User login
Is Red Meat Healthy? Multiverse Analysis Has Lessons Beyond Meat
Observational studies on red meat consumption and lifespan are prime examples of attempts to find signal in a sea of noise.
Randomized controlled trials are the best way to sort cause from mere correlation. But these are not possible in most matters of food consumption. So, we look back and observe groups with different exposures.
My most frequent complaint about these nonrandom comparison studies has been the chance that the two groups differ in important ways, and it’s these differences — not the food in question — that account for the disparate outcomes.
But selection biases are only one issue. There is also the matter of analytic flexibility. Observational studies are born from large databases. Researchers have many choices in how to analyze all these data.
A few years ago, Brian Nosek, PhD, and colleagues elegantly showed that analytic choices can affect results. His Many Analysts, One Data Set study had little uptake in the medical community, perhaps because he studied a social science question.
Multiple Ways to Slice the Data
Recently, a group from McMaster University, led by Dena Zeraatkar, PhD, has confirmed the analytic choices problem, using the question of red meat consumption and mortality.
Their idea was simple: Because there are many plausible and defensible ways to analyze a dataset, we should not choose one method; rather, we should choose thousands, combine the results, and see where the truth lies.
You might wonder how there could be thousands of ways to analyze a dataset. I surely did.
The answer stems from the choices that researchers face. For instance, there is the selection of eligible participants, the choice of analytic model (logistic, Poisson, etc.), and covariates for which to adjust. Think exponents when combining possible choices.
Dr. Zeraatkar and colleagues are research methodologists, so, sadly, they are comfortable with the clunky name of this approach: specification curve analysis. Don’t be deterred. It means that they analyze the data in thousands of ways using computers. Each way is a specification. In the end, the specifications give rise to a curve of hazard ratios for red meat and mortality. Another name for this approach is multiverse analysis.
For their paper in the Journal of Clinical Epidemiology, aptly named “Grilling the Data,” they didn’t just conjure up the many analytic ways to study the red meat–mortality question. Instead, they used a published systematic review of 15 studies on unprocessed red meat and early mortality. The studies included in this review reported 70 unique ways to analyze the association.
Is Red Meat Good or Bad?
Their first finding was that this analysis yielded widely disparate effect estimates, from 0.63 (reduced risk for early death) to 2.31 (a higher risk). The median hazard ratio was 1.14 with an interquartile range (IQR) of 1.02-1.23. One might conclude from this that eating red meat is associated with a slightly higher risk for early mortality.
Their second step was to calculate how many ways (specifications) there were to analyze the data by totaling all possible combinations of choices in the 70 ways found in the systematic review.
They calculated a total of 10 quadrillion possible unique analyses. A quadrillion is 1 with 15 zeros. Computing power cannot handle that amount of analyses yet. So, they generated 20 random unique combinations of covariates, which narrowed the number of analyses to about 1400. About 200 of these were excluded due to implausibly wide confidence intervals.
Voilà. They now had about 1200 different ways to analyze a dataset; they chose an NHANES longitudinal cohort study from 2007-2014. They deemed each of the more than 1200 approaches plausible because they were derived from peer-reviewed papers written by experts in epidemiology.
Specification Curve Analyses Results
Each analysis (or specification) yielded a hazard ratio for red meat exposure and death.
- The median HR was 0.94 (IQR, 0.83-1.05) for the effect of red meat on all-cause mortality — ie, not significant.
- The range of hazard ratios was large. They went from 0.51 — a 49% reduced risk for early mortality — to 1.75: a 75% increase in early mortality.
- Among all analyses, 36% yielded hazard ratios above 1.0 and 64% less than 1.0.
- As for statistical significance, defined as P ≤.05, only 4% (or 48 specifications) met this threshold. Zeraatkar reminded me that this is what you’d expect if unprocessed red meat has no effect on longevity.
- Of the 48 analyses deemed statistically significant, 40 indicated that red meat consumption reduced early death and eight indicated that eating red meat led to higher mortality.
- Nearly half the analyses yielded unexciting point estimates, with hazard ratios between 0.90 and 1.10.
Paradigm Changing
As a user of evidence, I find this a potentially paradigm-changing study. Observational studies far outnumber randomized trials. For many medical questions, observational data are all we have.
Now think about every observational study published. The authors tell you — post hoc — which method they used to analyze the data. The key point is that it is one method.
Dr. Zeraatkar and colleagues have shown that there are thousands of plausible ways to analyze the data, and this can lead to very different findings. In the specific question of red meat and mortality, their many analyses yielded a null result.
Now imagine other cases where the researchers did many analyses of a dataset and chose to publish only the significant ones. Observational studies are rarely preregistered, so a reader cannot know how a result would vary depending on analytic choices. A specification curve analysis of a dataset provides a much broader picture. In the case of red meat, you see some significant results, but the vast majority hover around null.
What about the difficulty in analyzing a dataset 1000 different ways? Dr. Zeraatkar told me that it is harder than just choosing one method, but it’s not impossible.
The main barrier to adopting this multiverse approach to data, she noted, was not the extra work but the entrenched belief among researchers that there is a best way to analyze data.
I hope you read this paper and think about it every time you read an observational study that finds a positive or negative association between two things. Ask: What if the researchers were as careful as Dr. Zeraatkar and colleagues and did multiple different analyses? Would the finding hold up to a series of plausible analytic choices?
Nutritional epidemiology would benefit greatly from this approach. But so would any observational study of an exposure and outcome. I suspect that the number of “positive” associations would diminish. And that would not be a bad thing.
Dr. Mandrola, a clinical electrophysiologist at Baptist Medical Associates, Louisville, Kentucky, disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Observational studies on red meat consumption and lifespan are prime examples of attempts to find signal in a sea of noise.
Randomized controlled trials are the best way to sort cause from mere correlation. But these are not possible in most matters of food consumption. So, we look back and observe groups with different exposures.
My most frequent complaint about these nonrandom comparison studies has been the chance that the two groups differ in important ways, and it’s these differences — not the food in question — that account for the disparate outcomes.
But selection biases are only one issue. There is also the matter of analytic flexibility. Observational studies are born from large databases. Researchers have many choices in how to analyze all these data.
A few years ago, Brian Nosek, PhD, and colleagues elegantly showed that analytic choices can affect results. His Many Analysts, One Data Set study had little uptake in the medical community, perhaps because he studied a social science question.
Multiple Ways to Slice the Data
Recently, a group from McMaster University, led by Dena Zeraatkar, PhD, has confirmed the analytic choices problem, using the question of red meat consumption and mortality.
Their idea was simple: Because there are many plausible and defensible ways to analyze a dataset, we should not choose one method; rather, we should choose thousands, combine the results, and see where the truth lies.
You might wonder how there could be thousands of ways to analyze a dataset. I surely did.
The answer stems from the choices that researchers face. For instance, there is the selection of eligible participants, the choice of analytic model (logistic, Poisson, etc.), and covariates for which to adjust. Think exponents when combining possible choices.
Dr. Zeraatkar and colleagues are research methodologists, so, sadly, they are comfortable with the clunky name of this approach: specification curve analysis. Don’t be deterred. It means that they analyze the data in thousands of ways using computers. Each way is a specification. In the end, the specifications give rise to a curve of hazard ratios for red meat and mortality. Another name for this approach is multiverse analysis.
For their paper in the Journal of Clinical Epidemiology, aptly named “Grilling the Data,” they didn’t just conjure up the many analytic ways to study the red meat–mortality question. Instead, they used a published systematic review of 15 studies on unprocessed red meat and early mortality. The studies included in this review reported 70 unique ways to analyze the association.
Is Red Meat Good or Bad?
Their first finding was that this analysis yielded widely disparate effect estimates, from 0.63 (reduced risk for early death) to 2.31 (a higher risk). The median hazard ratio was 1.14 with an interquartile range (IQR) of 1.02-1.23. One might conclude from this that eating red meat is associated with a slightly higher risk for early mortality.
Their second step was to calculate how many ways (specifications) there were to analyze the data by totaling all possible combinations of choices in the 70 ways found in the systematic review.
They calculated a total of 10 quadrillion possible unique analyses. A quadrillion is 1 with 15 zeros. Computing power cannot handle that amount of analyses yet. So, they generated 20 random unique combinations of covariates, which narrowed the number of analyses to about 1400. About 200 of these were excluded due to implausibly wide confidence intervals.
Voilà. They now had about 1200 different ways to analyze a dataset; they chose an NHANES longitudinal cohort study from 2007-2014. They deemed each of the more than 1200 approaches plausible because they were derived from peer-reviewed papers written by experts in epidemiology.
Specification Curve Analyses Results
Each analysis (or specification) yielded a hazard ratio for red meat exposure and death.
- The median HR was 0.94 (IQR, 0.83-1.05) for the effect of red meat on all-cause mortality — ie, not significant.
- The range of hazard ratios was large. They went from 0.51 — a 49% reduced risk for early mortality — to 1.75: a 75% increase in early mortality.
- Among all analyses, 36% yielded hazard ratios above 1.0 and 64% less than 1.0.
- As for statistical significance, defined as P ≤.05, only 4% (or 48 specifications) met this threshold. Zeraatkar reminded me that this is what you’d expect if unprocessed red meat has no effect on longevity.
- Of the 48 analyses deemed statistically significant, 40 indicated that red meat consumption reduced early death and eight indicated that eating red meat led to higher mortality.
- Nearly half the analyses yielded unexciting point estimates, with hazard ratios between 0.90 and 1.10.
Paradigm Changing
As a user of evidence, I find this a potentially paradigm-changing study. Observational studies far outnumber randomized trials. For many medical questions, observational data are all we have.
Now think about every observational study published. The authors tell you — post hoc — which method they used to analyze the data. The key point is that it is one method.
Dr. Zeraatkar and colleagues have shown that there are thousands of plausible ways to analyze the data, and this can lead to very different findings. In the specific question of red meat and mortality, their many analyses yielded a null result.
Now imagine other cases where the researchers did many analyses of a dataset and chose to publish only the significant ones. Observational studies are rarely preregistered, so a reader cannot know how a result would vary depending on analytic choices. A specification curve analysis of a dataset provides a much broader picture. In the case of red meat, you see some significant results, but the vast majority hover around null.
What about the difficulty in analyzing a dataset 1000 different ways? Dr. Zeraatkar told me that it is harder than just choosing one method, but it’s not impossible.
The main barrier to adopting this multiverse approach to data, she noted, was not the extra work but the entrenched belief among researchers that there is a best way to analyze data.
I hope you read this paper and think about it every time you read an observational study that finds a positive or negative association between two things. Ask: What if the researchers were as careful as Dr. Zeraatkar and colleagues and did multiple different analyses? Would the finding hold up to a series of plausible analytic choices?
Nutritional epidemiology would benefit greatly from this approach. But so would any observational study of an exposure and outcome. I suspect that the number of “positive” associations would diminish. And that would not be a bad thing.
Dr. Mandrola, a clinical electrophysiologist at Baptist Medical Associates, Louisville, Kentucky, disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Observational studies on red meat consumption and lifespan are prime examples of attempts to find signal in a sea of noise.
Randomized controlled trials are the best way to sort cause from mere correlation. But these are not possible in most matters of food consumption. So, we look back and observe groups with different exposures.
My most frequent complaint about these nonrandom comparison studies has been the chance that the two groups differ in important ways, and it’s these differences — not the food in question — that account for the disparate outcomes.
But selection biases are only one issue. There is also the matter of analytic flexibility. Observational studies are born from large databases. Researchers have many choices in how to analyze all these data.
A few years ago, Brian Nosek, PhD, and colleagues elegantly showed that analytic choices can affect results. His Many Analysts, One Data Set study had little uptake in the medical community, perhaps because he studied a social science question.
Multiple Ways to Slice the Data
Recently, a group from McMaster University, led by Dena Zeraatkar, PhD, has confirmed the analytic choices problem, using the question of red meat consumption and mortality.
Their idea was simple: Because there are many plausible and defensible ways to analyze a dataset, we should not choose one method; rather, we should choose thousands, combine the results, and see where the truth lies.
You might wonder how there could be thousands of ways to analyze a dataset. I surely did.
The answer stems from the choices that researchers face. For instance, there is the selection of eligible participants, the choice of analytic model (logistic, Poisson, etc.), and covariates for which to adjust. Think exponents when combining possible choices.
Dr. Zeraatkar and colleagues are research methodologists, so, sadly, they are comfortable with the clunky name of this approach: specification curve analysis. Don’t be deterred. It means that they analyze the data in thousands of ways using computers. Each way is a specification. In the end, the specifications give rise to a curve of hazard ratios for red meat and mortality. Another name for this approach is multiverse analysis.
For their paper in the Journal of Clinical Epidemiology, aptly named “Grilling the Data,” they didn’t just conjure up the many analytic ways to study the red meat–mortality question. Instead, they used a published systematic review of 15 studies on unprocessed red meat and early mortality. The studies included in this review reported 70 unique ways to analyze the association.
Is Red Meat Good or Bad?
Their first finding was that this analysis yielded widely disparate effect estimates, from 0.63 (reduced risk for early death) to 2.31 (a higher risk). The median hazard ratio was 1.14 with an interquartile range (IQR) of 1.02-1.23. One might conclude from this that eating red meat is associated with a slightly higher risk for early mortality.
Their second step was to calculate how many ways (specifications) there were to analyze the data by totaling all possible combinations of choices in the 70 ways found in the systematic review.
They calculated a total of 10 quadrillion possible unique analyses. A quadrillion is 1 with 15 zeros. Computing power cannot handle that amount of analyses yet. So, they generated 20 random unique combinations of covariates, which narrowed the number of analyses to about 1400. About 200 of these were excluded due to implausibly wide confidence intervals.
Voilà. They now had about 1200 different ways to analyze a dataset; they chose an NHANES longitudinal cohort study from 2007-2014. They deemed each of the more than 1200 approaches plausible because they were derived from peer-reviewed papers written by experts in epidemiology.
Specification Curve Analyses Results
Each analysis (or specification) yielded a hazard ratio for red meat exposure and death.
- The median HR was 0.94 (IQR, 0.83-1.05) for the effect of red meat on all-cause mortality — ie, not significant.
- The range of hazard ratios was large. They went from 0.51 — a 49% reduced risk for early mortality — to 1.75: a 75% increase in early mortality.
- Among all analyses, 36% yielded hazard ratios above 1.0 and 64% less than 1.0.
- As for statistical significance, defined as P ≤.05, only 4% (or 48 specifications) met this threshold. Zeraatkar reminded me that this is what you’d expect if unprocessed red meat has no effect on longevity.
- Of the 48 analyses deemed statistically significant, 40 indicated that red meat consumption reduced early death and eight indicated that eating red meat led to higher mortality.
- Nearly half the analyses yielded unexciting point estimates, with hazard ratios between 0.90 and 1.10.
Paradigm Changing
As a user of evidence, I find this a potentially paradigm-changing study. Observational studies far outnumber randomized trials. For many medical questions, observational data are all we have.
Now think about every observational study published. The authors tell you — post hoc — which method they used to analyze the data. The key point is that it is one method.
Dr. Zeraatkar and colleagues have shown that there are thousands of plausible ways to analyze the data, and this can lead to very different findings. In the specific question of red meat and mortality, their many analyses yielded a null result.
Now imagine other cases where the researchers did many analyses of a dataset and chose to publish only the significant ones. Observational studies are rarely preregistered, so a reader cannot know how a result would vary depending on analytic choices. A specification curve analysis of a dataset provides a much broader picture. In the case of red meat, you see some significant results, but the vast majority hover around null.
What about the difficulty in analyzing a dataset 1000 different ways? Dr. Zeraatkar told me that it is harder than just choosing one method, but it’s not impossible.
The main barrier to adopting this multiverse approach to data, she noted, was not the extra work but the entrenched belief among researchers that there is a best way to analyze data.
I hope you read this paper and think about it every time you read an observational study that finds a positive or negative association between two things. Ask: What if the researchers were as careful as Dr. Zeraatkar and colleagues and did multiple different analyses? Would the finding hold up to a series of plausible analytic choices?
Nutritional epidemiology would benefit greatly from this approach. But so would any observational study of an exposure and outcome. I suspect that the number of “positive” associations would diminish. And that would not be a bad thing.
Dr. Mandrola, a clinical electrophysiologist at Baptist Medical Associates, Louisville, Kentucky, disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Video Games Marketing Food Impacts Teens’ Eating
, according to research presented on May 12, 2024, at the 31st European Congress on Obesity in Venice, Italy.
The presentation by Rebecca Evans, University of Liverpool, United Kingdom, included findings from three recently published studies and a submitted randomized controlled trial. At the time of the research, the top VGLSPs globally were Twitch (with 77% of the market share by hours watched), YouTube Gaming (15%), and Facebook Gaming Live (7%).
“Endorsement deals for prominent streamers on Twitch can be worth many millions of dollars, and younger people, who are attractive to advertisers, are moving away from television to these more interactive forms of entertainment,” Evans said. “These deals involve collaborating with brands and promoting their products, including foods that are high in fats, salt, and/or sugar.”
To delve more deeply into the extent and consequences of VGLSP advertising for HFSS, the researchers first analyzed 52 hour-long Twitch videos uploaded to gaming platforms by three popular influencers. They found that food cues appeared at an average rate of 2.6 per hour, and the average duration of each cue was 20 minutes.
Most cues (70.7%) were for branded HFSS (80.5%), led by energy drinks (62.4%). Most (97.7%) were not accompanied by an advertising disclosure. Most food cues were either product placement (44.0%) and looping banners (40.6%) or features such as tie-ins, logos, or offers. Notably, these forms of advertising are always visible on the video game screen, so viewers cannot skip over them or close them.
Next, the team did a systematic review and meta-analysis to assess the relationship between exposure to digital game-based or influencer food marketing with food-related outcomes. They found that young people were twice as likely to prefer foods displayed via digital game-based marketing, and that influencer and digital game-based marketing was associated with increased HFSS food consumption of about 37 additional calories in one sitting.
Researchers then surveyed 490 youngsters (mean age, 16.8 years; 70%, female) to explore associations between recall of food marketing of the top VGLSPs and food-related outcomes. Recall was associated with more positive attitudes towards HFSS foods and, in turn, the purchase and consumption of the marketed HFSS foods.
In addition, the researchers conducted a lab-based randomized controlled trial to explore associations between HFSS food marketing via a mock Twitch stream and subsequent snack intake. A total of 91 youngsters (average age, 18 years; 69% women) viewed the mock stream, which contained either an advertisement (an image overlaid on the video featuring a brand logo and product) for an HFSS food, or a non-branded food. They were then offered a snack. Acute exposure to HFSS food marketing was not associated with immediate consumption, but more habitual use of VGLSPs was associated with increased intake of the marketed snack.
The observational studies could not prove cause and effect, and may not be generalizable to all teens, the authors acknowledged. They also noted that some of the findings are based on self-report surveys, which can lead to recall bias and may have affected the results.
Nevertheless, Ms. Evans said, “The high level of exposure to digital marketing of unhealthy food could drive excess calorie consumption and weight gain, particularly in adolescents who are more susceptible to advertising. It is important that digital food marketing restrictions encompass innovative and emerging digital media such as VGLSPs.”
The research formed Ms. Evans’ PhD work, which is funded by the University of Liverpool. Evans and colleagues declared no conflicts of interest.
A version of this article appeared on Medscape.com .
, according to research presented on May 12, 2024, at the 31st European Congress on Obesity in Venice, Italy.
The presentation by Rebecca Evans, University of Liverpool, United Kingdom, included findings from three recently published studies and a submitted randomized controlled trial. At the time of the research, the top VGLSPs globally were Twitch (with 77% of the market share by hours watched), YouTube Gaming (15%), and Facebook Gaming Live (7%).
“Endorsement deals for prominent streamers on Twitch can be worth many millions of dollars, and younger people, who are attractive to advertisers, are moving away from television to these more interactive forms of entertainment,” Evans said. “These deals involve collaborating with brands and promoting their products, including foods that are high in fats, salt, and/or sugar.”
To delve more deeply into the extent and consequences of VGLSP advertising for HFSS, the researchers first analyzed 52 hour-long Twitch videos uploaded to gaming platforms by three popular influencers. They found that food cues appeared at an average rate of 2.6 per hour, and the average duration of each cue was 20 minutes.
Most cues (70.7%) were for branded HFSS (80.5%), led by energy drinks (62.4%). Most (97.7%) were not accompanied by an advertising disclosure. Most food cues were either product placement (44.0%) and looping banners (40.6%) or features such as tie-ins, logos, or offers. Notably, these forms of advertising are always visible on the video game screen, so viewers cannot skip over them or close them.
Next, the team did a systematic review and meta-analysis to assess the relationship between exposure to digital game-based or influencer food marketing with food-related outcomes. They found that young people were twice as likely to prefer foods displayed via digital game-based marketing, and that influencer and digital game-based marketing was associated with increased HFSS food consumption of about 37 additional calories in one sitting.
Researchers then surveyed 490 youngsters (mean age, 16.8 years; 70%, female) to explore associations between recall of food marketing of the top VGLSPs and food-related outcomes. Recall was associated with more positive attitudes towards HFSS foods and, in turn, the purchase and consumption of the marketed HFSS foods.
In addition, the researchers conducted a lab-based randomized controlled trial to explore associations between HFSS food marketing via a mock Twitch stream and subsequent snack intake. A total of 91 youngsters (average age, 18 years; 69% women) viewed the mock stream, which contained either an advertisement (an image overlaid on the video featuring a brand logo and product) for an HFSS food, or a non-branded food. They were then offered a snack. Acute exposure to HFSS food marketing was not associated with immediate consumption, but more habitual use of VGLSPs was associated with increased intake of the marketed snack.
The observational studies could not prove cause and effect, and may not be generalizable to all teens, the authors acknowledged. They also noted that some of the findings are based on self-report surveys, which can lead to recall bias and may have affected the results.
Nevertheless, Ms. Evans said, “The high level of exposure to digital marketing of unhealthy food could drive excess calorie consumption and weight gain, particularly in adolescents who are more susceptible to advertising. It is important that digital food marketing restrictions encompass innovative and emerging digital media such as VGLSPs.”
The research formed Ms. Evans’ PhD work, which is funded by the University of Liverpool. Evans and colleagues declared no conflicts of interest.
A version of this article appeared on Medscape.com .
, according to research presented on May 12, 2024, at the 31st European Congress on Obesity in Venice, Italy.
The presentation by Rebecca Evans, University of Liverpool, United Kingdom, included findings from three recently published studies and a submitted randomized controlled trial. At the time of the research, the top VGLSPs globally were Twitch (with 77% of the market share by hours watched), YouTube Gaming (15%), and Facebook Gaming Live (7%).
“Endorsement deals for prominent streamers on Twitch can be worth many millions of dollars, and younger people, who are attractive to advertisers, are moving away from television to these more interactive forms of entertainment,” Evans said. “These deals involve collaborating with brands and promoting their products, including foods that are high in fats, salt, and/or sugar.”
To delve more deeply into the extent and consequences of VGLSP advertising for HFSS, the researchers first analyzed 52 hour-long Twitch videos uploaded to gaming platforms by three popular influencers. They found that food cues appeared at an average rate of 2.6 per hour, and the average duration of each cue was 20 minutes.
Most cues (70.7%) were for branded HFSS (80.5%), led by energy drinks (62.4%). Most (97.7%) were not accompanied by an advertising disclosure. Most food cues were either product placement (44.0%) and looping banners (40.6%) or features such as tie-ins, logos, or offers. Notably, these forms of advertising are always visible on the video game screen, so viewers cannot skip over them or close them.
Next, the team did a systematic review and meta-analysis to assess the relationship between exposure to digital game-based or influencer food marketing with food-related outcomes. They found that young people were twice as likely to prefer foods displayed via digital game-based marketing, and that influencer and digital game-based marketing was associated with increased HFSS food consumption of about 37 additional calories in one sitting.
Researchers then surveyed 490 youngsters (mean age, 16.8 years; 70%, female) to explore associations between recall of food marketing of the top VGLSPs and food-related outcomes. Recall was associated with more positive attitudes towards HFSS foods and, in turn, the purchase and consumption of the marketed HFSS foods.
In addition, the researchers conducted a lab-based randomized controlled trial to explore associations between HFSS food marketing via a mock Twitch stream and subsequent snack intake. A total of 91 youngsters (average age, 18 years; 69% women) viewed the mock stream, which contained either an advertisement (an image overlaid on the video featuring a brand logo and product) for an HFSS food, or a non-branded food. They were then offered a snack. Acute exposure to HFSS food marketing was not associated with immediate consumption, but more habitual use of VGLSPs was associated with increased intake of the marketed snack.
The observational studies could not prove cause and effect, and may not be generalizable to all teens, the authors acknowledged. They also noted that some of the findings are based on self-report surveys, which can lead to recall bias and may have affected the results.
Nevertheless, Ms. Evans said, “The high level of exposure to digital marketing of unhealthy food could drive excess calorie consumption and weight gain, particularly in adolescents who are more susceptible to advertising. It is important that digital food marketing restrictions encompass innovative and emerging digital media such as VGLSPs.”
The research formed Ms. Evans’ PhD work, which is funded by the University of Liverpool. Evans and colleagues declared no conflicts of interest.
A version of this article appeared on Medscape.com .
New and Emerging Treatments for Major Depressive Disorder
Outside of treating major depressive disorder (MDD) through the monoamine system with selective serotonin reuptake inhibitors and serotonin-norepinephrine reuptake inhibitors, exploration of other treatment pathways has opened the possibility of faster onset of action and fewer side effects.
In this ReCAP, Dr Joseph Goldberg, from Mount Sinai Hospital in New York, NY, outlines how a better understanding of the glutamate system has led to the emergence of ketamine and esketamine as important treatment options, as well as the combination therapy of dextromethorphan with bupropion.
Dr Goldberg also discusses new results from serotonin system modulation through the 5HT1A receptor with gepirone, or the 5HT2A receptor with psilocybin. He also reports on a new compound esmethadone, known as REL-1017. Finally, he discusses the first approval of a digital therapeutic app designed to augment pharmacotherapy, and the dopamine partial agonist cariprazine as an adjunctive therapy.
--
Joseph F. Goldberg, MD, Clinical Professor, Department of Psychiatry, Icahn School of Medicine at Mount Sinai; Teaching Attending, Department of Psychiatry, Mount Sinai Hospital, New York, NY
Joseph F. Goldberg, MD, has disclosed the following relevant financial relationships:
Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for: AbbVie; Genomind; Luye Pharma; Neuroma; Neurelis; Otsuka; Sunovion
Serve(d) as a speaker or a member of a speakers bureau for: AbbVie; Alkermes; Axsome; Intracellular Therapies
Receive(d) royalties from: American Psychiatric Publishing; Cambridge University Press
Outside of treating major depressive disorder (MDD) through the monoamine system with selective serotonin reuptake inhibitors and serotonin-norepinephrine reuptake inhibitors, exploration of other treatment pathways has opened the possibility of faster onset of action and fewer side effects.
In this ReCAP, Dr Joseph Goldberg, from Mount Sinai Hospital in New York, NY, outlines how a better understanding of the glutamate system has led to the emergence of ketamine and esketamine as important treatment options, as well as the combination therapy of dextromethorphan with bupropion.
Dr Goldberg also discusses new results from serotonin system modulation through the 5HT1A receptor with gepirone, or the 5HT2A receptor with psilocybin. He also reports on a new compound esmethadone, known as REL-1017. Finally, he discusses the first approval of a digital therapeutic app designed to augment pharmacotherapy, and the dopamine partial agonist cariprazine as an adjunctive therapy.
--
Joseph F. Goldberg, MD, Clinical Professor, Department of Psychiatry, Icahn School of Medicine at Mount Sinai; Teaching Attending, Department of Psychiatry, Mount Sinai Hospital, New York, NY
Joseph F. Goldberg, MD, has disclosed the following relevant financial relationships:
Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for: AbbVie; Genomind; Luye Pharma; Neuroma; Neurelis; Otsuka; Sunovion
Serve(d) as a speaker or a member of a speakers bureau for: AbbVie; Alkermes; Axsome; Intracellular Therapies
Receive(d) royalties from: American Psychiatric Publishing; Cambridge University Press
Outside of treating major depressive disorder (MDD) through the monoamine system with selective serotonin reuptake inhibitors and serotonin-norepinephrine reuptake inhibitors, exploration of other treatment pathways has opened the possibility of faster onset of action and fewer side effects.
In this ReCAP, Dr Joseph Goldberg, from Mount Sinai Hospital in New York, NY, outlines how a better understanding of the glutamate system has led to the emergence of ketamine and esketamine as important treatment options, as well as the combination therapy of dextromethorphan with bupropion.
Dr Goldberg also discusses new results from serotonin system modulation through the 5HT1A receptor with gepirone, or the 5HT2A receptor with psilocybin. He also reports on a new compound esmethadone, known as REL-1017. Finally, he discusses the first approval of a digital therapeutic app designed to augment pharmacotherapy, and the dopamine partial agonist cariprazine as an adjunctive therapy.
--
Joseph F. Goldberg, MD, Clinical Professor, Department of Psychiatry, Icahn School of Medicine at Mount Sinai; Teaching Attending, Department of Psychiatry, Mount Sinai Hospital, New York, NY
Joseph F. Goldberg, MD, has disclosed the following relevant financial relationships:
Serve(d) as a director, officer, partner, employee, advisor, consultant, or trustee for: AbbVie; Genomind; Luye Pharma; Neuroma; Neurelis; Otsuka; Sunovion
Serve(d) as a speaker or a member of a speakers bureau for: AbbVie; Alkermes; Axsome; Intracellular Therapies
Receive(d) royalties from: American Psychiatric Publishing; Cambridge University Press

Darker Skin Tones Underrepresented on Skin Cancer Education Websites
“Given the known disparities patients with darker skin tones face in terms of increased skin cancer morbidity and mortality, this lack of representation further disadvantages those patients by not providing them with an adequate representation of how skin cancers manifest on their skin tones,” the study’s first author, Alana Sadur, who recently completed her third year at the George Washington School of Medicine and Health Sciences, Washington, said in an interview. “By not having images to refer to, patients are less likely to self-identify and seek treatment for concerning skin lesions.”
For the study, which was published in Journal of Drugs in Dermatology, Ms. Sadur and coauthors evaluated the inclusivity and representation of skin tones in photos of skin cancer on the following patient-facing websites: CDC.gov, NIH.gov, skincancer.org, americancancerfund.org, mayoclinic.org, and cancer.org. The researchers counted each individual person or image showing skin as a separate representation, and three independent reviewers used the 5-color Pantone swatch as described in a dermatology atlas to categorize representations as “lighter-toned skin” (Pantones A-B or lighter) or “darker-toned skin” (Pantones C-E or darker).
Of the 372 total representations identified on the websites, only 49 (13.2%) showed darker skin tones. Of these, 44.9% depicted Pantone C, 34.7% depicted Pantone D, and 20.4% depicted Pantone E. The researchers also found that only 11% of nonmelanoma skin cancers (NMSC) and 5.8% of melanoma skin cancers (MSC) were shown on darker skin tones, while no cartoon portrayals of NMSC or MSC included darker skin tones.
In findings related to nondisease representations on the websites, darker skin tones were depicted in just 22.7% of stock photos and 26.1% of website front pages.
The study’s senior author, Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington, emphasized the need for trusted sources like national organizations and federally funded agencies to be purposeful with their selection of images to “ensure all visitors to the site are represented,” he told this news organization.
“This is very important when dealing with skin cancer as a lack of representation could easily be misinterpreted as epidemiological data, meaning this gap could suggest certain individuals do not get skin cancer because photos in those skin tones are not present,” he added. “This doesn’t even begin to touch upon the diversity of individuals in the stock photos or lack thereof, which can perpetuate the lack of diversity in our specialty. We need to do better.”
The authors reported having no relevant disclosures.
A version of this article first appeared on Medscape.com.
“Given the known disparities patients with darker skin tones face in terms of increased skin cancer morbidity and mortality, this lack of representation further disadvantages those patients by not providing them with an adequate representation of how skin cancers manifest on their skin tones,” the study’s first author, Alana Sadur, who recently completed her third year at the George Washington School of Medicine and Health Sciences, Washington, said in an interview. “By not having images to refer to, patients are less likely to self-identify and seek treatment for concerning skin lesions.”
For the study, which was published in Journal of Drugs in Dermatology, Ms. Sadur and coauthors evaluated the inclusivity and representation of skin tones in photos of skin cancer on the following patient-facing websites: CDC.gov, NIH.gov, skincancer.org, americancancerfund.org, mayoclinic.org, and cancer.org. The researchers counted each individual person or image showing skin as a separate representation, and three independent reviewers used the 5-color Pantone swatch as described in a dermatology atlas to categorize representations as “lighter-toned skin” (Pantones A-B or lighter) or “darker-toned skin” (Pantones C-E or darker).
Of the 372 total representations identified on the websites, only 49 (13.2%) showed darker skin tones. Of these, 44.9% depicted Pantone C, 34.7% depicted Pantone D, and 20.4% depicted Pantone E. The researchers also found that only 11% of nonmelanoma skin cancers (NMSC) and 5.8% of melanoma skin cancers (MSC) were shown on darker skin tones, while no cartoon portrayals of NMSC or MSC included darker skin tones.
In findings related to nondisease representations on the websites, darker skin tones were depicted in just 22.7% of stock photos and 26.1% of website front pages.
The study’s senior author, Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington, emphasized the need for trusted sources like national organizations and federally funded agencies to be purposeful with their selection of images to “ensure all visitors to the site are represented,” he told this news organization.
“This is very important when dealing with skin cancer as a lack of representation could easily be misinterpreted as epidemiological data, meaning this gap could suggest certain individuals do not get skin cancer because photos in those skin tones are not present,” he added. “This doesn’t even begin to touch upon the diversity of individuals in the stock photos or lack thereof, which can perpetuate the lack of diversity in our specialty. We need to do better.”
The authors reported having no relevant disclosures.
A version of this article first appeared on Medscape.com.
“Given the known disparities patients with darker skin tones face in terms of increased skin cancer morbidity and mortality, this lack of representation further disadvantages those patients by not providing them with an adequate representation of how skin cancers manifest on their skin tones,” the study’s first author, Alana Sadur, who recently completed her third year at the George Washington School of Medicine and Health Sciences, Washington, said in an interview. “By not having images to refer to, patients are less likely to self-identify and seek treatment for concerning skin lesions.”
For the study, which was published in Journal of Drugs in Dermatology, Ms. Sadur and coauthors evaluated the inclusivity and representation of skin tones in photos of skin cancer on the following patient-facing websites: CDC.gov, NIH.gov, skincancer.org, americancancerfund.org, mayoclinic.org, and cancer.org. The researchers counted each individual person or image showing skin as a separate representation, and three independent reviewers used the 5-color Pantone swatch as described in a dermatology atlas to categorize representations as “lighter-toned skin” (Pantones A-B or lighter) or “darker-toned skin” (Pantones C-E or darker).
Of the 372 total representations identified on the websites, only 49 (13.2%) showed darker skin tones. Of these, 44.9% depicted Pantone C, 34.7% depicted Pantone D, and 20.4% depicted Pantone E. The researchers also found that only 11% of nonmelanoma skin cancers (NMSC) and 5.8% of melanoma skin cancers (MSC) were shown on darker skin tones, while no cartoon portrayals of NMSC or MSC included darker skin tones.
In findings related to nondisease representations on the websites, darker skin tones were depicted in just 22.7% of stock photos and 26.1% of website front pages.
The study’s senior author, Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington, emphasized the need for trusted sources like national organizations and federally funded agencies to be purposeful with their selection of images to “ensure all visitors to the site are represented,” he told this news organization.
“This is very important when dealing with skin cancer as a lack of representation could easily be misinterpreted as epidemiological data, meaning this gap could suggest certain individuals do not get skin cancer because photos in those skin tones are not present,” he added. “This doesn’t even begin to touch upon the diversity of individuals in the stock photos or lack thereof, which can perpetuate the lack of diversity in our specialty. We need to do better.”
The authors reported having no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM JOURNAL OF DRUGS IN DERMATOLOGY
Throbbing headache and nausea
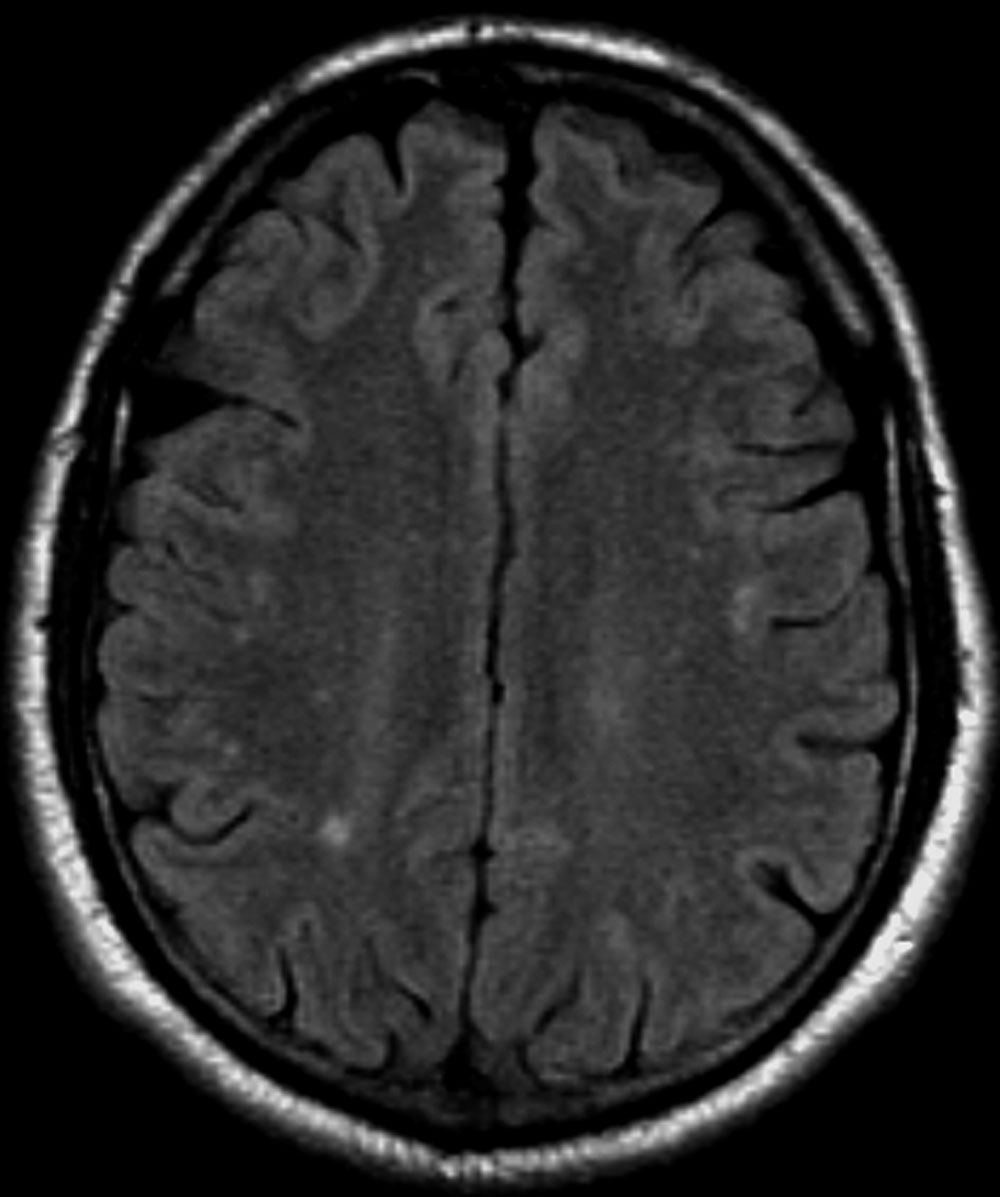
Migraine is a form of recurrent headache that can present as migraine with aura or migraine without aura, with the latter being the most common form. As in this patient, migraine without aura is a chronic form of headache of moderate to severe intensity that usually lasts for several hours but rarely may persist for up to 3 days. Headache pain is unilateral and often aggravated by triggers such as routine physical activity. The American Headache Society diagnostic criteria for migraine without aura include having symptoms of nausea and/or hypersensitivity to light or sound. This patient also described symptoms typical of the prodromal phase of migraine, which include yawning, temperature control, excessive thirst, and mood swings.
Patients who have migraine with aura also have unilateral headache pain of several hours' duration but experience visual (eg, dots or flashes) or sensory (prickly sensation on skin) symptoms, or may have brief difficulty with speech or motor function. These aura symptoms generally last 5 to 60 minutes before abating.
The worldwide impact of migraine potentially reaches a billion individuals. Its prevalence is second only to tension-type headaches. Migraine occurs in patients of all ages and affects women at a rate two to three times higher than in men. Prevalence appears to peak in the third and fourth decades of life and tends to be lower among older adults. Migraine also has a negative effect on patients' work, school, or social lives, and is associated with increased rates of depression and anxiety in adults. For patients who are prone to migraines, potential triggers include some foods and beverages (including those that contain caffeine and alcohol), menstrual cycles in women, exposure to strobing or bright lights or loud sounds, stressful situations, extra physical activity, and too much or too little sleep.
Migraine is a clinical diagnosis based on number of headaches (five or more episodes) plus two or more of the characteristic signs (unilateral, throbbing pain, pain intensity of ≥ 5 on a 10-point scale, and pain aggravated by routine physical motion, such as climbing stairs or bending over) plus nausea and/or photosensitivity or phonosensitivity. Prodrome symptoms are reported by about 70% of adult patients. Diagnosis rarely requires neuroimaging; however, before prescribing medication, a complete lab and metabolic workup should be done.
Management of migraine without aura includes acute and preventive interventions. Acute interventions cited by the American Headache Society include nonsteroidal anti-inflammatory drugs and acetaminophen for mild pain, and migraine-specific therapies such as the triptans, ergotamine derivatives, gepants (rimegepant, ubrogepant), and lasmiditan. Because response to any of these therapies will differ among patients with migraine, shared decision-making with patients about benefits and potential side effects is necessary and should include flexibility to change therapy if needed.
Preventive therapy should be offered to patients experiencing six or more migraines a month (regardless of impairment) and those, like this patient, with three or more migraines a month that significantly impair daily activities. Preventive therapy can be considered for those with fewer monthly episodes, depending on the degree of impairment. Oral preventive therapies with established efficacy include candesartan, certain beta-blockers, topiramate, and valproate. Parenteral monoclonal antibodies that inhibit calcitonin gene-related peptide activity (eptinezumab, erenumab, fremanezumab, and galcanezumab) and onabotulinumtoxinA may be considered if oral therapies provide inadequate prevention.
Tension-type headache is the most common form of primary headache. These headaches are bilateral and characterized by a pressing or dull sensation that is often mild in intensity. They are different from migraine in that they occur infrequently, lack sensory symptoms, and generally are of shorter duration (30 minutes to 24 hours). Fasting-related headache is characterized by diffuse, nonpulsating pain and is relieved with food.
Heidi Moawad, MD, Clinical Assistant Professor, Department of Medical Education, Case Western Reserve University School of Medicine, Cleveland, Ohio.
Heidi Moawad, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
Migraine is a form of recurrent headache that can present as migraine with aura or migraine without aura, with the latter being the most common form. As in this patient, migraine without aura is a chronic form of headache of moderate to severe intensity that usually lasts for several hours but rarely may persist for up to 3 days. Headache pain is unilateral and often aggravated by triggers such as routine physical activity. The American Headache Society diagnostic criteria for migraine without aura include having symptoms of nausea and/or hypersensitivity to light or sound. This patient also described symptoms typical of the prodromal phase of migraine, which include yawning, temperature control, excessive thirst, and mood swings.
Patients who have migraine with aura also have unilateral headache pain of several hours' duration but experience visual (eg, dots or flashes) or sensory (prickly sensation on skin) symptoms, or may have brief difficulty with speech or motor function. These aura symptoms generally last 5 to 60 minutes before abating.
The worldwide impact of migraine potentially reaches a billion individuals. Its prevalence is second only to tension-type headaches. Migraine occurs in patients of all ages and affects women at a rate two to three times higher than in men. Prevalence appears to peak in the third and fourth decades of life and tends to be lower among older adults. Migraine also has a negative effect on patients' work, school, or social lives, and is associated with increased rates of depression and anxiety in adults. For patients who are prone to migraines, potential triggers include some foods and beverages (including those that contain caffeine and alcohol), menstrual cycles in women, exposure to strobing or bright lights or loud sounds, stressful situations, extra physical activity, and too much or too little sleep.
Migraine is a clinical diagnosis based on number of headaches (five or more episodes) plus two or more of the characteristic signs (unilateral, throbbing pain, pain intensity of ≥ 5 on a 10-point scale, and pain aggravated by routine physical motion, such as climbing stairs or bending over) plus nausea and/or photosensitivity or phonosensitivity. Prodrome symptoms are reported by about 70% of adult patients. Diagnosis rarely requires neuroimaging; however, before prescribing medication, a complete lab and metabolic workup should be done.
Management of migraine without aura includes acute and preventive interventions. Acute interventions cited by the American Headache Society include nonsteroidal anti-inflammatory drugs and acetaminophen for mild pain, and migraine-specific therapies such as the triptans, ergotamine derivatives, gepants (rimegepant, ubrogepant), and lasmiditan. Because response to any of these therapies will differ among patients with migraine, shared decision-making with patients about benefits and potential side effects is necessary and should include flexibility to change therapy if needed.
Preventive therapy should be offered to patients experiencing six or more migraines a month (regardless of impairment) and those, like this patient, with three or more migraines a month that significantly impair daily activities. Preventive therapy can be considered for those with fewer monthly episodes, depending on the degree of impairment. Oral preventive therapies with established efficacy include candesartan, certain beta-blockers, topiramate, and valproate. Parenteral monoclonal antibodies that inhibit calcitonin gene-related peptide activity (eptinezumab, erenumab, fremanezumab, and galcanezumab) and onabotulinumtoxinA may be considered if oral therapies provide inadequate prevention.
Tension-type headache is the most common form of primary headache. These headaches are bilateral and characterized by a pressing or dull sensation that is often mild in intensity. They are different from migraine in that they occur infrequently, lack sensory symptoms, and generally are of shorter duration (30 minutes to 24 hours). Fasting-related headache is characterized by diffuse, nonpulsating pain and is relieved with food.
Heidi Moawad, MD, Clinical Assistant Professor, Department of Medical Education, Case Western Reserve University School of Medicine, Cleveland, Ohio.
Heidi Moawad, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
Migraine is a form of recurrent headache that can present as migraine with aura or migraine without aura, with the latter being the most common form. As in this patient, migraine without aura is a chronic form of headache of moderate to severe intensity that usually lasts for several hours but rarely may persist for up to 3 days. Headache pain is unilateral and often aggravated by triggers such as routine physical activity. The American Headache Society diagnostic criteria for migraine without aura include having symptoms of nausea and/or hypersensitivity to light or sound. This patient also described symptoms typical of the prodromal phase of migraine, which include yawning, temperature control, excessive thirst, and mood swings.
Patients who have migraine with aura also have unilateral headache pain of several hours' duration but experience visual (eg, dots or flashes) or sensory (prickly sensation on skin) symptoms, or may have brief difficulty with speech or motor function. These aura symptoms generally last 5 to 60 minutes before abating.
The worldwide impact of migraine potentially reaches a billion individuals. Its prevalence is second only to tension-type headaches. Migraine occurs in patients of all ages and affects women at a rate two to three times higher than in men. Prevalence appears to peak in the third and fourth decades of life and tends to be lower among older adults. Migraine also has a negative effect on patients' work, school, or social lives, and is associated with increased rates of depression and anxiety in adults. For patients who are prone to migraines, potential triggers include some foods and beverages (including those that contain caffeine and alcohol), menstrual cycles in women, exposure to strobing or bright lights or loud sounds, stressful situations, extra physical activity, and too much or too little sleep.
Migraine is a clinical diagnosis based on number of headaches (five or more episodes) plus two or more of the characteristic signs (unilateral, throbbing pain, pain intensity of ≥ 5 on a 10-point scale, and pain aggravated by routine physical motion, such as climbing stairs or bending over) plus nausea and/or photosensitivity or phonosensitivity. Prodrome symptoms are reported by about 70% of adult patients. Diagnosis rarely requires neuroimaging; however, before prescribing medication, a complete lab and metabolic workup should be done.
Management of migraine without aura includes acute and preventive interventions. Acute interventions cited by the American Headache Society include nonsteroidal anti-inflammatory drugs and acetaminophen for mild pain, and migraine-specific therapies such as the triptans, ergotamine derivatives, gepants (rimegepant, ubrogepant), and lasmiditan. Because response to any of these therapies will differ among patients with migraine, shared decision-making with patients about benefits and potential side effects is necessary and should include flexibility to change therapy if needed.
Preventive therapy should be offered to patients experiencing six or more migraines a month (regardless of impairment) and those, like this patient, with three or more migraines a month that significantly impair daily activities. Preventive therapy can be considered for those with fewer monthly episodes, depending on the degree of impairment. Oral preventive therapies with established efficacy include candesartan, certain beta-blockers, topiramate, and valproate. Parenteral monoclonal antibodies that inhibit calcitonin gene-related peptide activity (eptinezumab, erenumab, fremanezumab, and galcanezumab) and onabotulinumtoxinA may be considered if oral therapies provide inadequate prevention.
Tension-type headache is the most common form of primary headache. These headaches are bilateral and characterized by a pressing or dull sensation that is often mild in intensity. They are different from migraine in that they occur infrequently, lack sensory symptoms, and generally are of shorter duration (30 minutes to 24 hours). Fasting-related headache is characterized by diffuse, nonpulsating pain and is relieved with food.
Heidi Moawad, MD, Clinical Assistant Professor, Department of Medical Education, Case Western Reserve University School of Medicine, Cleveland, Ohio.
Heidi Moawad, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
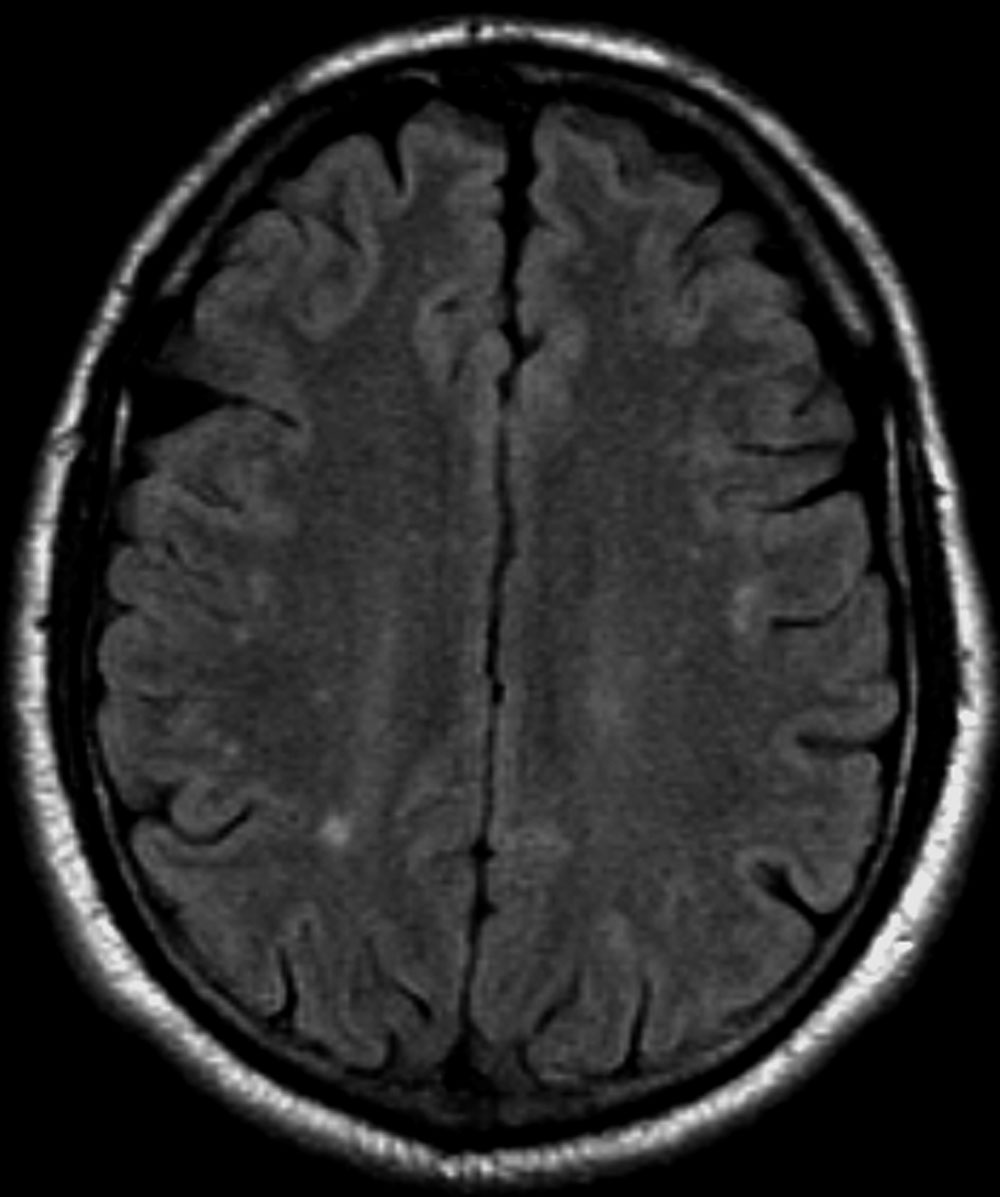
A 30-year-old female patient (140 lb and 5 ft 7 in; BMI 21.9) presents at the emergency department with a throbbing headache that began after dinner and was accompanied by queasy nausea. She reports immediately going to bed and sleeping through the night, but pain and other symptoms were still present in the morning. At this point, headache duration is approaching 15 hours. The patient describes the headache pain as throbbing and intense on the left side of her head.
The patient has a demanding job in advertising and often works very long hours on little sleep; this latest headache developed after working through the night before. When asked, she admits to feeling lethargic, yawning (to the point where coworkers commented), and experiencing intervals of excessive sweating earlier in the day before the headache emerged. The patient attributed these to being tired and hungry because of skipped meals since the previous night's dinner.
She has no history of cardiovascular or other chronic illness, and her blood pressure is within normal range. She describes having had about seven similar headaches of shorter duration, over the past 2 months; in each case, the headache led to a missed workday or having to leave work early and/or cancel social plans.
Want a healthy diet? Eat real food, GI physician advises
What exactly is a healthy diet?
Scott Ketover, MD, AGAF, FASGE, will be the first to admit that’s not an easy question to answer. “As much research and information as we have, we don’t really know what a healthy diet is,” said Dr. Ketover, president and CEO of MNGI Digestive Health in Minneapolis, Minnesota. He was recognized by AGA this year with the Distinguished Clinician Award in Private Practice.
When patients ask questions about a healthy diet, Dr. Ketover responds with a dose of common sense: “If it’s food that didn’t exist in the year 1900, don’t eat it.” Your grandmother’s apple pie is fine in moderation, he said, but the apple pie you get at the McDonald’s drive-through could sit on your shelf for 6 months and look the same.
That is not something you should eat, he emphasizes.

“I really do believe though, that what crosses our lips and gets into our GI tract really underlies our entire health. It’s just that we don’t have enough information yet to know how we can coach people in telling them: eat this, not that,” he added.
In an interview, Dr. Ketover spoke more about the link between the gut microbiome and health, and the young patient who inspired him to become a GI physician.
Q: Why did you choose GI?
Dr. Ketover: I was a medical student working on my pediatrics rotation at Children’s Minnesota (Minneapolis Pediatrics Hospital). A 17-year-old young man who had Crohn’s disease really turned this into my lifelong passion. The patient confided in me that when he was 11, he had an ileostomy. He wore an ileostomy bag for 6 years and kept it hidden from all his friends. He was petrified of their knowing. And he told me at the age of 17 that if he knew how hard it was going to be to keep that secret, he would’ve preferred to have died rather than have the ileostomy. That got me thinking a lot about Crohn’s disease, and certainly how it affects patients. It became a very motivating thing for me to be involved in something that could potentially prevent this situation for others.
Today, we have much better treatment for Crohn’s than we did 30 years ago. So that’s all a good thing.
Q: Wellness and therapeutic diets are a specific interest of yours. Can you talk about this?
Dr. Ketover: We talk about things like Cheetos, Twinkies — those are not real foods. I do direct patients to ‘think’ when they go to the grocery store. All the good stuff is in the perimeter of the store. When you walk down the aisles, it’s all the processed food with added chemicals. It’s hard to point at specific things though and say: this is bad for you, but we do know that we should eat real food as often as we can. And I think that will contribute to our knowledge and learning about the intestinal microbiome. Again, we’re really at the beginning of our infancy of this, even though there’s lots of probiotics and things out there that claim to make you healthier. We don’t really know yet. And it’s going to take more time.
Q: What role does diet play in improving the intestinal microbiome?
Dr. Ketover: When you look at people who are healthy and who have low incidence of chronic diseases or inflammatory conditions, obesity, cancer, we’re starting to study their microbiome to see how it differs from people who have those illnesses and conditions and try to understand what the different constituents are of the microbiome. And then the big question is: Okay, so once we know that, how do we take ‘the unhealthy microbiome’ and change it to the ‘healthy microbiome’?
The only method we currently have is fecal transplant for Clostridioides difficile. And that’s just not a feasible way to change the microbiome for most people.
Some studies are going on with this. There’s been laboratory studies done with lab animals that show that fecal transplant can reverse obesity.
Q: Describe your biggest practice-related challenge and what you are doing to address it.
Dr. Ketover: The biggest challenge these days for medical practices is the relationship with the payer world and prior authorization. Where we’ve seen the greatest impact of prior authorization, unfortunately, is in the Medicare Advantage programs. Payers receive money from the federal government on plans that they can better manage the patient on, rather than Medicare. That results in a tremendous amount of prior authorization.
I get particularly incensed when I see that a lot of payers are practicing medicine without a license and they’re not relying on the professionals who are actually in the exam room with patients and doing the history and physical examination to determine what is an appropriate course of diagnosis or therapy for a patient.
It comes around every January. We have patients who are stable on meds, then their insurance gets renewed and the pharmacy formulary changes. Patients stable on various therapies are either kicked off them, or we have to go through the prior authorization process again for the same patient for the umpteenth time to keep them on a stable therapy.
How do I address that? It’s in conversations with payers and policy makers. There’s a lot going on in Washington, talking about prior authorization. I’m not sure that non-practitioners fully feel the pain that it delivers to patients.
Q: What teacher or mentor had the greatest impact on you?
Dr. Ketover: Phillip M. Kibort, MD, the pediatric physician I worked with as a medical student who really turned me on to GI medicine. We worked together on several patients and I was able to develop an appreciation for the breadth and depth of GI-related abnormalities and diseases and therapies. And I really got excited by the spectrum of opportunity that I would have as a physician to help treat patients with GI illness.
Q: What would you do differently if you had a chance?
Dr. Ketover: I’d travel more both for work and for pleasure. I really enjoy my relationships that I’ve created with lots of other gastroenterologists as well as non-physicians around policy issues. I’m involved in a couple of national organizations that talk to politicians on Capitol Hill and at state houses about patient advocacy. I would have done more of that earlier in my career if I could have.
Q: What do you like to do in your free time?
Dr. Ketover: I like to run, bike, walk. I like being outside as much as possible and enjoy being active.
Lightning Round
Texting or talking?
Texting, very efficient
Favorite city in U.S. besides the one you live in?
Waikiki, Honolulu
Favorite breakfast?
Pancakes
Place you most want to travel to?
Australia and New Zealand
Favorite junk food?
Pretzels and ice cream
Favorite season?
Summer
How many cups of coffee do you drink per day?
2-3
If you weren’t a gastroenterologist, what would you be?
Public policy writer
Who inspires you?
My wife
Best Halloween costume you ever wore?
Cowboy
Favorite type of music?
Classic rock
Favorite movie genre?
Science fiction, space exploration
Cat person or dog person?
Dog
Favorite sport?
Football — to watch
What song do you have to sing along with when you hear it?
Bohemian Rhapsody
Introvert or extrovert?
Introvert
Optimist or pessimist?
Optimist
What exactly is a healthy diet?
Scott Ketover, MD, AGAF, FASGE, will be the first to admit that’s not an easy question to answer. “As much research and information as we have, we don’t really know what a healthy diet is,” said Dr. Ketover, president and CEO of MNGI Digestive Health in Minneapolis, Minnesota. He was recognized by AGA this year with the Distinguished Clinician Award in Private Practice.
When patients ask questions about a healthy diet, Dr. Ketover responds with a dose of common sense: “If it’s food that didn’t exist in the year 1900, don’t eat it.” Your grandmother’s apple pie is fine in moderation, he said, but the apple pie you get at the McDonald’s drive-through could sit on your shelf for 6 months and look the same.
That is not something you should eat, he emphasizes.
“I really do believe though, that what crosses our lips and gets into our GI tract really underlies our entire health. It’s just that we don’t have enough information yet to know how we can coach people in telling them: eat this, not that,” he added.
In an interview, Dr. Ketover spoke more about the link between the gut microbiome and health, and the young patient who inspired him to become a GI physician.
Q: Why did you choose GI?
Dr. Ketover: I was a medical student working on my pediatrics rotation at Children’s Minnesota (Minneapolis Pediatrics Hospital). A 17-year-old young man who had Crohn’s disease really turned this into my lifelong passion. The patient confided in me that when he was 11, he had an ileostomy. He wore an ileostomy bag for 6 years and kept it hidden from all his friends. He was petrified of their knowing. And he told me at the age of 17 that if he knew how hard it was going to be to keep that secret, he would’ve preferred to have died rather than have the ileostomy. That got me thinking a lot about Crohn’s disease, and certainly how it affects patients. It became a very motivating thing for me to be involved in something that could potentially prevent this situation for others.
Today, we have much better treatment for Crohn’s than we did 30 years ago. So that’s all a good thing.
Q: Wellness and therapeutic diets are a specific interest of yours. Can you talk about this?
Dr. Ketover: We talk about things like Cheetos, Twinkies — those are not real foods. I do direct patients to ‘think’ when they go to the grocery store. All the good stuff is in the perimeter of the store. When you walk down the aisles, it’s all the processed food with added chemicals. It’s hard to point at specific things though and say: this is bad for you, but we do know that we should eat real food as often as we can. And I think that will contribute to our knowledge and learning about the intestinal microbiome. Again, we’re really at the beginning of our infancy of this, even though there’s lots of probiotics and things out there that claim to make you healthier. We don’t really know yet. And it’s going to take more time.
Q: What role does diet play in improving the intestinal microbiome?
Dr. Ketover: When you look at people who are healthy and who have low incidence of chronic diseases or inflammatory conditions, obesity, cancer, we’re starting to study their microbiome to see how it differs from people who have those illnesses and conditions and try to understand what the different constituents are of the microbiome. And then the big question is: Okay, so once we know that, how do we take ‘the unhealthy microbiome’ and change it to the ‘healthy microbiome’?
The only method we currently have is fecal transplant for Clostridioides difficile. And that’s just not a feasible way to change the microbiome for most people.
Some studies are going on with this. There’s been laboratory studies done with lab animals that show that fecal transplant can reverse obesity.
Q: Describe your biggest practice-related challenge and what you are doing to address it.
Dr. Ketover: The biggest challenge these days for medical practices is the relationship with the payer world and prior authorization. Where we’ve seen the greatest impact of prior authorization, unfortunately, is in the Medicare Advantage programs. Payers receive money from the federal government on plans that they can better manage the patient on, rather than Medicare. That results in a tremendous amount of prior authorization.
I get particularly incensed when I see that a lot of payers are practicing medicine without a license and they’re not relying on the professionals who are actually in the exam room with patients and doing the history and physical examination to determine what is an appropriate course of diagnosis or therapy for a patient.
It comes around every January. We have patients who are stable on meds, then their insurance gets renewed and the pharmacy formulary changes. Patients stable on various therapies are either kicked off them, or we have to go through the prior authorization process again for the same patient for the umpteenth time to keep them on a stable therapy.
How do I address that? It’s in conversations with payers and policy makers. There’s a lot going on in Washington, talking about prior authorization. I’m not sure that non-practitioners fully feel the pain that it delivers to patients.
Q: What teacher or mentor had the greatest impact on you?
Dr. Ketover: Phillip M. Kibort, MD, the pediatric physician I worked with as a medical student who really turned me on to GI medicine. We worked together on several patients and I was able to develop an appreciation for the breadth and depth of GI-related abnormalities and diseases and therapies. And I really got excited by the spectrum of opportunity that I would have as a physician to help treat patients with GI illness.
Q: What would you do differently if you had a chance?
Dr. Ketover: I’d travel more both for work and for pleasure. I really enjoy my relationships that I’ve created with lots of other gastroenterologists as well as non-physicians around policy issues. I’m involved in a couple of national organizations that talk to politicians on Capitol Hill and at state houses about patient advocacy. I would have done more of that earlier in my career if I could have.
Q: What do you like to do in your free time?
Dr. Ketover: I like to run, bike, walk. I like being outside as much as possible and enjoy being active.
Lightning Round
Texting or talking?
Texting, very efficient
Favorite city in U.S. besides the one you live in?
Waikiki, Honolulu
Favorite breakfast?
Pancakes
Place you most want to travel to?
Australia and New Zealand
Favorite junk food?
Pretzels and ice cream
Favorite season?
Summer
How many cups of coffee do you drink per day?
2-3
If you weren’t a gastroenterologist, what would you be?
Public policy writer
Who inspires you?
My wife
Best Halloween costume you ever wore?
Cowboy
Favorite type of music?
Classic rock
Favorite movie genre?
Science fiction, space exploration
Cat person or dog person?
Dog
Favorite sport?
Football — to watch
What song do you have to sing along with when you hear it?
Bohemian Rhapsody
Introvert or extrovert?
Introvert
Optimist or pessimist?
Optimist
What exactly is a healthy diet?
Scott Ketover, MD, AGAF, FASGE, will be the first to admit that’s not an easy question to answer. “As much research and information as we have, we don’t really know what a healthy diet is,” said Dr. Ketover, president and CEO of MNGI Digestive Health in Minneapolis, Minnesota. He was recognized by AGA this year with the Distinguished Clinician Award in Private Practice.
When patients ask questions about a healthy diet, Dr. Ketover responds with a dose of common sense: “If it’s food that didn’t exist in the year 1900, don’t eat it.” Your grandmother’s apple pie is fine in moderation, he said, but the apple pie you get at the McDonald’s drive-through could sit on your shelf for 6 months and look the same.
That is not something you should eat, he emphasizes.
“I really do believe though, that what crosses our lips and gets into our GI tract really underlies our entire health. It’s just that we don’t have enough information yet to know how we can coach people in telling them: eat this, not that,” he added.
In an interview, Dr. Ketover spoke more about the link between the gut microbiome and health, and the young patient who inspired him to become a GI physician.
Q: Why did you choose GI?
Dr. Ketover: I was a medical student working on my pediatrics rotation at Children’s Minnesota (Minneapolis Pediatrics Hospital). A 17-year-old young man who had Crohn’s disease really turned this into my lifelong passion. The patient confided in me that when he was 11, he had an ileostomy. He wore an ileostomy bag for 6 years and kept it hidden from all his friends. He was petrified of their knowing. And he told me at the age of 17 that if he knew how hard it was going to be to keep that secret, he would’ve preferred to have died rather than have the ileostomy. That got me thinking a lot about Crohn’s disease, and certainly how it affects patients. It became a very motivating thing for me to be involved in something that could potentially prevent this situation for others.
Today, we have much better treatment for Crohn’s than we did 30 years ago. So that’s all a good thing.
Q: Wellness and therapeutic diets are a specific interest of yours. Can you talk about this?
Dr. Ketover: We talk about things like Cheetos, Twinkies — those are not real foods. I do direct patients to ‘think’ when they go to the grocery store. All the good stuff is in the perimeter of the store. When you walk down the aisles, it’s all the processed food with added chemicals. It’s hard to point at specific things though and say: this is bad for you, but we do know that we should eat real food as often as we can. And I think that will contribute to our knowledge and learning about the intestinal microbiome. Again, we’re really at the beginning of our infancy of this, even though there’s lots of probiotics and things out there that claim to make you healthier. We don’t really know yet. And it’s going to take more time.
Q: What role does diet play in improving the intestinal microbiome?
Dr. Ketover: When you look at people who are healthy and who have low incidence of chronic diseases or inflammatory conditions, obesity, cancer, we’re starting to study their microbiome to see how it differs from people who have those illnesses and conditions and try to understand what the different constituents are of the microbiome. And then the big question is: Okay, so once we know that, how do we take ‘the unhealthy microbiome’ and change it to the ‘healthy microbiome’?
The only method we currently have is fecal transplant for Clostridioides difficile. And that’s just not a feasible way to change the microbiome for most people.
Some studies are going on with this. There’s been laboratory studies done with lab animals that show that fecal transplant can reverse obesity.
Q: Describe your biggest practice-related challenge and what you are doing to address it.
Dr. Ketover: The biggest challenge these days for medical practices is the relationship with the payer world and prior authorization. Where we’ve seen the greatest impact of prior authorization, unfortunately, is in the Medicare Advantage programs. Payers receive money from the federal government on plans that they can better manage the patient on, rather than Medicare. That results in a tremendous amount of prior authorization.
I get particularly incensed when I see that a lot of payers are practicing medicine without a license and they’re not relying on the professionals who are actually in the exam room with patients and doing the history and physical examination to determine what is an appropriate course of diagnosis or therapy for a patient.
It comes around every January. We have patients who are stable on meds, then their insurance gets renewed and the pharmacy formulary changes. Patients stable on various therapies are either kicked off them, or we have to go through the prior authorization process again for the same patient for the umpteenth time to keep them on a stable therapy.
How do I address that? It’s in conversations with payers and policy makers. There’s a lot going on in Washington, talking about prior authorization. I’m not sure that non-practitioners fully feel the pain that it delivers to patients.
Q: What teacher or mentor had the greatest impact on you?
Dr. Ketover: Phillip M. Kibort, MD, the pediatric physician I worked with as a medical student who really turned me on to GI medicine. We worked together on several patients and I was able to develop an appreciation for the breadth and depth of GI-related abnormalities and diseases and therapies. And I really got excited by the spectrum of opportunity that I would have as a physician to help treat patients with GI illness.
Q: What would you do differently if you had a chance?
Dr. Ketover: I’d travel more both for work and for pleasure. I really enjoy my relationships that I’ve created with lots of other gastroenterologists as well as non-physicians around policy issues. I’m involved in a couple of national organizations that talk to politicians on Capitol Hill and at state houses about patient advocacy. I would have done more of that earlier in my career if I could have.
Q: What do you like to do in your free time?
Dr. Ketover: I like to run, bike, walk. I like being outside as much as possible and enjoy being active.
Lightning Round
Texting or talking?
Texting, very efficient
Favorite city in U.S. besides the one you live in?
Waikiki, Honolulu
Favorite breakfast?
Pancakes
Place you most want to travel to?
Australia and New Zealand
Favorite junk food?
Pretzels and ice cream
Favorite season?
Summer
How many cups of coffee do you drink per day?
2-3
If you weren’t a gastroenterologist, what would you be?
Public policy writer
Who inspires you?
My wife
Best Halloween costume you ever wore?
Cowboy
Favorite type of music?
Classic rock
Favorite movie genre?
Science fiction, space exploration
Cat person or dog person?
Dog
Favorite sport?
Football — to watch
What song do you have to sing along with when you hear it?
Bohemian Rhapsody
Introvert or extrovert?
Introvert
Optimist or pessimist?
Optimist
Myth of the Month: Is Contrast-Induced Acute Kidney Injury Real?
A 59-year-old man presents with abdominal pain. He has a history of small bowel obstruction and diverticulitis. His medical history includes chronic kidney disease (CKD; baseline creatinine, 1.8 mg/dL), hypertension, type 2 diabetes, and depression. He had a colectomy 6 years ago for colon cancer.
He takes the following medications: Semaglutide (1 mg weekly), amlodipine (5 mg once daily), and escitalopram (10 mg once daily). On physical exam his blood pressure is 130/80 mm Hg, his pulse is 90, and his temperature is 37.2 degrees C. He has normal bowel sounds but guarding in the right lower quadrant.

His hemoglobin is 14 g/dL, his blood sodium is 136 mEq/L, his blood potassium is 4.0 mmol/L, his BUN is 26 mg/dL, and his creatinine is 1.9 mg/dL. His kidney, ureter, bladder x-ray is unremarkable.
What imaging would you recommend?
A) CT without contrast
B) CT with contrast
C) MRI
D) Abdominal ultrasound
This patient has several potential causes for his abdominal pain that imaging may clarify. I think a contrast CT scan would be the most likely to provide helpful information. It is likely that if it were ordered, there may be hesitation by the radiologist to perform the scan with contrast because of the patient’s CKD.
Concern for contrast-induced kidney injury has limited diagnostic testing for many years. How strong is the evidence for contrast-induced kidney injury, and should we avoid testing that requires contrast in patients with CKD? McDonald and colleagues performed a meta-analysis with 13 studies meeting inclusion criteria, involving 25,950 patients.1 They found no increased risk of acute kidney injury (AKI) in patients who received contrast medium compared with those who did not receive contrast; relative risk of AKI for those receiving contrast was 0.79 (confidence interval: 0.62-1.02). Importantly, there was no difference in AKI in patients with diabetes or CKD.
Ehmann et al. looked at renal outcomes in patients who received IV contrast when they presented to an emergency department with AKI.2 They found that in patients with AKI, receiving contrast was not associated with persistent AKI at hospital discharge. Hinson and colleagues looked at patients arriving at the emergency department and needing imaging.3 They did a retrospective, cohort analysis of 17,934 patients who had CT with contrast, CT with no contrast, or no CT. Contrast administration was not associated with increased incidence of AKI (odds ratio, 0.96, CI: 0.85-1.08).
Aycock et al. did a meta-analysis of AKI after CT scanning, including 28 studies involving 107,335 patients.4 They found that compared with noncontrast CT, CT scanning with contrast was not associated with AKI (OR, 0.94, CI: 0.83-1.07). Elias and Aronson looked at the risk of AKI after contrast in patients receiving CT scans compared with those who received ventilation/perfusion scans to evaluate for pulmonary embolism.5 There were 44 AKI events (4.5%) in patients exposed to contrast media and 33 events (3.4%) in patients not exposed to contrast media (risk difference: 1.1%, 95% CI: -0.6% to 2.9%; OR, 1.39, CI: 0.86-2.26; P = .18).
Despite multiple studies showing no increased risk, there is still a concern that contrast can cause AKI.6 Animal models have shown iodinated contrast can have a deleterious effect on mitochondria and membrane function.6 Criticisms of the retrospective nature of many of the studies I have shared, and the lack of randomized, controlled trials are that there may be bias in these studies, as the highest-risk patients are the ones most likely not to receive contrast. In a joint guideline from the American College of Radiology and the National Kidney Foundation, this statement was made: “The risk of acute kidney injury developing in patients with reduced kidney function following exposure to intravenous iodinated contrast media has been overstated.”7 Their recommendation was to give contrast if needed in patients with glomerular filtration rates (GFRs) greater than 30.
Myth: Contrast-induced renal injury is a concern.
Clinical impact: For CT scanning, it is OK to give contrast when needed. A conservative cutoff for contrast use would be a GFR less than 30.
Dr. Paauw is professor of medicine in the Division of General Internal Medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at dpaauw@uw.edu.
References
1. McDonald JS et al. Radiology. 2013:267:119-128.
2. Ehmann MR et al. Intensive Care Med. 2023:49(2):205-215.
3. Hinson JS et al. Ann Emerg Med. 2017;69(5):577-586.
4. Aycock RD et al. Ann Emerg Med. 2018 Jan;71(1):44-53.
5. Elias A, Aronson D. Thromb Haemost. 2021 Jun;121(6):800-807.
6. Weisbord SD, du Cheryon D. Intensive Care Med. 2018;44(1):107-109.
7. Davenport MS et al. Radiology. 2020;294(3):660-668.
A 59-year-old man presents with abdominal pain. He has a history of small bowel obstruction and diverticulitis. His medical history includes chronic kidney disease (CKD; baseline creatinine, 1.8 mg/dL), hypertension, type 2 diabetes, and depression. He had a colectomy 6 years ago for colon cancer.
He takes the following medications: Semaglutide (1 mg weekly), amlodipine (5 mg once daily), and escitalopram (10 mg once daily). On physical exam his blood pressure is 130/80 mm Hg, his pulse is 90, and his temperature is 37.2 degrees C. He has normal bowel sounds but guarding in the right lower quadrant.
His hemoglobin is 14 g/dL, his blood sodium is 136 mEq/L, his blood potassium is 4.0 mmol/L, his BUN is 26 mg/dL, and his creatinine is 1.9 mg/dL. His kidney, ureter, bladder x-ray is unremarkable.
What imaging would you recommend?
A) CT without contrast
B) CT with contrast
C) MRI
D) Abdominal ultrasound
This patient has several potential causes for his abdominal pain that imaging may clarify. I think a contrast CT scan would be the most likely to provide helpful information. It is likely that if it were ordered, there may be hesitation by the radiologist to perform the scan with contrast because of the patient’s CKD.
Concern for contrast-induced kidney injury has limited diagnostic testing for many years. How strong is the evidence for contrast-induced kidney injury, and should we avoid testing that requires contrast in patients with CKD? McDonald and colleagues performed a meta-analysis with 13 studies meeting inclusion criteria, involving 25,950 patients.1 They found no increased risk of acute kidney injury (AKI) in patients who received contrast medium compared with those who did not receive contrast; relative risk of AKI for those receiving contrast was 0.79 (confidence interval: 0.62-1.02). Importantly, there was no difference in AKI in patients with diabetes or CKD.
Ehmann et al. looked at renal outcomes in patients who received IV contrast when they presented to an emergency department with AKI.2 They found that in patients with AKI, receiving contrast was not associated with persistent AKI at hospital discharge. Hinson and colleagues looked at patients arriving at the emergency department and needing imaging.3 They did a retrospective, cohort analysis of 17,934 patients who had CT with contrast, CT with no contrast, or no CT. Contrast administration was not associated with increased incidence of AKI (odds ratio, 0.96, CI: 0.85-1.08).
Aycock et al. did a meta-analysis of AKI after CT scanning, including 28 studies involving 107,335 patients.4 They found that compared with noncontrast CT, CT scanning with contrast was not associated with AKI (OR, 0.94, CI: 0.83-1.07). Elias and Aronson looked at the risk of AKI after contrast in patients receiving CT scans compared with those who received ventilation/perfusion scans to evaluate for pulmonary embolism.5 There were 44 AKI events (4.5%) in patients exposed to contrast media and 33 events (3.4%) in patients not exposed to contrast media (risk difference: 1.1%, 95% CI: -0.6% to 2.9%; OR, 1.39, CI: 0.86-2.26; P = .18).
Despite multiple studies showing no increased risk, there is still a concern that contrast can cause AKI.6 Animal models have shown iodinated contrast can have a deleterious effect on mitochondria and membrane function.6 Criticisms of the retrospective nature of many of the studies I have shared, and the lack of randomized, controlled trials are that there may be bias in these studies, as the highest-risk patients are the ones most likely not to receive contrast. In a joint guideline from the American College of Radiology and the National Kidney Foundation, this statement was made: “The risk of acute kidney injury developing in patients with reduced kidney function following exposure to intravenous iodinated contrast media has been overstated.”7 Their recommendation was to give contrast if needed in patients with glomerular filtration rates (GFRs) greater than 30.
Myth: Contrast-induced renal injury is a concern.
Clinical impact: For CT scanning, it is OK to give contrast when needed. A conservative cutoff for contrast use would be a GFR less than 30.
Dr. Paauw is professor of medicine in the Division of General Internal Medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at dpaauw@uw.edu.
References
1. McDonald JS et al. Radiology. 2013:267:119-128.
2. Ehmann MR et al. Intensive Care Med. 2023:49(2):205-215.
3. Hinson JS et al. Ann Emerg Med. 2017;69(5):577-586.
4. Aycock RD et al. Ann Emerg Med. 2018 Jan;71(1):44-53.
5. Elias A, Aronson D. Thromb Haemost. 2021 Jun;121(6):800-807.
6. Weisbord SD, du Cheryon D. Intensive Care Med. 2018;44(1):107-109.
7. Davenport MS et al. Radiology. 2020;294(3):660-668.
A 59-year-old man presents with abdominal pain. He has a history of small bowel obstruction and diverticulitis. His medical history includes chronic kidney disease (CKD; baseline creatinine, 1.8 mg/dL), hypertension, type 2 diabetes, and depression. He had a colectomy 6 years ago for colon cancer.
He takes the following medications: Semaglutide (1 mg weekly), amlodipine (5 mg once daily), and escitalopram (10 mg once daily). On physical exam his blood pressure is 130/80 mm Hg, his pulse is 90, and his temperature is 37.2 degrees C. He has normal bowel sounds but guarding in the right lower quadrant.
His hemoglobin is 14 g/dL, his blood sodium is 136 mEq/L, his blood potassium is 4.0 mmol/L, his BUN is 26 mg/dL, and his creatinine is 1.9 mg/dL. His kidney, ureter, bladder x-ray is unremarkable.
What imaging would you recommend?
A) CT without contrast
B) CT with contrast
C) MRI
D) Abdominal ultrasound
This patient has several potential causes for his abdominal pain that imaging may clarify. I think a contrast CT scan would be the most likely to provide helpful information. It is likely that if it were ordered, there may be hesitation by the radiologist to perform the scan with contrast because of the patient’s CKD.
Concern for contrast-induced kidney injury has limited diagnostic testing for many years. How strong is the evidence for contrast-induced kidney injury, and should we avoid testing that requires contrast in patients with CKD? McDonald and colleagues performed a meta-analysis with 13 studies meeting inclusion criteria, involving 25,950 patients.1 They found no increased risk of acute kidney injury (AKI) in patients who received contrast medium compared with those who did not receive contrast; relative risk of AKI for those receiving contrast was 0.79 (confidence interval: 0.62-1.02). Importantly, there was no difference in AKI in patients with diabetes or CKD.
Ehmann et al. looked at renal outcomes in patients who received IV contrast when they presented to an emergency department with AKI.2 They found that in patients with AKI, receiving contrast was not associated with persistent AKI at hospital discharge. Hinson and colleagues looked at patients arriving at the emergency department and needing imaging.3 They did a retrospective, cohort analysis of 17,934 patients who had CT with contrast, CT with no contrast, or no CT. Contrast administration was not associated with increased incidence of AKI (odds ratio, 0.96, CI: 0.85-1.08).
Aycock et al. did a meta-analysis of AKI after CT scanning, including 28 studies involving 107,335 patients.4 They found that compared with noncontrast CT, CT scanning with contrast was not associated with AKI (OR, 0.94, CI: 0.83-1.07). Elias and Aronson looked at the risk of AKI after contrast in patients receiving CT scans compared with those who received ventilation/perfusion scans to evaluate for pulmonary embolism.5 There were 44 AKI events (4.5%) in patients exposed to contrast media and 33 events (3.4%) in patients not exposed to contrast media (risk difference: 1.1%, 95% CI: -0.6% to 2.9%; OR, 1.39, CI: 0.86-2.26; P = .18).
Despite multiple studies showing no increased risk, there is still a concern that contrast can cause AKI.6 Animal models have shown iodinated contrast can have a deleterious effect on mitochondria and membrane function.6 Criticisms of the retrospective nature of many of the studies I have shared, and the lack of randomized, controlled trials are that there may be bias in these studies, as the highest-risk patients are the ones most likely not to receive contrast. In a joint guideline from the American College of Radiology and the National Kidney Foundation, this statement was made: “The risk of acute kidney injury developing in patients with reduced kidney function following exposure to intravenous iodinated contrast media has been overstated.”7 Their recommendation was to give contrast if needed in patients with glomerular filtration rates (GFRs) greater than 30.
Myth: Contrast-induced renal injury is a concern.
Clinical impact: For CT scanning, it is OK to give contrast when needed. A conservative cutoff for contrast use would be a GFR less than 30.
Dr. Paauw is professor of medicine in the Division of General Internal Medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at dpaauw@uw.edu.
References
1. McDonald JS et al. Radiology. 2013:267:119-128.
2. Ehmann MR et al. Intensive Care Med. 2023:49(2):205-215.
3. Hinson JS et al. Ann Emerg Med. 2017;69(5):577-586.
4. Aycock RD et al. Ann Emerg Med. 2018 Jan;71(1):44-53.
5. Elias A, Aronson D. Thromb Haemost. 2021 Jun;121(6):800-807.
6. Weisbord SD, du Cheryon D. Intensive Care Med. 2018;44(1):107-109.
7. Davenport MS et al. Radiology. 2020;294(3):660-668.
US Researchers Call for Robust Studies Into Dequalinium, a Bacterial Vaginosis Therapy Common in Europe
Interest is growing in a standard European treatment for bacterial vaginosis (BV).
In a commentary published in JAMA Network Open, researchers and doctors from the Johns Hopkins University School of Medicine in Baltimore and the University of Maryland, Baltimore, urged clinical trials in the United States to determine if dequalinium chloride — an antiseptic that inhibits the growth of bacteria and fungi — is on par with or better than treatments currently available.
Dequalinium has been used throughout Europe for decades and is recommended as an alternative or second-line BV treatment by the World Health Organization; the International Society for the Study of Vulvovaginal Disease; and the Austrian, German, Portuguese, Spanish, and Swiss Societies of Gynecology and Obstetrics. However, the product has not been approved for clinical use in the United States, no trials studying the drug have been registered on ClinicalTrials.gov, and the US Food and Drug Administration has not received an application for approval, according to agency records.
Treatments in the United States for BV include metronidazole and clindamycin that, while effective, have a recurrence rate of up to 60%.
“Current treatments for bacterial vaginosis often fall short, primarily due to frequent recurrences after treatment,” said Rebecca M. Brotman, PhD, MPH, a professor in the Department of Epidemiology and Public Health at the Institute for Genome Sciences at the University of Maryland School of Medicine, and the corresponding author of the commentary.
More than 40% of people with recurrent BV do not receive adequate treatment, according to Caroline M. Mitchell, MD, MPH, director of the Vulvovaginal Disorders Program at Massachusetts General Hospital Vincent Center for Reproductive Biology, Boston, Massachusetts.
“BV is very disruptive to people’s daily lives and causes significant distress,” said Dr. Mitchell, who was not a coauthor of the new article. “Additionally, BV is associated with higher risk for HPV [human papillomavirus] infection, progression of HPV to cervical dysplasia, as well as risk for acquisition of other sexually transmitted infections.”
Dr. Mitchell said she hopes a recent trial from Europe comparing dequalinium chloride to metronidazole spurs researchers to study its efficacy and safety among women in the United States.
“Dequalinium has some antifungal activity, so it might offer a lower chance of yeast infection after treatment, which is important because posttreatment vulvovaginal candidiasis is one of the downsides to conventional antibiotic treatments,” Dr. Mitchell said.
The recent clinical trial included 147 premenopausal women with BV who received 10 mg of dequalinium per day for 6 days or oral metronidazole (500 mg twice daily for 7 days).
Dr. Brotman said any studies in the United States would need to examine long-term recurrence of vaginosis after treatment with dequalinium chloride and its use during pregnancy.
The study was funded by various grants from the National Institutes of Health and the Gates Foundation. Various authors reported receiving royalties from UpToDate outside the submitted work or receiving a donation of sexually transmitted infection testing kits from Hologic for a study outside the submitted work. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
Interest is growing in a standard European treatment for bacterial vaginosis (BV).
In a commentary published in JAMA Network Open, researchers and doctors from the Johns Hopkins University School of Medicine in Baltimore and the University of Maryland, Baltimore, urged clinical trials in the United States to determine if dequalinium chloride — an antiseptic that inhibits the growth of bacteria and fungi — is on par with or better than treatments currently available.
Dequalinium has been used throughout Europe for decades and is recommended as an alternative or second-line BV treatment by the World Health Organization; the International Society for the Study of Vulvovaginal Disease; and the Austrian, German, Portuguese, Spanish, and Swiss Societies of Gynecology and Obstetrics. However, the product has not been approved for clinical use in the United States, no trials studying the drug have been registered on ClinicalTrials.gov, and the US Food and Drug Administration has not received an application for approval, according to agency records.
Treatments in the United States for BV include metronidazole and clindamycin that, while effective, have a recurrence rate of up to 60%.
“Current treatments for bacterial vaginosis often fall short, primarily due to frequent recurrences after treatment,” said Rebecca M. Brotman, PhD, MPH, a professor in the Department of Epidemiology and Public Health at the Institute for Genome Sciences at the University of Maryland School of Medicine, and the corresponding author of the commentary.
More than 40% of people with recurrent BV do not receive adequate treatment, according to Caroline M. Mitchell, MD, MPH, director of the Vulvovaginal Disorders Program at Massachusetts General Hospital Vincent Center for Reproductive Biology, Boston, Massachusetts.
“BV is very disruptive to people’s daily lives and causes significant distress,” said Dr. Mitchell, who was not a coauthor of the new article. “Additionally, BV is associated with higher risk for HPV [human papillomavirus] infection, progression of HPV to cervical dysplasia, as well as risk for acquisition of other sexually transmitted infections.”
Dr. Mitchell said she hopes a recent trial from Europe comparing dequalinium chloride to metronidazole spurs researchers to study its efficacy and safety among women in the United States.
“Dequalinium has some antifungal activity, so it might offer a lower chance of yeast infection after treatment, which is important because posttreatment vulvovaginal candidiasis is one of the downsides to conventional antibiotic treatments,” Dr. Mitchell said.
The recent clinical trial included 147 premenopausal women with BV who received 10 mg of dequalinium per day for 6 days or oral metronidazole (500 mg twice daily for 7 days).
Dr. Brotman said any studies in the United States would need to examine long-term recurrence of vaginosis after treatment with dequalinium chloride and its use during pregnancy.
The study was funded by various grants from the National Institutes of Health and the Gates Foundation. Various authors reported receiving royalties from UpToDate outside the submitted work or receiving a donation of sexually transmitted infection testing kits from Hologic for a study outside the submitted work. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
Interest is growing in a standard European treatment for bacterial vaginosis (BV).
In a commentary published in JAMA Network Open, researchers and doctors from the Johns Hopkins University School of Medicine in Baltimore and the University of Maryland, Baltimore, urged clinical trials in the United States to determine if dequalinium chloride — an antiseptic that inhibits the growth of bacteria and fungi — is on par with or better than treatments currently available.
Dequalinium has been used throughout Europe for decades and is recommended as an alternative or second-line BV treatment by the World Health Organization; the International Society for the Study of Vulvovaginal Disease; and the Austrian, German, Portuguese, Spanish, and Swiss Societies of Gynecology and Obstetrics. However, the product has not been approved for clinical use in the United States, no trials studying the drug have been registered on ClinicalTrials.gov, and the US Food and Drug Administration has not received an application for approval, according to agency records.
Treatments in the United States for BV include metronidazole and clindamycin that, while effective, have a recurrence rate of up to 60%.
“Current treatments for bacterial vaginosis often fall short, primarily due to frequent recurrences after treatment,” said Rebecca M. Brotman, PhD, MPH, a professor in the Department of Epidemiology and Public Health at the Institute for Genome Sciences at the University of Maryland School of Medicine, and the corresponding author of the commentary.
More than 40% of people with recurrent BV do not receive adequate treatment, according to Caroline M. Mitchell, MD, MPH, director of the Vulvovaginal Disorders Program at Massachusetts General Hospital Vincent Center for Reproductive Biology, Boston, Massachusetts.
“BV is very disruptive to people’s daily lives and causes significant distress,” said Dr. Mitchell, who was not a coauthor of the new article. “Additionally, BV is associated with higher risk for HPV [human papillomavirus] infection, progression of HPV to cervical dysplasia, as well as risk for acquisition of other sexually transmitted infections.”
Dr. Mitchell said she hopes a recent trial from Europe comparing dequalinium chloride to metronidazole spurs researchers to study its efficacy and safety among women in the United States.
“Dequalinium has some antifungal activity, so it might offer a lower chance of yeast infection after treatment, which is important because posttreatment vulvovaginal candidiasis is one of the downsides to conventional antibiotic treatments,” Dr. Mitchell said.
The recent clinical trial included 147 premenopausal women with BV who received 10 mg of dequalinium per day for 6 days or oral metronidazole (500 mg twice daily for 7 days).
Dr. Brotman said any studies in the United States would need to examine long-term recurrence of vaginosis after treatment with dequalinium chloride and its use during pregnancy.
The study was funded by various grants from the National Institutes of Health and the Gates Foundation. Various authors reported receiving royalties from UpToDate outside the submitted work or receiving a donation of sexually transmitted infection testing kits from Hologic for a study outside the submitted work. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Vibegron Seen Effective for Overactive Bladder in Men With BPH
The medication vibegron led to improvements in symptoms of overactive bladder and overall quality of life in men undergoing treatment for benign prostatic hyperplasia, according to findings from a phase 3 trial presented at the annual meeting of the American Urological Association (AUA) and data published in the Journal of Urology.
“Vibegron was associated with significant reductions in daily micturition and urgency episodes, as well as our secondary endpoints,” David R. Staskin, MD, an associate professor of urology at Tufts University School of Medicine in Boston, told attendees. “Symptoms really did improve compared to placebo as early as week 2.”
Vibegron is a selective beta-3 adrenergic receptor agonist approved in 2020 by the US Food and Drug Administration for the treatment of overactive bladder.
However, treating overactive bladder symptoms in patients undergoing benign prostatic hyperplasia treatment is more complex because benign prostatic hyperplasia itself can contribute to overactive bladder symptoms, said Kara Watts, MD, an associate professor of urology at Montefiore Einstein in New York City, who was not involved in the new research.
“Management of overactive bladder in this setting may require treatment of benign prostatic hyperplasia as well, but a discussion of the relationship between benign prostatic hyperplasia and overactive bladder symptoms is important,” Dr. Watts told this news organization. “Beyond consideration of treatment for benign prostatic hyperplasia — which can be in the form of medications or surgeries to reduce the size of the prostate — treatment of overactive bladder can include behavioral modification,” such as avoiding bladder irritants, timed voiding, managing constipation, and nighttime liquid restriction,” as well as “medications, percutaneous tibial nerve stimulation, and occasionally more invasive options.”
Vibegron “represents a very attractive and effective pharmaceutical management option for overactive bladder,” both in patients with and without benign prostatic hyperplasia, Dr. Watts said. “It has a favorable side-effect profile compared to other oral agents that can be prescribed for overactive bladder, such as anticholinergics, and also has the added benefit of a much lower risk of urinary retention in comparison to most other oral agents.”
Among 1104 men at least 45 years old who were undergoing treatment for benign prostatic hyperplasia and had symptoms of overactive bladder, 538 received 75 mg of vibegron and 542 received a placebo. The men in the vibegron group showed 2.04 fewer mean daily urinations at 12 weeks and 2.2 fewer at 24 weeks compared to 1.3 fewer at both 12 and 24 weeks for men in the placebo group (P < .0001), according to the researchers.
The drug also reduced urgency of urination. Mean daily episodes of urgency were 2.88 fewer at 12 weeks and 3.07 fewer at 24 weeks in the vibegron group compared to 1.93 and 2.17 fewer, respectively, in the placebo group (P < .0001).
In secondary endpoints, those taking vibegron experienced 0.22 fewer episodes of nocturia (P = .002), 0.8 fewer episodes of urgency incontinence (P = .003), a 0.9-point difference in improvement in the International Prostate Symptom Score (P < .0001), and about 15 mL more volume voided (P < .0001) compared to those receiving placebo, the researchers reported.
“The clinical significance of these findings is that vibegron represents an effective pharmacologic option for managing overactive bladder in the context of concomitant benign prostatic hyperplasia, which is a broader context than its original approval for overactive bladder alone,” Dr. Watts said.
Data from 969 patients on the overactive bladder quality-of-life questionnaire found that the symptom bother score was 6.2 points better for men in the vibegron group than those who took a placebo (P < .0001) at 12 weeks. Similarly, the total health-related quality-of-life score was 4.3 points better in the vibegron group (P < .0001). Measures of concern, coping, and sleep also improved significantly in the men taking vibegron and remained significant at 24 weeks (P < .0001).
Rates of adverse events were similar in the vibegron (45%) and placebo (39%) groups. The most common adverse event was hypertension, which occurred in 9% of the vibegron group and 8.3% of men in the placebo group.
The research was funded by Sumitomo Pharma America, Inc., which makes vibegron. Dr. Staskin is a consultant for Astellas, AzuraBio, Sumitomo Pharma America, Inc., and UroCure; is a lecturer for Astellas and Sumitomo; and holds other interests in UroCure, AzuraBio, and Quillitin Pharma. Three co-authors are Sumitomo employees; one is an investigator for Sumitomo, and another has consulted for Hologic, received research funding from Allergan/AbbVie and Uromedica, and been involved in clinical trials on behalf of Sumitomo. Dr. Watts reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
The medication vibegron led to improvements in symptoms of overactive bladder and overall quality of life in men undergoing treatment for benign prostatic hyperplasia, according to findings from a phase 3 trial presented at the annual meeting of the American Urological Association (AUA) and data published in the Journal of Urology.
“Vibegron was associated with significant reductions in daily micturition and urgency episodes, as well as our secondary endpoints,” David R. Staskin, MD, an associate professor of urology at Tufts University School of Medicine in Boston, told attendees. “Symptoms really did improve compared to placebo as early as week 2.”
Vibegron is a selective beta-3 adrenergic receptor agonist approved in 2020 by the US Food and Drug Administration for the treatment of overactive bladder.
However, treating overactive bladder symptoms in patients undergoing benign prostatic hyperplasia treatment is more complex because benign prostatic hyperplasia itself can contribute to overactive bladder symptoms, said Kara Watts, MD, an associate professor of urology at Montefiore Einstein in New York City, who was not involved in the new research.
“Management of overactive bladder in this setting may require treatment of benign prostatic hyperplasia as well, but a discussion of the relationship between benign prostatic hyperplasia and overactive bladder symptoms is important,” Dr. Watts told this news organization. “Beyond consideration of treatment for benign prostatic hyperplasia — which can be in the form of medications or surgeries to reduce the size of the prostate — treatment of overactive bladder can include behavioral modification,” such as avoiding bladder irritants, timed voiding, managing constipation, and nighttime liquid restriction,” as well as “medications, percutaneous tibial nerve stimulation, and occasionally more invasive options.”
Vibegron “represents a very attractive and effective pharmaceutical management option for overactive bladder,” both in patients with and without benign prostatic hyperplasia, Dr. Watts said. “It has a favorable side-effect profile compared to other oral agents that can be prescribed for overactive bladder, such as anticholinergics, and also has the added benefit of a much lower risk of urinary retention in comparison to most other oral agents.”
Among 1104 men at least 45 years old who were undergoing treatment for benign prostatic hyperplasia and had symptoms of overactive bladder, 538 received 75 mg of vibegron and 542 received a placebo. The men in the vibegron group showed 2.04 fewer mean daily urinations at 12 weeks and 2.2 fewer at 24 weeks compared to 1.3 fewer at both 12 and 24 weeks for men in the placebo group (P < .0001), according to the researchers.
The drug also reduced urgency of urination. Mean daily episodes of urgency were 2.88 fewer at 12 weeks and 3.07 fewer at 24 weeks in the vibegron group compared to 1.93 and 2.17 fewer, respectively, in the placebo group (P < .0001).
In secondary endpoints, those taking vibegron experienced 0.22 fewer episodes of nocturia (P = .002), 0.8 fewer episodes of urgency incontinence (P = .003), a 0.9-point difference in improvement in the International Prostate Symptom Score (P < .0001), and about 15 mL more volume voided (P < .0001) compared to those receiving placebo, the researchers reported.
“The clinical significance of these findings is that vibegron represents an effective pharmacologic option for managing overactive bladder in the context of concomitant benign prostatic hyperplasia, which is a broader context than its original approval for overactive bladder alone,” Dr. Watts said.
Data from 969 patients on the overactive bladder quality-of-life questionnaire found that the symptom bother score was 6.2 points better for men in the vibegron group than those who took a placebo (P < .0001) at 12 weeks. Similarly, the total health-related quality-of-life score was 4.3 points better in the vibegron group (P < .0001). Measures of concern, coping, and sleep also improved significantly in the men taking vibegron and remained significant at 24 weeks (P < .0001).
Rates of adverse events were similar in the vibegron (45%) and placebo (39%) groups. The most common adverse event was hypertension, which occurred in 9% of the vibegron group and 8.3% of men in the placebo group.
The research was funded by Sumitomo Pharma America, Inc., which makes vibegron. Dr. Staskin is a consultant for Astellas, AzuraBio, Sumitomo Pharma America, Inc., and UroCure; is a lecturer for Astellas and Sumitomo; and holds other interests in UroCure, AzuraBio, and Quillitin Pharma. Three co-authors are Sumitomo employees; one is an investigator for Sumitomo, and another has consulted for Hologic, received research funding from Allergan/AbbVie and Uromedica, and been involved in clinical trials on behalf of Sumitomo. Dr. Watts reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
The medication vibegron led to improvements in symptoms of overactive bladder and overall quality of life in men undergoing treatment for benign prostatic hyperplasia, according to findings from a phase 3 trial presented at the annual meeting of the American Urological Association (AUA) and data published in the Journal of Urology.
“Vibegron was associated with significant reductions in daily micturition and urgency episodes, as well as our secondary endpoints,” David R. Staskin, MD, an associate professor of urology at Tufts University School of Medicine in Boston, told attendees. “Symptoms really did improve compared to placebo as early as week 2.”
Vibegron is a selective beta-3 adrenergic receptor agonist approved in 2020 by the US Food and Drug Administration for the treatment of overactive bladder.
However, treating overactive bladder symptoms in patients undergoing benign prostatic hyperplasia treatment is more complex because benign prostatic hyperplasia itself can contribute to overactive bladder symptoms, said Kara Watts, MD, an associate professor of urology at Montefiore Einstein in New York City, who was not involved in the new research.
“Management of overactive bladder in this setting may require treatment of benign prostatic hyperplasia as well, but a discussion of the relationship between benign prostatic hyperplasia and overactive bladder symptoms is important,” Dr. Watts told this news organization. “Beyond consideration of treatment for benign prostatic hyperplasia — which can be in the form of medications or surgeries to reduce the size of the prostate — treatment of overactive bladder can include behavioral modification,” such as avoiding bladder irritants, timed voiding, managing constipation, and nighttime liquid restriction,” as well as “medications, percutaneous tibial nerve stimulation, and occasionally more invasive options.”
Vibegron “represents a very attractive and effective pharmaceutical management option for overactive bladder,” both in patients with and without benign prostatic hyperplasia, Dr. Watts said. “It has a favorable side-effect profile compared to other oral agents that can be prescribed for overactive bladder, such as anticholinergics, and also has the added benefit of a much lower risk of urinary retention in comparison to most other oral agents.”
Among 1104 men at least 45 years old who were undergoing treatment for benign prostatic hyperplasia and had symptoms of overactive bladder, 538 received 75 mg of vibegron and 542 received a placebo. The men in the vibegron group showed 2.04 fewer mean daily urinations at 12 weeks and 2.2 fewer at 24 weeks compared to 1.3 fewer at both 12 and 24 weeks for men in the placebo group (P < .0001), according to the researchers.
The drug also reduced urgency of urination. Mean daily episodes of urgency were 2.88 fewer at 12 weeks and 3.07 fewer at 24 weeks in the vibegron group compared to 1.93 and 2.17 fewer, respectively, in the placebo group (P < .0001).
In secondary endpoints, those taking vibegron experienced 0.22 fewer episodes of nocturia (P = .002), 0.8 fewer episodes of urgency incontinence (P = .003), a 0.9-point difference in improvement in the International Prostate Symptom Score (P < .0001), and about 15 mL more volume voided (P < .0001) compared to those receiving placebo, the researchers reported.
“The clinical significance of these findings is that vibegron represents an effective pharmacologic option for managing overactive bladder in the context of concomitant benign prostatic hyperplasia, which is a broader context than its original approval for overactive bladder alone,” Dr. Watts said.
Data from 969 patients on the overactive bladder quality-of-life questionnaire found that the symptom bother score was 6.2 points better for men in the vibegron group than those who took a placebo (P < .0001) at 12 weeks. Similarly, the total health-related quality-of-life score was 4.3 points better in the vibegron group (P < .0001). Measures of concern, coping, and sleep also improved significantly in the men taking vibegron and remained significant at 24 weeks (P < .0001).
Rates of adverse events were similar in the vibegron (45%) and placebo (39%) groups. The most common adverse event was hypertension, which occurred in 9% of the vibegron group and 8.3% of men in the placebo group.
The research was funded by Sumitomo Pharma America, Inc., which makes vibegron. Dr. Staskin is a consultant for Astellas, AzuraBio, Sumitomo Pharma America, Inc., and UroCure; is a lecturer for Astellas and Sumitomo; and holds other interests in UroCure, AzuraBio, and Quillitin Pharma. Three co-authors are Sumitomo employees; one is an investigator for Sumitomo, and another has consulted for Hologic, received research funding from Allergan/AbbVie and Uromedica, and been involved in clinical trials on behalf of Sumitomo. Dr. Watts reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
FROM AUA 2024
Kids and Anti-Obesity Medications: Real-World Challenges
DENVER — The ability to provide adolescents with highly effective anti-obesity medications that now carry approvals from the US Food and Drug Administration (FDA) and support in guidelines offers reassurance of their use; however, a reality check often awaits for clinicians in terms of challenges ranging from accessing and affording the medications to managing real and rumored side effects.
Weighing in on the issues, experts at Obesity Medicine (OMA) 2024 offered some key strategies and practice hacks for overcoming those hurdles.
The incentive to provide treatment with popular glucagon-like peptide 1 (GLP-1) drugs such as semaglutide or the dual glucose-dependent insulinotropic peptide (GIP) GLP-1 tirzepatide lies in the evidence that their high efficacy in promoting weight loss, and hence preventing metabolic syndrome, has benefits that far outweigh the potential side effects, said Alaina Vidmar, MD, in presenting at the meeting.
“We can look at all the evidence and without question acknowledge that the GLP-1s/GIP agonists are the most effective agents that we currently have, with the least heterogeneity in response, and the most high responders compared with other agents,” said Dr. Vidmar, an assistant professor of clinical pediatrics at the Keck School of Medicine of University of Southern California and director of obesity medicine and bariatric surgery at Children’s Hospital Los Angeles.
The strength of the evidence is reflected in the landmark American Academy of Pediatrics (AAP) Clinical Practice Guideline for the Evaluation and Treatment of Children and Adolescents With Obesity, which recommends that “pediatricians and other primary healthcare providers should offer adolescents 12 years and older with obesity weight loss pharmacotherapy, according to medication indications, risks and may offer adolescents 8 years old with obesity weight loss pharmacotherapy, according to medication indications, risks.”
The AAP guidance echoes the recommendations of the drug makers and FDA that “a combination of specific behavioral techniques within the context of family-based behavioral treatment and the use of pharmacotherapy may be necessary to prevent life-limiting complications over time.”
However, in real-world practice, with the various challenges in providing that intensive, comprehensive care, clinicians should be prepared to get creative: “We sometimes have to do the best we can with what we have because the watchful waiting approach is not effective and leads to more harm than good,” Dr. Vidmar said.
Facilitating Access
The ongoing reported shortages in the highly popular anti-obesity medications, as well as insurance denials and high costs, are among the leading obstacles, for adolescents and adults alike.
Dr. Vidmar noted that key strategies at her center, Children’s Hospital Los Angeles, have been essential, however, in helping at least facilitate the authorization process.
The center’s approach began with contacting all the payers the center has contracts with to determine which of their policies cover these medications for adults and pediatrics and which agents are covered.
“This took work on the front end, but it was worth it because it helped us understand the framework for what we were going to go up against every time that we prescribed these medications,” she said.
Furthermore, the center’s specialty pharmacy set up contracts to be able to provide the drugs within the institution.
While the strategy can’t entirely mitigate the ongoing distribution concerns, “our pharmacy is now able to share with our weight management program what GLP-1s are available so that we can be more efficient in our work,” Dr. Vidmar said.
The center also created a list of contacts to provide to patients and their families, detailing local pharmacies that were most likely to have the medications.
Another strategy Dr. Vidmar’s center has utilized to allow the timely implementation of a GLP-1 treatment plan while awaiting a drug to become available is to create an alternative protocol, for instance, using liraglutide when awaiting semaglutide.
“If we are unable to get the lower doses of a weekly agent for titration, we have a standard protocol to bridge instead with liraglutide, and our patients, pharmacies, and even our authorizations are aware of the protocol,” Dr. Vidmar said.
“We often do not have a lot of control or agency over the distribution concerns; however, we can be thoughtful within our programs about how we titrate patients up to their full doses,” Dr. Vidmar said.
Mitigating Side Effects
When the medications are available, the common gastrointestinal (GI) side effects of nausea, vomiting, and diarrhea of the once-weekly injections are well-known, and these side effects can affect quality of life and daily function, Dr. Vidmar noted.
“We have to acknowledge that the seminal trials of these agents showed that nausea and vomiting occur in more than half of young people who take these agents during the initial titration period, and while the side effects are tolerated by many, they can be disruptive to daily life,” she said.
Encouragingly, “we also do know that for the majority of patients, those effects improve over time, and for many, they can be mitigated with nutrition changes.”
Dr. Vidmar shared a handout her center issues with key recommendations for mitigating GI effects in youth. These include:
- Eat smaller meals and eat slower
- Eat about half of what you usually eat
- Take about 15-20 minutes to eat your meal
- Aim for 60 g of protein per day
- Add fruits, vegetables, whole grains, and lean proteins to meals
- Limit foods that are spicy, greasy, or fried
- Drink water instead of sweet drinks
Consider Zofran as needed during the titration period for GI symptoms. “We’ve started using this at our institution and are teaching patients how to use it; it can really help mitigate any ER visits when there is any vomiting by educating patients and families and providing appropriate expectations, and that has been very helpful,” Dr. Vidmar said.
Regarding the GI effects, Dr. Vidmar noted she has observed that tirzepatide use (though still off-label) in youths “tends to have milder GI side effects among younger people.”
Mood Concerns?
Another concern that has emerged in public discussion regarding side effects is that of possible mood and suicidal ideation, raising concerns for adults and adolescents alike.
Upon investigating the reports, the FDA, in a statement, offered cautious reassurance that their review, including reports and clinical trials, “did not find an association between use of GLP-1 RAs and the occurrence of suicidal thoughts or actions.”
Noting that the agency is continuing to look into the issue, however, the FDA recommends that “healthcare professionals should monitor for and advise patients using GLP-1 RAs to report new or worsening depression, suicidal thoughts, or any unusual changes in mood or behavior.”
Concurrent Psychiatric Pharmacotherapy
Meanwhile, with weight gain a known and often challenging side effect of various psychiatric drugs, particularly in younger patients, obesity treatment of adolescents may commonly involve patients who are also being treated with those therapies.
Key culprits include certain antidepressants and antipsychotic medications, such as tricyclic antidepressants, and second-generation antipsychotics, such as olanzapine.
In terms of the use of GLP-1 medications for those patients, research includes a recent study of semaglutide in patients who were also being treated with antidepressants.
The study, a post hoc analysis of the STEP trials, showed “clinically meaningful weight loss regardless of baseline antidepressant use, with an adverse event profile consistent with previous studies.”
First author Robert F. Kushner, MD, said the study offers “reassurance that individuals who are taking antidepressant medications have a similar weight loss response and side-effect profile compared to individuals who are not taking these medications.”
Dr. Kushner, a professor of medicine and medicine education at Northwestern University in Chicago, and his team have not evaluated the safety profile for concomitant use with antipsychotic drugs. However, he noted that “there are studies showing that the daily GLP-1 drug liraglutide has been shown to be useful in combating antipsychotic-induced weight gain.”
“Similar studies will need to be conducted for the more effective agents, semaglutide and tirzepatide,” he said.
To counter the weight gain effects of antispychotics, metformin has long been a standard recommendation, and Dr. Vidmar noted that “I have historically always used metformin in this setting and found it very effective.”
However, the newer anti-obesity medications could prove to be important in those cases, Dr. Vidmar added.
“I do think and predict that GLP-1 agonists will be as effective, if not more, in combating the weight gain-promoting effects of these agents and act as a nice adjuvant to this treatment paradigm for psychiatrists.”
Dr. Vidmar has participated in an advisory board for Rhythm Pharmaceuticals. Dr. Kushner is on the advisory boards for Novo Nordisk, Weight Watchers, Lilly, Boehringer Ingelheim, and Altimmune.
A version of this article appeared on Medscape.com.
DENVER — The ability to provide adolescents with highly effective anti-obesity medications that now carry approvals from the US Food and Drug Administration (FDA) and support in guidelines offers reassurance of their use; however, a reality check often awaits for clinicians in terms of challenges ranging from accessing and affording the medications to managing real and rumored side effects.
Weighing in on the issues, experts at Obesity Medicine (OMA) 2024 offered some key strategies and practice hacks for overcoming those hurdles.
The incentive to provide treatment with popular glucagon-like peptide 1 (GLP-1) drugs such as semaglutide or the dual glucose-dependent insulinotropic peptide (GIP) GLP-1 tirzepatide lies in the evidence that their high efficacy in promoting weight loss, and hence preventing metabolic syndrome, has benefits that far outweigh the potential side effects, said Alaina Vidmar, MD, in presenting at the meeting.
“We can look at all the evidence and without question acknowledge that the GLP-1s/GIP agonists are the most effective agents that we currently have, with the least heterogeneity in response, and the most high responders compared with other agents,” said Dr. Vidmar, an assistant professor of clinical pediatrics at the Keck School of Medicine of University of Southern California and director of obesity medicine and bariatric surgery at Children’s Hospital Los Angeles.
The strength of the evidence is reflected in the landmark American Academy of Pediatrics (AAP) Clinical Practice Guideline for the Evaluation and Treatment of Children and Adolescents With Obesity, which recommends that “pediatricians and other primary healthcare providers should offer adolescents 12 years and older with obesity weight loss pharmacotherapy, according to medication indications, risks and may offer adolescents 8 years old with obesity weight loss pharmacotherapy, according to medication indications, risks.”
The AAP guidance echoes the recommendations of the drug makers and FDA that “a combination of specific behavioral techniques within the context of family-based behavioral treatment and the use of pharmacotherapy may be necessary to prevent life-limiting complications over time.”
However, in real-world practice, with the various challenges in providing that intensive, comprehensive care, clinicians should be prepared to get creative: “We sometimes have to do the best we can with what we have because the watchful waiting approach is not effective and leads to more harm than good,” Dr. Vidmar said.
Facilitating Access
The ongoing reported shortages in the highly popular anti-obesity medications, as well as insurance denials and high costs, are among the leading obstacles, for adolescents and adults alike.
Dr. Vidmar noted that key strategies at her center, Children’s Hospital Los Angeles, have been essential, however, in helping at least facilitate the authorization process.
The center’s approach began with contacting all the payers the center has contracts with to determine which of their policies cover these medications for adults and pediatrics and which agents are covered.
“This took work on the front end, but it was worth it because it helped us understand the framework for what we were going to go up against every time that we prescribed these medications,” she said.
Furthermore, the center’s specialty pharmacy set up contracts to be able to provide the drugs within the institution.
While the strategy can’t entirely mitigate the ongoing distribution concerns, “our pharmacy is now able to share with our weight management program what GLP-1s are available so that we can be more efficient in our work,” Dr. Vidmar said.
The center also created a list of contacts to provide to patients and their families, detailing local pharmacies that were most likely to have the medications.
Another strategy Dr. Vidmar’s center has utilized to allow the timely implementation of a GLP-1 treatment plan while awaiting a drug to become available is to create an alternative protocol, for instance, using liraglutide when awaiting semaglutide.
“If we are unable to get the lower doses of a weekly agent for titration, we have a standard protocol to bridge instead with liraglutide, and our patients, pharmacies, and even our authorizations are aware of the protocol,” Dr. Vidmar said.
“We often do not have a lot of control or agency over the distribution concerns; however, we can be thoughtful within our programs about how we titrate patients up to their full doses,” Dr. Vidmar said.
Mitigating Side Effects
When the medications are available, the common gastrointestinal (GI) side effects of nausea, vomiting, and diarrhea of the once-weekly injections are well-known, and these side effects can affect quality of life and daily function, Dr. Vidmar noted.
“We have to acknowledge that the seminal trials of these agents showed that nausea and vomiting occur in more than half of young people who take these agents during the initial titration period, and while the side effects are tolerated by many, they can be disruptive to daily life,” she said.
Encouragingly, “we also do know that for the majority of patients, those effects improve over time, and for many, they can be mitigated with nutrition changes.”
Dr. Vidmar shared a handout her center issues with key recommendations for mitigating GI effects in youth. These include:
- Eat smaller meals and eat slower
- Eat about half of what you usually eat
- Take about 15-20 minutes to eat your meal
- Aim for 60 g of protein per day
- Add fruits, vegetables, whole grains, and lean proteins to meals
- Limit foods that are spicy, greasy, or fried
- Drink water instead of sweet drinks
Consider Zofran as needed during the titration period for GI symptoms. “We’ve started using this at our institution and are teaching patients how to use it; it can really help mitigate any ER visits when there is any vomiting by educating patients and families and providing appropriate expectations, and that has been very helpful,” Dr. Vidmar said.
Regarding the GI effects, Dr. Vidmar noted she has observed that tirzepatide use (though still off-label) in youths “tends to have milder GI side effects among younger people.”
Mood Concerns?
Another concern that has emerged in public discussion regarding side effects is that of possible mood and suicidal ideation, raising concerns for adults and adolescents alike.
Upon investigating the reports, the FDA, in a statement, offered cautious reassurance that their review, including reports and clinical trials, “did not find an association between use of GLP-1 RAs and the occurrence of suicidal thoughts or actions.”
Noting that the agency is continuing to look into the issue, however, the FDA recommends that “healthcare professionals should monitor for and advise patients using GLP-1 RAs to report new or worsening depression, suicidal thoughts, or any unusual changes in mood or behavior.”
Concurrent Psychiatric Pharmacotherapy
Meanwhile, with weight gain a known and often challenging side effect of various psychiatric drugs, particularly in younger patients, obesity treatment of adolescents may commonly involve patients who are also being treated with those therapies.
Key culprits include certain antidepressants and antipsychotic medications, such as tricyclic antidepressants, and second-generation antipsychotics, such as olanzapine.
In terms of the use of GLP-1 medications for those patients, research includes a recent study of semaglutide in patients who were also being treated with antidepressants.
The study, a post hoc analysis of the STEP trials, showed “clinically meaningful weight loss regardless of baseline antidepressant use, with an adverse event profile consistent with previous studies.”
First author Robert F. Kushner, MD, said the study offers “reassurance that individuals who are taking antidepressant medications have a similar weight loss response and side-effect profile compared to individuals who are not taking these medications.”
Dr. Kushner, a professor of medicine and medicine education at Northwestern University in Chicago, and his team have not evaluated the safety profile for concomitant use with antipsychotic drugs. However, he noted that “there are studies showing that the daily GLP-1 drug liraglutide has been shown to be useful in combating antipsychotic-induced weight gain.”
“Similar studies will need to be conducted for the more effective agents, semaglutide and tirzepatide,” he said.
To counter the weight gain effects of antispychotics, metformin has long been a standard recommendation, and Dr. Vidmar noted that “I have historically always used metformin in this setting and found it very effective.”
However, the newer anti-obesity medications could prove to be important in those cases, Dr. Vidmar added.
“I do think and predict that GLP-1 agonists will be as effective, if not more, in combating the weight gain-promoting effects of these agents and act as a nice adjuvant to this treatment paradigm for psychiatrists.”
Dr. Vidmar has participated in an advisory board for Rhythm Pharmaceuticals. Dr. Kushner is on the advisory boards for Novo Nordisk, Weight Watchers, Lilly, Boehringer Ingelheim, and Altimmune.
A version of this article appeared on Medscape.com.
DENVER — The ability to provide adolescents with highly effective anti-obesity medications that now carry approvals from the US Food and Drug Administration (FDA) and support in guidelines offers reassurance of their use; however, a reality check often awaits for clinicians in terms of challenges ranging from accessing and affording the medications to managing real and rumored side effects.
Weighing in on the issues, experts at Obesity Medicine (OMA) 2024 offered some key strategies and practice hacks for overcoming those hurdles.
The incentive to provide treatment with popular glucagon-like peptide 1 (GLP-1) drugs such as semaglutide or the dual glucose-dependent insulinotropic peptide (GIP) GLP-1 tirzepatide lies in the evidence that their high efficacy in promoting weight loss, and hence preventing metabolic syndrome, has benefits that far outweigh the potential side effects, said Alaina Vidmar, MD, in presenting at the meeting.
“We can look at all the evidence and without question acknowledge that the GLP-1s/GIP agonists are the most effective agents that we currently have, with the least heterogeneity in response, and the most high responders compared with other agents,” said Dr. Vidmar, an assistant professor of clinical pediatrics at the Keck School of Medicine of University of Southern California and director of obesity medicine and bariatric surgery at Children’s Hospital Los Angeles.
The strength of the evidence is reflected in the landmark American Academy of Pediatrics (AAP) Clinical Practice Guideline for the Evaluation and Treatment of Children and Adolescents With Obesity, which recommends that “pediatricians and other primary healthcare providers should offer adolescents 12 years and older with obesity weight loss pharmacotherapy, according to medication indications, risks and may offer adolescents 8 years old with obesity weight loss pharmacotherapy, according to medication indications, risks.”
The AAP guidance echoes the recommendations of the drug makers and FDA that “a combination of specific behavioral techniques within the context of family-based behavioral treatment and the use of pharmacotherapy may be necessary to prevent life-limiting complications over time.”
However, in real-world practice, with the various challenges in providing that intensive, comprehensive care, clinicians should be prepared to get creative: “We sometimes have to do the best we can with what we have because the watchful waiting approach is not effective and leads to more harm than good,” Dr. Vidmar said.
Facilitating Access
The ongoing reported shortages in the highly popular anti-obesity medications, as well as insurance denials and high costs, are among the leading obstacles, for adolescents and adults alike.
Dr. Vidmar noted that key strategies at her center, Children’s Hospital Los Angeles, have been essential, however, in helping at least facilitate the authorization process.
The center’s approach began with contacting all the payers the center has contracts with to determine which of their policies cover these medications for adults and pediatrics and which agents are covered.
“This took work on the front end, but it was worth it because it helped us understand the framework for what we were going to go up against every time that we prescribed these medications,” she said.
Furthermore, the center’s specialty pharmacy set up contracts to be able to provide the drugs within the institution.
While the strategy can’t entirely mitigate the ongoing distribution concerns, “our pharmacy is now able to share with our weight management program what GLP-1s are available so that we can be more efficient in our work,” Dr. Vidmar said.
The center also created a list of contacts to provide to patients and their families, detailing local pharmacies that were most likely to have the medications.
Another strategy Dr. Vidmar’s center has utilized to allow the timely implementation of a GLP-1 treatment plan while awaiting a drug to become available is to create an alternative protocol, for instance, using liraglutide when awaiting semaglutide.
“If we are unable to get the lower doses of a weekly agent for titration, we have a standard protocol to bridge instead with liraglutide, and our patients, pharmacies, and even our authorizations are aware of the protocol,” Dr. Vidmar said.
“We often do not have a lot of control or agency over the distribution concerns; however, we can be thoughtful within our programs about how we titrate patients up to their full doses,” Dr. Vidmar said.
Mitigating Side Effects
When the medications are available, the common gastrointestinal (GI) side effects of nausea, vomiting, and diarrhea of the once-weekly injections are well-known, and these side effects can affect quality of life and daily function, Dr. Vidmar noted.
“We have to acknowledge that the seminal trials of these agents showed that nausea and vomiting occur in more than half of young people who take these agents during the initial titration period, and while the side effects are tolerated by many, they can be disruptive to daily life,” she said.
Encouragingly, “we also do know that for the majority of patients, those effects improve over time, and for many, they can be mitigated with nutrition changes.”
Dr. Vidmar shared a handout her center issues with key recommendations for mitigating GI effects in youth. These include:
- Eat smaller meals and eat slower
- Eat about half of what you usually eat
- Take about 15-20 minutes to eat your meal
- Aim for 60 g of protein per day
- Add fruits, vegetables, whole grains, and lean proteins to meals
- Limit foods that are spicy, greasy, or fried
- Drink water instead of sweet drinks
Consider Zofran as needed during the titration period for GI symptoms. “We’ve started using this at our institution and are teaching patients how to use it; it can really help mitigate any ER visits when there is any vomiting by educating patients and families and providing appropriate expectations, and that has been very helpful,” Dr. Vidmar said.
Regarding the GI effects, Dr. Vidmar noted she has observed that tirzepatide use (though still off-label) in youths “tends to have milder GI side effects among younger people.”
Mood Concerns?
Another concern that has emerged in public discussion regarding side effects is that of possible mood and suicidal ideation, raising concerns for adults and adolescents alike.
Upon investigating the reports, the FDA, in a statement, offered cautious reassurance that their review, including reports and clinical trials, “did not find an association between use of GLP-1 RAs and the occurrence of suicidal thoughts or actions.”
Noting that the agency is continuing to look into the issue, however, the FDA recommends that “healthcare professionals should monitor for and advise patients using GLP-1 RAs to report new or worsening depression, suicidal thoughts, or any unusual changes in mood or behavior.”
Concurrent Psychiatric Pharmacotherapy
Meanwhile, with weight gain a known and often challenging side effect of various psychiatric drugs, particularly in younger patients, obesity treatment of adolescents may commonly involve patients who are also being treated with those therapies.
Key culprits include certain antidepressants and antipsychotic medications, such as tricyclic antidepressants, and second-generation antipsychotics, such as olanzapine.
In terms of the use of GLP-1 medications for those patients, research includes a recent study of semaglutide in patients who were also being treated with antidepressants.
The study, a post hoc analysis of the STEP trials, showed “clinically meaningful weight loss regardless of baseline antidepressant use, with an adverse event profile consistent with previous studies.”
First author Robert F. Kushner, MD, said the study offers “reassurance that individuals who are taking antidepressant medications have a similar weight loss response and side-effect profile compared to individuals who are not taking these medications.”
Dr. Kushner, a professor of medicine and medicine education at Northwestern University in Chicago, and his team have not evaluated the safety profile for concomitant use with antipsychotic drugs. However, he noted that “there are studies showing that the daily GLP-1 drug liraglutide has been shown to be useful in combating antipsychotic-induced weight gain.”
“Similar studies will need to be conducted for the more effective agents, semaglutide and tirzepatide,” he said.
To counter the weight gain effects of antispychotics, metformin has long been a standard recommendation, and Dr. Vidmar noted that “I have historically always used metformin in this setting and found it very effective.”
However, the newer anti-obesity medications could prove to be important in those cases, Dr. Vidmar added.
“I do think and predict that GLP-1 agonists will be as effective, if not more, in combating the weight gain-promoting effects of these agents and act as a nice adjuvant to this treatment paradigm for psychiatrists.”
Dr. Vidmar has participated in an advisory board for Rhythm Pharmaceuticals. Dr. Kushner is on the advisory boards for Novo Nordisk, Weight Watchers, Lilly, Boehringer Ingelheim, and Altimmune.
A version of this article appeared on Medscape.com.
FROM OBESITY MEDICINE 2024