User login
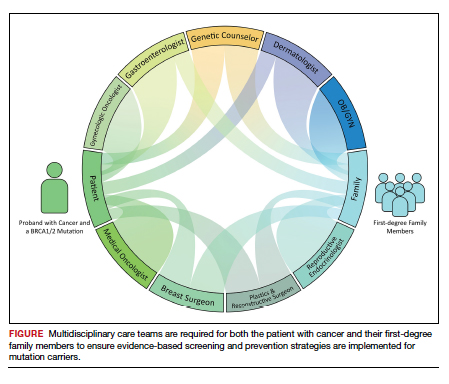
Cancer prevention through cascade genetic testing: A review of the current practice guidelines, barriers to testing and proposed solutions

CASE Woman with BRCA2 mutation
An 80-year-old woman presents for evaluation of newly diagnosed metastatic pancreatic adenocarcinoma. Her medical history is notable for breast cancer. Genetic testing of pancreatic tumor tissue detected a pathogenic variant in BRCA2. Family history revealed a history of melanoma as well as bladder, prostate, breast, and colon cancer. The patient subsequently underwent germline genetic testing with an 86-gene panel and a pathogenic mutation in BRCA2 was identified.
Watch a video of this patient and her clinician, Dr. Andrea Hagemann: https://www.youtube.com/watch?
Methods of genetic testing
It is estimated that 1 in 300 to 1 in 500 women in the United States carry a deleterious mutation in BRCA1 or BRCA2. This equates to between 250,000 and 415,000 women who are at high risk for breast and ovarian cancer.1 Looking at all women with cancer, 20% with ovarian,2 10% with breast,3 2% to 3% with endometrial,4 and 5% with colon cancer5 will have a germline mutation predisposing them to cancer. Identification of germline or somatic (tumor) mutations now inform treatment for patients with cancer. An equally important goal of germline genetic testing is cancer prevention. Cancer prevention strategies include risk-based screening for breast, colon, melanoma, and pancreatic cancer and prophylactic surgeries to reduce the risk of breast and ovarian cancer based on mutation type. Evidence-based screening guidelines by mutation type and absolute risk of associated cancers can be found on the National Comprehensive Cancer Network (NCCN).6,7
Multiple strategies have been proposed to identify patients for germline genetic testing. Patients can be identified based on a detailed multigenerational family history. This strategy requires clinicians or genetic counselors to take and update family histories, to recognize when a patient requires referral for testing, and for such testing to be completed. Even then the generation of a detailed pedigree is not very sensitive or specific. Population-based screening for high-penetrance breast and ovarian cancer susceptibility genes, regardless of family history, also has been proposed.8 Such a strategy has become increasingly realistic with decreasing cost and increasing availability of genetic testing. However, it would require increased genetic counseling resources to feasibly and equitably reach the target population and to explain the results to those patients and their relatives.
An alternative is to test the enriched population of family members of a patient with cancer who has been found to carry a pathogenic variant in a clinically relevant cancer susceptibility gene. This type of testing is termed cascade genetic testing. Cascade testing in first-degree family members carries a 50% probability of detecting the same pathogenic mutation. A related testing model is traceback testing where genetic testing is performed on pathology or tumor registry specimens from deceased patients with cancer.9 This genetic testing information is then provided to the family. Traceback models of genetic testing are an active area of research but can introduce ethical dilemmas. The more widely accepted cascade testing starts with the testing of a living patient affected with cancer. A recent article demonstrated the feasibility of a cascade testing model. Using a multiple linear regression model, the authors determined that all carriers of pathogenic mutations in 18 clinically relevant cancer susceptibility genes in the United States could be identified in 9.9 years if there was a 70% cascade testing rate of first-, second- and third-degree relatives, compared to 59.5 years with no cascade testing.10
Gaps in practice
Identification of mutation carriers, either through screening triggered by family history or through testing of patients affected with cancer, represents a gap between guidelines and clinical practice. Current NCCN guidelines outline genetic testing criteria for hereditary breast and ovarian cancer syndrome and for hereditary colorectal cancer. Despite well-established criteria, a survey in the United States revealed that only 19% of primary care providers were able to accurately assess family history for BRCA1 and 2 testing.11 Looking at patients who meet criteria for testing for Lynch syndrome, only 1 in 4 individuals have undergone genetic testing.12 Among patients diagnosed with breast and ovarian cancer, current NCCN guidelines recommend germline genetic testing for all patients with epithelial ovarian cancer; emerging evidence suggests all patients with breast cancer should be offered germline genetic testing.7,13 Large population-based studies have repeatedly demonstrated that testing rates fall short of this goal, with only 10% to 30% of patients undergoing genetic testing.9,14
Among families with a known hereditary mutation, rates of cascade genetic testing are also low, ranging from 17% to 50%.15-18 Evidence-based management guidelines, for both hereditary breast and ovarian cancer as well as Lynch syndrome, have been shown to reduce mortality.19,20 Failure to identify patients who carry these genetic mutations equates to increased mortality for our patients.
Barriers to cascade genetic testing
Cascade genetic testing ideally would be performed on entire families. Actual practice is far from ideal, and barriers to cascade testing exist. Barriers encompass resistance on the part of the family and provider as well as environmental or system factors.
Family factors
Because of privacy laws, the responsibility of disclosure of genetic testing results to family members falls primarily to the patient. Proband education is critical to ensure disclosure amongst family members. Family dynamics and geographic distribution of family members can further complicate disclosure. Following disclosure, family member gender, education, and demographics as well as personal views, attitudes, and emotions affect whether a family member decides to undergo testing.21 Furthermore, insurance status and awareness of and access to specialty-specific care for the proband’s family members may influence cascade genetic testing rates.
Provider factors
Provider factors that affect cascade genetic testing include awareness of testing guidelines, interpretation of genetic testing results, and education and knowledge of specific mutations. For instance, providers must recognize that cascade testing is not appropriate for variants of uncertain significance. This can lead to unnecessary surveillance testing and prophylactic surgeries. Providers, however, must continue to follow patients and periodically update testing results as variants may be reclassified over time. Additionally, providers must be knowledgeable about the complex and nuanced nature of the screening guidelines for each mutation. The NCCN provides detailed recommendations by mutation.7 Patients may benefit from care with cancer specialists who are aware of the guidelines, particularly for moderate-penetrance genes like BRIP1 and PALB2, as discussions about the timing of risk-reducing surgery are more nuanced in this population. Finally, which providers are responsible for facilitating cascade testing may be unclear; oncologists and genetic counselors not primarily treating probands’ relatives may assume the proper information has been passed along to family members without a practical means to follow up, and primary care providers may assume it is being taken care of by the oncology provider.
Continue to: Environmental or system factors...
Environmental or system factors
Accessibility of genetic counseling and testing is a common barrier to cascade testing. Family members may be geographically remote and connecting them to counseling and testing can be challenging. Working with local genetic counselors can facilitate this process. Insurance coverage of testing is a common perceived barrier; however, many testing companies now provide cascade testing free of charge if within a certain window from the initial test. Despite this, patients often site cost as a barrier to undergoing testing. Concerns about insurance coverage are common after a positive result. The Genetic Information Nondiscrimination Act of 2008 prohibits discrimination against employees or insurance applicants because of genetic information. Life insurance or long-term care policies, however, can incorporate genetic testing information into policy rates, so patients should be recommended to consider purchasing life insurance prior to undergoing genetic testing. This is especially important if the person considering testing has not yet been diagnosed with cancer.
Implications of a positive result
Family members who receive a positive test result should be referred for genetic counseling and to the appropriate specialists for evidence-based screening and discussion for risk-reducing surgery (FIGURE).7 For mutations associated with hereditary breast and ovarian cancer, referral to breast and gynecologic surgeons with expertise in risk reducing surgery is critical as the risk of diagnosing an occult malignancy is approximately 1%.22 Surgical technique with a 2-cm margin on the
Patient resources: decision aids, websites
As genetic testing becomes more accessible and people are tested at younger ages, studies examining the balance of risk reduction and quality of life (QOL) are increasingly important. Fertility concerns, effects of early menopause, and the interrelatedness between decisions for breast and gynecologic risk reduction should all be considered in the counseling for surgical risk reduction. Patient decision aids can help mutation carriers navigate the complex information and decisions.25 Websites specifically designed by advocacy groups can be useful adjuncts to in-office counseling (Facing Our Risk Empowered, FORCE; Facingourrisk.org).
Family letters
The American College of Obstetricians and Gynecologists recommends an ObGyn have a letter or documentation stating that the patient’s relative has a specific mutation before initiating cascade testing for an at-risk family member. The indicated test (such as BRCA1) should be ordered only after the patient has been counseled about potential outcomes and has expressly decided to be tested.26 Letters, such as the example given in the American College of Obstetricians and Gynecologists practice bulletin,26 are a key component of communication between oncology providers, probands, family members, and their primary care providers. ObGyn providers should work together with genetic counselors and gynecologic oncologists to determine the most efficient strategies in their communities.
Technology
Access to genetic testing and genetic counseling has been improved with the rise in telemedicine. Geographically remote patients can now access genetic counseling through medical center–based counselors as well as company-provided genetic counseling over the phone. Patients also can submit samples remotely without needing to be tested in a doctor’s office.
Databases from cancer centers that detail cascade genetic testing rates. As the preventive impact of cascade genetic testing becomes clearer, strategies to have recurrent discussions with cancer patients regarding their family members’ risk should be implemented. It is still unclear which providers—genetic counselors, gynecologic oncologists, medical oncologists, breast surgeons, ObGyns, to name a few—are primarily responsible for remembering to have these follow-up discussions, and despite advances, the burden still rests on the cancer patient themselves. Databases with automated follow-up surveys done every 6 to 12 months could provide some aid to busy providers in this regard.
Emerging research
If gynecologic risk-reducing surgery is chosen, clinical trial involvement should be encouraged. The Women Choosing Surgical Prevention (NCT02760849) in the United States and the TUBA study (NCT02321228) in the Netherlands were designed to compare menopause-related QOL between standard risk-reducing salpingo-oophorectomy (RRSO) and the innovative risk-reducing salpingectomy with delayed oophorectomy for mutation carriers. Results from the nonrandomized controlled TUBA trial suggest that patients have better menopause-related QOL after risk-reducing salpingectomy than after RRSO, regardless of hormone replacement therapy.27 International collaboration is continuing to better understand oncologic safety. In the United States, the SOROCk trial (NCT04251052) is a noninferiority surgical choice study underway for BRCA1 mutation carriers aged 35 to 50, powered to determine oncologic outcome differences in addition to QOL outcomes between RRSO and delayed oophorectomy arms.
Returning to the case
The patient and her family underwent genetic counseling. The patient’s 2 daughters, each in their 50s, underwent cascade genetic testing and were found to carry the same pathogenic mutation in BRCA2. After counseling from both breast and gynecologic surgeons, they both elected to undergo risk reducing bilateral salpingo-oophorectomy with hysterectomy. Both now complete regular screening for breast cancer and melanoma with plans to start screening for pancreatic cancer. Both are currently cancer free.
Summary
Cascade genetic testing is an efficient strategy to identify mutation carriers for hereditary breast and ovarian cancer syndrome. Implementation of the best patient-centric care will require continued collaboration and communication across and within disciplines. ●
Cascade, or targeted, genetic testing within families known to carry a hereditary mutation in a cancer susceptibility gene should be performed on all living first-degree family members over the age of 18. All mutation carriers should be connected to a multidisciplinary care team (FIGURE) to ensure implementation of evidence-based screening and risk-reducing surgery for cancer prevention. If gynecologic risk-reducing surgery is chosen, clinical trial involvement should be encouraged.
- Gabai-Kapara E, Lahad A, Kaufman B, et al. Population-based screening for breast and ovarian cancer risk due to BRCA1 and BRCA2. Proc Natl Acad Sci U S A. 2014;111:14205-14210.
- Norquist BM, Harrell MI, Brady MF, et al. Inherited mutations in women with ovarian carcinoma. JAMA Oncol. 2016;2:482-490.
- Yamauchi H, Takei J. Management of hereditary breast and ovarian cancer. Int J Clin Oncol. 2018;23:45-51.
- Kahn RM, Gordhandas S, Maddy BP, et al. Universal endometrial cancer tumor typing: how much has immunohistochemistry, microsatellite instability, and MLH1 methylation improved the diagnosis of Lynch syndrome across the population? Cancer. 2019;125:3172-3183.
- Jasperson KW, Tuohy TM, Neklason DW, et al. Hereditary and familial colon cancer. Gastroenterology. 2010;138:2044-2058.
- Gupta S, Provenzale D, Llor X, et al. NCCN guidelines insights: genetic/familial high-risk assessment: colorectal, version 2.2019. J Natl Compr Canc Netw. 2019;17:1032-1041.
- Daly MB, Pal T, Berry MP, et al. Genetic/familial high-risk assessment: breast, ovarian, and pancreatic, version 2.2021, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2021;19:77-102.
- King MC, Levy-Lahad E, Lahad A. Population-based screening for BRCA1 and BRCA2: 2014 Lasker Award. JAMA. 2014;312:1091-1092.
- Samimi G, et al. Traceback: a proposed framework to increase identification and genetic counseling of BRCA1 and BRCA2 mutation carriers through family-based outreach. J Clin Oncol. 2017;35:2329-2337.
- Offit K, Tkachuk KA, Stadler ZK, et al. Cascading after peridiagnostic cancer genetic testing: an alternative to population-based screening. J Clin Oncol. 2020;38:1398-1408.
- Bellcross CA, Kolor K, Goddard KAB, et al. Awareness and utilization of BRCA1/2 testing among U.S. primary care physicians. Am J Prev Med. 2011;40:61-66.
- Cross DS, Rahm AK, Kauffman TL, et al. Underutilization of Lynch syndrome screening in a multisite study of patients with colorectal cancer. Genet Med. 2013;15:933-940.
- Beitsch PD, Whitworth PW, Hughes K, et al. Underdiagnosis of hereditary breast cancer: are genetic testing guidelines a tool or an obstacle? J Clin Oncol. 2019;37:453-460.
- Childers CP, Childers KK, Maggard-Gibbons M, et al. National estimates of genetic testing in women with a history of breast or ovarian cancer. J Clin Oncol. 2017;35:3800-3806.
- Samadder NJ, Riegert-Johnson D, Boardman L, et al. Comparison of universal genetic testing vs guideline-directed targeted testing for patients with hereditary cancer syndrome. JAMA Oncol. 2021;7:230-237.
- Sharaf RN, Myer P, Stave CD, et al. Uptake of genetic testing by relatives of Lynch syndrome probands: a systematic review. Clin Gastroenterol Hepatol. 2013;11:1093-1100.
- Menko FH, Ter Stege JA, van der Kolk LE, et al. The uptake of presymptomatic genetic testing in hereditary breast-ovarian cancer and Lynch syndrome: a systematic review of the literature and implications for clinical practice. Fam Cancer. 2019;18:127-135.
- Griffin NE, Buchanan TR, Smith SH, et al. Low rates of cascade genetic testing among families with hereditary gynecologic cancer: an opportunity to improve cancer prevention. Gynecol Oncol. 2020;156:140-146.
- Roberts MC, Dotson WD, DeVore CS, et al. Delivery of cascade screening for hereditary conditions: a scoping review of the literature. Health Aff (Millwood). 2018;37:801-808.
- Finch AP, Lubinski J, Møller P, et al. Impact of oophorectomy on cancer incidence and mortality in women with a BRCA1 or BRCA2 mutation. J Clin Oncol. 2014;32:1547-1553.
- Srinivasan S, Won NY, Dotson WD, et al. Barriers and facilitators for cascade testing in genetic conditions: a systematic review. Eur J Hum Genet. 2020;28:1631-1644.
- Piedimonte S, Frank C, Laprise C, et al. Occult tubal carcinoma after risk-reducing salpingo-oophorectomy: a systematic review. Obstet Gynecol. 2020;135:498-508.
- Shu CA, Pike MC, Jotwani AR, et al. Uterine cancer after risk-reducing salpingo-oophorectomy without hysterectomy in women with BRCA mutations. JAMA Oncol. 2016;2:1434-1440.
- Gordhandas S, Norquist BM, Pennington KP, et al. Hormone replacement therapy after risk reducing salpingo-oophorectomy in patients with BRCA1 or BRCA2 mutations; a systematic review of risks and benefits. Gynecol Oncol. 2019;153:192-200.
- Steenbeek MP, van Bommel MHD, Harmsen MG, et al. Evaluation of a patient decision aid for BRCA1/2 pathogenic variant carriers choosing an ovarian cancer prevention strategy. Gynecol Oncol. 2021;163:371-377.
- Committee on Gynecologic Practice. ACOG committee opinion No. 727: Cascade testing: testing women for known hereditary genetic mutations associated with cancer. Obstet Gynecol. 2018;131:E31-E34.
- Steenbeek MP, Harmsen MG, Hoogerbrugge N, et al. Association of salpingectomy with delayed oophorectomy versus salpingo-oophorectomy with quality of life in BRCA1/2 pathogenic variant carriers: a nonrandomized controlled trial. JAMA Oncol. 2021;7:1203-1212.
Dr. Stock is a Fellow in the Division of Gynecologic Oncology, Washington University School of Medicine, St. Louis, Missouri.

Dr. Mutch is Ira C. and Judith Gall Professor and Vice Chair of Obstetrics and Gynecology in the Department of ObGyn, Division of Gynecologic Oncology, Washington University School of Medicine.

Dr. Hagemann is Associate Professor of Obstetrics and Gynecology, and Director of Hereditary Genetics Clinic in the Division of Gynecologic Oncology, Washington University School of Medicine.
The authors report no financial relationships relevant to this article.
Dr. Stock is a Fellow in the Division of Gynecologic Oncology, Washington University School of Medicine, St. Louis, Missouri.
Dr. Mutch is Ira C. and Judith Gall Professor and Vice Chair of Obstetrics and Gynecology in the Department of ObGyn, Division of Gynecologic Oncology, Washington University School of Medicine.
Dr. Hagemann is Associate Professor of Obstetrics and Gynecology, and Director of Hereditary Genetics Clinic in the Division of Gynecologic Oncology, Washington University School of Medicine.
The authors report no financial relationships relevant to this article.
Dr. Stock is a Fellow in the Division of Gynecologic Oncology, Washington University School of Medicine, St. Louis, Missouri.
Dr. Mutch is Ira C. and Judith Gall Professor and Vice Chair of Obstetrics and Gynecology in the Department of ObGyn, Division of Gynecologic Oncology, Washington University School of Medicine.
Dr. Hagemann is Associate Professor of Obstetrics and Gynecology, and Director of Hereditary Genetics Clinic in the Division of Gynecologic Oncology, Washington University School of Medicine.
The authors report no financial relationships relevant to this article.
CASE Woman with BRCA2 mutation
An 80-year-old woman presents for evaluation of newly diagnosed metastatic pancreatic adenocarcinoma. Her medical history is notable for breast cancer. Genetic testing of pancreatic tumor tissue detected a pathogenic variant in BRCA2. Family history revealed a history of melanoma as well as bladder, prostate, breast, and colon cancer. The patient subsequently underwent germline genetic testing with an 86-gene panel and a pathogenic mutation in BRCA2 was identified.
Watch a video of this patient and her clinician, Dr. Andrea Hagemann: https://www.youtube.com/watch?
Methods of genetic testing
It is estimated that 1 in 300 to 1 in 500 women in the United States carry a deleterious mutation in BRCA1 or BRCA2. This equates to between 250,000 and 415,000 women who are at high risk for breast and ovarian cancer.1 Looking at all women with cancer, 20% with ovarian,2 10% with breast,3 2% to 3% with endometrial,4 and 5% with colon cancer5 will have a germline mutation predisposing them to cancer. Identification of germline or somatic (tumor) mutations now inform treatment for patients with cancer. An equally important goal of germline genetic testing is cancer prevention. Cancer prevention strategies include risk-based screening for breast, colon, melanoma, and pancreatic cancer and prophylactic surgeries to reduce the risk of breast and ovarian cancer based on mutation type. Evidence-based screening guidelines by mutation type and absolute risk of associated cancers can be found on the National Comprehensive Cancer Network (NCCN).6,7
Multiple strategies have been proposed to identify patients for germline genetic testing. Patients can be identified based on a detailed multigenerational family history. This strategy requires clinicians or genetic counselors to take and update family histories, to recognize when a patient requires referral for testing, and for such testing to be completed. Even then the generation of a detailed pedigree is not very sensitive or specific. Population-based screening for high-penetrance breast and ovarian cancer susceptibility genes, regardless of family history, also has been proposed.8 Such a strategy has become increasingly realistic with decreasing cost and increasing availability of genetic testing. However, it would require increased genetic counseling resources to feasibly and equitably reach the target population and to explain the results to those patients and their relatives.
An alternative is to test the enriched population of family members of a patient with cancer who has been found to carry a pathogenic variant in a clinically relevant cancer susceptibility gene. This type of testing is termed cascade genetic testing. Cascade testing in first-degree family members carries a 50% probability of detecting the same pathogenic mutation. A related testing model is traceback testing where genetic testing is performed on pathology or tumor registry specimens from deceased patients with cancer.9 This genetic testing information is then provided to the family. Traceback models of genetic testing are an active area of research but can introduce ethical dilemmas. The more widely accepted cascade testing starts with the testing of a living patient affected with cancer. A recent article demonstrated the feasibility of a cascade testing model. Using a multiple linear regression model, the authors determined that all carriers of pathogenic mutations in 18 clinically relevant cancer susceptibility genes in the United States could be identified in 9.9 years if there was a 70% cascade testing rate of first-, second- and third-degree relatives, compared to 59.5 years with no cascade testing.10
Gaps in practice
Identification of mutation carriers, either through screening triggered by family history or through testing of patients affected with cancer, represents a gap between guidelines and clinical practice. Current NCCN guidelines outline genetic testing criteria for hereditary breast and ovarian cancer syndrome and for hereditary colorectal cancer. Despite well-established criteria, a survey in the United States revealed that only 19% of primary care providers were able to accurately assess family history for BRCA1 and 2 testing.11 Looking at patients who meet criteria for testing for Lynch syndrome, only 1 in 4 individuals have undergone genetic testing.12 Among patients diagnosed with breast and ovarian cancer, current NCCN guidelines recommend germline genetic testing for all patients with epithelial ovarian cancer; emerging evidence suggests all patients with breast cancer should be offered germline genetic testing.7,13 Large population-based studies have repeatedly demonstrated that testing rates fall short of this goal, with only 10% to 30% of patients undergoing genetic testing.9,14
Among families with a known hereditary mutation, rates of cascade genetic testing are also low, ranging from 17% to 50%.15-18 Evidence-based management guidelines, for both hereditary breast and ovarian cancer as well as Lynch syndrome, have been shown to reduce mortality.19,20 Failure to identify patients who carry these genetic mutations equates to increased mortality for our patients.
Barriers to cascade genetic testing
Cascade genetic testing ideally would be performed on entire families. Actual practice is far from ideal, and barriers to cascade testing exist. Barriers encompass resistance on the part of the family and provider as well as environmental or system factors.
Family factors
Because of privacy laws, the responsibility of disclosure of genetic testing results to family members falls primarily to the patient. Proband education is critical to ensure disclosure amongst family members. Family dynamics and geographic distribution of family members can further complicate disclosure. Following disclosure, family member gender, education, and demographics as well as personal views, attitudes, and emotions affect whether a family member decides to undergo testing.21 Furthermore, insurance status and awareness of and access to specialty-specific care for the proband’s family members may influence cascade genetic testing rates.
Provider factors
Provider factors that affect cascade genetic testing include awareness of testing guidelines, interpretation of genetic testing results, and education and knowledge of specific mutations. For instance, providers must recognize that cascade testing is not appropriate for variants of uncertain significance. This can lead to unnecessary surveillance testing and prophylactic surgeries. Providers, however, must continue to follow patients and periodically update testing results as variants may be reclassified over time. Additionally, providers must be knowledgeable about the complex and nuanced nature of the screening guidelines for each mutation. The NCCN provides detailed recommendations by mutation.7 Patients may benefit from care with cancer specialists who are aware of the guidelines, particularly for moderate-penetrance genes like BRIP1 and PALB2, as discussions about the timing of risk-reducing surgery are more nuanced in this population. Finally, which providers are responsible for facilitating cascade testing may be unclear; oncologists and genetic counselors not primarily treating probands’ relatives may assume the proper information has been passed along to family members without a practical means to follow up, and primary care providers may assume it is being taken care of by the oncology provider.
Continue to: Environmental or system factors...
Environmental or system factors
Accessibility of genetic counseling and testing is a common barrier to cascade testing. Family members may be geographically remote and connecting them to counseling and testing can be challenging. Working with local genetic counselors can facilitate this process. Insurance coverage of testing is a common perceived barrier; however, many testing companies now provide cascade testing free of charge if within a certain window from the initial test. Despite this, patients often site cost as a barrier to undergoing testing. Concerns about insurance coverage are common after a positive result. The Genetic Information Nondiscrimination Act of 2008 prohibits discrimination against employees or insurance applicants because of genetic information. Life insurance or long-term care policies, however, can incorporate genetic testing information into policy rates, so patients should be recommended to consider purchasing life insurance prior to undergoing genetic testing. This is especially important if the person considering testing has not yet been diagnosed with cancer.
Implications of a positive result
Family members who receive a positive test result should be referred for genetic counseling and to the appropriate specialists for evidence-based screening and discussion for risk-reducing surgery (FIGURE).7 For mutations associated with hereditary breast and ovarian cancer, referral to breast and gynecologic surgeons with expertise in risk reducing surgery is critical as the risk of diagnosing an occult malignancy is approximately 1%.22 Surgical technique with a 2-cm margin on the
Patient resources: decision aids, websites
As genetic testing becomes more accessible and people are tested at younger ages, studies examining the balance of risk reduction and quality of life (QOL) are increasingly important. Fertility concerns, effects of early menopause, and the interrelatedness between decisions for breast and gynecologic risk reduction should all be considered in the counseling for surgical risk reduction. Patient decision aids can help mutation carriers navigate the complex information and decisions.25 Websites specifically designed by advocacy groups can be useful adjuncts to in-office counseling (Facing Our Risk Empowered, FORCE; Facingourrisk.org).
Family letters
The American College of Obstetricians and Gynecologists recommends an ObGyn have a letter or documentation stating that the patient’s relative has a specific mutation before initiating cascade testing for an at-risk family member. The indicated test (such as BRCA1) should be ordered only after the patient has been counseled about potential outcomes and has expressly decided to be tested.26 Letters, such as the example given in the American College of Obstetricians and Gynecologists practice bulletin,26 are a key component of communication between oncology providers, probands, family members, and their primary care providers. ObGyn providers should work together with genetic counselors and gynecologic oncologists to determine the most efficient strategies in their communities.
Technology
Access to genetic testing and genetic counseling has been improved with the rise in telemedicine. Geographically remote patients can now access genetic counseling through medical center–based counselors as well as company-provided genetic counseling over the phone. Patients also can submit samples remotely without needing to be tested in a doctor’s office.
Databases from cancer centers that detail cascade genetic testing rates. As the preventive impact of cascade genetic testing becomes clearer, strategies to have recurrent discussions with cancer patients regarding their family members’ risk should be implemented. It is still unclear which providers—genetic counselors, gynecologic oncologists, medical oncologists, breast surgeons, ObGyns, to name a few—are primarily responsible for remembering to have these follow-up discussions, and despite advances, the burden still rests on the cancer patient themselves. Databases with automated follow-up surveys done every 6 to 12 months could provide some aid to busy providers in this regard.
Emerging research
If gynecologic risk-reducing surgery is chosen, clinical trial involvement should be encouraged. The Women Choosing Surgical Prevention (NCT02760849) in the United States and the TUBA study (NCT02321228) in the Netherlands were designed to compare menopause-related QOL between standard risk-reducing salpingo-oophorectomy (RRSO) and the innovative risk-reducing salpingectomy with delayed oophorectomy for mutation carriers. Results from the nonrandomized controlled TUBA trial suggest that patients have better menopause-related QOL after risk-reducing salpingectomy than after RRSO, regardless of hormone replacement therapy.27 International collaboration is continuing to better understand oncologic safety. In the United States, the SOROCk trial (NCT04251052) is a noninferiority surgical choice study underway for BRCA1 mutation carriers aged 35 to 50, powered to determine oncologic outcome differences in addition to QOL outcomes between RRSO and delayed oophorectomy arms.
Returning to the case
The patient and her family underwent genetic counseling. The patient’s 2 daughters, each in their 50s, underwent cascade genetic testing and were found to carry the same pathogenic mutation in BRCA2. After counseling from both breast and gynecologic surgeons, they both elected to undergo risk reducing bilateral salpingo-oophorectomy with hysterectomy. Both now complete regular screening for breast cancer and melanoma with plans to start screening for pancreatic cancer. Both are currently cancer free.
Summary
Cascade genetic testing is an efficient strategy to identify mutation carriers for hereditary breast and ovarian cancer syndrome. Implementation of the best patient-centric care will require continued collaboration and communication across and within disciplines. ●
Cascade, or targeted, genetic testing within families known to carry a hereditary mutation in a cancer susceptibility gene should be performed on all living first-degree family members over the age of 18. All mutation carriers should be connected to a multidisciplinary care team (FIGURE) to ensure implementation of evidence-based screening and risk-reducing surgery for cancer prevention. If gynecologic risk-reducing surgery is chosen, clinical trial involvement should be encouraged.
CASE Woman with BRCA2 mutation
An 80-year-old woman presents for evaluation of newly diagnosed metastatic pancreatic adenocarcinoma. Her medical history is notable for breast cancer. Genetic testing of pancreatic tumor tissue detected a pathogenic variant in BRCA2. Family history revealed a history of melanoma as well as bladder, prostate, breast, and colon cancer. The patient subsequently underwent germline genetic testing with an 86-gene panel and a pathogenic mutation in BRCA2 was identified.
Watch a video of this patient and her clinician, Dr. Andrea Hagemann: https://www.youtube.com/watch?
Methods of genetic testing
It is estimated that 1 in 300 to 1 in 500 women in the United States carry a deleterious mutation in BRCA1 or BRCA2. This equates to between 250,000 and 415,000 women who are at high risk for breast and ovarian cancer.1 Looking at all women with cancer, 20% with ovarian,2 10% with breast,3 2% to 3% with endometrial,4 and 5% with colon cancer5 will have a germline mutation predisposing them to cancer. Identification of germline or somatic (tumor) mutations now inform treatment for patients with cancer. An equally important goal of germline genetic testing is cancer prevention. Cancer prevention strategies include risk-based screening for breast, colon, melanoma, and pancreatic cancer and prophylactic surgeries to reduce the risk of breast and ovarian cancer based on mutation type. Evidence-based screening guidelines by mutation type and absolute risk of associated cancers can be found on the National Comprehensive Cancer Network (NCCN).6,7
Multiple strategies have been proposed to identify patients for germline genetic testing. Patients can be identified based on a detailed multigenerational family history. This strategy requires clinicians or genetic counselors to take and update family histories, to recognize when a patient requires referral for testing, and for such testing to be completed. Even then the generation of a detailed pedigree is not very sensitive or specific. Population-based screening for high-penetrance breast and ovarian cancer susceptibility genes, regardless of family history, also has been proposed.8 Such a strategy has become increasingly realistic with decreasing cost and increasing availability of genetic testing. However, it would require increased genetic counseling resources to feasibly and equitably reach the target population and to explain the results to those patients and their relatives.
An alternative is to test the enriched population of family members of a patient with cancer who has been found to carry a pathogenic variant in a clinically relevant cancer susceptibility gene. This type of testing is termed cascade genetic testing. Cascade testing in first-degree family members carries a 50% probability of detecting the same pathogenic mutation. A related testing model is traceback testing where genetic testing is performed on pathology or tumor registry specimens from deceased patients with cancer.9 This genetic testing information is then provided to the family. Traceback models of genetic testing are an active area of research but can introduce ethical dilemmas. The more widely accepted cascade testing starts with the testing of a living patient affected with cancer. A recent article demonstrated the feasibility of a cascade testing model. Using a multiple linear regression model, the authors determined that all carriers of pathogenic mutations in 18 clinically relevant cancer susceptibility genes in the United States could be identified in 9.9 years if there was a 70% cascade testing rate of first-, second- and third-degree relatives, compared to 59.5 years with no cascade testing.10
Gaps in practice
Identification of mutation carriers, either through screening triggered by family history or through testing of patients affected with cancer, represents a gap between guidelines and clinical practice. Current NCCN guidelines outline genetic testing criteria for hereditary breast and ovarian cancer syndrome and for hereditary colorectal cancer. Despite well-established criteria, a survey in the United States revealed that only 19% of primary care providers were able to accurately assess family history for BRCA1 and 2 testing.11 Looking at patients who meet criteria for testing for Lynch syndrome, only 1 in 4 individuals have undergone genetic testing.12 Among patients diagnosed with breast and ovarian cancer, current NCCN guidelines recommend germline genetic testing for all patients with epithelial ovarian cancer; emerging evidence suggests all patients with breast cancer should be offered germline genetic testing.7,13 Large population-based studies have repeatedly demonstrated that testing rates fall short of this goal, with only 10% to 30% of patients undergoing genetic testing.9,14
Among families with a known hereditary mutation, rates of cascade genetic testing are also low, ranging from 17% to 50%.15-18 Evidence-based management guidelines, for both hereditary breast and ovarian cancer as well as Lynch syndrome, have been shown to reduce mortality.19,20 Failure to identify patients who carry these genetic mutations equates to increased mortality for our patients.
Barriers to cascade genetic testing
Cascade genetic testing ideally would be performed on entire families. Actual practice is far from ideal, and barriers to cascade testing exist. Barriers encompass resistance on the part of the family and provider as well as environmental or system factors.
Family factors
Because of privacy laws, the responsibility of disclosure of genetic testing results to family members falls primarily to the patient. Proband education is critical to ensure disclosure amongst family members. Family dynamics and geographic distribution of family members can further complicate disclosure. Following disclosure, family member gender, education, and demographics as well as personal views, attitudes, and emotions affect whether a family member decides to undergo testing.21 Furthermore, insurance status and awareness of and access to specialty-specific care for the proband’s family members may influence cascade genetic testing rates.
Provider factors
Provider factors that affect cascade genetic testing include awareness of testing guidelines, interpretation of genetic testing results, and education and knowledge of specific mutations. For instance, providers must recognize that cascade testing is not appropriate for variants of uncertain significance. This can lead to unnecessary surveillance testing and prophylactic surgeries. Providers, however, must continue to follow patients and periodically update testing results as variants may be reclassified over time. Additionally, providers must be knowledgeable about the complex and nuanced nature of the screening guidelines for each mutation. The NCCN provides detailed recommendations by mutation.7 Patients may benefit from care with cancer specialists who are aware of the guidelines, particularly for moderate-penetrance genes like BRIP1 and PALB2, as discussions about the timing of risk-reducing surgery are more nuanced in this population. Finally, which providers are responsible for facilitating cascade testing may be unclear; oncologists and genetic counselors not primarily treating probands’ relatives may assume the proper information has been passed along to family members without a practical means to follow up, and primary care providers may assume it is being taken care of by the oncology provider.
Continue to: Environmental or system factors...
Environmental or system factors
Accessibility of genetic counseling and testing is a common barrier to cascade testing. Family members may be geographically remote and connecting them to counseling and testing can be challenging. Working with local genetic counselors can facilitate this process. Insurance coverage of testing is a common perceived barrier; however, many testing companies now provide cascade testing free of charge if within a certain window from the initial test. Despite this, patients often site cost as a barrier to undergoing testing. Concerns about insurance coverage are common after a positive result. The Genetic Information Nondiscrimination Act of 2008 prohibits discrimination against employees or insurance applicants because of genetic information. Life insurance or long-term care policies, however, can incorporate genetic testing information into policy rates, so patients should be recommended to consider purchasing life insurance prior to undergoing genetic testing. This is especially important if the person considering testing has not yet been diagnosed with cancer.
Implications of a positive result
Family members who receive a positive test result should be referred for genetic counseling and to the appropriate specialists for evidence-based screening and discussion for risk-reducing surgery (FIGURE).7 For mutations associated with hereditary breast and ovarian cancer, referral to breast and gynecologic surgeons with expertise in risk reducing surgery is critical as the risk of diagnosing an occult malignancy is approximately 1%.22 Surgical technique with a 2-cm margin on the
Patient resources: decision aids, websites
As genetic testing becomes more accessible and people are tested at younger ages, studies examining the balance of risk reduction and quality of life (QOL) are increasingly important. Fertility concerns, effects of early menopause, and the interrelatedness between decisions for breast and gynecologic risk reduction should all be considered in the counseling for surgical risk reduction. Patient decision aids can help mutation carriers navigate the complex information and decisions.25 Websites specifically designed by advocacy groups can be useful adjuncts to in-office counseling (Facing Our Risk Empowered, FORCE; Facingourrisk.org).
Family letters
The American College of Obstetricians and Gynecologists recommends an ObGyn have a letter or documentation stating that the patient’s relative has a specific mutation before initiating cascade testing for an at-risk family member. The indicated test (such as BRCA1) should be ordered only after the patient has been counseled about potential outcomes and has expressly decided to be tested.26 Letters, such as the example given in the American College of Obstetricians and Gynecologists practice bulletin,26 are a key component of communication between oncology providers, probands, family members, and their primary care providers. ObGyn providers should work together with genetic counselors and gynecologic oncologists to determine the most efficient strategies in their communities.
Technology
Access to genetic testing and genetic counseling has been improved with the rise in telemedicine. Geographically remote patients can now access genetic counseling through medical center–based counselors as well as company-provided genetic counseling over the phone. Patients also can submit samples remotely without needing to be tested in a doctor’s office.
Databases from cancer centers that detail cascade genetic testing rates. As the preventive impact of cascade genetic testing becomes clearer, strategies to have recurrent discussions with cancer patients regarding their family members’ risk should be implemented. It is still unclear which providers—genetic counselors, gynecologic oncologists, medical oncologists, breast surgeons, ObGyns, to name a few—are primarily responsible for remembering to have these follow-up discussions, and despite advances, the burden still rests on the cancer patient themselves. Databases with automated follow-up surveys done every 6 to 12 months could provide some aid to busy providers in this regard.
Emerging research
If gynecologic risk-reducing surgery is chosen, clinical trial involvement should be encouraged. The Women Choosing Surgical Prevention (NCT02760849) in the United States and the TUBA study (NCT02321228) in the Netherlands were designed to compare menopause-related QOL between standard risk-reducing salpingo-oophorectomy (RRSO) and the innovative risk-reducing salpingectomy with delayed oophorectomy for mutation carriers. Results from the nonrandomized controlled TUBA trial suggest that patients have better menopause-related QOL after risk-reducing salpingectomy than after RRSO, regardless of hormone replacement therapy.27 International collaboration is continuing to better understand oncologic safety. In the United States, the SOROCk trial (NCT04251052) is a noninferiority surgical choice study underway for BRCA1 mutation carriers aged 35 to 50, powered to determine oncologic outcome differences in addition to QOL outcomes between RRSO and delayed oophorectomy arms.
Returning to the case
The patient and her family underwent genetic counseling. The patient’s 2 daughters, each in their 50s, underwent cascade genetic testing and were found to carry the same pathogenic mutation in BRCA2. After counseling from both breast and gynecologic surgeons, they both elected to undergo risk reducing bilateral salpingo-oophorectomy with hysterectomy. Both now complete regular screening for breast cancer and melanoma with plans to start screening for pancreatic cancer. Both are currently cancer free.
Summary
Cascade genetic testing is an efficient strategy to identify mutation carriers for hereditary breast and ovarian cancer syndrome. Implementation of the best patient-centric care will require continued collaboration and communication across and within disciplines. ●
Cascade, or targeted, genetic testing within families known to carry a hereditary mutation in a cancer susceptibility gene should be performed on all living first-degree family members over the age of 18. All mutation carriers should be connected to a multidisciplinary care team (FIGURE) to ensure implementation of evidence-based screening and risk-reducing surgery for cancer prevention. If gynecologic risk-reducing surgery is chosen, clinical trial involvement should be encouraged.
- Gabai-Kapara E, Lahad A, Kaufman B, et al. Population-based screening for breast and ovarian cancer risk due to BRCA1 and BRCA2. Proc Natl Acad Sci U S A. 2014;111:14205-14210.
- Norquist BM, Harrell MI, Brady MF, et al. Inherited mutations in women with ovarian carcinoma. JAMA Oncol. 2016;2:482-490.
- Yamauchi H, Takei J. Management of hereditary breast and ovarian cancer. Int J Clin Oncol. 2018;23:45-51.
- Kahn RM, Gordhandas S, Maddy BP, et al. Universal endometrial cancer tumor typing: how much has immunohistochemistry, microsatellite instability, and MLH1 methylation improved the diagnosis of Lynch syndrome across the population? Cancer. 2019;125:3172-3183.
- Jasperson KW, Tuohy TM, Neklason DW, et al. Hereditary and familial colon cancer. Gastroenterology. 2010;138:2044-2058.
- Gupta S, Provenzale D, Llor X, et al. NCCN guidelines insights: genetic/familial high-risk assessment: colorectal, version 2.2019. J Natl Compr Canc Netw. 2019;17:1032-1041.
- Daly MB, Pal T, Berry MP, et al. Genetic/familial high-risk assessment: breast, ovarian, and pancreatic, version 2.2021, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2021;19:77-102.
- King MC, Levy-Lahad E, Lahad A. Population-based screening for BRCA1 and BRCA2: 2014 Lasker Award. JAMA. 2014;312:1091-1092.
- Samimi G, et al. Traceback: a proposed framework to increase identification and genetic counseling of BRCA1 and BRCA2 mutation carriers through family-based outreach. J Clin Oncol. 2017;35:2329-2337.
- Offit K, Tkachuk KA, Stadler ZK, et al. Cascading after peridiagnostic cancer genetic testing: an alternative to population-based screening. J Clin Oncol. 2020;38:1398-1408.
- Bellcross CA, Kolor K, Goddard KAB, et al. Awareness and utilization of BRCA1/2 testing among U.S. primary care physicians. Am J Prev Med. 2011;40:61-66.
- Cross DS, Rahm AK, Kauffman TL, et al. Underutilization of Lynch syndrome screening in a multisite study of patients with colorectal cancer. Genet Med. 2013;15:933-940.
- Beitsch PD, Whitworth PW, Hughes K, et al. Underdiagnosis of hereditary breast cancer: are genetic testing guidelines a tool or an obstacle? J Clin Oncol. 2019;37:453-460.
- Childers CP, Childers KK, Maggard-Gibbons M, et al. National estimates of genetic testing in women with a history of breast or ovarian cancer. J Clin Oncol. 2017;35:3800-3806.
- Samadder NJ, Riegert-Johnson D, Boardman L, et al. Comparison of universal genetic testing vs guideline-directed targeted testing for patients with hereditary cancer syndrome. JAMA Oncol. 2021;7:230-237.
- Sharaf RN, Myer P, Stave CD, et al. Uptake of genetic testing by relatives of Lynch syndrome probands: a systematic review. Clin Gastroenterol Hepatol. 2013;11:1093-1100.
- Menko FH, Ter Stege JA, van der Kolk LE, et al. The uptake of presymptomatic genetic testing in hereditary breast-ovarian cancer and Lynch syndrome: a systematic review of the literature and implications for clinical practice. Fam Cancer. 2019;18:127-135.
- Griffin NE, Buchanan TR, Smith SH, et al. Low rates of cascade genetic testing among families with hereditary gynecologic cancer: an opportunity to improve cancer prevention. Gynecol Oncol. 2020;156:140-146.
- Roberts MC, Dotson WD, DeVore CS, et al. Delivery of cascade screening for hereditary conditions: a scoping review of the literature. Health Aff (Millwood). 2018;37:801-808.
- Finch AP, Lubinski J, Møller P, et al. Impact of oophorectomy on cancer incidence and mortality in women with a BRCA1 or BRCA2 mutation. J Clin Oncol. 2014;32:1547-1553.
- Srinivasan S, Won NY, Dotson WD, et al. Barriers and facilitators for cascade testing in genetic conditions: a systematic review. Eur J Hum Genet. 2020;28:1631-1644.
- Piedimonte S, Frank C, Laprise C, et al. Occult tubal carcinoma after risk-reducing salpingo-oophorectomy: a systematic review. Obstet Gynecol. 2020;135:498-508.
- Shu CA, Pike MC, Jotwani AR, et al. Uterine cancer after risk-reducing salpingo-oophorectomy without hysterectomy in women with BRCA mutations. JAMA Oncol. 2016;2:1434-1440.
- Gordhandas S, Norquist BM, Pennington KP, et al. Hormone replacement therapy after risk reducing salpingo-oophorectomy in patients with BRCA1 or BRCA2 mutations; a systematic review of risks and benefits. Gynecol Oncol. 2019;153:192-200.
- Steenbeek MP, van Bommel MHD, Harmsen MG, et al. Evaluation of a patient decision aid for BRCA1/2 pathogenic variant carriers choosing an ovarian cancer prevention strategy. Gynecol Oncol. 2021;163:371-377.
- Committee on Gynecologic Practice. ACOG committee opinion No. 727: Cascade testing: testing women for known hereditary genetic mutations associated with cancer. Obstet Gynecol. 2018;131:E31-E34.
- Steenbeek MP, Harmsen MG, Hoogerbrugge N, et al. Association of salpingectomy with delayed oophorectomy versus salpingo-oophorectomy with quality of life in BRCA1/2 pathogenic variant carriers: a nonrandomized controlled trial. JAMA Oncol. 2021;7:1203-1212.
- Gabai-Kapara E, Lahad A, Kaufman B, et al. Population-based screening for breast and ovarian cancer risk due to BRCA1 and BRCA2. Proc Natl Acad Sci U S A. 2014;111:14205-14210.
- Norquist BM, Harrell MI, Brady MF, et al. Inherited mutations in women with ovarian carcinoma. JAMA Oncol. 2016;2:482-490.
- Yamauchi H, Takei J. Management of hereditary breast and ovarian cancer. Int J Clin Oncol. 2018;23:45-51.
- Kahn RM, Gordhandas S, Maddy BP, et al. Universal endometrial cancer tumor typing: how much has immunohistochemistry, microsatellite instability, and MLH1 methylation improved the diagnosis of Lynch syndrome across the population? Cancer. 2019;125:3172-3183.
- Jasperson KW, Tuohy TM, Neklason DW, et al. Hereditary and familial colon cancer. Gastroenterology. 2010;138:2044-2058.
- Gupta S, Provenzale D, Llor X, et al. NCCN guidelines insights: genetic/familial high-risk assessment: colorectal, version 2.2019. J Natl Compr Canc Netw. 2019;17:1032-1041.
- Daly MB, Pal T, Berry MP, et al. Genetic/familial high-risk assessment: breast, ovarian, and pancreatic, version 2.2021, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2021;19:77-102.
- King MC, Levy-Lahad E, Lahad A. Population-based screening for BRCA1 and BRCA2: 2014 Lasker Award. JAMA. 2014;312:1091-1092.
- Samimi G, et al. Traceback: a proposed framework to increase identification and genetic counseling of BRCA1 and BRCA2 mutation carriers through family-based outreach. J Clin Oncol. 2017;35:2329-2337.
- Offit K, Tkachuk KA, Stadler ZK, et al. Cascading after peridiagnostic cancer genetic testing: an alternative to population-based screening. J Clin Oncol. 2020;38:1398-1408.
- Bellcross CA, Kolor K, Goddard KAB, et al. Awareness and utilization of BRCA1/2 testing among U.S. primary care physicians. Am J Prev Med. 2011;40:61-66.
- Cross DS, Rahm AK, Kauffman TL, et al. Underutilization of Lynch syndrome screening in a multisite study of patients with colorectal cancer. Genet Med. 2013;15:933-940.
- Beitsch PD, Whitworth PW, Hughes K, et al. Underdiagnosis of hereditary breast cancer: are genetic testing guidelines a tool or an obstacle? J Clin Oncol. 2019;37:453-460.
- Childers CP, Childers KK, Maggard-Gibbons M, et al. National estimates of genetic testing in women with a history of breast or ovarian cancer. J Clin Oncol. 2017;35:3800-3806.
- Samadder NJ, Riegert-Johnson D, Boardman L, et al. Comparison of universal genetic testing vs guideline-directed targeted testing for patients with hereditary cancer syndrome. JAMA Oncol. 2021;7:230-237.
- Sharaf RN, Myer P, Stave CD, et al. Uptake of genetic testing by relatives of Lynch syndrome probands: a systematic review. Clin Gastroenterol Hepatol. 2013;11:1093-1100.
- Menko FH, Ter Stege JA, van der Kolk LE, et al. The uptake of presymptomatic genetic testing in hereditary breast-ovarian cancer and Lynch syndrome: a systematic review of the literature and implications for clinical practice. Fam Cancer. 2019;18:127-135.
- Griffin NE, Buchanan TR, Smith SH, et al. Low rates of cascade genetic testing among families with hereditary gynecologic cancer: an opportunity to improve cancer prevention. Gynecol Oncol. 2020;156:140-146.
- Roberts MC, Dotson WD, DeVore CS, et al. Delivery of cascade screening for hereditary conditions: a scoping review of the literature. Health Aff (Millwood). 2018;37:801-808.
- Finch AP, Lubinski J, Møller P, et al. Impact of oophorectomy on cancer incidence and mortality in women with a BRCA1 or BRCA2 mutation. J Clin Oncol. 2014;32:1547-1553.
- Srinivasan S, Won NY, Dotson WD, et al. Barriers and facilitators for cascade testing in genetic conditions: a systematic review. Eur J Hum Genet. 2020;28:1631-1644.
- Piedimonte S, Frank C, Laprise C, et al. Occult tubal carcinoma after risk-reducing salpingo-oophorectomy: a systematic review. Obstet Gynecol. 2020;135:498-508.
- Shu CA, Pike MC, Jotwani AR, et al. Uterine cancer after risk-reducing salpingo-oophorectomy without hysterectomy in women with BRCA mutations. JAMA Oncol. 2016;2:1434-1440.
- Gordhandas S, Norquist BM, Pennington KP, et al. Hormone replacement therapy after risk reducing salpingo-oophorectomy in patients with BRCA1 or BRCA2 mutations; a systematic review of risks and benefits. Gynecol Oncol. 2019;153:192-200.
- Steenbeek MP, van Bommel MHD, Harmsen MG, et al. Evaluation of a patient decision aid for BRCA1/2 pathogenic variant carriers choosing an ovarian cancer prevention strategy. Gynecol Oncol. 2021;163:371-377.
- Committee on Gynecologic Practice. ACOG committee opinion No. 727: Cascade testing: testing women for known hereditary genetic mutations associated with cancer. Obstet Gynecol. 2018;131:E31-E34.
- Steenbeek MP, Harmsen MG, Hoogerbrugge N, et al. Association of salpingectomy with delayed oophorectomy versus salpingo-oophorectomy with quality of life in BRCA1/2 pathogenic variant carriers: a nonrandomized controlled trial. JAMA Oncol. 2021;7:1203-1212.

Large analysis confirms safety of nipple-sparing mastectomy
A new analysis of over 22,000 mastectomy patients confirms what smaller studies have indicated: Patients who undergo nipple-sparing mastectomy have overall and disease-free survival similar to that of those who receive a total mastectomy.
When nipple-sparing mastectomy was introduced, many experts felt uneasy about opting for the less invasive procedure, recalled Rosa Hwang, MD, associate medical director for breast surgery at MD Anderson Cancer Center in Houston. “The concern was leaving all this skin,” said Dr. Hwang. “Are you going to leave cancer behind” and increase the risk of local recurrence?
Over the past 2 decades, the number of patients undergoing nipple-sparing mastectomy increased and, in turn, studies began to demonstrate the safety of the procedure.
However, large analyses evaluating long-term outcomes – namely, overall survival and breast cancer-specific survival – of nipple-sparing mastectomy were still lacking.
The latest study, published online Nov. 20 in Annals of Surgical Oncology, compared the long-term prognosis and survival benefits of nipple-sparing to total mastectomy in thousands of women. The analysis, which pulled data from the SEER cancer database, included 5,765 patients who underwent the nipple-sparing procedure and 17,289 patients who had a total mastectomy.
The authors found that overall survival and breast cancer–specific survival were similar for women undergoing nipple-sparing mastectomy and those receiving a total mastectomy. In fact, over the long-term, the nipple-sparing group slightly edged out the total mastectomy group in overall survival (94.61% vs. 93% at 5 years and 86.34% vs. 83.48% at 10 years, respectively) and in breast cancer-specific survival rates (96.16% vs. 95.74% at 5 years, and 92.2% vs. 91.37% at 10 years). The differences, however, were not significant.
The study also found that certain subgroups – including White women, women over age 46, those with a median household income of $70,000 or more, hormone receptor-positive, and HER2 negative – had significantly better overall survival rate with the nipple-sparing procedure (P < .05). However, the authors noted, the survival advantage in the nipple-sparing group did not extend to breast cancer–specific survival.
Dr. Hwang, who was not involved in the current analysis, said the significant overall survival result in the subgroup analysis was surprising because “there’s no biological reason why one would expect that to be true.”
Given that the subgroups did not demonstrate better breast cancer–specific survival, Dr. Hwang believes the overall survival finding may have more to do with comorbidities, which the study did not account for, than type of mastectomy.
When choosing who is eligible for a nipple-sparing mastectomy, “We’re more selective,” Dr. Hwang said. For instance, patients with uncontrolled diabetes or who smoke are unlikely to be candidates. “So, I think it’s possible that medical comorbidities and medical conditions between these groups [were] different.”
According to the authors, coding inconsistencies represent another possible weakness of the study. From 1998 to 2010, “the term ‘nipple-sparing mastectomy’ was coded as a [total mastectomy] with the ‘subcutaneous mastectomy’ code.” It’s possible that some patients receiving the nipple-sparing procedure before 2011 were not appropriately coded in the current study.
Moving forward, a large prospective study that includes comorbidities would be helpful, but overall the study helps validate that “nipple-sparing mastectomy is a safe operation for selected patients,” Dr. Hwang said.
A version of this article first appeared on Medscape.com.
A new analysis of over 22,000 mastectomy patients confirms what smaller studies have indicated: Patients who undergo nipple-sparing mastectomy have overall and disease-free survival similar to that of those who receive a total mastectomy.
When nipple-sparing mastectomy was introduced, many experts felt uneasy about opting for the less invasive procedure, recalled Rosa Hwang, MD, associate medical director for breast surgery at MD Anderson Cancer Center in Houston. “The concern was leaving all this skin,” said Dr. Hwang. “Are you going to leave cancer behind” and increase the risk of local recurrence?
Over the past 2 decades, the number of patients undergoing nipple-sparing mastectomy increased and, in turn, studies began to demonstrate the safety of the procedure.
However, large analyses evaluating long-term outcomes – namely, overall survival and breast cancer-specific survival – of nipple-sparing mastectomy were still lacking.
The latest study, published online Nov. 20 in Annals of Surgical Oncology, compared the long-term prognosis and survival benefits of nipple-sparing to total mastectomy in thousands of women. The analysis, which pulled data from the SEER cancer database, included 5,765 patients who underwent the nipple-sparing procedure and 17,289 patients who had a total mastectomy.
The authors found that overall survival and breast cancer–specific survival were similar for women undergoing nipple-sparing mastectomy and those receiving a total mastectomy. In fact, over the long-term, the nipple-sparing group slightly edged out the total mastectomy group in overall survival (94.61% vs. 93% at 5 years and 86.34% vs. 83.48% at 10 years, respectively) and in breast cancer-specific survival rates (96.16% vs. 95.74% at 5 years, and 92.2% vs. 91.37% at 10 years). The differences, however, were not significant.
The study also found that certain subgroups – including White women, women over age 46, those with a median household income of $70,000 or more, hormone receptor-positive, and HER2 negative – had significantly better overall survival rate with the nipple-sparing procedure (P < .05). However, the authors noted, the survival advantage in the nipple-sparing group did not extend to breast cancer–specific survival.
Dr. Hwang, who was not involved in the current analysis, said the significant overall survival result in the subgroup analysis was surprising because “there’s no biological reason why one would expect that to be true.”
Given that the subgroups did not demonstrate better breast cancer–specific survival, Dr. Hwang believes the overall survival finding may have more to do with comorbidities, which the study did not account for, than type of mastectomy.
When choosing who is eligible for a nipple-sparing mastectomy, “We’re more selective,” Dr. Hwang said. For instance, patients with uncontrolled diabetes or who smoke are unlikely to be candidates. “So, I think it’s possible that medical comorbidities and medical conditions between these groups [were] different.”
According to the authors, coding inconsistencies represent another possible weakness of the study. From 1998 to 2010, “the term ‘nipple-sparing mastectomy’ was coded as a [total mastectomy] with the ‘subcutaneous mastectomy’ code.” It’s possible that some patients receiving the nipple-sparing procedure before 2011 were not appropriately coded in the current study.
Moving forward, a large prospective study that includes comorbidities would be helpful, but overall the study helps validate that “nipple-sparing mastectomy is a safe operation for selected patients,” Dr. Hwang said.
A version of this article first appeared on Medscape.com.
A new analysis of over 22,000 mastectomy patients confirms what smaller studies have indicated: Patients who undergo nipple-sparing mastectomy have overall and disease-free survival similar to that of those who receive a total mastectomy.
When nipple-sparing mastectomy was introduced, many experts felt uneasy about opting for the less invasive procedure, recalled Rosa Hwang, MD, associate medical director for breast surgery at MD Anderson Cancer Center in Houston. “The concern was leaving all this skin,” said Dr. Hwang. “Are you going to leave cancer behind” and increase the risk of local recurrence?
Over the past 2 decades, the number of patients undergoing nipple-sparing mastectomy increased and, in turn, studies began to demonstrate the safety of the procedure.
However, large analyses evaluating long-term outcomes – namely, overall survival and breast cancer-specific survival – of nipple-sparing mastectomy were still lacking.
The latest study, published online Nov. 20 in Annals of Surgical Oncology, compared the long-term prognosis and survival benefits of nipple-sparing to total mastectomy in thousands of women. The analysis, which pulled data from the SEER cancer database, included 5,765 patients who underwent the nipple-sparing procedure and 17,289 patients who had a total mastectomy.
The authors found that overall survival and breast cancer–specific survival were similar for women undergoing nipple-sparing mastectomy and those receiving a total mastectomy. In fact, over the long-term, the nipple-sparing group slightly edged out the total mastectomy group in overall survival (94.61% vs. 93% at 5 years and 86.34% vs. 83.48% at 10 years, respectively) and in breast cancer-specific survival rates (96.16% vs. 95.74% at 5 years, and 92.2% vs. 91.37% at 10 years). The differences, however, were not significant.
The study also found that certain subgroups – including White women, women over age 46, those with a median household income of $70,000 or more, hormone receptor-positive, and HER2 negative – had significantly better overall survival rate with the nipple-sparing procedure (P < .05). However, the authors noted, the survival advantage in the nipple-sparing group did not extend to breast cancer–specific survival.
Dr. Hwang, who was not involved in the current analysis, said the significant overall survival result in the subgroup analysis was surprising because “there’s no biological reason why one would expect that to be true.”
Given that the subgroups did not demonstrate better breast cancer–specific survival, Dr. Hwang believes the overall survival finding may have more to do with comorbidities, which the study did not account for, than type of mastectomy.
When choosing who is eligible for a nipple-sparing mastectomy, “We’re more selective,” Dr. Hwang said. For instance, patients with uncontrolled diabetes or who smoke are unlikely to be candidates. “So, I think it’s possible that medical comorbidities and medical conditions between these groups [were] different.”
According to the authors, coding inconsistencies represent another possible weakness of the study. From 1998 to 2010, “the term ‘nipple-sparing mastectomy’ was coded as a [total mastectomy] with the ‘subcutaneous mastectomy’ code.” It’s possible that some patients receiving the nipple-sparing procedure before 2011 were not appropriately coded in the current study.
Moving forward, a large prospective study that includes comorbidities would be helpful, but overall the study helps validate that “nipple-sparing mastectomy is a safe operation for selected patients,” Dr. Hwang said.
A version of this article first appeared on Medscape.com.
IUDs may increase background enhancement on breast MRI
Intrauterine contraceptive devices (IUDs) have been linked to increased background enhancement on breast MRI, according to research presented at the Radiological Society of North America 2021 annual meeting.
About 10.4% of women 15-49 years of age who use contraception have an IUD or contraceptive implant, according to the Centers for Disease Control and Prevention. Unlike oral or transdermal hormonal contraceptives and hormone replacement therapy, levonorgestrel-releasing IUDs release a small amount of the hormone directly into the uterus and are thought to have a much more localized effect, Luisa Huck, MD, the lead author of the study, said in an interview.
But women with IUDs have long reported adverse effects associated with other hormonal medication. “In the past, some women reported depression, headaches, sleep disorders, and panic attacks,” noted Dr. Huck, a radiology resident at RWTH Aachen University in Germany.
Christiane Kuhl, MD, chief of the department of radiology at RWTH Aachen University and senior author of the research, had also observed that women with hormonal IUDs often have increased background parenchymal enhancement (BPE) on contrast-enhanced MRI. BPE “has been established as a sensitive marker of hormonal stimulation of breast,” the study authors wrote, and previous studies have shown that women using hormonal medications have higher BPE on breast MRIs.
To better understand whether IUDs can increase BPE, Dr. Huck and colleagues used the hospital database to search for premenopausal women who had undergone breast MRIs for screening between January 2014 and July 2020. To be included, women had to have had at least two scans: one with and one without an IUD in place, with the scan conducted at least 4 weeks after IUD placement or removal. All women in the study had no history of breast cancer or hormone or antihormone intake.
The study involved 48 women with an average age of 45 years and a median of 27 months between the two scans. Forty-six of the women had the Mirena levonorgestrel-releasing IUD and two had the Jaydess IUD. To account for hormone variations between patients, the researchers used each patient as their own reference point. To control for age-related effects, 25 women had their first MRI without an IUD and their second scan with an IUD in place. The second group of 23 women underwent their first MRI with an IUD and had it removed before the second scan.
Hormonal effects on breast enhancement are very complex, and hormonal stimulation is not always predictably correlated with changes on MRI imaging.
For 23 women in the study, background enhancement was higher on scans with the IUD than without (P < .001). For 24 women, there was no change in BPE with or without an IUD, and one woman had lower BPE with an IUD than without.
“It is very interesting and relevant to practice to consider that the presence of an intrauterine device would have potential impact on the enhancement we see in the breast on MRI imaging,” Samantha Heller, MD, PhD, associate professor of radiology at New York University, said in an interview.
However, the study used BPE as a measure for hormonal shifts, and “hormonal effects on breast enhancement are very complex, and hormonal stimulation is not always predictably correlated with changes on MRI imaging,” she noted. BPE on MRI can fluctuate, so testing actual hormone levels in patients with elevated BPE could be helpful to identify hormonal shifts, she added. It is also important to understand why half of the women in the study showed no variation in BPE, she said.
The study findings are not very surprising, considering that it is known that low levels of progesterone from IUDs circulate in the blood stream, Frances Casey, MD, MPH, associate professor in the department of obstetrics and gynecology at Virginia Commonwealth University in Richmond, said in an interview. They do not suggest that there should be any changes to IUD guidelines, she added.
However, “the study findings raise the question as to whether IUD status should be documented as a matter of course prior to performing breast MRI,” said Dr. Heller. “It is standard to document the timing of a woman’s menstrual cycle, as well as to note any hormone suppression or replacement therapy. This is in part so that the radiologist may understand the etiology of any observed variation in background enhancement,” she explained.
Although increased enhancement on MRI has sometimes been linked to higher chances of recommendations for additional imaging or biopsies, she noted, “more work would be needed to understand the impact – if any – of an IUD on breast MRI recommendations due to enhancement changes.”
Dr. Huck, Dr. Heller, and Dr. Casey disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Intrauterine contraceptive devices (IUDs) have been linked to increased background enhancement on breast MRI, according to research presented at the Radiological Society of North America 2021 annual meeting.
About 10.4% of women 15-49 years of age who use contraception have an IUD or contraceptive implant, according to the Centers for Disease Control and Prevention. Unlike oral or transdermal hormonal contraceptives and hormone replacement therapy, levonorgestrel-releasing IUDs release a small amount of the hormone directly into the uterus and are thought to have a much more localized effect, Luisa Huck, MD, the lead author of the study, said in an interview.
But women with IUDs have long reported adverse effects associated with other hormonal medication. “In the past, some women reported depression, headaches, sleep disorders, and panic attacks,” noted Dr. Huck, a radiology resident at RWTH Aachen University in Germany.
Christiane Kuhl, MD, chief of the department of radiology at RWTH Aachen University and senior author of the research, had also observed that women with hormonal IUDs often have increased background parenchymal enhancement (BPE) on contrast-enhanced MRI. BPE “has been established as a sensitive marker of hormonal stimulation of breast,” the study authors wrote, and previous studies have shown that women using hormonal medications have higher BPE on breast MRIs.
To better understand whether IUDs can increase BPE, Dr. Huck and colleagues used the hospital database to search for premenopausal women who had undergone breast MRIs for screening between January 2014 and July 2020. To be included, women had to have had at least two scans: one with and one without an IUD in place, with the scan conducted at least 4 weeks after IUD placement or removal. All women in the study had no history of breast cancer or hormone or antihormone intake.
The study involved 48 women with an average age of 45 years and a median of 27 months between the two scans. Forty-six of the women had the Mirena levonorgestrel-releasing IUD and two had the Jaydess IUD. To account for hormone variations between patients, the researchers used each patient as their own reference point. To control for age-related effects, 25 women had their first MRI without an IUD and their second scan with an IUD in place. The second group of 23 women underwent their first MRI with an IUD and had it removed before the second scan.
Hormonal effects on breast enhancement are very complex, and hormonal stimulation is not always predictably correlated with changes on MRI imaging.
For 23 women in the study, background enhancement was higher on scans with the IUD than without (P < .001). For 24 women, there was no change in BPE with or without an IUD, and one woman had lower BPE with an IUD than without.
“It is very interesting and relevant to practice to consider that the presence of an intrauterine device would have potential impact on the enhancement we see in the breast on MRI imaging,” Samantha Heller, MD, PhD, associate professor of radiology at New York University, said in an interview.
However, the study used BPE as a measure for hormonal shifts, and “hormonal effects on breast enhancement are very complex, and hormonal stimulation is not always predictably correlated with changes on MRI imaging,” she noted. BPE on MRI can fluctuate, so testing actual hormone levels in patients with elevated BPE could be helpful to identify hormonal shifts, she added. It is also important to understand why half of the women in the study showed no variation in BPE, she said.
The study findings are not very surprising, considering that it is known that low levels of progesterone from IUDs circulate in the blood stream, Frances Casey, MD, MPH, associate professor in the department of obstetrics and gynecology at Virginia Commonwealth University in Richmond, said in an interview. They do not suggest that there should be any changes to IUD guidelines, she added.
However, “the study findings raise the question as to whether IUD status should be documented as a matter of course prior to performing breast MRI,” said Dr. Heller. “It is standard to document the timing of a woman’s menstrual cycle, as well as to note any hormone suppression or replacement therapy. This is in part so that the radiologist may understand the etiology of any observed variation in background enhancement,” she explained.
Although increased enhancement on MRI has sometimes been linked to higher chances of recommendations for additional imaging or biopsies, she noted, “more work would be needed to understand the impact – if any – of an IUD on breast MRI recommendations due to enhancement changes.”
Dr. Huck, Dr. Heller, and Dr. Casey disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Intrauterine contraceptive devices (IUDs) have been linked to increased background enhancement on breast MRI, according to research presented at the Radiological Society of North America 2021 annual meeting.
About 10.4% of women 15-49 years of age who use contraception have an IUD or contraceptive implant, according to the Centers for Disease Control and Prevention. Unlike oral or transdermal hormonal contraceptives and hormone replacement therapy, levonorgestrel-releasing IUDs release a small amount of the hormone directly into the uterus and are thought to have a much more localized effect, Luisa Huck, MD, the lead author of the study, said in an interview.
But women with IUDs have long reported adverse effects associated with other hormonal medication. “In the past, some women reported depression, headaches, sleep disorders, and panic attacks,” noted Dr. Huck, a radiology resident at RWTH Aachen University in Germany.
Christiane Kuhl, MD, chief of the department of radiology at RWTH Aachen University and senior author of the research, had also observed that women with hormonal IUDs often have increased background parenchymal enhancement (BPE) on contrast-enhanced MRI. BPE “has been established as a sensitive marker of hormonal stimulation of breast,” the study authors wrote, and previous studies have shown that women using hormonal medications have higher BPE on breast MRIs.
To better understand whether IUDs can increase BPE, Dr. Huck and colleagues used the hospital database to search for premenopausal women who had undergone breast MRIs for screening between January 2014 and July 2020. To be included, women had to have had at least two scans: one with and one without an IUD in place, with the scan conducted at least 4 weeks after IUD placement or removal. All women in the study had no history of breast cancer or hormone or antihormone intake.
The study involved 48 women with an average age of 45 years and a median of 27 months between the two scans. Forty-six of the women had the Mirena levonorgestrel-releasing IUD and two had the Jaydess IUD. To account for hormone variations between patients, the researchers used each patient as their own reference point. To control for age-related effects, 25 women had their first MRI without an IUD and their second scan with an IUD in place. The second group of 23 women underwent their first MRI with an IUD and had it removed before the second scan.
Hormonal effects on breast enhancement are very complex, and hormonal stimulation is not always predictably correlated with changes on MRI imaging.
For 23 women in the study, background enhancement was higher on scans with the IUD than without (P < .001). For 24 women, there was no change in BPE with or without an IUD, and one woman had lower BPE with an IUD than without.
“It is very interesting and relevant to practice to consider that the presence of an intrauterine device would have potential impact on the enhancement we see in the breast on MRI imaging,” Samantha Heller, MD, PhD, associate professor of radiology at New York University, said in an interview.
However, the study used BPE as a measure for hormonal shifts, and “hormonal effects on breast enhancement are very complex, and hormonal stimulation is not always predictably correlated with changes on MRI imaging,” she noted. BPE on MRI can fluctuate, so testing actual hormone levels in patients with elevated BPE could be helpful to identify hormonal shifts, she added. It is also important to understand why half of the women in the study showed no variation in BPE, she said.
The study findings are not very surprising, considering that it is known that low levels of progesterone from IUDs circulate in the blood stream, Frances Casey, MD, MPH, associate professor in the department of obstetrics and gynecology at Virginia Commonwealth University in Richmond, said in an interview. They do not suggest that there should be any changes to IUD guidelines, she added.
However, “the study findings raise the question as to whether IUD status should be documented as a matter of course prior to performing breast MRI,” said Dr. Heller. “It is standard to document the timing of a woman’s menstrual cycle, as well as to note any hormone suppression or replacement therapy. This is in part so that the radiologist may understand the etiology of any observed variation in background enhancement,” she explained.
Although increased enhancement on MRI has sometimes been linked to higher chances of recommendations for additional imaging or biopsies, she noted, “more work would be needed to understand the impact – if any – of an IUD on breast MRI recommendations due to enhancement changes.”
Dr. Huck, Dr. Heller, and Dr. Casey disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Risk for breast cancer recurrence persists past 30 years
The data come from a Danish study involving 20,315 women who were treated for early operable breast cancer between 1987 and 2004, all of whom were disease-free at 10 years.
Further follow-up showed that 2,595 women had a breast cancer recurrence more than 10 years after their primary diagnosis.
The cumulative incidence of recurrence was 8.5% at 15 years; 12.5% at 20 years; 15.2% at 25 years, and 16.6% at 32 years.
Recurrence risk was greatest early in the study period.
Women who had primary tumors larger than 20 mm, lymph node-positive disease, and estrogen receptor-positive tumors were at higher risk for late recurrence.
“Such patients may warrant extended surveillance, more aggressive treatment, or new therapy approaches,” said the investigators, led by Rikke Pedersen, MD, a PhD candidate in epidemiology at Aarhus University Hospital, Denmark.
“Our observed high cumulative incidence of late breast cancer recurrence is a concern given the increasing prevalence of long-term survivors.” Among other things, a new model to better select women for prolonged surveillance is needed, they said.
The new findings were published online Nov. 8 in the Journal of the National Cancer Institute (NCI).
This study confirms previous investigations, but it is the first to report that breast cancer can recur more than 30 years after diagnosis, note the authors of an accompanying editorial, Serban Negoita, MD, DrPH, and Esmeralda Ramirez-Peña, PhD, MPH, both from the National Cancer Institute.
The caveat is that treatment has evolved considerably since the women in the study were diagnosed, so the prognostic value of the findings with current treatment regimens is uncertain, they note. Some studies haven’t found a recurrence benefit for aggressive upfront treatment, but those studies had shorter follow-ups.
Research into the issue is “increasingly important” to guide clinical management and counsel women who are living longer after their primary diagnosis, they comment.
Further details from the study
Data for the study came from the Danish Breast Cancer Group clinical database and other national databases. The researchers focused on women who were disease-free at 10 years after their primary diagnosis, which was stage I or II disease. Median age was 55 years.
Cumulative incidence for breast cancer recurrence was highest for grade 1 tumors with four or more positive lymph nodes (37.9% 10-25 years after the primary diagnosis) and was lowest for patients with grade 3 disease and no involved lymph nodes (7.5%).
The finding of higher recurrence incidence with lower grade tumors goes against some previous reports, the researchers commented. It may be that some tumors considered lower risk decades ago, and treated accordingly, would be considered higher risk in more recent times.
The cumulative incidence of late recurrence was also higher in younger patients and those treated with breast-conserving surgery instead of mastectomy, the team reported.
Adjusted hazard ratios followed the incidence trends, with higher hazards of recurrence for women diagnosed before age 40 as well as those who had breast-conserving surgery, four or more positive lymph nodes, and primary tumors 20 mm or more across.
The work was funded by the Danish Cancer Society and Aarhus University. Lead author Dr. Pedersen reports no disclosures, but coauthors report ties to Amgen, Novo Nordisk, Roche, and other companies. The editorialists have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The data come from a Danish study involving 20,315 women who were treated for early operable breast cancer between 1987 and 2004, all of whom were disease-free at 10 years.
Further follow-up showed that 2,595 women had a breast cancer recurrence more than 10 years after their primary diagnosis.
The cumulative incidence of recurrence was 8.5% at 15 years; 12.5% at 20 years; 15.2% at 25 years, and 16.6% at 32 years.
Recurrence risk was greatest early in the study period.
Women who had primary tumors larger than 20 mm, lymph node-positive disease, and estrogen receptor-positive tumors were at higher risk for late recurrence.
“Such patients may warrant extended surveillance, more aggressive treatment, or new therapy approaches,” said the investigators, led by Rikke Pedersen, MD, a PhD candidate in epidemiology at Aarhus University Hospital, Denmark.
“Our observed high cumulative incidence of late breast cancer recurrence is a concern given the increasing prevalence of long-term survivors.” Among other things, a new model to better select women for prolonged surveillance is needed, they said.
The new findings were published online Nov. 8 in the Journal of the National Cancer Institute (NCI).
This study confirms previous investigations, but it is the first to report that breast cancer can recur more than 30 years after diagnosis, note the authors of an accompanying editorial, Serban Negoita, MD, DrPH, and Esmeralda Ramirez-Peña, PhD, MPH, both from the National Cancer Institute.
The caveat is that treatment has evolved considerably since the women in the study were diagnosed, so the prognostic value of the findings with current treatment regimens is uncertain, they note. Some studies haven’t found a recurrence benefit for aggressive upfront treatment, but those studies had shorter follow-ups.
Research into the issue is “increasingly important” to guide clinical management and counsel women who are living longer after their primary diagnosis, they comment.
Further details from the study
Data for the study came from the Danish Breast Cancer Group clinical database and other national databases. The researchers focused on women who were disease-free at 10 years after their primary diagnosis, which was stage I or II disease. Median age was 55 years.
Cumulative incidence for breast cancer recurrence was highest for grade 1 tumors with four or more positive lymph nodes (37.9% 10-25 years after the primary diagnosis) and was lowest for patients with grade 3 disease and no involved lymph nodes (7.5%).
The finding of higher recurrence incidence with lower grade tumors goes against some previous reports, the researchers commented. It may be that some tumors considered lower risk decades ago, and treated accordingly, would be considered higher risk in more recent times.
The cumulative incidence of late recurrence was also higher in younger patients and those treated with breast-conserving surgery instead of mastectomy, the team reported.
Adjusted hazard ratios followed the incidence trends, with higher hazards of recurrence for women diagnosed before age 40 as well as those who had breast-conserving surgery, four or more positive lymph nodes, and primary tumors 20 mm or more across.
The work was funded by the Danish Cancer Society and Aarhus University. Lead author Dr. Pedersen reports no disclosures, but coauthors report ties to Amgen, Novo Nordisk, Roche, and other companies. The editorialists have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The data come from a Danish study involving 20,315 women who were treated for early operable breast cancer between 1987 and 2004, all of whom were disease-free at 10 years.
Further follow-up showed that 2,595 women had a breast cancer recurrence more than 10 years after their primary diagnosis.
The cumulative incidence of recurrence was 8.5% at 15 years; 12.5% at 20 years; 15.2% at 25 years, and 16.6% at 32 years.
Recurrence risk was greatest early in the study period.
Women who had primary tumors larger than 20 mm, lymph node-positive disease, and estrogen receptor-positive tumors were at higher risk for late recurrence.
“Such patients may warrant extended surveillance, more aggressive treatment, or new therapy approaches,” said the investigators, led by Rikke Pedersen, MD, a PhD candidate in epidemiology at Aarhus University Hospital, Denmark.
“Our observed high cumulative incidence of late breast cancer recurrence is a concern given the increasing prevalence of long-term survivors.” Among other things, a new model to better select women for prolonged surveillance is needed, they said.
The new findings were published online Nov. 8 in the Journal of the National Cancer Institute (NCI).
This study confirms previous investigations, but it is the first to report that breast cancer can recur more than 30 years after diagnosis, note the authors of an accompanying editorial, Serban Negoita, MD, DrPH, and Esmeralda Ramirez-Peña, PhD, MPH, both from the National Cancer Institute.
The caveat is that treatment has evolved considerably since the women in the study were diagnosed, so the prognostic value of the findings with current treatment regimens is uncertain, they note. Some studies haven’t found a recurrence benefit for aggressive upfront treatment, but those studies had shorter follow-ups.
Research into the issue is “increasingly important” to guide clinical management and counsel women who are living longer after their primary diagnosis, they comment.
Further details from the study
Data for the study came from the Danish Breast Cancer Group clinical database and other national databases. The researchers focused on women who were disease-free at 10 years after their primary diagnosis, which was stage I or II disease. Median age was 55 years.
Cumulative incidence for breast cancer recurrence was highest for grade 1 tumors with four or more positive lymph nodes (37.9% 10-25 years after the primary diagnosis) and was lowest for patients with grade 3 disease and no involved lymph nodes (7.5%).
The finding of higher recurrence incidence with lower grade tumors goes against some previous reports, the researchers commented. It may be that some tumors considered lower risk decades ago, and treated accordingly, would be considered higher risk in more recent times.
The cumulative incidence of late recurrence was also higher in younger patients and those treated with breast-conserving surgery instead of mastectomy, the team reported.
Adjusted hazard ratios followed the incidence trends, with higher hazards of recurrence for women diagnosed before age 40 as well as those who had breast-conserving surgery, four or more positive lymph nodes, and primary tumors 20 mm or more across.
The work was funded by the Danish Cancer Society and Aarhus University. Lead author Dr. Pedersen reports no disclosures, but coauthors report ties to Amgen, Novo Nordisk, Roche, and other companies. The editorialists have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Many breast cancer patients use cannabis for symptom relief
Most (75%) of the patients who reported using cannabis said it was extremely helpful or very helpful in alleviating symptoms.
The authors warn of potential safety concerns with cannabis, especially with the use of unregulated products.
In addition, the survey found that physicians were not highly regarded as a source of information about cannabis use. Only 39% of patients said that they discussed cannabis with their physicians; 28% reported feeling uncomfortable when broaching the topic. Only 4% indicated that physicians were the most helpful source of information about cannabis.
The survey involved 612 patients with breast cancer. The results were published online Oct. 12 in Cancer.
“Our study highlights an important opportunity for providers to initiate informed conversations about medical cannabis with their patients, as the evidence shows that many are using medical cannabis without our knowledge or guidance,” said lead author Marisa Weiss, MD, of Breastcancer.org and the Lankenau Medical Center, near Philadelphia. “Not knowing whether or not our cancer patients are using cannabis is a major blind spot in our ability to provide optimal care,” she said.
Cannabis in one form or another has been legalized in many states across America, and even in states where it hasn’t been legalized, people are using it.
“Even though many states have relaxed their laws on cannabis, it remains a Schedule I drug on the federal level and is essentially still considered illegal,” commented Donald I. Abrams, MD, professor of medicine at the University of California, San Francisco, and an integrative oncologist at the UCSF Osher Center for Integrative Medicine. “This is why many physicians are uncomfortable discussing it with patients,” he said.
“Cannabis use isn’t taught in medical school, and until that changes, I don’t know how physicians are going to be advisers for this,” said Dr. Abrams, who was approached by this news organization for comment.
This “is a really nice study in that it looks at a large group of breast cancer patients from the community ... It’s not from a single institution [such as this previous study] and so a more representative mix,” Dr. Abrams said.
However, he also commented that the article had a “scent of ‘reefer madness’” about it, given its emphasis on potential harms and safety concerns.
“It’s interesting how alcohol is considered mainstream but cannabis has been demonized,” he said. “Especially for women with breast cancer, it’s so clear that alcohol is related to the development of postmenopausal breast cancer. As a recreational intervention, cannabis in my mind appears to be much safer for women for relaxation.”
“The one thing I worry about are patients who take highly concentrated CBD [cannabidiol] oil, as it can block the metabolism of prescription drugs and allow them to build up in the blood,” Dr. Abrams said. “I advise people against using these products.”
Cannabis to relieve symptoms
Previous studies have noted widespread use of cannabis among patients with cancer. For example, a large study from Israel that included nearly 3,000 participants found that cannabis use improved a variety of cancer-related symptoms, including nausea and vomiting, sleep disorders, pain, anxiety, and depression. Among those with cancer who survived to 6 months and who finished the study protocol, 60% achieved “treatment success.” Of note, at 6 months, 36% of patients had stopped taking opioids, and for 9.9%, the dose of opioids had decreased.
In the current study, dubbed the Coala-T-Cannabis study, the investigators approached U.S. members of the Breastcancer.org and Healthline.com communities who self-reported that they had been diagnosed with breast cancer within the past 5 years; 612 surveys were completed.
Half of all respondents said they had looked for information on medical cannabis, but most were unsatisfied with the information that they had received. Only 6% were extremely satisfied; 25% were very satisfied with the information.
Most patients (39%) did not discuss cannabis use with their physicians. Of those who did, 28% reported feeling uncomfortable discussing the topic. Only 4% of survey respondents indicated that physicians were the most helpful source of cannabis information.
Regarding which source of information was most helpful, 22% said websites, 18% said family members or friends, 12% said staffers and pharmacists in dispensaries, and 7% said other patients with breast cancer.
Forty-two percent of the survey respondents said they used cannabis for medical purposes and for relief of symptoms, which included pain (78%), insomnia (70%), anxiety (57%), stress (51%), and nausea/vomiting (46%).
In addition, 49% believed that medical cannabis could be used to treat the cancer itself.
A fair number were also using cannabis for recreational purposes. Of those who used cannabis, only 23% reported that they used it for medical purposes only.
Participants used cannabis in a variety of forms. The most popular form of consumption was as edibles (70%), followed by liquids/tinctures (65%), smoking (51%), topicals (46%), and vape pens (45%). Participants reported using an average of 3.7 different products.
Safety concerns?
The authors caution about the use of cannabis while receiving anticancer therapies because such use “raises important efficacy and safety concerns.”
“Many chemotherapy agents as well as cannabinoids are metabolized in the liver’s p450 cytochrome system,” Dr. Weiss and colleagues note, and the mechanism by which cannabinoids interact with particular CYP450 isoenzymes “has the potential to alter the metabolism of other medications and lead to adverse side effects.”
They also question the safety of some of the cannabis products that are being used. Participants reported receiving cannabis from a variety of sources, which included state-regulated dispensaries, “dealers,” and family/friends.
Three-quarters of respondents believed that cannabis was better than “chemicals” and that the benefits outweighed the risks. But many of the products used are unregulated, the authors point out.
“Providers should communicate clearly about the health and safety concerns associated with certain cannabis products and methods of delivery,” they conclude. “Without these measures, patients may make these decisions without qualified medical guidance, obtain poor-quality cannabis products, and consume them through potentially hazardous delivery methods during various types of cancer therapies.”
The study was supported by research grants from Ananda Health/Ecofibre and the Dr. Philip Reeves Legacy Fund. Several coauthors reported relationships with industry, as noted in the article. Dr. Abrams owns stock in Cannformatics and Lumen; he has received honorarium from Clever Leaves and Maui Grown Therapies and speaker honorarium from GW Pharmaceuticals.
A version of this article first appeared on Medscape.com.
Most (75%) of the patients who reported using cannabis said it was extremely helpful or very helpful in alleviating symptoms.
The authors warn of potential safety concerns with cannabis, especially with the use of unregulated products.
In addition, the survey found that physicians were not highly regarded as a source of information about cannabis use. Only 39% of patients said that they discussed cannabis with their physicians; 28% reported feeling uncomfortable when broaching the topic. Only 4% indicated that physicians were the most helpful source of information about cannabis.
The survey involved 612 patients with breast cancer. The results were published online Oct. 12 in Cancer.
“Our study highlights an important opportunity for providers to initiate informed conversations about medical cannabis with their patients, as the evidence shows that many are using medical cannabis without our knowledge or guidance,” said lead author Marisa Weiss, MD, of Breastcancer.org and the Lankenau Medical Center, near Philadelphia. “Not knowing whether or not our cancer patients are using cannabis is a major blind spot in our ability to provide optimal care,” she said.
Cannabis in one form or another has been legalized in many states across America, and even in states where it hasn’t been legalized, people are using it.
“Even though many states have relaxed their laws on cannabis, it remains a Schedule I drug on the federal level and is essentially still considered illegal,” commented Donald I. Abrams, MD, professor of medicine at the University of California, San Francisco, and an integrative oncologist at the UCSF Osher Center for Integrative Medicine. “This is why many physicians are uncomfortable discussing it with patients,” he said.
“Cannabis use isn’t taught in medical school, and until that changes, I don’t know how physicians are going to be advisers for this,” said Dr. Abrams, who was approached by this news organization for comment.
This “is a really nice study in that it looks at a large group of breast cancer patients from the community ... It’s not from a single institution [such as this previous study] and so a more representative mix,” Dr. Abrams said.
However, he also commented that the article had a “scent of ‘reefer madness’” about it, given its emphasis on potential harms and safety concerns.
“It’s interesting how alcohol is considered mainstream but cannabis has been demonized,” he said. “Especially for women with breast cancer, it’s so clear that alcohol is related to the development of postmenopausal breast cancer. As a recreational intervention, cannabis in my mind appears to be much safer for women for relaxation.”
“The one thing I worry about are patients who take highly concentrated CBD [cannabidiol] oil, as it can block the metabolism of prescription drugs and allow them to build up in the blood,” Dr. Abrams said. “I advise people against using these products.”
Cannabis to relieve symptoms
Previous studies have noted widespread use of cannabis among patients with cancer. For example, a large study from Israel that included nearly 3,000 participants found that cannabis use improved a variety of cancer-related symptoms, including nausea and vomiting, sleep disorders, pain, anxiety, and depression. Among those with cancer who survived to 6 months and who finished the study protocol, 60% achieved “treatment success.” Of note, at 6 months, 36% of patients had stopped taking opioids, and for 9.9%, the dose of opioids had decreased.
In the current study, dubbed the Coala-T-Cannabis study, the investigators approached U.S. members of the Breastcancer.org and Healthline.com communities who self-reported that they had been diagnosed with breast cancer within the past 5 years; 612 surveys were completed.
Half of all respondents said they had looked for information on medical cannabis, but most were unsatisfied with the information that they had received. Only 6% were extremely satisfied; 25% were very satisfied with the information.
Most patients (39%) did not discuss cannabis use with their physicians. Of those who did, 28% reported feeling uncomfortable discussing the topic. Only 4% of survey respondents indicated that physicians were the most helpful source of cannabis information.
Regarding which source of information was most helpful, 22% said websites, 18% said family members or friends, 12% said staffers and pharmacists in dispensaries, and 7% said other patients with breast cancer.
Forty-two percent of the survey respondents said they used cannabis for medical purposes and for relief of symptoms, which included pain (78%), insomnia (70%), anxiety (57%), stress (51%), and nausea/vomiting (46%).
In addition, 49% believed that medical cannabis could be used to treat the cancer itself.
A fair number were also using cannabis for recreational purposes. Of those who used cannabis, only 23% reported that they used it for medical purposes only.
Participants used cannabis in a variety of forms. The most popular form of consumption was as edibles (70%), followed by liquids/tinctures (65%), smoking (51%), topicals (46%), and vape pens (45%). Participants reported using an average of 3.7 different products.
Safety concerns?
The authors caution about the use of cannabis while receiving anticancer therapies because such use “raises important efficacy and safety concerns.”
“Many chemotherapy agents as well as cannabinoids are metabolized in the liver’s p450 cytochrome system,” Dr. Weiss and colleagues note, and the mechanism by which cannabinoids interact with particular CYP450 isoenzymes “has the potential to alter the metabolism of other medications and lead to adverse side effects.”
They also question the safety of some of the cannabis products that are being used. Participants reported receiving cannabis from a variety of sources, which included state-regulated dispensaries, “dealers,” and family/friends.
Three-quarters of respondents believed that cannabis was better than “chemicals” and that the benefits outweighed the risks. But many of the products used are unregulated, the authors point out.
“Providers should communicate clearly about the health and safety concerns associated with certain cannabis products and methods of delivery,” they conclude. “Without these measures, patients may make these decisions without qualified medical guidance, obtain poor-quality cannabis products, and consume them through potentially hazardous delivery methods during various types of cancer therapies.”
The study was supported by research grants from Ananda Health/Ecofibre and the Dr. Philip Reeves Legacy Fund. Several coauthors reported relationships with industry, as noted in the article. Dr. Abrams owns stock in Cannformatics and Lumen; he has received honorarium from Clever Leaves and Maui Grown Therapies and speaker honorarium from GW Pharmaceuticals.
A version of this article first appeared on Medscape.com.
Most (75%) of the patients who reported using cannabis said it was extremely helpful or very helpful in alleviating symptoms.
The authors warn of potential safety concerns with cannabis, especially with the use of unregulated products.
In addition, the survey found that physicians were not highly regarded as a source of information about cannabis use. Only 39% of patients said that they discussed cannabis with their physicians; 28% reported feeling uncomfortable when broaching the topic. Only 4% indicated that physicians were the most helpful source of information about cannabis.
The survey involved 612 patients with breast cancer. The results were published online Oct. 12 in Cancer.
“Our study highlights an important opportunity for providers to initiate informed conversations about medical cannabis with their patients, as the evidence shows that many are using medical cannabis without our knowledge or guidance,” said lead author Marisa Weiss, MD, of Breastcancer.org and the Lankenau Medical Center, near Philadelphia. “Not knowing whether or not our cancer patients are using cannabis is a major blind spot in our ability to provide optimal care,” she said.
Cannabis in one form or another has been legalized in many states across America, and even in states where it hasn’t been legalized, people are using it.
“Even though many states have relaxed their laws on cannabis, it remains a Schedule I drug on the federal level and is essentially still considered illegal,” commented Donald I. Abrams, MD, professor of medicine at the University of California, San Francisco, and an integrative oncologist at the UCSF Osher Center for Integrative Medicine. “This is why many physicians are uncomfortable discussing it with patients,” he said.
“Cannabis use isn’t taught in medical school, and until that changes, I don’t know how physicians are going to be advisers for this,” said Dr. Abrams, who was approached by this news organization for comment.
This “is a really nice study in that it looks at a large group of breast cancer patients from the community ... It’s not from a single institution [such as this previous study] and so a more representative mix,” Dr. Abrams said.
However, he also commented that the article had a “scent of ‘reefer madness’” about it, given its emphasis on potential harms and safety concerns.
“It’s interesting how alcohol is considered mainstream but cannabis has been demonized,” he said. “Especially for women with breast cancer, it’s so clear that alcohol is related to the development of postmenopausal breast cancer. As a recreational intervention, cannabis in my mind appears to be much safer for women for relaxation.”
“The one thing I worry about are patients who take highly concentrated CBD [cannabidiol] oil, as it can block the metabolism of prescription drugs and allow them to build up in the blood,” Dr. Abrams said. “I advise people against using these products.”
Cannabis to relieve symptoms
Previous studies have noted widespread use of cannabis among patients with cancer. For example, a large study from Israel that included nearly 3,000 participants found that cannabis use improved a variety of cancer-related symptoms, including nausea and vomiting, sleep disorders, pain, anxiety, and depression. Among those with cancer who survived to 6 months and who finished the study protocol, 60% achieved “treatment success.” Of note, at 6 months, 36% of patients had stopped taking opioids, and for 9.9%, the dose of opioids had decreased.
In the current study, dubbed the Coala-T-Cannabis study, the investigators approached U.S. members of the Breastcancer.org and Healthline.com communities who self-reported that they had been diagnosed with breast cancer within the past 5 years; 612 surveys were completed.
Half of all respondents said they had looked for information on medical cannabis, but most were unsatisfied with the information that they had received. Only 6% were extremely satisfied; 25% were very satisfied with the information.
Most patients (39%) did not discuss cannabis use with their physicians. Of those who did, 28% reported feeling uncomfortable discussing the topic. Only 4% of survey respondents indicated that physicians were the most helpful source of cannabis information.
Regarding which source of information was most helpful, 22% said websites, 18% said family members or friends, 12% said staffers and pharmacists in dispensaries, and 7% said other patients with breast cancer.
Forty-two percent of the survey respondents said they used cannabis for medical purposes and for relief of symptoms, which included pain (78%), insomnia (70%), anxiety (57%), stress (51%), and nausea/vomiting (46%).
In addition, 49% believed that medical cannabis could be used to treat the cancer itself.
A fair number were also using cannabis for recreational purposes. Of those who used cannabis, only 23% reported that they used it for medical purposes only.
Participants used cannabis in a variety of forms. The most popular form of consumption was as edibles (70%), followed by liquids/tinctures (65%), smoking (51%), topicals (46%), and vape pens (45%). Participants reported using an average of 3.7 different products.
Safety concerns?
The authors caution about the use of cannabis while receiving anticancer therapies because such use “raises important efficacy and safety concerns.”
“Many chemotherapy agents as well as cannabinoids are metabolized in the liver’s p450 cytochrome system,” Dr. Weiss and colleagues note, and the mechanism by which cannabinoids interact with particular CYP450 isoenzymes “has the potential to alter the metabolism of other medications and lead to adverse side effects.”
They also question the safety of some of the cannabis products that are being used. Participants reported receiving cannabis from a variety of sources, which included state-regulated dispensaries, “dealers,” and family/friends.
Three-quarters of respondents believed that cannabis was better than “chemicals” and that the benefits outweighed the risks. But many of the products used are unregulated, the authors point out.
“Providers should communicate clearly about the health and safety concerns associated with certain cannabis products and methods of delivery,” they conclude. “Without these measures, patients may make these decisions without qualified medical guidance, obtain poor-quality cannabis products, and consume them through potentially hazardous delivery methods during various types of cancer therapies.”
The study was supported by research grants from Ananda Health/Ecofibre and the Dr. Philip Reeves Legacy Fund. Several coauthors reported relationships with industry, as noted in the article. Dr. Abrams owns stock in Cannformatics and Lumen; he has received honorarium from Clever Leaves and Maui Grown Therapies and speaker honorarium from GW Pharmaceuticals.
A version of this article first appeared on Medscape.com.

Gastric cancer prevalent in hereditary breast cancer patients
a prospective cohort study has shown.
“In short, what we are putting forward with these data is that pathogenic/likely pathogenic (P/LP) variants in the CDH1 gene confer a very high risk, at the very least, of occult early-stage gastric cancer in patients with HLBC,” said Jeremy Davis, MD, of the surgical oncology program, Center for Cancer Research at the National Cancer Institute.
“So patients that are referred to as ‘HLBC’ due to a CDH1 variant should at least undergo annual endoscopic surveillance but the real questions is whether or not they should also consider prophylactic total gastrectomy – as many patients in our study did,” he said.
The study, which was published online Oct. 13, 2021, in JAMA Surgery, included a cohort of 151 families totaling 283 patients with a CDH1 pathogenic or likely pathogenic (P/LP) variant. Analyses were conducted on three patient groups, which included those with HLBC and a family history of breast cancer but no gastric cancer, those with hereditary diffuse gastric cancer (HDGC) but no history of breast cancer, and those with a family history of both gastric and breast cancer in the mixed group. Of these, 15.5% had a history of HLBC, 16.2% had a history of HDGC, and 52.6% made up the mixed group.
“We examined the HLBC group with specific attention to CDH1 genotype and prevalence of occult gastric cancer,” the authors explained. The group consisted of 31 families with 19 CDH1 variants, 10 of which were also present in the HDGC and mixed groups.
Among this group of patients, almost 73% underwent one or more surveillance endoscopies and on endoscopy, occult signet ring cell carcinoma was detected in over one-third of patients.
The median age at the time of endoscopic carcinoma detection was only 33 years.
“Nearly all of the patients with HLBC (93.8%) ... who elected for risk-reducing total gastrectomy owing to their underlying CDH1 P/LP variant harbored occult signet ring cell gastric adenocarcinoma on final pathology,” investigators observed.
The median age at the time patients elected to undergo total gastrectomy was 50 years.
The prevalence of occult gastric cancer among asymptomatic patients in the HDGC group was similarly high, affecting almost 95% of this group of patients.
Some 18 out of 19 CDH1 P/LP variants were responsible for this high prevalence of occult gastric cancer, as the investigators pointed out.
“Hereditary cancer risk is informed by the presence of a germline gene variant more so than by family history of cancer,” the authors stressed. “[And we found that] germline CDH1 P/LP variants appear to have a highly penetrant gastric phenotype irrespective of family history.”
Given this finding, the authors stressed that it is “paramount” patients previously assigned a diagnosis of HLBC not be excluded from undergoing gastric cancer risk assessment and counseling.
Furthermore, “the mere presence of a germline CDH1 P/LP variant, regardless of family history, may be reason enough to consider prophylactic total gastrectomy,” the authors wrote.
Limitations of the study included the fact that the disease phenotype was established from family pedigrees which has the potential for recall bias by family members.
The study was supported in part by the Intramural Research Program of the National Cancer Institute. None of the authors had conflicts of interest to disclose.
a prospective cohort study has shown.
“In short, what we are putting forward with these data is that pathogenic/likely pathogenic (P/LP) variants in the CDH1 gene confer a very high risk, at the very least, of occult early-stage gastric cancer in patients with HLBC,” said Jeremy Davis, MD, of the surgical oncology program, Center for Cancer Research at the National Cancer Institute.
“So patients that are referred to as ‘HLBC’ due to a CDH1 variant should at least undergo annual endoscopic surveillance but the real questions is whether or not they should also consider prophylactic total gastrectomy – as many patients in our study did,” he said.
The study, which was published online Oct. 13, 2021, in JAMA Surgery, included a cohort of 151 families totaling 283 patients with a CDH1 pathogenic or likely pathogenic (P/LP) variant. Analyses were conducted on three patient groups, which included those with HLBC and a family history of breast cancer but no gastric cancer, those with hereditary diffuse gastric cancer (HDGC) but no history of breast cancer, and those with a family history of both gastric and breast cancer in the mixed group. Of these, 15.5% had a history of HLBC, 16.2% had a history of HDGC, and 52.6% made up the mixed group.
“We examined the HLBC group with specific attention to CDH1 genotype and prevalence of occult gastric cancer,” the authors explained. The group consisted of 31 families with 19 CDH1 variants, 10 of which were also present in the HDGC and mixed groups.
Among this group of patients, almost 73% underwent one or more surveillance endoscopies and on endoscopy, occult signet ring cell carcinoma was detected in over one-third of patients.
The median age at the time of endoscopic carcinoma detection was only 33 years.
“Nearly all of the patients with HLBC (93.8%) ... who elected for risk-reducing total gastrectomy owing to their underlying CDH1 P/LP variant harbored occult signet ring cell gastric adenocarcinoma on final pathology,” investigators observed.
The median age at the time patients elected to undergo total gastrectomy was 50 years.
The prevalence of occult gastric cancer among asymptomatic patients in the HDGC group was similarly high, affecting almost 95% of this group of patients.
Some 18 out of 19 CDH1 P/LP variants were responsible for this high prevalence of occult gastric cancer, as the investigators pointed out.
“Hereditary cancer risk is informed by the presence of a germline gene variant more so than by family history of cancer,” the authors stressed. “[And we found that] germline CDH1 P/LP variants appear to have a highly penetrant gastric phenotype irrespective of family history.”
Given this finding, the authors stressed that it is “paramount” patients previously assigned a diagnosis of HLBC not be excluded from undergoing gastric cancer risk assessment and counseling.
Furthermore, “the mere presence of a germline CDH1 P/LP variant, regardless of family history, may be reason enough to consider prophylactic total gastrectomy,” the authors wrote.
Limitations of the study included the fact that the disease phenotype was established from family pedigrees which has the potential for recall bias by family members.
The study was supported in part by the Intramural Research Program of the National Cancer Institute. None of the authors had conflicts of interest to disclose.
a prospective cohort study has shown.
“In short, what we are putting forward with these data is that pathogenic/likely pathogenic (P/LP) variants in the CDH1 gene confer a very high risk, at the very least, of occult early-stage gastric cancer in patients with HLBC,” said Jeremy Davis, MD, of the surgical oncology program, Center for Cancer Research at the National Cancer Institute.
“So patients that are referred to as ‘HLBC’ due to a CDH1 variant should at least undergo annual endoscopic surveillance but the real questions is whether or not they should also consider prophylactic total gastrectomy – as many patients in our study did,” he said.
The study, which was published online Oct. 13, 2021, in JAMA Surgery, included a cohort of 151 families totaling 283 patients with a CDH1 pathogenic or likely pathogenic (P/LP) variant. Analyses were conducted on three patient groups, which included those with HLBC and a family history of breast cancer but no gastric cancer, those with hereditary diffuse gastric cancer (HDGC) but no history of breast cancer, and those with a family history of both gastric and breast cancer in the mixed group. Of these, 15.5% had a history of HLBC, 16.2% had a history of HDGC, and 52.6% made up the mixed group.
“We examined the HLBC group with specific attention to CDH1 genotype and prevalence of occult gastric cancer,” the authors explained. The group consisted of 31 families with 19 CDH1 variants, 10 of which were also present in the HDGC and mixed groups.
Among this group of patients, almost 73% underwent one or more surveillance endoscopies and on endoscopy, occult signet ring cell carcinoma was detected in over one-third of patients.
The median age at the time of endoscopic carcinoma detection was only 33 years.
“Nearly all of the patients with HLBC (93.8%) ... who elected for risk-reducing total gastrectomy owing to their underlying CDH1 P/LP variant harbored occult signet ring cell gastric adenocarcinoma on final pathology,” investigators observed.
The median age at the time patients elected to undergo total gastrectomy was 50 years.
The prevalence of occult gastric cancer among asymptomatic patients in the HDGC group was similarly high, affecting almost 95% of this group of patients.
Some 18 out of 19 CDH1 P/LP variants were responsible for this high prevalence of occult gastric cancer, as the investigators pointed out.
“Hereditary cancer risk is informed by the presence of a germline gene variant more so than by family history of cancer,” the authors stressed. “[And we found that] germline CDH1 P/LP variants appear to have a highly penetrant gastric phenotype irrespective of family history.”
Given this finding, the authors stressed that it is “paramount” patients previously assigned a diagnosis of HLBC not be excluded from undergoing gastric cancer risk assessment and counseling.
Furthermore, “the mere presence of a germline CDH1 P/LP variant, regardless of family history, may be reason enough to consider prophylactic total gastrectomy,” the authors wrote.
Limitations of the study included the fact that the disease phenotype was established from family pedigrees which has the potential for recall bias by family members.
The study was supported in part by the Intramural Research Program of the National Cancer Institute. None of the authors had conflicts of interest to disclose.
FROM JAMA SURGERY
Success in closing racial survival gap in lung and breast cancer
When barriers to completing radiation therapy were identified and addressed in a cohort of patients with early-stage lung and breast cancer, 5-year survival rates improved for all patients and closed the racial disparity gap, researchers reported at the annual meeting of the American Society for Radiation Oncology (ASTRO).
The findings come from the ACCURE clinical trial. This is the first prospective study designed to erase gaps in cancer treatment completion and survival among Black and White patient populations, explained lead author Matthew A. Manning, MD, a radiation oncologist and chief of oncology at Cone Health in Greensboro, N.C.
“Thousands of studies have looked at racial disparities in health care, but until recently, very few studies have implemented interventions to eliminate those disparities,” he said.
“This study shows that the implementation of ‘systems-change’ can eliminate racial disparities in cancer survival while improving survival for all,” he added.
“These results add to a growing body of evidence that health care disparities in cancer outcomes are eliminated or minimized by providing supportive, timely, and guideline-directed care,” said Lannis Hall, MD, MPH, director of radiation oncology, Siteman Cancer Center, and associate professor of radiation oncology at Washington University School of Medicine, St. Louis, who was approached for comment
“This research supports that access to care and timely treatment completion is critical to eliminating health care disparities,” she told this news organization. The system-based intervention in this trial was designed to reduce treatment delays and provide a supportive matrix for patients confronting real-world difficulties like transportation issues, childcare complications, and work absence, she explained.
Eliminating racial disparities
Previous findings from the ACCURE trial showed that it eliminated Black-White disparities in treatment completion rates, which was the study’s primary endpoint (Cancer Med. 2019;8:1095-1102). “It also improved treatment for all patients,” said Dr. Manning. “The current study is a follow-up on the survival of eligible patients treated during the ACCURE enrollment as compared to historical data.”
ACCURE was a multi-institutional trial designed to test a community-created intervention to reduce racial disparities. The intervention involved multiple changes to the way patients were supported while receiving cancer treatment and had four components:
- an electronic health record with automatic alerts to flag missed appointments or unmet milestones in expected care
- a nurse navigator trained in race-specific barriers to help patients overcome obstacles to care when alerts are flagged
- a physician champion to engage health care teams with race-related feedback on treatment completion
- regular health equity education training sessions for staff
The cohort was comprised of 1,413 patients with lung and breast cancer (stage 0-II) who were diagnosed from 2013-2015, and survival was compared to historical cases – 2,016 patients who had been treated from 2007-2011.
The results showed a significant improvement in survival for both Black and White patients with breast and lung cancer over time, and the racial gap in survival was reduced.
The 5-year survival rate for breast cancer increased from 91% for White patients and 89% in Black patients in historical cases, to 94% for both during the study period.
For patients with lung cancer, the 5-year survival rate improved from 43% in White patients and 37% in Black patients to 56% and 54%, respectively.
A subgroup analysis showed that patients with lung cancer who underwent surgery had 5-year survival rates of 78.5% for White and 70.1% for Black patients, whereas for those who underwent stereotactic body radiation therapy (SBRT) the rates were 41.9% and 50% respectively.
“We’ve shown it’s possible to eliminate disparities in cancer treatment completion and that this change has the potential to close cancer survival gaps downstream,” said Dr. Manning. “But we think the application can be much broader.”
The ACCURE study was sponsored by the National Institutes of Health. Dr. Manning and Dr. Hall have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
When barriers to completing radiation therapy were identified and addressed in a cohort of patients with early-stage lung and breast cancer, 5-year survival rates improved for all patients and closed the racial disparity gap, researchers reported at the annual meeting of the American Society for Radiation Oncology (ASTRO).
The findings come from the ACCURE clinical trial. This is the first prospective study designed to erase gaps in cancer treatment completion and survival among Black and White patient populations, explained lead author Matthew A. Manning, MD, a radiation oncologist and chief of oncology at Cone Health in Greensboro, N.C.
“Thousands of studies have looked at racial disparities in health care, but until recently, very few studies have implemented interventions to eliminate those disparities,” he said.
“This study shows that the implementation of ‘systems-change’ can eliminate racial disparities in cancer survival while improving survival for all,” he added.
“These results add to a growing body of evidence that health care disparities in cancer outcomes are eliminated or minimized by providing supportive, timely, and guideline-directed care,” said Lannis Hall, MD, MPH, director of radiation oncology, Siteman Cancer Center, and associate professor of radiation oncology at Washington University School of Medicine, St. Louis, who was approached for comment
“This research supports that access to care and timely treatment completion is critical to eliminating health care disparities,” she told this news organization. The system-based intervention in this trial was designed to reduce treatment delays and provide a supportive matrix for patients confronting real-world difficulties like transportation issues, childcare complications, and work absence, she explained.
Eliminating racial disparities
Previous findings from the ACCURE trial showed that it eliminated Black-White disparities in treatment completion rates, which was the study’s primary endpoint (Cancer Med. 2019;8:1095-1102). “It also improved treatment for all patients,” said Dr. Manning. “The current study is a follow-up on the survival of eligible patients treated during the ACCURE enrollment as compared to historical data.”
ACCURE was a multi-institutional trial designed to test a community-created intervention to reduce racial disparities. The intervention involved multiple changes to the way patients were supported while receiving cancer treatment and had four components:
- an electronic health record with automatic alerts to flag missed appointments or unmet milestones in expected care
- a nurse navigator trained in race-specific barriers to help patients overcome obstacles to care when alerts are flagged
- a physician champion to engage health care teams with race-related feedback on treatment completion
- regular health equity education training sessions for staff
The cohort was comprised of 1,413 patients with lung and breast cancer (stage 0-II) who were diagnosed from 2013-2015, and survival was compared to historical cases – 2,016 patients who had been treated from 2007-2011.
The results showed a significant improvement in survival for both Black and White patients with breast and lung cancer over time, and the racial gap in survival was reduced.
The 5-year survival rate for breast cancer increased from 91% for White patients and 89% in Black patients in historical cases, to 94% for both during the study period.
For patients with lung cancer, the 5-year survival rate improved from 43% in White patients and 37% in Black patients to 56% and 54%, respectively.
A subgroup analysis showed that patients with lung cancer who underwent surgery had 5-year survival rates of 78.5% for White and 70.1% for Black patients, whereas for those who underwent stereotactic body radiation therapy (SBRT) the rates were 41.9% and 50% respectively.
“We’ve shown it’s possible to eliminate disparities in cancer treatment completion and that this change has the potential to close cancer survival gaps downstream,” said Dr. Manning. “But we think the application can be much broader.”
The ACCURE study was sponsored by the National Institutes of Health. Dr. Manning and Dr. Hall have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
When barriers to completing radiation therapy were identified and addressed in a cohort of patients with early-stage lung and breast cancer, 5-year survival rates improved for all patients and closed the racial disparity gap, researchers reported at the annual meeting of the American Society for Radiation Oncology (ASTRO).
The findings come from the ACCURE clinical trial. This is the first prospective study designed to erase gaps in cancer treatment completion and survival among Black and White patient populations, explained lead author Matthew A. Manning, MD, a radiation oncologist and chief of oncology at Cone Health in Greensboro, N.C.
“Thousands of studies have looked at racial disparities in health care, but until recently, very few studies have implemented interventions to eliminate those disparities,” he said.
“This study shows that the implementation of ‘systems-change’ can eliminate racial disparities in cancer survival while improving survival for all,” he added.
“These results add to a growing body of evidence that health care disparities in cancer outcomes are eliminated or minimized by providing supportive, timely, and guideline-directed care,” said Lannis Hall, MD, MPH, director of radiation oncology, Siteman Cancer Center, and associate professor of radiation oncology at Washington University School of Medicine, St. Louis, who was approached for comment
“This research supports that access to care and timely treatment completion is critical to eliminating health care disparities,” she told this news organization. The system-based intervention in this trial was designed to reduce treatment delays and provide a supportive matrix for patients confronting real-world difficulties like transportation issues, childcare complications, and work absence, she explained.
Eliminating racial disparities
Previous findings from the ACCURE trial showed that it eliminated Black-White disparities in treatment completion rates, which was the study’s primary endpoint (Cancer Med. 2019;8:1095-1102). “It also improved treatment for all patients,” said Dr. Manning. “The current study is a follow-up on the survival of eligible patients treated during the ACCURE enrollment as compared to historical data.”
ACCURE was a multi-institutional trial designed to test a community-created intervention to reduce racial disparities. The intervention involved multiple changes to the way patients were supported while receiving cancer treatment and had four components:
- an electronic health record with automatic alerts to flag missed appointments or unmet milestones in expected care
- a nurse navigator trained in race-specific barriers to help patients overcome obstacles to care when alerts are flagged
- a physician champion to engage health care teams with race-related feedback on treatment completion
- regular health equity education training sessions for staff
The cohort was comprised of 1,413 patients with lung and breast cancer (stage 0-II) who were diagnosed from 2013-2015, and survival was compared to historical cases – 2,016 patients who had been treated from 2007-2011.
The results showed a significant improvement in survival for both Black and White patients with breast and lung cancer over time, and the racial gap in survival was reduced.
The 5-year survival rate for breast cancer increased from 91% for White patients and 89% in Black patients in historical cases, to 94% for both during the study period.
For patients with lung cancer, the 5-year survival rate improved from 43% in White patients and 37% in Black patients to 56% and 54%, respectively.
A subgroup analysis showed that patients with lung cancer who underwent surgery had 5-year survival rates of 78.5% for White and 70.1% for Black patients, whereas for those who underwent stereotactic body radiation therapy (SBRT) the rates were 41.9% and 50% respectively.
“We’ve shown it’s possible to eliminate disparities in cancer treatment completion and that this change has the potential to close cancer survival gaps downstream,” said Dr. Manning. “But we think the application can be much broader.”
The ACCURE study was sponsored by the National Institutes of Health. Dr. Manning and Dr. Hall have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ASTRO 2021
NCI mammography trial mostly a ‘waste,’ says expert
Funding for this trial is largely misspent money, it may produce misleading results, and it should be abandoned, he says.
Dr. Kopans has been an outspoken critic of the trial, describing it as a “huge waste of money” in comments made last year. Now he has set out his criticisms of the trial in an essay published in the October issue of Clinical Imaging, which outlines his objections and concerns for the first time in a peer-reviewed journal.
The Tomosynthesis Mammographic Imaging Screening Trial (TMIST) is comparing digital breast tomosynthesis (DBT), also known as 3-D mammography, with the older 2-D technology or full-field digital mammography (FFDM).
Dr. Kopans coined the term DBT and formerly held a now-expired patent on the first version of this technology.
“It could be argued that the imaging part of TMIST is a waste of valuable resources,” he writes in the essay.
The “imaging part” of the trial refers to the primary outcome measure and driving purpose of the trial, which is designed to learn which technology is better at finding – and reducing the rate of – potentially lethal “advanced” cancers.
These cancers include larger HER2-positive and triple-negative malignancies; those associated with positive nodes; and metastatic disease. These malignancies correlate with breast cancer mortality, TMIST’s principal investigator Etta Pisano, MD, of the American College of Radiology, has said in the past.
However, Dr. Kopans says that this surrogate endpoint is problematic. “TMIST will only investigate whether or not digital breast tomography results in a decline in advanced cancers, ignoring the fact that many women still die from cancers that are not advanced at the time of diagnosis,” he writes.
“Clearly reducing the rate of advanced cancers is not the only way that early detection saves lives. Lives are also saved by finding cancers at a smaller size within stages,” Dr. Kopans writes. He adds that DBT has been proven in observational cohort studies to find more smaller breast cancers than FFDM.
Dr. Kopans’ opinion that TMIST is largely a waste of resources is not shared by the National Cancer Institute. “We feel strongly that TMIST is a critical study,” an NCI spokesperson told this news organization.
Study power concerns
Another concern is that TMIST “may be underpowered,” Dr. Kopans writes. That concern arises in part from a recent review of TMIST by an advisory committee (that was prompted by low patient accrual rates), which proposed reducing the size of the trial. Dr. Kopans says this would result in “a reduction of the planned power of the trial.”
The NCI says that reducing the study size has been discussed but has not yet been implemented. “Any reduction in size would, of course, have appropriate statistical considerations in mind,” according to the NCI spokesperson.
Dr. Kopans’ concern about statistical power extends beyond downsizing the trial. An advanced cancer in TMIST is counted “if it occurs at any time while the participant is on study,” according to the NCI. Dr. Kopans says that is a problem.
“Since DBT cannot have any effect on advanced cancers in the prevalence year (they are already there), data from the first year (prevalence cancers are likely the largest number) will be unusable, and if used will, inappropriately, dilute the results,” he writes.
Dr. Kopans hopes that the investigators address the statistical power issues with the trial because, if not, “its results may be grossly misleading.”
American radiology practice
Dr. Kopans praises one aspect of TMIST – the trial’s effort to create a repository of blood and oral swab specimens, along with participant genetic data. The goal, say TMIST investigators, is to individualize or optimize screening strategies by tying molecular data to clinical outcomes in the trial.
However, apart from that one aspect, Dr. Kopans is highly critical of the trial.
It is now too late to compare the two technologies, he suggests, as DBT is already replacing FFDM for breast cancer screening in the U.S.
He notes that 76% of mammography facilities in the United States have 3-D devices (as of April 2021). That percentage has climbed steadily in recent years. “By the time the TMIST study is completed, DBT will, almost certainly, have become the ‘standard of care,’” he asserts, echoing others who have commented on the trial, including some participating physicians.
The money being spent on TMIST “should not be used for looking backwards,” says Dr. Kopans.
The NCI responded to that criticism. “TMIST is looking to clarify the best screening for women based on the science and is not solely about access. We are seeking to determine which technology is better and [are] providing access to the trial across the country in diverse practices and populations,” the NCI said in an email.
In his essay, Dr. Kopans says it is time to stop TMIST and put the money into other pressing breast cancer issues and questions. “... it makes no sense to continue this flawed trial whose results will be obsolete by the time they become available,” he writes.
Dr. Kopans reports consulting with DART Imaging in China, which is developing a digital breast tomosynthesis machine.
A version of this article first appeared on Medscape.com.
Funding for this trial is largely misspent money, it may produce misleading results, and it should be abandoned, he says.
Dr. Kopans has been an outspoken critic of the trial, describing it as a “huge waste of money” in comments made last year. Now he has set out his criticisms of the trial in an essay published in the October issue of Clinical Imaging, which outlines his objections and concerns for the first time in a peer-reviewed journal.
The Tomosynthesis Mammographic Imaging Screening Trial (TMIST) is comparing digital breast tomosynthesis (DBT), also known as 3-D mammography, with the older 2-D technology or full-field digital mammography (FFDM).
Dr. Kopans coined the term DBT and formerly held a now-expired patent on the first version of this technology.
“It could be argued that the imaging part of TMIST is a waste of valuable resources,” he writes in the essay.
The “imaging part” of the trial refers to the primary outcome measure and driving purpose of the trial, which is designed to learn which technology is better at finding – and reducing the rate of – potentially lethal “advanced” cancers.
These cancers include larger HER2-positive and triple-negative malignancies; those associated with positive nodes; and metastatic disease. These malignancies correlate with breast cancer mortality, TMIST’s principal investigator Etta Pisano, MD, of the American College of Radiology, has said in the past.
However, Dr. Kopans says that this surrogate endpoint is problematic. “TMIST will only investigate whether or not digital breast tomography results in a decline in advanced cancers, ignoring the fact that many women still die from cancers that are not advanced at the time of diagnosis,” he writes.
“Clearly reducing the rate of advanced cancers is not the only way that early detection saves lives. Lives are also saved by finding cancers at a smaller size within stages,” Dr. Kopans writes. He adds that DBT has been proven in observational cohort studies to find more smaller breast cancers than FFDM.
Dr. Kopans’ opinion that TMIST is largely a waste of resources is not shared by the National Cancer Institute. “We feel strongly that TMIST is a critical study,” an NCI spokesperson told this news organization.
Study power concerns
Another concern is that TMIST “may be underpowered,” Dr. Kopans writes. That concern arises in part from a recent review of TMIST by an advisory committee (that was prompted by low patient accrual rates), which proposed reducing the size of the trial. Dr. Kopans says this would result in “a reduction of the planned power of the trial.”
The NCI says that reducing the study size has been discussed but has not yet been implemented. “Any reduction in size would, of course, have appropriate statistical considerations in mind,” according to the NCI spokesperson.
Dr. Kopans’ concern about statistical power extends beyond downsizing the trial. An advanced cancer in TMIST is counted “if it occurs at any time while the participant is on study,” according to the NCI. Dr. Kopans says that is a problem.
“Since DBT cannot have any effect on advanced cancers in the prevalence year (they are already there), data from the first year (prevalence cancers are likely the largest number) will be unusable, and if used will, inappropriately, dilute the results,” he writes.
Dr. Kopans hopes that the investigators address the statistical power issues with the trial because, if not, “its results may be grossly misleading.”
American radiology practice
Dr. Kopans praises one aspect of TMIST – the trial’s effort to create a repository of blood and oral swab specimens, along with participant genetic data. The goal, say TMIST investigators, is to individualize or optimize screening strategies by tying molecular data to clinical outcomes in the trial.
However, apart from that one aspect, Dr. Kopans is highly critical of the trial.
It is now too late to compare the two technologies, he suggests, as DBT is already replacing FFDM for breast cancer screening in the U.S.
He notes that 76% of mammography facilities in the United States have 3-D devices (as of April 2021). That percentage has climbed steadily in recent years. “By the time the TMIST study is completed, DBT will, almost certainly, have become the ‘standard of care,’” he asserts, echoing others who have commented on the trial, including some participating physicians.
The money being spent on TMIST “should not be used for looking backwards,” says Dr. Kopans.
The NCI responded to that criticism. “TMIST is looking to clarify the best screening for women based on the science and is not solely about access. We are seeking to determine which technology is better and [are] providing access to the trial across the country in diverse practices and populations,” the NCI said in an email.
In his essay, Dr. Kopans says it is time to stop TMIST and put the money into other pressing breast cancer issues and questions. “... it makes no sense to continue this flawed trial whose results will be obsolete by the time they become available,” he writes.
Dr. Kopans reports consulting with DART Imaging in China, which is developing a digital breast tomosynthesis machine.
A version of this article first appeared on Medscape.com.
Funding for this trial is largely misspent money, it may produce misleading results, and it should be abandoned, he says.
Dr. Kopans has been an outspoken critic of the trial, describing it as a “huge waste of money” in comments made last year. Now he has set out his criticisms of the trial in an essay published in the October issue of Clinical Imaging, which outlines his objections and concerns for the first time in a peer-reviewed journal.
The Tomosynthesis Mammographic Imaging Screening Trial (TMIST) is comparing digital breast tomosynthesis (DBT), also known as 3-D mammography, with the older 2-D technology or full-field digital mammography (FFDM).
Dr. Kopans coined the term DBT and formerly held a now-expired patent on the first version of this technology.
“It could be argued that the imaging part of TMIST is a waste of valuable resources,” he writes in the essay.
The “imaging part” of the trial refers to the primary outcome measure and driving purpose of the trial, which is designed to learn which technology is better at finding – and reducing the rate of – potentially lethal “advanced” cancers.
These cancers include larger HER2-positive and triple-negative malignancies; those associated with positive nodes; and metastatic disease. These malignancies correlate with breast cancer mortality, TMIST’s principal investigator Etta Pisano, MD, of the American College of Radiology, has said in the past.
However, Dr. Kopans says that this surrogate endpoint is problematic. “TMIST will only investigate whether or not digital breast tomography results in a decline in advanced cancers, ignoring the fact that many women still die from cancers that are not advanced at the time of diagnosis,” he writes.
“Clearly reducing the rate of advanced cancers is not the only way that early detection saves lives. Lives are also saved by finding cancers at a smaller size within stages,” Dr. Kopans writes. He adds that DBT has been proven in observational cohort studies to find more smaller breast cancers than FFDM.
Dr. Kopans’ opinion that TMIST is largely a waste of resources is not shared by the National Cancer Institute. “We feel strongly that TMIST is a critical study,” an NCI spokesperson told this news organization.
Study power concerns
Another concern is that TMIST “may be underpowered,” Dr. Kopans writes. That concern arises in part from a recent review of TMIST by an advisory committee (that was prompted by low patient accrual rates), which proposed reducing the size of the trial. Dr. Kopans says this would result in “a reduction of the planned power of the trial.”
The NCI says that reducing the study size has been discussed but has not yet been implemented. “Any reduction in size would, of course, have appropriate statistical considerations in mind,” according to the NCI spokesperson.
Dr. Kopans’ concern about statistical power extends beyond downsizing the trial. An advanced cancer in TMIST is counted “if it occurs at any time while the participant is on study,” according to the NCI. Dr. Kopans says that is a problem.
“Since DBT cannot have any effect on advanced cancers in the prevalence year (they are already there), data from the first year (prevalence cancers are likely the largest number) will be unusable, and if used will, inappropriately, dilute the results,” he writes.
Dr. Kopans hopes that the investigators address the statistical power issues with the trial because, if not, “its results may be grossly misleading.”
American radiology practice
Dr. Kopans praises one aspect of TMIST – the trial’s effort to create a repository of blood and oral swab specimens, along with participant genetic data. The goal, say TMIST investigators, is to individualize or optimize screening strategies by tying molecular data to clinical outcomes in the trial.
However, apart from that one aspect, Dr. Kopans is highly critical of the trial.
It is now too late to compare the two technologies, he suggests, as DBT is already replacing FFDM for breast cancer screening in the U.S.
He notes that 76% of mammography facilities in the United States have 3-D devices (as of April 2021). That percentage has climbed steadily in recent years. “By the time the TMIST study is completed, DBT will, almost certainly, have become the ‘standard of care,’” he asserts, echoing others who have commented on the trial, including some participating physicians.
The money being spent on TMIST “should not be used for looking backwards,” says Dr. Kopans.
The NCI responded to that criticism. “TMIST is looking to clarify the best screening for women based on the science and is not solely about access. We are seeking to determine which technology is better and [are] providing access to the trial across the country in diverse practices and populations,” the NCI said in an email.
In his essay, Dr. Kopans says it is time to stop TMIST and put the money into other pressing breast cancer issues and questions. “... it makes no sense to continue this flawed trial whose results will be obsolete by the time they become available,” he writes.
Dr. Kopans reports consulting with DART Imaging in China, which is developing a digital breast tomosynthesis machine.
A version of this article first appeared on Medscape.com.
‘First reliable estimate’ of breast cancer metastasis
The data come from a massive meta-analysis of more than 400 studies conducted around the world, involving tens of thousands of women.
It found that the overall risk of metastasis is between 6% and 22%, with younger women having a higher risk.
While women aged 50 years or older when they were diagnosed with breast cancer have a risk of developing metastasis that ranged from 3.7% to 28.6%, women diagnosed with breast cancer before age 35 had a higher risk – 12.7% to 38%. The investigators speculate that this may be because younger women have a more aggressive form of breast cancer or because they are diagnosed at a later stage.
The risk of metastasis also varies by tumor type, with luminal B cancers having a 4.2% to 35.5% risk of metastasis versus a 2.3% to 11.8% risk with luminal A tumors.
“The quantification of recurrence and disease progression is important to assess the effectiveness of treatment, evaluate prognosis, and allocate resources,” commented lead investigator Eileen Morgan, PhD, of the International Agency for Research on Cancer.
Dr. Morgan and colleagues presented the new meta-analysis at the virtual Advanced Breast Cancer Sixth International Consensus Conference.
She added that this information has not been available until now “because cancer registries have not been routinely collecting this data.”
In fact, the U.S. National Cancer Institute began a project earlier this year to track this information, after 48 years of not doing so.
Reacting to the findings, Shani Paluch-Shimon, MBBS, director of the Breast Unit at Hadassah University Hospital, Jerusalem, commented that this work “provides the first reliable estimate of how many breast cancer patients go on to develop advanced disease in contemporary cohorts.”
“This information is, of course, important for patients who want to understand their prognosis,” she continued.
“But it’s also vital at a public health level for those of us working to treat and prevent advanced breast cancer, to help us understand the scale of the disease around the world,” she said. “It will help us identify at-risk groups across different populations and demonstrate how disease course is changing with contemporary treatments.”
“It will also help us understand what resources are needed and where, to ensure we can collect and analyze quality data in real-time as this is key for resource allocation and planning future studies.”
The work was funded by a grant from the Susan G. Komen Foundation.
A version of this article first appeared on Medscape.com.
The data come from a massive meta-analysis of more than 400 studies conducted around the world, involving tens of thousands of women.
It found that the overall risk of metastasis is between 6% and 22%, with younger women having a higher risk.
While women aged 50 years or older when they were diagnosed with breast cancer have a risk of developing metastasis that ranged from 3.7% to 28.6%, women diagnosed with breast cancer before age 35 had a higher risk – 12.7% to 38%. The investigators speculate that this may be because younger women have a more aggressive form of breast cancer or because they are diagnosed at a later stage.
The risk of metastasis also varies by tumor type, with luminal B cancers having a 4.2% to 35.5% risk of metastasis versus a 2.3% to 11.8% risk with luminal A tumors.
“The quantification of recurrence and disease progression is important to assess the effectiveness of treatment, evaluate prognosis, and allocate resources,” commented lead investigator Eileen Morgan, PhD, of the International Agency for Research on Cancer.
Dr. Morgan and colleagues presented the new meta-analysis at the virtual Advanced Breast Cancer Sixth International Consensus Conference.
She added that this information has not been available until now “because cancer registries have not been routinely collecting this data.”
In fact, the U.S. National Cancer Institute began a project earlier this year to track this information, after 48 years of not doing so.
Reacting to the findings, Shani Paluch-Shimon, MBBS, director of the Breast Unit at Hadassah University Hospital, Jerusalem, commented that this work “provides the first reliable estimate of how many breast cancer patients go on to develop advanced disease in contemporary cohorts.”
“This information is, of course, important for patients who want to understand their prognosis,” she continued.
“But it’s also vital at a public health level for those of us working to treat and prevent advanced breast cancer, to help us understand the scale of the disease around the world,” she said. “It will help us identify at-risk groups across different populations and demonstrate how disease course is changing with contemporary treatments.”
“It will also help us understand what resources are needed and where, to ensure we can collect and analyze quality data in real-time as this is key for resource allocation and planning future studies.”
The work was funded by a grant from the Susan G. Komen Foundation.
A version of this article first appeared on Medscape.com.
The data come from a massive meta-analysis of more than 400 studies conducted around the world, involving tens of thousands of women.
It found that the overall risk of metastasis is between 6% and 22%, with younger women having a higher risk.
While women aged 50 years or older when they were diagnosed with breast cancer have a risk of developing metastasis that ranged from 3.7% to 28.6%, women diagnosed with breast cancer before age 35 had a higher risk – 12.7% to 38%. The investigators speculate that this may be because younger women have a more aggressive form of breast cancer or because they are diagnosed at a later stage.
The risk of metastasis also varies by tumor type, with luminal B cancers having a 4.2% to 35.5% risk of metastasis versus a 2.3% to 11.8% risk with luminal A tumors.
“The quantification of recurrence and disease progression is important to assess the effectiveness of treatment, evaluate prognosis, and allocate resources,” commented lead investigator Eileen Morgan, PhD, of the International Agency for Research on Cancer.
Dr. Morgan and colleagues presented the new meta-analysis at the virtual Advanced Breast Cancer Sixth International Consensus Conference.
She added that this information has not been available until now “because cancer registries have not been routinely collecting this data.”
In fact, the U.S. National Cancer Institute began a project earlier this year to track this information, after 48 years of not doing so.
Reacting to the findings, Shani Paluch-Shimon, MBBS, director of the Breast Unit at Hadassah University Hospital, Jerusalem, commented that this work “provides the first reliable estimate of how many breast cancer patients go on to develop advanced disease in contemporary cohorts.”
“This information is, of course, important for patients who want to understand their prognosis,” she continued.
“But it’s also vital at a public health level for those of us working to treat and prevent advanced breast cancer, to help us understand the scale of the disease around the world,” she said. “It will help us identify at-risk groups across different populations and demonstrate how disease course is changing with contemporary treatments.”
“It will also help us understand what resources are needed and where, to ensure we can collect and analyze quality data in real-time as this is key for resource allocation and planning future studies.”
The work was funded by a grant from the Susan G. Komen Foundation.
A version of this article first appeared on Medscape.com.
Severe COVID two times higher for cancer patients
A new systematic review and meta-analysis finds that unvaccinated cancer patients who contracted COVID-19 last year, were more than two times more likely – than people without cancer – to develop a case of COVID-19 so severe it required hospitalization in an intensive care unit.
“Our study provides the most precise measure to date of the effect of COVID-19 in cancer patients,” wrote researchers who were led by Paolo Boffetta, MD, MPH, a specialist in population science with the Stony Brook Cancer Center in New York.
Dr. Boffetta and colleagues also found that patients with hematologic neoplasms had a higher mortality rate from COVID-19 comparable to that of all cancers combined.
Cancer patients have long been considered to be among those patients who are at high risk of developing COVID-19, and if they contract the disease, they are at high risk of having poor outcomes. Other high-risk patients include those with hypertension, diabetes, chronic kidney disease, or COPD, or the elderly. But how high the risk of developing severe COVID-19 disease is for cancer patients hasn’t yet been documented on a wide scale.
The study, which was made available as a preprint on medRxiv on Oct. 23, is based on an analysis of COVID-19 cases that were documented in 35 reviews, meta-analyses, case reports, and studies indexed in PubMed from authors in North America, Europe, and Asia.
In this study, the pooled odds ratio for mortality for all patients with any cancer was 2.32 (95% confidence interval, 1.82-2.94; 24 studies). For ICU admission, the odds ratio was 2.39 (95% CI, 1.90-3.02; I2 0.0%; 5 studies). And, for disease severity or hospitalization, it was 2.08 (95% CI, 1.60-2.72; I2 92.1%; 15 studies). The pooled mortality odds ratio for hematologic neoplasms was 2.14 (95% CI, 1.87-2.44; I2 20.8%; 8 studies).
Their findings, which have not yet been peer reviewed, confirmed the results of a similar analysis from China published as a preprint in May 2020. The analysis included 181,323 patients (23,736 cancer patients) from 26 studies reported an odds ratio of 2.54 (95% CI, 1.47-4.42). “Cancer patients with COVID-19 have an increased likelihood of death compared to non-cancer COVID-19 patients,” Venkatesulu et al. wrote. And a systematic review and meta-analysis of five studies of 2,619 patients published in October 2020 in Medicine also found a significantly higher risk of death from COVID-19 among cancer patients (odds ratio, 2.63; 95% confidence interval, 1.14-6.06; P = .023; I2 = 26.4%).
Fakih et al., writing in the journal Hematology/Oncology and Stem Cell Therapy conducted a meta-analysis early last year finding a threefold increase for admission to the intensive care unit, an almost fourfold increase for a severe SARS-CoV-2 infection, and a fivefold increase for being intubated.
The three studies show that mortality rates were higher early in the pandemic “when diagnosis and treatment for SARS-CoV-2 might have been delayed, resulting in higher death rate,” Boffetta et al. wrote, adding that their analysis showed only a twofold increase most likely because it was a year-long analysis.
“Future studies will be able to better analyze this association for the different subtypes of cancer. Furthermore, they will eventually be able to evaluate whether the difference among vaccinated population is reduced,” Boffetta et al. wrote.
The authors noted several limitations for the study, including the fact that many of the studies included in the analysis did not include sex, age, comorbidities, and therapy. Nor were the authors able to analyze specific cancers other than hematologic neoplasms.
The authors declared no conflicts of interest.
A new systematic review and meta-analysis finds that unvaccinated cancer patients who contracted COVID-19 last year, were more than two times more likely – than people without cancer – to develop a case of COVID-19 so severe it required hospitalization in an intensive care unit.
“Our study provides the most precise measure to date of the effect of COVID-19 in cancer patients,” wrote researchers who were led by Paolo Boffetta, MD, MPH, a specialist in population science with the Stony Brook Cancer Center in New York.
Dr. Boffetta and colleagues also found that patients with hematologic neoplasms had a higher mortality rate from COVID-19 comparable to that of all cancers combined.
Cancer patients have long been considered to be among those patients who are at high risk of developing COVID-19, and if they contract the disease, they are at high risk of having poor outcomes. Other high-risk patients include those with hypertension, diabetes, chronic kidney disease, or COPD, or the elderly. But how high the risk of developing severe COVID-19 disease is for cancer patients hasn’t yet been documented on a wide scale.
The study, which was made available as a preprint on medRxiv on Oct. 23, is based on an analysis of COVID-19 cases that were documented in 35 reviews, meta-analyses, case reports, and studies indexed in PubMed from authors in North America, Europe, and Asia.
In this study, the pooled odds ratio for mortality for all patients with any cancer was 2.32 (95% confidence interval, 1.82-2.94; 24 studies). For ICU admission, the odds ratio was 2.39 (95% CI, 1.90-3.02; I2 0.0%; 5 studies). And, for disease severity or hospitalization, it was 2.08 (95% CI, 1.60-2.72; I2 92.1%; 15 studies). The pooled mortality odds ratio for hematologic neoplasms was 2.14 (95% CI, 1.87-2.44; I2 20.8%; 8 studies).
Their findings, which have not yet been peer reviewed, confirmed the results of a similar analysis from China published as a preprint in May 2020. The analysis included 181,323 patients (23,736 cancer patients) from 26 studies reported an odds ratio of 2.54 (95% CI, 1.47-4.42). “Cancer patients with COVID-19 have an increased likelihood of death compared to non-cancer COVID-19 patients,” Venkatesulu et al. wrote. And a systematic review and meta-analysis of five studies of 2,619 patients published in October 2020 in Medicine also found a significantly higher risk of death from COVID-19 among cancer patients (odds ratio, 2.63; 95% confidence interval, 1.14-6.06; P = .023; I2 = 26.4%).
Fakih et al., writing in the journal Hematology/Oncology and Stem Cell Therapy conducted a meta-analysis early last year finding a threefold increase for admission to the intensive care unit, an almost fourfold increase for a severe SARS-CoV-2 infection, and a fivefold increase for being intubated.
The three studies show that mortality rates were higher early in the pandemic “when diagnosis and treatment for SARS-CoV-2 might have been delayed, resulting in higher death rate,” Boffetta et al. wrote, adding that their analysis showed only a twofold increase most likely because it was a year-long analysis.
“Future studies will be able to better analyze this association for the different subtypes of cancer. Furthermore, they will eventually be able to evaluate whether the difference among vaccinated population is reduced,” Boffetta et al. wrote.
The authors noted several limitations for the study, including the fact that many of the studies included in the analysis did not include sex, age, comorbidities, and therapy. Nor were the authors able to analyze specific cancers other than hematologic neoplasms.
The authors declared no conflicts of interest.
A new systematic review and meta-analysis finds that unvaccinated cancer patients who contracted COVID-19 last year, were more than two times more likely – than people without cancer – to develop a case of COVID-19 so severe it required hospitalization in an intensive care unit.
“Our study provides the most precise measure to date of the effect of COVID-19 in cancer patients,” wrote researchers who were led by Paolo Boffetta, MD, MPH, a specialist in population science with the Stony Brook Cancer Center in New York.
Dr. Boffetta and colleagues also found that patients with hematologic neoplasms had a higher mortality rate from COVID-19 comparable to that of all cancers combined.
Cancer patients have long been considered to be among those patients who are at high risk of developing COVID-19, and if they contract the disease, they are at high risk of having poor outcomes. Other high-risk patients include those with hypertension, diabetes, chronic kidney disease, or COPD, or the elderly. But how high the risk of developing severe COVID-19 disease is for cancer patients hasn’t yet been documented on a wide scale.
The study, which was made available as a preprint on medRxiv on Oct. 23, is based on an analysis of COVID-19 cases that were documented in 35 reviews, meta-analyses, case reports, and studies indexed in PubMed from authors in North America, Europe, and Asia.
In this study, the pooled odds ratio for mortality for all patients with any cancer was 2.32 (95% confidence interval, 1.82-2.94; 24 studies). For ICU admission, the odds ratio was 2.39 (95% CI, 1.90-3.02; I2 0.0%; 5 studies). And, for disease severity or hospitalization, it was 2.08 (95% CI, 1.60-2.72; I2 92.1%; 15 studies). The pooled mortality odds ratio for hematologic neoplasms was 2.14 (95% CI, 1.87-2.44; I2 20.8%; 8 studies).
Their findings, which have not yet been peer reviewed, confirmed the results of a similar analysis from China published as a preprint in May 2020. The analysis included 181,323 patients (23,736 cancer patients) from 26 studies reported an odds ratio of 2.54 (95% CI, 1.47-4.42). “Cancer patients with COVID-19 have an increased likelihood of death compared to non-cancer COVID-19 patients,” Venkatesulu et al. wrote. And a systematic review and meta-analysis of five studies of 2,619 patients published in October 2020 in Medicine also found a significantly higher risk of death from COVID-19 among cancer patients (odds ratio, 2.63; 95% confidence interval, 1.14-6.06; P = .023; I2 = 26.4%).
Fakih et al., writing in the journal Hematology/Oncology and Stem Cell Therapy conducted a meta-analysis early last year finding a threefold increase for admission to the intensive care unit, an almost fourfold increase for a severe SARS-CoV-2 infection, and a fivefold increase for being intubated.
The three studies show that mortality rates were higher early in the pandemic “when diagnosis and treatment for SARS-CoV-2 might have been delayed, resulting in higher death rate,” Boffetta et al. wrote, adding that their analysis showed only a twofold increase most likely because it was a year-long analysis.
“Future studies will be able to better analyze this association for the different subtypes of cancer. Furthermore, they will eventually be able to evaluate whether the difference among vaccinated population is reduced,” Boffetta et al. wrote.
The authors noted several limitations for the study, including the fact that many of the studies included in the analysis did not include sex, age, comorbidities, and therapy. Nor were the authors able to analyze specific cancers other than hematologic neoplasms.
The authors declared no conflicts of interest.
FROM MEDRXIV