User login
Children and teens with food allergies face quality-of-life issues
Children and adolescents with food allergies appear to fare worse physically, socially, and emotionally, and have poorer overall health-related quality of life (HRQL) than their food allergy–free peers, a new systematic review suggests.
“Findings from the current review suggest that food allergy has a negative impact on the HRQL of children and teens, particularly older children and those with severe food allergy,” the authors wrote. “By comparison, the link between food allergy and psychosocial functioning is less clear.
“Evidence from the qualitative literature suggests that the burden of childhood food allergy largely stems from worries surrounding exposures outside of the home and the social consequences of the condition,” they added.
Lead study author Michael A. Golding, a research coordinator at Children’s Hospital Research Institute of Manitoba in Winnipeg, Canada, and colleagues searched PubMed, Scopus, PsycInfo, and CINAHL (Cumulative Index to Nursing and Allied Health Literature) databases on several days between November 2019 and March 2021 for peer-reviewed articles published in English in any year.
They reviewed articles focused on HRQL, psychological health, or social well-being in children and teens with food allergy from birth through 19 years of age. Food allergy comprised both immunoglobulin E (IgE)-mediated food allergies and non-IgE-mediated allergies, including food protein–induced enterocolitis, enteropathy, and proctocolitis.
From the 3,789 publications the researchers screened, they included 8,202 patients in 45 studies in their quantitative synthesis and 186 patients in 9 studies in their qualitative synthesis. Using a segregated, mixed research synthesis design, they analyzed and synthesized the quantitative and qualitative articles separately, then integrated those findings.
Navigating through many challenges
The authors found that food allergy lowered the young people’s HRQL. In 11 of the 14 studies (78%) that included a comparison group, young patients with food allergy showed significantly lower HRQL in at least one domain. Most significant differences occurred in domains related to total HRQL (66%), social functioning (58%), emotional functioning (54%), and physical functioning (54%).
Parents were often more likely than their children to perceive that the child’s food allergy was causing problems.
Between 20% and 32% of children reported bullying related to their food allergy. Many children reported that their allergy sometimes isolated them from their classmates.
Many children described feeling comfortable at home but worried in places where they had less control, such as school, restaurants, or when traveling.
Children and teens tended to downplay their limitations and the negative impacts of their condition.
Older children who had been diagnosed early in life tended to accept managing their food allergy as a way of life, whereas those diagnosed when they were older reported the need to adapt, accept, and grieve the loss of foods and experiences.
“This study highlights the importance of addressing the underlying impact that food allergy can have on patients’ mental health and social functioning,” Kelly Marie O’Shea, MD, assistant professor of allergy and immunology at University of Michigan Health in Ann Arbor, said in an interview.
“While it has been shown previously that food-allergic patients have lower HRQL, this systematic review aptly reveals that for children and teens with food allergy, overall quality of life, including psychosocial functioning, can also be negatively affected,” said Dr. O’Shea, who was not involved in the study.
“Symptoms of anxiety and depression are reported at higher rates in the food-allergic population, and social limitations have been shown to play a role,” she explained. “However, as revealed in this study, longitudinal and appropriately controlled studies to investigate the impact of food allergy on psychosocial outcomes in children and teens are scarce.”
Robert Alan Wood, MD, professor of pediatrics at Johns Hopkins University and director of pediatric allergy and immunology at Johns Hopkins Children’s Center, Baltimore, told this news organization that the effects of food allergy on mental health are not fully appreciated by the public or by many clinicians.
“These findings emphasize the need to recognize the emotional consequences of food allergy and to take steps to be proactive in managing these issues among our patients,” said Dr. Wood, who was not associated with the study.
More research is needed
The authors noted that more research is needed to examine links between food allergy, HRQL, and psychosocial outcome; links between food allergy and bullying; and how challenges change over time. They recommend exploring the relative impacts of specific types of food allergy and whether specific traits in young people with food allergy make them more susceptible to its psychological effects. They also call for efforts to identify and help young people with food allergy overcome their many challenges.
The study was funded by the Canadian Institutes for Health Research, the Children’s Hospital Research Institute of Manitoba, and the University of Manitoba.
Study senior author Jennifer L. P. Protudjer, PhD, reported involvement with Canada’s National Food Allergy Action Plan and Allied Health at the Canadian Society of Allergy and Clinical Immunology, and receipt of fees from Novartis. The remaining authors, as well as Dr. O’Shea and Dr. Wood, reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Children and adolescents with food allergies appear to fare worse physically, socially, and emotionally, and have poorer overall health-related quality of life (HRQL) than their food allergy–free peers, a new systematic review suggests.
“Findings from the current review suggest that food allergy has a negative impact on the HRQL of children and teens, particularly older children and those with severe food allergy,” the authors wrote. “By comparison, the link between food allergy and psychosocial functioning is less clear.
“Evidence from the qualitative literature suggests that the burden of childhood food allergy largely stems from worries surrounding exposures outside of the home and the social consequences of the condition,” they added.
Lead study author Michael A. Golding, a research coordinator at Children’s Hospital Research Institute of Manitoba in Winnipeg, Canada, and colleagues searched PubMed, Scopus, PsycInfo, and CINAHL (Cumulative Index to Nursing and Allied Health Literature) databases on several days between November 2019 and March 2021 for peer-reviewed articles published in English in any year.
They reviewed articles focused on HRQL, psychological health, or social well-being in children and teens with food allergy from birth through 19 years of age. Food allergy comprised both immunoglobulin E (IgE)-mediated food allergies and non-IgE-mediated allergies, including food protein–induced enterocolitis, enteropathy, and proctocolitis.
From the 3,789 publications the researchers screened, they included 8,202 patients in 45 studies in their quantitative synthesis and 186 patients in 9 studies in their qualitative synthesis. Using a segregated, mixed research synthesis design, they analyzed and synthesized the quantitative and qualitative articles separately, then integrated those findings.
Navigating through many challenges
The authors found that food allergy lowered the young people’s HRQL. In 11 of the 14 studies (78%) that included a comparison group, young patients with food allergy showed significantly lower HRQL in at least one domain. Most significant differences occurred in domains related to total HRQL (66%), social functioning (58%), emotional functioning (54%), and physical functioning (54%).
Parents were often more likely than their children to perceive that the child’s food allergy was causing problems.
Between 20% and 32% of children reported bullying related to their food allergy. Many children reported that their allergy sometimes isolated them from their classmates.
Many children described feeling comfortable at home but worried in places where they had less control, such as school, restaurants, or when traveling.
Children and teens tended to downplay their limitations and the negative impacts of their condition.
Older children who had been diagnosed early in life tended to accept managing their food allergy as a way of life, whereas those diagnosed when they were older reported the need to adapt, accept, and grieve the loss of foods and experiences.
“This study highlights the importance of addressing the underlying impact that food allergy can have on patients’ mental health and social functioning,” Kelly Marie O’Shea, MD, assistant professor of allergy and immunology at University of Michigan Health in Ann Arbor, said in an interview.
“While it has been shown previously that food-allergic patients have lower HRQL, this systematic review aptly reveals that for children and teens with food allergy, overall quality of life, including psychosocial functioning, can also be negatively affected,” said Dr. O’Shea, who was not involved in the study.
“Symptoms of anxiety and depression are reported at higher rates in the food-allergic population, and social limitations have been shown to play a role,” she explained. “However, as revealed in this study, longitudinal and appropriately controlled studies to investigate the impact of food allergy on psychosocial outcomes in children and teens are scarce.”
Robert Alan Wood, MD, professor of pediatrics at Johns Hopkins University and director of pediatric allergy and immunology at Johns Hopkins Children’s Center, Baltimore, told this news organization that the effects of food allergy on mental health are not fully appreciated by the public or by many clinicians.
“These findings emphasize the need to recognize the emotional consequences of food allergy and to take steps to be proactive in managing these issues among our patients,” said Dr. Wood, who was not associated with the study.
More research is needed
The authors noted that more research is needed to examine links between food allergy, HRQL, and psychosocial outcome; links between food allergy and bullying; and how challenges change over time. They recommend exploring the relative impacts of specific types of food allergy and whether specific traits in young people with food allergy make them more susceptible to its psychological effects. They also call for efforts to identify and help young people with food allergy overcome their many challenges.
The study was funded by the Canadian Institutes for Health Research, the Children’s Hospital Research Institute of Manitoba, and the University of Manitoba.
Study senior author Jennifer L. P. Protudjer, PhD, reported involvement with Canada’s National Food Allergy Action Plan and Allied Health at the Canadian Society of Allergy and Clinical Immunology, and receipt of fees from Novartis. The remaining authors, as well as Dr. O’Shea and Dr. Wood, reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Children and adolescents with food allergies appear to fare worse physically, socially, and emotionally, and have poorer overall health-related quality of life (HRQL) than their food allergy–free peers, a new systematic review suggests.
“Findings from the current review suggest that food allergy has a negative impact on the HRQL of children and teens, particularly older children and those with severe food allergy,” the authors wrote. “By comparison, the link between food allergy and psychosocial functioning is less clear.
“Evidence from the qualitative literature suggests that the burden of childhood food allergy largely stems from worries surrounding exposures outside of the home and the social consequences of the condition,” they added.
Lead study author Michael A. Golding, a research coordinator at Children’s Hospital Research Institute of Manitoba in Winnipeg, Canada, and colleagues searched PubMed, Scopus, PsycInfo, and CINAHL (Cumulative Index to Nursing and Allied Health Literature) databases on several days between November 2019 and March 2021 for peer-reviewed articles published in English in any year.
They reviewed articles focused on HRQL, psychological health, or social well-being in children and teens with food allergy from birth through 19 years of age. Food allergy comprised both immunoglobulin E (IgE)-mediated food allergies and non-IgE-mediated allergies, including food protein–induced enterocolitis, enteropathy, and proctocolitis.
From the 3,789 publications the researchers screened, they included 8,202 patients in 45 studies in their quantitative synthesis and 186 patients in 9 studies in their qualitative synthesis. Using a segregated, mixed research synthesis design, they analyzed and synthesized the quantitative and qualitative articles separately, then integrated those findings.
Navigating through many challenges
The authors found that food allergy lowered the young people’s HRQL. In 11 of the 14 studies (78%) that included a comparison group, young patients with food allergy showed significantly lower HRQL in at least one domain. Most significant differences occurred in domains related to total HRQL (66%), social functioning (58%), emotional functioning (54%), and physical functioning (54%).
Parents were often more likely than their children to perceive that the child’s food allergy was causing problems.
Between 20% and 32% of children reported bullying related to their food allergy. Many children reported that their allergy sometimes isolated them from their classmates.
Many children described feeling comfortable at home but worried in places where they had less control, such as school, restaurants, or when traveling.
Children and teens tended to downplay their limitations and the negative impacts of their condition.
Older children who had been diagnosed early in life tended to accept managing their food allergy as a way of life, whereas those diagnosed when they were older reported the need to adapt, accept, and grieve the loss of foods and experiences.
“This study highlights the importance of addressing the underlying impact that food allergy can have on patients’ mental health and social functioning,” Kelly Marie O’Shea, MD, assistant professor of allergy and immunology at University of Michigan Health in Ann Arbor, said in an interview.
“While it has been shown previously that food-allergic patients have lower HRQL, this systematic review aptly reveals that for children and teens with food allergy, overall quality of life, including psychosocial functioning, can also be negatively affected,” said Dr. O’Shea, who was not involved in the study.
“Symptoms of anxiety and depression are reported at higher rates in the food-allergic population, and social limitations have been shown to play a role,” she explained. “However, as revealed in this study, longitudinal and appropriately controlled studies to investigate the impact of food allergy on psychosocial outcomes in children and teens are scarce.”
Robert Alan Wood, MD, professor of pediatrics at Johns Hopkins University and director of pediatric allergy and immunology at Johns Hopkins Children’s Center, Baltimore, told this news organization that the effects of food allergy on mental health are not fully appreciated by the public or by many clinicians.
“These findings emphasize the need to recognize the emotional consequences of food allergy and to take steps to be proactive in managing these issues among our patients,” said Dr. Wood, who was not associated with the study.
More research is needed
The authors noted that more research is needed to examine links between food allergy, HRQL, and psychosocial outcome; links between food allergy and bullying; and how challenges change over time. They recommend exploring the relative impacts of specific types of food allergy and whether specific traits in young people with food allergy make them more susceptible to its psychological effects. They also call for efforts to identify and help young people with food allergy overcome their many challenges.
The study was funded by the Canadian Institutes for Health Research, the Children’s Hospital Research Institute of Manitoba, and the University of Manitoba.
Study senior author Jennifer L. P. Protudjer, PhD, reported involvement with Canada’s National Food Allergy Action Plan and Allied Health at the Canadian Society of Allergy and Clinical Immunology, and receipt of fees from Novartis. The remaining authors, as well as Dr. O’Shea and Dr. Wood, reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Performance anxiety highly common among surgeons
a new study of surgeons in the United Kingdom shows.
“Performance anxiety or stage fright is a widely recognized problem in music and sports, and there are many similarities between these arenas and the operating theater,” first author Robert Miller, MRCS, of the Surgical Psychology and Performance Group and the department of plastic and reconstructive surgery at St. George’s Hospital NHS Trust, London, said in an interview. “We were aware of it anecdotally in a surgical context, but for one reason or another, perhaps professional pride and fear of negative perception, this is rarely openly discussed amongst surgeons.”
In the cross-sectional study, published in Annals of Surgery, Dr. Miller and colleagues surveyed surgeons in all specialties working in the United Kingdom who had at least 1 year of postgraduate surgical training.
Of a total of 631 responses received, 523 (83%) were included in the analysis. The median age of those who responded was 41.2 years, and the mean duration of surgical experience was 15.3 years (range, 1-52 years). Among them, 62% were men, and 52% were of consultant/attending grade.
All of the respondents – 100% – said they believed that performance anxiety affected surgeons, 87% reported having experienced it themselves, and 65% said they felt that performance anxiety had an effect on their surgical performance.
Both male and female surgeons who reported experiencing performance anxiety had significantly worse mental well-being, as assessed using the Short Warwick Edinburgh Mental Wellbeing Scale, compared with those who did not have performance anxiety (P < .0001 for men and P < .001 for women).
Overall, however, male surgeons had significantly better mental well-being, compared with female surgeons (P = .003), yet both genders had significantly lower mental well-being scores compared with U.K. population norms (P = .0019 for men and P = .0001 for women).
The gender differences are “clearly an important topic, which is likely multifactorial,” Dr. Miller told this news organization. “The gender well-being gap requires more in-depth research, and qualitative work involving female surgeons is critical.”
Surgical perfectionism was significantly more common among respondents who did have performance anxiety in comparison with those who did not (P < .0001).
“Although perfectionism may be a beneficial trait in surgery, our findings from hierarchical multiple regression analysis also indicate that perfectionism, [as well as] sex and experience, may drive surgical performance anxiety and help predict those experiencing [the anxiety],” the authors noted.
Performing in presence of colleagues a key trigger
By far, the leading trigger that was identified as prompting surgeon performance anxiety was the presence – and scrutiny – of colleagues within the parent specialty. This was reported by 151 respondents. Other triggers were having to perform on highly complex or high-risk cases (66 responses) and a lack of experience (30 responses).
Next to planning and preparation, opening up and talking about the anxiety and shedding light on the issue was seen as a leading strategy to help with the problem, but very few respondents reported openly sharing their struggles. Only 9% reported that they had shared it openly; 27% said they had confided in someone, and 47% did not respond to the question.
“I wish we talked about it more and shared our insecurities,” one respondent lamented. “Most of my colleagues pretend they are living gods.”
Only about 45% of respondents reported a specific technique for overcoming their anxiety. In addition to being open about the problem, other techniques included self-care, such as exercise; and distraction outside of work to get perspective; relaxation techniques such as deep or controlled breathing; music; mindfulness; and positive self-statements.
About 9% said they had received psychological counseling for performance anxiety, and only 3% reported using medication for the problem.
Anxiety a positive factor?
Surprisingly, 70% of respondents reported feeling that surgical performance anxiety could have a positive impact on surgical performance, which the authors noted is consistent with some theories.
“This may be explained by the traditional bell-curve relationship between arousal and performance, which describes a dose-dependent relationship between performance and arousal until a ‘tipping point,’ after which performance declines,” the authors explained. “A heightened awareness secondary to anxiety may be beneficial, but at high doses, anxiety can negatively affect attentional control and cause somatic symptoms.”
They noted that “the challenge would be to reap the benefits of low-level stimulation without incurring possible adverse effects.”
Dr. Miller said that, in determining whether selection bias had a role in the results, a detailed analysis showed that “our respondents were not skewed to those with only high levels of trait anxiety.
“We also had a good spread of consultants versus trainees [about half and half], and different specialties, so we feel this is likely to be a representative sample,” he told this news organization.
That being said, the results underscore the need for increased awareness – and open discussion – of the issue of surgical performance anxiety.
“Within other professions, particularly the performing arts and sports, performance psychology is becoming an integral part of training and development,” Dr. Miller said. “We feel surgeons should be supported in a similar manner.
“Surgical performance anxiety is normal for surgeons at all levels and not something to be ashamed about,” Dr. Miller added. “Talk about it, acknowledge it, and be supportive to your colleagues.”
Many keep it to themselves in ‘prevailing culture of stoicism’
Commenting on the study, Carter C. Lebares, MD, an associate professor of surgery and director of the Center for Mindfulness in Surgery, department of surgery, University of California, San Francisco, said she was not surprised to see the high rates of performance anxiety among surgeons.
“As surgeons, no matter how hard we train or how thoroughly we prepare our intellectual understanding or the patient, the disease process, and the operation, there may be surprises, unforeseen challenges, or off days,” Dr. Lebares said.
“And whatever we encounter, we are managing these things directly under the scrutiny of others – people who can affect our reputation, operating privileges, and mental health. So, I am not surprised this is a prevalent and widely recognized issue.”
Dr. Lebares noted that the reluctance to share the anxiety is part of a “challenging and recognized conundrum in both medicine and surgery and is a matter of the prevailing culture of stoicism.
“We often are called to shoulder tremendous weight intraoperatively (having perseverance, self-confidence, or sustained focus), and in owning the weight of complications (which eventually we all will have),” she said.
“So, we do need to be strong and not complain, [but] we also need to be able to set that aside [when appropriate] and ask for help or allow others to shoulder the weight for a while, and this is not [yet] a common part of surgical culture.”
Dr. Lebares added that randomized, controlled trials have shown benefits of mindfulness interventions on burnout and anxiety.
“We have observed positive effects on mental noise, self-perception, conflict resolution, and resilience in surgical residents trained in mindfulness-based cognitive skills,” she said. “[Residents] report applying these skills in the OR, in their home lives, and in how they approach their training/education.”
The authors disclosed no relevant financial relationships. Dr. Lebares has developed mindfulness-based cognitive skills training for surgeons but receives no financial compensation for the activities.
A version of this article first appeared on Medscape.com.
a new study of surgeons in the United Kingdom shows.
“Performance anxiety or stage fright is a widely recognized problem in music and sports, and there are many similarities between these arenas and the operating theater,” first author Robert Miller, MRCS, of the Surgical Psychology and Performance Group and the department of plastic and reconstructive surgery at St. George’s Hospital NHS Trust, London, said in an interview. “We were aware of it anecdotally in a surgical context, but for one reason or another, perhaps professional pride and fear of negative perception, this is rarely openly discussed amongst surgeons.”
In the cross-sectional study, published in Annals of Surgery, Dr. Miller and colleagues surveyed surgeons in all specialties working in the United Kingdom who had at least 1 year of postgraduate surgical training.
Of a total of 631 responses received, 523 (83%) were included in the analysis. The median age of those who responded was 41.2 years, and the mean duration of surgical experience was 15.3 years (range, 1-52 years). Among them, 62% were men, and 52% were of consultant/attending grade.
All of the respondents – 100% – said they believed that performance anxiety affected surgeons, 87% reported having experienced it themselves, and 65% said they felt that performance anxiety had an effect on their surgical performance.
Both male and female surgeons who reported experiencing performance anxiety had significantly worse mental well-being, as assessed using the Short Warwick Edinburgh Mental Wellbeing Scale, compared with those who did not have performance anxiety (P < .0001 for men and P < .001 for women).
Overall, however, male surgeons had significantly better mental well-being, compared with female surgeons (P = .003), yet both genders had significantly lower mental well-being scores compared with U.K. population norms (P = .0019 for men and P = .0001 for women).
The gender differences are “clearly an important topic, which is likely multifactorial,” Dr. Miller told this news organization. “The gender well-being gap requires more in-depth research, and qualitative work involving female surgeons is critical.”
Surgical perfectionism was significantly more common among respondents who did have performance anxiety in comparison with those who did not (P < .0001).
“Although perfectionism may be a beneficial trait in surgery, our findings from hierarchical multiple regression analysis also indicate that perfectionism, [as well as] sex and experience, may drive surgical performance anxiety and help predict those experiencing [the anxiety],” the authors noted.
Performing in presence of colleagues a key trigger
By far, the leading trigger that was identified as prompting surgeon performance anxiety was the presence – and scrutiny – of colleagues within the parent specialty. This was reported by 151 respondents. Other triggers were having to perform on highly complex or high-risk cases (66 responses) and a lack of experience (30 responses).
Next to planning and preparation, opening up and talking about the anxiety and shedding light on the issue was seen as a leading strategy to help with the problem, but very few respondents reported openly sharing their struggles. Only 9% reported that they had shared it openly; 27% said they had confided in someone, and 47% did not respond to the question.
“I wish we talked about it more and shared our insecurities,” one respondent lamented. “Most of my colleagues pretend they are living gods.”
Only about 45% of respondents reported a specific technique for overcoming their anxiety. In addition to being open about the problem, other techniques included self-care, such as exercise; and distraction outside of work to get perspective; relaxation techniques such as deep or controlled breathing; music; mindfulness; and positive self-statements.
About 9% said they had received psychological counseling for performance anxiety, and only 3% reported using medication for the problem.
Anxiety a positive factor?
Surprisingly, 70% of respondents reported feeling that surgical performance anxiety could have a positive impact on surgical performance, which the authors noted is consistent with some theories.
“This may be explained by the traditional bell-curve relationship between arousal and performance, which describes a dose-dependent relationship between performance and arousal until a ‘tipping point,’ after which performance declines,” the authors explained. “A heightened awareness secondary to anxiety may be beneficial, but at high doses, anxiety can negatively affect attentional control and cause somatic symptoms.”
They noted that “the challenge would be to reap the benefits of low-level stimulation without incurring possible adverse effects.”
Dr. Miller said that, in determining whether selection bias had a role in the results, a detailed analysis showed that “our respondents were not skewed to those with only high levels of trait anxiety.
“We also had a good spread of consultants versus trainees [about half and half], and different specialties, so we feel this is likely to be a representative sample,” he told this news organization.
That being said, the results underscore the need for increased awareness – and open discussion – of the issue of surgical performance anxiety.
“Within other professions, particularly the performing arts and sports, performance psychology is becoming an integral part of training and development,” Dr. Miller said. “We feel surgeons should be supported in a similar manner.
“Surgical performance anxiety is normal for surgeons at all levels and not something to be ashamed about,” Dr. Miller added. “Talk about it, acknowledge it, and be supportive to your colleagues.”
Many keep it to themselves in ‘prevailing culture of stoicism’
Commenting on the study, Carter C. Lebares, MD, an associate professor of surgery and director of the Center for Mindfulness in Surgery, department of surgery, University of California, San Francisco, said she was not surprised to see the high rates of performance anxiety among surgeons.
“As surgeons, no matter how hard we train or how thoroughly we prepare our intellectual understanding or the patient, the disease process, and the operation, there may be surprises, unforeseen challenges, or off days,” Dr. Lebares said.
“And whatever we encounter, we are managing these things directly under the scrutiny of others – people who can affect our reputation, operating privileges, and mental health. So, I am not surprised this is a prevalent and widely recognized issue.”
Dr. Lebares noted that the reluctance to share the anxiety is part of a “challenging and recognized conundrum in both medicine and surgery and is a matter of the prevailing culture of stoicism.
“We often are called to shoulder tremendous weight intraoperatively (having perseverance, self-confidence, or sustained focus), and in owning the weight of complications (which eventually we all will have),” she said.
“So, we do need to be strong and not complain, [but] we also need to be able to set that aside [when appropriate] and ask for help or allow others to shoulder the weight for a while, and this is not [yet] a common part of surgical culture.”
Dr. Lebares added that randomized, controlled trials have shown benefits of mindfulness interventions on burnout and anxiety.
“We have observed positive effects on mental noise, self-perception, conflict resolution, and resilience in surgical residents trained in mindfulness-based cognitive skills,” she said. “[Residents] report applying these skills in the OR, in their home lives, and in how they approach their training/education.”
The authors disclosed no relevant financial relationships. Dr. Lebares has developed mindfulness-based cognitive skills training for surgeons but receives no financial compensation for the activities.
A version of this article first appeared on Medscape.com.
a new study of surgeons in the United Kingdom shows.
“Performance anxiety or stage fright is a widely recognized problem in music and sports, and there are many similarities between these arenas and the operating theater,” first author Robert Miller, MRCS, of the Surgical Psychology and Performance Group and the department of plastic and reconstructive surgery at St. George’s Hospital NHS Trust, London, said in an interview. “We were aware of it anecdotally in a surgical context, but for one reason or another, perhaps professional pride and fear of negative perception, this is rarely openly discussed amongst surgeons.”
In the cross-sectional study, published in Annals of Surgery, Dr. Miller and colleagues surveyed surgeons in all specialties working in the United Kingdom who had at least 1 year of postgraduate surgical training.
Of a total of 631 responses received, 523 (83%) were included in the analysis. The median age of those who responded was 41.2 years, and the mean duration of surgical experience was 15.3 years (range, 1-52 years). Among them, 62% were men, and 52% were of consultant/attending grade.
All of the respondents – 100% – said they believed that performance anxiety affected surgeons, 87% reported having experienced it themselves, and 65% said they felt that performance anxiety had an effect on their surgical performance.
Both male and female surgeons who reported experiencing performance anxiety had significantly worse mental well-being, as assessed using the Short Warwick Edinburgh Mental Wellbeing Scale, compared with those who did not have performance anxiety (P < .0001 for men and P < .001 for women).
Overall, however, male surgeons had significantly better mental well-being, compared with female surgeons (P = .003), yet both genders had significantly lower mental well-being scores compared with U.K. population norms (P = .0019 for men and P = .0001 for women).
The gender differences are “clearly an important topic, which is likely multifactorial,” Dr. Miller told this news organization. “The gender well-being gap requires more in-depth research, and qualitative work involving female surgeons is critical.”
Surgical perfectionism was significantly more common among respondents who did have performance anxiety in comparison with those who did not (P < .0001).
“Although perfectionism may be a beneficial trait in surgery, our findings from hierarchical multiple regression analysis also indicate that perfectionism, [as well as] sex and experience, may drive surgical performance anxiety and help predict those experiencing [the anxiety],” the authors noted.
Performing in presence of colleagues a key trigger
By far, the leading trigger that was identified as prompting surgeon performance anxiety was the presence – and scrutiny – of colleagues within the parent specialty. This was reported by 151 respondents. Other triggers were having to perform on highly complex or high-risk cases (66 responses) and a lack of experience (30 responses).
Next to planning and preparation, opening up and talking about the anxiety and shedding light on the issue was seen as a leading strategy to help with the problem, but very few respondents reported openly sharing their struggles. Only 9% reported that they had shared it openly; 27% said they had confided in someone, and 47% did not respond to the question.
“I wish we talked about it more and shared our insecurities,” one respondent lamented. “Most of my colleagues pretend they are living gods.”
Only about 45% of respondents reported a specific technique for overcoming their anxiety. In addition to being open about the problem, other techniques included self-care, such as exercise; and distraction outside of work to get perspective; relaxation techniques such as deep or controlled breathing; music; mindfulness; and positive self-statements.
About 9% said they had received psychological counseling for performance anxiety, and only 3% reported using medication for the problem.
Anxiety a positive factor?
Surprisingly, 70% of respondents reported feeling that surgical performance anxiety could have a positive impact on surgical performance, which the authors noted is consistent with some theories.
“This may be explained by the traditional bell-curve relationship between arousal and performance, which describes a dose-dependent relationship between performance and arousal until a ‘tipping point,’ after which performance declines,” the authors explained. “A heightened awareness secondary to anxiety may be beneficial, but at high doses, anxiety can negatively affect attentional control and cause somatic symptoms.”
They noted that “the challenge would be to reap the benefits of low-level stimulation without incurring possible adverse effects.”
Dr. Miller said that, in determining whether selection bias had a role in the results, a detailed analysis showed that “our respondents were not skewed to those with only high levels of trait anxiety.
“We also had a good spread of consultants versus trainees [about half and half], and different specialties, so we feel this is likely to be a representative sample,” he told this news organization.
That being said, the results underscore the need for increased awareness – and open discussion – of the issue of surgical performance anxiety.
“Within other professions, particularly the performing arts and sports, performance psychology is becoming an integral part of training and development,” Dr. Miller said. “We feel surgeons should be supported in a similar manner.
“Surgical performance anxiety is normal for surgeons at all levels and not something to be ashamed about,” Dr. Miller added. “Talk about it, acknowledge it, and be supportive to your colleagues.”
Many keep it to themselves in ‘prevailing culture of stoicism’
Commenting on the study, Carter C. Lebares, MD, an associate professor of surgery and director of the Center for Mindfulness in Surgery, department of surgery, University of California, San Francisco, said she was not surprised to see the high rates of performance anxiety among surgeons.
“As surgeons, no matter how hard we train or how thoroughly we prepare our intellectual understanding or the patient, the disease process, and the operation, there may be surprises, unforeseen challenges, or off days,” Dr. Lebares said.
“And whatever we encounter, we are managing these things directly under the scrutiny of others – people who can affect our reputation, operating privileges, and mental health. So, I am not surprised this is a prevalent and widely recognized issue.”
Dr. Lebares noted that the reluctance to share the anxiety is part of a “challenging and recognized conundrum in both medicine and surgery and is a matter of the prevailing culture of stoicism.
“We often are called to shoulder tremendous weight intraoperatively (having perseverance, self-confidence, or sustained focus), and in owning the weight of complications (which eventually we all will have),” she said.
“So, we do need to be strong and not complain, [but] we also need to be able to set that aside [when appropriate] and ask for help or allow others to shoulder the weight for a while, and this is not [yet] a common part of surgical culture.”
Dr. Lebares added that randomized, controlled trials have shown benefits of mindfulness interventions on burnout and anxiety.
“We have observed positive effects on mental noise, self-perception, conflict resolution, and resilience in surgical residents trained in mindfulness-based cognitive skills,” she said. “[Residents] report applying these skills in the OR, in their home lives, and in how they approach their training/education.”
The authors disclosed no relevant financial relationships. Dr. Lebares has developed mindfulness-based cognitive skills training for surgeons but receives no financial compensation for the activities.
A version of this article first appeared on Medscape.com.
FROM ANNALS OF SURGERY
Migraine linked to preeclampsia and other pregnancy complications
, new research suggests. In a large prospective study, researchers also found a link between migraine with aura and increased preeclampsia risk.
Overall, the findings suggest women with a history of migraine may benefit from enhanced monitoring during pregnancy, said coinvestigator Alexandra Purdue-Smithe, PhD, associate epidemiologist at Brigham and Women’s Hospital and instructor of medicine at Harvard Medical School, Boston. “Our results suggest that migraine history may be an important consideration in obstetric risk assessment,” Dr. Purdue-Smithe added.
The findings will be presented at the 2022 annual meeting of the American Academy of Neurology.
Common neurovascular disorder
Migraine is a common neurovascular disorder, affecting about 15% of adults. The condition carries “a pretty remarkable sex bias” as it affects up to three times more women than men, and about a quarter of women in the reproductive age bracket of 18-44 years, Dr. Purdue-Smithe noted.
Despite this, relatively little is known about migraine and pregnancy risks, she said.
What is known is that women with migraine have a higher burden of cardiovascular risk factors such as obesity and chronic hypertension, and these factors can also increase risk for pregnancy complications, she added.
In the study, researchers analyzed data on 30,555 pregnancies in about 19,000 women without a history of cardiovascular disease, type 2 diabetes, or cancer during a 20-year period ending in 2009.
The data came from the Nurses’ Health Study II, a large prospective cohort study established in 1989 when it enrolled women aged 25-42 years. Participants in the ongoing study complete questionnaires every 2 years, reporting information on various health conditions as well as pregnancy and reproductive events.
The investigators estimated associations of physician-diagnosed prepregnancy migraine with preterm delivery, gestational diabetes, gestational hypertension, preeclampsia, and low birth weight (<2,500 grams [5.5 lb]).
About 11% of the women in the study had migraine diagnosed by a physician before pregnancy.
Researchers adjusted for age at pregnancy, race/ethnicity, age at menarche, and prepregnancy chronic hypertension, body mass index, physical activity, smoking status, alcohol intake, history of infertility, parity, oral contraceptive use, and analgesic use.
‘A bit surprising’
Results showed that compared with women without a history of migraine, those with such a history had higher risk for preterm delivery (relative risk [RR], 1.17; 95% confidence interval [CI], 1.05-1.30), gestational hypertension (RR, 1.28; 95% CI, 1.11-1.48), and preeclampsia (RR, 1.40; 95% CI, 1.19-1.65).
Prepregnancy migraine was not associated with low birth weight (RR, 0.99; 95% CI, 0.85-1.16) or gestational diabetes (RR, 1.05; 95% CI, .91-1.22).
It was a “bit surprising” that women with migraine had a higher risk for preterm delivery but their babies were not necessarily underweight – although some prior literature had similar findings, said Dr. Purdue-Smithe.
She noted that in her study the association was limited to moderate preterm delivery (gestational age, 32-37 weeks) and not with very preterm births (before 32 weeks).
Researchers also assessed adverse pregnancy outcomes by aura phenotype. “Women with migraine with aura have a higher risk of cardiovascular disease later in life, so we hypothesized that aura might be more strongly associated with adverse pregnancy outcomes with underlying vascular pathology,” Dr. Purdue-Smithe said.
Women with and without aura had elevated risks for preterm delivery and gestational hypertension. Those with aura had a slightly higher risk for preeclampsia (RR, 1.51; 95% CI, 1.22-1.88) than those without aura (RR, 1.29; 95% CI, 1.04-1.61).
As the association between migraine and adverse pregnancy outcomes persisted after adjustment for established cardiovascular and obstetric risk factors, “this suggests there may be subclinical factors that are contributing to elevated risks of these outcomes in women with migraine,” said Dr. Purdue-Smithe.
Such factors could include platelet activation, chronic inflammation, and endothelial dysfunction, she added.
While findings of some previous case-control and retrospective studies suggested a possible link between migraine and adverse pregnancy outcomes, until now few large prospective studies have examined the association.
“Strengths of our study include its prospective design, very large sample size, and more complete adjustment for potential prepregnancy confounders,” Dr. Purdue-Smithe said.
Independent risk factor?
In the past, it has been somewhat unclear whether migraine is an independent risk factor for these complications or whether women with migraine just have greater risk factors for adverse pregnancy outcomes.
“Our preliminary findings suggest that migraine is independently associated with these adverse pregnancy outcomes, or at least that’s what it seems,” said Dr. Purdue-Smithe.
The new results could be used by clinicians to “flag” women who may be at risk for complications, she added. “These women may benefit from closer monitoring in pregnancy so that if issues arise, physicians can act quickly.”
She noted that preeclampsia “can come on suddenly and escalate rapidly,” and there are few interventions to treat it besides delivery.
However, low-dose aspirin may be worth investigating. Various health care groups and the U.S. Preventive Services Task Force recommend pregnant women at high risk for preeclampsia take low-dose aspirin (81 mg/d) after 12 weeks’ gestation.
“It would be interesting to see if women with migraine who take aspirin in pregnancy can reduce their risk of preeclampsia, and future research should address this question,” said Dr. Purdue-Smithe.
Additional testing showed that associations with preeclampsia and gestational hypertension did not vary according to age and other obstetrical risks.
The Nurses’ Health Study II did not have information on number and severity of migraine attacks, so the researchers were unable to determine if these factors affect pregnancy outcomes.
“Understanding whether specific migraine features, such as attack frequency, are associated with adverse pregnancy outcomes will be an important area for future research,” said Dr. Purdue-Smithe. She noted prior studies showed the frequency of migraine attacks is related to ischemic stroke and other cardiovascular outcomes.
The authors acknowledged a limitation for the current study: Although migraine history was reported prior to pregnancy, information on migraine aura was collected after most of the pregnancies in the cohort were over. So the findings for migraine aura may have been influenced by participants’ ability to accurately remember their experiences.
Collaboration is key
Commenting on the research, Nina Riggins, MD, PhD, director of the Headache and Traumatic Brain Injury Center in the department of neurosciences at the University of California, San Diego, said the study “stands out” because it distinguishes pregnancy complications between those with and without aura among women with migraine.
Dr. Riggins noted the investigators found the risk of preeclampsia, which on average occurs in about 3%-5% of pregnancies, is higher among women with migraine with aura.
“The good news is that treatments are available,” she said. “Preconception planning should include this discussion for patients living with migraine.”
However, the study did not compare risks for patients who have frequent migraine attacks versus episodic migraine, Dr. Riggins noted. “We need to learn more about whether any treatments can be safe and effective to decrease risks of complications during pregnancy in this population,” she said.
“I believe, ultimately, what this study reveals is that collaboration among primary care, ob.gyn., maternal-fetal medicine specialists, and neurologists will likely benefit pregnant patients with migraine,” Dr. Riggins said.
The study received funding from the National Institutes of Health. Dr. Purdue-Smithe has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests. In a large prospective study, researchers also found a link between migraine with aura and increased preeclampsia risk.
Overall, the findings suggest women with a history of migraine may benefit from enhanced monitoring during pregnancy, said coinvestigator Alexandra Purdue-Smithe, PhD, associate epidemiologist at Brigham and Women’s Hospital and instructor of medicine at Harvard Medical School, Boston. “Our results suggest that migraine history may be an important consideration in obstetric risk assessment,” Dr. Purdue-Smithe added.
The findings will be presented at the 2022 annual meeting of the American Academy of Neurology.
Common neurovascular disorder
Migraine is a common neurovascular disorder, affecting about 15% of adults. The condition carries “a pretty remarkable sex bias” as it affects up to three times more women than men, and about a quarter of women in the reproductive age bracket of 18-44 years, Dr. Purdue-Smithe noted.
Despite this, relatively little is known about migraine and pregnancy risks, she said.
What is known is that women with migraine have a higher burden of cardiovascular risk factors such as obesity and chronic hypertension, and these factors can also increase risk for pregnancy complications, she added.
In the study, researchers analyzed data on 30,555 pregnancies in about 19,000 women without a history of cardiovascular disease, type 2 diabetes, or cancer during a 20-year period ending in 2009.
The data came from the Nurses’ Health Study II, a large prospective cohort study established in 1989 when it enrolled women aged 25-42 years. Participants in the ongoing study complete questionnaires every 2 years, reporting information on various health conditions as well as pregnancy and reproductive events.
The investigators estimated associations of physician-diagnosed prepregnancy migraine with preterm delivery, gestational diabetes, gestational hypertension, preeclampsia, and low birth weight (<2,500 grams [5.5 lb]).
About 11% of the women in the study had migraine diagnosed by a physician before pregnancy.
Researchers adjusted for age at pregnancy, race/ethnicity, age at menarche, and prepregnancy chronic hypertension, body mass index, physical activity, smoking status, alcohol intake, history of infertility, parity, oral contraceptive use, and analgesic use.
‘A bit surprising’
Results showed that compared with women without a history of migraine, those with such a history had higher risk for preterm delivery (relative risk [RR], 1.17; 95% confidence interval [CI], 1.05-1.30), gestational hypertension (RR, 1.28; 95% CI, 1.11-1.48), and preeclampsia (RR, 1.40; 95% CI, 1.19-1.65).
Prepregnancy migraine was not associated with low birth weight (RR, 0.99; 95% CI, 0.85-1.16) or gestational diabetes (RR, 1.05; 95% CI, .91-1.22).
It was a “bit surprising” that women with migraine had a higher risk for preterm delivery but their babies were not necessarily underweight – although some prior literature had similar findings, said Dr. Purdue-Smithe.
She noted that in her study the association was limited to moderate preterm delivery (gestational age, 32-37 weeks) and not with very preterm births (before 32 weeks).
Researchers also assessed adverse pregnancy outcomes by aura phenotype. “Women with migraine with aura have a higher risk of cardiovascular disease later in life, so we hypothesized that aura might be more strongly associated with adverse pregnancy outcomes with underlying vascular pathology,” Dr. Purdue-Smithe said.
Women with and without aura had elevated risks for preterm delivery and gestational hypertension. Those with aura had a slightly higher risk for preeclampsia (RR, 1.51; 95% CI, 1.22-1.88) than those without aura (RR, 1.29; 95% CI, 1.04-1.61).
As the association between migraine and adverse pregnancy outcomes persisted after adjustment for established cardiovascular and obstetric risk factors, “this suggests there may be subclinical factors that are contributing to elevated risks of these outcomes in women with migraine,” said Dr. Purdue-Smithe.
Such factors could include platelet activation, chronic inflammation, and endothelial dysfunction, she added.
While findings of some previous case-control and retrospective studies suggested a possible link between migraine and adverse pregnancy outcomes, until now few large prospective studies have examined the association.
“Strengths of our study include its prospective design, very large sample size, and more complete adjustment for potential prepregnancy confounders,” Dr. Purdue-Smithe said.
Independent risk factor?
In the past, it has been somewhat unclear whether migraine is an independent risk factor for these complications or whether women with migraine just have greater risk factors for adverse pregnancy outcomes.
“Our preliminary findings suggest that migraine is independently associated with these adverse pregnancy outcomes, or at least that’s what it seems,” said Dr. Purdue-Smithe.
The new results could be used by clinicians to “flag” women who may be at risk for complications, she added. “These women may benefit from closer monitoring in pregnancy so that if issues arise, physicians can act quickly.”
She noted that preeclampsia “can come on suddenly and escalate rapidly,” and there are few interventions to treat it besides delivery.
However, low-dose aspirin may be worth investigating. Various health care groups and the U.S. Preventive Services Task Force recommend pregnant women at high risk for preeclampsia take low-dose aspirin (81 mg/d) after 12 weeks’ gestation.
“It would be interesting to see if women with migraine who take aspirin in pregnancy can reduce their risk of preeclampsia, and future research should address this question,” said Dr. Purdue-Smithe.
Additional testing showed that associations with preeclampsia and gestational hypertension did not vary according to age and other obstetrical risks.
The Nurses’ Health Study II did not have information on number and severity of migraine attacks, so the researchers were unable to determine if these factors affect pregnancy outcomes.
“Understanding whether specific migraine features, such as attack frequency, are associated with adverse pregnancy outcomes will be an important area for future research,” said Dr. Purdue-Smithe. She noted prior studies showed the frequency of migraine attacks is related to ischemic stroke and other cardiovascular outcomes.
The authors acknowledged a limitation for the current study: Although migraine history was reported prior to pregnancy, information on migraine aura was collected after most of the pregnancies in the cohort were over. So the findings for migraine aura may have been influenced by participants’ ability to accurately remember their experiences.
Collaboration is key
Commenting on the research, Nina Riggins, MD, PhD, director of the Headache and Traumatic Brain Injury Center in the department of neurosciences at the University of California, San Diego, said the study “stands out” because it distinguishes pregnancy complications between those with and without aura among women with migraine.
Dr. Riggins noted the investigators found the risk of preeclampsia, which on average occurs in about 3%-5% of pregnancies, is higher among women with migraine with aura.
“The good news is that treatments are available,” she said. “Preconception planning should include this discussion for patients living with migraine.”
However, the study did not compare risks for patients who have frequent migraine attacks versus episodic migraine, Dr. Riggins noted. “We need to learn more about whether any treatments can be safe and effective to decrease risks of complications during pregnancy in this population,” she said.
“I believe, ultimately, what this study reveals is that collaboration among primary care, ob.gyn., maternal-fetal medicine specialists, and neurologists will likely benefit pregnant patients with migraine,” Dr. Riggins said.
The study received funding from the National Institutes of Health. Dr. Purdue-Smithe has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests. In a large prospective study, researchers also found a link between migraine with aura and increased preeclampsia risk.
Overall, the findings suggest women with a history of migraine may benefit from enhanced monitoring during pregnancy, said coinvestigator Alexandra Purdue-Smithe, PhD, associate epidemiologist at Brigham and Women’s Hospital and instructor of medicine at Harvard Medical School, Boston. “Our results suggest that migraine history may be an important consideration in obstetric risk assessment,” Dr. Purdue-Smithe added.
The findings will be presented at the 2022 annual meeting of the American Academy of Neurology.
Common neurovascular disorder
Migraine is a common neurovascular disorder, affecting about 15% of adults. The condition carries “a pretty remarkable sex bias” as it affects up to three times more women than men, and about a quarter of women in the reproductive age bracket of 18-44 years, Dr. Purdue-Smithe noted.
Despite this, relatively little is known about migraine and pregnancy risks, she said.
What is known is that women with migraine have a higher burden of cardiovascular risk factors such as obesity and chronic hypertension, and these factors can also increase risk for pregnancy complications, she added.
In the study, researchers analyzed data on 30,555 pregnancies in about 19,000 women without a history of cardiovascular disease, type 2 diabetes, or cancer during a 20-year period ending in 2009.
The data came from the Nurses’ Health Study II, a large prospective cohort study established in 1989 when it enrolled women aged 25-42 years. Participants in the ongoing study complete questionnaires every 2 years, reporting information on various health conditions as well as pregnancy and reproductive events.
The investigators estimated associations of physician-diagnosed prepregnancy migraine with preterm delivery, gestational diabetes, gestational hypertension, preeclampsia, and low birth weight (<2,500 grams [5.5 lb]).
About 11% of the women in the study had migraine diagnosed by a physician before pregnancy.
Researchers adjusted for age at pregnancy, race/ethnicity, age at menarche, and prepregnancy chronic hypertension, body mass index, physical activity, smoking status, alcohol intake, history of infertility, parity, oral contraceptive use, and analgesic use.
‘A bit surprising’
Results showed that compared with women without a history of migraine, those with such a history had higher risk for preterm delivery (relative risk [RR], 1.17; 95% confidence interval [CI], 1.05-1.30), gestational hypertension (RR, 1.28; 95% CI, 1.11-1.48), and preeclampsia (RR, 1.40; 95% CI, 1.19-1.65).
Prepregnancy migraine was not associated with low birth weight (RR, 0.99; 95% CI, 0.85-1.16) or gestational diabetes (RR, 1.05; 95% CI, .91-1.22).
It was a “bit surprising” that women with migraine had a higher risk for preterm delivery but their babies were not necessarily underweight – although some prior literature had similar findings, said Dr. Purdue-Smithe.
She noted that in her study the association was limited to moderate preterm delivery (gestational age, 32-37 weeks) and not with very preterm births (before 32 weeks).
Researchers also assessed adverse pregnancy outcomes by aura phenotype. “Women with migraine with aura have a higher risk of cardiovascular disease later in life, so we hypothesized that aura might be more strongly associated with adverse pregnancy outcomes with underlying vascular pathology,” Dr. Purdue-Smithe said.
Women with and without aura had elevated risks for preterm delivery and gestational hypertension. Those with aura had a slightly higher risk for preeclampsia (RR, 1.51; 95% CI, 1.22-1.88) than those without aura (RR, 1.29; 95% CI, 1.04-1.61).
As the association between migraine and adverse pregnancy outcomes persisted after adjustment for established cardiovascular and obstetric risk factors, “this suggests there may be subclinical factors that are contributing to elevated risks of these outcomes in women with migraine,” said Dr. Purdue-Smithe.
Such factors could include platelet activation, chronic inflammation, and endothelial dysfunction, she added.
While findings of some previous case-control and retrospective studies suggested a possible link between migraine and adverse pregnancy outcomes, until now few large prospective studies have examined the association.
“Strengths of our study include its prospective design, very large sample size, and more complete adjustment for potential prepregnancy confounders,” Dr. Purdue-Smithe said.
Independent risk factor?
In the past, it has been somewhat unclear whether migraine is an independent risk factor for these complications or whether women with migraine just have greater risk factors for adverse pregnancy outcomes.
“Our preliminary findings suggest that migraine is independently associated with these adverse pregnancy outcomes, or at least that’s what it seems,” said Dr. Purdue-Smithe.
The new results could be used by clinicians to “flag” women who may be at risk for complications, she added. “These women may benefit from closer monitoring in pregnancy so that if issues arise, physicians can act quickly.”
She noted that preeclampsia “can come on suddenly and escalate rapidly,” and there are few interventions to treat it besides delivery.
However, low-dose aspirin may be worth investigating. Various health care groups and the U.S. Preventive Services Task Force recommend pregnant women at high risk for preeclampsia take low-dose aspirin (81 mg/d) after 12 weeks’ gestation.
“It would be interesting to see if women with migraine who take aspirin in pregnancy can reduce their risk of preeclampsia, and future research should address this question,” said Dr. Purdue-Smithe.
Additional testing showed that associations with preeclampsia and gestational hypertension did not vary according to age and other obstetrical risks.
The Nurses’ Health Study II did not have information on number and severity of migraine attacks, so the researchers were unable to determine if these factors affect pregnancy outcomes.
“Understanding whether specific migraine features, such as attack frequency, are associated with adverse pregnancy outcomes will be an important area for future research,” said Dr. Purdue-Smithe. She noted prior studies showed the frequency of migraine attacks is related to ischemic stroke and other cardiovascular outcomes.
The authors acknowledged a limitation for the current study: Although migraine history was reported prior to pregnancy, information on migraine aura was collected after most of the pregnancies in the cohort were over. So the findings for migraine aura may have been influenced by participants’ ability to accurately remember their experiences.
Collaboration is key
Commenting on the research, Nina Riggins, MD, PhD, director of the Headache and Traumatic Brain Injury Center in the department of neurosciences at the University of California, San Diego, said the study “stands out” because it distinguishes pregnancy complications between those with and without aura among women with migraine.
Dr. Riggins noted the investigators found the risk of preeclampsia, which on average occurs in about 3%-5% of pregnancies, is higher among women with migraine with aura.
“The good news is that treatments are available,” she said. “Preconception planning should include this discussion for patients living with migraine.”
However, the study did not compare risks for patients who have frequent migraine attacks versus episodic migraine, Dr. Riggins noted. “We need to learn more about whether any treatments can be safe and effective to decrease risks of complications during pregnancy in this population,” she said.
“I believe, ultimately, what this study reveals is that collaboration among primary care, ob.gyn., maternal-fetal medicine specialists, and neurologists will likely benefit pregnant patients with migraine,” Dr. Riggins said.
The study received funding from the National Institutes of Health. Dr. Purdue-Smithe has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AAN 2022
Keto diet in MS tied to less disability, better quality of life
, new research suggests.
High-fat, low-carbohydrate ketogenic diets mimic a fasting state and promote a more efficient use of energy – and have previously been shown to affect immune regulation. The diet helps lower blood sugar in individuals with type 2 diabetes and has been used for years to improve seizure control in patients with epilepsy, researchers note.
However, “there is a paucity of literature on the ketogenic diet in MS currently,” said principal investigator J. Nicholas Brenton, MD, University of Virginia, Charlottesville.
“The current study demonstrates the safety, tolerability, and potential clinical benefits of a ketogenic diet over 6 months in patients with relapsing MS,” Dr. Brenton said.
The were presented at the 2022 annual meeting of the American Academy of Neurology.
Palatable, beneficial
The open-label, uncontrolled study included 65 patients with relapsing MS who followed a ketogenic diet for 6 months. Investigators monitored adherence by daily urine ketone testing.
Patient-reported fatigue, depression, and quality-of-life scores were obtained at baseline, in addition to fasting adipokines and pertinent MS-related clinical outcome metrics. Baseline study metrics were repeated at 3 and/or 6 months while on the ketogenic diet.
Of the patient group, 83% adhered to the ketogenic diet for the full 6-month study period.
The ketogenic diet was associated with reductions in fat mass from baseline to 6 months (41.3 vs. 32.0 kg; P < .001) and a significant decline in fatigue and depression scores, the investigators reported.
MS quality-of-life physical and mental composite scores also improved while on the ketogenic diet (P < .001 for both).
A significant decrease from baseline to 6 months in Expanded Disability Status Scale scores, signifying improvement, was observed (2.3 vs. 1.9; P < .001).
Improvements were also shown on the 6-minute walk (1,631 vs. 1,733 feet; P < .001) and the nine-hole peg test (21.5 vs. 20.3 seconds; P < .001).
At 6 months on the diet, fasting serum leptin was significantly lower (25.5 vs. 14 ng/mL; P <.001), and adiponectin was higher (11.4 vs. 13.5 μg/mL, P = .002).
Justifies further research
The current study builds on an earlier one that Dr. Brenton and colleagues conducted in 2019 that showed that the ketogenic diet was feasible in patients with MS. “Our data justify the need for future studies of ketogenic diets as a complementary therapeutic approach to the treatment of MS,” Dr. Brenton said.
He noted that there may be multiple mechanisms of benefit when considering the ketogenic diet. “One avenue is via reduction in total body fat. This is an important aspect as we continue to learn more about the role of obesity and fat-derived inflammation in MS,” Dr. Brenton said.
“Ketogenic diets also have immunomodulatory properties,” such as the capacity to reduce oxidative damage from metabolic stress, increase mitochondrial biogenesis, and reduce systemic inflammation, he added. “These intrinsic properties of the ketogenic diet make it appealing to study in immune-mediated diseases, such as MS.”
Dr. Brenton cautioned that the data demonstrate the diet’s safety over 6 months but that the study was not designed to assess its long-term implications in MS. “Thus, while our results support the rationale for a larger-scale study of ketogenic diets as a complementary treatment for MS, our data does not support its widespread adoption outside of a clinical trial,” he said.
Remarkable adherence
Commenting on the study, Shaheen E. Lakhan, MD, PhD, a neurologist in Boston, noted that “variations of the ketogenic diet have been popularized in the general population for weight loss and further studied for other medical conditions [that are] largely immune-related, including MS.”
He noted that it was “remarkable” that the vast majority of study participants with MS adhered to the very regimented ketogenic diet for 6 months.
Seeing this translate into the real world “will be the next milestone, in addition to its impact on relapses and brain lesions as seen on MRI,” which are the classic markers of MS, said Dr. Lakhan, who was not involved with the research.
He cautioned that “even if one can follow the ketogenic diet, certain conditions can be made worse. This includes kidney stones, liver disease, reflux, constipation, and other metabolic disorders.”
The study was funded by the National Center for Advancing Translational Sciences of the National Institutes of Health and by the ZiMS Foundation. Dr. Brenton and Dr. Lakhan have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests.
High-fat, low-carbohydrate ketogenic diets mimic a fasting state and promote a more efficient use of energy – and have previously been shown to affect immune regulation. The diet helps lower blood sugar in individuals with type 2 diabetes and has been used for years to improve seizure control in patients with epilepsy, researchers note.
However, “there is a paucity of literature on the ketogenic diet in MS currently,” said principal investigator J. Nicholas Brenton, MD, University of Virginia, Charlottesville.
“The current study demonstrates the safety, tolerability, and potential clinical benefits of a ketogenic diet over 6 months in patients with relapsing MS,” Dr. Brenton said.
The were presented at the 2022 annual meeting of the American Academy of Neurology.
Palatable, beneficial
The open-label, uncontrolled study included 65 patients with relapsing MS who followed a ketogenic diet for 6 months. Investigators monitored adherence by daily urine ketone testing.
Patient-reported fatigue, depression, and quality-of-life scores were obtained at baseline, in addition to fasting adipokines and pertinent MS-related clinical outcome metrics. Baseline study metrics were repeated at 3 and/or 6 months while on the ketogenic diet.
Of the patient group, 83% adhered to the ketogenic diet for the full 6-month study period.
The ketogenic diet was associated with reductions in fat mass from baseline to 6 months (41.3 vs. 32.0 kg; P < .001) and a significant decline in fatigue and depression scores, the investigators reported.
MS quality-of-life physical and mental composite scores also improved while on the ketogenic diet (P < .001 for both).
A significant decrease from baseline to 6 months in Expanded Disability Status Scale scores, signifying improvement, was observed (2.3 vs. 1.9; P < .001).
Improvements were also shown on the 6-minute walk (1,631 vs. 1,733 feet; P < .001) and the nine-hole peg test (21.5 vs. 20.3 seconds; P < .001).
At 6 months on the diet, fasting serum leptin was significantly lower (25.5 vs. 14 ng/mL; P <.001), and adiponectin was higher (11.4 vs. 13.5 μg/mL, P = .002).
Justifies further research
The current study builds on an earlier one that Dr. Brenton and colleagues conducted in 2019 that showed that the ketogenic diet was feasible in patients with MS. “Our data justify the need for future studies of ketogenic diets as a complementary therapeutic approach to the treatment of MS,” Dr. Brenton said.
He noted that there may be multiple mechanisms of benefit when considering the ketogenic diet. “One avenue is via reduction in total body fat. This is an important aspect as we continue to learn more about the role of obesity and fat-derived inflammation in MS,” Dr. Brenton said.
“Ketogenic diets also have immunomodulatory properties,” such as the capacity to reduce oxidative damage from metabolic stress, increase mitochondrial biogenesis, and reduce systemic inflammation, he added. “These intrinsic properties of the ketogenic diet make it appealing to study in immune-mediated diseases, such as MS.”
Dr. Brenton cautioned that the data demonstrate the diet’s safety over 6 months but that the study was not designed to assess its long-term implications in MS. “Thus, while our results support the rationale for a larger-scale study of ketogenic diets as a complementary treatment for MS, our data does not support its widespread adoption outside of a clinical trial,” he said.
Remarkable adherence
Commenting on the study, Shaheen E. Lakhan, MD, PhD, a neurologist in Boston, noted that “variations of the ketogenic diet have been popularized in the general population for weight loss and further studied for other medical conditions [that are] largely immune-related, including MS.”
He noted that it was “remarkable” that the vast majority of study participants with MS adhered to the very regimented ketogenic diet for 6 months.
Seeing this translate into the real world “will be the next milestone, in addition to its impact on relapses and brain lesions as seen on MRI,” which are the classic markers of MS, said Dr. Lakhan, who was not involved with the research.
He cautioned that “even if one can follow the ketogenic diet, certain conditions can be made worse. This includes kidney stones, liver disease, reflux, constipation, and other metabolic disorders.”
The study was funded by the National Center for Advancing Translational Sciences of the National Institutes of Health and by the ZiMS Foundation. Dr. Brenton and Dr. Lakhan have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests.
High-fat, low-carbohydrate ketogenic diets mimic a fasting state and promote a more efficient use of energy – and have previously been shown to affect immune regulation. The diet helps lower blood sugar in individuals with type 2 diabetes and has been used for years to improve seizure control in patients with epilepsy, researchers note.
However, “there is a paucity of literature on the ketogenic diet in MS currently,” said principal investigator J. Nicholas Brenton, MD, University of Virginia, Charlottesville.
“The current study demonstrates the safety, tolerability, and potential clinical benefits of a ketogenic diet over 6 months in patients with relapsing MS,” Dr. Brenton said.
The were presented at the 2022 annual meeting of the American Academy of Neurology.
Palatable, beneficial
The open-label, uncontrolled study included 65 patients with relapsing MS who followed a ketogenic diet for 6 months. Investigators monitored adherence by daily urine ketone testing.
Patient-reported fatigue, depression, and quality-of-life scores were obtained at baseline, in addition to fasting adipokines and pertinent MS-related clinical outcome metrics. Baseline study metrics were repeated at 3 and/or 6 months while on the ketogenic diet.
Of the patient group, 83% adhered to the ketogenic diet for the full 6-month study period.
The ketogenic diet was associated with reductions in fat mass from baseline to 6 months (41.3 vs. 32.0 kg; P < .001) and a significant decline in fatigue and depression scores, the investigators reported.
MS quality-of-life physical and mental composite scores also improved while on the ketogenic diet (P < .001 for both).
A significant decrease from baseline to 6 months in Expanded Disability Status Scale scores, signifying improvement, was observed (2.3 vs. 1.9; P < .001).
Improvements were also shown on the 6-minute walk (1,631 vs. 1,733 feet; P < .001) and the nine-hole peg test (21.5 vs. 20.3 seconds; P < .001).
At 6 months on the diet, fasting serum leptin was significantly lower (25.5 vs. 14 ng/mL; P <.001), and adiponectin was higher (11.4 vs. 13.5 μg/mL, P = .002).
Justifies further research
The current study builds on an earlier one that Dr. Brenton and colleagues conducted in 2019 that showed that the ketogenic diet was feasible in patients with MS. “Our data justify the need for future studies of ketogenic diets as a complementary therapeutic approach to the treatment of MS,” Dr. Brenton said.
He noted that there may be multiple mechanisms of benefit when considering the ketogenic diet. “One avenue is via reduction in total body fat. This is an important aspect as we continue to learn more about the role of obesity and fat-derived inflammation in MS,” Dr. Brenton said.
“Ketogenic diets also have immunomodulatory properties,” such as the capacity to reduce oxidative damage from metabolic stress, increase mitochondrial biogenesis, and reduce systemic inflammation, he added. “These intrinsic properties of the ketogenic diet make it appealing to study in immune-mediated diseases, such as MS.”
Dr. Brenton cautioned that the data demonstrate the diet’s safety over 6 months but that the study was not designed to assess its long-term implications in MS. “Thus, while our results support the rationale for a larger-scale study of ketogenic diets as a complementary treatment for MS, our data does not support its widespread adoption outside of a clinical trial,” he said.
Remarkable adherence
Commenting on the study, Shaheen E. Lakhan, MD, PhD, a neurologist in Boston, noted that “variations of the ketogenic diet have been popularized in the general population for weight loss and further studied for other medical conditions [that are] largely immune-related, including MS.”
He noted that it was “remarkable” that the vast majority of study participants with MS adhered to the very regimented ketogenic diet for 6 months.
Seeing this translate into the real world “will be the next milestone, in addition to its impact on relapses and brain lesions as seen on MRI,” which are the classic markers of MS, said Dr. Lakhan, who was not involved with the research.
He cautioned that “even if one can follow the ketogenic diet, certain conditions can be made worse. This includes kidney stones, liver disease, reflux, constipation, and other metabolic disorders.”
The study was funded by the National Center for Advancing Translational Sciences of the National Institutes of Health and by the ZiMS Foundation. Dr. Brenton and Dr. Lakhan have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AAN 2022
Pembro provides DFS benefit in early NSCLC
Adjuvant pembrolizumab significantly improves disease-free survival (DFS) compared to placebo in patients with early-stage non–small cell lung cancer (NSCLC) who have undergone complete resection, according to findings from the phase 3 PEARLS/KEYNOTE-091 (PEARLS) study.
Patients in the pembrolizumab arm demonstrated median DFS nearly 12 months longer than those in the placebo arm (53.6 vs. 42.0 months). Investigators observed a DFS benefit for patients with any programmed death-ligand 1 (PD-L1) expression.
“We believe that pembrolizumab has the potential to become a new adjuvant treatment option for patient with [stage IB to IIIA] non–small cell lung cancer following complete resection and adjuvant chemotherapy when recommended,” concluded first author Luis Paz-Ares, MD, chair of the clinical research unit at Hospital Universitario 12 de Octubre, CNIO & Universidad Complutense, Madrid. “Pembrolizumab provided a benefit regardless of pathological stage and PD-L1 progression subgroup.”
The findings were presented by Dr. Paz-Ares at the European Society for Medical Oncology (ESMO) March virtual plenary session and published March 17 in Annals of Oncology.
Pembrolizumab is the standard treatment for patients with advanced NSCLC, but its efficacy in early-stage disease remains unclear. To determine whether patients with early-stage disease benefit from pembrolizumab, Dr. Paz-Ares and colleagues randomized 1,177 adults with stage IB, II, or IIIA NSCLC to 200 mg of pembrolizumab (n = 590) or placebo (n = 587) every 3 weeks.
All patients had Eastern Cooperative Oncology Group performance status of 0-1, and any level of PD-L1 expression. Of the study participants, 168 in the pembrolizumab arm and 165 in the placebo arm had PD-L1 expression and a tumor proportion score (TPS) of at least 50%.
Overall, patients receiving pembrolizumab had a DFS of 53.6 months compared to 42.0 months in the placebo arm (hazard ratio [HR], 0.76; P = .0014). The DFS benefit was generally consistent across patients with PD-L1 TPS <1%, 1%-49%, and ≥50%. In the subset of patients with PD-L1 TPS ≥50%, a slightly higher percentage of patients in the pembrolizumab group demonstrated DFS at 18 months (71.7% vs. 70.2%), but the difference did not reach statistical significance (HR, 0.82; P = .14).
Overall survival (OS) at 18 months was 91.7% in the treatment arm and 91.3% in the placebo arm (HR, 0.87; P = .17), but the data were immature.
“The disease-free survival benefit was observed across most prespecified subgroups,” Dr. Paz-Ares said.
No new safety concerns were raised. Grade 3 or greater adverse events occurred in 34.1% of patients in the treatment arm and 25.8% in the placebo arm. Adverse events led to discontinuation in 19.8% of patients receiving pembrolizumab and 5.9% of patients in the placebo group.
Invited discussant Martin Reck, MD, said these findings represent forward progress. “We do see many patients with distant relapse, which indicates that we have to improve our control of the systemic relapse,” said Dr. Reck, head of the department of thoracic oncology and the clinical trial department at the Lungen Clinic Grosshansdorf, Germany.
Prior data provide a rationale for using immune checkpoint inhibition in early-stage NSCLC, and both the PEARLS study and the IMpower010 trial evaluating atezolizumab in a similar setting have demonstrated relevant improvements in DFS.
“I think we are entering the times of perioperative immunotherapies. We are seeing the first signals of efficacy for adjuvant immunotherapy in two large, randomized trials,” Dr. Reck said.
Based on the PEARLS trial results, Dr. Reck said that PD-L1 appears to have predictive and prognostic value but noted that “several other clinical trials say PD-L1 expression is a poor prognostic marker” for sensitivity to immune checkpoint inhibitor. Given this potential inconsistency, Dr. Reck called for further follow-up in this patient population and for studies in larger groups of patients to further delineate the role of PD-L1 as well as EGFR mutations and adjuvant chemotherapy in patients with early NSCLC.
The PEARLS study was funded by Merck Sharp & Dohme Corp. Dr. Paz-Ares and Dr. Reck disclosed numerous relationships with pharmaceutical companies.
Adjuvant pembrolizumab significantly improves disease-free survival (DFS) compared to placebo in patients with early-stage non–small cell lung cancer (NSCLC) who have undergone complete resection, according to findings from the phase 3 PEARLS/KEYNOTE-091 (PEARLS) study.
Patients in the pembrolizumab arm demonstrated median DFS nearly 12 months longer than those in the placebo arm (53.6 vs. 42.0 months). Investigators observed a DFS benefit for patients with any programmed death-ligand 1 (PD-L1) expression.
“We believe that pembrolizumab has the potential to become a new adjuvant treatment option for patient with [stage IB to IIIA] non–small cell lung cancer following complete resection and adjuvant chemotherapy when recommended,” concluded first author Luis Paz-Ares, MD, chair of the clinical research unit at Hospital Universitario 12 de Octubre, CNIO & Universidad Complutense, Madrid. “Pembrolizumab provided a benefit regardless of pathological stage and PD-L1 progression subgroup.”
The findings were presented by Dr. Paz-Ares at the European Society for Medical Oncology (ESMO) March virtual plenary session and published March 17 in Annals of Oncology.
Pembrolizumab is the standard treatment for patients with advanced NSCLC, but its efficacy in early-stage disease remains unclear. To determine whether patients with early-stage disease benefit from pembrolizumab, Dr. Paz-Ares and colleagues randomized 1,177 adults with stage IB, II, or IIIA NSCLC to 200 mg of pembrolizumab (n = 590) or placebo (n = 587) every 3 weeks.
All patients had Eastern Cooperative Oncology Group performance status of 0-1, and any level of PD-L1 expression. Of the study participants, 168 in the pembrolizumab arm and 165 in the placebo arm had PD-L1 expression and a tumor proportion score (TPS) of at least 50%.
Overall, patients receiving pembrolizumab had a DFS of 53.6 months compared to 42.0 months in the placebo arm (hazard ratio [HR], 0.76; P = .0014). The DFS benefit was generally consistent across patients with PD-L1 TPS <1%, 1%-49%, and ≥50%. In the subset of patients with PD-L1 TPS ≥50%, a slightly higher percentage of patients in the pembrolizumab group demonstrated DFS at 18 months (71.7% vs. 70.2%), but the difference did not reach statistical significance (HR, 0.82; P = .14).
Overall survival (OS) at 18 months was 91.7% in the treatment arm and 91.3% in the placebo arm (HR, 0.87; P = .17), but the data were immature.
“The disease-free survival benefit was observed across most prespecified subgroups,” Dr. Paz-Ares said.
No new safety concerns were raised. Grade 3 or greater adverse events occurred in 34.1% of patients in the treatment arm and 25.8% in the placebo arm. Adverse events led to discontinuation in 19.8% of patients receiving pembrolizumab and 5.9% of patients in the placebo group.
Invited discussant Martin Reck, MD, said these findings represent forward progress. “We do see many patients with distant relapse, which indicates that we have to improve our control of the systemic relapse,” said Dr. Reck, head of the department of thoracic oncology and the clinical trial department at the Lungen Clinic Grosshansdorf, Germany.
Prior data provide a rationale for using immune checkpoint inhibition in early-stage NSCLC, and both the PEARLS study and the IMpower010 trial evaluating atezolizumab in a similar setting have demonstrated relevant improvements in DFS.
“I think we are entering the times of perioperative immunotherapies. We are seeing the first signals of efficacy for adjuvant immunotherapy in two large, randomized trials,” Dr. Reck said.
Based on the PEARLS trial results, Dr. Reck said that PD-L1 appears to have predictive and prognostic value but noted that “several other clinical trials say PD-L1 expression is a poor prognostic marker” for sensitivity to immune checkpoint inhibitor. Given this potential inconsistency, Dr. Reck called for further follow-up in this patient population and for studies in larger groups of patients to further delineate the role of PD-L1 as well as EGFR mutations and adjuvant chemotherapy in patients with early NSCLC.
The PEARLS study was funded by Merck Sharp & Dohme Corp. Dr. Paz-Ares and Dr. Reck disclosed numerous relationships with pharmaceutical companies.
Adjuvant pembrolizumab significantly improves disease-free survival (DFS) compared to placebo in patients with early-stage non–small cell lung cancer (NSCLC) who have undergone complete resection, according to findings from the phase 3 PEARLS/KEYNOTE-091 (PEARLS) study.
Patients in the pembrolizumab arm demonstrated median DFS nearly 12 months longer than those in the placebo arm (53.6 vs. 42.0 months). Investigators observed a DFS benefit for patients with any programmed death-ligand 1 (PD-L1) expression.
“We believe that pembrolizumab has the potential to become a new adjuvant treatment option for patient with [stage IB to IIIA] non–small cell lung cancer following complete resection and adjuvant chemotherapy when recommended,” concluded first author Luis Paz-Ares, MD, chair of the clinical research unit at Hospital Universitario 12 de Octubre, CNIO & Universidad Complutense, Madrid. “Pembrolizumab provided a benefit regardless of pathological stage and PD-L1 progression subgroup.”
The findings were presented by Dr. Paz-Ares at the European Society for Medical Oncology (ESMO) March virtual plenary session and published March 17 in Annals of Oncology.
Pembrolizumab is the standard treatment for patients with advanced NSCLC, but its efficacy in early-stage disease remains unclear. To determine whether patients with early-stage disease benefit from pembrolizumab, Dr. Paz-Ares and colleagues randomized 1,177 adults with stage IB, II, or IIIA NSCLC to 200 mg of pembrolizumab (n = 590) or placebo (n = 587) every 3 weeks.
All patients had Eastern Cooperative Oncology Group performance status of 0-1, and any level of PD-L1 expression. Of the study participants, 168 in the pembrolizumab arm and 165 in the placebo arm had PD-L1 expression and a tumor proportion score (TPS) of at least 50%.
Overall, patients receiving pembrolizumab had a DFS of 53.6 months compared to 42.0 months in the placebo arm (hazard ratio [HR], 0.76; P = .0014). The DFS benefit was generally consistent across patients with PD-L1 TPS <1%, 1%-49%, and ≥50%. In the subset of patients with PD-L1 TPS ≥50%, a slightly higher percentage of patients in the pembrolizumab group demonstrated DFS at 18 months (71.7% vs. 70.2%), but the difference did not reach statistical significance (HR, 0.82; P = .14).
Overall survival (OS) at 18 months was 91.7% in the treatment arm and 91.3% in the placebo arm (HR, 0.87; P = .17), but the data were immature.
“The disease-free survival benefit was observed across most prespecified subgroups,” Dr. Paz-Ares said.
No new safety concerns were raised. Grade 3 or greater adverse events occurred in 34.1% of patients in the treatment arm and 25.8% in the placebo arm. Adverse events led to discontinuation in 19.8% of patients receiving pembrolizumab and 5.9% of patients in the placebo group.
Invited discussant Martin Reck, MD, said these findings represent forward progress. “We do see many patients with distant relapse, which indicates that we have to improve our control of the systemic relapse,” said Dr. Reck, head of the department of thoracic oncology and the clinical trial department at the Lungen Clinic Grosshansdorf, Germany.
Prior data provide a rationale for using immune checkpoint inhibition in early-stage NSCLC, and both the PEARLS study and the IMpower010 trial evaluating atezolizumab in a similar setting have demonstrated relevant improvements in DFS.
“I think we are entering the times of perioperative immunotherapies. We are seeing the first signals of efficacy for adjuvant immunotherapy in two large, randomized trials,” Dr. Reck said.
Based on the PEARLS trial results, Dr. Reck said that PD-L1 appears to have predictive and prognostic value but noted that “several other clinical trials say PD-L1 expression is a poor prognostic marker” for sensitivity to immune checkpoint inhibitor. Given this potential inconsistency, Dr. Reck called for further follow-up in this patient population and for studies in larger groups of patients to further delineate the role of PD-L1 as well as EGFR mutations and adjuvant chemotherapy in patients with early NSCLC.
The PEARLS study was funded by Merck Sharp & Dohme Corp. Dr. Paz-Ares and Dr. Reck disclosed numerous relationships with pharmaceutical companies.
FROM THE ESMO MARCH PLENARY
New COVID combo-variant XE found in U.K.
As of last week, the U.K. Health Security Agency had found 637 cases of the variant, known as XE. The earliest case was found Jan. 19.
The new strain is known as a recombinant, which means it is a combination of two variants or viruses.
XE makes up less than 1% of sequenced cases in the United Kingdom so far, and there is no evidence yet that the strain leads to more severe disease or less vaccine protection.
“Right now, there’s really no public health concern,” John Brownstein, PhD, an epidemiologist and chief innovation officer at Boston Children’s Hospital, told ABC. “Recombinant variants happen over and over. In fact, the reason that this is the XE variant recombinant is that we’ve had XA, XB, XC, XD already, and none of those have turned out to be any real concern.”
A World Health Organization update published March 29 notes XE’s high transmissibility and says it may have a growth advantage of 10% over the BA.2 subvariant that now makes up more than 70% of cases in the United States.
A version of this article first appeared on WebMD.com.
As of last week, the U.K. Health Security Agency had found 637 cases of the variant, known as XE. The earliest case was found Jan. 19.
The new strain is known as a recombinant, which means it is a combination of two variants or viruses.
XE makes up less than 1% of sequenced cases in the United Kingdom so far, and there is no evidence yet that the strain leads to more severe disease or less vaccine protection.
“Right now, there’s really no public health concern,” John Brownstein, PhD, an epidemiologist and chief innovation officer at Boston Children’s Hospital, told ABC. “Recombinant variants happen over and over. In fact, the reason that this is the XE variant recombinant is that we’ve had XA, XB, XC, XD already, and none of those have turned out to be any real concern.”
A World Health Organization update published March 29 notes XE’s high transmissibility and says it may have a growth advantage of 10% over the BA.2 subvariant that now makes up more than 70% of cases in the United States.
A version of this article first appeared on WebMD.com.
As of last week, the U.K. Health Security Agency had found 637 cases of the variant, known as XE. The earliest case was found Jan. 19.
The new strain is known as a recombinant, which means it is a combination of two variants or viruses.
XE makes up less than 1% of sequenced cases in the United Kingdom so far, and there is no evidence yet that the strain leads to more severe disease or less vaccine protection.
“Right now, there’s really no public health concern,” John Brownstein, PhD, an epidemiologist and chief innovation officer at Boston Children’s Hospital, told ABC. “Recombinant variants happen over and over. In fact, the reason that this is the XE variant recombinant is that we’ve had XA, XB, XC, XD already, and none of those have turned out to be any real concern.”
A World Health Organization update published March 29 notes XE’s high transmissibility and says it may have a growth advantage of 10% over the BA.2 subvariant that now makes up more than 70% of cases in the United States.
A version of this article first appeared on WebMD.com.
Children and COVID-19: Decline in new cases may be leveling off
Even as a number of states see increases in new COVID-19 cases among all ages, the trend remains downward for children, albeit at a slower pace than in recent weeks, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
New pediatric cases in the United States totaled 27,521 for the most recent week, March 25-31, down by 5.2% from the previous week. Earlier weekly declines, going backward through March and into late February, were 9.3%, 23%, 39.5%, and 46%, according to data collected by the AAP and CHA from state and territorial health agencies. The lowest weekly total recorded since the initial wave in 2020 was just under 8,500 during the week of June 18-24, 2021.
Reported COVID-19 cases in children now total over 12.8 million since the beginning of the pandemic in March 2020, and those infections represent 19.0% of all cases. That share of new cases has not increased in the last 7 weeks, the AAP and CHA noted in their weekly COVID report, suggesting that children have not been bearing a disproportionate share of the declining Omicron burden.
As for Omicron, the BA.2 subvariant now makes up about 55% of COVID-19 infections, the Centers for Disease Control and Prevention said in its COVID Data Tracker Weekly Review, and New York, Massachusetts, and New Jersey are among the states reporting BA.2-driven increases in new cases of as much as 30%, the New York Times said.
Rates of new cases for the latest week available (March 27 to April 2) and at their Omicron peaks in January were 11.3 per 100,000 and 1,011 per 100,000 (ages 0-4 years), 12.5 and 1,505 per 100,000 (5-11 years), 12.7 and 1,779 per 100,000 (12-15 years), and 13.1 and 1,982 per 100,000 (16-17 years), the CDC said on its COVID Data Tracker.
Hospitalization rates, however, were a bit of a mixed bag. The last 2 weeks (March 13-19 and March 20-26) of data available from the CDC’s COVID-NET show that hospitalizations were up slightly in children aged 0-4 years (1.3 per 100,000 to 1.4 per 100,000), down for 5- to 11-year-olds (0.6 to 0.2), and steady for those aged 12-17 (0.4 to 0.4). COVID-NET collects data from nearly 100 counties in 10 states and from a separate four-state network.
Vaccinations got a small boost in the last week, the first one since early February. Initial doses and completions climbed slightly in the 12- to 17-year-olds, while just first doses were up a bit among the 5- to 11-year-olds during the week of March 24-30, compared with the previous week, although both groups are still well below the highest counts recorded so far in 2022, which are, in turn, far short of 2021’s peaks, according to CDC data analyzed by the AAP.
Even as a number of states see increases in new COVID-19 cases among all ages, the trend remains downward for children, albeit at a slower pace than in recent weeks, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
New pediatric cases in the United States totaled 27,521 for the most recent week, March 25-31, down by 5.2% from the previous week. Earlier weekly declines, going backward through March and into late February, were 9.3%, 23%, 39.5%, and 46%, according to data collected by the AAP and CHA from state and territorial health agencies. The lowest weekly total recorded since the initial wave in 2020 was just under 8,500 during the week of June 18-24, 2021.
Reported COVID-19 cases in children now total over 12.8 million since the beginning of the pandemic in March 2020, and those infections represent 19.0% of all cases. That share of new cases has not increased in the last 7 weeks, the AAP and CHA noted in their weekly COVID report, suggesting that children have not been bearing a disproportionate share of the declining Omicron burden.
As for Omicron, the BA.2 subvariant now makes up about 55% of COVID-19 infections, the Centers for Disease Control and Prevention said in its COVID Data Tracker Weekly Review, and New York, Massachusetts, and New Jersey are among the states reporting BA.2-driven increases in new cases of as much as 30%, the New York Times said.
Rates of new cases for the latest week available (March 27 to April 2) and at their Omicron peaks in January were 11.3 per 100,000 and 1,011 per 100,000 (ages 0-4 years), 12.5 and 1,505 per 100,000 (5-11 years), 12.7 and 1,779 per 100,000 (12-15 years), and 13.1 and 1,982 per 100,000 (16-17 years), the CDC said on its COVID Data Tracker.
Hospitalization rates, however, were a bit of a mixed bag. The last 2 weeks (March 13-19 and March 20-26) of data available from the CDC’s COVID-NET show that hospitalizations were up slightly in children aged 0-4 years (1.3 per 100,000 to 1.4 per 100,000), down for 5- to 11-year-olds (0.6 to 0.2), and steady for those aged 12-17 (0.4 to 0.4). COVID-NET collects data from nearly 100 counties in 10 states and from a separate four-state network.
Vaccinations got a small boost in the last week, the first one since early February. Initial doses and completions climbed slightly in the 12- to 17-year-olds, while just first doses were up a bit among the 5- to 11-year-olds during the week of March 24-30, compared with the previous week, although both groups are still well below the highest counts recorded so far in 2022, which are, in turn, far short of 2021’s peaks, according to CDC data analyzed by the AAP.
Even as a number of states see increases in new COVID-19 cases among all ages, the trend remains downward for children, albeit at a slower pace than in recent weeks, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
New pediatric cases in the United States totaled 27,521 for the most recent week, March 25-31, down by 5.2% from the previous week. Earlier weekly declines, going backward through March and into late February, were 9.3%, 23%, 39.5%, and 46%, according to data collected by the AAP and CHA from state and territorial health agencies. The lowest weekly total recorded since the initial wave in 2020 was just under 8,500 during the week of June 18-24, 2021.
Reported COVID-19 cases in children now total over 12.8 million since the beginning of the pandemic in March 2020, and those infections represent 19.0% of all cases. That share of new cases has not increased in the last 7 weeks, the AAP and CHA noted in their weekly COVID report, suggesting that children have not been bearing a disproportionate share of the declining Omicron burden.
As for Omicron, the BA.2 subvariant now makes up about 55% of COVID-19 infections, the Centers for Disease Control and Prevention said in its COVID Data Tracker Weekly Review, and New York, Massachusetts, and New Jersey are among the states reporting BA.2-driven increases in new cases of as much as 30%, the New York Times said.
Rates of new cases for the latest week available (March 27 to April 2) and at their Omicron peaks in January were 11.3 per 100,000 and 1,011 per 100,000 (ages 0-4 years), 12.5 and 1,505 per 100,000 (5-11 years), 12.7 and 1,779 per 100,000 (12-15 years), and 13.1 and 1,982 per 100,000 (16-17 years), the CDC said on its COVID Data Tracker.
Hospitalization rates, however, were a bit of a mixed bag. The last 2 weeks (March 13-19 and March 20-26) of data available from the CDC’s COVID-NET show that hospitalizations were up slightly in children aged 0-4 years (1.3 per 100,000 to 1.4 per 100,000), down for 5- to 11-year-olds (0.6 to 0.2), and steady for those aged 12-17 (0.4 to 0.4). COVID-NET collects data from nearly 100 counties in 10 states and from a separate four-state network.
Vaccinations got a small boost in the last week, the first one since early February. Initial doses and completions climbed slightly in the 12- to 17-year-olds, while just first doses were up a bit among the 5- to 11-year-olds during the week of March 24-30, compared with the previous week, although both groups are still well below the highest counts recorded so far in 2022, which are, in turn, far short of 2021’s peaks, according to CDC data analyzed by the AAP.
Photoprotection strategies for melasma are increasing
BOSTON – Untinted chemical sunscreens on the market are not sufficient to protect the skin from the effects of visible light, complicating sun protection efforts for patients with melasma and other conditions aggravated by sun exposure, according to Henry W. Lim, MD.
A , Dr. Lim, former chair of the department of dermatology at Henry Ford Health, Detroit, said at the annual meeting of the American Academy of Dermatology. Tinted sunscreens contain iron oxides; some also contain pigmentary titanium dioxide.

“Black, red, and yellow iron oxide all reflect visible light,” he added, noting that currently, there are no regulations as to how tinted sunscreens are marketed, making it difficult for practicing clinicians to advise patients about what products to choose. However, he said, “unlike ‘SPF’ and ‘broad spectrum’ labeling, there is no specific guidance on tinted sunscreens. “ ‘Universal’ shade is a good start but might not be ideal for users with very fair or deep skin tones,” he noted.
In December 2021, a guide to tinted sunscreens, written by Dr. Lim and colleagues, was published, recommending that consumers choose a product that contains iron oxides, is labeled as broad spectrum, and has an SPF of at least 30.
A comprehensive list of 54 tinted sunscreens with an SPF of 30 or greater that contain iron oxide is also available . The authors of the guide contributed to this resource, which lists sunscreens by average price per ounce.
At the meeting, Dr. Lim highlighted tinted sunscreens that cost about $20 or less per ounce. They include Supergoop 100% Mineral CC Cream (SPF 50); Bare Republic Mineral Tinted Face Sunscreen Lotion (SPF 30); CeraVe Hydrating Sunscreen with Sheer Tint (SPF 30); Tizo Ultra Zinc Body & Face Sunscreen (SPF 40); Vichy Capital Soleil Tinted Face Mineral Sunscreen (SPF 60); EltaMD UV Elements Tinted (SPF 44); La Roche-Posay Anthelios Ultra-Light Tinted Mineral (SPF 50), SkinMedica Essential Defense Mineral Shield (SPF 32), ISDIN Eryfotona Ageless Ultralight Tinted Mineral Sunscreen (SPF 50), and SkinCeuticals Physical Fusion UV Defense (SPF 50).
Sunscreens with antioxidants
Sunscreens with biologically active antioxidants may be another option for patients with melasma. A proof-of-concept study that Dr. Lim and colleagues conducted in 20 patients found that application of a blend of topical antioxidants (2%) was associated with less erythema at the application sites among those with skin phototypes I-III and less pigmentation at the application sites among those with skin phototypes IV-VI after exposure to visible light and UVA-1, compared with controls.
Certain antioxidants have been added to sunscreens currently on the market, including niacinamide (vitamin B3), licochalcone A, carotenoids (beta-carotene), vitamin E, vitamin C, glycyrrhetinic acid, and diethylhexyl syringylidenemalonate.
A recently published paper on the role of antioxidants and free radical quenchers in protecting skin from visible light referred to unpublished data from Dr. Lim (the first author) and colleagues, which demonstrated a significant reduction in visual light–induced hyperpigmentation on skin with sunscreen that contained the antioxidants vitamin E, vitamin C, diethylhexyl syringylidenemalonate, licochalcone A, and a glycyrrhetinic acid, compared with sunscreen that had no antioxidants.
Novel filters
Another emerging option is sunscreen with new filters that cover UVA-1 and visible light. In a randomized, controlled trial of 19 patients, researchers evaluated the addition of methoxypropylamino cyclohexenylidene ethoxyethylcyanoacetate (MCE) absorber, a new UVA-1 filter known as Mexoryl 400, which has a peak absorption of 385 nm, to a sunscreen formulation.
“Currently, peak absorption in the U.S. is with avobenzone, which peaks at about 357 nm,” but MCE “covers a longer spectrum of UVA-1,” Dr. Lim said. The researchers found that the addition of MCE reduced UVA-1-induced dermal and epidermal alterations at cellular, biochemical, and molecular levels; and decreased UVA-1-induced pigmentation.
Another relatively new filter, phenylene bis-diphenyltriazine (also known as TriAsorB) not only protects against UVA but it extends into the blue light portion of visible light, according to a recently published paper. According to a press release from Pierre Fabre, which has developed the filter, studies have shown that TriAsorB is not toxic for three key species of marine biodiversity: a coral species, a phytoplankton species, and a zooplankton.
This filter and MCE are available in Europe but not in the United States.
Dr. Lim reported that he is an investigator for Incyte, L’Oréal, Pfizer, and the Patient-Centered Outcomes Research Institute.
BOSTON – Untinted chemical sunscreens on the market are not sufficient to protect the skin from the effects of visible light, complicating sun protection efforts for patients with melasma and other conditions aggravated by sun exposure, according to Henry W. Lim, MD.
A , Dr. Lim, former chair of the department of dermatology at Henry Ford Health, Detroit, said at the annual meeting of the American Academy of Dermatology. Tinted sunscreens contain iron oxides; some also contain pigmentary titanium dioxide.
“Black, red, and yellow iron oxide all reflect visible light,” he added, noting that currently, there are no regulations as to how tinted sunscreens are marketed, making it difficult for practicing clinicians to advise patients about what products to choose. However, he said, “unlike ‘SPF’ and ‘broad spectrum’ labeling, there is no specific guidance on tinted sunscreens. “ ‘Universal’ shade is a good start but might not be ideal for users with very fair or deep skin tones,” he noted.
In December 2021, a guide to tinted sunscreens, written by Dr. Lim and colleagues, was published, recommending that consumers choose a product that contains iron oxides, is labeled as broad spectrum, and has an SPF of at least 30.
A comprehensive list of 54 tinted sunscreens with an SPF of 30 or greater that contain iron oxide is also available . The authors of the guide contributed to this resource, which lists sunscreens by average price per ounce.
At the meeting, Dr. Lim highlighted tinted sunscreens that cost about $20 or less per ounce. They include Supergoop 100% Mineral CC Cream (SPF 50); Bare Republic Mineral Tinted Face Sunscreen Lotion (SPF 30); CeraVe Hydrating Sunscreen with Sheer Tint (SPF 30); Tizo Ultra Zinc Body & Face Sunscreen (SPF 40); Vichy Capital Soleil Tinted Face Mineral Sunscreen (SPF 60); EltaMD UV Elements Tinted (SPF 44); La Roche-Posay Anthelios Ultra-Light Tinted Mineral (SPF 50), SkinMedica Essential Defense Mineral Shield (SPF 32), ISDIN Eryfotona Ageless Ultralight Tinted Mineral Sunscreen (SPF 50), and SkinCeuticals Physical Fusion UV Defense (SPF 50).
Sunscreens with antioxidants
Sunscreens with biologically active antioxidants may be another option for patients with melasma. A proof-of-concept study that Dr. Lim and colleagues conducted in 20 patients found that application of a blend of topical antioxidants (2%) was associated with less erythema at the application sites among those with skin phototypes I-III and less pigmentation at the application sites among those with skin phototypes IV-VI after exposure to visible light and UVA-1, compared with controls.
Certain antioxidants have been added to sunscreens currently on the market, including niacinamide (vitamin B3), licochalcone A, carotenoids (beta-carotene), vitamin E, vitamin C, glycyrrhetinic acid, and diethylhexyl syringylidenemalonate.
A recently published paper on the role of antioxidants and free radical quenchers in protecting skin from visible light referred to unpublished data from Dr. Lim (the first author) and colleagues, which demonstrated a significant reduction in visual light–induced hyperpigmentation on skin with sunscreen that contained the antioxidants vitamin E, vitamin C, diethylhexyl syringylidenemalonate, licochalcone A, and a glycyrrhetinic acid, compared with sunscreen that had no antioxidants.
Novel filters
Another emerging option is sunscreen with new filters that cover UVA-1 and visible light. In a randomized, controlled trial of 19 patients, researchers evaluated the addition of methoxypropylamino cyclohexenylidene ethoxyethylcyanoacetate (MCE) absorber, a new UVA-1 filter known as Mexoryl 400, which has a peak absorption of 385 nm, to a sunscreen formulation.
“Currently, peak absorption in the U.S. is with avobenzone, which peaks at about 357 nm,” but MCE “covers a longer spectrum of UVA-1,” Dr. Lim said. The researchers found that the addition of MCE reduced UVA-1-induced dermal and epidermal alterations at cellular, biochemical, and molecular levels; and decreased UVA-1-induced pigmentation.
Another relatively new filter, phenylene bis-diphenyltriazine (also known as TriAsorB) not only protects against UVA but it extends into the blue light portion of visible light, according to a recently published paper. According to a press release from Pierre Fabre, which has developed the filter, studies have shown that TriAsorB is not toxic for three key species of marine biodiversity: a coral species, a phytoplankton species, and a zooplankton.
This filter and MCE are available in Europe but not in the United States.
Dr. Lim reported that he is an investigator for Incyte, L’Oréal, Pfizer, and the Patient-Centered Outcomes Research Institute.
BOSTON – Untinted chemical sunscreens on the market are not sufficient to protect the skin from the effects of visible light, complicating sun protection efforts for patients with melasma and other conditions aggravated by sun exposure, according to Henry W. Lim, MD.
A , Dr. Lim, former chair of the department of dermatology at Henry Ford Health, Detroit, said at the annual meeting of the American Academy of Dermatology. Tinted sunscreens contain iron oxides; some also contain pigmentary titanium dioxide.
“Black, red, and yellow iron oxide all reflect visible light,” he added, noting that currently, there are no regulations as to how tinted sunscreens are marketed, making it difficult for practicing clinicians to advise patients about what products to choose. However, he said, “unlike ‘SPF’ and ‘broad spectrum’ labeling, there is no specific guidance on tinted sunscreens. “ ‘Universal’ shade is a good start but might not be ideal for users with very fair or deep skin tones,” he noted.
In December 2021, a guide to tinted sunscreens, written by Dr. Lim and colleagues, was published, recommending that consumers choose a product that contains iron oxides, is labeled as broad spectrum, and has an SPF of at least 30.
A comprehensive list of 54 tinted sunscreens with an SPF of 30 or greater that contain iron oxide is also available . The authors of the guide contributed to this resource, which lists sunscreens by average price per ounce.
At the meeting, Dr. Lim highlighted tinted sunscreens that cost about $20 or less per ounce. They include Supergoop 100% Mineral CC Cream (SPF 50); Bare Republic Mineral Tinted Face Sunscreen Lotion (SPF 30); CeraVe Hydrating Sunscreen with Sheer Tint (SPF 30); Tizo Ultra Zinc Body & Face Sunscreen (SPF 40); Vichy Capital Soleil Tinted Face Mineral Sunscreen (SPF 60); EltaMD UV Elements Tinted (SPF 44); La Roche-Posay Anthelios Ultra-Light Tinted Mineral (SPF 50), SkinMedica Essential Defense Mineral Shield (SPF 32), ISDIN Eryfotona Ageless Ultralight Tinted Mineral Sunscreen (SPF 50), and SkinCeuticals Physical Fusion UV Defense (SPF 50).
Sunscreens with antioxidants
Sunscreens with biologically active antioxidants may be another option for patients with melasma. A proof-of-concept study that Dr. Lim and colleagues conducted in 20 patients found that application of a blend of topical antioxidants (2%) was associated with less erythema at the application sites among those with skin phototypes I-III and less pigmentation at the application sites among those with skin phototypes IV-VI after exposure to visible light and UVA-1, compared with controls.
Certain antioxidants have been added to sunscreens currently on the market, including niacinamide (vitamin B3), licochalcone A, carotenoids (beta-carotene), vitamin E, vitamin C, glycyrrhetinic acid, and diethylhexyl syringylidenemalonate.
A recently published paper on the role of antioxidants and free radical quenchers in protecting skin from visible light referred to unpublished data from Dr. Lim (the first author) and colleagues, which demonstrated a significant reduction in visual light–induced hyperpigmentation on skin with sunscreen that contained the antioxidants vitamin E, vitamin C, diethylhexyl syringylidenemalonate, licochalcone A, and a glycyrrhetinic acid, compared with sunscreen that had no antioxidants.
Novel filters
Another emerging option is sunscreen with new filters that cover UVA-1 and visible light. In a randomized, controlled trial of 19 patients, researchers evaluated the addition of methoxypropylamino cyclohexenylidene ethoxyethylcyanoacetate (MCE) absorber, a new UVA-1 filter known as Mexoryl 400, which has a peak absorption of 385 nm, to a sunscreen formulation.
“Currently, peak absorption in the U.S. is with avobenzone, which peaks at about 357 nm,” but MCE “covers a longer spectrum of UVA-1,” Dr. Lim said. The researchers found that the addition of MCE reduced UVA-1-induced dermal and epidermal alterations at cellular, biochemical, and molecular levels; and decreased UVA-1-induced pigmentation.
Another relatively new filter, phenylene bis-diphenyltriazine (also known as TriAsorB) not only protects against UVA but it extends into the blue light portion of visible light, according to a recently published paper. According to a press release from Pierre Fabre, which has developed the filter, studies have shown that TriAsorB is not toxic for three key species of marine biodiversity: a coral species, a phytoplankton species, and a zooplankton.
This filter and MCE are available in Europe but not in the United States.
Dr. Lim reported that he is an investigator for Incyte, L’Oréal, Pfizer, and the Patient-Centered Outcomes Research Institute.
AT AAD 22
On the receiving end of care
It’s tough being on the receiving end of care. I’ve tried to avoid it as much as possible, being ever mindful of the law from Samuel Shem’s The House of God: “They can always hurt you more.”
Fortunately, each procedure went more smoothly than the prior one.
The first was not so elective. I had some uncomfortable symptoms while exercising and, not wanting to totally be in denial, contacted my doctor to ensure that it was not cardiac in origin since symptoms are often atypical in women.
My physician promptly saw me, then scheduled a nuclear stress test. There was a series of needless glitches. Registration at the diagnostic center had me on their schedule but did not have an order. They would have canceled the procedure had I not been able to get hold of the doctor’s office. Why isn’t an order automatically entered when the physician schedules the test?
While I was given the euphemistic “Patient Rights” brochure, asking to have reports sent to a physician outside of the University of Pittsburgh Medical Center empire is apparently not included.
The staff canceled the stress test because I was not fasting. I had received no instructions from diagnostic cardiology. They suggested it was my internist’s responsibility.
I deliberately ate (2 hours earlier) because my trainer always wants me to eat a light meal so I don’t get hypoglycemic during our workouts, and an exercise stress test, is, of course, a workout. The nurse practitioner said that they were concerned I would vomit. I offered to sign a waiver. She parried, saying they would not be able to get adequate images, so I was out of luck.
When I expressed concern about getting hypoglycemic and having difficulty with the test if fasting, the tech said I should bring a soda and snack. Who tells a “borderline” diabetic to bring a soda?
The tech also said she had called our home to give instructions but encountered a busy signal and had not had time to call back. I had not left the house during the prior week (or most of the past 2 years), so this was a pretty lame excuse.
I suggested to the administration that the hospital offer to email the patient instructions well ahead of time (and perhaps ask for confirmation of receipt). If calling, they should try more than once. They should also have patient instruction sheets at the physician’s office and perhaps have them on their website.
It turns out that the hospital mailed me instructions, not on the date it was ordered, but with the postmark being the day of the procedure itself. With Trump donor Louis DeJoy in charge of the U.S. Postal Service, mail across town now has to travel to Baltimore, 3 hours away, be sorted, and returned.
I did finally have the stress test, which was reassuringly normal. I was not surprised, given that the fury I felt on the first attempt had not precipitated symptoms. The hospital sent a patient ombudsman to meet me there to discuss my previous complaints. I have no idea if they implemented any of the changes I had suggested. In 2021, when I urgently had to take my husband to the ED, I couldn’t see the sign pointing toward the ED and had to ask for directions at the main entrance. They said they would fix that promptly but still have not improved the signage. How I miss the friendly community hospital we had before!
Next was trigger-finger surgery. I had developed that in 1978 from using crutches after a fall. I figured that the relative lull in COVID and my activities made it as good a time as any to finally have it fixed. The surgicenter was great; the surgeon was someone I had worked with and respected for decades. The only glitch was not really knowing how long I was going to be out of commission.
The third encounter (at yet another institution) went really well, despite some early administrative glitches. My major complaint was with the lack of communication between preoperative anesthesia and the operating room and the lack of personalization of preoperative instructions. Despite EPIC, medicines were not correctly reconciled between the different encounters, even on the same day!
After about 15 years of diplopia, which has been gradually worsening, my eye doc had suggested that I consider strabismus surgery as a sort of last-ditch effort to improve my quality of life.
Anesthesiology has stock instructions, which they made no effort to individualize. For example, there is no reason to stop NSAIDs a week before such minor surgery. That’s a problem if you depend on NSAIDs for pain control. Similarly, nothing by mouth after midnight is passé and could be tailored for the patient. I felt particularly inconvenienced that I had to go out of town for the preoperative visit and then have a redundant preoperative clearance by my physician.
The nurses in the preoperative area made me feel quite comfortable and as relaxed as I could be under the circumstances. They had a good sense of humor, which helped too. And from the time I met him a few weeks earlier, I instantly liked my surgeon and felt very comfortable with him and had complete trust.
I was pleased that the chief anesthesiologist responded promptly and undefensively to my letter expressing concerns. I do believe that he will try to improve the systemic problems.
The best part: The surgery appears to have been successful and I should have a significantly improved quality of life.
Hospitals could do so much better by improving communications with patients and by viewing them as customers whose loyalty they must earn and will value. With monopolies growing, memories of such care are quickly fading, soon to be as extinct as the family doc who made house calls.
Dr. Stone is an infectious disease specialist and author of Resilience: One Family’s Story of Hope and Triumph over Evil and Conducting Clinical Research: A Practical Guide. She disclosed no relevant financial relationships. A version of this article first appeared on Medscape.com.
It’s tough being on the receiving end of care. I’ve tried to avoid it as much as possible, being ever mindful of the law from Samuel Shem’s The House of God: “They can always hurt you more.”
Fortunately, each procedure went more smoothly than the prior one.
The first was not so elective. I had some uncomfortable symptoms while exercising and, not wanting to totally be in denial, contacted my doctor to ensure that it was not cardiac in origin since symptoms are often atypical in women.
My physician promptly saw me, then scheduled a nuclear stress test. There was a series of needless glitches. Registration at the diagnostic center had me on their schedule but did not have an order. They would have canceled the procedure had I not been able to get hold of the doctor’s office. Why isn’t an order automatically entered when the physician schedules the test?
While I was given the euphemistic “Patient Rights” brochure, asking to have reports sent to a physician outside of the University of Pittsburgh Medical Center empire is apparently not included.
The staff canceled the stress test because I was not fasting. I had received no instructions from diagnostic cardiology. They suggested it was my internist’s responsibility.
I deliberately ate (2 hours earlier) because my trainer always wants me to eat a light meal so I don’t get hypoglycemic during our workouts, and an exercise stress test, is, of course, a workout. The nurse practitioner said that they were concerned I would vomit. I offered to sign a waiver. She parried, saying they would not be able to get adequate images, so I was out of luck.
When I expressed concern about getting hypoglycemic and having difficulty with the test if fasting, the tech said I should bring a soda and snack. Who tells a “borderline” diabetic to bring a soda?
The tech also said she had called our home to give instructions but encountered a busy signal and had not had time to call back. I had not left the house during the prior week (or most of the past 2 years), so this was a pretty lame excuse.
I suggested to the administration that the hospital offer to email the patient instructions well ahead of time (and perhaps ask for confirmation of receipt). If calling, they should try more than once. They should also have patient instruction sheets at the physician’s office and perhaps have them on their website.
It turns out that the hospital mailed me instructions, not on the date it was ordered, but with the postmark being the day of the procedure itself. With Trump donor Louis DeJoy in charge of the U.S. Postal Service, mail across town now has to travel to Baltimore, 3 hours away, be sorted, and returned.
I did finally have the stress test, which was reassuringly normal. I was not surprised, given that the fury I felt on the first attempt had not precipitated symptoms. The hospital sent a patient ombudsman to meet me there to discuss my previous complaints. I have no idea if they implemented any of the changes I had suggested. In 2021, when I urgently had to take my husband to the ED, I couldn’t see the sign pointing toward the ED and had to ask for directions at the main entrance. They said they would fix that promptly but still have not improved the signage. How I miss the friendly community hospital we had before!
Next was trigger-finger surgery. I had developed that in 1978 from using crutches after a fall. I figured that the relative lull in COVID and my activities made it as good a time as any to finally have it fixed. The surgicenter was great; the surgeon was someone I had worked with and respected for decades. The only glitch was not really knowing how long I was going to be out of commission.
The third encounter (at yet another institution) went really well, despite some early administrative glitches. My major complaint was with the lack of communication between preoperative anesthesia and the operating room and the lack of personalization of preoperative instructions. Despite EPIC, medicines were not correctly reconciled between the different encounters, even on the same day!
After about 15 years of diplopia, which has been gradually worsening, my eye doc had suggested that I consider strabismus surgery as a sort of last-ditch effort to improve my quality of life.
Anesthesiology has stock instructions, which they made no effort to individualize. For example, there is no reason to stop NSAIDs a week before such minor surgery. That’s a problem if you depend on NSAIDs for pain control. Similarly, nothing by mouth after midnight is passé and could be tailored for the patient. I felt particularly inconvenienced that I had to go out of town for the preoperative visit and then have a redundant preoperative clearance by my physician.
The nurses in the preoperative area made me feel quite comfortable and as relaxed as I could be under the circumstances. They had a good sense of humor, which helped too. And from the time I met him a few weeks earlier, I instantly liked my surgeon and felt very comfortable with him and had complete trust.
I was pleased that the chief anesthesiologist responded promptly and undefensively to my letter expressing concerns. I do believe that he will try to improve the systemic problems.
The best part: The surgery appears to have been successful and I should have a significantly improved quality of life.
Hospitals could do so much better by improving communications with patients and by viewing them as customers whose loyalty they must earn and will value. With monopolies growing, memories of such care are quickly fading, soon to be as extinct as the family doc who made house calls.
Dr. Stone is an infectious disease specialist and author of Resilience: One Family’s Story of Hope and Triumph over Evil and Conducting Clinical Research: A Practical Guide. She disclosed no relevant financial relationships. A version of this article first appeared on Medscape.com.
It’s tough being on the receiving end of care. I’ve tried to avoid it as much as possible, being ever mindful of the law from Samuel Shem’s The House of God: “They can always hurt you more.”
Fortunately, each procedure went more smoothly than the prior one.
The first was not so elective. I had some uncomfortable symptoms while exercising and, not wanting to totally be in denial, contacted my doctor to ensure that it was not cardiac in origin since symptoms are often atypical in women.
My physician promptly saw me, then scheduled a nuclear stress test. There was a series of needless glitches. Registration at the diagnostic center had me on their schedule but did not have an order. They would have canceled the procedure had I not been able to get hold of the doctor’s office. Why isn’t an order automatically entered when the physician schedules the test?
While I was given the euphemistic “Patient Rights” brochure, asking to have reports sent to a physician outside of the University of Pittsburgh Medical Center empire is apparently not included.
The staff canceled the stress test because I was not fasting. I had received no instructions from diagnostic cardiology. They suggested it was my internist’s responsibility.
I deliberately ate (2 hours earlier) because my trainer always wants me to eat a light meal so I don’t get hypoglycemic during our workouts, and an exercise stress test, is, of course, a workout. The nurse practitioner said that they were concerned I would vomit. I offered to sign a waiver. She parried, saying they would not be able to get adequate images, so I was out of luck.
When I expressed concern about getting hypoglycemic and having difficulty with the test if fasting, the tech said I should bring a soda and snack. Who tells a “borderline” diabetic to bring a soda?
The tech also said she had called our home to give instructions but encountered a busy signal and had not had time to call back. I had not left the house during the prior week (or most of the past 2 years), so this was a pretty lame excuse.
I suggested to the administration that the hospital offer to email the patient instructions well ahead of time (and perhaps ask for confirmation of receipt). If calling, they should try more than once. They should also have patient instruction sheets at the physician’s office and perhaps have them on their website.
It turns out that the hospital mailed me instructions, not on the date it was ordered, but with the postmark being the day of the procedure itself. With Trump donor Louis DeJoy in charge of the U.S. Postal Service, mail across town now has to travel to Baltimore, 3 hours away, be sorted, and returned.
I did finally have the stress test, which was reassuringly normal. I was not surprised, given that the fury I felt on the first attempt had not precipitated symptoms. The hospital sent a patient ombudsman to meet me there to discuss my previous complaints. I have no idea if they implemented any of the changes I had suggested. In 2021, when I urgently had to take my husband to the ED, I couldn’t see the sign pointing toward the ED and had to ask for directions at the main entrance. They said they would fix that promptly but still have not improved the signage. How I miss the friendly community hospital we had before!
Next was trigger-finger surgery. I had developed that in 1978 from using crutches after a fall. I figured that the relative lull in COVID and my activities made it as good a time as any to finally have it fixed. The surgicenter was great; the surgeon was someone I had worked with and respected for decades. The only glitch was not really knowing how long I was going to be out of commission.
The third encounter (at yet another institution) went really well, despite some early administrative glitches. My major complaint was with the lack of communication between preoperative anesthesia and the operating room and the lack of personalization of preoperative instructions. Despite EPIC, medicines were not correctly reconciled between the different encounters, even on the same day!
After about 15 years of diplopia, which has been gradually worsening, my eye doc had suggested that I consider strabismus surgery as a sort of last-ditch effort to improve my quality of life.
Anesthesiology has stock instructions, which they made no effort to individualize. For example, there is no reason to stop NSAIDs a week before such minor surgery. That’s a problem if you depend on NSAIDs for pain control. Similarly, nothing by mouth after midnight is passé and could be tailored for the patient. I felt particularly inconvenienced that I had to go out of town for the preoperative visit and then have a redundant preoperative clearance by my physician.
The nurses in the preoperative area made me feel quite comfortable and as relaxed as I could be under the circumstances. They had a good sense of humor, which helped too. And from the time I met him a few weeks earlier, I instantly liked my surgeon and felt very comfortable with him and had complete trust.
I was pleased that the chief anesthesiologist responded promptly and undefensively to my letter expressing concerns. I do believe that he will try to improve the systemic problems.
The best part: The surgery appears to have been successful and I should have a significantly improved quality of life.
Hospitals could do so much better by improving communications with patients and by viewing them as customers whose loyalty they must earn and will value. With monopolies growing, memories of such care are quickly fading, soon to be as extinct as the family doc who made house calls.
Dr. Stone is an infectious disease specialist and author of Resilience: One Family’s Story of Hope and Triumph over Evil and Conducting Clinical Research: A Practical Guide. She disclosed no relevant financial relationships. A version of this article first appeared on Medscape.com.
Global melanoma incidence high and on the rise
Even by cautious calculations,
An estimated 325,000 people worldwide received a new diagnosis of cutaneous melanoma in 2020, and if present trends continue, the incidence of new cases is predicted to increase by about 50% in 2040, with melanoma deaths expected to rise by almost 70%, Melina Arnold, PhD, from the Cancer Surveillance Branch of the International Agency for Research on Cancer in Lyon, France, and colleagues reported.
“Melanoma is the most lethal form of skin cancer; this epidemiological assessment found a heavy public health and economic burden, and our projections suggest that it will remain so in the coming decades,” they wrote in a study published online in JAMA Dermatology.
In an accompanying editorial, Mavis Obeng-Kusi, MPharm and Ivo Abraham, PhD from the Center for Health Outcomes and PharmacoEconomic Research at the University of Arizona, Tucson, commented that the findings are “sobering,” but may substantially underestimate the gravity of the problem in low- and middle-income countries (LMIC).
“The study by Arnold et al. brings to the fore a public health concern that requires global attention and initiates conversations particularly related to LMIC settings, where the incidence and mortality of melanoma is thought to be minimal and for which preventive measures may be insufficient,” they wrote.
Down Under nations lead
Dr. Arnold and colleagues looked at data on age-standardized melanoma incidence and mortality rates per 100,000 person-years (PY) by country, each of 20 world regions as defined by the United Nations, and according to the UN’s four-tier Human Development Index, which stratifies countries into low-, medium-, high-, and very high–income categories.
As noted previously, the researchers estimated that there were 325,000 new melanoma cases worldwide in 2020 (174,000 cases in males and 151,000 in females). There were 57,000 estimated melanoma deaths the same year (32,000 in males and 25,000 in females.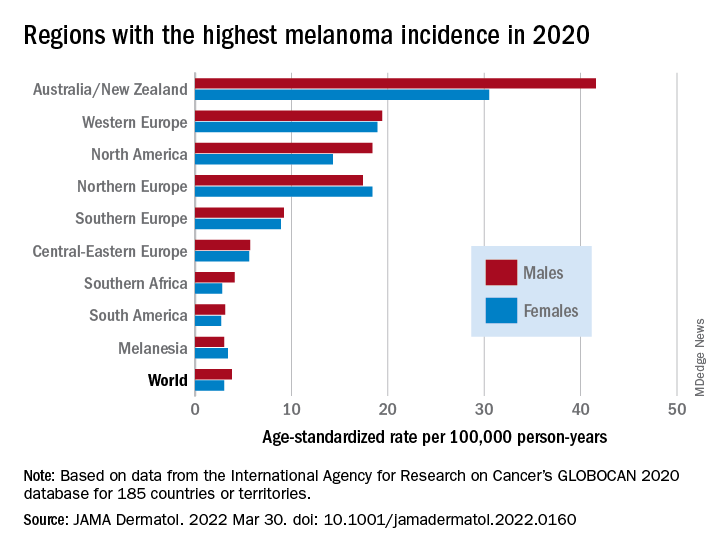
The highest incidence rates were seen in Australia and New Zealand, at 42 per 100,000 PY among males and 31 per 100,000 PY in females, followed by Western Europe with 19 per 100,000 PY in both males and females, North America with 18 and 14 cases per 100,000 PY in males and females respectively, and Northern Europe, with 17 per 100,000 PY in males, and 18 per 100,000 PY in females.
In contrast, in most African and Asian countries melanoma was rare, with rates commonly less than 1 per 100,000 PY, the investigators noted.
The melanoma mortality rate was highest in New Zealand, at 5 per 100,000 PY. Mortality rates worldwide varied less widely than incidence rates. In most other regions of the world, mortality rates were “much lower,” ranging between 0.2-1.0 per 100,000 PY, they wrote.
The authors estimated that, if 2020 rates remain stable, the global burden from melanoma in 2040 will increase to approximately 510,000 new cases and 96,000 deaths.
Public health efforts needed
In their editorial, Ms. Obeng-Kusi and Dr. Abraham pointed out that the study was hampered by the limited availability of cancer data from LMICs, leading the authors to estimate incidence and mortality rates based on proxy data, such as statistical modeling or averaged rates from neighboring countries.
They emphasized the need for going beyond the statistics: “Specific to cutaneous melanoma data, what is most important globally, knowing the exact numbers of cases and deaths or understanding the order of magnitude of the present and future epidemiology? No doubt the latter. Melanoma can be treated more easily if caught at earlier stages.”
Projections such as those provided by Dr. Arnold and colleagues could help to raise awareness of the importance of decreasing exposure to UV radiation, which accounts for three-fourths of all incident melanomas, the editorialists said.
The study was funded in part by a grant to coauthor Anna E. Cust, PhD, MPH. Dr. Cust reported receiving a fellowship from the Australian National Health and Medical Research Council outside the submitted work. Dr. Arnold had no conflicts of interested to disclose. Dr. Abraham reported financial relationships with various entities. Ms. Obeng-Kusi had no disclosures.
Even by cautious calculations,
An estimated 325,000 people worldwide received a new diagnosis of cutaneous melanoma in 2020, and if present trends continue, the incidence of new cases is predicted to increase by about 50% in 2040, with melanoma deaths expected to rise by almost 70%, Melina Arnold, PhD, from the Cancer Surveillance Branch of the International Agency for Research on Cancer in Lyon, France, and colleagues reported.
“Melanoma is the most lethal form of skin cancer; this epidemiological assessment found a heavy public health and economic burden, and our projections suggest that it will remain so in the coming decades,” they wrote in a study published online in JAMA Dermatology.
In an accompanying editorial, Mavis Obeng-Kusi, MPharm and Ivo Abraham, PhD from the Center for Health Outcomes and PharmacoEconomic Research at the University of Arizona, Tucson, commented that the findings are “sobering,” but may substantially underestimate the gravity of the problem in low- and middle-income countries (LMIC).
“The study by Arnold et al. brings to the fore a public health concern that requires global attention and initiates conversations particularly related to LMIC settings, where the incidence and mortality of melanoma is thought to be minimal and for which preventive measures may be insufficient,” they wrote.
Down Under nations lead
Dr. Arnold and colleagues looked at data on age-standardized melanoma incidence and mortality rates per 100,000 person-years (PY) by country, each of 20 world regions as defined by the United Nations, and according to the UN’s four-tier Human Development Index, which stratifies countries into low-, medium-, high-, and very high–income categories.
As noted previously, the researchers estimated that there were 325,000 new melanoma cases worldwide in 2020 (174,000 cases in males and 151,000 in females). There were 57,000 estimated melanoma deaths the same year (32,000 in males and 25,000 in females.
The highest incidence rates were seen in Australia and New Zealand, at 42 per 100,000 PY among males and 31 per 100,000 PY in females, followed by Western Europe with 19 per 100,000 PY in both males and females, North America with 18 and 14 cases per 100,000 PY in males and females respectively, and Northern Europe, with 17 per 100,000 PY in males, and 18 per 100,000 PY in females.
In contrast, in most African and Asian countries melanoma was rare, with rates commonly less than 1 per 100,000 PY, the investigators noted.
The melanoma mortality rate was highest in New Zealand, at 5 per 100,000 PY. Mortality rates worldwide varied less widely than incidence rates. In most other regions of the world, mortality rates were “much lower,” ranging between 0.2-1.0 per 100,000 PY, they wrote.
The authors estimated that, if 2020 rates remain stable, the global burden from melanoma in 2040 will increase to approximately 510,000 new cases and 96,000 deaths.
Public health efforts needed
In their editorial, Ms. Obeng-Kusi and Dr. Abraham pointed out that the study was hampered by the limited availability of cancer data from LMICs, leading the authors to estimate incidence and mortality rates based on proxy data, such as statistical modeling or averaged rates from neighboring countries.
They emphasized the need for going beyond the statistics: “Specific to cutaneous melanoma data, what is most important globally, knowing the exact numbers of cases and deaths or understanding the order of magnitude of the present and future epidemiology? No doubt the latter. Melanoma can be treated more easily if caught at earlier stages.”
Projections such as those provided by Dr. Arnold and colleagues could help to raise awareness of the importance of decreasing exposure to UV radiation, which accounts for three-fourths of all incident melanomas, the editorialists said.
The study was funded in part by a grant to coauthor Anna E. Cust, PhD, MPH. Dr. Cust reported receiving a fellowship from the Australian National Health and Medical Research Council outside the submitted work. Dr. Arnold had no conflicts of interested to disclose. Dr. Abraham reported financial relationships with various entities. Ms. Obeng-Kusi had no disclosures.
Even by cautious calculations,
An estimated 325,000 people worldwide received a new diagnosis of cutaneous melanoma in 2020, and if present trends continue, the incidence of new cases is predicted to increase by about 50% in 2040, with melanoma deaths expected to rise by almost 70%, Melina Arnold, PhD, from the Cancer Surveillance Branch of the International Agency for Research on Cancer in Lyon, France, and colleagues reported.
“Melanoma is the most lethal form of skin cancer; this epidemiological assessment found a heavy public health and economic burden, and our projections suggest that it will remain so in the coming decades,” they wrote in a study published online in JAMA Dermatology.
In an accompanying editorial, Mavis Obeng-Kusi, MPharm and Ivo Abraham, PhD from the Center for Health Outcomes and PharmacoEconomic Research at the University of Arizona, Tucson, commented that the findings are “sobering,” but may substantially underestimate the gravity of the problem in low- and middle-income countries (LMIC).
“The study by Arnold et al. brings to the fore a public health concern that requires global attention and initiates conversations particularly related to LMIC settings, where the incidence and mortality of melanoma is thought to be minimal and for which preventive measures may be insufficient,” they wrote.
Down Under nations lead
Dr. Arnold and colleagues looked at data on age-standardized melanoma incidence and mortality rates per 100,000 person-years (PY) by country, each of 20 world regions as defined by the United Nations, and according to the UN’s four-tier Human Development Index, which stratifies countries into low-, medium-, high-, and very high–income categories.
As noted previously, the researchers estimated that there were 325,000 new melanoma cases worldwide in 2020 (174,000 cases in males and 151,000 in females). There were 57,000 estimated melanoma deaths the same year (32,000 in males and 25,000 in females.
The highest incidence rates were seen in Australia and New Zealand, at 42 per 100,000 PY among males and 31 per 100,000 PY in females, followed by Western Europe with 19 per 100,000 PY in both males and females, North America with 18 and 14 cases per 100,000 PY in males and females respectively, and Northern Europe, with 17 per 100,000 PY in males, and 18 per 100,000 PY in females.
In contrast, in most African and Asian countries melanoma was rare, with rates commonly less than 1 per 100,000 PY, the investigators noted.
The melanoma mortality rate was highest in New Zealand, at 5 per 100,000 PY. Mortality rates worldwide varied less widely than incidence rates. In most other regions of the world, mortality rates were “much lower,” ranging between 0.2-1.0 per 100,000 PY, they wrote.
The authors estimated that, if 2020 rates remain stable, the global burden from melanoma in 2040 will increase to approximately 510,000 new cases and 96,000 deaths.
Public health efforts needed
In their editorial, Ms. Obeng-Kusi and Dr. Abraham pointed out that the study was hampered by the limited availability of cancer data from LMICs, leading the authors to estimate incidence and mortality rates based on proxy data, such as statistical modeling or averaged rates from neighboring countries.
They emphasized the need for going beyond the statistics: “Specific to cutaneous melanoma data, what is most important globally, knowing the exact numbers of cases and deaths or understanding the order of magnitude of the present and future epidemiology? No doubt the latter. Melanoma can be treated more easily if caught at earlier stages.”
Projections such as those provided by Dr. Arnold and colleagues could help to raise awareness of the importance of decreasing exposure to UV radiation, which accounts for three-fourths of all incident melanomas, the editorialists said.
The study was funded in part by a grant to coauthor Anna E. Cust, PhD, MPH. Dr. Cust reported receiving a fellowship from the Australian National Health and Medical Research Council outside the submitted work. Dr. Arnold had no conflicts of interested to disclose. Dr. Abraham reported financial relationships with various entities. Ms. Obeng-Kusi had no disclosures.
FROM JAMA DERMATOLOGY