User login
For MD-IQ use only
Hospital patient catches on fire, highlighting need for prevention
On Thanksgiving Day 2022, Kathy Stark watched as her husband of 35 years, Bobby Ray Stark, caught fire at a Nashville hospital. According to Clint Kelly, Kathy Stark’s attorney, the hospital staff was performing cardioversion to restore Bobby Ray’s heart rhythm when a spark ignited the oxygen and set the patient aflame.
Mr. Stark, 64, died of “a combination of cardiovascular disease and thermal burns,” according to a local news report. In May, Kathy Stark filed a malpractice lawsuit in U.S. District Court. Mr. Kelly hopes that the lawsuit will help improve patient safety. Meanwhile, Kathy Stark “goes to bed at night and sees her husband on fire,” Mr. Kelly says. A similar incident occurred last December in the operating room at Oregon Health & Science University, resulting in minor injuries to a patient.
Underreported, but likely dropping
Reliable data on the incidence of surgical fires is lacking because incidents may go unreported over litigation fears, says Jeffrey Feldman, MD, MSE, anesthesiologist at Children’s Hospital of Philadelphia and chair of the Anesthesia Patient Safety Foundation’s Committee on Technology.
The Pennsylvania Patient Safety Authority has been tracking surgical fires for decades, however, and experts have used the agency’s data to extrapolate how often they occur in the United States.
In 2005, nationwide incidence was estimated to be somewhere in the neighborhood of 550-600 fires annually, says Barbara G. Malanga, acting director of health care incident investigation and technology consulting at ECRI (formerly the Emergency Care Research Institute). By 2011, that number appeared to have dropped to 200-240 incidents per year.
A similar analysis in 2018 found the incidence may now be as low as 88-105 a year. The drop is likely a result of increased awareness because of educational efforts on the part of the ECRI and the APSF, including a widely disseminated video on fire safety.
The decline of surgical fires “sounds great,” says Dr. Feldman, “except that it’s a 100% preventable complication, and they’re still happening.”
Accidents waiting to happen
How do these fires happen? It comes down to the ‘fire triangle’ often taught in grade school. Fire requires three things: an ignition source, fuel, and oxygen or an oxidizing agent. Ignition sources are plentiful in a surgical suite, including any of a variety of electrical devices commonly used in surgical procedures, including defibrillators. Gowns, gauze, drapes, sponges, oxygen masks, nasal cannulae, a patient’s hair or their clothing – all provide the necessary fuel.
But the key factor for surgical fire risk is the presence of high concentrations of oxygen.
Safety protocols
The best and most obvious way to mitigate risk is to reduce the amount of supplemental oxygen, explains Dr. Feldman.
“Many patients do not require a high concentration of oxygen during sedation,” he says.
When a patient does require a higher concentration for their safety, the APSF and ECRI recommend placing an endotracheal tube or supraglottic airway rather than using an oxygen mask or a nasal cannula. “You want to deliver the oxygen in such a way that high concentration doesn’t exist in the surgical field,” Dr. Feldman says. In cases where supplemental oxygen is necessary, ECRI and APSF recommend reducing the oxygen concentration to less than 30%.
In addition, safety protocols include giving flammable prep solutions time to dry before applying towels or drapes and beginning the procedure. These precautions to ensure the safety of patients take just a moment, says Chester H. Lake Jr, MD, MS, of the department of anesthesiology at the University of Mississippi Medical Center, Jackson.
Making fire safety part of the preop routine
These safety protocols are straightforward but not always observed, experts say. Part of the reason is a matter of culture. Both anesthesiologists and surgeons have absorbed the attitude that placing an airway escalates the procedure beyond what the patient needs, says Dr. Feldman. And indeed, according to a 2013 analysis of the American Society of Anesthesiologists closed claims database, 85% of surgical fires occur in outpatient settings where airways are less likely to be placed, and 81% of those claims were for procedures that used monitored anesthesia care.
In an article on prevention of surgical fires, Dr. Lake and colleagues recommend in-house education on preventing and responding to fires at least once a year. But it shouldn’t stop there. Because these fires – horrific as they are – are fairly rare, it’s important to maintain awareness. Making fire safety a regular part of the surgical “time-out” can help further reduce incidents, he says. ECRI and the APSF have teamed up to create a poster that can help surgical teams make fire safety a regular part of their routines.
Although the national decline in surgical fires is encouraging, the problem remains serious. “You can classify these incidents as low, but it’s not low if it happens to you or a family member,” says Dr. Lake. “One is too many.”
ECRI’s Ms. Malanga agrees. “I do like to emphasize that it’s rare,” she says. “But I’d like to see us reduce this until it’s zero.”
A version of this article originally appeared on Medscape.com.
On Thanksgiving Day 2022, Kathy Stark watched as her husband of 35 years, Bobby Ray Stark, caught fire at a Nashville hospital. According to Clint Kelly, Kathy Stark’s attorney, the hospital staff was performing cardioversion to restore Bobby Ray’s heart rhythm when a spark ignited the oxygen and set the patient aflame.
Mr. Stark, 64, died of “a combination of cardiovascular disease and thermal burns,” according to a local news report. In May, Kathy Stark filed a malpractice lawsuit in U.S. District Court. Mr. Kelly hopes that the lawsuit will help improve patient safety. Meanwhile, Kathy Stark “goes to bed at night and sees her husband on fire,” Mr. Kelly says. A similar incident occurred last December in the operating room at Oregon Health & Science University, resulting in minor injuries to a patient.
Underreported, but likely dropping
Reliable data on the incidence of surgical fires is lacking because incidents may go unreported over litigation fears, says Jeffrey Feldman, MD, MSE, anesthesiologist at Children’s Hospital of Philadelphia and chair of the Anesthesia Patient Safety Foundation’s Committee on Technology.
The Pennsylvania Patient Safety Authority has been tracking surgical fires for decades, however, and experts have used the agency’s data to extrapolate how often they occur in the United States.
In 2005, nationwide incidence was estimated to be somewhere in the neighborhood of 550-600 fires annually, says Barbara G. Malanga, acting director of health care incident investigation and technology consulting at ECRI (formerly the Emergency Care Research Institute). By 2011, that number appeared to have dropped to 200-240 incidents per year.
A similar analysis in 2018 found the incidence may now be as low as 88-105 a year. The drop is likely a result of increased awareness because of educational efforts on the part of the ECRI and the APSF, including a widely disseminated video on fire safety.
The decline of surgical fires “sounds great,” says Dr. Feldman, “except that it’s a 100% preventable complication, and they’re still happening.”
Accidents waiting to happen
How do these fires happen? It comes down to the ‘fire triangle’ often taught in grade school. Fire requires three things: an ignition source, fuel, and oxygen or an oxidizing agent. Ignition sources are plentiful in a surgical suite, including any of a variety of electrical devices commonly used in surgical procedures, including defibrillators. Gowns, gauze, drapes, sponges, oxygen masks, nasal cannulae, a patient’s hair or their clothing – all provide the necessary fuel.
But the key factor for surgical fire risk is the presence of high concentrations of oxygen.
Safety protocols
The best and most obvious way to mitigate risk is to reduce the amount of supplemental oxygen, explains Dr. Feldman.
“Many patients do not require a high concentration of oxygen during sedation,” he says.
When a patient does require a higher concentration for their safety, the APSF and ECRI recommend placing an endotracheal tube or supraglottic airway rather than using an oxygen mask or a nasal cannula. “You want to deliver the oxygen in such a way that high concentration doesn’t exist in the surgical field,” Dr. Feldman says. In cases where supplemental oxygen is necessary, ECRI and APSF recommend reducing the oxygen concentration to less than 30%.
In addition, safety protocols include giving flammable prep solutions time to dry before applying towels or drapes and beginning the procedure. These precautions to ensure the safety of patients take just a moment, says Chester H. Lake Jr, MD, MS, of the department of anesthesiology at the University of Mississippi Medical Center, Jackson.
Making fire safety part of the preop routine
These safety protocols are straightforward but not always observed, experts say. Part of the reason is a matter of culture. Both anesthesiologists and surgeons have absorbed the attitude that placing an airway escalates the procedure beyond what the patient needs, says Dr. Feldman. And indeed, according to a 2013 analysis of the American Society of Anesthesiologists closed claims database, 85% of surgical fires occur in outpatient settings where airways are less likely to be placed, and 81% of those claims were for procedures that used monitored anesthesia care.
In an article on prevention of surgical fires, Dr. Lake and colleagues recommend in-house education on preventing and responding to fires at least once a year. But it shouldn’t stop there. Because these fires – horrific as they are – are fairly rare, it’s important to maintain awareness. Making fire safety a regular part of the surgical “time-out” can help further reduce incidents, he says. ECRI and the APSF have teamed up to create a poster that can help surgical teams make fire safety a regular part of their routines.
Although the national decline in surgical fires is encouraging, the problem remains serious. “You can classify these incidents as low, but it’s not low if it happens to you or a family member,” says Dr. Lake. “One is too many.”
ECRI’s Ms. Malanga agrees. “I do like to emphasize that it’s rare,” she says. “But I’d like to see us reduce this until it’s zero.”
A version of this article originally appeared on Medscape.com.
On Thanksgiving Day 2022, Kathy Stark watched as her husband of 35 years, Bobby Ray Stark, caught fire at a Nashville hospital. According to Clint Kelly, Kathy Stark’s attorney, the hospital staff was performing cardioversion to restore Bobby Ray’s heart rhythm when a spark ignited the oxygen and set the patient aflame.
Mr. Stark, 64, died of “a combination of cardiovascular disease and thermal burns,” according to a local news report. In May, Kathy Stark filed a malpractice lawsuit in U.S. District Court. Mr. Kelly hopes that the lawsuit will help improve patient safety. Meanwhile, Kathy Stark “goes to bed at night and sees her husband on fire,” Mr. Kelly says. A similar incident occurred last December in the operating room at Oregon Health & Science University, resulting in minor injuries to a patient.
Underreported, but likely dropping
Reliable data on the incidence of surgical fires is lacking because incidents may go unreported over litigation fears, says Jeffrey Feldman, MD, MSE, anesthesiologist at Children’s Hospital of Philadelphia and chair of the Anesthesia Patient Safety Foundation’s Committee on Technology.
The Pennsylvania Patient Safety Authority has been tracking surgical fires for decades, however, and experts have used the agency’s data to extrapolate how often they occur in the United States.
In 2005, nationwide incidence was estimated to be somewhere in the neighborhood of 550-600 fires annually, says Barbara G. Malanga, acting director of health care incident investigation and technology consulting at ECRI (formerly the Emergency Care Research Institute). By 2011, that number appeared to have dropped to 200-240 incidents per year.
A similar analysis in 2018 found the incidence may now be as low as 88-105 a year. The drop is likely a result of increased awareness because of educational efforts on the part of the ECRI and the APSF, including a widely disseminated video on fire safety.
The decline of surgical fires “sounds great,” says Dr. Feldman, “except that it’s a 100% preventable complication, and they’re still happening.”
Accidents waiting to happen
How do these fires happen? It comes down to the ‘fire triangle’ often taught in grade school. Fire requires three things: an ignition source, fuel, and oxygen or an oxidizing agent. Ignition sources are plentiful in a surgical suite, including any of a variety of electrical devices commonly used in surgical procedures, including defibrillators. Gowns, gauze, drapes, sponges, oxygen masks, nasal cannulae, a patient’s hair or their clothing – all provide the necessary fuel.
But the key factor for surgical fire risk is the presence of high concentrations of oxygen.
Safety protocols
The best and most obvious way to mitigate risk is to reduce the amount of supplemental oxygen, explains Dr. Feldman.
“Many patients do not require a high concentration of oxygen during sedation,” he says.
When a patient does require a higher concentration for their safety, the APSF and ECRI recommend placing an endotracheal tube or supraglottic airway rather than using an oxygen mask or a nasal cannula. “You want to deliver the oxygen in such a way that high concentration doesn’t exist in the surgical field,” Dr. Feldman says. In cases where supplemental oxygen is necessary, ECRI and APSF recommend reducing the oxygen concentration to less than 30%.
In addition, safety protocols include giving flammable prep solutions time to dry before applying towels or drapes and beginning the procedure. These precautions to ensure the safety of patients take just a moment, says Chester H. Lake Jr, MD, MS, of the department of anesthesiology at the University of Mississippi Medical Center, Jackson.
Making fire safety part of the preop routine
These safety protocols are straightforward but not always observed, experts say. Part of the reason is a matter of culture. Both anesthesiologists and surgeons have absorbed the attitude that placing an airway escalates the procedure beyond what the patient needs, says Dr. Feldman. And indeed, according to a 2013 analysis of the American Society of Anesthesiologists closed claims database, 85% of surgical fires occur in outpatient settings where airways are less likely to be placed, and 81% of those claims were for procedures that used monitored anesthesia care.
In an article on prevention of surgical fires, Dr. Lake and colleagues recommend in-house education on preventing and responding to fires at least once a year. But it shouldn’t stop there. Because these fires – horrific as they are – are fairly rare, it’s important to maintain awareness. Making fire safety a regular part of the surgical “time-out” can help further reduce incidents, he says. ECRI and the APSF have teamed up to create a poster that can help surgical teams make fire safety a regular part of their routines.
Although the national decline in surgical fires is encouraging, the problem remains serious. “You can classify these incidents as low, but it’s not low if it happens to you or a family member,” says Dr. Lake. “One is too many.”
ECRI’s Ms. Malanga agrees. “I do like to emphasize that it’s rare,” she says. “But I’d like to see us reduce this until it’s zero.”
A version of this article originally appeared on Medscape.com.
Dramatic rise in hallucinogen use among young adults
With the exception of lysergic acid diethylamide,
In 2018, the prevalence of young adults’ past-year use of non-LSD hallucinogens was 3.4%. By 2021, it had jumped to 6.6%.
The increase in non-LSD hallucinogen use occurred while LSD use remained stable at around 4% in 2018 and 2021.
“While non-LSD hallucinogen use remains substantially less prevalent than use of substances such as alcohol and cannabis, a doubling of prevalence in just three years is a dramatic increase and raises possible public health concerns,” co-author Megan Patrick, PhD, with the University of Michigan Institute for Social Research, Ann Arbor, said in a news release.
The results were published online in the journal Addiction.
Health concerns
The estimates are derived from the Monitoring the Future study, which includes annual assessments of adolescent and adult health in the United States.
The analysis focused on 11,304 persons (52% female) aged 9-30 years from the U.S. general population who were interviewed between 2018 and 2021.
Participants were asked about past 12-month use of LSD, as well as use of non-LSD hallucinogens, such as psilocybin.
From 2018 to 2021, past 12-month use of LSD remained relatively stable; it was 3.7% in 2018 and 4.2% in 2021.
However, non-LSD hallucinogen use increased in prevalence from 3.4% to 6.6% from 2018 to 2021.
Across years, the odds of non-LSD use were higher among males, White people, and individuals from households with higher parental education – a proxy for higher socioeconomic status.
The most commonly used non-LSD hallucinogen was psilocybin.
The survey did not ask whether young adults used non-LSD hallucinogens for therapeutic or medical reasons.
“The use of psychedelic and hallucinogenic drugs for a range of therapeutic uses is increasing, given accumulating yet still preliminary data from randomized trials on clinical effectiveness,” lead author Katherine Keyes, PhD, with Columbia University Mailman School of Public Health, New York, said in the release.
“With increased visibility for medical and therapeutic use, however, potentially comes diversion and unregulated product availability, as well as a lack of understanding among the public of potential risks,” Dr. Keyes added.
“However, approved therapeutic use of psychedelics under a trained health professional’s care remains uncommon in the United States, thus the trends we observe here are undoubtedly in nonmedical and nontherapeutic use,” Dr. Keyes noted.
Dr. Patrick said the increased use of hallucinogens raises “concern for young adult health” and is not without risk. While hallucinogen dependence has historically been rare in the U.S. population, it could become more common as use increases, she noted.
The researchers will continue to track these trends to see whether the increases continue.
“We need additional research, including about the motives for hallucinogen use and how young adults are using these substances, in order to be able to mitigate the associated negative consequences,” Dr. Patrick said.
The study was funded by the National Institute on Drug Abuse, part of the National Institutes of Health. Dr. Keyes and Dr. Patrick have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
With the exception of lysergic acid diethylamide,
In 2018, the prevalence of young adults’ past-year use of non-LSD hallucinogens was 3.4%. By 2021, it had jumped to 6.6%.
The increase in non-LSD hallucinogen use occurred while LSD use remained stable at around 4% in 2018 and 2021.
“While non-LSD hallucinogen use remains substantially less prevalent than use of substances such as alcohol and cannabis, a doubling of prevalence in just three years is a dramatic increase and raises possible public health concerns,” co-author Megan Patrick, PhD, with the University of Michigan Institute for Social Research, Ann Arbor, said in a news release.
The results were published online in the journal Addiction.
Health concerns
The estimates are derived from the Monitoring the Future study, which includes annual assessments of adolescent and adult health in the United States.
The analysis focused on 11,304 persons (52% female) aged 9-30 years from the U.S. general population who were interviewed between 2018 and 2021.
Participants were asked about past 12-month use of LSD, as well as use of non-LSD hallucinogens, such as psilocybin.
From 2018 to 2021, past 12-month use of LSD remained relatively stable; it was 3.7% in 2018 and 4.2% in 2021.
However, non-LSD hallucinogen use increased in prevalence from 3.4% to 6.6% from 2018 to 2021.
Across years, the odds of non-LSD use were higher among males, White people, and individuals from households with higher parental education – a proxy for higher socioeconomic status.
The most commonly used non-LSD hallucinogen was psilocybin.
The survey did not ask whether young adults used non-LSD hallucinogens for therapeutic or medical reasons.
“The use of psychedelic and hallucinogenic drugs for a range of therapeutic uses is increasing, given accumulating yet still preliminary data from randomized trials on clinical effectiveness,” lead author Katherine Keyes, PhD, with Columbia University Mailman School of Public Health, New York, said in the release.
“With increased visibility for medical and therapeutic use, however, potentially comes diversion and unregulated product availability, as well as a lack of understanding among the public of potential risks,” Dr. Keyes added.
“However, approved therapeutic use of psychedelics under a trained health professional’s care remains uncommon in the United States, thus the trends we observe here are undoubtedly in nonmedical and nontherapeutic use,” Dr. Keyes noted.
Dr. Patrick said the increased use of hallucinogens raises “concern for young adult health” and is not without risk. While hallucinogen dependence has historically been rare in the U.S. population, it could become more common as use increases, she noted.
The researchers will continue to track these trends to see whether the increases continue.
“We need additional research, including about the motives for hallucinogen use and how young adults are using these substances, in order to be able to mitigate the associated negative consequences,” Dr. Patrick said.
The study was funded by the National Institute on Drug Abuse, part of the National Institutes of Health. Dr. Keyes and Dr. Patrick have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
With the exception of lysergic acid diethylamide,
In 2018, the prevalence of young adults’ past-year use of non-LSD hallucinogens was 3.4%. By 2021, it had jumped to 6.6%.
The increase in non-LSD hallucinogen use occurred while LSD use remained stable at around 4% in 2018 and 2021.
“While non-LSD hallucinogen use remains substantially less prevalent than use of substances such as alcohol and cannabis, a doubling of prevalence in just three years is a dramatic increase and raises possible public health concerns,” co-author Megan Patrick, PhD, with the University of Michigan Institute for Social Research, Ann Arbor, said in a news release.
The results were published online in the journal Addiction.
Health concerns
The estimates are derived from the Monitoring the Future study, which includes annual assessments of adolescent and adult health in the United States.
The analysis focused on 11,304 persons (52% female) aged 9-30 years from the U.S. general population who were interviewed between 2018 and 2021.
Participants were asked about past 12-month use of LSD, as well as use of non-LSD hallucinogens, such as psilocybin.
From 2018 to 2021, past 12-month use of LSD remained relatively stable; it was 3.7% in 2018 and 4.2% in 2021.
However, non-LSD hallucinogen use increased in prevalence from 3.4% to 6.6% from 2018 to 2021.
Across years, the odds of non-LSD use were higher among males, White people, and individuals from households with higher parental education – a proxy for higher socioeconomic status.
The most commonly used non-LSD hallucinogen was psilocybin.
The survey did not ask whether young adults used non-LSD hallucinogens for therapeutic or medical reasons.
“The use of psychedelic and hallucinogenic drugs for a range of therapeutic uses is increasing, given accumulating yet still preliminary data from randomized trials on clinical effectiveness,” lead author Katherine Keyes, PhD, with Columbia University Mailman School of Public Health, New York, said in the release.
“With increased visibility for medical and therapeutic use, however, potentially comes diversion and unregulated product availability, as well as a lack of understanding among the public of potential risks,” Dr. Keyes added.
“However, approved therapeutic use of psychedelics under a trained health professional’s care remains uncommon in the United States, thus the trends we observe here are undoubtedly in nonmedical and nontherapeutic use,” Dr. Keyes noted.
Dr. Patrick said the increased use of hallucinogens raises “concern for young adult health” and is not without risk. While hallucinogen dependence has historically been rare in the U.S. population, it could become more common as use increases, she noted.
The researchers will continue to track these trends to see whether the increases continue.
“We need additional research, including about the motives for hallucinogen use and how young adults are using these substances, in order to be able to mitigate the associated negative consequences,” Dr. Patrick said.
The study was funded by the National Institute on Drug Abuse, part of the National Institutes of Health. Dr. Keyes and Dr. Patrick have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ADDICTION
The road to weight loss is paved with collusion and sabotage
Three big bumps on the weight-loss journey
The search for the Holy Grail. The destruction of the One Ring. The never-ending struggle to Lose Weight.
Like most legendary quests, weight loss is a journey, and we need support to help us achieve our goal. Maybe it’s gaining a new workout partner or finding a similarly-goaled Facebook Group. For a lot of people, it’s as simple as your friends and family. A recent study, however, suggests that the people closest to you may be your worst weight-loss enemies, and they might not even know it.
Researchers at the University of Surrey reviewed the literature on the positives and negatives of social support when it comes to weight loss and identified three types of negative effects: acts of sabotage, feeding behavior, and collusion.
Let’s start with the softest of intentions and work our way up. Collusion is the least negative. Friends and family may just go with the flow, even if it doesn’t agree with the goals of the person who’s trying to lose weight. It can even happen when health care professionals try to help their patients navigate or avoid obesity, ultimately killing with kindness, so to speak.
Next up, feeding behavior. Maybe you know someone whose love language is cooking. There are also people who share food because they don’t want to waste it or because they’re trying to be polite. They act out of the goodness of their hearts, but they’re putting up roadblocks to someone’s goals. These types of acts are usually one-sided, the researchers found. Remember, it’s okay to say, “No thanks.”
The last method, sabotage, is the most sinister. The saboteur may discourage others from eating healthy, undermine their efforts to be physically active, or take jabs at their confidence or self-esteem. Something as simple as criticizing someone for eating a salad or refusing to go on a walk with them can cause a setback.
“We need to explore this area further to develop interventions which could target family and friends and help them be more supportive in helping those they are close to lose weight,” said lead author Jane Odgen, PhD, of the University of Surrey, Guildford, England.
Like we said before, weight loss is a journey. The right support can only improve the odds of success.
Robots vs. mosquitoes
If there’s one thing robots are bad at, it’s giving solid mental health advice to people in crisis. If there’s one thing robots are very, very good at, it’s causing apocalypses. And joyous day for humanity, this time we’re not the ones being apocalypsed.
Yet.
Taiwan has a big mosquito problem. Not only do the mosquitoes in Taiwan carry dengue – among other dangerous diseases – but they’ve urbanized. Not urbanized in the sense that they’ve acquired a taste for organic coffee and avocado toast (that would be the millennial mosquito, a separate but even more terrifying creature), but more that they’ve adapted to reproduce literally anywhere and everywhere. Taiwanese mosquitoes like to breed in roadside sewer ditches, and this is where our genocidal robot comes in.
To combat the new, dangerous form of street-savvy mosquito, researchers built a robot armed with both insecticide and high-temperature, high-pressure water jets and sent it into the sewers of Kaohsiung City. The robot’s goal was simple: Whenever it came across signs of heavy mosquito breeding – eggs, larvae, pupae, and so on – the robot went to work. Utilizing both its primary weapons, the robot scrubbed numerous breeding sites across the city clean.
The researchers could just sit back and wait to see how effective their robot was. In the immediate aftermath, at various monitoring sites placed alongside the ditches, adult mosquito density fell by two-thirds in areas targeted by the robot. That’s nothing to sniff at, and it does make sense. After all, mosquitoes are quite difficult to kill in their adult stage, why not target them when they’re young and basically immobile?
The researchers saw promise with their mosquito-killing robot, but we’ve noticed a rather large issue. Killing two-thirds of mosquitoes is fine, but the third that’s left will be very angry. Very angry indeed. After all, we’re targeting the mosquito equivalent of children. Let’s hope our mosquito Terminator managed to kill mosquito Sarah Connor, or we’re going to have a big problem on our hands a bit later down the line.
This is knot what you were expecting
Physicians who aren’t surgeons probably don’t realize it, but the big thing that’s been getting between the knot-tying specialists and perfect suturing technique all these years is a lack of physics. Don’t believe us? Well, maybe you’ll believe plastic surgeon Samia Guerid, MD, of Lausanne, Switzerland: “The lack of physics-based analysis has been a limitation.” Nuff said.

That’s not enough for you, is it? Fine, we were warned.
Any surgical knot, Dr. Guerid and associates explained in a written statement, involves the “complex interplay” between six key factors: topology, geometry, elasticity, contact, friction, and polymer plasticity of the suturing filament. The strength of a suture “depends on the tension applied during the tying of the knot, [which] permanently deforms, or stretches the filament, creating a holding force.” Not enough tension and the knot comes undone, while too much snaps the filament.
For the experiment, Dr. Guerid tied a few dozen surgical knots, which were then scanned using x-ray micro–computed tomography to facilitate finite element modeling with a “3D continuum-level constitutive model for elastic-viscoplastic mechanical behavior” – no, we have no idea what that means, either – developed by the research team.
That model, and a great deal of math – so much math – allowed the researchers to define a threshold between loose and tight knots and uncover “relationships between knot strength and pretension, friction, and number of throws,” they said.
But what about the big question? The one about the ideal amount of tension? You may want to sit down. The answer to the ultimate question of the relationship between knot pretension and strength is … Did we mention that the team had its own mathematician? Their predictive model for safe knot-tying is … You’re not going to like this. The best way to teach safe knot-tying to both trainees and robots is … not ready yet.
The secret to targeting the knot tension sweet spot, for now, anyway, is still intuition gained from years of experience. Nobody ever said science was perfect … or easy … or quick.
Three big bumps on the weight-loss journey
The search for the Holy Grail. The destruction of the One Ring. The never-ending struggle to Lose Weight.
Like most legendary quests, weight loss is a journey, and we need support to help us achieve our goal. Maybe it’s gaining a new workout partner or finding a similarly-goaled Facebook Group. For a lot of people, it’s as simple as your friends and family. A recent study, however, suggests that the people closest to you may be your worst weight-loss enemies, and they might not even know it.
Researchers at the University of Surrey reviewed the literature on the positives and negatives of social support when it comes to weight loss and identified three types of negative effects: acts of sabotage, feeding behavior, and collusion.
Let’s start with the softest of intentions and work our way up. Collusion is the least negative. Friends and family may just go with the flow, even if it doesn’t agree with the goals of the person who’s trying to lose weight. It can even happen when health care professionals try to help their patients navigate or avoid obesity, ultimately killing with kindness, so to speak.
Next up, feeding behavior. Maybe you know someone whose love language is cooking. There are also people who share food because they don’t want to waste it or because they’re trying to be polite. They act out of the goodness of their hearts, but they’re putting up roadblocks to someone’s goals. These types of acts are usually one-sided, the researchers found. Remember, it’s okay to say, “No thanks.”
The last method, sabotage, is the most sinister. The saboteur may discourage others from eating healthy, undermine their efforts to be physically active, or take jabs at their confidence or self-esteem. Something as simple as criticizing someone for eating a salad or refusing to go on a walk with them can cause a setback.
“We need to explore this area further to develop interventions which could target family and friends and help them be more supportive in helping those they are close to lose weight,” said lead author Jane Odgen, PhD, of the University of Surrey, Guildford, England.
Like we said before, weight loss is a journey. The right support can only improve the odds of success.
Robots vs. mosquitoes
If there’s one thing robots are bad at, it’s giving solid mental health advice to people in crisis. If there’s one thing robots are very, very good at, it’s causing apocalypses. And joyous day for humanity, this time we’re not the ones being apocalypsed.
Yet.
Taiwan has a big mosquito problem. Not only do the mosquitoes in Taiwan carry dengue – among other dangerous diseases – but they’ve urbanized. Not urbanized in the sense that they’ve acquired a taste for organic coffee and avocado toast (that would be the millennial mosquito, a separate but even more terrifying creature), but more that they’ve adapted to reproduce literally anywhere and everywhere. Taiwanese mosquitoes like to breed in roadside sewer ditches, and this is where our genocidal robot comes in.
To combat the new, dangerous form of street-savvy mosquito, researchers built a robot armed with both insecticide and high-temperature, high-pressure water jets and sent it into the sewers of Kaohsiung City. The robot’s goal was simple: Whenever it came across signs of heavy mosquito breeding – eggs, larvae, pupae, and so on – the robot went to work. Utilizing both its primary weapons, the robot scrubbed numerous breeding sites across the city clean.
The researchers could just sit back and wait to see how effective their robot was. In the immediate aftermath, at various monitoring sites placed alongside the ditches, adult mosquito density fell by two-thirds in areas targeted by the robot. That’s nothing to sniff at, and it does make sense. After all, mosquitoes are quite difficult to kill in their adult stage, why not target them when they’re young and basically immobile?
The researchers saw promise with their mosquito-killing robot, but we’ve noticed a rather large issue. Killing two-thirds of mosquitoes is fine, but the third that’s left will be very angry. Very angry indeed. After all, we’re targeting the mosquito equivalent of children. Let’s hope our mosquito Terminator managed to kill mosquito Sarah Connor, or we’re going to have a big problem on our hands a bit later down the line.
This is knot what you were expecting
Physicians who aren’t surgeons probably don’t realize it, but the big thing that’s been getting between the knot-tying specialists and perfect suturing technique all these years is a lack of physics. Don’t believe us? Well, maybe you’ll believe plastic surgeon Samia Guerid, MD, of Lausanne, Switzerland: “The lack of physics-based analysis has been a limitation.” Nuff said.
That’s not enough for you, is it? Fine, we were warned.
Any surgical knot, Dr. Guerid and associates explained in a written statement, involves the “complex interplay” between six key factors: topology, geometry, elasticity, contact, friction, and polymer plasticity of the suturing filament. The strength of a suture “depends on the tension applied during the tying of the knot, [which] permanently deforms, or stretches the filament, creating a holding force.” Not enough tension and the knot comes undone, while too much snaps the filament.
For the experiment, Dr. Guerid tied a few dozen surgical knots, which were then scanned using x-ray micro–computed tomography to facilitate finite element modeling with a “3D continuum-level constitutive model for elastic-viscoplastic mechanical behavior” – no, we have no idea what that means, either – developed by the research team.
That model, and a great deal of math – so much math – allowed the researchers to define a threshold between loose and tight knots and uncover “relationships between knot strength and pretension, friction, and number of throws,” they said.
But what about the big question? The one about the ideal amount of tension? You may want to sit down. The answer to the ultimate question of the relationship between knot pretension and strength is … Did we mention that the team had its own mathematician? Their predictive model for safe knot-tying is … You’re not going to like this. The best way to teach safe knot-tying to both trainees and robots is … not ready yet.
The secret to targeting the knot tension sweet spot, for now, anyway, is still intuition gained from years of experience. Nobody ever said science was perfect … or easy … or quick.
Three big bumps on the weight-loss journey
The search for the Holy Grail. The destruction of the One Ring. The never-ending struggle to Lose Weight.
Like most legendary quests, weight loss is a journey, and we need support to help us achieve our goal. Maybe it’s gaining a new workout partner or finding a similarly-goaled Facebook Group. For a lot of people, it’s as simple as your friends and family. A recent study, however, suggests that the people closest to you may be your worst weight-loss enemies, and they might not even know it.
Researchers at the University of Surrey reviewed the literature on the positives and negatives of social support when it comes to weight loss and identified three types of negative effects: acts of sabotage, feeding behavior, and collusion.
Let’s start with the softest of intentions and work our way up. Collusion is the least negative. Friends and family may just go with the flow, even if it doesn’t agree with the goals of the person who’s trying to lose weight. It can even happen when health care professionals try to help their patients navigate or avoid obesity, ultimately killing with kindness, so to speak.
Next up, feeding behavior. Maybe you know someone whose love language is cooking. There are also people who share food because they don’t want to waste it or because they’re trying to be polite. They act out of the goodness of their hearts, but they’re putting up roadblocks to someone’s goals. These types of acts are usually one-sided, the researchers found. Remember, it’s okay to say, “No thanks.”
The last method, sabotage, is the most sinister. The saboteur may discourage others from eating healthy, undermine their efforts to be physically active, or take jabs at their confidence or self-esteem. Something as simple as criticizing someone for eating a salad or refusing to go on a walk with them can cause a setback.
“We need to explore this area further to develop interventions which could target family and friends and help them be more supportive in helping those they are close to lose weight,” said lead author Jane Odgen, PhD, of the University of Surrey, Guildford, England.
Like we said before, weight loss is a journey. The right support can only improve the odds of success.
Robots vs. mosquitoes
If there’s one thing robots are bad at, it’s giving solid mental health advice to people in crisis. If there’s one thing robots are very, very good at, it’s causing apocalypses. And joyous day for humanity, this time we’re not the ones being apocalypsed.
Yet.
Taiwan has a big mosquito problem. Not only do the mosquitoes in Taiwan carry dengue – among other dangerous diseases – but they’ve urbanized. Not urbanized in the sense that they’ve acquired a taste for organic coffee and avocado toast (that would be the millennial mosquito, a separate but even more terrifying creature), but more that they’ve adapted to reproduce literally anywhere and everywhere. Taiwanese mosquitoes like to breed in roadside sewer ditches, and this is where our genocidal robot comes in.
To combat the new, dangerous form of street-savvy mosquito, researchers built a robot armed with both insecticide and high-temperature, high-pressure water jets and sent it into the sewers of Kaohsiung City. The robot’s goal was simple: Whenever it came across signs of heavy mosquito breeding – eggs, larvae, pupae, and so on – the robot went to work. Utilizing both its primary weapons, the robot scrubbed numerous breeding sites across the city clean.
The researchers could just sit back and wait to see how effective their robot was. In the immediate aftermath, at various monitoring sites placed alongside the ditches, adult mosquito density fell by two-thirds in areas targeted by the robot. That’s nothing to sniff at, and it does make sense. After all, mosquitoes are quite difficult to kill in their adult stage, why not target them when they’re young and basically immobile?
The researchers saw promise with their mosquito-killing robot, but we’ve noticed a rather large issue. Killing two-thirds of mosquitoes is fine, but the third that’s left will be very angry. Very angry indeed. After all, we’re targeting the mosquito equivalent of children. Let’s hope our mosquito Terminator managed to kill mosquito Sarah Connor, or we’re going to have a big problem on our hands a bit later down the line.
This is knot what you were expecting
Physicians who aren’t surgeons probably don’t realize it, but the big thing that’s been getting between the knot-tying specialists and perfect suturing technique all these years is a lack of physics. Don’t believe us? Well, maybe you’ll believe plastic surgeon Samia Guerid, MD, of Lausanne, Switzerland: “The lack of physics-based analysis has been a limitation.” Nuff said.
That’s not enough for you, is it? Fine, we were warned.
Any surgical knot, Dr. Guerid and associates explained in a written statement, involves the “complex interplay” between six key factors: topology, geometry, elasticity, contact, friction, and polymer plasticity of the suturing filament. The strength of a suture “depends on the tension applied during the tying of the knot, [which] permanently deforms, or stretches the filament, creating a holding force.” Not enough tension and the knot comes undone, while too much snaps the filament.
For the experiment, Dr. Guerid tied a few dozen surgical knots, which were then scanned using x-ray micro–computed tomography to facilitate finite element modeling with a “3D continuum-level constitutive model for elastic-viscoplastic mechanical behavior” – no, we have no idea what that means, either – developed by the research team.
That model, and a great deal of math – so much math – allowed the researchers to define a threshold between loose and tight knots and uncover “relationships between knot strength and pretension, friction, and number of throws,” they said.
But what about the big question? The one about the ideal amount of tension? You may want to sit down. The answer to the ultimate question of the relationship between knot pretension and strength is … Did we mention that the team had its own mathematician? Their predictive model for safe knot-tying is … You’re not going to like this. The best way to teach safe knot-tying to both trainees and robots is … not ready yet.
The secret to targeting the knot tension sweet spot, for now, anyway, is still intuition gained from years of experience. Nobody ever said science was perfect … or easy … or quick.
Investing in the future of GI
This leads to promising investigators walking away from GI research frustrated by a lack of support. Investigators in the early stages of their careers are particularly hard hit.
Decades of research have revolutionized the care of many digestive disease patients. These patients, as well as everyone in the GI field – clinicians and researchers alike – have benefited from discoveries made by dedicated investigators, past and present.
Creative young researchers are poised to make groundbreaking discoveries that will shape the future of gastroenterology. Unfortunately, declining government funding for biomedical research puts this potential in jeopardy. We’re at risk of losing an entire generation of researchers if we don’t act now.
To fill this gap, the AGA Research Foundation invites you to support young investigators’ research careers, allowing them to make discoveries that could ultimately improve patient care and even cure diseases.
“We are at the threshold of key research advances that will cure digestive diseases. We have the manpower, we have trained the people, now we need to have the security that they can stay in research and advance these cures,” said Kim Elaine Barrett, PhD, AGAF, AGA legacy society donor and AGA governing board member.

By joining others in supporting the AGA Research Foundation, you will ensure that young researchers have opportunities to continue their life-saving work.
Learn more or make a contribution at www.foundation.gastro.org.
This leads to promising investigators walking away from GI research frustrated by a lack of support. Investigators in the early stages of their careers are particularly hard hit.
Decades of research have revolutionized the care of many digestive disease patients. These patients, as well as everyone in the GI field – clinicians and researchers alike – have benefited from discoveries made by dedicated investigators, past and present.
Creative young researchers are poised to make groundbreaking discoveries that will shape the future of gastroenterology. Unfortunately, declining government funding for biomedical research puts this potential in jeopardy. We’re at risk of losing an entire generation of researchers if we don’t act now.
To fill this gap, the AGA Research Foundation invites you to support young investigators’ research careers, allowing them to make discoveries that could ultimately improve patient care and even cure diseases.
“We are at the threshold of key research advances that will cure digestive diseases. We have the manpower, we have trained the people, now we need to have the security that they can stay in research and advance these cures,” said Kim Elaine Barrett, PhD, AGAF, AGA legacy society donor and AGA governing board member.
By joining others in supporting the AGA Research Foundation, you will ensure that young researchers have opportunities to continue their life-saving work.
Learn more or make a contribution at www.foundation.gastro.org.
This leads to promising investigators walking away from GI research frustrated by a lack of support. Investigators in the early stages of their careers are particularly hard hit.
Decades of research have revolutionized the care of many digestive disease patients. These patients, as well as everyone in the GI field – clinicians and researchers alike – have benefited from discoveries made by dedicated investigators, past and present.
Creative young researchers are poised to make groundbreaking discoveries that will shape the future of gastroenterology. Unfortunately, declining government funding for biomedical research puts this potential in jeopardy. We’re at risk of losing an entire generation of researchers if we don’t act now.
To fill this gap, the AGA Research Foundation invites you to support young investigators’ research careers, allowing them to make discoveries that could ultimately improve patient care and even cure diseases.
“We are at the threshold of key research advances that will cure digestive diseases. We have the manpower, we have trained the people, now we need to have the security that they can stay in research and advance these cures,” said Kim Elaine Barrett, PhD, AGAF, AGA legacy society donor and AGA governing board member.
By joining others in supporting the AGA Research Foundation, you will ensure that young researchers have opportunities to continue their life-saving work.
Learn more or make a contribution at www.foundation.gastro.org.
Trailblazer for women in gastroenterology, Dr. Barbara H. Jung takes over as AGA president
She currently serves as the first woman Robert G. Petersdorf professor and chair of internal medicine at the University of Washington, Seattle, and is the fourth woman to lead the American Gastroenterological Association as its president.
Dr. Jung is an international expert in the field of transforming growth factor–beta superfamily signaling in colon cancer and has made significant contributions at AGA prior to becoming president, most recently as a member of the finance and operations committee, chair-elect of the audit committee and vice chair of the AGA Research Foundation.

Born in Portland, Ore., and raised in Munich, Germany, Dr. Jung’s parents provided unconditional support for her career choice in medicine and nurtured her leadership skills throughout her childhood.
Her academic career began at Ludwig Maximilians University of Munich followed by postdoctoral studies in colon cancer at the Sidney Kimmel Cancer Center in San Diego and eventually culminating in an internal medicine residency at the University of California, San Diego.
Dr. Jung joined the AGA Governing Board in June 2021 as vice president and served as president-elect prior to assuming the top leadership role. Over her time as an AGA member (which started during fellowship), Dr. Jung has also served on the AGA Audit Committee, AGA Registry Research and Publications Committee, AGA Research Policy Committee, and AGA Innovation and Technology Task Force. In 2017, she co-organized the AGA Academic Skills Workshop to train the next generation of gastroenterologists.
She currently serves as the first woman Robert G. Petersdorf professor and chair of internal medicine at the University of Washington, Seattle, and is the fourth woman to lead the American Gastroenterological Association as its president.
Dr. Jung is an international expert in the field of transforming growth factor–beta superfamily signaling in colon cancer and has made significant contributions at AGA prior to becoming president, most recently as a member of the finance and operations committee, chair-elect of the audit committee and vice chair of the AGA Research Foundation.
Born in Portland, Ore., and raised in Munich, Germany, Dr. Jung’s parents provided unconditional support for her career choice in medicine and nurtured her leadership skills throughout her childhood.
Her academic career began at Ludwig Maximilians University of Munich followed by postdoctoral studies in colon cancer at the Sidney Kimmel Cancer Center in San Diego and eventually culminating in an internal medicine residency at the University of California, San Diego.
Dr. Jung joined the AGA Governing Board in June 2021 as vice president and served as president-elect prior to assuming the top leadership role. Over her time as an AGA member (which started during fellowship), Dr. Jung has also served on the AGA Audit Committee, AGA Registry Research and Publications Committee, AGA Research Policy Committee, and AGA Innovation and Technology Task Force. In 2017, she co-organized the AGA Academic Skills Workshop to train the next generation of gastroenterologists.
She currently serves as the first woman Robert G. Petersdorf professor and chair of internal medicine at the University of Washington, Seattle, and is the fourth woman to lead the American Gastroenterological Association as its president.
Dr. Jung is an international expert in the field of transforming growth factor–beta superfamily signaling in colon cancer and has made significant contributions at AGA prior to becoming president, most recently as a member of the finance and operations committee, chair-elect of the audit committee and vice chair of the AGA Research Foundation.
Born in Portland, Ore., and raised in Munich, Germany, Dr. Jung’s parents provided unconditional support for her career choice in medicine and nurtured her leadership skills throughout her childhood.
Her academic career began at Ludwig Maximilians University of Munich followed by postdoctoral studies in colon cancer at the Sidney Kimmel Cancer Center in San Diego and eventually culminating in an internal medicine residency at the University of California, San Diego.
Dr. Jung joined the AGA Governing Board in June 2021 as vice president and served as president-elect prior to assuming the top leadership role. Over her time as an AGA member (which started during fellowship), Dr. Jung has also served on the AGA Audit Committee, AGA Registry Research and Publications Committee, AGA Research Policy Committee, and AGA Innovation and Technology Task Force. In 2017, she co-organized the AGA Academic Skills Workshop to train the next generation of gastroenterologists.
The cardiopulmonary effects of mask wearing
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
There was a time when I would have had to explain to you what an N95 mask is, how it is designed to filter out 95% of fine particles, defined as stuff in the air less than 2.5 microns in size.
But of course, you know that now. The N95 had its moment – a moment that seemed to be passing as the concentration of airborne coronavirus particles decreased.
But, as the poet said, all that is less than 2.5 microns in size is not coronavirus. Wildfire smoke is also chock full of fine particulate matter. And so, N95s are having something of a comeback.
That’s why an article that took a deep look at what happens to our cardiovascular system when we wear N95 masks caught my eye.
Mask wearing has been the subject of intense debate around the country. While the vast majority of evidence, as well as the personal experience of thousands of doctors, suggests that wearing a mask has no significant physiologic effects, it’s not hard to find those who suggest that mask wearing depletes oxygen levels, or leads to infection, or has other bizarre effects.
In a world of conflicting opinions, a controlled study is a wonderful thing, and that’s what appeared in JAMA Network Open.
This isn’t a huge study, but it’s big enough to make some important conclusions. Thirty individuals, all young and healthy, half female, were enrolled. Each participant spent 3 days in a metabolic chamber; this is essentially a giant, airtight room where all the inputs (oxygen levels and so on) and outputs (carbon dioxide levels and so on) can be precisely measured.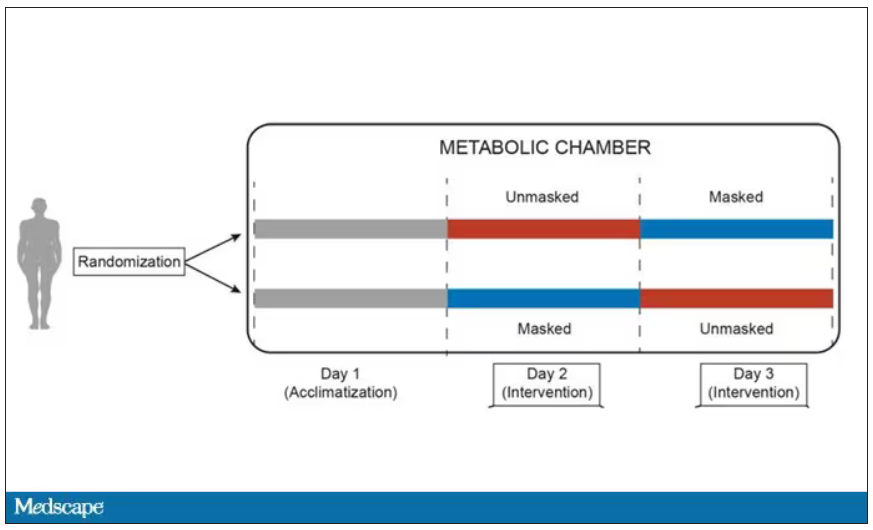
After a day of getting used to the environment, the participants spent a day either wearing an N95 mask or not for 16 waking hours. On the next day, they switched. Every other variable was controlled, from the calories in their diet to the temperature of the room itself.
They engaged in light exercise twice during the day – riding a stationary bike – and a host of physiologic parameters were measured. The question being, would the wearing of the mask for 16 hours straight change anything?
And the answer is yes, some things changed, but not by much.
Here’s a graph of the heart rate over time. You can see some separation, with higher heart rates during the mask-wearing day, particularly around 11 a.m. – when light exercise was scheduled.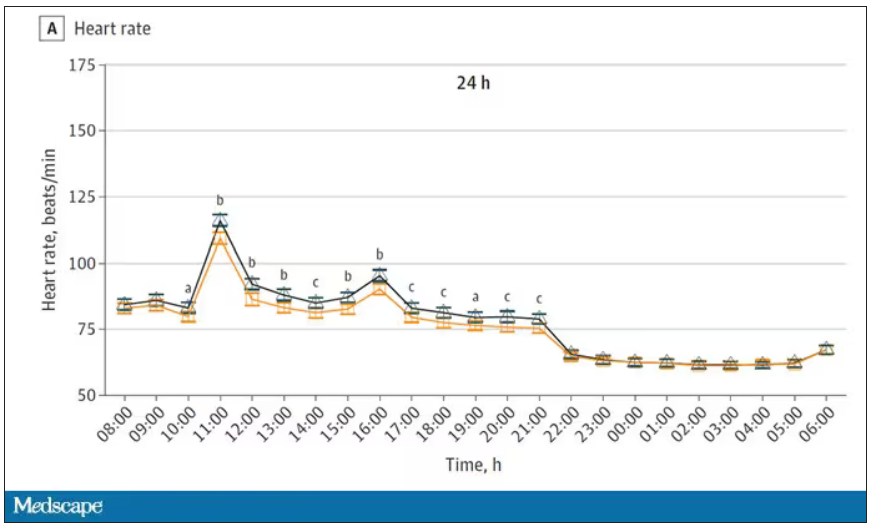
Zooming in on the exercise period makes the difference more clear. The heart rate was about eight beats/min higher while masked and engaging in exercise. Systolic blood pressure was about 6 mm Hg higher. Oxygen saturation was lower by 0.7%.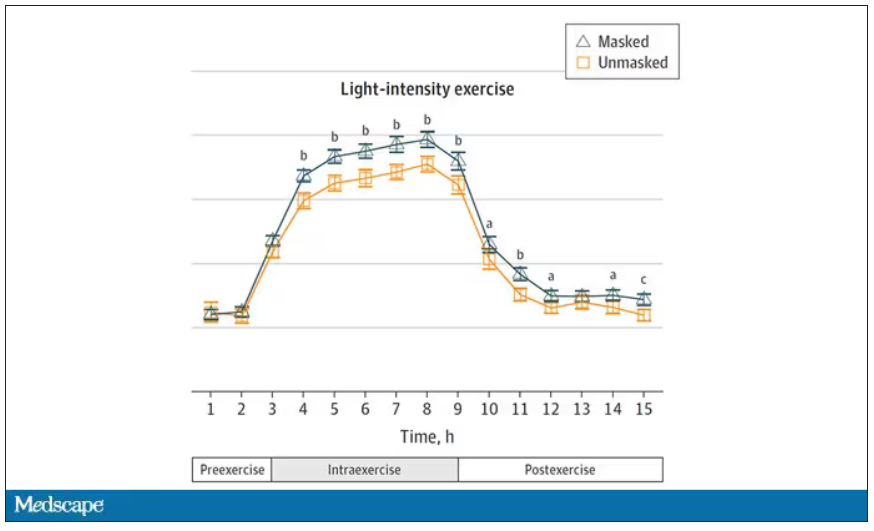
So yes, exercising while wearing an N95 mask might be different from exercising without an N95 mask. But nothing here looks dangerous to me. The 0.7% decrease in oxygen saturation is smaller than the typical measurement error of a pulse oximeter. The authors write that venous pH decreased during the masked day, which is of more interest to me as a nephrologist, but they don’t show that data even in the supplement. I suspect it didn’t decrease much.
They also showed that respiratory rate during exercise decreased in the masked condition. That doesn’t really make sense when you think about it in the context of the other findings, which are all suggestive of increased metabolic rate and sympathetic drive. Does that call the whole procedure into question? No, but it’s worth noting.
These were young, healthy people. You could certainly argue that those with more vulnerable cardiopulmonary status might have had different effects from mask wearing, but without a specific study in those people, it’s just conjecture. Clearly, this study lets us conclude that mask wearing at rest has less of an effect than mask wearing during exercise.
But remember that, in reality, we are wearing masks for a reason. One could imagine a study where this metabolic chamber was filled with wildfire smoke at a concentration similar to what we saw in New York. In that situation, we might find that wearing an N95 is quite helpful. The thing is, studying masks in isolation is useful because you can control so many variables. But masks aren’t used in isolation. In fact, that’s sort of their defining characteristic.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
There was a time when I would have had to explain to you what an N95 mask is, how it is designed to filter out 95% of fine particles, defined as stuff in the air less than 2.5 microns in size.
But of course, you know that now. The N95 had its moment – a moment that seemed to be passing as the concentration of airborne coronavirus particles decreased.
But, as the poet said, all that is less than 2.5 microns in size is not coronavirus. Wildfire smoke is also chock full of fine particulate matter. And so, N95s are having something of a comeback.
That’s why an article that took a deep look at what happens to our cardiovascular system when we wear N95 masks caught my eye.
Mask wearing has been the subject of intense debate around the country. While the vast majority of evidence, as well as the personal experience of thousands of doctors, suggests that wearing a mask has no significant physiologic effects, it’s not hard to find those who suggest that mask wearing depletes oxygen levels, or leads to infection, or has other bizarre effects.
In a world of conflicting opinions, a controlled study is a wonderful thing, and that’s what appeared in JAMA Network Open.
This isn’t a huge study, but it’s big enough to make some important conclusions. Thirty individuals, all young and healthy, half female, were enrolled. Each participant spent 3 days in a metabolic chamber; this is essentially a giant, airtight room where all the inputs (oxygen levels and so on) and outputs (carbon dioxide levels and so on) can be precisely measured.
After a day of getting used to the environment, the participants spent a day either wearing an N95 mask or not for 16 waking hours. On the next day, they switched. Every other variable was controlled, from the calories in their diet to the temperature of the room itself.
They engaged in light exercise twice during the day – riding a stationary bike – and a host of physiologic parameters were measured. The question being, would the wearing of the mask for 16 hours straight change anything?
And the answer is yes, some things changed, but not by much.
Here’s a graph of the heart rate over time. You can see some separation, with higher heart rates during the mask-wearing day, particularly around 11 a.m. – when light exercise was scheduled.
Zooming in on the exercise period makes the difference more clear. The heart rate was about eight beats/min higher while masked and engaging in exercise. Systolic blood pressure was about 6 mm Hg higher. Oxygen saturation was lower by 0.7%.
So yes, exercising while wearing an N95 mask might be different from exercising without an N95 mask. But nothing here looks dangerous to me. The 0.7% decrease in oxygen saturation is smaller than the typical measurement error of a pulse oximeter. The authors write that venous pH decreased during the masked day, which is of more interest to me as a nephrologist, but they don’t show that data even in the supplement. I suspect it didn’t decrease much.
They also showed that respiratory rate during exercise decreased in the masked condition. That doesn’t really make sense when you think about it in the context of the other findings, which are all suggestive of increased metabolic rate and sympathetic drive. Does that call the whole procedure into question? No, but it’s worth noting.
These were young, healthy people. You could certainly argue that those with more vulnerable cardiopulmonary status might have had different effects from mask wearing, but without a specific study in those people, it’s just conjecture. Clearly, this study lets us conclude that mask wearing at rest has less of an effect than mask wearing during exercise.
But remember that, in reality, we are wearing masks for a reason. One could imagine a study where this metabolic chamber was filled with wildfire smoke at a concentration similar to what we saw in New York. In that situation, we might find that wearing an N95 is quite helpful. The thing is, studying masks in isolation is useful because you can control so many variables. But masks aren’t used in isolation. In fact, that’s sort of their defining characteristic.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
There was a time when I would have had to explain to you what an N95 mask is, how it is designed to filter out 95% of fine particles, defined as stuff in the air less than 2.5 microns in size.
But of course, you know that now. The N95 had its moment – a moment that seemed to be passing as the concentration of airborne coronavirus particles decreased.
But, as the poet said, all that is less than 2.5 microns in size is not coronavirus. Wildfire smoke is also chock full of fine particulate matter. And so, N95s are having something of a comeback.
That’s why an article that took a deep look at what happens to our cardiovascular system when we wear N95 masks caught my eye.
Mask wearing has been the subject of intense debate around the country. While the vast majority of evidence, as well as the personal experience of thousands of doctors, suggests that wearing a mask has no significant physiologic effects, it’s not hard to find those who suggest that mask wearing depletes oxygen levels, or leads to infection, or has other bizarre effects.
In a world of conflicting opinions, a controlled study is a wonderful thing, and that’s what appeared in JAMA Network Open.
This isn’t a huge study, but it’s big enough to make some important conclusions. Thirty individuals, all young and healthy, half female, were enrolled. Each participant spent 3 days in a metabolic chamber; this is essentially a giant, airtight room where all the inputs (oxygen levels and so on) and outputs (carbon dioxide levels and so on) can be precisely measured.
After a day of getting used to the environment, the participants spent a day either wearing an N95 mask or not for 16 waking hours. On the next day, they switched. Every other variable was controlled, from the calories in their diet to the temperature of the room itself.
They engaged in light exercise twice during the day – riding a stationary bike – and a host of physiologic parameters were measured. The question being, would the wearing of the mask for 16 hours straight change anything?
And the answer is yes, some things changed, but not by much.
Here’s a graph of the heart rate over time. You can see some separation, with higher heart rates during the mask-wearing day, particularly around 11 a.m. – when light exercise was scheduled.
Zooming in on the exercise period makes the difference more clear. The heart rate was about eight beats/min higher while masked and engaging in exercise. Systolic blood pressure was about 6 mm Hg higher. Oxygen saturation was lower by 0.7%.
So yes, exercising while wearing an N95 mask might be different from exercising without an N95 mask. But nothing here looks dangerous to me. The 0.7% decrease in oxygen saturation is smaller than the typical measurement error of a pulse oximeter. The authors write that venous pH decreased during the masked day, which is of more interest to me as a nephrologist, but they don’t show that data even in the supplement. I suspect it didn’t decrease much.
They also showed that respiratory rate during exercise decreased in the masked condition. That doesn’t really make sense when you think about it in the context of the other findings, which are all suggestive of increased metabolic rate and sympathetic drive. Does that call the whole procedure into question? No, but it’s worth noting.
These were young, healthy people. You could certainly argue that those with more vulnerable cardiopulmonary status might have had different effects from mask wearing, but without a specific study in those people, it’s just conjecture. Clearly, this study lets us conclude that mask wearing at rest has less of an effect than mask wearing during exercise.
But remember that, in reality, we are wearing masks for a reason. One could imagine a study where this metabolic chamber was filled with wildfire smoke at a concentration similar to what we saw in New York. In that situation, we might find that wearing an N95 is quite helpful. The thing is, studying masks in isolation is useful because you can control so many variables. But masks aren’t used in isolation. In fact, that’s sort of their defining characteristic.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Good COP, bad COP. Is this cardiorespiratory measure the best predictor of early death?
according to clinicians who champion the assessment. The COP is easier to obtain than cardiorespiratory measures that require people to exercise to their limit, advocates say; rather than running full speed, someone can walk or lightly jog on a treadmill, with a COP value obtained easily.
But other clinicians argue that maximal exercise tests have many prognostic benefits, and that physicians should do everything in their power to push patients to exercise as hard as possible. In particular, the VO2 max test captures the maximum amount of oxygen someone uses when exercising at their capacity and is the preferred method for measuring cardiovascular endurance.
The COP is a measure of the minimum number of liters of air during breathing required to move one liter of oxygen through the bloodstream. The lower the COP the better, because this means that someone is working less strenuously than someone else to transport the same amount of oxygen, denoting a more efficient interaction between their heart and lungs.
The COP for a fit person might be 15, about 20-25 for a healthy person, and 35 for someone with heart failure, according to Claudio Gil Araújo, MD, PhD, director of research and education at CLINIMEX, an exercise medicine clinic in Rio de Janeiro.
“Max VO2 is very important, that’s indisputable. But when do you use max VO2 in your daily life? Never,” Dr. Araújo said. But almost anyone can generate a COP.
Emerging uses for the COP
“I can put someone on the treadmill or bike, and after 3 or 4 minutes I have the COP. It’s like a walking pace,” Dr. Araújo said. Yet the values are obtained with roughly half the effort as VO2 max. Other clinicians argue exercising to the limits of endurance offers unique clinical insights.
“We should do everything in our power to exercise our patients to maximum. How long a patient is able to go is really important,” said Anu Lala, MD, a cardiologist who specializes in heart failure treatment at Mount Sinai Hospital in New York. A full-capacity exercise test gives useful insights into someone’s heart rate, heart rate recovery, blood pressure, and ECG response to vigorous exercise, Dr. Lala added, all of which are important clues to someone’s overall health.
In 2012 Dr. Araújo coauthored a study that first defined the COP, which is calculated by measuring expired gasses people produce while gently exercising, perhaps to the point where they begin to perspire, and then dividing their breathing capacity by their oxygen uptake every minute. The lowest value obtained during any exercise session is the COP.
Various studies show that higher COP values are associated with more severe heart lesions in patients with congenital heart disease; higher levels of mortality in seemingly healthy male adults; and with worse prognoses in patients with heart failure. These studies all appeared within the last 7 months.
The mortality study, which Dr. Araújo coauthored, compared COP in more than 3,000 U.S. men and women who completed an exercise test from 1973 to 2018 and were tracked for an average of 23 years. Although COP was introduced as an assessment in 2012, calculating the value from tests prior to that date was possible because those tests had captured the relevant breathing rate and oxygen uptake. In males aged 18-85 years, a worse COP was significantly associated with an increased risk for earlier death. This finding did not hold for females, however; Dr. Araújo noted that more research is needed to understand the discrepancy in COP’s predictive power by sex.
In the heart failure study, everyone enrolled had heart failure and completed a COP test. People with the worse COPs also had the worst symptoms of heart failure, but completing an exercise rehabilitation program improved COP values when researchers measured them again. Dr. Araújo was also part of this study, based in the Netherlands.
“I think the COP could become a novel parameter in clinical care,” for most people, said Thijs Eijsvogels, PhD, an exercise physiologist at Radboud University in Nijmegen, the Netherlands, and the senior author of the heart failure study. That said, Dr. Eijsvogels said elite athletes will always be more interested in measuring VO2 max.
Dr. Lala agreed that tests such as the COP have some value. Her own work has shown that measuring the efficiency of someone’s breathing patterns for exhaling carbon dioxide, which can also be done without making people exercise full strength, has prognostic value for patients with advanced heart failure. Even so, she said she would like to see maximal effort tests used as much as possible.
“I worry about saying we’re going to settle for a parameter that can be achieved at 50% of peak VO2 and then we don’t exercise our patients,” Dr. Lala said.
Dr. Araújo said he plans to continue to measure VO2 max but he believes COP has utility – even for elite athletes. One of his patients is a frequent Ironman competitor who competes well despite having a solid but not amazing VO2 max level. But her COP is quite low, Dr. Araújo said, which to him suggests an especially efficient interaction between her respiratory and cardiovascular systems.
“We have a new player in the game,” Dr. Araújo said.
The sources in this study report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to clinicians who champion the assessment. The COP is easier to obtain than cardiorespiratory measures that require people to exercise to their limit, advocates say; rather than running full speed, someone can walk or lightly jog on a treadmill, with a COP value obtained easily.
But other clinicians argue that maximal exercise tests have many prognostic benefits, and that physicians should do everything in their power to push patients to exercise as hard as possible. In particular, the VO2 max test captures the maximum amount of oxygen someone uses when exercising at their capacity and is the preferred method for measuring cardiovascular endurance.
The COP is a measure of the minimum number of liters of air during breathing required to move one liter of oxygen through the bloodstream. The lower the COP the better, because this means that someone is working less strenuously than someone else to transport the same amount of oxygen, denoting a more efficient interaction between their heart and lungs.
The COP for a fit person might be 15, about 20-25 for a healthy person, and 35 for someone with heart failure, according to Claudio Gil Araújo, MD, PhD, director of research and education at CLINIMEX, an exercise medicine clinic in Rio de Janeiro.
“Max VO2 is very important, that’s indisputable. But when do you use max VO2 in your daily life? Never,” Dr. Araújo said. But almost anyone can generate a COP.
Emerging uses for the COP
“I can put someone on the treadmill or bike, and after 3 or 4 minutes I have the COP. It’s like a walking pace,” Dr. Araújo said. Yet the values are obtained with roughly half the effort as VO2 max. Other clinicians argue exercising to the limits of endurance offers unique clinical insights.
“We should do everything in our power to exercise our patients to maximum. How long a patient is able to go is really important,” said Anu Lala, MD, a cardiologist who specializes in heart failure treatment at Mount Sinai Hospital in New York. A full-capacity exercise test gives useful insights into someone’s heart rate, heart rate recovery, blood pressure, and ECG response to vigorous exercise, Dr. Lala added, all of which are important clues to someone’s overall health.
In 2012 Dr. Araújo coauthored a study that first defined the COP, which is calculated by measuring expired gasses people produce while gently exercising, perhaps to the point where they begin to perspire, and then dividing their breathing capacity by their oxygen uptake every minute. The lowest value obtained during any exercise session is the COP.
Various studies show that higher COP values are associated with more severe heart lesions in patients with congenital heart disease; higher levels of mortality in seemingly healthy male adults; and with worse prognoses in patients with heart failure. These studies all appeared within the last 7 months.
The mortality study, which Dr. Araújo coauthored, compared COP in more than 3,000 U.S. men and women who completed an exercise test from 1973 to 2018 and were tracked for an average of 23 years. Although COP was introduced as an assessment in 2012, calculating the value from tests prior to that date was possible because those tests had captured the relevant breathing rate and oxygen uptake. In males aged 18-85 years, a worse COP was significantly associated with an increased risk for earlier death. This finding did not hold for females, however; Dr. Araújo noted that more research is needed to understand the discrepancy in COP’s predictive power by sex.
In the heart failure study, everyone enrolled had heart failure and completed a COP test. People with the worse COPs also had the worst symptoms of heart failure, but completing an exercise rehabilitation program improved COP values when researchers measured them again. Dr. Araújo was also part of this study, based in the Netherlands.
“I think the COP could become a novel parameter in clinical care,” for most people, said Thijs Eijsvogels, PhD, an exercise physiologist at Radboud University in Nijmegen, the Netherlands, and the senior author of the heart failure study. That said, Dr. Eijsvogels said elite athletes will always be more interested in measuring VO2 max.
Dr. Lala agreed that tests such as the COP have some value. Her own work has shown that measuring the efficiency of someone’s breathing patterns for exhaling carbon dioxide, which can also be done without making people exercise full strength, has prognostic value for patients with advanced heart failure. Even so, she said she would like to see maximal effort tests used as much as possible.
“I worry about saying we’re going to settle for a parameter that can be achieved at 50% of peak VO2 and then we don’t exercise our patients,” Dr. Lala said.
Dr. Araújo said he plans to continue to measure VO2 max but he believes COP has utility – even for elite athletes. One of his patients is a frequent Ironman competitor who competes well despite having a solid but not amazing VO2 max level. But her COP is quite low, Dr. Araújo said, which to him suggests an especially efficient interaction between her respiratory and cardiovascular systems.
“We have a new player in the game,” Dr. Araújo said.
The sources in this study report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to clinicians who champion the assessment. The COP is easier to obtain than cardiorespiratory measures that require people to exercise to their limit, advocates say; rather than running full speed, someone can walk or lightly jog on a treadmill, with a COP value obtained easily.
But other clinicians argue that maximal exercise tests have many prognostic benefits, and that physicians should do everything in their power to push patients to exercise as hard as possible. In particular, the VO2 max test captures the maximum amount of oxygen someone uses when exercising at their capacity and is the preferred method for measuring cardiovascular endurance.
The COP is a measure of the minimum number of liters of air during breathing required to move one liter of oxygen through the bloodstream. The lower the COP the better, because this means that someone is working less strenuously than someone else to transport the same amount of oxygen, denoting a more efficient interaction between their heart and lungs.
The COP for a fit person might be 15, about 20-25 for a healthy person, and 35 for someone with heart failure, according to Claudio Gil Araújo, MD, PhD, director of research and education at CLINIMEX, an exercise medicine clinic in Rio de Janeiro.
“Max VO2 is very important, that’s indisputable. But when do you use max VO2 in your daily life? Never,” Dr. Araújo said. But almost anyone can generate a COP.
Emerging uses for the COP
“I can put someone on the treadmill or bike, and after 3 or 4 minutes I have the COP. It’s like a walking pace,” Dr. Araújo said. Yet the values are obtained with roughly half the effort as VO2 max. Other clinicians argue exercising to the limits of endurance offers unique clinical insights.
“We should do everything in our power to exercise our patients to maximum. How long a patient is able to go is really important,” said Anu Lala, MD, a cardiologist who specializes in heart failure treatment at Mount Sinai Hospital in New York. A full-capacity exercise test gives useful insights into someone’s heart rate, heart rate recovery, blood pressure, and ECG response to vigorous exercise, Dr. Lala added, all of which are important clues to someone’s overall health.
In 2012 Dr. Araújo coauthored a study that first defined the COP, which is calculated by measuring expired gasses people produce while gently exercising, perhaps to the point where they begin to perspire, and then dividing their breathing capacity by their oxygen uptake every minute. The lowest value obtained during any exercise session is the COP.
Various studies show that higher COP values are associated with more severe heart lesions in patients with congenital heart disease; higher levels of mortality in seemingly healthy male adults; and with worse prognoses in patients with heart failure. These studies all appeared within the last 7 months.
The mortality study, which Dr. Araújo coauthored, compared COP in more than 3,000 U.S. men and women who completed an exercise test from 1973 to 2018 and were tracked for an average of 23 years. Although COP was introduced as an assessment in 2012, calculating the value from tests prior to that date was possible because those tests had captured the relevant breathing rate and oxygen uptake. In males aged 18-85 years, a worse COP was significantly associated with an increased risk for earlier death. This finding did not hold for females, however; Dr. Araújo noted that more research is needed to understand the discrepancy in COP’s predictive power by sex.
In the heart failure study, everyone enrolled had heart failure and completed a COP test. People with the worse COPs also had the worst symptoms of heart failure, but completing an exercise rehabilitation program improved COP values when researchers measured them again. Dr. Araújo was also part of this study, based in the Netherlands.
“I think the COP could become a novel parameter in clinical care,” for most people, said Thijs Eijsvogels, PhD, an exercise physiologist at Radboud University in Nijmegen, the Netherlands, and the senior author of the heart failure study. That said, Dr. Eijsvogels said elite athletes will always be more interested in measuring VO2 max.
Dr. Lala agreed that tests such as the COP have some value. Her own work has shown that measuring the efficiency of someone’s breathing patterns for exhaling carbon dioxide, which can also be done without making people exercise full strength, has prognostic value for patients with advanced heart failure. Even so, she said she would like to see maximal effort tests used as much as possible.
“I worry about saying we’re going to settle for a parameter that can be achieved at 50% of peak VO2 and then we don’t exercise our patients,” Dr. Lala said.
Dr. Araújo said he plans to continue to measure VO2 max but he believes COP has utility – even for elite athletes. One of his patients is a frequent Ironman competitor who competes well despite having a solid but not amazing VO2 max level. But her COP is quite low, Dr. Araújo said, which to him suggests an especially efficient interaction between her respiratory and cardiovascular systems.
“We have a new player in the game,” Dr. Araújo said.
The sources in this study report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Low-dose oral minoxidil for hair loss soars after NYT article
.

The weekly rate of first-time low-dose oral minoxidil (LDOM) prescriptions per 10,000 outpatient encounters was “significantly higher 8 weeks after vs. 8 weeks before article publication,” at 0.9 prescriptions, compared with 0.5 per 10,000, wrote the authors of the research letter, published in JAMA Network Open. There was no similar bump for first-time finasteride or hypertension prescriptions, wrote the authors, from Harvard Medical School and Massachusetts General Hospital, Boston, and Truveta, a company that provides EHR data from U.S. health care systems.
The New York Times article noted that LDOM was relatively unknown to patients and doctors – and not approved by the Food and Drug Administration for treating hair loss – but that it was inexpensive, safe, and very effective for many individuals. “The article did not report new research findings or large-scale randomized evidence,” wrote the authors of the JAMA study.

Rodney Sinclair, MD, professor of dermatology at the University of Melbourne, who conducted the original research on LDOM and hair loss and was quoted in the Times story, told this news organization that “the sharp uplift after the New York Times article was on the back of a gradual increase.” He added that “the momentum for minoxidil prescriptions is increasing,” so much so that it has led to a global shortage of LDOM. The drug appears to still be widely available in the United States, however. It is not on the ASHP shortages list.
“There has been growing momentum for minoxidil use since I first presented our data about 6 years ago,” Dr. Sinclair said. He noted that 2022 International Society of Hair Restoration Surgery survey data found that 26% of treating physicians always or often prescribed off-label oral minoxidil, up from 10% in 2019 and 0% in 2017, while another 20% said they prescribed it sometimes.
The authors of the new study looked at prescriptions for patients at eight health care systems before and after the Times article was published in August 2022. They calculated the rate of first-time oral minoxidil prescriptions for 2.5 mg and 5 mg tablets, excluding 10 mg tablets, which are prescribed for hypertension.
Among those receiving first-time prescriptions, 2,846 received them in the 7 months before the article and 3,695 in the 5 months after publication. Men (43.6% after vs. 37.7% before publication) and White individuals (68.6% after vs. 60.8% before publication) accounted for a higher proportion of prescriptions after the article was published. There was a 2.4-fold increase in first-time prescriptions among men, and a 1.7-fold increase among females, while people with comorbidities accounted for a smaller proportion after the publication.
“Socioeconomic factors, such as access to health care and education and income levels, may be associated with individuals seeking low-dose oral minoxidil after article publication,” wrote the authors.

In an interview, Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington, said that he was not surprised to see an uptick in prescriptions after the Times article.
He and his colleagues were curious as to whether the article might have prompted newfound interest in LDOM. They experienced an uptick at George Washington, which Dr. Friedman thought could have been because he was quoted in the Times story. He and colleagues conducted a national survey of dermatologists asking if more patients had called, emailed, or come in to the office asking about LDOM after the article’s publication. “Over 85% said yes,” Dr. Friedman said in the interview. He and his coauthors also found a huge increase in Google searches for terms such as hair loss, alopecia, and minoxidil in the weeks after the article, he said.
The results are expected to published soon in the Journal of Drugs in Dermatology.
“I think a lot of people know about [LDOM] and it’s certainly has gained a lot more attention and acceptance in recent years,” said Dr. Friedman, but he added that “there’s no question” that the Times article increased interest.
That is not necessarily a bad thing, he said. “With one article, education on a common disease was disseminated worldwide in a way that no one doctor can do,” he said. The article was truthful, evidence-based, and included expert dermatologists, he noted.
“It probably got people who never thought twice about their hair thinning to actually think that there’s hope,” he said, adding that it also likely prompted them to seek care, and, more importantly, “to seek care from the person who should be taking care of this, which is the dermatologist.”
However, the article might also inspire some people to think LDOM can help when it can’t, or they might insist on a prescription when another medication is more appropriate, said Dr. Friedman.
Both he and Dr. Sinclair expect demand for LDOM to continue increasing.
“Word of mouth will drive the next wave of prescriptions,” said Dr. Sinclair. “We are continuing to do work to improve safety, to understand its mechanism of action, and identify ways to improve equity of access to treatment for men and women who are concerned about their hair loss and motivated to treat it,” he said.
Dr. Sinclair and Dr. Friedman report no relevant financial relationships.
.
The weekly rate of first-time low-dose oral minoxidil (LDOM) prescriptions per 10,000 outpatient encounters was “significantly higher 8 weeks after vs. 8 weeks before article publication,” at 0.9 prescriptions, compared with 0.5 per 10,000, wrote the authors of the research letter, published in JAMA Network Open. There was no similar bump for first-time finasteride or hypertension prescriptions, wrote the authors, from Harvard Medical School and Massachusetts General Hospital, Boston, and Truveta, a company that provides EHR data from U.S. health care systems.
The New York Times article noted that LDOM was relatively unknown to patients and doctors – and not approved by the Food and Drug Administration for treating hair loss – but that it was inexpensive, safe, and very effective for many individuals. “The article did not report new research findings or large-scale randomized evidence,” wrote the authors of the JAMA study.
Rodney Sinclair, MD, professor of dermatology at the University of Melbourne, who conducted the original research on LDOM and hair loss and was quoted in the Times story, told this news organization that “the sharp uplift after the New York Times article was on the back of a gradual increase.” He added that “the momentum for minoxidil prescriptions is increasing,” so much so that it has led to a global shortage of LDOM. The drug appears to still be widely available in the United States, however. It is not on the ASHP shortages list.
“There has been growing momentum for minoxidil use since I first presented our data about 6 years ago,” Dr. Sinclair said. He noted that 2022 International Society of Hair Restoration Surgery survey data found that 26% of treating physicians always or often prescribed off-label oral minoxidil, up from 10% in 2019 and 0% in 2017, while another 20% said they prescribed it sometimes.
The authors of the new study looked at prescriptions for patients at eight health care systems before and after the Times article was published in August 2022. They calculated the rate of first-time oral minoxidil prescriptions for 2.5 mg and 5 mg tablets, excluding 10 mg tablets, which are prescribed for hypertension.
Among those receiving first-time prescriptions, 2,846 received them in the 7 months before the article and 3,695 in the 5 months after publication. Men (43.6% after vs. 37.7% before publication) and White individuals (68.6% after vs. 60.8% before publication) accounted for a higher proportion of prescriptions after the article was published. There was a 2.4-fold increase in first-time prescriptions among men, and a 1.7-fold increase among females, while people with comorbidities accounted for a smaller proportion after the publication.
“Socioeconomic factors, such as access to health care and education and income levels, may be associated with individuals seeking low-dose oral minoxidil after article publication,” wrote the authors.
In an interview, Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington, said that he was not surprised to see an uptick in prescriptions after the Times article.
He and his colleagues were curious as to whether the article might have prompted newfound interest in LDOM. They experienced an uptick at George Washington, which Dr. Friedman thought could have been because he was quoted in the Times story. He and colleagues conducted a national survey of dermatologists asking if more patients had called, emailed, or come in to the office asking about LDOM after the article’s publication. “Over 85% said yes,” Dr. Friedman said in the interview. He and his coauthors also found a huge increase in Google searches for terms such as hair loss, alopecia, and minoxidil in the weeks after the article, he said.
The results are expected to published soon in the Journal of Drugs in Dermatology.
“I think a lot of people know about [LDOM] and it’s certainly has gained a lot more attention and acceptance in recent years,” said Dr. Friedman, but he added that “there’s no question” that the Times article increased interest.
That is not necessarily a bad thing, he said. “With one article, education on a common disease was disseminated worldwide in a way that no one doctor can do,” he said. The article was truthful, evidence-based, and included expert dermatologists, he noted.
“It probably got people who never thought twice about their hair thinning to actually think that there’s hope,” he said, adding that it also likely prompted them to seek care, and, more importantly, “to seek care from the person who should be taking care of this, which is the dermatologist.”
However, the article might also inspire some people to think LDOM can help when it can’t, or they might insist on a prescription when another medication is more appropriate, said Dr. Friedman.
Both he and Dr. Sinclair expect demand for LDOM to continue increasing.
“Word of mouth will drive the next wave of prescriptions,” said Dr. Sinclair. “We are continuing to do work to improve safety, to understand its mechanism of action, and identify ways to improve equity of access to treatment for men and women who are concerned about their hair loss and motivated to treat it,” he said.
Dr. Sinclair and Dr. Friedman report no relevant financial relationships.
.
The weekly rate of first-time low-dose oral minoxidil (LDOM) prescriptions per 10,000 outpatient encounters was “significantly higher 8 weeks after vs. 8 weeks before article publication,” at 0.9 prescriptions, compared with 0.5 per 10,000, wrote the authors of the research letter, published in JAMA Network Open. There was no similar bump for first-time finasteride or hypertension prescriptions, wrote the authors, from Harvard Medical School and Massachusetts General Hospital, Boston, and Truveta, a company that provides EHR data from U.S. health care systems.
The New York Times article noted that LDOM was relatively unknown to patients and doctors – and not approved by the Food and Drug Administration for treating hair loss – but that it was inexpensive, safe, and very effective for many individuals. “The article did not report new research findings or large-scale randomized evidence,” wrote the authors of the JAMA study.
Rodney Sinclair, MD, professor of dermatology at the University of Melbourne, who conducted the original research on LDOM and hair loss and was quoted in the Times story, told this news organization that “the sharp uplift after the New York Times article was on the back of a gradual increase.” He added that “the momentum for minoxidil prescriptions is increasing,” so much so that it has led to a global shortage of LDOM. The drug appears to still be widely available in the United States, however. It is not on the ASHP shortages list.
“There has been growing momentum for minoxidil use since I first presented our data about 6 years ago,” Dr. Sinclair said. He noted that 2022 International Society of Hair Restoration Surgery survey data found that 26% of treating physicians always or often prescribed off-label oral minoxidil, up from 10% in 2019 and 0% in 2017, while another 20% said they prescribed it sometimes.
The authors of the new study looked at prescriptions for patients at eight health care systems before and after the Times article was published in August 2022. They calculated the rate of first-time oral minoxidil prescriptions for 2.5 mg and 5 mg tablets, excluding 10 mg tablets, which are prescribed for hypertension.
Among those receiving first-time prescriptions, 2,846 received them in the 7 months before the article and 3,695 in the 5 months after publication. Men (43.6% after vs. 37.7% before publication) and White individuals (68.6% after vs. 60.8% before publication) accounted for a higher proportion of prescriptions after the article was published. There was a 2.4-fold increase in first-time prescriptions among men, and a 1.7-fold increase among females, while people with comorbidities accounted for a smaller proportion after the publication.
“Socioeconomic factors, such as access to health care and education and income levels, may be associated with individuals seeking low-dose oral minoxidil after article publication,” wrote the authors.
In an interview, Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington, said that he was not surprised to see an uptick in prescriptions after the Times article.
He and his colleagues were curious as to whether the article might have prompted newfound interest in LDOM. They experienced an uptick at George Washington, which Dr. Friedman thought could have been because he was quoted in the Times story. He and colleagues conducted a national survey of dermatologists asking if more patients had called, emailed, or come in to the office asking about LDOM after the article’s publication. “Over 85% said yes,” Dr. Friedman said in the interview. He and his coauthors also found a huge increase in Google searches for terms such as hair loss, alopecia, and minoxidil in the weeks after the article, he said.
The results are expected to published soon in the Journal of Drugs in Dermatology.
“I think a lot of people know about [LDOM] and it’s certainly has gained a lot more attention and acceptance in recent years,” said Dr. Friedman, but he added that “there’s no question” that the Times article increased interest.
That is not necessarily a bad thing, he said. “With one article, education on a common disease was disseminated worldwide in a way that no one doctor can do,” he said. The article was truthful, evidence-based, and included expert dermatologists, he noted.
“It probably got people who never thought twice about their hair thinning to actually think that there’s hope,” he said, adding that it also likely prompted them to seek care, and, more importantly, “to seek care from the person who should be taking care of this, which is the dermatologist.”
However, the article might also inspire some people to think LDOM can help when it can’t, or they might insist on a prescription when another medication is more appropriate, said Dr. Friedman.
Both he and Dr. Sinclair expect demand for LDOM to continue increasing.
“Word of mouth will drive the next wave of prescriptions,” said Dr. Sinclair. “We are continuing to do work to improve safety, to understand its mechanism of action, and identify ways to improve equity of access to treatment for men and women who are concerned about their hair loss and motivated to treat it,” he said.
Dr. Sinclair and Dr. Friedman report no relevant financial relationships.
FROM JAMA NETWORK OPEN
Increase in message volume begs the question: ‘Should we be compensated for our time?’
The American Gastroenterological Association and other gastrointestinal-specific organizations have excellent resources available to members that focus on optimizing reimbursement in your clinical and endoscopic practice.
During the COVID-19 pandemic and public health emergency (PHE), many previously noncovered services were now covered under rules of the Centers for Medicare & Medicaid Services. During the pandemic, patient portal messages increased by 157%, meaning more work for health care teams, negatively impacting physician satisfaction, and increasing burnout.1 Medical burnout has been associated with increased time spent on electronic health records, with some subspeciality gastroenterology (GI) groups having a high EHR burden, according to a recently published article in the American Journal of Gastroenterology.2

This topic is a timely discussion as several large health systems have implemented processes to bill for non–face-to-face services (termed “asynchronous care”), some of which have not been well received in the lay media. It is important to note that despite these implementations, studies have shown only 1% of all incoming portal messages would meet criteria to be submitted for reimbursement. This impact might be slightly higher in chronic care management practices.
Providers and practices have several options when considering billing for non–face-to-face encounters, which we outline in Table 1.3
The focus of this article will be to review the more common non–face-to-face evaluation and management services, such as telephone E/M (patient phone call) and e-visits (patient portal messages) as these have recently generated the most interest and discussion amongst health care providers.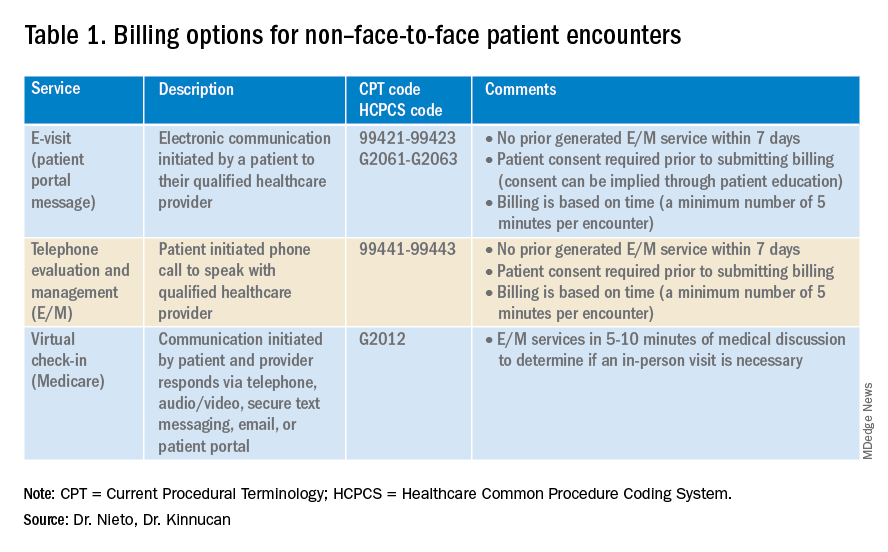
Telemedicine after COVID-19 pandemic
During the beginning of the pandemic, a web-based survey study found that almost all providers in GI practices implemented some form of telemedicine to continue to provide care for patients, compared to 32% prior to the pandemic.4,5 The high demand and essential requirement for telehealth evaluation facilitated its reimbursement, eliminating the primary barrier to previous use.6

One of the new covered benefits by CMS was asynchronous telehealth care.7 The PHE ended in May 2023, and since then a qualified health care provider (QHCP) does not have the full flexibility to deliver telemedicine services across state lines. The U.S. Department of Health and Human Services has considered some telehealth policy changes after the COVID-19 PHE and many of those will be extended, at least through 2024.8 As during the pandemic, where the U.S. national payer network (CMS, state Medicaid, and private payers) and state health agencies assisted to ensure patients get the care they need by authorizing providers to be compensated for non–face-to-face services, we believe this service will continue to be part of our clinical practice.
We recommend you stay informed about local and federal laws, regulations, and alternatives for reimbursement as they may be modified at the beginning of a new calendar year. Remember, you can always talk with your revenue cycle team to clarify any query.
Telephone evaluation and management services
The patient requests to speak with you.
Telephone evaluation and management services became more widely used after the pandemic and were recognized by CMS as a covered medical service under PHE. As outlined in Table 1, there are associated codes with this service and it can only apply to an established patient in your practice. The cumulative time spent over a 7-day period without generating an immediate follow-up visit could qualify for this CPT code. However, for a patient with a high-complexity diagnosis and/or decisions being made about care, it might be better to consider a virtual office visit as this would value the complex care at a higher level than the time spent during the telephone E/M encounter.
A common question comes up: Can my nurse or support team bill for telephone care? No, only QHCP can, which means physicians and advanced practice providers can bill for this E/M service, and it does not include time spent by other members of clinical staff in patient care. However, there are CPT codes for chronic care management, which is not covered in this article.
Virtual evaluation and management services
You respond to a patient-initiated portal message.
Patient portal messages increased exponentially during the pandemic with 2.5 more minutes spent per message, resulting in more EHR work by practitioners, compared with prior to the pandemic. One study showed an immediate postpandemic increase in EHR patient-initiated messages with no return to prepandemic baseline.1
Although studies evaluating postpandemic telemedicine services are needed, we believe that this trend will continue, and for this reason, it is important to create sustainable workflows to continue to provide this patient driven avenue of care.9
E-visits are asynchronous patient or guardian portal messages that require a minimum of 5 minutes to provide medical decision-making without prior E/M services in the last 7 days. To obtain reimbursement for this service, it cannot be initiated by the provider, and patient consent must be obtained. Documentation should include this information and the time spent in the encounter. The associated CPT codes with this e-service are outlined in Table 1.
A common question is, “Are there additional codes I should use if a portal message E/M visit lasts more than 30 minutes?” No. If an e-visit lasts more than 30 minutes, the QHCP should bill the CPT code 99423. However, we would advise that, if this care requires more than 30 minutes, then either virtual or face-to-face E/M be considered for the optimal reimbursement for provider time spent. Another common question is around consent for services, and we advise providers to review this requirement with their compliance colleagues as each institution has different policies.
Virtual check-in
Medicare also covers brief communication technology–based services also known as virtual check-ins, where patients can communicate with their provider after having established care. During this brief conversation that can be via telephone, audio/video, secure text messaging, email, or patient portal, providers will determine if an in-person visit is necessary. CMS has designed G codes for these virtual check-ins that are from the Healthcare Common Procedure Coding System (HCPCS). Two codes are available for this E/M service: G2012, which is outlined in Table 1, and G2010, which covers the evaluation of images and/or recorded videos. In order to be reimbursed for a G2010 code, providers need at least a 5-minute response to make a clinical determination or give the patient a medical impression.
Patient satisfaction, physician well-being and quality of care outcomes
Large health care systems like Kaiser Permanente implemented secure message patient-physician communication (the patient portal) even before the pandemic, showing promising results in 2010 with reduction in office visits, improvement in measurable quality outcomes, and high level of patient satisfaction.10 Post pandemic, several large health care centers opted to announce the billing implementation for patient-initiated portal messages.11 A focus was placed on educating their patients about when a message will and will not be billed. Using this type of strategy can help to improve patient awareness about potential billing without affecting patient satisfaction and care outcomes. Studies have shown the EHR has contributed to physician burnout and some physicians reducing their clinical time or leaving medicine; a reduction in messaging might have a positive impact on physician well-being.
The challenge is that medical billing is not routinely included as a curriculum topic in many residency and fellowship programs; however, trainees are part of E/M services and have limited knowledge of billing processes. Unfortunately, at this time, trainees cannot submit for reimbursement for asynchronous care as described above. We hope that this brief article will help junior gastroenterologists optimize their outpatient billing practices.
Dr. Nieto is an internal medicine chief resident with WellStar Cobb Medical Center, Austell, Ga. Dr. Kinnucan is a gastroenterologist with Mayo Clinic, Jacksonville, Fla. The authors have no conflicts of interest to disclose for this article. The authors certify that no financial and grant support has been received for this article.
References
1. Holmgren AJ et al. J Am Med Inform Assoc. 2021 Dec 9. doi: 10.1093/jamia/ocab268.
2. Bali AS et al. Am J Gastroenterol. 2023 Apr 24. doi: 10.14309/ajg.0000000000002254.
3. AAFP. Family Physician. “Coding Scenario: Coding for Virtual-Digital Visits”
4. Keihanian T. et al. Telehealth Utilization in Gastroenterology Clinics Amid the COVID-19 Pandemic: Impact on Clinical Practice and Gastroenterology Training. Gastroenterology. 2020 Jun 20. doi: 10.1053/j.gastro.2020.06.040.
5. Lewin S et al. J Crohns Colitis. 2020 Oct 21. doi: 10.1093/ecco-jcc/jjaa140.
6. Perisetti A and H Goyal. Dig Dis Sci. 2021 Mar 3. doi: 10.1007/s10620-021-06874-x.
7. Telehealth.HHS.gov. Medicaid and Medicare billing for asynchronous telehealth. Updated: 2022 May 4.
8. Telehealth.HHS.gov. Telehealth policy changes after the COVID-19 public health emergency. Last updated: 2023 Jan 23.
9. Fox B and Sizemore JO. Telehealth: Fad or the future. Epic Health Research Network. 2020 Aug 18.
10. Baer D. Patient-physician e-mail communication: the kaiser permanente experience. J Oncol Pract. 2011 Jul. doi: 10.1200/JOP.2011.000323.
11. Myclevelandclinic.org. MyChart Messaging.
12. Sinsky CA et al. J Gen Intern Med. 2022 Aug 29. doi: 10.1007/s11606-022-07766-0.
The American Gastroenterological Association and other gastrointestinal-specific organizations have excellent resources available to members that focus on optimizing reimbursement in your clinical and endoscopic practice.
During the COVID-19 pandemic and public health emergency (PHE), many previously noncovered services were now covered under rules of the Centers for Medicare & Medicaid Services. During the pandemic, patient portal messages increased by 157%, meaning more work for health care teams, negatively impacting physician satisfaction, and increasing burnout.1 Medical burnout has been associated with increased time spent on electronic health records, with some subspeciality gastroenterology (GI) groups having a high EHR burden, according to a recently published article in the American Journal of Gastroenterology.2
This topic is a timely discussion as several large health systems have implemented processes to bill for non–face-to-face services (termed “asynchronous care”), some of which have not been well received in the lay media. It is important to note that despite these implementations, studies have shown only 1% of all incoming portal messages would meet criteria to be submitted for reimbursement. This impact might be slightly higher in chronic care management practices.
Providers and practices have several options when considering billing for non–face-to-face encounters, which we outline in Table 1.3
The focus of this article will be to review the more common non–face-to-face evaluation and management services, such as telephone E/M (patient phone call) and e-visits (patient portal messages) as these have recently generated the most interest and discussion amongst health care providers.
Telemedicine after COVID-19 pandemic
During the beginning of the pandemic, a web-based survey study found that almost all providers in GI practices implemented some form of telemedicine to continue to provide care for patients, compared to 32% prior to the pandemic.4,5 The high demand and essential requirement for telehealth evaluation facilitated its reimbursement, eliminating the primary barrier to previous use.6
One of the new covered benefits by CMS was asynchronous telehealth care.7 The PHE ended in May 2023, and since then a qualified health care provider (QHCP) does not have the full flexibility to deliver telemedicine services across state lines. The U.S. Department of Health and Human Services has considered some telehealth policy changes after the COVID-19 PHE and many of those will be extended, at least through 2024.8 As during the pandemic, where the U.S. national payer network (CMS, state Medicaid, and private payers) and state health agencies assisted to ensure patients get the care they need by authorizing providers to be compensated for non–face-to-face services, we believe this service will continue to be part of our clinical practice.
We recommend you stay informed about local and federal laws, regulations, and alternatives for reimbursement as they may be modified at the beginning of a new calendar year. Remember, you can always talk with your revenue cycle team to clarify any query.
Telephone evaluation and management services
The patient requests to speak with you.
Telephone evaluation and management services became more widely used after the pandemic and were recognized by CMS as a covered medical service under PHE. As outlined in Table 1, there are associated codes with this service and it can only apply to an established patient in your practice. The cumulative time spent over a 7-day period without generating an immediate follow-up visit could qualify for this CPT code. However, for a patient with a high-complexity diagnosis and/or decisions being made about care, it might be better to consider a virtual office visit as this would value the complex care at a higher level than the time spent during the telephone E/M encounter.
A common question comes up: Can my nurse or support team bill for telephone care? No, only QHCP can, which means physicians and advanced practice providers can bill for this E/M service, and it does not include time spent by other members of clinical staff in patient care. However, there are CPT codes for chronic care management, which is not covered in this article.
Virtual evaluation and management services
You respond to a patient-initiated portal message.
Patient portal messages increased exponentially during the pandemic with 2.5 more minutes spent per message, resulting in more EHR work by practitioners, compared with prior to the pandemic. One study showed an immediate postpandemic increase in EHR patient-initiated messages with no return to prepandemic baseline.1
Although studies evaluating postpandemic telemedicine services are needed, we believe that this trend will continue, and for this reason, it is important to create sustainable workflows to continue to provide this patient driven avenue of care.9
E-visits are asynchronous patient or guardian portal messages that require a minimum of 5 minutes to provide medical decision-making without prior E/M services in the last 7 days. To obtain reimbursement for this service, it cannot be initiated by the provider, and patient consent must be obtained. Documentation should include this information and the time spent in the encounter. The associated CPT codes with this e-service are outlined in Table 1.
A common question is, “Are there additional codes I should use if a portal message E/M visit lasts more than 30 minutes?” No. If an e-visit lasts more than 30 minutes, the QHCP should bill the CPT code 99423. However, we would advise that, if this care requires more than 30 minutes, then either virtual or face-to-face E/M be considered for the optimal reimbursement for provider time spent. Another common question is around consent for services, and we advise providers to review this requirement with their compliance colleagues as each institution has different policies.
Virtual check-in
Medicare also covers brief communication technology–based services also known as virtual check-ins, where patients can communicate with their provider after having established care. During this brief conversation that can be via telephone, audio/video, secure text messaging, email, or patient portal, providers will determine if an in-person visit is necessary. CMS has designed G codes for these virtual check-ins that are from the Healthcare Common Procedure Coding System (HCPCS). Two codes are available for this E/M service: G2012, which is outlined in Table 1, and G2010, which covers the evaluation of images and/or recorded videos. In order to be reimbursed for a G2010 code, providers need at least a 5-minute response to make a clinical determination or give the patient a medical impression.
Patient satisfaction, physician well-being and quality of care outcomes
Large health care systems like Kaiser Permanente implemented secure message patient-physician communication (the patient portal) even before the pandemic, showing promising results in 2010 with reduction in office visits, improvement in measurable quality outcomes, and high level of patient satisfaction.10 Post pandemic, several large health care centers opted to announce the billing implementation for patient-initiated portal messages.11 A focus was placed on educating their patients about when a message will and will not be billed. Using this type of strategy can help to improve patient awareness about potential billing without affecting patient satisfaction and care outcomes. Studies have shown the EHR has contributed to physician burnout and some physicians reducing their clinical time or leaving medicine; a reduction in messaging might have a positive impact on physician well-being.
The challenge is that medical billing is not routinely included as a curriculum topic in many residency and fellowship programs; however, trainees are part of E/M services and have limited knowledge of billing processes. Unfortunately, at this time, trainees cannot submit for reimbursement for asynchronous care as described above. We hope that this brief article will help junior gastroenterologists optimize their outpatient billing practices.
Dr. Nieto is an internal medicine chief resident with WellStar Cobb Medical Center, Austell, Ga. Dr. Kinnucan is a gastroenterologist with Mayo Clinic, Jacksonville, Fla. The authors have no conflicts of interest to disclose for this article. The authors certify that no financial and grant support has been received for this article.
References
1. Holmgren AJ et al. J Am Med Inform Assoc. 2021 Dec 9. doi: 10.1093/jamia/ocab268.
2. Bali AS et al. Am J Gastroenterol. 2023 Apr 24. doi: 10.14309/ajg.0000000000002254.
3. AAFP. Family Physician. “Coding Scenario: Coding for Virtual-Digital Visits”
4. Keihanian T. et al. Telehealth Utilization in Gastroenterology Clinics Amid the COVID-19 Pandemic: Impact on Clinical Practice and Gastroenterology Training. Gastroenterology. 2020 Jun 20. doi: 10.1053/j.gastro.2020.06.040.
5. Lewin S et al. J Crohns Colitis. 2020 Oct 21. doi: 10.1093/ecco-jcc/jjaa140.
6. Perisetti A and H Goyal. Dig Dis Sci. 2021 Mar 3. doi: 10.1007/s10620-021-06874-x.
7. Telehealth.HHS.gov. Medicaid and Medicare billing for asynchronous telehealth. Updated: 2022 May 4.
8. Telehealth.HHS.gov. Telehealth policy changes after the COVID-19 public health emergency. Last updated: 2023 Jan 23.
9. Fox B and Sizemore JO. Telehealth: Fad or the future. Epic Health Research Network. 2020 Aug 18.
10. Baer D. Patient-physician e-mail communication: the kaiser permanente experience. J Oncol Pract. 2011 Jul. doi: 10.1200/JOP.2011.000323.
11. Myclevelandclinic.org. MyChart Messaging.
12. Sinsky CA et al. J Gen Intern Med. 2022 Aug 29. doi: 10.1007/s11606-022-07766-0.
The American Gastroenterological Association and other gastrointestinal-specific organizations have excellent resources available to members that focus on optimizing reimbursement in your clinical and endoscopic practice.
During the COVID-19 pandemic and public health emergency (PHE), many previously noncovered services were now covered under rules of the Centers for Medicare & Medicaid Services. During the pandemic, patient portal messages increased by 157%, meaning more work for health care teams, negatively impacting physician satisfaction, and increasing burnout.1 Medical burnout has been associated with increased time spent on electronic health records, with some subspeciality gastroenterology (GI) groups having a high EHR burden, according to a recently published article in the American Journal of Gastroenterology.2
This topic is a timely discussion as several large health systems have implemented processes to bill for non–face-to-face services (termed “asynchronous care”), some of which have not been well received in the lay media. It is important to note that despite these implementations, studies have shown only 1% of all incoming portal messages would meet criteria to be submitted for reimbursement. This impact might be slightly higher in chronic care management practices.
Providers and practices have several options when considering billing for non–face-to-face encounters, which we outline in Table 1.3
The focus of this article will be to review the more common non–face-to-face evaluation and management services, such as telephone E/M (patient phone call) and e-visits (patient portal messages) as these have recently generated the most interest and discussion amongst health care providers.
Telemedicine after COVID-19 pandemic
During the beginning of the pandemic, a web-based survey study found that almost all providers in GI practices implemented some form of telemedicine to continue to provide care for patients, compared to 32% prior to the pandemic.4,5 The high demand and essential requirement for telehealth evaluation facilitated its reimbursement, eliminating the primary barrier to previous use.6
One of the new covered benefits by CMS was asynchronous telehealth care.7 The PHE ended in May 2023, and since then a qualified health care provider (QHCP) does not have the full flexibility to deliver telemedicine services across state lines. The U.S. Department of Health and Human Services has considered some telehealth policy changes after the COVID-19 PHE and many of those will be extended, at least through 2024.8 As during the pandemic, where the U.S. national payer network (CMS, state Medicaid, and private payers) and state health agencies assisted to ensure patients get the care they need by authorizing providers to be compensated for non–face-to-face services, we believe this service will continue to be part of our clinical practice.
We recommend you stay informed about local and federal laws, regulations, and alternatives for reimbursement as they may be modified at the beginning of a new calendar year. Remember, you can always talk with your revenue cycle team to clarify any query.
Telephone evaluation and management services
The patient requests to speak with you.
Telephone evaluation and management services became more widely used after the pandemic and were recognized by CMS as a covered medical service under PHE. As outlined in Table 1, there are associated codes with this service and it can only apply to an established patient in your practice. The cumulative time spent over a 7-day period without generating an immediate follow-up visit could qualify for this CPT code. However, for a patient with a high-complexity diagnosis and/or decisions being made about care, it might be better to consider a virtual office visit as this would value the complex care at a higher level than the time spent during the telephone E/M encounter.
A common question comes up: Can my nurse or support team bill for telephone care? No, only QHCP can, which means physicians and advanced practice providers can bill for this E/M service, and it does not include time spent by other members of clinical staff in patient care. However, there are CPT codes for chronic care management, which is not covered in this article.
Virtual evaluation and management services
You respond to a patient-initiated portal message.
Patient portal messages increased exponentially during the pandemic with 2.5 more minutes spent per message, resulting in more EHR work by practitioners, compared with prior to the pandemic. One study showed an immediate postpandemic increase in EHR patient-initiated messages with no return to prepandemic baseline.1
Although studies evaluating postpandemic telemedicine services are needed, we believe that this trend will continue, and for this reason, it is important to create sustainable workflows to continue to provide this patient driven avenue of care.9
E-visits are asynchronous patient or guardian portal messages that require a minimum of 5 minutes to provide medical decision-making without prior E/M services in the last 7 days. To obtain reimbursement for this service, it cannot be initiated by the provider, and patient consent must be obtained. Documentation should include this information and the time spent in the encounter. The associated CPT codes with this e-service are outlined in Table 1.
A common question is, “Are there additional codes I should use if a portal message E/M visit lasts more than 30 minutes?” No. If an e-visit lasts more than 30 minutes, the QHCP should bill the CPT code 99423. However, we would advise that, if this care requires more than 30 minutes, then either virtual or face-to-face E/M be considered for the optimal reimbursement for provider time spent. Another common question is around consent for services, and we advise providers to review this requirement with their compliance colleagues as each institution has different policies.
Virtual check-in
Medicare also covers brief communication technology–based services also known as virtual check-ins, where patients can communicate with their provider after having established care. During this brief conversation that can be via telephone, audio/video, secure text messaging, email, or patient portal, providers will determine if an in-person visit is necessary. CMS has designed G codes for these virtual check-ins that are from the Healthcare Common Procedure Coding System (HCPCS). Two codes are available for this E/M service: G2012, which is outlined in Table 1, and G2010, which covers the evaluation of images and/or recorded videos. In order to be reimbursed for a G2010 code, providers need at least a 5-minute response to make a clinical determination or give the patient a medical impression.
Patient satisfaction, physician well-being and quality of care outcomes
Large health care systems like Kaiser Permanente implemented secure message patient-physician communication (the patient portal) even before the pandemic, showing promising results in 2010 with reduction in office visits, improvement in measurable quality outcomes, and high level of patient satisfaction.10 Post pandemic, several large health care centers opted to announce the billing implementation for patient-initiated portal messages.11 A focus was placed on educating their patients about when a message will and will not be billed. Using this type of strategy can help to improve patient awareness about potential billing without affecting patient satisfaction and care outcomes. Studies have shown the EHR has contributed to physician burnout and some physicians reducing their clinical time or leaving medicine; a reduction in messaging might have a positive impact on physician well-being.
The challenge is that medical billing is not routinely included as a curriculum topic in many residency and fellowship programs; however, trainees are part of E/M services and have limited knowledge of billing processes. Unfortunately, at this time, trainees cannot submit for reimbursement for asynchronous care as described above. We hope that this brief article will help junior gastroenterologists optimize their outpatient billing practices.
Dr. Nieto is an internal medicine chief resident with WellStar Cobb Medical Center, Austell, Ga. Dr. Kinnucan is a gastroenterologist with Mayo Clinic, Jacksonville, Fla. The authors have no conflicts of interest to disclose for this article. The authors certify that no financial and grant support has been received for this article.
References
1. Holmgren AJ et al. J Am Med Inform Assoc. 2021 Dec 9. doi: 10.1093/jamia/ocab268.
2. Bali AS et al. Am J Gastroenterol. 2023 Apr 24. doi: 10.14309/ajg.0000000000002254.
3. AAFP. Family Physician. “Coding Scenario: Coding for Virtual-Digital Visits”
4. Keihanian T. et al. Telehealth Utilization in Gastroenterology Clinics Amid the COVID-19 Pandemic: Impact on Clinical Practice and Gastroenterology Training. Gastroenterology. 2020 Jun 20. doi: 10.1053/j.gastro.2020.06.040.
5. Lewin S et al. J Crohns Colitis. 2020 Oct 21. doi: 10.1093/ecco-jcc/jjaa140.
6. Perisetti A and H Goyal. Dig Dis Sci. 2021 Mar 3. doi: 10.1007/s10620-021-06874-x.
7. Telehealth.HHS.gov. Medicaid and Medicare billing for asynchronous telehealth. Updated: 2022 May 4.
8. Telehealth.HHS.gov. Telehealth policy changes after the COVID-19 public health emergency. Last updated: 2023 Jan 23.
9. Fox B and Sizemore JO. Telehealth: Fad or the future. Epic Health Research Network. 2020 Aug 18.
10. Baer D. Patient-physician e-mail communication: the kaiser permanente experience. J Oncol Pract. 2011 Jul. doi: 10.1200/JOP.2011.000323.
11. Myclevelandclinic.org. MyChart Messaging.
12. Sinsky CA et al. J Gen Intern Med. 2022 Aug 29. doi: 10.1007/s11606-022-07766-0.
Applications of ChatGPT and Large Language Models in Medicine and Health Care: Benefits and Pitfalls
The development of [artificial intelligence] is as fundamental as the creation of the microprocessor, the personal computer, the Internet, and the mobile phone. It will change the way people work, learn, travel, get health care, and communicate with each other.
Bill Gates 1
As the world emerges from the pandemic and the health care system faces new challenges, technology has become an increasingly important tool for health care professionals (HCPs). One such technology is the large language model (LLM), which has the potential to revolutionize the health care industry. ChatGPT, a popular LLM developed by OpenAI, has gained particular attention in the medical community for its ability to pass the United States Medical Licensing Exam.2 This article will explore the benefits and potential pitfalls of using LLMs like ChatGPT in medicine and health care.
Benefits
HCP burnout is a serious issue that can lead to lower productivity, increased medical errors, and decreased patient satisfaction.3 LLMs can alleviate some administrative burdens on HCPs, allowing them to focus on patient care. By assisting with billing, coding, insurance claims, and organizing schedules, LLMs like ChatGPT can free up time for HCPs to focus on what they do best: providing quality patient care.4 ChatGPT also can assist with diagnoses by providing accurate and reliable information based on a vast amount of clinical data. By learning the relationships between different medical conditions, symptoms, and treatment options, ChatGPT can provide an appropriate differential diagnosis (Figure 1). 
Imaging medical specialists like radiologists, pathologists, dermatologists, and others can benefit from combining computer vision diagnostics with ChatGPT report creation abilities to streamline the diagnostic workflow and improve diagnostic accuracy (Figure 2). 
Although using ChatGPT and other LLMs in mental health care has potential benefits, it is essential to note that they are not a substitute for human interaction and personalized care. While ChatGPT can remember information from previous conversations, it cannot provide the same level of personalized, high-quality care that a professional therapist or HCP can. However, by augmenting the work of HCPs, ChatGPT and other LLMs have the potential to make mental health care more accessible and efficient. In addition to providing effective screening in underserved areas, ChatGPT technology may improve the competence of physician assistants and nurse practitioners in delivering mental health care. With the increased incidence of mental health problems in veterans, the pertinence of a ChatGPT-like feature will only increase with time.9
ChatGPT can also be integrated into health care organizations’ websites and mobile apps, providing patients instant access to medical information, self-care advice, symptom checkers, scheduling appointments, and arranging transportation. These features can reduce the burden on health care staff and help patients stay informed and motivated to take an active role in their health. Additionally, health care organizations can use ChatGPT to engage patients by providing reminders for medication renewals and assistance with self-care.4,6,10,11
The potential of artificial intelligence (AI) in the field of medical education and research is immense. According to a study by Gilson and colleagues, ChatGPT has shown promising results as a medical education tool.12 ChatGPT can simulate clinical scenarios, provide real-time feedback, and improve diagnostic skills. It also offers new interactive and personalized learning opportunities for medical students and HCPs.13 ChatGPT can help researchers by streamlining the process of data analysis. It can also administer surveys or questionnaires, facilitate data collection on preferences and experiences, and help in writing scientific publications.14 Nevertheless, to fully unlock the potential of these AI models, additional models that perform checks for factual accuracy, plagiarism, and copyright infringement must be developed.15,16
AI Bill of Rights
In order to protect the American public, the White House Office of Science and Technology Policy (OSTP) has released a blueprint for an AI Bill of Rights that emphasizes 5 principles to protect the public from the harmful effects of AI models, including safe and effective systems; algorithmic discrimination protection; data privacy; notice and explanation; and human alternatives, considerations, and fallback (Figure 3).17 
One of the biggest challenges with LLMs like ChatGPT is the prevalence of inaccurate information or so-called hallucinations.16 These inaccuracies stem from the inability of LLMs to distinguish between real and fake information. To prevent hallucinations, researchers have proposed several methods, including training models on more diverse data, using adversarial training methods, and human-in-the-loop approaches.21 In addition, medicine-specific models like GatorTron, medPaLM, and Almanac were developed, increasing the accuracy of factual results.22-24 Unfortunately, only the GatorTron model is available to the public through the NVIDIA developers’ program.25
Despite these shortcomings, the future of LLMs in health care is promising. Although these models will not replace HCPs, they can help reduce the unnecessary burden on them, prevent burnout, and enable HCPs and patients spend more time together. Establishing an official hospital AI oversight governing body that would promote best practices could ensure the trustworthy implementation of these new technologies.26
Conclusions
The use of ChatGPT and other LLMs in health care has the potential to revolutionize the industry. By assisting HCPs with administrative tasks, improving the accuracy and reliability of diagnoses, and engaging patients, ChatGPT can help health care organizations provide better care to their patients. While LLMs are not a substitute for human interaction and personalized care, they can augment the work of HCPs, making health care more accessible and efficient. As the health care industry continues to evolve, it will be exciting to see how ChatGPT and other LLMs are used to improve patient outcomes and quality of care. In addition, AI technologies like ChatGPT offer enormous potential in medical education and research. To ensure that the benefits outweigh the risks, developing trustworthy AI health care products and establishing oversight governing bodies to ensure their implementation is essential. By doing so, we can help HCPs focus on what matters most, providing high-quality care to patients.
Acknowledgments
This material is the result of work supported by resources and the use of facilities at the James A. Haley Veterans’ Hospital.
1. Bill Gates. The age of AI has begun. March 21, 2023. Accessed May 10, 2023. https://www.gatesnotes.com/the-age-of-ai-has-begun
2. Kung TH, Cheatham M, Medenilla A, et al. Performance of ChatGPT on USMLE: Potential for AI-assisted medical education using large language models. PLOS Digit Health. 2023;2(2):e0000198. Published 2023 Feb 9. doi:10.1371/journal.pdig.0000198
3. Shanafelt TD, West CP, Sinsky C, et al. Changes in burnout and satisfaction with work-life integration in physicians and the general US working population between 2011 and 2020. Mayo Clin Proc. 2022;97(3):491-506. doi:10.1016/j.mayocp.2021.11.021
4. Goodman RS, Patrinely JR Jr, Osterman T, Wheless L, Johnson DB. On the cusp: considering the impact of artificial intelligence language models in healthcare. Med. 2023;4(3):139-140. doi:10.1016/j.medj.2023.02.008
5. Will ChatGPT transform healthcare? Nat Med. 2023;29(3):505-506. doi:10.1038/s41591-023-02289-5
6. Hopkins AM, Logan JM, Kichenadasse G, Sorich MJ. Artificial intelligence chatbots will revolutionize how cancer patients access information: ChatGPT represents a paradigm-shift. JNCI Cancer Spectr. 2023;7(2):pkad010. doi:10.1093/jncics/pkad010
7. Babar Z, van Laarhoven T, Zanzotto FM, Marchiori E. Evaluating diagnostic content of AI-generated radiology reports of chest X-rays. Artif Intell Med. 2021;116:102075. doi:10.1016/j.artmed.2021.102075
8. Lecler A, Duron L, Soyer P. Revolutionizing radiology with GPT-based models: current applications, future possibilities and limitations of ChatGPT. Diagn Interv Imaging. 2023;S2211-5684(23)00027-X. doi:10.1016/j.diii.2023.02.003
9. Germain JM. Is ChatGPT smart enough to practice mental health therapy? March 23, 2023. Accessed May 11, 2023. https://www.technewsworld.com/story/is-chatgpt-smart-enough-to-practice-mental-health-therapy-178064.html
10. Cascella M, Montomoli J, Bellini V, Bignami E. Evaluating the feasibility of ChatGPT in healthcare: an analysis of multiple clinical and research scenarios. J Med Syst. 2023;47(1):33. Published 2023 Mar 4. doi:10.1007/s10916-023-01925-4
11. Jungwirth D, Haluza D. Artificial intelligence and public health: an exploratory study. Int J Environ Res Public Health. 2023;20(5):4541. Published 2023 Mar 3. doi:10.3390/ijerph20054541
12. Gilson A, Safranek CW, Huang T, et al. How does ChatGPT perform on the United States Medical Licensing Examination? The implications of large language models for medical education and knowledge assessment. JMIR Med Educ. 2023;9:e45312. Published 2023 Feb 8. doi:10.2196/45312
13. Eysenbach G. The role of ChatGPT, generative language models, and artificial intelligence in medical education: a conversation with ChatGPT and a call for papers. JMIR Med Educ. 2023;9:e46885. Published 2023 Mar 6. doi:10.2196/46885
14. Macdonald C, Adeloye D, Sheikh A, Rudan I. Can ChatGPT draft a research article? An example of population-level vaccine effectiveness analysis. J Glob Health. 2023;13:01003. Published 2023 Feb 17. doi:10.7189/jogh.13.01003
15. Masters K. Ethical use of artificial intelligence in health professions education: AMEE Guide No.158. Med Teach. 2023;1-11. doi:10.1080/0142159X.2023.2186203
16. Smith CS. Hallucinations could blunt ChatGPT’s success. IEEE Spectrum. March 13, 2023. Accessed May 11, 2023. https://spectrum.ieee.org/ai-hallucination
17. Executive Office of the President, Office of Science and Technology Policy. Blueprint for an AI Bill of Rights. Accessed May 11, 2023. https://www.whitehouse.gov/ostp/ai-bill-of-rights
18. Executive office of the President. Executive Order 13960: promoting the use of trustworthy artificial intelligence in the federal government. Fed Regist. 2020;89(236):78939-78943.
19. US Department of Commerce, National institute of Standards and Technology. Artificial Intelligence Risk Management Framework (AI RMF 1.0). Published January 2023. doi:10.6028/NIST.AI.100-1
20. Microsoft. Azure Cognitive Search—Cloud Search Service. Accessed May 11, 2023. https://azure.microsoft.com/en-us/products/search
21. Aiyappa R, An J, Kwak H, Ahn YY. Can we trust the evaluation on ChatGPT? March 22, 2023. Accessed May 11, 2023. https://arxiv.org/abs/2303.12767v1
22. Yang X, Chen A, Pournejatian N, et al. GatorTron: a large clinical language model to unlock patient information from unstructured electronic health records. Updated December 16, 2022. Accessed May 11, 2023. https://arxiv.org/abs/2203.03540v3
23. Singhal K, Azizi S, Tu T, et al. Large language models encode clinical knowledge. December 26, 2022. Accessed May 11, 2023. https://arxiv.org/abs/2212.13138v1
24. Zakka C, Chaurasia A, Shad R, Hiesinger W. Almanac: knowledge-grounded language models for clinical medicine. March 1, 2023. Accessed May 11, 2023. https://arxiv.org/abs/2303.01229v1
25. NVIDIA. GatorTron-OG. Accessed May 11, 2023. https://catalog.ngc.nvidia.com/orgs/nvidia/teams/clara/models/gatortron_og
26. Borkowski AA, Jakey CE, Thomas LB, Viswanadhan N, Mastorides SM. Establishing a hospital artificial intelligence committee to improve patient care. Fed Pract. 2022;39(8):334-336. doi:10.12788/fp.0299
The development of [artificial intelligence] is as fundamental as the creation of the microprocessor, the personal computer, the Internet, and the mobile phone. It will change the way people work, learn, travel, get health care, and communicate with each other.
Bill Gates 1
As the world emerges from the pandemic and the health care system faces new challenges, technology has become an increasingly important tool for health care professionals (HCPs). One such technology is the large language model (LLM), which has the potential to revolutionize the health care industry. ChatGPT, a popular LLM developed by OpenAI, has gained particular attention in the medical community for its ability to pass the United States Medical Licensing Exam.2 This article will explore the benefits and potential pitfalls of using LLMs like ChatGPT in medicine and health care.
Benefits
HCP burnout is a serious issue that can lead to lower productivity, increased medical errors, and decreased patient satisfaction.3 LLMs can alleviate some administrative burdens on HCPs, allowing them to focus on patient care. By assisting with billing, coding, insurance claims, and organizing schedules, LLMs like ChatGPT can free up time for HCPs to focus on what they do best: providing quality patient care.4 ChatGPT also can assist with diagnoses by providing accurate and reliable information based on a vast amount of clinical data. By learning the relationships between different medical conditions, symptoms, and treatment options, ChatGPT can provide an appropriate differential diagnosis (Figure 1).
Imaging medical specialists like radiologists, pathologists, dermatologists, and others can benefit from combining computer vision diagnostics with ChatGPT report creation abilities to streamline the diagnostic workflow and improve diagnostic accuracy (Figure 2).
Although using ChatGPT and other LLMs in mental health care has potential benefits, it is essential to note that they are not a substitute for human interaction and personalized care. While ChatGPT can remember information from previous conversations, it cannot provide the same level of personalized, high-quality care that a professional therapist or HCP can. However, by augmenting the work of HCPs, ChatGPT and other LLMs have the potential to make mental health care more accessible and efficient. In addition to providing effective screening in underserved areas, ChatGPT technology may improve the competence of physician assistants and nurse practitioners in delivering mental health care. With the increased incidence of mental health problems in veterans, the pertinence of a ChatGPT-like feature will only increase with time.9
ChatGPT can also be integrated into health care organizations’ websites and mobile apps, providing patients instant access to medical information, self-care advice, symptom checkers, scheduling appointments, and arranging transportation. These features can reduce the burden on health care staff and help patients stay informed and motivated to take an active role in their health. Additionally, health care organizations can use ChatGPT to engage patients by providing reminders for medication renewals and assistance with self-care.4,6,10,11
The potential of artificial intelligence (AI) in the field of medical education and research is immense. According to a study by Gilson and colleagues, ChatGPT has shown promising results as a medical education tool.12 ChatGPT can simulate clinical scenarios, provide real-time feedback, and improve diagnostic skills. It also offers new interactive and personalized learning opportunities for medical students and HCPs.13 ChatGPT can help researchers by streamlining the process of data analysis. It can also administer surveys or questionnaires, facilitate data collection on preferences and experiences, and help in writing scientific publications.14 Nevertheless, to fully unlock the potential of these AI models, additional models that perform checks for factual accuracy, plagiarism, and copyright infringement must be developed.15,16
AI Bill of Rights
In order to protect the American public, the White House Office of Science and Technology Policy (OSTP) has released a blueprint for an AI Bill of Rights that emphasizes 5 principles to protect the public from the harmful effects of AI models, including safe and effective systems; algorithmic discrimination protection; data privacy; notice and explanation; and human alternatives, considerations, and fallback (Figure 3).17
One of the biggest challenges with LLMs like ChatGPT is the prevalence of inaccurate information or so-called hallucinations.16 These inaccuracies stem from the inability of LLMs to distinguish between real and fake information. To prevent hallucinations, researchers have proposed several methods, including training models on more diverse data, using adversarial training methods, and human-in-the-loop approaches.21 In addition, medicine-specific models like GatorTron, medPaLM, and Almanac were developed, increasing the accuracy of factual results.22-24 Unfortunately, only the GatorTron model is available to the public through the NVIDIA developers’ program.25
Despite these shortcomings, the future of LLMs in health care is promising. Although these models will not replace HCPs, they can help reduce the unnecessary burden on them, prevent burnout, and enable HCPs and patients spend more time together. Establishing an official hospital AI oversight governing body that would promote best practices could ensure the trustworthy implementation of these new technologies.26
Conclusions
The use of ChatGPT and other LLMs in health care has the potential to revolutionize the industry. By assisting HCPs with administrative tasks, improving the accuracy and reliability of diagnoses, and engaging patients, ChatGPT can help health care organizations provide better care to their patients. While LLMs are not a substitute for human interaction and personalized care, they can augment the work of HCPs, making health care more accessible and efficient. As the health care industry continues to evolve, it will be exciting to see how ChatGPT and other LLMs are used to improve patient outcomes and quality of care. In addition, AI technologies like ChatGPT offer enormous potential in medical education and research. To ensure that the benefits outweigh the risks, developing trustworthy AI health care products and establishing oversight governing bodies to ensure their implementation is essential. By doing so, we can help HCPs focus on what matters most, providing high-quality care to patients.
Acknowledgments
This material is the result of work supported by resources and the use of facilities at the James A. Haley Veterans’ Hospital.
The development of [artificial intelligence] is as fundamental as the creation of the microprocessor, the personal computer, the Internet, and the mobile phone. It will change the way people work, learn, travel, get health care, and communicate with each other.
Bill Gates 1
As the world emerges from the pandemic and the health care system faces new challenges, technology has become an increasingly important tool for health care professionals (HCPs). One such technology is the large language model (LLM), which has the potential to revolutionize the health care industry. ChatGPT, a popular LLM developed by OpenAI, has gained particular attention in the medical community for its ability to pass the United States Medical Licensing Exam.2 This article will explore the benefits and potential pitfalls of using LLMs like ChatGPT in medicine and health care.
Benefits
HCP burnout is a serious issue that can lead to lower productivity, increased medical errors, and decreased patient satisfaction.3 LLMs can alleviate some administrative burdens on HCPs, allowing them to focus on patient care. By assisting with billing, coding, insurance claims, and organizing schedules, LLMs like ChatGPT can free up time for HCPs to focus on what they do best: providing quality patient care.4 ChatGPT also can assist with diagnoses by providing accurate and reliable information based on a vast amount of clinical data. By learning the relationships between different medical conditions, symptoms, and treatment options, ChatGPT can provide an appropriate differential diagnosis (Figure 1).
Imaging medical specialists like radiologists, pathologists, dermatologists, and others can benefit from combining computer vision diagnostics with ChatGPT report creation abilities to streamline the diagnostic workflow and improve diagnostic accuracy (Figure 2).
Although using ChatGPT and other LLMs in mental health care has potential benefits, it is essential to note that they are not a substitute for human interaction and personalized care. While ChatGPT can remember information from previous conversations, it cannot provide the same level of personalized, high-quality care that a professional therapist or HCP can. However, by augmenting the work of HCPs, ChatGPT and other LLMs have the potential to make mental health care more accessible and efficient. In addition to providing effective screening in underserved areas, ChatGPT technology may improve the competence of physician assistants and nurse practitioners in delivering mental health care. With the increased incidence of mental health problems in veterans, the pertinence of a ChatGPT-like feature will only increase with time.9
ChatGPT can also be integrated into health care organizations’ websites and mobile apps, providing patients instant access to medical information, self-care advice, symptom checkers, scheduling appointments, and arranging transportation. These features can reduce the burden on health care staff and help patients stay informed and motivated to take an active role in their health. Additionally, health care organizations can use ChatGPT to engage patients by providing reminders for medication renewals and assistance with self-care.4,6,10,11
The potential of artificial intelligence (AI) in the field of medical education and research is immense. According to a study by Gilson and colleagues, ChatGPT has shown promising results as a medical education tool.12 ChatGPT can simulate clinical scenarios, provide real-time feedback, and improve diagnostic skills. It also offers new interactive and personalized learning opportunities for medical students and HCPs.13 ChatGPT can help researchers by streamlining the process of data analysis. It can also administer surveys or questionnaires, facilitate data collection on preferences and experiences, and help in writing scientific publications.14 Nevertheless, to fully unlock the potential of these AI models, additional models that perform checks for factual accuracy, plagiarism, and copyright infringement must be developed.15,16
AI Bill of Rights
In order to protect the American public, the White House Office of Science and Technology Policy (OSTP) has released a blueprint for an AI Bill of Rights that emphasizes 5 principles to protect the public from the harmful effects of AI models, including safe and effective systems; algorithmic discrimination protection; data privacy; notice and explanation; and human alternatives, considerations, and fallback (Figure 3).17
One of the biggest challenges with LLMs like ChatGPT is the prevalence of inaccurate information or so-called hallucinations.16 These inaccuracies stem from the inability of LLMs to distinguish between real and fake information. To prevent hallucinations, researchers have proposed several methods, including training models on more diverse data, using adversarial training methods, and human-in-the-loop approaches.21 In addition, medicine-specific models like GatorTron, medPaLM, and Almanac were developed, increasing the accuracy of factual results.22-24 Unfortunately, only the GatorTron model is available to the public through the NVIDIA developers’ program.25
Despite these shortcomings, the future of LLMs in health care is promising. Although these models will not replace HCPs, they can help reduce the unnecessary burden on them, prevent burnout, and enable HCPs and patients spend more time together. Establishing an official hospital AI oversight governing body that would promote best practices could ensure the trustworthy implementation of these new technologies.26
Conclusions
The use of ChatGPT and other LLMs in health care has the potential to revolutionize the industry. By assisting HCPs with administrative tasks, improving the accuracy and reliability of diagnoses, and engaging patients, ChatGPT can help health care organizations provide better care to their patients. While LLMs are not a substitute for human interaction and personalized care, they can augment the work of HCPs, making health care more accessible and efficient. As the health care industry continues to evolve, it will be exciting to see how ChatGPT and other LLMs are used to improve patient outcomes and quality of care. In addition, AI technologies like ChatGPT offer enormous potential in medical education and research. To ensure that the benefits outweigh the risks, developing trustworthy AI health care products and establishing oversight governing bodies to ensure their implementation is essential. By doing so, we can help HCPs focus on what matters most, providing high-quality care to patients.
Acknowledgments
This material is the result of work supported by resources and the use of facilities at the James A. Haley Veterans’ Hospital.
1. Bill Gates. The age of AI has begun. March 21, 2023. Accessed May 10, 2023. https://www.gatesnotes.com/the-age-of-ai-has-begun
2. Kung TH, Cheatham M, Medenilla A, et al. Performance of ChatGPT on USMLE: Potential for AI-assisted medical education using large language models. PLOS Digit Health. 2023;2(2):e0000198. Published 2023 Feb 9. doi:10.1371/journal.pdig.0000198
3. Shanafelt TD, West CP, Sinsky C, et al. Changes in burnout and satisfaction with work-life integration in physicians and the general US working population between 2011 and 2020. Mayo Clin Proc. 2022;97(3):491-506. doi:10.1016/j.mayocp.2021.11.021
4. Goodman RS, Patrinely JR Jr, Osterman T, Wheless L, Johnson DB. On the cusp: considering the impact of artificial intelligence language models in healthcare. Med. 2023;4(3):139-140. doi:10.1016/j.medj.2023.02.008
5. Will ChatGPT transform healthcare? Nat Med. 2023;29(3):505-506. doi:10.1038/s41591-023-02289-5
6. Hopkins AM, Logan JM, Kichenadasse G, Sorich MJ. Artificial intelligence chatbots will revolutionize how cancer patients access information: ChatGPT represents a paradigm-shift. JNCI Cancer Spectr. 2023;7(2):pkad010. doi:10.1093/jncics/pkad010
7. Babar Z, van Laarhoven T, Zanzotto FM, Marchiori E. Evaluating diagnostic content of AI-generated radiology reports of chest X-rays. Artif Intell Med. 2021;116:102075. doi:10.1016/j.artmed.2021.102075
8. Lecler A, Duron L, Soyer P. Revolutionizing radiology with GPT-based models: current applications, future possibilities and limitations of ChatGPT. Diagn Interv Imaging. 2023;S2211-5684(23)00027-X. doi:10.1016/j.diii.2023.02.003
9. Germain JM. Is ChatGPT smart enough to practice mental health therapy? March 23, 2023. Accessed May 11, 2023. https://www.technewsworld.com/story/is-chatgpt-smart-enough-to-practice-mental-health-therapy-178064.html
10. Cascella M, Montomoli J, Bellini V, Bignami E. Evaluating the feasibility of ChatGPT in healthcare: an analysis of multiple clinical and research scenarios. J Med Syst. 2023;47(1):33. Published 2023 Mar 4. doi:10.1007/s10916-023-01925-4
11. Jungwirth D, Haluza D. Artificial intelligence and public health: an exploratory study. Int J Environ Res Public Health. 2023;20(5):4541. Published 2023 Mar 3. doi:10.3390/ijerph20054541
12. Gilson A, Safranek CW, Huang T, et al. How does ChatGPT perform on the United States Medical Licensing Examination? The implications of large language models for medical education and knowledge assessment. JMIR Med Educ. 2023;9:e45312. Published 2023 Feb 8. doi:10.2196/45312
13. Eysenbach G. The role of ChatGPT, generative language models, and artificial intelligence in medical education: a conversation with ChatGPT and a call for papers. JMIR Med Educ. 2023;9:e46885. Published 2023 Mar 6. doi:10.2196/46885
14. Macdonald C, Adeloye D, Sheikh A, Rudan I. Can ChatGPT draft a research article? An example of population-level vaccine effectiveness analysis. J Glob Health. 2023;13:01003. Published 2023 Feb 17. doi:10.7189/jogh.13.01003
15. Masters K. Ethical use of artificial intelligence in health professions education: AMEE Guide No.158. Med Teach. 2023;1-11. doi:10.1080/0142159X.2023.2186203
16. Smith CS. Hallucinations could blunt ChatGPT’s success. IEEE Spectrum. March 13, 2023. Accessed May 11, 2023. https://spectrum.ieee.org/ai-hallucination
17. Executive Office of the President, Office of Science and Technology Policy. Blueprint for an AI Bill of Rights. Accessed May 11, 2023. https://www.whitehouse.gov/ostp/ai-bill-of-rights
18. Executive office of the President. Executive Order 13960: promoting the use of trustworthy artificial intelligence in the federal government. Fed Regist. 2020;89(236):78939-78943.
19. US Department of Commerce, National institute of Standards and Technology. Artificial Intelligence Risk Management Framework (AI RMF 1.0). Published January 2023. doi:10.6028/NIST.AI.100-1
20. Microsoft. Azure Cognitive Search—Cloud Search Service. Accessed May 11, 2023. https://azure.microsoft.com/en-us/products/search
21. Aiyappa R, An J, Kwak H, Ahn YY. Can we trust the evaluation on ChatGPT? March 22, 2023. Accessed May 11, 2023. https://arxiv.org/abs/2303.12767v1
22. Yang X, Chen A, Pournejatian N, et al. GatorTron: a large clinical language model to unlock patient information from unstructured electronic health records. Updated December 16, 2022. Accessed May 11, 2023. https://arxiv.org/abs/2203.03540v3
23. Singhal K, Azizi S, Tu T, et al. Large language models encode clinical knowledge. December 26, 2022. Accessed May 11, 2023. https://arxiv.org/abs/2212.13138v1
24. Zakka C, Chaurasia A, Shad R, Hiesinger W. Almanac: knowledge-grounded language models for clinical medicine. March 1, 2023. Accessed May 11, 2023. https://arxiv.org/abs/2303.01229v1
25. NVIDIA. GatorTron-OG. Accessed May 11, 2023. https://catalog.ngc.nvidia.com/orgs/nvidia/teams/clara/models/gatortron_og
26. Borkowski AA, Jakey CE, Thomas LB, Viswanadhan N, Mastorides SM. Establishing a hospital artificial intelligence committee to improve patient care. Fed Pract. 2022;39(8):334-336. doi:10.12788/fp.0299
1. Bill Gates. The age of AI has begun. March 21, 2023. Accessed May 10, 2023. https://www.gatesnotes.com/the-age-of-ai-has-begun
2. Kung TH, Cheatham M, Medenilla A, et al. Performance of ChatGPT on USMLE: Potential for AI-assisted medical education using large language models. PLOS Digit Health. 2023;2(2):e0000198. Published 2023 Feb 9. doi:10.1371/journal.pdig.0000198
3. Shanafelt TD, West CP, Sinsky C, et al. Changes in burnout and satisfaction with work-life integration in physicians and the general US working population between 2011 and 2020. Mayo Clin Proc. 2022;97(3):491-506. doi:10.1016/j.mayocp.2021.11.021
4. Goodman RS, Patrinely JR Jr, Osterman T, Wheless L, Johnson DB. On the cusp: considering the impact of artificial intelligence language models in healthcare. Med. 2023;4(3):139-140. doi:10.1016/j.medj.2023.02.008
5. Will ChatGPT transform healthcare? Nat Med. 2023;29(3):505-506. doi:10.1038/s41591-023-02289-5
6. Hopkins AM, Logan JM, Kichenadasse G, Sorich MJ. Artificial intelligence chatbots will revolutionize how cancer patients access information: ChatGPT represents a paradigm-shift. JNCI Cancer Spectr. 2023;7(2):pkad010. doi:10.1093/jncics/pkad010
7. Babar Z, van Laarhoven T, Zanzotto FM, Marchiori E. Evaluating diagnostic content of AI-generated radiology reports of chest X-rays. Artif Intell Med. 2021;116:102075. doi:10.1016/j.artmed.2021.102075
8. Lecler A, Duron L, Soyer P. Revolutionizing radiology with GPT-based models: current applications, future possibilities and limitations of ChatGPT. Diagn Interv Imaging. 2023;S2211-5684(23)00027-X. doi:10.1016/j.diii.2023.02.003
9. Germain JM. Is ChatGPT smart enough to practice mental health therapy? March 23, 2023. Accessed May 11, 2023. https://www.technewsworld.com/story/is-chatgpt-smart-enough-to-practice-mental-health-therapy-178064.html
10. Cascella M, Montomoli J, Bellini V, Bignami E. Evaluating the feasibility of ChatGPT in healthcare: an analysis of multiple clinical and research scenarios. J Med Syst. 2023;47(1):33. Published 2023 Mar 4. doi:10.1007/s10916-023-01925-4
11. Jungwirth D, Haluza D. Artificial intelligence and public health: an exploratory study. Int J Environ Res Public Health. 2023;20(5):4541. Published 2023 Mar 3. doi:10.3390/ijerph20054541
12. Gilson A, Safranek CW, Huang T, et al. How does ChatGPT perform on the United States Medical Licensing Examination? The implications of large language models for medical education and knowledge assessment. JMIR Med Educ. 2023;9:e45312. Published 2023 Feb 8. doi:10.2196/45312
13. Eysenbach G. The role of ChatGPT, generative language models, and artificial intelligence in medical education: a conversation with ChatGPT and a call for papers. JMIR Med Educ. 2023;9:e46885. Published 2023 Mar 6. doi:10.2196/46885
14. Macdonald C, Adeloye D, Sheikh A, Rudan I. Can ChatGPT draft a research article? An example of population-level vaccine effectiveness analysis. J Glob Health. 2023;13:01003. Published 2023 Feb 17. doi:10.7189/jogh.13.01003
15. Masters K. Ethical use of artificial intelligence in health professions education: AMEE Guide No.158. Med Teach. 2023;1-11. doi:10.1080/0142159X.2023.2186203
16. Smith CS. Hallucinations could blunt ChatGPT’s success. IEEE Spectrum. March 13, 2023. Accessed May 11, 2023. https://spectrum.ieee.org/ai-hallucination
17. Executive Office of the President, Office of Science and Technology Policy. Blueprint for an AI Bill of Rights. Accessed May 11, 2023. https://www.whitehouse.gov/ostp/ai-bill-of-rights
18. Executive office of the President. Executive Order 13960: promoting the use of trustworthy artificial intelligence in the federal government. Fed Regist. 2020;89(236):78939-78943.
19. US Department of Commerce, National institute of Standards and Technology. Artificial Intelligence Risk Management Framework (AI RMF 1.0). Published January 2023. doi:10.6028/NIST.AI.100-1
20. Microsoft. Azure Cognitive Search—Cloud Search Service. Accessed May 11, 2023. https://azure.microsoft.com/en-us/products/search
21. Aiyappa R, An J, Kwak H, Ahn YY. Can we trust the evaluation on ChatGPT? March 22, 2023. Accessed May 11, 2023. https://arxiv.org/abs/2303.12767v1
22. Yang X, Chen A, Pournejatian N, et al. GatorTron: a large clinical language model to unlock patient information from unstructured electronic health records. Updated December 16, 2022. Accessed May 11, 2023. https://arxiv.org/abs/2203.03540v3
23. Singhal K, Azizi S, Tu T, et al. Large language models encode clinical knowledge. December 26, 2022. Accessed May 11, 2023. https://arxiv.org/abs/2212.13138v1
24. Zakka C, Chaurasia A, Shad R, Hiesinger W. Almanac: knowledge-grounded language models for clinical medicine. March 1, 2023. Accessed May 11, 2023. https://arxiv.org/abs/2303.01229v1
25. NVIDIA. GatorTron-OG. Accessed May 11, 2023. https://catalog.ngc.nvidia.com/orgs/nvidia/teams/clara/models/gatortron_og
26. Borkowski AA, Jakey CE, Thomas LB, Viswanadhan N, Mastorides SM. Establishing a hospital artificial intelligence committee to improve patient care. Fed Pract. 2022;39(8):334-336. doi:10.12788/fp.0299