User login
Optimizing Patch Testing in Clinical Practice: Insights From Amber Reck Atwater, MD
Optimizing Patch Testing in Clinical Practice: Insights From Amber Reck Atwater, MD
What evidence exists on the impact of systemic immunosuppressants, biologics, and small-molecule inhibitors on patch test sensitivity and specificity?
DR. ATWATER: Guidance on this topic recently was published by the North American Contact Dermatitis Group (NACDG) in the Journal of the American Academy of Dermatology in June 2025. The article outlined expert recommendations on whether systemic immunosuppressants, biologics, and small-molecule inhibitors should be held before patch testing, how long they should be withheld, and the maximum recommended doses that can be used during testing.
How can dermatologists perform patch testing or use alternative diagnostic strategies when systemic therapy cannot safely be withheld?
DR. ATWATER: When systemic therapy cannot safely be withheld and patch testing is needed for diagnostic purposes, I typically proceed with the understanding that there is risk of false-negative reactions. If the patient has dermatitis on systemic therapy, it suggests that an allergic response on patch testing is also possible. I generally follow the NACDG guidelines mentioned above, and I hold systemic medications during the week of testing, when possible. If the patient has diffuse dermatitis on systemic therapy and their skin is not clear enough to proceed, I prescribe a prednisone taper and patch test on 10 mg per day for the entire week of testing. In patients taking systemic medications, I typically consider doubtful (+/−) patch test reactions to be the equivalent of a positive (1+) reaction.
One alternative diagnostic strategy is to create a safe list that avoids common allergens and have the patient use only products on this list. If their skin clears with avoidance, it suggests that they may have a contact allergy, and you can proceed with patch testing.
In patients with a convincing history of contact dermatitis but a negative patch test, what are the most common causes of false negatives, and how do you distinguish those from true negatives?
DR. ATWATER: In this setting, the most common cause of a false-negative patch test is not testing the correct allergens. This may occur when too few allergens are tested or when relevant allergens are not tested. Other potential causes of false negatives are incorrect timing of allergen exposure and readings, inadequate allergen adherence, expired allergens, and testing with the incorrect vehicle or concentration of allergen. Some immunosuppressant medications also can cause a false-negative patch test. The only way to distinguish false negatives from true negatives is to be aware of these potential pitfalls and continuously work to avoid errors whenever possible.
What technical and practical factors most influence false negatives/positives, and what steps do you recommend to standardize and improve test yield?
DR. ATWATER: Not testing the correct allergens is a potential pitfall in patch testing. For example, when comparing the 35 allergens in the T.R.U.E. Test (thin layer rapid-use epicutaneous test) to the 80 allergens tested by the NACDG in 2021 to 2022, up to 48% of NACDG allergens are missed when testing with only the T.R.U.E. Test. This argues for comprehensive patch testing and testing of at least 80 to 90 allergens whenever possible. Another example is failure to test allergens relevant to occupational exposures, such as in the case of a hairdresser or nail technician. When patches are not applied for the correct period (48 hours) and the final reading isn’t completed in the recommended timeframe (96 to 168 hours), there is increased risk for false negatives and positives. Both false negatives and positives can occur if you complete your final reading too early, whereas false negatives may be more likely if you complete your final reading late. Poor allergen adherence, which can be caused by hair, sweat, poor tape application, water, and exercise, also can result in false negatives. Allergen concentration that is too low to elicit a reaction, as well as too little allergen placed into the chamber, also could increase the risk of false negatives. Too much allergen in the chamber or too high a concentration of the allergen can result in false positives.
Topical medications applied to the patch test site prior to or during patch testing, as well as phototherapy, sun exposure, intramuscular triamcinolone, immunosuppressants, biologics, and small-molecule inhibitors can suppress the immune response to allergen exposure.
To identify true positive patch test reactions, use side lighting and palpate the skin. Be aware of the appearance of irritant reactions, patch test reaction variants such as follicular reactions, and the poral reaction, which can be seen with cobalt. Strong knowledge of how to read patch test reactions will decrease your risk of false-positive and -negative reactions. Training and protocols are vital for standardization and accurate patch testing. We train our staff on the technicalities of patch testing and utilize patch test orders and checklists in our office. We take photos to confirm application sites and visually track reactions between visits. We also provide verbal and written patch test care instructions for our patients and reinforce instructions at each clinic visit.
What are your top practical tips for dermatologists to maximize diagnostic accuracy and patient safety?
DR. ATWATER: My first tip is to develop patch test protocols that are followed by staff and physicians—every time—for every patient. My second tip is to make sure you understand and are comfortable with the patch test process. There are several great patch test resources that can help, including Introduction to Patch Testing, a recently developed CME module in the AAD Learning Center (https://learning.aad.org/Listing/Introduction-to-Patch- Testing-20366). There also are patch test training courses and other resources offered by the American Contact Dermatitis Society (https://www.contactderm.org/).
What single guideline change would most improve patch testing?
DR. ATWATER: The single guideline change that would most improve the practice of patch testing is removal of payer limitations on the number of patches that can be applied per day. For many payers in the United States, this limit is 80 to 90 allergens, and it is sometimes lower. Limits on the number of allergens that can be applied per day may result in false-negative patch testing (when limits are applied), patient inconvenience (if testing is completed over 2 different application days), and insufficient reimbursement (if more allergens are tested than the limit allows).
What evidence exists on the impact of systemic immunosuppressants, biologics, and small-molecule inhibitors on patch test sensitivity and specificity?
DR. ATWATER: Guidance on this topic recently was published by the North American Contact Dermatitis Group (NACDG) in the Journal of the American Academy of Dermatology in June 2025. The article outlined expert recommendations on whether systemic immunosuppressants, biologics, and small-molecule inhibitors should be held before patch testing, how long they should be withheld, and the maximum recommended doses that can be used during testing.
How can dermatologists perform patch testing or use alternative diagnostic strategies when systemic therapy cannot safely be withheld?
DR. ATWATER: When systemic therapy cannot safely be withheld and patch testing is needed for diagnostic purposes, I typically proceed with the understanding that there is risk of false-negative reactions. If the patient has dermatitis on systemic therapy, it suggests that an allergic response on patch testing is also possible. I generally follow the NACDG guidelines mentioned above, and I hold systemic medications during the week of testing, when possible. If the patient has diffuse dermatitis on systemic therapy and their skin is not clear enough to proceed, I prescribe a prednisone taper and patch test on 10 mg per day for the entire week of testing. In patients taking systemic medications, I typically consider doubtful (+/−) patch test reactions to be the equivalent of a positive (1+) reaction.
One alternative diagnostic strategy is to create a safe list that avoids common allergens and have the patient use only products on this list. If their skin clears with avoidance, it suggests that they may have a contact allergy, and you can proceed with patch testing.
In patients with a convincing history of contact dermatitis but a negative patch test, what are the most common causes of false negatives, and how do you distinguish those from true negatives?
DR. ATWATER: In this setting, the most common cause of a false-negative patch test is not testing the correct allergens. This may occur when too few allergens are tested or when relevant allergens are not tested. Other potential causes of false negatives are incorrect timing of allergen exposure and readings, inadequate allergen adherence, expired allergens, and testing with the incorrect vehicle or concentration of allergen. Some immunosuppressant medications also can cause a false-negative patch test. The only way to distinguish false negatives from true negatives is to be aware of these potential pitfalls and continuously work to avoid errors whenever possible.
What technical and practical factors most influence false negatives/positives, and what steps do you recommend to standardize and improve test yield?
DR. ATWATER: Not testing the correct allergens is a potential pitfall in patch testing. For example, when comparing the 35 allergens in the T.R.U.E. Test (thin layer rapid-use epicutaneous test) to the 80 allergens tested by the NACDG in 2021 to 2022, up to 48% of NACDG allergens are missed when testing with only the T.R.U.E. Test. This argues for comprehensive patch testing and testing of at least 80 to 90 allergens whenever possible. Another example is failure to test allergens relevant to occupational exposures, such as in the case of a hairdresser or nail technician. When patches are not applied for the correct period (48 hours) and the final reading isn’t completed in the recommended timeframe (96 to 168 hours), there is increased risk for false negatives and positives. Both false negatives and positives can occur if you complete your final reading too early, whereas false negatives may be more likely if you complete your final reading late. Poor allergen adherence, which can be caused by hair, sweat, poor tape application, water, and exercise, also can result in false negatives. Allergen concentration that is too low to elicit a reaction, as well as too little allergen placed into the chamber, also could increase the risk of false negatives. Too much allergen in the chamber or too high a concentration of the allergen can result in false positives.
Topical medications applied to the patch test site prior to or during patch testing, as well as phototherapy, sun exposure, intramuscular triamcinolone, immunosuppressants, biologics, and small-molecule inhibitors can suppress the immune response to allergen exposure.
To identify true positive patch test reactions, use side lighting and palpate the skin. Be aware of the appearance of irritant reactions, patch test reaction variants such as follicular reactions, and the poral reaction, which can be seen with cobalt. Strong knowledge of how to read patch test reactions will decrease your risk of false-positive and -negative reactions. Training and protocols are vital for standardization and accurate patch testing. We train our staff on the technicalities of patch testing and utilize patch test orders and checklists in our office. We take photos to confirm application sites and visually track reactions between visits. We also provide verbal and written patch test care instructions for our patients and reinforce instructions at each clinic visit.
What are your top practical tips for dermatologists to maximize diagnostic accuracy and patient safety?
DR. ATWATER: My first tip is to develop patch test protocols that are followed by staff and physicians—every time—for every patient. My second tip is to make sure you understand and are comfortable with the patch test process. There are several great patch test resources that can help, including Introduction to Patch Testing, a recently developed CME module in the AAD Learning Center (https://learning.aad.org/Listing/Introduction-to-Patch- Testing-20366). There also are patch test training courses and other resources offered by the American Contact Dermatitis Society (https://www.contactderm.org/).
What single guideline change would most improve patch testing?
DR. ATWATER: The single guideline change that would most improve the practice of patch testing is removal of payer limitations on the number of patches that can be applied per day. For many payers in the United States, this limit is 80 to 90 allergens, and it is sometimes lower. Limits on the number of allergens that can be applied per day may result in false-negative patch testing (when limits are applied), patient inconvenience (if testing is completed over 2 different application days), and insufficient reimbursement (if more allergens are tested than the limit allows).
What evidence exists on the impact of systemic immunosuppressants, biologics, and small-molecule inhibitors on patch test sensitivity and specificity?
DR. ATWATER: Guidance on this topic recently was published by the North American Contact Dermatitis Group (NACDG) in the Journal of the American Academy of Dermatology in June 2025. The article outlined expert recommendations on whether systemic immunosuppressants, biologics, and small-molecule inhibitors should be held before patch testing, how long they should be withheld, and the maximum recommended doses that can be used during testing.
How can dermatologists perform patch testing or use alternative diagnostic strategies when systemic therapy cannot safely be withheld?
DR. ATWATER: When systemic therapy cannot safely be withheld and patch testing is needed for diagnostic purposes, I typically proceed with the understanding that there is risk of false-negative reactions. If the patient has dermatitis on systemic therapy, it suggests that an allergic response on patch testing is also possible. I generally follow the NACDG guidelines mentioned above, and I hold systemic medications during the week of testing, when possible. If the patient has diffuse dermatitis on systemic therapy and their skin is not clear enough to proceed, I prescribe a prednisone taper and patch test on 10 mg per day for the entire week of testing. In patients taking systemic medications, I typically consider doubtful (+/−) patch test reactions to be the equivalent of a positive (1+) reaction.
One alternative diagnostic strategy is to create a safe list that avoids common allergens and have the patient use only products on this list. If their skin clears with avoidance, it suggests that they may have a contact allergy, and you can proceed with patch testing.
In patients with a convincing history of contact dermatitis but a negative patch test, what are the most common causes of false negatives, and how do you distinguish those from true negatives?
DR. ATWATER: In this setting, the most common cause of a false-negative patch test is not testing the correct allergens. This may occur when too few allergens are tested or when relevant allergens are not tested. Other potential causes of false negatives are incorrect timing of allergen exposure and readings, inadequate allergen adherence, expired allergens, and testing with the incorrect vehicle or concentration of allergen. Some immunosuppressant medications also can cause a false-negative patch test. The only way to distinguish false negatives from true negatives is to be aware of these potential pitfalls and continuously work to avoid errors whenever possible.
What technical and practical factors most influence false negatives/positives, and what steps do you recommend to standardize and improve test yield?
DR. ATWATER: Not testing the correct allergens is a potential pitfall in patch testing. For example, when comparing the 35 allergens in the T.R.U.E. Test (thin layer rapid-use epicutaneous test) to the 80 allergens tested by the NACDG in 2021 to 2022, up to 48% of NACDG allergens are missed when testing with only the T.R.U.E. Test. This argues for comprehensive patch testing and testing of at least 80 to 90 allergens whenever possible. Another example is failure to test allergens relevant to occupational exposures, such as in the case of a hairdresser or nail technician. When patches are not applied for the correct period (48 hours) and the final reading isn’t completed in the recommended timeframe (96 to 168 hours), there is increased risk for false negatives and positives. Both false negatives and positives can occur if you complete your final reading too early, whereas false negatives may be more likely if you complete your final reading late. Poor allergen adherence, which can be caused by hair, sweat, poor tape application, water, and exercise, also can result in false negatives. Allergen concentration that is too low to elicit a reaction, as well as too little allergen placed into the chamber, also could increase the risk of false negatives. Too much allergen in the chamber or too high a concentration of the allergen can result in false positives.
Topical medications applied to the patch test site prior to or during patch testing, as well as phototherapy, sun exposure, intramuscular triamcinolone, immunosuppressants, biologics, and small-molecule inhibitors can suppress the immune response to allergen exposure.
To identify true positive patch test reactions, use side lighting and palpate the skin. Be aware of the appearance of irritant reactions, patch test reaction variants such as follicular reactions, and the poral reaction, which can be seen with cobalt. Strong knowledge of how to read patch test reactions will decrease your risk of false-positive and -negative reactions. Training and protocols are vital for standardization and accurate patch testing. We train our staff on the technicalities of patch testing and utilize patch test orders and checklists in our office. We take photos to confirm application sites and visually track reactions between visits. We also provide verbal and written patch test care instructions for our patients and reinforce instructions at each clinic visit.
What are your top practical tips for dermatologists to maximize diagnostic accuracy and patient safety?
DR. ATWATER: My first tip is to develop patch test protocols that are followed by staff and physicians—every time—for every patient. My second tip is to make sure you understand and are comfortable with the patch test process. There are several great patch test resources that can help, including Introduction to Patch Testing, a recently developed CME module in the AAD Learning Center (https://learning.aad.org/Listing/Introduction-to-Patch- Testing-20366). There also are patch test training courses and other resources offered by the American Contact Dermatitis Society (https://www.contactderm.org/).
What single guideline change would most improve patch testing?
DR. ATWATER: The single guideline change that would most improve the practice of patch testing is removal of payer limitations on the number of patches that can be applied per day. For many payers in the United States, this limit is 80 to 90 allergens, and it is sometimes lower. Limits on the number of allergens that can be applied per day may result in false-negative patch testing (when limits are applied), patient inconvenience (if testing is completed over 2 different application days), and insufficient reimbursement (if more allergens are tested than the limit allows).
Optimizing Patch Testing in Clinical Practice: Insights From Amber Reck Atwater, MD
Optimizing Patch Testing in Clinical Practice: Insights From Amber Reck Atwater, MD

Dupilumab for Bullous Pemphigoid: To Treat or Not to Treat?
Dupilumab for Bullous Pemphigoid: To Treat or Not to Treat?
Bullous pemphigoid (BP) is a chronic autoimmune skin condition characterized by large, fluid-filled blisters (bullae) on the skin. There usually is severe itching, which may antedate the bullae by several weeks. Bullous pemphigoid most commonly affects adults aged 60 years and older with comorbidities such as metabolic syndrome or other autoimmune diseases. The typical blistering is subepidermal, and its occurrence seems to be driven by autoantibodies targeting the epidermal basement membrane zone.
Conventional treatment for BP has long included systemic corticosteroids and immunosuppressants; this combination of drugs effectively controls inflammation but also is associated with considerable risks such as infection, hyperglycemia with worsening diabetes, hypertension, osteoporosis and fracture risk, and delirium, particularly in older patients. Recent developments in biologic therapy have supported the utilization of potentially safer alternatives. Specifically, dupilumab has demonstrated efficacy in the treatment of atopic dermatitis. Case reports and small research studies included in a recent review have suggested that dupilumab could be effective in managing BP, potentially offering a safer treatment option.1 Importantly, dupilumab recently was approved for BP by the US Food and Drug Administration, making it the first biologic approved for treating this condition.2 In this article, we discuss dupilumab as an option for clinicians to prescribe as an initial therapy for BP.
Pathophysiology of Bullous Pemphigoid and Dupilumab
Bullous pemphigoid pathophysiology is driven by 2 main components: immunologic and inflammatory processes. The immune-mediated attack consists of autoantibodies against the hemidesmosomal proteins BP180 and BP230 in the basement membrane zone, which anchor the epidermis to the dermis.1 When these proteins are targeted, a cascade of responses is triggered, including the release of inflammatory cells, particularly eosinophils and neutrophils, into the skin. These cells release inflammatory mediators that break down the basement membrane, resulting in the separation of the epidermis from the dermis and leading to subepidermal blister formation.
The inflammation associated with BP largely is driven by a T helper 2–dominant immune response, with increased levels of cytokines such as interleukin (IL) 4 and IL-13.1 The chronic inflammation contributes to the characteristic blisters and intense pruritus seen in patients with BP. Traditional treatments such as corticosteroids work broadly to suppress this inflammation by reducing the production of all proinflammatory cytokines; however, they lack specificity, which dampens the targeted immune response against BP and broadly suppresses the immune system, increasing the risk for infection and other adverse effects. For older patients with multiple health conditions, these adverse effects can impact quality of life and pose health risks.
Interleukin 4 and IL-13 contribute to eosinophilia by upregulating the expression of eosinophil chemoattractant cytokines that promote eosinophil migration and adhesion.1 This is where dupilumab presents a promising alternative. Dupilumab is a monoclonal antibody that selectively targets the key cytokines implicated in BP. It binds to the IL-4 receptor alpha subunit, which IL-4 and IL-13 share, thereby inhibiting the signaling of both cytokines.1
Dupilumab Reports and Case Series
Current evidence supporting the use of dupilumab for BP consists primarily of case series and uncontrolled clinical observations, both of which are useful to formulate but not to test hypotheses.3 One case series of 13 patients diagnosed with BP reported that 92.3% (12/13) of patients achieved disease clearance or satisfactory control, with 53.8% (7/13) achieving total lesion clearance and no adverse events observed.4 In a larger case series, 87.0% of 146 patients achieved disease control with an initial dose of dupilumab 600 mg followed by 300 mg every 2 weeks for 4 weeks, though the study also looked at secondary outcomes for up to 64 weeks.5 Both these findings are compatible with the idea that dupilumab has efficacy in BP, but they cannot be used to test hypotheses.3,4
In a single case report of refractory BP, the combination of dupilumab and omalizumab—a monoclonal antibody that blocks the binding of IgE to mast cells, basophils, and dendritic cells—has shown efficacy, particularly when BP is unresponsive to standard therapies.6 The case involved a 72-year-old woman with unresponsive BP who was treated with a combination of dupilumab and omalizumab. She experienced marked improvement in pruritus and bullae accompanied by normalization of anti-BP180 autoantibody levels. This result points to the possibility that IL-4 and IL-13 blockade could influence autoantibody production. The authors attributed the reduction in pruritus to dupilumab, although the drug was administered in combination with omalizumab.6
Small Randomized Trial of Dupilumab
In addition to these uncontrolled clinical observations, dupilumab recently demonstrated positive results in a small randomized trial.7 Patients who were assigned to receive dupilumab were 5 times more likely to achieve sustained remission compared to those assigned to a placebo. All randomized patients also were treated with a standard-of-care oral corticosteroid regimen, which complicated the ability to isolate the specific effects of dupilumab.7 Finally, a completed totality of evidence on the prescription of dupilumab for refractory BP should include more reliable results from larger randomized trials.8
Final Thoughts
Dupilumab is now approved by the US Food and Drug Administration for the treatment of BP, marking an important milestone as the first targeted biologic therapy for this condition. While the totality of evidence is still evolving, the available data indicate both efficacy and a favorable safety profile when compared to traditional corticosteroids and immunosuppressants. Based on the available data, we suggest that health care providers consider dupilumab as a first-line monotherapy in appropriate patients with BP without specific contraindications, particularly as a practical and safe alternative to corticosteroids and immunosuppressive therapies in older adults with comorbidities. If the patient demonstrates clinical improvement in symptom relief, the therapy can be continued. This strategy minimizes initial exposure to more potent biologics or therapies with higher toxicity profiles. For patients without adequate disease control or with severe initial presentations requiring rapid improvement, clinicians may consider escalation to adjunctive or alternative therapies, such as rituximab, omalizumab, or a short course of systemic corticosteroids for acute management.
Emerging data suggest that dupilumab is a promising therapy for BP. We suggest that it may be a safer targeted alternative to traditional corticosteroids and immunosuppressive therapies. The ability of dupilumab to mitigate inflammation without broadly suppressing the immune system suggests that it may turn out to be an especially valuable option for older patients and those with comorbid conditions.
Acknowledgement—The authors thank Jodi Fiedler, MD (Boca Raton, FL), for her expert advice and assistance.
- Zhang L, Chen Z, Wang L, et al. Bullous pemphigoid: the role of type 2 inflammation in its pathogenesis and the prospect of targeted therapy. Front Immunol. 2023;14:1115083. doi:10.3389/fimmu.2023.1115083
- Sanofi. Dupixent approved in the US as the only targeted medicine to treat patients with bullous pemphigoid. News release. June 20, 2025. Accessed September 8, 2025. https://www.sanofi.com/en/media-room/press-releases/2025/2025-06-20-05-00-00-3102518
- Hennekens CH, DeMets D. Statistical association and causation: contributions of different types of evidence. JAMA. 2011;306:1134-1136. doi:10.1001/jama.2011.322
- Abdat R, Waldman RA, de Bedout V, et al. Dupilumab as a novel therapy for bullous pemphigoid: a multicenter case series. J Am Acad Dermatol. 2020;83:46-52. doi:10.1016/j.jaad.2020.01.089
- Zhao L, Wang Q, Liang G, et al. Evaluation of dupilumab in patients with bullous pemphigoid. JAMA Dermatol. 2023;159:953-960. doi:10.1001/jamadermatol.2023.2428
- Seyed Jafari SM, Feldmeyer L, Bossart S, et al. Case report: combination of omalizumab and dupilumab for recalcitrant bullous pemphigoid. Front Immunol. 2021;11:611549. doi:10.3389/fimmu.2020.611549
- US National Library of Medicine. A multicenter, randomized, double-blind, placebo-controlled, parallel-group study to evaluate the efficacy and safety of dupilumab in adult patients with bullous pemphigoid. ClinicalTrials.gov. Published 2019. Accessed March 10, 2026. https://clinicaltrials.gov/ct2/show/NCT04206553
- Hennekens CH, DeMets D. The need for large scale randomized evidence without undue emphasis on small trials, meta-analyses or subgroup analyses. JAMA. 2009;302:2361-2362. doi:10.1001/jama.2009.1829
Bullous pemphigoid (BP) is a chronic autoimmune skin condition characterized by large, fluid-filled blisters (bullae) on the skin. There usually is severe itching, which may antedate the bullae by several weeks. Bullous pemphigoid most commonly affects adults aged 60 years and older with comorbidities such as metabolic syndrome or other autoimmune diseases. The typical blistering is subepidermal, and its occurrence seems to be driven by autoantibodies targeting the epidermal basement membrane zone.
Conventional treatment for BP has long included systemic corticosteroids and immunosuppressants; this combination of drugs effectively controls inflammation but also is associated with considerable risks such as infection, hyperglycemia with worsening diabetes, hypertension, osteoporosis and fracture risk, and delirium, particularly in older patients. Recent developments in biologic therapy have supported the utilization of potentially safer alternatives. Specifically, dupilumab has demonstrated efficacy in the treatment of atopic dermatitis. Case reports and small research studies included in a recent review have suggested that dupilumab could be effective in managing BP, potentially offering a safer treatment option.1 Importantly, dupilumab recently was approved for BP by the US Food and Drug Administration, making it the first biologic approved for treating this condition.2 In this article, we discuss dupilumab as an option for clinicians to prescribe as an initial therapy for BP.
Pathophysiology of Bullous Pemphigoid and Dupilumab
Bullous pemphigoid pathophysiology is driven by 2 main components: immunologic and inflammatory processes. The immune-mediated attack consists of autoantibodies against the hemidesmosomal proteins BP180 and BP230 in the basement membrane zone, which anchor the epidermis to the dermis.1 When these proteins are targeted, a cascade of responses is triggered, including the release of inflammatory cells, particularly eosinophils and neutrophils, into the skin. These cells release inflammatory mediators that break down the basement membrane, resulting in the separation of the epidermis from the dermis and leading to subepidermal blister formation.
The inflammation associated with BP largely is driven by a T helper 2–dominant immune response, with increased levels of cytokines such as interleukin (IL) 4 and IL-13.1 The chronic inflammation contributes to the characteristic blisters and intense pruritus seen in patients with BP. Traditional treatments such as corticosteroids work broadly to suppress this inflammation by reducing the production of all proinflammatory cytokines; however, they lack specificity, which dampens the targeted immune response against BP and broadly suppresses the immune system, increasing the risk for infection and other adverse effects. For older patients with multiple health conditions, these adverse effects can impact quality of life and pose health risks.
Interleukin 4 and IL-13 contribute to eosinophilia by upregulating the expression of eosinophil chemoattractant cytokines that promote eosinophil migration and adhesion.1 This is where dupilumab presents a promising alternative. Dupilumab is a monoclonal antibody that selectively targets the key cytokines implicated in BP. It binds to the IL-4 receptor alpha subunit, which IL-4 and IL-13 share, thereby inhibiting the signaling of both cytokines.1
Dupilumab Reports and Case Series
Current evidence supporting the use of dupilumab for BP consists primarily of case series and uncontrolled clinical observations, both of which are useful to formulate but not to test hypotheses.3 One case series of 13 patients diagnosed with BP reported that 92.3% (12/13) of patients achieved disease clearance or satisfactory control, with 53.8% (7/13) achieving total lesion clearance and no adverse events observed.4 In a larger case series, 87.0% of 146 patients achieved disease control with an initial dose of dupilumab 600 mg followed by 300 mg every 2 weeks for 4 weeks, though the study also looked at secondary outcomes for up to 64 weeks.5 Both these findings are compatible with the idea that dupilumab has efficacy in BP, but they cannot be used to test hypotheses.3,4
In a single case report of refractory BP, the combination of dupilumab and omalizumab—a monoclonal antibody that blocks the binding of IgE to mast cells, basophils, and dendritic cells—has shown efficacy, particularly when BP is unresponsive to standard therapies.6 The case involved a 72-year-old woman with unresponsive BP who was treated with a combination of dupilumab and omalizumab. She experienced marked improvement in pruritus and bullae accompanied by normalization of anti-BP180 autoantibody levels. This result points to the possibility that IL-4 and IL-13 blockade could influence autoantibody production. The authors attributed the reduction in pruritus to dupilumab, although the drug was administered in combination with omalizumab.6
Small Randomized Trial of Dupilumab
In addition to these uncontrolled clinical observations, dupilumab recently demonstrated positive results in a small randomized trial.7 Patients who were assigned to receive dupilumab were 5 times more likely to achieve sustained remission compared to those assigned to a placebo. All randomized patients also were treated with a standard-of-care oral corticosteroid regimen, which complicated the ability to isolate the specific effects of dupilumab.7 Finally, a completed totality of evidence on the prescription of dupilumab for refractory BP should include more reliable results from larger randomized trials.8
Final Thoughts
Dupilumab is now approved by the US Food and Drug Administration for the treatment of BP, marking an important milestone as the first targeted biologic therapy for this condition. While the totality of evidence is still evolving, the available data indicate both efficacy and a favorable safety profile when compared to traditional corticosteroids and immunosuppressants. Based on the available data, we suggest that health care providers consider dupilumab as a first-line monotherapy in appropriate patients with BP without specific contraindications, particularly as a practical and safe alternative to corticosteroids and immunosuppressive therapies in older adults with comorbidities. If the patient demonstrates clinical improvement in symptom relief, the therapy can be continued. This strategy minimizes initial exposure to more potent biologics or therapies with higher toxicity profiles. For patients without adequate disease control or with severe initial presentations requiring rapid improvement, clinicians may consider escalation to adjunctive or alternative therapies, such as rituximab, omalizumab, or a short course of systemic corticosteroids for acute management.
Emerging data suggest that dupilumab is a promising therapy for BP. We suggest that it may be a safer targeted alternative to traditional corticosteroids and immunosuppressive therapies. The ability of dupilumab to mitigate inflammation without broadly suppressing the immune system suggests that it may turn out to be an especially valuable option for older patients and those with comorbid conditions.
Acknowledgement—The authors thank Jodi Fiedler, MD (Boca Raton, FL), for her expert advice and assistance.
Bullous pemphigoid (BP) is a chronic autoimmune skin condition characterized by large, fluid-filled blisters (bullae) on the skin. There usually is severe itching, which may antedate the bullae by several weeks. Bullous pemphigoid most commonly affects adults aged 60 years and older with comorbidities such as metabolic syndrome or other autoimmune diseases. The typical blistering is subepidermal, and its occurrence seems to be driven by autoantibodies targeting the epidermal basement membrane zone.
Conventional treatment for BP has long included systemic corticosteroids and immunosuppressants; this combination of drugs effectively controls inflammation but also is associated with considerable risks such as infection, hyperglycemia with worsening diabetes, hypertension, osteoporosis and fracture risk, and delirium, particularly in older patients. Recent developments in biologic therapy have supported the utilization of potentially safer alternatives. Specifically, dupilumab has demonstrated efficacy in the treatment of atopic dermatitis. Case reports and small research studies included in a recent review have suggested that dupilumab could be effective in managing BP, potentially offering a safer treatment option.1 Importantly, dupilumab recently was approved for BP by the US Food and Drug Administration, making it the first biologic approved for treating this condition.2 In this article, we discuss dupilumab as an option for clinicians to prescribe as an initial therapy for BP.
Pathophysiology of Bullous Pemphigoid and Dupilumab
Bullous pemphigoid pathophysiology is driven by 2 main components: immunologic and inflammatory processes. The immune-mediated attack consists of autoantibodies against the hemidesmosomal proteins BP180 and BP230 in the basement membrane zone, which anchor the epidermis to the dermis.1 When these proteins are targeted, a cascade of responses is triggered, including the release of inflammatory cells, particularly eosinophils and neutrophils, into the skin. These cells release inflammatory mediators that break down the basement membrane, resulting in the separation of the epidermis from the dermis and leading to subepidermal blister formation.
The inflammation associated with BP largely is driven by a T helper 2–dominant immune response, with increased levels of cytokines such as interleukin (IL) 4 and IL-13.1 The chronic inflammation contributes to the characteristic blisters and intense pruritus seen in patients with BP. Traditional treatments such as corticosteroids work broadly to suppress this inflammation by reducing the production of all proinflammatory cytokines; however, they lack specificity, which dampens the targeted immune response against BP and broadly suppresses the immune system, increasing the risk for infection and other adverse effects. For older patients with multiple health conditions, these adverse effects can impact quality of life and pose health risks.
Interleukin 4 and IL-13 contribute to eosinophilia by upregulating the expression of eosinophil chemoattractant cytokines that promote eosinophil migration and adhesion.1 This is where dupilumab presents a promising alternative. Dupilumab is a monoclonal antibody that selectively targets the key cytokines implicated in BP. It binds to the IL-4 receptor alpha subunit, which IL-4 and IL-13 share, thereby inhibiting the signaling of both cytokines.1
Dupilumab Reports and Case Series
Current evidence supporting the use of dupilumab for BP consists primarily of case series and uncontrolled clinical observations, both of which are useful to formulate but not to test hypotheses.3 One case series of 13 patients diagnosed with BP reported that 92.3% (12/13) of patients achieved disease clearance or satisfactory control, with 53.8% (7/13) achieving total lesion clearance and no adverse events observed.4 In a larger case series, 87.0% of 146 patients achieved disease control with an initial dose of dupilumab 600 mg followed by 300 mg every 2 weeks for 4 weeks, though the study also looked at secondary outcomes for up to 64 weeks.5 Both these findings are compatible with the idea that dupilumab has efficacy in BP, but they cannot be used to test hypotheses.3,4
In a single case report of refractory BP, the combination of dupilumab and omalizumab—a monoclonal antibody that blocks the binding of IgE to mast cells, basophils, and dendritic cells—has shown efficacy, particularly when BP is unresponsive to standard therapies.6 The case involved a 72-year-old woman with unresponsive BP who was treated with a combination of dupilumab and omalizumab. She experienced marked improvement in pruritus and bullae accompanied by normalization of anti-BP180 autoantibody levels. This result points to the possibility that IL-4 and IL-13 blockade could influence autoantibody production. The authors attributed the reduction in pruritus to dupilumab, although the drug was administered in combination with omalizumab.6
Small Randomized Trial of Dupilumab
In addition to these uncontrolled clinical observations, dupilumab recently demonstrated positive results in a small randomized trial.7 Patients who were assigned to receive dupilumab were 5 times more likely to achieve sustained remission compared to those assigned to a placebo. All randomized patients also were treated with a standard-of-care oral corticosteroid regimen, which complicated the ability to isolate the specific effects of dupilumab.7 Finally, a completed totality of evidence on the prescription of dupilumab for refractory BP should include more reliable results from larger randomized trials.8
Final Thoughts
Dupilumab is now approved by the US Food and Drug Administration for the treatment of BP, marking an important milestone as the first targeted biologic therapy for this condition. While the totality of evidence is still evolving, the available data indicate both efficacy and a favorable safety profile when compared to traditional corticosteroids and immunosuppressants. Based on the available data, we suggest that health care providers consider dupilumab as a first-line monotherapy in appropriate patients with BP without specific contraindications, particularly as a practical and safe alternative to corticosteroids and immunosuppressive therapies in older adults with comorbidities. If the patient demonstrates clinical improvement in symptom relief, the therapy can be continued. This strategy minimizes initial exposure to more potent biologics or therapies with higher toxicity profiles. For patients without adequate disease control or with severe initial presentations requiring rapid improvement, clinicians may consider escalation to adjunctive or alternative therapies, such as rituximab, omalizumab, or a short course of systemic corticosteroids for acute management.
Emerging data suggest that dupilumab is a promising therapy for BP. We suggest that it may be a safer targeted alternative to traditional corticosteroids and immunosuppressive therapies. The ability of dupilumab to mitigate inflammation without broadly suppressing the immune system suggests that it may turn out to be an especially valuable option for older patients and those with comorbid conditions.
Acknowledgement—The authors thank Jodi Fiedler, MD (Boca Raton, FL), for her expert advice and assistance.
- Zhang L, Chen Z, Wang L, et al. Bullous pemphigoid: the role of type 2 inflammation in its pathogenesis and the prospect of targeted therapy. Front Immunol. 2023;14:1115083. doi:10.3389/fimmu.2023.1115083
- Sanofi. Dupixent approved in the US as the only targeted medicine to treat patients with bullous pemphigoid. News release. June 20, 2025. Accessed September 8, 2025. https://www.sanofi.com/en/media-room/press-releases/2025/2025-06-20-05-00-00-3102518
- Hennekens CH, DeMets D. Statistical association and causation: contributions of different types of evidence. JAMA. 2011;306:1134-1136. doi:10.1001/jama.2011.322
- Abdat R, Waldman RA, de Bedout V, et al. Dupilumab as a novel therapy for bullous pemphigoid: a multicenter case series. J Am Acad Dermatol. 2020;83:46-52. doi:10.1016/j.jaad.2020.01.089
- Zhao L, Wang Q, Liang G, et al. Evaluation of dupilumab in patients with bullous pemphigoid. JAMA Dermatol. 2023;159:953-960. doi:10.1001/jamadermatol.2023.2428
- Seyed Jafari SM, Feldmeyer L, Bossart S, et al. Case report: combination of omalizumab and dupilumab for recalcitrant bullous pemphigoid. Front Immunol. 2021;11:611549. doi:10.3389/fimmu.2020.611549
- US National Library of Medicine. A multicenter, randomized, double-blind, placebo-controlled, parallel-group study to evaluate the efficacy and safety of dupilumab in adult patients with bullous pemphigoid. ClinicalTrials.gov. Published 2019. Accessed March 10, 2026. https://clinicaltrials.gov/ct2/show/NCT04206553
- Hennekens CH, DeMets D. The need for large scale randomized evidence without undue emphasis on small trials, meta-analyses or subgroup analyses. JAMA. 2009;302:2361-2362. doi:10.1001/jama.2009.1829
- Zhang L, Chen Z, Wang L, et al. Bullous pemphigoid: the role of type 2 inflammation in its pathogenesis and the prospect of targeted therapy. Front Immunol. 2023;14:1115083. doi:10.3389/fimmu.2023.1115083
- Sanofi. Dupixent approved in the US as the only targeted medicine to treat patients with bullous pemphigoid. News release. June 20, 2025. Accessed September 8, 2025. https://www.sanofi.com/en/media-room/press-releases/2025/2025-06-20-05-00-00-3102518
- Hennekens CH, DeMets D. Statistical association and causation: contributions of different types of evidence. JAMA. 2011;306:1134-1136. doi:10.1001/jama.2011.322
- Abdat R, Waldman RA, de Bedout V, et al. Dupilumab as a novel therapy for bullous pemphigoid: a multicenter case series. J Am Acad Dermatol. 2020;83:46-52. doi:10.1016/j.jaad.2020.01.089
- Zhao L, Wang Q, Liang G, et al. Evaluation of dupilumab in patients with bullous pemphigoid. JAMA Dermatol. 2023;159:953-960. doi:10.1001/jamadermatol.2023.2428
- Seyed Jafari SM, Feldmeyer L, Bossart S, et al. Case report: combination of omalizumab and dupilumab for recalcitrant bullous pemphigoid. Front Immunol. 2021;11:611549. doi:10.3389/fimmu.2020.611549
- US National Library of Medicine. A multicenter, randomized, double-blind, placebo-controlled, parallel-group study to evaluate the efficacy and safety of dupilumab in adult patients with bullous pemphigoid. ClinicalTrials.gov. Published 2019. Accessed March 10, 2026. https://clinicaltrials.gov/ct2/show/NCT04206553
- Hennekens CH, DeMets D. The need for large scale randomized evidence without undue emphasis on small trials, meta-analyses or subgroup analyses. JAMA. 2009;302:2361-2362. doi:10.1001/jama.2009.1829
Dupilumab for Bullous Pemphigoid: To Treat or Not to Treat?
Dupilumab for Bullous Pemphigoid: To Treat or Not to Treat?
PRACTICE POINTS
- Bullous pemphigoid (BP) is a pruritic autoimmune blistering disease in older adults that often requires systemic therapy with associated risks.
- Dupilumab targets interleukin (IL) 4/IL-13–driven inflammation and shows promising efficacy in BP.
- As the first approved biologic for BP, dupilumab may offer a safer alternative to corticosteroids in select patients.

Choosing the Right Electronic Medical Record: Key Features and Considerations for Dermatology Practices
Choosing the Right Electronic Medical Record: Key Features and Considerations for Dermatology Practices
Choosing an electronic medical record (EMR) is one of the most important clinical and financial decisions a dermatology practice will make. An effective system can help streamline workflows, support high-quality patient care, and protect revenue, while the wrong choice can slow clinicians down and add to the administrative burden.
Dermatology workflows involve unique documentation, imaging, and billing needs that are not always well served by generic EMR platforms. To help guide the selection of an EMR, the following framework outlines key features and practice considerations specific to dermatology practices.
While many general EMRs offer customization, dermatology practices benefit greatly from ready-built, specialty-specific documentation tools. Key elements to evaluate include the following:
- Preconfigured dermatology templates for common conditions and procedures (eg, acne, psoriasis, melanoma, biopsies, cosmetic treatments)
- Smart-phrase libraries tailored to dermatologic language and examinations
- Ability to create, modify, and share custom templates across providers
Why It Matters—Efficient charting reduces documentation time, improves consistency, and supports accurate coding.
Dermatology is a highly visual specialty, making clinical photography and image management essential. Important capabilities of an EMR include the following:
- Easy capture, annotation, and longitudinal tracking of clinical images
- Seamless embedding of photographs directly into the patient chart
- Side-by-side comparison of current and prior images
- Secure image storage and camera integration
- Body-mapping tools to mark and track lesion locations visually
Why It Matters—A high-quality image workflow supports diagnosis, treatment planning, patient education, and medicolegal documentation.
For insurance-based practices, robust billing and revenue cycle management (RCM) tools are critical. For direct-care models, some of these items may be prioritized lower. Key features to compare include the following:
- Support for International Classification of Diseases, 10th Revision, Clinical Modification; Current Procedural Terminology; and dermatology-specific code sets
- Automated coding suggestions tied to clinical documentation
- Reviewing claims for errors and inconsistencies prior to submitting to payers’ insurance eligibility verification
- Electronic Remittance Advice/Explanation of Benefits posting and denial management workflows
- Support for cosmetic and self-pay billing
- Ability to generate superbills (itemized receipts for medical services that include International Classification of Diseases Tenth Revision and Current Procedural Terminology codes; patients can submit these directly to their insurance company for reimbursement) for direct-pay practices
Why It Matters—Strong RCM functionality protects revenue, reduces denials, and minimizes staff workload.
The most effective EMRs tightly integrate clinical charting with daily practice operations. Features to evaluate include the following:
- Integrated scheduling with color-coded calendars
- Appointment-type templates and block scheduling
- Automated patient reminders via text or email
- Support for multiprovider and multilocation practices
- Integration with outside pathology or lab services
Why It Matters—Clear and templated scheduling and practice integration help practices run more smoothly by reducing administrative workload and errors and coordinating communication between providers and even ancillary services.
Patient communication and virtual care are increasingly important in dermatology. When evaluating EMRs, compare the following:
- Built-in telehealth functionality vs third-party integrations
- Automated appointment reminders
- Patient portal features (forms, messaging, results)
- Online booking capabilities
Why It Matters—Integrated telehealth and patient communication tools improve access to care, enhance patient engagement, and streamline scheduling, messaging, and virtual visits within dermatology workflows.
Reporting capabilities support clinical quality, compliance, and business decision-making. Key reporting areas include the following:
- Clinical reports (outcomes, lesion tracking, disease management)
- Financial reports (revenue per provider, payer mix, visit types)
- Customizable or exportable reporting tools
Why It Matters—Robust reporting and analytics help dermatology practices track clinical outcomes, monitor financial performance, and make data-driven decisions to improve both patient care and practice management.
The user experience after implementation of the EMR is just as important as the software itself. Evaluate the following after the EMR is implemented:
- Initial training and onboarding resources
- Availability of dermatology-specific support teams
- Ongoing education, help centers, or user communities
- Access to dedicated implementation or success managers
Why It Matters—Strong training and support resources help ensure a smoother EMR implementation, faster staff adoption, and ongoing optimization of the system for dermatology workflows.
Finally, look beyond the sticker price. The total cost of ownership includes far more than monthly fees. Compare the following:
- Upfront costs (implementation, data migration, training)
- Subscription pricing (per provider or per user)
- Billing or RCM fees (including percentages of collections if applicable) and payment processing fees
- Costs for add-on modules (telehealth, imaging, analytics)
- Contract length and termination terms
Why It Matters—Understanding the full cost of ownership helps dermatology practices choose an EMR that fits their budget long-term while avoiding unexpected fees and contractual limitations.
There is no single “best” EMR for every dermatology practice. The right choice depends on your practice model, payer mix, clinical focus, and growth plans. By evaluating EMRs through a dermatology-specific lens and asking the right questions, you can choose a system that supports both excellent patient care and long-term practice success.
Choosing an electronic medical record (EMR) is one of the most important clinical and financial decisions a dermatology practice will make. An effective system can help streamline workflows, support high-quality patient care, and protect revenue, while the wrong choice can slow clinicians down and add to the administrative burden.
Dermatology workflows involve unique documentation, imaging, and billing needs that are not always well served by generic EMR platforms. To help guide the selection of an EMR, the following framework outlines key features and practice considerations specific to dermatology practices.
While many general EMRs offer customization, dermatology practices benefit greatly from ready-built, specialty-specific documentation tools. Key elements to evaluate include the following:
- Preconfigured dermatology templates for common conditions and procedures (eg, acne, psoriasis, melanoma, biopsies, cosmetic treatments)
- Smart-phrase libraries tailored to dermatologic language and examinations
- Ability to create, modify, and share custom templates across providers
Why It Matters—Efficient charting reduces documentation time, improves consistency, and supports accurate coding.
Dermatology is a highly visual specialty, making clinical photography and image management essential. Important capabilities of an EMR include the following:
- Easy capture, annotation, and longitudinal tracking of clinical images
- Seamless embedding of photographs directly into the patient chart
- Side-by-side comparison of current and prior images
- Secure image storage and camera integration
- Body-mapping tools to mark and track lesion locations visually
Why It Matters—A high-quality image workflow supports diagnosis, treatment planning, patient education, and medicolegal documentation.
For insurance-based practices, robust billing and revenue cycle management (RCM) tools are critical. For direct-care models, some of these items may be prioritized lower. Key features to compare include the following:
- Support for International Classification of Diseases, 10th Revision, Clinical Modification; Current Procedural Terminology; and dermatology-specific code sets
- Automated coding suggestions tied to clinical documentation
- Reviewing claims for errors and inconsistencies prior to submitting to payers’ insurance eligibility verification
- Electronic Remittance Advice/Explanation of Benefits posting and denial management workflows
- Support for cosmetic and self-pay billing
- Ability to generate superbills (itemized receipts for medical services that include International Classification of Diseases Tenth Revision and Current Procedural Terminology codes; patients can submit these directly to their insurance company for reimbursement) for direct-pay practices
Why It Matters—Strong RCM functionality protects revenue, reduces denials, and minimizes staff workload.
The most effective EMRs tightly integrate clinical charting with daily practice operations. Features to evaluate include the following:
- Integrated scheduling with color-coded calendars
- Appointment-type templates and block scheduling
- Automated patient reminders via text or email
- Support for multiprovider and multilocation practices
- Integration with outside pathology or lab services
Why It Matters—Clear and templated scheduling and practice integration help practices run more smoothly by reducing administrative workload and errors and coordinating communication between providers and even ancillary services.
Patient communication and virtual care are increasingly important in dermatology. When evaluating EMRs, compare the following:
- Built-in telehealth functionality vs third-party integrations
- Automated appointment reminders
- Patient portal features (forms, messaging, results)
- Online booking capabilities
Why It Matters—Integrated telehealth and patient communication tools improve access to care, enhance patient engagement, and streamline scheduling, messaging, and virtual visits within dermatology workflows.
Reporting capabilities support clinical quality, compliance, and business decision-making. Key reporting areas include the following:
- Clinical reports (outcomes, lesion tracking, disease management)
- Financial reports (revenue per provider, payer mix, visit types)
- Customizable or exportable reporting tools
Why It Matters—Robust reporting and analytics help dermatology practices track clinical outcomes, monitor financial performance, and make data-driven decisions to improve both patient care and practice management.
The user experience after implementation of the EMR is just as important as the software itself. Evaluate the following after the EMR is implemented:
- Initial training and onboarding resources
- Availability of dermatology-specific support teams
- Ongoing education, help centers, or user communities
- Access to dedicated implementation or success managers
Why It Matters—Strong training and support resources help ensure a smoother EMR implementation, faster staff adoption, and ongoing optimization of the system for dermatology workflows.
Finally, look beyond the sticker price. The total cost of ownership includes far more than monthly fees. Compare the following:
- Upfront costs (implementation, data migration, training)
- Subscription pricing (per provider or per user)
- Billing or RCM fees (including percentages of collections if applicable) and payment processing fees
- Costs for add-on modules (telehealth, imaging, analytics)
- Contract length and termination terms
Why It Matters—Understanding the full cost of ownership helps dermatology practices choose an EMR that fits their budget long-term while avoiding unexpected fees and contractual limitations.
There is no single “best” EMR for every dermatology practice. The right choice depends on your practice model, payer mix, clinical focus, and growth plans. By evaluating EMRs through a dermatology-specific lens and asking the right questions, you can choose a system that supports both excellent patient care and long-term practice success.
Choosing an electronic medical record (EMR) is one of the most important clinical and financial decisions a dermatology practice will make. An effective system can help streamline workflows, support high-quality patient care, and protect revenue, while the wrong choice can slow clinicians down and add to the administrative burden.
Dermatology workflows involve unique documentation, imaging, and billing needs that are not always well served by generic EMR platforms. To help guide the selection of an EMR, the following framework outlines key features and practice considerations specific to dermatology practices.
While many general EMRs offer customization, dermatology practices benefit greatly from ready-built, specialty-specific documentation tools. Key elements to evaluate include the following:
- Preconfigured dermatology templates for common conditions and procedures (eg, acne, psoriasis, melanoma, biopsies, cosmetic treatments)
- Smart-phrase libraries tailored to dermatologic language and examinations
- Ability to create, modify, and share custom templates across providers
Why It Matters—Efficient charting reduces documentation time, improves consistency, and supports accurate coding.
Dermatology is a highly visual specialty, making clinical photography and image management essential. Important capabilities of an EMR include the following:
- Easy capture, annotation, and longitudinal tracking of clinical images
- Seamless embedding of photographs directly into the patient chart
- Side-by-side comparison of current and prior images
- Secure image storage and camera integration
- Body-mapping tools to mark and track lesion locations visually
Why It Matters—A high-quality image workflow supports diagnosis, treatment planning, patient education, and medicolegal documentation.
For insurance-based practices, robust billing and revenue cycle management (RCM) tools are critical. For direct-care models, some of these items may be prioritized lower. Key features to compare include the following:
- Support for International Classification of Diseases, 10th Revision, Clinical Modification; Current Procedural Terminology; and dermatology-specific code sets
- Automated coding suggestions tied to clinical documentation
- Reviewing claims for errors and inconsistencies prior to submitting to payers’ insurance eligibility verification
- Electronic Remittance Advice/Explanation of Benefits posting and denial management workflows
- Support for cosmetic and self-pay billing
- Ability to generate superbills (itemized receipts for medical services that include International Classification of Diseases Tenth Revision and Current Procedural Terminology codes; patients can submit these directly to their insurance company for reimbursement) for direct-pay practices
Why It Matters—Strong RCM functionality protects revenue, reduces denials, and minimizes staff workload.
The most effective EMRs tightly integrate clinical charting with daily practice operations. Features to evaluate include the following:
- Integrated scheduling with color-coded calendars
- Appointment-type templates and block scheduling
- Automated patient reminders via text or email
- Support for multiprovider and multilocation practices
- Integration with outside pathology or lab services
Why It Matters—Clear and templated scheduling and practice integration help practices run more smoothly by reducing administrative workload and errors and coordinating communication between providers and even ancillary services.
Patient communication and virtual care are increasingly important in dermatology. When evaluating EMRs, compare the following:
- Built-in telehealth functionality vs third-party integrations
- Automated appointment reminders
- Patient portal features (forms, messaging, results)
- Online booking capabilities
Why It Matters—Integrated telehealth and patient communication tools improve access to care, enhance patient engagement, and streamline scheduling, messaging, and virtual visits within dermatology workflows.
Reporting capabilities support clinical quality, compliance, and business decision-making. Key reporting areas include the following:
- Clinical reports (outcomes, lesion tracking, disease management)
- Financial reports (revenue per provider, payer mix, visit types)
- Customizable or exportable reporting tools
Why It Matters—Robust reporting and analytics help dermatology practices track clinical outcomes, monitor financial performance, and make data-driven decisions to improve both patient care and practice management.
The user experience after implementation of the EMR is just as important as the software itself. Evaluate the following after the EMR is implemented:
- Initial training and onboarding resources
- Availability of dermatology-specific support teams
- Ongoing education, help centers, or user communities
- Access to dedicated implementation or success managers
Why It Matters—Strong training and support resources help ensure a smoother EMR implementation, faster staff adoption, and ongoing optimization of the system for dermatology workflows.
Finally, look beyond the sticker price. The total cost of ownership includes far more than monthly fees. Compare the following:
- Upfront costs (implementation, data migration, training)
- Subscription pricing (per provider or per user)
- Billing or RCM fees (including percentages of collections if applicable) and payment processing fees
- Costs for add-on modules (telehealth, imaging, analytics)
- Contract length and termination terms
Why It Matters—Understanding the full cost of ownership helps dermatology practices choose an EMR that fits their budget long-term while avoiding unexpected fees and contractual limitations.
There is no single “best” EMR for every dermatology practice. The right choice depends on your practice model, payer mix, clinical focus, and growth plans. By evaluating EMRs through a dermatology-specific lens and asking the right questions, you can choose a system that supports both excellent patient care and long-term practice success.
Choosing the Right Electronic Medical Record: Key Features and Considerations for Dermatology Practices
Choosing the Right Electronic Medical Record: Key Features and Considerations for Dermatology Practices
PRACTICE POINTS
- Choosing an electronic medical record (EMR) built for dermatology workflow is a critical part of practice management.
- Features of an EMR that should be evaluated include support for clinical documentation, scheduling and billing, and customer support.
- The proper EMR can reduce administrative tasks and protect practice revenue, but there is no one-size-fits-all option.

Beyond Conventional Paradigms: Rethinking the Evaluation and Management of Melasma
Beyond Conventional Paradigms: Rethinking the Evaluation and Management of Melasma
Melasma is a chronic hyperpigmentation disorder with a high recurrence rate. Advances in pathogenesis, diagnosis, and treatment have shifted dermatologic approaches for both initial management and long-term care. These advances highlight the need to move beyond conventional paradigms for melasma to adopt a more comprehensive and holistic approach to evaluation and management.
Diagnosis: Beyond the Wood Lamp
Diagnosis of melasma is primarily clinical, based on visual examination, with tools such as a Wood lamp (320-400 nm) aiding in classification as epidermal, dermal, or mixed types.1 Dermoscopy is another useful tool that commonly demonstrates a brown reticular pseudonetwork, vascular patterns, and brown clods.2 Reflectance confocal microscopy allows detailed assessment of pigment distribution across skin layers and may serve as a useful diagnostic adjunct.3 Two-photon excitation microscopy also has shown concordance with reflectance confocal microscopy in identifying key pathologic features of melasma and allows quantitative assessment of pigment burden.4,5 Biopsy remains warranted in cases when the diagnosis is unclear.6,7 These advanced tools provide additional options for noninvasive imaging of melasma, which may be useful during both diagnosis and treatment.
Pathogenesis: Beyond the Melanocyte
Recent insights into pathogenesis have shifted the view of melasma from a purely melanocyte-driven disorder to one involving complex epidermal-dermal interactions influenced by chronic UV and visible light exposure and sustained cutaneous inflammation. Evidence suggests involvement of additional cell types and structural components, including epidermal barrier dysfunction, basement membrane alterations, senescent fibroblasts, mast cell activity, vascular remodeling, and dermal solar elastosis. Senescent fibroblasts secrete melanogenic and angiogenic mediators (including stem cell factor, vascular endothelial growth factor, endothelin 1, and matrix metalloproteinases) while mast cell degranulation releases histamine, tryptase, and other proteases that drive melanocyte activation, extracellular matrix degradation, and persistent hyperpigmentation.8 New research highlights the importance of epidermal-dermal communication in melasma disease activity.8,9 Exposure to UV and visible light leads to keratinocyte injury and fibroblast dysfunction, promoting the release of inflammatory and melanogenic mediators that stimulate melanocytes and weaken the basement membrane.8 Mast cell activation and vascular signaling also have been implicated, reinforcing the contribution of inflammation and dermal remodeling to ongoing pigmentation.9 This broader understanding helps explain the difficulty of sustaining long-term remission.8,9 The multifaceted and evolving understanding of melasma’s complex pathogenesis highlights areas for future therapeutic targets beyond melanin, which may help lead to greater clearance and remission periods.
Treatment: Beyond Hydroquinone
Melasma treatment has shifted toward a longitudinal approach reflecting its chronic relapsing nature. Effective management should include combination therapy of broad-spectrum photoprotection, topical therapies, systemic therapies (when appropriate), and adjunctive procedural modalities, while emphasizing the importance of maintenance therapy and relapse prevention.10,11 Growing evidence demonstrates that UV and visible light contribute to melanogenesis and prolonged pigmentation, particularly in individuals with skin of color.12,13 Visible light, particularly within the high-energy blue wavelength spectrum (400-500 nm), induces reactive oxygen species and stimulates melanogenesis, resulting in persistent hyperpigmentation and exacerbation of melasma in darker skin types.13 Iron oxide, a mineral-based physical filter commonly used in tinted mineral sunscreens, enhances protection from visible light, thus improving melasma outcomes.12,13 In a randomized double-blind placebo-controlled trial, oral polypodium leucotomos extract, an antioxidant with photoprotective effects, improved Melasma Area and Severity Index (MASI)/modified MASI (mMASI) scores and melasma-rated quality of life measures when used as an adjunct to sunscreen with or without topical hydroquinone.14
Topical therapy serves as the mainstay of melasma treatment. Hydroquinone- and retinoid-based regimens including triple-combination therapy remain an effective gold standard for active disease; however, there still are concerns about irritant dermatitis with both as well as ochronosis with long-term use of hydroquinone.15 Recent studies highlight the efficacy of nonhydroquinone topical therapies such as azelaic acid, tranexamic acid (TXA), thiamidol, cysteamine, metformin, malassezin, 2-mercaptonicotinoyl glycine, niacinamide, kojic acid, ascorbic acid, and botanical-derived compounds, many of which demonstrate reductions in disease severity and more favorable tolerability profiles.16-19 Combinations of these ingredients can allow for addressing the various pathogenic factors of melasma beyond pigmentation, including vascularity, inflammation, and solar damage.
Systemic therapy, particularly oral TXA, has emerged as an option for patients with moderate to severe or refractory melasma. Clinical trials and observational studies demonstrate improvement with oral TXA; however, relapse after discontinuation is common, emphasizing the importance of careful patient selection, established treatment duration, and concurrent maintenance therapy.16,20 Although it is well tolerated, adverse effects include gastrointestinal discomfort, menstrual irregularities, and headache. Additionally, prescreening for contraindications and clotting risk factors is needed to avoid thromboembolic events.21
Procedural interventions are best used as adjunctive therapies rather than primary treatment. Superficial and medium peels can be used depending on baseline skin type.22 Platelet-rich plasma is a promising adjunctive therapy for melasma, demonstrating reductions in MASI scores following intradermal or microneedling-assisted delivery, likely mediated through growth factor–driven inhibition of melanogenesis and modulation of tyrosinase activity. Platelet-rich plasma promotes dermal remodeling through angiogenesis, collagen synthesis, and extracellular matrix production improving skin texture and pigmentation.23 Botulinum toxin A may improve pigmentation by modulating melanogenesis as well as inflammatory and vascular pathways.24
Radiofrequency microneedling provides a dermal-targeting therapeutic approach, with some evidence showing that monthly treatments can help maintain improvements achieved with conventional therapy by modulating photoaged dermal structures impacted by melanogenic signaling.25 Histopathologic correlation studies suggest that microneedling used alone or as a delivery platform alongside topical agents may be beneficial in dermal-predominant disease, while laser-based therapies should be reserved for recalcitrant cases due to the risk for postinflammatory hyperpigmentation and melasma recurrence, particularly in those with darker skin types.26 Lasers such as Q-switched 1064-nm Nd:YAG as well as nonablative lasers used in conservative settings are options for melasma treatment, including in patients with skin of color.26,27 Laser toning with serial low-fluence (<3 J/cm2), large-spot 1064-nm Nd:YAG has been used to reduce inflammation and risk for postinflammatory hyperpigmentation.28 Additionally, randomized split-face data demonstrate that picosecond 1064-nm devices achieve comparable reductions in mMASI scores to traditional nanosecond devices, and combination strategies incorporating intense pulsed light (IPL) have shown greater MASI improvement compared with IPL alone.28,29 However, IPL generally is limited to lighter skin phototypes due to the risk for postinflammatory hyperpigmentation in darker skin.30
Lastly, long-term management requires patient education on the importance of year-round maintenance therapy, consistency, and compliance. Reinforcing adherence to photoprotection, supporting barrier repair, and setting expectations regarding prognosis are essential components to optimizing melasma treatment outcomes.12
Future Insights: Beyond the Current State of Melasma Research and Treatment
Future advances in melasma management likely will focus on improving disease assessment and long-term treatment durability. Tools such as the MASI and mMASI are widely used but are limited by interobserver variability and reduced sensitivity in darker skin types, highlighting the need to incorporate objective measures such as colorimetry.10,26 There also is a need for studies that relate clinical improvement to underlying pathology. Histopathologic correlation remains limited across most therapeutic trials, and more studies should assess long-term outcomes and quality-of-life measures given the relapsing nature of melasma.26
Future interventions will continue to move past the treatment of pigment alone. Increasing recognition of vascular, inflammatory, and barrier-related contributions to melasma, as well as targeting of other cell types affected by melasma, will be important considerations in future treatment innovations.8,11 In summary, improved inclusion of patients with skin of color in clinical trials, expansion of clinical outcomes measures and objective parameters of disease evaluation, novel approaches to treatment and relapse prevention, and greater attention to patient adherence and education will be essential to achieving advancements in melasma care.12
- Sanchez NP, Pathak MA, Sato S, et al. Melasma: a clinical, light microscopic, ultrastructural, and immunofluorescence study. J Am Acad Dermatol. 1981;4:698-710.
- Bostan E, Cakir A. The dermoscopic characteristics of melasma in relation to different skin phototypes, distribution patterns and wood lamp findings: a cross-sectional study of 236 melasma lesions. Arch Dermatol Res. 2023;315:1927-1938.
- Guida S, Longo C, Ronga R, et al. Melasma and reflectance confocal microscopy: from baseline to treatment monitoring. Int J Dermatol. 2024;63:1007-1012.
- Ning X, Yang J, Ouyang H, et al. In vivo evaluation of melasma pathologic features and treatment response by 2-photon microscopy. JAMA Dermatol. 2025;161:1039-1047.
- Chen K-J, Han Y, Wang Z-Y, et al. Submicron resolution techniques: multiphoton microscopy in skin disease. Exp Dermatol. 2023;32:1613-1623.
- Philipp-Dormston WG. Melasma: a step-by-step approach towards a multimodal combination therapy. Clin Cosmet Investig Dermatol. 2024;17:1203-1216.
- Doolan B, Gupta M. Melasma. Aust J Gen Pract. 2021;50:880-885.
- Ali L, Al Niaimi F. Pathogenesis of melasma explained. Int J Dermatol. 2025;64:1201-1212.
- Artzi O, Horovitz T, Bar-Ilan E, et al. The pathogenesis of melasma and implications for treatment. J Cosmet Dermatol. 2021;20:3432-3445.
- Gan C, Rodrigues M. An update on new and existing treatments for the management of melasma. Am J Clin Dermatol. 2024;25:717-733.
- Sarkar R, Desai SR, Sinha S, et al. Delphi consensus on melasma management by international experts and pigmentary disorders society. J Eur Acad Dermatol Venereol. Published online September 25, 2025.
- Desai SR, Alexis AF, Elbuluk N, et al. Best practices in the treatment of melasma with a focus on patients with skin of color. J Am Acad Dermatol. 2024;90:269-279.
- Lim HW, Kohli I, Ruvolo E, et al. Impact of visible light on skin health: the role of antioxidants and free radical quenchers in skin protection. J Am Acad Deramtol. 2022;86(3 suppl):S27-S37.
- Goh CL, Chuah SY, Tien S, et al. Double-blind, placebo-controlled trial to evaluate the effectiveness of polypodium leucotomos extract in the treatment of melasma in Asian skin: a pilot study. J Clin Aesthet Dermatol. 2018;11:14-19.
- Mahajan VK, Patil A, Blicharz L, et al. Medical therapies for melasma. J Cosmet Dermatol. 2022;21:3707-3728.
- Suliman RS, Alhuwayshil J, Almuflehi AA, et al. Emerging topical therapies for melasma: a comparative analysis of efficacy and safety. J Dermatolog Treat. 2025;36:2591502.
- Austin E, Nguyen JK, Jagdeo J. Topical treatments for melasma: a systematic review of randomized controlled trials. J Drugs Dermatol. 2019;18:S1545961619P1156X.
- Grimes PE, Dias S, Oparaugo NC, et al. A randomized, controlled, split-face, double-blind study comparing topical malassezin to hydroquinone 4% for melasma. J Drugs Dermatol. 2026;25:25-29.
- Passeron T, Kerob D, Le Dantec G, et al. Efficacy and tolerability of a new facial 2-mercaptonicotinoyl glycine-containing depigmenting serum versus hydroquinone 4% over 3-month treatment of facial melasma. Dermatol Ther (Heidelb). 2025;15:2379-2390.
- McKesey J, Tovar-Garza A, Pandya AG. Melasma treatment: an evidence-based review. Am J Clin Dermatol. 2020;21:173-225.
- Bala HR, Lee S, Wong C, et al. Oral tranexamic acid for the treatment of melasma: a review. Dermatol Surg. 2018;44:814-825.
- Sarkar R, Katoch S. Chemical peels in treatment of melasma. Dermatol Clin. 2024;42:21-32.
- Sarkar R, Gupta M. Platelet-rich plasma in melasma—a systematic review. Dermatol Surg. 2022;48:131-134.
- Pongklaokam J, Manuskiatti W, Wanitphakdeedecha R, et al. Efficacy and safety of letibotulinum toxin A for the treatment of melasma in two different dilutions: a randomized double-blind split-face study. Toxins (Basel). 2025;17:349.
- Han HJ, Kim JC, Park YJ, et al. Targeting the dermis for melasma maintenance treatment. Sci Rep. 2024;14:949.
- Zhang AD, Lazar M, Akhundova E, et al. A scoping review on melasma treatments and their histopathologic correlates. Dermatopathology (Basel). 2025;12:13.
- Goldman MP, Wu DC, Khetarpal S, et al. Dual 1550-nm erbium glass fiber and 1927-nm thulium fiber non-ablative fractional laser system treatment in patients with skin of color: a review of clinical studies and unmet needs. Lasers Surg Med. Published online February 10, 2026.
- Chen J, Yu N, Peng L, et al. Efficacy of low-fluence 1064 nm Q-switched Nd: YAG laser for the treatment of melasma: a meta-analysis and systematic review. J Cosmet Dermatol. 2022;21.
- Feng J, Huang L. Comparison of picosecond and nanosecond Nd:YAG 1064-nm lasers in the treatment of melasma: a split-face randomized clinical trial. Plast Reconstr Surg. 2023;151:772-777.
- Passeron T, Genedy R, Salah L, et al., Laser treatment of hyperpigmented lesions: position statement of the European Society of Laser in Dermatology. J Eur Acad Dermatol Venereol. 2019;33:987-1005.
Melasma is a chronic hyperpigmentation disorder with a high recurrence rate. Advances in pathogenesis, diagnosis, and treatment have shifted dermatologic approaches for both initial management and long-term care. These advances highlight the need to move beyond conventional paradigms for melasma to adopt a more comprehensive and holistic approach to evaluation and management.
Diagnosis: Beyond the Wood Lamp
Diagnosis of melasma is primarily clinical, based on visual examination, with tools such as a Wood lamp (320-400 nm) aiding in classification as epidermal, dermal, or mixed types.1 Dermoscopy is another useful tool that commonly demonstrates a brown reticular pseudonetwork, vascular patterns, and brown clods.2 Reflectance confocal microscopy allows detailed assessment of pigment distribution across skin layers and may serve as a useful diagnostic adjunct.3 Two-photon excitation microscopy also has shown concordance with reflectance confocal microscopy in identifying key pathologic features of melasma and allows quantitative assessment of pigment burden.4,5 Biopsy remains warranted in cases when the diagnosis is unclear.6,7 These advanced tools provide additional options for noninvasive imaging of melasma, which may be useful during both diagnosis and treatment.
Pathogenesis: Beyond the Melanocyte
Recent insights into pathogenesis have shifted the view of melasma from a purely melanocyte-driven disorder to one involving complex epidermal-dermal interactions influenced by chronic UV and visible light exposure and sustained cutaneous inflammation. Evidence suggests involvement of additional cell types and structural components, including epidermal barrier dysfunction, basement membrane alterations, senescent fibroblasts, mast cell activity, vascular remodeling, and dermal solar elastosis. Senescent fibroblasts secrete melanogenic and angiogenic mediators (including stem cell factor, vascular endothelial growth factor, endothelin 1, and matrix metalloproteinases) while mast cell degranulation releases histamine, tryptase, and other proteases that drive melanocyte activation, extracellular matrix degradation, and persistent hyperpigmentation.8 New research highlights the importance of epidermal-dermal communication in melasma disease activity.8,9 Exposure to UV and visible light leads to keratinocyte injury and fibroblast dysfunction, promoting the release of inflammatory and melanogenic mediators that stimulate melanocytes and weaken the basement membrane.8 Mast cell activation and vascular signaling also have been implicated, reinforcing the contribution of inflammation and dermal remodeling to ongoing pigmentation.9 This broader understanding helps explain the difficulty of sustaining long-term remission.8,9 The multifaceted and evolving understanding of melasma’s complex pathogenesis highlights areas for future therapeutic targets beyond melanin, which may help lead to greater clearance and remission periods.
Treatment: Beyond Hydroquinone
Melasma treatment has shifted toward a longitudinal approach reflecting its chronic relapsing nature. Effective management should include combination therapy of broad-spectrum photoprotection, topical therapies, systemic therapies (when appropriate), and adjunctive procedural modalities, while emphasizing the importance of maintenance therapy and relapse prevention.10,11 Growing evidence demonstrates that UV and visible light contribute to melanogenesis and prolonged pigmentation, particularly in individuals with skin of color.12,13 Visible light, particularly within the high-energy blue wavelength spectrum (400-500 nm), induces reactive oxygen species and stimulates melanogenesis, resulting in persistent hyperpigmentation and exacerbation of melasma in darker skin types.13 Iron oxide, a mineral-based physical filter commonly used in tinted mineral sunscreens, enhances protection from visible light, thus improving melasma outcomes.12,13 In a randomized double-blind placebo-controlled trial, oral polypodium leucotomos extract, an antioxidant with photoprotective effects, improved Melasma Area and Severity Index (MASI)/modified MASI (mMASI) scores and melasma-rated quality of life measures when used as an adjunct to sunscreen with or without topical hydroquinone.14
Topical therapy serves as the mainstay of melasma treatment. Hydroquinone- and retinoid-based regimens including triple-combination therapy remain an effective gold standard for active disease; however, there still are concerns about irritant dermatitis with both as well as ochronosis with long-term use of hydroquinone.15 Recent studies highlight the efficacy of nonhydroquinone topical therapies such as azelaic acid, tranexamic acid (TXA), thiamidol, cysteamine, metformin, malassezin, 2-mercaptonicotinoyl glycine, niacinamide, kojic acid, ascorbic acid, and botanical-derived compounds, many of which demonstrate reductions in disease severity and more favorable tolerability profiles.16-19 Combinations of these ingredients can allow for addressing the various pathogenic factors of melasma beyond pigmentation, including vascularity, inflammation, and solar damage.
Systemic therapy, particularly oral TXA, has emerged as an option for patients with moderate to severe or refractory melasma. Clinical trials and observational studies demonstrate improvement with oral TXA; however, relapse after discontinuation is common, emphasizing the importance of careful patient selection, established treatment duration, and concurrent maintenance therapy.16,20 Although it is well tolerated, adverse effects include gastrointestinal discomfort, menstrual irregularities, and headache. Additionally, prescreening for contraindications and clotting risk factors is needed to avoid thromboembolic events.21
Procedural interventions are best used as adjunctive therapies rather than primary treatment. Superficial and medium peels can be used depending on baseline skin type.22 Platelet-rich plasma is a promising adjunctive therapy for melasma, demonstrating reductions in MASI scores following intradermal or microneedling-assisted delivery, likely mediated through growth factor–driven inhibition of melanogenesis and modulation of tyrosinase activity. Platelet-rich plasma promotes dermal remodeling through angiogenesis, collagen synthesis, and extracellular matrix production improving skin texture and pigmentation.23 Botulinum toxin A may improve pigmentation by modulating melanogenesis as well as inflammatory and vascular pathways.24
Radiofrequency microneedling provides a dermal-targeting therapeutic approach, with some evidence showing that monthly treatments can help maintain improvements achieved with conventional therapy by modulating photoaged dermal structures impacted by melanogenic signaling.25 Histopathologic correlation studies suggest that microneedling used alone or as a delivery platform alongside topical agents may be beneficial in dermal-predominant disease, while laser-based therapies should be reserved for recalcitrant cases due to the risk for postinflammatory hyperpigmentation and melasma recurrence, particularly in those with darker skin types.26 Lasers such as Q-switched 1064-nm Nd:YAG as well as nonablative lasers used in conservative settings are options for melasma treatment, including in patients with skin of color.26,27 Laser toning with serial low-fluence (<3 J/cm2), large-spot 1064-nm Nd:YAG has been used to reduce inflammation and risk for postinflammatory hyperpigmentation.28 Additionally, randomized split-face data demonstrate that picosecond 1064-nm devices achieve comparable reductions in mMASI scores to traditional nanosecond devices, and combination strategies incorporating intense pulsed light (IPL) have shown greater MASI improvement compared with IPL alone.28,29 However, IPL generally is limited to lighter skin phototypes due to the risk for postinflammatory hyperpigmentation in darker skin.30
Lastly, long-term management requires patient education on the importance of year-round maintenance therapy, consistency, and compliance. Reinforcing adherence to photoprotection, supporting barrier repair, and setting expectations regarding prognosis are essential components to optimizing melasma treatment outcomes.12
Future Insights: Beyond the Current State of Melasma Research and Treatment
Future advances in melasma management likely will focus on improving disease assessment and long-term treatment durability. Tools such as the MASI and mMASI are widely used but are limited by interobserver variability and reduced sensitivity in darker skin types, highlighting the need to incorporate objective measures such as colorimetry.10,26 There also is a need for studies that relate clinical improvement to underlying pathology. Histopathologic correlation remains limited across most therapeutic trials, and more studies should assess long-term outcomes and quality-of-life measures given the relapsing nature of melasma.26
Future interventions will continue to move past the treatment of pigment alone. Increasing recognition of vascular, inflammatory, and barrier-related contributions to melasma, as well as targeting of other cell types affected by melasma, will be important considerations in future treatment innovations.8,11 In summary, improved inclusion of patients with skin of color in clinical trials, expansion of clinical outcomes measures and objective parameters of disease evaluation, novel approaches to treatment and relapse prevention, and greater attention to patient adherence and education will be essential to achieving advancements in melasma care.12
Melasma is a chronic hyperpigmentation disorder with a high recurrence rate. Advances in pathogenesis, diagnosis, and treatment have shifted dermatologic approaches for both initial management and long-term care. These advances highlight the need to move beyond conventional paradigms for melasma to adopt a more comprehensive and holistic approach to evaluation and management.
Diagnosis: Beyond the Wood Lamp
Diagnosis of melasma is primarily clinical, based on visual examination, with tools such as a Wood lamp (320-400 nm) aiding in classification as epidermal, dermal, or mixed types.1 Dermoscopy is another useful tool that commonly demonstrates a brown reticular pseudonetwork, vascular patterns, and brown clods.2 Reflectance confocal microscopy allows detailed assessment of pigment distribution across skin layers and may serve as a useful diagnostic adjunct.3 Two-photon excitation microscopy also has shown concordance with reflectance confocal microscopy in identifying key pathologic features of melasma and allows quantitative assessment of pigment burden.4,5 Biopsy remains warranted in cases when the diagnosis is unclear.6,7 These advanced tools provide additional options for noninvasive imaging of melasma, which may be useful during both diagnosis and treatment.
Pathogenesis: Beyond the Melanocyte
Recent insights into pathogenesis have shifted the view of melasma from a purely melanocyte-driven disorder to one involving complex epidermal-dermal interactions influenced by chronic UV and visible light exposure and sustained cutaneous inflammation. Evidence suggests involvement of additional cell types and structural components, including epidermal barrier dysfunction, basement membrane alterations, senescent fibroblasts, mast cell activity, vascular remodeling, and dermal solar elastosis. Senescent fibroblasts secrete melanogenic and angiogenic mediators (including stem cell factor, vascular endothelial growth factor, endothelin 1, and matrix metalloproteinases) while mast cell degranulation releases histamine, tryptase, and other proteases that drive melanocyte activation, extracellular matrix degradation, and persistent hyperpigmentation.8 New research highlights the importance of epidermal-dermal communication in melasma disease activity.8,9 Exposure to UV and visible light leads to keratinocyte injury and fibroblast dysfunction, promoting the release of inflammatory and melanogenic mediators that stimulate melanocytes and weaken the basement membrane.8 Mast cell activation and vascular signaling also have been implicated, reinforcing the contribution of inflammation and dermal remodeling to ongoing pigmentation.9 This broader understanding helps explain the difficulty of sustaining long-term remission.8,9 The multifaceted and evolving understanding of melasma’s complex pathogenesis highlights areas for future therapeutic targets beyond melanin, which may help lead to greater clearance and remission periods.
Treatment: Beyond Hydroquinone
Melasma treatment has shifted toward a longitudinal approach reflecting its chronic relapsing nature. Effective management should include combination therapy of broad-spectrum photoprotection, topical therapies, systemic therapies (when appropriate), and adjunctive procedural modalities, while emphasizing the importance of maintenance therapy and relapse prevention.10,11 Growing evidence demonstrates that UV and visible light contribute to melanogenesis and prolonged pigmentation, particularly in individuals with skin of color.12,13 Visible light, particularly within the high-energy blue wavelength spectrum (400-500 nm), induces reactive oxygen species and stimulates melanogenesis, resulting in persistent hyperpigmentation and exacerbation of melasma in darker skin types.13 Iron oxide, a mineral-based physical filter commonly used in tinted mineral sunscreens, enhances protection from visible light, thus improving melasma outcomes.12,13 In a randomized double-blind placebo-controlled trial, oral polypodium leucotomos extract, an antioxidant with photoprotective effects, improved Melasma Area and Severity Index (MASI)/modified MASI (mMASI) scores and melasma-rated quality of life measures when used as an adjunct to sunscreen with or without topical hydroquinone.14
Topical therapy serves as the mainstay of melasma treatment. Hydroquinone- and retinoid-based regimens including triple-combination therapy remain an effective gold standard for active disease; however, there still are concerns about irritant dermatitis with both as well as ochronosis with long-term use of hydroquinone.15 Recent studies highlight the efficacy of nonhydroquinone topical therapies such as azelaic acid, tranexamic acid (TXA), thiamidol, cysteamine, metformin, malassezin, 2-mercaptonicotinoyl glycine, niacinamide, kojic acid, ascorbic acid, and botanical-derived compounds, many of which demonstrate reductions in disease severity and more favorable tolerability profiles.16-19 Combinations of these ingredients can allow for addressing the various pathogenic factors of melasma beyond pigmentation, including vascularity, inflammation, and solar damage.
Systemic therapy, particularly oral TXA, has emerged as an option for patients with moderate to severe or refractory melasma. Clinical trials and observational studies demonstrate improvement with oral TXA; however, relapse after discontinuation is common, emphasizing the importance of careful patient selection, established treatment duration, and concurrent maintenance therapy.16,20 Although it is well tolerated, adverse effects include gastrointestinal discomfort, menstrual irregularities, and headache. Additionally, prescreening for contraindications and clotting risk factors is needed to avoid thromboembolic events.21
Procedural interventions are best used as adjunctive therapies rather than primary treatment. Superficial and medium peels can be used depending on baseline skin type.22 Platelet-rich plasma is a promising adjunctive therapy for melasma, demonstrating reductions in MASI scores following intradermal or microneedling-assisted delivery, likely mediated through growth factor–driven inhibition of melanogenesis and modulation of tyrosinase activity. Platelet-rich plasma promotes dermal remodeling through angiogenesis, collagen synthesis, and extracellular matrix production improving skin texture and pigmentation.23 Botulinum toxin A may improve pigmentation by modulating melanogenesis as well as inflammatory and vascular pathways.24
Radiofrequency microneedling provides a dermal-targeting therapeutic approach, with some evidence showing that monthly treatments can help maintain improvements achieved with conventional therapy by modulating photoaged dermal structures impacted by melanogenic signaling.25 Histopathologic correlation studies suggest that microneedling used alone or as a delivery platform alongside topical agents may be beneficial in dermal-predominant disease, while laser-based therapies should be reserved for recalcitrant cases due to the risk for postinflammatory hyperpigmentation and melasma recurrence, particularly in those with darker skin types.26 Lasers such as Q-switched 1064-nm Nd:YAG as well as nonablative lasers used in conservative settings are options for melasma treatment, including in patients with skin of color.26,27 Laser toning with serial low-fluence (<3 J/cm2), large-spot 1064-nm Nd:YAG has been used to reduce inflammation and risk for postinflammatory hyperpigmentation.28 Additionally, randomized split-face data demonstrate that picosecond 1064-nm devices achieve comparable reductions in mMASI scores to traditional nanosecond devices, and combination strategies incorporating intense pulsed light (IPL) have shown greater MASI improvement compared with IPL alone.28,29 However, IPL generally is limited to lighter skin phototypes due to the risk for postinflammatory hyperpigmentation in darker skin.30
Lastly, long-term management requires patient education on the importance of year-round maintenance therapy, consistency, and compliance. Reinforcing adherence to photoprotection, supporting barrier repair, and setting expectations regarding prognosis are essential components to optimizing melasma treatment outcomes.12
Future Insights: Beyond the Current State of Melasma Research and Treatment
Future advances in melasma management likely will focus on improving disease assessment and long-term treatment durability. Tools such as the MASI and mMASI are widely used but are limited by interobserver variability and reduced sensitivity in darker skin types, highlighting the need to incorporate objective measures such as colorimetry.10,26 There also is a need for studies that relate clinical improvement to underlying pathology. Histopathologic correlation remains limited across most therapeutic trials, and more studies should assess long-term outcomes and quality-of-life measures given the relapsing nature of melasma.26
Future interventions will continue to move past the treatment of pigment alone. Increasing recognition of vascular, inflammatory, and barrier-related contributions to melasma, as well as targeting of other cell types affected by melasma, will be important considerations in future treatment innovations.8,11 In summary, improved inclusion of patients with skin of color in clinical trials, expansion of clinical outcomes measures and objective parameters of disease evaluation, novel approaches to treatment and relapse prevention, and greater attention to patient adherence and education will be essential to achieving advancements in melasma care.12
- Sanchez NP, Pathak MA, Sato S, et al. Melasma: a clinical, light microscopic, ultrastructural, and immunofluorescence study. J Am Acad Dermatol. 1981;4:698-710.
- Bostan E, Cakir A. The dermoscopic characteristics of melasma in relation to different skin phototypes, distribution patterns and wood lamp findings: a cross-sectional study of 236 melasma lesions. Arch Dermatol Res. 2023;315:1927-1938.
- Guida S, Longo C, Ronga R, et al. Melasma and reflectance confocal microscopy: from baseline to treatment monitoring. Int J Dermatol. 2024;63:1007-1012.
- Ning X, Yang J, Ouyang H, et al. In vivo evaluation of melasma pathologic features and treatment response by 2-photon microscopy. JAMA Dermatol. 2025;161:1039-1047.
- Chen K-J, Han Y, Wang Z-Y, et al. Submicron resolution techniques: multiphoton microscopy in skin disease. Exp Dermatol. 2023;32:1613-1623.
- Philipp-Dormston WG. Melasma: a step-by-step approach towards a multimodal combination therapy. Clin Cosmet Investig Dermatol. 2024;17:1203-1216.
- Doolan B, Gupta M. Melasma. Aust J Gen Pract. 2021;50:880-885.
- Ali L, Al Niaimi F. Pathogenesis of melasma explained. Int J Dermatol. 2025;64:1201-1212.
- Artzi O, Horovitz T, Bar-Ilan E, et al. The pathogenesis of melasma and implications for treatment. J Cosmet Dermatol. 2021;20:3432-3445.
- Gan C, Rodrigues M. An update on new and existing treatments for the management of melasma. Am J Clin Dermatol. 2024;25:717-733.
- Sarkar R, Desai SR, Sinha S, et al. Delphi consensus on melasma management by international experts and pigmentary disorders society. J Eur Acad Dermatol Venereol. Published online September 25, 2025.
- Desai SR, Alexis AF, Elbuluk N, et al. Best practices in the treatment of melasma with a focus on patients with skin of color. J Am Acad Dermatol. 2024;90:269-279.
- Lim HW, Kohli I, Ruvolo E, et al. Impact of visible light on skin health: the role of antioxidants and free radical quenchers in skin protection. J Am Acad Deramtol. 2022;86(3 suppl):S27-S37.
- Goh CL, Chuah SY, Tien S, et al. Double-blind, placebo-controlled trial to evaluate the effectiveness of polypodium leucotomos extract in the treatment of melasma in Asian skin: a pilot study. J Clin Aesthet Dermatol. 2018;11:14-19.
- Mahajan VK, Patil A, Blicharz L, et al. Medical therapies for melasma. J Cosmet Dermatol. 2022;21:3707-3728.
- Suliman RS, Alhuwayshil J, Almuflehi AA, et al. Emerging topical therapies for melasma: a comparative analysis of efficacy and safety. J Dermatolog Treat. 2025;36:2591502.
- Austin E, Nguyen JK, Jagdeo J. Topical treatments for melasma: a systematic review of randomized controlled trials. J Drugs Dermatol. 2019;18:S1545961619P1156X.
- Grimes PE, Dias S, Oparaugo NC, et al. A randomized, controlled, split-face, double-blind study comparing topical malassezin to hydroquinone 4% for melasma. J Drugs Dermatol. 2026;25:25-29.
- Passeron T, Kerob D, Le Dantec G, et al. Efficacy and tolerability of a new facial 2-mercaptonicotinoyl glycine-containing depigmenting serum versus hydroquinone 4% over 3-month treatment of facial melasma. Dermatol Ther (Heidelb). 2025;15:2379-2390.
- McKesey J, Tovar-Garza A, Pandya AG. Melasma treatment: an evidence-based review. Am J Clin Dermatol. 2020;21:173-225.
- Bala HR, Lee S, Wong C, et al. Oral tranexamic acid for the treatment of melasma: a review. Dermatol Surg. 2018;44:814-825.
- Sarkar R, Katoch S. Chemical peels in treatment of melasma. Dermatol Clin. 2024;42:21-32.
- Sarkar R, Gupta M. Platelet-rich plasma in melasma—a systematic review. Dermatol Surg. 2022;48:131-134.
- Pongklaokam J, Manuskiatti W, Wanitphakdeedecha R, et al. Efficacy and safety of letibotulinum toxin A for the treatment of melasma in two different dilutions: a randomized double-blind split-face study. Toxins (Basel). 2025;17:349.
- Han HJ, Kim JC, Park YJ, et al. Targeting the dermis for melasma maintenance treatment. Sci Rep. 2024;14:949.
- Zhang AD, Lazar M, Akhundova E, et al. A scoping review on melasma treatments and their histopathologic correlates. Dermatopathology (Basel). 2025;12:13.
- Goldman MP, Wu DC, Khetarpal S, et al. Dual 1550-nm erbium glass fiber and 1927-nm thulium fiber non-ablative fractional laser system treatment in patients with skin of color: a review of clinical studies and unmet needs. Lasers Surg Med. Published online February 10, 2026.
- Chen J, Yu N, Peng L, et al. Efficacy of low-fluence 1064 nm Q-switched Nd: YAG laser for the treatment of melasma: a meta-analysis and systematic review. J Cosmet Dermatol. 2022;21.
- Feng J, Huang L. Comparison of picosecond and nanosecond Nd:YAG 1064-nm lasers in the treatment of melasma: a split-face randomized clinical trial. Plast Reconstr Surg. 2023;151:772-777.
- Passeron T, Genedy R, Salah L, et al., Laser treatment of hyperpigmented lesions: position statement of the European Society of Laser in Dermatology. J Eur Acad Dermatol Venereol. 2019;33:987-1005.
- Sanchez NP, Pathak MA, Sato S, et al. Melasma: a clinical, light microscopic, ultrastructural, and immunofluorescence study. J Am Acad Dermatol. 1981;4:698-710.
- Bostan E, Cakir A. The dermoscopic characteristics of melasma in relation to different skin phototypes, distribution patterns and wood lamp findings: a cross-sectional study of 236 melasma lesions. Arch Dermatol Res. 2023;315:1927-1938.
- Guida S, Longo C, Ronga R, et al. Melasma and reflectance confocal microscopy: from baseline to treatment monitoring. Int J Dermatol. 2024;63:1007-1012.
- Ning X, Yang J, Ouyang H, et al. In vivo evaluation of melasma pathologic features and treatment response by 2-photon microscopy. JAMA Dermatol. 2025;161:1039-1047.
- Chen K-J, Han Y, Wang Z-Y, et al. Submicron resolution techniques: multiphoton microscopy in skin disease. Exp Dermatol. 2023;32:1613-1623.
- Philipp-Dormston WG. Melasma: a step-by-step approach towards a multimodal combination therapy. Clin Cosmet Investig Dermatol. 2024;17:1203-1216.
- Doolan B, Gupta M. Melasma. Aust J Gen Pract. 2021;50:880-885.
- Ali L, Al Niaimi F. Pathogenesis of melasma explained. Int J Dermatol. 2025;64:1201-1212.
- Artzi O, Horovitz T, Bar-Ilan E, et al. The pathogenesis of melasma and implications for treatment. J Cosmet Dermatol. 2021;20:3432-3445.
- Gan C, Rodrigues M. An update on new and existing treatments for the management of melasma. Am J Clin Dermatol. 2024;25:717-733.
- Sarkar R, Desai SR, Sinha S, et al. Delphi consensus on melasma management by international experts and pigmentary disorders society. J Eur Acad Dermatol Venereol. Published online September 25, 2025.
- Desai SR, Alexis AF, Elbuluk N, et al. Best practices in the treatment of melasma with a focus on patients with skin of color. J Am Acad Dermatol. 2024;90:269-279.
- Lim HW, Kohli I, Ruvolo E, et al. Impact of visible light on skin health: the role of antioxidants and free radical quenchers in skin protection. J Am Acad Deramtol. 2022;86(3 suppl):S27-S37.
- Goh CL, Chuah SY, Tien S, et al. Double-blind, placebo-controlled trial to evaluate the effectiveness of polypodium leucotomos extract in the treatment of melasma in Asian skin: a pilot study. J Clin Aesthet Dermatol. 2018;11:14-19.
- Mahajan VK, Patil A, Blicharz L, et al. Medical therapies for melasma. J Cosmet Dermatol. 2022;21:3707-3728.
- Suliman RS, Alhuwayshil J, Almuflehi AA, et al. Emerging topical therapies for melasma: a comparative analysis of efficacy and safety. J Dermatolog Treat. 2025;36:2591502.
- Austin E, Nguyen JK, Jagdeo J. Topical treatments for melasma: a systematic review of randomized controlled trials. J Drugs Dermatol. 2019;18:S1545961619P1156X.
- Grimes PE, Dias S, Oparaugo NC, et al. A randomized, controlled, split-face, double-blind study comparing topical malassezin to hydroquinone 4% for melasma. J Drugs Dermatol. 2026;25:25-29.
- Passeron T, Kerob D, Le Dantec G, et al. Efficacy and tolerability of a new facial 2-mercaptonicotinoyl glycine-containing depigmenting serum versus hydroquinone 4% over 3-month treatment of facial melasma. Dermatol Ther (Heidelb). 2025;15:2379-2390.
- McKesey J, Tovar-Garza A, Pandya AG. Melasma treatment: an evidence-based review. Am J Clin Dermatol. 2020;21:173-225.
- Bala HR, Lee S, Wong C, et al. Oral tranexamic acid for the treatment of melasma: a review. Dermatol Surg. 2018;44:814-825.
- Sarkar R, Katoch S. Chemical peels in treatment of melasma. Dermatol Clin. 2024;42:21-32.
- Sarkar R, Gupta M. Platelet-rich plasma in melasma—a systematic review. Dermatol Surg. 2022;48:131-134.
- Pongklaokam J, Manuskiatti W, Wanitphakdeedecha R, et al. Efficacy and safety of letibotulinum toxin A for the treatment of melasma in two different dilutions: a randomized double-blind split-face study. Toxins (Basel). 2025;17:349.
- Han HJ, Kim JC, Park YJ, et al. Targeting the dermis for melasma maintenance treatment. Sci Rep. 2024;14:949.
- Zhang AD, Lazar M, Akhundova E, et al. A scoping review on melasma treatments and their histopathologic correlates. Dermatopathology (Basel). 2025;12:13.
- Goldman MP, Wu DC, Khetarpal S, et al. Dual 1550-nm erbium glass fiber and 1927-nm thulium fiber non-ablative fractional laser system treatment in patients with skin of color: a review of clinical studies and unmet needs. Lasers Surg Med. Published online February 10, 2026.
- Chen J, Yu N, Peng L, et al. Efficacy of low-fluence 1064 nm Q-switched Nd: YAG laser for the treatment of melasma: a meta-analysis and systematic review. J Cosmet Dermatol. 2022;21.
- Feng J, Huang L. Comparison of picosecond and nanosecond Nd:YAG 1064-nm lasers in the treatment of melasma: a split-face randomized clinical trial. Plast Reconstr Surg. 2023;151:772-777.
- Passeron T, Genedy R, Salah L, et al., Laser treatment of hyperpigmented lesions: position statement of the European Society of Laser in Dermatology. J Eur Acad Dermatol Venereol. 2019;33:987-1005.
Beyond Conventional Paradigms: Rethinking the Evaluation and Management of Melasma
Beyond Conventional Paradigms: Rethinking the Evaluation and Management of Melasma

Is Ken Kizer’s Legacy at Risk? The Future of the Veterans Health Administration
Is Ken Kizer’s Legacy at Risk? The Future of the Veterans Health Administration
Mostly it is loss that teaches us about the worth of things.
Arthur Schopenhauer1
One of the leaders I most respected in my US Department of Veterans Affairs (VA) career was a man who had worked his way up through the ranks to become a medical center director. Usually calm, cool, and collected, he would wax poetic when discussing the hero of the VA Health Care System revolution, Ken Kizer, MD, MPH.
In this issue of Federal Practitioner, journalist Randy Dotinga interviews Kizer about the current challenges facing the VA. Though many readers will have participated in or at least know about Kizer’s unprecedented overhaul of the agency, many others, especially those new to VA, may not. It seemed a fitting time to offer an outline of the immense and positive accomplishments that occurred in the agency during his tenure, especially as, under the current administration, many of his most forward-thinking initiatives seem to be moving backward.2
When President Clinton nominated Kizer to serve as the Under Secretary for Health for the Veterans Health Administration in 1994, the poor quality care the agency delivered was castigated in popular movies like Born on the Fourth of July. Veterans who were seen in that era, and who eventually returned to a far better, kinder VA thanks to Kizer, would often tell me, “Doc, the VA was really bad then, and I was afraid to come back.” The critique of VA health care in the mid-1990s sounds like a bureaucratic déjà vu of many of the concerns Kizer raised in his interview, including fragmentation of care, access barriers, and poor coordination of treatment.3
If anyone was prepared and qualified to take on this seeming mission impossible, it was Kizer. A US Navy veteran with 6 board certifications, he came to the VA following a brave and innovative stint as the top health official in California, where he successfully took on the tobacco lobby and dramatically reduced the state’s rates of smoking and related diseases.4
Long before it was the subject of reality TV shows, Kizer dubbed his major renovation of the VA’s antiquated structure an “extreme makeover.”3 Though this description is an oversimplification of Kizer’s monumental efforts, the makeover can be considered in 4 to 6 buckets, depending on how various health policy experts parse the re-engineering efforts.5-7
Decentralization. Kizer instituted the Veterans Integrated Service Network (VISN) system to coordinate the management and operations of all the hospitals, clinics, and other VA health care entities in what is roughly a region. The locus of decision-making shifted from the VA Central Office to the VISNs, intended to promote more efficient, economical, and streamlined health care delivery.
Capitation. Accompanying this restructuring was a shift to a capitated system focused on preventive care. The Veterans Equitable Resource Allocation system was designed to logically link workload and funding. This was a major shift away from VA’s previous emphasis on inpatient and specialty care and resulted in the closing of multiple hospitals.4
Information Systems. I can still remember the first time I sat down at a prehistoric computer to use the Computerized Patient Record System (CPRS). Though now much maligned, then it was like something out of Star Trek, at a time when almost every other health care institution was buried in paper charts. With CPRS, VA suddenly had a pioneering and much-envied electronic medical record that facilitated continuity of care, communication between professionals, and accuracy and completeness of documentation.
Data Driven Performance Improvement. The VISNs and information systems inaugurated a new era of data-driven quality improvement. The assembly and analysis of data enabled VISNs to have real-time input about comparative facility performance.
Performance Measures. The data enabled evidence-based performance measures to be developed and monitored. Though these have now become the bane of many Federal Practitioner readers’ existence, they were originally intended for VISN directors and members of the senior executive service at VA central office. These were tied to incentives that, though recently the subject of watchdog investigation, were intended to motivate and reward high-quality care.6
Even this cursory look at Kizer’s accomplishments is more than enough to demonstrate the magnitude of the makeover, and when the time frame of the achievements is factored in, the transformation is the equivalent of a planet changing its orbit at light speed. Rhetoric aside, there are now hundreds of research articles published in top medical and health policy journals, many of them authored by Kizer,7,8 that have amply demonstrated that when he departed the VA in 1999, it had become “the best care anywhere.” 9 For example, a 2000 New England Journal of Medicine article found that from 1994 to 2000, the percentage of veterans whose care met ≥ 90% of 9 of 17 quality standards was > 70% for 13 of the measures, outperforming fee-for-service Medicare.10
There had been uncertainty about whether Kizer would seek a second term as Under Secretary when he announced that he was leaving. With concise modesty, Kizer said he had met his charge to, “re-engineer the veterans’ health care system so that it could effectively function in the 21st century.”11
Despite openly and critically discussing the many difficulties the VA currently confronts, Kizer ends his interview on a note of hope. Since he likely knows more about VA than any person alive, we need to trust his judgment that his legacy, which currently seems more in jeopardy than ever before, will somehow prevail. Perhaps I am too melancholic, but I believe it will take a professional of the stature of Dr. Kizer to take us back to that future, and I fear we will not see his likes again.
- Schopenhaur A, translated by Saunders TB. Parerga and Paralipomena: A Collection of Philosophical Essays. Cosimo Classics: 2007.
- Spotswood, S. Massive VA restructuring would cut number of VISNS, reduce high-level leadership. U.S. Medicine. January 15, 2026. Accessed March 23, 2026. https://www .usmedicine.com/non-clinical-topics/policy/massive -va-restructuring-would-cut-number-of-visns-reduce-high -level-leadership/
- Kizer KW, Dudley RA. Extreme makeover: transformation of the veterans health ca re system. Annu Rev Public Health. 2009;30:313-339. doi:10.1146/annurev.publhealth.29.020907.090940
- Payne D. How Kizer healed the VA. BMJ. 2012;344:e3324. doi:10.1136/bmj.e3324
- Jha AK. What can the rest of the health care system learn from VA’s quality and safety transformation? Agency for Healthcare Research and Quality. Patient Safety Network. September 1, 2006. Accessed March 23, 2026. https://psnet .ahrq.gov/perspective/what-can-rest-health-care-system -learn-vas-quality-and-safety-transformation
- US Department of Veterans Affairs, Office of Inspector General. VA improperly awarded 10.8 million in incentives to central office senior executives. Report # 23-03773-169. May 9, 2024. Accessed March 23, 2026. https://www.vaoig.gov /reports/administrative-investigation/va-improperly-awarded -108-million-incentives-central-office
- Kizer KW. The “new VA”: a national laboratory for health care quality management. Am J Med Qual. 1999;14:3-20. doi:10.1177/106286069901400103
- Kizer KW, Pane GA. The “new VA”: delivering health care value through integrated service networks. Ann Emerg Med. 1997;30:804-807. doi:10.1016/s0196-0644(97)70053-2
- Longman P. Best Care Anywhere: Why VA Health Care is Better than Yours. 3rd ed. Berrett-Koehler Publishers; 2012.
- Jha AK, Perlin JB, Kizer KW, Dudley RA. Effect of the transformation of the Veterans Affairs Health Care System on the quality of care. N Engl J Med. 2003;348:2218-2227. doi:10.1056/NEJMsa021899
- US Department of Veterans Affairs. Kizer withdraws name from consideration for second term as VA Under Secretary for Health. Vanguard. June/July 1999. Accessed March 23, 2026. https://www.va.gov/opa/publications/archives /vanguard/99junjulvg.pdf
Mostly it is loss that teaches us about the worth of things.
Arthur Schopenhauer1
One of the leaders I most respected in my US Department of Veterans Affairs (VA) career was a man who had worked his way up through the ranks to become a medical center director. Usually calm, cool, and collected, he would wax poetic when discussing the hero of the VA Health Care System revolution, Ken Kizer, MD, MPH.
In this issue of Federal Practitioner, journalist Randy Dotinga interviews Kizer about the current challenges facing the VA. Though many readers will have participated in or at least know about Kizer’s unprecedented overhaul of the agency, many others, especially those new to VA, may not. It seemed a fitting time to offer an outline of the immense and positive accomplishments that occurred in the agency during his tenure, especially as, under the current administration, many of his most forward-thinking initiatives seem to be moving backward.2
When President Clinton nominated Kizer to serve as the Under Secretary for Health for the Veterans Health Administration in 1994, the poor quality care the agency delivered was castigated in popular movies like Born on the Fourth of July. Veterans who were seen in that era, and who eventually returned to a far better, kinder VA thanks to Kizer, would often tell me, “Doc, the VA was really bad then, and I was afraid to come back.” The critique of VA health care in the mid-1990s sounds like a bureaucratic déjà vu of many of the concerns Kizer raised in his interview, including fragmentation of care, access barriers, and poor coordination of treatment.3
If anyone was prepared and qualified to take on this seeming mission impossible, it was Kizer. A US Navy veteran with 6 board certifications, he came to the VA following a brave and innovative stint as the top health official in California, where he successfully took on the tobacco lobby and dramatically reduced the state’s rates of smoking and related diseases.4
Long before it was the subject of reality TV shows, Kizer dubbed his major renovation of the VA’s antiquated structure an “extreme makeover.”3 Though this description is an oversimplification of Kizer’s monumental efforts, the makeover can be considered in 4 to 6 buckets, depending on how various health policy experts parse the re-engineering efforts.5-7
Decentralization. Kizer instituted the Veterans Integrated Service Network (VISN) system to coordinate the management and operations of all the hospitals, clinics, and other VA health care entities in what is roughly a region. The locus of decision-making shifted from the VA Central Office to the VISNs, intended to promote more efficient, economical, and streamlined health care delivery.
Capitation. Accompanying this restructuring was a shift to a capitated system focused on preventive care. The Veterans Equitable Resource Allocation system was designed to logically link workload and funding. This was a major shift away from VA’s previous emphasis on inpatient and specialty care and resulted in the closing of multiple hospitals.4
Information Systems. I can still remember the first time I sat down at a prehistoric computer to use the Computerized Patient Record System (CPRS). Though now much maligned, then it was like something out of Star Trek, at a time when almost every other health care institution was buried in paper charts. With CPRS, VA suddenly had a pioneering and much-envied electronic medical record that facilitated continuity of care, communication between professionals, and accuracy and completeness of documentation.
Data Driven Performance Improvement. The VISNs and information systems inaugurated a new era of data-driven quality improvement. The assembly and analysis of data enabled VISNs to have real-time input about comparative facility performance.
Performance Measures. The data enabled evidence-based performance measures to be developed and monitored. Though these have now become the bane of many Federal Practitioner readers’ existence, they were originally intended for VISN directors and members of the senior executive service at VA central office. These were tied to incentives that, though recently the subject of watchdog investigation, were intended to motivate and reward high-quality care.6
Even this cursory look at Kizer’s accomplishments is more than enough to demonstrate the magnitude of the makeover, and when the time frame of the achievements is factored in, the transformation is the equivalent of a planet changing its orbit at light speed. Rhetoric aside, there are now hundreds of research articles published in top medical and health policy journals, many of them authored by Kizer,7,8 that have amply demonstrated that when he departed the VA in 1999, it had become “the best care anywhere.” 9 For example, a 2000 New England Journal of Medicine article found that from 1994 to 2000, the percentage of veterans whose care met ≥ 90% of 9 of 17 quality standards was > 70% for 13 of the measures, outperforming fee-for-service Medicare.10
There had been uncertainty about whether Kizer would seek a second term as Under Secretary when he announced that he was leaving. With concise modesty, Kizer said he had met his charge to, “re-engineer the veterans’ health care system so that it could effectively function in the 21st century.”11
Despite openly and critically discussing the many difficulties the VA currently confronts, Kizer ends his interview on a note of hope. Since he likely knows more about VA than any person alive, we need to trust his judgment that his legacy, which currently seems more in jeopardy than ever before, will somehow prevail. Perhaps I am too melancholic, but I believe it will take a professional of the stature of Dr. Kizer to take us back to that future, and I fear we will not see his likes again.
Mostly it is loss that teaches us about the worth of things.
Arthur Schopenhauer1
One of the leaders I most respected in my US Department of Veterans Affairs (VA) career was a man who had worked his way up through the ranks to become a medical center director. Usually calm, cool, and collected, he would wax poetic when discussing the hero of the VA Health Care System revolution, Ken Kizer, MD, MPH.
In this issue of Federal Practitioner, journalist Randy Dotinga interviews Kizer about the current challenges facing the VA. Though many readers will have participated in or at least know about Kizer’s unprecedented overhaul of the agency, many others, especially those new to VA, may not. It seemed a fitting time to offer an outline of the immense and positive accomplishments that occurred in the agency during his tenure, especially as, under the current administration, many of his most forward-thinking initiatives seem to be moving backward.2
When President Clinton nominated Kizer to serve as the Under Secretary for Health for the Veterans Health Administration in 1994, the poor quality care the agency delivered was castigated in popular movies like Born on the Fourth of July. Veterans who were seen in that era, and who eventually returned to a far better, kinder VA thanks to Kizer, would often tell me, “Doc, the VA was really bad then, and I was afraid to come back.” The critique of VA health care in the mid-1990s sounds like a bureaucratic déjà vu of many of the concerns Kizer raised in his interview, including fragmentation of care, access barriers, and poor coordination of treatment.3
If anyone was prepared and qualified to take on this seeming mission impossible, it was Kizer. A US Navy veteran with 6 board certifications, he came to the VA following a brave and innovative stint as the top health official in California, where he successfully took on the tobacco lobby and dramatically reduced the state’s rates of smoking and related diseases.4
Long before it was the subject of reality TV shows, Kizer dubbed his major renovation of the VA’s antiquated structure an “extreme makeover.”3 Though this description is an oversimplification of Kizer’s monumental efforts, the makeover can be considered in 4 to 6 buckets, depending on how various health policy experts parse the re-engineering efforts.5-7
Decentralization. Kizer instituted the Veterans Integrated Service Network (VISN) system to coordinate the management and operations of all the hospitals, clinics, and other VA health care entities in what is roughly a region. The locus of decision-making shifted from the VA Central Office to the VISNs, intended to promote more efficient, economical, and streamlined health care delivery.
Capitation. Accompanying this restructuring was a shift to a capitated system focused on preventive care. The Veterans Equitable Resource Allocation system was designed to logically link workload and funding. This was a major shift away from VA’s previous emphasis on inpatient and specialty care and resulted in the closing of multiple hospitals.4
Information Systems. I can still remember the first time I sat down at a prehistoric computer to use the Computerized Patient Record System (CPRS). Though now much maligned, then it was like something out of Star Trek, at a time when almost every other health care institution was buried in paper charts. With CPRS, VA suddenly had a pioneering and much-envied electronic medical record that facilitated continuity of care, communication between professionals, and accuracy and completeness of documentation.
Data Driven Performance Improvement. The VISNs and information systems inaugurated a new era of data-driven quality improvement. The assembly and analysis of data enabled VISNs to have real-time input about comparative facility performance.
Performance Measures. The data enabled evidence-based performance measures to be developed and monitored. Though these have now become the bane of many Federal Practitioner readers’ existence, they were originally intended for VISN directors and members of the senior executive service at VA central office. These were tied to incentives that, though recently the subject of watchdog investigation, were intended to motivate and reward high-quality care.6
Even this cursory look at Kizer’s accomplishments is more than enough to demonstrate the magnitude of the makeover, and when the time frame of the achievements is factored in, the transformation is the equivalent of a planet changing its orbit at light speed. Rhetoric aside, there are now hundreds of research articles published in top medical and health policy journals, many of them authored by Kizer,7,8 that have amply demonstrated that when he departed the VA in 1999, it had become “the best care anywhere.” 9 For example, a 2000 New England Journal of Medicine article found that from 1994 to 2000, the percentage of veterans whose care met ≥ 90% of 9 of 17 quality standards was > 70% for 13 of the measures, outperforming fee-for-service Medicare.10
There had been uncertainty about whether Kizer would seek a second term as Under Secretary when he announced that he was leaving. With concise modesty, Kizer said he had met his charge to, “re-engineer the veterans’ health care system so that it could effectively function in the 21st century.”11
Despite openly and critically discussing the many difficulties the VA currently confronts, Kizer ends his interview on a note of hope. Since he likely knows more about VA than any person alive, we need to trust his judgment that his legacy, which currently seems more in jeopardy than ever before, will somehow prevail. Perhaps I am too melancholic, but I believe it will take a professional of the stature of Dr. Kizer to take us back to that future, and I fear we will not see his likes again.
- Schopenhaur A, translated by Saunders TB. Parerga and Paralipomena: A Collection of Philosophical Essays. Cosimo Classics: 2007.
- Spotswood, S. Massive VA restructuring would cut number of VISNS, reduce high-level leadership. U.S. Medicine. January 15, 2026. Accessed March 23, 2026. https://www .usmedicine.com/non-clinical-topics/policy/massive -va-restructuring-would-cut-number-of-visns-reduce-high -level-leadership/
- Kizer KW, Dudley RA. Extreme makeover: transformation of the veterans health ca re system. Annu Rev Public Health. 2009;30:313-339. doi:10.1146/annurev.publhealth.29.020907.090940
- Payne D. How Kizer healed the VA. BMJ. 2012;344:e3324. doi:10.1136/bmj.e3324
- Jha AK. What can the rest of the health care system learn from VA’s quality and safety transformation? Agency for Healthcare Research and Quality. Patient Safety Network. September 1, 2006. Accessed March 23, 2026. https://psnet .ahrq.gov/perspective/what-can-rest-health-care-system -learn-vas-quality-and-safety-transformation
- US Department of Veterans Affairs, Office of Inspector General. VA improperly awarded 10.8 million in incentives to central office senior executives. Report # 23-03773-169. May 9, 2024. Accessed March 23, 2026. https://www.vaoig.gov /reports/administrative-investigation/va-improperly-awarded -108-million-incentives-central-office
- Kizer KW. The “new VA”: a national laboratory for health care quality management. Am J Med Qual. 1999;14:3-20. doi:10.1177/106286069901400103
- Kizer KW, Pane GA. The “new VA”: delivering health care value through integrated service networks. Ann Emerg Med. 1997;30:804-807. doi:10.1016/s0196-0644(97)70053-2
- Longman P. Best Care Anywhere: Why VA Health Care is Better than Yours. 3rd ed. Berrett-Koehler Publishers; 2012.
- Jha AK, Perlin JB, Kizer KW, Dudley RA. Effect of the transformation of the Veterans Affairs Health Care System on the quality of care. N Engl J Med. 2003;348:2218-2227. doi:10.1056/NEJMsa021899
- US Department of Veterans Affairs. Kizer withdraws name from consideration for second term as VA Under Secretary for Health. Vanguard. June/July 1999. Accessed March 23, 2026. https://www.va.gov/opa/publications/archives /vanguard/99junjulvg.pdf
- Schopenhaur A, translated by Saunders TB. Parerga and Paralipomena: A Collection of Philosophical Essays. Cosimo Classics: 2007.
- Spotswood, S. Massive VA restructuring would cut number of VISNS, reduce high-level leadership. U.S. Medicine. January 15, 2026. Accessed March 23, 2026. https://www .usmedicine.com/non-clinical-topics/policy/massive -va-restructuring-would-cut-number-of-visns-reduce-high -level-leadership/
- Kizer KW, Dudley RA. Extreme makeover: transformation of the veterans health ca re system. Annu Rev Public Health. 2009;30:313-339. doi:10.1146/annurev.publhealth.29.020907.090940
- Payne D. How Kizer healed the VA. BMJ. 2012;344:e3324. doi:10.1136/bmj.e3324
- Jha AK. What can the rest of the health care system learn from VA’s quality and safety transformation? Agency for Healthcare Research and Quality. Patient Safety Network. September 1, 2006. Accessed March 23, 2026. https://psnet .ahrq.gov/perspective/what-can-rest-health-care-system -learn-vas-quality-and-safety-transformation
- US Department of Veterans Affairs, Office of Inspector General. VA improperly awarded 10.8 million in incentives to central office senior executives. Report # 23-03773-169. May 9, 2024. Accessed March 23, 2026. https://www.vaoig.gov /reports/administrative-investigation/va-improperly-awarded -108-million-incentives-central-office
- Kizer KW. The “new VA”: a national laboratory for health care quality management. Am J Med Qual. 1999;14:3-20. doi:10.1177/106286069901400103
- Kizer KW, Pane GA. The “new VA”: delivering health care value through integrated service networks. Ann Emerg Med. 1997;30:804-807. doi:10.1016/s0196-0644(97)70053-2
- Longman P. Best Care Anywhere: Why VA Health Care is Better than Yours. 3rd ed. Berrett-Koehler Publishers; 2012.
- Jha AK, Perlin JB, Kizer KW, Dudley RA. Effect of the transformation of the Veterans Affairs Health Care System on the quality of care. N Engl J Med. 2003;348:2218-2227. doi:10.1056/NEJMsa021899
- US Department of Veterans Affairs. Kizer withdraws name from consideration for second term as VA Under Secretary for Health. Vanguard. June/July 1999. Accessed March 23, 2026. https://www.va.gov/opa/publications/archives /vanguard/99junjulvg.pdf
Is Ken Kizer’s Legacy at Risk? The Future of the Veterans Health Administration
Is Ken Kizer’s Legacy at Risk? The Future of the Veterans Health Administration
The Gap in VA Dental Care is Nothing to Smile About
The Gap in VA Dental Care is Nothing to Smile About
For there was never yet philosopher that could endure the toothache patiently
Much Ado About Nothing by William Shakespeare
Almost anyone who has worked for a long time in a US Department of Veterans Affairs (VA) clinic or hospital has had patients in dire need of dental services who could neither access nor pay for them. I have seen dental problems ranging from older veterans who were nearly edentulous and needed expensive dentures or implants to younger veterans who never had regular dental care and needed a periodontist to save their teeth, to individuals with terrible toothaches that antibiotics could not cure. As Shakespeare quips in Much Ado About Nothing, almost nothing is worse than a toothache.
Many VA primary care practitioners and social workers kept lists of local sliding-scale dentists or arranged for veterans to visit dental and hygiene school clinics for reduced fees. Even when VA dentists were not permitted to see a veteran, many would assist in finding them affordable care in the community. However, that was never enough to meet the oral health needs of veterans. One of the most common complaints of patients who otherwise were pleased with their VA health care was that it did not cover dental services.1
Most veterans qualify for health care and other VA benefits. Dental care is an exception, with only about a quarter (26%) of the > 9 million veterans active in the Veterans Health Administration (VHA) eligible for care. Even under this restricted eligibility, about 888,000 veterans have received dental services either through the VHA or in the community. In 2025, the VA paid community-based dentists for > 3.5 million procedures for veterans, which underscores the magnitude of the demand.2
Given the gap in dental care, many veterans and their caregivers both personal and professional will likely be encouraged that in February the VA announced plans to improve access to dental care through expanding community care dental services. “Dental health is a critical component of overall well-being,” VA Secretary Doug Collins noted. VA issued a request for proposals (RFP) for a new dental administrator who would oversee the operations of a new network of dental practitioners. The new vendor contract would operationalize general dental services, like tooth extractions, as well as specialized services such as periodontics, dentures, and pharmacy support for dental medications. Most importantly, the new program would cover preventive care to help avoid many of the dental problems veterans now experience. Proposals are due March 16.2
Yet, there is a catch. The community care program will only be available to eligible veterans just like previous dental services both in the VA and the community. I was always somewhat ashamed that despite my working decades at the VHA, I never had a satisfactory answer for veterans who asked me why they were not eligible for dental care. The regulatory response is that eligibility for dental services is a complex determination depending on service-connected military service, and specialized clinical indices. Dental coverage is provided for veterans who have 100% service-connected or total disability, prisoners of war, and veterans whose dental disease exacerbates a comorbid medical condition. Those not eligible for VA dental coverage may still get treatment if they, for example, have a cancer diagnosis and without dental work the chemotherapy treatment would place them at a higher risk of an oral infection. Veterans participating in a rehabilitation program who have poor dentition that prevents them from reaching their rehabilitative goals also may receive VA dental care. In addition, some veterans who are experiencing homelessness and others who did not receive a dental examination prior to discharge from active duty may be eligible for dental benefits.3 VA also offers lower-priced dental insurance for ineligible veterans.4
The new RFP does little to expand eligibility of veterans to receive VA dental care, and it is hard to not see the announcement as another step in the privatization of VHA. Medically and ethically, it seems to perpetuate a double standard between physical and oral health that makes no scientific sense.5-7 I sometimes joke that in medical school we had maybe 2 days of teaching about teeth and even that limited exposure to dental pathology was sufficient for us to learn that chronic conditions like respiratory disease and lifestyle choices like poor diet cause and contribute to dental problems.
Like so many areas of veteran care, dental health in veterans is worse compared with those who never served, making it harder to justify the exclusion of dental services from veteran health benefits. A study in Military Medicine looked at 11,539 former service members and found a higher prevalence of individuals with tooth decay, missing teeth, tooth fillings, caries, and periodontitis. While military service per se was not associated with the findings, higher rates of hypertension, hyperlipidemia, depression, and diabetes in veterans compared with nonveterans, which are related to serving in uniform, were covariates.8
That depression is an indirect factor in dental disease may seem surprising. However, this is more evidence that human health is truly holistic, with mutual interactions between the body (including the teeth) and mind. Oral care needs to be incorporated into the VA whole health approach for all veterans. In a series of articles in Psychiatric News, VA psychiatrist Antoinette Shappell and VA dentist Pierre Cartier identify several links between dental and mental health.9,10 Veterans with anxiety disorders may fear going to the dentist even when care is needed. Serious mental illness may result in poor diet, and difficulty performing preventive care. Many psychotropic medications may cause xerostomia that worsens tooth decay and veterans with posttraumatic stress disorder may suffer from bruxism. I regularly saw these conditions when I worked in a primary care psychiatry clinic. Being able to coordinate with VA dentists and staff to provide integrated care would have benefited these already burdened veterans.
An estimated $5.4 billion has been spent on 3.6 million veterans who were seen in emergency departments for dental problems. That cost alone should convince policy makers that the deficit in VA dental care needs to be filled with efficacious high-quality comprehensive dental services for as many veterans as possible. And there are signs that is exactly what is happening in Congress. A bill in the House of Representatives proposes to expand dental care benefits to all veterans eligible for other VA health benefits.11 There are also other legislative initiatives in the works.4 Together with the VA’s plans for a new community care dental network, that does give veterans and federal practitioners something to smile about.
- Shane L III. A dental debacle: why veterans struggle to navigate VA’s oral care. Military Times. June 17, 2024. Accessed February 25, 2026. https://www.militarytimes.com/news/your-military/2024/06/17/a-dental-debacle-why-veterans-struggle-to-navigate-vas-oral-care/
- US Dept of Veterans Affairs Office of Media Relations. VA moves to improve dental care access to eligible veterans. VA News. February 18, 2026. Accessed February 23, 2026. https://news.va.gov/145117/va-improve-dental-care-access-eligible-veterans/
- Wile B. VA launches plans to expand dental care access for veterans. Military.com. February 16, 2026. Accessed February 23, 2026. https://www.military.com/benefits/veterans-healthcare/va-launches-plan-expand-dental-care-access-veterans.html
- US Department of Veterans Affairs. VA Dental Insurance Program (VADIP). Updated May 1, 2024. Accessed February 23, 2026. https://www.va.gov/health-care/about-va-health-benefits/dental-care/dental-insurance/
- McMains V. Healthy mouth, healthy body. National Institutes of Health, National Institute of Dental and Craniofacial Research. May 8, 2024. Accessed February 23, 2026. https:// www.nidcr.nih.gov/news-events/nidcr-news/2024/healthy-mouth-healthy-body
- Seymour GJ. Good oral health is essential for good general health: the oral–systemic connection. Clin Microbiol Infect. 2007;13:1-2. doi:10.1111/j.1469-0691.2007.01797.x
- Martin SA, Simon L. Oral health and medicine integration: overcoming historical artifact to relieve suffering. Am J Public Health. 2017;107:S30-S31. doi:10.2105/AJPH.2017.303683
- Schindler DK, Lopez Mitnik GV, Solivan-Ortiz DC, et al. Oral health status among adults with and without prior active duty service in the US Armed Forces, NHANES 2011-2014. Mil Med. 2021;186:e149-e159. doi:10.1093/milmed/usaa355
- Shappell AV, Cartier PM. Understanding the mental-dental health connection said to be integral to patient care. Psychiatr News. 2023;58. doi:10.1176/appi.pn.2023.07.6.15
- Shappell AV, Cartier PM. Good ‘mental-dental’ health important in preventing, slowing dementia. Psychiatr News. 2023;58. doi:10.1176/appi.pn.2023.08.8.64
- Dental Care for Veterans Act, HR 210, 119th Cong (2025- 2026). Accessed February 23, 2026. https://www.congress.gov/bill/119th-congress/house-bill/210
For there was never yet philosopher that could endure the toothache patiently
Much Ado About Nothing by William Shakespeare
Almost anyone who has worked for a long time in a US Department of Veterans Affairs (VA) clinic or hospital has had patients in dire need of dental services who could neither access nor pay for them. I have seen dental problems ranging from older veterans who were nearly edentulous and needed expensive dentures or implants to younger veterans who never had regular dental care and needed a periodontist to save their teeth, to individuals with terrible toothaches that antibiotics could not cure. As Shakespeare quips in Much Ado About Nothing, almost nothing is worse than a toothache.
Many VA primary care practitioners and social workers kept lists of local sliding-scale dentists or arranged for veterans to visit dental and hygiene school clinics for reduced fees. Even when VA dentists were not permitted to see a veteran, many would assist in finding them affordable care in the community. However, that was never enough to meet the oral health needs of veterans. One of the most common complaints of patients who otherwise were pleased with their VA health care was that it did not cover dental services.1
Most veterans qualify for health care and other VA benefits. Dental care is an exception, with only about a quarter (26%) of the > 9 million veterans active in the Veterans Health Administration (VHA) eligible for care. Even under this restricted eligibility, about 888,000 veterans have received dental services either through the VHA or in the community. In 2025, the VA paid community-based dentists for > 3.5 million procedures for veterans, which underscores the magnitude of the demand.2
Given the gap in dental care, many veterans and their caregivers both personal and professional will likely be encouraged that in February the VA announced plans to improve access to dental care through expanding community care dental services. “Dental health is a critical component of overall well-being,” VA Secretary Doug Collins noted. VA issued a request for proposals (RFP) for a new dental administrator who would oversee the operations of a new network of dental practitioners. The new vendor contract would operationalize general dental services, like tooth extractions, as well as specialized services such as periodontics, dentures, and pharmacy support for dental medications. Most importantly, the new program would cover preventive care to help avoid many of the dental problems veterans now experience. Proposals are due March 16.2
Yet, there is a catch. The community care program will only be available to eligible veterans just like previous dental services both in the VA and the community. I was always somewhat ashamed that despite my working decades at the VHA, I never had a satisfactory answer for veterans who asked me why they were not eligible for dental care. The regulatory response is that eligibility for dental services is a complex determination depending on service-connected military service, and specialized clinical indices. Dental coverage is provided for veterans who have 100% service-connected or total disability, prisoners of war, and veterans whose dental disease exacerbates a comorbid medical condition. Those not eligible for VA dental coverage may still get treatment if they, for example, have a cancer diagnosis and without dental work the chemotherapy treatment would place them at a higher risk of an oral infection. Veterans participating in a rehabilitation program who have poor dentition that prevents them from reaching their rehabilitative goals also may receive VA dental care. In addition, some veterans who are experiencing homelessness and others who did not receive a dental examination prior to discharge from active duty may be eligible for dental benefits.3 VA also offers lower-priced dental insurance for ineligible veterans.4
The new RFP does little to expand eligibility of veterans to receive VA dental care, and it is hard to not see the announcement as another step in the privatization of VHA. Medically and ethically, it seems to perpetuate a double standard between physical and oral health that makes no scientific sense.5-7 I sometimes joke that in medical school we had maybe 2 days of teaching about teeth and even that limited exposure to dental pathology was sufficient for us to learn that chronic conditions like respiratory disease and lifestyle choices like poor diet cause and contribute to dental problems.
Like so many areas of veteran care, dental health in veterans is worse compared with those who never served, making it harder to justify the exclusion of dental services from veteran health benefits. A study in Military Medicine looked at 11,539 former service members and found a higher prevalence of individuals with tooth decay, missing teeth, tooth fillings, caries, and periodontitis. While military service per se was not associated with the findings, higher rates of hypertension, hyperlipidemia, depression, and diabetes in veterans compared with nonveterans, which are related to serving in uniform, were covariates.8
That depression is an indirect factor in dental disease may seem surprising. However, this is more evidence that human health is truly holistic, with mutual interactions between the body (including the teeth) and mind. Oral care needs to be incorporated into the VA whole health approach for all veterans. In a series of articles in Psychiatric News, VA psychiatrist Antoinette Shappell and VA dentist Pierre Cartier identify several links between dental and mental health.9,10 Veterans with anxiety disorders may fear going to the dentist even when care is needed. Serious mental illness may result in poor diet, and difficulty performing preventive care. Many psychotropic medications may cause xerostomia that worsens tooth decay and veterans with posttraumatic stress disorder may suffer from bruxism. I regularly saw these conditions when I worked in a primary care psychiatry clinic. Being able to coordinate with VA dentists and staff to provide integrated care would have benefited these already burdened veterans.
An estimated $5.4 billion has been spent on 3.6 million veterans who were seen in emergency departments for dental problems. That cost alone should convince policy makers that the deficit in VA dental care needs to be filled with efficacious high-quality comprehensive dental services for as many veterans as possible. And there are signs that is exactly what is happening in Congress. A bill in the House of Representatives proposes to expand dental care benefits to all veterans eligible for other VA health benefits.11 There are also other legislative initiatives in the works.4 Together with the VA’s plans for a new community care dental network, that does give veterans and federal practitioners something to smile about.
For there was never yet philosopher that could endure the toothache patiently
Much Ado About Nothing by William Shakespeare
Almost anyone who has worked for a long time in a US Department of Veterans Affairs (VA) clinic or hospital has had patients in dire need of dental services who could neither access nor pay for them. I have seen dental problems ranging from older veterans who were nearly edentulous and needed expensive dentures or implants to younger veterans who never had regular dental care and needed a periodontist to save their teeth, to individuals with terrible toothaches that antibiotics could not cure. As Shakespeare quips in Much Ado About Nothing, almost nothing is worse than a toothache.
Many VA primary care practitioners and social workers kept lists of local sliding-scale dentists or arranged for veterans to visit dental and hygiene school clinics for reduced fees. Even when VA dentists were not permitted to see a veteran, many would assist in finding them affordable care in the community. However, that was never enough to meet the oral health needs of veterans. One of the most common complaints of patients who otherwise were pleased with their VA health care was that it did not cover dental services.1
Most veterans qualify for health care and other VA benefits. Dental care is an exception, with only about a quarter (26%) of the > 9 million veterans active in the Veterans Health Administration (VHA) eligible for care. Even under this restricted eligibility, about 888,000 veterans have received dental services either through the VHA or in the community. In 2025, the VA paid community-based dentists for > 3.5 million procedures for veterans, which underscores the magnitude of the demand.2
Given the gap in dental care, many veterans and their caregivers both personal and professional will likely be encouraged that in February the VA announced plans to improve access to dental care through expanding community care dental services. “Dental health is a critical component of overall well-being,” VA Secretary Doug Collins noted. VA issued a request for proposals (RFP) for a new dental administrator who would oversee the operations of a new network of dental practitioners. The new vendor contract would operationalize general dental services, like tooth extractions, as well as specialized services such as periodontics, dentures, and pharmacy support for dental medications. Most importantly, the new program would cover preventive care to help avoid many of the dental problems veterans now experience. Proposals are due March 16.2
Yet, there is a catch. The community care program will only be available to eligible veterans just like previous dental services both in the VA and the community. I was always somewhat ashamed that despite my working decades at the VHA, I never had a satisfactory answer for veterans who asked me why they were not eligible for dental care. The regulatory response is that eligibility for dental services is a complex determination depending on service-connected military service, and specialized clinical indices. Dental coverage is provided for veterans who have 100% service-connected or total disability, prisoners of war, and veterans whose dental disease exacerbates a comorbid medical condition. Those not eligible for VA dental coverage may still get treatment if they, for example, have a cancer diagnosis and without dental work the chemotherapy treatment would place them at a higher risk of an oral infection. Veterans participating in a rehabilitation program who have poor dentition that prevents them from reaching their rehabilitative goals also may receive VA dental care. In addition, some veterans who are experiencing homelessness and others who did not receive a dental examination prior to discharge from active duty may be eligible for dental benefits.3 VA also offers lower-priced dental insurance for ineligible veterans.4
The new RFP does little to expand eligibility of veterans to receive VA dental care, and it is hard to not see the announcement as another step in the privatization of VHA. Medically and ethically, it seems to perpetuate a double standard between physical and oral health that makes no scientific sense.5-7 I sometimes joke that in medical school we had maybe 2 days of teaching about teeth and even that limited exposure to dental pathology was sufficient for us to learn that chronic conditions like respiratory disease and lifestyle choices like poor diet cause and contribute to dental problems.
Like so many areas of veteran care, dental health in veterans is worse compared with those who never served, making it harder to justify the exclusion of dental services from veteran health benefits. A study in Military Medicine looked at 11,539 former service members and found a higher prevalence of individuals with tooth decay, missing teeth, tooth fillings, caries, and periodontitis. While military service per se was not associated with the findings, higher rates of hypertension, hyperlipidemia, depression, and diabetes in veterans compared with nonveterans, which are related to serving in uniform, were covariates.8
That depression is an indirect factor in dental disease may seem surprising. However, this is more evidence that human health is truly holistic, with mutual interactions between the body (including the teeth) and mind. Oral care needs to be incorporated into the VA whole health approach for all veterans. In a series of articles in Psychiatric News, VA psychiatrist Antoinette Shappell and VA dentist Pierre Cartier identify several links between dental and mental health.9,10 Veterans with anxiety disorders may fear going to the dentist even when care is needed. Serious mental illness may result in poor diet, and difficulty performing preventive care. Many psychotropic medications may cause xerostomia that worsens tooth decay and veterans with posttraumatic stress disorder may suffer from bruxism. I regularly saw these conditions when I worked in a primary care psychiatry clinic. Being able to coordinate with VA dentists and staff to provide integrated care would have benefited these already burdened veterans.
An estimated $5.4 billion has been spent on 3.6 million veterans who were seen in emergency departments for dental problems. That cost alone should convince policy makers that the deficit in VA dental care needs to be filled with efficacious high-quality comprehensive dental services for as many veterans as possible. And there are signs that is exactly what is happening in Congress. A bill in the House of Representatives proposes to expand dental care benefits to all veterans eligible for other VA health benefits.11 There are also other legislative initiatives in the works.4 Together with the VA’s plans for a new community care dental network, that does give veterans and federal practitioners something to smile about.
- Shane L III. A dental debacle: why veterans struggle to navigate VA’s oral care. Military Times. June 17, 2024. Accessed February 25, 2026. https://www.militarytimes.com/news/your-military/2024/06/17/a-dental-debacle-why-veterans-struggle-to-navigate-vas-oral-care/
- US Dept of Veterans Affairs Office of Media Relations. VA moves to improve dental care access to eligible veterans. VA News. February 18, 2026. Accessed February 23, 2026. https://news.va.gov/145117/va-improve-dental-care-access-eligible-veterans/
- Wile B. VA launches plans to expand dental care access for veterans. Military.com. February 16, 2026. Accessed February 23, 2026. https://www.military.com/benefits/veterans-healthcare/va-launches-plan-expand-dental-care-access-veterans.html
- US Department of Veterans Affairs. VA Dental Insurance Program (VADIP). Updated May 1, 2024. Accessed February 23, 2026. https://www.va.gov/health-care/about-va-health-benefits/dental-care/dental-insurance/
- McMains V. Healthy mouth, healthy body. National Institutes of Health, National Institute of Dental and Craniofacial Research. May 8, 2024. Accessed February 23, 2026. https:// www.nidcr.nih.gov/news-events/nidcr-news/2024/healthy-mouth-healthy-body
- Seymour GJ. Good oral health is essential for good general health: the oral–systemic connection. Clin Microbiol Infect. 2007;13:1-2. doi:10.1111/j.1469-0691.2007.01797.x
- Martin SA, Simon L. Oral health and medicine integration: overcoming historical artifact to relieve suffering. Am J Public Health. 2017;107:S30-S31. doi:10.2105/AJPH.2017.303683
- Schindler DK, Lopez Mitnik GV, Solivan-Ortiz DC, et al. Oral health status among adults with and without prior active duty service in the US Armed Forces, NHANES 2011-2014. Mil Med. 2021;186:e149-e159. doi:10.1093/milmed/usaa355
- Shappell AV, Cartier PM. Understanding the mental-dental health connection said to be integral to patient care. Psychiatr News. 2023;58. doi:10.1176/appi.pn.2023.07.6.15
- Shappell AV, Cartier PM. Good ‘mental-dental’ health important in preventing, slowing dementia. Psychiatr News. 2023;58. doi:10.1176/appi.pn.2023.08.8.64
- Dental Care for Veterans Act, HR 210, 119th Cong (2025- 2026). Accessed February 23, 2026. https://www.congress.gov/bill/119th-congress/house-bill/210
- Shane L III. A dental debacle: why veterans struggle to navigate VA’s oral care. Military Times. June 17, 2024. Accessed February 25, 2026. https://www.militarytimes.com/news/your-military/2024/06/17/a-dental-debacle-why-veterans-struggle-to-navigate-vas-oral-care/
- US Dept of Veterans Affairs Office of Media Relations. VA moves to improve dental care access to eligible veterans. VA News. February 18, 2026. Accessed February 23, 2026. https://news.va.gov/145117/va-improve-dental-care-access-eligible-veterans/
- Wile B. VA launches plans to expand dental care access for veterans. Military.com. February 16, 2026. Accessed February 23, 2026. https://www.military.com/benefits/veterans-healthcare/va-launches-plan-expand-dental-care-access-veterans.html
- US Department of Veterans Affairs. VA Dental Insurance Program (VADIP). Updated May 1, 2024. Accessed February 23, 2026. https://www.va.gov/health-care/about-va-health-benefits/dental-care/dental-insurance/
- McMains V. Healthy mouth, healthy body. National Institutes of Health, National Institute of Dental and Craniofacial Research. May 8, 2024. Accessed February 23, 2026. https:// www.nidcr.nih.gov/news-events/nidcr-news/2024/healthy-mouth-healthy-body
- Seymour GJ. Good oral health is essential for good general health: the oral–systemic connection. Clin Microbiol Infect. 2007;13:1-2. doi:10.1111/j.1469-0691.2007.01797.x
- Martin SA, Simon L. Oral health and medicine integration: overcoming historical artifact to relieve suffering. Am J Public Health. 2017;107:S30-S31. doi:10.2105/AJPH.2017.303683
- Schindler DK, Lopez Mitnik GV, Solivan-Ortiz DC, et al. Oral health status among adults with and without prior active duty service in the US Armed Forces, NHANES 2011-2014. Mil Med. 2021;186:e149-e159. doi:10.1093/milmed/usaa355
- Shappell AV, Cartier PM. Understanding the mental-dental health connection said to be integral to patient care. Psychiatr News. 2023;58. doi:10.1176/appi.pn.2023.07.6.15
- Shappell AV, Cartier PM. Good ‘mental-dental’ health important in preventing, slowing dementia. Psychiatr News. 2023;58. doi:10.1176/appi.pn.2023.08.8.64
- Dental Care for Veterans Act, HR 210, 119th Cong (2025- 2026). Accessed February 23, 2026. https://www.congress.gov/bill/119th-congress/house-bill/210
The Gap in VA Dental Care is Nothing to Smile About
The Gap in VA Dental Care is Nothing to Smile About
Scarring Alopecia in Skin of Color: Practical Guidance From Dr. Amy J. McMichael
Scarring Alopecia in Skin of Color: Practical Guidance From Dr. Amy J. McMichael
How do you distinguish active cicatricial alopecia from chronic nonprogressive hair loss in patients with skin of color, and which clinical or trichoscopic features suggest ongoing inflammation requiring treatment?
DR. McMICHAEL: Typically, I use trichoscopy to help determine if there are fine or vellus hairs in the affected area. Often, if there are vellus hairs, that means there is the potential to lengthen growth time and have thicker longer hairs in the area, even in a chronic nonprogressive hair loss state. If there is clinical or trichoscopic erythema (suggesting inflammation), that is a sure sign of active scarring. Patient-reported symptoms of itch, stinging, or pain are a sign of active scarring as well. Finally, even if none of the above are true, a biopsy can help determine if there is active inflammation, as can increasing size of the affected area on the scalp upon return visit to the clinic.
What is your initial diagnostic workup for suspected scarring alopecia in patients with skin of color, including key history, trichoscopy, and biopsy approach?
DR. McMICHAEL: In terms of historical info, I want to know how long the patient has had hair loss, what symptoms they have/had, and if there is a family history of hair loss. Also, if the patient has been treated in the past, it is helpful to know if any of the previous treatments worked. For me, the clinical exam is going to tell the most. Just the clinical location will give the first cues, followed by trichoscopy. I don’t biopsy every patient, but when there is any doubt about the form of hair loss the patient has, biopsy is important. I use the dermatoscope to guide the biopsy and perform two 4-mm punch biopsies in the appropriate area.
How do you manage active inflammatory scarring alopecias in skin of color, including first-line therapies and criteria for escalation?
DR. McMICHAEL: I like to discuss and give guidance on hair care first. Sometimes this will include increased frequency of hair washing and/or use of an antidandruff shampoo. Next, I usually start patients on a potent or ultrapotent steroid several times per week. If there is very symptomatic or clinically raging inflammation, I will begin either an oral antibiotic for 3 to 6 months or a series of intralesional steroids. Depending on the condition and patient preference, a stronger anti-inflammatory agent such as hydroxychloroquine, methotrexate, or dapsone may be used. Monitoring depends on the medication that is started. Many of the anti-inflammatory medications require laboratory monitoring every 4 or 6 months, and the drug dictates this timing. For monitoring of disease progression, questions for the patient on continued symptoms and serial clinical and trichoscopic photographs make the difference.
When and how do you use adjunctive or emerging therapies for scarring alopecias in skin of color, and what evidence and outcomes guide their use?
DR. McMICHAEL: Our research group has shown via small clinical trials and case series that both platelet-rich plasma and low-level laser light can be helpful for central centrifugal cicatricial alopecia, so I tend to begin these treatments once the inflammation is at a mild or minimal level. I often begin low-dose oral minoxidil right at the start or at any time during the course of treatment. I do not use topical minoxidil when the patient is symptomatic but often use this when patients are asymptomatic and do not wish to take oral minoxidil. There are now good case series to show minoxidil can be helpful for scarring forms of alopecia. Patients can show improvement on these treatments, but I only promise stabilization. It is difficult to predict who will have increased growth prior to treatment, and that is what I tell patients.
When are surgical options appropriate for scarring alopecia in patients with skin of color, and what precautions or criteria are required?
DR. McMICHAEL: Once everything has been done medically for scarring alopecia, surgical options can be considered. Unfortunately, these options typically are not covered by insurance, so patients have to be willing and able to pay out of pocket. Other criteria include that patients must have quiescent inflammation and enough donor hair for hair restoration via transplant. I do not personally perform hair transplantation, but I do like to refer patients with tightly coiled hair and scarring alopecia to physicians who specialize in this kind of treatment. Not all transplant surgeons have experience with skin of color or follicular unit extraction, which is sometimes needed.
What culturally tailored strategies help prevent scarring alopecia in patients with skin of color, and where are research or practice gaps?
DR. McMICHAEL: For all patients, it is important to ask about daily hair care practices, hair care at the salon, and night-time hair care before making recommendations. Any hair style that puts tension on the hair shaft needs to be discontinued as do those that are tight around the frontal or posterior hair line. Hair washing should be once per week or every 2 weeks at the least, and conditioning of the hair is important with hair trims every 2 to 3 months.
How do you distinguish active cicatricial alopecia from chronic nonprogressive hair loss in patients with skin of color, and which clinical or trichoscopic features suggest ongoing inflammation requiring treatment?
DR. McMICHAEL: Typically, I use trichoscopy to help determine if there are fine or vellus hairs in the affected area. Often, if there are vellus hairs, that means there is the potential to lengthen growth time and have thicker longer hairs in the area, even in a chronic nonprogressive hair loss state. If there is clinical or trichoscopic erythema (suggesting inflammation), that is a sure sign of active scarring. Patient-reported symptoms of itch, stinging, or pain are a sign of active scarring as well. Finally, even if none of the above are true, a biopsy can help determine if there is active inflammation, as can increasing size of the affected area on the scalp upon return visit to the clinic.
What is your initial diagnostic workup for suspected scarring alopecia in patients with skin of color, including key history, trichoscopy, and biopsy approach?
DR. McMICHAEL: In terms of historical info, I want to know how long the patient has had hair loss, what symptoms they have/had, and if there is a family history of hair loss. Also, if the patient has been treated in the past, it is helpful to know if any of the previous treatments worked. For me, the clinical exam is going to tell the most. Just the clinical location will give the first cues, followed by trichoscopy. I don’t biopsy every patient, but when there is any doubt about the form of hair loss the patient has, biopsy is important. I use the dermatoscope to guide the biopsy and perform two 4-mm punch biopsies in the appropriate area.
How do you manage active inflammatory scarring alopecias in skin of color, including first-line therapies and criteria for escalation?
DR. McMICHAEL: I like to discuss and give guidance on hair care first. Sometimes this will include increased frequency of hair washing and/or use of an antidandruff shampoo. Next, I usually start patients on a potent or ultrapotent steroid several times per week. If there is very symptomatic or clinically raging inflammation, I will begin either an oral antibiotic for 3 to 6 months or a series of intralesional steroids. Depending on the condition and patient preference, a stronger anti-inflammatory agent such as hydroxychloroquine, methotrexate, or dapsone may be used. Monitoring depends on the medication that is started. Many of the anti-inflammatory medications require laboratory monitoring every 4 or 6 months, and the drug dictates this timing. For monitoring of disease progression, questions for the patient on continued symptoms and serial clinical and trichoscopic photographs make the difference.
When and how do you use adjunctive or emerging therapies for scarring alopecias in skin of color, and what evidence and outcomes guide their use?
DR. McMICHAEL: Our research group has shown via small clinical trials and case series that both platelet-rich plasma and low-level laser light can be helpful for central centrifugal cicatricial alopecia, so I tend to begin these treatments once the inflammation is at a mild or minimal level. I often begin low-dose oral minoxidil right at the start or at any time during the course of treatment. I do not use topical minoxidil when the patient is symptomatic but often use this when patients are asymptomatic and do not wish to take oral minoxidil. There are now good case series to show minoxidil can be helpful for scarring forms of alopecia. Patients can show improvement on these treatments, but I only promise stabilization. It is difficult to predict who will have increased growth prior to treatment, and that is what I tell patients.
When are surgical options appropriate for scarring alopecia in patients with skin of color, and what precautions or criteria are required?
DR. McMICHAEL: Once everything has been done medically for scarring alopecia, surgical options can be considered. Unfortunately, these options typically are not covered by insurance, so patients have to be willing and able to pay out of pocket. Other criteria include that patients must have quiescent inflammation and enough donor hair for hair restoration via transplant. I do not personally perform hair transplantation, but I do like to refer patients with tightly coiled hair and scarring alopecia to physicians who specialize in this kind of treatment. Not all transplant surgeons have experience with skin of color or follicular unit extraction, which is sometimes needed.
What culturally tailored strategies help prevent scarring alopecia in patients with skin of color, and where are research or practice gaps?
DR. McMICHAEL: For all patients, it is important to ask about daily hair care practices, hair care at the salon, and night-time hair care before making recommendations. Any hair style that puts tension on the hair shaft needs to be discontinued as do those that are tight around the frontal or posterior hair line. Hair washing should be once per week or every 2 weeks at the least, and conditioning of the hair is important with hair trims every 2 to 3 months.
How do you distinguish active cicatricial alopecia from chronic nonprogressive hair loss in patients with skin of color, and which clinical or trichoscopic features suggest ongoing inflammation requiring treatment?
DR. McMICHAEL: Typically, I use trichoscopy to help determine if there are fine or vellus hairs in the affected area. Often, if there are vellus hairs, that means there is the potential to lengthen growth time and have thicker longer hairs in the area, even in a chronic nonprogressive hair loss state. If there is clinical or trichoscopic erythema (suggesting inflammation), that is a sure sign of active scarring. Patient-reported symptoms of itch, stinging, or pain are a sign of active scarring as well. Finally, even if none of the above are true, a biopsy can help determine if there is active inflammation, as can increasing size of the affected area on the scalp upon return visit to the clinic.
What is your initial diagnostic workup for suspected scarring alopecia in patients with skin of color, including key history, trichoscopy, and biopsy approach?
DR. McMICHAEL: In terms of historical info, I want to know how long the patient has had hair loss, what symptoms they have/had, and if there is a family history of hair loss. Also, if the patient has been treated in the past, it is helpful to know if any of the previous treatments worked. For me, the clinical exam is going to tell the most. Just the clinical location will give the first cues, followed by trichoscopy. I don’t biopsy every patient, but when there is any doubt about the form of hair loss the patient has, biopsy is important. I use the dermatoscope to guide the biopsy and perform two 4-mm punch biopsies in the appropriate area.
How do you manage active inflammatory scarring alopecias in skin of color, including first-line therapies and criteria for escalation?
DR. McMICHAEL: I like to discuss and give guidance on hair care first. Sometimes this will include increased frequency of hair washing and/or use of an antidandruff shampoo. Next, I usually start patients on a potent or ultrapotent steroid several times per week. If there is very symptomatic or clinically raging inflammation, I will begin either an oral antibiotic for 3 to 6 months or a series of intralesional steroids. Depending on the condition and patient preference, a stronger anti-inflammatory agent such as hydroxychloroquine, methotrexate, or dapsone may be used. Monitoring depends on the medication that is started. Many of the anti-inflammatory medications require laboratory monitoring every 4 or 6 months, and the drug dictates this timing. For monitoring of disease progression, questions for the patient on continued symptoms and serial clinical and trichoscopic photographs make the difference.
When and how do you use adjunctive or emerging therapies for scarring alopecias in skin of color, and what evidence and outcomes guide their use?
DR. McMICHAEL: Our research group has shown via small clinical trials and case series that both platelet-rich plasma and low-level laser light can be helpful for central centrifugal cicatricial alopecia, so I tend to begin these treatments once the inflammation is at a mild or minimal level. I often begin low-dose oral minoxidil right at the start or at any time during the course of treatment. I do not use topical minoxidil when the patient is symptomatic but often use this when patients are asymptomatic and do not wish to take oral minoxidil. There are now good case series to show minoxidil can be helpful for scarring forms of alopecia. Patients can show improvement on these treatments, but I only promise stabilization. It is difficult to predict who will have increased growth prior to treatment, and that is what I tell patients.
When are surgical options appropriate for scarring alopecia in patients with skin of color, and what precautions or criteria are required?
DR. McMICHAEL: Once everything has been done medically for scarring alopecia, surgical options can be considered. Unfortunately, these options typically are not covered by insurance, so patients have to be willing and able to pay out of pocket. Other criteria include that patients must have quiescent inflammation and enough donor hair for hair restoration via transplant. I do not personally perform hair transplantation, but I do like to refer patients with tightly coiled hair and scarring alopecia to physicians who specialize in this kind of treatment. Not all transplant surgeons have experience with skin of color or follicular unit extraction, which is sometimes needed.
What culturally tailored strategies help prevent scarring alopecia in patients with skin of color, and where are research or practice gaps?
DR. McMICHAEL: For all patients, it is important to ask about daily hair care practices, hair care at the salon, and night-time hair care before making recommendations. Any hair style that puts tension on the hair shaft needs to be discontinued as do those that are tight around the frontal or posterior hair line. Hair washing should be once per week or every 2 weeks at the least, and conditioning of the hair is important with hair trims every 2 to 3 months.
Scarring Alopecia in Skin of Color: Practical Guidance From Dr. Amy J. McMichael
Scarring Alopecia in Skin of Color: Practical Guidance From Dr. Amy J. McMichael

The Future of Psoriasis Care
The Future of Psoriasis Care
Psoriasis research and treatment have come a long way in the past 2 to 3 decades. With the advent of biologic therapy, increasingly more targeted therapies, and a better pathophysiological understanding, our treatment paradigms and ability to treat psoriatic disease have shown great improvement; however, despite these advances, there remain several areas in need of further development to continue to improve our care of patients with psoriasis, including comorbidities, access to care, technology, and clinical care.
Treatment Implications of Comorbidities
It has become increasingly clear that psoriasis carries with it numerous medical and psychiatric comorbidities; however, our ability to utilize these factors in treatment decision-making is still nascent. Clinically, multiple studies have demonstrated a connection between cardiovascular disease (CVD) and psoriasis, often with a direct relationship between CVD and psoriasis severity.1-3 The cytokines involved (interleukin [IL]–17) and cell types (primarily neutrophils) are the same in psoriatic disease and evolving atherosclerotic plaques.4,5 In contrast, other analyses do not support a relationship between CVD and psoriasis, and there has been no direct and definitive demonstration that giving patients a specific psoriasis treatment could help reduce cardiovascular risk. Perhaps this is due to the sample sizes and time needed to demonstrate such a connection, as we are dealing with fairly rare events overall. Strategies to identify patients at risk for cardiovascular events, such as starting from a cohort with existing CVD and investigating treatment effects in that population, may yield worthwhile dividends. Perhaps one day we will be able to offer treatments that not only help clear psoriasis but also modulate cardiovascular health.
Our understanding of the psychiatric effects of psoriasis is even less developed. The strongest links have been demonstrated between psoriasis and depression, anxiety, and suicidal ideation.6 Some of these connections have been recognized for more than 3 decades: one study from 1993 showed that almost 10% of patients with psoriasis wished to be dead and 5.6% reported active suicidal ideation at the time of the study.7 Why is it, then, that we still do not have a good understanding of the interrelationship between psoriasis, mental health, and therapeutics? There likely is a connection between these components, as it is now well accepted that cytokines (eg, interferons) can have a considerable impact on depression and that treatment with biologics for psoriasis tends to improve depressive symptoms.8 This is an area in which we need better awareness and understanding as well as some guidance on how to approach this topic with our patients—particularly how mental health may play into therapeutic decisions for psoriasis, such as earlier escalation to rapid-acting systemic therapy in patients with psychiatric comorbidities.
Access to Psoriasis Care
With so many effective treatments for psoriasis, one of the most frustrating challenges we face is that many patients with psoriasis still experience notable barriers to care. While access in urban areas generally is reasonable, in rural areas, 75% of patients have no psoriasis-treating providers in their ZIP code and have to seek psoriasis-related care outside the 3-digit ZIP code prefix.9 Unfortunately, in most cases, even after traveling and waiting for an appointment patients will not be offered the full spectrum of available psoriasis treatments. Dermatologists already are much harder to find in rural areas, but the proportion of rural counties without a dermatologist who prescribes biologics approaches 90%.10 Functionally, this places a huge burden on our patients, who frustratingly see commercials for highly effective psoriasis treatments on television but are not able to access them. What good is having medicines that can help more than two-thirds of patients achieve 100% clearance11 when patients cannot access them?
Technology and Treatment Optimization
As our society becomes ever more technologically advanced, medicine seems to be caught in a bit of a quagmire, with our practices often using outdated technology in the name of HIPAA compliance and communicating via fax on important matters such as medication coverage. Nevertheless, dermatologists are beginning to increase integration of artificial intelligence (AI) and advanced technologies to make patient care more efficient and effective via education/awareness, image analysis, remote management, and telemedicine.12 Recently, the National Psoriasis Foundation published guidance for the use of telemedicine, suggesting that it could be used for expanded access and expedited care in appropriate settings.13 However, some caution should be used when interpreting data in this sphere. While AI technology has been purported to outpace dermatologists’ diagnosis of psoriasis in some cases, the conditions tested (ie, the training set and evaluation image bank) and special tools used (such as dermoscopy, which is not routinely used in clinical practice for psoriasis diagnosis) may make the results inapplicable to general care.14
Perhaps more promising is the use of digital aids to help with long-term care, treatment reminders, and comorbidity evaluation/screening. Similarly, telemedicine can be utilized to provide skilled psoriasis care to patients in rural areas who otherwise might not have access. One such program demonstrated that asynchronous e-consults were able to achieve Psoriasis Area and Severity Index (PASI) and body surface area outcomes similar to in-person dermatologist care.15 Using AI and technology also could assist with drug development and guide treatment. For example, a psoriatic arthritis (PsA) risk model developed in a Danish cohort suggested that early treatment with an IL-17 inhibitor in high-risk patients could reduce PsA incidence by 64%.16
Personalized Clinical Care
Even as we become accustomed to higher PASI 90, PASI 100, and mean PASI improvement numbers with our newer biologics, drug development in psoriasis has not stopped. Pipeline medications include an oral peptide-based IL-23 inhibitor17 and targeted tyrosine kinase 2 inhibitors.18,19 What is perhaps most interesting is to envision a future in which we could select treatments based on either patient phenotype (eg, involvement of hands and feet could suggest a certain single or class of medicine) or genotype.20 This has clear impacts on patient care, as dedicated trials of psoriasis medications tend to result in lower achievement of outcome measure thresholds than subanalyses of clinical trials; for example, in a dedicated trial of risankizumab for nonpustular palmoplantar psoriasis, achievement of a palmoplantar Investigator Global Assessment score of clear or almost clear was demonstrated in 33.3% of treated patients vs 16.1% of those receiving placebo at week 16 (P=.006).21 A subanalysis from the pivotal UltiMMA trials showed that more than 70% of risankizumab-treated patients achieved complete clearance (palmoplantar PASI score of 0) by week 16.22 Indeed, there is some evidence to suggest that the pathophysiology of plaque psoriasis, nonpustular palmoplantar psoriasis, and palmoplantar pustular psoriasis are different, with more interferon-γ signaling involved in nonpustular palmoplantar psoriasis23—which may explain why some limited case reports have suggested the use of Janus kinase inhibitors for recalcitrant cases of palmoplantar plaque psoriasis.24
Even with such high rates of skin clearance, the treatment landscape in PsA lags behind. There is a need for higher-efficacy treatments in PsA. On a positive note, it may be reflective of how advanced our treatment conversations about psoriasis have become that rather than analyzing gross PASI improvements between one drug and another, we now are able to address nuanced differences between various presentations of psoriasis to help us select the right tool from our treatment toolbox.
Final Thoughts
We are lucky to practice dermatology in a time when there has been so much development, with many good treatment options for patients with psoriasis. What we had thought of as the ultimate goal in the past—to get the skin relatively clear—is now a realistic outcome for most patients. This allows us to focus on other important considerations, such as assessing and addressing comorbidities, improving access to care, implementing technology to improve psoriasis care, and refining our understanding of how different manifestations of psoriasis should alter our approach to treating patients. And though we have come a long way in recent years, there still is much to be done to lift up the psoriasis community as a whole. It’s reassuring to know that many are still working toward this goal.
- Cui P, Li D, Shi L, et al. Cardiovascular comorbidities among patients with psoriasis: a national register-based study in China. Sci Rep. 2024;14:19683.
- Tinggaard AB, Hjuler KF, Andersen IT, et al. Prevalence and severity of coronary artery disease linked to prognosis in psoriasis and psoriatic arthritis patients: a multi-centre cohort study. J Intern Med. 2021;290:693-703.
- Yang YW, Keller JJ, Lin HC. Medical comorbidity associated with psoriasis in adults: a population-based study. Br J Dermatol. 2011;165:1037-1043.
- Silvestre-Roig C, Braster Q, Ortega-Gomez A, et al. Neutrophils as regulators of cardiovascular inflammation. Nat Rev Cardiol. 2020;17:327-340.
- von Stebut E, Boehncke WH, Ghoreschi K, et al. IL-17A in psoriasis and beyond: cardiovascular and metabolic implications. Front Immunol. 2019;10:3096.
- Kurd SK, Troxel AB, Crits-Christoph P, et al. The risk of depression, anxiety, and suicidality in patients with psoriasis: a population-based cohort study. Arch Dermatol. 2010;146:891-895.
- Gupta MA, Schork NJ, Gupta AK, et al. Suicidal ideation in psoriasis. Int J Dermatol. 1993;32:188-190.
- Mrowietz U, Sumbul M, Gerdes S. Depression, a major comorbidity of psoriatic disease, is caused by metabolic inflammation. J Eur Acad Dermatol Venereol. 2023;37:1731-1738.
- Seigel L, Shoaib S, Maughn K, et al. Health disparities in psoriasis: geographic barriers to access in the United States. J Dermatolog Treat. 2024;35:2365820.
- Sun QW, Feng H, Cohen JM. Geographic trends in psoriasis injectable biologic prescriptions by dermatologists among Medicare beneficiaries. J Am Acad Dermatol. 2024;91:1214-1216.
- Reich K, Warren RB, Lebwohl M, et al. Bimekizumab versus secukinumab in plaque psoriasis. N Engl J Med. 2021;385:142-152.
- Wongvibulsin S, Lee I. Artificial intelligence and dermatology. JAMA Dermatol. 2025;161:344.
- Pelet Del Toro N, Yahia R, Feldman SR, et al. National Psoriasis Foundation Telemedicine Task Force guidance for management of psoriatic disease via telemedicine. JAAD Int. 2023;12:32-36.
- Yang Y, Wang J, Xie F, et al. A convolutional neural network trained with dermoscopic images of psoriasis performed on par with 230 dermatologists. Comput Biol Med. 2021;139:104924.
- Armstrong AW, Chambers CJ, Maverakis E, et al. Effectiveness of online vs in-person care for adults with psoriasis: a randomized clinical trial. JAMA Netw Open. 2018;1:E183062.
- Gong Z, Cheng Y, Wei X, et al. Digital technologies in psoriasis management: from precision diagnosis to therapeutic innovation and holistic care. Front Digit Health. 2025;8:1656585.
- Bissonnette R, Soung J, Hebert AA, et al. Oral icotrokinra for plaque psoriasis in adults and adolescents. N Engl J Med. 2025;393:1784-1795.
- Armstrong AW, Gooderham M, Lynde C, et al. Tyrosine kinase 2 inhibition with zasocitinib (TAK-279) in psoriasis: a randomized clinical trial. JAMA Dermatol. 2024;160:1066-1074.
- Blauvelt A, Arenberger P, Sauder MB, et al. Highly selective, allosteric inhibition of TYK2 with oral ESK-001 in patients with moderate-to-severe plaque psoriasis: results from STRIDE, a 12-week, randomized, double-blinded, placebo-controlled, dose-ranging phase 2 study. J Am Acad Dermatol. 2026;94:57-65.
- Tchack M KN, Sandeep R, Muller E, et al. Gene expression or mutational profile for psoriasis in guiding treatment: a systematic review. JAAD Reviews. 2025;5:100-102.
- Lebwohl M, Bukhalo M, Stein Gold L, et al. A randomized phase 3b study evaluating the safety and efficacy of risankizumab in adult patients with moderate-to-severe plaque psoriasis with non-pustular palmoplantar involvement. J Am Acad Dermatol. 2024;91:1150-1157.
- Strober B, Bachelez H, Crowley J, et al. Efficacy of long-term risankizumab treatment for moderate-to-severe plaque psoriasis: subgroup analyses by baseline characteristics and psoriatic disease manifestations through 256 weeks (LIMMitless trial). J Eur Acad Dermatol Venereol. 2024;38:864-872.
- Wang CQ, Haxhinasto S, Garcet S, et al. Comparison of the inflammatory circuits in psoriasis vulgaris, non‒pustular palmoplantar psoriasis, and palmoplantar pustular psoriasis. J Invest Dermatol. 2023;143:87-97.
- Choi B, Li HO, Glassman SJ. Palmoplantar plaque psoriasis responsive to upadacitinib: a report of two cases. SAGE Open Med Case Rep. 2025;13:2050313X251317763.
Psoriasis research and treatment have come a long way in the past 2 to 3 decades. With the advent of biologic therapy, increasingly more targeted therapies, and a better pathophysiological understanding, our treatment paradigms and ability to treat psoriatic disease have shown great improvement; however, despite these advances, there remain several areas in need of further development to continue to improve our care of patients with psoriasis, including comorbidities, access to care, technology, and clinical care.
Treatment Implications of Comorbidities
It has become increasingly clear that psoriasis carries with it numerous medical and psychiatric comorbidities; however, our ability to utilize these factors in treatment decision-making is still nascent. Clinically, multiple studies have demonstrated a connection between cardiovascular disease (CVD) and psoriasis, often with a direct relationship between CVD and psoriasis severity.1-3 The cytokines involved (interleukin [IL]–17) and cell types (primarily neutrophils) are the same in psoriatic disease and evolving atherosclerotic plaques.4,5 In contrast, other analyses do not support a relationship between CVD and psoriasis, and there has been no direct and definitive demonstration that giving patients a specific psoriasis treatment could help reduce cardiovascular risk. Perhaps this is due to the sample sizes and time needed to demonstrate such a connection, as we are dealing with fairly rare events overall. Strategies to identify patients at risk for cardiovascular events, such as starting from a cohort with existing CVD and investigating treatment effects in that population, may yield worthwhile dividends. Perhaps one day we will be able to offer treatments that not only help clear psoriasis but also modulate cardiovascular health.
Our understanding of the psychiatric effects of psoriasis is even less developed. The strongest links have been demonstrated between psoriasis and depression, anxiety, and suicidal ideation.6 Some of these connections have been recognized for more than 3 decades: one study from 1993 showed that almost 10% of patients with psoriasis wished to be dead and 5.6% reported active suicidal ideation at the time of the study.7 Why is it, then, that we still do not have a good understanding of the interrelationship between psoriasis, mental health, and therapeutics? There likely is a connection between these components, as it is now well accepted that cytokines (eg, interferons) can have a considerable impact on depression and that treatment with biologics for psoriasis tends to improve depressive symptoms.8 This is an area in which we need better awareness and understanding as well as some guidance on how to approach this topic with our patients—particularly how mental health may play into therapeutic decisions for psoriasis, such as earlier escalation to rapid-acting systemic therapy in patients with psychiatric comorbidities.
Access to Psoriasis Care
With so many effective treatments for psoriasis, one of the most frustrating challenges we face is that many patients with psoriasis still experience notable barriers to care. While access in urban areas generally is reasonable, in rural areas, 75% of patients have no psoriasis-treating providers in their ZIP code and have to seek psoriasis-related care outside the 3-digit ZIP code prefix.9 Unfortunately, in most cases, even after traveling and waiting for an appointment patients will not be offered the full spectrum of available psoriasis treatments. Dermatologists already are much harder to find in rural areas, but the proportion of rural counties without a dermatologist who prescribes biologics approaches 90%.10 Functionally, this places a huge burden on our patients, who frustratingly see commercials for highly effective psoriasis treatments on television but are not able to access them. What good is having medicines that can help more than two-thirds of patients achieve 100% clearance11 when patients cannot access them?
Technology and Treatment Optimization
As our society becomes ever more technologically advanced, medicine seems to be caught in a bit of a quagmire, with our practices often using outdated technology in the name of HIPAA compliance and communicating via fax on important matters such as medication coverage. Nevertheless, dermatologists are beginning to increase integration of artificial intelligence (AI) and advanced technologies to make patient care more efficient and effective via education/awareness, image analysis, remote management, and telemedicine.12 Recently, the National Psoriasis Foundation published guidance for the use of telemedicine, suggesting that it could be used for expanded access and expedited care in appropriate settings.13 However, some caution should be used when interpreting data in this sphere. While AI technology has been purported to outpace dermatologists’ diagnosis of psoriasis in some cases, the conditions tested (ie, the training set and evaluation image bank) and special tools used (such as dermoscopy, which is not routinely used in clinical practice for psoriasis diagnosis) may make the results inapplicable to general care.14
Perhaps more promising is the use of digital aids to help with long-term care, treatment reminders, and comorbidity evaluation/screening. Similarly, telemedicine can be utilized to provide skilled psoriasis care to patients in rural areas who otherwise might not have access. One such program demonstrated that asynchronous e-consults were able to achieve Psoriasis Area and Severity Index (PASI) and body surface area outcomes similar to in-person dermatologist care.15 Using AI and technology also could assist with drug development and guide treatment. For example, a psoriatic arthritis (PsA) risk model developed in a Danish cohort suggested that early treatment with an IL-17 inhibitor in high-risk patients could reduce PsA incidence by 64%.16
Personalized Clinical Care
Even as we become accustomed to higher PASI 90, PASI 100, and mean PASI improvement numbers with our newer biologics, drug development in psoriasis has not stopped. Pipeline medications include an oral peptide-based IL-23 inhibitor17 and targeted tyrosine kinase 2 inhibitors.18,19 What is perhaps most interesting is to envision a future in which we could select treatments based on either patient phenotype (eg, involvement of hands and feet could suggest a certain single or class of medicine) or genotype.20 This has clear impacts on patient care, as dedicated trials of psoriasis medications tend to result in lower achievement of outcome measure thresholds than subanalyses of clinical trials; for example, in a dedicated trial of risankizumab for nonpustular palmoplantar psoriasis, achievement of a palmoplantar Investigator Global Assessment score of clear or almost clear was demonstrated in 33.3% of treated patients vs 16.1% of those receiving placebo at week 16 (P=.006).21 A subanalysis from the pivotal UltiMMA trials showed that more than 70% of risankizumab-treated patients achieved complete clearance (palmoplantar PASI score of 0) by week 16.22 Indeed, there is some evidence to suggest that the pathophysiology of plaque psoriasis, nonpustular palmoplantar psoriasis, and palmoplantar pustular psoriasis are different, with more interferon-γ signaling involved in nonpustular palmoplantar psoriasis23—which may explain why some limited case reports have suggested the use of Janus kinase inhibitors for recalcitrant cases of palmoplantar plaque psoriasis.24
Even with such high rates of skin clearance, the treatment landscape in PsA lags behind. There is a need for higher-efficacy treatments in PsA. On a positive note, it may be reflective of how advanced our treatment conversations about psoriasis have become that rather than analyzing gross PASI improvements between one drug and another, we now are able to address nuanced differences between various presentations of psoriasis to help us select the right tool from our treatment toolbox.
Final Thoughts
We are lucky to practice dermatology in a time when there has been so much development, with many good treatment options for patients with psoriasis. What we had thought of as the ultimate goal in the past—to get the skin relatively clear—is now a realistic outcome for most patients. This allows us to focus on other important considerations, such as assessing and addressing comorbidities, improving access to care, implementing technology to improve psoriasis care, and refining our understanding of how different manifestations of psoriasis should alter our approach to treating patients. And though we have come a long way in recent years, there still is much to be done to lift up the psoriasis community as a whole. It’s reassuring to know that many are still working toward this goal.
Psoriasis research and treatment have come a long way in the past 2 to 3 decades. With the advent of biologic therapy, increasingly more targeted therapies, and a better pathophysiological understanding, our treatment paradigms and ability to treat psoriatic disease have shown great improvement; however, despite these advances, there remain several areas in need of further development to continue to improve our care of patients with psoriasis, including comorbidities, access to care, technology, and clinical care.
Treatment Implications of Comorbidities
It has become increasingly clear that psoriasis carries with it numerous medical and psychiatric comorbidities; however, our ability to utilize these factors in treatment decision-making is still nascent. Clinically, multiple studies have demonstrated a connection between cardiovascular disease (CVD) and psoriasis, often with a direct relationship between CVD and psoriasis severity.1-3 The cytokines involved (interleukin [IL]–17) and cell types (primarily neutrophils) are the same in psoriatic disease and evolving atherosclerotic plaques.4,5 In contrast, other analyses do not support a relationship between CVD and psoriasis, and there has been no direct and definitive demonstration that giving patients a specific psoriasis treatment could help reduce cardiovascular risk. Perhaps this is due to the sample sizes and time needed to demonstrate such a connection, as we are dealing with fairly rare events overall. Strategies to identify patients at risk for cardiovascular events, such as starting from a cohort with existing CVD and investigating treatment effects in that population, may yield worthwhile dividends. Perhaps one day we will be able to offer treatments that not only help clear psoriasis but also modulate cardiovascular health.
Our understanding of the psychiatric effects of psoriasis is even less developed. The strongest links have been demonstrated between psoriasis and depression, anxiety, and suicidal ideation.6 Some of these connections have been recognized for more than 3 decades: one study from 1993 showed that almost 10% of patients with psoriasis wished to be dead and 5.6% reported active suicidal ideation at the time of the study.7 Why is it, then, that we still do not have a good understanding of the interrelationship between psoriasis, mental health, and therapeutics? There likely is a connection between these components, as it is now well accepted that cytokines (eg, interferons) can have a considerable impact on depression and that treatment with biologics for psoriasis tends to improve depressive symptoms.8 This is an area in which we need better awareness and understanding as well as some guidance on how to approach this topic with our patients—particularly how mental health may play into therapeutic decisions for psoriasis, such as earlier escalation to rapid-acting systemic therapy in patients with psychiatric comorbidities.
Access to Psoriasis Care
With so many effective treatments for psoriasis, one of the most frustrating challenges we face is that many patients with psoriasis still experience notable barriers to care. While access in urban areas generally is reasonable, in rural areas, 75% of patients have no psoriasis-treating providers in their ZIP code and have to seek psoriasis-related care outside the 3-digit ZIP code prefix.9 Unfortunately, in most cases, even after traveling and waiting for an appointment patients will not be offered the full spectrum of available psoriasis treatments. Dermatologists already are much harder to find in rural areas, but the proportion of rural counties without a dermatologist who prescribes biologics approaches 90%.10 Functionally, this places a huge burden on our patients, who frustratingly see commercials for highly effective psoriasis treatments on television but are not able to access them. What good is having medicines that can help more than two-thirds of patients achieve 100% clearance11 when patients cannot access them?
Technology and Treatment Optimization
As our society becomes ever more technologically advanced, medicine seems to be caught in a bit of a quagmire, with our practices often using outdated technology in the name of HIPAA compliance and communicating via fax on important matters such as medication coverage. Nevertheless, dermatologists are beginning to increase integration of artificial intelligence (AI) and advanced technologies to make patient care more efficient and effective via education/awareness, image analysis, remote management, and telemedicine.12 Recently, the National Psoriasis Foundation published guidance for the use of telemedicine, suggesting that it could be used for expanded access and expedited care in appropriate settings.13 However, some caution should be used when interpreting data in this sphere. While AI technology has been purported to outpace dermatologists’ diagnosis of psoriasis in some cases, the conditions tested (ie, the training set and evaluation image bank) and special tools used (such as dermoscopy, which is not routinely used in clinical practice for psoriasis diagnosis) may make the results inapplicable to general care.14
Perhaps more promising is the use of digital aids to help with long-term care, treatment reminders, and comorbidity evaluation/screening. Similarly, telemedicine can be utilized to provide skilled psoriasis care to patients in rural areas who otherwise might not have access. One such program demonstrated that asynchronous e-consults were able to achieve Psoriasis Area and Severity Index (PASI) and body surface area outcomes similar to in-person dermatologist care.15 Using AI and technology also could assist with drug development and guide treatment. For example, a psoriatic arthritis (PsA) risk model developed in a Danish cohort suggested that early treatment with an IL-17 inhibitor in high-risk patients could reduce PsA incidence by 64%.16
Personalized Clinical Care
Even as we become accustomed to higher PASI 90, PASI 100, and mean PASI improvement numbers with our newer biologics, drug development in psoriasis has not stopped. Pipeline medications include an oral peptide-based IL-23 inhibitor17 and targeted tyrosine kinase 2 inhibitors.18,19 What is perhaps most interesting is to envision a future in which we could select treatments based on either patient phenotype (eg, involvement of hands and feet could suggest a certain single or class of medicine) or genotype.20 This has clear impacts on patient care, as dedicated trials of psoriasis medications tend to result in lower achievement of outcome measure thresholds than subanalyses of clinical trials; for example, in a dedicated trial of risankizumab for nonpustular palmoplantar psoriasis, achievement of a palmoplantar Investigator Global Assessment score of clear or almost clear was demonstrated in 33.3% of treated patients vs 16.1% of those receiving placebo at week 16 (P=.006).21 A subanalysis from the pivotal UltiMMA trials showed that more than 70% of risankizumab-treated patients achieved complete clearance (palmoplantar PASI score of 0) by week 16.22 Indeed, there is some evidence to suggest that the pathophysiology of plaque psoriasis, nonpustular palmoplantar psoriasis, and palmoplantar pustular psoriasis are different, with more interferon-γ signaling involved in nonpustular palmoplantar psoriasis23—which may explain why some limited case reports have suggested the use of Janus kinase inhibitors for recalcitrant cases of palmoplantar plaque psoriasis.24
Even with such high rates of skin clearance, the treatment landscape in PsA lags behind. There is a need for higher-efficacy treatments in PsA. On a positive note, it may be reflective of how advanced our treatment conversations about psoriasis have become that rather than analyzing gross PASI improvements between one drug and another, we now are able to address nuanced differences between various presentations of psoriasis to help us select the right tool from our treatment toolbox.
Final Thoughts
We are lucky to practice dermatology in a time when there has been so much development, with many good treatment options for patients with psoriasis. What we had thought of as the ultimate goal in the past—to get the skin relatively clear—is now a realistic outcome for most patients. This allows us to focus on other important considerations, such as assessing and addressing comorbidities, improving access to care, implementing technology to improve psoriasis care, and refining our understanding of how different manifestations of psoriasis should alter our approach to treating patients. And though we have come a long way in recent years, there still is much to be done to lift up the psoriasis community as a whole. It’s reassuring to know that many are still working toward this goal.
- Cui P, Li D, Shi L, et al. Cardiovascular comorbidities among patients with psoriasis: a national register-based study in China. Sci Rep. 2024;14:19683.
- Tinggaard AB, Hjuler KF, Andersen IT, et al. Prevalence and severity of coronary artery disease linked to prognosis in psoriasis and psoriatic arthritis patients: a multi-centre cohort study. J Intern Med. 2021;290:693-703.
- Yang YW, Keller JJ, Lin HC. Medical comorbidity associated with psoriasis in adults: a population-based study. Br J Dermatol. 2011;165:1037-1043.
- Silvestre-Roig C, Braster Q, Ortega-Gomez A, et al. Neutrophils as regulators of cardiovascular inflammation. Nat Rev Cardiol. 2020;17:327-340.
- von Stebut E, Boehncke WH, Ghoreschi K, et al. IL-17A in psoriasis and beyond: cardiovascular and metabolic implications. Front Immunol. 2019;10:3096.
- Kurd SK, Troxel AB, Crits-Christoph P, et al. The risk of depression, anxiety, and suicidality in patients with psoriasis: a population-based cohort study. Arch Dermatol. 2010;146:891-895.
- Gupta MA, Schork NJ, Gupta AK, et al. Suicidal ideation in psoriasis. Int J Dermatol. 1993;32:188-190.
- Mrowietz U, Sumbul M, Gerdes S. Depression, a major comorbidity of psoriatic disease, is caused by metabolic inflammation. J Eur Acad Dermatol Venereol. 2023;37:1731-1738.
- Seigel L, Shoaib S, Maughn K, et al. Health disparities in psoriasis: geographic barriers to access in the United States. J Dermatolog Treat. 2024;35:2365820.
- Sun QW, Feng H, Cohen JM. Geographic trends in psoriasis injectable biologic prescriptions by dermatologists among Medicare beneficiaries. J Am Acad Dermatol. 2024;91:1214-1216.
- Reich K, Warren RB, Lebwohl M, et al. Bimekizumab versus secukinumab in plaque psoriasis. N Engl J Med. 2021;385:142-152.
- Wongvibulsin S, Lee I. Artificial intelligence and dermatology. JAMA Dermatol. 2025;161:344.
- Pelet Del Toro N, Yahia R, Feldman SR, et al. National Psoriasis Foundation Telemedicine Task Force guidance for management of psoriatic disease via telemedicine. JAAD Int. 2023;12:32-36.
- Yang Y, Wang J, Xie F, et al. A convolutional neural network trained with dermoscopic images of psoriasis performed on par with 230 dermatologists. Comput Biol Med. 2021;139:104924.
- Armstrong AW, Chambers CJ, Maverakis E, et al. Effectiveness of online vs in-person care for adults with psoriasis: a randomized clinical trial. JAMA Netw Open. 2018;1:E183062.
- Gong Z, Cheng Y, Wei X, et al. Digital technologies in psoriasis management: from precision diagnosis to therapeutic innovation and holistic care. Front Digit Health. 2025;8:1656585.
- Bissonnette R, Soung J, Hebert AA, et al. Oral icotrokinra for plaque psoriasis in adults and adolescents. N Engl J Med. 2025;393:1784-1795.
- Armstrong AW, Gooderham M, Lynde C, et al. Tyrosine kinase 2 inhibition with zasocitinib (TAK-279) in psoriasis: a randomized clinical trial. JAMA Dermatol. 2024;160:1066-1074.
- Blauvelt A, Arenberger P, Sauder MB, et al. Highly selective, allosteric inhibition of TYK2 with oral ESK-001 in patients with moderate-to-severe plaque psoriasis: results from STRIDE, a 12-week, randomized, double-blinded, placebo-controlled, dose-ranging phase 2 study. J Am Acad Dermatol. 2026;94:57-65.
- Tchack M KN, Sandeep R, Muller E, et al. Gene expression or mutational profile for psoriasis in guiding treatment: a systematic review. JAAD Reviews. 2025;5:100-102.
- Lebwohl M, Bukhalo M, Stein Gold L, et al. A randomized phase 3b study evaluating the safety and efficacy of risankizumab in adult patients with moderate-to-severe plaque psoriasis with non-pustular palmoplantar involvement. J Am Acad Dermatol. 2024;91:1150-1157.
- Strober B, Bachelez H, Crowley J, et al. Efficacy of long-term risankizumab treatment for moderate-to-severe plaque psoriasis: subgroup analyses by baseline characteristics and psoriatic disease manifestations through 256 weeks (LIMMitless trial). J Eur Acad Dermatol Venereol. 2024;38:864-872.
- Wang CQ, Haxhinasto S, Garcet S, et al. Comparison of the inflammatory circuits in psoriasis vulgaris, non‒pustular palmoplantar psoriasis, and palmoplantar pustular psoriasis. J Invest Dermatol. 2023;143:87-97.
- Choi B, Li HO, Glassman SJ. Palmoplantar plaque psoriasis responsive to upadacitinib: a report of two cases. SAGE Open Med Case Rep. 2025;13:2050313X251317763.
- Cui P, Li D, Shi L, et al. Cardiovascular comorbidities among patients with psoriasis: a national register-based study in China. Sci Rep. 2024;14:19683.
- Tinggaard AB, Hjuler KF, Andersen IT, et al. Prevalence and severity of coronary artery disease linked to prognosis in psoriasis and psoriatic arthritis patients: a multi-centre cohort study. J Intern Med. 2021;290:693-703.
- Yang YW, Keller JJ, Lin HC. Medical comorbidity associated with psoriasis in adults: a population-based study. Br J Dermatol. 2011;165:1037-1043.
- Silvestre-Roig C, Braster Q, Ortega-Gomez A, et al. Neutrophils as regulators of cardiovascular inflammation. Nat Rev Cardiol. 2020;17:327-340.
- von Stebut E, Boehncke WH, Ghoreschi K, et al. IL-17A in psoriasis and beyond: cardiovascular and metabolic implications. Front Immunol. 2019;10:3096.
- Kurd SK, Troxel AB, Crits-Christoph P, et al. The risk of depression, anxiety, and suicidality in patients with psoriasis: a population-based cohort study. Arch Dermatol. 2010;146:891-895.
- Gupta MA, Schork NJ, Gupta AK, et al. Suicidal ideation in psoriasis. Int J Dermatol. 1993;32:188-190.
- Mrowietz U, Sumbul M, Gerdes S. Depression, a major comorbidity of psoriatic disease, is caused by metabolic inflammation. J Eur Acad Dermatol Venereol. 2023;37:1731-1738.
- Seigel L, Shoaib S, Maughn K, et al. Health disparities in psoriasis: geographic barriers to access in the United States. J Dermatolog Treat. 2024;35:2365820.
- Sun QW, Feng H, Cohen JM. Geographic trends in psoriasis injectable biologic prescriptions by dermatologists among Medicare beneficiaries. J Am Acad Dermatol. 2024;91:1214-1216.
- Reich K, Warren RB, Lebwohl M, et al. Bimekizumab versus secukinumab in plaque psoriasis. N Engl J Med. 2021;385:142-152.
- Wongvibulsin S, Lee I. Artificial intelligence and dermatology. JAMA Dermatol. 2025;161:344.
- Pelet Del Toro N, Yahia R, Feldman SR, et al. National Psoriasis Foundation Telemedicine Task Force guidance for management of psoriatic disease via telemedicine. JAAD Int. 2023;12:32-36.
- Yang Y, Wang J, Xie F, et al. A convolutional neural network trained with dermoscopic images of psoriasis performed on par with 230 dermatologists. Comput Biol Med. 2021;139:104924.
- Armstrong AW, Chambers CJ, Maverakis E, et al. Effectiveness of online vs in-person care for adults with psoriasis: a randomized clinical trial. JAMA Netw Open. 2018;1:E183062.
- Gong Z, Cheng Y, Wei X, et al. Digital technologies in psoriasis management: from precision diagnosis to therapeutic innovation and holistic care. Front Digit Health. 2025;8:1656585.
- Bissonnette R, Soung J, Hebert AA, et al. Oral icotrokinra for plaque psoriasis in adults and adolescents. N Engl J Med. 2025;393:1784-1795.
- Armstrong AW, Gooderham M, Lynde C, et al. Tyrosine kinase 2 inhibition with zasocitinib (TAK-279) in psoriasis: a randomized clinical trial. JAMA Dermatol. 2024;160:1066-1074.
- Blauvelt A, Arenberger P, Sauder MB, et al. Highly selective, allosteric inhibition of TYK2 with oral ESK-001 in patients with moderate-to-severe plaque psoriasis: results from STRIDE, a 12-week, randomized, double-blinded, placebo-controlled, dose-ranging phase 2 study. J Am Acad Dermatol. 2026;94:57-65.
- Tchack M KN, Sandeep R, Muller E, et al. Gene expression or mutational profile for psoriasis in guiding treatment: a systematic review. JAAD Reviews. 2025;5:100-102.
- Lebwohl M, Bukhalo M, Stein Gold L, et al. A randomized phase 3b study evaluating the safety and efficacy of risankizumab in adult patients with moderate-to-severe plaque psoriasis with non-pustular palmoplantar involvement. J Am Acad Dermatol. 2024;91:1150-1157.
- Strober B, Bachelez H, Crowley J, et al. Efficacy of long-term risankizumab treatment for moderate-to-severe plaque psoriasis: subgroup analyses by baseline characteristics and psoriatic disease manifestations through 256 weeks (LIMMitless trial). J Eur Acad Dermatol Venereol. 2024;38:864-872.
- Wang CQ, Haxhinasto S, Garcet S, et al. Comparison of the inflammatory circuits in psoriasis vulgaris, non‒pustular palmoplantar psoriasis, and palmoplantar pustular psoriasis. J Invest Dermatol. 2023;143:87-97.
- Choi B, Li HO, Glassman SJ. Palmoplantar plaque psoriasis responsive to upadacitinib: a report of two cases. SAGE Open Med Case Rep. 2025;13:2050313X251317763.
The Future of Psoriasis Care
The Future of Psoriasis Care

Managing Resistance to Change Along the Journey to High Reliability
Managing Resistance to Change Along the Journey to High Reliability
To improve safety performance, many health care organizations have embarked on the journey to becoming high reliability organizations (HROs). HROs operate in complex, high-risk, constantly changing environments and avoid catastrophic events despite the inherent risks.1 HROs maintain high levels of safety and reliability by adhering to core principles, foundational practices, rigorous processes, a strong organizational culture, and continuous learning and process improvement.1-3
Becoming an HRO requires understanding what makes systems safer for patients and staff at all levels by taking ownership of 5 principles: (1) sensitivity to operations (increased awareness of the current status of systems); (2) reluctance to simplify (avoiding oversimplification of the cause[s] of problems); (3) preoccupation with failure (anticipating risks that might be symptomatic of a larger problem); (4) deference to expertise (relying on the most qualified individuals to make decisions); and (5) commitment to resilience (planning for potential failure and being prepared to respond).1,2,4 In addition to these, the Veterans Health Administration has identified 3 pillars of HROs: leadership commitment (safety and reliability are central to leadership vision, decision-making, and action-oriented behaviors), safety culture (across the organization, safety values are key to preventing harm and learning from mistakes), and continuous process improvement (promoting constant learning and improvement with evidence-based tools and methodologies).5
Implementing these principles is not enough to achieve high reliability. This transition requires significant change, which can be met with resistance. Without attending to organizational change, implementation of HRO principles can be superficial, scattered, and isolated.6 Large organizations often struggle with change as it conflicts with the fundamental human need for stability and security.7 Consequently, the journey to becoming an HRO requires an understanding of the reasons for resistance to change (RtC) as well as evidence-based strategies.
REASONS FOR RESISTANCE TO CHANGE
RtC is the informal and covert behavior of an individual or group to a particular change. RtC is commonly recognized as the failure of employees to do anything requested by managers and is a main reason change initiatives fail.8 While some staff see change as opportunities for learning and growth, others resist based on uncertainty about how the changes will impact their current work situation, or fear, frustration, confusion, and distrust.8,9 Resistance can overtly manifest with some staff publicly expressing their discontent in public without offering solutions, or covertly by ignoring the change or avoiding participation in any aspect of the change process. Both forms of RtC are equally detrimental.8
Frequent changes in organizations can also cause cynicism. Employees will view the change as something initially popular, but will only last until another change comes along.8,9 Resistance can result in the failure to achieve desired objectives, wasted time, effort, and resources, decreased momentum, and loss of confidence and trust in leaders to effectively manage the change process.9 To understand RtC, 3 main factors must be considered: individual, interpersonal, and organizational.
Individual
An individual’s personality can be an important indicator for how they will respond to change. Some individuals welcome and thrive on change while others resist in preference for the status quo.8,10 Individuals will also resist change if they believe their position, power, or prestige within the organization are in jeopardy or that the change is contrary to current personal or organizational values, principles, and objectives.8-12 Resistance can also be the result of uncertainty about what the change means, lack of information regarding the change, or questioning motives for the change.9
Interpersonal
Another influence on RtC is the interpersonal factors of employees. The personal satisfaction individuals receive from their work and the type of interactions they experience with colleagues can impact RtC. When communication with colleagues is lacking before and during change implementation, negative reactions to the change can fuel resistance.11 Cross-functional and bidirectional communication is vital; its absence can leave staff feeling inadequately informed and less supportive of the change.8 Employees’ understanding of changes through communication between other members of the organization is critical to success.11
Organizational
How organizational leaders introduce change affects the extent to which staff respond.10 RtC can emerge if staff feel change is imposed on them. Change is better received when people are actively engaged in the process and adopt a sense of ownership that will ultimately affect them and their role within the organization.12,13 Organizations are also better equipped to address potential RtC when leadership is respected and have a genuine concern for the overall well-being of staff members. Organizational leaders who mainly focus on the bottom line and have little regard for staff are more likely to be perceived as untrustworthy, which contributes to RtC.9,13 Lack of proper education and guidance from organizational leaders, as well as poor communication, can lead to RtC.8,13
MANAGING RESISTANCE TO CHANGE
RtC can be a significant factor in the success or failure of the change process. Poorly managed change can exponentially increase resistance, necessitating a multifaceted approach to managing RtC, while well-managed change can result in a high success rate. Evidence-based strategies to counter RtC focus on communication, employee participation, education and training, and engaging managers.8
Communication
Open and effective communication is critical to managing RtC, as uncertainty often exaggerates the negative aspects of change. Effective communication involves active listening, with leadership and management addressing employee concerns in a clear and concise manner. A psychologically safe culture for open dialogue is essential when addressing RtC.9,14,15 Psychological safety empowers staff to speak up, ask questions, and offer ideas, forming a solid basis for open and effective communication and participation. Leaders and managers should create opportunities for open dialogue for all members of the organization throughout the process. This can be accomplished with one-on-one meetings, open forums, town hall meetings, electronic mail, newsletters, and social media. Topics should cover the reasons for change, details of what is changing, the individual, organizational, and patient risks of not changing, as well as the benefits of changing.9 Encouraging staff to ask questions and provide feedback to promote bidirectional and closed-loop communication is essential to avoid misunderstandings.9,15 While open communication is essential, leaders must carefully plan what information to share, how much to share, and how to avoid information overload. Information about the change should be timely, adequate, applicable, and informative.15 The HRO practice of leader rounding for high reliability can be instrumental to ensure effective, bidirectional communication and collaboration among all disciplines across a health care organization through improving leadership visibility during times of change and enhancing interactions and communication with staff.3
Employee Participation
Involving staff in the change process significantly reduces RtC. Engagement fosters ownership in the change process, increasing the likelihood employees will support and even champion it. Health care professionals welcome opportunities to be involved in helping with aspects of organizational change, especially when invited to participate in the change early in the process and throughout the course of change.7,14,15
Leaders should encourage staff to provide feedback to understand the impact the change is having on them and their roles and responsibilities within the organization. This exemplifies the HRO principle of deference to expertise as the employee often has the most in-depth knowledge of their work setting. Employee perspectives can significantly influence the success of change initatives.7,14 Participation is impactful in providing employees with a sense of agency facilitating acceptance and improving desire to adopt the change.14
Tiered safety huddles and visual management systems (VMSs) also can engage staff. Tiered safety huddles provide a forum for transparent communication, increasing situational awareness, and improving a health care organization’s ability to appropriately respond to staff questions, suggestions, and concerns. VMSs display the status and progress toward organizational goals during the change process, and are highly effective in creating environments where staff feel empowered to voice concerns related to the change process.3
Education and Training
Educating employees on the value of change is crucial to overcome RtC. RtC often stems from employees not feeling prepared to adapt or adopt new processes. Health care professionals who do not receive information about change are less likely to support it.7,12,15 Staff are more likely to accept change when they understand why it is needed and how it impacts the organization’s long-term mission.11,15 Timely, compelling, and informative education on how to adapt to the change will promote more positive appraisal of the change and reduce RtC.8,15 Employees must feel confident they will receive the appropriate training, resources, and support to successfully adapt to the change. This requires leaders and managers taking time to clarify expectations, conduct a gap analysis to identify the skills and knowledge needed to support the planned change, and provide sufficient educational opportunities to fill those gaps.8 For example, the US Department of Veterans Affairs offers classes to employees on the Prosci ADKAR (Awareness, Desire, Knowledge, Ability, and Reinforcement) Model. This training provides individuals with the information and skills needed for change to be successful.16
Safety forums can be influential and allow leadership to educate staff on updates related to change processes and promote bidirectional communication.3 In safety forums, staff have an opportunity to ask questions, especially as they relate to learning about available resources to become more informed about the organizational changes.
Engaging Managers
Managers are pivotal to the successful implementation of organizational change.8 They serve as the bridge between senior leadership and frontline employees and are positioned to influence the adoption and success of change initiatives. Often the first point of contact for employees, managers can effectively communicate the need for change, and act as the liaison to align it with individual employee motivations. Since they are often the first to encounter resistance among employees, managers serve as advocates through the process. Through a coaching role, managers can help employees develop the knowledge and ability to be successful and thrive in the new environment. The Table summarizes the evidence-based strategies.
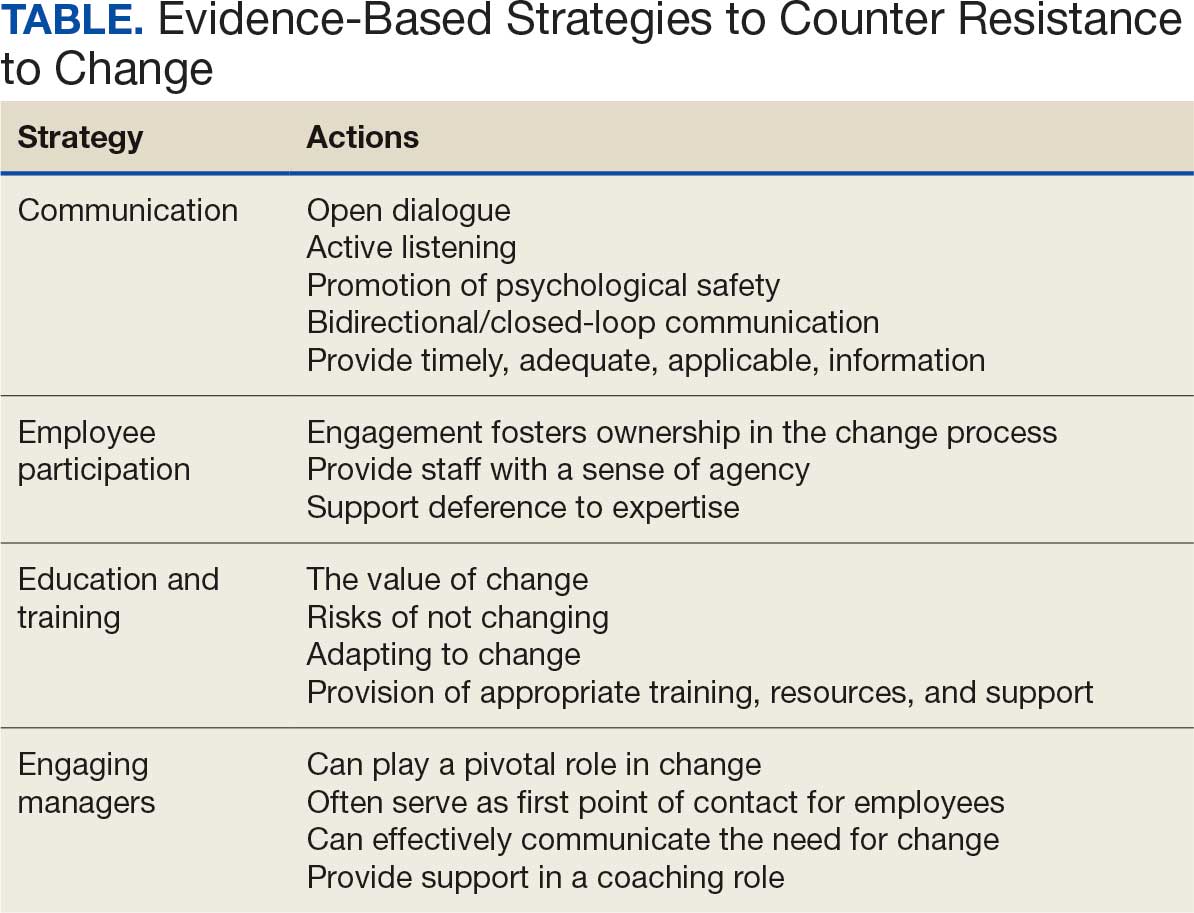
CONCLUSIONS
Implementing change in health care organizations can be challenging, especially on the journey to high reliability. RtC is the result of factors at the individual, interpersonal, and organizational levels that leaders must address to increase chances for success. Organizational changes in health care are more likely to succeed when staff understand why the change is needed through open and continuous communication, can influence the change by sharing their own perspectives, and have the knowledge, skills, and resources to prepare for and participate in the process.
- Merchant NB, O’Neal J, Dealing-Perez C, et al. A high-reliability organization mindset. Am J Med Qual. 2022;37:504-510. doi:10.1097/JMQ.0000000000000086
- Veazie S, Peterson K, Bourne D, et al. Implementing high-reliability organization principles into practice: a rapid evidence review. J Patient Saf. 2022;18:e320-e328. doi:10.1097/PTS.0000000000000768
- Murray JS, Baghdadi A, Dannenberg W, et al. The role of high reliability organization foundational practices in building a culture of safety. Fed Pract. 2024;41:214-221. doi:10.12788/fp.0486
- Ford J, Isaacks DB, Anderson T. Creating, executing and sustaining a high-reliability organization in health care. The Learning Organization: An International Journal. 2024;31:817-833. doi:10.1108/TLO-03-2023-0048
- Cox GR, Starr LM. VHA’s movement for change: implementing high-reliability principles and practices. J Healthc Manag. 2023;68:151-157. doi:10.1097/JHM-D-00056
- Myers CG, Sutcliffe KM. High reliability organising in healthcare: still a long way left to go. BMJ Qual Saf. 2022;31:845-848. doi:10.1136/bmjqs-2021-014141
- Nilsen P, Seing I, Ericsson C, et al. Characteristics of successful changes in health care organizations: an interview study with physicians, registered nurses and assistant nurses. BMC Health Serv Res. 2020;20:147. doi:10.1186/s12913-020-4999-8
- Cheraghi R, Ebrahimi H, Kheibar N, et al. Reasons for resistance to change in nursing: an integrative review. BMC Nurs. 2023;22:310. doi:10/1186/s12912-023-01460-0
- Warrick DD. Revisiting resistance to change and how to manage it: what has been learned and what organizations need to do. Bus Horiz. 2023;66:433-441. doi:10.1016/j.bushor.2022.09.001
- Sverdlik N, Oreg S. Beyond the individual-level conceptualization of dispositional resistance to change: multilevel effects on the response to organizational change. J Organ Behav. 2023;44:1066-1077. doi:10.1002/job.2678
- Khaw KW, Alnoor A, Al-Abrrow H, et al. Reactions towards organizational change: a systematic literature review. Curr Psychol. 2022;13:1-24. doi:10.1007/s12144-022-03070-6
- Pomare C, Churruca K, Long JC, et al. Organisational change in hospitals: a qualitative case-study of staff perspectives. BMC Health Serv Res. 2019;19:840. doi:10.1186/s12913-019-4704-y
- DuBose BM, Mayo AM. RtC: a concept analysis. Nurs Forum. 2020;55:631-636. doi:10.1111/nuf.12479
- Sahay S, Goldthwaite C. Participatory practices during organizational change: rethinking participation and resistance. Manag Commun Q. 2024;38(2):279-306. doi:10.1177/08933189231187883
- Damawan AH, Azizah S. Resistance to change: causes and strategies as an organizational challenge. ASSEHR. 2020;395(2020):49-53. doi:10.2991/assehr.k.200120.010
- Wong Q, Lacombe M, Keller R, et al. Leading change with ADKAR. Nurs Manage. 2019;50:28-35. doi:10.1097/01.NUMA.0000554341.70508.75
To improve safety performance, many health care organizations have embarked on the journey to becoming high reliability organizations (HROs). HROs operate in complex, high-risk, constantly changing environments and avoid catastrophic events despite the inherent risks.1 HROs maintain high levels of safety and reliability by adhering to core principles, foundational practices, rigorous processes, a strong organizational culture, and continuous learning and process improvement.1-3
Becoming an HRO requires understanding what makes systems safer for patients and staff at all levels by taking ownership of 5 principles: (1) sensitivity to operations (increased awareness of the current status of systems); (2) reluctance to simplify (avoiding oversimplification of the cause[s] of problems); (3) preoccupation with failure (anticipating risks that might be symptomatic of a larger problem); (4) deference to expertise (relying on the most qualified individuals to make decisions); and (5) commitment to resilience (planning for potential failure and being prepared to respond).1,2,4 In addition to these, the Veterans Health Administration has identified 3 pillars of HROs: leadership commitment (safety and reliability are central to leadership vision, decision-making, and action-oriented behaviors), safety culture (across the organization, safety values are key to preventing harm and learning from mistakes), and continuous process improvement (promoting constant learning and improvement with evidence-based tools and methodologies).5
Implementing these principles is not enough to achieve high reliability. This transition requires significant change, which can be met with resistance. Without attending to organizational change, implementation of HRO principles can be superficial, scattered, and isolated.6 Large organizations often struggle with change as it conflicts with the fundamental human need for stability and security.7 Consequently, the journey to becoming an HRO requires an understanding of the reasons for resistance to change (RtC) as well as evidence-based strategies.
REASONS FOR RESISTANCE TO CHANGE
RtC is the informal and covert behavior of an individual or group to a particular change. RtC is commonly recognized as the failure of employees to do anything requested by managers and is a main reason change initiatives fail.8 While some staff see change as opportunities for learning and growth, others resist based on uncertainty about how the changes will impact their current work situation, or fear, frustration, confusion, and distrust.8,9 Resistance can overtly manifest with some staff publicly expressing their discontent in public without offering solutions, or covertly by ignoring the change or avoiding participation in any aspect of the change process. Both forms of RtC are equally detrimental.8
Frequent changes in organizations can also cause cynicism. Employees will view the change as something initially popular, but will only last until another change comes along.8,9 Resistance can result in the failure to achieve desired objectives, wasted time, effort, and resources, decreased momentum, and loss of confidence and trust in leaders to effectively manage the change process.9 To understand RtC, 3 main factors must be considered: individual, interpersonal, and organizational.
Individual
An individual’s personality can be an important indicator for how they will respond to change. Some individuals welcome and thrive on change while others resist in preference for the status quo.8,10 Individuals will also resist change if they believe their position, power, or prestige within the organization are in jeopardy or that the change is contrary to current personal or organizational values, principles, and objectives.8-12 Resistance can also be the result of uncertainty about what the change means, lack of information regarding the change, or questioning motives for the change.9
Interpersonal
Another influence on RtC is the interpersonal factors of employees. The personal satisfaction individuals receive from their work and the type of interactions they experience with colleagues can impact RtC. When communication with colleagues is lacking before and during change implementation, negative reactions to the change can fuel resistance.11 Cross-functional and bidirectional communication is vital; its absence can leave staff feeling inadequately informed and less supportive of the change.8 Employees’ understanding of changes through communication between other members of the organization is critical to success.11
Organizational
How organizational leaders introduce change affects the extent to which staff respond.10 RtC can emerge if staff feel change is imposed on them. Change is better received when people are actively engaged in the process and adopt a sense of ownership that will ultimately affect them and their role within the organization.12,13 Organizations are also better equipped to address potential RtC when leadership is respected and have a genuine concern for the overall well-being of staff members. Organizational leaders who mainly focus on the bottom line and have little regard for staff are more likely to be perceived as untrustworthy, which contributes to RtC.9,13 Lack of proper education and guidance from organizational leaders, as well as poor communication, can lead to RtC.8,13
MANAGING RESISTANCE TO CHANGE
RtC can be a significant factor in the success or failure of the change process. Poorly managed change can exponentially increase resistance, necessitating a multifaceted approach to managing RtC, while well-managed change can result in a high success rate. Evidence-based strategies to counter RtC focus on communication, employee participation, education and training, and engaging managers.8
Communication
Open and effective communication is critical to managing RtC, as uncertainty often exaggerates the negative aspects of change. Effective communication involves active listening, with leadership and management addressing employee concerns in a clear and concise manner. A psychologically safe culture for open dialogue is essential when addressing RtC.9,14,15 Psychological safety empowers staff to speak up, ask questions, and offer ideas, forming a solid basis for open and effective communication and participation. Leaders and managers should create opportunities for open dialogue for all members of the organization throughout the process. This can be accomplished with one-on-one meetings, open forums, town hall meetings, electronic mail, newsletters, and social media. Topics should cover the reasons for change, details of what is changing, the individual, organizational, and patient risks of not changing, as well as the benefits of changing.9 Encouraging staff to ask questions and provide feedback to promote bidirectional and closed-loop communication is essential to avoid misunderstandings.9,15 While open communication is essential, leaders must carefully plan what information to share, how much to share, and how to avoid information overload. Information about the change should be timely, adequate, applicable, and informative.15 The HRO practice of leader rounding for high reliability can be instrumental to ensure effective, bidirectional communication and collaboration among all disciplines across a health care organization through improving leadership visibility during times of change and enhancing interactions and communication with staff.3
Employee Participation
Involving staff in the change process significantly reduces RtC. Engagement fosters ownership in the change process, increasing the likelihood employees will support and even champion it. Health care professionals welcome opportunities to be involved in helping with aspects of organizational change, especially when invited to participate in the change early in the process and throughout the course of change.7,14,15
Leaders should encourage staff to provide feedback to understand the impact the change is having on them and their roles and responsibilities within the organization. This exemplifies the HRO principle of deference to expertise as the employee often has the most in-depth knowledge of their work setting. Employee perspectives can significantly influence the success of change initatives.7,14 Participation is impactful in providing employees with a sense of agency facilitating acceptance and improving desire to adopt the change.14
Tiered safety huddles and visual management systems (VMSs) also can engage staff. Tiered safety huddles provide a forum for transparent communication, increasing situational awareness, and improving a health care organization’s ability to appropriately respond to staff questions, suggestions, and concerns. VMSs display the status and progress toward organizational goals during the change process, and are highly effective in creating environments where staff feel empowered to voice concerns related to the change process.3
Education and Training
Educating employees on the value of change is crucial to overcome RtC. RtC often stems from employees not feeling prepared to adapt or adopt new processes. Health care professionals who do not receive information about change are less likely to support it.7,12,15 Staff are more likely to accept change when they understand why it is needed and how it impacts the organization’s long-term mission.11,15 Timely, compelling, and informative education on how to adapt to the change will promote more positive appraisal of the change and reduce RtC.8,15 Employees must feel confident they will receive the appropriate training, resources, and support to successfully adapt to the change. This requires leaders and managers taking time to clarify expectations, conduct a gap analysis to identify the skills and knowledge needed to support the planned change, and provide sufficient educational opportunities to fill those gaps.8 For example, the US Department of Veterans Affairs offers classes to employees on the Prosci ADKAR (Awareness, Desire, Knowledge, Ability, and Reinforcement) Model. This training provides individuals with the information and skills needed for change to be successful.16
Safety forums can be influential and allow leadership to educate staff on updates related to change processes and promote bidirectional communication.3 In safety forums, staff have an opportunity to ask questions, especially as they relate to learning about available resources to become more informed about the organizational changes.
Engaging Managers
Managers are pivotal to the successful implementation of organizational change.8 They serve as the bridge between senior leadership and frontline employees and are positioned to influence the adoption and success of change initiatives. Often the first point of contact for employees, managers can effectively communicate the need for change, and act as the liaison to align it with individual employee motivations. Since they are often the first to encounter resistance among employees, managers serve as advocates through the process. Through a coaching role, managers can help employees develop the knowledge and ability to be successful and thrive in the new environment. The Table summarizes the evidence-based strategies.
CONCLUSIONS
Implementing change in health care organizations can be challenging, especially on the journey to high reliability. RtC is the result of factors at the individual, interpersonal, and organizational levels that leaders must address to increase chances for success. Organizational changes in health care are more likely to succeed when staff understand why the change is needed through open and continuous communication, can influence the change by sharing their own perspectives, and have the knowledge, skills, and resources to prepare for and participate in the process.
To improve safety performance, many health care organizations have embarked on the journey to becoming high reliability organizations (HROs). HROs operate in complex, high-risk, constantly changing environments and avoid catastrophic events despite the inherent risks.1 HROs maintain high levels of safety and reliability by adhering to core principles, foundational practices, rigorous processes, a strong organizational culture, and continuous learning and process improvement.1-3
Becoming an HRO requires understanding what makes systems safer for patients and staff at all levels by taking ownership of 5 principles: (1) sensitivity to operations (increased awareness of the current status of systems); (2) reluctance to simplify (avoiding oversimplification of the cause[s] of problems); (3) preoccupation with failure (anticipating risks that might be symptomatic of a larger problem); (4) deference to expertise (relying on the most qualified individuals to make decisions); and (5) commitment to resilience (planning for potential failure and being prepared to respond).1,2,4 In addition to these, the Veterans Health Administration has identified 3 pillars of HROs: leadership commitment (safety and reliability are central to leadership vision, decision-making, and action-oriented behaviors), safety culture (across the organization, safety values are key to preventing harm and learning from mistakes), and continuous process improvement (promoting constant learning and improvement with evidence-based tools and methodologies).5
Implementing these principles is not enough to achieve high reliability. This transition requires significant change, which can be met with resistance. Without attending to organizational change, implementation of HRO principles can be superficial, scattered, and isolated.6 Large organizations often struggle with change as it conflicts with the fundamental human need for stability and security.7 Consequently, the journey to becoming an HRO requires an understanding of the reasons for resistance to change (RtC) as well as evidence-based strategies.
REASONS FOR RESISTANCE TO CHANGE
RtC is the informal and covert behavior of an individual or group to a particular change. RtC is commonly recognized as the failure of employees to do anything requested by managers and is a main reason change initiatives fail.8 While some staff see change as opportunities for learning and growth, others resist based on uncertainty about how the changes will impact their current work situation, or fear, frustration, confusion, and distrust.8,9 Resistance can overtly manifest with some staff publicly expressing their discontent in public without offering solutions, or covertly by ignoring the change or avoiding participation in any aspect of the change process. Both forms of RtC are equally detrimental.8
Frequent changes in organizations can also cause cynicism. Employees will view the change as something initially popular, but will only last until another change comes along.8,9 Resistance can result in the failure to achieve desired objectives, wasted time, effort, and resources, decreased momentum, and loss of confidence and trust in leaders to effectively manage the change process.9 To understand RtC, 3 main factors must be considered: individual, interpersonal, and organizational.
Individual
An individual’s personality can be an important indicator for how they will respond to change. Some individuals welcome and thrive on change while others resist in preference for the status quo.8,10 Individuals will also resist change if they believe their position, power, or prestige within the organization are in jeopardy or that the change is contrary to current personal or organizational values, principles, and objectives.8-12 Resistance can also be the result of uncertainty about what the change means, lack of information regarding the change, or questioning motives for the change.9
Interpersonal
Another influence on RtC is the interpersonal factors of employees. The personal satisfaction individuals receive from their work and the type of interactions they experience with colleagues can impact RtC. When communication with colleagues is lacking before and during change implementation, negative reactions to the change can fuel resistance.11 Cross-functional and bidirectional communication is vital; its absence can leave staff feeling inadequately informed and less supportive of the change.8 Employees’ understanding of changes through communication between other members of the organization is critical to success.11
Organizational
How organizational leaders introduce change affects the extent to which staff respond.10 RtC can emerge if staff feel change is imposed on them. Change is better received when people are actively engaged in the process and adopt a sense of ownership that will ultimately affect them and their role within the organization.12,13 Organizations are also better equipped to address potential RtC when leadership is respected and have a genuine concern for the overall well-being of staff members. Organizational leaders who mainly focus on the bottom line and have little regard for staff are more likely to be perceived as untrustworthy, which contributes to RtC.9,13 Lack of proper education and guidance from organizational leaders, as well as poor communication, can lead to RtC.8,13
MANAGING RESISTANCE TO CHANGE
RtC can be a significant factor in the success or failure of the change process. Poorly managed change can exponentially increase resistance, necessitating a multifaceted approach to managing RtC, while well-managed change can result in a high success rate. Evidence-based strategies to counter RtC focus on communication, employee participation, education and training, and engaging managers.8
Communication
Open and effective communication is critical to managing RtC, as uncertainty often exaggerates the negative aspects of change. Effective communication involves active listening, with leadership and management addressing employee concerns in a clear and concise manner. A psychologically safe culture for open dialogue is essential when addressing RtC.9,14,15 Psychological safety empowers staff to speak up, ask questions, and offer ideas, forming a solid basis for open and effective communication and participation. Leaders and managers should create opportunities for open dialogue for all members of the organization throughout the process. This can be accomplished with one-on-one meetings, open forums, town hall meetings, electronic mail, newsletters, and social media. Topics should cover the reasons for change, details of what is changing, the individual, organizational, and patient risks of not changing, as well as the benefits of changing.9 Encouraging staff to ask questions and provide feedback to promote bidirectional and closed-loop communication is essential to avoid misunderstandings.9,15 While open communication is essential, leaders must carefully plan what information to share, how much to share, and how to avoid information overload. Information about the change should be timely, adequate, applicable, and informative.15 The HRO practice of leader rounding for high reliability can be instrumental to ensure effective, bidirectional communication and collaboration among all disciplines across a health care organization through improving leadership visibility during times of change and enhancing interactions and communication with staff.3
Employee Participation
Involving staff in the change process significantly reduces RtC. Engagement fosters ownership in the change process, increasing the likelihood employees will support and even champion it. Health care professionals welcome opportunities to be involved in helping with aspects of organizational change, especially when invited to participate in the change early in the process and throughout the course of change.7,14,15
Leaders should encourage staff to provide feedback to understand the impact the change is having on them and their roles and responsibilities within the organization. This exemplifies the HRO principle of deference to expertise as the employee often has the most in-depth knowledge of their work setting. Employee perspectives can significantly influence the success of change initatives.7,14 Participation is impactful in providing employees with a sense of agency facilitating acceptance and improving desire to adopt the change.14
Tiered safety huddles and visual management systems (VMSs) also can engage staff. Tiered safety huddles provide a forum for transparent communication, increasing situational awareness, and improving a health care organization’s ability to appropriately respond to staff questions, suggestions, and concerns. VMSs display the status and progress toward organizational goals during the change process, and are highly effective in creating environments where staff feel empowered to voice concerns related to the change process.3
Education and Training
Educating employees on the value of change is crucial to overcome RtC. RtC often stems from employees not feeling prepared to adapt or adopt new processes. Health care professionals who do not receive information about change are less likely to support it.7,12,15 Staff are more likely to accept change when they understand why it is needed and how it impacts the organization’s long-term mission.11,15 Timely, compelling, and informative education on how to adapt to the change will promote more positive appraisal of the change and reduce RtC.8,15 Employees must feel confident they will receive the appropriate training, resources, and support to successfully adapt to the change. This requires leaders and managers taking time to clarify expectations, conduct a gap analysis to identify the skills and knowledge needed to support the planned change, and provide sufficient educational opportunities to fill those gaps.8 For example, the US Department of Veterans Affairs offers classes to employees on the Prosci ADKAR (Awareness, Desire, Knowledge, Ability, and Reinforcement) Model. This training provides individuals with the information and skills needed for change to be successful.16
Safety forums can be influential and allow leadership to educate staff on updates related to change processes and promote bidirectional communication.3 In safety forums, staff have an opportunity to ask questions, especially as they relate to learning about available resources to become more informed about the organizational changes.
Engaging Managers
Managers are pivotal to the successful implementation of organizational change.8 They serve as the bridge between senior leadership and frontline employees and are positioned to influence the adoption and success of change initiatives. Often the first point of contact for employees, managers can effectively communicate the need for change, and act as the liaison to align it with individual employee motivations. Since they are often the first to encounter resistance among employees, managers serve as advocates through the process. Through a coaching role, managers can help employees develop the knowledge and ability to be successful and thrive in the new environment. The Table summarizes the evidence-based strategies.
CONCLUSIONS
Implementing change in health care organizations can be challenging, especially on the journey to high reliability. RtC is the result of factors at the individual, interpersonal, and organizational levels that leaders must address to increase chances for success. Organizational changes in health care are more likely to succeed when staff understand why the change is needed through open and continuous communication, can influence the change by sharing their own perspectives, and have the knowledge, skills, and resources to prepare for and participate in the process.
- Merchant NB, O’Neal J, Dealing-Perez C, et al. A high-reliability organization mindset. Am J Med Qual. 2022;37:504-510. doi:10.1097/JMQ.0000000000000086
- Veazie S, Peterson K, Bourne D, et al. Implementing high-reliability organization principles into practice: a rapid evidence review. J Patient Saf. 2022;18:e320-e328. doi:10.1097/PTS.0000000000000768
- Murray JS, Baghdadi A, Dannenberg W, et al. The role of high reliability organization foundational practices in building a culture of safety. Fed Pract. 2024;41:214-221. doi:10.12788/fp.0486
- Ford J, Isaacks DB, Anderson T. Creating, executing and sustaining a high-reliability organization in health care. The Learning Organization: An International Journal. 2024;31:817-833. doi:10.1108/TLO-03-2023-0048
- Cox GR, Starr LM. VHA’s movement for change: implementing high-reliability principles and practices. J Healthc Manag. 2023;68:151-157. doi:10.1097/JHM-D-00056
- Myers CG, Sutcliffe KM. High reliability organising in healthcare: still a long way left to go. BMJ Qual Saf. 2022;31:845-848. doi:10.1136/bmjqs-2021-014141
- Nilsen P, Seing I, Ericsson C, et al. Characteristics of successful changes in health care organizations: an interview study with physicians, registered nurses and assistant nurses. BMC Health Serv Res. 2020;20:147. doi:10.1186/s12913-020-4999-8
- Cheraghi R, Ebrahimi H, Kheibar N, et al. Reasons for resistance to change in nursing: an integrative review. BMC Nurs. 2023;22:310. doi:10/1186/s12912-023-01460-0
- Warrick DD. Revisiting resistance to change and how to manage it: what has been learned and what organizations need to do. Bus Horiz. 2023;66:433-441. doi:10.1016/j.bushor.2022.09.001
- Sverdlik N, Oreg S. Beyond the individual-level conceptualization of dispositional resistance to change: multilevel effects on the response to organizational change. J Organ Behav. 2023;44:1066-1077. doi:10.1002/job.2678
- Khaw KW, Alnoor A, Al-Abrrow H, et al. Reactions towards organizational change: a systematic literature review. Curr Psychol. 2022;13:1-24. doi:10.1007/s12144-022-03070-6
- Pomare C, Churruca K, Long JC, et al. Organisational change in hospitals: a qualitative case-study of staff perspectives. BMC Health Serv Res. 2019;19:840. doi:10.1186/s12913-019-4704-y
- DuBose BM, Mayo AM. RtC: a concept analysis. Nurs Forum. 2020;55:631-636. doi:10.1111/nuf.12479
- Sahay S, Goldthwaite C. Participatory practices during organizational change: rethinking participation and resistance. Manag Commun Q. 2024;38(2):279-306. doi:10.1177/08933189231187883
- Damawan AH, Azizah S. Resistance to change: causes and strategies as an organizational challenge. ASSEHR. 2020;395(2020):49-53. doi:10.2991/assehr.k.200120.010
- Wong Q, Lacombe M, Keller R, et al. Leading change with ADKAR. Nurs Manage. 2019;50:28-35. doi:10.1097/01.NUMA.0000554341.70508.75
- Merchant NB, O’Neal J, Dealing-Perez C, et al. A high-reliability organization mindset. Am J Med Qual. 2022;37:504-510. doi:10.1097/JMQ.0000000000000086
- Veazie S, Peterson K, Bourne D, et al. Implementing high-reliability organization principles into practice: a rapid evidence review. J Patient Saf. 2022;18:e320-e328. doi:10.1097/PTS.0000000000000768
- Murray JS, Baghdadi A, Dannenberg W, et al. The role of high reliability organization foundational practices in building a culture of safety. Fed Pract. 2024;41:214-221. doi:10.12788/fp.0486
- Ford J, Isaacks DB, Anderson T. Creating, executing and sustaining a high-reliability organization in health care. The Learning Organization: An International Journal. 2024;31:817-833. doi:10.1108/TLO-03-2023-0048
- Cox GR, Starr LM. VHA’s movement for change: implementing high-reliability principles and practices. J Healthc Manag. 2023;68:151-157. doi:10.1097/JHM-D-00056
- Myers CG, Sutcliffe KM. High reliability organising in healthcare: still a long way left to go. BMJ Qual Saf. 2022;31:845-848. doi:10.1136/bmjqs-2021-014141
- Nilsen P, Seing I, Ericsson C, et al. Characteristics of successful changes in health care organizations: an interview study with physicians, registered nurses and assistant nurses. BMC Health Serv Res. 2020;20:147. doi:10.1186/s12913-020-4999-8
- Cheraghi R, Ebrahimi H, Kheibar N, et al. Reasons for resistance to change in nursing: an integrative review. BMC Nurs. 2023;22:310. doi:10/1186/s12912-023-01460-0
- Warrick DD. Revisiting resistance to change and how to manage it: what has been learned and what organizations need to do. Bus Horiz. 2023;66:433-441. doi:10.1016/j.bushor.2022.09.001
- Sverdlik N, Oreg S. Beyond the individual-level conceptualization of dispositional resistance to change: multilevel effects on the response to organizational change. J Organ Behav. 2023;44:1066-1077. doi:10.1002/job.2678
- Khaw KW, Alnoor A, Al-Abrrow H, et al. Reactions towards organizational change: a systematic literature review. Curr Psychol. 2022;13:1-24. doi:10.1007/s12144-022-03070-6
- Pomare C, Churruca K, Long JC, et al. Organisational change in hospitals: a qualitative case-study of staff perspectives. BMC Health Serv Res. 2019;19:840. doi:10.1186/s12913-019-4704-y
- DuBose BM, Mayo AM. RtC: a concept analysis. Nurs Forum. 2020;55:631-636. doi:10.1111/nuf.12479
- Sahay S, Goldthwaite C. Participatory practices during organizational change: rethinking participation and resistance. Manag Commun Q. 2024;38(2):279-306. doi:10.1177/08933189231187883
- Damawan AH, Azizah S. Resistance to change: causes and strategies as an organizational challenge. ASSEHR. 2020;395(2020):49-53. doi:10.2991/assehr.k.200120.010
- Wong Q, Lacombe M, Keller R, et al. Leading change with ADKAR. Nurs Manage. 2019;50:28-35. doi:10.1097/01.NUMA.0000554341.70508.75
Managing Resistance to Change Along the Journey to High Reliability
Managing Resistance to Change Along the Journey to High Reliability

Treating Dermatophyte Onychomycosis: Clinical Insights From Dr. Shari R. Lipner
Treating Dermatophyte Onychomycosis: Clinical Insights From Dr. Shari R. Lipner
With increasing reports of terbinafine resistance, how has your strategy for treating dermatophyte onychomycosis evolved?
DR. LIPNER: Most cases of onychomycosis are not resistant to terbinafine, so for a patient newly diagnosed with onychomycosis, my approach involves evaluating the severity of disease, number of nails affected, comorbid conditions, and concomitant medications and then discussing the risks and benefits of oral vs topical treatment. If a patient’s onychomycosis previously did not resolve with oral terbinafine, I would test for terbinafine resistance. If positive, I would treat with itraconazole for more severe cases and efinaconazole for mild to moderate cases.
Are there any new systemic or topical antifungals for onychomycosis that dermatologists should be aware of?
DR. LIPNER: There have been no new US Food and Drug Administration–approved antifungals for onychomycosis since 2014 (efinaconazole and tavaborole). For most patients, our current antifungals generally have good efficacy. For treatment failures, I would recommend reconfirming the diagnosis and testing for terbinafine resistance.
When do you choose oral antifungal therapy vs topical/combination therapy?
DR. LIPNER: almost never prescribe combination antifungal therapy because monotherapy alone is usually effective, and there is no obvious benefit to combination therapy. If treatment is working (or not working), it is hard to know which agent (if any) is effective. The one time I would use combination therapy (eg, oral terbinafine and topical efinaconazole) would be if the patient has distal lateral subungual onychomycosis and a dermatophytoma. Oral terbinafine would generally be most effective for distal lateral subungual onychomycosis, and topical efinaconazole would likely be most effective for dermatophytoma.
What is the role of adjunctive therapies in onychomycosis?
DR. LIPNER: Debridement can be effective for patients with very thick nails, combined with oral or topical antifungals. Nail avulsion generally is not helpful and should be avoided because it causes permanent shortening of the nail bed. Devices (eg, lasers, photodynamic therapy) are not subject to the same stringent endpoints as medication-based approvals. Because studies to date are small and have different efficacy endpoints, I do not use devices for treatment of onychomycosis.
How do you counsel patients about expectations and timelines for onychomycosis therapy and cure vs improvement?
DR. LIPNER: Oral treatments for toenail onychomycosis are generally given for 3-month courses, but patients should be counseled that the nail could take up to 12 to 18 months to fully grow out and look normal. If patients also have mechanical nail dystrophy, the fungus may be cured with antifungal therapy, but the nail may look better but not perfect, so it is important to manage long-term expectations.
With increasing reports of terbinafine resistance, how has your strategy for treating dermatophyte onychomycosis evolved?
DR. LIPNER: Most cases of onychomycosis are not resistant to terbinafine, so for a patient newly diagnosed with onychomycosis, my approach involves evaluating the severity of disease, number of nails affected, comorbid conditions, and concomitant medications and then discussing the risks and benefits of oral vs topical treatment. If a patient’s onychomycosis previously did not resolve with oral terbinafine, I would test for terbinafine resistance. If positive, I would treat with itraconazole for more severe cases and efinaconazole for mild to moderate cases.
Are there any new systemic or topical antifungals for onychomycosis that dermatologists should be aware of?
DR. LIPNER: There have been no new US Food and Drug Administration–approved antifungals for onychomycosis since 2014 (efinaconazole and tavaborole). For most patients, our current antifungals generally have good efficacy. For treatment failures, I would recommend reconfirming the diagnosis and testing for terbinafine resistance.
When do you choose oral antifungal therapy vs topical/combination therapy?
DR. LIPNER: almost never prescribe combination antifungal therapy because monotherapy alone is usually effective, and there is no obvious benefit to combination therapy. If treatment is working (or not working), it is hard to know which agent (if any) is effective. The one time I would use combination therapy (eg, oral terbinafine and topical efinaconazole) would be if the patient has distal lateral subungual onychomycosis and a dermatophytoma. Oral terbinafine would generally be most effective for distal lateral subungual onychomycosis, and topical efinaconazole would likely be most effective for dermatophytoma.
What is the role of adjunctive therapies in onychomycosis?
DR. LIPNER: Debridement can be effective for patients with very thick nails, combined with oral or topical antifungals. Nail avulsion generally is not helpful and should be avoided because it causes permanent shortening of the nail bed. Devices (eg, lasers, photodynamic therapy) are not subject to the same stringent endpoints as medication-based approvals. Because studies to date are small and have different efficacy endpoints, I do not use devices for treatment of onychomycosis.
How do you counsel patients about expectations and timelines for onychomycosis therapy and cure vs improvement?
DR. LIPNER: Oral treatments for toenail onychomycosis are generally given for 3-month courses, but patients should be counseled that the nail could take up to 12 to 18 months to fully grow out and look normal. If patients also have mechanical nail dystrophy, the fungus may be cured with antifungal therapy, but the nail may look better but not perfect, so it is important to manage long-term expectations.
With increasing reports of terbinafine resistance, how has your strategy for treating dermatophyte onychomycosis evolved?
DR. LIPNER: Most cases of onychomycosis are not resistant to terbinafine, so for a patient newly diagnosed with onychomycosis, my approach involves evaluating the severity of disease, number of nails affected, comorbid conditions, and concomitant medications and then discussing the risks and benefits of oral vs topical treatment. If a patient’s onychomycosis previously did not resolve with oral terbinafine, I would test for terbinafine resistance. If positive, I would treat with itraconazole for more severe cases and efinaconazole for mild to moderate cases.
Are there any new systemic or topical antifungals for onychomycosis that dermatologists should be aware of?
DR. LIPNER: There have been no new US Food and Drug Administration–approved antifungals for onychomycosis since 2014 (efinaconazole and tavaborole). For most patients, our current antifungals generally have good efficacy. For treatment failures, I would recommend reconfirming the diagnosis and testing for terbinafine resistance.
When do you choose oral antifungal therapy vs topical/combination therapy?
DR. LIPNER: almost never prescribe combination antifungal therapy because monotherapy alone is usually effective, and there is no obvious benefit to combination therapy. If treatment is working (or not working), it is hard to know which agent (if any) is effective. The one time I would use combination therapy (eg, oral terbinafine and topical efinaconazole) would be if the patient has distal lateral subungual onychomycosis and a dermatophytoma. Oral terbinafine would generally be most effective for distal lateral subungual onychomycosis, and topical efinaconazole would likely be most effective for dermatophytoma.
What is the role of adjunctive therapies in onychomycosis?
DR. LIPNER: Debridement can be effective for patients with very thick nails, combined with oral or topical antifungals. Nail avulsion generally is not helpful and should be avoided because it causes permanent shortening of the nail bed. Devices (eg, lasers, photodynamic therapy) are not subject to the same stringent endpoints as medication-based approvals. Because studies to date are small and have different efficacy endpoints, I do not use devices for treatment of onychomycosis.
How do you counsel patients about expectations and timelines for onychomycosis therapy and cure vs improvement?
DR. LIPNER: Oral treatments for toenail onychomycosis are generally given for 3-month courses, but patients should be counseled that the nail could take up to 12 to 18 months to fully grow out and look normal. If patients also have mechanical nail dystrophy, the fungus may be cured with antifungal therapy, but the nail may look better but not perfect, so it is important to manage long-term expectations.
Treating Dermatophyte Onychomycosis: Clinical Insights From Dr. Shari R. Lipner
Treating Dermatophyte Onychomycosis: Clinical Insights From Dr. Shari R. Lipner
