User login
For MD-IQ use only
Using Active Surveillance to Identify Monoclonal Antibody Candidates Among COVID-19–Positive Veterans in the Atlanta VA Health Care System
Early in the COVID-19 pandemic, monoclonal antibody (Mab) therapy was the only outpatient therapy for patients with COVID-19 experiencing mild-to-moderate symptoms. The Blocking Viral Attachment and Cell Entry with SARS-CoV-2 Neutralizing Antibodies (BLAZE-1) and the REGN-COV2 (Regeneron) clinical trials found participants treated with Mab had a shorter duration of symptoms and fewer hospitalizations compared with those receiving placebo.1,2 Mab therapy was most efficacious early in the disease course, and the initial US Food and Drug Administration (FDA) Emergency Use Authorization (EUA) of Mab therapies required use within 10 days of symptom onset.3
The impact of the COVID-19 pandemic has been felt disproportionately among marginalized racial and ethnic groups in the US. The COVID-19 Associated Hospitalization Surveillance Network found that non-Hispanic Black persons have significantly higher rates of hospitalization and death by COVID-19 compared with White persons.4-7 However, marginalized groups are underrepresented in the receipt of therapeutic agents for COVID-19. From March 2020 through August 2021, the mean monthly Mab use among Black patients (2.8%) was lower compared with White patients (4.0%), and Black patients received Mab 22.4% less often than White patients.7
The Mab clinical trials BLAZE-1 and REGN-COV2 study populations consisted of > 80% White participants.1,2 Receipt of COVID-19 outpatient treatments may not align with the disease burden in marginalized racial and ethnic groups, leading to health disparities. Although not exhaustive, reasons for these disparities include patient, health care practitioner, and systems-level issues: patient awareness, trust, and engagement with the health care system; health care practitioner awareness and advocacy to pursue COVID-19 treatment for the patient; and health care capacity to provide the medication and service.7
Here, we describe a novel, quality improvement initiative at the Atlanta Veterans Affairs Health Care System (AVAHCS) in Georgia that paired a proactive laboratory-based surveillance strategy to identify and engage veterans for Mab. By centralizing the surveillance and outreach process, we sought to reduce barriers to the Mab referral process and optimize access to life-saving medication.
Implementation
AVAHCS serves a diverse population of more than 129,000 (50.8% non-Hispanic Black veterans, 37.5% White veterans, and 11.7% of other races) at a main medical campus and 18 surrounding community-based outpatient clinics. From December 28, 2020, to August 31, 2021, veterans with a positive COVID-19 nasopharyngeal polymerase chain reaction (PCR) test at AVAHCS were screened daily. A central Mab team consisting of infectious disease (ID) clinical pharmacists and physicians reviewed daily lists of positive laboratory results and identified high-risk individuals for Mab eligibility, using the FDA EUA inclusion criteria. Eligible patients were called by a Mab team member to discuss Mab treatment, provide anticipatory guidance, obtain verbal consent, and schedule the infusion. Conventional referrals from non-Mab team members (eg, primary care physicians) were also accepted into the screening process and underwent the same procedures and risk prioritization strategy as those identified by the Mab team.
Clinic resources allowed for 1 to 2 patients per day to be given Mab, increasing to a maximum of 5 patients per day during the COVID-19 Delta variant surge. We followed our best clinical judgment in prioritizing patient selection, and we aligned our practice with the standards of our affiliated partner, Emory University. In circumstances where patients who were Mab-eligible outnumbered infusion availability, patients were prioritized using the Veterans Health Administration (VHA) COVID-19 (VACO) Index for 30-day COVID-19 mortality.8 As COVID-19 variants developed resistance to the recommended Mab infusions, bamlanivimab, bamlanivimab-etesevimab, or casirivimab-imdevimab, local protocols adapted to EUA revisions. The Mab team also adopted FDA eligibility criteria revisions as they were available.9,10
We describe the outcomes of our centralized screening process for Mab therapy, as measured by screening, uptake, and time to receipt of Mab from screening. We also describe the demographic and clinical characteristics of Mab recipients. Clinical outcomes include postinfusion adverse events (AEs) at day 1 and day 7, emergency department (ED) visits, inpatient hospitalization, and death.
Results
The Mab team screened 2028 veterans who were COVID-19 positive between December 28, 2020, and August 31, 2021, and identified 289 veterans (14%) who met the EUA criteria. One hundred thirty-two veterans (46%) completed Mab infusion, and of the remaining 145 veterans, 124 (86%) declined treatment, and 21 (14%) veterans did not complete Mab infusion largely due to not keeping the appointment. The Mab team active surveillance strategy identified 101 of 132 infusion candidates (77%); 82% had outpatient Mab infusion.
The mean age of veterans who received Mab was 55 years (range, 29-90), and 75% of veterans were aged ≥ 65 years; most were male (84%) and 86 (65%) identified as non-Hispanic Black individuals (Table 1).

Postinfusion AEs reported at day 1 and day 7 occurred for 38 veterans (29%) and 11 veterans (8%), respectively. Sixteen patients (12%) had postinfusion ED visit, and 12 patients (9%) required hospitalization. Eleven of the 12 hospitalized patients (92%) had worsening respiratory symptoms. No deaths occurred in the 132 patients who received Mab.
Discussion
This novel initiative to optimize access to outpatient COVID-19 treatment demonstrated how the Mab team proactively screened and reached out to eligible veterans with COVID-19 promptly. This approach removed layers in the traditional referral process that could be barriers to accessing care. More than three-quarters of patients who received Mab were identified through this strategy, and the uptake was high at 46%. Conventional passive referrals were suboptimal for identifying candidates, which was also the case at a neighboring institution.
In an Emory University study, referrals to the Mab clinic were made through a traditional, decentralized referral system and resulted in a lower uptake of Mab treatment (4.6%).11 One of the key advantages of the AVAHCS program was that we were able to provide individual education about COVID-19 and counsel on the benefits and risks of therapy. Having a structured, telehealth follow-up plan provided additional reassurance and support to the patient. These personalized patient connections likely helped increase acceptance of the Mab therapy.
Our surveillance and outreach strategy had high uptake among Black patients (65%), which exceeded the proportion of AVAHCS Black veterans (54%).12 In the Emory study, just 30% of the participants were Black patients.11 In a study of bamlanivimab use in Chicago, Black individuals represented just 11% of the study population. White patients were more likely to receive bamlanivimab compared with others races, and the likelihood of receiving bamlanivimab was significantly worse for Black patients (odds ratio, 0.28) compared with White patients.13 These studies highlight the disparity in COVID-19 outpatient treatment that does not reflect the racial and minority group representation of the community at large.
Limitations
The VHA medication allocation system at times created a significant mismatch in supply and demand, which significantly limited the AVAHCS Mab program. VHA facilities nationwide with Mab programs received discrete allocations through the US Department of Health and Human Services via VHA pharmacy benefits management services. Despite our large catchment, AVAHCS was allocated 6 or fewer doses of Mab per week during the evaluated period.
Without formal national guidance in the early period of Mab, the AVAHCS Mab team conferred with Emory University Mab clinicians as well as at other VHA facilities in the country to develop an optimal approach to resource allocation. The Mab team considered all EUA criteria to be as inclusive as possible. However, during times of high demand, our utilitarian approach tried to identify the highest-risk patients who would benefit the most from Mab. The VACO index was validated in early 2021, which facilitated decision making when demand was greater than supply. One limitation of the VACO index is its exclusion of several original Mab EUA criteria, including weight, hypertension, and nonmalignancy-related immunosuppression, into its algorithm.3,8
Conclusions
Through proactive screening and direct outreach to patients, the AVAHCS was able to achieve timely administration of Mab infusion that was well within the initial EUA time frame of 10 days and comparable with the time frame in the REGN-COV2 and BLAZE-1 trials. Improving access to resources by changing the referral structure helped engage veterans who may have otherwise missed the time frame for Mab therapy. The experience of the Mab infusion program at the AVAHCS provided valuable insight into how a health care system could effectively screen a large population and distribute the limited resource of Mab therapy in a timely and proportionate fashion among its represented demographic groups.
Acknowledgments
The authors acknowledge the Veterans Health Administration VISN 7 Clinical Resource Hub and Tele Primary Care group for their support.
1. Chen P, Nirula A, Heller B, et al; BLAZE-1 Investigators. SARS-CoV-2 neutralizing antibody LY-CoV555 in outpatients with COVID-19. N Engl J Med. 2021;384(3):229-237. doi:10.1056/NEJMoa2029849
2. Weinreich DM, Sivapalasingam S, Norton T, et al; Trial Investigators. REGN-COV2, a neutralizing antibody cocktail, in outpatients with COVID-19. N Engl J Med. 2021;384(3):238-251. doi:10.1056/NEJMoa2035002
3. US Food and Drug Administration. Fact sheet for health care providers, emergency use authorization (EUA) of bamlanivimab and etesevimab. Accessed August 6, 2023. https://www.fda.gov/media/145802/download
4. Centers for Disease Control and Prevention. Coronavirus disease 2019 (COVID-19)-associated hospitalization surveillance network (COVID-net). Updated March 24, 2023. Accessed August 6, 2023. https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covid-net/purpose-methods.html
5. Centers for Disease Control and Prevention, National Center for Health Statistics. Provisional COVID-19 deaths: distribution of deaths by race and Hispanic origin. Updated July 26, 2023. Accessed August 8, 2023. https://data.cdc.gov/NCHS/Provisional-COVID-19-Deaths-Distribution-of-Deaths/pj7m-y5uh
6. Price-Haywood EG, Burton J, Fort D, Seoane L. Hospitalization and mortality among Black patients and White patients with COVID-19. N Engl J Med. 2020;382(26):2534-2543. doi:10.1056NEJMsa2011686
7. Wiltz JL, Feehan AK, Mollinari AM, et al. Racial and ethnic disparities in receipt of medications for treatment of COVID-19 - United States, March 2020-August 2021. MMWR Morb Mortal Wkly Rep. 2022;71(3):96-102. doi:10.15585/mmwr.mm7103e1
8. King JT Jr, Yoon JS, Rentsch CT, et al. Development and validation of a 30-day mortality index based on pre-existing medical administrative data from 13,323 COVID-19 patients: the Veterans Health Administration COVID-19 (VACO) Index. PLoS One. 2020;15(11):e0241825. doi:10.1371/journal.pone.0241825
9. US Food and Drug Administration, Office of Media Affairs. Coronavirus (COVID-19) update: FDA revokes emergency use authorization for monoclonal antibody bamlanivimab. Accessed August 8, 2023. https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-revokes-emergency-use-authorization-monoclonal-antibody-bamlanivimab
10. National Institutes of Health. Information on COVID-19 treatment, prevention and research. Accessed August 8, 2023. https://www.covid19treatmentguidelines.nih.gov
11. Anderson B, Smith Z, Edupuganti S, Yan X, Masi CM, Wu HM. Effect of monoclonal antibody treatment on clinical outcomes in ambulatory patients with coronavirus disease 2019. Open Forum Infect Dis. 2021;8(7):ofab315. Published 2021 Jun 12. doi:10.1093/ofid/ofab315
12. United States Census Bureau. Quick facts: DeKalb County, Georgia. Updated July 1, 2022. Accessed August 8, 2023. www.census.gov/quickfacts/dekalbcountygeorgia
13. Kumar R, Wu EL, Stosor V, et al. Real-world experience of bamlanivimab for coronavirus disease 2019 (COVID-19): a case-control study. Clin Infect Dis. 2022;74(1):24-31. doi:10.1093/cid/ciab305
Early in the COVID-19 pandemic, monoclonal antibody (Mab) therapy was the only outpatient therapy for patients with COVID-19 experiencing mild-to-moderate symptoms. The Blocking Viral Attachment and Cell Entry with SARS-CoV-2 Neutralizing Antibodies (BLAZE-1) and the REGN-COV2 (Regeneron) clinical trials found participants treated with Mab had a shorter duration of symptoms and fewer hospitalizations compared with those receiving placebo.1,2 Mab therapy was most efficacious early in the disease course, and the initial US Food and Drug Administration (FDA) Emergency Use Authorization (EUA) of Mab therapies required use within 10 days of symptom onset.3
The impact of the COVID-19 pandemic has been felt disproportionately among marginalized racial and ethnic groups in the US. The COVID-19 Associated Hospitalization Surveillance Network found that non-Hispanic Black persons have significantly higher rates of hospitalization and death by COVID-19 compared with White persons.4-7 However, marginalized groups are underrepresented in the receipt of therapeutic agents for COVID-19. From March 2020 through August 2021, the mean monthly Mab use among Black patients (2.8%) was lower compared with White patients (4.0%), and Black patients received Mab 22.4% less often than White patients.7
The Mab clinical trials BLAZE-1 and REGN-COV2 study populations consisted of > 80% White participants.1,2 Receipt of COVID-19 outpatient treatments may not align with the disease burden in marginalized racial and ethnic groups, leading to health disparities. Although not exhaustive, reasons for these disparities include patient, health care practitioner, and systems-level issues: patient awareness, trust, and engagement with the health care system; health care practitioner awareness and advocacy to pursue COVID-19 treatment for the patient; and health care capacity to provide the medication and service.7
Here, we describe a novel, quality improvement initiative at the Atlanta Veterans Affairs Health Care System (AVAHCS) in Georgia that paired a proactive laboratory-based surveillance strategy to identify and engage veterans for Mab. By centralizing the surveillance and outreach process, we sought to reduce barriers to the Mab referral process and optimize access to life-saving medication.
Implementation
AVAHCS serves a diverse population of more than 129,000 (50.8% non-Hispanic Black veterans, 37.5% White veterans, and 11.7% of other races) at a main medical campus and 18 surrounding community-based outpatient clinics. From December 28, 2020, to August 31, 2021, veterans with a positive COVID-19 nasopharyngeal polymerase chain reaction (PCR) test at AVAHCS were screened daily. A central Mab team consisting of infectious disease (ID) clinical pharmacists and physicians reviewed daily lists of positive laboratory results and identified high-risk individuals for Mab eligibility, using the FDA EUA inclusion criteria. Eligible patients were called by a Mab team member to discuss Mab treatment, provide anticipatory guidance, obtain verbal consent, and schedule the infusion. Conventional referrals from non-Mab team members (eg, primary care physicians) were also accepted into the screening process and underwent the same procedures and risk prioritization strategy as those identified by the Mab team.
Clinic resources allowed for 1 to 2 patients per day to be given Mab, increasing to a maximum of 5 patients per day during the COVID-19 Delta variant surge. We followed our best clinical judgment in prioritizing patient selection, and we aligned our practice with the standards of our affiliated partner, Emory University. In circumstances where patients who were Mab-eligible outnumbered infusion availability, patients were prioritized using the Veterans Health Administration (VHA) COVID-19 (VACO) Index for 30-day COVID-19 mortality.8 As COVID-19 variants developed resistance to the recommended Mab infusions, bamlanivimab, bamlanivimab-etesevimab, or casirivimab-imdevimab, local protocols adapted to EUA revisions. The Mab team also adopted FDA eligibility criteria revisions as they were available.9,10
We describe the outcomes of our centralized screening process for Mab therapy, as measured by screening, uptake, and time to receipt of Mab from screening. We also describe the demographic and clinical characteristics of Mab recipients. Clinical outcomes include postinfusion adverse events (AEs) at day 1 and day 7, emergency department (ED) visits, inpatient hospitalization, and death.
Results
The Mab team screened 2028 veterans who were COVID-19 positive between December 28, 2020, and August 31, 2021, and identified 289 veterans (14%) who met the EUA criteria. One hundred thirty-two veterans (46%) completed Mab infusion, and of the remaining 145 veterans, 124 (86%) declined treatment, and 21 (14%) veterans did not complete Mab infusion largely due to not keeping the appointment. The Mab team active surveillance strategy identified 101 of 132 infusion candidates (77%); 82% had outpatient Mab infusion.
The mean age of veterans who received Mab was 55 years (range, 29-90), and 75% of veterans were aged ≥ 65 years; most were male (84%) and 86 (65%) identified as non-Hispanic Black individuals (Table 1).
Postinfusion AEs reported at day 1 and day 7 occurred for 38 veterans (29%) and 11 veterans (8%), respectively. Sixteen patients (12%) had postinfusion ED visit, and 12 patients (9%) required hospitalization. Eleven of the 12 hospitalized patients (92%) had worsening respiratory symptoms. No deaths occurred in the 132 patients who received Mab.
Discussion
This novel initiative to optimize access to outpatient COVID-19 treatment demonstrated how the Mab team proactively screened and reached out to eligible veterans with COVID-19 promptly. This approach removed layers in the traditional referral process that could be barriers to accessing care. More than three-quarters of patients who received Mab were identified through this strategy, and the uptake was high at 46%. Conventional passive referrals were suboptimal for identifying candidates, which was also the case at a neighboring institution.
In an Emory University study, referrals to the Mab clinic were made through a traditional, decentralized referral system and resulted in a lower uptake of Mab treatment (4.6%).11 One of the key advantages of the AVAHCS program was that we were able to provide individual education about COVID-19 and counsel on the benefits and risks of therapy. Having a structured, telehealth follow-up plan provided additional reassurance and support to the patient. These personalized patient connections likely helped increase acceptance of the Mab therapy.
Our surveillance and outreach strategy had high uptake among Black patients (65%), which exceeded the proportion of AVAHCS Black veterans (54%).12 In the Emory study, just 30% of the participants were Black patients.11 In a study of bamlanivimab use in Chicago, Black individuals represented just 11% of the study population. White patients were more likely to receive bamlanivimab compared with others races, and the likelihood of receiving bamlanivimab was significantly worse for Black patients (odds ratio, 0.28) compared with White patients.13 These studies highlight the disparity in COVID-19 outpatient treatment that does not reflect the racial and minority group representation of the community at large.
Limitations
The VHA medication allocation system at times created a significant mismatch in supply and demand, which significantly limited the AVAHCS Mab program. VHA facilities nationwide with Mab programs received discrete allocations through the US Department of Health and Human Services via VHA pharmacy benefits management services. Despite our large catchment, AVAHCS was allocated 6 or fewer doses of Mab per week during the evaluated period.
Without formal national guidance in the early period of Mab, the AVAHCS Mab team conferred with Emory University Mab clinicians as well as at other VHA facilities in the country to develop an optimal approach to resource allocation. The Mab team considered all EUA criteria to be as inclusive as possible. However, during times of high demand, our utilitarian approach tried to identify the highest-risk patients who would benefit the most from Mab. The VACO index was validated in early 2021, which facilitated decision making when demand was greater than supply. One limitation of the VACO index is its exclusion of several original Mab EUA criteria, including weight, hypertension, and nonmalignancy-related immunosuppression, into its algorithm.3,8
Conclusions
Through proactive screening and direct outreach to patients, the AVAHCS was able to achieve timely administration of Mab infusion that was well within the initial EUA time frame of 10 days and comparable with the time frame in the REGN-COV2 and BLAZE-1 trials. Improving access to resources by changing the referral structure helped engage veterans who may have otherwise missed the time frame for Mab therapy. The experience of the Mab infusion program at the AVAHCS provided valuable insight into how a health care system could effectively screen a large population and distribute the limited resource of Mab therapy in a timely and proportionate fashion among its represented demographic groups.
Acknowledgments
The authors acknowledge the Veterans Health Administration VISN 7 Clinical Resource Hub and Tele Primary Care group for their support.
Early in the COVID-19 pandemic, monoclonal antibody (Mab) therapy was the only outpatient therapy for patients with COVID-19 experiencing mild-to-moderate symptoms. The Blocking Viral Attachment and Cell Entry with SARS-CoV-2 Neutralizing Antibodies (BLAZE-1) and the REGN-COV2 (Regeneron) clinical trials found participants treated with Mab had a shorter duration of symptoms and fewer hospitalizations compared with those receiving placebo.1,2 Mab therapy was most efficacious early in the disease course, and the initial US Food and Drug Administration (FDA) Emergency Use Authorization (EUA) of Mab therapies required use within 10 days of symptom onset.3
The impact of the COVID-19 pandemic has been felt disproportionately among marginalized racial and ethnic groups in the US. The COVID-19 Associated Hospitalization Surveillance Network found that non-Hispanic Black persons have significantly higher rates of hospitalization and death by COVID-19 compared with White persons.4-7 However, marginalized groups are underrepresented in the receipt of therapeutic agents for COVID-19. From March 2020 through August 2021, the mean monthly Mab use among Black patients (2.8%) was lower compared with White patients (4.0%), and Black patients received Mab 22.4% less often than White patients.7
The Mab clinical trials BLAZE-1 and REGN-COV2 study populations consisted of > 80% White participants.1,2 Receipt of COVID-19 outpatient treatments may not align with the disease burden in marginalized racial and ethnic groups, leading to health disparities. Although not exhaustive, reasons for these disparities include patient, health care practitioner, and systems-level issues: patient awareness, trust, and engagement with the health care system; health care practitioner awareness and advocacy to pursue COVID-19 treatment for the patient; and health care capacity to provide the medication and service.7
Here, we describe a novel, quality improvement initiative at the Atlanta Veterans Affairs Health Care System (AVAHCS) in Georgia that paired a proactive laboratory-based surveillance strategy to identify and engage veterans for Mab. By centralizing the surveillance and outreach process, we sought to reduce barriers to the Mab referral process and optimize access to life-saving medication.
Implementation
AVAHCS serves a diverse population of more than 129,000 (50.8% non-Hispanic Black veterans, 37.5% White veterans, and 11.7% of other races) at a main medical campus and 18 surrounding community-based outpatient clinics. From December 28, 2020, to August 31, 2021, veterans with a positive COVID-19 nasopharyngeal polymerase chain reaction (PCR) test at AVAHCS were screened daily. A central Mab team consisting of infectious disease (ID) clinical pharmacists and physicians reviewed daily lists of positive laboratory results and identified high-risk individuals for Mab eligibility, using the FDA EUA inclusion criteria. Eligible patients were called by a Mab team member to discuss Mab treatment, provide anticipatory guidance, obtain verbal consent, and schedule the infusion. Conventional referrals from non-Mab team members (eg, primary care physicians) were also accepted into the screening process and underwent the same procedures and risk prioritization strategy as those identified by the Mab team.
Clinic resources allowed for 1 to 2 patients per day to be given Mab, increasing to a maximum of 5 patients per day during the COVID-19 Delta variant surge. We followed our best clinical judgment in prioritizing patient selection, and we aligned our practice with the standards of our affiliated partner, Emory University. In circumstances where patients who were Mab-eligible outnumbered infusion availability, patients were prioritized using the Veterans Health Administration (VHA) COVID-19 (VACO) Index for 30-day COVID-19 mortality.8 As COVID-19 variants developed resistance to the recommended Mab infusions, bamlanivimab, bamlanivimab-etesevimab, or casirivimab-imdevimab, local protocols adapted to EUA revisions. The Mab team also adopted FDA eligibility criteria revisions as they were available.9,10
We describe the outcomes of our centralized screening process for Mab therapy, as measured by screening, uptake, and time to receipt of Mab from screening. We also describe the demographic and clinical characteristics of Mab recipients. Clinical outcomes include postinfusion adverse events (AEs) at day 1 and day 7, emergency department (ED) visits, inpatient hospitalization, and death.
Results
The Mab team screened 2028 veterans who were COVID-19 positive between December 28, 2020, and August 31, 2021, and identified 289 veterans (14%) who met the EUA criteria. One hundred thirty-two veterans (46%) completed Mab infusion, and of the remaining 145 veterans, 124 (86%) declined treatment, and 21 (14%) veterans did not complete Mab infusion largely due to not keeping the appointment. The Mab team active surveillance strategy identified 101 of 132 infusion candidates (77%); 82% had outpatient Mab infusion.
The mean age of veterans who received Mab was 55 years (range, 29-90), and 75% of veterans were aged ≥ 65 years; most were male (84%) and 86 (65%) identified as non-Hispanic Black individuals (Table 1).
Postinfusion AEs reported at day 1 and day 7 occurred for 38 veterans (29%) and 11 veterans (8%), respectively. Sixteen patients (12%) had postinfusion ED visit, and 12 patients (9%) required hospitalization. Eleven of the 12 hospitalized patients (92%) had worsening respiratory symptoms. No deaths occurred in the 132 patients who received Mab.
Discussion
This novel initiative to optimize access to outpatient COVID-19 treatment demonstrated how the Mab team proactively screened and reached out to eligible veterans with COVID-19 promptly. This approach removed layers in the traditional referral process that could be barriers to accessing care. More than three-quarters of patients who received Mab were identified through this strategy, and the uptake was high at 46%. Conventional passive referrals were suboptimal for identifying candidates, which was also the case at a neighboring institution.
In an Emory University study, referrals to the Mab clinic were made through a traditional, decentralized referral system and resulted in a lower uptake of Mab treatment (4.6%).11 One of the key advantages of the AVAHCS program was that we were able to provide individual education about COVID-19 and counsel on the benefits and risks of therapy. Having a structured, telehealth follow-up plan provided additional reassurance and support to the patient. These personalized patient connections likely helped increase acceptance of the Mab therapy.
Our surveillance and outreach strategy had high uptake among Black patients (65%), which exceeded the proportion of AVAHCS Black veterans (54%).12 In the Emory study, just 30% of the participants were Black patients.11 In a study of bamlanivimab use in Chicago, Black individuals represented just 11% of the study population. White patients were more likely to receive bamlanivimab compared with others races, and the likelihood of receiving bamlanivimab was significantly worse for Black patients (odds ratio, 0.28) compared with White patients.13 These studies highlight the disparity in COVID-19 outpatient treatment that does not reflect the racial and minority group representation of the community at large.
Limitations
The VHA medication allocation system at times created a significant mismatch in supply and demand, which significantly limited the AVAHCS Mab program. VHA facilities nationwide with Mab programs received discrete allocations through the US Department of Health and Human Services via VHA pharmacy benefits management services. Despite our large catchment, AVAHCS was allocated 6 or fewer doses of Mab per week during the evaluated period.
Without formal national guidance in the early period of Mab, the AVAHCS Mab team conferred with Emory University Mab clinicians as well as at other VHA facilities in the country to develop an optimal approach to resource allocation. The Mab team considered all EUA criteria to be as inclusive as possible. However, during times of high demand, our utilitarian approach tried to identify the highest-risk patients who would benefit the most from Mab. The VACO index was validated in early 2021, which facilitated decision making when demand was greater than supply. One limitation of the VACO index is its exclusion of several original Mab EUA criteria, including weight, hypertension, and nonmalignancy-related immunosuppression, into its algorithm.3,8
Conclusions
Through proactive screening and direct outreach to patients, the AVAHCS was able to achieve timely administration of Mab infusion that was well within the initial EUA time frame of 10 days and comparable with the time frame in the REGN-COV2 and BLAZE-1 trials. Improving access to resources by changing the referral structure helped engage veterans who may have otherwise missed the time frame for Mab therapy. The experience of the Mab infusion program at the AVAHCS provided valuable insight into how a health care system could effectively screen a large population and distribute the limited resource of Mab therapy in a timely and proportionate fashion among its represented demographic groups.
Acknowledgments
The authors acknowledge the Veterans Health Administration VISN 7 Clinical Resource Hub and Tele Primary Care group for their support.
1. Chen P, Nirula A, Heller B, et al; BLAZE-1 Investigators. SARS-CoV-2 neutralizing antibody LY-CoV555 in outpatients with COVID-19. N Engl J Med. 2021;384(3):229-237. doi:10.1056/NEJMoa2029849
2. Weinreich DM, Sivapalasingam S, Norton T, et al; Trial Investigators. REGN-COV2, a neutralizing antibody cocktail, in outpatients with COVID-19. N Engl J Med. 2021;384(3):238-251. doi:10.1056/NEJMoa2035002
3. US Food and Drug Administration. Fact sheet for health care providers, emergency use authorization (EUA) of bamlanivimab and etesevimab. Accessed August 6, 2023. https://www.fda.gov/media/145802/download
4. Centers for Disease Control and Prevention. Coronavirus disease 2019 (COVID-19)-associated hospitalization surveillance network (COVID-net). Updated March 24, 2023. Accessed August 6, 2023. https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covid-net/purpose-methods.html
5. Centers for Disease Control and Prevention, National Center for Health Statistics. Provisional COVID-19 deaths: distribution of deaths by race and Hispanic origin. Updated July 26, 2023. Accessed August 8, 2023. https://data.cdc.gov/NCHS/Provisional-COVID-19-Deaths-Distribution-of-Deaths/pj7m-y5uh
6. Price-Haywood EG, Burton J, Fort D, Seoane L. Hospitalization and mortality among Black patients and White patients with COVID-19. N Engl J Med. 2020;382(26):2534-2543. doi:10.1056NEJMsa2011686
7. Wiltz JL, Feehan AK, Mollinari AM, et al. Racial and ethnic disparities in receipt of medications for treatment of COVID-19 - United States, March 2020-August 2021. MMWR Morb Mortal Wkly Rep. 2022;71(3):96-102. doi:10.15585/mmwr.mm7103e1
8. King JT Jr, Yoon JS, Rentsch CT, et al. Development and validation of a 30-day mortality index based on pre-existing medical administrative data from 13,323 COVID-19 patients: the Veterans Health Administration COVID-19 (VACO) Index. PLoS One. 2020;15(11):e0241825. doi:10.1371/journal.pone.0241825
9. US Food and Drug Administration, Office of Media Affairs. Coronavirus (COVID-19) update: FDA revokes emergency use authorization for monoclonal antibody bamlanivimab. Accessed August 8, 2023. https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-revokes-emergency-use-authorization-monoclonal-antibody-bamlanivimab
10. National Institutes of Health. Information on COVID-19 treatment, prevention and research. Accessed August 8, 2023. https://www.covid19treatmentguidelines.nih.gov
11. Anderson B, Smith Z, Edupuganti S, Yan X, Masi CM, Wu HM. Effect of monoclonal antibody treatment on clinical outcomes in ambulatory patients with coronavirus disease 2019. Open Forum Infect Dis. 2021;8(7):ofab315. Published 2021 Jun 12. doi:10.1093/ofid/ofab315
12. United States Census Bureau. Quick facts: DeKalb County, Georgia. Updated July 1, 2022. Accessed August 8, 2023. www.census.gov/quickfacts/dekalbcountygeorgia
13. Kumar R, Wu EL, Stosor V, et al. Real-world experience of bamlanivimab for coronavirus disease 2019 (COVID-19): a case-control study. Clin Infect Dis. 2022;74(1):24-31. doi:10.1093/cid/ciab305
1. Chen P, Nirula A, Heller B, et al; BLAZE-1 Investigators. SARS-CoV-2 neutralizing antibody LY-CoV555 in outpatients with COVID-19. N Engl J Med. 2021;384(3):229-237. doi:10.1056/NEJMoa2029849
2. Weinreich DM, Sivapalasingam S, Norton T, et al; Trial Investigators. REGN-COV2, a neutralizing antibody cocktail, in outpatients with COVID-19. N Engl J Med. 2021;384(3):238-251. doi:10.1056/NEJMoa2035002
3. US Food and Drug Administration. Fact sheet for health care providers, emergency use authorization (EUA) of bamlanivimab and etesevimab. Accessed August 6, 2023. https://www.fda.gov/media/145802/download
4. Centers for Disease Control and Prevention. Coronavirus disease 2019 (COVID-19)-associated hospitalization surveillance network (COVID-net). Updated March 24, 2023. Accessed August 6, 2023. https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covid-net/purpose-methods.html
5. Centers for Disease Control and Prevention, National Center for Health Statistics. Provisional COVID-19 deaths: distribution of deaths by race and Hispanic origin. Updated July 26, 2023. Accessed August 8, 2023. https://data.cdc.gov/NCHS/Provisional-COVID-19-Deaths-Distribution-of-Deaths/pj7m-y5uh
6. Price-Haywood EG, Burton J, Fort D, Seoane L. Hospitalization and mortality among Black patients and White patients with COVID-19. N Engl J Med. 2020;382(26):2534-2543. doi:10.1056NEJMsa2011686
7. Wiltz JL, Feehan AK, Mollinari AM, et al. Racial and ethnic disparities in receipt of medications for treatment of COVID-19 - United States, March 2020-August 2021. MMWR Morb Mortal Wkly Rep. 2022;71(3):96-102. doi:10.15585/mmwr.mm7103e1
8. King JT Jr, Yoon JS, Rentsch CT, et al. Development and validation of a 30-day mortality index based on pre-existing medical administrative data from 13,323 COVID-19 patients: the Veterans Health Administration COVID-19 (VACO) Index. PLoS One. 2020;15(11):e0241825. doi:10.1371/journal.pone.0241825
9. US Food and Drug Administration, Office of Media Affairs. Coronavirus (COVID-19) update: FDA revokes emergency use authorization for monoclonal antibody bamlanivimab. Accessed August 8, 2023. https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-revokes-emergency-use-authorization-monoclonal-antibody-bamlanivimab
10. National Institutes of Health. Information on COVID-19 treatment, prevention and research. Accessed August 8, 2023. https://www.covid19treatmentguidelines.nih.gov
11. Anderson B, Smith Z, Edupuganti S, Yan X, Masi CM, Wu HM. Effect of monoclonal antibody treatment on clinical outcomes in ambulatory patients with coronavirus disease 2019. Open Forum Infect Dis. 2021;8(7):ofab315. Published 2021 Jun 12. doi:10.1093/ofid/ofab315
12. United States Census Bureau. Quick facts: DeKalb County, Georgia. Updated July 1, 2022. Accessed August 8, 2023. www.census.gov/quickfacts/dekalbcountygeorgia
13. Kumar R, Wu EL, Stosor V, et al. Real-world experience of bamlanivimab for coronavirus disease 2019 (COVID-19): a case-control study. Clin Infect Dis. 2022;74(1):24-31. doi:10.1093/cid/ciab305
MASLD: Promising treatments for a newly renamed disease
In the week leading up to this, Intercept Pharmaceuticals announced that their program to develop obeticholic acid (OCA) as a first-to-market, long-awaited potential drug therapy for metabolic dysfunction–associated steatohepatitis (MASH), the more pathogenic form of this disease, was being abandoned after the Food and Drug Administration Gastrointestinal Drugs Advisory Committee voted against accelerated approval of the drug. This decision was made in large part owing to data showing modest efficacy coupled with multiple drug-related side effects, including worsening metabolic dysfunction.
The juxtaposition of these two events highlights what could be a fundamental change in perspective when it comes to the management of patients with MASLD and the development of therapies for this disease.
A more precise nomenclature for a broad-spectrum disease
The updating of the NAFLD nomenclature to MASLD represents an important change in the way that the medical community is being asked to view and approach the disease of “fatty liver.”
The previous nomenclature clarified that pathogenic liver steatosis can exist in the absence of alcohol. However, it failed to define the primary drivers of the most common form of NAFLD: that is, metabolic syndrome diseases. The new nomenclature not only better defines the broad spectrum of steatotic liver diseases (alcohol, metabolic, drug/genetic, cryptogenic) but also refocuses the attention of providers on the fundamental basis of MASLD as a critical member of the metabolic syndrome spectrum of diseases.
This is in line with the recently updated American Association for the Study of Liver Disease Practice Guidelines for NAFLD (now MASLD), which focus on active screening to identify patients at risk for advanced MASLD, in particular those with medically complicated obesity or high-risk metabolic characteristics such as diabetes. This is a change from previous versions of the guidelines that were cautious to recommend broad screening guidelines in part owing to the lack of “available therapies.”
The increasing clinical burden of MASH has led to the recognition that patients do not have the luxury of waiting for “anticipated therapies” that have frequently shown only marginal or insignificant efficacy. As a result, some providers have refocused their efforts on the development of care pathways that can efficiently provide comprehensive lifestyle interventions to treat MASH and related metabolic comorbidities within hepatology or other subspecialty clinics.
Learning from OCA’s limitations
The approach to drug development for MASH seems to be shifting in a similar, metabolic syndrome–focused way.
The risk-benefit analysis from the FDA advisory committee evaluating OCA noted that the drug provided only modest (albeit statistically significant) benefits over placebo in achieving one of two primary clinical endpoints (improvement in fibrosis by one stage without worsening of NASH), but was associated with toxicity as well as significant drug-related side effects, including new or worsening dyslipidemia, accelerated progression to prediabetes or diabetes, and worsening glycemic control in patients with diabetes.
Worsening clinical markers of metabolic health were an important factor in the advisory committee’s decision to not provide accelerated approval of OCA. This informs the criteria upon which future MASH therapies will be evaluated for approval: that an ideal agent for MASH not only will have a significant impact on MASH pathophysiology but will also provide benefit for (or at least not worsen) the metabolic comorbidities associated with MASH.
New treatments on the horizon
Fortunately, several new MASH therapeutics in development seem to have promising metabolic profiles.
In the phase 3 MAESTRO-NASH biopsy trial, treatment with resmetirom, a thyroid hormone receptor–beta selective agonist versus placebo resulted in a clinically significant improvement in liver fibrosis by one stage or more (26% vs. 14%) and NASH resolution (30% vs. 10%). Unlike OCA, resmetirom was associated with a clinically significant reduction in LDL cholesterol (–16% compared with placebo).
Resmetirom has received a breakthrough therapy designation, and Madrigal Pharmaceuticals recently completed submission of a new drug application for accelerated approval of this agent to the FDA.
Semaglutide is a glucagonlike peptide–1 receptor agonist that is already FDA approved for treatment of diabetes and obesity and is being studied in a phase 3 analysis for NASH.
In a phase 2 trial, daily dosing of semaglutide vs placebo led to clinically significant improvement in NASH resolution (59% vs. 17%) but not significant improvement in fibrosis (43% vs 33%). Although it is impossible to make a meaningful comparison in outcomes between clinical trials, it should be noted that the absolute rate of response in this trial was higher than is routinely seen in other NASH trials and that the placebo rate for improvement in fibrosis was higher than expected, a common problem with NASH trials.
As expected, treatment with semaglutide was associated with dose-dependent reduction in body weight and hemoglobin A1c, highlighting the global metabolic benefit of this agent.
Another major class of agents being studied for NASH treatment are the fibroblast growth factor (FGF) 21 analogs.
In the recently published phase 2b ENLIVEN trial, treatment with the FGF21 analog pegozafermin versus placebo led to a statistically significant improvement in liver fibrosis by one stage (27% vs. 7%) and a numerical improvement in NASH resolution (26% vs. 2%).
In addition to its effects directly in the liver, FGF21 has been associated with promoting positive global metabolic effects, including improved peripheral insulin sensitivity and amelioration of dyslipidemia. Consistent with this, treatment with pegozafermin resulted in a decrease in serum triglycerides and an increase in serum HDL cholesterol and adiponectin levels.
Ultimately, the best therapeutic strategy for MASH may be one that uses combination therapy to maximize liver-directed effects and also ameliorate concomitant or contributing metabolic dysfunction. This approach is already being investigated. What seems clear, however, is that MASH therapy without concurrent treatment of metabolic comorbidities is probably destined to be ineffective, if not counterproductive.
So, what’s in a name? When it comes to MASLD, it seems quite a bit.
Dr. Janardhan is an assistant professor, department of internal medicine, at Rush University Medical Center, Chicago. Dr. Reau is a professor, department of internal medicine, Rush University. Dr. Janardhan reported conflicts of interest with Target RWE, Novo Nordisk, Intercept, and Enanta. Dr. Reau reported conflicts of interest with AbbVie, Gilead, and AASLD.
A version of this article appeared on Medscape.com.
In the week leading up to this, Intercept Pharmaceuticals announced that their program to develop obeticholic acid (OCA) as a first-to-market, long-awaited potential drug therapy for metabolic dysfunction–associated steatohepatitis (MASH), the more pathogenic form of this disease, was being abandoned after the Food and Drug Administration Gastrointestinal Drugs Advisory Committee voted against accelerated approval of the drug. This decision was made in large part owing to data showing modest efficacy coupled with multiple drug-related side effects, including worsening metabolic dysfunction.
The juxtaposition of these two events highlights what could be a fundamental change in perspective when it comes to the management of patients with MASLD and the development of therapies for this disease.
A more precise nomenclature for a broad-spectrum disease
The updating of the NAFLD nomenclature to MASLD represents an important change in the way that the medical community is being asked to view and approach the disease of “fatty liver.”
The previous nomenclature clarified that pathogenic liver steatosis can exist in the absence of alcohol. However, it failed to define the primary drivers of the most common form of NAFLD: that is, metabolic syndrome diseases. The new nomenclature not only better defines the broad spectrum of steatotic liver diseases (alcohol, metabolic, drug/genetic, cryptogenic) but also refocuses the attention of providers on the fundamental basis of MASLD as a critical member of the metabolic syndrome spectrum of diseases.
This is in line with the recently updated American Association for the Study of Liver Disease Practice Guidelines for NAFLD (now MASLD), which focus on active screening to identify patients at risk for advanced MASLD, in particular those with medically complicated obesity or high-risk metabolic characteristics such as diabetes. This is a change from previous versions of the guidelines that were cautious to recommend broad screening guidelines in part owing to the lack of “available therapies.”
The increasing clinical burden of MASH has led to the recognition that patients do not have the luxury of waiting for “anticipated therapies” that have frequently shown only marginal or insignificant efficacy. As a result, some providers have refocused their efforts on the development of care pathways that can efficiently provide comprehensive lifestyle interventions to treat MASH and related metabolic comorbidities within hepatology or other subspecialty clinics.
Learning from OCA’s limitations
The approach to drug development for MASH seems to be shifting in a similar, metabolic syndrome–focused way.
The risk-benefit analysis from the FDA advisory committee evaluating OCA noted that the drug provided only modest (albeit statistically significant) benefits over placebo in achieving one of two primary clinical endpoints (improvement in fibrosis by one stage without worsening of NASH), but was associated with toxicity as well as significant drug-related side effects, including new or worsening dyslipidemia, accelerated progression to prediabetes or diabetes, and worsening glycemic control in patients with diabetes.
Worsening clinical markers of metabolic health were an important factor in the advisory committee’s decision to not provide accelerated approval of OCA. This informs the criteria upon which future MASH therapies will be evaluated for approval: that an ideal agent for MASH not only will have a significant impact on MASH pathophysiology but will also provide benefit for (or at least not worsen) the metabolic comorbidities associated with MASH.
New treatments on the horizon
Fortunately, several new MASH therapeutics in development seem to have promising metabolic profiles.
In the phase 3 MAESTRO-NASH biopsy trial, treatment with resmetirom, a thyroid hormone receptor–beta selective agonist versus placebo resulted in a clinically significant improvement in liver fibrosis by one stage or more (26% vs. 14%) and NASH resolution (30% vs. 10%). Unlike OCA, resmetirom was associated with a clinically significant reduction in LDL cholesterol (–16% compared with placebo).
Resmetirom has received a breakthrough therapy designation, and Madrigal Pharmaceuticals recently completed submission of a new drug application for accelerated approval of this agent to the FDA.
Semaglutide is a glucagonlike peptide–1 receptor agonist that is already FDA approved for treatment of diabetes and obesity and is being studied in a phase 3 analysis for NASH.
In a phase 2 trial, daily dosing of semaglutide vs placebo led to clinically significant improvement in NASH resolution (59% vs. 17%) but not significant improvement in fibrosis (43% vs 33%). Although it is impossible to make a meaningful comparison in outcomes between clinical trials, it should be noted that the absolute rate of response in this trial was higher than is routinely seen in other NASH trials and that the placebo rate for improvement in fibrosis was higher than expected, a common problem with NASH trials.
As expected, treatment with semaglutide was associated with dose-dependent reduction in body weight and hemoglobin A1c, highlighting the global metabolic benefit of this agent.
Another major class of agents being studied for NASH treatment are the fibroblast growth factor (FGF) 21 analogs.
In the recently published phase 2b ENLIVEN trial, treatment with the FGF21 analog pegozafermin versus placebo led to a statistically significant improvement in liver fibrosis by one stage (27% vs. 7%) and a numerical improvement in NASH resolution (26% vs. 2%).
In addition to its effects directly in the liver, FGF21 has been associated with promoting positive global metabolic effects, including improved peripheral insulin sensitivity and amelioration of dyslipidemia. Consistent with this, treatment with pegozafermin resulted in a decrease in serum triglycerides and an increase in serum HDL cholesterol and adiponectin levels.
Ultimately, the best therapeutic strategy for MASH may be one that uses combination therapy to maximize liver-directed effects and also ameliorate concomitant or contributing metabolic dysfunction. This approach is already being investigated. What seems clear, however, is that MASH therapy without concurrent treatment of metabolic comorbidities is probably destined to be ineffective, if not counterproductive.
So, what’s in a name? When it comes to MASLD, it seems quite a bit.
Dr. Janardhan is an assistant professor, department of internal medicine, at Rush University Medical Center, Chicago. Dr. Reau is a professor, department of internal medicine, Rush University. Dr. Janardhan reported conflicts of interest with Target RWE, Novo Nordisk, Intercept, and Enanta. Dr. Reau reported conflicts of interest with AbbVie, Gilead, and AASLD.
A version of this article appeared on Medscape.com.
In the week leading up to this, Intercept Pharmaceuticals announced that their program to develop obeticholic acid (OCA) as a first-to-market, long-awaited potential drug therapy for metabolic dysfunction–associated steatohepatitis (MASH), the more pathogenic form of this disease, was being abandoned after the Food and Drug Administration Gastrointestinal Drugs Advisory Committee voted against accelerated approval of the drug. This decision was made in large part owing to data showing modest efficacy coupled with multiple drug-related side effects, including worsening metabolic dysfunction.
The juxtaposition of these two events highlights what could be a fundamental change in perspective when it comes to the management of patients with MASLD and the development of therapies for this disease.
A more precise nomenclature for a broad-spectrum disease
The updating of the NAFLD nomenclature to MASLD represents an important change in the way that the medical community is being asked to view and approach the disease of “fatty liver.”
The previous nomenclature clarified that pathogenic liver steatosis can exist in the absence of alcohol. However, it failed to define the primary drivers of the most common form of NAFLD: that is, metabolic syndrome diseases. The new nomenclature not only better defines the broad spectrum of steatotic liver diseases (alcohol, metabolic, drug/genetic, cryptogenic) but also refocuses the attention of providers on the fundamental basis of MASLD as a critical member of the metabolic syndrome spectrum of diseases.
This is in line with the recently updated American Association for the Study of Liver Disease Practice Guidelines for NAFLD (now MASLD), which focus on active screening to identify patients at risk for advanced MASLD, in particular those with medically complicated obesity or high-risk metabolic characteristics such as diabetes. This is a change from previous versions of the guidelines that were cautious to recommend broad screening guidelines in part owing to the lack of “available therapies.”
The increasing clinical burden of MASH has led to the recognition that patients do not have the luxury of waiting for “anticipated therapies” that have frequently shown only marginal or insignificant efficacy. As a result, some providers have refocused their efforts on the development of care pathways that can efficiently provide comprehensive lifestyle interventions to treat MASH and related metabolic comorbidities within hepatology or other subspecialty clinics.
Learning from OCA’s limitations
The approach to drug development for MASH seems to be shifting in a similar, metabolic syndrome–focused way.
The risk-benefit analysis from the FDA advisory committee evaluating OCA noted that the drug provided only modest (albeit statistically significant) benefits over placebo in achieving one of two primary clinical endpoints (improvement in fibrosis by one stage without worsening of NASH), but was associated with toxicity as well as significant drug-related side effects, including new or worsening dyslipidemia, accelerated progression to prediabetes or diabetes, and worsening glycemic control in patients with diabetes.
Worsening clinical markers of metabolic health were an important factor in the advisory committee’s decision to not provide accelerated approval of OCA. This informs the criteria upon which future MASH therapies will be evaluated for approval: that an ideal agent for MASH not only will have a significant impact on MASH pathophysiology but will also provide benefit for (or at least not worsen) the metabolic comorbidities associated with MASH.
New treatments on the horizon
Fortunately, several new MASH therapeutics in development seem to have promising metabolic profiles.
In the phase 3 MAESTRO-NASH biopsy trial, treatment with resmetirom, a thyroid hormone receptor–beta selective agonist versus placebo resulted in a clinically significant improvement in liver fibrosis by one stage or more (26% vs. 14%) and NASH resolution (30% vs. 10%). Unlike OCA, resmetirom was associated with a clinically significant reduction in LDL cholesterol (–16% compared with placebo).
Resmetirom has received a breakthrough therapy designation, and Madrigal Pharmaceuticals recently completed submission of a new drug application for accelerated approval of this agent to the FDA.
Semaglutide is a glucagonlike peptide–1 receptor agonist that is already FDA approved for treatment of diabetes and obesity and is being studied in a phase 3 analysis for NASH.
In a phase 2 trial, daily dosing of semaglutide vs placebo led to clinically significant improvement in NASH resolution (59% vs. 17%) but not significant improvement in fibrosis (43% vs 33%). Although it is impossible to make a meaningful comparison in outcomes between clinical trials, it should be noted that the absolute rate of response in this trial was higher than is routinely seen in other NASH trials and that the placebo rate for improvement in fibrosis was higher than expected, a common problem with NASH trials.
As expected, treatment with semaglutide was associated with dose-dependent reduction in body weight and hemoglobin A1c, highlighting the global metabolic benefit of this agent.
Another major class of agents being studied for NASH treatment are the fibroblast growth factor (FGF) 21 analogs.
In the recently published phase 2b ENLIVEN trial, treatment with the FGF21 analog pegozafermin versus placebo led to a statistically significant improvement in liver fibrosis by one stage (27% vs. 7%) and a numerical improvement in NASH resolution (26% vs. 2%).
In addition to its effects directly in the liver, FGF21 has been associated with promoting positive global metabolic effects, including improved peripheral insulin sensitivity and amelioration of dyslipidemia. Consistent with this, treatment with pegozafermin resulted in a decrease in serum triglycerides and an increase in serum HDL cholesterol and adiponectin levels.
Ultimately, the best therapeutic strategy for MASH may be one that uses combination therapy to maximize liver-directed effects and also ameliorate concomitant or contributing metabolic dysfunction. This approach is already being investigated. What seems clear, however, is that MASH therapy without concurrent treatment of metabolic comorbidities is probably destined to be ineffective, if not counterproductive.
So, what’s in a name? When it comes to MASLD, it seems quite a bit.
Dr. Janardhan is an assistant professor, department of internal medicine, at Rush University Medical Center, Chicago. Dr. Reau is a professor, department of internal medicine, Rush University. Dr. Janardhan reported conflicts of interest with Target RWE, Novo Nordisk, Intercept, and Enanta. Dr. Reau reported conflicts of interest with AbbVie, Gilead, and AASLD.
A version of this article appeared on Medscape.com.
Salute to Service Dogs
The psychological and moral comfort of a presence at once humble and understanding—this is the greatest benefit that the dog has bestowed upon man. Percy Bysshe Shelley
The nature of their special training to perform specific tasks for the safety and well-being of veterans distinguishes service dogs from pets or emotional support animals. Most of us recognize the happiness and meaning animals bring to our lives. What we may not appreciate is the impressive contribution service dogs make to the health and rehabilitation of those who have served their country. Veteran patients with neurologic conditions such as seizures know the difference a service dog trained to warn them of an emerging seizure makes for their freedom of movement and peace of mind. Veterans with diabetes have described times when their service dogs sought help before they realized their blood sugar was dangerously low.
Patients, friends, and neighbors who have been paired with service dogs describe ways their new companion helped them transition from a life in which even surviving was a struggle to one of holistic thriving. A Vietnam veteran neighbor with a significant tremor due to Parkinson disease benefitted from the ability of his dog to fetch and bring, retrieve, and carry. His dog has learned to hold essential items still, which would otherwise be too shaky in human hands, enabling the veteran to open his closet door and dress independently each morning. One veteran classmate avoided all forms of public transportation due to memories of a traumatic mobile-based mass evacuation she assisted with during her military service. She dreaded her long, inconvenient daily drive back and forth to work. She was then partnered with a large dog breed that was trained to stand a short distance from her to protect her sense of space and open air. The dog would stretch out his body to claim more space for her among crowds. This veteran started to ride the bus to campus each morning and appreciated the interaction with other riders as well as the saved travel time, mileage, gasoline expense, and parking stress.
A veteran brought his sweet retriever to the neighborhood weekly “Paws-itive Reading” program for children in the local public library. When MW’s daughter was busy reading to his furry friend, the veteran shared that for at least 5 years after his combat tours, he rarely left his window-shuttered home. His dog’s steady comfort re-established his ability to participate in his community. He now generously shares his dog’s patient affection with children learning to read.
MW recently witnessed the profound and protective presence of a service dog in comforting a veteran during a posttraumatic stress disorder (PTSD)–related crisis. The service dog offered a lean and reassuring paw pressure on the veteran’s shoulder if he was reexperiencing trauma. The dog’s steady breathing and familiar warmth helped to reorient their human companion to the safety of his present physical surroundings. Bearing witness to the dog’s trained interaction with the veteran left MW speechless. The trust between them was therapeutic in a way that transcended her ability to articulate what she experienced. This compelled MW to investigate whether this was a rare relationship or whether there was existing data on the impact of trained service dogs and PTSD.
Service dog placement with veterans with PTSD has been shown to have a positive influence on both physiological (arousal-related functioning and cortisol awakening response) and psychosocial well-being, including decreased isolation and increased physical activity.1,2 Veterans with PTSD paired with service dogs showed significantly fewer PTSD-related symptoms, better sleep quality, and improved well-being, compared with those with just a pet.3 A recent meta-analysis revealed that veteran partnerships with a service dog had a clinically meaningful, significant, and large effect on PTSD severity scores (P < .001).2 The mechanism for impact is thought to be not only the dog’s working role but also the transcendent loyalty of the canine-veteran bond.
Many accredited dog training programs describe a certain reciprocity to the dog-human relationship. Some use rescue puppies to give the dogs a new life and purpose. Dogs who have undergone challenges often need patience, time, safe relationships, and trustworthy new experiences to maximize their potential. Reciprocally, trained service dogs have the potential to foster access to these same emotional, relational, existential, and physical safety needs for veterans exposed to trauma.
Recent legislation has made progress in recognizing the role of service dogs for veterans and improving access. The Puppies Assisting Wounded Servicemembers (PAWS) for Veterans Therapy Act (38 USC §1705, 1714) was passed in 2021. The PAWS Act implemented a policy and 5-year pilot program to connect trained canines to eligible veterans diagnosed with PTSD as an element of an integrative health program, regardless of whether the veteran has a mobility impairment. The PAWS Act gives federal funding to accredited dog training organizations to help pair eligible veterans with service dogs by covering veteran travel expenses for the training, training program participation, and relevant veterinary expenses. The bipartisan Service Dogs Assisting Veterans Act (SAVES) Act was introduced this summer to award grants to nonprofit organizations Assistance Dog International has accredited to help these groups provide service dogs to veterans.
The US Department of Veterans Affairs (VA) has made strides in welcoming service dogs. Trained service dogs of all breeds under the control of a human companion are now allowed in VA facilities other than in areas where safety and infection control standards would be compromised (ie, sterile equipment rooms).4 A prescribing clinician can now evaluate eligible veterans to determine their ability, resources, and goals for having a service dog.5 An assessment of the veteran’s ability to care for a dog and education on expectations for the partnership is critical to success and animal welfare. Those veterans approved for a service dog are then referred to accredited agencies. The VA Veterinary Health Insurance Benefit includes aspects of coverage for the veteran to attend service dog training, veterinary wellness (preventive care, immunizations, dental cleanings, certain prescriptions, etc), and care for the dog’s illnesses when treatment enables the dog to perform duties in service to the veteran.6
The productive purpose and friendship of a service dog become a formidable force in a veteran’s life. Veterans spent an average of 82% of their time with service dogs (assessed via Bluetooth proximity between collar and smartphone).7 Human partners of veterans with service dogs may experience improved quality of life and relationship functioning with the inclusion of a service dog in the family unit.8 Veterans depict increased community engagement, social connectedness, and personal confidence as a result of the canine companionship.9,10 Veterans with service dogs often speak of the ways the dog’s presence transformed their lives and many speak of the dog literally saving their lives.11 Meta-analyses showed improved mental health treatment engagement, medication adherence, and decreased suicidality.2,12
A story was recently shared with us about the compassion and competence of VA staff in a perioperative unit. A veteran was scheduled for a life-altering surgery and yet was anxious about entering the room for his scheduled pre-anesthesia check-in, knowing his service dog could not accompany him through the entire procedure. The staff recognized that the veteran was increasingly nervous and even started to question whether he would stay for the scheduled procedure they deemed would benefit his health. The perioperative team then proactively worked together to safely walk the veteran through the preparation processes in a sterile setting while keeping the dog within sight of the veteran. They then ensured that the veteran’s service dog was by his side early in the recovery room so that the veteran woke to wags and licks. In these months of canine recognition, we honor the ways the VA has fostered companionship and courage in veterans’ lives through the inclusion of service dogs in so many aspects of their care and life.
1. Rodriguez KE, Bryce CI, Granger DA, O’Haire ME. The effect of a service dog on salivary cortisol awakening response in a military population with posttraumatic stress disorder (PTSD). Psychoneuroendocrinology. 2018;98:202-210. doi:10.1016/j.psyneuen.2018.04.026
2. Leighton SC, Nieforth LO, O’Haire ME. Assistance dogs for military veterans with PTSD: A systematic review, meta-analysis, and meta-synthesis. PloS One. 2022;17(9):e0274960. doi:10.1371/journal.pone.0274960
3. Van Houtert EAE, Rodenburg TB, Vermetten E, Endenburg N. The impact of service dogs on military veterans and (ex) first aid responders with post-traumatic stress disorder. Front Psychiatry. 2022;13:834291. doi:10.3389/fpsyt.2022.834291
4. VHA Directive 1188(1). Animals on Veterans Health Administration (VHA) Property. Veterans Health Administration. August 26, 2015. Amended April 25, 2019. https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=3138
5. Veteran Affairs Rehabilitation and Prosthetic Services. Service Dog Veterinary Health Benefit. US Department of Veterans Affairs. Updated September 19, 2019. Accessed August 21, 2023. https://www.prosthetics.va.gov/serviceandguidedogs.asp
6. Service Dog Veterinary Health Insurance (VHIB) Benefit Rules. US Department of Veterans Affairs Rehabilitation and Prosthetic Services. Updated December 2022. Accessed August 21, 2023. https://www.prosthetics.va.gov/factsheet/PSAS-FactSheet-ServiceDogs.pdf
7. Jensen CL, Rodriguez KE, MacLean EL, Abdul Wahab AH, Sabbaghi A, O’Haire ME. Characterizing veteran and PTSD service dog teams: exploring potential mechanisms of symptom change and canine predictors of efficacy. PloS One. 2022;17(7):e0269186. doi:10.1371/journal.pone.0269186
8. McCall CE, Rodriguez KE, Wadsworth SMM, Meis LA, O’Haire ME. “A Part of Our Family”? Effects of psychiatric service dogs on quality of life and relationship functioning in military-connected couples. Mil Behav Health. 2020;8(4):410-423. doi:10.1080/21635781.2020.1825243
9. Krause-Parello CA, Sarni S, Padden E. Military veterans and canine assistance for post-traumatic stress disorder: a narrative review of the literature. Nurse Educ Today. 2016;47:43-50. doi:10.1016/j.nedt.2016.04.020
10. Van Houtert EAE, Endenburg N, Wijnker JJ, Rodenburg B, Vermetten E. The study of service dogs for veterans with post-traumatic stress disorder: a scoping literature review. Eur J Psychotraumatol. 2018;9(suppl 3):1503523. doi:10.1080/20008198.2018.1503523
11. Sherman M, Hutchinson AD, Bowen H, Iannos M, Van Hooff M. Effectiveness of Operation K9 assistance dogs on suicidality in Australian veterans with PTSD: a 12-month mixed-methods follow-up study. Int J Environ Res Public Health. 2023;20(4):3607. Published 2023 Feb 17. doi:10.3390/ijerph20043607
12. Richerson JT, Saunders GH, Skelton K, et al. A randomized trial of differential effectiveness of service dog pairing to improve quality of life for veterans with PTSD. Office of Research and Development, Veterans Health Administration. 2020:186. https://www.research.va.gov/REPORT-Study-of-Costs-and-Benefits-Associated-with-the-Use-of-Service-Dogs-Monograph1.pdf
The psychological and moral comfort of a presence at once humble and understanding—this is the greatest benefit that the dog has bestowed upon man. Percy Bysshe Shelley
The nature of their special training to perform specific tasks for the safety and well-being of veterans distinguishes service dogs from pets or emotional support animals. Most of us recognize the happiness and meaning animals bring to our lives. What we may not appreciate is the impressive contribution service dogs make to the health and rehabilitation of those who have served their country. Veteran patients with neurologic conditions such as seizures know the difference a service dog trained to warn them of an emerging seizure makes for their freedom of movement and peace of mind. Veterans with diabetes have described times when their service dogs sought help before they realized their blood sugar was dangerously low.
Patients, friends, and neighbors who have been paired with service dogs describe ways their new companion helped them transition from a life in which even surviving was a struggle to one of holistic thriving. A Vietnam veteran neighbor with a significant tremor due to Parkinson disease benefitted from the ability of his dog to fetch and bring, retrieve, and carry. His dog has learned to hold essential items still, which would otherwise be too shaky in human hands, enabling the veteran to open his closet door and dress independently each morning. One veteran classmate avoided all forms of public transportation due to memories of a traumatic mobile-based mass evacuation she assisted with during her military service. She dreaded her long, inconvenient daily drive back and forth to work. She was then partnered with a large dog breed that was trained to stand a short distance from her to protect her sense of space and open air. The dog would stretch out his body to claim more space for her among crowds. This veteran started to ride the bus to campus each morning and appreciated the interaction with other riders as well as the saved travel time, mileage, gasoline expense, and parking stress.
A veteran brought his sweet retriever to the neighborhood weekly “Paws-itive Reading” program for children in the local public library. When MW’s daughter was busy reading to his furry friend, the veteran shared that for at least 5 years after his combat tours, he rarely left his window-shuttered home. His dog’s steady comfort re-established his ability to participate in his community. He now generously shares his dog’s patient affection with children learning to read.
MW recently witnessed the profound and protective presence of a service dog in comforting a veteran during a posttraumatic stress disorder (PTSD)–related crisis. The service dog offered a lean and reassuring paw pressure on the veteran’s shoulder if he was reexperiencing trauma. The dog’s steady breathing and familiar warmth helped to reorient their human companion to the safety of his present physical surroundings. Bearing witness to the dog’s trained interaction with the veteran left MW speechless. The trust between them was therapeutic in a way that transcended her ability to articulate what she experienced. This compelled MW to investigate whether this was a rare relationship or whether there was existing data on the impact of trained service dogs and PTSD.
Service dog placement with veterans with PTSD has been shown to have a positive influence on both physiological (arousal-related functioning and cortisol awakening response) and psychosocial well-being, including decreased isolation and increased physical activity.1,2 Veterans with PTSD paired with service dogs showed significantly fewer PTSD-related symptoms, better sleep quality, and improved well-being, compared with those with just a pet.3 A recent meta-analysis revealed that veteran partnerships with a service dog had a clinically meaningful, significant, and large effect on PTSD severity scores (P < .001).2 The mechanism for impact is thought to be not only the dog’s working role but also the transcendent loyalty of the canine-veteran bond.
Many accredited dog training programs describe a certain reciprocity to the dog-human relationship. Some use rescue puppies to give the dogs a new life and purpose. Dogs who have undergone challenges often need patience, time, safe relationships, and trustworthy new experiences to maximize their potential. Reciprocally, trained service dogs have the potential to foster access to these same emotional, relational, existential, and physical safety needs for veterans exposed to trauma.
Recent legislation has made progress in recognizing the role of service dogs for veterans and improving access. The Puppies Assisting Wounded Servicemembers (PAWS) for Veterans Therapy Act (38 USC §1705, 1714) was passed in 2021. The PAWS Act implemented a policy and 5-year pilot program to connect trained canines to eligible veterans diagnosed with PTSD as an element of an integrative health program, regardless of whether the veteran has a mobility impairment. The PAWS Act gives federal funding to accredited dog training organizations to help pair eligible veterans with service dogs by covering veteran travel expenses for the training, training program participation, and relevant veterinary expenses. The bipartisan Service Dogs Assisting Veterans Act (SAVES) Act was introduced this summer to award grants to nonprofit organizations Assistance Dog International has accredited to help these groups provide service dogs to veterans.
The US Department of Veterans Affairs (VA) has made strides in welcoming service dogs. Trained service dogs of all breeds under the control of a human companion are now allowed in VA facilities other than in areas where safety and infection control standards would be compromised (ie, sterile equipment rooms).4 A prescribing clinician can now evaluate eligible veterans to determine their ability, resources, and goals for having a service dog.5 An assessment of the veteran’s ability to care for a dog and education on expectations for the partnership is critical to success and animal welfare. Those veterans approved for a service dog are then referred to accredited agencies. The VA Veterinary Health Insurance Benefit includes aspects of coverage for the veteran to attend service dog training, veterinary wellness (preventive care, immunizations, dental cleanings, certain prescriptions, etc), and care for the dog’s illnesses when treatment enables the dog to perform duties in service to the veteran.6
The productive purpose and friendship of a service dog become a formidable force in a veteran’s life. Veterans spent an average of 82% of their time with service dogs (assessed via Bluetooth proximity between collar and smartphone).7 Human partners of veterans with service dogs may experience improved quality of life and relationship functioning with the inclusion of a service dog in the family unit.8 Veterans depict increased community engagement, social connectedness, and personal confidence as a result of the canine companionship.9,10 Veterans with service dogs often speak of the ways the dog’s presence transformed their lives and many speak of the dog literally saving their lives.11 Meta-analyses showed improved mental health treatment engagement, medication adherence, and decreased suicidality.2,12
A story was recently shared with us about the compassion and competence of VA staff in a perioperative unit. A veteran was scheduled for a life-altering surgery and yet was anxious about entering the room for his scheduled pre-anesthesia check-in, knowing his service dog could not accompany him through the entire procedure. The staff recognized that the veteran was increasingly nervous and even started to question whether he would stay for the scheduled procedure they deemed would benefit his health. The perioperative team then proactively worked together to safely walk the veteran through the preparation processes in a sterile setting while keeping the dog within sight of the veteran. They then ensured that the veteran’s service dog was by his side early in the recovery room so that the veteran woke to wags and licks. In these months of canine recognition, we honor the ways the VA has fostered companionship and courage in veterans’ lives through the inclusion of service dogs in so many aspects of their care and life.
The psychological and moral comfort of a presence at once humble and understanding—this is the greatest benefit that the dog has bestowed upon man. Percy Bysshe Shelley
The nature of their special training to perform specific tasks for the safety and well-being of veterans distinguishes service dogs from pets or emotional support animals. Most of us recognize the happiness and meaning animals bring to our lives. What we may not appreciate is the impressive contribution service dogs make to the health and rehabilitation of those who have served their country. Veteran patients with neurologic conditions such as seizures know the difference a service dog trained to warn them of an emerging seizure makes for their freedom of movement and peace of mind. Veterans with diabetes have described times when their service dogs sought help before they realized their blood sugar was dangerously low.
Patients, friends, and neighbors who have been paired with service dogs describe ways their new companion helped them transition from a life in which even surviving was a struggle to one of holistic thriving. A Vietnam veteran neighbor with a significant tremor due to Parkinson disease benefitted from the ability of his dog to fetch and bring, retrieve, and carry. His dog has learned to hold essential items still, which would otherwise be too shaky in human hands, enabling the veteran to open his closet door and dress independently each morning. One veteran classmate avoided all forms of public transportation due to memories of a traumatic mobile-based mass evacuation she assisted with during her military service. She dreaded her long, inconvenient daily drive back and forth to work. She was then partnered with a large dog breed that was trained to stand a short distance from her to protect her sense of space and open air. The dog would stretch out his body to claim more space for her among crowds. This veteran started to ride the bus to campus each morning and appreciated the interaction with other riders as well as the saved travel time, mileage, gasoline expense, and parking stress.
A veteran brought his sweet retriever to the neighborhood weekly “Paws-itive Reading” program for children in the local public library. When MW’s daughter was busy reading to his furry friend, the veteran shared that for at least 5 years after his combat tours, he rarely left his window-shuttered home. His dog’s steady comfort re-established his ability to participate in his community. He now generously shares his dog’s patient affection with children learning to read.
MW recently witnessed the profound and protective presence of a service dog in comforting a veteran during a posttraumatic stress disorder (PTSD)–related crisis. The service dog offered a lean and reassuring paw pressure on the veteran’s shoulder if he was reexperiencing trauma. The dog’s steady breathing and familiar warmth helped to reorient their human companion to the safety of his present physical surroundings. Bearing witness to the dog’s trained interaction with the veteran left MW speechless. The trust between them was therapeutic in a way that transcended her ability to articulate what she experienced. This compelled MW to investigate whether this was a rare relationship or whether there was existing data on the impact of trained service dogs and PTSD.
Service dog placement with veterans with PTSD has been shown to have a positive influence on both physiological (arousal-related functioning and cortisol awakening response) and psychosocial well-being, including decreased isolation and increased physical activity.1,2 Veterans with PTSD paired with service dogs showed significantly fewer PTSD-related symptoms, better sleep quality, and improved well-being, compared with those with just a pet.3 A recent meta-analysis revealed that veteran partnerships with a service dog had a clinically meaningful, significant, and large effect on PTSD severity scores (P < .001).2 The mechanism for impact is thought to be not only the dog’s working role but also the transcendent loyalty of the canine-veteran bond.
Many accredited dog training programs describe a certain reciprocity to the dog-human relationship. Some use rescue puppies to give the dogs a new life and purpose. Dogs who have undergone challenges often need patience, time, safe relationships, and trustworthy new experiences to maximize their potential. Reciprocally, trained service dogs have the potential to foster access to these same emotional, relational, existential, and physical safety needs for veterans exposed to trauma.
Recent legislation has made progress in recognizing the role of service dogs for veterans and improving access. The Puppies Assisting Wounded Servicemembers (PAWS) for Veterans Therapy Act (38 USC §1705, 1714) was passed in 2021. The PAWS Act implemented a policy and 5-year pilot program to connect trained canines to eligible veterans diagnosed with PTSD as an element of an integrative health program, regardless of whether the veteran has a mobility impairment. The PAWS Act gives federal funding to accredited dog training organizations to help pair eligible veterans with service dogs by covering veteran travel expenses for the training, training program participation, and relevant veterinary expenses. The bipartisan Service Dogs Assisting Veterans Act (SAVES) Act was introduced this summer to award grants to nonprofit organizations Assistance Dog International has accredited to help these groups provide service dogs to veterans.
The US Department of Veterans Affairs (VA) has made strides in welcoming service dogs. Trained service dogs of all breeds under the control of a human companion are now allowed in VA facilities other than in areas where safety and infection control standards would be compromised (ie, sterile equipment rooms).4 A prescribing clinician can now evaluate eligible veterans to determine their ability, resources, and goals for having a service dog.5 An assessment of the veteran’s ability to care for a dog and education on expectations for the partnership is critical to success and animal welfare. Those veterans approved for a service dog are then referred to accredited agencies. The VA Veterinary Health Insurance Benefit includes aspects of coverage for the veteran to attend service dog training, veterinary wellness (preventive care, immunizations, dental cleanings, certain prescriptions, etc), and care for the dog’s illnesses when treatment enables the dog to perform duties in service to the veteran.6
The productive purpose and friendship of a service dog become a formidable force in a veteran’s life. Veterans spent an average of 82% of their time with service dogs (assessed via Bluetooth proximity between collar and smartphone).7 Human partners of veterans with service dogs may experience improved quality of life and relationship functioning with the inclusion of a service dog in the family unit.8 Veterans depict increased community engagement, social connectedness, and personal confidence as a result of the canine companionship.9,10 Veterans with service dogs often speak of the ways the dog’s presence transformed their lives and many speak of the dog literally saving their lives.11 Meta-analyses showed improved mental health treatment engagement, medication adherence, and decreased suicidality.2,12
A story was recently shared with us about the compassion and competence of VA staff in a perioperative unit. A veteran was scheduled for a life-altering surgery and yet was anxious about entering the room for his scheduled pre-anesthesia check-in, knowing his service dog could not accompany him through the entire procedure. The staff recognized that the veteran was increasingly nervous and even started to question whether he would stay for the scheduled procedure they deemed would benefit his health. The perioperative team then proactively worked together to safely walk the veteran through the preparation processes in a sterile setting while keeping the dog within sight of the veteran. They then ensured that the veteran’s service dog was by his side early in the recovery room so that the veteran woke to wags and licks. In these months of canine recognition, we honor the ways the VA has fostered companionship and courage in veterans’ lives through the inclusion of service dogs in so many aspects of their care and life.
1. Rodriguez KE, Bryce CI, Granger DA, O’Haire ME. The effect of a service dog on salivary cortisol awakening response in a military population with posttraumatic stress disorder (PTSD). Psychoneuroendocrinology. 2018;98:202-210. doi:10.1016/j.psyneuen.2018.04.026
2. Leighton SC, Nieforth LO, O’Haire ME. Assistance dogs for military veterans with PTSD: A systematic review, meta-analysis, and meta-synthesis. PloS One. 2022;17(9):e0274960. doi:10.1371/journal.pone.0274960
3. Van Houtert EAE, Rodenburg TB, Vermetten E, Endenburg N. The impact of service dogs on military veterans and (ex) first aid responders with post-traumatic stress disorder. Front Psychiatry. 2022;13:834291. doi:10.3389/fpsyt.2022.834291
4. VHA Directive 1188(1). Animals on Veterans Health Administration (VHA) Property. Veterans Health Administration. August 26, 2015. Amended April 25, 2019. https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=3138
5. Veteran Affairs Rehabilitation and Prosthetic Services. Service Dog Veterinary Health Benefit. US Department of Veterans Affairs. Updated September 19, 2019. Accessed August 21, 2023. https://www.prosthetics.va.gov/serviceandguidedogs.asp
6. Service Dog Veterinary Health Insurance (VHIB) Benefit Rules. US Department of Veterans Affairs Rehabilitation and Prosthetic Services. Updated December 2022. Accessed August 21, 2023. https://www.prosthetics.va.gov/factsheet/PSAS-FactSheet-ServiceDogs.pdf
7. Jensen CL, Rodriguez KE, MacLean EL, Abdul Wahab AH, Sabbaghi A, O’Haire ME. Characterizing veteran and PTSD service dog teams: exploring potential mechanisms of symptom change and canine predictors of efficacy. PloS One. 2022;17(7):e0269186. doi:10.1371/journal.pone.0269186
8. McCall CE, Rodriguez KE, Wadsworth SMM, Meis LA, O’Haire ME. “A Part of Our Family”? Effects of psychiatric service dogs on quality of life and relationship functioning in military-connected couples. Mil Behav Health. 2020;8(4):410-423. doi:10.1080/21635781.2020.1825243
9. Krause-Parello CA, Sarni S, Padden E. Military veterans and canine assistance for post-traumatic stress disorder: a narrative review of the literature. Nurse Educ Today. 2016;47:43-50. doi:10.1016/j.nedt.2016.04.020
10. Van Houtert EAE, Endenburg N, Wijnker JJ, Rodenburg B, Vermetten E. The study of service dogs for veterans with post-traumatic stress disorder: a scoping literature review. Eur J Psychotraumatol. 2018;9(suppl 3):1503523. doi:10.1080/20008198.2018.1503523
11. Sherman M, Hutchinson AD, Bowen H, Iannos M, Van Hooff M. Effectiveness of Operation K9 assistance dogs on suicidality in Australian veterans with PTSD: a 12-month mixed-methods follow-up study. Int J Environ Res Public Health. 2023;20(4):3607. Published 2023 Feb 17. doi:10.3390/ijerph20043607
12. Richerson JT, Saunders GH, Skelton K, et al. A randomized trial of differential effectiveness of service dog pairing to improve quality of life for veterans with PTSD. Office of Research and Development, Veterans Health Administration. 2020:186. https://www.research.va.gov/REPORT-Study-of-Costs-and-Benefits-Associated-with-the-Use-of-Service-Dogs-Monograph1.pdf
1. Rodriguez KE, Bryce CI, Granger DA, O’Haire ME. The effect of a service dog on salivary cortisol awakening response in a military population with posttraumatic stress disorder (PTSD). Psychoneuroendocrinology. 2018;98:202-210. doi:10.1016/j.psyneuen.2018.04.026
2. Leighton SC, Nieforth LO, O’Haire ME. Assistance dogs for military veterans with PTSD: A systematic review, meta-analysis, and meta-synthesis. PloS One. 2022;17(9):e0274960. doi:10.1371/journal.pone.0274960
3. Van Houtert EAE, Rodenburg TB, Vermetten E, Endenburg N. The impact of service dogs on military veterans and (ex) first aid responders with post-traumatic stress disorder. Front Psychiatry. 2022;13:834291. doi:10.3389/fpsyt.2022.834291
4. VHA Directive 1188(1). Animals on Veterans Health Administration (VHA) Property. Veterans Health Administration. August 26, 2015. Amended April 25, 2019. https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=3138
5. Veteran Affairs Rehabilitation and Prosthetic Services. Service Dog Veterinary Health Benefit. US Department of Veterans Affairs. Updated September 19, 2019. Accessed August 21, 2023. https://www.prosthetics.va.gov/serviceandguidedogs.asp
6. Service Dog Veterinary Health Insurance (VHIB) Benefit Rules. US Department of Veterans Affairs Rehabilitation and Prosthetic Services. Updated December 2022. Accessed August 21, 2023. https://www.prosthetics.va.gov/factsheet/PSAS-FactSheet-ServiceDogs.pdf
7. Jensen CL, Rodriguez KE, MacLean EL, Abdul Wahab AH, Sabbaghi A, O’Haire ME. Characterizing veteran and PTSD service dog teams: exploring potential mechanisms of symptom change and canine predictors of efficacy. PloS One. 2022;17(7):e0269186. doi:10.1371/journal.pone.0269186
8. McCall CE, Rodriguez KE, Wadsworth SMM, Meis LA, O’Haire ME. “A Part of Our Family”? Effects of psychiatric service dogs on quality of life and relationship functioning in military-connected couples. Mil Behav Health. 2020;8(4):410-423. doi:10.1080/21635781.2020.1825243
9. Krause-Parello CA, Sarni S, Padden E. Military veterans and canine assistance for post-traumatic stress disorder: a narrative review of the literature. Nurse Educ Today. 2016;47:43-50. doi:10.1016/j.nedt.2016.04.020
10. Van Houtert EAE, Endenburg N, Wijnker JJ, Rodenburg B, Vermetten E. The study of service dogs for veterans with post-traumatic stress disorder: a scoping literature review. Eur J Psychotraumatol. 2018;9(suppl 3):1503523. doi:10.1080/20008198.2018.1503523
11. Sherman M, Hutchinson AD, Bowen H, Iannos M, Van Hooff M. Effectiveness of Operation K9 assistance dogs on suicidality in Australian veterans with PTSD: a 12-month mixed-methods follow-up study. Int J Environ Res Public Health. 2023;20(4):3607. Published 2023 Feb 17. doi:10.3390/ijerph20043607
12. Richerson JT, Saunders GH, Skelton K, et al. A randomized trial of differential effectiveness of service dog pairing to improve quality of life for veterans with PTSD. Office of Research and Development, Veterans Health Administration. 2020:186. https://www.research.va.gov/REPORT-Study-of-Costs-and-Benefits-Associated-with-the-Use-of-Service-Dogs-Monograph1.pdf
Survey: Lack of awareness hampers cancer prevention efforts
The survey, commissioned by Bayer U.S. to identify patient behaviors and care barriers, indicates that more than one in four adults in the United States (27%) would rather not know if they have cancer, and nearly a third (31%) – particularly younger patients aged 18-44 years – avoid going to the doctor because they are afraid of what they might learn.
Similarly, 26% of 2,079 respondents said that fear and anxiety are the main reasons why they don’t make or keep doctor appointments. Those with lower household income and education levels, those with children under age 18 years, and Hispanic adults were most likely to cite this reason.
Almost half (up to 49%) lacked knowledge about certain cancers and risk factors.
For example, 48% of respondents were unaware that breast density affects breast cancer risk and diagnosis, and 38% said they were not very knowledgeable about breast cancer.
Regarding prostate cancer, 49% were unaware that race impacts risk and 49% said they were not knowledgeable about the disease.
The survey highlighted a lack of trust in treatments and health care processes among most adults, especially those with lower income and education levels. Overall, 53% said they have little or no trust in treatments developed by pharmaceutical companies, and 31% said they have little or no trust in medical tests, test results, and other medical processes.
The findings of the survey, which was conducted online June 6-8, 2023, among U.S. adults aged 18 years and older, underscore the need to better educate individuals about cancer risk factors and the benefits of preventative care.
“The increase of fear and anxiety, heightened by a lack of education and in some cases trust barriers, creates an environment where people may not access basic preventative care to ensure early diagnosis,” Sebastian Guth, president of Bayer U.S. and Pharmaceuticals North America, stated in a press release. “This is compounded by the fact that around 27.4 million people of all ages (8.3%) don’t have access to health insurance.
“Companies like Bayer have a responsibility to provide resources that increase health education on the importance of understanding disease risks, early disease screenings, and preventative health care,” Mr. Guth added, noting that the company is partnering with multiple patient advocacy groups to increase trust, awareness, and knowledge “to help individuals understand the resources available to them and their risks for a specific disease.”
Public health initiatives have had mixed results with respect to changing patient behaviors over time, but Breast Cancer Awareness Month (BCAM) in October of each year is a stand-out initiative that could serve as a model for other patient education initiatives, according to a 2022 study.
The Google trends analysis showed that from 2012 to 2021, BCAM was associated with improved public awareness of breast cancer, whereas Lung Cancer Awareness Month and Prostate Cancer Awareness Month had no impact on lung and prostate cancer awareness, respectively, over time, reported Yoshita Nishimura, MD, of Okayama University Graduate School of Medicine, Dentistry, and Pharmaceutical Sciences in Japan, and Jared D. Acoba, MD, of the University of Hawaii, Honolulu.
Dr. Nishimura and Dr. Acoba concluded that the success of BCAM, which was launched in 1985 and is now led by the National Breast Cancer Foundation, is likely a result of “the effective involvement of non-medical industries, influencers affected by breast cancer, and an awareness symbol.”
As for the role of physicians in raising awareness and increasing knowledge at the patient level, various guidelines focus on assessing patient needs and readiness to learn, communicating clearly, and identifying barriers, such as a lack of support and low health literacy.
An American Society of Clinical Oncology consensus guideline for physician-patient communication, for example, provides guidance on core communication skills that apply across the continuum of care, as well as specific topics to address, such as patient goals, treatment options, and support systems – all with an eye toward using “effective communication to optimize the patient-clinician relationship, patient and clinician well-being and family well-being.”
The survey, commissioned by Bayer U.S. to identify patient behaviors and care barriers, indicates that more than one in four adults in the United States (27%) would rather not know if they have cancer, and nearly a third (31%) – particularly younger patients aged 18-44 years – avoid going to the doctor because they are afraid of what they might learn.
Similarly, 26% of 2,079 respondents said that fear and anxiety are the main reasons why they don’t make or keep doctor appointments. Those with lower household income and education levels, those with children under age 18 years, and Hispanic adults were most likely to cite this reason.
Almost half (up to 49%) lacked knowledge about certain cancers and risk factors.
For example, 48% of respondents were unaware that breast density affects breast cancer risk and diagnosis, and 38% said they were not very knowledgeable about breast cancer.
Regarding prostate cancer, 49% were unaware that race impacts risk and 49% said they were not knowledgeable about the disease.
The survey highlighted a lack of trust in treatments and health care processes among most adults, especially those with lower income and education levels. Overall, 53% said they have little or no trust in treatments developed by pharmaceutical companies, and 31% said they have little or no trust in medical tests, test results, and other medical processes.
The findings of the survey, which was conducted online June 6-8, 2023, among U.S. adults aged 18 years and older, underscore the need to better educate individuals about cancer risk factors and the benefits of preventative care.
“The increase of fear and anxiety, heightened by a lack of education and in some cases trust barriers, creates an environment where people may not access basic preventative care to ensure early diagnosis,” Sebastian Guth, president of Bayer U.S. and Pharmaceuticals North America, stated in a press release. “This is compounded by the fact that around 27.4 million people of all ages (8.3%) don’t have access to health insurance.
“Companies like Bayer have a responsibility to provide resources that increase health education on the importance of understanding disease risks, early disease screenings, and preventative health care,” Mr. Guth added, noting that the company is partnering with multiple patient advocacy groups to increase trust, awareness, and knowledge “to help individuals understand the resources available to them and their risks for a specific disease.”
Public health initiatives have had mixed results with respect to changing patient behaviors over time, but Breast Cancer Awareness Month (BCAM) in October of each year is a stand-out initiative that could serve as a model for other patient education initiatives, according to a 2022 study.
The Google trends analysis showed that from 2012 to 2021, BCAM was associated with improved public awareness of breast cancer, whereas Lung Cancer Awareness Month and Prostate Cancer Awareness Month had no impact on lung and prostate cancer awareness, respectively, over time, reported Yoshita Nishimura, MD, of Okayama University Graduate School of Medicine, Dentistry, and Pharmaceutical Sciences in Japan, and Jared D. Acoba, MD, of the University of Hawaii, Honolulu.
Dr. Nishimura and Dr. Acoba concluded that the success of BCAM, which was launched in 1985 and is now led by the National Breast Cancer Foundation, is likely a result of “the effective involvement of non-medical industries, influencers affected by breast cancer, and an awareness symbol.”
As for the role of physicians in raising awareness and increasing knowledge at the patient level, various guidelines focus on assessing patient needs and readiness to learn, communicating clearly, and identifying barriers, such as a lack of support and low health literacy.
An American Society of Clinical Oncology consensus guideline for physician-patient communication, for example, provides guidance on core communication skills that apply across the continuum of care, as well as specific topics to address, such as patient goals, treatment options, and support systems – all with an eye toward using “effective communication to optimize the patient-clinician relationship, patient and clinician well-being and family well-being.”
The survey, commissioned by Bayer U.S. to identify patient behaviors and care barriers, indicates that more than one in four adults in the United States (27%) would rather not know if they have cancer, and nearly a third (31%) – particularly younger patients aged 18-44 years – avoid going to the doctor because they are afraid of what they might learn.
Similarly, 26% of 2,079 respondents said that fear and anxiety are the main reasons why they don’t make or keep doctor appointments. Those with lower household income and education levels, those with children under age 18 years, and Hispanic adults were most likely to cite this reason.
Almost half (up to 49%) lacked knowledge about certain cancers and risk factors.
For example, 48% of respondents were unaware that breast density affects breast cancer risk and diagnosis, and 38% said they were not very knowledgeable about breast cancer.
Regarding prostate cancer, 49% were unaware that race impacts risk and 49% said they were not knowledgeable about the disease.
The survey highlighted a lack of trust in treatments and health care processes among most adults, especially those with lower income and education levels. Overall, 53% said they have little or no trust in treatments developed by pharmaceutical companies, and 31% said they have little or no trust in medical tests, test results, and other medical processes.
The findings of the survey, which was conducted online June 6-8, 2023, among U.S. adults aged 18 years and older, underscore the need to better educate individuals about cancer risk factors and the benefits of preventative care.
“The increase of fear and anxiety, heightened by a lack of education and in some cases trust barriers, creates an environment where people may not access basic preventative care to ensure early diagnosis,” Sebastian Guth, president of Bayer U.S. and Pharmaceuticals North America, stated in a press release. “This is compounded by the fact that around 27.4 million people of all ages (8.3%) don’t have access to health insurance.
“Companies like Bayer have a responsibility to provide resources that increase health education on the importance of understanding disease risks, early disease screenings, and preventative health care,” Mr. Guth added, noting that the company is partnering with multiple patient advocacy groups to increase trust, awareness, and knowledge “to help individuals understand the resources available to them and their risks for a specific disease.”
Public health initiatives have had mixed results with respect to changing patient behaviors over time, but Breast Cancer Awareness Month (BCAM) in October of each year is a stand-out initiative that could serve as a model for other patient education initiatives, according to a 2022 study.
The Google trends analysis showed that from 2012 to 2021, BCAM was associated with improved public awareness of breast cancer, whereas Lung Cancer Awareness Month and Prostate Cancer Awareness Month had no impact on lung and prostate cancer awareness, respectively, over time, reported Yoshita Nishimura, MD, of Okayama University Graduate School of Medicine, Dentistry, and Pharmaceutical Sciences in Japan, and Jared D. Acoba, MD, of the University of Hawaii, Honolulu.
Dr. Nishimura and Dr. Acoba concluded that the success of BCAM, which was launched in 1985 and is now led by the National Breast Cancer Foundation, is likely a result of “the effective involvement of non-medical industries, influencers affected by breast cancer, and an awareness symbol.”
As for the role of physicians in raising awareness and increasing knowledge at the patient level, various guidelines focus on assessing patient needs and readiness to learn, communicating clearly, and identifying barriers, such as a lack of support and low health literacy.
An American Society of Clinical Oncology consensus guideline for physician-patient communication, for example, provides guidance on core communication skills that apply across the continuum of care, as well as specific topics to address, such as patient goals, treatment options, and support systems – all with an eye toward using “effective communication to optimize the patient-clinician relationship, patient and clinician well-being and family well-being.”
Patisiran (Onpattro) for ATTR cardiomyopathy gets FDA panel thumbs up
The Cardiovascular and Renal Drugs Advisory Committee of the Food and Drug Administration has voted 9 to 3 that the benefits of patisiran outweigh the risks for the treatment of ATTR amyloidosis cardiomyopathy – although many panel members questioned whether the benefits are clinically meaningful.
ATTR amyloidosis is an underdiagnosed, rapidly progressive, debilitating, and fatal disease caused by misfolded TTR proteins, which accumulate as amyloid deposits in various parts of the body, including the heart.
Intravenously administered patisiran is already approved in the United States and Canada for the treatment of the polyneuropathy of hereditary ATTR amyloidosis in adults.
In the APOLLO-B trial, patisiran showed a statistically significant and clinically meaningful benefit on functional capacity, as measured by the 6-minute walk test, compared with placebo, in patients with ATTR amyloidosis with cardiomyopathy.
The study also met its first secondary endpoint, demonstrating a statistically significant and clinically meaningful benefit on health status and quality of life.
But in explaining her “no” vote, committee member C. Noel Bairey Merz, MD, Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles, said she “did not feel like there was benefit” using existing clinically relevant thresholds typically used in cardiology.
Committee chair Javed Butler, MD, MPH, Baylor Scott & White Research Institute, Dallas, who also voted no, said he “struggled” with this vote and emphasized that it “absolutely does not reflect that there is not a potential with the therapy.”
Dr. Butler said he voted no largely because he wasn’t sure whether the benefits are clinically meaningful in the context of the study design and how it was conducted. He did not have any safety concerns, which was the general feeling of the committee.
Edward Kasper, MD, Johns Hopkins University, Baltimore, who voted in favor of patisiran for ATTR amyloidosis with cardiomyopathy, said there is a “light wind for benefit and no wind for risk. So, if you’re asking do benefits outweigh the risks, the answer is yes.”
But Dr. Kasper also noted: “It would have been a more difficult question to answer: Is there clinically meaningful benefit versus risk? But that’s not what the question asked.”
In explaining his “yes” vote, Ravi Thadhani, MD, MPH, Emory University, Atlanta, said: “We’re dealing with a rare disease with few options and devastating consequences. We heard from clinicians loud and clear, and from patients for that matter, that options and alternatives are critical, and that there is a continuous decline of cardiac function and worsening of disease in a number of patients that have received the current standard of care. For me, the benefits outweigh the risks.”
Dr. Thadhani also noted that from the data provided, no benefit was shown – ”disappointingly” he lamented – for women, for Black persons, and among individuals who were receiving tafamidis, and he urged the FDA and sponsor to consider this.
The FDA has set a target action date for patisiran for ATTR amyloidosis cardiomyopathy of Oct. 8.
A version of this article first appeared on Medscape.com.
The Cardiovascular and Renal Drugs Advisory Committee of the Food and Drug Administration has voted 9 to 3 that the benefits of patisiran outweigh the risks for the treatment of ATTR amyloidosis cardiomyopathy – although many panel members questioned whether the benefits are clinically meaningful.
ATTR amyloidosis is an underdiagnosed, rapidly progressive, debilitating, and fatal disease caused by misfolded TTR proteins, which accumulate as amyloid deposits in various parts of the body, including the heart.
Intravenously administered patisiran is already approved in the United States and Canada for the treatment of the polyneuropathy of hereditary ATTR amyloidosis in adults.
In the APOLLO-B trial, patisiran showed a statistically significant and clinically meaningful benefit on functional capacity, as measured by the 6-minute walk test, compared with placebo, in patients with ATTR amyloidosis with cardiomyopathy.
The study also met its first secondary endpoint, demonstrating a statistically significant and clinically meaningful benefit on health status and quality of life.
But in explaining her “no” vote, committee member C. Noel Bairey Merz, MD, Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles, said she “did not feel like there was benefit” using existing clinically relevant thresholds typically used in cardiology.
Committee chair Javed Butler, MD, MPH, Baylor Scott & White Research Institute, Dallas, who also voted no, said he “struggled” with this vote and emphasized that it “absolutely does not reflect that there is not a potential with the therapy.”
Dr. Butler said he voted no largely because he wasn’t sure whether the benefits are clinically meaningful in the context of the study design and how it was conducted. He did not have any safety concerns, which was the general feeling of the committee.
Edward Kasper, MD, Johns Hopkins University, Baltimore, who voted in favor of patisiran for ATTR amyloidosis with cardiomyopathy, said there is a “light wind for benefit and no wind for risk. So, if you’re asking do benefits outweigh the risks, the answer is yes.”
But Dr. Kasper also noted: “It would have been a more difficult question to answer: Is there clinically meaningful benefit versus risk? But that’s not what the question asked.”
In explaining his “yes” vote, Ravi Thadhani, MD, MPH, Emory University, Atlanta, said: “We’re dealing with a rare disease with few options and devastating consequences. We heard from clinicians loud and clear, and from patients for that matter, that options and alternatives are critical, and that there is a continuous decline of cardiac function and worsening of disease in a number of patients that have received the current standard of care. For me, the benefits outweigh the risks.”
Dr. Thadhani also noted that from the data provided, no benefit was shown – ”disappointingly” he lamented – for women, for Black persons, and among individuals who were receiving tafamidis, and he urged the FDA and sponsor to consider this.
The FDA has set a target action date for patisiran for ATTR amyloidosis cardiomyopathy of Oct. 8.
A version of this article first appeared on Medscape.com.
The Cardiovascular and Renal Drugs Advisory Committee of the Food and Drug Administration has voted 9 to 3 that the benefits of patisiran outweigh the risks for the treatment of ATTR amyloidosis cardiomyopathy – although many panel members questioned whether the benefits are clinically meaningful.
ATTR amyloidosis is an underdiagnosed, rapidly progressive, debilitating, and fatal disease caused by misfolded TTR proteins, which accumulate as amyloid deposits in various parts of the body, including the heart.
Intravenously administered patisiran is already approved in the United States and Canada for the treatment of the polyneuropathy of hereditary ATTR amyloidosis in adults.
In the APOLLO-B trial, patisiran showed a statistically significant and clinically meaningful benefit on functional capacity, as measured by the 6-minute walk test, compared with placebo, in patients with ATTR amyloidosis with cardiomyopathy.
The study also met its first secondary endpoint, demonstrating a statistically significant and clinically meaningful benefit on health status and quality of life.
But in explaining her “no” vote, committee member C. Noel Bairey Merz, MD, Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles, said she “did not feel like there was benefit” using existing clinically relevant thresholds typically used in cardiology.
Committee chair Javed Butler, MD, MPH, Baylor Scott & White Research Institute, Dallas, who also voted no, said he “struggled” with this vote and emphasized that it “absolutely does not reflect that there is not a potential with the therapy.”
Dr. Butler said he voted no largely because he wasn’t sure whether the benefits are clinically meaningful in the context of the study design and how it was conducted. He did not have any safety concerns, which was the general feeling of the committee.
Edward Kasper, MD, Johns Hopkins University, Baltimore, who voted in favor of patisiran for ATTR amyloidosis with cardiomyopathy, said there is a “light wind for benefit and no wind for risk. So, if you’re asking do benefits outweigh the risks, the answer is yes.”
But Dr. Kasper also noted: “It would have been a more difficult question to answer: Is there clinically meaningful benefit versus risk? But that’s not what the question asked.”
In explaining his “yes” vote, Ravi Thadhani, MD, MPH, Emory University, Atlanta, said: “We’re dealing with a rare disease with few options and devastating consequences. We heard from clinicians loud and clear, and from patients for that matter, that options and alternatives are critical, and that there is a continuous decline of cardiac function and worsening of disease in a number of patients that have received the current standard of care. For me, the benefits outweigh the risks.”
Dr. Thadhani also noted that from the data provided, no benefit was shown – ”disappointingly” he lamented – for women, for Black persons, and among individuals who were receiving tafamidis, and he urged the FDA and sponsor to consider this.
The FDA has set a target action date for patisiran for ATTR amyloidosis cardiomyopathy of Oct. 8.
A version of this article first appeared on Medscape.com.
The role of social media in aesthetic trends
Recently, but I had never heard it before. Not too long afterwards, patients were asking me about it in the office, using the same terminology, and I had several calls about it in one day. When I asked one trusted patient where she’d heard this term, which seemed to be trending, she told me that she had seen it on Instagram, as an ad or a “suggested for you” post.
Whether it’s a different name or term for a cosmetic procedure or laser we use that I’ve never heard before – such as “lip flip” or trap tox (also known as “Barbie Botox”) – many of these trendy terms spread like wildfire on social media. Some of the terms may be marketing tools started and spread by doctors who perform aesthetic procedures, something I don’t recommend as it only creates confusion for patients and practitioners, similar to the confusion consumers face regarding the plethora of over-the-counter skin care options and the marketing terms used for them. Other terms and trends are also started by nonphysician or non–professionally trained providers, sometimes leading to an unsafe or misleading term for an aesthetic procedure.

Over the past few years, several articles about the impact of social media in aesthetics have been published. In one recent paper, published in 2022, Boen and Jerdan noted that 72% of people in the United States use social media, up from 5% of American adults in 2005. In the United States, they note, “YouTube is the most popular platform with 73% of adult users, followed by Facebook (69%), Instagram (37%), SnapChat (24%), and Twitter (22%). Of the sites used daily, Facebook has the most activity (74%), followed by Instagram (64%), SnapChat (63%), YouTube (51%), and Twitter (42%).” They argue that the pros of social media in aesthetic medicine include its use as an educational tool by medical professionals to educate and provide accurate information about cosmetic procedures, and that “providing factual and evidence-based medical information to the public can help to counteract the abundant misinformation that is out there.” The cons include misinformation, no credentialing verification of the provider of the information – essentially anyone can be an “influencer” – as well as the addictive nature of social media for the consumer.
Along the same lines, younger patients tend to rely more on social media in choosing treatments and providers, further perpetuating any anxiety created from misinformation and unrealistic expectations from nonmedical influencers regarding procedures, filters used on photographs, photo editing, etc., in achieving an aesthetic result.
Physicians, particularly fellowship-trained aesthetic and surgical dermatologists, plastic and reconstructive surgeons, oculoplastic surgeons, and ENT facial plastic surgeons, who have the most training, knowledge, and expertise about aesthetic procedures, often have the least amount of time to devote to education via social media, compared with nonmedical influencers. Unless sponsored, they are also not being compensated for using it as an educational tool, except for potential indirect compensation from using it as a marketing tool for themselves and their practices. In contrast, nonmedical influencers often have many followers and time to create content, and in some cases, this is their full-time job.
All in all, most authors agree that social media has been associated with an increased acceptance of cosmetic surgery and procedures. Whether it be a trend seen on social media, or viewing one’s appearance in a filtered or photoediting app, or seeing an image of how another person looks (similar to how people in magazines, films and on television, were viewed in the past), social media has piqued people’s interest in aesthetics. It remains a balance for interested physicians to help keep information about cosmetic procedures presented in a healthy, interesting, professional, and accurate manner, and in a non–time-consuming way.
Dr. Wesley practices dermatology in Beverly Hills, Calif. Write to her at dermnews@mdedge.com. She had no relevant disclosures.
References
Boen M and Jerdan K. Clin Dermatol. 2022 Jan-Feb;40(1):45-8.
Chen J et al. JAMA Facial Plast Surg. 2019 Sep 1;21(5):361-7.
Chopan M et al. Plast Reconstr Surg. 2019 Apr;143(4):1259-65.
Recently, but I had never heard it before. Not too long afterwards, patients were asking me about it in the office, using the same terminology, and I had several calls about it in one day. When I asked one trusted patient where she’d heard this term, which seemed to be trending, she told me that she had seen it on Instagram, as an ad or a “suggested for you” post.
Whether it’s a different name or term for a cosmetic procedure or laser we use that I’ve never heard before – such as “lip flip” or trap tox (also known as “Barbie Botox”) – many of these trendy terms spread like wildfire on social media. Some of the terms may be marketing tools started and spread by doctors who perform aesthetic procedures, something I don’t recommend as it only creates confusion for patients and practitioners, similar to the confusion consumers face regarding the plethora of over-the-counter skin care options and the marketing terms used for them. Other terms and trends are also started by nonphysician or non–professionally trained providers, sometimes leading to an unsafe or misleading term for an aesthetic procedure.
Over the past few years, several articles about the impact of social media in aesthetics have been published. In one recent paper, published in 2022, Boen and Jerdan noted that 72% of people in the United States use social media, up from 5% of American adults in 2005. In the United States, they note, “YouTube is the most popular platform with 73% of adult users, followed by Facebook (69%), Instagram (37%), SnapChat (24%), and Twitter (22%). Of the sites used daily, Facebook has the most activity (74%), followed by Instagram (64%), SnapChat (63%), YouTube (51%), and Twitter (42%).” They argue that the pros of social media in aesthetic medicine include its use as an educational tool by medical professionals to educate and provide accurate information about cosmetic procedures, and that “providing factual and evidence-based medical information to the public can help to counteract the abundant misinformation that is out there.” The cons include misinformation, no credentialing verification of the provider of the information – essentially anyone can be an “influencer” – as well as the addictive nature of social media for the consumer.
Along the same lines, younger patients tend to rely more on social media in choosing treatments and providers, further perpetuating any anxiety created from misinformation and unrealistic expectations from nonmedical influencers regarding procedures, filters used on photographs, photo editing, etc., in achieving an aesthetic result.
Physicians, particularly fellowship-trained aesthetic and surgical dermatologists, plastic and reconstructive surgeons, oculoplastic surgeons, and ENT facial plastic surgeons, who have the most training, knowledge, and expertise about aesthetic procedures, often have the least amount of time to devote to education via social media, compared with nonmedical influencers. Unless sponsored, they are also not being compensated for using it as an educational tool, except for potential indirect compensation from using it as a marketing tool for themselves and their practices. In contrast, nonmedical influencers often have many followers and time to create content, and in some cases, this is their full-time job.
All in all, most authors agree that social media has been associated with an increased acceptance of cosmetic surgery and procedures. Whether it be a trend seen on social media, or viewing one’s appearance in a filtered or photoediting app, or seeing an image of how another person looks (similar to how people in magazines, films and on television, were viewed in the past), social media has piqued people’s interest in aesthetics. It remains a balance for interested physicians to help keep information about cosmetic procedures presented in a healthy, interesting, professional, and accurate manner, and in a non–time-consuming way.
Dr. Wesley practices dermatology in Beverly Hills, Calif. Write to her at dermnews@mdedge.com. She had no relevant disclosures.
References
Boen M and Jerdan K. Clin Dermatol. 2022 Jan-Feb;40(1):45-8.
Chen J et al. JAMA Facial Plast Surg. 2019 Sep 1;21(5):361-7.
Chopan M et al. Plast Reconstr Surg. 2019 Apr;143(4):1259-65.
Recently, but I had never heard it before. Not too long afterwards, patients were asking me about it in the office, using the same terminology, and I had several calls about it in one day. When I asked one trusted patient where she’d heard this term, which seemed to be trending, she told me that she had seen it on Instagram, as an ad or a “suggested for you” post.
Whether it’s a different name or term for a cosmetic procedure or laser we use that I’ve never heard before – such as “lip flip” or trap tox (also known as “Barbie Botox”) – many of these trendy terms spread like wildfire on social media. Some of the terms may be marketing tools started and spread by doctors who perform aesthetic procedures, something I don’t recommend as it only creates confusion for patients and practitioners, similar to the confusion consumers face regarding the plethora of over-the-counter skin care options and the marketing terms used for them. Other terms and trends are also started by nonphysician or non–professionally trained providers, sometimes leading to an unsafe or misleading term for an aesthetic procedure.
Over the past few years, several articles about the impact of social media in aesthetics have been published. In one recent paper, published in 2022, Boen and Jerdan noted that 72% of people in the United States use social media, up from 5% of American adults in 2005. In the United States, they note, “YouTube is the most popular platform with 73% of adult users, followed by Facebook (69%), Instagram (37%), SnapChat (24%), and Twitter (22%). Of the sites used daily, Facebook has the most activity (74%), followed by Instagram (64%), SnapChat (63%), YouTube (51%), and Twitter (42%).” They argue that the pros of social media in aesthetic medicine include its use as an educational tool by medical professionals to educate and provide accurate information about cosmetic procedures, and that “providing factual and evidence-based medical information to the public can help to counteract the abundant misinformation that is out there.” The cons include misinformation, no credentialing verification of the provider of the information – essentially anyone can be an “influencer” – as well as the addictive nature of social media for the consumer.
Along the same lines, younger patients tend to rely more on social media in choosing treatments and providers, further perpetuating any anxiety created from misinformation and unrealistic expectations from nonmedical influencers regarding procedures, filters used on photographs, photo editing, etc., in achieving an aesthetic result.
Physicians, particularly fellowship-trained aesthetic and surgical dermatologists, plastic and reconstructive surgeons, oculoplastic surgeons, and ENT facial plastic surgeons, who have the most training, knowledge, and expertise about aesthetic procedures, often have the least amount of time to devote to education via social media, compared with nonmedical influencers. Unless sponsored, they are also not being compensated for using it as an educational tool, except for potential indirect compensation from using it as a marketing tool for themselves and their practices. In contrast, nonmedical influencers often have many followers and time to create content, and in some cases, this is their full-time job.
All in all, most authors agree that social media has been associated with an increased acceptance of cosmetic surgery and procedures. Whether it be a trend seen on social media, or viewing one’s appearance in a filtered or photoediting app, or seeing an image of how another person looks (similar to how people in magazines, films and on television, were viewed in the past), social media has piqued people’s interest in aesthetics. It remains a balance for interested physicians to help keep information about cosmetic procedures presented in a healthy, interesting, professional, and accurate manner, and in a non–time-consuming way.
Dr. Wesley practices dermatology in Beverly Hills, Calif. Write to her at dermnews@mdedge.com. She had no relevant disclosures.
References
Boen M and Jerdan K. Clin Dermatol. 2022 Jan-Feb;40(1):45-8.
Chen J et al. JAMA Facial Plast Surg. 2019 Sep 1;21(5):361-7.
Chopan M et al. Plast Reconstr Surg. 2019 Apr;143(4):1259-65.
Can skin bleaching lead to cancer?
SINGAPORE –
This question was posed by Ousmane Faye, MD, PhD, director general of Mali’s Bamako Dermatology Hospital, at the World Congress of Dermatology.
Dr. Faye explored the issue during a hot topics session at the meeting, prefacing that it was an important question to ask because “in West Africa, skin bleaching is very common.”
“There are many local names” for skin bleaching, he said. “For example, in Senegal, it’s called xessal; in Mali and Ivory Coast, its name is caco; in South Africa, there are many names, like ukutsheyisa.”
Skin bleaching refers to the cosmetic misuse of topical agents to change one’s natural skin color. It’s a centuries-old practice that people, mainly women, adopt “to increase attractiveness and self-esteem,” explained Dr. Faye.
To demonstrate how pervasive skin bleaching is on the continent, he presented a slide that summarized figures from six studies spanning the past 2 decades. Prevalence ranged from 25% in Mali (based on a 1993 survey of 210 women) to a high of 79.25% in Benin (from a sample size of 511 women in 2019). In other studies of women in Burkina Faso and Togo, the figures were 44.3% and 58.9%, respectively. The most recently conducted study, which involved 2,689 Senegalese women and was published in 2022, found that nearly 6 in 10 (59.2%) respondents used skin-lightening products.
But skin bleaching isn’t just limited to Africa, said session moderator Omar Lupi, MD, PhD, associate professor of dermatology at the Federal University of the State of Rio de Janeiro, when approached for an independent comment. “It’s a traditional practice around the world. Maybe not in the developed countries, but it’s quite common in Africa, in South America, and in Asia.”
His sentiments are echoed in a meta-analysis that was published in the International Journal of Dermatology in 2019. The work examined 68 studies involving more than 67,000 people across Africa, Asia, Europe, the Middle East, and North America. It found that the pooled lifetime prevalence of skin bleaching was 27.7% (95% confidence interval, 19.6-37.5; P < .01).
“This is an important and interesting topic because our world is shrinking,” Dr. Lupi told this news organization. “Even in countries that don’t have bleaching as a common situation, we now have patients who are migrating from one part [of the world] to another, so bleaching is something that can knock on your door and you need to be prepared.”
Misuse leads to complications
The issue is pertinent to dermatologists because skin bleaching is associated with a wide range of complications. Take, for example, topical steroids, which are the most common products used for bleaching, said Dr. Faye in his talk.
“Clobetasol can suppress the hypothalamic-pituitary-adrenal (HPA) function,” he said, referring to the body’s main stress response system. “It can also foster skin infection, including bacterial, fungal, viral, and parasitic infection.”
In addition, topical steroids that are misused as skin lighteners have been reported to cause stretch marks, skin atrophy, inflammatory acne, and even metabolic disorders such as diabetes and hypertension, said Dr. Faye.
To further his point, he cited a 2021 prospective case-control study conducted across five sub-Saharan countries, which found that the use of “voluntary cosmetic depigmentation” significantly increased a person’s risk for necrotizing fasciitis of the lower limbs (odds ratio, 2.29; 95% CI, 1.19-3.73; P = .0226).
Similarly, mercury, another substance found in products commonly used to bleach skin, has been associated with problems ranging from rashes to renal toxicity. And because it’s so incredibly harmful, mercury is also known to cause neurologic abnormalities.
Apart from causing certain conditions, prolonged use of skin-lightening products can change the way existing diseases present themselves as well as their severity, added Dr. Faye.
An increased risk
But what about skin bleaching’s link with cancer? “Skin cancer on Black skin is uncommon, yet it occurs in skin-bleaching women,” said Dr. Faye.
“Since 2000, we have had some cases of skin cancer associated with skin bleaching,” he continued, adding that squamous cell carcinoma (SCC) is the most frequent type of cancer observed.
If you look at what’s been published on the topic so far, you’ll see that “all the cases of skin cancer are located over the neck or some exposed area when skin bleaching products are used for more than 10 years,” said Dr. Faye. “And most of the time, the age of the patient ranges from 30 to 60 years.”
The first known case in Africa was reported in a 58-year-old woman from Ghana, who had been using skin bleaching products for close to 30 years. The patient presented with tumors on her face, neck, and arms.
Dr. Faye then proceeded to share more than 10 such carcinoma cases. “These previous reports strongly suggest a relationship between skin bleaching and skin cancers,” said Dr. Faye.
Indeed, there have been reports and publications in the literature that support his observation, including one last year, which found that use of the tyrosinase inhibitor hydroquinone was associated with approximately a threefold increased risk for skin cancer.
For some, including Brazil’s Dr. Lupi, Dr. Faye’s talk was enlightening: “I didn’t know about this relationship [of bleaching] with skin cancer, it was something new for me.”
But the prevalence of SCC is very low, compared with that of skin bleaching, Dr. Faye acknowledged. Moreover, the cancer observed in the cases reported could have resulted from a number of reasons, including exposure to harmful ultraviolet rays from the sun and genetic predisposition in addition to the use of bleaching products such as hydroquinone. “Other causes of skin cancer are not excluded,” he said.
To further explore the link between skin bleaching and cancer, “we need case-control studies to provide more evidence,” he added. Until then, dermatologists “should keep on promoting messages” to prevent SCC from occurring. This includes encouraging the use of proper sun protection in addition to discouraging the practice of skin bleaching, which still persists despite more than 10 African nations banning the use of toxic skin-lightening products.
Dr. Faye and Dr. Lupi report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SINGAPORE –
This question was posed by Ousmane Faye, MD, PhD, director general of Mali’s Bamako Dermatology Hospital, at the World Congress of Dermatology.
Dr. Faye explored the issue during a hot topics session at the meeting, prefacing that it was an important question to ask because “in West Africa, skin bleaching is very common.”
“There are many local names” for skin bleaching, he said. “For example, in Senegal, it’s called xessal; in Mali and Ivory Coast, its name is caco; in South Africa, there are many names, like ukutsheyisa.”
Skin bleaching refers to the cosmetic misuse of topical agents to change one’s natural skin color. It’s a centuries-old practice that people, mainly women, adopt “to increase attractiveness and self-esteem,” explained Dr. Faye.
To demonstrate how pervasive skin bleaching is on the continent, he presented a slide that summarized figures from six studies spanning the past 2 decades. Prevalence ranged from 25% in Mali (based on a 1993 survey of 210 women) to a high of 79.25% in Benin (from a sample size of 511 women in 2019). In other studies of women in Burkina Faso and Togo, the figures were 44.3% and 58.9%, respectively. The most recently conducted study, which involved 2,689 Senegalese women and was published in 2022, found that nearly 6 in 10 (59.2%) respondents used skin-lightening products.
But skin bleaching isn’t just limited to Africa, said session moderator Omar Lupi, MD, PhD, associate professor of dermatology at the Federal University of the State of Rio de Janeiro, when approached for an independent comment. “It’s a traditional practice around the world. Maybe not in the developed countries, but it’s quite common in Africa, in South America, and in Asia.”
His sentiments are echoed in a meta-analysis that was published in the International Journal of Dermatology in 2019. The work examined 68 studies involving more than 67,000 people across Africa, Asia, Europe, the Middle East, and North America. It found that the pooled lifetime prevalence of skin bleaching was 27.7% (95% confidence interval, 19.6-37.5; P < .01).
“This is an important and interesting topic because our world is shrinking,” Dr. Lupi told this news organization. “Even in countries that don’t have bleaching as a common situation, we now have patients who are migrating from one part [of the world] to another, so bleaching is something that can knock on your door and you need to be prepared.”
Misuse leads to complications
The issue is pertinent to dermatologists because skin bleaching is associated with a wide range of complications. Take, for example, topical steroids, which are the most common products used for bleaching, said Dr. Faye in his talk.
“Clobetasol can suppress the hypothalamic-pituitary-adrenal (HPA) function,” he said, referring to the body’s main stress response system. “It can also foster skin infection, including bacterial, fungal, viral, and parasitic infection.”
In addition, topical steroids that are misused as skin lighteners have been reported to cause stretch marks, skin atrophy, inflammatory acne, and even metabolic disorders such as diabetes and hypertension, said Dr. Faye.
To further his point, he cited a 2021 prospective case-control study conducted across five sub-Saharan countries, which found that the use of “voluntary cosmetic depigmentation” significantly increased a person’s risk for necrotizing fasciitis of the lower limbs (odds ratio, 2.29; 95% CI, 1.19-3.73; P = .0226).
Similarly, mercury, another substance found in products commonly used to bleach skin, has been associated with problems ranging from rashes to renal toxicity. And because it’s so incredibly harmful, mercury is also known to cause neurologic abnormalities.
Apart from causing certain conditions, prolonged use of skin-lightening products can change the way existing diseases present themselves as well as their severity, added Dr. Faye.
An increased risk
But what about skin bleaching’s link with cancer? “Skin cancer on Black skin is uncommon, yet it occurs in skin-bleaching women,” said Dr. Faye.
“Since 2000, we have had some cases of skin cancer associated with skin bleaching,” he continued, adding that squamous cell carcinoma (SCC) is the most frequent type of cancer observed.
If you look at what’s been published on the topic so far, you’ll see that “all the cases of skin cancer are located over the neck or some exposed area when skin bleaching products are used for more than 10 years,” said Dr. Faye. “And most of the time, the age of the patient ranges from 30 to 60 years.”
The first known case in Africa was reported in a 58-year-old woman from Ghana, who had been using skin bleaching products for close to 30 years. The patient presented with tumors on her face, neck, and arms.
Dr. Faye then proceeded to share more than 10 such carcinoma cases. “These previous reports strongly suggest a relationship between skin bleaching and skin cancers,” said Dr. Faye.
Indeed, there have been reports and publications in the literature that support his observation, including one last year, which found that use of the tyrosinase inhibitor hydroquinone was associated with approximately a threefold increased risk for skin cancer.
For some, including Brazil’s Dr. Lupi, Dr. Faye’s talk was enlightening: “I didn’t know about this relationship [of bleaching] with skin cancer, it was something new for me.”
But the prevalence of SCC is very low, compared with that of skin bleaching, Dr. Faye acknowledged. Moreover, the cancer observed in the cases reported could have resulted from a number of reasons, including exposure to harmful ultraviolet rays from the sun and genetic predisposition in addition to the use of bleaching products such as hydroquinone. “Other causes of skin cancer are not excluded,” he said.
To further explore the link between skin bleaching and cancer, “we need case-control studies to provide more evidence,” he added. Until then, dermatologists “should keep on promoting messages” to prevent SCC from occurring. This includes encouraging the use of proper sun protection in addition to discouraging the practice of skin bleaching, which still persists despite more than 10 African nations banning the use of toxic skin-lightening products.
Dr. Faye and Dr. Lupi report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SINGAPORE –
This question was posed by Ousmane Faye, MD, PhD, director general of Mali’s Bamako Dermatology Hospital, at the World Congress of Dermatology.
Dr. Faye explored the issue during a hot topics session at the meeting, prefacing that it was an important question to ask because “in West Africa, skin bleaching is very common.”
“There are many local names” for skin bleaching, he said. “For example, in Senegal, it’s called xessal; in Mali and Ivory Coast, its name is caco; in South Africa, there are many names, like ukutsheyisa.”
Skin bleaching refers to the cosmetic misuse of topical agents to change one’s natural skin color. It’s a centuries-old practice that people, mainly women, adopt “to increase attractiveness and self-esteem,” explained Dr. Faye.
To demonstrate how pervasive skin bleaching is on the continent, he presented a slide that summarized figures from six studies spanning the past 2 decades. Prevalence ranged from 25% in Mali (based on a 1993 survey of 210 women) to a high of 79.25% in Benin (from a sample size of 511 women in 2019). In other studies of women in Burkina Faso and Togo, the figures were 44.3% and 58.9%, respectively. The most recently conducted study, which involved 2,689 Senegalese women and was published in 2022, found that nearly 6 in 10 (59.2%) respondents used skin-lightening products.
But skin bleaching isn’t just limited to Africa, said session moderator Omar Lupi, MD, PhD, associate professor of dermatology at the Federal University of the State of Rio de Janeiro, when approached for an independent comment. “It’s a traditional practice around the world. Maybe not in the developed countries, but it’s quite common in Africa, in South America, and in Asia.”
His sentiments are echoed in a meta-analysis that was published in the International Journal of Dermatology in 2019. The work examined 68 studies involving more than 67,000 people across Africa, Asia, Europe, the Middle East, and North America. It found that the pooled lifetime prevalence of skin bleaching was 27.7% (95% confidence interval, 19.6-37.5; P < .01).
“This is an important and interesting topic because our world is shrinking,” Dr. Lupi told this news organization. “Even in countries that don’t have bleaching as a common situation, we now have patients who are migrating from one part [of the world] to another, so bleaching is something that can knock on your door and you need to be prepared.”
Misuse leads to complications
The issue is pertinent to dermatologists because skin bleaching is associated with a wide range of complications. Take, for example, topical steroids, which are the most common products used for bleaching, said Dr. Faye in his talk.
“Clobetasol can suppress the hypothalamic-pituitary-adrenal (HPA) function,” he said, referring to the body’s main stress response system. “It can also foster skin infection, including bacterial, fungal, viral, and parasitic infection.”
In addition, topical steroids that are misused as skin lighteners have been reported to cause stretch marks, skin atrophy, inflammatory acne, and even metabolic disorders such as diabetes and hypertension, said Dr. Faye.
To further his point, he cited a 2021 prospective case-control study conducted across five sub-Saharan countries, which found that the use of “voluntary cosmetic depigmentation” significantly increased a person’s risk for necrotizing fasciitis of the lower limbs (odds ratio, 2.29; 95% CI, 1.19-3.73; P = .0226).
Similarly, mercury, another substance found in products commonly used to bleach skin, has been associated with problems ranging from rashes to renal toxicity. And because it’s so incredibly harmful, mercury is also known to cause neurologic abnormalities.
Apart from causing certain conditions, prolonged use of skin-lightening products can change the way existing diseases present themselves as well as their severity, added Dr. Faye.
An increased risk
But what about skin bleaching’s link with cancer? “Skin cancer on Black skin is uncommon, yet it occurs in skin-bleaching women,” said Dr. Faye.
“Since 2000, we have had some cases of skin cancer associated with skin bleaching,” he continued, adding that squamous cell carcinoma (SCC) is the most frequent type of cancer observed.
If you look at what’s been published on the topic so far, you’ll see that “all the cases of skin cancer are located over the neck or some exposed area when skin bleaching products are used for more than 10 years,” said Dr. Faye. “And most of the time, the age of the patient ranges from 30 to 60 years.”
The first known case in Africa was reported in a 58-year-old woman from Ghana, who had been using skin bleaching products for close to 30 years. The patient presented with tumors on her face, neck, and arms.
Dr. Faye then proceeded to share more than 10 such carcinoma cases. “These previous reports strongly suggest a relationship between skin bleaching and skin cancers,” said Dr. Faye.
Indeed, there have been reports and publications in the literature that support his observation, including one last year, which found that use of the tyrosinase inhibitor hydroquinone was associated with approximately a threefold increased risk for skin cancer.
For some, including Brazil’s Dr. Lupi, Dr. Faye’s talk was enlightening: “I didn’t know about this relationship [of bleaching] with skin cancer, it was something new for me.”
But the prevalence of SCC is very low, compared with that of skin bleaching, Dr. Faye acknowledged. Moreover, the cancer observed in the cases reported could have resulted from a number of reasons, including exposure to harmful ultraviolet rays from the sun and genetic predisposition in addition to the use of bleaching products such as hydroquinone. “Other causes of skin cancer are not excluded,” he said.
To further explore the link between skin bleaching and cancer, “we need case-control studies to provide more evidence,” he added. Until then, dermatologists “should keep on promoting messages” to prevent SCC from occurring. This includes encouraging the use of proper sun protection in addition to discouraging the practice of skin bleaching, which still persists despite more than 10 African nations banning the use of toxic skin-lightening products.
Dr. Faye and Dr. Lupi report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT WCD 2023
FDA panel deems phenylephrine ineffective
The Nonprescription Drug Advisory Committee discussed the efficacy and pharmacokinetic data for phenylephrine. The committee’s next move is to determine if the drug’s status as Generally Recognized as Safe and Effective should be revoked. This would mean manufacturers would have to come up with new formulations, or products containing the drug would be removed from store shelves. NDAC did not disclose a timeline for assessing GRASE status.
The vote that formally declared phenylephrine ineffective was in line with a review of pharmacology and clinical data presented by the FDA on Sept. 11, which found that the oral bioavailability of the drug is less than 1%, compared with 38%, a number often cited in the literature and based on outdated technology.
A mechanism potentially responsible for inefficacy may be the half-life of phenylephrine.
“The half-life of the parent phenylephrine is much shorter than that of total phenylephrine, suggesting that the duration of action for active parent phenylephrine is far shorter than the monographed dosing interval of every 4 hours and is therefore open to question,” the review states.
The side effects of phenylephrine include headaches, insomnia, and nervousness. At higher doses, it can increase blood pressure.
The review also found that original studies used to support the efficacy of phenylephrine were inconclusive at best and contained potential methodological, statistical, and data integrity issues.
Pseudoephedrine is the only other nonprescription oral nasal decongestant on the retail market but is only available behind the counter due to its use as a potential narcotic.
Manufacturers have used phenylephrine instead of pseudoephedrine in many products due to this limitation.
Revoking the GRASE status of phenylephrine would leave patients without an over-the-counter option.
According to the FDA review, 242 million packages or bottles of phenylephrine products were sold in 2022, resulting in $1.76 billion in sales. A little over 50 million packages of pseudoephedrine were sold that same year, resulting in $542 million in sales.
“I think there’s a huge potential for consumer concern,” Diane B. Ginsburg, PhD, MS, RPh, the pharmacy practice division associate dean for Healthcare Partnerships at The University of Texas at Austin, said during the panel.
She said patients may be confused and concerned about the panel vote, especially those who feel they have benefitted from phenylephrine products. In the event of GRASE removal, she advised reassuring patients that phenylephrine is being pulled from shelves due to inefficacy rather than immediate health risks.
“The real positive here to me is the opportunity from an educational perspective to show consumers the fact that there are a lot more ways to treat” conditions that present with the symptom of congestion, such as rhinitis.
According to the FDA review, “most consumers may simply need instruction on the alternatives, including how to obtain ‘behind-the-counter’ pseudoephedrine or to use alternative treatments, including intranasal decongestants (including intranasal phenylephrine), intranasal steroids, intranasal antihistamines, or intranasal saline products.”
Despite these complications, “there are a number of potential benefits that would be derived by changing the GRASE status of oral phenylephrine.”
These include avoiding unnecessary costs of taking an ineffective drug, potential allergic reactions and side effects, and the risks of patients taking a higher dosage.
A version of this article appeared on Medscape.com.
The Nonprescription Drug Advisory Committee discussed the efficacy and pharmacokinetic data for phenylephrine. The committee’s next move is to determine if the drug’s status as Generally Recognized as Safe and Effective should be revoked. This would mean manufacturers would have to come up with new formulations, or products containing the drug would be removed from store shelves. NDAC did not disclose a timeline for assessing GRASE status.
The vote that formally declared phenylephrine ineffective was in line with a review of pharmacology and clinical data presented by the FDA on Sept. 11, which found that the oral bioavailability of the drug is less than 1%, compared with 38%, a number often cited in the literature and based on outdated technology.
A mechanism potentially responsible for inefficacy may be the half-life of phenylephrine.
“The half-life of the parent phenylephrine is much shorter than that of total phenylephrine, suggesting that the duration of action for active parent phenylephrine is far shorter than the monographed dosing interval of every 4 hours and is therefore open to question,” the review states.
The side effects of phenylephrine include headaches, insomnia, and nervousness. At higher doses, it can increase blood pressure.
The review also found that original studies used to support the efficacy of phenylephrine were inconclusive at best and contained potential methodological, statistical, and data integrity issues.
Pseudoephedrine is the only other nonprescription oral nasal decongestant on the retail market but is only available behind the counter due to its use as a potential narcotic.
Manufacturers have used phenylephrine instead of pseudoephedrine in many products due to this limitation.
Revoking the GRASE status of phenylephrine would leave patients without an over-the-counter option.
According to the FDA review, 242 million packages or bottles of phenylephrine products were sold in 2022, resulting in $1.76 billion in sales. A little over 50 million packages of pseudoephedrine were sold that same year, resulting in $542 million in sales.
“I think there’s a huge potential for consumer concern,” Diane B. Ginsburg, PhD, MS, RPh, the pharmacy practice division associate dean for Healthcare Partnerships at The University of Texas at Austin, said during the panel.
She said patients may be confused and concerned about the panel vote, especially those who feel they have benefitted from phenylephrine products. In the event of GRASE removal, she advised reassuring patients that phenylephrine is being pulled from shelves due to inefficacy rather than immediate health risks.
“The real positive here to me is the opportunity from an educational perspective to show consumers the fact that there are a lot more ways to treat” conditions that present with the symptom of congestion, such as rhinitis.
According to the FDA review, “most consumers may simply need instruction on the alternatives, including how to obtain ‘behind-the-counter’ pseudoephedrine or to use alternative treatments, including intranasal decongestants (including intranasal phenylephrine), intranasal steroids, intranasal antihistamines, or intranasal saline products.”
Despite these complications, “there are a number of potential benefits that would be derived by changing the GRASE status of oral phenylephrine.”
These include avoiding unnecessary costs of taking an ineffective drug, potential allergic reactions and side effects, and the risks of patients taking a higher dosage.
A version of this article appeared on Medscape.com.
The Nonprescription Drug Advisory Committee discussed the efficacy and pharmacokinetic data for phenylephrine. The committee’s next move is to determine if the drug’s status as Generally Recognized as Safe and Effective should be revoked. This would mean manufacturers would have to come up with new formulations, or products containing the drug would be removed from store shelves. NDAC did not disclose a timeline for assessing GRASE status.
The vote that formally declared phenylephrine ineffective was in line with a review of pharmacology and clinical data presented by the FDA on Sept. 11, which found that the oral bioavailability of the drug is less than 1%, compared with 38%, a number often cited in the literature and based on outdated technology.
A mechanism potentially responsible for inefficacy may be the half-life of phenylephrine.
“The half-life of the parent phenylephrine is much shorter than that of total phenylephrine, suggesting that the duration of action for active parent phenylephrine is far shorter than the monographed dosing interval of every 4 hours and is therefore open to question,” the review states.
The side effects of phenylephrine include headaches, insomnia, and nervousness. At higher doses, it can increase blood pressure.
The review also found that original studies used to support the efficacy of phenylephrine were inconclusive at best and contained potential methodological, statistical, and data integrity issues.
Pseudoephedrine is the only other nonprescription oral nasal decongestant on the retail market but is only available behind the counter due to its use as a potential narcotic.
Manufacturers have used phenylephrine instead of pseudoephedrine in many products due to this limitation.
Revoking the GRASE status of phenylephrine would leave patients without an over-the-counter option.
According to the FDA review, 242 million packages or bottles of phenylephrine products were sold in 2022, resulting in $1.76 billion in sales. A little over 50 million packages of pseudoephedrine were sold that same year, resulting in $542 million in sales.
“I think there’s a huge potential for consumer concern,” Diane B. Ginsburg, PhD, MS, RPh, the pharmacy practice division associate dean for Healthcare Partnerships at The University of Texas at Austin, said during the panel.
She said patients may be confused and concerned about the panel vote, especially those who feel they have benefitted from phenylephrine products. In the event of GRASE removal, she advised reassuring patients that phenylephrine is being pulled from shelves due to inefficacy rather than immediate health risks.
“The real positive here to me is the opportunity from an educational perspective to show consumers the fact that there are a lot more ways to treat” conditions that present with the symptom of congestion, such as rhinitis.
According to the FDA review, “most consumers may simply need instruction on the alternatives, including how to obtain ‘behind-the-counter’ pseudoephedrine or to use alternative treatments, including intranasal decongestants (including intranasal phenylephrine), intranasal steroids, intranasal antihistamines, or intranasal saline products.”
Despite these complications, “there are a number of potential benefits that would be derived by changing the GRASE status of oral phenylephrine.”
These include avoiding unnecessary costs of taking an ineffective drug, potential allergic reactions and side effects, and the risks of patients taking a higher dosage.
A version of this article appeared on Medscape.com.
Bad blood: Could brain bleeds be contagious?
This transcript has been edited for clarity.
How do you tell if a condition is caused by an infection?
It seems like an obvious question, right? In the post–van Leeuwenhoek era we can look at whatever part of the body is diseased under a microscope and see microbes – you know, the usual suspects.
Except when we can’t. And there are plenty of cases where we can’t: where the microbe is too small to be seen without more advanced imaging techniques, like with viruses; or when the pathogen is sparsely populated or hard to culture, like Mycobacterium.
Finding out that a condition is the result of an infection is not only an exercise for 19th century physicians. After all, it was 2008 when Barry Marshall and Robin Warren won their Nobel Prize for proving that stomach ulcers, long thought to be due to “stress,” were actually caused by a tiny microbe called Helicobacter pylori.
And this week, we are looking at a study which, once again, begins to suggest that a condition thought to be more or less random – cerebral amyloid angiopathy – may actually be the result of an infectious disease.
We’re talking about this paper, appearing in JAMA, which is just a great example of old-fashioned shoe-leather epidemiology. But let’s get up to speed on cerebral amyloid angiopathy (CAA) first.
CAA is characterized by the deposition of amyloid protein in the brain. While there are some genetic causes, they are quite rare, and most cases are thought to be idiopathic. Recent analyses suggest that somewhere between 5% and 7% of cognitively normal older adults have CAA, but the rate is much higher among those with intracerebral hemorrhage – brain bleeds. In fact, CAA is the second-most common cause of bleeding in the brain, second only to severe hypertension.
An article in Nature highlights cases that seemed to develop after the administration of cadaveric pituitary hormone.
Other studies have shown potential transmission via dura mater grafts and neurosurgical instruments. But despite those clues, no infectious organism has been identified. Some have suggested that the long latent period and difficulty of finding a responsible microbe points to a prion-like disease not yet known. But these studies are more or less case series. The new JAMA paper gives us, if not a smoking gun, a pretty decent set of fingerprints.
Here’s the idea: If CAA is caused by some infectious agent, it may be transmitted in the blood. We know that a decent percentage of people who have spontaneous brain bleeds have CAA. If those people donated blood in the past, maybe the people who received that blood would be at risk for brain bleeds too.
Of course, to really test that hypothesis, you’d need to know who every blood donor in a country was and every person who received that blood and all their subsequent diagnoses for basically their entire lives. No one has that kind of data, right?
Well, if you’ve been watching this space, you’ll know that a few countries do. Enter Sweden and Denmark, with their national electronic health record that captures all of this information, and much more, on every single person who lives or has lived in those countries since before 1970. Unbelievable.
So that’s exactly what the researchers, led by Jingchen Zhao at Karolinska (Sweden) University, did. They identified roughly 760,000 individuals in Sweden and 330,000 people in Denmark who had received a blood transfusion between 1970 and 2017.
Of course, most of those blood donors – 99% of them, actually – never went on to have any bleeding in the brain. It is a rare thing, fortunately.
But some of the donors did, on average within about 5 years of the time they donated blood. The researchers characterized each donor as either never having a brain bleed, having a single bleed, or having multiple bleeds. The latter is most strongly associated with CAA.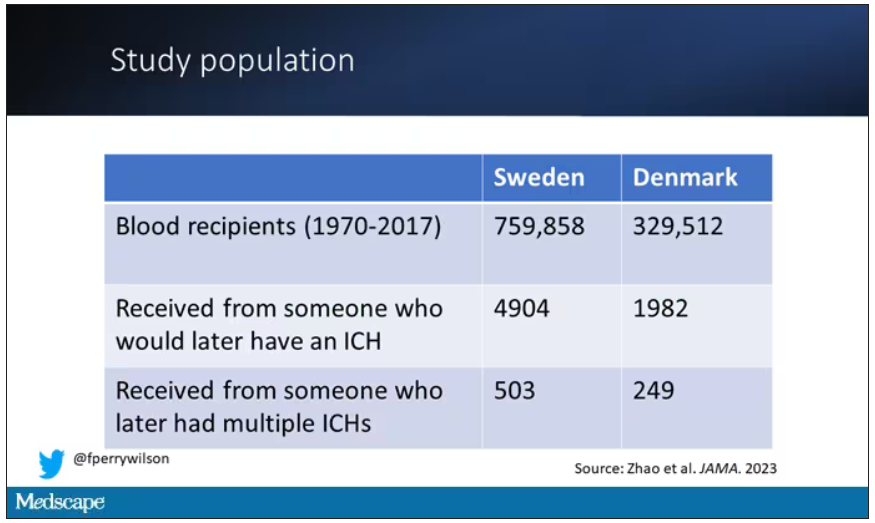
The big question: Would recipients who got blood from individuals who later on had brain bleeds, have brain bleeds themselves?
The answer is yes, though with an asterisk. You can see the results here. The risk of recipients having a brain bleed was lowest if the blood they received was from people who never had a brain bleed, higher if the individual had a single brain bleed, and highest if they got blood from a donor who would go on to have multiple brain bleeds.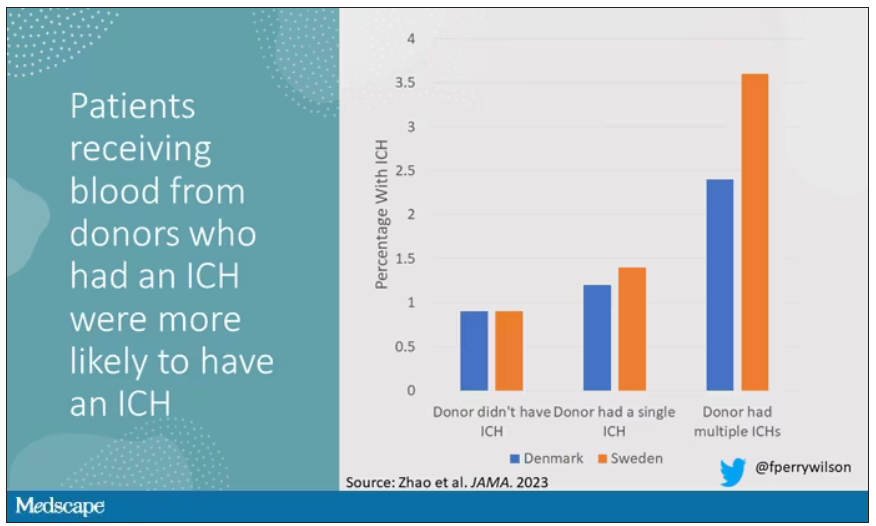
All in all, individuals who received blood from someone who would later have multiple hemorrhages were three times more likely to themselves develop bleeds themselves. It’s fairly compelling evidence of a transmissible agent.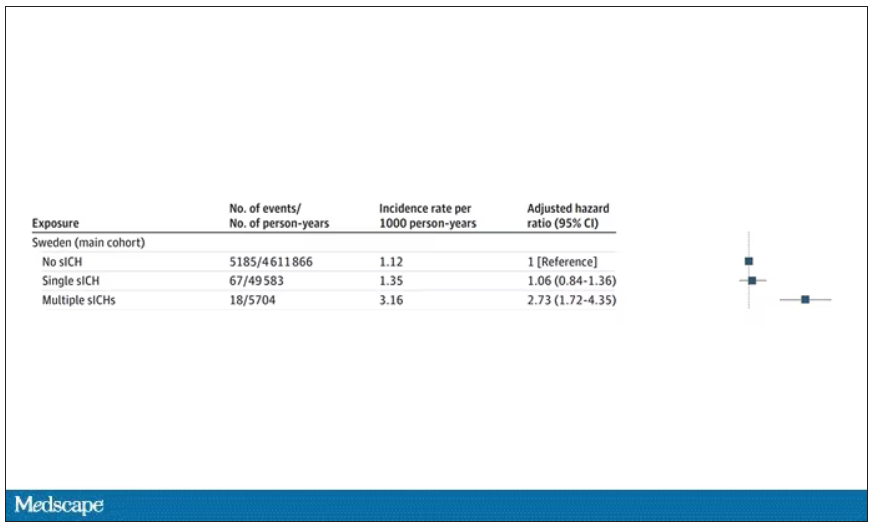
Of course, there are some potential confounders to consider here. Whose blood you get is not totally random. If, for example, people with type O blood are just more likely to have brain bleeds, then you could get results like this, as type O tends to donate to type O and both groups would have higher risk after donation. But the authors adjusted for blood type. They also adjusted for number of transfusions, calendar year, age, sex, and indication for transfusion.
Perhaps most compelling, and most clever, is that they used ischemic stroke as a negative control. Would people who received blood from someone who later had an ischemic stroke themselves be more likely to go on to have an ischemic stroke? No signal at all. It does not appear that there is a transmissible agent associated with ischemic stroke – only the brain bleeds.
I know what you’re thinking. What’s the agent? What’s the microbe, or virus, or prion, or toxin? The study gives us no insight there. These nationwide databases are awesome but they can only do so much. Because of the vagaries of medical coding and the difficulty of making the CAA diagnosis, the authors are using brain bleeds as a proxy here; we don’t even know for sure whether these were CAA-associated brain bleeds.
It’s also worth noting that there’s little we can do about this. None of the blood donors in this study had a brain bleed prior to donation; it’s not like we could screen people out of donating in the future. We have no test for whatever this agent is, if it even exists, nor do we have a potential treatment. Fortunately, whatever it is, it is extremely rare.
Still, this paper feels like a shot across the bow. At this point, the probability has shifted strongly away from CAA being a purely random disease and toward it being an infectious one. It may be time to round up some of the unusual suspects.
Dr. F. Perry Wilson is an associate professor of medicine and public health and director of Yale University’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
How do you tell if a condition is caused by an infection?
It seems like an obvious question, right? In the post–van Leeuwenhoek era we can look at whatever part of the body is diseased under a microscope and see microbes – you know, the usual suspects.
Except when we can’t. And there are plenty of cases where we can’t: where the microbe is too small to be seen without more advanced imaging techniques, like with viruses; or when the pathogen is sparsely populated or hard to culture, like Mycobacterium.
Finding out that a condition is the result of an infection is not only an exercise for 19th century physicians. After all, it was 2008 when Barry Marshall and Robin Warren won their Nobel Prize for proving that stomach ulcers, long thought to be due to “stress,” were actually caused by a tiny microbe called Helicobacter pylori.
And this week, we are looking at a study which, once again, begins to suggest that a condition thought to be more or less random – cerebral amyloid angiopathy – may actually be the result of an infectious disease.
We’re talking about this paper, appearing in JAMA, which is just a great example of old-fashioned shoe-leather epidemiology. But let’s get up to speed on cerebral amyloid angiopathy (CAA) first.
CAA is characterized by the deposition of amyloid protein in the brain. While there are some genetic causes, they are quite rare, and most cases are thought to be idiopathic. Recent analyses suggest that somewhere between 5% and 7% of cognitively normal older adults have CAA, but the rate is much higher among those with intracerebral hemorrhage – brain bleeds. In fact, CAA is the second-most common cause of bleeding in the brain, second only to severe hypertension.
An article in Nature highlights cases that seemed to develop after the administration of cadaveric pituitary hormone.
Other studies have shown potential transmission via dura mater grafts and neurosurgical instruments. But despite those clues, no infectious organism has been identified. Some have suggested that the long latent period and difficulty of finding a responsible microbe points to a prion-like disease not yet known. But these studies are more or less case series. The new JAMA paper gives us, if not a smoking gun, a pretty decent set of fingerprints.
Here’s the idea: If CAA is caused by some infectious agent, it may be transmitted in the blood. We know that a decent percentage of people who have spontaneous brain bleeds have CAA. If those people donated blood in the past, maybe the people who received that blood would be at risk for brain bleeds too.
Of course, to really test that hypothesis, you’d need to know who every blood donor in a country was and every person who received that blood and all their subsequent diagnoses for basically their entire lives. No one has that kind of data, right?
Well, if you’ve been watching this space, you’ll know that a few countries do. Enter Sweden and Denmark, with their national electronic health record that captures all of this information, and much more, on every single person who lives or has lived in those countries since before 1970. Unbelievable.
So that’s exactly what the researchers, led by Jingchen Zhao at Karolinska (Sweden) University, did. They identified roughly 760,000 individuals in Sweden and 330,000 people in Denmark who had received a blood transfusion between 1970 and 2017.
Of course, most of those blood donors – 99% of them, actually – never went on to have any bleeding in the brain. It is a rare thing, fortunately.
But some of the donors did, on average within about 5 years of the time they donated blood. The researchers characterized each donor as either never having a brain bleed, having a single bleed, or having multiple bleeds. The latter is most strongly associated with CAA.
The big question: Would recipients who got blood from individuals who later on had brain bleeds, have brain bleeds themselves?
The answer is yes, though with an asterisk. You can see the results here. The risk of recipients having a brain bleed was lowest if the blood they received was from people who never had a brain bleed, higher if the individual had a single brain bleed, and highest if they got blood from a donor who would go on to have multiple brain bleeds.
All in all, individuals who received blood from someone who would later have multiple hemorrhages were three times more likely to themselves develop bleeds themselves. It’s fairly compelling evidence of a transmissible agent.
Of course, there are some potential confounders to consider here. Whose blood you get is not totally random. If, for example, people with type O blood are just more likely to have brain bleeds, then you could get results like this, as type O tends to donate to type O and both groups would have higher risk after donation. But the authors adjusted for blood type. They also adjusted for number of transfusions, calendar year, age, sex, and indication for transfusion.
Perhaps most compelling, and most clever, is that they used ischemic stroke as a negative control. Would people who received blood from someone who later had an ischemic stroke themselves be more likely to go on to have an ischemic stroke? No signal at all. It does not appear that there is a transmissible agent associated with ischemic stroke – only the brain bleeds.
I know what you’re thinking. What’s the agent? What’s the microbe, or virus, or prion, or toxin? The study gives us no insight there. These nationwide databases are awesome but they can only do so much. Because of the vagaries of medical coding and the difficulty of making the CAA diagnosis, the authors are using brain bleeds as a proxy here; we don’t even know for sure whether these were CAA-associated brain bleeds.
It’s also worth noting that there’s little we can do about this. None of the blood donors in this study had a brain bleed prior to donation; it’s not like we could screen people out of donating in the future. We have no test for whatever this agent is, if it even exists, nor do we have a potential treatment. Fortunately, whatever it is, it is extremely rare.
Still, this paper feels like a shot across the bow. At this point, the probability has shifted strongly away from CAA being a purely random disease and toward it being an infectious one. It may be time to round up some of the unusual suspects.
Dr. F. Perry Wilson is an associate professor of medicine and public health and director of Yale University’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
How do you tell if a condition is caused by an infection?
It seems like an obvious question, right? In the post–van Leeuwenhoek era we can look at whatever part of the body is diseased under a microscope and see microbes – you know, the usual suspects.
Except when we can’t. And there are plenty of cases where we can’t: where the microbe is too small to be seen without more advanced imaging techniques, like with viruses; or when the pathogen is sparsely populated or hard to culture, like Mycobacterium.
Finding out that a condition is the result of an infection is not only an exercise for 19th century physicians. After all, it was 2008 when Barry Marshall and Robin Warren won their Nobel Prize for proving that stomach ulcers, long thought to be due to “stress,” were actually caused by a tiny microbe called Helicobacter pylori.
And this week, we are looking at a study which, once again, begins to suggest that a condition thought to be more or less random – cerebral amyloid angiopathy – may actually be the result of an infectious disease.
We’re talking about this paper, appearing in JAMA, which is just a great example of old-fashioned shoe-leather epidemiology. But let’s get up to speed on cerebral amyloid angiopathy (CAA) first.
CAA is characterized by the deposition of amyloid protein in the brain. While there are some genetic causes, they are quite rare, and most cases are thought to be idiopathic. Recent analyses suggest that somewhere between 5% and 7% of cognitively normal older adults have CAA, but the rate is much higher among those with intracerebral hemorrhage – brain bleeds. In fact, CAA is the second-most common cause of bleeding in the brain, second only to severe hypertension.
An article in Nature highlights cases that seemed to develop after the administration of cadaveric pituitary hormone.
Other studies have shown potential transmission via dura mater grafts and neurosurgical instruments. But despite those clues, no infectious organism has been identified. Some have suggested that the long latent period and difficulty of finding a responsible microbe points to a prion-like disease not yet known. But these studies are more or less case series. The new JAMA paper gives us, if not a smoking gun, a pretty decent set of fingerprints.
Here’s the idea: If CAA is caused by some infectious agent, it may be transmitted in the blood. We know that a decent percentage of people who have spontaneous brain bleeds have CAA. If those people donated blood in the past, maybe the people who received that blood would be at risk for brain bleeds too.
Of course, to really test that hypothesis, you’d need to know who every blood donor in a country was and every person who received that blood and all their subsequent diagnoses for basically their entire lives. No one has that kind of data, right?
Well, if you’ve been watching this space, you’ll know that a few countries do. Enter Sweden and Denmark, with their national electronic health record that captures all of this information, and much more, on every single person who lives or has lived in those countries since before 1970. Unbelievable.
So that’s exactly what the researchers, led by Jingchen Zhao at Karolinska (Sweden) University, did. They identified roughly 760,000 individuals in Sweden and 330,000 people in Denmark who had received a blood transfusion between 1970 and 2017.
Of course, most of those blood donors – 99% of them, actually – never went on to have any bleeding in the brain. It is a rare thing, fortunately.
But some of the donors did, on average within about 5 years of the time they donated blood. The researchers characterized each donor as either never having a brain bleed, having a single bleed, or having multiple bleeds. The latter is most strongly associated with CAA.
The big question: Would recipients who got blood from individuals who later on had brain bleeds, have brain bleeds themselves?
The answer is yes, though with an asterisk. You can see the results here. The risk of recipients having a brain bleed was lowest if the blood they received was from people who never had a brain bleed, higher if the individual had a single brain bleed, and highest if they got blood from a donor who would go on to have multiple brain bleeds.
All in all, individuals who received blood from someone who would later have multiple hemorrhages were three times more likely to themselves develop bleeds themselves. It’s fairly compelling evidence of a transmissible agent.
Of course, there are some potential confounders to consider here. Whose blood you get is not totally random. If, for example, people with type O blood are just more likely to have brain bleeds, then you could get results like this, as type O tends to donate to type O and both groups would have higher risk after donation. But the authors adjusted for blood type. They also adjusted for number of transfusions, calendar year, age, sex, and indication for transfusion.
Perhaps most compelling, and most clever, is that they used ischemic stroke as a negative control. Would people who received blood from someone who later had an ischemic stroke themselves be more likely to go on to have an ischemic stroke? No signal at all. It does not appear that there is a transmissible agent associated with ischemic stroke – only the brain bleeds.
I know what you’re thinking. What’s the agent? What’s the microbe, or virus, or prion, or toxin? The study gives us no insight there. These nationwide databases are awesome but they can only do so much. Because of the vagaries of medical coding and the difficulty of making the CAA diagnosis, the authors are using brain bleeds as a proxy here; we don’t even know for sure whether these were CAA-associated brain bleeds.
It’s also worth noting that there’s little we can do about this. None of the blood donors in this study had a brain bleed prior to donation; it’s not like we could screen people out of donating in the future. We have no test for whatever this agent is, if it even exists, nor do we have a potential treatment. Fortunately, whatever it is, it is extremely rare.
Still, this paper feels like a shot across the bow. At this point, the probability has shifted strongly away from CAA being a purely random disease and toward it being an infectious one. It may be time to round up some of the unusual suspects.
Dr. F. Perry Wilson is an associate professor of medicine and public health and director of Yale University’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Stress, insomnia tied to increased AFib risk for older women
TOPLINE:
Eight psychosocial factors, grouped into two distinct clusters, are significantly associated with risk for atrial fibrillation in postmenopausal women, with insomnia and stressful life events (SLEs) being the most strongly associated with AFib, a large new study has found.
METHODOLOGY:
- In addition to traditional risk factors such as obesity, advanced age, ethnicity, smoking, alcohol, hypertension, diabetes, coronary artery disease, heart failure, and emotional and psychological distress may also affect AFib.
- The study included 83,736 postmenopausal women in the Women’s Health Initiative (mean age, 63.9 years; 88.1% White) who did not have AFib at baseline.
- From questionnaires, researchers collected information on psychosocial stressors and used hierarchical cluster analysis to identify patterns of psychosocial predictors.
- They separated these clusters into quartiles, identified associations between psychosocial exposure variables, and adjusted for traditional risk factors.
- Over an average follow-up of 10.5 years, 23,954 participants (28.6%) developed incident AFib.
TAKEAWAY:
- The analysis generated two clusters of distinct psychosocial variables that were significantly associated with AFib: the Stress Cluster, including SLEs, depressive symptoms, and insomnia; and the Strain Cluster, including three personality traits: optimism, cynical hostility, and emotional expressiveness; and two social measures: social support, and social strain.
- Those in the highest quartiles of both the Stress Cluster and the Strain Cluster had greater rates of AFib, compared with those in the lowest quartiles.
- In a final model, the association between SLEs (hazard ratio, 1.02; 95% confidence interval, 1.01-1.04) and insomnia (HR, 1.04; 95% CI, 1.03-1.06) were most strongly linked to increased incidence of AFib, and a sensitivity analysis using snoring as a surrogate marker for sleep apnea didn’t change this outcome, supporting the independent effect of insomnia on AFib.
- In subgroup analyses, the Stress Cluster had a stronger association with AFib incidence in younger (50-69 years) versus older women (70-79 years), and in non-Hispanic White and Asian women versus Hispanic and non-Hispanic Black women.
IN PRACTICE:
The results support the hypothesis that psychosocial predictors account for additional risk for AFib “above and beyond” traditional risk factors, the authors wrote. Identifying and addressing sex-specific, modifiable risk factors, including insomnia, “may help reduce the burden of AF[ib] in aging women.”
SOURCE:
The study was conducted by Susan X. Zhao, MD, division of cardiology, department of medicine, Santa Clara Valley Medical Center, San Jose, Calif., and colleagues. It was published online in the Journal of the American Heart Association.
LIMITATIONS:
The psychometric questionnaires were administered only at study entry, but psychosocial variables may change over time. Data on sleep apnea and other sleep disorders, which may confound the relationship between insomnia and AFib, were not available, and although the study included a sensitivity analysis controlling for snoring, this is an imperfect surrogate for sleep apnea. Generalizability to other demographic, racial, and ethnic groups is limited.
DISCLOSURES:
The Women’s Health Initiative program is funded by the National Heart, Lung, and Blood Institute; National Institutes of Health; and the Department of Health & Human Services. The authors have no relevant conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
Eight psychosocial factors, grouped into two distinct clusters, are significantly associated with risk for atrial fibrillation in postmenopausal women, with insomnia and stressful life events (SLEs) being the most strongly associated with AFib, a large new study has found.
METHODOLOGY:
- In addition to traditional risk factors such as obesity, advanced age, ethnicity, smoking, alcohol, hypertension, diabetes, coronary artery disease, heart failure, and emotional and psychological distress may also affect AFib.
- The study included 83,736 postmenopausal women in the Women’s Health Initiative (mean age, 63.9 years; 88.1% White) who did not have AFib at baseline.
- From questionnaires, researchers collected information on psychosocial stressors and used hierarchical cluster analysis to identify patterns of psychosocial predictors.
- They separated these clusters into quartiles, identified associations between psychosocial exposure variables, and adjusted for traditional risk factors.
- Over an average follow-up of 10.5 years, 23,954 participants (28.6%) developed incident AFib.
TAKEAWAY:
- The analysis generated two clusters of distinct psychosocial variables that were significantly associated with AFib: the Stress Cluster, including SLEs, depressive symptoms, and insomnia; and the Strain Cluster, including three personality traits: optimism, cynical hostility, and emotional expressiveness; and two social measures: social support, and social strain.
- Those in the highest quartiles of both the Stress Cluster and the Strain Cluster had greater rates of AFib, compared with those in the lowest quartiles.
- In a final model, the association between SLEs (hazard ratio, 1.02; 95% confidence interval, 1.01-1.04) and insomnia (HR, 1.04; 95% CI, 1.03-1.06) were most strongly linked to increased incidence of AFib, and a sensitivity analysis using snoring as a surrogate marker for sleep apnea didn’t change this outcome, supporting the independent effect of insomnia on AFib.
- In subgroup analyses, the Stress Cluster had a stronger association with AFib incidence in younger (50-69 years) versus older women (70-79 years), and in non-Hispanic White and Asian women versus Hispanic and non-Hispanic Black women.
IN PRACTICE:
The results support the hypothesis that psychosocial predictors account for additional risk for AFib “above and beyond” traditional risk factors, the authors wrote. Identifying and addressing sex-specific, modifiable risk factors, including insomnia, “may help reduce the burden of AF[ib] in aging women.”
SOURCE:
The study was conducted by Susan X. Zhao, MD, division of cardiology, department of medicine, Santa Clara Valley Medical Center, San Jose, Calif., and colleagues. It was published online in the Journal of the American Heart Association.
LIMITATIONS:
The psychometric questionnaires were administered only at study entry, but psychosocial variables may change over time. Data on sleep apnea and other sleep disorders, which may confound the relationship between insomnia and AFib, were not available, and although the study included a sensitivity analysis controlling for snoring, this is an imperfect surrogate for sleep apnea. Generalizability to other demographic, racial, and ethnic groups is limited.
DISCLOSURES:
The Women’s Health Initiative program is funded by the National Heart, Lung, and Blood Institute; National Institutes of Health; and the Department of Health & Human Services. The authors have no relevant conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
Eight psychosocial factors, grouped into two distinct clusters, are significantly associated with risk for atrial fibrillation in postmenopausal women, with insomnia and stressful life events (SLEs) being the most strongly associated with AFib, a large new study has found.
METHODOLOGY:
- In addition to traditional risk factors such as obesity, advanced age, ethnicity, smoking, alcohol, hypertension, diabetes, coronary artery disease, heart failure, and emotional and psychological distress may also affect AFib.
- The study included 83,736 postmenopausal women in the Women’s Health Initiative (mean age, 63.9 years; 88.1% White) who did not have AFib at baseline.
- From questionnaires, researchers collected information on psychosocial stressors and used hierarchical cluster analysis to identify patterns of psychosocial predictors.
- They separated these clusters into quartiles, identified associations between psychosocial exposure variables, and adjusted for traditional risk factors.
- Over an average follow-up of 10.5 years, 23,954 participants (28.6%) developed incident AFib.
TAKEAWAY:
- The analysis generated two clusters of distinct psychosocial variables that were significantly associated with AFib: the Stress Cluster, including SLEs, depressive symptoms, and insomnia; and the Strain Cluster, including three personality traits: optimism, cynical hostility, and emotional expressiveness; and two social measures: social support, and social strain.
- Those in the highest quartiles of both the Stress Cluster and the Strain Cluster had greater rates of AFib, compared with those in the lowest quartiles.
- In a final model, the association between SLEs (hazard ratio, 1.02; 95% confidence interval, 1.01-1.04) and insomnia (HR, 1.04; 95% CI, 1.03-1.06) were most strongly linked to increased incidence of AFib, and a sensitivity analysis using snoring as a surrogate marker for sleep apnea didn’t change this outcome, supporting the independent effect of insomnia on AFib.
- In subgroup analyses, the Stress Cluster had a stronger association with AFib incidence in younger (50-69 years) versus older women (70-79 years), and in non-Hispanic White and Asian women versus Hispanic and non-Hispanic Black women.
IN PRACTICE:
The results support the hypothesis that psychosocial predictors account for additional risk for AFib “above and beyond” traditional risk factors, the authors wrote. Identifying and addressing sex-specific, modifiable risk factors, including insomnia, “may help reduce the burden of AF[ib] in aging women.”
SOURCE:
The study was conducted by Susan X. Zhao, MD, division of cardiology, department of medicine, Santa Clara Valley Medical Center, San Jose, Calif., and colleagues. It was published online in the Journal of the American Heart Association.
LIMITATIONS:
The psychometric questionnaires were administered only at study entry, but psychosocial variables may change over time. Data on sleep apnea and other sleep disorders, which may confound the relationship between insomnia and AFib, were not available, and although the study included a sensitivity analysis controlling for snoring, this is an imperfect surrogate for sleep apnea. Generalizability to other demographic, racial, and ethnic groups is limited.
DISCLOSURES:
The Women’s Health Initiative program is funded by the National Heart, Lung, and Blood Institute; National Institutes of Health; and the Department of Health & Human Services. The authors have no relevant conflicts of interest.
A version of this article appeared on Medscape.com.
FROM JOURNAL OF THE AMERICAN HEART ASSOCIATION