User login
Liquid biopsy in metastatic breast cancer management: Where does it stand in clinical practice?
Tissue biopsy remains the gold standard for characterizing tumor biology and guiding therapeutic decisions, but liquid biopsies — blood analyses that allow oncologists to detect circulating tumor cells (CTCs) and circulating tumor DNA (ctDNA) in the blood — are increasingly demonstrating their value. Last year, the U.S. Food and Drug Administration (FDA) approved two liquid biopsy tests, Guardant360 CDx and FoundationOne Liquid CDx, that can identify more than 300 cancer-related genes in the blood. In 2019, the FDA also approved the first companion diagnostic test, therascreen, to pinpoint PIK3CA gene mutations in patients’ ctDNA and determine whether patients should receive the PI3K inhibitor alpelisib along with fulvestrant.
Here’s an overview of how liquid biopsy is being used in monitoring MBC progression and treatment — and what some oncologists think of it.
What we do and don’t know
“Identifying a patient’s targetable mutations, most notably PIK3CA mutations, is currently the main use of liquid biopsy,” said Pedram Razavi, MD, PhD, a medical oncologist who leads the liquid biopsy program for breast cancer at Memorial Sloan Kettering (MSK) Cancer Center in New York City. “Patients who come to MSK are offered a tumor and liquid biopsy at the time of metastatic diagnosis as part of the standard of care.”
Liquid and tissue biopsy analyses can provide a more complete picture of a patient’s condition. Whereas tissue biopsy allows oncologists to target a more saturated sample of the cancer ecosystem and a wider array of biomarkers, liquid biopsy offers important advantages as well, including a less invasive way to sequence a sample, monitor patients’ treatment response, or track tumor evolution. Liquid biopsy also provides a bigger picture view of tumor heterogeneity by pooling information from many tumor locations as opposed to one.
But, cautioned Yuan Yuan, MD, PhD, liquid biopsy technology is not always sensitive enough to detect CTCs, ctDNA, or all relevant mutations. “When you collect a small tube of blood, you’re essentially trying to catch a small fish in a big sea and wading through a lot of background noise,” said Dr. Yuan, medical oncologist at City of Hope, a comprehensive cancer center in Los Angeles County. “The results may be hard to interpret or come back inconclusive.”
And although emerging data suggest that liquid biopsy provides important insights about tumor dynamics — including mapping disease progression, predicting survival, and even detecting signs of cancer recurrence before metastasis develops — the tool has limited utility in clinical practice outside of identifying sensitivity to various therapies or drugs.
“Right now, a lot of research is being done to understand how to use CTC and ctDNA in particular as a means of surveillance in breast cancer, but we’re still in the beginning stages of applying that outside of clinical trials,” said Joseph A. Sparano, MD, deputy director of the Tisch Cancer Institute and chief of the division of hematology and medical oncology, Icahn School of Medicine at Mount Sinai, New York City.
Personalizing treatment
The companion diagnostic test therascreen marked the beginning stages of using liquid biopsy to match treatments to genetic abnormalities in MBC. The SOLAR-1 phase 3 trial, which led to the approval of alpelisib and therascreen, found that the PI3K inhibitor plus fulvestrant almost doubled progression-free survival (PFS) (11 months vs 5.7 months in placebo-fulvestrant group) in patients with PIK3CA-mutated, HR-positive, HER2-negative advanced breast cancer.
More recent studies have shown that liquid biopsy tests can also identify ESR1 mutations and predict responses to inhibitors that target AKT1 and HER2. Investigators presenting at the 2021 American Society of Clinical Oncology meeting reported that next-generation sequencing of ctDNA in patients with HR-positive MBC, HER-positive MBC, or triple-negative breast cancer detected ESR1 mutations in 14% of patients (71 of 501). Moreover, ESR1 mutations were found only in HR-positive patients who had already received endocrine therapy. (The study also examined PIK3CA mutations, which occurred in about one third of patients). A more in-depth look revealed that ESR1 mutations were strongly associated with liver and bone metastases and that mutations along specific codons negatively affected overall survival (OS) and PFS: codons 537 and 538 for OS and codons 380 and 536 for PFS.
According to Debasish Tripathy, MD, professor and chairman of the department of breast medical oncology at the University of Texas MD Anderson Cancer Center in Houston, in addition to tumor sequencing, “liquid biopsy has become a great research tool to track patients in real time and predict, for instance, who will respond to a treatment and identify emerging resistance.”
In terms of predicting responses to treatment, the plasmaMATCH trial assessed ctDNA in 1,034 patients with advanced breast cancer for mutations in ESR1, HER2, and AKT1 using digital droplet polymerase chain reaction (PCR) and Guardant360. Results showed that 357 (34.5%) of these patients had potentially targetable aberrations, including 222 patients with ESR1 mutations, 36 patients with HER2 mutations, and 30 patients with AKT1 mutations.
Agreement between digital droplet PCR and Guardant360 testing was 96%-99%, and liquid biopsy showed 93% sensitivity compared with tumor samples. The investigators also used liquid biopsy findings to match patients’ mutations to targeted treatments: fulvestrant for those with ESR1 mutations, neratinib for HER2 (ERBB2) mutations, and the selective AKT inhibitor capivasertib for estrogen receptor–positive tumors with AKT1 mutations.
Overall, the investigators concluded that ctDNA testing offers “accurate tumor genotyping” in line with tissue-based testing and is ready for routine clinical practice to identify common as well as rare genetic alterations, such as HER2 and AKT1 mutations, that affect only about 5% of patients with advanced disease.
Predicting survival and recurrence
A particularly promising area for liquid biopsy is its usefulness in helping to predict survival outcomes and monitor patients for early signs of recurrence before metastasis occurs. But the data to support this are still in their infancy.
A highly cited study, published over 15 years ago in the New England Journal of Medicine, found that patients with MBC who had five or more CTCs per 7.5 mL of whole blood before receiving first-line therapy exhibited significantly shorter median PFS (2.7 vs 7.0 months) and OS (10 vs > 18 months) compared with patients with fewer than five CTCs. Subsequent analyses performed more than a decade later, including a meta-analysis published last year, helped validate these early findings that levels of CTCs detected in the blood independently and strongly predicted PFS and OS in patients with MBC.
In addition, ctDNA can provide important information about patients’ survival odds. In a retrospective study published last year, investigators tracked changes in ctDNA in 291 plasma samples from 84 patients with locally advanced breast cancer who participated in the I-SPY trial. Patients who remained ctDNA-positive after 3 weeks of neoadjuvant chemotherapy were significantly more likely to have residual disease after completing their treatment compared with patients who cleared ctDNA at that early stage (83% for those with nonpathologic complete response vs 52%). Notably, the presence of ctDNA between therapy initiation and completion was associated with a significantly greater risk for metastatic recurrence, whereas clearance of ctDNA after neoadjuvant therapy was linked to improved survival.
“The study is important because it highlights how tracking circulating ctDNA status in neoadjuvant-treated breast cancer can expose a patient’s risk for distant metastasis,” said Dr. Yuan. But, she added, “I think the biggest attraction of liquid biopsy will be the ability to detect molecular disease even before imaging can, and identify who has a high risk for recurrence.”
Dr. Razavi agreed that the potential to prevent metastasis by finding minimal residual disease (MRD) is the most exciting area of liquid biopsy research. “If we can find tumor DNA early before tumors have a chance to establish themselves, we could potentially change the trajectory of the disease for patients,” he said.
Several studies suggest that monitoring patients’ ctDNA levels after neoadjuvant treatment and surgery may help predict their risk for relapse and progression to metastatic disease. A 2015 analysis, which followed 20 patients with breast cancer after surgery, found that ctDNA monitoring accurately differentiated those who ultimately developed metastatic disease from those who didn’t (sensitivity, 93%; specificity, 100%) and detected metastatic disease 11 months earlier, on average, than imaging did. Another 2015 study found that the presence of ctDNA in plasma after neoadjuvant chemotherapy and surgery predicted metastatic relapse a median of almost 8 months before clinical detection. Other recent data show the power of ultrasensitive blood tests to detect MRD and potentially find metastatic disease early.
Although an increasing number of studies show that ctDNA and CTCs are prognostic for breast cancer recurrence, a major question remains: For patients with ctDNA or CTCs but no overt disease after imaging, will initiating therapy prevent or delay the development of metastatic disease?
“We still have to do those clinical trials to determine whether detecting MRD and treating patients early actually positively affects their survival and quality of life,” Dr. Razavi said.
Tissue biopsy remains the gold standard for characterizing tumor biology and guiding therapeutic decisions, but liquid biopsies — blood analyses that allow oncologists to detect circulating tumor cells (CTCs) and circulating tumor DNA (ctDNA) in the blood — are increasingly demonstrating their value. Last year, the U.S. Food and Drug Administration (FDA) approved two liquid biopsy tests, Guardant360 CDx and FoundationOne Liquid CDx, that can identify more than 300 cancer-related genes in the blood. In 2019, the FDA also approved the first companion diagnostic test, therascreen, to pinpoint PIK3CA gene mutations in patients’ ctDNA and determine whether patients should receive the PI3K inhibitor alpelisib along with fulvestrant.
Here’s an overview of how liquid biopsy is being used in monitoring MBC progression and treatment — and what some oncologists think of it.
What we do and don’t know
“Identifying a patient’s targetable mutations, most notably PIK3CA mutations, is currently the main use of liquid biopsy,” said Pedram Razavi, MD, PhD, a medical oncologist who leads the liquid biopsy program for breast cancer at Memorial Sloan Kettering (MSK) Cancer Center in New York City. “Patients who come to MSK are offered a tumor and liquid biopsy at the time of metastatic diagnosis as part of the standard of care.”
Liquid and tissue biopsy analyses can provide a more complete picture of a patient’s condition. Whereas tissue biopsy allows oncologists to target a more saturated sample of the cancer ecosystem and a wider array of biomarkers, liquid biopsy offers important advantages as well, including a less invasive way to sequence a sample, monitor patients’ treatment response, or track tumor evolution. Liquid biopsy also provides a bigger picture view of tumor heterogeneity by pooling information from many tumor locations as opposed to one.
But, cautioned Yuan Yuan, MD, PhD, liquid biopsy technology is not always sensitive enough to detect CTCs, ctDNA, or all relevant mutations. “When you collect a small tube of blood, you’re essentially trying to catch a small fish in a big sea and wading through a lot of background noise,” said Dr. Yuan, medical oncologist at City of Hope, a comprehensive cancer center in Los Angeles County. “The results may be hard to interpret or come back inconclusive.”
And although emerging data suggest that liquid biopsy provides important insights about tumor dynamics — including mapping disease progression, predicting survival, and even detecting signs of cancer recurrence before metastasis develops — the tool has limited utility in clinical practice outside of identifying sensitivity to various therapies or drugs.
“Right now, a lot of research is being done to understand how to use CTC and ctDNA in particular as a means of surveillance in breast cancer, but we’re still in the beginning stages of applying that outside of clinical trials,” said Joseph A. Sparano, MD, deputy director of the Tisch Cancer Institute and chief of the division of hematology and medical oncology, Icahn School of Medicine at Mount Sinai, New York City.
Personalizing treatment
The companion diagnostic test therascreen marked the beginning stages of using liquid biopsy to match treatments to genetic abnormalities in MBC. The SOLAR-1 phase 3 trial, which led to the approval of alpelisib and therascreen, found that the PI3K inhibitor plus fulvestrant almost doubled progression-free survival (PFS) (11 months vs 5.7 months in placebo-fulvestrant group) in patients with PIK3CA-mutated, HR-positive, HER2-negative advanced breast cancer.
More recent studies have shown that liquid biopsy tests can also identify ESR1 mutations and predict responses to inhibitors that target AKT1 and HER2. Investigators presenting at the 2021 American Society of Clinical Oncology meeting reported that next-generation sequencing of ctDNA in patients with HR-positive MBC, HER-positive MBC, or triple-negative breast cancer detected ESR1 mutations in 14% of patients (71 of 501). Moreover, ESR1 mutations were found only in HR-positive patients who had already received endocrine therapy. (The study also examined PIK3CA mutations, which occurred in about one third of patients). A more in-depth look revealed that ESR1 mutations were strongly associated with liver and bone metastases and that mutations along specific codons negatively affected overall survival (OS) and PFS: codons 537 and 538 for OS and codons 380 and 536 for PFS.
According to Debasish Tripathy, MD, professor and chairman of the department of breast medical oncology at the University of Texas MD Anderson Cancer Center in Houston, in addition to tumor sequencing, “liquid biopsy has become a great research tool to track patients in real time and predict, for instance, who will respond to a treatment and identify emerging resistance.”
In terms of predicting responses to treatment, the plasmaMATCH trial assessed ctDNA in 1,034 patients with advanced breast cancer for mutations in ESR1, HER2, and AKT1 using digital droplet polymerase chain reaction (PCR) and Guardant360. Results showed that 357 (34.5%) of these patients had potentially targetable aberrations, including 222 patients with ESR1 mutations, 36 patients with HER2 mutations, and 30 patients with AKT1 mutations.
Agreement between digital droplet PCR and Guardant360 testing was 96%-99%, and liquid biopsy showed 93% sensitivity compared with tumor samples. The investigators also used liquid biopsy findings to match patients’ mutations to targeted treatments: fulvestrant for those with ESR1 mutations, neratinib for HER2 (ERBB2) mutations, and the selective AKT inhibitor capivasertib for estrogen receptor–positive tumors with AKT1 mutations.
Overall, the investigators concluded that ctDNA testing offers “accurate tumor genotyping” in line with tissue-based testing and is ready for routine clinical practice to identify common as well as rare genetic alterations, such as HER2 and AKT1 mutations, that affect only about 5% of patients with advanced disease.
Predicting survival and recurrence
A particularly promising area for liquid biopsy is its usefulness in helping to predict survival outcomes and monitor patients for early signs of recurrence before metastasis occurs. But the data to support this are still in their infancy.
A highly cited study, published over 15 years ago in the New England Journal of Medicine, found that patients with MBC who had five or more CTCs per 7.5 mL of whole blood before receiving first-line therapy exhibited significantly shorter median PFS (2.7 vs 7.0 months) and OS (10 vs > 18 months) compared with patients with fewer than five CTCs. Subsequent analyses performed more than a decade later, including a meta-analysis published last year, helped validate these early findings that levels of CTCs detected in the blood independently and strongly predicted PFS and OS in patients with MBC.
In addition, ctDNA can provide important information about patients’ survival odds. In a retrospective study published last year, investigators tracked changes in ctDNA in 291 plasma samples from 84 patients with locally advanced breast cancer who participated in the I-SPY trial. Patients who remained ctDNA-positive after 3 weeks of neoadjuvant chemotherapy were significantly more likely to have residual disease after completing their treatment compared with patients who cleared ctDNA at that early stage (83% for those with nonpathologic complete response vs 52%). Notably, the presence of ctDNA between therapy initiation and completion was associated with a significantly greater risk for metastatic recurrence, whereas clearance of ctDNA after neoadjuvant therapy was linked to improved survival.
“The study is important because it highlights how tracking circulating ctDNA status in neoadjuvant-treated breast cancer can expose a patient’s risk for distant metastasis,” said Dr. Yuan. But, she added, “I think the biggest attraction of liquid biopsy will be the ability to detect molecular disease even before imaging can, and identify who has a high risk for recurrence.”
Dr. Razavi agreed that the potential to prevent metastasis by finding minimal residual disease (MRD) is the most exciting area of liquid biopsy research. “If we can find tumor DNA early before tumors have a chance to establish themselves, we could potentially change the trajectory of the disease for patients,” he said.
Several studies suggest that monitoring patients’ ctDNA levels after neoadjuvant treatment and surgery may help predict their risk for relapse and progression to metastatic disease. A 2015 analysis, which followed 20 patients with breast cancer after surgery, found that ctDNA monitoring accurately differentiated those who ultimately developed metastatic disease from those who didn’t (sensitivity, 93%; specificity, 100%) and detected metastatic disease 11 months earlier, on average, than imaging did. Another 2015 study found that the presence of ctDNA in plasma after neoadjuvant chemotherapy and surgery predicted metastatic relapse a median of almost 8 months before clinical detection. Other recent data show the power of ultrasensitive blood tests to detect MRD and potentially find metastatic disease early.
Although an increasing number of studies show that ctDNA and CTCs are prognostic for breast cancer recurrence, a major question remains: For patients with ctDNA or CTCs but no overt disease after imaging, will initiating therapy prevent or delay the development of metastatic disease?
“We still have to do those clinical trials to determine whether detecting MRD and treating patients early actually positively affects their survival and quality of life,” Dr. Razavi said.
Tissue biopsy remains the gold standard for characterizing tumor biology and guiding therapeutic decisions, but liquid biopsies — blood analyses that allow oncologists to detect circulating tumor cells (CTCs) and circulating tumor DNA (ctDNA) in the blood — are increasingly demonstrating their value. Last year, the U.S. Food and Drug Administration (FDA) approved two liquid biopsy tests, Guardant360 CDx and FoundationOne Liquid CDx, that can identify more than 300 cancer-related genes in the blood. In 2019, the FDA also approved the first companion diagnostic test, therascreen, to pinpoint PIK3CA gene mutations in patients’ ctDNA and determine whether patients should receive the PI3K inhibitor alpelisib along with fulvestrant.
Here’s an overview of how liquid biopsy is being used in monitoring MBC progression and treatment — and what some oncologists think of it.
What we do and don’t know
“Identifying a patient’s targetable mutations, most notably PIK3CA mutations, is currently the main use of liquid biopsy,” said Pedram Razavi, MD, PhD, a medical oncologist who leads the liquid biopsy program for breast cancer at Memorial Sloan Kettering (MSK) Cancer Center in New York City. “Patients who come to MSK are offered a tumor and liquid biopsy at the time of metastatic diagnosis as part of the standard of care.”
Liquid and tissue biopsy analyses can provide a more complete picture of a patient’s condition. Whereas tissue biopsy allows oncologists to target a more saturated sample of the cancer ecosystem and a wider array of biomarkers, liquid biopsy offers important advantages as well, including a less invasive way to sequence a sample, monitor patients’ treatment response, or track tumor evolution. Liquid biopsy also provides a bigger picture view of tumor heterogeneity by pooling information from many tumor locations as opposed to one.
But, cautioned Yuan Yuan, MD, PhD, liquid biopsy technology is not always sensitive enough to detect CTCs, ctDNA, or all relevant mutations. “When you collect a small tube of blood, you’re essentially trying to catch a small fish in a big sea and wading through a lot of background noise,” said Dr. Yuan, medical oncologist at City of Hope, a comprehensive cancer center in Los Angeles County. “The results may be hard to interpret or come back inconclusive.”
And although emerging data suggest that liquid biopsy provides important insights about tumor dynamics — including mapping disease progression, predicting survival, and even detecting signs of cancer recurrence before metastasis develops — the tool has limited utility in clinical practice outside of identifying sensitivity to various therapies or drugs.
“Right now, a lot of research is being done to understand how to use CTC and ctDNA in particular as a means of surveillance in breast cancer, but we’re still in the beginning stages of applying that outside of clinical trials,” said Joseph A. Sparano, MD, deputy director of the Tisch Cancer Institute and chief of the division of hematology and medical oncology, Icahn School of Medicine at Mount Sinai, New York City.
Personalizing treatment
The companion diagnostic test therascreen marked the beginning stages of using liquid biopsy to match treatments to genetic abnormalities in MBC. The SOLAR-1 phase 3 trial, which led to the approval of alpelisib and therascreen, found that the PI3K inhibitor plus fulvestrant almost doubled progression-free survival (PFS) (11 months vs 5.7 months in placebo-fulvestrant group) in patients with PIK3CA-mutated, HR-positive, HER2-negative advanced breast cancer.
More recent studies have shown that liquid biopsy tests can also identify ESR1 mutations and predict responses to inhibitors that target AKT1 and HER2. Investigators presenting at the 2021 American Society of Clinical Oncology meeting reported that next-generation sequencing of ctDNA in patients with HR-positive MBC, HER-positive MBC, or triple-negative breast cancer detected ESR1 mutations in 14% of patients (71 of 501). Moreover, ESR1 mutations were found only in HR-positive patients who had already received endocrine therapy. (The study also examined PIK3CA mutations, which occurred in about one third of patients). A more in-depth look revealed that ESR1 mutations were strongly associated with liver and bone metastases and that mutations along specific codons negatively affected overall survival (OS) and PFS: codons 537 and 538 for OS and codons 380 and 536 for PFS.
According to Debasish Tripathy, MD, professor and chairman of the department of breast medical oncology at the University of Texas MD Anderson Cancer Center in Houston, in addition to tumor sequencing, “liquid biopsy has become a great research tool to track patients in real time and predict, for instance, who will respond to a treatment and identify emerging resistance.”
In terms of predicting responses to treatment, the plasmaMATCH trial assessed ctDNA in 1,034 patients with advanced breast cancer for mutations in ESR1, HER2, and AKT1 using digital droplet polymerase chain reaction (PCR) and Guardant360. Results showed that 357 (34.5%) of these patients had potentially targetable aberrations, including 222 patients with ESR1 mutations, 36 patients with HER2 mutations, and 30 patients with AKT1 mutations.
Agreement between digital droplet PCR and Guardant360 testing was 96%-99%, and liquid biopsy showed 93% sensitivity compared with tumor samples. The investigators also used liquid biopsy findings to match patients’ mutations to targeted treatments: fulvestrant for those with ESR1 mutations, neratinib for HER2 (ERBB2) mutations, and the selective AKT inhibitor capivasertib for estrogen receptor–positive tumors with AKT1 mutations.
Overall, the investigators concluded that ctDNA testing offers “accurate tumor genotyping” in line with tissue-based testing and is ready for routine clinical practice to identify common as well as rare genetic alterations, such as HER2 and AKT1 mutations, that affect only about 5% of patients with advanced disease.
Predicting survival and recurrence
A particularly promising area for liquid biopsy is its usefulness in helping to predict survival outcomes and monitor patients for early signs of recurrence before metastasis occurs. But the data to support this are still in their infancy.
A highly cited study, published over 15 years ago in the New England Journal of Medicine, found that patients with MBC who had five or more CTCs per 7.5 mL of whole blood before receiving first-line therapy exhibited significantly shorter median PFS (2.7 vs 7.0 months) and OS (10 vs > 18 months) compared with patients with fewer than five CTCs. Subsequent analyses performed more than a decade later, including a meta-analysis published last year, helped validate these early findings that levels of CTCs detected in the blood independently and strongly predicted PFS and OS in patients with MBC.
In addition, ctDNA can provide important information about patients’ survival odds. In a retrospective study published last year, investigators tracked changes in ctDNA in 291 plasma samples from 84 patients with locally advanced breast cancer who participated in the I-SPY trial. Patients who remained ctDNA-positive after 3 weeks of neoadjuvant chemotherapy were significantly more likely to have residual disease after completing their treatment compared with patients who cleared ctDNA at that early stage (83% for those with nonpathologic complete response vs 52%). Notably, the presence of ctDNA between therapy initiation and completion was associated with a significantly greater risk for metastatic recurrence, whereas clearance of ctDNA after neoadjuvant therapy was linked to improved survival.
“The study is important because it highlights how tracking circulating ctDNA status in neoadjuvant-treated breast cancer can expose a patient’s risk for distant metastasis,” said Dr. Yuan. But, she added, “I think the biggest attraction of liquid biopsy will be the ability to detect molecular disease even before imaging can, and identify who has a high risk for recurrence.”
Dr. Razavi agreed that the potential to prevent metastasis by finding minimal residual disease (MRD) is the most exciting area of liquid biopsy research. “If we can find tumor DNA early before tumors have a chance to establish themselves, we could potentially change the trajectory of the disease for patients,” he said.
Several studies suggest that monitoring patients’ ctDNA levels after neoadjuvant treatment and surgery may help predict their risk for relapse and progression to metastatic disease. A 2015 analysis, which followed 20 patients with breast cancer after surgery, found that ctDNA monitoring accurately differentiated those who ultimately developed metastatic disease from those who didn’t (sensitivity, 93%; specificity, 100%) and detected metastatic disease 11 months earlier, on average, than imaging did. Another 2015 study found that the presence of ctDNA in plasma after neoadjuvant chemotherapy and surgery predicted metastatic relapse a median of almost 8 months before clinical detection. Other recent data show the power of ultrasensitive blood tests to detect MRD and potentially find metastatic disease early.
Although an increasing number of studies show that ctDNA and CTCs are prognostic for breast cancer recurrence, a major question remains: For patients with ctDNA or CTCs but no overt disease after imaging, will initiating therapy prevent or delay the development of metastatic disease?
“We still have to do those clinical trials to determine whether detecting MRD and treating patients early actually positively affects their survival and quality of life,” Dr. Razavi said.
Dogs show potential as medical detectives in breast cancer
Breast cancer screening using urine samples based on the volatile organic compounds (VOCs) sensed by a trained dog is feasible, according to a preliminary study published in the journal Biology June 10.
“The extrapolation of our results to widespread implementation is still uncertain,” wrote Shoko Kure, MD, PhD, of Nippon Medical School in Tokyo, and colleagues. “However, even if few dogs could be trained to detect breast cancer, the result may open the door to a robust and inexpensive way to detect breast cancer.” They added that “dog cancer detection is entirely noninvasive, safe and easy for both patients and everyone.”
Early detection of breast cancer, which is the leading cause of death globally, is essential for more efficient treatment. While mammography can detect asymptomatic breast cancer and reduce mortality, it has a poor compliance, is less sensitive in dense breast tissue, detects nonmalignant lesions, and has not been shown to reduce mortality in women younger than 40. VOCs are emitted in the breath, blood, and urine, with different volatile patterns correlated with a variety of diseases including cancers, which dogs can be trained to detect. Breast cancer screening by dog sniffing of the VOCs in urine samples has not been attempted.
Dogs have been used as medical detectives for several cancers and conditions. A study published in 2018 showed that trained dogs who were able to differentiate the specific odor from the metabolic waste of breast cancer in vitro could identify that of colorectal cancer, and vice versa. More recently, research showed that trained dogs could detect advanced prostate cancer in urine samples with high specificity and sensitivity. In this double-blinded pilot study, two dogs were trained to detect Gleason 9 prostate cancer in urine collected from biopsy-confirmed patients. The canine olfaction system was 71% sensitive and as much as 76% specific at detecting Gleason 9 cancer. Along with cancer, trained dogs have been shown to identify people with COVID-19, even those who were asymptomatic. In this study, dogs who sniffed swab samples of armpit sweat could identify which samples came from patients infected with COVID-19 with up to 100% accuracy, while ruling out infection with up to 99% accuracy.
The double-blind study by Dr. Kure aimed to assess the potential of VOCs in urine samples for breast cancer screening by using a single trained sniffer dog – in this case a 9-year-old female Labrador retriever. Urine samples from 40 patients with primary breast cancer and 142 patients with non-breast malignant diseases were included along with samples from 18 healthy volunteers. In 40 times out of 40 runs of the double-blind test, the dog correctly identified urine samples of patients with breast cancer, with 100% sensitivity and 100% specificity.
“The dog in this test successfully differentiated breast cancer from non-breast malignancies and healthy controls,” the authors wrote. “This is the first, preliminary study indicating the feasibility of developing a new breast cancer screening method using urine samples based on VOCs.”
While the authors noted that the study was limited as it relied on one trained dog, they suggested that this method has potential in low-income countries where access to mammography is inadequate.
“Some well-trained sniffing dogs traveling around medically underserved [countries] all over the world could save many lives. Even when a healthy control was indicated by a trained dog, there would be a suspicion of undiagnosed/early-stage cancer, and the person would be advised to undergo medical screening,” the authors wrote.
The authors declared no conflicts of interest.
Breast cancer screening using urine samples based on the volatile organic compounds (VOCs) sensed by a trained dog is feasible, according to a preliminary study published in the journal Biology June 10.
“The extrapolation of our results to widespread implementation is still uncertain,” wrote Shoko Kure, MD, PhD, of Nippon Medical School in Tokyo, and colleagues. “However, even if few dogs could be trained to detect breast cancer, the result may open the door to a robust and inexpensive way to detect breast cancer.” They added that “dog cancer detection is entirely noninvasive, safe and easy for both patients and everyone.”
Early detection of breast cancer, which is the leading cause of death globally, is essential for more efficient treatment. While mammography can detect asymptomatic breast cancer and reduce mortality, it has a poor compliance, is less sensitive in dense breast tissue, detects nonmalignant lesions, and has not been shown to reduce mortality in women younger than 40. VOCs are emitted in the breath, blood, and urine, with different volatile patterns correlated with a variety of diseases including cancers, which dogs can be trained to detect. Breast cancer screening by dog sniffing of the VOCs in urine samples has not been attempted.
Dogs have been used as medical detectives for several cancers and conditions. A study published in 2018 showed that trained dogs who were able to differentiate the specific odor from the metabolic waste of breast cancer in vitro could identify that of colorectal cancer, and vice versa. More recently, research showed that trained dogs could detect advanced prostate cancer in urine samples with high specificity and sensitivity. In this double-blinded pilot study, two dogs were trained to detect Gleason 9 prostate cancer in urine collected from biopsy-confirmed patients. The canine olfaction system was 71% sensitive and as much as 76% specific at detecting Gleason 9 cancer. Along with cancer, trained dogs have been shown to identify people with COVID-19, even those who were asymptomatic. In this study, dogs who sniffed swab samples of armpit sweat could identify which samples came from patients infected with COVID-19 with up to 100% accuracy, while ruling out infection with up to 99% accuracy.
The double-blind study by Dr. Kure aimed to assess the potential of VOCs in urine samples for breast cancer screening by using a single trained sniffer dog – in this case a 9-year-old female Labrador retriever. Urine samples from 40 patients with primary breast cancer and 142 patients with non-breast malignant diseases were included along with samples from 18 healthy volunteers. In 40 times out of 40 runs of the double-blind test, the dog correctly identified urine samples of patients with breast cancer, with 100% sensitivity and 100% specificity.
“The dog in this test successfully differentiated breast cancer from non-breast malignancies and healthy controls,” the authors wrote. “This is the first, preliminary study indicating the feasibility of developing a new breast cancer screening method using urine samples based on VOCs.”
While the authors noted that the study was limited as it relied on one trained dog, they suggested that this method has potential in low-income countries where access to mammography is inadequate.
“Some well-trained sniffing dogs traveling around medically underserved [countries] all over the world could save many lives. Even when a healthy control was indicated by a trained dog, there would be a suspicion of undiagnosed/early-stage cancer, and the person would be advised to undergo medical screening,” the authors wrote.
The authors declared no conflicts of interest.
Breast cancer screening using urine samples based on the volatile organic compounds (VOCs) sensed by a trained dog is feasible, according to a preliminary study published in the journal Biology June 10.
“The extrapolation of our results to widespread implementation is still uncertain,” wrote Shoko Kure, MD, PhD, of Nippon Medical School in Tokyo, and colleagues. “However, even if few dogs could be trained to detect breast cancer, the result may open the door to a robust and inexpensive way to detect breast cancer.” They added that “dog cancer detection is entirely noninvasive, safe and easy for both patients and everyone.”
Early detection of breast cancer, which is the leading cause of death globally, is essential for more efficient treatment. While mammography can detect asymptomatic breast cancer and reduce mortality, it has a poor compliance, is less sensitive in dense breast tissue, detects nonmalignant lesions, and has not been shown to reduce mortality in women younger than 40. VOCs are emitted in the breath, blood, and urine, with different volatile patterns correlated with a variety of diseases including cancers, which dogs can be trained to detect. Breast cancer screening by dog sniffing of the VOCs in urine samples has not been attempted.
Dogs have been used as medical detectives for several cancers and conditions. A study published in 2018 showed that trained dogs who were able to differentiate the specific odor from the metabolic waste of breast cancer in vitro could identify that of colorectal cancer, and vice versa. More recently, research showed that trained dogs could detect advanced prostate cancer in urine samples with high specificity and sensitivity. In this double-blinded pilot study, two dogs were trained to detect Gleason 9 prostate cancer in urine collected from biopsy-confirmed patients. The canine olfaction system was 71% sensitive and as much as 76% specific at detecting Gleason 9 cancer. Along with cancer, trained dogs have been shown to identify people with COVID-19, even those who were asymptomatic. In this study, dogs who sniffed swab samples of armpit sweat could identify which samples came from patients infected with COVID-19 with up to 100% accuracy, while ruling out infection with up to 99% accuracy.
The double-blind study by Dr. Kure aimed to assess the potential of VOCs in urine samples for breast cancer screening by using a single trained sniffer dog – in this case a 9-year-old female Labrador retriever. Urine samples from 40 patients with primary breast cancer and 142 patients with non-breast malignant diseases were included along with samples from 18 healthy volunteers. In 40 times out of 40 runs of the double-blind test, the dog correctly identified urine samples of patients with breast cancer, with 100% sensitivity and 100% specificity.
“The dog in this test successfully differentiated breast cancer from non-breast malignancies and healthy controls,” the authors wrote. “This is the first, preliminary study indicating the feasibility of developing a new breast cancer screening method using urine samples based on VOCs.”
While the authors noted that the study was limited as it relied on one trained dog, they suggested that this method has potential in low-income countries where access to mammography is inadequate.
“Some well-trained sniffing dogs traveling around medically underserved [countries] all over the world could save many lives. Even when a healthy control was indicated by a trained dog, there would be a suspicion of undiagnosed/early-stage cancer, and the person would be advised to undergo medical screening,” the authors wrote.
The authors declared no conflicts of interest.
FROM BIOLOGY
3D vs 2D mammography for detecting cancer in dense breasts
Text copyright DenseBreast-info.org.
Answer
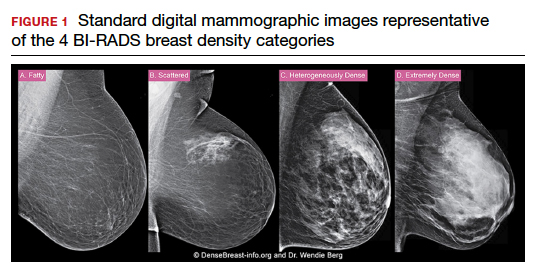
C. Overall, tomosynthesis depicts an additional 1 to 2 cancers per thousand women screened in the first round of screening when added to standard digital mammography;1-3 however, this improvement in cancer detection is only observed in women with fatty breasts (category A), scattered fibroglandular tissue (category B), and heterogeneously dense breasts (category C). Importantly, tomosynthesis does not significantly improve breast cancer detection in women with extremely dense breasts (category D).2,4
Digital breast tomosynthesis, also referred to as “3-dimensional mammography” (3D mammography) or tomosynthesis, uses a dedicated electronic detector system to obtain multiple projection images that are reconstructed by the computer to create thin slices or slabs of multiple slices of the breast. These slices can be individually “scrolled through” by the radiologist to reduce tissue overlap that may obscure breast cancers on a standard mammogram. While tomosynthesis improves breast cancer detection in women with fatty, scattered fibroglandular density, and heterogeneously dense breasts, there is very little soft tissue contrast in extremely dense breasts due to insufficient fat, and some cancers will remain hidden by dense tissue even on sliced images through the breast.
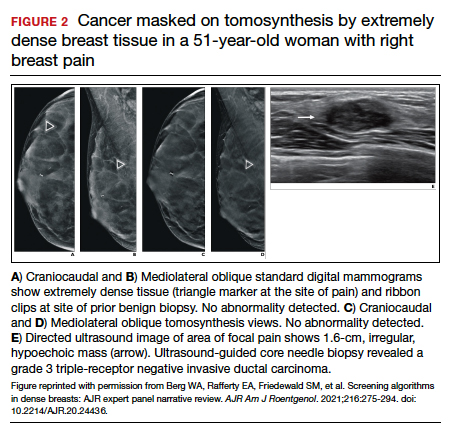
FIGURE 2 shows an example of cancer that was missed on tomosynthesis in a 51-year-old woman with extremely dense breasts and right breast pain. The cancer was masked by extremely dense tissue on standard digital mammography and tomosynthesis; no abnormalities were detected. Ultrasonography showed a 1.6-cm, irregular, hypoechoic mass at the site of pain, and biopsy revealed a grade 3 triple-receptor negative invasive ductal carcinoma.
In women with dense breasts, especially extremely dense breasts, supplemental screening beyond tomosynthesis should be considered. Although tomosynthesis doesn’t improve cancer detection in extremely dense breasts, it does reduce callbacks for additional testing in all breast densities compared with standard digital mammography. Callbacks are reduced from approximately 100‒120 per 1,000 women screened with standard digital mammography alone1,5 to an average of 80 per 1,000 women when tomosynthesis and standard mammography are interpreted together.1-3 ●
For more information, visit medically sourced DenseBreast-info.org. Comprehensive resources include a free CME opportunity, Dense Breasts and Supplemental Screening.
- Conant EF, Zuckerman SP, McDonald ES, et al. Five consecutive years of screening with digital breast tomosynthesis: outcomes by screening year and round. Radiology. 2020;295:285-293.
- Rafferty EA, Durand MA, Conant EF, et al. Breast cancer screening using tomosynthesis and digital mammography in dense and nondense breasts. JAMA. 2016;315:1784-1786.
- Skaane P, Bandos AI, Niklason LT, et al. Digital mammography versus digital mammography plus tomosynthesis in breast cancer screening: the Oslo Tomosynthesis Screening Trial. Radiology. 2019;291:23-30.
- Lowry KP, Coley RY, Miglioretti DL, et al. Screening performance of digital breast tomosynthesis vs digital mammography in community practice by patient age, screening round, and breast density. JAMA Netw Open. 2020;3:e2011792.
- Lee CS, Sengupta D, Bhargavan-Chatfield M, et al. Association of patient age with outcomes of current-era, large-scale screening mammography: analysis of data from the National Mammography Database. JAMA Oncol. 2017;3:1134-1136.
Text copyright DenseBreast-info.org.
Answer
C. Overall, tomosynthesis depicts an additional 1 to 2 cancers per thousand women screened in the first round of screening when added to standard digital mammography;1-3 however, this improvement in cancer detection is only observed in women with fatty breasts (category A), scattered fibroglandular tissue (category B), and heterogeneously dense breasts (category C). Importantly, tomosynthesis does not significantly improve breast cancer detection in women with extremely dense breasts (category D).2,4
Digital breast tomosynthesis, also referred to as “3-dimensional mammography” (3D mammography) or tomosynthesis, uses a dedicated electronic detector system to obtain multiple projection images that are reconstructed by the computer to create thin slices or slabs of multiple slices of the breast. These slices can be individually “scrolled through” by the radiologist to reduce tissue overlap that may obscure breast cancers on a standard mammogram. While tomosynthesis improves breast cancer detection in women with fatty, scattered fibroglandular density, and heterogeneously dense breasts, there is very little soft tissue contrast in extremely dense breasts due to insufficient fat, and some cancers will remain hidden by dense tissue even on sliced images through the breast.
FIGURE 2 shows an example of cancer that was missed on tomosynthesis in a 51-year-old woman with extremely dense breasts and right breast pain. The cancer was masked by extremely dense tissue on standard digital mammography and tomosynthesis; no abnormalities were detected. Ultrasonography showed a 1.6-cm, irregular, hypoechoic mass at the site of pain, and biopsy revealed a grade 3 triple-receptor negative invasive ductal carcinoma.
In women with dense breasts, especially extremely dense breasts, supplemental screening beyond tomosynthesis should be considered. Although tomosynthesis doesn’t improve cancer detection in extremely dense breasts, it does reduce callbacks for additional testing in all breast densities compared with standard digital mammography. Callbacks are reduced from approximately 100‒120 per 1,000 women screened with standard digital mammography alone1,5 to an average of 80 per 1,000 women when tomosynthesis and standard mammography are interpreted together.1-3 ●
For more information, visit medically sourced DenseBreast-info.org. Comprehensive resources include a free CME opportunity, Dense Breasts and Supplemental Screening.
Text copyright DenseBreast-info.org.
Answer
C. Overall, tomosynthesis depicts an additional 1 to 2 cancers per thousand women screened in the first round of screening when added to standard digital mammography;1-3 however, this improvement in cancer detection is only observed in women with fatty breasts (category A), scattered fibroglandular tissue (category B), and heterogeneously dense breasts (category C). Importantly, tomosynthesis does not significantly improve breast cancer detection in women with extremely dense breasts (category D).2,4
Digital breast tomosynthesis, also referred to as “3-dimensional mammography” (3D mammography) or tomosynthesis, uses a dedicated electronic detector system to obtain multiple projection images that are reconstructed by the computer to create thin slices or slabs of multiple slices of the breast. These slices can be individually “scrolled through” by the radiologist to reduce tissue overlap that may obscure breast cancers on a standard mammogram. While tomosynthesis improves breast cancer detection in women with fatty, scattered fibroglandular density, and heterogeneously dense breasts, there is very little soft tissue contrast in extremely dense breasts due to insufficient fat, and some cancers will remain hidden by dense tissue even on sliced images through the breast.
FIGURE 2 shows an example of cancer that was missed on tomosynthesis in a 51-year-old woman with extremely dense breasts and right breast pain. The cancer was masked by extremely dense tissue on standard digital mammography and tomosynthesis; no abnormalities were detected. Ultrasonography showed a 1.6-cm, irregular, hypoechoic mass at the site of pain, and biopsy revealed a grade 3 triple-receptor negative invasive ductal carcinoma.
In women with dense breasts, especially extremely dense breasts, supplemental screening beyond tomosynthesis should be considered. Although tomosynthesis doesn’t improve cancer detection in extremely dense breasts, it does reduce callbacks for additional testing in all breast densities compared with standard digital mammography. Callbacks are reduced from approximately 100‒120 per 1,000 women screened with standard digital mammography alone1,5 to an average of 80 per 1,000 women when tomosynthesis and standard mammography are interpreted together.1-3 ●
For more information, visit medically sourced DenseBreast-info.org. Comprehensive resources include a free CME opportunity, Dense Breasts and Supplemental Screening.
- Conant EF, Zuckerman SP, McDonald ES, et al. Five consecutive years of screening with digital breast tomosynthesis: outcomes by screening year and round. Radiology. 2020;295:285-293.
- Rafferty EA, Durand MA, Conant EF, et al. Breast cancer screening using tomosynthesis and digital mammography in dense and nondense breasts. JAMA. 2016;315:1784-1786.
- Skaane P, Bandos AI, Niklason LT, et al. Digital mammography versus digital mammography plus tomosynthesis in breast cancer screening: the Oslo Tomosynthesis Screening Trial. Radiology. 2019;291:23-30.
- Lowry KP, Coley RY, Miglioretti DL, et al. Screening performance of digital breast tomosynthesis vs digital mammography in community practice by patient age, screening round, and breast density. JAMA Netw Open. 2020;3:e2011792.
- Lee CS, Sengupta D, Bhargavan-Chatfield M, et al. Association of patient age with outcomes of current-era, large-scale screening mammography: analysis of data from the National Mammography Database. JAMA Oncol. 2017;3:1134-1136.
- Conant EF, Zuckerman SP, McDonald ES, et al. Five consecutive years of screening with digital breast tomosynthesis: outcomes by screening year and round. Radiology. 2020;295:285-293.
- Rafferty EA, Durand MA, Conant EF, et al. Breast cancer screening using tomosynthesis and digital mammography in dense and nondense breasts. JAMA. 2016;315:1784-1786.
- Skaane P, Bandos AI, Niklason LT, et al. Digital mammography versus digital mammography plus tomosynthesis in breast cancer screening: the Oslo Tomosynthesis Screening Trial. Radiology. 2019;291:23-30.
- Lowry KP, Coley RY, Miglioretti DL, et al. Screening performance of digital breast tomosynthesis vs digital mammography in community practice by patient age, screening round, and breast density. JAMA Netw Open. 2020;3:e2011792.
- Lee CS, Sengupta D, Bhargavan-Chatfield M, et al. Association of patient age with outcomes of current-era, large-scale screening mammography: analysis of data from the National Mammography Database. JAMA Oncol. 2017;3:1134-1136.
Quiz developed in collaboration with ![]()
Hair follicle miniaturization common in persistent chemo-induced alopecia, case series suggests
and treatment with minoxidil (sometimes with antiandrogen therapy) was associated with improved hair density, according to a recently published retrospective case series.
“An improvement in hair density was observed in most of the patients treated with topical minoxidil or LDOM [low-dose oral minoxidil], with a more favorable outcome seen with LDOM with or without antiandrogens,” reported Bevin Bhoyrul, MBBS, of Sinclair Dermatology in Melbourne and coauthors from the United Kingdom and Germany.
The findings, published in JAMA Dermatology, suggest that pCIA “may be at least partly reversible,” they wrote.
The investigators analyzed the clinicopathologic characteristics of pCIA in 100 patients presenting to the hair clinics, as well as the results of trichoscopy performed in 90 of the patients and biopsies in 18. The researchers also assessed the effectiveness of treatment in 49 of these patients who met their criteria of completing at least 6 months of therapy with minoxidil.
Almost all patients in their series – 92% – were treated with taxanes and had more severe alopecia than those who weren’t exposed to taxanes (a median Sinclair scale grade of 4 vs. 2). Defined as absent or incomplete hair regrowth 6 months or more after completion of chemotherapy, pCIA has been increasingly reported in the literature, the authors note.
Of the 100 patients, all but one of whom were women, 39 had globally-reduced hair density that also involved the occipital area (diffuse alopecia), and 55 patients had thinning of the centroparietal scalp hair in a female pattern hair loss (FPHL) distribution. Patients presented between November 2011 and February 2020 and had a mean age of 54. The Sinclair scale, which grades from 1 to 5, was used to assess the severity of hair loss in these patients.
Five female patients had bitemporal recession or balding of the crown in a male pattern hair loss (MPHL) distribution, and the one male patient had extensive baldness resembling Hamilton-Norwood type VII.
The vast majority of patients who had trichoscopy performed – 88% – had trichoscopic features that were “indistinguishable from those of androgenetic alopecia,” most commonly hair shaft diameter variability, increased vellus hairs, and predominant single-hair follicular units, the authors reported.
Of the 18 patients who had biopsies, 14 had androgenetic alopecia-like features with decreased terminal hairs, increased vellus hairs, and fibrous streamers. The reduced terminal-to-vellus ratio characterizes hair follicle miniaturization, a hallmark of androgenetic alopecia, they said. (Two patients had cicatricial alopecia, and two had features of both.)
“The predominant phenotypes of pCIA show prominent vellus hairs both clinically and histologically, suggesting that terminal hair follicles undergo miniaturization,” Dr. Bhoyrul and coauthors wrote. Among the 49 patients who completed 6 months or more of treatment, the median Sinclair grade improved from 4 to 3 in 21 patients who received topical minoxidil for a median duration of 17 months; from 4 to 2.5 in 18 patients who received LDOM for a median duration of 29 months; and from 5 to 3 in 10 patients who received LDOM combined with an antiandrogen, such as spironolactone, for a median of 33 months.
Almost three-quarters of the patients in the series received adjuvant hormone therapy, which is independently associated with hair loss, the authors noted. However, there was no statistically significant difference in the pattern or severity of alopecia between patients who were treated with endocrine therapy and those who weren’t.
Asked to comment on the study and on the care of patients with pCIA, Maria K. Hordinsky, MD, professor and chair of dermatology at the University of Minnesota, Minneapolis, and an expert in hair diseases, said the case series points to the value of biopsies in patients with pCIA.
“Some patients really do have a loss of hair follicles,” she said. “But if you do a biopsy and see this miniaturization of the hair follicles, then we have tools to stimulate the hair follicles to become more normal. ... These patients can be successfully treated.”
For patients who do not want to do a biopsy, a therapeutic trial is acceptable. “But knowing helps set expectations for people,” she said. “If the follicles are really small, it will take months [of therapy].”
In addition to topical minoxidil, which she said “is always a good tool,” and LDOM, which is “becoming very popular,” Dr. Hordinsky has used low-level laser light successfully. She cautioned against the use of spironolactone and other hair-growth promoting therapies with potentially significant hormonal impacts unless there is discussion between the dermatologist, oncologist, and patient.
The authors of the case series called in their conclusion for wider use of hair-protective strategies such as scalp hypothermia. But Dr. Hordinsky said that, in the United States, there are divergent opinions among oncologists and among cancer centers on the use of scalp cooling and whether or not it might lessen response to chemotherapy.
More research is needed, she noted, on chemotherapy-induced hair loss in patients of different races and ethnicities. Of the 100 patients in the case series, 91 were European; others were Afro Caribbean, Middle Eastern, and South Asian.
Dr. Bhoyrul is supported by the Geoffrey Dowling Fellowship from the British Association of Dermatologists. One coauthor disclosed serving as a principal investigator and/or scientific board member for various pharmaceutical companies, outside of the submitted study. There were no other disclosures reported. Dr. Hordinsky, the immediate past president of the American Hair Research Society and a section editor for hair diseases in UpToDate, had no relevant disclosures.
and treatment with minoxidil (sometimes with antiandrogen therapy) was associated with improved hair density, according to a recently published retrospective case series.
“An improvement in hair density was observed in most of the patients treated with topical minoxidil or LDOM [low-dose oral minoxidil], with a more favorable outcome seen with LDOM with or without antiandrogens,” reported Bevin Bhoyrul, MBBS, of Sinclair Dermatology in Melbourne and coauthors from the United Kingdom and Germany.
The findings, published in JAMA Dermatology, suggest that pCIA “may be at least partly reversible,” they wrote.
The investigators analyzed the clinicopathologic characteristics of pCIA in 100 patients presenting to the hair clinics, as well as the results of trichoscopy performed in 90 of the patients and biopsies in 18. The researchers also assessed the effectiveness of treatment in 49 of these patients who met their criteria of completing at least 6 months of therapy with minoxidil.
Almost all patients in their series – 92% – were treated with taxanes and had more severe alopecia than those who weren’t exposed to taxanes (a median Sinclair scale grade of 4 vs. 2). Defined as absent or incomplete hair regrowth 6 months or more after completion of chemotherapy, pCIA has been increasingly reported in the literature, the authors note.
Of the 100 patients, all but one of whom were women, 39 had globally-reduced hair density that also involved the occipital area (diffuse alopecia), and 55 patients had thinning of the centroparietal scalp hair in a female pattern hair loss (FPHL) distribution. Patients presented between November 2011 and February 2020 and had a mean age of 54. The Sinclair scale, which grades from 1 to 5, was used to assess the severity of hair loss in these patients.
Five female patients had bitemporal recession or balding of the crown in a male pattern hair loss (MPHL) distribution, and the one male patient had extensive baldness resembling Hamilton-Norwood type VII.
The vast majority of patients who had trichoscopy performed – 88% – had trichoscopic features that were “indistinguishable from those of androgenetic alopecia,” most commonly hair shaft diameter variability, increased vellus hairs, and predominant single-hair follicular units, the authors reported.
Of the 18 patients who had biopsies, 14 had androgenetic alopecia-like features with decreased terminal hairs, increased vellus hairs, and fibrous streamers. The reduced terminal-to-vellus ratio characterizes hair follicle miniaturization, a hallmark of androgenetic alopecia, they said. (Two patients had cicatricial alopecia, and two had features of both.)
“The predominant phenotypes of pCIA show prominent vellus hairs both clinically and histologically, suggesting that terminal hair follicles undergo miniaturization,” Dr. Bhoyrul and coauthors wrote. Among the 49 patients who completed 6 months or more of treatment, the median Sinclair grade improved from 4 to 3 in 21 patients who received topical minoxidil for a median duration of 17 months; from 4 to 2.5 in 18 patients who received LDOM for a median duration of 29 months; and from 5 to 3 in 10 patients who received LDOM combined with an antiandrogen, such as spironolactone, for a median of 33 months.
Almost three-quarters of the patients in the series received adjuvant hormone therapy, which is independently associated with hair loss, the authors noted. However, there was no statistically significant difference in the pattern or severity of alopecia between patients who were treated with endocrine therapy and those who weren’t.
Asked to comment on the study and on the care of patients with pCIA, Maria K. Hordinsky, MD, professor and chair of dermatology at the University of Minnesota, Minneapolis, and an expert in hair diseases, said the case series points to the value of biopsies in patients with pCIA.
“Some patients really do have a loss of hair follicles,” she said. “But if you do a biopsy and see this miniaturization of the hair follicles, then we have tools to stimulate the hair follicles to become more normal. ... These patients can be successfully treated.”
For patients who do not want to do a biopsy, a therapeutic trial is acceptable. “But knowing helps set expectations for people,” she said. “If the follicles are really small, it will take months [of therapy].”
In addition to topical minoxidil, which she said “is always a good tool,” and LDOM, which is “becoming very popular,” Dr. Hordinsky has used low-level laser light successfully. She cautioned against the use of spironolactone and other hair-growth promoting therapies with potentially significant hormonal impacts unless there is discussion between the dermatologist, oncologist, and patient.
The authors of the case series called in their conclusion for wider use of hair-protective strategies such as scalp hypothermia. But Dr. Hordinsky said that, in the United States, there are divergent opinions among oncologists and among cancer centers on the use of scalp cooling and whether or not it might lessen response to chemotherapy.
More research is needed, she noted, on chemotherapy-induced hair loss in patients of different races and ethnicities. Of the 100 patients in the case series, 91 were European; others were Afro Caribbean, Middle Eastern, and South Asian.
Dr. Bhoyrul is supported by the Geoffrey Dowling Fellowship from the British Association of Dermatologists. One coauthor disclosed serving as a principal investigator and/or scientific board member for various pharmaceutical companies, outside of the submitted study. There were no other disclosures reported. Dr. Hordinsky, the immediate past president of the American Hair Research Society and a section editor for hair diseases in UpToDate, had no relevant disclosures.
and treatment with minoxidil (sometimes with antiandrogen therapy) was associated with improved hair density, according to a recently published retrospective case series.
“An improvement in hair density was observed in most of the patients treated with topical minoxidil or LDOM [low-dose oral minoxidil], with a more favorable outcome seen with LDOM with or without antiandrogens,” reported Bevin Bhoyrul, MBBS, of Sinclair Dermatology in Melbourne and coauthors from the United Kingdom and Germany.
The findings, published in JAMA Dermatology, suggest that pCIA “may be at least partly reversible,” they wrote.
The investigators analyzed the clinicopathologic characteristics of pCIA in 100 patients presenting to the hair clinics, as well as the results of trichoscopy performed in 90 of the patients and biopsies in 18. The researchers also assessed the effectiveness of treatment in 49 of these patients who met their criteria of completing at least 6 months of therapy with minoxidil.
Almost all patients in their series – 92% – were treated with taxanes and had more severe alopecia than those who weren’t exposed to taxanes (a median Sinclair scale grade of 4 vs. 2). Defined as absent or incomplete hair regrowth 6 months or more after completion of chemotherapy, pCIA has been increasingly reported in the literature, the authors note.
Of the 100 patients, all but one of whom were women, 39 had globally-reduced hair density that also involved the occipital area (diffuse alopecia), and 55 patients had thinning of the centroparietal scalp hair in a female pattern hair loss (FPHL) distribution. Patients presented between November 2011 and February 2020 and had a mean age of 54. The Sinclair scale, which grades from 1 to 5, was used to assess the severity of hair loss in these patients.
Five female patients had bitemporal recession or balding of the crown in a male pattern hair loss (MPHL) distribution, and the one male patient had extensive baldness resembling Hamilton-Norwood type VII.
The vast majority of patients who had trichoscopy performed – 88% – had trichoscopic features that were “indistinguishable from those of androgenetic alopecia,” most commonly hair shaft diameter variability, increased vellus hairs, and predominant single-hair follicular units, the authors reported.
Of the 18 patients who had biopsies, 14 had androgenetic alopecia-like features with decreased terminal hairs, increased vellus hairs, and fibrous streamers. The reduced terminal-to-vellus ratio characterizes hair follicle miniaturization, a hallmark of androgenetic alopecia, they said. (Two patients had cicatricial alopecia, and two had features of both.)
“The predominant phenotypes of pCIA show prominent vellus hairs both clinically and histologically, suggesting that terminal hair follicles undergo miniaturization,” Dr. Bhoyrul and coauthors wrote. Among the 49 patients who completed 6 months or more of treatment, the median Sinclair grade improved from 4 to 3 in 21 patients who received topical minoxidil for a median duration of 17 months; from 4 to 2.5 in 18 patients who received LDOM for a median duration of 29 months; and from 5 to 3 in 10 patients who received LDOM combined with an antiandrogen, such as spironolactone, for a median of 33 months.
Almost three-quarters of the patients in the series received adjuvant hormone therapy, which is independently associated with hair loss, the authors noted. However, there was no statistically significant difference in the pattern or severity of alopecia between patients who were treated with endocrine therapy and those who weren’t.
Asked to comment on the study and on the care of patients with pCIA, Maria K. Hordinsky, MD, professor and chair of dermatology at the University of Minnesota, Minneapolis, and an expert in hair diseases, said the case series points to the value of biopsies in patients with pCIA.
“Some patients really do have a loss of hair follicles,” she said. “But if you do a biopsy and see this miniaturization of the hair follicles, then we have tools to stimulate the hair follicles to become more normal. ... These patients can be successfully treated.”
For patients who do not want to do a biopsy, a therapeutic trial is acceptable. “But knowing helps set expectations for people,” she said. “If the follicles are really small, it will take months [of therapy].”
In addition to topical minoxidil, which she said “is always a good tool,” and LDOM, which is “becoming very popular,” Dr. Hordinsky has used low-level laser light successfully. She cautioned against the use of spironolactone and other hair-growth promoting therapies with potentially significant hormonal impacts unless there is discussion between the dermatologist, oncologist, and patient.
The authors of the case series called in their conclusion for wider use of hair-protective strategies such as scalp hypothermia. But Dr. Hordinsky said that, in the United States, there are divergent opinions among oncologists and among cancer centers on the use of scalp cooling and whether or not it might lessen response to chemotherapy.
More research is needed, she noted, on chemotherapy-induced hair loss in patients of different races and ethnicities. Of the 100 patients in the case series, 91 were European; others were Afro Caribbean, Middle Eastern, and South Asian.
Dr. Bhoyrul is supported by the Geoffrey Dowling Fellowship from the British Association of Dermatologists. One coauthor disclosed serving as a principal investigator and/or scientific board member for various pharmaceutical companies, outside of the submitted study. There were no other disclosures reported. Dr. Hordinsky, the immediate past president of the American Hair Research Society and a section editor for hair diseases in UpToDate, had no relevant disclosures.
FROM JAMA DERMATOLOGY
In and out surgeries become the norm during pandemic
Urologist Ronney Abaza, MD, a robotic surgery specialist in Dublin, Ohio, and colleagues, reviewed robotic surgeries at their hospital during COVID-19 restrictions on surgery in Ohio between March 17 and June 5, 2020, and compared them with robotic procedures before COVID-19 and after restrictions were lifted. They published their results in Urology.
Since 2016, the hospital has offered the option of same-day discharge (SDD) to all robotic urologic surgery patients, regardless of procedure or patient-specific factors.
Among patients who had surgery during COVID-19 restrictions, 98% (87/89 patients) opted for SDD versus 52% in the group having surgery before the restrictions (P < .00001). After the COVID-19 surgery restrictions were lifted, the higher rate of SDD remained at 98%.
“There were no differences in 30-day complications or readmissions between SDD and overnight patients,” the authors write.
The right patient, the right motivation for successful surgery
Brian Lane, MD, PhD, a urologic oncologist with Spectrum Health in Grand Rapids, Michigan, told this news organization that, for nephrectomies, uptake of same-day discharge will continue to be slow.
“You have to have the right patient, the right patient motivation, and the surgery has to go smoothly,” he said. “If you start sending everyone home the same day, you will certainly see readmissions,” he said.
Dr. Lane is part of the Michigan Urologic Surgery Improvement Collaborative and he said the group recently looked at same-day discharge outcomes after robotic prostatectomies with SDD as compared with 1-2 nights in the hospital.
The work has not yet been published but, “There was a slight signal that there were increased readmissions with same-day discharge vs. 0-1 day,” he said.
A paper on outcomes of same-day discharge in total knee arthroplasty in the Journal of Bone & Joint Surgery found a higher risk of perioperative complications “including component failure, surgical site infection, knee stiffness, and deep vein thrombosis.” Researchers compared outcomes between 4,391 patients who underwent outpatient TKA and 128,951 patients who underwent inpatient TKA.
But for other many surgeries, same-day discharge numbers are increasing without worsening outcomes.
A paper in the Journal of Robotic Surgery found that same-day discharge following robotic-assisted endometrial cancer staging is “safe and feasible.”
Stephen Bradley, MD, MPH, with the Minneapolis Heart Institute in Minneapolis, and colleagues write in the Journal of the American College of Cardiology: Cardiovascular Interventions that they found a large increase in the use of same-day discharge after elective percutaneous coronary intervention (PCI) was not associated with worse 30-day mortality rates or readmission.
In that study, 114,461 patients were discharged the same day they underwent PCI. The proportion of patients who had a same-day discharge increased from 4.5% in 2009 to 28.6% in the fourth quarter of 2017.
Risk-adjusted 30-day mortality did not change in that time, while risk-adjusted rehospitalization decreased over time and more quickly when patients had same-day discharge.
Deepak L. Bhatt, MD, MPH, and Jonathan G. Sung, MBCHB, both of Brigham and Women’s Hospital Heart & Vascular Center, Harvard Medical School, Boston, wrote in an accompanying article that, “Advances in the devices and techniques of PCI have improved the safety and efficacy of the procedure. In selected patients, same-day discharge has become possible, and overnight in-hospital observation can be avoided. By reducing unnecessary hospital stays, both patients and hospitals could benefit.”
Evan Garden, a medical student at Icahn School of Medicine at Mount Sinai in New York, presented findings at the American Urological Association 2021 annual meeting that show patients selected for same-day discharge after partial or radical nephrectomy did not have increased rates of postoperative complications or readmissions in the immediate postoperative period, compared with standard discharge of 1-3 days.
Case studies in nephrectomy
While several case studies have looked at the feasibility and safety of performing partial and radical nephrectomy with same-day discharge in select cases, “this topic has not been addressed on a national level,” Mr. Garden said.
Few patients who have partial or radical nephrectomies have same-day discharges. The researchers found that fewer than 1% of patients who have either procedure in the sample studied were discharged the same day.
Researchers used the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database, a nationally representative deidentified database that prospectively tracks patient characteristics and 30-day perioperative outcomes for major inpatient and outpatient surgical procedures at more than 700 hospitals.
They extracted all minimally invasive partial and radical nephrectomies from 2012 to 2019 and refined the cohort to 28,140 patients who were theoretically eligible for same-day discharge: Of those, 237 (0.8%) had SSD, and 27,903 (99.2%) had a standard-length discharge (SLD).
The team found that there were no differences in 30-day complications or readmissions between same-day discharge (Clavien-Dindo [CD] I/II, 4.22%; CD III, 0%; CD IV, 1.27%; readmission, 4.64%); and SLD (CD I/II, 4.11%; CD III, 0.95%; CD IV, 0.79%; readmission, 3.90%; all P > .05).
Controlling for demographic and clinical variables, SDD was not associated with greater risk of 30-day complications or readmissions (CD I/II: odds ratio, 1.08; 95% confidence interval, 0.57-2.048; P = .813; CD IV: OR 1.699; 95% CI, 0.537-5.375; P = .367; readmission: OR, 1.254; 95% CI, 0.681-2.31; P = .467).
Mr. Garden and coauthors report no relevant financial relationships.
Dr. Lane reports no relevant financial relationships.
Urologist Ronney Abaza, MD, a robotic surgery specialist in Dublin, Ohio, and colleagues, reviewed robotic surgeries at their hospital during COVID-19 restrictions on surgery in Ohio between March 17 and June 5, 2020, and compared them with robotic procedures before COVID-19 and after restrictions were lifted. They published their results in Urology.
Since 2016, the hospital has offered the option of same-day discharge (SDD) to all robotic urologic surgery patients, regardless of procedure or patient-specific factors.
Among patients who had surgery during COVID-19 restrictions, 98% (87/89 patients) opted for SDD versus 52% in the group having surgery before the restrictions (P < .00001). After the COVID-19 surgery restrictions were lifted, the higher rate of SDD remained at 98%.
“There were no differences in 30-day complications or readmissions between SDD and overnight patients,” the authors write.
The right patient, the right motivation for successful surgery
Brian Lane, MD, PhD, a urologic oncologist with Spectrum Health in Grand Rapids, Michigan, told this news organization that, for nephrectomies, uptake of same-day discharge will continue to be slow.
“You have to have the right patient, the right patient motivation, and the surgery has to go smoothly,” he said. “If you start sending everyone home the same day, you will certainly see readmissions,” he said.
Dr. Lane is part of the Michigan Urologic Surgery Improvement Collaborative and he said the group recently looked at same-day discharge outcomes after robotic prostatectomies with SDD as compared with 1-2 nights in the hospital.
The work has not yet been published but, “There was a slight signal that there were increased readmissions with same-day discharge vs. 0-1 day,” he said.
A paper on outcomes of same-day discharge in total knee arthroplasty in the Journal of Bone & Joint Surgery found a higher risk of perioperative complications “including component failure, surgical site infection, knee stiffness, and deep vein thrombosis.” Researchers compared outcomes between 4,391 patients who underwent outpatient TKA and 128,951 patients who underwent inpatient TKA.
But for other many surgeries, same-day discharge numbers are increasing without worsening outcomes.
A paper in the Journal of Robotic Surgery found that same-day discharge following robotic-assisted endometrial cancer staging is “safe and feasible.”
Stephen Bradley, MD, MPH, with the Minneapolis Heart Institute in Minneapolis, and colleagues write in the Journal of the American College of Cardiology: Cardiovascular Interventions that they found a large increase in the use of same-day discharge after elective percutaneous coronary intervention (PCI) was not associated with worse 30-day mortality rates or readmission.
In that study, 114,461 patients were discharged the same day they underwent PCI. The proportion of patients who had a same-day discharge increased from 4.5% in 2009 to 28.6% in the fourth quarter of 2017.
Risk-adjusted 30-day mortality did not change in that time, while risk-adjusted rehospitalization decreased over time and more quickly when patients had same-day discharge.
Deepak L. Bhatt, MD, MPH, and Jonathan G. Sung, MBCHB, both of Brigham and Women’s Hospital Heart & Vascular Center, Harvard Medical School, Boston, wrote in an accompanying article that, “Advances in the devices and techniques of PCI have improved the safety and efficacy of the procedure. In selected patients, same-day discharge has become possible, and overnight in-hospital observation can be avoided. By reducing unnecessary hospital stays, both patients and hospitals could benefit.”
Evan Garden, a medical student at Icahn School of Medicine at Mount Sinai in New York, presented findings at the American Urological Association 2021 annual meeting that show patients selected for same-day discharge after partial or radical nephrectomy did not have increased rates of postoperative complications or readmissions in the immediate postoperative period, compared with standard discharge of 1-3 days.
Case studies in nephrectomy
While several case studies have looked at the feasibility and safety of performing partial and radical nephrectomy with same-day discharge in select cases, “this topic has not been addressed on a national level,” Mr. Garden said.
Few patients who have partial or radical nephrectomies have same-day discharges. The researchers found that fewer than 1% of patients who have either procedure in the sample studied were discharged the same day.
Researchers used the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database, a nationally representative deidentified database that prospectively tracks patient characteristics and 30-day perioperative outcomes for major inpatient and outpatient surgical procedures at more than 700 hospitals.
They extracted all minimally invasive partial and radical nephrectomies from 2012 to 2019 and refined the cohort to 28,140 patients who were theoretically eligible for same-day discharge: Of those, 237 (0.8%) had SSD, and 27,903 (99.2%) had a standard-length discharge (SLD).
The team found that there were no differences in 30-day complications or readmissions between same-day discharge (Clavien-Dindo [CD] I/II, 4.22%; CD III, 0%; CD IV, 1.27%; readmission, 4.64%); and SLD (CD I/II, 4.11%; CD III, 0.95%; CD IV, 0.79%; readmission, 3.90%; all P > .05).
Controlling for demographic and clinical variables, SDD was not associated with greater risk of 30-day complications or readmissions (CD I/II: odds ratio, 1.08; 95% confidence interval, 0.57-2.048; P = .813; CD IV: OR 1.699; 95% CI, 0.537-5.375; P = .367; readmission: OR, 1.254; 95% CI, 0.681-2.31; P = .467).
Mr. Garden and coauthors report no relevant financial relationships.
Dr. Lane reports no relevant financial relationships.
Urologist Ronney Abaza, MD, a robotic surgery specialist in Dublin, Ohio, and colleagues, reviewed robotic surgeries at their hospital during COVID-19 restrictions on surgery in Ohio between March 17 and June 5, 2020, and compared them with robotic procedures before COVID-19 and after restrictions were lifted. They published their results in Urology.
Since 2016, the hospital has offered the option of same-day discharge (SDD) to all robotic urologic surgery patients, regardless of procedure or patient-specific factors.
Among patients who had surgery during COVID-19 restrictions, 98% (87/89 patients) opted for SDD versus 52% in the group having surgery before the restrictions (P < .00001). After the COVID-19 surgery restrictions were lifted, the higher rate of SDD remained at 98%.
“There were no differences in 30-day complications or readmissions between SDD and overnight patients,” the authors write.
The right patient, the right motivation for successful surgery
Brian Lane, MD, PhD, a urologic oncologist with Spectrum Health in Grand Rapids, Michigan, told this news organization that, for nephrectomies, uptake of same-day discharge will continue to be slow.
“You have to have the right patient, the right patient motivation, and the surgery has to go smoothly,” he said. “If you start sending everyone home the same day, you will certainly see readmissions,” he said.
Dr. Lane is part of the Michigan Urologic Surgery Improvement Collaborative and he said the group recently looked at same-day discharge outcomes after robotic prostatectomies with SDD as compared with 1-2 nights in the hospital.
The work has not yet been published but, “There was a slight signal that there were increased readmissions with same-day discharge vs. 0-1 day,” he said.
A paper on outcomes of same-day discharge in total knee arthroplasty in the Journal of Bone & Joint Surgery found a higher risk of perioperative complications “including component failure, surgical site infection, knee stiffness, and deep vein thrombosis.” Researchers compared outcomes between 4,391 patients who underwent outpatient TKA and 128,951 patients who underwent inpatient TKA.
But for other many surgeries, same-day discharge numbers are increasing without worsening outcomes.
A paper in the Journal of Robotic Surgery found that same-day discharge following robotic-assisted endometrial cancer staging is “safe and feasible.”
Stephen Bradley, MD, MPH, with the Minneapolis Heart Institute in Minneapolis, and colleagues write in the Journal of the American College of Cardiology: Cardiovascular Interventions that they found a large increase in the use of same-day discharge after elective percutaneous coronary intervention (PCI) was not associated with worse 30-day mortality rates or readmission.
In that study, 114,461 patients were discharged the same day they underwent PCI. The proportion of patients who had a same-day discharge increased from 4.5% in 2009 to 28.6% in the fourth quarter of 2017.
Risk-adjusted 30-day mortality did not change in that time, while risk-adjusted rehospitalization decreased over time and more quickly when patients had same-day discharge.
Deepak L. Bhatt, MD, MPH, and Jonathan G. Sung, MBCHB, both of Brigham and Women’s Hospital Heart & Vascular Center, Harvard Medical School, Boston, wrote in an accompanying article that, “Advances in the devices and techniques of PCI have improved the safety and efficacy of the procedure. In selected patients, same-day discharge has become possible, and overnight in-hospital observation can be avoided. By reducing unnecessary hospital stays, both patients and hospitals could benefit.”
Evan Garden, a medical student at Icahn School of Medicine at Mount Sinai in New York, presented findings at the American Urological Association 2021 annual meeting that show patients selected for same-day discharge after partial or radical nephrectomy did not have increased rates of postoperative complications or readmissions in the immediate postoperative period, compared with standard discharge of 1-3 days.
Case studies in nephrectomy
While several case studies have looked at the feasibility and safety of performing partial and radical nephrectomy with same-day discharge in select cases, “this topic has not been addressed on a national level,” Mr. Garden said.
Few patients who have partial or radical nephrectomies have same-day discharges. The researchers found that fewer than 1% of patients who have either procedure in the sample studied were discharged the same day.
Researchers used the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database, a nationally representative deidentified database that prospectively tracks patient characteristics and 30-day perioperative outcomes for major inpatient and outpatient surgical procedures at more than 700 hospitals.
They extracted all minimally invasive partial and radical nephrectomies from 2012 to 2019 and refined the cohort to 28,140 patients who were theoretically eligible for same-day discharge: Of those, 237 (0.8%) had SSD, and 27,903 (99.2%) had a standard-length discharge (SLD).
The team found that there were no differences in 30-day complications or readmissions between same-day discharge (Clavien-Dindo [CD] I/II, 4.22%; CD III, 0%; CD IV, 1.27%; readmission, 4.64%); and SLD (CD I/II, 4.11%; CD III, 0.95%; CD IV, 0.79%; readmission, 3.90%; all P > .05).
Controlling for demographic and clinical variables, SDD was not associated with greater risk of 30-day complications or readmissions (CD I/II: odds ratio, 1.08; 95% confidence interval, 0.57-2.048; P = .813; CD IV: OR 1.699; 95% CI, 0.537-5.375; P = .367; readmission: OR, 1.254; 95% CI, 0.681-2.31; P = .467).
Mr. Garden and coauthors report no relevant financial relationships.
Dr. Lane reports no relevant financial relationships.
FDA issues stronger safety requirements for breast implants
The Food and Drug Administration on Oct. 27 announced stronger safety requirements for breast implants, restricting sales of implants only to providers and health facilities that review potential risks of the devices with patients before surgery, via a “Patient Decision Checklist.” The agency also placed a boxed warning – the strongest warning that the FDA requires – on all legally marketed breast implants.
“Protecting patients’ health when they are treated with a medical device is our most important priority,” Binita Ashar, MD, director of the Office of Surgical and Infection Control Devices in the FDA’s Center for Devices and Radiological Health, said in a press release. “In recent years, the FDA has sought more ways to increase patients’ access to clear and understandable information about the benefits and risks of breast implants. By strengthening the safety requirements for manufacturers, the FDA is working to close information gaps for anyone who may be considering breast implant surgery.”
This announcement comes 10 years after the FDA issued a comprehensive safety update on silicone gel–filled implants, which reported a possible association between these devices and anaplastic large cell lymphoma (ALCL). The studies reviewed in the 2011 document also noted that a “significant percentage of women who receive silicone gel–filled breast implants experience complications and adverse outcomes,” the most common being repeat operation, implant removal, rupture, or capsular contracture (scar tissue tightening around the implant).
Breast augmentation has been one of the top five cosmetic procedures in the United States since 2006, according to the American Society for Plastic Surgery, with more than 400,000 people getting breast implants in 2019. Nearly 300,000 were for cosmetic reasons, and more than 100,000 were for breast reconstruction after mastectomies.
In 2019, the FDA proposed adding a boxed warning for breast implants, stating that the devices do not last an entire lifetime; that over time the risk for complications increases; and that breast implants have been associated with ALCL, and also may be associated with systemic symptoms such as fatigue, joint pain, and brain fog. The Oct. 27 FDA action now requires that manufacturers update breast implant packaging to include that information in a boxed warning, as well as the following:
- A patient-decision checklist
- Updated silicone gel–filled breast implant rupture screening recommendations
- A device description including materials used in the device
- Patient device ID cards
The updated label changes must be present on manufacturers’ websites in 30 days, the FDA said.
The new requirements have received largely positive reactions from both physicians and patient organizations. In an emailed statement to this news organization, Lynn Jeffers, MD, MBA, the immediate past president of the American Society of Plastic Surgeons, said that “ASPS has always supported patients being fully informed about their choices and the risks, benefits, and alternatives of the options available. “We look forward to our continued collaboration with the FDA on the safety of implants and other devices.”
Maria Gmitro, president and cofounder of the Breast Implant Safety Alliance, an all-volunteer nonprofit based in Charleston, S.C., said that some of the language in the patient checklist could be stronger, especially when referring to breast implant–associated ALCL.
To inform patients of risks more clearly, “it’s the words like ‘associated with’ that we feel need to be stronger” she said in an interview. She also noted that women who already have breast implants may not be aware of these potential complications, which these new FDA requirements do not address.
But overall, the nonprofit was “thrilled” with the announcement, Ms. Gmitro said. “Placing restrictions on breast implants is a really big step, and we applaud the FDA’s efforts. This is information that every patient considering breast implants should know, and we’ve been advocating for better informed consent.”
A version of this article first appeared on Medscape.com.
The Food and Drug Administration on Oct. 27 announced stronger safety requirements for breast implants, restricting sales of implants only to providers and health facilities that review potential risks of the devices with patients before surgery, via a “Patient Decision Checklist.” The agency also placed a boxed warning – the strongest warning that the FDA requires – on all legally marketed breast implants.
“Protecting patients’ health when they are treated with a medical device is our most important priority,” Binita Ashar, MD, director of the Office of Surgical and Infection Control Devices in the FDA’s Center for Devices and Radiological Health, said in a press release. “In recent years, the FDA has sought more ways to increase patients’ access to clear and understandable information about the benefits and risks of breast implants. By strengthening the safety requirements for manufacturers, the FDA is working to close information gaps for anyone who may be considering breast implant surgery.”
This announcement comes 10 years after the FDA issued a comprehensive safety update on silicone gel–filled implants, which reported a possible association between these devices and anaplastic large cell lymphoma (ALCL). The studies reviewed in the 2011 document also noted that a “significant percentage of women who receive silicone gel–filled breast implants experience complications and adverse outcomes,” the most common being repeat operation, implant removal, rupture, or capsular contracture (scar tissue tightening around the implant).
Breast augmentation has been one of the top five cosmetic procedures in the United States since 2006, according to the American Society for Plastic Surgery, with more than 400,000 people getting breast implants in 2019. Nearly 300,000 were for cosmetic reasons, and more than 100,000 were for breast reconstruction after mastectomies.
In 2019, the FDA proposed adding a boxed warning for breast implants, stating that the devices do not last an entire lifetime; that over time the risk for complications increases; and that breast implants have been associated with ALCL, and also may be associated with systemic symptoms such as fatigue, joint pain, and brain fog. The Oct. 27 FDA action now requires that manufacturers update breast implant packaging to include that information in a boxed warning, as well as the following:
- A patient-decision checklist
- Updated silicone gel–filled breast implant rupture screening recommendations
- A device description including materials used in the device
- Patient device ID cards
The updated label changes must be present on manufacturers’ websites in 30 days, the FDA said.
The new requirements have received largely positive reactions from both physicians and patient organizations. In an emailed statement to this news organization, Lynn Jeffers, MD, MBA, the immediate past president of the American Society of Plastic Surgeons, said that “ASPS has always supported patients being fully informed about their choices and the risks, benefits, and alternatives of the options available. “We look forward to our continued collaboration with the FDA on the safety of implants and other devices.”
Maria Gmitro, president and cofounder of the Breast Implant Safety Alliance, an all-volunteer nonprofit based in Charleston, S.C., said that some of the language in the patient checklist could be stronger, especially when referring to breast implant–associated ALCL.
To inform patients of risks more clearly, “it’s the words like ‘associated with’ that we feel need to be stronger” she said in an interview. She also noted that women who already have breast implants may not be aware of these potential complications, which these new FDA requirements do not address.
But overall, the nonprofit was “thrilled” with the announcement, Ms. Gmitro said. “Placing restrictions on breast implants is a really big step, and we applaud the FDA’s efforts. This is information that every patient considering breast implants should know, and we’ve been advocating for better informed consent.”
A version of this article first appeared on Medscape.com.
The Food and Drug Administration on Oct. 27 announced stronger safety requirements for breast implants, restricting sales of implants only to providers and health facilities that review potential risks of the devices with patients before surgery, via a “Patient Decision Checklist.” The agency also placed a boxed warning – the strongest warning that the FDA requires – on all legally marketed breast implants.
“Protecting patients’ health when they are treated with a medical device is our most important priority,” Binita Ashar, MD, director of the Office of Surgical and Infection Control Devices in the FDA’s Center for Devices and Radiological Health, said in a press release. “In recent years, the FDA has sought more ways to increase patients’ access to clear and understandable information about the benefits and risks of breast implants. By strengthening the safety requirements for manufacturers, the FDA is working to close information gaps for anyone who may be considering breast implant surgery.”
This announcement comes 10 years after the FDA issued a comprehensive safety update on silicone gel–filled implants, which reported a possible association between these devices and anaplastic large cell lymphoma (ALCL). The studies reviewed in the 2011 document also noted that a “significant percentage of women who receive silicone gel–filled breast implants experience complications and adverse outcomes,” the most common being repeat operation, implant removal, rupture, or capsular contracture (scar tissue tightening around the implant).
Breast augmentation has been one of the top five cosmetic procedures in the United States since 2006, according to the American Society for Plastic Surgery, with more than 400,000 people getting breast implants in 2019. Nearly 300,000 were for cosmetic reasons, and more than 100,000 were for breast reconstruction after mastectomies.
In 2019, the FDA proposed adding a boxed warning for breast implants, stating that the devices do not last an entire lifetime; that over time the risk for complications increases; and that breast implants have been associated with ALCL, and also may be associated with systemic symptoms such as fatigue, joint pain, and brain fog. The Oct. 27 FDA action now requires that manufacturers update breast implant packaging to include that information in a boxed warning, as well as the following:
- A patient-decision checklist
- Updated silicone gel–filled breast implant rupture screening recommendations
- A device description including materials used in the device
- Patient device ID cards
The updated label changes must be present on manufacturers’ websites in 30 days, the FDA said.
The new requirements have received largely positive reactions from both physicians and patient organizations. In an emailed statement to this news organization, Lynn Jeffers, MD, MBA, the immediate past president of the American Society of Plastic Surgeons, said that “ASPS has always supported patients being fully informed about their choices and the risks, benefits, and alternatives of the options available. “We look forward to our continued collaboration with the FDA on the safety of implants and other devices.”
Maria Gmitro, president and cofounder of the Breast Implant Safety Alliance, an all-volunteer nonprofit based in Charleston, S.C., said that some of the language in the patient checklist could be stronger, especially when referring to breast implant–associated ALCL.
To inform patients of risks more clearly, “it’s the words like ‘associated with’ that we feel need to be stronger” she said in an interview. She also noted that women who already have breast implants may not be aware of these potential complications, which these new FDA requirements do not address.
But overall, the nonprofit was “thrilled” with the announcement, Ms. Gmitro said. “Placing restrictions on breast implants is a really big step, and we applaud the FDA’s efforts. This is information that every patient considering breast implants should know, and we’ve been advocating for better informed consent.”
A version of this article first appeared on Medscape.com.
Antibiotic and glucocorticoid use before cancer therapy could have detrimental effect on outcomes
“Our results confirm the detrimental impact on oncological outcomes of antibiotics and glucocorticoids at a dosage ≥10 mg/day when given within 1 month before or after ICI onset,” Marie Kostine, MD, of Bordeaux (France) University Hospital, and colleagues wrote in the European Journal of Cancer. “Moreover, we show that other comedications may significantly alter the antitumoral response of ICI, such as proton pump inhibitors, psychotropic drugs, morphine, aspirin, and insulin, whereas others seem to have no impact.”
While immune checkpoint inhibitors are transforming the treatment of advanced cancers, gut microbiota composition is an important determinant of response to ICIs. Antibiotic treatments are known to alter the gut microbiota. Other drugs, such as proton pump inhibitors, antidiabetic agents, aspirin, NSAIDs, glucocorticoids, immunomodulators, psychotropic drugs, and analgesics, have been associated with changes in microbiome composition. Since many patients with advanced cancer are exposed to such drugs, this study looked at the possible influence of these comedications on the antitumor effect and safety of ICIs.
The observational study included 635 patients with advanced cancer treated with ICIs between May 2015 and September 2017. Comedications given within 1 month before or 1 month after the first administration of an ICI were reviewed from medical records. Psychotropic drugs, proton pump inhibitors, ACE inhibitors and/or angiotensin II receptor blockers (ARBs), glucocorticoids, antibiotics, statins, and morphine were the most prescribed comedications.
Baseline use of antibiotics, glucocorticoids greater than 10 mg/day, proton pump inhibitors, psychotropic drugs, morphine, and insulin was associated with decreased overall survival and tumor response. However, the coadministration of statins, ACE inhibitors and/or ARBs, NSAIDs, aspirin, and oral diabetes drugs did not impact patient outcomes. Additionally, treatments that altered the response to ICIs were associated with a decreased incidence of immune-related adverse events.
“These results suggest some practical advice in a patient candidate to ICIs,” the authors wrote. “First, antibiotic treatment should be limited to documented infections,” and “withdrawal of proton pump inhibitors and psychotropic drugs should be considered.
“Regarding baseline glucocorticoids use, the cutoff of 10 mg/day should be respected, considering the deleterious effect of higher dosage. Moreover, because of the lack of impact of inhaled or topical glucocorticoids, local routes should be preferred,” the authors wrote. “Conversely, our study brings reassuring data regarding the use of glucocorticoids for the management of immune-related adverse events, which did not alter ICI efficacy, confirming previous reports.”
The authors noted that the observational nature of the study does not allow any causal conclusion, adding that it remains unknown whether the effect of comedications “on cancer outcomes is thoroughly mediated by changes in microbiota or other immunomodulatory properties.”
Along with the retrospective design, study limitations included reporting bias and missing data on baseline comedications, specific prognostic factors and cancer outcomes.
The authors noted no conflicts of interest.
“Our results confirm the detrimental impact on oncological outcomes of antibiotics and glucocorticoids at a dosage ≥10 mg/day when given within 1 month before or after ICI onset,” Marie Kostine, MD, of Bordeaux (France) University Hospital, and colleagues wrote in the European Journal of Cancer. “Moreover, we show that other comedications may significantly alter the antitumoral response of ICI, such as proton pump inhibitors, psychotropic drugs, morphine, aspirin, and insulin, whereas others seem to have no impact.”
While immune checkpoint inhibitors are transforming the treatment of advanced cancers, gut microbiota composition is an important determinant of response to ICIs. Antibiotic treatments are known to alter the gut microbiota. Other drugs, such as proton pump inhibitors, antidiabetic agents, aspirin, NSAIDs, glucocorticoids, immunomodulators, psychotropic drugs, and analgesics, have been associated with changes in microbiome composition. Since many patients with advanced cancer are exposed to such drugs, this study looked at the possible influence of these comedications on the antitumor effect and safety of ICIs.
The observational study included 635 patients with advanced cancer treated with ICIs between May 2015 and September 2017. Comedications given within 1 month before or 1 month after the first administration of an ICI were reviewed from medical records. Psychotropic drugs, proton pump inhibitors, ACE inhibitors and/or angiotensin II receptor blockers (ARBs), glucocorticoids, antibiotics, statins, and morphine were the most prescribed comedications.
Baseline use of antibiotics, glucocorticoids greater than 10 mg/day, proton pump inhibitors, psychotropic drugs, morphine, and insulin was associated with decreased overall survival and tumor response. However, the coadministration of statins, ACE inhibitors and/or ARBs, NSAIDs, aspirin, and oral diabetes drugs did not impact patient outcomes. Additionally, treatments that altered the response to ICIs were associated with a decreased incidence of immune-related adverse events.
“These results suggest some practical advice in a patient candidate to ICIs,” the authors wrote. “First, antibiotic treatment should be limited to documented infections,” and “withdrawal of proton pump inhibitors and psychotropic drugs should be considered.
“Regarding baseline glucocorticoids use, the cutoff of 10 mg/day should be respected, considering the deleterious effect of higher dosage. Moreover, because of the lack of impact of inhaled or topical glucocorticoids, local routes should be preferred,” the authors wrote. “Conversely, our study brings reassuring data regarding the use of glucocorticoids for the management of immune-related adverse events, which did not alter ICI efficacy, confirming previous reports.”
The authors noted that the observational nature of the study does not allow any causal conclusion, adding that it remains unknown whether the effect of comedications “on cancer outcomes is thoroughly mediated by changes in microbiota or other immunomodulatory properties.”
Along with the retrospective design, study limitations included reporting bias and missing data on baseline comedications, specific prognostic factors and cancer outcomes.
The authors noted no conflicts of interest.
“Our results confirm the detrimental impact on oncological outcomes of antibiotics and glucocorticoids at a dosage ≥10 mg/day when given within 1 month before or after ICI onset,” Marie Kostine, MD, of Bordeaux (France) University Hospital, and colleagues wrote in the European Journal of Cancer. “Moreover, we show that other comedications may significantly alter the antitumoral response of ICI, such as proton pump inhibitors, psychotropic drugs, morphine, aspirin, and insulin, whereas others seem to have no impact.”
While immune checkpoint inhibitors are transforming the treatment of advanced cancers, gut microbiota composition is an important determinant of response to ICIs. Antibiotic treatments are known to alter the gut microbiota. Other drugs, such as proton pump inhibitors, antidiabetic agents, aspirin, NSAIDs, glucocorticoids, immunomodulators, psychotropic drugs, and analgesics, have been associated with changes in microbiome composition. Since many patients with advanced cancer are exposed to such drugs, this study looked at the possible influence of these comedications on the antitumor effect and safety of ICIs.
The observational study included 635 patients with advanced cancer treated with ICIs between May 2015 and September 2017. Comedications given within 1 month before or 1 month after the first administration of an ICI were reviewed from medical records. Psychotropic drugs, proton pump inhibitors, ACE inhibitors and/or angiotensin II receptor blockers (ARBs), glucocorticoids, antibiotics, statins, and morphine were the most prescribed comedications.
Baseline use of antibiotics, glucocorticoids greater than 10 mg/day, proton pump inhibitors, psychotropic drugs, morphine, and insulin was associated with decreased overall survival and tumor response. However, the coadministration of statins, ACE inhibitors and/or ARBs, NSAIDs, aspirin, and oral diabetes drugs did not impact patient outcomes. Additionally, treatments that altered the response to ICIs were associated with a decreased incidence of immune-related adverse events.
“These results suggest some practical advice in a patient candidate to ICIs,” the authors wrote. “First, antibiotic treatment should be limited to documented infections,” and “withdrawal of proton pump inhibitors and psychotropic drugs should be considered.
“Regarding baseline glucocorticoids use, the cutoff of 10 mg/day should be respected, considering the deleterious effect of higher dosage. Moreover, because of the lack of impact of inhaled or topical glucocorticoids, local routes should be preferred,” the authors wrote. “Conversely, our study brings reassuring data regarding the use of glucocorticoids for the management of immune-related adverse events, which did not alter ICI efficacy, confirming previous reports.”
The authors noted that the observational nature of the study does not allow any causal conclusion, adding that it remains unknown whether the effect of comedications “on cancer outcomes is thoroughly mediated by changes in microbiota or other immunomodulatory properties.”
Along with the retrospective design, study limitations included reporting bias and missing data on baseline comedications, specific prognostic factors and cancer outcomes.
The authors noted no conflicts of interest.
FROM THE EUROPEAN JOURNAL OF CANCER
Convenience, not outcomes may drive robot-assisted surgeries
“The problem in minimally invasive surgery, especially in cancer surgery, is that the concept has been flip-flopped,” said Hooman Noorchashm, MD, PhD, a retired cardiothoracic surgeon turned patient advocate. “The main purpose of surgery should be removal of diseased tissue or repair of damaged tissue with adequate safety. The size of the incision on that triage scheme is secondary.”
In 2013, Dr. Noorchashm’s wife, Amy Reed, MD, an anesthesiologist, had a hysterectomy for treatment of severe uterine fibroids. The surgery was performed with a laparoscopic power morcellator, which led to the dissemination of cells from a previously undetected abdominal lesion. She was later diagnosed with stage 4 leiomyosarcoma and died in May 2017.
Dr. Noorchashm said the problem with robotic surgery isn’t the technology itself or how it’s used, but why it’s used in the first place. “Not only was there an extreme level of laxity with respect to the malignant potential of fibroids, but also that the size of the incision supersedes the safety of the procedure.”
The ultimate goal of oncologic surgery is to achieve an en bloc resection with clean surgical margins and removal of the tumor intact, Dr. Noorchashm said. The only scientific way of showing the benefits or therapeutic equivalence of new technology is through noninferiority comparison trials.
Robotic surgery inching toward $14 billion in revenue by 2028
Although robotic surgical technology has been in use since the 1990s, the technology is still considered to be its infancy. The first Food and Drug Administration–approved robotics platform, the da Vinci Surgical System (Intuitive Surgical) was approved by the FDA in 2000. And, now, with its patent expiring in 2022, competitors will be developing and launching new products for abdominal and colorectal surgery, partial knee replacements, cardiovascular procedures, head and neck surgery, and spinal procedures.
Robotic surgery is a rapidly expanding area with new product launches announced daily. In August 2021, the market research firm Grand View Research, reported the surgical robot marketplace is projected to reach $14 billion by 2028, up from $3.6 billion this year.
“This new era of robotic-assisted surgery attracts both surgeons and patients. Robotic surgery has reshaped our surgeries over the last 2 decades, and robots are now used in almost in every surgical field. Still, as surgeons, we continue to look – with great interest – to new robotic companies that may be able to provide better robots in a more cost-effective manner,” wrote urologists Ahmad Almujalhem and Koon Ho Rha in a review published in the journal BJUI Compass.
However, the authors wrote that, although the market is competitive, cost remains an issue, as are competing interests. In addition, many companies are creating replicas of existing technologies instead of focusing on new designs and new technology. “Although the da Vinci system propelled many robots to market, there has been no significant improvement in the console,” they added.
The technology is attractive to both surgeons and patients. “Surgeons are attracted to newer technologies, better vision, and easier learning curves. Patients are also attracted to robotic surgery, as this technology is considered state of the art and is associated with reduced pain and scar size,” the authors wrote.
Outcomes depend on many variables
In terms of outcomes, the literature is mixed. It largely depends on a number of variables from the site of surgery, the type of cancer, technology used, and the surgeon’s skill.
Jung Mogg Kim, MD, PhD, a microbiologist with Hanyang University, Seoul, South Korea, published a systemic review and meta-analysis of 27 clinical reports in PLoS ONE assessing clinical outcomes. They found that robot-assisted laparoscopic surgery did not result in statistically superior outcomes, compared with conventional laparoscopic surgery, except for lower estimated blood loss with robots. Operative time and total complications rates were “significantly more favorable” with conventional laparoscopic procedures.
Thomas E. Ahlering, MD, a robotic prostatectomy specialist at the University of California, Irvine, explained that the success or failure of robot-assisted surgery can be highly dependent on the body site and tumor type.
“The oncologic outcome, as long as the surgeon is up to speed, is not going to be better, but the goal is to be as good,” he said in an interview.
In most cases, Dr. Ahlering said, the goal of surgery is to remove a viable tumor with clean margins while leaving the organ intact. But in prostate surgery, the goal is to remove the entire organ while trying to preserve urinary continence and sexual function.
“One of the biggest benefits of the robot is that we’re able to use it in a laparoscopic environment meaning that we need a pneumoperitoneum [which] dramatically decreases bleeding. In prostate cancer, the area is so highly vascular that bleeding is a major issue,” he said.
The same benefits of reduced bleeding, improved visualization, and precision are also seen with robotic-assisted surgery for renal cancer, he noted.
He also emphasized that positive surgical margins, while less desirable than complete elimination of malignant cells, is not nearly as dire in prostate cancer as it is in surgery for other malignancies, such as soft-tissue sarcomas.
“The majority of cases are never going to recur, and if they do recur they essentially never lead to metastatic disease to bone, much less to prostate cancer–related death. The only thing they can do is slightly increase the PSA [prostate-specific antigen] recurrence,” he said.
Assuming that outcomes are comparable between an open procedure, conventional laparoscopic procedure, or robot-assisted approach, surgeons “will almost all go for the robot. It’s easier on the surgeon and it’s easier on the system,” Dr. Ahlering said.
In skilled hands for select patients, the use of a carefully researched and well-designed surgical assistive device can result in outcomes that are comparable with those seen in open surgical procedures, with robot-assisted surgery offering the possibility of less perioperative bleeding, lower postoperative morbidity, and faster recovery times.
“In our program we have been using robots to perform robotic radical prostatectomy and nephron-sparing surgery – partial nephrectomy and we’re also using them to perform intracorporeal bowel reconstruction and robotic radical cystectomy,” said Ashutosh Tewari, MD, of the Icahn School of Medicine at Mount Sinai, New York.
Robot-assisted surgery can be used “anywhere where you have to be selective, anywhere where you have to be reconstructive, anywhere where [assisted] vision can help, anywhere where the lack of bleeding will be of help to patients, and anywhere where a smaller incision can achieve the same goals,” Dr. Tewari said in an interview. Dr. Tewari’s Mount Sinai colleagues reported at the 2021 American Urological Association annual meeting, robotic-assisted salvage radical and partial nephrectomies were found to be safe and feasible procedures in patients with metachronous kidney tumors. For patients with early invasive cancer (stage pT1), oncologic outcomes with robotic-assisted partial nephrectomy were similar to those of patients who underwent radical surgery. The authors concluded that salvage robotic-assisted partial nephrectomy “can be considered in this group of patients due to the risk of future recurrences and need to preserve renal function.”
The National Comprehensive Cancer Network guideline for prostate cancer, updated in September 2021, states that “laparoscopic and robot-assisted radical prostatectomy are commonly used and are considered comparable to conventional approaches in experienced hands.”
In 2018, researchers in a multinational comparison trial reported that patients with cervical cancer who were randomly assigned to minimally invasive robot-assisted radical hysterectomy had significantly lower rates of both disease-free survival and overall survival than women randomized to open abdominal radical hysterectomy. The study results were published in the New England Journal of Medicine.
The use of robotically assisted surgical (RAS) devices could possibly create a “shielding layer” between the surgical team and patient reducing the risk of infection, according to Ajmal Zemmar, MD, PhD, FMH, a neurosurgeon with the University of Louisville (Ky.) Dr. Zemmar and colleagues recently published a perspective in Nature Machine Intelligence on trends in the use of surgical robots.
“In the operating theatre, robots can place intravascular lines, intubate the patient and manage the airway. The integration of a robot as a shielding layer, physically separating the health care worker and patient, is a powerful tool to combat the omnipresent fear of pathogen contamination and maintain surgical volumes,” Dr. Zemmar and colleagues wrote.
Surgical vs. clinical outcomes
In July 2021, this news organization reported that clinical trials of RAS for nipple-sparing mastectomy procedures were looking primarily at cosmetic or surgical outcomes and were not collecting cancer outcomes and if they were, it was secondary to cosmetic or surgical outcomes.
The FDA followed up by issuing a safety communication in August warning patients and providers that neither the safety nor efficacy of RAS for use in mastectomy procedures or treatment of breast cancer have been established.
“In addition, the FDA is aware of allegations that clinical studies are being conducted using RAS devices to perform mastectomies for the prevention or treatment of cancer without the FDA oversight required for such significant risk studies,” the communication stated.
Dr. Tewari disclosed relationships with various companies. Dr. Noorchashm had no relevant disclosures. Dr. Ahlering disclosed past funding or other considerations from Intuitive Robotics.
“The problem in minimally invasive surgery, especially in cancer surgery, is that the concept has been flip-flopped,” said Hooman Noorchashm, MD, PhD, a retired cardiothoracic surgeon turned patient advocate. “The main purpose of surgery should be removal of diseased tissue or repair of damaged tissue with adequate safety. The size of the incision on that triage scheme is secondary.”
In 2013, Dr. Noorchashm’s wife, Amy Reed, MD, an anesthesiologist, had a hysterectomy for treatment of severe uterine fibroids. The surgery was performed with a laparoscopic power morcellator, which led to the dissemination of cells from a previously undetected abdominal lesion. She was later diagnosed with stage 4 leiomyosarcoma and died in May 2017.
Dr. Noorchashm said the problem with robotic surgery isn’t the technology itself or how it’s used, but why it’s used in the first place. “Not only was there an extreme level of laxity with respect to the malignant potential of fibroids, but also that the size of the incision supersedes the safety of the procedure.”
The ultimate goal of oncologic surgery is to achieve an en bloc resection with clean surgical margins and removal of the tumor intact, Dr. Noorchashm said. The only scientific way of showing the benefits or therapeutic equivalence of new technology is through noninferiority comparison trials.
Robotic surgery inching toward $14 billion in revenue by 2028
Although robotic surgical technology has been in use since the 1990s, the technology is still considered to be its infancy. The first Food and Drug Administration–approved robotics platform, the da Vinci Surgical System (Intuitive Surgical) was approved by the FDA in 2000. And, now, with its patent expiring in 2022, competitors will be developing and launching new products for abdominal and colorectal surgery, partial knee replacements, cardiovascular procedures, head and neck surgery, and spinal procedures.
Robotic surgery is a rapidly expanding area with new product launches announced daily. In August 2021, the market research firm Grand View Research, reported the surgical robot marketplace is projected to reach $14 billion by 2028, up from $3.6 billion this year.
“This new era of robotic-assisted surgery attracts both surgeons and patients. Robotic surgery has reshaped our surgeries over the last 2 decades, and robots are now used in almost in every surgical field. Still, as surgeons, we continue to look – with great interest – to new robotic companies that may be able to provide better robots in a more cost-effective manner,” wrote urologists Ahmad Almujalhem and Koon Ho Rha in a review published in the journal BJUI Compass.
However, the authors wrote that, although the market is competitive, cost remains an issue, as are competing interests. In addition, many companies are creating replicas of existing technologies instead of focusing on new designs and new technology. “Although the da Vinci system propelled many robots to market, there has been no significant improvement in the console,” they added.
The technology is attractive to both surgeons and patients. “Surgeons are attracted to newer technologies, better vision, and easier learning curves. Patients are also attracted to robotic surgery, as this technology is considered state of the art and is associated with reduced pain and scar size,” the authors wrote.
Outcomes depend on many variables
In terms of outcomes, the literature is mixed. It largely depends on a number of variables from the site of surgery, the type of cancer, technology used, and the surgeon’s skill.
Jung Mogg Kim, MD, PhD, a microbiologist with Hanyang University, Seoul, South Korea, published a systemic review and meta-analysis of 27 clinical reports in PLoS ONE assessing clinical outcomes. They found that robot-assisted laparoscopic surgery did not result in statistically superior outcomes, compared with conventional laparoscopic surgery, except for lower estimated blood loss with robots. Operative time and total complications rates were “significantly more favorable” with conventional laparoscopic procedures.
Thomas E. Ahlering, MD, a robotic prostatectomy specialist at the University of California, Irvine, explained that the success or failure of robot-assisted surgery can be highly dependent on the body site and tumor type.
“The oncologic outcome, as long as the surgeon is up to speed, is not going to be better, but the goal is to be as good,” he said in an interview.
In most cases, Dr. Ahlering said, the goal of surgery is to remove a viable tumor with clean margins while leaving the organ intact. But in prostate surgery, the goal is to remove the entire organ while trying to preserve urinary continence and sexual function.
“One of the biggest benefits of the robot is that we’re able to use it in a laparoscopic environment meaning that we need a pneumoperitoneum [which] dramatically decreases bleeding. In prostate cancer, the area is so highly vascular that bleeding is a major issue,” he said.
The same benefits of reduced bleeding, improved visualization, and precision are also seen with robotic-assisted surgery for renal cancer, he noted.
He also emphasized that positive surgical margins, while less desirable than complete elimination of malignant cells, is not nearly as dire in prostate cancer as it is in surgery for other malignancies, such as soft-tissue sarcomas.
“The majority of cases are never going to recur, and if they do recur they essentially never lead to metastatic disease to bone, much less to prostate cancer–related death. The only thing they can do is slightly increase the PSA [prostate-specific antigen] recurrence,” he said.
Assuming that outcomes are comparable between an open procedure, conventional laparoscopic procedure, or robot-assisted approach, surgeons “will almost all go for the robot. It’s easier on the surgeon and it’s easier on the system,” Dr. Ahlering said.
In skilled hands for select patients, the use of a carefully researched and well-designed surgical assistive device can result in outcomes that are comparable with those seen in open surgical procedures, with robot-assisted surgery offering the possibility of less perioperative bleeding, lower postoperative morbidity, and faster recovery times.
“In our program we have been using robots to perform robotic radical prostatectomy and nephron-sparing surgery – partial nephrectomy and we’re also using them to perform intracorporeal bowel reconstruction and robotic radical cystectomy,” said Ashutosh Tewari, MD, of the Icahn School of Medicine at Mount Sinai, New York.
Robot-assisted surgery can be used “anywhere where you have to be selective, anywhere where you have to be reconstructive, anywhere where [assisted] vision can help, anywhere where the lack of bleeding will be of help to patients, and anywhere where a smaller incision can achieve the same goals,” Dr. Tewari said in an interview. Dr. Tewari’s Mount Sinai colleagues reported at the 2021 American Urological Association annual meeting, robotic-assisted salvage radical and partial nephrectomies were found to be safe and feasible procedures in patients with metachronous kidney tumors. For patients with early invasive cancer (stage pT1), oncologic outcomes with robotic-assisted partial nephrectomy were similar to those of patients who underwent radical surgery. The authors concluded that salvage robotic-assisted partial nephrectomy “can be considered in this group of patients due to the risk of future recurrences and need to preserve renal function.”
The National Comprehensive Cancer Network guideline for prostate cancer, updated in September 2021, states that “laparoscopic and robot-assisted radical prostatectomy are commonly used and are considered comparable to conventional approaches in experienced hands.”
In 2018, researchers in a multinational comparison trial reported that patients with cervical cancer who were randomly assigned to minimally invasive robot-assisted radical hysterectomy had significantly lower rates of both disease-free survival and overall survival than women randomized to open abdominal radical hysterectomy. The study results were published in the New England Journal of Medicine.
The use of robotically assisted surgical (RAS) devices could possibly create a “shielding layer” between the surgical team and patient reducing the risk of infection, according to Ajmal Zemmar, MD, PhD, FMH, a neurosurgeon with the University of Louisville (Ky.) Dr. Zemmar and colleagues recently published a perspective in Nature Machine Intelligence on trends in the use of surgical robots.
“In the operating theatre, robots can place intravascular lines, intubate the patient and manage the airway. The integration of a robot as a shielding layer, physically separating the health care worker and patient, is a powerful tool to combat the omnipresent fear of pathogen contamination and maintain surgical volumes,” Dr. Zemmar and colleagues wrote.
Surgical vs. clinical outcomes
In July 2021, this news organization reported that clinical trials of RAS for nipple-sparing mastectomy procedures were looking primarily at cosmetic or surgical outcomes and were not collecting cancer outcomes and if they were, it was secondary to cosmetic or surgical outcomes.
The FDA followed up by issuing a safety communication in August warning patients and providers that neither the safety nor efficacy of RAS for use in mastectomy procedures or treatment of breast cancer have been established.
“In addition, the FDA is aware of allegations that clinical studies are being conducted using RAS devices to perform mastectomies for the prevention or treatment of cancer without the FDA oversight required for such significant risk studies,” the communication stated.
Dr. Tewari disclosed relationships with various companies. Dr. Noorchashm had no relevant disclosures. Dr. Ahlering disclosed past funding or other considerations from Intuitive Robotics.
“The problem in minimally invasive surgery, especially in cancer surgery, is that the concept has been flip-flopped,” said Hooman Noorchashm, MD, PhD, a retired cardiothoracic surgeon turned patient advocate. “The main purpose of surgery should be removal of diseased tissue or repair of damaged tissue with adequate safety. The size of the incision on that triage scheme is secondary.”
In 2013, Dr. Noorchashm’s wife, Amy Reed, MD, an anesthesiologist, had a hysterectomy for treatment of severe uterine fibroids. The surgery was performed with a laparoscopic power morcellator, which led to the dissemination of cells from a previously undetected abdominal lesion. She was later diagnosed with stage 4 leiomyosarcoma and died in May 2017.
Dr. Noorchashm said the problem with robotic surgery isn’t the technology itself or how it’s used, but why it’s used in the first place. “Not only was there an extreme level of laxity with respect to the malignant potential of fibroids, but also that the size of the incision supersedes the safety of the procedure.”
The ultimate goal of oncologic surgery is to achieve an en bloc resection with clean surgical margins and removal of the tumor intact, Dr. Noorchashm said. The only scientific way of showing the benefits or therapeutic equivalence of new technology is through noninferiority comparison trials.
Robotic surgery inching toward $14 billion in revenue by 2028
Although robotic surgical technology has been in use since the 1990s, the technology is still considered to be its infancy. The first Food and Drug Administration–approved robotics platform, the da Vinci Surgical System (Intuitive Surgical) was approved by the FDA in 2000. And, now, with its patent expiring in 2022, competitors will be developing and launching new products for abdominal and colorectal surgery, partial knee replacements, cardiovascular procedures, head and neck surgery, and spinal procedures.
Robotic surgery is a rapidly expanding area with new product launches announced daily. In August 2021, the market research firm Grand View Research, reported the surgical robot marketplace is projected to reach $14 billion by 2028, up from $3.6 billion this year.
“This new era of robotic-assisted surgery attracts both surgeons and patients. Robotic surgery has reshaped our surgeries over the last 2 decades, and robots are now used in almost in every surgical field. Still, as surgeons, we continue to look – with great interest – to new robotic companies that may be able to provide better robots in a more cost-effective manner,” wrote urologists Ahmad Almujalhem and Koon Ho Rha in a review published in the journal BJUI Compass.
However, the authors wrote that, although the market is competitive, cost remains an issue, as are competing interests. In addition, many companies are creating replicas of existing technologies instead of focusing on new designs and new technology. “Although the da Vinci system propelled many robots to market, there has been no significant improvement in the console,” they added.
The technology is attractive to both surgeons and patients. “Surgeons are attracted to newer technologies, better vision, and easier learning curves. Patients are also attracted to robotic surgery, as this technology is considered state of the art and is associated with reduced pain and scar size,” the authors wrote.
Outcomes depend on many variables
In terms of outcomes, the literature is mixed. It largely depends on a number of variables from the site of surgery, the type of cancer, technology used, and the surgeon’s skill.
Jung Mogg Kim, MD, PhD, a microbiologist with Hanyang University, Seoul, South Korea, published a systemic review and meta-analysis of 27 clinical reports in PLoS ONE assessing clinical outcomes. They found that robot-assisted laparoscopic surgery did not result in statistically superior outcomes, compared with conventional laparoscopic surgery, except for lower estimated blood loss with robots. Operative time and total complications rates were “significantly more favorable” with conventional laparoscopic procedures.
Thomas E. Ahlering, MD, a robotic prostatectomy specialist at the University of California, Irvine, explained that the success or failure of robot-assisted surgery can be highly dependent on the body site and tumor type.
“The oncologic outcome, as long as the surgeon is up to speed, is not going to be better, but the goal is to be as good,” he said in an interview.
In most cases, Dr. Ahlering said, the goal of surgery is to remove a viable tumor with clean margins while leaving the organ intact. But in prostate surgery, the goal is to remove the entire organ while trying to preserve urinary continence and sexual function.
“One of the biggest benefits of the robot is that we’re able to use it in a laparoscopic environment meaning that we need a pneumoperitoneum [which] dramatically decreases bleeding. In prostate cancer, the area is so highly vascular that bleeding is a major issue,” he said.
The same benefits of reduced bleeding, improved visualization, and precision are also seen with robotic-assisted surgery for renal cancer, he noted.
He also emphasized that positive surgical margins, while less desirable than complete elimination of malignant cells, is not nearly as dire in prostate cancer as it is in surgery for other malignancies, such as soft-tissue sarcomas.
“The majority of cases are never going to recur, and if they do recur they essentially never lead to metastatic disease to bone, much less to prostate cancer–related death. The only thing they can do is slightly increase the PSA [prostate-specific antigen] recurrence,” he said.
Assuming that outcomes are comparable between an open procedure, conventional laparoscopic procedure, or robot-assisted approach, surgeons “will almost all go for the robot. It’s easier on the surgeon and it’s easier on the system,” Dr. Ahlering said.
In skilled hands for select patients, the use of a carefully researched and well-designed surgical assistive device can result in outcomes that are comparable with those seen in open surgical procedures, with robot-assisted surgery offering the possibility of less perioperative bleeding, lower postoperative morbidity, and faster recovery times.
“In our program we have been using robots to perform robotic radical prostatectomy and nephron-sparing surgery – partial nephrectomy and we’re also using them to perform intracorporeal bowel reconstruction and robotic radical cystectomy,” said Ashutosh Tewari, MD, of the Icahn School of Medicine at Mount Sinai, New York.
Robot-assisted surgery can be used “anywhere where you have to be selective, anywhere where you have to be reconstructive, anywhere where [assisted] vision can help, anywhere where the lack of bleeding will be of help to patients, and anywhere where a smaller incision can achieve the same goals,” Dr. Tewari said in an interview. Dr. Tewari’s Mount Sinai colleagues reported at the 2021 American Urological Association annual meeting, robotic-assisted salvage radical and partial nephrectomies were found to be safe and feasible procedures in patients with metachronous kidney tumors. For patients with early invasive cancer (stage pT1), oncologic outcomes with robotic-assisted partial nephrectomy were similar to those of patients who underwent radical surgery. The authors concluded that salvage robotic-assisted partial nephrectomy “can be considered in this group of patients due to the risk of future recurrences and need to preserve renal function.”
The National Comprehensive Cancer Network guideline for prostate cancer, updated in September 2021, states that “laparoscopic and robot-assisted radical prostatectomy are commonly used and are considered comparable to conventional approaches in experienced hands.”
In 2018, researchers in a multinational comparison trial reported that patients with cervical cancer who were randomly assigned to minimally invasive robot-assisted radical hysterectomy had significantly lower rates of both disease-free survival and overall survival than women randomized to open abdominal radical hysterectomy. The study results were published in the New England Journal of Medicine.
The use of robotically assisted surgical (RAS) devices could possibly create a “shielding layer” between the surgical team and patient reducing the risk of infection, according to Ajmal Zemmar, MD, PhD, FMH, a neurosurgeon with the University of Louisville (Ky.) Dr. Zemmar and colleagues recently published a perspective in Nature Machine Intelligence on trends in the use of surgical robots.
“In the operating theatre, robots can place intravascular lines, intubate the patient and manage the airway. The integration of a robot as a shielding layer, physically separating the health care worker and patient, is a powerful tool to combat the omnipresent fear of pathogen contamination and maintain surgical volumes,” Dr. Zemmar and colleagues wrote.
Surgical vs. clinical outcomes
In July 2021, this news organization reported that clinical trials of RAS for nipple-sparing mastectomy procedures were looking primarily at cosmetic or surgical outcomes and were not collecting cancer outcomes and if they were, it was secondary to cosmetic or surgical outcomes.
The FDA followed up by issuing a safety communication in August warning patients and providers that neither the safety nor efficacy of RAS for use in mastectomy procedures or treatment of breast cancer have been established.
“In addition, the FDA is aware of allegations that clinical studies are being conducted using RAS devices to perform mastectomies for the prevention or treatment of cancer without the FDA oversight required for such significant risk studies,” the communication stated.
Dr. Tewari disclosed relationships with various companies. Dr. Noorchashm had no relevant disclosures. Dr. Ahlering disclosed past funding or other considerations from Intuitive Robotics.
Does eating nuts lead to better breast cancer outcomes?
In the first study of its kind, , compared with those who said they had not eaten nuts.

There was also an improvement in overall survival, but this was not statistically significant.
The finding comes from a study of more than 3,000 patients conducted in China, published online in the International Journal of Cancer. Patients were queried about nut consumption on only one occasion, 5 years after their breast cancer diagnosis.
The investigators report a dose-response pattern between nut eating and the risk of both breast cancer recurrence and overall mortality, with those consuming the largest amounts having the lowest risks.
“Nuts are important components of healthy diets. Promoting this modifiable lifestyle factor should be emphasized in breast cancer survivor guidelines,” conclude Xiao-Ou Shu, MD, PhD, of Vanderbilt University, Nashville, Tenn., and colleagues in the study.
“The association for disease-free survival is quite strong and robust,” Dr. Shu told this news organization.
However, as with all observational studies, this report shows an association and not causation.
“Based upon this study alone, the evidence is weak,” said Wendy Chen, MD, MPH, a breast oncologist at Dana-Farber Cancer Institute in Boston, who was approached for comment.
The people who consumed nuts generally had more education, higher income, lower body mass index, earlier-stage cancers, and more physically active lives – all factors associated with better breast cancer survival, she observed. “The authors tried to control for these factors,” Dr. Chen acknowledged. But it’s hard to know whether nut consumption was “truly” the difference maker, she said.
Furthermore, the study population is also “a bit unusual” because people had to survive 5 years after diagnosis to be included in the analysis – and thus is not representative of breast cancer survivors, she noted.
Erin Van Blarigan, PhD, an epidemiologist at the University of California, San Francisco, described the overall evidence of the beneficial relationship between nut eating and breast cancer – including this study – as “limited.” She previously led a study that observed benefits of nut intake for patients with colon cancer.
Dr. Van Blarigan also noted that nut intake in this study was “very low” – with the median intake less than one serving per week.
She also offered some general advice about eating nuts.
“Nuts are an energy-dense food, so portion sizes should be kept small,” she said, explaining a portion should be about 1 ounce or 1/4 cup of nuts or 1-2 tablespoons of nut butter.
A little may go a long way, she suggested, as research to date “suggests only small amounts may be needed to gain potential benefits.”
The level of nut consumption was low in the Chinese study population (median = 17.3 grams/week) compared with the 42.5 grams/week recommended by the American Heart Association, the study authors acknowledge.
“Nuts, particularly tree nuts, are expensive in China. Traditionally, nut consumption level has been low among Chinese, particularly in the old generation,” commented Dr. Shu.
Study authors did an adjusted analysis
The new study was conducted among 3,449 participants of the Shanghai Breast Cancer Survival Study.
Nut consumption (including peanuts and tree nuts such as walnuts) was assessed with a food questionnaire at 5 years post-diagnosis.
An analysis was conducted at 10 years post-diagnosis (and 5 years after the diet questionnaire). At this 10-year mark, there were 252 breast cancer-specific deaths. Among 3,274 survivors without previous recurrence at the dietary assessment, 209 went on to develop breast cancer-specific events – either recurrence, metastasis, or breast cancer mortality.
Nut consumers had higher overall survival (93.7% vs. 89%; P = .003) and disease-free survival (94.1% vs. 86.2%; P <.001) rates than nonconsumers.
However, the two groups had many differences, as noted by the authors and outside experts.
The consumers had a younger age at diagnosis, lower BMI, higher total energy intake, higher diet quality score, and higher soy food intake. In addition, nut consumers were more likely to have a higher education, personal income, and physical activity level (≥7.5 metabolic equivalent of task-hour/week) as well as to have received immunotherapy.
So the investigators adjusted for many of those variables and found that nut consumption was associated with significantly better disease-free survival (hazard ratio, 0.52; 95% confidence interval, 0.35-0.75), but a nonsignificantly improved overall survival (HR, 0.90; 95% CI, 0.66-1.23), as noted above.
Analyses by amount of nut intake showed a dose-response relationship for both overall survival (P trend = .022) and disease-free survival (P trend = .003).
The authors say that “there has been no strong evidence to support individual food items in favor of breast cancer survival,” citing a 2018 report entitled “Diet, Nutrition, Physical Activity and Breast Cancer Survivors” from the World Cancer Research Fund/American Institute for Cancer Research.
The new study provides evidence that nuts may be such a food, they say, while also calling for studies to confirm their findings.
Study limitations include that fact that the statuses of recurrence and metastasis were self-reported. Misclassification, particularly regarding the event date, is likely, the team says.
The study authors and Dr. Van Blarigan and Dr. Chen have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In the first study of its kind, , compared with those who said they had not eaten nuts.
There was also an improvement in overall survival, but this was not statistically significant.
The finding comes from a study of more than 3,000 patients conducted in China, published online in the International Journal of Cancer. Patients were queried about nut consumption on only one occasion, 5 years after their breast cancer diagnosis.
The investigators report a dose-response pattern between nut eating and the risk of both breast cancer recurrence and overall mortality, with those consuming the largest amounts having the lowest risks.
“Nuts are important components of healthy diets. Promoting this modifiable lifestyle factor should be emphasized in breast cancer survivor guidelines,” conclude Xiao-Ou Shu, MD, PhD, of Vanderbilt University, Nashville, Tenn., and colleagues in the study.
“The association for disease-free survival is quite strong and robust,” Dr. Shu told this news organization.
However, as with all observational studies, this report shows an association and not causation.
“Based upon this study alone, the evidence is weak,” said Wendy Chen, MD, MPH, a breast oncologist at Dana-Farber Cancer Institute in Boston, who was approached for comment.
The people who consumed nuts generally had more education, higher income, lower body mass index, earlier-stage cancers, and more physically active lives – all factors associated with better breast cancer survival, she observed. “The authors tried to control for these factors,” Dr. Chen acknowledged. But it’s hard to know whether nut consumption was “truly” the difference maker, she said.
Furthermore, the study population is also “a bit unusual” because people had to survive 5 years after diagnosis to be included in the analysis – and thus is not representative of breast cancer survivors, she noted.
Erin Van Blarigan, PhD, an epidemiologist at the University of California, San Francisco, described the overall evidence of the beneficial relationship between nut eating and breast cancer – including this study – as “limited.” She previously led a study that observed benefits of nut intake for patients with colon cancer.
Dr. Van Blarigan also noted that nut intake in this study was “very low” – with the median intake less than one serving per week.
She also offered some general advice about eating nuts.
“Nuts are an energy-dense food, so portion sizes should be kept small,” she said, explaining a portion should be about 1 ounce or 1/4 cup of nuts or 1-2 tablespoons of nut butter.
A little may go a long way, she suggested, as research to date “suggests only small amounts may be needed to gain potential benefits.”
The level of nut consumption was low in the Chinese study population (median = 17.3 grams/week) compared with the 42.5 grams/week recommended by the American Heart Association, the study authors acknowledge.
“Nuts, particularly tree nuts, are expensive in China. Traditionally, nut consumption level has been low among Chinese, particularly in the old generation,” commented Dr. Shu.
Study authors did an adjusted analysis
The new study was conducted among 3,449 participants of the Shanghai Breast Cancer Survival Study.
Nut consumption (including peanuts and tree nuts such as walnuts) was assessed with a food questionnaire at 5 years post-diagnosis.
An analysis was conducted at 10 years post-diagnosis (and 5 years after the diet questionnaire). At this 10-year mark, there were 252 breast cancer-specific deaths. Among 3,274 survivors without previous recurrence at the dietary assessment, 209 went on to develop breast cancer-specific events – either recurrence, metastasis, or breast cancer mortality.
Nut consumers had higher overall survival (93.7% vs. 89%; P = .003) and disease-free survival (94.1% vs. 86.2%; P <.001) rates than nonconsumers.
However, the two groups had many differences, as noted by the authors and outside experts.
The consumers had a younger age at diagnosis, lower BMI, higher total energy intake, higher diet quality score, and higher soy food intake. In addition, nut consumers were more likely to have a higher education, personal income, and physical activity level (≥7.5 metabolic equivalent of task-hour/week) as well as to have received immunotherapy.
So the investigators adjusted for many of those variables and found that nut consumption was associated with significantly better disease-free survival (hazard ratio, 0.52; 95% confidence interval, 0.35-0.75), but a nonsignificantly improved overall survival (HR, 0.90; 95% CI, 0.66-1.23), as noted above.
Analyses by amount of nut intake showed a dose-response relationship for both overall survival (P trend = .022) and disease-free survival (P trend = .003).
The authors say that “there has been no strong evidence to support individual food items in favor of breast cancer survival,” citing a 2018 report entitled “Diet, Nutrition, Physical Activity and Breast Cancer Survivors” from the World Cancer Research Fund/American Institute for Cancer Research.
The new study provides evidence that nuts may be such a food, they say, while also calling for studies to confirm their findings.
Study limitations include that fact that the statuses of recurrence and metastasis were self-reported. Misclassification, particularly regarding the event date, is likely, the team says.
The study authors and Dr. Van Blarigan and Dr. Chen have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In the first study of its kind, , compared with those who said they had not eaten nuts.
There was also an improvement in overall survival, but this was not statistically significant.
The finding comes from a study of more than 3,000 patients conducted in China, published online in the International Journal of Cancer. Patients were queried about nut consumption on only one occasion, 5 years after their breast cancer diagnosis.
The investigators report a dose-response pattern between nut eating and the risk of both breast cancer recurrence and overall mortality, with those consuming the largest amounts having the lowest risks.
“Nuts are important components of healthy diets. Promoting this modifiable lifestyle factor should be emphasized in breast cancer survivor guidelines,” conclude Xiao-Ou Shu, MD, PhD, of Vanderbilt University, Nashville, Tenn., and colleagues in the study.
“The association for disease-free survival is quite strong and robust,” Dr. Shu told this news organization.
However, as with all observational studies, this report shows an association and not causation.
“Based upon this study alone, the evidence is weak,” said Wendy Chen, MD, MPH, a breast oncologist at Dana-Farber Cancer Institute in Boston, who was approached for comment.
The people who consumed nuts generally had more education, higher income, lower body mass index, earlier-stage cancers, and more physically active lives – all factors associated with better breast cancer survival, she observed. “The authors tried to control for these factors,” Dr. Chen acknowledged. But it’s hard to know whether nut consumption was “truly” the difference maker, she said.
Furthermore, the study population is also “a bit unusual” because people had to survive 5 years after diagnosis to be included in the analysis – and thus is not representative of breast cancer survivors, she noted.
Erin Van Blarigan, PhD, an epidemiologist at the University of California, San Francisco, described the overall evidence of the beneficial relationship between nut eating and breast cancer – including this study – as “limited.” She previously led a study that observed benefits of nut intake for patients with colon cancer.
Dr. Van Blarigan also noted that nut intake in this study was “very low” – with the median intake less than one serving per week.
She also offered some general advice about eating nuts.
“Nuts are an energy-dense food, so portion sizes should be kept small,” she said, explaining a portion should be about 1 ounce or 1/4 cup of nuts or 1-2 tablespoons of nut butter.
A little may go a long way, she suggested, as research to date “suggests only small amounts may be needed to gain potential benefits.”
The level of nut consumption was low in the Chinese study population (median = 17.3 grams/week) compared with the 42.5 grams/week recommended by the American Heart Association, the study authors acknowledge.
“Nuts, particularly tree nuts, are expensive in China. Traditionally, nut consumption level has been low among Chinese, particularly in the old generation,” commented Dr. Shu.
Study authors did an adjusted analysis
The new study was conducted among 3,449 participants of the Shanghai Breast Cancer Survival Study.
Nut consumption (including peanuts and tree nuts such as walnuts) was assessed with a food questionnaire at 5 years post-diagnosis.
An analysis was conducted at 10 years post-diagnosis (and 5 years after the diet questionnaire). At this 10-year mark, there were 252 breast cancer-specific deaths. Among 3,274 survivors without previous recurrence at the dietary assessment, 209 went on to develop breast cancer-specific events – either recurrence, metastasis, or breast cancer mortality.
Nut consumers had higher overall survival (93.7% vs. 89%; P = .003) and disease-free survival (94.1% vs. 86.2%; P <.001) rates than nonconsumers.
However, the two groups had many differences, as noted by the authors and outside experts.
The consumers had a younger age at diagnosis, lower BMI, higher total energy intake, higher diet quality score, and higher soy food intake. In addition, nut consumers were more likely to have a higher education, personal income, and physical activity level (≥7.5 metabolic equivalent of task-hour/week) as well as to have received immunotherapy.
So the investigators adjusted for many of those variables and found that nut consumption was associated with significantly better disease-free survival (hazard ratio, 0.52; 95% confidence interval, 0.35-0.75), but a nonsignificantly improved overall survival (HR, 0.90; 95% CI, 0.66-1.23), as noted above.
Analyses by amount of nut intake showed a dose-response relationship for both overall survival (P trend = .022) and disease-free survival (P trend = .003).
The authors say that “there has been no strong evidence to support individual food items in favor of breast cancer survival,” citing a 2018 report entitled “Diet, Nutrition, Physical Activity and Breast Cancer Survivors” from the World Cancer Research Fund/American Institute for Cancer Research.
The new study provides evidence that nuts may be such a food, they say, while also calling for studies to confirm their findings.
Study limitations include that fact that the statuses of recurrence and metastasis were self-reported. Misclassification, particularly regarding the event date, is likely, the team says.
The study authors and Dr. Van Blarigan and Dr. Chen have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Neuroimaging may predict cognitive decline after chemotherapy for breast cancer
“Cognitive decline is frequently observed after chemotherapy,” according to Michiel B. de Ruiter, PhD, a research scientist with the Netherlands Cancer Institute in Amsterdam. He specializes in cognitive neuroscience and was the lead author of a study published online Sept. 30, 2021, in the Journal of Clinical Oncology. Dr. de Ruiter and colleagues found that fractional anisotropy may demonstrate a low brain white-matter reserve which could be a risk factor for cognitive decline after chemotherapy for breast cancer treatment.
Cognitive decline after chemotherapy has been reported in 20%-40% of patients with cancer affecting quality of life and daily living skills. Studies have suggested that genetic makeup, advanced age, fatigue, and premorbid intelligence quotient are risk factors for chemotherapy-associated cognitive decline. Changes in the microstructure of brain white matter, known as brain reserve, have been reported after exposure to chemotherapy, but its link to cognitive decline is understudied. Several studies outside of oncology have used MRI to derive fractional anisotropy as a measure for brain reserve.
In the new JCO study, researchers examined fractional anisotropy, as measured by MRI, before chemotherapy. The analysis included 49 patients who underwent neuropsychological tests before treatment with anthracycline-based chemotherapy, then again at 6 months and 2 years after chemotherapy.
The results were compared with those of patients with breast cancer who did not receive systemic therapy and then with a control group consisting of patients without cancer.
A low fractional anisotropy score suggested cognitive decline more than 3 years after receiving chemotherapy treatment. The finding was independent of age, premorbid intelligence quotient, baseline fatigue and baseline cognitive complaints. And, having low premorbid intelligence quotient was an independent risk factor for chemotherapy-associated cognitive decline, which the authors said is in line with previous findings.
Fractional anisotropy did not predict cognitive decline in patients who did not receive systemic therapy, as well as patients in the control group.
The findings could possibly lead to the development a pretreatment assessment to screen for patients who may at risk for cognitive decline, the authors wrote. “Clinically validated assessments of white-matter reserve as assessed with an MRI scan may be part of a pretreatment screening. This could also aid in early identification of cognitive decline after chemotherapy, allowing targeted and early interventions to improve cognitive problems,” such as psychoeducation and cognitive rehabilitation.
No potential conflicts of interest were reported.
“Cognitive decline is frequently observed after chemotherapy,” according to Michiel B. de Ruiter, PhD, a research scientist with the Netherlands Cancer Institute in Amsterdam. He specializes in cognitive neuroscience and was the lead author of a study published online Sept. 30, 2021, in the Journal of Clinical Oncology. Dr. de Ruiter and colleagues found that fractional anisotropy may demonstrate a low brain white-matter reserve which could be a risk factor for cognitive decline after chemotherapy for breast cancer treatment.
Cognitive decline after chemotherapy has been reported in 20%-40% of patients with cancer affecting quality of life and daily living skills. Studies have suggested that genetic makeup, advanced age, fatigue, and premorbid intelligence quotient are risk factors for chemotherapy-associated cognitive decline. Changes in the microstructure of brain white matter, known as brain reserve, have been reported after exposure to chemotherapy, but its link to cognitive decline is understudied. Several studies outside of oncology have used MRI to derive fractional anisotropy as a measure for brain reserve.
In the new JCO study, researchers examined fractional anisotropy, as measured by MRI, before chemotherapy. The analysis included 49 patients who underwent neuropsychological tests before treatment with anthracycline-based chemotherapy, then again at 6 months and 2 years after chemotherapy.
The results were compared with those of patients with breast cancer who did not receive systemic therapy and then with a control group consisting of patients without cancer.
A low fractional anisotropy score suggested cognitive decline more than 3 years after receiving chemotherapy treatment. The finding was independent of age, premorbid intelligence quotient, baseline fatigue and baseline cognitive complaints. And, having low premorbid intelligence quotient was an independent risk factor for chemotherapy-associated cognitive decline, which the authors said is in line with previous findings.
Fractional anisotropy did not predict cognitive decline in patients who did not receive systemic therapy, as well as patients in the control group.
The findings could possibly lead to the development a pretreatment assessment to screen for patients who may at risk for cognitive decline, the authors wrote. “Clinically validated assessments of white-matter reserve as assessed with an MRI scan may be part of a pretreatment screening. This could also aid in early identification of cognitive decline after chemotherapy, allowing targeted and early interventions to improve cognitive problems,” such as psychoeducation and cognitive rehabilitation.
No potential conflicts of interest were reported.
“Cognitive decline is frequently observed after chemotherapy,” according to Michiel B. de Ruiter, PhD, a research scientist with the Netherlands Cancer Institute in Amsterdam. He specializes in cognitive neuroscience and was the lead author of a study published online Sept. 30, 2021, in the Journal of Clinical Oncology. Dr. de Ruiter and colleagues found that fractional anisotropy may demonstrate a low brain white-matter reserve which could be a risk factor for cognitive decline after chemotherapy for breast cancer treatment.
Cognitive decline after chemotherapy has been reported in 20%-40% of patients with cancer affecting quality of life and daily living skills. Studies have suggested that genetic makeup, advanced age, fatigue, and premorbid intelligence quotient are risk factors for chemotherapy-associated cognitive decline. Changes in the microstructure of brain white matter, known as brain reserve, have been reported after exposure to chemotherapy, but its link to cognitive decline is understudied. Several studies outside of oncology have used MRI to derive fractional anisotropy as a measure for brain reserve.
In the new JCO study, researchers examined fractional anisotropy, as measured by MRI, before chemotherapy. The analysis included 49 patients who underwent neuropsychological tests before treatment with anthracycline-based chemotherapy, then again at 6 months and 2 years after chemotherapy.
The results were compared with those of patients with breast cancer who did not receive systemic therapy and then with a control group consisting of patients without cancer.
A low fractional anisotropy score suggested cognitive decline more than 3 years after receiving chemotherapy treatment. The finding was independent of age, premorbid intelligence quotient, baseline fatigue and baseline cognitive complaints. And, having low premorbid intelligence quotient was an independent risk factor for chemotherapy-associated cognitive decline, which the authors said is in line with previous findings.
Fractional anisotropy did not predict cognitive decline in patients who did not receive systemic therapy, as well as patients in the control group.
The findings could possibly lead to the development a pretreatment assessment to screen for patients who may at risk for cognitive decline, the authors wrote. “Clinically validated assessments of white-matter reserve as assessed with an MRI scan may be part of a pretreatment screening. This could also aid in early identification of cognitive decline after chemotherapy, allowing targeted and early interventions to improve cognitive problems,” such as psychoeducation and cognitive rehabilitation.
No potential conflicts of interest were reported.
FROM THE JOURNAL OF CLINICAL ONCOLOGY