General Hospital in Boston.
In a 2016 study, researchers found that follow-up rates after abnormal cancer screenings varied widely. While 95.6% of patients with abnormal breast cancer screenings underwent timely follow-up testing, only 68.1% of patients with colorectal abnormalities and 44.8% of patients with cervical abnormalities did so.
Researchers for the new study used guideline recommendations and specialist input to create automated EHR algorithms that determined a follow-up period and diagnostic test.
They put the algorithm into practice with 11,980 patients who were part of 44 primary care practices within three health networks between August 2020 and December 2021. All patients had received abnormal test results for colorectal, breast, cervical, or lung cancer in varying risk categories.
All patients received usual care from their providers, which consisted of a “hodgepodge of whatever their clinic usually does,” Dr. Haas said. Without standards and systems in place for follow-up, the burden of testing and tracking patients with abnormal results typically falls on the primary care provider.
The researchers intervened only when patients were overdue for completion of follow-up. They then staggered the interventions sequentially.
All study participants received an automated, algorithm-triggered EHR reminder for follow-up in their patient portal along with routine health maintenance reminders. To view the reminder, patients had to log into their portal. Participants in the outreach and outreach and navigation groups also received a phone call, an EHR message, or a physical letter 2 weeks after receiving an EHR notification if they hadn’t completed follow-up. Research assistants performed the outreach after having been prompted by the algorithm.
After another 4 weeks, those in the EHR, outreach, and navigation group received a call from a patient navigator who helped them address nine barriers to health care, chiefly by providing them with referrals to free resources.
Among patients who received navigation, outcomes were not significantly better than among those who received EHR and outreach, indicating social determinants of health did not significantly affect the population studied or that the modest approach to navigation and the resources provided were insufficient, Dr. Haas said.
The complexity of an automated platform that encompasses many types of cancers, test results, and other data elements could prove difficult to apply in settings with less infrastructure, said Steven Atlas, MD, MPH, director of the Practice-Based Research and Quality Improvement Network in the division of general internal medicine at Mass General.
“I think there’s a role for the federal government to take on these initiatives,” Dr. Atlas said. Government intervention could help create “national IT systems to create standards for creating code for what an abnormal result is and how it should be followed,” he said.
While interventions improved patient follow-up, the overall rates were still low.
“What concerns me is that despite the various interventions implemented to encourage and support patients to return for follow-up testing, over 60% of patients still did not return for the recommended testing,” said Joann G. Elmore, MD, MPH, professor of medicine at the University of California, Los Angeles. Dr. Elmore was not involved with the study.
The research took place during the COVID-19 pandemic, which may have reduced follow-up, the study authors wrote. Still, given that previous research has shown that follow-up tends to be low, the rates highlight “the need to understand factors associated with not completing follow-up that go beyond reminder effort,” they wrote. These include a need for patient education about the meaning of test results and what follow-up procedures involve.
The study was supported by the National Cancer Institute and the American Cancer Society. The authors have disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM JAMA
Higher RT doses can boost lifespan, reduce risk of death in LS-SCLC patients
SAN DIEGO – , according to a new multicenter, open-label, randomized phase III trial.
Among 224 patients in China, aged 18-70, those randomly assigned to receive volumetric-modulated arc radiotherapy of high-dose, hypofractionated thoracic radiotherapy of 54 Gy in 30 fractions had a much higher median overall survival (62.4 months) than those who received the standard dose of 45 Gy in 30 fractions (43.1 months, P = .001), reported Jiayi Yu, PhD, of Beijing University Cancer Hospital and Institute and colleagues at the annual meeting of the American Society for Radiation Oncology.
Median progression-free survival was also higher in the 54 Gy group (30.5 months vs. 16.7 months in the 45 Gy group, P = .044).
Kristin Higgins, MD, of Winship Cancer Institute of Emory University, Atlanta, provided perspective at the ASTRO session following Dr. Yu’s presentation. She noted that the study population is quite different than that of LS-SCLC patients in the United States, where patients are often older and more likely to have a history of smoking.
“We need more technical details to understand how to deliver this regimen in clinical practice, and it may not be applicable for all patients,” she said. Still, she added that “a key takeaway here is that optimizing the radiotherapy component of treatment is very important.”
Both groups received chemotherapy. “Higher-dose thoracic radiation therapy concurrently with chemotherapy is an alternative therapeutic option,” Dr. Yu said at an ASTRO presentation.
As Dr. Yu noted, twice-daily thoracic radiotherapy of 45 Gy in 30 fractions and concurrent chemotherapy has been the standard treatment for LS-SCLC for the last 20 years. Trials failed to show benefits for once-daily 66-Gy (33 fractions) or 70-Gy treatment (35 fractions), but a phase 2 trial published in 2023 did indicate that twice-daily treatment of 60 Gy (40 fractions) improved survival without boosting side effects.
For the new study, researchers tracked 224 patients from 2017 to 2021 who were previously untreated or had received specific chemotherapy treatments and had ECOG performance status scores of 0 or 1; 108 patients were randomly assigned to the 54-Gy arm and 116 to the 45-Gy arm. All were recruited at 16 public hospitals in China.
The median age in the two groups were 60 in the 54-Gy arm and 62 in the 45-Gy arm; the percentages of women were similar (45.4% and 45.7%, respectively). Most were current or former smokers (62.0% and 61.2%, respectively).
The researchers closed the trial in April 2021 because of the survival benefit in the 54-Gy arm, and patients were tracked through January 2023 for a median 45 months.
Nearly three-quarters of patients in the 54-Gy arm survived to 2 years (77.7%) vs. 53.4% in the 45-Gy arm, a 41% reduction in risk of death. Adverse events were similar between the groups, with 1 reported treatment-related death (myocardial infarction), in the 54-Gy group.
In an interview, Kenneth Rosenzweig, MD, chairman of the department of radiation oncology at Icahn School of Medicine at Mount Sinai, New York, praised the study. It’s “no surprise” that higher radiation doses are well-tolerated since “our ability to shield normal tissue has improved” over the years, said Dr. Rosenzweig, who served as a moderator of the ASTRO session where the research was presented.
However, he cautioned that hypofractionation is still “intense” and may not be appropriate for certain patients. And he added that some clinics may not be set up to provide twice-daily treatments.
Information about study funding was not provided. The study authors have no disclosures. Dr. Higgins discloses relationships with AstraZeneca and Regeneron (advisory board), Jazz (funded research), and Janssen and Picture Health (consulting). Dr. Rosenzweig has no disclosures.
SAN DIEGO – , according to a new multicenter, open-label, randomized phase III trial.
Among 224 patients in China, aged 18-70, those randomly assigned to receive volumetric-modulated arc radiotherapy of high-dose, hypofractionated thoracic radiotherapy of 54 Gy in 30 fractions had a much higher median overall survival (62.4 months) than those who received the standard dose of 45 Gy in 30 fractions (43.1 months, P = .001), reported Jiayi Yu, PhD, of Beijing University Cancer Hospital and Institute and colleagues at the annual meeting of the American Society for Radiation Oncology.
Median progression-free survival was also higher in the 54 Gy group (30.5 months vs. 16.7 months in the 45 Gy group, P = .044).
Kristin Higgins, MD, of Winship Cancer Institute of Emory University, Atlanta, provided perspective at the ASTRO session following Dr. Yu’s presentation. She noted that the study population is quite different than that of LS-SCLC patients in the United States, where patients are often older and more likely to have a history of smoking.
“We need more technical details to understand how to deliver this regimen in clinical practice, and it may not be applicable for all patients,” she said. Still, she added that “a key takeaway here is that optimizing the radiotherapy component of treatment is very important.”
Both groups received chemotherapy. “Higher-dose thoracic radiation therapy concurrently with chemotherapy is an alternative therapeutic option,” Dr. Yu said at an ASTRO presentation.
As Dr. Yu noted, twice-daily thoracic radiotherapy of 45 Gy in 30 fractions and concurrent chemotherapy has been the standard treatment for LS-SCLC for the last 20 years. Trials failed to show benefits for once-daily 66-Gy (33 fractions) or 70-Gy treatment (35 fractions), but a phase 2 trial published in 2023 did indicate that twice-daily treatment of 60 Gy (40 fractions) improved survival without boosting side effects.
For the new study, researchers tracked 224 patients from 2017 to 2021 who were previously untreated or had received specific chemotherapy treatments and had ECOG performance status scores of 0 or 1; 108 patients were randomly assigned to the 54-Gy arm and 116 to the 45-Gy arm. All were recruited at 16 public hospitals in China.
The median age in the two groups were 60 in the 54-Gy arm and 62 in the 45-Gy arm; the percentages of women were similar (45.4% and 45.7%, respectively). Most were current or former smokers (62.0% and 61.2%, respectively).
The researchers closed the trial in April 2021 because of the survival benefit in the 54-Gy arm, and patients were tracked through January 2023 for a median 45 months.
Nearly three-quarters of patients in the 54-Gy arm survived to 2 years (77.7%) vs. 53.4% in the 45-Gy arm, a 41% reduction in risk of death. Adverse events were similar between the groups, with 1 reported treatment-related death (myocardial infarction), in the 54-Gy group.
In an interview, Kenneth Rosenzweig, MD, chairman of the department of radiation oncology at Icahn School of Medicine at Mount Sinai, New York, praised the study. It’s “no surprise” that higher radiation doses are well-tolerated since “our ability to shield normal tissue has improved” over the years, said Dr. Rosenzweig, who served as a moderator of the ASTRO session where the research was presented.
However, he cautioned that hypofractionation is still “intense” and may not be appropriate for certain patients. And he added that some clinics may not be set up to provide twice-daily treatments.
Information about study funding was not provided. The study authors have no disclosures. Dr. Higgins discloses relationships with AstraZeneca and Regeneron (advisory board), Jazz (funded research), and Janssen and Picture Health (consulting). Dr. Rosenzweig has no disclosures.
SAN DIEGO – , according to a new multicenter, open-label, randomized phase III trial.
Among 224 patients in China, aged 18-70, those randomly assigned to receive volumetric-modulated arc radiotherapy of high-dose, hypofractionated thoracic radiotherapy of 54 Gy in 30 fractions had a much higher median overall survival (62.4 months) than those who received the standard dose of 45 Gy in 30 fractions (43.1 months, P = .001), reported Jiayi Yu, PhD, of Beijing University Cancer Hospital and Institute and colleagues at the annual meeting of the American Society for Radiation Oncology.
Median progression-free survival was also higher in the 54 Gy group (30.5 months vs. 16.7 months in the 45 Gy group, P = .044).
Kristin Higgins, MD, of Winship Cancer Institute of Emory University, Atlanta, provided perspective at the ASTRO session following Dr. Yu’s presentation. She noted that the study population is quite different than that of LS-SCLC patients in the United States, where patients are often older and more likely to have a history of smoking.
“We need more technical details to understand how to deliver this regimen in clinical practice, and it may not be applicable for all patients,” she said. Still, she added that “a key takeaway here is that optimizing the radiotherapy component of treatment is very important.”
Both groups received chemotherapy. “Higher-dose thoracic radiation therapy concurrently with chemotherapy is an alternative therapeutic option,” Dr. Yu said at an ASTRO presentation.
As Dr. Yu noted, twice-daily thoracic radiotherapy of 45 Gy in 30 fractions and concurrent chemotherapy has been the standard treatment for LS-SCLC for the last 20 years. Trials failed to show benefits for once-daily 66-Gy (33 fractions) or 70-Gy treatment (35 fractions), but a phase 2 trial published in 2023 did indicate that twice-daily treatment of 60 Gy (40 fractions) improved survival without boosting side effects.
For the new study, researchers tracked 224 patients from 2017 to 2021 who were previously untreated or had received specific chemotherapy treatments and had ECOG performance status scores of 0 or 1; 108 patients were randomly assigned to the 54-Gy arm and 116 to the 45-Gy arm. All were recruited at 16 public hospitals in China.
The median age in the two groups were 60 in the 54-Gy arm and 62 in the 45-Gy arm; the percentages of women were similar (45.4% and 45.7%, respectively). Most were current or former smokers (62.0% and 61.2%, respectively).
The researchers closed the trial in April 2021 because of the survival benefit in the 54-Gy arm, and patients were tracked through January 2023 for a median 45 months.
Nearly three-quarters of patients in the 54-Gy arm survived to 2 years (77.7%) vs. 53.4% in the 45-Gy arm, a 41% reduction in risk of death. Adverse events were similar between the groups, with 1 reported treatment-related death (myocardial infarction), in the 54-Gy group.
In an interview, Kenneth Rosenzweig, MD, chairman of the department of radiation oncology at Icahn School of Medicine at Mount Sinai, New York, praised the study. It’s “no surprise” that higher radiation doses are well-tolerated since “our ability to shield normal tissue has improved” over the years, said Dr. Rosenzweig, who served as a moderator of the ASTRO session where the research was presented.
However, he cautioned that hypofractionation is still “intense” and may not be appropriate for certain patients. And he added that some clinics may not be set up to provide twice-daily treatments.
Information about study funding was not provided. The study authors have no disclosures. Dr. Higgins discloses relationships with AstraZeneca and Regeneron (advisory board), Jazz (funded research), and Janssen and Picture Health (consulting). Dr. Rosenzweig has no disclosures.
AT ASTRO 2023
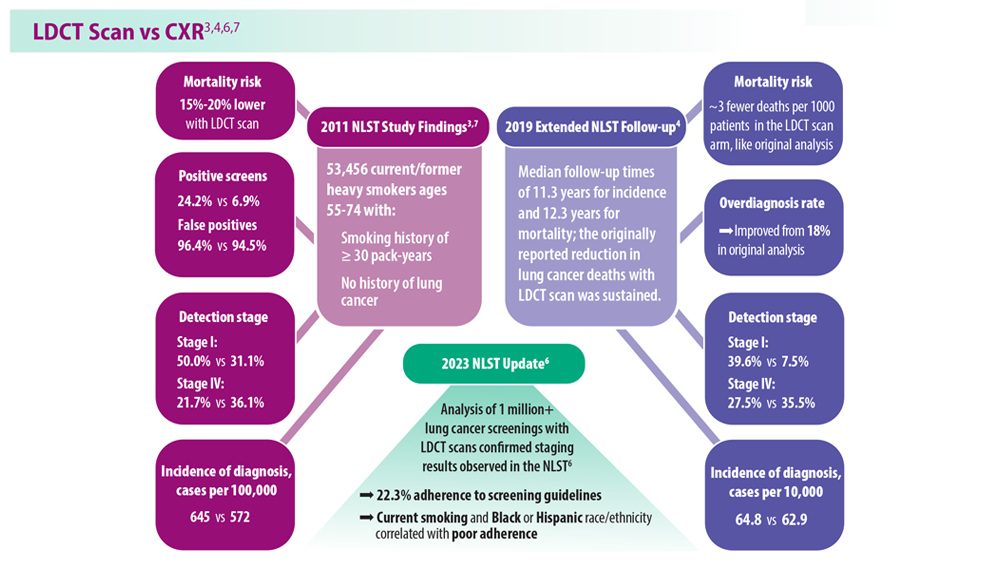
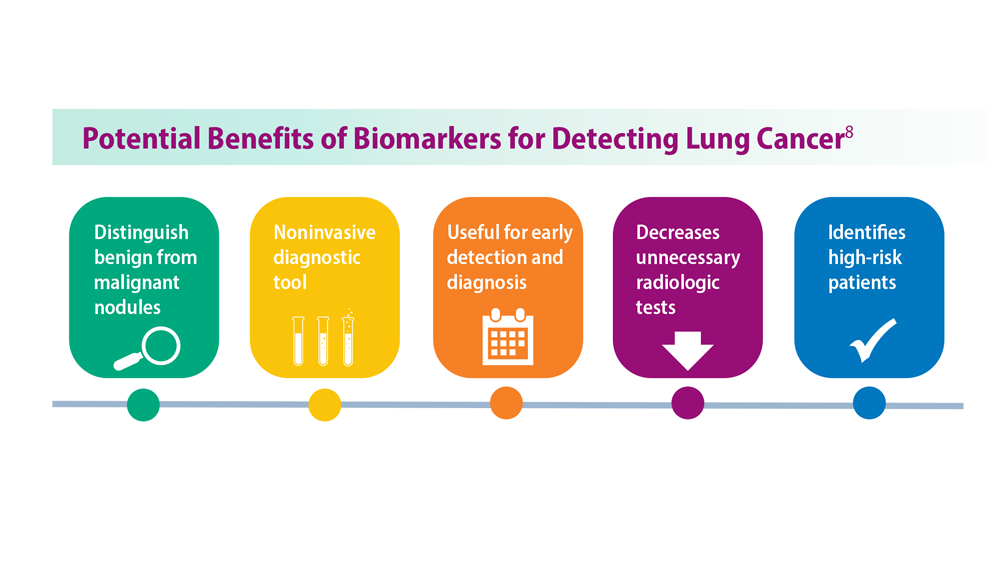
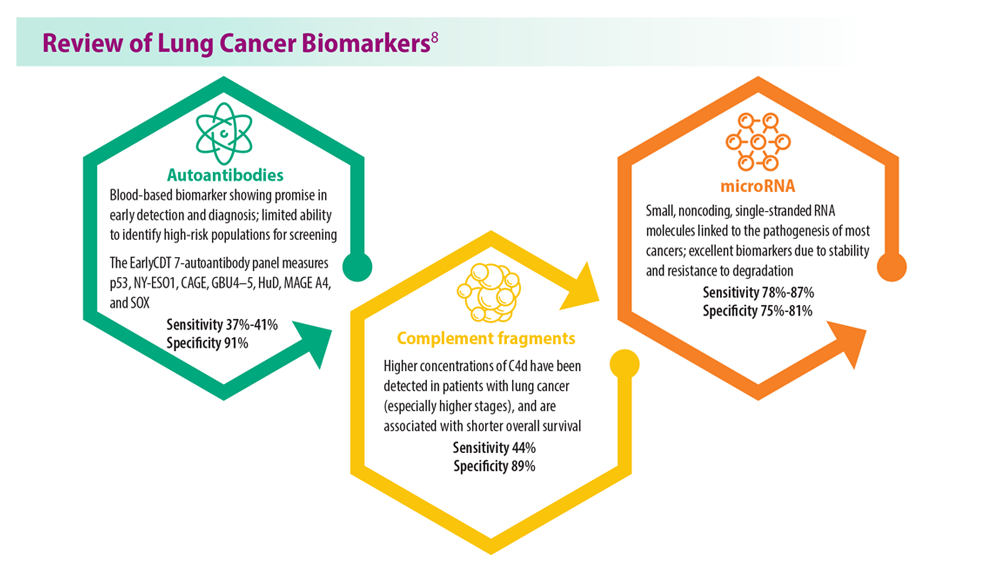
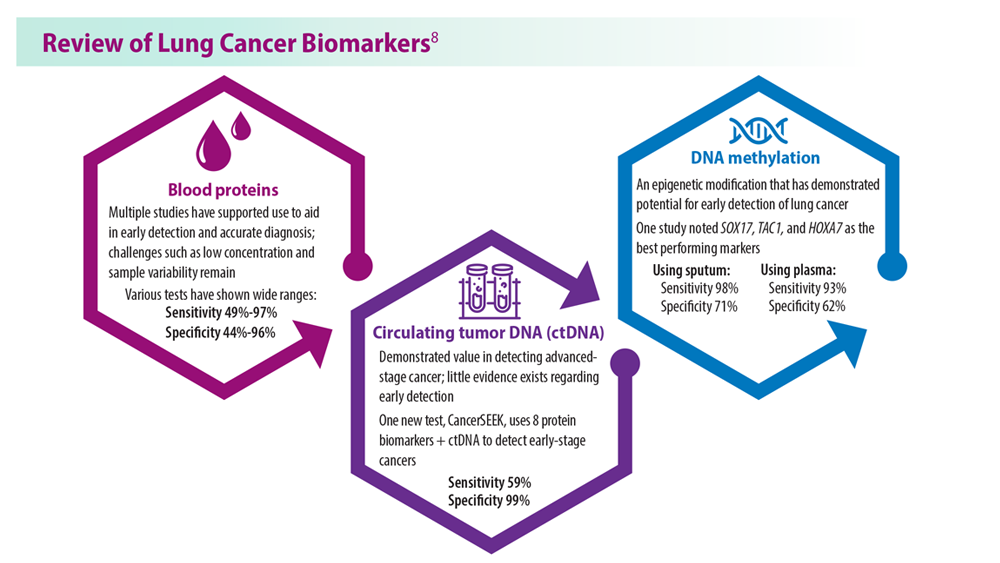
Lung Cancer Screening: A Need for Adjunctive Testing
- Naidch DP et al. Radiology. 1990;175(3):729-731. doi:10.1148/radiology.175.3.2343122
- Kaneko M et al. Radiology. 1996;201(3):798-802. doi:10.1148/radiology.201.3.8939234
- National Lung Screening Trial Research Team. Radiology. 2011;258(1):243-253. doi:10.1148/radiol.10091808
- National Lung Screening Trial Research Team. J Thorac Oncol. 2019;14(10):1732-1742. doi:10.1016/j.jtho.2019.05.044
- Mazzone PJ et al. Chest. 2021;160(5):e427-e494. doi:10.1016/j.chest.2021.06.063
- Tanner NT et al. Chest. 2023;S0012-3692(23)00175-7. doi:10.1016/j.chest.2023.02.003
- National Lung Screening Trial Research Team. N Engl J Med. 2011;365(5):395- 409. doi:10.1056/NEJMoa1102873
- Marmor HN et al. Curr Chall Thorac Surg. 2023;5:5. doi:10.21037/ccts-20-171
- Naidch DP et al. Radiology. 1990;175(3):729-731. doi:10.1148/radiology.175.3.2343122
- Kaneko M et al. Radiology. 1996;201(3):798-802. doi:10.1148/radiology.201.3.8939234
- National Lung Screening Trial Research Team. Radiology. 2011;258(1):243-253. doi:10.1148/radiol.10091808
- National Lung Screening Trial Research Team. J Thorac Oncol. 2019;14(10):1732-1742. doi:10.1016/j.jtho.2019.05.044
- Mazzone PJ et al. Chest. 2021;160(5):e427-e494. doi:10.1016/j.chest.2021.06.063
- Tanner NT et al. Chest. 2023;S0012-3692(23)00175-7. doi:10.1016/j.chest.2023.02.003
- National Lung Screening Trial Research Team. N Engl J Med. 2011;365(5):395- 409. doi:10.1056/NEJMoa1102873
- Marmor HN et al. Curr Chall Thorac Surg. 2023;5:5. doi:10.21037/ccts-20-171
- Naidch DP et al. Radiology. 1990;175(3):729-731. doi:10.1148/radiology.175.3.2343122
- Kaneko M et al. Radiology. 1996;201(3):798-802. doi:10.1148/radiology.201.3.8939234
- National Lung Screening Trial Research Team. Radiology. 2011;258(1):243-253. doi:10.1148/radiol.10091808
- National Lung Screening Trial Research Team. J Thorac Oncol. 2019;14(10):1732-1742. doi:10.1016/j.jtho.2019.05.044
- Mazzone PJ et al. Chest. 2021;160(5):e427-e494. doi:10.1016/j.chest.2021.06.063
- Tanner NT et al. Chest. 2023;S0012-3692(23)00175-7. doi:10.1016/j.chest.2023.02.003
- National Lung Screening Trial Research Team. N Engl J Med. 2011;365(5):395- 409. doi:10.1056/NEJMoa1102873
- Marmor HN et al. Curr Chall Thorac Surg. 2023;5:5. doi:10.21037/ccts-20-171
Reducing cognitive impairment from SCLC brain metastases
For patients with up to 10 brain metastases from small cell lung cancer (SCLC), stereotactic radiosurgery was associated with less cognitive impairment than whole-brain radiation therapy (WBRT) without compromising overall survival, results of the randomized ENCEPHALON (ARO 2018-9) trial suggest.
Among 56 patients with one to 10 SCLC brain metastases, 24% of those who received WBRT demonstrated significant declines in memory function 3 months after treatment, compared with 7% of patients whose metastases were treated with stereotactic radiosurgery alone. Preliminary data showed no significant differences in overall survival between the treatment groups at 6 months of follow-up, Denise Bernhardt, MD, from the Technical University of Munich, reported at the American Society of Radiation Oncology (ASTRO) annual meeting.
“We propose stereotactic radiosurgery should be an option for patients with up to 10 brain metastases in small cell lung cancer,” Dr. Bernhardt said during her presentation.
Vinai Gondi, MD, who was not involved in the study, said that the primary results from the trial – while limited by the study’s small size and missing data – are notable.
Patients with brain metastases from most cancer types typically receive stereotactic radiosurgery but WBRT has remained the standard of care to control brain metastases among patients with SCLC.
“This is the first prospective trial of radiosurgery versus whole-brain radiotherapy for small cell lung cancer brain metastases, and it’s important to recognize how important this is,” said Dr. Gondi, director of Radiation Oncology and codirector of the Brain Tumor Center at Northwestern Medicine Cancer Center, Warrenville, Ill.
Prior trials that have asked the same question did not include SCLC because many of those patients received prophylactic cranial irradiation, Dr. Gondi explained. Prophylactic cranial irradiation, however, has been on the decline among patients with brain metastases from SCLC, following a study from Japan showing no difference in survival among those who received the therapy and those followed with observation as well as evidence demonstrating significant toxicities associated with the technique.
Now “with the declining use of prophylactic cranial irradiation, the emergence of brain metastases is increasing significantly in volume in the small cell lung cancer population,” said Dr. Gondi, who is principal investigator on a phase 3 trial exploring stereotactic radiosurgery versus WBRT in a similar patient population.
In a previous retrospective trial), Dr. Bernhardt and colleagues found that first-line stereotactic radiosurgery did not compromise survival, compared with WBRT, but patients receiving stereotactic radiosurgery did have a higher risk for intracranial failure.
In the current study, the investigators compared the neurocognitive responses in patients with brain metastases from SCLC treated with stereotactic radiosurgery or WBRT.
Enrolled patients had histologically confirmed extensive disease with up to 10 metastatic brain lesions and had not previously received either therapeutic or prophylactic brain irradiation. After stratifying patients by synchronous versus metachronous disease, 56 patients were randomly assigned to either WBRT, at a total dose of 30 Gy delivered in 10 fractions, or to stereotactic radiosurgery with 20 Gy, 18 Gy, or fractionated stereotactic radiosurgery with 30 Gy in 5 Gy fractions for lesions larger than 3 cm.
The primary endpoint was neurocognition after radiation therapy as defined by a decline from baseline of at least five points on the Hopkins Verbal Learning Test-Revised (HVLT-R) total recall subscale at 3 months. Secondary endpoints included survival outcomes, additional neurocognitive assessments of motor skills, executive function, attention, memory, and processing as well as quality-of-life measures.
The investigators expected a high rate of study dropout and planned their statistical analysis accordingly, using a method for estimating the likely values of missing data based on observed data.
Among 26 patients who eventually underwent stereotactic radiosurgery, 18 did not meet the primary endpoint and 2 (7%) demonstrated declines on the HVLT-R subscale of 5 or more points. Data for the remaining 6 patients were missing.
Among the 25 who underwent WBRT, 13 did not meet the primary endpoint and 6 (24%) demonstrated declines of at least 5 points. Data for 6 of the remaining patients were missing.
Although more patients in the WBRT arm had significant declines in neurocognitive function, the difference between the groups was not significant, due to the high proportion of study dropouts – approximately one-fourth of patients in each arm. But the analysis suggested that the neuroprotective effect of stereotactic radiosurgery was notable, Dr. Bernhardt said.
At 6 months, the team also found no significant difference in the survival probability between the treatment groups (P = .36). The median time to death was 124 days among patients who received stereotactic radiosurgery and 131 days among patients who received WBRT.
Dr. Gondi said the data from ENCEPHALON, while promising, need to be carefully scrutinized because of the small sample sizes and the possibility for unintended bias.
ARO 2018-9 is an investigator-initiated trial funded by Accuray. Dr. Bernhardt disclosed consulting actives, fees, travel expenses, and research funding from Accuray and others. Dr. Gondi disclosed honoraria from UpToDate.
A version of this article appeared on Medscape.com.
For patients with up to 10 brain metastases from small cell lung cancer (SCLC), stereotactic radiosurgery was associated with less cognitive impairment than whole-brain radiation therapy (WBRT) without compromising overall survival, results of the randomized ENCEPHALON (ARO 2018-9) trial suggest.
Among 56 patients with one to 10 SCLC brain metastases, 24% of those who received WBRT demonstrated significant declines in memory function 3 months after treatment, compared with 7% of patients whose metastases were treated with stereotactic radiosurgery alone. Preliminary data showed no significant differences in overall survival between the treatment groups at 6 months of follow-up, Denise Bernhardt, MD, from the Technical University of Munich, reported at the American Society of Radiation Oncology (ASTRO) annual meeting.
“We propose stereotactic radiosurgery should be an option for patients with up to 10 brain metastases in small cell lung cancer,” Dr. Bernhardt said during her presentation.
Vinai Gondi, MD, who was not involved in the study, said that the primary results from the trial – while limited by the study’s small size and missing data – are notable.
Patients with brain metastases from most cancer types typically receive stereotactic radiosurgery but WBRT has remained the standard of care to control brain metastases among patients with SCLC.
“This is the first prospective trial of radiosurgery versus whole-brain radiotherapy for small cell lung cancer brain metastases, and it’s important to recognize how important this is,” said Dr. Gondi, director of Radiation Oncology and codirector of the Brain Tumor Center at Northwestern Medicine Cancer Center, Warrenville, Ill.
Prior trials that have asked the same question did not include SCLC because many of those patients received prophylactic cranial irradiation, Dr. Gondi explained. Prophylactic cranial irradiation, however, has been on the decline among patients with brain metastases from SCLC, following a study from Japan showing no difference in survival among those who received the therapy and those followed with observation as well as evidence demonstrating significant toxicities associated with the technique.
Now “with the declining use of prophylactic cranial irradiation, the emergence of brain metastases is increasing significantly in volume in the small cell lung cancer population,” said Dr. Gondi, who is principal investigator on a phase 3 trial exploring stereotactic radiosurgery versus WBRT in a similar patient population.
In a previous retrospective trial), Dr. Bernhardt and colleagues found that first-line stereotactic radiosurgery did not compromise survival, compared with WBRT, but patients receiving stereotactic radiosurgery did have a higher risk for intracranial failure.
In the current study, the investigators compared the neurocognitive responses in patients with brain metastases from SCLC treated with stereotactic radiosurgery or WBRT.
Enrolled patients had histologically confirmed extensive disease with up to 10 metastatic brain lesions and had not previously received either therapeutic or prophylactic brain irradiation. After stratifying patients by synchronous versus metachronous disease, 56 patients were randomly assigned to either WBRT, at a total dose of 30 Gy delivered in 10 fractions, or to stereotactic radiosurgery with 20 Gy, 18 Gy, or fractionated stereotactic radiosurgery with 30 Gy in 5 Gy fractions for lesions larger than 3 cm.
The primary endpoint was neurocognition after radiation therapy as defined by a decline from baseline of at least five points on the Hopkins Verbal Learning Test-Revised (HVLT-R) total recall subscale at 3 months. Secondary endpoints included survival outcomes, additional neurocognitive assessments of motor skills, executive function, attention, memory, and processing as well as quality-of-life measures.
The investigators expected a high rate of study dropout and planned their statistical analysis accordingly, using a method for estimating the likely values of missing data based on observed data.
Among 26 patients who eventually underwent stereotactic radiosurgery, 18 did not meet the primary endpoint and 2 (7%) demonstrated declines on the HVLT-R subscale of 5 or more points. Data for the remaining 6 patients were missing.
Among the 25 who underwent WBRT, 13 did not meet the primary endpoint and 6 (24%) demonstrated declines of at least 5 points. Data for 6 of the remaining patients were missing.
Although more patients in the WBRT arm had significant declines in neurocognitive function, the difference between the groups was not significant, due to the high proportion of study dropouts – approximately one-fourth of patients in each arm. But the analysis suggested that the neuroprotective effect of stereotactic radiosurgery was notable, Dr. Bernhardt said.
At 6 months, the team also found no significant difference in the survival probability between the treatment groups (P = .36). The median time to death was 124 days among patients who received stereotactic radiosurgery and 131 days among patients who received WBRT.
Dr. Gondi said the data from ENCEPHALON, while promising, need to be carefully scrutinized because of the small sample sizes and the possibility for unintended bias.
ARO 2018-9 is an investigator-initiated trial funded by Accuray. Dr. Bernhardt disclosed consulting actives, fees, travel expenses, and research funding from Accuray and others. Dr. Gondi disclosed honoraria from UpToDate.
A version of this article appeared on Medscape.com.
For patients with up to 10 brain metastases from small cell lung cancer (SCLC), stereotactic radiosurgery was associated with less cognitive impairment than whole-brain radiation therapy (WBRT) without compromising overall survival, results of the randomized ENCEPHALON (ARO 2018-9) trial suggest.
Among 56 patients with one to 10 SCLC brain metastases, 24% of those who received WBRT demonstrated significant declines in memory function 3 months after treatment, compared with 7% of patients whose metastases were treated with stereotactic radiosurgery alone. Preliminary data showed no significant differences in overall survival between the treatment groups at 6 months of follow-up, Denise Bernhardt, MD, from the Technical University of Munich, reported at the American Society of Radiation Oncology (ASTRO) annual meeting.
“We propose stereotactic radiosurgery should be an option for patients with up to 10 brain metastases in small cell lung cancer,” Dr. Bernhardt said during her presentation.
Vinai Gondi, MD, who was not involved in the study, said that the primary results from the trial – while limited by the study’s small size and missing data – are notable.
Patients with brain metastases from most cancer types typically receive stereotactic radiosurgery but WBRT has remained the standard of care to control brain metastases among patients with SCLC.
“This is the first prospective trial of radiosurgery versus whole-brain radiotherapy for small cell lung cancer brain metastases, and it’s important to recognize how important this is,” said Dr. Gondi, director of Radiation Oncology and codirector of the Brain Tumor Center at Northwestern Medicine Cancer Center, Warrenville, Ill.
Prior trials that have asked the same question did not include SCLC because many of those patients received prophylactic cranial irradiation, Dr. Gondi explained. Prophylactic cranial irradiation, however, has been on the decline among patients with brain metastases from SCLC, following a study from Japan showing no difference in survival among those who received the therapy and those followed with observation as well as evidence demonstrating significant toxicities associated with the technique.
Now “with the declining use of prophylactic cranial irradiation, the emergence of brain metastases is increasing significantly in volume in the small cell lung cancer population,” said Dr. Gondi, who is principal investigator on a phase 3 trial exploring stereotactic radiosurgery versus WBRT in a similar patient population.
In a previous retrospective trial), Dr. Bernhardt and colleagues found that first-line stereotactic radiosurgery did not compromise survival, compared with WBRT, but patients receiving stereotactic radiosurgery did have a higher risk for intracranial failure.
In the current study, the investigators compared the neurocognitive responses in patients with brain metastases from SCLC treated with stereotactic radiosurgery or WBRT.
Enrolled patients had histologically confirmed extensive disease with up to 10 metastatic brain lesions and had not previously received either therapeutic or prophylactic brain irradiation. After stratifying patients by synchronous versus metachronous disease, 56 patients were randomly assigned to either WBRT, at a total dose of 30 Gy delivered in 10 fractions, or to stereotactic radiosurgery with 20 Gy, 18 Gy, or fractionated stereotactic radiosurgery with 30 Gy in 5 Gy fractions for lesions larger than 3 cm.
The primary endpoint was neurocognition after radiation therapy as defined by a decline from baseline of at least five points on the Hopkins Verbal Learning Test-Revised (HVLT-R) total recall subscale at 3 months. Secondary endpoints included survival outcomes, additional neurocognitive assessments of motor skills, executive function, attention, memory, and processing as well as quality-of-life measures.
The investigators expected a high rate of study dropout and planned their statistical analysis accordingly, using a method for estimating the likely values of missing data based on observed data.
Among 26 patients who eventually underwent stereotactic radiosurgery, 18 did not meet the primary endpoint and 2 (7%) demonstrated declines on the HVLT-R subscale of 5 or more points. Data for the remaining 6 patients were missing.
Among the 25 who underwent WBRT, 13 did not meet the primary endpoint and 6 (24%) demonstrated declines of at least 5 points. Data for 6 of the remaining patients were missing.
Although more patients in the WBRT arm had significant declines in neurocognitive function, the difference between the groups was not significant, due to the high proportion of study dropouts – approximately one-fourth of patients in each arm. But the analysis suggested that the neuroprotective effect of stereotactic radiosurgery was notable, Dr. Bernhardt said.
At 6 months, the team also found no significant difference in the survival probability between the treatment groups (P = .36). The median time to death was 124 days among patients who received stereotactic radiosurgery and 131 days among patients who received WBRT.
Dr. Gondi said the data from ENCEPHALON, while promising, need to be carefully scrutinized because of the small sample sizes and the possibility for unintended bias.
ARO 2018-9 is an investigator-initiated trial funded by Accuray. Dr. Bernhardt disclosed consulting actives, fees, travel expenses, and research funding from Accuray and others. Dr. Gondi disclosed honoraria from UpToDate.
A version of this article appeared on Medscape.com.
These adverse events linked to improved cancer prognosis
TOPLINE:
.
METHODOLOGY:
- Emerging evidence suggests that the presence of cutaneous immune-related adverse events may be linked with favorable outcomes among patients with cancer who receive ICIs.
- Researchers conducted a systematic review and meta-analysis that included 23 studies and a total of 22,749 patients with cancer who received ICI treatment; studies compared outcomes among patients with and those without cutaneous immune-related adverse events.
- The major outcomes evaluated in the analysis were overall survival and progression-free survival (PFS); subgroup analyses assessed cutaneous immune-related adverse event type, cancer type, and other factors.
TAKEAWAY:
- The occurrence of cutaneous immune-related adverse events was associated with improved PFS (hazard ratio, 0.52; P < .001) and overall survival (HR, 0.61; P < .001).
- In the subgroup analysis, patients with eczematous (HR, 0.69), lichenoid or lichen planus–like skin lesions (HR, 0.51), pruritus without rash (HR, 0.70), psoriasis (HR, 0.63), or vitiligo (HR, 0.30) demonstrated a significant overall survival advantage. Vitiligo was the only adverse event associated with a PFS advantage (HR, 0.28).
- Among patients with melanoma, analyses revealed a significant association between the incidence of cutaneous immune-related adverse events and improved overall survival (HR, 0.51) and PFS (HR, 0.45). The authors highlighted similar findings among patients with non–small cell lung cancer (HR, 0.50 for overall survival and 0.61 for PFS).
IN PRACTICE:
“These data suggest that [cutaneous immune-related adverse events] may have useful prognostic value in ICI treatment,” the authors concluded.
SOURCE:
The analysis, led by Fei Wang, MD, Zhong Da Hospital, School of Medicine, Southeast University, Nanjing, China, was published online in JAMA Dermatology.
LIMITATIONS:
Most of the data came from retrospective studies, and there were limited data on specific patient subgroups. The Egger tests, used to assess potential publication bias in meta-analyses, revealed publication bias.
DISCLOSURES:
No disclosures were reported. The study was supported by a grant from the Postgraduate Research and Practice Innovation Program of Jiangsu Province.
A version of this article first appeared on Medscape.com.
TOPLINE:
.
METHODOLOGY:
- Emerging evidence suggests that the presence of cutaneous immune-related adverse events may be linked with favorable outcomes among patients with cancer who receive ICIs.
- Researchers conducted a systematic review and meta-analysis that included 23 studies and a total of 22,749 patients with cancer who received ICI treatment; studies compared outcomes among patients with and those without cutaneous immune-related adverse events.
- The major outcomes evaluated in the analysis were overall survival and progression-free survival (PFS); subgroup analyses assessed cutaneous immune-related adverse event type, cancer type, and other factors.
TAKEAWAY:
- The occurrence of cutaneous immune-related adverse events was associated with improved PFS (hazard ratio, 0.52; P < .001) and overall survival (HR, 0.61; P < .001).
- In the subgroup analysis, patients with eczematous (HR, 0.69), lichenoid or lichen planus–like skin lesions (HR, 0.51), pruritus without rash (HR, 0.70), psoriasis (HR, 0.63), or vitiligo (HR, 0.30) demonstrated a significant overall survival advantage. Vitiligo was the only adverse event associated with a PFS advantage (HR, 0.28).
- Among patients with melanoma, analyses revealed a significant association between the incidence of cutaneous immune-related adverse events and improved overall survival (HR, 0.51) and PFS (HR, 0.45). The authors highlighted similar findings among patients with non–small cell lung cancer (HR, 0.50 for overall survival and 0.61 for PFS).
IN PRACTICE:
“These data suggest that [cutaneous immune-related adverse events] may have useful prognostic value in ICI treatment,” the authors concluded.
SOURCE:
The analysis, led by Fei Wang, MD, Zhong Da Hospital, School of Medicine, Southeast University, Nanjing, China, was published online in JAMA Dermatology.
LIMITATIONS:
Most of the data came from retrospective studies, and there were limited data on specific patient subgroups. The Egger tests, used to assess potential publication bias in meta-analyses, revealed publication bias.
DISCLOSURES:
No disclosures were reported. The study was supported by a grant from the Postgraduate Research and Practice Innovation Program of Jiangsu Province.
A version of this article first appeared on Medscape.com.
TOPLINE:
.
METHODOLOGY:
- Emerging evidence suggests that the presence of cutaneous immune-related adverse events may be linked with favorable outcomes among patients with cancer who receive ICIs.
- Researchers conducted a systematic review and meta-analysis that included 23 studies and a total of 22,749 patients with cancer who received ICI treatment; studies compared outcomes among patients with and those without cutaneous immune-related adverse events.
- The major outcomes evaluated in the analysis were overall survival and progression-free survival (PFS); subgroup analyses assessed cutaneous immune-related adverse event type, cancer type, and other factors.
TAKEAWAY:
- The occurrence of cutaneous immune-related adverse events was associated with improved PFS (hazard ratio, 0.52; P < .001) and overall survival (HR, 0.61; P < .001).
- In the subgroup analysis, patients with eczematous (HR, 0.69), lichenoid or lichen planus–like skin lesions (HR, 0.51), pruritus without rash (HR, 0.70), psoriasis (HR, 0.63), or vitiligo (HR, 0.30) demonstrated a significant overall survival advantage. Vitiligo was the only adverse event associated with a PFS advantage (HR, 0.28).
- Among patients with melanoma, analyses revealed a significant association between the incidence of cutaneous immune-related adverse events and improved overall survival (HR, 0.51) and PFS (HR, 0.45). The authors highlighted similar findings among patients with non–small cell lung cancer (HR, 0.50 for overall survival and 0.61 for PFS).
IN PRACTICE:
“These data suggest that [cutaneous immune-related adverse events] may have useful prognostic value in ICI treatment,” the authors concluded.
SOURCE:
The analysis, led by Fei Wang, MD, Zhong Da Hospital, School of Medicine, Southeast University, Nanjing, China, was published online in JAMA Dermatology.
LIMITATIONS:
Most of the data came from retrospective studies, and there were limited data on specific patient subgroups. The Egger tests, used to assess potential publication bias in meta-analyses, revealed publication bias.
DISCLOSURES:
No disclosures were reported. The study was supported by a grant from the Postgraduate Research and Practice Innovation Program of Jiangsu Province.
A version of this article first appeared on Medscape.com.
Therapeutic vaccine shows promise in treating lung cancer
SINGAPORE – A few months after releasing its phase 1 and 2 data, OSE Immunotherapeutics, which is based in Nantes, France, has announced positive results for its therapeutic vaccine to treat cancer. Following its promising findings concerning early-stage melanoma, pancreatic cancer, ENT cancers, and HPV-associated anogenital cancer,
The results suggest that Tedopi is the most developmentally advanced therapeutic vaccine for cancer.
The data from Atalante-1 were presented at the World Conference on Lung Cancer and were simultaneously published in Annals of Oncology.
Tedopi is composed of synthetic tumoral neo-epitopes (peptide fragments) that target five tumoral antigens, permitting the activation of tumor-specific T-lymphocytes for patients who are HLA-A2 positive. In 95% of cases, tumors express at least one of these five antigens. The aim of integrating these five antigens is to prevent immune escape. The technology uses the human leukocyte antigen (HLA) system, one of the keys for presenting antigens to T-lymphocytes. The vaccine is effective for patients who express the HLA-A2 gene, which is present in around half of the population. The HLA-A2 biomarker, detected via a blood test, can identify appropriate patients.
Study protocol
In the Atalante-1 trial, participants had locally advanced (unresectable and not eligible for radiotherapy) or metastatic (without alteration of the EGFR and ALK genes) non–small cell lung cancer that was resistant to previous immunotherapy. They had an HLA-A2 phenotype, as determined by a blood draw to determine whether their immune system could respond to the vaccine.
In this trial, 219 patients were randomly assigned in a 2:1 ratio to receive the vaccine or standard-of-care chemotherapy (80% received docetaxel). The vaccine was administered subcutaneously on day 1 every 3 weeks for six cycles. After that point, the vaccine was administered every 8 weeks until 1 year of treatment and every 12 weeks thereafter. The primary endpoint was overall survival.
Secondary resistance
The plan was to enroll 363 patients in the protocol, but the study did not complete its recruitment phase because of the COVID-19 pandemic. As a result, the study was stopped after the enrollment of 219 patients.
“It didn’t have the power we would have liked, but it helped us understand that the people who benefited the most from the vaccine were patients who had responded to immunotherapy in the past. These patients have what is called ‘secondary resistance,’ ” explained Benjamin Besse, MD, PhD, during a press conference organized by OSE Immunotherapeutics. Dr. Besse, the study’s principal investigator, is the director of clinical research at Gustave Roussy, Villejuif, France.
Overall, the results weren’t significant. But the results were positive for patients who had previously responded well to immunotherapy for at least 3 months. Of the 219 patients, 118 (54%) had a positive response.
Among these patients with secondary resistance to immunotherapy, median OS was 11.1 months with Tedopi versus 7.5 months with docetaxel.
For these patients, the risk of death was reduced by 41% with the vaccine, compared with chemotherapy. Overall, 44% of patients lived for another year after receiving Tedopi, versus 27.5% with docetaxel.
“This study is a positive signal for overall survival in the selected population. In this study of 219 patients, we realized that just half of patients really benefited from the vaccine: those who had previously responded to immunotherapy,” said Dr. Besse. “The study needs confirmation from a further, larger phase 3 study in more than 300 patients with secondary resistance to immunotherapy to give us the statistical power we need to convince the regulatory authorities.”
Tolerability profile
Fewer serious adverse effects were reported with the vaccine than with chemotherapy (11.4% with Tedopi and 35.1% with docetaxel).
The vaccine also allowed patients to maintain a better quality of life. Scores from the Quality of Life Questionnaire Core 30, which explores several areas of daily life, were better with the vaccine. Change in patients’ overall well-being was delayed in the vaccine group: 3.3 months in the chemotherapy arm versus 9 months in the vaccine arm.
“The vaccine was well tolerated. It has benefits in terms of controlling disease symptoms and causes few side effects. Chemotherapy with docetaxel, meanwhile, is more toxic and may affect a patient’s overall well-being. It causes hair loss in practically 100% of patients, induces neuropathy, makes hands and feet swell, damages the nails, is associated with nausea and vomiting ...” noted Dr. Besse. He went on to say that after the trial, of the patients who stopped receiving the vaccine or chemotherapy (either for toxicity reasons or for disease progression), those who had been given the vaccine responded better to the subsequent chemotherapy “because their overall health was better.”
Clinical development
The clinical development of Tedopi is ongoing. Three trials are currently taking place. One study is comparing the Tedopi vaccine plus docetaxel with Tedopi plus nivolumab (immunotherapy not used as a first-line treatment) to determine whether the effects of these treatment combinations might might be enhanced for patients with previously treated lung cancer.
Another study relating to ovarian cancer is in the recruitment phase. The researchers seek to evaluate the vaccine alone or in combination with pembrolizumab for patients with platinum-sensitive ovarian cancer. Results from both trials are expected in 2025.
The third trial seeks to assess FOLFIRI as maintenance therapy or FOLFIRI as maintenance plus Tedopi for patients with pancreatic cancer to improve disease management. Efficacy data are expected next year.
OSE Immunotherapeutics is simultaneously working on a companion biomarker, the HLA-A2 test.
The study was funded by OSE Immunotherapeutics. Dr. Besse disclosed the following conflicts of interest (research funding, institution): AbbVie, Amgen, AstraZeneca, Chugai Pharmaceutical, Daiichi-Sankyo, Ellipse Pharma, EISAI, Genmab, Genzyme Corporation, Hedera Dx, Inivata, IPSEN, Janssen, MSD, Pharmamar, Roche-Genentech, Sanofi, Socar Research, Taiho Oncology, and Turning Point Therapeutics.
This article was translated from the Medscape French Edition and a version appeared on Medscape.com.
SINGAPORE – A few months after releasing its phase 1 and 2 data, OSE Immunotherapeutics, which is based in Nantes, France, has announced positive results for its therapeutic vaccine to treat cancer. Following its promising findings concerning early-stage melanoma, pancreatic cancer, ENT cancers, and HPV-associated anogenital cancer,
The results suggest that Tedopi is the most developmentally advanced therapeutic vaccine for cancer.
The data from Atalante-1 were presented at the World Conference on Lung Cancer and were simultaneously published in Annals of Oncology.
Tedopi is composed of synthetic tumoral neo-epitopes (peptide fragments) that target five tumoral antigens, permitting the activation of tumor-specific T-lymphocytes for patients who are HLA-A2 positive. In 95% of cases, tumors express at least one of these five antigens. The aim of integrating these five antigens is to prevent immune escape. The technology uses the human leukocyte antigen (HLA) system, one of the keys for presenting antigens to T-lymphocytes. The vaccine is effective for patients who express the HLA-A2 gene, which is present in around half of the population. The HLA-A2 biomarker, detected via a blood test, can identify appropriate patients.
Study protocol
In the Atalante-1 trial, participants had locally advanced (unresectable and not eligible for radiotherapy) or metastatic (without alteration of the EGFR and ALK genes) non–small cell lung cancer that was resistant to previous immunotherapy. They had an HLA-A2 phenotype, as determined by a blood draw to determine whether their immune system could respond to the vaccine.
In this trial, 219 patients were randomly assigned in a 2:1 ratio to receive the vaccine or standard-of-care chemotherapy (80% received docetaxel). The vaccine was administered subcutaneously on day 1 every 3 weeks for six cycles. After that point, the vaccine was administered every 8 weeks until 1 year of treatment and every 12 weeks thereafter. The primary endpoint was overall survival.
Secondary resistance
The plan was to enroll 363 patients in the protocol, but the study did not complete its recruitment phase because of the COVID-19 pandemic. As a result, the study was stopped after the enrollment of 219 patients.
“It didn’t have the power we would have liked, but it helped us understand that the people who benefited the most from the vaccine were patients who had responded to immunotherapy in the past. These patients have what is called ‘secondary resistance,’ ” explained Benjamin Besse, MD, PhD, during a press conference organized by OSE Immunotherapeutics. Dr. Besse, the study’s principal investigator, is the director of clinical research at Gustave Roussy, Villejuif, France.
Overall, the results weren’t significant. But the results were positive for patients who had previously responded well to immunotherapy for at least 3 months. Of the 219 patients, 118 (54%) had a positive response.
Among these patients with secondary resistance to immunotherapy, median OS was 11.1 months with Tedopi versus 7.5 months with docetaxel.
For these patients, the risk of death was reduced by 41% with the vaccine, compared with chemotherapy. Overall, 44% of patients lived for another year after receiving Tedopi, versus 27.5% with docetaxel.
“This study is a positive signal for overall survival in the selected population. In this study of 219 patients, we realized that just half of patients really benefited from the vaccine: those who had previously responded to immunotherapy,” said Dr. Besse. “The study needs confirmation from a further, larger phase 3 study in more than 300 patients with secondary resistance to immunotherapy to give us the statistical power we need to convince the regulatory authorities.”
Tolerability profile
Fewer serious adverse effects were reported with the vaccine than with chemotherapy (11.4% with Tedopi and 35.1% with docetaxel).
The vaccine also allowed patients to maintain a better quality of life. Scores from the Quality of Life Questionnaire Core 30, which explores several areas of daily life, were better with the vaccine. Change in patients’ overall well-being was delayed in the vaccine group: 3.3 months in the chemotherapy arm versus 9 months in the vaccine arm.
“The vaccine was well tolerated. It has benefits in terms of controlling disease symptoms and causes few side effects. Chemotherapy with docetaxel, meanwhile, is more toxic and may affect a patient’s overall well-being. It causes hair loss in practically 100% of patients, induces neuropathy, makes hands and feet swell, damages the nails, is associated with nausea and vomiting ...” noted Dr. Besse. He went on to say that after the trial, of the patients who stopped receiving the vaccine or chemotherapy (either for toxicity reasons or for disease progression), those who had been given the vaccine responded better to the subsequent chemotherapy “because their overall health was better.”
Clinical development
The clinical development of Tedopi is ongoing. Three trials are currently taking place. One study is comparing the Tedopi vaccine plus docetaxel with Tedopi plus nivolumab (immunotherapy not used as a first-line treatment) to determine whether the effects of these treatment combinations might might be enhanced for patients with previously treated lung cancer.
Another study relating to ovarian cancer is in the recruitment phase. The researchers seek to evaluate the vaccine alone or in combination with pembrolizumab for patients with platinum-sensitive ovarian cancer. Results from both trials are expected in 2025.
The third trial seeks to assess FOLFIRI as maintenance therapy or FOLFIRI as maintenance plus Tedopi for patients with pancreatic cancer to improve disease management. Efficacy data are expected next year.
OSE Immunotherapeutics is simultaneously working on a companion biomarker, the HLA-A2 test.
The study was funded by OSE Immunotherapeutics. Dr. Besse disclosed the following conflicts of interest (research funding, institution): AbbVie, Amgen, AstraZeneca, Chugai Pharmaceutical, Daiichi-Sankyo, Ellipse Pharma, EISAI, Genmab, Genzyme Corporation, Hedera Dx, Inivata, IPSEN, Janssen, MSD, Pharmamar, Roche-Genentech, Sanofi, Socar Research, Taiho Oncology, and Turning Point Therapeutics.
This article was translated from the Medscape French Edition and a version appeared on Medscape.com.
SINGAPORE – A few months after releasing its phase 1 and 2 data, OSE Immunotherapeutics, which is based in Nantes, France, has announced positive results for its therapeutic vaccine to treat cancer. Following its promising findings concerning early-stage melanoma, pancreatic cancer, ENT cancers, and HPV-associated anogenital cancer,
The results suggest that Tedopi is the most developmentally advanced therapeutic vaccine for cancer.
The data from Atalante-1 were presented at the World Conference on Lung Cancer and were simultaneously published in Annals of Oncology.
Tedopi is composed of synthetic tumoral neo-epitopes (peptide fragments) that target five tumoral antigens, permitting the activation of tumor-specific T-lymphocytes for patients who are HLA-A2 positive. In 95% of cases, tumors express at least one of these five antigens. The aim of integrating these five antigens is to prevent immune escape. The technology uses the human leukocyte antigen (HLA) system, one of the keys for presenting antigens to T-lymphocytes. The vaccine is effective for patients who express the HLA-A2 gene, which is present in around half of the population. The HLA-A2 biomarker, detected via a blood test, can identify appropriate patients.
Study protocol
In the Atalante-1 trial, participants had locally advanced (unresectable and not eligible for radiotherapy) or metastatic (without alteration of the EGFR and ALK genes) non–small cell lung cancer that was resistant to previous immunotherapy. They had an HLA-A2 phenotype, as determined by a blood draw to determine whether their immune system could respond to the vaccine.
In this trial, 219 patients were randomly assigned in a 2:1 ratio to receive the vaccine or standard-of-care chemotherapy (80% received docetaxel). The vaccine was administered subcutaneously on day 1 every 3 weeks for six cycles. After that point, the vaccine was administered every 8 weeks until 1 year of treatment and every 12 weeks thereafter. The primary endpoint was overall survival.
Secondary resistance
The plan was to enroll 363 patients in the protocol, but the study did not complete its recruitment phase because of the COVID-19 pandemic. As a result, the study was stopped after the enrollment of 219 patients.
“It didn’t have the power we would have liked, but it helped us understand that the people who benefited the most from the vaccine were patients who had responded to immunotherapy in the past. These patients have what is called ‘secondary resistance,’ ” explained Benjamin Besse, MD, PhD, during a press conference organized by OSE Immunotherapeutics. Dr. Besse, the study’s principal investigator, is the director of clinical research at Gustave Roussy, Villejuif, France.
Overall, the results weren’t significant. But the results were positive for patients who had previously responded well to immunotherapy for at least 3 months. Of the 219 patients, 118 (54%) had a positive response.
Among these patients with secondary resistance to immunotherapy, median OS was 11.1 months with Tedopi versus 7.5 months with docetaxel.
For these patients, the risk of death was reduced by 41% with the vaccine, compared with chemotherapy. Overall, 44% of patients lived for another year after receiving Tedopi, versus 27.5% with docetaxel.
“This study is a positive signal for overall survival in the selected population. In this study of 219 patients, we realized that just half of patients really benefited from the vaccine: those who had previously responded to immunotherapy,” said Dr. Besse. “The study needs confirmation from a further, larger phase 3 study in more than 300 patients with secondary resistance to immunotherapy to give us the statistical power we need to convince the regulatory authorities.”
Tolerability profile
Fewer serious adverse effects were reported with the vaccine than with chemotherapy (11.4% with Tedopi and 35.1% with docetaxel).
The vaccine also allowed patients to maintain a better quality of life. Scores from the Quality of Life Questionnaire Core 30, which explores several areas of daily life, were better with the vaccine. Change in patients’ overall well-being was delayed in the vaccine group: 3.3 months in the chemotherapy arm versus 9 months in the vaccine arm.
“The vaccine was well tolerated. It has benefits in terms of controlling disease symptoms and causes few side effects. Chemotherapy with docetaxel, meanwhile, is more toxic and may affect a patient’s overall well-being. It causes hair loss in practically 100% of patients, induces neuropathy, makes hands and feet swell, damages the nails, is associated with nausea and vomiting ...” noted Dr. Besse. He went on to say that after the trial, of the patients who stopped receiving the vaccine or chemotherapy (either for toxicity reasons or for disease progression), those who had been given the vaccine responded better to the subsequent chemotherapy “because their overall health was better.”
Clinical development
The clinical development of Tedopi is ongoing. Three trials are currently taking place. One study is comparing the Tedopi vaccine plus docetaxel with Tedopi plus nivolumab (immunotherapy not used as a first-line treatment) to determine whether the effects of these treatment combinations might might be enhanced for patients with previously treated lung cancer.
Another study relating to ovarian cancer is in the recruitment phase. The researchers seek to evaluate the vaccine alone or in combination with pembrolizumab for patients with platinum-sensitive ovarian cancer. Results from both trials are expected in 2025.
The third trial seeks to assess FOLFIRI as maintenance therapy or FOLFIRI as maintenance plus Tedopi for patients with pancreatic cancer to improve disease management. Efficacy data are expected next year.
OSE Immunotherapeutics is simultaneously working on a companion biomarker, the HLA-A2 test.
The study was funded by OSE Immunotherapeutics. Dr. Besse disclosed the following conflicts of interest (research funding, institution): AbbVie, Amgen, AstraZeneca, Chugai Pharmaceutical, Daiichi-Sankyo, Ellipse Pharma, EISAI, Genmab, Genzyme Corporation, Hedera Dx, Inivata, IPSEN, Janssen, MSD, Pharmamar, Roche-Genentech, Sanofi, Socar Research, Taiho Oncology, and Turning Point Therapeutics.
This article was translated from the Medscape French Edition and a version appeared on Medscape.com.
AT WCLC 2023
New ‘C word’: Cure should be the goal for patients with lung cancer
This transcript has been edited for clarity.
Hello. It’s Mark Kris from Memorial Sloan-Kettering, still musing on things I learned at ASCO 2023.
I learned that there is a new C word.
People used to be afraid to use the word “cancer,” so they would call it the C word. Hopefully we’ve gotten over that stigma, that cancer is an illness that can be fought like any other illness.
There’s a new C word now that people seem, again, afraid to use, and that word is “cure.” It’s almost a true rarity that – again, I’m talking about the lung cancer world in particular – folks use the word “cure.” I didn’t hear it at ASCO, but the truth of the matter is that’s a word we should be using and be using more.
What do our patients want? I think if you truly ask a patient what their goal of care should be, it would be to cure the illness. What I mean by “cure” is to eradicate the cancer that is in their body, keep the cancer and its effects from interfering with their ability to continue their lives, and to do it for the length of their natural life. That’s what our patients want. Yes, overall survival is important, but not as much as a life free of cancer and the burden that it puts on people having cancer in the body.
When you start thinking about cure and how to make it a goal of care, a number of issues immediately crop up. The first one is defining what is meant by “cure.” We don’t have a strict definition of cure. Again, I would probably go to the patients and ask them what they mean by it. There may be some landmark part of the definition that needs to be discussed and addressed, but again, to me it’s having your life not disturbed by cancer, and that generally comes by eradicating cancer. Living with cancer is harder than the living after cancer has been cured. But we don’t have a good definition.
We also don’t have a good way of designing clinical trials to assess whether the regimen is curative. I don’t think I’ve ever seen a trial in lung cancer that looked at the ability of any given treatment to cure patients. We need to come up with ways to design trials to do that. Now, in addition to clinical trials, we don’t have a good body of evidence to design our preclinical experiments to look for those treatments that can lead to cures, or total eradication of cancer in whatever model system might be used. If we make cure the goal, then we need to find ways preclinically to identify those strategies that could lead to that.
Also in the realm of clinical trials, we need a very clear statistical underpinning to show that one or another treatment has a better chance of cure and to show with scientific rigor that one treatment is better than the other when it comes to cure. I think there needs to be more attention to this, and as we think about revamping the clinical trial process, we need to focus more on cure.
I’m saving the most important step for last. None of this can happen unless we try to make it happen and we say cure is possible. My mentor, George Boswell, always taught us that we would, in every single patient with cancer, try to develop a curative strategy. Is there a curative strategy for this patient? If so, pursue it with all the tools and vigor that we have. We really need to think that way.
Obviously, not every patient with cancer can be cured with our current armamentarium of anticancer treatments, but we need to make sure we put it on the table. We need to [confirm] that a strategy does not currently exist that could lead to cure. And of course, if we do find that strategy, we need to pursue it with all the energy and resources that we have.
Please don’t be afraid to use the word “cure.” Our patients want that. They deserve it. We should work hard to try to provide it and work toward developing strategies that we can propose and cure more patients.
Mark G. Kris, MD, is chief of the thoracic oncology service and the William and Joy Ruane Chair in Thoracic Oncology at Memorial Sloan Kettering Cancer Center in New York. His research interests include targeted therapies for lung cancer, multimodality therapy, the development of new anticancer drugs, and symptom management with a focus on preventing emesis.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hello. It’s Mark Kris from Memorial Sloan-Kettering, still musing on things I learned at ASCO 2023.
I learned that there is a new C word.
People used to be afraid to use the word “cancer,” so they would call it the C word. Hopefully we’ve gotten over that stigma, that cancer is an illness that can be fought like any other illness.
There’s a new C word now that people seem, again, afraid to use, and that word is “cure.” It’s almost a true rarity that – again, I’m talking about the lung cancer world in particular – folks use the word “cure.” I didn’t hear it at ASCO, but the truth of the matter is that’s a word we should be using and be using more.
What do our patients want? I think if you truly ask a patient what their goal of care should be, it would be to cure the illness. What I mean by “cure” is to eradicate the cancer that is in their body, keep the cancer and its effects from interfering with their ability to continue their lives, and to do it for the length of their natural life. That’s what our patients want. Yes, overall survival is important, but not as much as a life free of cancer and the burden that it puts on people having cancer in the body.
When you start thinking about cure and how to make it a goal of care, a number of issues immediately crop up. The first one is defining what is meant by “cure.” We don’t have a strict definition of cure. Again, I would probably go to the patients and ask them what they mean by it. There may be some landmark part of the definition that needs to be discussed and addressed, but again, to me it’s having your life not disturbed by cancer, and that generally comes by eradicating cancer. Living with cancer is harder than the living after cancer has been cured. But we don’t have a good definition.
We also don’t have a good way of designing clinical trials to assess whether the regimen is curative. I don’t think I’ve ever seen a trial in lung cancer that looked at the ability of any given treatment to cure patients. We need to come up with ways to design trials to do that. Now, in addition to clinical trials, we don’t have a good body of evidence to design our preclinical experiments to look for those treatments that can lead to cures, or total eradication of cancer in whatever model system might be used. If we make cure the goal, then we need to find ways preclinically to identify those strategies that could lead to that.
Also in the realm of clinical trials, we need a very clear statistical underpinning to show that one or another treatment has a better chance of cure and to show with scientific rigor that one treatment is better than the other when it comes to cure. I think there needs to be more attention to this, and as we think about revamping the clinical trial process, we need to focus more on cure.
I’m saving the most important step for last. None of this can happen unless we try to make it happen and we say cure is possible. My mentor, George Boswell, always taught us that we would, in every single patient with cancer, try to develop a curative strategy. Is there a curative strategy for this patient? If so, pursue it with all the tools and vigor that we have. We really need to think that way.
Obviously, not every patient with cancer can be cured with our current armamentarium of anticancer treatments, but we need to make sure we put it on the table. We need to [confirm] that a strategy does not currently exist that could lead to cure. And of course, if we do find that strategy, we need to pursue it with all the energy and resources that we have.
Please don’t be afraid to use the word “cure.” Our patients want that. They deserve it. We should work hard to try to provide it and work toward developing strategies that we can propose and cure more patients.
Mark G. Kris, MD, is chief of the thoracic oncology service and the William and Joy Ruane Chair in Thoracic Oncology at Memorial Sloan Kettering Cancer Center in New York. His research interests include targeted therapies for lung cancer, multimodality therapy, the development of new anticancer drugs, and symptom management with a focus on preventing emesis.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hello. It’s Mark Kris from Memorial Sloan-Kettering, still musing on things I learned at ASCO 2023.
I learned that there is a new C word.
People used to be afraid to use the word “cancer,” so they would call it the C word. Hopefully we’ve gotten over that stigma, that cancer is an illness that can be fought like any other illness.
There’s a new C word now that people seem, again, afraid to use, and that word is “cure.” It’s almost a true rarity that – again, I’m talking about the lung cancer world in particular – folks use the word “cure.” I didn’t hear it at ASCO, but the truth of the matter is that’s a word we should be using and be using more.
What do our patients want? I think if you truly ask a patient what their goal of care should be, it would be to cure the illness. What I mean by “cure” is to eradicate the cancer that is in their body, keep the cancer and its effects from interfering with their ability to continue their lives, and to do it for the length of their natural life. That’s what our patients want. Yes, overall survival is important, but not as much as a life free of cancer and the burden that it puts on people having cancer in the body.
When you start thinking about cure and how to make it a goal of care, a number of issues immediately crop up. The first one is defining what is meant by “cure.” We don’t have a strict definition of cure. Again, I would probably go to the patients and ask them what they mean by it. There may be some landmark part of the definition that needs to be discussed and addressed, but again, to me it’s having your life not disturbed by cancer, and that generally comes by eradicating cancer. Living with cancer is harder than the living after cancer has been cured. But we don’t have a good definition.
We also don’t have a good way of designing clinical trials to assess whether the regimen is curative. I don’t think I’ve ever seen a trial in lung cancer that looked at the ability of any given treatment to cure patients. We need to come up with ways to design trials to do that. Now, in addition to clinical trials, we don’t have a good body of evidence to design our preclinical experiments to look for those treatments that can lead to cures, or total eradication of cancer in whatever model system might be used. If we make cure the goal, then we need to find ways preclinically to identify those strategies that could lead to that.
Also in the realm of clinical trials, we need a very clear statistical underpinning to show that one or another treatment has a better chance of cure and to show with scientific rigor that one treatment is better than the other when it comes to cure. I think there needs to be more attention to this, and as we think about revamping the clinical trial process, we need to focus more on cure.
I’m saving the most important step for last. None of this can happen unless we try to make it happen and we say cure is possible. My mentor, George Boswell, always taught us that we would, in every single patient with cancer, try to develop a curative strategy. Is there a curative strategy for this patient? If so, pursue it with all the tools and vigor that we have. We really need to think that way.
Obviously, not every patient with cancer can be cured with our current armamentarium of anticancer treatments, but we need to make sure we put it on the table. We need to [confirm] that a strategy does not currently exist that could lead to cure. And of course, if we do find that strategy, we need to pursue it with all the energy and resources that we have.
Please don’t be afraid to use the word “cure.” Our patients want that. They deserve it. We should work hard to try to provide it and work toward developing strategies that we can propose and cure more patients.
Mark G. Kris, MD, is chief of the thoracic oncology service and the William and Joy Ruane Chair in Thoracic Oncology at Memorial Sloan Kettering Cancer Center in New York. His research interests include targeted therapies for lung cancer, multimodality therapy, the development of new anticancer drugs, and symptom management with a focus on preventing emesis.
A version of this article first appeared on Medscape.com.